Embed Size (px)
Citation preview

Non-operative ACL Management Webinar
Mr Mick HughesM. Sports Physio, B. Physio. B. Ex Sci
Chaired by Simon Price
4 February 2020

ESSA Presentation
Non-operative management of
ACL injuries
By Mick Hughes
APA Titled Sports & Exercise Physiotherapist
Co-founder of Melbourne ACL Rehabilitation Guide and www.learn.physio
www.mickhughes.physio www.learn.physio

Overview
• Evidence supporting non-operative ACL management
• Potential copers vs non-copers
• Does non-operative ACL management increase risk of knee osteoarthritis?
• Non-operative rehabilitation
www.mickhughes.physio www.learn.physio

Evidence to support non-operative ACL rehab
www.mickhughes.physio www.learn.physio

KANON trial
• Prospective, RCT of 141 active patients (18-35yrs) who injured their ACL for the first time
• 5 year follow-up outcome measures:
• PROMs (KOOS4, SF-36)
• Tegner activity levels
• Meniscal surgery
• Radiographic OA changes
• Return to pre-injury levels of sport
www.mickhughes.physio www.learn.physio

KANON Trial: Treatment Groups
Rehab + Early ACLR
N=61
Rehab + Delayed ACLR
N=59
www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

KANON Trial: Participants
www.mickhughes.physio www.learn.physio

KANON Trial: 5 Year Follow-Up Results
• Analysis was performed on 120/121 patients:
• N= 61 early ACLR group (1 lost to follow-up
in this group)
• N= 59 delayed ACLR group
• 51% opted for delayed ACLR over the 5 years
• N=23 in the first 2 years
• N=7 between 2-5 years
• 49% continuing to manage their ACL injury
without surgery 5 years after their injury
www.mickhughes.physio www.learn.physio

KANON Trial: 5 Year Follow-Up Results
• No significant difference between groups
from baseline to 5 years, or between 2-5 year
follow-up:
• KOOS4, SF-36, Tegner activity levels, pre-
injury Tegner activity levels
• No significant difference between groups
from baseline to 5 years in regards to
radiographic OA of PFJ and TFJ
• No significant differences between groups in
number of meniscus surgeries performed
www.mickhughes.physio www.learn.physio
KANON Trial: Summary
After 5 years following ACL injury, no statistically
significant differences between early ACLR
group and those who have the option of having a
delayed ACLR in:
• KOOS4
• general physical/mental health (SF-36)
• current physical activity level (Tegner)
• return to pre-injury activity level
• radiographic OA
• meniscus surgery
www.mickhughes.physio www.learn.physio

