Embed Size (px)
Citation preview

Non-medicalManagementofBreathlessness
ProjectLeader:PaulLidgate
ProjectTeam:VijayLutchmee,AnnammaWilson,CatarinaTexieira
AuthoroftheReport:AnnammaWilson
DurationofProject:March2014toJune2016
Location:RoyalBromptonHospital,London
SummaryoftheProject
FollowingasnapshotauditundertakenintherespiratorydirectorateoftheRoyalBromptonHospital, it became apparent that despite using medical interventions such as oxygentherapy, inhaledandororalmedication,asignificantnumberofpatientsreceivingcare inthedirectoratewerestrugglingwithbreathlessness.Asaresult,aprojectteamwasformedtodevelopandimplementatoolkitofnon-medicalinterventionsthatcanbeusedalongsidemedicalmanagementtohelpreducebreathlessness.Aliteraturereviewwasundertakentoidentify evidence of non-medical interventions to relieve breathlessness. 17 techniqueswereinitiallyidentified,butthiswasreducedtoninefollowingdiscussionwithintheprojectteam aboutwhichwould bemost relevant to the patient groups involved in the project.Initially, theproject teamhadplannedtouseanexperienceco-designapproach;howeverdue to real concernsaboutcross-infection risks forpatients, itwasnotpossible toholdapatientevent.Patientswerethereforeengagedthrough individual interviewsand face-to-facemeetingswithamemberoftheprojectteam.Staffwereengagedthroughinterviewsandastaffevent.Throughtheseprocessestheninetechniquesweresharedanddiscussedandfivewereselectedtopilot.Thesewere ‘positioning’, ‘pursed lipbreathing’, ‘handheldfan’, ‘relaxation’ and ‘diaphragmatic breathing’. Each project team member chose atechniquetopilotintheirclinicalareaanddevelopedinformationandresourcestosupportthis.Feedbackwascollectedfromatleastfivepatientsusingeachofthetechniques.Overallpatientswerepositiveaboutallthetechniquesandmanysaidtheywouldrecommendthemtootherpatients.Theteamhavedevelopedatoolkittosharethesetechniquesacrossthedirectorate and areworkingmore closelywith thewidermultidisciplinary team to createopportunitiesforlearningabouttheminstaffworkshops.
ThisprojectwassupportedbytheFoNSPracticeBasedDevelopmentandResearchProgrammeinpartnershipwiththeGeneralNursingCouncilforEnglandandWalesTrust.

2
Background
The respiratory directorate at Royal Brompton Hospital is comprised of three inpatientwards-twowardsprovidinglevel1andlevel2care,includingafivebeddedhighdependentunit (HDU ); one day care unit; a bronchoscopy suite with three recovery beds; and anoutpatientdepartment.
Thedirectorateprovidescareforpatientswithawiderangeofconditionsincludingsevereasthma, cystic fibrosis, interstitial lung disease, host defence disease (infection andbronchiectasis), lung failure, neuromuscular lung disorders e.g. motor neurone disease,duchene muscular dystrophy and kyphoscoliosis, chronic obstructive pulmonary disease(COPD),sleepdisorderedbreathing.Allthesepatientsrequirecomplexandspecialistcare.
Lindwardhasafive-day,shortstaywardforambulantpatientsundergoingassessmentandinvestigationsfortreatment.Italsohasabusydayunitwherepatientsattendforcomplexmulti-professional review and treatment including I.V. and subcutaneous therapy and abronchoscopyinterventionistsuite.Around150-180patientsareseeneachweek.Specialistnursinginputisprovidedbythenursingteamsandclinicalnursespecialists.
Foulis ward is a 35 bedded unit with 28 single rooms where patients with a range ofcomplexrespiratoryconditionsarecaredfor.ItisthelargestcysticfibrosisunitintheUK.Itprovides162nursinghoursovera24hourday.
Victoriawardisa26beddedwardarrangedinbayswithasinglesideroom,afive-beddedhighdependencyunitandfoursingleroomsforsleepassessment.Thewardhasspecialistexpertise innon-invasiveventilationandcares forpatientswith large rangeof respiratoryconditions.135nursinghoursovera24hourdayisprovided.
Regardless of the care group, disease or stage of disease, patients receiving care in thisdirectoratefrequentlyexperiencebreathlessness.Formany,thetreatmentcanonlymakeasmalldifferenceandthebreathlessnesswillworsenastheirconditiondeteriorates(Brewis,1995;Chapmanetal.,2005). It isthereforeimportantforpatientstolearntomanagethissensation. According to Brewis (1995) breathlessness is a sensation or perception thatremainsnotoriouslydifficulttoquantify. It isacknowledgedasoneofthemostdistressingsymptoms(Bauseweinetal.,2010,BoothandWade,2002).Brewis(1995)alsocommentedthatanxiety canworsenbreathlessnessand itsexperience.Therearehowevera rangeofnon-medical and non pharmacological management strategies that can be employed forexample, acupuncture/ acupressure, music, relaxation, walking aids, chest wall vibration,neuromuscular electrical stimulation, fan therapy, counselling and support, breathingtraining, case management or psychotherapy (Bausewein, et al., 2008). Nurses shouldconsider therefore a toolkit of strategies to sharewith patients to assist them in findingwaysthattheycanbestmanagetheirfeelingsofbreathlessness.
A snap shot audit was conducted in the trust involving attendees/admissions to therespiratorymedicinedepartmentsattheRoyalBromptonHospitalonMarch2014.Ofthe41patients, 93% reported that theywerebreathless sometimesand29%werebreathlessat

3
the time of attendance/admission to the departments. Reviewing the results of the datacollected,itwasclearthatthispatientgroupwerestrugglingwiththisdebilitatingsymptomof their disease process. This was despite using medical interventions such as oxygentherapy, inhaledandororalmedication. It seemedthatvery fewpatientshadanycopingstrategies beyond being outside to catch fresh air, resting, and using oxygen and inhaledmedicine.Thissuggestedthatpatientswerenotawareofotherstrategies,werenotabletousethem,orthattheydidnotfindthemeffective.Theauditpromptedtheprojectteamtoreflect on how they could help patients to reduce the unpleasant sensation ofbreathlessnessusingnon-medicaltechniquesinadditiontotheirmedicaltherapy.Aprojectwasthereforedevelopedtocreateatoolkitofnon-medicalinterventionsforpatientsandtosupport nurses in implementing these strategies. The project was discussed with therespiratorymedicalconsultantswhogavetheirsupport.
ProjectTeam
The initial teamconsistedof sixmembers:Matron,MandySimpsonas theproject leader;and five project team members; Charge Nurse, Paul Lidgate; Practice Educator, VijayLutchmee;SeniorStaffNurse/PracticeFacilitator,AnnammaWilson;DeputySister,CatarinaTexeira; and Clinical Nurse Specialist, Lucy Pigrim. Throughout the course of the projectseveralmembersoftheteamleftforvariousreasonsandtherewerechanges inpostsforotherteammembers.Currentlytherearefourmembersoftheoriginal team,withoneofthose on long-term leave. The project leader is now Senior Nurse/Matron, Paul Lidgate,supportedbyPracticeEducators,VijayLutchmeeandAnnammaWilson.
