Embed Size (px)
Citation preview
1
Kate O’Mara, DOAOCR Annual ConferenceApril 21, 2015
• None to report
• Review pertinent anatomy
• Discuss typical appearance of injured ligaments & tendons
• Consider commonly associated injuries• Recognize injury patterns
• Normal tendon• Low signal T1 & T2
• Magic angle common
• Trace fluid surrounding
• Tendinosis• Increased diameter
• Increased signal T2
• Occasional thinning/attrition (PT & PB)
• Longitudinal split tears• Discrete linear high T2 signal parallel to tendon fibers
• Transverse tendon rupture• Partial or complete
• Acute
• Focally increased signal• Edema
• Hemorrhage
• Chronic
• Scarring/fibrosis may bridge the gap
• Extent of involvement
• Important for treatment planning
• Length, percentage of cross sectional area involved

2
• Posterior• Achilles• Plantaris
• Medial• Tibialis Posterior• Flexor Digitorum Longus• Flexor Hallucis Longus
• Lateral• Peroneus Brevis• Peroneus Longus
• Anterior• Tibialis Anterior• Extensor Digitorum Longus• Extensor Hallucis Longus
• Largest tendon in body, pathology common
• Gastrocnemius/soleus to midposterior calcaneal tuberosity
• Normal AP diameter 4-7mm, flat or concave (90%)
• No sheath
• Normal tendon has punctate & linear high signal distally (connective tissue & vessels)
• Kager’s fat pad anterior
• Two distal bursae (normally <1mm AP)• Retro-Achilles (superficial)
• Retro-calcaneal
• Action: plantar flexion of ankle, heel inversion (minor contribution)
• Most common location of injury is 2-6cm proximal to insertion (critical zone)• Poor vascularity, slower repair
• Degeneration by 4 main mechanisms• Hypoxic-fibromatosis
• Myxoid
• Lipoid
• Osseous-calcific

3
• Most frequent type seen in tendon rupture
• Relative hypovascularity of critical zone
• Follows multiple symptomatic episodes
• Microtears – not visible on imaging
• MRI• Fusiform thickening
• Loss of normal concave anterior margin
AJR 2013;200: 845-855
• Most common asymptomatic type• Initial presentation is tendon tear
• Mucoid patches & vacuoles intersperse between thinned tendonfibers
• MRI• Mucoid deposits are hyperintense on T1 & PD
• Interrupted irregular increased signal on T2 & STIR
1.JAAOS January 2009vol. 17 no. 1 3-14
JAAOS 2009; 17 (1): 3-14
• Fatty deposits in tendon
• Does not predispose to tear
• Age dependent
• Related to xanthofibromatosis• Nodular thickening
• Low to intermediate signal on all sequences
• enhances
• Patients with familial hyperlipidemia
• Focal/diffuse increased intratendinous signal T1 & T2
• Marked thickening
• Bilateral
• DDx: tendon infiltration related to amyloid & gout

4
FAOJ.org
ISMRM
Amyloid
Achilles thickening & ossification, ossification in Kager’s fat pad and joints
• Dystrophic calcification
• Cortical bone & trabeculae form
• Chronic, repetitive trauma with microtears
• Ballet dancers, runners, jumping athletes
• RA, seronegative arthropathies
• Haglund deformity
• MRI• Tendon thickening at insertion
• Loss of concavity along anterior margin
• Intratendinous increased signal
• Soft tissue edema
• Edema in adjacent calcaneal tuberosity
• Retrocalcaneal bursitis
Summerdoc.blogspot

5
• Men 30-50 years old, leisure athletics involving concentricloading (basketball, tennis)
• Most common at watershed region (critical zone)
• Systemic disease (RA, gout, lupus, DM) & fluoroquinolones
• Interstitial – myxoid degeneration• Longitudinal orientation, surrounding fibers intact• Linear increased T1, PD, T2 signal
radRounds, Cabanillas
• Partial – incomplete interruption of fibers• Torn fibers may partially retract
• Frayed, corkscrew, heterogeneous high signal on fluid sensitive sequences
AJR 2013;200: 845-855.
• Complete tears – high signal, fluid-filled gap• Distracted or overlapping fibers
• Intratendinous & peritendinous edema when acute
• Palpable defect, loss of plantar flexion
• Determines surgical repair of complete & partial tears
• Based on size of gap• Type I: partial tear, 50% or less
• Type II: complete tear, gap <3cm
• Type III: complete tear, gap 3-6cm
• Type IV: complete tear, gap >6cm
• Type I & II: end-to-end anastomosis
• Type III: autogenous tendon graft flap
• Type IV: free tendon graft or synthetic graft

6
AJR 2013;200: 845-855
• Inflammation of connective tissue peritenon that surrounds tendon
• High T2 signal around tendon (mostly posterior)
AJR 2013;200: 845-855
• Inflammation of pre-Achilles (Kager) fat pad
• High T2 signal, edema, irregularity in fat pad along tendon (anterior)
• Superficial posterior muscle compartment
• Tendon courses obliquely between the gastrocnemius and the soleus (S), along deepmedial aspect of Achilles
• Inserts to distal Achilles on medial aspect ofcalcaneal tuberosity
• Action: Minor role in knee flexion and foot plantar flexion
DDx: Partial tear medial head gastrocnemius
• Deep posterior muscle compartment
• Tendon forms lower 1/3 of calf• Passes posterior to medial
malleolus (TDnH) along medialcalcaneus via tarsal tunnel
• Divides into several fascicles• 1° insert: navicular tuberosity• 3 cuneiforms• 2,3,4 metatarsal bases• Cuboid
• Normal diameter 2x flexordigitorum longus tendon
AJR. 2000;175: 627-635.

