Embed Size (px)
Citation preview

Non-operative Management of Neck Pain and Cervical Radiculopathy
What treatment protocol is rational and effective
W Porter McRoberts MD
wwwinternationalhouseofpaincom
bullInterventional physiatrist bullDirector Holy Cross interventional Pain Spine and Neurosurgery bullResearcher Writer Scientist Husband Father bullStudent of the game
Disclosures McRoberts
bull Research ndash St Jude Vertiflex Medtronic Nevro Flowonix
Mesoblast Bioness SPR Sanofi-Aventis Main-Stay Neuros
bull Consulting bull St Jude Vertiflex Medtronic Nevro Flowonix Nalu
Bioness Boston Scientific SPR Guidepoint Gore Industries
bull I have received no financial compensation for any portion of this lecture
bull There will be off label discussion during this talk
Objectives
1 To understand the structures which contribute to both axial neck pain and cervical radicular pain
2 To understand the stepwise approach to evaluation of the above sources of pain
3 To understand the EBM and approaches to treatment of cervical axial and radicular pain
bull The above free of commercial bias
Causes of Pain AXIAL vs RADICULAR
bull Axial Neck Pain
bull High Pain
ndash AA Joint AO Joint
ndash High Cervical Facets(common)
ndash High Cervical Discs(rare)
bull Luschka Joints
ndash OndontoidAlar
ndash Chiari
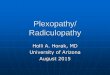
The distribution of pain in normal volunteers after stimulation of the zygapophysial joints indicated (From Cooper G Bailey B Bogduk N Cervical
zygapophysial joint pain maps Pain Med 20078344ndash53)
The distribution of pain relieved in patients with neck pain after anesthetization of the synovial joints indicated using controlled diagnostic blocks The density of shading is proportional to the number of patients whose pain extended into the area indicated (From Cooper G Bailey B Bogduk N Cervical zygapophysial joint
pain maps Pain Med 20078344ndash53)
Causes of Axial Pain
bull Mid and Low Pain
ndash Discs
ndash Facets
ndash Muscle
ndash Ligaments
bull Taxes Exrsquos Hangovers
Causes of Axial neck pain
ndash TON GON LON (C2 Mediated)
ndash MuscleLigament
ndash CSF Leak
ndash CAInfxnFxOther
bull Rare
bull Vertrbral tumors
bull Discitis
bull Septic Arthritis
bull Osteomyleitis
bull Meningitis
bull RAAS CA-GoutFx
Causes of Radicular Pain
bull Radiculopathy is a disease of neural irritation and or compression
bull Disc ProtrusionHerniation Ostophytic compresison
bull Z-Joint OspeophyteGanglionTumorRAGoutASFx
bull V-BodyTumorPagetrsquos Fx Osteomyelitis
bull Meninges CystsMengiomacystsEpidural abcessHematoma
bull Nerve Sheath NeurofibromaSchwannoma
bull Nerve GlioblastomaGanglioneuroma
Epidemiology of Neck Pain
bull 2000-2010 Task Force on Neck Pain and Its Associated Disorders performed a systematic search and critical review of literature published between 1980 and 2006 to assemble the best evidence on neck pain
bull 469 studies 249 to be scientifically admissible bull 101 articles related to the burden and determinants of neck pain in the general
population bull Incidence ranged from 0055 per 1000 person years(disc herniation with
radiculopathy) to bull 213 per 1000 persons (self-reported neck pain) bull Incidence of neck injuries during competitive sports ranged from 002 to 21 per
1000 exposures bull The 12-month prevalence of pain typically ranged between 30 and 50 the 12-
month prevalence of activity-limiting pain was 17 to 115 bull Neck pain was more prevalent among women and prevalence peaked in middle
age bull Risk factors for neck pain included genetics poor psychological health and
exposure to tobacco Disc degeneration was not identified as a risk factor bull The use of sporting gear (helmets face shields) to prevent other types of injury
was not associated with increased neck injuries in bicycling hockey or skiing
European Spine JournalApril 2008 Volume 17 Supplement 1 pp 39-51
Prevalence of Cervical Axial Pain of zygopophyseal origin
bull Prospective study of 318 patients with intractable neck pain
bull Provocation discography Z-Joint blocks
bull Z-joints 38 suffered zygapophyseal pain Aprill C Bogduk N The Prevalence of Cervical Zygapophyseal Joint Pain A First Approximation PhDSpine (Phila Pa 1976) 1992 Jul17(7)744-7
Summary Controlled studies facet or zygapophysial joint pain in 36 to 67 of these patients when disc herniation radiculitis and discogenic are not pathognomic
Falco FJ1 Manchikanti L Datta S Wargo BW Geffert S Bryce DA Atluri S Singh V Benyamin RM Sehgal N Ward SP Helm S 2nd Gupta S Boswell MV Systematic review of the therapeutic effectiveness of cervical facet joint interventions an update Pain Physician 2012 Nov-Dec15(6)E839-68
Diagnosis of Cervical Axial Pain
bull Consecutive patients seen between January 2003 and January 2005 in whom a diagnosis of neck pain was made MBBF-IAI vs Disco vs AAAO
bull Pain Med 2008 Mar9(2)196-203 doi 101111j1526-4637200700369xThe nature of neck pain in a private pain clinic in the United StatesYin W Bogduk N
ZFacet Joint Pain Treatment
bullHaving failed PTother conservative measures bullDiagnostic Medical Branch Block of the Dorsal Primary Ramus ldquoMBB or FJNBrdquo bullDual Block Paradigm
ZFacet Joint Pain Treatment
bull Facet Joint Nerve Ablation
bull FJNA
bull Typically 6-18 months of relief
ZFacet Joint Pain Treatment
bull The median time that elapsed before the pain returned to at least 50 percent of the preoperative level was 263 days in the active-treatment group and 8 days in the control group (P = 004) At 27 weeks seven patients in the active-treatment group and one patient in the control group were free of pain Five patients in the active-treatment group had numbness in the territory of the treated nerves but none considered it troubling
ZFacet Joint Pain Treatment
ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Disclosures McRoberts
bull Research ndash St Jude Vertiflex Medtronic Nevro Flowonix
Mesoblast Bioness SPR Sanofi-Aventis Main-Stay Neuros
bull Consulting bull St Jude Vertiflex Medtronic Nevro Flowonix Nalu
Bioness Boston Scientific SPR Guidepoint Gore Industries
bull I have received no financial compensation for any portion of this lecture
bull There will be off label discussion during this talk
Objectives
1 To understand the structures which contribute to both axial neck pain and cervical radicular pain
2 To understand the stepwise approach to evaluation of the above sources of pain
3 To understand the EBM and approaches to treatment of cervical axial and radicular pain
bull The above free of commercial bias
Causes of Pain AXIAL vs RADICULAR
bull Axial Neck Pain
bull High Pain
ndash AA Joint AO Joint
ndash High Cervical Facets(common)
ndash High Cervical Discs(rare)
bull Luschka Joints
ndash OndontoidAlar
ndash Chiari
The distribution of pain in normal volunteers after stimulation of the zygapophysial joints indicated (From Cooper G Bailey B Bogduk N Cervical
zygapophysial joint pain maps Pain Med 20078344ndash53)
The distribution of pain relieved in patients with neck pain after anesthetization of the synovial joints indicated using controlled diagnostic blocks The density of shading is proportional to the number of patients whose pain extended into the area indicated (From Cooper G Bailey B Bogduk N Cervical zygapophysial joint
pain maps Pain Med 20078344ndash53)
Causes of Axial Pain
bull Mid and Low Pain
ndash Discs
ndash Facets
ndash Muscle
ndash Ligaments
bull Taxes Exrsquos Hangovers
Causes of Axial neck pain
ndash TON GON LON (C2 Mediated)
ndash MuscleLigament
ndash CSF Leak
ndash CAInfxnFxOther
bull Rare
bull Vertrbral tumors
bull Discitis
bull Septic Arthritis
bull Osteomyleitis
bull Meningitis
bull RAAS CA-GoutFx
Causes of Radicular Pain
bull Radiculopathy is a disease of neural irritation and or compression
bull Disc ProtrusionHerniation Ostophytic compresison
bull Z-Joint OspeophyteGanglionTumorRAGoutASFx
bull V-BodyTumorPagetrsquos Fx Osteomyelitis
bull Meninges CystsMengiomacystsEpidural abcessHematoma
bull Nerve Sheath NeurofibromaSchwannoma
bull Nerve GlioblastomaGanglioneuroma
Epidemiology of Neck Pain
bull 2000-2010 Task Force on Neck Pain and Its Associated Disorders performed a systematic search and critical review of literature published between 1980 and 2006 to assemble the best evidence on neck pain
bull 469 studies 249 to be scientifically admissible bull 101 articles related to the burden and determinants of neck pain in the general
population bull Incidence ranged from 0055 per 1000 person years(disc herniation with
radiculopathy) to bull 213 per 1000 persons (self-reported neck pain) bull Incidence of neck injuries during competitive sports ranged from 002 to 21 per
1000 exposures bull The 12-month prevalence of pain typically ranged between 30 and 50 the 12-
month prevalence of activity-limiting pain was 17 to 115 bull Neck pain was more prevalent among women and prevalence peaked in middle
age bull Risk factors for neck pain included genetics poor psychological health and
exposure to tobacco Disc degeneration was not identified as a risk factor bull The use of sporting gear (helmets face shields) to prevent other types of injury
was not associated with increased neck injuries in bicycling hockey or skiing
European Spine JournalApril 2008 Volume 17 Supplement 1 pp 39-51
Prevalence of Cervical Axial Pain of zygopophyseal origin
bull Prospective study of 318 patients with intractable neck pain
bull Provocation discography Z-Joint blocks
bull Z-joints 38 suffered zygapophyseal pain Aprill C Bogduk N The Prevalence of Cervical Zygapophyseal Joint Pain A First Approximation PhDSpine (Phila Pa 1976) 1992 Jul17(7)744-7
Summary Controlled studies facet or zygapophysial joint pain in 36 to 67 of these patients when disc herniation radiculitis and discogenic are not pathognomic
Falco FJ1 Manchikanti L Datta S Wargo BW Geffert S Bryce DA Atluri S Singh V Benyamin RM Sehgal N Ward SP Helm S 2nd Gupta S Boswell MV Systematic review of the therapeutic effectiveness of cervical facet joint interventions an update Pain Physician 2012 Nov-Dec15(6)E839-68
Diagnosis of Cervical Axial Pain
bull Consecutive patients seen between January 2003 and January 2005 in whom a diagnosis of neck pain was made MBBF-IAI vs Disco vs AAAO
bull Pain Med 2008 Mar9(2)196-203 doi 101111j1526-4637200700369xThe nature of neck pain in a private pain clinic in the United StatesYin W Bogduk N
ZFacet Joint Pain Treatment