ProjectAimandObjectives
Theaimofthisprojectwastoimplementatoolkitofnon-medicalinterventionsthatcanbeusedalongsidemedicalmanagementtohelpreducebreathlessness.
Toachievethisaim,anumberofobjectiveswereidentified.
Objectives
• Reviewtheliteraturetoidentifynon-medicalinterventionstoreducebreathlessness• Engagestaffandpatientstoidentifymostpopularinterventions/keyinterventionsto
bepiloted• Pilotinterventionswiththepatients• Developatoolkittosuuprtwiderimplementation• Exploreopportunitiesforimplementationacrossrespiratorydirectorate

4
MethodsandApproaches
Initially,theprojectgrouphadintendedtouseanexperiencebasedco-designapproach,sothat the toolkit could be developed in collaboration with patients and staff; however, itbecame apparent that this approach was impractical due to the significant risk of crossinfection within the patient groups. A service improvement approach had thereforeadopted,usingalternativemethodstoengagepatientsonanindividualbasis.
Asthiswasaserviceimprovementproject,formalethicalapprovalwasnotrequired;howevertheprojectwasregisteredwiththetrust’sauditregistry.
Anumberofmethodsandapproacheswereusedintheproject;theseareoutlinedinTable1andwillbediscussedindetailbelow.
Table1:SummaryofProjectMethods
ProjectStages MethodsStage1:Literaturesearch(March2014-April2014)
Aliteraturesearchwasconductedtoidentifynon-medical interventions to relievebreathlessness
Stage2:Initialpatientandstaffinterviews(June2014–July2014)
Development of interview/topic guide andconsentform15interviewsconductedIdentificationofcommonthemes
Stage3:Eventsheld(StaffandPatient)(October2014–November2014)
A staff event was held to introduce theprojectandtoinvitestafftoselecttheirtopfivetechniquesMitigating the risk of cross infection forpatients, the ‘patient event’ involved theprojectteamaskingpatientstovotefortheirtopfivetechniquesindividually
Stage4:Interventionspiloted(March2014–July2014)
Individual members of the project teamchoseoneinterventioneachtopilotintheirclinicalareas
Stage 5: Review of interventions andredesign(March2015–July2015)
The toolkit was designed. This includedappropriate resources for teaching thetechniques.Deputysisters,matron,practiceeducatorshelpedtoimplementthetoolkit.
5
LiteratureSearch
A literature search was undertaken to identify evidence of non-medical interventions torelievebreathlessness.Thesearchstrategyinvolved:
• AsearchofPubMeddatabase• Usingtheterm‘dyspnoeamanagement’• With the additional filters of – publishedwithin last five years,written in English,
articlesonhumanbeings
1260 articleswere identified. Thesewere divided amongst the project teammembers toreview and to identify the papers which were relevant to the project i.e. non-medicalinterventions.Eachmemberreviewedtheirallocatedliteraturesearchunderthesetcriteria.Thesewerediscussedbytheprojectteamtoidentifyexclusioncriteria.Itwasdecidedthatthefollowingshouldbeexcluded:
• Any intervention thatwas already being used by another teamwithin thetrust-thiswasTaichiandreflexology
• Theinterventionsthatneededspecialistinput/equipmente.g.acupuncture,acutens,acupressure,alternatenosebreathingetc.
Overall,theliteratureevidenceonusingnon-medicalinterventionstorelievebreathlessnesswas limited, with most of the research evidence was associated with patients with lungcancer.However, therewas some research available that showedpositive support of thefollowinginterventions.Overall14paperswerefounduseful;thesewillbediscussedbelow.
LiteratureReviewFindings
Barnes (2010) documented that effective treatment of breathlessness begins with acomprehensive assessment, which includes full medical history, examination andinvestigations. According to Laviolette and Laveneziana (2014) dyspnoea is a debilitatingsymptom that affects patient’s quality of life, exercise endurance and mortality. Theliterature identifies thatbreathlessness isacomplexandcommonlysymptomreportedbypatients with chronic respiratory problems. The team recognised that as a specialistrespiratory hospital, it is important that staff are able to help patients self-manage theirbreathlessness, alleviate or reduce breathlessness andmoreover improve their quality oflife.
Asummaryoftheliteratureisprovidedbelow:
• ACochranereviewbyHollandetal.(2012)showedthatbreathingexercisessuchasdiaphragmatic breathing (DB), pursed lipped breathing (PLB), pranayama yogabreathing(timedbreathingwithafocusonexhalation) inpatientswithCOPDwereconsidered safe to be used. These exercises showed improvement in a sixminutewalk test but the evidence on shortness of breath/dyspnoea and wellbeing werevariable, in fact it showed no consistent effect on dyspnoea. This review
6
documentedthatbreathingexercisesover4-15weeksimprovedfunctionalexercisecapacityinpeoplewithCOPDcomparedtonointervention
• Milgoreetal.(2005)provedthatPLB,breathingretraining,compensatorypostures(combining breathing techniques and activity training work) directly optimisephysicalfunction.Aneffectofthisisreductionofdyspnoearelatedanxiety
• Corneretal.(1996)conductedapilotrandomisedcontrolledtrialandlookedatnonpharmacological interventions for breathlessness in lung cancer patients, theresearchers used ‘nurse led clinical interventions’ or ‘best supportive care’. Thenursepractitionerprovidedcounselling,breathingre-training,taughtrelaxationandcoping strategies for three-sixweeks. This study showed that the nurse led groupexperienced significant reduction in perception of breathlessness and distresscaused by breathlessness, therefore improvement in breathlessness at worst(p=0.02)andfunctionalcapacity(p=0.03)
• A literature review by Facchiano et al. (2011) strongly suggested that regularlypracticedPLB isaneffectiveself-managementtechniqueforpatientswithCOPDtoimprovetheirdyspnoea
• A RCT by Louise (2004) demonstrated that a ‘guided imagery’ technique forrelaxationusedforpatientswithbreathlessnessandCOPDfoundsignificantincreaseinoxygensaturations
• Zhao and Yates (2008) conducted a literature reviewof non-medical interventionsforbreathlessnessinpatientswithlungcancerandconcludedthatthesetechniquesareusefulbutnotveryusefulwhenthefunctionalcapacitiesofpatientsarealreadyaffected.Theyalsosuggestedthatmultiplestrategiescouldbeusedaccordingtothepatient’s needs such as using different techniques in conjunction, like relaxation,PLB, handheld fans etc. This suggests that a package of care tailored to individualneedmaybemorepreferable,somethingwhichatoolkitmightbeabletoaddress
• Moore et al. (2002) showed that a nurse led follow up intervention service toconventionalmedicalfollowupshowedsignificantimprovementindyspnoearatingbypatientsusingavisualanaloguescale.ThisresultwasstrengthenedbyastudybyHatelyetal.(2003),whichalsoshowedsignificantimprovementindyspnoeascoresafterinterventionssuchasbreathingcontrol,relaxationandenergyconservation
• An exploratory study by Dellon et al. (2010) documented that themost commonsymptomsexperiencedby80%ofpatientswithcystic fibrosis in their lastweekoflife is dyspnoea and fatigue andmore than 50% of patients suffer with pain andanxiety.Thisstudyshowedthatmanyfamilymembersandcaregivershadaverylowexpectationofsymptomcontrol.Thiswasquitearevealingpieceofresearch,astheproject teamhad always thought that the directoratewere good at controlling ormanagingsymptoms.Thismadetheteamthinkthattherewereopportunitiestodomorethanwhatisoccurringatthepresenttime
• Kamaletal.(2012)suggestedinhisreviewthatasimplenon-medicalinterventionofusingahandheldfantorelievedyspnoea issafeandcosteffective.Galbraithetal.(2010)conductedarandomisedcontrolledcrossovertrial,whereahandheldelectricfan was directed towards face versus towards the leg for five minutes, showed
7
improvement indyspnoeawhen itwasdirected towards the face.Theparticipantswereinanadvancedstageoftheirdiseaseconditionbutwerenotonsupplementaryoxygen
• Booth et al. (2011)wrote a review based on evidence provided in the systematicliterature review by Bausewein et al. (2008) and identified the techniques whichshowedevidence to support their use in breathlessness. The techniqueswereDB,PLB, handheld fans, breathing control, positioning, activity pacing and energyconservation,walkingaids,anxietyreductionetc.