7
• Action• Strongest invertor of foot
• Maintains longitudinal arch
• Dynamic stabilizer
• Spring ligament is static stabilizer
• Aids in ankle plantar flexion, forefoot adduction
• Black without any internal signalintensity
• Prone to magic angle artifact as it curves around the medialmalleolus
• Small amount of fluid in the synovial sheath of the posterior tibialis tendon is normal• No more than 1-2 mm • Almost never circumferential • No normal sheath around the
distal PTT, fluid observed at the distal 1-2 cm is abnormal and related to the metaplastic synovium
AJR. 2000;175: 627-635
• Abnormal size may be the only indicator of tendon dysfunction
• Normal posterior tibialis tendon is roughly twice the size of the two adjacent tendons (FDL, solid straight arrow)
• PTT should be slightly smaller than the anterior tibialis tendon
• PTT should be slightly smaller than the summated measurements of the peroneusbrevis and peroneus longus tendons (curved arrow)
20-year-old healthy man
AJR. 2000;175: 627-635
T1FS• Stress reaction re accessory navicular (types 2 & 3)• Tendon dysfunction/failure
• Doesn’t typically rupture, but becomes dysfunctional• Associated with stretching of spring ligament
• Progressive, painful flat foot deformity• Hindfoot valgus• Over pronation with collapse of medial longitudinal arch
• Type I tears • Interstitial tearing • Increased size
• Type II tears • Decreased diameter, equal to or less than that of the flexor digitorum longus tendon
• Type III tears • Complete rupture of the tendon
AJR. 2000;175: 627-635
• Axial T2 FS: posteriortibialis tendon withmultifocal speckledinternal signal intensitysurrounded by excessivesynovial fluid (arrow)
AJR. 2000;175: 627-635

8
• Thickening, synovitis, &internal signal intensity(white arrow)• Diameter of the PTT
increased as much as 5 –10x the diameter of the adjacent flexor digitorum longus tendon
• Normal diameter isapproximately 2x that of theflexor digitorum longus tendon
T1
T2FSAJR. 2000;175: 627-635 http://radsource.us/posterior-tibial-tendinopathy
• Abnormally small PTT (white arrow)• equal to or less than that of the flexor
digitorum longus tendon
http://radsource.us/posterior-tibial-tendinopathy
T2FS
http://radsource.us/posterior-tibial-tendinopathy
• nearly fluid-filled posterior tibial tendon sheath (arrow), with onlya few edematous irregulartendon fibers
T2
Enlarged posterior tibialis tendon with linear signal splitting posterior tibialis tendon into fascicles (arrow)
AJR. 2000;175: 627-635 http://radsource.us/posterior-tibial-tendinopathy
Sag T1: loss of fat signal in the sinus tarsi (arrow) in this patient who also had a type I PTT tear at the medial malleolus
• Strong association• Important secondary sign of
tendon disease • Fluid or edema within the
sinus tarsi obliterates the normal fat signal intensitysurrounding the interosseous and cervical ligaments

9
http://radsource.us/posterior-tibial-tendinopathy
Thickening & increased fluid signal intensity within the spring ligament (arrows) consistent with tear is noted in this patient with a proximal PTT tear (not shown)
• Spring ligament abnormalities have high association (92%) with advanced posterior tibial tendon injury
• Spring ligament runs deep to PTT, and contiguous with the deltoid ligament superiorly (Tibiospring ligament)
• 4% of the population• Present in a much higher
percentage of patients with PTT disorders
• PTT inserts onto the accessory navicular
• Accessory navicular or a cornuate navicular is riskfactor for PTT tears• (most people with an accessory
or cornuate navicular will not have a disorder of the posterior tibialis tendon)
30-year-old man at risk for posterior tibialis dysfunction. Axial T2FS: hypertrophy of navicular tubercle (arrow), consistent with cornuate navicular.
AJR. 2000;175: 627-635
• Unfused accessory navicular ossicle (normal variant)• Type 1(os tibiale externum)
• Small, round, completely separate• Not associated with tendon dysfunction
• Type 2• Joined to navicular bone via
synchondrosis or syndesmosis• Tendon inserts on ossicle• Abnormal stress at junction of ossicle and
navicular bone• Type 3 “cornuate navicular”
• Osseous fusion of type 2• Prominent medial tubercle• Tendon inserts more proximally & at
steeper angle
• 28-year-old man at risk for posterior tibialis dysfunction
• Sagittal T2 • Accessory navicular (a)• Normal low signal intensity between
accessory navicular and nativenavicular (curved arrow)
• Straight line (instead of normal smooth curve) that posterior tibialis tendon makes as it extends frommedial malleolus. This abnormality causes focal point of friction at medial malleolus (straight arrow).
• Axial PD • Accessory navicular with low-signal-
intensity synchondrosis (arrow).
AJR. 2000;175: 627-635
AJR. 2000;175: 627-635
• Fluid between navicular and accessory navicular
• Edema in both bones (arrows) representingaltered mechanics
AJR. 2000;175: 627-635

10
• Deep posterior muscle compartment
• Passes post to medial malleolusbetween PT and FHL
• Crosses FHL at master knot of Henry
• Tendon divides into 4 slips
• Inserts base 2-5 distal phalanges
• Action: flex 2nd – 5th metatarsals &phalanges, ankle, invert foot
• FDL tendon crossessuperficially over the FHLin the plantar midfoot atthe knot of Henry• Usually located near
navicular and medialcuneiform
• Fibrous slip connects the FHL and FDL at the knot of Henry
• Tendon sheaths of the FHL and FDL usually communicate
• allows inflammation of onestructure to spread to the adjacent tendon
http://radsource.us/tendon-intersection-syndromes
• Deep posterior muscle compartment
• Passes through fibro-osseous tunnel between medial and lateral tubercles of posterior process of talus
• Along medial malleolus and tarsal tunnel
• Below sustentaculum tali
• Crosses FDL at master knot of Henry
• Inserts distal phalanx great toe
• Predisposed to tendinosis, tenosynovitis, partial & completetears (overuse related)
• Action: plantar flex great toe IP & MTP, ankle