bullHaving failed PTother conservative measures bullDiagnostic Medical Branch Block of the Dorsal Primary Ramus ldquoMBB or FJNBrdquo bullDual Block Paradigm
ZFacet Joint Pain Treatment
bull Facet Joint Nerve Ablation
bull FJNA
bull Typically 6-18 months of relief
ZFacet Joint Pain Treatment
bull The median time that elapsed before the pain returned to at least 50 percent of the preoperative level was 263 days in the active-treatment group and 8 days in the control group (P = 004) At 27 weeks seven patients in the active-treatment group and one patient in the control group were free of pain Five patients in the active-treatment group had numbness in the territory of the treated nerves but none considered it troubling
ZFacet Joint Pain Treatment
ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Objectives
1 To understand the structures which contribute to both axial neck pain and cervical radicular pain
2 To understand the stepwise approach to evaluation of the above sources of pain
3 To understand the EBM and approaches to treatment of cervical axial and radicular pain
bull The above free of commercial bias
Causes of Pain AXIAL vs RADICULAR
bull Axial Neck Pain
bull High Pain
ndash AA Joint AO Joint
ndash High Cervical Facets(common)
ndash High Cervical Discs(rare)
bull Luschka Joints
ndash OndontoidAlar
ndash Chiari
The distribution of pain in normal volunteers after stimulation of the zygapophysial joints indicated (From Cooper G Bailey B Bogduk N Cervical
zygapophysial joint pain maps Pain Med 20078344ndash53)
The distribution of pain relieved in patients with neck pain after anesthetization of the synovial joints indicated using controlled diagnostic blocks The density of shading is proportional to the number of patients whose pain extended into the area indicated (From Cooper G Bailey B Bogduk N Cervical zygapophysial joint
pain maps Pain Med 20078344ndash53)
Causes of Axial Pain
bull Mid and Low Pain
ndash Discs
ndash Facets
ndash Muscle
ndash Ligaments
bull Taxes Exrsquos Hangovers
Causes of Axial neck pain
ndash TON GON LON (C2 Mediated)
ndash MuscleLigament
ndash CSF Leak
ndash CAInfxnFxOther
bull Rare
bull Vertrbral tumors
bull Discitis
bull Septic Arthritis
bull Osteomyleitis
bull Meningitis
bull RAAS CA-GoutFx
Causes of Radicular Pain
bull Radiculopathy is a disease of neural irritation and or compression
bull Disc ProtrusionHerniation Ostophytic compresison
bull Z-Joint OspeophyteGanglionTumorRAGoutASFx
bull V-BodyTumorPagetrsquos Fx Osteomyelitis
bull Meninges CystsMengiomacystsEpidural abcessHematoma
bull Nerve Sheath NeurofibromaSchwannoma
bull Nerve GlioblastomaGanglioneuroma
Epidemiology of Neck Pain
bull 2000-2010 Task Force on Neck Pain and Its Associated Disorders performed a systematic search and critical review of literature published between 1980 and 2006 to assemble the best evidence on neck pain
bull 469 studies 249 to be scientifically admissible bull 101 articles related to the burden and determinants of neck pain in the general
population bull Incidence ranged from 0055 per 1000 person years(disc herniation with
radiculopathy) to bull 213 per 1000 persons (self-reported neck pain) bull Incidence of neck injuries during competitive sports ranged from 002 to 21 per
1000 exposures bull The 12-month prevalence of pain typically ranged between 30 and 50 the 12-
month prevalence of activity-limiting pain was 17 to 115 bull Neck pain was more prevalent among women and prevalence peaked in middle
age bull Risk factors for neck pain included genetics poor psychological health and
exposure to tobacco Disc degeneration was not identified as a risk factor bull The use of sporting gear (helmets face shields) to prevent other types of injury
was not associated with increased neck injuries in bicycling hockey or skiing
European Spine JournalApril 2008 Volume 17 Supplement 1 pp 39-51
Prevalence of Cervical Axial Pain of zygopophyseal origin
bull Prospective study of 318 patients with intractable neck pain
bull Provocation discography Z-Joint blocks
bull Z-joints 38 suffered zygapophyseal pain Aprill C Bogduk N The Prevalence of Cervical Zygapophyseal Joint Pain A First Approximation PhDSpine (Phila Pa 1976) 1992 Jul17(7)744-7
Summary Controlled studies facet or zygapophysial joint pain in 36 to 67 of these patients when disc herniation radiculitis and discogenic are not pathognomic
Falco FJ1 Manchikanti L Datta S Wargo BW Geffert S Bryce DA Atluri S Singh V Benyamin RM Sehgal N Ward SP Helm S 2nd Gupta S Boswell MV Systematic review of the therapeutic effectiveness of cervical facet joint interventions an update Pain Physician 2012 Nov-Dec15(6)E839-68
Diagnosis of Cervical Axial Pain
bull Consecutive patients seen between January 2003 and January 2005 in whom a diagnosis of neck pain was made MBBF-IAI vs Disco vs AAAO
bull Pain Med 2008 Mar9(2)196-203 doi 101111j1526-4637200700369xThe nature of neck pain in a private pain clinic in the United StatesYin W Bogduk N
ZFacet Joint Pain Treatment
bullHaving failed PTother conservative measures bullDiagnostic Medical Branch Block of the Dorsal Primary Ramus ldquoMBB or FJNBrdquo bullDual Block Paradigm
ZFacet Joint Pain Treatment
bull Facet Joint Nerve Ablation
bull FJNA
bull Typically 6-18 months of relief
ZFacet Joint Pain Treatment
bull The median time that elapsed before the pain returned to at least 50 percent of the preoperative level was 263 days in the active-treatment group and 8 days in the control group (P = 004) At 27 weeks seven patients in the active-treatment group and one patient in the control group were free of pain Five patients in the active-treatment group had numbness in the territory of the treated nerves but none considered it troubling
ZFacet Joint Pain Treatment
ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Causes of Pain AXIAL vs RADICULAR
bull Axial Neck Pain
bull High Pain
ndash AA Joint AO Joint
ndash High Cervical Facets(common)
ndash High Cervical Discs(rare)
bull Luschka Joints
ndash OndontoidAlar
ndash Chiari
The distribution of pain in normal volunteers after stimulation of the zygapophysial joints indicated (From Cooper G Bailey B Bogduk N Cervical
zygapophysial joint pain maps Pain Med 20078344ndash53)
The distribution of pain relieved in patients with neck pain after anesthetization of the synovial joints indicated using controlled diagnostic blocks The density of shading is proportional to the number of patients whose pain extended into the area indicated (From Cooper G Bailey B Bogduk N Cervical zygapophysial joint
pain maps Pain Med 20078344ndash53)
Causes of Axial Pain
bull Mid and Low Pain
ndash Discs
ndash Facets
ndash Muscle
ndash Ligaments
bull Taxes Exrsquos Hangovers
Causes of Axial neck pain
ndash TON GON LON (C2 Mediated)
ndash MuscleLigament
ndash CSF Leak
ndash CAInfxnFxOther
bull Rare
bull Vertrbral tumors
bull Discitis
bull Septic Arthritis
bull Osteomyleitis
bull Meningitis
bull RAAS CA-GoutFx
Causes of Radicular Pain
bull Radiculopathy is a disease of neural irritation and or compression
bull Disc ProtrusionHerniation Ostophytic compresison
bull Z-Joint OspeophyteGanglionTumorRAGoutASFx
bull V-BodyTumorPagetrsquos Fx Osteomyelitis
bull Meninges CystsMengiomacystsEpidural abcessHematoma
bull Nerve Sheath NeurofibromaSchwannoma
bull Nerve GlioblastomaGanglioneuroma
Epidemiology of Neck Pain
bull 2000-2010 Task Force on Neck Pain and Its Associated Disorders performed a systematic search and critical review of literature published between 1980 and 2006 to assemble the best evidence on neck pain
bull 469 studies 249 to be scientifically admissible bull 101 articles related to the burden and determinants of neck pain in the general
population bull Incidence ranged from 0055 per 1000 person years(disc herniation with
radiculopathy) to bull 213 per 1000 persons (self-reported neck pain) bull Incidence of neck injuries during competitive sports ranged from 002 to 21 per
1000 exposures bull The 12-month prevalence of pain typically ranged between 30 and 50 the 12-
month prevalence of activity-limiting pain was 17 to 115 bull Neck pain was more prevalent among women and prevalence peaked in middle
age bull Risk factors for neck pain included genetics poor psychological health and
exposure to tobacco Disc degeneration was not identified as a risk factor bull The use of sporting gear (helmets face shields) to prevent other types of injury
was not associated with increased neck injuries in bicycling hockey or skiing
European Spine JournalApril 2008 Volume 17 Supplement 1 pp 39-51
Prevalence of Cervical Axial Pain of zygopophyseal origin
bull Prospective study of 318 patients with intractable neck pain
bull Provocation discography Z-Joint blocks
bull Z-joints 38 suffered zygapophyseal pain Aprill C Bogduk N The Prevalence of Cervical Zygapophyseal Joint Pain A First Approximation PhDSpine (Phila Pa 1976) 1992 Jul17(7)744-7
Summary Controlled studies facet or zygapophysial joint pain in 36 to 67 of these patients when disc herniation radiculitis and discogenic are not pathognomic
Falco FJ1 Manchikanti L Datta S Wargo BW Geffert S Bryce DA Atluri S Singh V Benyamin RM Sehgal N Ward SP Helm S 2nd Gupta S Boswell MV Systematic review of the therapeutic effectiveness of cervical facet joint interventions an update Pain Physician 2012 Nov-Dec15(6)E839-68
Diagnosis of Cervical Axial Pain
bull Consecutive patients seen between January 2003 and January 2005 in whom a diagnosis of neck pain was made MBBF-IAI vs Disco vs AAAO
bull Pain Med 2008 Mar9(2)196-203 doi 101111j1526-4637200700369xThe nature of neck pain in a private pain clinic in the United StatesYin W Bogduk N
ZFacet Joint Pain Treatment
bullHaving failed PTother conservative measures bullDiagnostic Medical Branch Block of the Dorsal Primary Ramus ldquoMBB or FJNBrdquo bullDual Block Paradigm
ZFacet Joint Pain Treatment
bull Facet Joint Nerve Ablation
bull FJNA
bull Typically 6-18 months of relief
ZFacet Joint Pain Treatment
bull The median time that elapsed before the pain returned to at least 50 percent of the preoperative level was 263 days in the active-treatment group and 8 days in the control group (P = 004) At 27 weeks seven patients in the active-treatment group and one patient in the control group were free of pain Five patients in the active-treatment group had numbness in the territory of the treated nerves but none considered it troubling
ZFacet Joint Pain Treatment
ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