In summary, this review of the literature challenged the project team’s beliefs that theywere good at controlling or managing symptoms for patients and identified theopportunitiestodomore.Thissupportedtheideafordevelopingpackagesofcaretailoredtoindividualneeds,somethingwhicha‘toolkit’ofnon-medicalinterventionsmightbeabletoaddress.
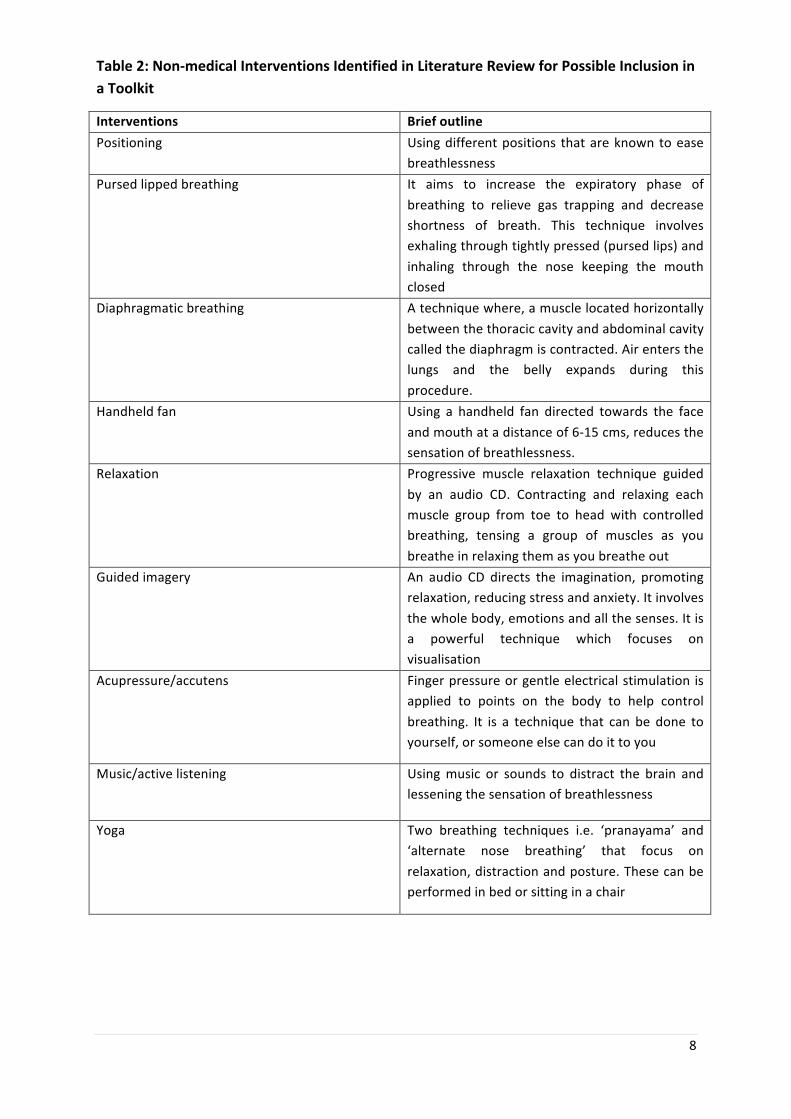
Informedby the literature review, theprojectgroup initiallydiscussed17 interventions indetailandcametoaconclusionthattherewereonlyninetechniqueswhichwererelevanttotheirpatientgroupsandwhichshouldbeconsideredforinclusioninthetoolkit(seeTable2).
8
Table2:Non-medicalInterventionsIdentifiedinLiteratureReviewforPossibleInclusioninaToolkit
Interventions BriefoutlinePositioning Usingdifferentpositions thatareknowntoease
breathlessnessPursedlippedbreathing It aims to increase the expiratory phase of
breathing to relieve gas trapping and decreaseshortness of breath. This technique involvesexhalingthroughtightlypressed(pursedlips)andinhaling through the nose keeping the mouthclosed
Diaphragmaticbreathing Atechniquewhere,amusclelocatedhorizontallybetweenthethoraciccavityandabdominalcavitycalledthediaphragmiscontracted.Airentersthelungs and the belly expands during thisprocedure.
Handheldfan Using a handheld fan directed towards the faceandmouthatadistanceof6-15cms,reducesthesensationofbreathlessness.
