Embed Size (px)
Citation preview
1
TITLE: Non-neutralizing antibodies against factor VIII and risk of inhibitor
development in patients with severe hemophilia A.
Short Title: Anti-FVIII non-neutralizing antibodies and inhibitor.
Antonino Cannavò1, Carla Valsecchi1, Isabella Garagiola2, Roberta Palla2, Pier Mannuccio
Mannucci1, Frits R. Rosendaal3, Flora Peyvandi1-2.
1Angelo Bianchi Bonomi Hemophilia and Thrombosis Center, Fondazione IRCCS Ca'
Granda Ospedale Maggiore Policlinico and Luigi Villa Foundation, Milan, Italy; 2Department
of Pathophysiology and Transplantation, Università degli Studi di Milano, Milan, Italy; and
3Department of Clinical Epidemiology, Leiden University Medical Center, Leiden, The
Netherlands
Corresponding Author:
Flora Peyvandi, MD PhD. Angelo Bianchi Bonomi Hemophilia and Thrombosis Center,
IRCCS Ca’ Granda Maggiore Policlinico Hospital Foundation and Department of
Pathophysiology and Transplantation, University of Milan, via Pace 9, 20122 Milan, Italy at
Tel: +39 02 55 03 4456, fax +39 02 54 100 125.
e-mail: [email protected]
Text count: 2785 words
Abstract count: 232 words
Figure/table count: 1 figure/3 tables.
Reference count: 51
Blood First Edition Paper, prepublished online December 29, 2016; DOI 10.1182/blood-2016-06-720086
Copyright © 2016 American Society of Hematology
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

2
Key points:
Non-neutralizing antibodies against factor VIII are detected in untreated or minimally
treated patients with hemophilia A.
The presence of non-neutralizing antibodies is associated with a substantially
increased risk of inhibitor development.
BLOOD/2016/720086
Keywords: severe hemophilia A, inhibitor, non-neutralizing antibody, previously
untreated patient.
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom
3
ABSTRACT
The development of anti-factor VIII (FVIII) neutralizing antibodies (inhibitors) is the major
complication in hemophilia A. Non-neutralizing antibodies (NNAs) have not only been
detected in hemophilia patients but also in unaffected individuals. The aim of this study was
to assess the prevalence of NNAs in a cohort of previously untreated or minimally treated
patients with hemophilia A, and to evaluate whether their presence is associated with the
development of inhibitors. Plasma samples of 237 patients with severe hemophilia A enrolled
in the SIPPET trial were collected before any exposure to FVIII concentrates and analyzed
for the presence of anti-FVIII NNAs. Patients were followed for the development of
neutralizing antibodies. NNAs were found in 18/237 (7.6%) of patients at screening, with a
clear age gradient. Of those with NNAs, seven patients subsequently developed an inhibitor,
for a cumulative incidence of 45.4% (95% confidence interval (CI95) 19.5-71.3%), whereas
among those without NNAs 64/219 (29%) developed an inhibitor (cumulative incidence
34.0%, CI95 27.1-40.9%). In Cox regression, patients with NNAs at screening had a 83%
higher incidence of inhibitor development than patients without NNAs (hazard ratio (HR)
1.83, CI95 0.84-3.99). For high-titer inhibitors, the rate was almost 3-fold increased (HR
2.74, CI95 1.23-6.12). These associations did not materially change after adjustment. The
presence of anti-FVIII NNAs in patients with severe hemophilia A not previously exposed to
FVIII concentrates is associated with an increased incidence of inhibitors.
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

4
INTRODUCTION
The development of alloantibodies neutralizing factor VIII (FVIII) coagulant activity
(inhibitors) represents the main complication of treatment of hemophilia A. It occurs in
approximately one third of previously untreated patients (PUPs) and causes substantial
morbidity, mortality and costs for the healthcare system1-3. The causes for inhibitor
development are not fully understood, but some risk factors have been identified4-9 .
FVIII inhibitors consist of a polyclonal population of antibodies that are targeted to multiple
antigenic sites within the A2, A3 and C2 domains of the protein10. In addition to inhibitors,
anti-FVIII antibodies are present in healthy individuals and patients affected with hemophilia
A without exerting coagulant inhibitory activity. Several laboratory platforms for the
detection of total FVIII binding antibodies have been developed, based upon immunoblotting
assay, fluorescence immune assay and enzyme-linked immunosorbent assay (ELISA)11-31.
With these assays non-neutralizing antibodies (NNAs) directed towards non-functional FVIII
epitopes that escape detection by means of functional assays have been identified. Their
prevalence is approximately 2-3% in healthy individuals16,18,21,24, while estimates in
hemophilia patients with different degrees of severity of disease vary widely, from 12% to
54%13-22,24-25,29-31. Although NNAs and inhibitors are not distinguishable based on their
isotypes, clonality and epitopes32, recent data published by Hofbauer33 indicate that anti-
FVIII IgG with inhibitory activity have an up to 100-fold higher affinity for FVIII than those
without inhibitory activity. Based on studies on cross-reactivity it has been also suggested
that FVIII inhibitors in hemophilia A patients originate from the expansion of a natural anti-
FVIII clone of B lymphocytes that exists before any treatment with FVIII and secretes anti-
FVIII antibodies similar to the natural antibodies found in healthy individuals. Furthermore,
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