The distribution of pain in normal volunteers after stimulation of the zygapophysial joints indicated (From Cooper G Bailey B Bogduk N Cervical
zygapophysial joint pain maps Pain Med 20078344ndash53)
The distribution of pain relieved in patients with neck pain after anesthetization of the synovial joints indicated using controlled diagnostic blocks The density of shading is proportional to the number of patients whose pain extended into the area indicated (From Cooper G Bailey B Bogduk N Cervical zygapophysial joint
pain maps Pain Med 20078344ndash53)
Causes of Axial Pain
bull Mid and Low Pain
ndash Discs
ndash Facets
ndash Muscle
ndash Ligaments
bull Taxes Exrsquos Hangovers
Causes of Axial neck pain
ndash TON GON LON (C2 Mediated)
ndash MuscleLigament
ndash CSF Leak
ndash CAInfxnFxOther
bull Rare
bull Vertrbral tumors
bull Discitis
bull Septic Arthritis
bull Osteomyleitis
bull Meningitis
bull RAAS CA-GoutFx
Causes of Radicular Pain
bull Radiculopathy is a disease of neural irritation and or compression
bull Disc ProtrusionHerniation Ostophytic compresison
bull Z-Joint OspeophyteGanglionTumorRAGoutASFx
bull V-BodyTumorPagetrsquos Fx Osteomyelitis
bull Meninges CystsMengiomacystsEpidural abcessHematoma
bull Nerve Sheath NeurofibromaSchwannoma
bull Nerve GlioblastomaGanglioneuroma
Epidemiology of Neck Pain
bull 2000-2010 Task Force on Neck Pain and Its Associated Disorders performed a systematic search and critical review of literature published between 1980 and 2006 to assemble the best evidence on neck pain
bull 469 studies 249 to be scientifically admissible bull 101 articles related to the burden and determinants of neck pain in the general
population bull Incidence ranged from 0055 per 1000 person years(disc herniation with
radiculopathy) to bull 213 per 1000 persons (self-reported neck pain) bull Incidence of neck injuries during competitive sports ranged from 002 to 21 per
1000 exposures bull The 12-month prevalence of pain typically ranged between 30 and 50 the 12-
month prevalence of activity-limiting pain was 17 to 115 bull Neck pain was more prevalent among women and prevalence peaked in middle
age bull Risk factors for neck pain included genetics poor psychological health and
exposure to tobacco Disc degeneration was not identified as a risk factor bull The use of sporting gear (helmets face shields) to prevent other types of injury
was not associated with increased neck injuries in bicycling hockey or skiing
European Spine JournalApril 2008 Volume 17 Supplement 1 pp 39-51
Prevalence of Cervical Axial Pain of zygopophyseal origin
bull Prospective study of 318 patients with intractable neck pain
bull Provocation discography Z-Joint blocks
bull Z-joints 38 suffered zygapophyseal pain Aprill C Bogduk N The Prevalence of Cervical Zygapophyseal Joint Pain A First Approximation PhDSpine (Phila Pa 1976) 1992 Jul17(7)744-7
Summary Controlled studies facet or zygapophysial joint pain in 36 to 67 of these patients when disc herniation radiculitis and discogenic are not pathognomic
Falco FJ1 Manchikanti L Datta S Wargo BW Geffert S Bryce DA Atluri S Singh V Benyamin RM Sehgal N Ward SP Helm S 2nd Gupta S Boswell MV Systematic review of the therapeutic effectiveness of cervical facet joint interventions an update Pain Physician 2012 Nov-Dec15(6)E839-68
Diagnosis of Cervical Axial Pain
bull Consecutive patients seen between January 2003 and January 2005 in whom a diagnosis of neck pain was made MBBF-IAI vs Disco vs AAAO
bull Pain Med 2008 Mar9(2)196-203 doi 101111j1526-4637200700369xThe nature of neck pain in a private pain clinic in the United StatesYin W Bogduk N
ZFacet Joint Pain Treatment
bullHaving failed PTother conservative measures bullDiagnostic Medical Branch Block of the Dorsal Primary Ramus ldquoMBB or FJNBrdquo bullDual Block Paradigm
ZFacet Joint Pain Treatment
bull Facet Joint Nerve Ablation
bull FJNA
bull Typically 6-18 months of relief
ZFacet Joint Pain Treatment
bull The median time that elapsed before the pain returned to at least 50 percent of the preoperative level was 263 days in the active-treatment group and 8 days in the control group (P = 004) At 27 weeks seven patients in the active-treatment group and one patient in the control group were free of pain Five patients in the active-treatment group had numbness in the territory of the treated nerves but none considered it troubling
ZFacet Joint Pain Treatment
ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