Relaxation Progressive muscle relaxation technique guidedby an audio CD. Contracting and relaxing eachmuscle group from toe to head with controlledbreathing, tensing a group of muscles as youbreatheinrelaxingthemasyoubreatheout
Guidedimagery An audio CD directs the imagination, promotingrelaxation,reducingstressandanxiety.Itinvolvesthewholebody,emotionsandallthesenses.Itisa powerful technique which focuses onvisualisation
Acupressure/accutens Fingerpressureorgentleelectricalstimulation isapplied to points on the body to help controlbreathing. It is a technique that can be done toyourself,orsomeoneelsecandoittoyou
Music/activelistening Usingmusic or sounds to distract the brain andlesseningthesensationofbreathlessness
Yoga Two breathing techniques i.e. ‘pranayama’ and‘alternate nose breathing’ that focus onrelaxation,distractionandposture.Thesecanbeperformedinbedorsittinginachair

9
PatientandStaffInterviews
Followingthe identificationofthenine interventions, theprojectteamplannedtoengagewithpatientsandstafftoexploretheirexperienceofusingtheseapproaches.Thiswouldbeuseful to identify the benefits and the reasonswhy they thought these techniqueswerehelpful. Through this process, the team planned to identify which techniques should bepiloted,theteamselectednineinterventionsoutofwhichacupressure/accutensewasalsoa technique.Althoughweoriginally saidwewouldnot selectany techniques thatneededspecialist input, we decided to include this technique, on the understanding that if ourparticipantsvotedforthistechnique,thenwewouldhavetolearnthistechniqueourselvesandteachothers.Originally the teamhadhopedtoholdanevent includingbothpatientsand staff, where the interventions could be shared and discussed together. However, itbecameapparentthatthiswouldnotbepossibleduetotherisksofinfectionforpatients.Theteamthereforedecidedtoconductindividualinterviewswithpatientsandstaff.
Atopic/interviewguidewasdevelopedbytheprojectteamforthepurposeofinterviewingthepatientsandstaff.Theguideencouragedparticipantstotalkaboutthetechniquestheyusedtomanagebreathlessness.Therewasthenanopportunity togainparticipantsviewsontheninetechniquesthathadbeenselected.Fivemembersoftheteamweresupposedtointerview, but 2 members left the trust for different reasons, only 3 members could dointerviewsandtheyinterviewed12participantstheseincluded;patients(10),consultant(1)andwardnurse(1).Apurposiveapproachwasusedtorecruit interviewparticipants.Eachsteeringgroupmemberapproachedpossibleparticipantsonthedaytheywerescheduledto interview, randomly selecting people who were either patients who experiencebreathlessness or staff members who were treating patients with breathlessness. Thepurposeoftheinterviewwasexplainedfullytopatientsandstaffandtheirwrittenconsenttoparticipatewasobtained.The interviewswereaudiotaped.The interviewswere storedon trust computers which were encrypted by passwords to maintain confidentiality. Allinterviewsweretranscribedandtomaintaintheanonymityof theparticipants, theyweregivennamessuchas‘ParticipantA/B/C’.
The interviews provided descriptive accounts of why patients used non-medicalinterventions to relieve breathlessness. It also identified which techniques were morebeneficialforthoseparticularparticipants.Someoftheparticipants’strategiesresonatedtothetechniquesfoundfromtheliteraturereview.Thetranscriptswerereadbyalltheprojectteam members individually and then we came together to discuss them and identifiedcommonthemes.Someofthethemeswhichemergedwere:
• Positioning• Controllingandcalmingdowntheirbreathlessness• ShallowbreathingtechniquebyButeko• Stopdoingthings• Sitquietly,concentrateandfocusonbreathing• Knowwhatmakesyoubreathless• Reflexology

10
• Reducepanicsituations• Gosomewherequiet• Qi-gong
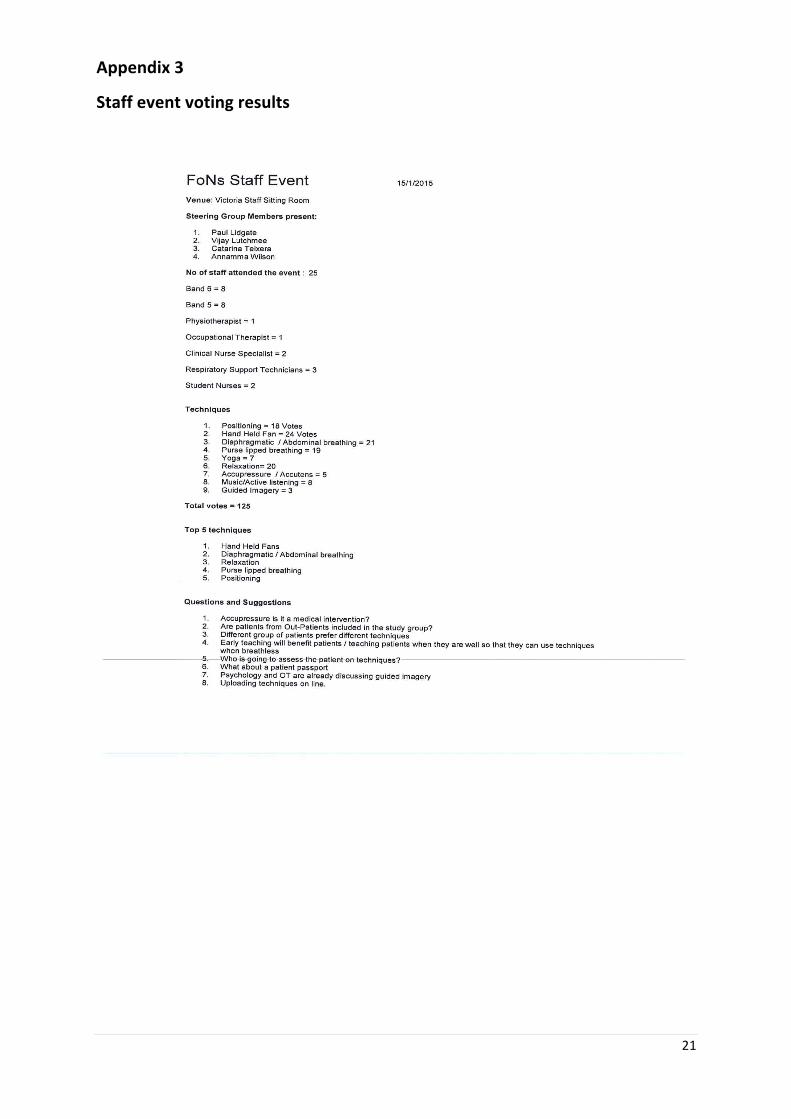
These identified themes informed theprojectgreatlyasmostof the techniqueswere thesameasthosethattheprojectteamidentifiedintheliteraturereview.Thisgaveuspositivefeedbackthatweweregoingintherightdirection.Thenextphaseoftheprojectwasstaffandpatientevents.The‘staffevent’wasattendedbynurses,physiotherapists,occupationaltherapists, respiratory technicians and students. A posterwas produced and displayed indifferentclinicalareastoinvitestaffmemberstoattendtheevent.Attheeventparticipantswere given a brief summary of the project via PowerPoint presentation and the projectgroup introduced themselvesandansweredanyquestions staffhad regarding theprojectand the interventions identified.Participantswere thengiven fivestickynotes tovote fortheir topfivetechniques.Thetotalnumberofstaffmembersattendingtheeventwas25,which included eight band 6 nurses, eight band 5 nurses, one physiotherapist, oneoccupational therapist, twoclinicalnursespecialists, three respiratory support techniciansand two student nurses. The results of the voting are summarised in Table 3 and thedetaileddatashowninAppendix3.