11
• Common in ballet dancers
• Constant repetitive plantar flexion(overuse injury)
• Tendinosis & tenosynovitis
• “Trigger toe” (stenosing tenosynovitis)• Focal tendon enlargement
• Tendinosis, partial ruptures
• Entrapment in fibro-osseous tunnel along medial calcaneus
• Results in snapping & locking of toe in flexion or extension
www.mdguidelines.comAJR. 2001;176: 1145-1148.
• Originate along posterior fibula
• Posterior to lateral malleolus via common peroneal tunnel• Common synovial sheath
• Brevis anteromedial to longus
• Retromalleolar groove is small sulcus near fibula tip
• Contained in groove by superior peroneal retinaculum
• Retinaculum attaches to calcaneus with calcaneofibular ligament
http://radsource.us/peroneal-tendon-dislocation-and-superior-peroneal-retinaculum-injury
• Pass along lateral calcaneus
• Separated by peroneal tubercle (small bony prominence)• Via 2nd fibro-osseous tunnel
• Covered by inferior peroneal retinaculum
http://uwmsk.org/residentprojects/peronealtendon.html http://radsource.us/peroneal-tendon-dislocation-and-superior-peroneal-retinaculum-injury
• Brevis inserts base of 5th metatarsal• Action: everts and dorsiflexes ankle
• Injury: Distal fibula (forcibly compressed during inversion injury)
• Longus sharp turn under calcaneocuboid joint, inserts base of 1st
metatarsal and medial cuneiform• Action: plantar flex ankle
• Injury: Along peroneal tubercle or at cuboid tunnel
12
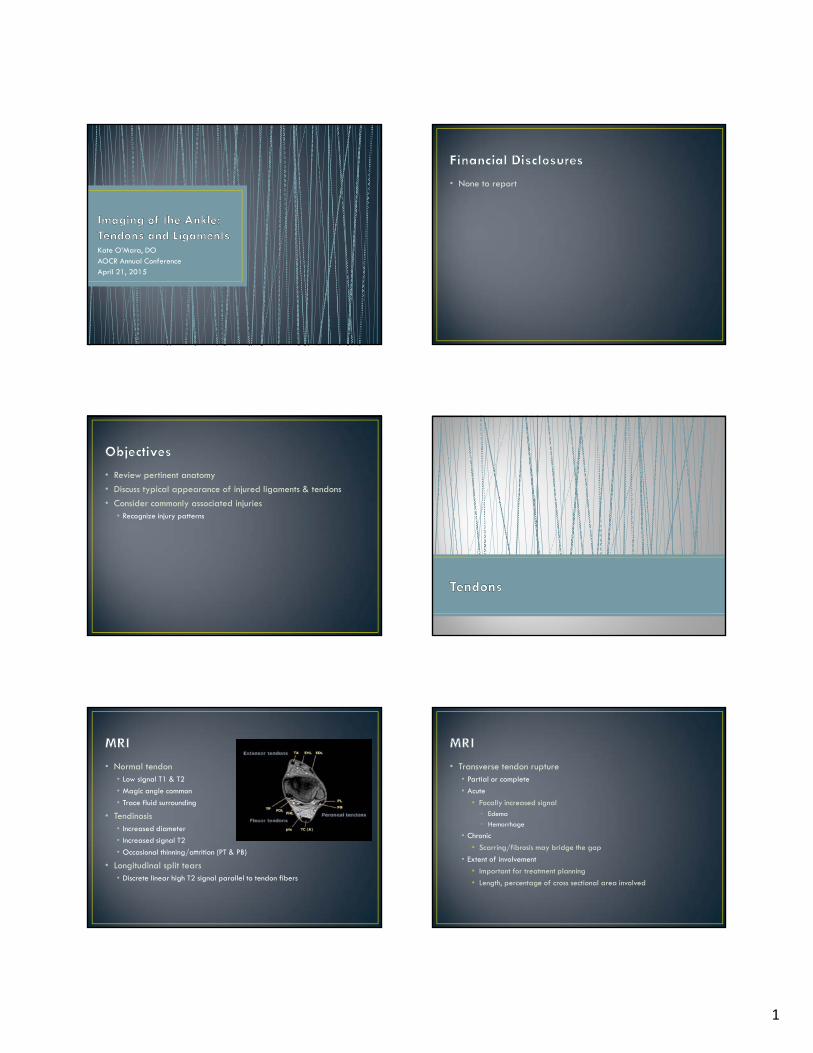
• Tendinopathy associated with lateral ligament injuries
• Injury results in loss of eversion
• Longitudinal split tear of peroneus brevis
• Subluxation/dislocation
• Peroneus brevis may avulse from base of 5th MT
• Large peroneal tubercle with peroneus longus tendinosis
• Os peroneum
• Most common lateral tendon injury
• PB tendon thin, may be separated by anteriorlydisplaced peroneus longus
• Separates brevis & longus
• Enlarged• Longus tendon injury
• Tendon sheath inflammation
radsource.us
13
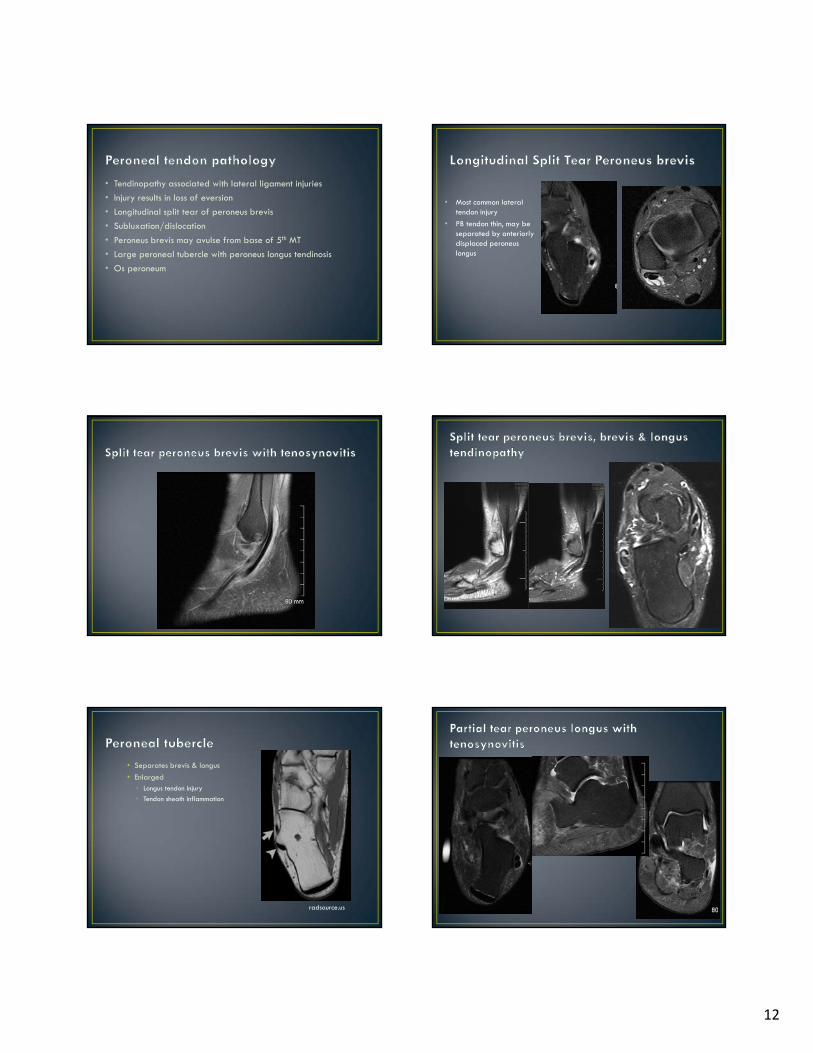
• Peroneus longus dislocated lateral to the fibula• Peroneus brevis remains located• Superior peroneal retinaculum (green arrowheads) is laterally displaced
• Shallow peroneal groove predisposes • Absent retromalleolar groove (20%)
• Lateral calcaneal osseous prominences• Peroneal tubercle (ant) (40%)
• Retrotrochlear eminence (post) (98%)
• Peroneus quartus muscle (20%)
• Os peroneum
• Flat or convexposterodistal fibula
• Predisposes to tendon subluxation
radsource.us