Important to note however…
“No significant difference ≠ return to normal”
www.mickhughes.physio www.learn.physio
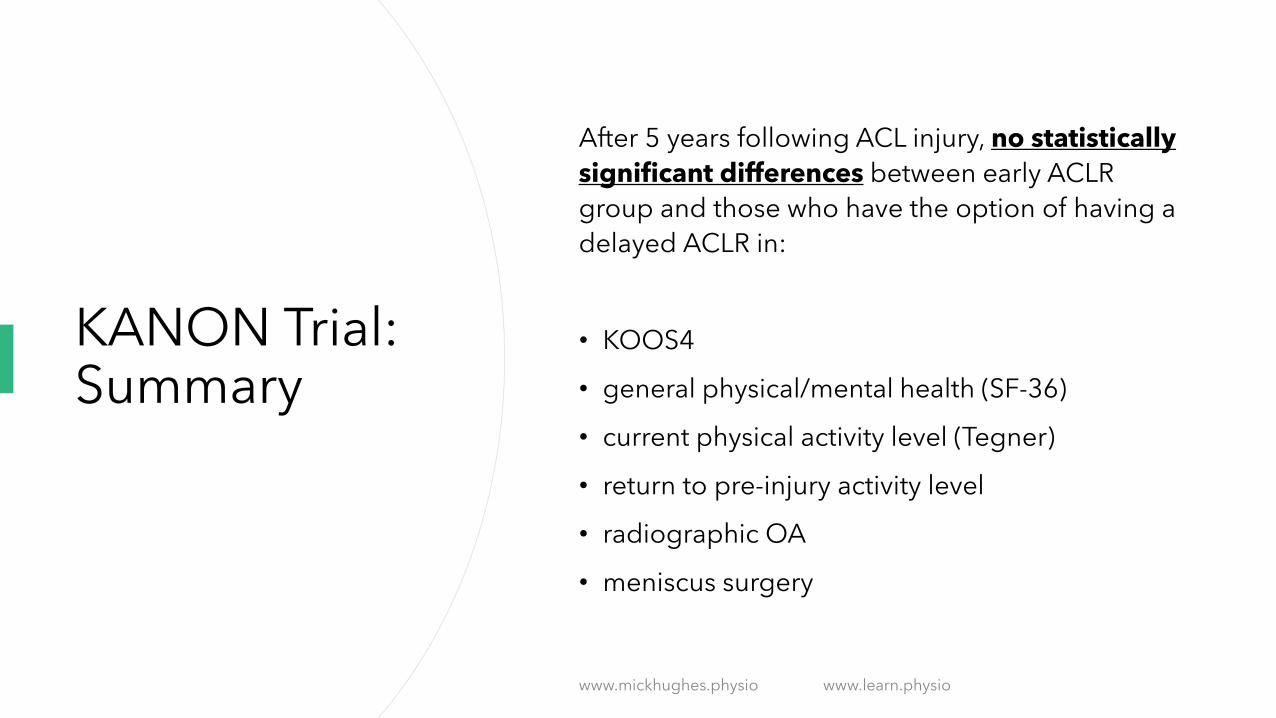
KANON Trial: 2-year follow-up results
www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio
But Wait!!
Before you all get excited and start recommending every patient for non-operative ACL management..
Understand that there were inclusion and exclusion criteria to the KANON trial.
www.mickhughes.physio www.learn.physio

KANON Trial: Not Eligible
www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

KANON Trial: Inclusion Criteria
www.mickhughes.physio www.learn.physio

Successful non-operative case studies
www.mickhughes.physio www.learn.physio

• Case study of a 32 year old male
professional Soccer player
• Right ACL injury occurred in the first half
of a competitive EPL match
• Non-contact mechanism of injury
• MRI confirmed ACL injury + G1 MCL +
osteochondral injury to lateral femoral
sulcus
• NB: follow-up MRI at 10months
showed healing of osteochondral injury
www.mickhughes.physio www.learn.physio

Weiler et al 2015
• Consulted with 2 independent surgeons; both recommended ACLR
• Player chose to pursue a nonoperative treatment plan
• Progressive, criterion-driven rehab and return to sport plan commenced 1 week after injury (once knee had settled)
• Player able to return to full-training at 8 weeks post-injury
• Was selected to play in 5 games after the injury
• At 18 months post-injury at the time of case study publication, he remained fully fit and available for team selection and was aregular starting player at his new club
www.mickhughes.physio www.learn.physio

• 86 ACL injured elite European Handball athletes (53F/33M) were prospectively followed for up to 11 years
• Short term (return to play) and long term (function, OA changes & QOL) outcomes were recorded and analysed
www.mickhughes.physio www.learn.physio

Results
• 79/86 (91%) completed follow-up questionnaires (mean 7 years post injury)
• 72% had ACLR and 28% were treated nonoperatively
• 82% of nonoperative group returned to pre-injury sport and played for a further 4.1 years
• 58% of ACLR group returned to pre-injury sport and played for a further 3.8
• 22% of ACLR group sustained ACL graft failures
• Close to half of each treatment group reported pain, instability or reduced QOL 6-11 years after ACL injury
www.mickhughes.physio www.learn.physio

Authors Summary
“If long term knee health is the primary concern, the results of this study show that knee
function is compromised in about half of the elite players 6-11 years after ACL injury
regardless of treatment choice.”
www.mickhughes.physio www.learn.physio

But what about when non-operative management
doesn’t go so well?
www.mickhughes.physio www.learn.physio
www.mickhughes.physio www.learn.physio