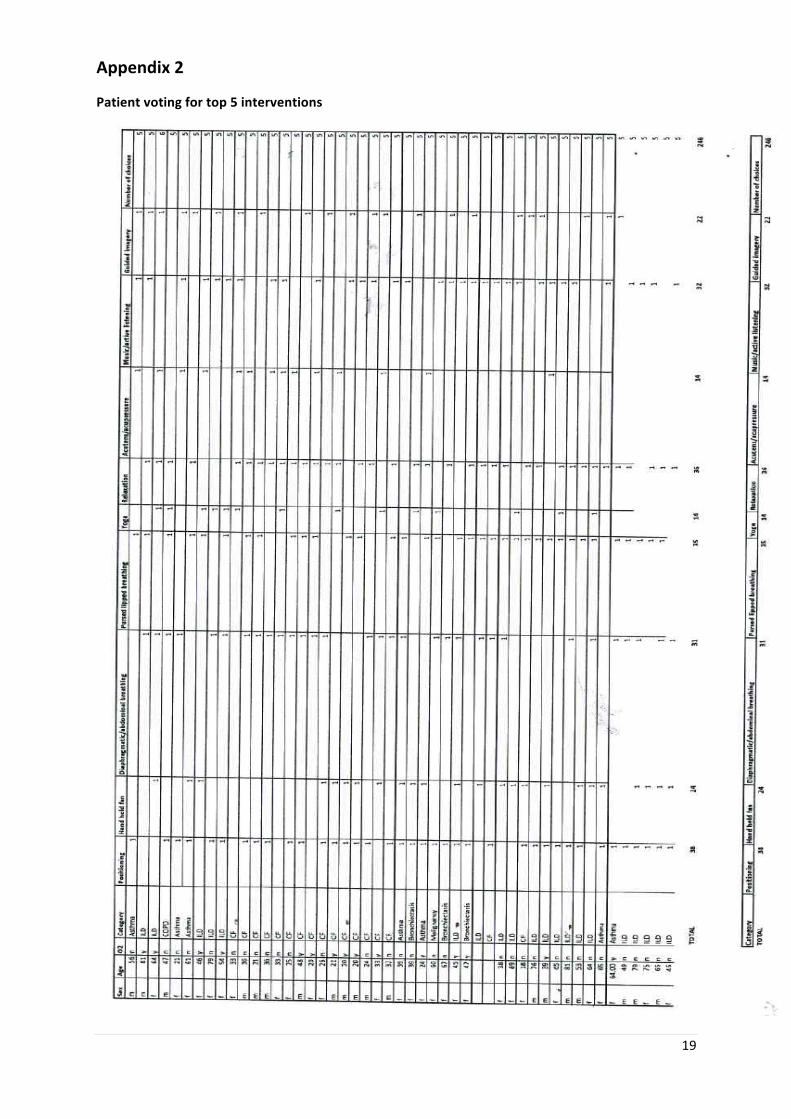
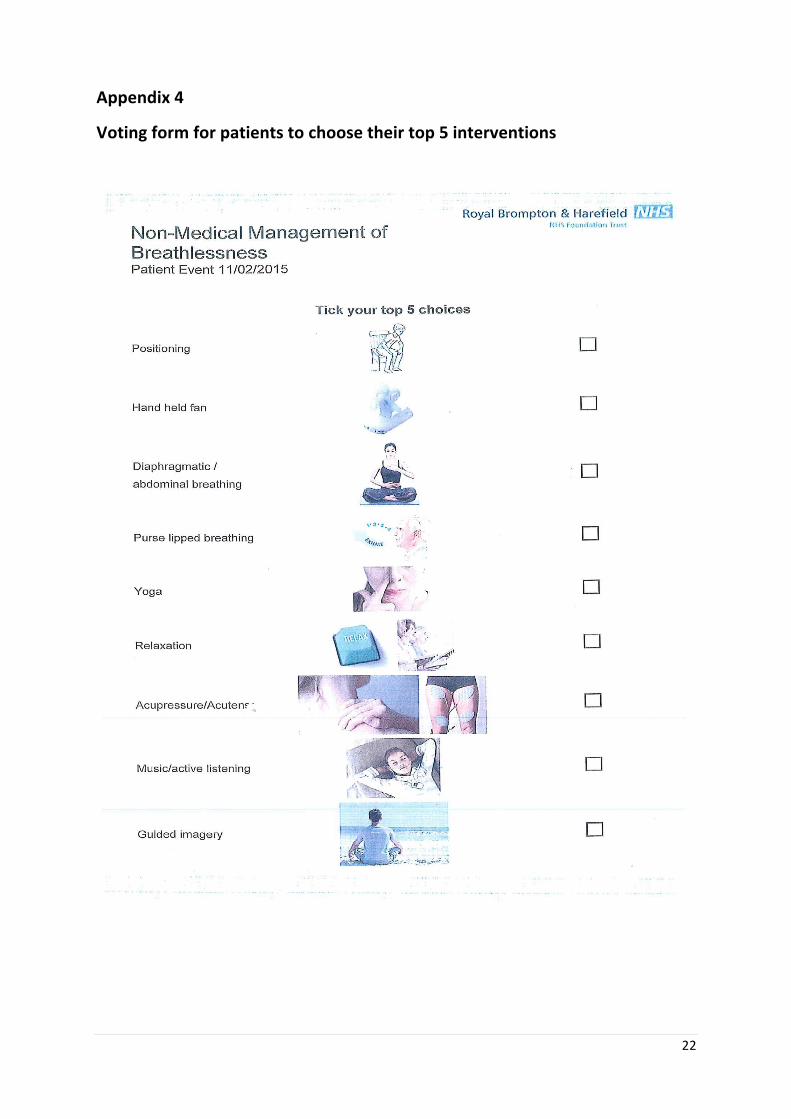
Aspreviouslyidentifieda‘PatientEvent’couldnotbearrangedbecauseofinfectioncontrolconstraints. The project team therefore decided to approach patients individually, givingthemanoverviewofwhattheprojectwasallabout,andaskingthemtovotefortheirtopfivetechniques.Againapurposiveapproachwasusedtoselectpatientsonthedayofthe‘event’ that would be helpful to the project i.e. those patients who experiencebreathlessness.Theparticipantsweregivenavotingform(seeAppendix4)andtheywereasked to choose their top five interventions. Their votes are captured in Table 3 and thedetaileddatashowninAppendix2.