14
• Insertion of peroneus quartus muscle (normal variant)
• Peroneus quartus (PQ) arises from the peroneus brevis muscle (PB) • Courses medial and posterior to
the peroneus longus (PL) and peroneus brevis (PB) muscles and tendons
• Inserts on retroctrochlear eminence of the calcaneus
radsource.us
T1: fleshy accessory peroneus quartus muscle (arrows) coursing posterior to the peroneal longus (PL) and peroneus brevis (PB) tendons and inserting onto the retrotrochlear eminence of the calcaneus (asterisk)
http://radsource.us/accessory-muscles-of-the-ankle
• Sesamoid bone in peroneus longus (at cuboid tunnel)
• Always present but ossified in only 20%
• Mass effect in peroneal groove
• Mimics longitudinal split ofperoneus brevis
Empty sheath
Complete tear distal PL tendon with proximal displacement of os proximal to calcaneocuboid joint (rare)
• Os Peroneum Stress Reaction with associated PL Tendinopathyand tenosynovitis• X-ray: sclerotic or fragmented os

15
• Deep anterior muscle compartment
• Under superior extensor retinaculum at ankle (THnD)
• Under inferior extensor retinaculum
• Inserts medial cuneiform & 1st metatarsalbase
• Action: main dorsiflexor of ankle
• Typically tears completely and retracts• Tender mass above ankle joint
• Elderly patients, minor or no trauma
• Tendinopathy• Extreme focal tendon enlargement
• Courses lateral to tibialis anterior
• Inserts dorsal base 1st distal phalanx
• Action: dorsiflex IP & MTP joints, foot eversion
• Courses lateral to EHL
• Inserts dorsal base 2nd-5th distalphalanges
• Action: dorsiflex IP & MTP joints, foot eversion

16
• Lateral Complex• Anterior talofibular
• Calcaneofibular
• Posterior talofibular
• Medial Complex (Deltoid Ligaments)• Superficial
• Deep
• Syndesmosis• Anterior Inferior Tibiofibular
• Posterior Inferior Tibiofibular
• (Inferior transverse tibiofibular)
• Inferior Interosseous Ligament (membrane)
• Spring (Calcaneonavicular) Ligament Complex• Superomedial Calcaneonavicular Ligament
• Medioplantar Calcaneonavicular Ligament
• Inferoplantar Calcaneonavicular Ligament
• Improves visualization of ankle ligaments• Lateral
• Syndesmotic
• Analyzing soft tissue impingement syndromes
• AMA Classification of Ligamentous Sprain
Grade Ligament Injury
1 Stretched Ligament
2 Partial tear
3 Complete Rupture
Adapted from Rachun A Standard Nomenclature of Athletic Injuries. Chicago, American Medical
Association, 1968.
• Discontinuity/attenuation
• Thickening
• Heterogeneity
• Wavy appearance
• Poorly defined margins
• Periarticular edema
• Fluid in adjacent tendon sheaths and extravasating outside joint capsule
• MRI rarely indicated in acute setting• Injuries initially treated conservatively