The distribution of pain relieved in patients with neck pain after anesthetization of the synovial joints indicated using controlled diagnostic blocks The density of shading is proportional to the number of patients whose pain extended into the area indicated (From Cooper G Bailey B Bogduk N Cervical zygapophysial joint
pain maps Pain Med 20078344ndash53)
Causes of Axial Pain
bull Mid and Low Pain
ndash Discs
ndash Facets
ndash Muscle
ndash Ligaments
bull Taxes Exrsquos Hangovers
Causes of Axial neck pain
ndash TON GON LON (C2 Mediated)
ndash MuscleLigament
ndash CSF Leak
ndash CAInfxnFxOther
bull Rare
bull Vertrbral tumors
bull Discitis
bull Septic Arthritis
bull Osteomyleitis
bull Meningitis
bull RAAS CA-GoutFx
Causes of Radicular Pain
bull Radiculopathy is a disease of neural irritation and or compression
bull Disc ProtrusionHerniation Ostophytic compresison
bull Z-Joint OspeophyteGanglionTumorRAGoutASFx
bull V-BodyTumorPagetrsquos Fx Osteomyelitis
bull Meninges CystsMengiomacystsEpidural abcessHematoma
bull Nerve Sheath NeurofibromaSchwannoma
bull Nerve GlioblastomaGanglioneuroma
Epidemiology of Neck Pain
bull 2000-2010 Task Force on Neck Pain and Its Associated Disorders performed a systematic search and critical review of literature published between 1980 and 2006 to assemble the best evidence on neck pain
bull 469 studies 249 to be scientifically admissible bull 101 articles related to the burden and determinants of neck pain in the general
population bull Incidence ranged from 0055 per 1000 person years(disc herniation with
radiculopathy) to bull 213 per 1000 persons (self-reported neck pain) bull Incidence of neck injuries during competitive sports ranged from 002 to 21 per
1000 exposures bull The 12-month prevalence of pain typically ranged between 30 and 50 the 12-
month prevalence of activity-limiting pain was 17 to 115 bull Neck pain was more prevalent among women and prevalence peaked in middle
age bull Risk factors for neck pain included genetics poor psychological health and
exposure to tobacco Disc degeneration was not identified as a risk factor bull The use of sporting gear (helmets face shields) to prevent other types of injury
was not associated with increased neck injuries in bicycling hockey or skiing
European Spine JournalApril 2008 Volume 17 Supplement 1 pp 39-51
Prevalence of Cervical Axial Pain of zygopophyseal origin
bull Prospective study of 318 patients with intractable neck pain
bull Provocation discography Z-Joint blocks
bull Z-joints 38 suffered zygapophyseal pain Aprill C Bogduk N The Prevalence of Cervical Zygapophyseal Joint Pain A First Approximation PhDSpine (Phila Pa 1976) 1992 Jul17(7)744-7
Summary Controlled studies facet or zygapophysial joint pain in 36 to 67 of these patients when disc herniation radiculitis and discogenic are not pathognomic
Falco FJ1 Manchikanti L Datta S Wargo BW Geffert S Bryce DA Atluri S Singh V Benyamin RM Sehgal N Ward SP Helm S 2nd Gupta S Boswell MV Systematic review of the therapeutic effectiveness of cervical facet joint interventions an update Pain Physician 2012 Nov-Dec15(6)E839-68
Diagnosis of Cervical Axial Pain
bull Consecutive patients seen between January 2003 and January 2005 in whom a diagnosis of neck pain was made MBBF-IAI vs Disco vs AAAO
bull Pain Med 2008 Mar9(2)196-203 doi 101111j1526-4637200700369xThe nature of neck pain in a private pain clinic in the United StatesYin W Bogduk N
ZFacet Joint Pain Treatment
bullHaving failed PTother conservative measures bullDiagnostic Medical Branch Block of the Dorsal Primary Ramus ldquoMBB or FJNBrdquo bullDual Block Paradigm
ZFacet Joint Pain Treatment
bull Facet Joint Nerve Ablation
bull FJNA
bull Typically 6-18 months of relief
ZFacet Joint Pain Treatment
bull The median time that elapsed before the pain returned to at least 50 percent of the preoperative level was 263 days in the active-treatment group and 8 days in the control group (P = 004) At 27 weeks seven patients in the active-treatment group and one patient in the control group were free of pain Five patients in the active-treatment group had numbness in the territory of the treated nerves but none considered it troubling
ZFacet Joint Pain Treatment
ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Causes of Axial Pain
bull Mid and Low Pain
ndash Discs
ndash Facets
ndash Muscle
ndash Ligaments
bull Taxes Exrsquos Hangovers
Causes of Axial neck pain
ndash TON GON LON (C2 Mediated)
ndash MuscleLigament
ndash CSF Leak
ndash CAInfxnFxOther
bull Rare
bull Vertrbral tumors
bull Discitis
bull Septic Arthritis
bull Osteomyleitis
bull Meningitis
bull RAAS CA-GoutFx
Causes of Radicular Pain
bull Radiculopathy is a disease of neural irritation and or compression
bull Disc ProtrusionHerniation Ostophytic compresison
bull Z-Joint OspeophyteGanglionTumorRAGoutASFx
bull V-BodyTumorPagetrsquos Fx Osteomyelitis
bull Meninges CystsMengiomacystsEpidural abcessHematoma
bull Nerve Sheath NeurofibromaSchwannoma
bull Nerve GlioblastomaGanglioneuroma
Epidemiology of Neck Pain
bull 2000-2010 Task Force on Neck Pain and Its Associated Disorders performed a systematic search and critical review of literature published between 1980 and 2006 to assemble the best evidence on neck pain
bull 469 studies 249 to be scientifically admissible bull 101 articles related to the burden and determinants of neck pain in the general
population bull Incidence ranged from 0055 per 1000 person years(disc herniation with
radiculopathy) to bull 213 per 1000 persons (self-reported neck pain) bull Incidence of neck injuries during competitive sports ranged from 002 to 21 per
1000 exposures bull The 12-month prevalence of pain typically ranged between 30 and 50 the 12-
month prevalence of activity-limiting pain was 17 to 115 bull Neck pain was more prevalent among women and prevalence peaked in middle
age bull Risk factors for neck pain included genetics poor psychological health and
exposure to tobacco Disc degeneration was not identified as a risk factor bull The use of sporting gear (helmets face shields) to prevent other types of injury
was not associated with increased neck injuries in bicycling hockey or skiing
European Spine JournalApril 2008 Volume 17 Supplement 1 pp 39-51
Prevalence of Cervical Axial Pain of zygopophyseal origin
bull Prospective study of 318 patients with intractable neck pain
bull Provocation discography Z-Joint blocks
bull Z-joints 38 suffered zygapophyseal pain Aprill C Bogduk N The Prevalence of Cervical Zygapophyseal Joint Pain A First Approximation PhDSpine (Phila Pa 1976) 1992 Jul17(7)744-7
Summary Controlled studies facet or zygapophysial joint pain in 36 to 67 of these patients when disc herniation radiculitis and discogenic are not pathognomic
Falco FJ1 Manchikanti L Datta S Wargo BW Geffert S Bryce DA Atluri S Singh V Benyamin RM Sehgal N Ward SP Helm S 2nd Gupta S Boswell MV Systematic review of the therapeutic effectiveness of cervical facet joint interventions an update Pain Physician 2012 Nov-Dec15(6)E839-68
Diagnosis of Cervical Axial Pain
bull Consecutive patients seen between January 2003 and January 2005 in whom a diagnosis of neck pain was made MBBF-IAI vs Disco vs AAAO
bull Pain Med 2008 Mar9(2)196-203 doi 101111j1526-4637200700369xThe nature of neck pain in a private pain clinic in the United StatesYin W Bogduk N
ZFacet Joint Pain Treatment
bullHaving failed PTother conservative measures bullDiagnostic Medical Branch Block of the Dorsal Primary Ramus ldquoMBB or FJNBrdquo bullDual Block Paradigm
ZFacet Joint Pain Treatment
bull Facet Joint Nerve Ablation
bull FJNA
bull Typically 6-18 months of relief
ZFacet Joint Pain Treatment
bull The median time that elapsed before the pain returned to at least 50 percent of the preoperative level was 263 days in the active-treatment group and 8 days in the control group (P = 004) At 27 weeks seven patients in the active-treatment group and one patient in the control group were free of pain Five patients in the active-treatment group had numbness in the territory of the treated nerves but none considered it troubling
ZFacet Joint Pain Treatment
ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Causes of Axial neck pain
ndash TON GON LON (C2 Mediated)
ndash MuscleLigament
ndash CSF Leak
ndash CAInfxnFxOther
bull Rare
bull Vertrbral tumors
bull Discitis
bull Septic Arthritis
bull Osteomyleitis
bull Meningitis
bull RAAS CA-GoutFx
Causes of Radicular Pain
bull Radiculopathy is a disease of neural irritation and or compression
bull Disc ProtrusionHerniation Ostophytic compresison
bull Z-Joint OspeophyteGanglionTumorRAGoutASFx
bull V-BodyTumorPagetrsquos Fx Osteomyelitis
bull Meninges CystsMengiomacystsEpidural abcessHematoma
bull Nerve Sheath NeurofibromaSchwannoma
bull Nerve GlioblastomaGanglioneuroma
Epidemiology of Neck Pain
bull 2000-2010 Task Force on Neck Pain and Its Associated Disorders performed a systematic search and critical review of literature published between 1980 and 2006 to assemble the best evidence on neck pain
bull 469 studies 249 to be scientifically admissible bull 101 articles related to the burden and determinants of neck pain in the general
population bull Incidence ranged from 0055 per 1000 person years(disc herniation with
radiculopathy) to bull 213 per 1000 persons (self-reported neck pain) bull Incidence of neck injuries during competitive sports ranged from 002 to 21 per
1000 exposures bull The 12-month prevalence of pain typically ranged between 30 and 50 the 12-
month prevalence of activity-limiting pain was 17 to 115 bull Neck pain was more prevalent among women and prevalence peaked in middle
age bull Risk factors for neck pain included genetics poor psychological health and
exposure to tobacco Disc degeneration was not identified as a risk factor bull The use of sporting gear (helmets face shields) to prevent other types of injury
was not associated with increased neck injuries in bicycling hockey or skiing
European Spine JournalApril 2008 Volume 17 Supplement 1 pp 39-51
Prevalence of Cervical Axial Pain of zygopophyseal origin
bull Prospective study of 318 patients with intractable neck pain
bull Provocation discography Z-Joint blocks
bull Z-joints 38 suffered zygapophyseal pain Aprill C Bogduk N The Prevalence of Cervical Zygapophyseal Joint Pain A First Approximation PhDSpine (Phila Pa 1976) 1992 Jul17(7)744-7
Summary Controlled studies facet or zygapophysial joint pain in 36 to 67 of these patients when disc herniation radiculitis and discogenic are not pathognomic
Falco FJ1 Manchikanti L Datta S Wargo BW Geffert S Bryce DA Atluri S Singh V Benyamin RM Sehgal N Ward SP Helm S 2nd Gupta S Boswell MV Systematic review of the therapeutic effectiveness of cervical facet joint interventions an update Pain Physician 2012 Nov-Dec15(6)E839-68
Diagnosis of Cervical Axial Pain