5
FVIII inhibitors seem to be produced by a B cell clone that has undergone an antigen-driven
affinity-maturation and hypermutation of the V-region33. With this as background, what is not
known pertaining to NNAs is their presence before any exposure to FVIII concentrates and
their relationship with subsequent inhibitor development, even though Boylan et al.15 already
suggested that NNAs could be an early sign of subsequent inhibitor development. Currently
available data on NNAs stem from large but heterogeneous cohorts of multi-transfused
patients, some with previous but then eradicated inhibitors, and others during immune
tolerance induction for inhibitor eradication. Furthermore, the majority of studies were cross-
sectional in design, and could not assess temporal relations. In particular, none of the
previous studies was performed on plasma samples collected before any FVIII concentrate
exposure11-31.
The aim of this study was to determine the prevalence and significance of anti-FVIII NNAs
in patients enrolled in the prospective randomized SIPPET study who were screened for
neutralizing and non-neutralizing anti-FVIII antibodies before any treatment with FVIII
concentrates.
MATERIAL AND METHODS
Patients:
This was a cohort study performed in the frame of SIPPET randomized trial35. Patients aged
<6 years, affected with severe hemophilia A, never exposed to FVIII concentrates, not or
minimally exposed (less than 5 EDs) to blood components (whole blood, fresh frozen plasma,
packed red cells, platelets or cryoprecipitate) and inhibitor negative by modified Bethesda
assay were included and then randomized to treatment with a single plasma-derived
(pdFVIII) or recombinant (rFVIII) FVIII concentrate. Patients were followed and monitored
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

6
at scheduled time-points for FVIII inhibitor occurrence35. Data were collected on family
history of hemophilia and inhibitor, age at screening, country site, FVIII gene mutations and
FVIII sources (for more details, see reference35); FVIII antigen levels (measured at screening
by Asserachrom VIII:C Ag, Diagnostica Stago, Asnières sur Seine, France) were categorized
as <1% and ≥ 1%. Minimally treated patients (MTPs) were defined as those exposed to less
than 5 EDs with blood components before screening, whereas previously untreated patients
(PUPs) were those never exposed to blood components. Screening was defined as the time of
inclusion in the SIPPET trial, before any exposure to FVIII concentrate. At this time a blood
sample was collected and patients were screened both for the presence of inhibitory
antibodies using the Bethesda assay with the Nijmegen modification and stored for future
determination of the presence of NNAs using an ELISA assay. Plasma samples collected at
screening were available for 237 patients and were tested for anti-FVIII NNAs.
Approval was obtained from medical ethics committee at each study center. Parents or
guardians of all children provided written informed consent.
Inhibitor testing
Inhibitor testing at screening and follow-up was performed centrally at the Angelo Bianchi
Bonomi Hemophilia and Thrombosis Centre, Milan, Italy, using the Bethesda assay with the
Nijmegen modification35. In case of inhibitor occurrence during follow-up, inhibitor levels
were confirmed on a second sample within 14 days after the first positivity, and patients were
followed for six months to establish whether the inhibitor was transient or persistent.
Non-neutralizing antibody testing
ELISA plates (96-wells NUNC Maxisorp, St. Louis, MO) were coated overnight at 4°C with
1.2 ug/mL of the full length rFVIII product Advate® (Baxter Healthcare Corporation,
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

7
Westlake Village, CA) previously dialyzed against phosphate buffered saline (PBS). The
plates were then blocked for 2 h at room temperature with PBS containing 5% skim milk
powder (Merck, Kenilworth, NJ). After blocking, the plates were washed 3 times with PBS
0.1% Tween-20 (Sigma, Merck, Kenilworth, NJ). The same washing procedure was
performed between the different incubation steps. Samples were diluted in PBS, 1% skim
milk powder (Merck, Kenilworth, NJ), 0.01% Tween-20 (Sigma, Merck, Kenilworth, NJ),
added to the coated plates and incubated for 2 h at room temperature. After a washing step,
the plates were incubated 1 h at room temperature with horseradish peroxidase (HRP)- anti
human IgG (GE Healthcare, Little Chalfont, UK ) diluted 1/2000 in PBS, 1% skim milk
powder (Merck, Kenilworth, NJ), 0.01% Tween-20. O-phenylenediamine dihydrochloride
(OPD) substrate (Sigma, Merck, Kenilworth, NJ) was added and the reaction stopped by
adding 3 mol/L H₂SO₄. Absorbance was read at 492 and corrected for background at 620 nm.
Each plasma sample was analyzed twice in different assay runs. In case of discrepancy with
values deviating from the range of interassay variability (CV= 25%), a third assay was
performed. The mean of two assay results or of the two closest values in the case of three
assays was used. In the first run all plasma samples were diluted 1/10 and, in the second,
samples with high IgG concentration were further diluted to have an absorbance value that
fell within the linear portion of the standard curve. In each assay, a positive control sample
(plasma with a high-titer inhibitor) diluted 1/40 and a negative control sample (normal pool
plasma) diluted 1/10 were also used.
Standard curve: Total IgG from a plasma of a patient with hemophilia A and a high-titer
inhibitor (600 BU) were purified on a Protein G-Sepharose (GE Healthcare, Little Chalfont,
UK ) column. Specific anti-FVIII IgG were then isolated by using affinity chromatography
on Affi-Gel 10 (Bio-Rad, Hercules, CA) coupled with rFVIII (Advate®), 4000 IU/2mL of
slurry gel. The affinity purified anti-FVIII specific IgGs were checked for purity by means of
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