17
• Indistinct margins improve• Defect fills with fibrous scar
• Replaced by thickened band inseparable from joint capsule
• Periarticular edema• Up to 6 months
• Lateral sprain is most common ankle injury in athletes
• Mechanism: plantar flexion, inversion, internal rotation
• Associated injuries• Syndesmotic ligaments
• Deltoid ligament
• Sinus tarsi ligaments
• Anterior Talofibular Ligament (ATAF)• Inserts anterior to lateral talar articular
facet
• Weakest, most frequently injured
• Calcaneofibular Ligament (CF)• 2nd most frequently injured
• Peroneal tendons just superficial to CFL
• Posterior Talofibular Ligament (PTAF)
• Usually sequentially injured anterior to posterior
Eorthopod.com
• Weakest of lateral ligaments
• 2/3 of ankle sprains are isolated ATAF injury
• Midsubstance rupture or avulsion
• Anterolateral malleolar tip to talar neck, stabilizing talus
• Well visualized on fluid-sensitive sequences (axial T2)
• Uninjured ligament is of uniform thickness and low T1 and T2 signal intensity (arrow)
AJR. 2009;193: 687-695.
• 17-year-old boy with remote ankle injury
• Thickened ligament • Increased internal signal (arrowhead)
AJR. 2009;193: 687-695.
T2 Axial
• 17-year-old boy with recent injury
• Axial T2-weighted image • Discontinuous ligament • Surrounded by extensive fluid signal
(arrow)
AJR. 2009;193: 687-695.

18
• Meniscoid lesion• Hyalinization of tissue in anterolateral
recess
• Injury of ATAF
• Contributes to anterolateral Impingement
• 19-year-old woman with continued anklepain after sprain
• Nodular soft tissue occupying anterolateral gutter (arrow)
• Torn anterior talofibular ligament, seen in more distal image, is not included
AJR. 2009;193: 687-695.
T2• Usually torn in conjunction with ATAF• Lies deep to peroneal tendons • Extends from lateral malleolar tip to
trochlear eminence, stabilizing subtalarjoint
• Often partially imaged in coronal oraxial planes; multiple images are often needed to visualize its entire course
• Oblique axial proton density–weighted image of intact calcaneofibular ligament(arrow) shows regular contour and homogeneously low signal
AJR. 2009;193: 687-695.
• 24-year-old man with Weber type B fracture of fibula
• Fluid signal in ligament • Mildly irregular contour (arrowhead)
AJR. 2009;193: 687-695.
T2
• 41-year-old woman with ankle trauma
• Discontinuous ligament • Adjacent fluid signal (arrow)• Distal ligament at its calcaneal insertion
(asterisk)• Associated peroneal
tendon/sheath/posterior retinaculum injury
AJR. 2009;193: 687-695.
T2
• Least frequently injured• Extending from posterior talus (lateral
tubercle) to fibular malleolar fossa• Normal posterior talofibular ligament
(arrow) has linear striations (fibrofatty composition)
AJR. 2009;193: 687-695.
Axial PD

19
• 17-year-old boy with recent injury
• Complete tear of posterior talofibularligament: ligament defect
• Torn ends of discontinuous ligament are surrounded by fluid signal (arrow)
AJR. 2009;193: 687-695.
T2
• Triangular fibers with apex at medial malleolus• Deep ligaments
• Deep anterior and posterior tibiotalar ligaments• Talar attachments• Cross one joint
• Superficial ligaments• Tibionavicular, tibiospring, tibiocalcaneal, superficial posterior tibiotalar
ligaments• insert on navicular tuberosity, sustentaculum tali, talus • Cross two joints (ankle joint and talonavicular or subtalar joint)
• Most commonly seen on MRI• Tibiospring (superficial)• Tibionavicular (superficial)• Posterior tibiotalar (deep)
• Primary stabilizer against excessive valgus tilt of the talus
• Injured via eversion or abduction force
• Isolated injuries rare
• Associations• Malleolar fractures
• Lateral ankle sprains
• Syndesmotic diastasis
• Posterior tibial tendon dysfunction
• Widened Medial Clear Space (X-ray)• ≥4mm
• Related to deep deltoid ligament injury
• Acute tear• Fascicular disruption
• Heterogeneity
• Increased signal
• Loss of normal striation (deep)
• Contusion• Increased interstitial signal
• Chronic• Thickening
• Attenuation
Tibionavicular ligament • Inserts onto navicular• Visible on only 55% of MR images of
asymptomatic subjects• unreliable in assessing ligament
injury• Intact tibionavicular ligament (arrow)
AJR. 2009;193: 687-695.
Coronal T2
Tibiospring ligament • Connects medial malleolar colliculus to
superomedial spring ligament• Intact tibiospring ligament with
attachment to spring ligament (arrow)
AJR. 2009;193: 687-695.
Coronal PD

20
• 20-year-old woman with Weber type B fracture
• Coronal T2-weighted image• Complete tear of tibiospring ligament • Discontinuous, irregular fibers (arrow)
AJR. 2009;193: 687-695.
Posterior tibiotalar ligament• Thickest of medial ligaments• Intervening fat separating its
fascicles, resulting in striatedappearance in normal ligament
• Intact posterior tibiotalar ligament • Continuous fibers• Intervening fat between
fascicles (arrow)
AJR. 2009;193: 687-695.
Coronal T2
• Fascicular disruption, irregularity, and lossof striation are indicators of injury
• Partial tear of posterior tibiotalar ligament• Irregular contour• Disrupted fibers with fluid signal near
its talar attachment (arrow)
AJR. 2009;193: 687-695.
Coronal T2
• Complete disruption of posterior tibiotalar ligament
• Irregular contour of visible fibers, none ofwhich appears attached at its talar insertion (arrowhead)
AJR. 2009;193: 687-695.
Coronal T2
• Interosseous Ligament• Thickened distal portion of interosseous membrane
• Syndesmotic recess
• Triangular defect distally
• Normal height 0.5cm on MRI
• Anterior (AITF) & Posterior (PITF) Inferior Tibiofibular Ligaments• Anterior weaker
• Posterior avulsion more common than ligament injury
• Transverse Ligament (Posterior Intermalleolar Ligament)• Lateral malleolus to posterior articular margin of tibia
• Anterior to PITFL