bull Consecutive patients seen between January 2003 and January 2005 in whom a diagnosis of neck pain was made MBBF-IAI vs Disco vs AAAO
bull Pain Med 2008 Mar9(2)196-203 doi 101111j1526-4637200700369xThe nature of neck pain in a private pain clinic in the United StatesYin W Bogduk N
ZFacet Joint Pain Treatment
bullHaving failed PTother conservative measures bullDiagnostic Medical Branch Block of the Dorsal Primary Ramus ldquoMBB or FJNBrdquo bullDual Block Paradigm
ZFacet Joint Pain Treatment
bull Facet Joint Nerve Ablation
bull FJNA
bull Typically 6-18 months of relief
ZFacet Joint Pain Treatment
bull The median time that elapsed before the pain returned to at least 50 percent of the preoperative level was 263 days in the active-treatment group and 8 days in the control group (P = 004) At 27 weeks seven patients in the active-treatment group and one patient in the control group were free of pain Five patients in the active-treatment group had numbness in the territory of the treated nerves but none considered it troubling
ZFacet Joint Pain Treatment
ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Causes of Radicular Pain
bull Radiculopathy is a disease of neural irritation and or compression
bull Disc ProtrusionHerniation Ostophytic compresison
bull Z-Joint OspeophyteGanglionTumorRAGoutASFx
bull V-BodyTumorPagetrsquos Fx Osteomyelitis
bull Meninges CystsMengiomacystsEpidural abcessHematoma
bull Nerve Sheath NeurofibromaSchwannoma
bull Nerve GlioblastomaGanglioneuroma
Epidemiology of Neck Pain
bull 2000-2010 Task Force on Neck Pain and Its Associated Disorders performed a systematic search and critical review of literature published between 1980 and 2006 to assemble the best evidence on neck pain
bull 469 studies 249 to be scientifically admissible bull 101 articles related to the burden and determinants of neck pain in the general
population bull Incidence ranged from 0055 per 1000 person years(disc herniation with
radiculopathy) to bull 213 per 1000 persons (self-reported neck pain) bull Incidence of neck injuries during competitive sports ranged from 002 to 21 per
1000 exposures bull The 12-month prevalence of pain typically ranged between 30 and 50 the 12-
month prevalence of activity-limiting pain was 17 to 115 bull Neck pain was more prevalent among women and prevalence peaked in middle
age bull Risk factors for neck pain included genetics poor psychological health and
exposure to tobacco Disc degeneration was not identified as a risk factor bull The use of sporting gear (helmets face shields) to prevent other types of injury
was not associated with increased neck injuries in bicycling hockey or skiing
European Spine JournalApril 2008 Volume 17 Supplement 1 pp 39-51
Prevalence of Cervical Axial Pain of zygopophyseal origin
bull Prospective study of 318 patients with intractable neck pain
bull Provocation discography Z-Joint blocks
bull Z-joints 38 suffered zygapophyseal pain Aprill C Bogduk N The Prevalence of Cervical Zygapophyseal Joint Pain A First Approximation PhDSpine (Phila Pa 1976) 1992 Jul17(7)744-7
Summary Controlled studies facet or zygapophysial joint pain in 36 to 67 of these patients when disc herniation radiculitis and discogenic are not pathognomic
Falco FJ1 Manchikanti L Datta S Wargo BW Geffert S Bryce DA Atluri S Singh V Benyamin RM Sehgal N Ward SP Helm S 2nd Gupta S Boswell MV Systematic review of the therapeutic effectiveness of cervical facet joint interventions an update Pain Physician 2012 Nov-Dec15(6)E839-68
Diagnosis of Cervical Axial Pain
bull Consecutive patients seen between January 2003 and January 2005 in whom a diagnosis of neck pain was made MBBF-IAI vs Disco vs AAAO
bull Pain Med 2008 Mar9(2)196-203 doi 101111j1526-4637200700369xThe nature of neck pain in a private pain clinic in the United StatesYin W Bogduk N
ZFacet Joint Pain Treatment
bullHaving failed PTother conservative measures bullDiagnostic Medical Branch Block of the Dorsal Primary Ramus ldquoMBB or FJNBrdquo bullDual Block Paradigm
ZFacet Joint Pain Treatment
bull Facet Joint Nerve Ablation
bull FJNA
bull Typically 6-18 months of relief
ZFacet Joint Pain Treatment
bull The median time that elapsed before the pain returned to at least 50 percent of the preoperative level was 263 days in the active-treatment group and 8 days in the control group (P = 004) At 27 weeks seven patients in the active-treatment group and one patient in the control group were free of pain Five patients in the active-treatment group had numbness in the territory of the treated nerves but none considered it troubling
ZFacet Joint Pain Treatment
ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Epidemiology of Neck Pain
bull 2000-2010 Task Force on Neck Pain and Its Associated Disorders performed a systematic search and critical review of literature published between 1980 and 2006 to assemble the best evidence on neck pain
bull 469 studies 249 to be scientifically admissible bull 101 articles related to the burden and determinants of neck pain in the general
population bull Incidence ranged from 0055 per 1000 person years(disc herniation with
radiculopathy) to bull 213 per 1000 persons (self-reported neck pain) bull Incidence of neck injuries during competitive sports ranged from 002 to 21 per
1000 exposures bull The 12-month prevalence of pain typically ranged between 30 and 50 the 12-
month prevalence of activity-limiting pain was 17 to 115 bull Neck pain was more prevalent among women and prevalence peaked in middle
age bull Risk factors for neck pain included genetics poor psychological health and
exposure to tobacco Disc degeneration was not identified as a risk factor bull The use of sporting gear (helmets face shields) to prevent other types of injury
was not associated with increased neck injuries in bicycling hockey or skiing
European Spine JournalApril 2008 Volume 17 Supplement 1 pp 39-51
Prevalence of Cervical Axial Pain of zygopophyseal origin
bull Prospective study of 318 patients with intractable neck pain
bull Provocation discography Z-Joint blocks
bull Z-joints 38 suffered zygapophyseal pain Aprill C Bogduk N The Prevalence of Cervical Zygapophyseal Joint Pain A First Approximation PhDSpine (Phila Pa 1976) 1992 Jul17(7)744-7
Summary Controlled studies facet or zygapophysial joint pain in 36 to 67 of these patients when disc herniation radiculitis and discogenic are not pathognomic
Falco FJ1 Manchikanti L Datta S Wargo BW Geffert S Bryce DA Atluri S Singh V Benyamin RM Sehgal N Ward SP Helm S 2nd Gupta S Boswell MV Systematic review of the therapeutic effectiveness of cervical facet joint interventions an update Pain Physician 2012 Nov-Dec15(6)E839-68
Diagnosis of Cervical Axial Pain
bull Consecutive patients seen between January 2003 and January 2005 in whom a diagnosis of neck pain was made MBBF-IAI vs Disco vs AAAO
bull Pain Med 2008 Mar9(2)196-203 doi 101111j1526-4637200700369xThe nature of neck pain in a private pain clinic in the United StatesYin W Bogduk N
ZFacet Joint Pain Treatment
bullHaving failed PTother conservative measures bullDiagnostic Medical Branch Block of the Dorsal Primary Ramus ldquoMBB or FJNBrdquo bullDual Block Paradigm
ZFacet Joint Pain Treatment
bull Facet Joint Nerve Ablation
bull FJNA
bull Typically 6-18 months of relief
ZFacet Joint Pain Treatment
bull The median time that elapsed before the pain returned to at least 50 percent of the preoperative level was 263 days in the active-treatment group and 8 days in the control group (P = 004) At 27 weeks seven patients in the active-treatment group and one patient in the control group were free of pain Five patients in the active-treatment group had numbness in the territory of the treated nerves but none considered it troubling
ZFacet Joint Pain Treatment
ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Prevalence of Cervical Axial Pain of zygopophyseal origin
bull Prospective study of 318 patients with intractable neck pain
bull Provocation discography Z-Joint blocks
bull Z-joints 38 suffered zygapophyseal pain Aprill C Bogduk N The Prevalence of Cervical Zygapophyseal Joint Pain A First Approximation PhDSpine (Phila Pa 1976) 1992 Jul17(7)744-7
Summary Controlled studies facet or zygapophysial joint pain in 36 to 67 of these patients when disc herniation radiculitis and discogenic are not pathognomic
Falco FJ1 Manchikanti L Datta S Wargo BW Geffert S Bryce DA Atluri S Singh V Benyamin RM Sehgal N Ward SP Helm S 2nd Gupta S Boswell MV Systematic review of the therapeutic effectiveness of cervical facet joint interventions an update Pain Physician 2012 Nov-Dec15(6)E839-68
Diagnosis of Cervical Axial Pain
bull Consecutive patients seen between January 2003 and January 2005 in whom a diagnosis of neck pain was made MBBF-IAI vs Disco vs AAAO
bull Pain Med 2008 Mar9(2)196-203 doi 101111j1526-4637200700369xThe nature of neck pain in a private pain clinic in the United StatesYin W Bogduk N
ZFacet Joint Pain Treatment
bullHaving failed PTother conservative measures bullDiagnostic Medical Branch Block of the Dorsal Primary Ramus ldquoMBB or FJNBrdquo bullDual Block Paradigm
ZFacet Joint Pain Treatment
bull Facet Joint Nerve Ablation
bull FJNA
bull Typically 6-18 months of relief
ZFacet Joint Pain Treatment
bull The median time that elapsed before the pain returned to at least 50 percent of the preoperative level was 263 days in the active-treatment group and 8 days in the control group (P = 004) At 27 weeks seven patients in the active-treatment group and one patient in the control group were free of pain Five patients in the active-treatment group had numbness in the territory of the treated nerves but none considered it troubling
ZFacet Joint Pain Treatment
ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Diagnosis of Cervical Axial Pain
bull Consecutive patients seen between January 2003 and January 2005 in whom a diagnosis of neck pain was made MBBF-IAI vs Disco vs AAAO
bull Pain Med 2008 Mar9(2)196-203 doi 101111j1526-4637200700369xThe nature of neck pain in a private pain clinic in the United StatesYin W Bogduk N
ZFacet Joint Pain Treatment
bullHaving failed PTother conservative measures bullDiagnostic Medical Branch Block of the Dorsal Primary Ramus ldquoMBB or FJNBrdquo bullDual Block Paradigm
ZFacet Joint Pain Treatment
bull Facet Joint Nerve Ablation
bull FJNA
bull Typically 6-18 months of relief
ZFacet Joint Pain Treatment
bull The median time that elapsed before the pain returned to at least 50 percent of the preoperative level was 263 days in the active-treatment group and 8 days in the control group (P = 004) At 27 weeks seven patients in the active-treatment group and one patient in the control group were free of pain Five patients in the active-treatment group had numbness in the territory of the treated nerves but none considered it troubling
ZFacet Joint Pain Treatment
ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