8
sodium dodecyl sulphate – poly acrylamide gel electrophoresis (SDS PAGE electrophoresis)
and used in the ELISA assay to construct the standard curve. The cut-off for positive anti-
FVIII NNA was set at 1.64 µg/mL specific anti-FVIII IgG, corresponding to 100% specificity
and 96% of sensitivity in the ROC curve constructed with the results of anti-FVIII IgG
measured in 107 healthy individuals and 101 hemophilia A patients with positive FVIII
inhibitor detected by Bethesda assay (mean 103.9 BU, median 14.5 BU, range: 0.5-1400
BU).
Statistical analysis
Prevalences were estimated as proportions with confidence intervals obtained by the exact
binomial method of Clopper-Pearson. We used odds ratio (OR) and 95% confidence intervals
(CI95) to assess putative determinants of NNA. Analysis by age at screening was done by
stratifying patients in 5 age categories. Independent samples t-test was used to compare age
between the two groups.
Kaplan-Meier survival analyses were performed to assess the cumulative incidence for both
all inhibitors and high-titer inhibitors by NNAs serotype, and the incidence rates were
compared with Cox regression survival analyses taking into account as covariates FVIII gene
mutations (categorized as null- vs non-null mutation)35, FVIII antigen levels, self-reported
family history for inhibitor, trial treatment arm (pdFVIII or rFVIII), age at screening (in
months) and country site. Adjustments in multivariate Cox models were each made
individually, as there were too few events to include all variables in a single multivariate
model. Confidence intervals were derived from this model. Due to the occurrence of two
deaths during the trial35, we performed a sensitivity analysis assuming that both patients had
developed a high-titer inhibitor at the truncated follow-up instead of dying. Statistical
analyses were performed within SPSS, version 23.0 (IBM Corp., Armonk, NY).
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

9
RESULTS
Characteristics of the study cohort
The mean age at screening was 18.3 months (median 13 months; range: 0-67 months). FVIII
gene causative mutations were detected in 94.1% of the cases (n=223): 185 of them (83%)
were carrying a null-mutation (large deletions, nonsense mutations, inversions and
frameshift). In 107 of 237 patients (45.1%) there was a positive history of hemophilia in
relatives, and 23 (21.5%) reported a positive family history of inhibitor. One hundred and
twenty-one patients (51.1%) were randomized to treatment with pdFVIII and 116 (48.9%) to
rFVIII. Of 237 patients followed for a mean of 27 ED (median 23 days; range: 1-50 days), 71
developed a FVIII inhibitor (30.0%), which in 48 (67.6%) was at high-titer.
Determinants of non-neutralizing antibodies towards FVIII
NNAs were detected at screening in 18/237 patients (7.6%; CI 95 4.9-11.7%). Table 1 shows
the general characteristics of NNA-positive and NNA-negative subjects. Patients with NNAs
were older than those without (mean 27.4 months; median 24 months; range: 2-59 months vs
mean 17.5 months; median 12 months; range 0-67months; p-value: 0.007), and NNA
prevalence clearly increased with age (Table 2). Non-null mutations, measurable FVIII
antigen levels in plasma and a positive family history of inhibitor were also associated with a
higher prevalence of NNAs at screening (Table 2). Previous exposure to blood components
was associated with a reduced prevalence (OR 0.49, CI95 0.17-1.43). For all these
associations, confidence intervals were wide due to the limited sample size, and none
changed after adjustment for age.
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

10
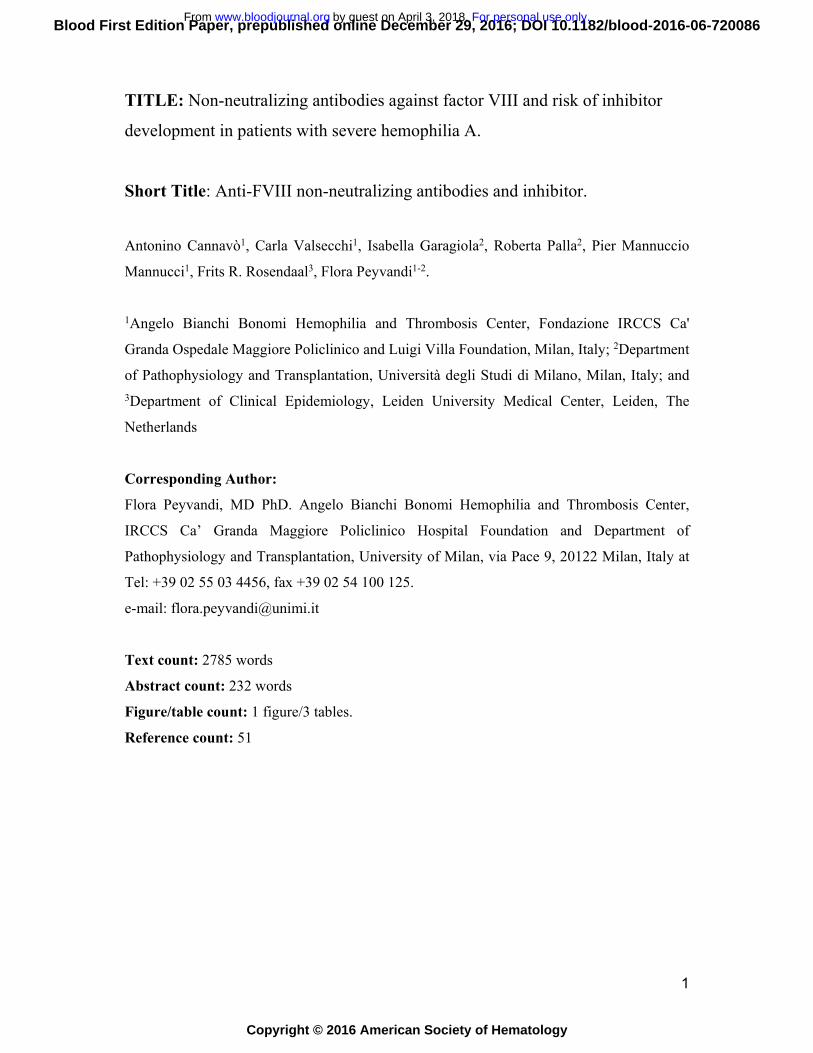
NNAs and inhibitor development
Among patients positive for NNAs at screening (n = 18), seven subsequently developed an
inhibitor, for a cumulative incidence of 45.4% (CI95 19.5-71.3%), whereas among those
negative (n = 219) 64 developed an inhibitor, for a cumulative incidence of 34.0% (CI95
27.1-40.9%). In the NNA-positive group, all inhibitors were high-titer, whereas in the NNA-
negative group, 41 of 64 inhibitors were high-titer, for a cumulative incidence of 21.9%
(CI95 15.8-28.0%). Importantly, no inhibitor among NNA-positive subjects was transient,
compared with 26.6% (17 out of 64 patients) of inhibitors in the NNA-negative group which
were transient and disappeared within 6 months.
Figure 1 shows the Kaplan-Meier plots for all and high-titer inhibitors by the presence or
absence of NNAs at screening. In univariate Cox regression, presence of NNAs was
associated with an 83% higher incidence of inhibitors than in its absence (hazard ratio (HR)
1.83, CI95 0.84-3.99). For high-titer inhibitors the rate was almost three-fold increased (HR
2.74, CI95 1.23-6.12). In adjusted models, the effect of NNAs on inhibitor development if
anything became stronger (Table 3).
Due to the stringency of our cut-off value for non-neutralizing anti-FVIII antibody positivity
we also analyzed data using a lower cut-off of 1.035 µg/mL, corresponding to the highest
value of the Younden index obtained from the ROC curve (99% of sensitivity, 98% of
specificity) and results did not change: all inhibitors by NNA positivity HR 1.69 (CI95%:
0.97-2.96) and high-titer inhibitors HR 2.33 (CI95% 1.25-4.34) . Two deaths occurred during
the trial, both among NNA-negative patients. We performed a sensitivity analysis assuming
that both patients had developed a high-titer inhibitor at the truncated follow-up instead of
dying. We recalculated the crude hazard ratio by the presence of NNAs and the results did
not change. The hazard ratio by NNAs presence was 1.78 (0.81-3.87) for all inhibitors, and
2.62 (1.18-5.84) for high-titer inhibitors. Severe non-fatal adverse events were nine episodes
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