21
• May be isolated
• Associated with• Weber B & C fractures
• Lateral & medial collateral ligament injuries
• High impact activities
• Requires longer recovery time
• Surgery indicated if diastasis
• Wagstaffe fracture• Vertical fibular fracture
• AITF ligament avulsion
• Associated with ankle diastasis & syndesmosis injury
• MRI syndesmotic interruption• Ligament
• Discontinuity
• Contour alterations
• Nonvisualization
• Tibiofibular recess
• Increase in height
• 1.2cm acute tears
• 1.4cm chronic tears
• Extends from anterior tibial tubercle to fibular tubercle
• Best visualized on axial images• Normal AITF ligament may show
fascicular appearance, which should not be confused with injury or tear
• Intact anterior inferior tibiofibular ligament is low in signal intensity (arrow)
AJR. 2009;193: 687-695.
PD
• 19-year-old man with right-ankle pain after injury
• Fluid signal in thickened, irregular ligament (arrowhead)
AJR. 2009;193: 687-695.
T2
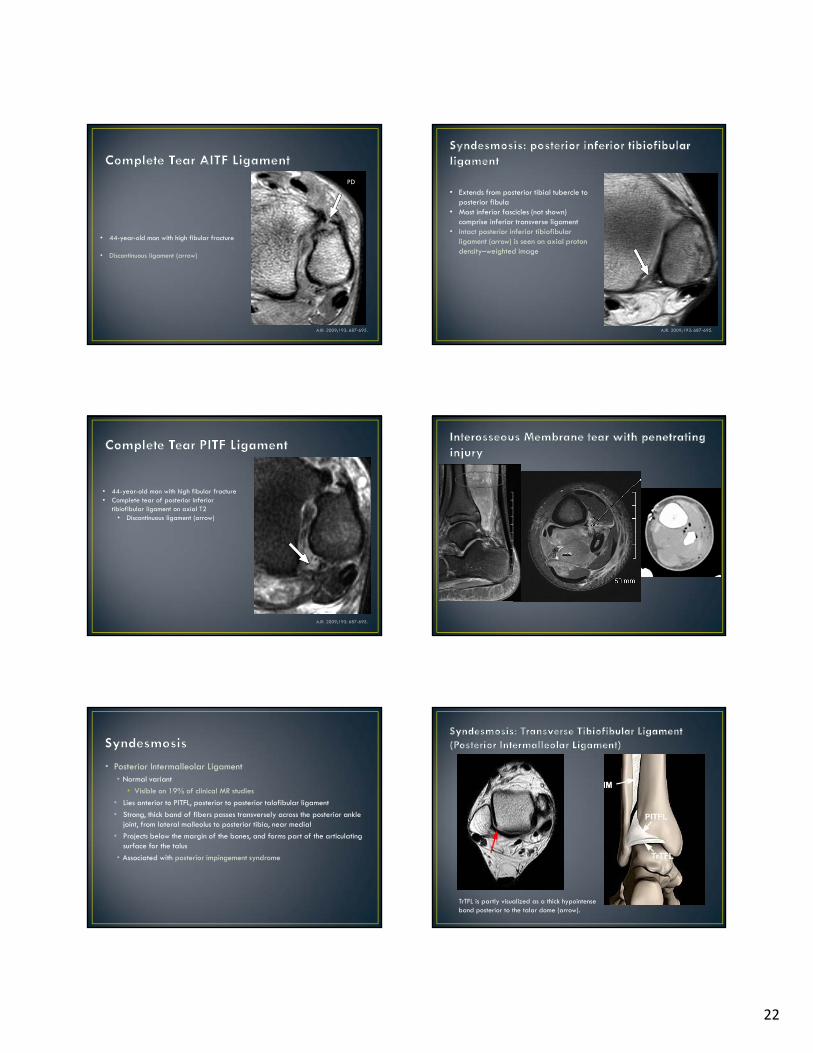
22
• 44-year-old man with high fibular fracture
• Discontinuous ligament (arrow)
AJR. 2009;193: 687-695.
PD
• Extends from posterior tibial tubercle to posterior fibula
• Most inferior fascicles (not shown) comprise inferior transverse ligament
• Intact posterior inferior tibiofibular ligament (arrow) is seen on axial proton density–weighted image
AJR. 2009;193: 687-695.
• 44-year-old man with high fibular fracture• Complete tear of posterior inferior
tibiofibular ligament on axial T2• Discontinuous ligament (arrow)
AJR. 2009;193: 687-695.
• Posterior Intermalleolar Ligament• Normal variant
• Visible on 19% of clinical MR studies
• Lies anterior to PITFL, posterior to posterior talofibular ligament
• Strong, thick band of fibers passes transversely across the posterior anklejoint, from lateral malleolus to posterior tibia, near medial
• Projects below the margin of the bones, and forms part of the articulatingsurface for the talus
• Associated with posterior impingement syndrome
TrTFL is partly visualized as a thick hypointense band posterior to the talar dome (arrow).