Gray et al (2017)
• 21 year old female, elite level college, soccer player
• Non-contact ACL injury during a competitive game
• Confirmed isolated ACL rupture 1 day later via MRI
• Expressed a desire to RTS as soon as possible, and keen to try non-operative strategy as she had previous ACLR to contralateral knee
www.mickhughes.physio www.learn.physio

Gray et al (2017)
• Went through “coper screening” algorithm
• Identified as a “potential coper”
• Rehabilitation started ASAP keeping in line with Eitzen protocol
• Was cleared to start team practice 3 weeks after injury
• 4 weeks post-injury, was cleared to play and played 10mins as a substitution (wearing a de-rotational brace)
• Able to play out the remainder of the season, including multiple post-season games
www.mickhughes.physio www.learn.physio

Gray et al (2017)
• But…
• 6 months later playing a recreational game of soccer, had an instability episode that injured her medial meniscus
• Consulted with medical staff at her club and opted to have an ACLR and meniscus repair
www.mickhughes.physio www.learn.physio

A case study of a not-so-good result for one of my patients…
www.mickhughes.physio www.learn.physio

Case Study
• 29 year old Male
• First F2F consult in the clinic 8/1/2020 for R) ACL injury sustained 9 weeks previous
• Had consulted with Ortho surgeon and Sports Physician prior and both happy to
support non-op ACL plan
• Consulted F2F in clinic 3x up until 2/3/2020 for rehab progressions; including return to
running straight lines and commencing skipping and jump/land drills

Case Study
• Had tolerated the first month of running and jumping well
• Had instability episode during a box jump on 2/4/2020
• Telehealth Consultation on 3/4/2020
• Difficulty weight-bearing
• Obvious and large effusion
• AROM -45ext – 90deg flexion

Case Study
• Advised to rest, ice, compression and elevation
• AROM as tolerated
• Advised that we would review regularly over the next 5-7 days via emails and phone
conversations
• Gradually improved over the next 7-10 days; but still had a 5deg loss of extension
• Call Sports Physician to arrange a F2F follow-up ASAP

Case Study
• Sports Physician follow-up 27/4/20
• MRI performed on 28/4/20
• Bucket-handle tear of medial meniscus
• R) ACLR and partial medial menisectomy performed 5/5/20
• First post-op ACLR F2F consultation on 26/5/20

In summary..
• Some people can return back to their pre-injury level of
sport without ACLR..
• Some people unfortunately will not and will go on to worsen
their knee..
• Importantly, we have a discussion that the athlete has a
choice other than ACLR following ACL injury.
www.mickhughes.physio www.learn.physio
Identifying potential copers and potential non-copers
www.mickhughes.physio www.learn.physio

• Describe the outcomes of “potential copers” who elected to pursue non-op ACL management
• Potential Coper: able to cope with ongoing rehabilitation after ACL injury (Fitzgerald et al, 2000)

Hurd et al (2008): Methods
• Inclusion criteria:
• Clinical evaluation within 7 months of injury
• Regular participation in level I or II sports
• MRI confirmed ACL injury
• Exclusion criteria: repairable meniscus tear, or full thickness cartilage lesions on MRI in
addition to ACL injury
• Coper screening test was performed once the knee was “quiet”

Hurd et al (2008): Results
• 345 subjects met inclusion criteria and completed “Coper Screening” examination mean 6 weeks post ACL injury
• Mean 27yrs (13-57yrs; 63% males)
• 42% potential copers and 58% non-copers
• 72% of potential copers returned to pre-injury levels of sport without ACLR
• None of the 72% sustained further chondral or meniscal injuries
• None of those who elected delayed ACLR due to instability worsened their knee
• 10 year follow-up: 40% still potential copers whilst 57% elected to have delayed ACLR


Coper Screen Assessment: The Quiet Knee
La Trobe University: PTY5WSP

Coper Screening Assessment: Instability?
La Trobe University: PTY5WSP

Coper Screening Assessment: Goal: >80% LSI 6m Timed Hop
La Trobe University: PTY5WSP