11
of intracranial bleeding and two episodes of gastro-intestinal bleeds, all of them occurred in
the NNA-negative group. Per protocol these adverse events were not considered a reason for
withdrawal of the study, and subjects continued to be treated and completed the study.
Further sensitivity analyses were performed for patients who were censored before reaching
the predefined end-point of three years follow-up or 50 EDs, and no major deviations from
the overall findings were found.
DISCUSSION
We studied a cohort of 237 patients with severe hemophilia A, previously untreated and
minimally exposed to blood components and thereby at risk for FVIII inhibitor development
after exposure to FVIII concentrates. A sensitive ELISA assay was used to detect NNAs at
screening before any exposure to FVIII, which were present in 7.6% of patients. Age, non-
null mutation, FVIII antigen levels and family history of inhibitor seemed to influence NNAs
prevalence. Importantly, the presence of NNAs was associated with an increased risk of
inhibitor development, particularly for high-titer inhibitors, with an nearly three-fold
increased incidence rate.
In previously reports, NNA prevalence ranged from 2% to 3% in healthy people16,18,21,24 and
from 12.2% to 53.8% in patients with hemophilia A13-22,24-25,29-30. Several factors, particularly
that all previous studies predominantly included multi-transfused patients, explain this large
variation and the gaps of knowledge on their potential clinical role. For instance, the intron
22 inversion of FVIII mutation was associated with an increased frequency of NNAs in
multi-transfused patients in one study29, which was not confirmed in another20. Among multi-
transfused patients those with NNA were older than those with no NNAs in one study20, but
not in others13,30.
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

12
Given the increasing prevalence with age projected at 20% at an age of more than 40 months,
NNAs can be considered an age-related phenomenon in patients previously untreated and
minimally exposed to blood components, which may reflect maturation of the immune
system and in particular of the adaptive immune system in growing children37. This finding is
also supported by the increase of natural IgGs during the first years to remain stable with
aging38.
We found a higher prevalence of NNAs at screening in untreated patients with non-null
mutations than those with null mutations. One may hypothesize that patients with minor gene
variations have residual non-functional plasma levels of FVIII antigen, which elicit an
immune response before exposure to concentrates. This view is supported by the association
between detectable FVIII antigen and NNAs. Measurable FVIII antigen in plasma39, potential
contamination with maternal blood during delivery40, and the presence of milk fat globule
epidermal growth factor-FVIII (MFGEGF-F8) (a glycoprotein with a strong homology with
circulating FVIII in breast milk) might all be examples of early exposure41. Possibly, the
presence of NNAs before any specific treatment may be the expression of a natural anti-FVIII
B cell clone, that exists independently to any environmental FVIII exposure42.
Whereas some findings, particular those on determinants of NNAs had considerable
statistical uncertainty and should be confirmed in a larger cohort, the association of NNAs at
screening with subsequent inhibitor development was robust .
In our study, the presence of NNAs at screening in children not previously treated with any
FVIII concentrate was associated with an almost 3-fold increased risk of development of
high-titer inhibitors. In auto-immune diseases, such as systemic lupus erythematosus or
rheumatoid arthritis, the appearance of autoantibodies often precedes the clinical onset of
disease43-45. A hypothetical explanation is that the autoantibody response needs to mature
before acquiring such distinct characteristics as specificity of antigen recognition, or an
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