23
• Inferior most portion of interosseous membrane
• Connects medial fibula to lateral tibia• Inferior margin lies adjacent to tibiofibular
recess , lined with synovium• Tibiofibular recess extends superiorly 5 mm
from joint line on MR images of healthy subjects
• When fluid signal extends more than 12 mminto tibiofibular recess, syndesmotic injury should be considered
• Intact interosseous ligament or membrane is seen on coronal T2-weighted image. Note absence of fluid in tibiofibular recess (arrows).
AJR. 2009;193: 687-695.
• 44-year-old woman with ankle pain• Coronal T2-weighted image
• Fluid signal extends into tibiotalar recess 13 mm superior to joint line (arrow), indicating high likelihood of interosseous ligament or membrane tear
AJR. 2009;193: 687-695.
• Plantar calcaneonavicular ligament
• Fibrocartilagenous complex • Talar head rests on articular surface
(acetabulum pedis)
• Three components
• Superomedial calcaneonavicular ligament (smCNL)• Most medial, widest, strongest
• Most common tear
• Sustentaculum tali to superomedial navicular
• Medioplantar oblique CNL (mpoCNL)
• Inferoplantar longitudinal CNL (iplCNL)
http://radsource.us/spring-ligament-tear
• Helps stabilize plantar arch (static)• Associated with posterior tibial tendon
dysfunction• Contiguous with deltoid ligament of ankle• Extends from calcaneus to navicular tuberosity
• Superomedial calcaneonavicular (Sp1)• Medioplantar oblique calcaneonavicular
(Sp2)• Inferoplantar longitudinal
calcaneonavicular (Sp3)• Tibiospring ligament (M3) belongs to
superficial layer of medial complex and is included here to show its insertion to superomedial calcaneonavicular ligament.
AJR. 2009;193: 687-695.
• Commonly associated with degenerative flatfoot deformity• PTT dysfunction
• Rheumatoid arthritis
• Diabetic arthropathy
• Isolated injury rare (traumatic)
• Symptoms• Medial/dorsal pain
• Perceived instability
• Acquired progressive planovalgus foot deformity
• Inconsistent visualization
• Subtle signal heterogeneity
• Abnormal caliber• Thickened (5-6.5mm)
• Associated with PTT dysfunction• Disrupted or attenuated ligament
• Markedly pronated talar head

24
• Best seen on coronal ortransverse obliqueimages
• Low signal
• Wraps medially aroundtalar head
• Deep to PTT (blue arrow)
http://radsource.us/spring-ligament-tear
• Striated (interposedfat)
• Obliquely oriented
• Best seen on sagittal,axial, transverseoblique
http://radsource.us/spring-ligament-tear
• Best seen on coronal andsagittal
• Short, intermediatesignal
AJR. 2009;193: 687-695.
• Originates: sustentaculum tali of calcaneus• Inserts: superomedial tarsal navicular• Deep to posterior tibial tendon (PTT)• Superficial surface of superomedial
calcaneonavicular ligament is composed offibrocartilaginous gliding zone
• Most likely to be injured• PTT dysfunction is often associated with
spring ligament injury.• Coronal T2-weighted image shows intact
superomedial calcaneonavicular ligament (straight arrow) and adjacent PTT (curved arrow). Normal tibiospring ligament is also visible (arrowhead). Asterisk indicates fibrocartilaginous gliding zone.
AJR. 2009;193: 687-695.
Axial T2-weighted image shows normal contour and homogeneously low signal in superomedial calcaneonavicular ligament (arrowhead).
AJR. 2009;193: 687-695.
• 50-year-old man with foot and ankle pain• Oblique axial T2-weighted image
• Abnormally thickened, irregular superomedial calcaneonavicular ligament contains bright fluid signal
AJR. 2009;193: 687-695.

25
• Coronal PD fat sat:• Abnormal thickening and increased
signal intensity of the distal posterior tibial tendon (arrow).
• Superomedial portion of the calcaneonavicular (spring) ligament is diffusely thinned and attenuated (arrowheads).
http://radsource.us/spring-ligament-tear
T2-weighted axial oblique:• Thickened posterior tibial tendon with partial
tear along the deep surface (arrow). • Superomedial portion of the
calcaneonavicular (spring) ligament is diffusely thinned (arrowheads) and torn distally at the navicular insertion (small arrow)
http://radsource.us/spring-ligament-tear
• Extends from medial portion of navicularbone to calcaneal coronoid fossa
• Best visualized in axial plane. • Normal striated appearance of uninjured
medioplantar oblique calcaneonavicular ligament is shown on axial T2-weighted image (arrow).
AJR. 2009;193: 687-695.
• 50-year-old man with foot and ankle pain• Axial T2-weighted image
• Irregular, wavy contour of ligament • Interruption at its calcaneal attachment
(arrow)
AJR. 2009;193: 687-695.
• Lies anterior to medioplantar oblique calcaneonavicular ligament
• Extends from inferior navicular bone to calcaneal coronoid fossa
• Thickest of three components of spring ligaments
• Seen in 91% of asymptomatic subjects • Sagittal T1-weighted image shows intact
inferoplantar longitudinal calcaneonavicular ligament (arrow)
AJR. 2009;193: 687-695.