Coper screening assessment:Goal: >80% KOS-ADLs
La Trobe University: PTY5WSP


Coper Screening AssessmentGoal: >60% Global Rating of Knee Scale
“How would you rate your level of functioning during your usual daily activities on a scale from 0 to 100, with 100 being your level of function prior to your knee problem, and 0 being the inability to perform any of your
usually daily activities?”
La Trobe University: PTY5WSP

But what if someone is a “non-coper”?
www.mickhughes.physio www.learn.physio

Don’t stress…
Maybe they need more rehab.
Maybe they need more time.
www.mickhughes.physio www.learn.physio

• Purpose of this study was 2-fold:
• Evaluate coper classification
before and after 10 sessions of
neuromuscular strength training
(NMST) early after ACL injury
• Evaluate the association of early
coper classification with 2 year
outcomes

Thoma et al (2019): Methods
• Prospective cohort study of 300 ACL injured
athletes
• Performed coper screening before and after 10
sessions of NMST and classified at each testing
session as either a potential coper or non-
coper
• Outcomes measured also at 6 months, 1 year
and 2 years after self-selecting treatment
option

Thoma et al (2019): Results
Main findings:
• 55% were potential copers at screening; Increased to 68% after 10 sessions of NMST
• 45% of the initial non-copers became potential copers after 10 sessions of NMST
At 2yr follow-up:
• 64% of ACLR group and 74% of nonoperative group had “successful” rehab
• ACLR and nonoperative potential copers had nearly 3x the odds of success as compared to ACLR non-copers
Another reason why we should be encouraging ACL injured patients into extended rehabilitation…
www.mickhughes.physio www.learn.physio

Can the ACL heal???Can the ACL heal???
www.mickhughes.physio www.learn.physio

Can the ACL heal??
• Historically it has been reported that the ACL has little capacity to heal
2 main proposed physiological reasons behind the inability for it to heal:
• Inability of blood clots to form during the initial healing, that results in a lack of scaffolding between the 2 ruptured end-points.
• Layer of synovial tissue forming over the ruptured ACL end points impeding tissue healing.
www.mickhughes.physio www.learn.physio

Case Study: 25 year-old Male
www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

39 year-old Male (credit: Dr Louise Tulloh)
www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

Ihara & Kawano (2017)
• 102 ACL injured patients were included in this study
• 44 males and 58 females (mean age 28 years).
• Exclusion criteria:
• ACL rupture was older than 20 days,
• if they sustained a concomitant PCL injury,
• any other lower limb injury that made wearing a knee brace impossible
• Stratified into 2 groups:
• aged under 20 years of age (n=39)
• aged over 20 years of age (n= 63)
www.mickhughes.physio www.learn.physio
Ihara & Kawano (2017)
• At the time of their injury, they had MRI and their images of their ACL injury were classified into 4 different types according to the degree of injury:
• Type I – straight and continuous band (n=23)
• Type II – curved and continuous band (n= 34)
• Type III – displacement (n= 24)
• Type IV – disrupted or horizontally orientated or unclear (n=21)
• Note: at time of injury mean difference between limbs on KT-1000 testing was 5mm
www.mickhughes.physio www.learn.physio

Ihara & Kawano (2017)
MRI images at initial injury
www.mickhughes.physio www.learn.physio

Ihara & Kawano (2017)
• At minimum 6 months follow-up post ACL injury, MRI was performed again.
• This time the ACL injury was classified into 4 grades according to the morphological recovery:
• Grade I – taut and straight band
• Grade II – straight band with partial thinning
• Grade III – thinned
• Grade IV – unclear
www.mickhughes.physio www.learn.physio

Ihara & Kawano (2017)
• MRI images of at least 6 months follow-up
www.mickhughes.physio www.learn.physio

Ihara & Kawano (2017)
Results:
• Classification of MRI at final MRI assessment for all participants:
• 41/102 were classified as Grade I
• 17/102 were classified as Grade II
• 25/102 were classified as Grade III
• 19/102 were classified as Grade IV
• Athletes <20yrs were significantly less likely to “heal”; only 30% showing type I or type II morphology at follow-up
• Compared to 72% of those athletes >20yrs showing type I or type II morphology at follow-up.
www.mickhughes.physio www.learn.physio