13
increase or shift in antigen recognition43-46. Similarly, we found that detectable inhibitors, and
mostly high-titer inhibitors, can be preceded by NNAs.
Furthermore, the effect of NNA on inhibitor development did not change its direction when
adjusted for other variables, but the hazard ratio increased after adjustment for mutation. This
can be explained by the inverse relations of null mutation with NNA presence on the one
hand and inhibitor development on the other.
This study has some limitations. The follow-up of patients started from screening and not
from birth, and therefore patients who died early were missed. Given the low fatality rate of
hemophilia, and the implausibility of a differential death rate by NNAs, this is an unlikely
source of bias.
In conclusion, the development of anti-FVIII inhibitors is a multicausal event and although
several factors have been identified4-9,35,47-51, none of them suffice to reliably predict the risk
for an individual patient. The identification of NNAs as an additional marker for inhibitor
development needs to be validated in further studies and once confirmed it could be useful to
measure NNA immediately at diagnosis or before any exposure to FVIII products. This may
contribute to improve prediction scores, which in turn may lead to individualized
interventions tailored to reduce the risk of inhibitor formation.
Acknowledgements: we thank SIPPET investigators groups for patient recruitment and data
collection. See the appendix for the full list.
Authors’ contributions. A.C., F.R.R. and F.P. designed the study, interpreted data and wrote
the manuscript. C.V. developed and validated ELISA assay, and performed the laboratory
workout. I.G. collected data and did the literature search. R.P. performed data analysis and
contributed in writing the manuscript. P.M.M. critically revised the manuscript. All authors
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

14
revised critically the work providing substantial input and gave final approval of the version
to be published.
Disclosure of interests. R.P. has received travel support from Pfizer. P.M.M. reports
honoraria for participating at advisory boards or as speaker at satellite symposia and
educational meetings organized by Baxalta, Bayer, Grifols, Kedrion Biopharma, Novo
Nordisk, Biotest and LFB. FP has received honoraria for participating as a speaker at satellite
symposia and educational meetings organized by Bayer, Biotest, CSL Behring, Grifols, Novo
Nordisk, and Sobi and she has received consulting fees from Kedrion Biopharma, LFB and
Octapharma. She is recipient of research grant funding from Alexion, Biotest, Kedrion
Biopharma, and Novo Nordisk received by Fondazione Luigi Villa. She is member of the
Ablynx scientific advisory board.
The other authors have no conflicts to declare.
Funding source. The work was supported by research grants from Fellowship project
Haemophilia Bayer Awards (to Dr Antonino Cannavò, 2014). The funder had no role in study
design, protocol preparation, patient recruitment, data collection, handling, analysis and
interpretation, or writing of the report
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

15
REFERENCES:
1. Mannucci PM, Tuddenham EG. The hemophilias: from royal genes to gene therapy. N
Engl J Med. 2001;344(23):1773-1779.
2. Peyvandi F, Garagiola I, Young G. The past and future of haemophilia: diagnosis,
treatments, and its complications. Lancet. 2016;388(10040):187-197.
3. Walsh CE, Soucie JM, Miller CH; United States Hemophilia Treatment Center
Network. Impact of inhibitors on hemophilia A mortality in the United States. Am J
Hematol. 2015;90(5):400-405.
4. Gouw SC, van den Berg HM, Oldenburg J, Astermark J, de Groot PG, Margaglione M,
Thompson AR, van Heerde W, Boekhorst J, Miller CH, le Cessie S, van der Bom JG.
F8 gene mutation type and inhibitor development in patients with severe hemophilia A:
systematic review and meta-analysis. Blood. 2012;119(12):2922-2934
5. ter Avest PC, Fischer K, Mancuso ME, Santagostino E, Yuste VJ, van den Berg HM,
van der Bom JG; CANAL Study Group. Risk stratification for inhibitor development at
first treatment for severe hemophilia A: a tool for clinical practice. J Thromb Haemost.
2008;6(12):2048-2054.
6. Oldenburg J, Schroder J, Brackmann HH, Muller-Reible C, Schwaab R, Tuddenham E.
Environmental and genetic factors influencing inhibitor development. Semin Hematol
2004;41(1 Suppl 1):82–88.
7. Astermark J, Oldenburg J, Escobar M, White GC, Berntorp E. The Malmo International
Brother Study (MIBS). Genetic defects and inhibitor development in siblings with
severe hemophilia A. Haematologica 2005;90(7):924–931.
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

16
8. Gouw SC, van den Berg HM, Fischer K, Auerswald G, Carcao M, Chalmers E,
Chambost H, Kurnik K, Liesner R, Petrini P, Platokouki H, Altisent C, Oldenburg J,
Nolan B, Garrido RP, Mancuso ME, Rafowicz A, Williams M, Clausen N, Middelburg
RA, Ljung R, van der Bom JG; PedNet and Research of determinants of inhibitor
development (RODIN) Study Group. Intensity of factor VIII treatment and inhibitor
development in children with severe hemophilia A: the RODIN study. Blood.
2013;121(20):4046-4055.
9. Iorio A, Halimeh S, Holzhauer S, Goldenberg N, Marchesini E, Marcucci M, Young G,
Bidlingmaier C, Brandao LR, Ettingshausen CE, Gringeri A, Kenet G, Knöfler R, Kreuz
W, Kurnik K, Manner D, Santagostino E, Mannucci PM, Nowak-Göttl U. Rate of
inhibitor development in previously untreated hemophilia A patients treated with
plasma-derived or recombinant factor VIII concentrates: a systematic review. J Thromb
Haemost. 2010;8(6):1256-1265.
10. Lollar, P. Pathogenic antibodies to coagulation factors. Part one: factor VIII and factor
IX. J Thromb Haemost. 2004; 2 (7): 1082–1095.
11. van Helden PM, van den Berg HM, Gouw SC, Kaijen PH, Zuurveld MG, Mauser-
Bunschoten EP, Aalberse RC, Vidarsson G, Voorberg J. IgG subclasses of anti-FVIII
antibodies during immune tolerance induction in patients with hemophilia A. Br J
Haematol. 2008;142(2):644-652.
12. Favaloro EJ, Bonar R, Duncan E, Earl G, Low J, Aboud M, Just S, Sioufi J, Street A,
Marsden K. Misidentification of factor inhibitors by diagnostic haemostasis
laboratories: recognition of pitfalls and elucidation of strategies. A follow up to a large
multicentre evaluation. Pathology. 2007;39(5):504–511.
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