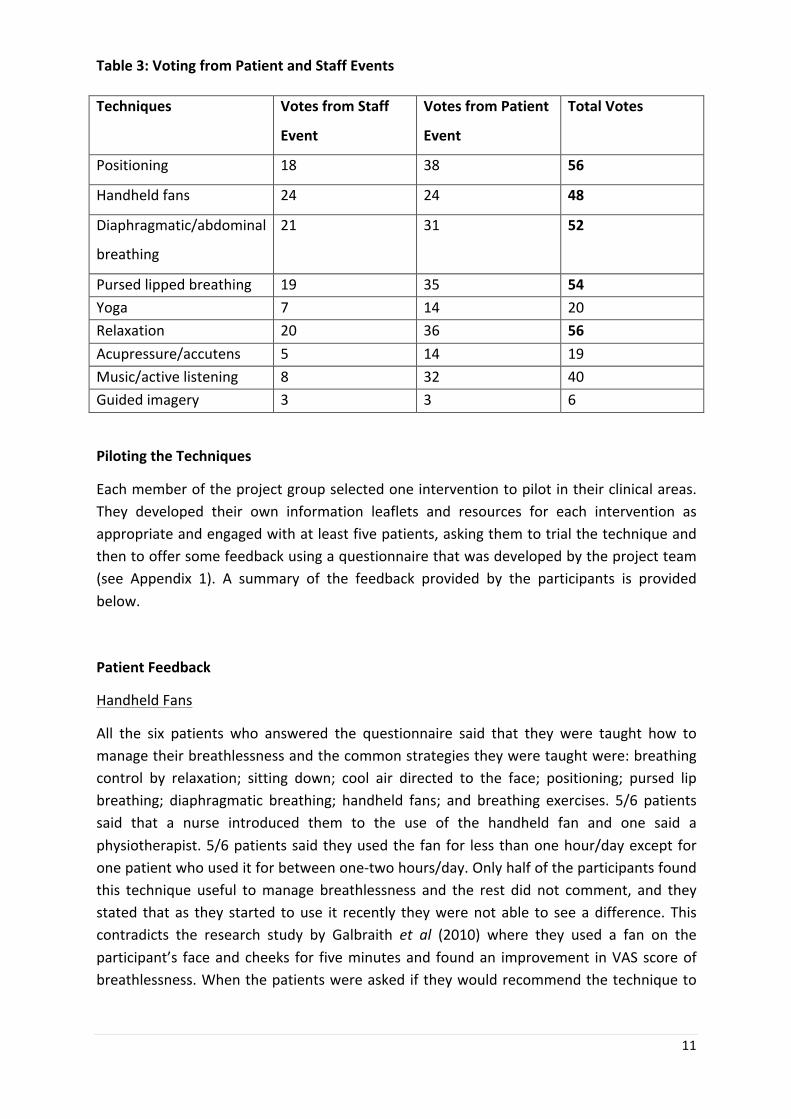
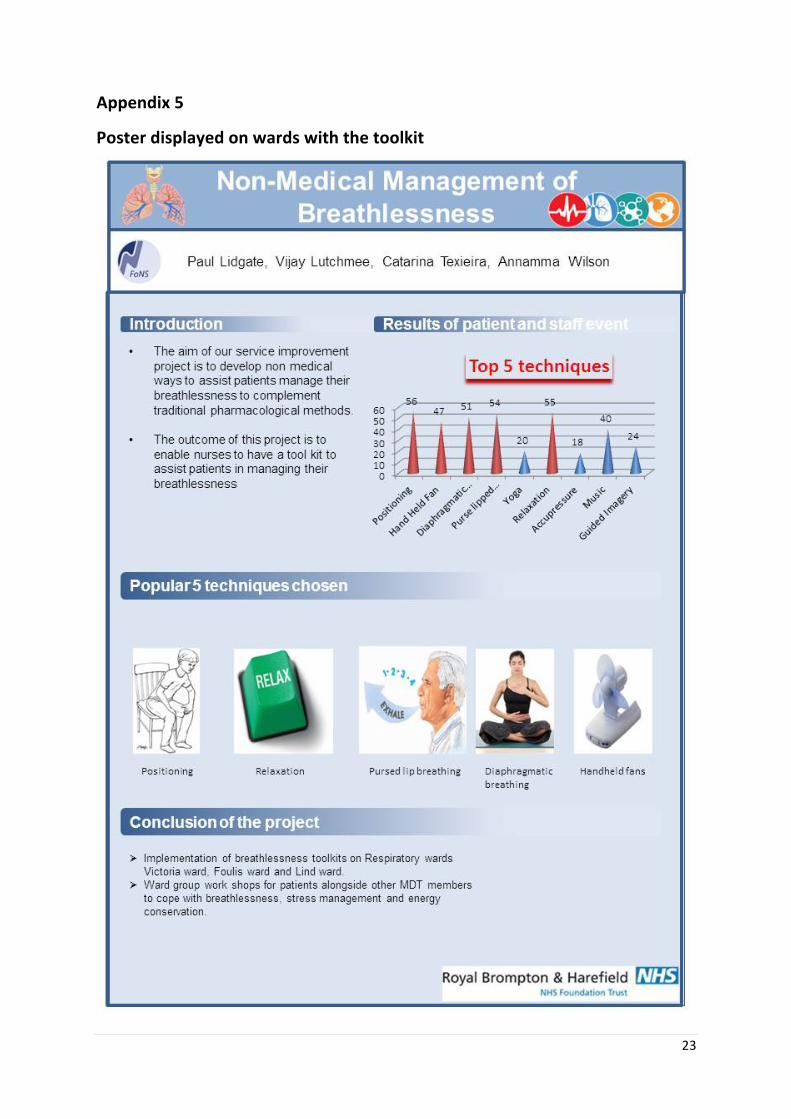
Thecombinedtopfivetechniqueschosenbystaffandpatientswere ‘positioning’, ‘pursedlipbreathing’,‘handheldfan’,‘relaxation’and‘diaphragmaticbreathing’.