Ihara & Kawano (2017)
Case study of healing ACL tissue in 28 year-old within this study
www.mickhughes.physio www.learn.physio

Ihara & Kawano (2017)
Discussion:
• The authors believe that the type I and type II ACL injuries are a sub-type of ACL injury, and represents an avulsion injury from the femoral attachment; ACL stays in tact but remains nearby its footprint and/or the torn ACL fibres form a bundle with minor displacement away from the femoral stump of tissue.
?? Partial tears:
• The authors report that the degree of laxity in type I injuries was similar to types II/III/IV, and that type I injuries were in fact complete tears and not partial tears
www.mickhughes.physio www.learn.physio

Ihara & Kawano (2017)
Conclusion:
• This present study demonstrated that in a sub-type of ACL tears limited to straight and continuous bands (avulsion injuries, proximal tears with little displacement), the ACL has a high intrinsic ability to morphologically and mechanically heal (as assessed via MRI and clinical tests).
• However, in younger patients with more severe ACL injuries (type III+IV) the morphologically recovery is less likely than older adults aged over 20yrs.
www.mickhughes.physio www.learn.physio
In summary..
We can’t guarantee to our patients that their ACL will heal, but we should give them a fighting chance to see if they can be one of the lucky ones.
www.mickhughes.physio www.learn.physio
Does Non-operative Management Increase Risk of Knee Osteoarthritis?
www.mickhughes.physio www.learn.physio

Short answer…
No.
www.mickhughes.physio www.learn.physio

• Further analysis of 5 year follow-up data from KANON Trial
• Early ACLR was associated with greater patellofemoral
cartilage thickness loss over 2 years and 5 years compared
to the optional/delayed ACLR group
www.mickhughes.physio www.learn.physio

• Comprehensive systematic review and meta-analysis to ascertain risk of knee OA development in adults following isolated ACL injury, isolated meniscus injury or combined ACL and meniscus injury
• Included studies: prospective or retrospective in design, minimum 2 year follow-up, patients aged 18yrs or older at time of injury, studies that compared injured knee to uninjured contralateral knee or non-injured control group
www.mickhughes.physio www.learn.physio

Poulsen et al (2019)
www.mickhughes.physio www.learn.physio
53 papers included in meta-analysis
11 investigated isolated ACL
(185, 219 subjects)
22 investigated isolated meniscus
(83, 267 subjects)
25 investigated combined ACL and meniscus (725, 362 subjects)
Risk of OA development was assessed regardless of treatment option in all 3 groups

Poulsen et al (2019)
The odds ratio for developing knee OA in comparison with a non-injured knee are as follows:
• 4.2x greater risk for isolated ACL
• 6.3x greater risk for isolated meniscus
• 6.4x greater risk for combined ACL and meniscus injury
For 80% of the included studies, the follow-up period was more than 10years and activity level prior to the injury (either high or low) did not influence the risk of knee OA development
www.mickhughes.physio www.learn.physio

Tib-Fem OA
www.mickhughes.physio www.learn.physio

• Purpose: determine Tib-Fem OA prevalence, associated meniscus injuries, and menisectomies, patient function and symptoms in nonoperative treatment of ACL injury 15 years after injury
• Prospective cohort study of 100 ACL injured patients (mean age 26yrs)
• Only 14% had isolated ACL tears
• All were referred to high, quality rehab for 5-8 months
www.mickhughes.physio www.learn.physio

Neuman et al (2008): Results
• 94 were available for 15yr follow-up
• 23% had delayed ACLR at mean 4yrs post-injury (BPTB grafts)
• 15% had radiographic Tib-Fem OA
• No significant difference in BMI or Tegner activity levels between those with or without OA at 15yrs
• All of those who had OA had a menisectomy at some point between index injury (n=5) or 15yr follow-up (n=8)
www.mickhughes.physio www.learn.physio