17
13. Lebreton A, Lapalud P, Chambost H, Biron-Andréani C, Morange PE, Combescure C,
Marquès-Verdier A, Berger C, Schved JF, Granier C, Lavigne-Lissalde G. Prevalence
and epitope specificity of non-neutralising antibodies in a large cohort of hemophilia A
patients without inhibitors. Thromb Haemost. 2011;105(6):954-961
14. Vincent AM, Lillicrap D, Boulanger A, Meilleur C, Amesse C, St-Louis J, Rivard GE.
Non-neutralizing anti-FVIII antibodies: different binding specificity to different
recombinant FVIII concentrates. Haemophilia. 2009;15(1):374-376.
15. Boylan B, Rice AS, Dunn AL, Tarantino MD, Brettler DB, Barrett JC, Miller
CH; Hemophilia Inhibitor Research Study Investigators; Hemophilia Inhibitor Research
Study Investigators. Characterization of the anti-factor VIII immunoglobulin profile in
patients with hemophilia A by use of a fluorescence-based immunoassay. J Thromb
Haemost. 2015;13(1):47-53.
16. Hofbauer CJ, Whelan SF, Hirschler M, Allacher P, Horling FM, Lawo JP, Oldenburg J,
Tiede A, Male C, Windyga J, Greinacher A, Knöbl PN, Schrenk G, Koehn J,
Scheiflinger F, Reipert BM. Affinity of FVIII-specific antibodies reveals major
differences between neutralizing and non-neutralizing antibodies in humans.
Blood. 2015;125(7):1180-1188.
17. Montalvão SA, Tucunduva AC, Siqueira LH, Sambo AL, Medina SS, Ozelo MC A
longitudinal evaluation of anti-FVIII antibodies demonstrated IgG4 subclass is mainly
correlated with high-titre inhibitor in hemophilia A patients. Haemophilia.
2015;21(5):686-692.
18. Whelan SF, Hofbauer CJ, Horling FM, Allacher P, Wolfsegger MJ, Oldenburg J, Male
C, Windyga J, Tiede A, Schwarz HP, Scheiflinger F, Reipert BM.
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

18
Distinct characteristics of antibody responses against factor VIII in healthy individuals
and in different cohorts of hemophilia A patients. Blood. 2013;121(6):1039-1048.
19. Klintman J, Hillarp A, Berntorp E, Astermark J. Long-term anti-FVIII antibody
response in Bethesda-negative hemophilia A patients receiving continuous replacement
therapy. Br J Haematol. 2013;163(3):385-392.
20. Klintman J, Hillarp A, Donfield S, Berntorp E, Astermark J. Antibody formation and
specificity in Bethesda-negative brother pairs with hemophilia A. Quantitation of anti-
factor VIII antibodies in human plasma. Haemophilia. 2013;19(1):106-112.
21. Krudysz-Amblo J, Parhami-Seren B, Butenas S, Brummel-Ziedins KE, Gomperts
ED, Rivard GE, Mann KG. Quantitation of anti-factor VIII antibodies in human plasma.
Blood. 2009;113(11):2587-2594.
22. Zakarija A, Harris S, Rademaker AW, Brewer J, Krudysz-Amblo J, Butenas S, Mann
KG, Green D. Alloantibodies to factor VIII in hemophilia. Haemophilia. 2011;
17(4):636-640.
23. Gilles JG, Saint-Remy JM. Healthy subjects produce both anti-factor VIII and specific
anti-idiotypic antibodies. J Clin Invest. 1994; 94(4):1496–1505.
24. Batlle J, Gomez E, Rendal E et al. Antibodies to factor VIII in plasma of patients with
hemophilia A and normal subjects. Ann Hematol. 1996;72(5):321–326.
25. Dazzi F, Tison T, Vianello F et al. High incidence of anti-FVIII antibodies against
non-coagulant epitopes in hemophilia A patients: a possible role for the half-life of
transfused FVIII. Br J Haematol. 1996;93(3):688–693.
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

19
26. Scandella D, Mondorf W, Klinge J. The natural history of the immune response to
exogenous factor VIII in severe hemophilia A. Haemophilia. 1998;4(4):546–551.
27. Kempton CL, Meeks SL, Donald Harvey R, Abshire TC. Evaluation of factor VIII
pharmacokinetics and anti-factor VIII anti-bodies in four boys with hemophilia A and a
poor clinical response to factor VIII. Haemophilia. 2011;17(1):155–156.
28. Martin PG, Sukhu K, Chambers E, Giangrande PL. Evaluation of a novel ELISA
screening test for detection of factor VIII inhibitory antibodies in hemophiliacs. Clin
Lab Haematol. 1999;21(2):125-128.
29. Vianello F, Radossi P, Tison T, Dazzi F, Tagariello G, Davoli PG, Girolami A.
Prevalence of anti-FVIII antibodies in severe haemophilia A patients with inversion of
intron 22. Br J Haematol. 1997;97(4):807-809.
30. Ling M, Duncan EM, Rodgers SE, Street AM, Lloyd JV. Low detection rate of
antibodies to non-functional epitopes on factor VIII in patients with hemophilia A and
negative for inhibitors by Bethesda assay. J Thromb Haemost. 2003;1(12):2548-2553.
31. Hofbauer CJ, Kepa S, Schemper M, Quehenberger P, Reitter-Pfoertner S, Mannhalter C,
Reipert BM, Pabinger I. FVIII-binding IgG modulates FVIII half-life in patients with
severe and moderate hemophilia A without inhibitors. Blood. 2016;128(2):293-296
32. Lacroix-Desmazes S, Misra N, Bayry J, Mohanty D, Kaveri SV, Kazatchkine MD.
Autoantibodies to factor VIII. Autoimmun Rev. 2002;1(1-2):105-110.
33. Hofbauer CJ, Whelan SF, Hirschler M, Allacher P, Horling FM, Lawo JP, Oldenburg J,
Tiede A, Male C, Windyga J, Greinacher A, Knöbl PN, Schrenk G, Koehn J,
Scheiflinger F, Reipert BM. Affinity of FVIII-specific antibodies reveals major
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