11
Table3:VotingfromPatientandStaffEvents
Techniques VotesfromStaff
Event
VotesfromPatient
Event
TotalVotes
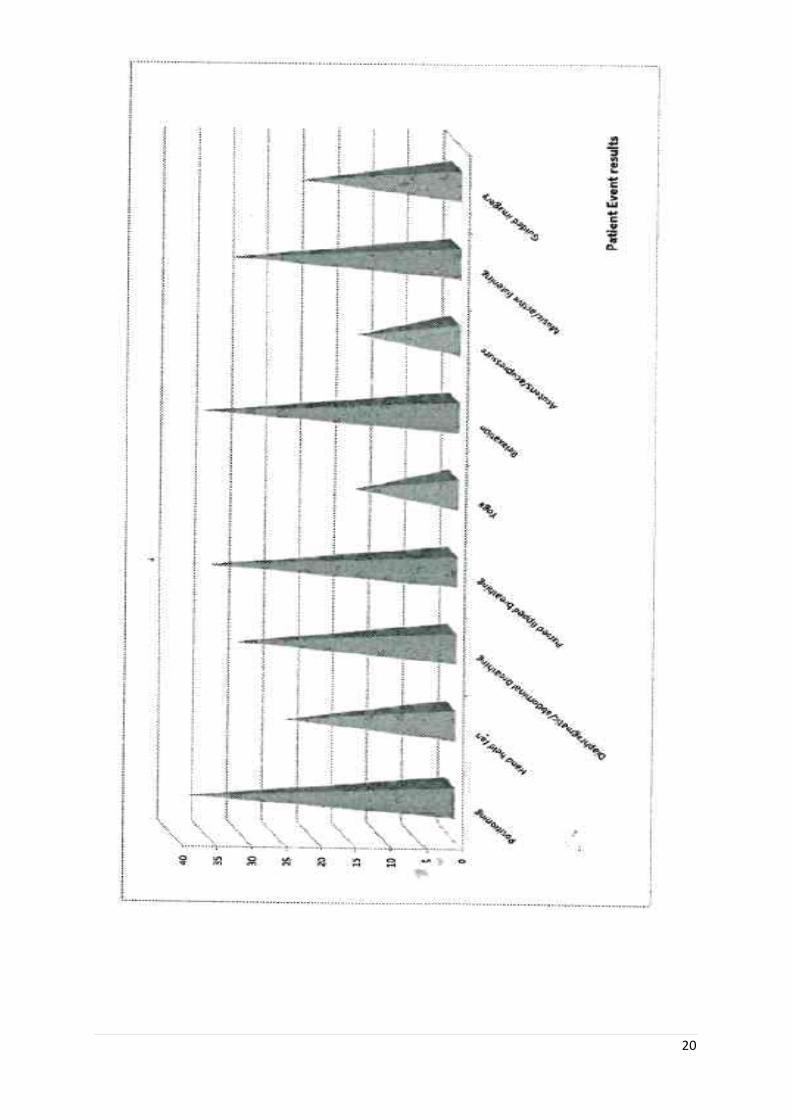
Positioning 18 38 56
Handheldfans 24 24 48
Diaphragmatic/abdominal
breathing
21 31 52
Pursedlippedbreathing 19 35 54Yoga 7 14 20Relaxation 20 36 56Acupressure/accutens 5 14 19Music/activelistening 8 32 40Guidedimagery 3 3 6
PilotingtheTechniques
Eachmemberoftheprojectgroupselectedoneinterventiontopilotintheirclinicalareas.They developed their own information leaflets and resources for each intervention asappropriateandengagedwithatleastfivepatients,askingthemtotrialthetechniqueandthentooffersomefeedbackusingaquestionnairethatwasdevelopedbytheprojectteam(see Appendix 1). A summary of the feedback provided by the participants is providedbelow.
PatientFeedback
HandheldFans
All the six patients who answered the questionnaire said that they were taught how tomanagetheirbreathlessnessandthecommonstrategiestheyweretaughtwere:breathingcontrol by relaxation; sitting down; cool air directed to the face; positioning; pursed lipbreathing; diaphragmatic breathing; handheld fans; and breathing exercises. 5/6 patientssaid that a nurse introduced them to the use of the handheld fan and one said aphysiotherapist.5/6patientssaidtheyusedthefanfor lessthanonehour/dayexcept foronepatientwhouseditforbetweenone-twohours/day.Onlyhalfoftheparticipantsfoundthis technique useful tomanage breathlessness and the rest did not comment, and theystated that as they started touse it recently theywerenotable to seeadifference. Thiscontradicts the research study by Galbraith et al (2010) where they used a fan on theparticipant’s faceandcheeks for fiveminutesand foundan improvement inVASscoreofbreathlessness.Whenthepatientswereaskediftheywouldrecommendthetechniqueto

12
others,mostofthepatientssaid‘yes’,exceptonepatientwhosaid‘no’becausethepersonwasundecidedifthetoolwouldhelp.
Relaxation
Most of the patients (4/5) answered that they were taught how to manage theirbreathlessnessandsomeof thestrategies theyusedwerebreathingexercises, relaxation,yogaandabdominalbreathing;onepatientwasnottaughtanystrategies.Whenaskedwhotaughtthemtouserelaxation,thenthemajorityidentifiedthenurse;butsomementionedmulti-disciplinary teammembers including the physiotherapist and doctor.Most of themcommentedthattheywereinstructedonhowtousetherelaxationtechniqueexceptone,who mentioned that no instructions were provided for the technique. 3/5 patientsmentionedthattheyusedthistechniqueforlessthanonehour/day;onepatientuseditforbetweenone-twohours/dayandonepatientdidnotcomment.Uponasking iftheyfoundrelaxation helpful to relieve breathlessness, 3/5 responded they did, and 100% of thepatientssaidtheywouldrecommendthistoanotherpatient.
Diaphragmatic/AbdominalBreathing
4/5patientsdocumented that theywere taughtmanagementof theirbreathlessnessandthetechniquestheyweretaughtweresimilartothepatientsabove.Forthistechnique2/5patients said the nurse talked to them about the technique, although one patient saidmultiplemembersoftheteamintroducedthistechniqueandonepatientdidnotcomment.3/5ofthepatientsusedthistechniquebetweenone-twohours/day,onesaidtheyuseditforlessthanonehour/dayandonepatientdidnotcomment.Uponaskingiftheyfoundthistechniqueuseful,4/5patientssaidyesandonedidnotcomment.4/5ofthesepatientssaidthattheywouldrecommendthistechniquetoanotherpatient.
Positioning
4/5of this groupofpatientswhoweregiven feedback formscommented that theyweretaughthowtomanagetheirbreathlessness,andthetechniquestheyusedwerethesameasabove except some additional techniques such as Tai Chi, weight management andimproving fitness. 3/5 of the patients commented that physiotherapists demonstratedpositioning for breathlessness and two patients documented that the nurse explainedpositioning.Themajorityofthepatientswere instructedhowtousedifferentpositionstorelieve breathlessness. Enquiring about how often they used positioning, 2/5 patientscommentedthattheyuseditvariabletimesaccordingtotheirbreathlessness,onepatientdidnotcomment,onesaidbetweenone-twohours/dayandanothercommentedtwo-fourhours/day.4/5patientsmentionedthatpositioningwasusefulinmanagingbreathlessnessandthattheywouldrecommendittoanotherpatient.
Pursedlippedbreathing
4/5 of this group of respondents commented that they were taught to manage theirbreathlessness. The strategies they mentioned were more or less similar to what othergroups mentioned such as pursed lip breathing, wearing loose clothings, positioning,

13
relaxation, pacing, and diaphragmatic breathing. Upon asking the participants aboutwhoshowed them this technique in past then they mentioned physiotherapists, doctors andmembers of family, and no-onementioned nurses taught them this technique. But theywere all shown this technique by the nurse who collected the questionnaires. All therespondentsmetionedvariabletimestheyhaveusedthistechnique,butallofthemfoundthistechniqueusefulandsaidtheywouldrecommendittoothers.