ZFacet Joint Pain Treatment
bullHaving failed PTother conservative measures bullDiagnostic Medical Branch Block of the Dorsal Primary Ramus ldquoMBB or FJNBrdquo bullDual Block Paradigm
ZFacet Joint Pain Treatment
bull Facet Joint Nerve Ablation
bull FJNA
bull Typically 6-18 months of relief
ZFacet Joint Pain Treatment
bull The median time that elapsed before the pain returned to at least 50 percent of the preoperative level was 263 days in the active-treatment group and 8 days in the control group (P = 004) At 27 weeks seven patients in the active-treatment group and one patient in the control group were free of pain Five patients in the active-treatment group had numbness in the territory of the treated nerves but none considered it troubling
ZFacet Joint Pain Treatment
ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

ZFacet Joint Pain Treatment
bull Facet Joint Nerve Ablation
bull FJNA
bull Typically 6-18 months of relief
ZFacet Joint Pain Treatment
bull The median time that elapsed before the pain returned to at least 50 percent of the preoperative level was 263 days in the active-treatment group and 8 days in the control group (P = 004) At 27 weeks seven patients in the active-treatment group and one patient in the control group were free of pain Five patients in the active-treatment group had numbness in the territory of the treated nerves but none considered it troubling
ZFacet Joint Pain Treatment
ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