20
differences between neutralizing and nonneutralizing antibodies in humans. Blood.
2015;125(7):1180-1188.
34. Moreau A, Lacroix-Desmazes S, Stieltjes N, Saenko E, Kaveri SV, D'Oiron R, Sultan
Y, Scandella D, Kazatchkine MD. Antibodies to the FVIII light chain that neutralize
FVIII procoagulant activity are present in plasma of nonresponder patients with severe
hemophilia A and in normal polyclonal human IgG. Blood. 2000;95(11):3435-3441.
35. Peyvandi F, Mannucci PM, Garagiola I, El-Beshlawy A, Elalfy M, Ramanan V, Eshghi
P, Hanagavadi S, Varadarajan R, Karimi M, Manglani MV, Ross C, Young G, Seth T,
Apte S, Nayak DM, Santagostino E, Mancuso ME, Sandoval Gonzalez AC, Mahlangu
JN, Bonanad Boix S, Cerqueira M, Ewing NP, Male C, Owaidah T, Soto Arellano V,
Kobrinsky NL, Majumdar S, Perez Garrido R, Sachdeva A, Simpson M, Thomas M,
Zanon E, Antmen B, Kavakli K, Manco-Johnson MJ, Martinez M, Marzouka E,
Mazzucconi MG, Neme D, Palomo Bravo A, Paredes Aguilera R, Prezotti A, Schmitt
K, Wicklund BM, Zulfikar B, Rosendaal FR. A Randomized Trial of Factor VIII and
Neutralizing Antibodies in Hemophilia A. N Engl J Med. 2016;374(21):2054-2064.
36. Verbruggen B, van Heerde W, Novakova I, Lillicrap D, Giles A. A 4% solution of
bovine serum albumin may be used in pace of factor VIII:C deficient plasma in the
control sample in the Nijmegen modification of the Bethesda factor VIII:C inhibitor
assay. Thromb Haemost. 2002;88(2):362-364.
37. Goenka A, Kollmann TR. Development of immunity in early life. J Infect. 2015;7
(Suppl 1): S112-120.
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

21
38. Lacroix-Desmazes S, Kaveri SV, Mouthon L, Ayouba A, Malanchère E, Coutinho A,
Kazatchkine MD. Self-reactive antibodies (natural autoantibodies) in healthy
individuals. J Immunol Methods. 1998;216(1-2):117-137.
39. Santagostino E, Mancuso ME, Tripodi A, Chantarangkul V, Clerici M, Garagiola I,
Mannucci PM. Severe hemophilia with mild bleeding phenotype: molecular
characterization and global coagulation profile. J Thromb Haemost. 2010;8(4):737-743.
40. Lo YM, Lo ES, Watson N, Noakes L, Sargent IL, Thilaganathan B, Wainscoat JS.
Two-way cell traffic between mother and fetus: biologic and clinical implications.
Blood. 1996;88(11):4390-4395.
41. Larocca D, Peterson JA, Urrea R, Kuniyoshi J, Bistrain AM, Ceriani RL. A Mr 46,000
human milk fat globule protein that is highly expressed in human breast tumours
contains factor VIII-like domains. Cancer Res. 1991;51(18):4994-4998.
42. Gunti S, Notkins AL. Polyreactive Antibodies: Function and Quantification. J Infect
Dis. 2015;212 (Suppl 1):S42-46.
43. Arbuckle MR, McClain MT, Rubertone MV, Scofield RH, Dennis GJ, James JA, Harley
JB. Development of autoantibodies before the clinical onset of systemic lupus
erythematosus. N Engl J Med. 2003;349(16):1526-1533.
44. van der Woude D, Rantapää-Dahlqvist S, Ioan-Facsinay A, Onnekink C, Schwarte CM,
Verpoort KN, Drijfhout JW, Huizinga TW, Toes RE, Pruijn GJ. Epitope spreading of
the anti-citrullinated protein antibody response occurs before disease onset and is
associated with the disease course of early arthritis. Ann Rheum Dis. 2010; 69(8):1554-
1561.
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