26
• Linear high frequency transducer (8-12MHz)
• Doppler (hyperemia associated with tendinosis & tenosynovitis)
• Normal• Echogenic, fibrillar architecture
• Scant vascularity
• Must orient 90° to tendon axis to avoid anisotropic artifact
• Hypoechoic
• Mimics tendon tears
• Most common as tendons curve around malleoli
Distal Achilles
http://www.ultrasoundcases.info/
Trans peroneus longus & brevis
Long peroneus longusLong Flexor hallucis longus
• Tendinosis• Expansion early
• Loss of normal fibrillar architecture
• Chronic: thinning of tendon
• Partial tear• Focal linear discontinuity of tendon
• Tenosynovitis• Fluid in sheath
• Hyperemia
• Thickened synovium
Rupture of the proximal peroneal retinaculum with instability of the tendons. The peroneal tendons are inhomogeneous and thickened
Healio Orthopedics: July 2010 - Volume 33 · Issue 7: 486-487
http://www.ultrasoundcases.info/
http://www.ultrasoundcases.info/
Full thickness Achilles tendon rupture
Achilles tendon rupture with an organized hematoma in the defect, but there is no continuity of the tendon fibers
http://www.ultrasoundcases.info/
27
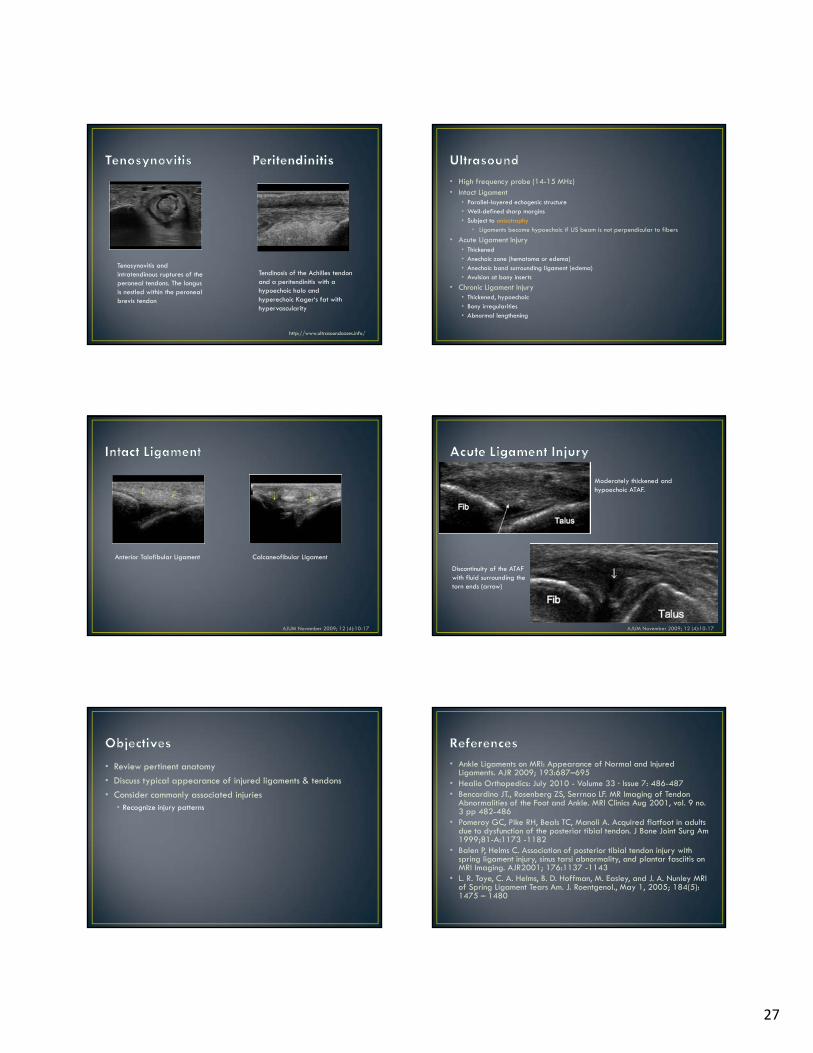
Tenosynovitis and intratendinous ruptures of the peroneal tendons. The longus is nestled within the peroneal brevis tendon
Tendinosis of the Achilles tendon and a peritendinitis with a hypoechoic halo and hyperechoic Kager‘s fat with hypervascularity
http://www.ultrasoundcases.info/
• High frequency probe (14-15 MHz)• Intact Ligament
• Parallel-layered echogenic structure• Well-defined sharp margins• Subject to anisotrophy
• Ligaments become hypoechoic if US beam is not perpendicular to fibers
• Acute Ligament Injury• Thickened• Anechoic zone (hematoma or edema)• Anechoic band surrounding ligament (edema)• Avulsion at bony inserts
• Chronic Ligament Injury• Thickened, hypoechoic• Bony irregularities• Abnormal lengthening
Anterior Talofibular Ligament Calcaneofibular Ligament
AJUM November 2009; 12 (4):10-17
Moderately thickened and hypoechoic ATAF.
Discontinuity of the ATAF with fluid surrounding the torn ends (arrow)
AJUM November 2009; 12 (4):10-17
• Review pertinent anatomy
• Discuss typical appearance of injured ligaments & tendons
• Consider commonly associated injuries• Recognize injury patterns
• Ankle Ligaments on MRI: Appearance of Normal and Injured Ligaments. AJR 2009; 193:687–695
• Healio Orthopedics: July 2010 - Volume 33 · Issue 7: 486-487• Bencardino JT., Rosenberg ZS, Serrnao LF. MR Imaging of Tendon
Abnormalities of the Foot and Ankle. MRI Clinics Aug 2001, vol. 9 no.3 pp 482-486
• Pomeroy GC, Pike RH, Beals TC, Manoli A. Acquired flatfoot in adults due to dysfunction of the posterior tibial tendon. J Bone Joint Surg Am 1999;81-A:1173 -1182
• Balen P, Helms C. Association of posterior tibial tendon injury with spring ligament injury, sinus tarsi abnormality, and plantar fasciitis on MRI Imaging. AJR2001; 176:1137 -1143
• L. R. Toye, C. A. Helms, B. D. Hoffman, M. Easley, and J. A. Nunley MRI of Spring Ligament Tears Am. J. Roentgenol., May 1, 2005; 184(5): 1475 – 1480

28
• MR Imaging of Disorders of the Posterior Tibialis Tendon. AJR. 2000;175: 627-635.
• MR Imaging Findings of Entrapment of the Flexor Hallucis Longus Tendon. AJR. 2001;176: 1145-1148.