ZFacet Joint Pain Treatment
bull The median time that elapsed before the pain returned to at least 50 percent of the preoperative level was 263 days in the active-treatment group and 8 days in the control group (P = 004) At 27 weeks seven patients in the active-treatment group and one patient in the control group were free of pain Five patients in the active-treatment group had numbness in the territory of the treated nerves but none considered it troubling
ZFacet Joint Pain Treatment
ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

ZFacet Joint Pain Treatment
ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

ZFacet Joint Pain Treatment
bull RetrospectiveObjective To assess the incidence of complications associated with fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facet joints
bull facet joint radiofrequency denervation procedures performed at the Mayo Clinic in Jacksonville during a 5-year period
bull Ninety-two patients received a total of 616 radiofrequency lesions during 116 separate denervation procedures An average of 5 plusmn 3 lesions were performed during each radiofrequency denervation procedure
bull Six minor complications were identified yielding a 10 overall incidence of minor complications per radiofrequency site
bull Complications included 3 cases of localized pain lasting more than 2 weeks (05) and 3 cases of neuritic pain lasting less than 2 weeks (05) No cases of infection new motor deficits or new sensory deficits were identified
bull Conclusions Fluoroscopically guided percutaneous radiofrequency denervation of the lumbar facets is associated with an overall 10 incidence of minor complications per lesion site
Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Cervical Degenerative Disc Disease (C-DDD)
Abstract Cervical MRI 497 ASYMPTOMATIC subjects
bull five disc levels from C2ndashC3 to C6ndashC7 were evaluated bull The frequency of all degenerative findings increased linearly with age bull Disc degeneration was the most common observation
bull 20s 17 of discs of men 12 of those of women bull 60lt 86 and 89 of discs of both men and women
bull demonstrable compression of the spinal cord was observed in 76 of subjects mostly over 50 years of age
bull ldquoOur results should be taken into account when interpreting the MRI findings in patients with symptomatic disorders of the cervical spinerdquo
1998
Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Cervical Degenerative Disc Disease (C-DDD)
bull89 asymptomatic volunteers aged 9 to 63 years bullThe degree of DD (disc darkening on T2-weighted images) disc protrusions and prolapses narrowing of disc spaces dorsal osteophytes and spinal canal stenosis were assessed bullAbnormalities were commoner in older subjects
bull62 of being seen in those over 40 bullsubjects aged less than 30 years there were virtually no abnormalities bullDD was the most common abnormality seen in 10 of discs bull 57 DD was in subjects aged over 40 bullDD at the C56 level was the most common finding bullNo differences in abnormal findings between males and females was observed
Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Cervical Degenerative Disc Disease (C-DDD)
bullldquoRole of pathology visualized by magnetic resonance imaging (MRI) remains unclearrdquo bullThe study aimed to determine whether subjects with persistent or recurrent neck and shoulder pain were more likely to have abnormal MRI findings of cervical spine than those without neck and shoulder pain bullRandom 826 high-school students investigated 17ndash19 years and AGAIN 24ndash26 years of age 87 initial participation 76 took part in follow-up bullNordic Musculoskeletal Questionnaire was used to collect data about neck and shoulder symptoms bullTwo groups G1reported no neck and shoulder symptoms in either of the inquirie bull G2 suffering from neck and shoulder symptoms once a week or more often bullThe study found that abnormal MRI findings were common in both study groups bullDisc herniation was the only MRI finding that was significantly associated with neck pain
E J of Spine 2002
When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

When Is C-DDD Clinically significant (C-DDD)
Results A systematic review of the literature demonstrated that cervical discography plays a significant role in selecting surgical candidates and improving outcomes despite concerns regarding the false-positive rate lack of standardization and assorted potential confounding factors Based on the studies utilizing the International Association for the Study of Pain (IASP) criteria the data show a prevalence rate ranging between 16 and 20 Based on the 3 studies that utilized IASP criteria during the performance of cervical discography the evidence derived from studies evaluating the diagnostic validity of the procedure the indicated level of evidence is Level II-2 based on modified US Preventive Services Task Force (USPSTF) criteria
bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

bullBeyond the debate regarding its efficacy in identifying the site of cervical symptomatology and directing appropriate intervention are the potential morbidity and mortality associated with this diagnostic procedure bullDiscitis subdural empyema spinal cord injury vascular injury and prevertebral abscess have all been reported as complications of diagnostic cervical disc injection bullRetrospective 4400 cervical disc injections in 1357 patients performed by an experienced radiologist between 1988 and 1993 to define the morbidity and mortality associated with discography bullIn addition we reviewed the extant medical literature on the complications of this controversial procedure bull This study demonstrates significant complications from diagnostic discography procedures occurring in less than 06 of the patients and 016 of the cervical disc injections
Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Why I rarely do Cervical Discography
bull Excluding facetogenic pain rare to find purely axial non-tender pain that is NOT C-DDD
bull Whats the literature reveal on cervical fusion and replacement
bull Pretty good outcomes
bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