22
45. Recke A, Rose C, Schmidt E, Bröcker EB, Zillikens D, Sitaru C. Transition from
pemphigus foliaceus to bullous pemphigoid: intermolecular B-cell epitope spreading
without IgG subclass shifting. J Am Acad Dermatol. 2009;61(2):333-336.
46. Leslie D, Lipsky P, Notkins AL. Autoantibodies as predictors of disease. J Clin Invest.
2001;108(10):1417-1422.
47. Goudemand J, Rothschild C, Demiguel V, Vinciguerrat C, Lambert T, Chambost H,
Borel-Derlon A, Claeyssens S, Laurian Y, Calvez T. Influence of the type of factor VIII
concentrate on the incidence of factor VIII inhibitors in previously untreated patients
with severe hemophilia A. Blood. 2006;107(1):46–51.
48. Astermark J, Berntorp E, White GC, Kroner BL. The Malmo International Brother
Study (MIBS): further support for genetic predisposition to inhibitor development in
hemophilia patients. Haemophilia. 2001;7(3):267–272.
49. Fischer K, Lassila R, Peyvandi F, Calizzani G, Gatt A, Lambert T, Windyga J, Iorio A,
Gilman E, Makris M; EUHASS participants. Inhibitor development in haemophilia
according to concentrate. Four-year results from the European Haemophilia Safety
Surveillance (EUHASS) project. Thromb Haemost. 2015;113(5):968-975.
50. Gouw SC, Van Den Berg HM, Le CS, Van Der Bom JG. Treatment characteristics and
the risk of inhibitor development: a multi-center cohort study among previously
untreated patients with severe hemophilia A. J Thromb Haemost. 2007;5(7):1383–90.
51. Sharathkumar A, Lillicrap D, Blanchette VS, Kern M,Leggo J, Stain AM, Brooker
L, Carcao MD. Intensive exposure to factor VIII is a risk factor for inhibitor
development in mild hemophilia A. J Thromb Haemost 2003;1(6):1228–36.
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

23
Table 1: General characteristics and prevalence of non-neutralizing antibodies (NNAs) in the study cohort. Crude and age-adjusted odds ratio for the presence of NNAs according to potential determinants.
Characteristic NNA negative
NNA positive
Crude odds ratio (CI 95%) p-value
Age-adjusted odds ratio (CI
95%) p-value
Age at screening (months) Mean 17.5 27.4Median 12 24Max 67 59Min 0 2
FVIII mutation - n (%) null-mutation 173 (93.5) 12 (6.5) 1.0 1.0 non-null mutation 33 (86.8) 5 (13.2) 2.18 (0.72-6.61) 0.167 2.29 (0.74-7.10) 0.153
FVIII antigen levels
< 1% 195 (92.9) 15 (7.1) 1.0 1.0 ≥ 1% 21(87.5) 3 (12.5) 1.86 (0.50-6.94) 0.358 1.71 (0.45-6.50) 0.434
Family history of inhibitors - n (%)
No 69 (95.8) 3 (4.2) 1.0 1.0 Yes 21 (91.3) 2 (8.7) 2.19 (0.34-14.00) 0.407 2.93 (0.41-20.95) 0.284
Previous exposure to blood components (<5) - n (%)
No 123 (90.4) 13 (9.6) 1.0 1.0 Yes 96 (95.0) 5 (5.0) 0.49 (0.17-1.43) 0.193 0.41 (0.14-1.22) 0.110
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

24
Table 2: Distribution of NNAs over each age category and the corresponding risk estimates for the presence of NNAs.
Age at screening (months)
Total NNA-negative patients n (%)
NNA-positive patients n (%)
Odds ratio (CI95)
p-value*
All 237 219 (92.4) 18 (7.6)
≥ 40 25 20 (80.0) 5 (20.0) 6.50 (1.43-29.52) 0.018
30 - 39 23 20 (87.0) 3 (13.0) 3.90 (0.73-20.80) 0.101
20 - 29 41 38 (92.7) 3 (7.3) 2.05 (0.40-10.65) 0.319
10-19 67 63 (94.0) 4 (6.0) 1.65 (0.36-7.65) 0.331
0 - 9 81 78 (96.3) 3 (3.7) 1.0 ref.
* p-value is the comparison of each age-category to the reference
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

25
Table 3. Cox regression for inhibitor development by NNA presence. Hazard ratio compares the risk of inhibitor development among those with NNA at screening versus those without. Adjustments in multivariate Cox models were each performed individually.
Hazard ratio (CI95)
Adjustment variable all inhibitor High-titer inhibitorCrude* 1.83 (0.84-3.99) 2.74 (1.23-6.12)Age at screening 1.91 (0.85-4.26) 2.75 (1.20-6.32)Mutation 2.33 (1.05-5.15) 3.53 (1.56-8.00)FVIII antigen level 1.73 (0.79-3.78) 2.95 (1.32-6.60)Countries 2.36 (1.03-5.42) 3.91 (1.62-9.44)Familiar history of inhibitor 1.96 (0.89-4.29) 3.03 (1.35-6.81)Arm of treatment 1.73 (0.79-3.78) 2.61 (1.17-5.84)Exposure to blood components 1.75 (0.80-3.86) 2.75 (1.22-6.22)
Mutation, countries 3.62 (1.49-9.42) 5.76 (2.17-15.26)*un-adjusted model
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

26
Figures legend
Figure 1: Kaplan-Meier survival curves for inhibitor development by NNA presence. In
figure 1A cumulative incidence for all inhibitor is plotted; in figure 1B cumulative incidence
for high-titer inhibitor is plotted.
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom

doi:10.1182/blood-2016-06-720086Prepublished online December 29, 2016;
Rosendaal and Flora PeyvandiAntonino Cannavò, Carla Valsecchi, Isabella Garagiola, Roberta Palla, Pier Mannuccio Mannucci, Frits R. development in patients with severe hemophilia ANon-neutralizing antibodies against factor VIII and risk of inhibitor
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
digital object identifier (DOIs) and date of initial publication. indexed by PubMed from initial publication. Citations to Advance online articles must include final publication). Advance online articles are citable and establish publication priority; they areappeared in the paper journal (edited, typeset versions may be posted when available prior to Advance online articles have been peer reviewed and accepted for publication but have not yet
Copyright 2011 by The American Society of Hematology; all rights reserved.Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of
For personal use only.on April 3, 2018. by guest www.bloodjournal.orgFrom





