PFJOA
www.mickhughes.physio www.learn.physio

• Same cohort of ACL injured
patients followed up at 15yrs
• 16% had radiographic PFOA
• 58% also had Tib-Fem OA
• 46% of those that had
delayed ACLR had PFOA
• Whereas only 8% of those
continuing nonoperative
management had PFOA
www.mickhughes.physio www.learn.physio

OA summary
• ACL injuries and meniscus injuries are strong individual risk factors for the
development of knee OA at 10 or more years following injury
• Results from Poulsen et al (2019) also indicate that meniscus injury (either isolated or
with ACL injury) is a more important risk factor for OA development
• OA risk after knee injury is time dependent and increases with longer follow-up time
• It appears unfortunately that ACL injured patients are unable to avoid knee OA, and OA
changes are likely to occur over time regardless of treatment option
www.mickhughes.physio www.learn.physio

Non-operative rehabilitation
www.mickhughes.physio www.learn.physio

Acute ACL Injury
Most ACL injuries are ineffectively loaded
Get the knee “Quiet”
Don’t be afraid of heavy strengthening exercises
www.mickhughes.physio www.learn.physio

What is a “Quiet” Knee?
Full or almost full AROM
Minimal knee effusion
No quads lag
www.mickhughes.physio www.learn.physio

What can I do if the Knee is not “Quiet”?
Active low-impact CV exercise and therapeutic exercises
(reduce pain/swelling, maintain muscle)
Manual therapy
(reduce pain and swelling)
Electrotherapy
(maintain quad strength and reduce pain)
www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

What can I do when the Knee is “Quiet”?
LOAD UP! ACSM STRENGTH GUIDELINES
3-4 SETS OF 6-10 REPS PER EXERCISE
2-3X PER WEEK
www.mickhughes.physio www.learn.physio

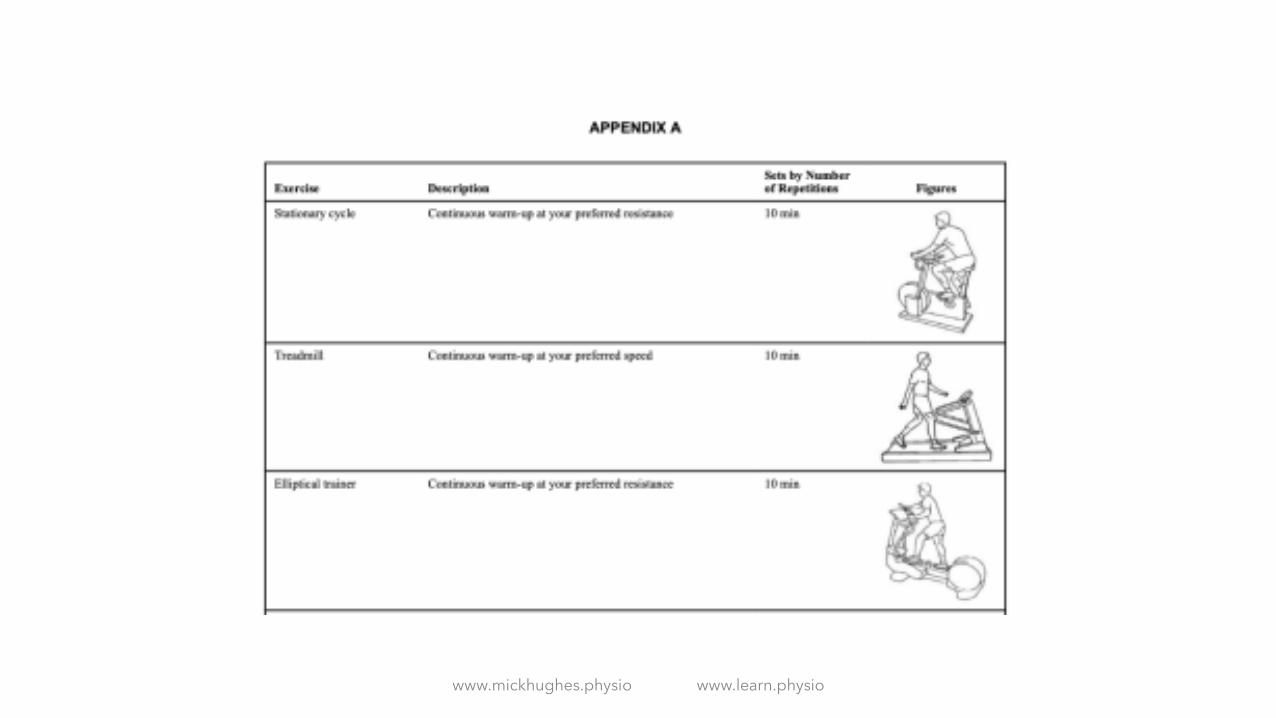
• Aims of the study:
• present in detail 5-week progressive exercise therapy program for
patients with ACL injury
• evaluate changes in strength and knee function from pre-test to
post-test after completion of the exercise therapy program
www.mickhughes.physio www.learn.physio