bull Medicine (Baltimore) 2016 Jan95(4)e2568 doi 101097MD0000000000002568Comparison of Clinical Efficacy Between Interlaminar and Transforaminal Epidural Injection in Patients With Axial Pain due to Cervical Disc
bull Herniation
bull Axial neck pain is originated from sinuvertebral nerve located in ventral epidural spaces which has been described to be related to central or paramedian disc herniation
bull 108 patients who underwent IL and TF epidural injections axial neckinterscapular pain due to central or paramedian cervical disc herniation were included
bull Successful pain relief was defined if a 50 or more reduction of NRS score was achieved in comparison with pretreatment one
bull Overall 79 (731) and 57 (528) 2 and 8 weeks respectively Seventy-six (704) and 52 (481) had successful functional improvement at 2 and 8 weeks Cervical epidural injection showed favorable results in 2 weeks and moderate results in 8 weeks in patients with axial pain due to cervical disc herniation
Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Epidemiology of Cervical Radiculopathy
bull 561 patients (332 males and 229 females)
bull 13 to 91 years the mean age plusmnSD was 476plusmn131 years for males and 482plusmn138 years for females
bull A history of trauma preceding= 148 of cases
bull A past history of lumbar radiculopathy was present in 41
bull A monoradiculopathy involving C7 nerve root was the most frequent followed by C6
bull A confirmed disc protrusion was responsible for cervical radiculopathy in 219 of patients
Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Epidemiology of Cervical Radiculopathy
bull 684 were related to spondylosis disc or both bull During the median duration of follow-up of 49 years recurrence
of the condition occurred in 317 and 26 underwent surgery for cervical radiculopathy
bull At last follow-up 90 of our population-based patients were asymptomatic or only mildly incapacitated due to cervical radiculopathy
bull Annual incidence rates per 100k ndash 832 for the total ndash 1073 for males and ndash 635 for females
bull The age-specific annual incidence rate per 100 000 population reached a peak of 2029 for the age group 50ndash54 years
Kurupath Radhakrishnan William J Litchy W Michael OFallon Leonard T Kurland Epidemiology of cervical radiculopathy A population-based study from Rochester Minnesota 1976 through 1990 BrainA Journal of Neurology
Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Cervical Radiculopathy
Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Cervical Radiculopathy bull Common etiologies
bull Cervical Disc Herniation
bull Lateral recess stenosis
ndash DiscLuschka vs ligament
bull Foraminal stenosis
ndash Facet vs Luschka
Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Cervical Radiculopathy
C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

C-Radic Non-operative Management
bull ldquoThe axons of these nerves are either compressed directly or are rendered ischemic by compression of their blood supply Symptoms of sensory or motor loss arise as a result of block of conduction along the affected axons The features of cervical radiculopathy therefore are essentially negative in nature they reflect loss of function In contrast pain is a positive feature not caused by loss of nerve function
bull For this reason cervical radicular pain cannot be summarily attributed to the same causes as those of radiculopathy Compression of axons does not elicit pain If compression is to be invoked as a mechanism for pain it must explicitly relate to compression of a dorsal root ganglionldquo
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Cervical Radiculopathy
bull ldquoAs opposed to compression there are growing contentions that cervical radicular pain may be caused by inflammation of the cervical nerve roots This mechanism might be applicable to radicular pain caused by disc protrusions because inflammatory exudates have now been isolated from cervical disc material However inflammation cannot be invoked as the mechanism of radicular pain caused by noninflammatory lesions such as tumors cysts and osteophytes For these conditions compression of the dorsal root ganglion is the only mechanism for which there is experimental evidence
bull However none of these considerations bear on the causes and mechanisms of neck pain Whatever its cause and whatever its mechanism cervical radicular pain is perceived in the upper limb
bull -Nikolai Bogduk bull Phys Med Rehabil Clin N Am 2011 Aug22(3)367-82 vii doi
101016jpmr201103008The anatomy and pathophysiology of neck painBogduk N1
bull The Nerve Moves- Porter McRoberts
Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Cervical Radiculopathy Non-operative treatment
bull Non-operative treatment
ndash Physical therapy
ndash Chiropractic
ndash Traction
ndash Epidural steroid injections
bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

bull This prospective study with independent clinical review was set up to monitor the clinical outcome of patients when using serial periradicularepidural corticosteroid injection techniques in managing cervical radiculopathy
bull Over a 10 year period between 1986 and 1995 a consecutive series of 68 secondary referral patients presenting with cervical radiculopathy were entered into the study
bull Of the 64 patients (94) who under-went imaging relevant pathology thought to correlate with the clinical presentation was demonstrated in all but one patient
bull Serial periradicularepidural corticosteroid injections were used to control pain an average of 25 injections was administered per patient (range 1ndash6)
bull Patients underwent a final clinical examination when their pain had remained satisfactorily under control for an average of 7 months (range 1ndash23 months) They subsequently were reassessed by an independent clinician at an average of 39 months (range 4ndash112 months) after initial presentation via a telephone interview
bull Despite the fact that all 68 patients were potential surgical candidates they all made a satisfactory recovery without the need for surgical intervention
bull Forty-eight patients (76) did not experience any arm pain and of the 15 patients (24) who did this improved from 10 to an average of 2 (range 1ndash4) on a 10-point pain scale Thus patients with cervical radiculopathy make a satisfactory recovery with serial periradicularepidural corticosteroid injections without the need for surgical intervention
bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

bull Complications of Cervical Epidural Nerve Blocks with Steroids A Prospective Study of 790 Consecutive Blocks WALDMAN STEVEN D MD MayJune 1989 - Volume 14 - Issue 3pp 99-159
790 consecutive cervical epidural nerve blocks were followed prospectively for a six-week period for early as well as delayed complications
bull Two patients sustained unintentional dural puncture Both patients ultimately required cervical epidural blood patch
bull Three patients experienced vasovagal syncope during CSENB They were easily resuscitated
bull One late complication of superficial infection at the injection site was noted The patient recovered without sequela
bull From the above data it appears that CSENB represents a safe modality in the treatment of a variety of painful conditions
bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

bull Study Design A prospective concurrently controlled randomized multicenter trial of an anterior Bagby and Kuslich cervical fusion cage (BAKC Sulzer Spine-Tech Minneapolis MN) for treatment of degenerative disc disease of the cervical spineObjectives To report clinical results with maximum 24-month follow-up of fusions performed with the BAKC fusion cageSummary of Background Data Threaded lumbar cages have been used during the past decade as a safe and effective surgical solution for chronic disabling low back pain Threaded cages have now been developed for use in anterior cervical interbody fusions to obviate the need for allografts or autogenous bone grafting procedures while providing initial stability during the fusion processMethods Patients with symptomatic cervical discogenic radiculopathy were treated with either anterior cervical discectomy with uninstrumented bone-only fusion (ACDF) or BAKC fusion cage(s) Independent radiographic assessment of fusion was made and patient-based outcome was assessed by visual analog pain scale and a Short Form (SF)-36 Health Status QuestionnaireResults Data analysis included 344 patients at 1 year and 180 at 2 years When the two cage groups (hydroxya patite-coated or noncoated) were compared with the ACDF group similar outcomes were noted for duration of surgery hospital stay improvements in neck pain and radicular pain in the affected limb improvements in the SF-36 Physical Component subscale and Mental Component subscale and the patientsrsquo perception of overall surgical outcome Symptom improvements were maintained at 2 years A greater percentage of patients with ACDF needed an iliac crest bone harvest than did BAKC patients (67vsmdash 3)
bull Successful fusion for one-level procedures at 12 months was 979 for the BAKC groups and 897 for the ACDF group (P lt 005)
bull The complication rate for the ACDF group was 204 compared with an overall complication rate of 118 with BAKC
Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

Summary
bull McRoberts WP Cairns KD Current Surgical Options for the Treatment of Cervical and Lumbar Degenerative Disc Disease IN Kapural L (ed) Diagnosis Management amp Treatment of Discogenic Pain Elsevier Philadelphia 2011
ldquoWhile this chapter seeks to investigate and present the available surgical options the greater importance already appreciated by many patients may lie not on the selection of surgical method but rather on the selection of surgeon ldquo
bullExamine and read the patient bullTake course of highest safety with best outcome bullMany cases of cervicogenic pain recover without intervention bullEvaluate the risk of your intervention BUT
bullALSO EVALUATE THE RISK ASSOCIATED WITH NONTREATMENT bullINACTIVITY IN OLDER AGE GROUPS CAN BE DEVESTATING AND GREAT MORBIDITY AND MORTALITY IS ASSOCIATED WITH TORPOR
In Conclusion Come Here for Help

In Conclusion Come Here for Help