Eitzen et al (2010)
10 SESSION PROGRAM
(MAX 75MINS PER SESSION)
2X PER WEEK OVER 5 WEEK
KEEPING IN LINE WITH ACSM PROGRESSIVE STRENGTH GUIDELINES IN HEALTHY ADULTS
PLYOMETRIC AND PERTURBATION EXERCISES TO ENHANCE NEUROMUSCULAR
DEVELOPMENT AND CO-ORDINATION
www.mickhughes.physio www.learn.physio
Eitzen et al (2010)Key Exercises
• Single leg squat
• Step up
• Squat on Bosu
• Single leg press
• Single leg knee extension
• Squats
• Leg curls
• Hamstrings on fitball
• Single hop
• Skating
www.mickhughes.physio www.learn.physio
www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

Eitzen et al (2010): Perturbations
• Progressions by adding perturbation to;
• Rocker Board
• Roller Board/Platform
• Roller Board
www.mickhughes.physio www.learn.physio

www.mickhughes.physio www.learn.physio

The Results
This study showed that performing these exercises results in improving strength and function outcomes in both those pursuing ACLR or non-operative plan
This same program has also been shown to change around 50% of “non-copers” to “potential copers” in as little as 5 weeks (Thoma et al, 2019)
The same program has also been shown to increase the likelihood of returning to pre-injury level of sport in ACLR patients; as compared to those who don’t do the program prior to ACLR (Failla et al 2016)
www.mickhughes.physio www.learn.physio

Clinical Trials vs “Real World”
I modify and stretch this program out for 3 months
First 4 weeks build strength via progressive overload
Weeks 4-8 progress to single leg loaded exercises
Weeks 8-12 add in the plyometrics and perturbations
www.mickhughes.physio www.learn.physio

Exceptions to this Plan:Surgical Opinion Necessary
Fracture Full thickness cartilage loss injury
Repairable meniscus injury
Multi-ligament trauma
www.mickhughes.physio www.learn.physio

Early Rehab Summary
High quality rehab for at least 5 weeks; preferably
12 weeks!
Get the knee “quiet” as early as possible
When the knee is “quiet” don’t be afraid of load
If non-operative pathway, continue this rehab at
least 12 months
If ACLR being performed, start this plan up again
when the knee is “quiet” post-op
www.mickhughes.physio www.learn.physio
Summary
• Non-operative ACL management is an appropriate strategy following ACL injury
• Unfortunately not enough people are given the choice
• Osteoarthritis is likely to occur at least 10 years after the injury regardless of treatment
choice
• We should be encouraging all ACL patients into high-quality rehabilitation as a long
term management strategy regardless of treatment choice
www.mickhughes.physio www.learn.physio













![Winners List - Motor Car [ACL] (motor car).pdfareej 14 Motor Car ACL 016 2,000 15,000 ACL-35202****9025-016 Shamaila Shafique 15 Motor Car ACL 017 2,000 10,100 ACL-35202****4553-017](https://img.dokumen.tips/doc/110x75/60e41d8b31ed9359ad784c32/winners-list-motor-car-acl-motor-carpdf-areej-14-motor-car-acl-016-2000.jpg)