Summary
Theoveralloutcomeofthefeedbackfromthepatientswasthatthemajorityofthemhadbeenshownhowtomanagetheirbreathlessness.Thisfeedbackhighlightedthatmembersofthemultidisciplinaryteamhaveanimportantroletoplayinhelpingpatientstoidentifyatechnique that is beneficial for them.Upon realisation of this fact, the project teammetwith the occupational therapist and psychologists who were getting together to arrangeworkshops for respiratory patients for different issues such as stress management,relaxation, energy conservation etc. The project team intend towork in partnershipwiththemandhope to contribute to theirworkshops so that the toolkit canbe introducedasthereisanoverlapandsynegywithinbothprojects.
The five interventions that were piloted were well accepted and patients were keen onusing them tomanage their breathlessness.Moreover, themajority of them commentedthattheywouldactuallyrecommendthemtoanotherpatient.
Basedontheliterature,staffandpatientfeedback,theprojectteamhasproducedatoolkit,which is a box with information leaflets about handheld fans, pursed lipped breathing,positioning,relaxationanddiaphragmaticbreathingandalsohandheldfans.Thetoolkitboxis placed in clinical areaswith a poster (seeAppendix 5) to demonstratewhat thebox isabout andhowwas thebox created. In addition, resources areprovided ineachward tosupport the implementationof these techniques.Theprocessof implementing the toolkitwillallowustoteachthenursestheseinterventionswhowillinturnteachthepatientsandtheir carers. In futureweaspire to setupabreathlessness clinic for inpatients aswell asoutpatients. Thewardmanagers, deputy nurses and the practice educatorswill be giveneducationontheuseoftoolkitandtheywillinturneducatenursesonthewardstousethetoolkit inneed.One toone teachingwillbearrangedand teachingsessions in respiratoryteamdaystudydayswillensureongoingeducationisgiventonursesregardinguseofnon-medicalinterventions.
ReflectionsoftheProjectTeam
On reflection of thewhole journey of this project, the team can confidently say thatwehavemet our aim of implementing a toolkit of non-medical interventions for respiratorypatientstohelprelievetheirbreathlessness.Thiswasalearningopportunityfortheteamaswell,aswebecamemoreconfidentininterviewingpeople,organisingeventsandcollecting
14
data.Thematicallyanalysingtheinterviewsandwritingthereportoftheprojecthavealsohelpedtheteamdeveloptogether.
Whatwentwell?
Wegatheredagoodteamwithabreadthofknowledgeandexperienceaboutrespiratorydisease, indifferentspecialitiessuchasasthma,interstitial lungdiseaseandcysticfibrosis.Theteamwasveryenthusiasticaboutusingthe‘experiencebasedco-design’methodologybecause onemember of teamhad already used thismethodology previously for anotherproject.Weweredisappointedthatwecouldnotfollowthisapproachfullyduetoinfectioncontrolriskbutontheotherhandweregladthatweinvestedtimetoexplorethisstrategyand followedsomeaspectsof it.Wescheduledmeetingseverymonth tokeepa trackontheprogress.Wehadgoodadministrativesupporttoarrangemeetings.Themajorityofourpatientsarebreathlesstovaringdegreessotheywereallquitehappytotryanythingtohelpwith this symptomandwebelieve that this is the reasonourpatientsandstaffmembersparticipatedwellintheproject.
Whatwentwrong?
Aswedisclosedearlier,membersoftheprojectteamleftandsointheend,theremainingthree members did the majority of work for the project, especially the practicalimplementationaspectofthetoolkit.Theclinicalareasallhavehighpressuredactivityandtime is restricted. The projectworkloadwas redistributed to those left in the group.WecompromisedtheEBCDapproachaswerealisedlateronlythatourpatientscouldnotmixwitheachotherdueto infectioncontrolprotocolandadaptedthebestwecould. Duetostaffingitwasnotpossibletoalwaysbackfilltheprojectteammemberspoststofacilitateasmuch inwork timeaswewouldhavehoped. Thegroupat timesdidnotmeet stagedtargetsasplanned.
Whatwouldyoudodifferently?
Thinkingabout futurework, thegroupwouldrecommendrecruitinga largerproject teamwithwardlinknursesupportandconsistentadministrativesupport.Anotheraspectisthat,theproject leadershouldensureall themembersof theproject teamarereallywillingtocommittotheproject.Wewouldalsoseeksupportfromthecommunicationsdepartmentearlyintheproject.Themonthlymeetingsoccurred,butdidlosemomentumduetoclinicalpressures and became irregular midpoint through the project. This did not allow anyproblemsfacedbythememberstobediscussed,therefore,creatingfrustrationintheteamattimes.
Conclusion
Thisserviceimprovementprojectstartedwithasnapshotauditwhichshowedasignificantneedtoimprovetheserviceregardingbreathlessnessmanagementofrespiratorypatients.This ledateamofnursesto lookintonon-medical interventionstorelievebreathlessness.
15
Wegot supportand funding fromFoNS,whichgaveusmotivation to implementa toolkitwhichwillbetaughttopatientsbynursesandthewidermultidisciplinaryteam.
A literaturesearch led to the identificationof17 techniques,whichwasreduceddowntoninetechniques.TheteamwantedtouseanEBCDapproach,butcouldnotgoaheadwiththisapproachduetoissuesrelatingtoinfectioncontrol.Patientinterviewsmadeusrealisethattheywerewillingtotryalltheseninetechniques,andsotheywereaskedtoselecttheirtop five techniques. At a staff event they were also asked to vote for their top fivetechniquesandtheresultofthecombinedvoteswastheidentificationoffivetechniquestoinclude in a toolkit. These are positioning, pursed lipped breathing, relaxation, handheldfansandabdominalbreathing.
There were barriers to implementing these techniques such as high activity within thewards, staffing at times and project teammembers leaving. However, the team adaptedwellandmanagedtopilotthetechniquesandimplementatoolkit.Nursesaremadeawareofthistoolkitandtheseniormembersofthenursingteamareadvisedtocontinuewiththeteachingssothechangecanbesustained.
Recommendations
Whentheprojectteamembarkedontheproject,consideringthethemesidentifiedinthepatient/staff interviews and the result of literature search,we identified that our patientgroup could have benefitedwith somemodifications but as the approvalwas sought forimplementationofatoolkitfornon-medicalinterventionstomanagebreathlessness,itwasnot possible. Therefore we made some recommendations for future research/serviceimprovementprojects.Therecommendationsare:
• Reviewpatient feedback to identify if there is anypreferenceof interventionsperspeciality
• Involvemedicalteaminimplementingnon-medicalinterventions• Involve multidisciplinary team in amalgmating non-medical breathlessness
managementintheirworkshops
16
References
Barnes, D. (2010) Breathlessness in advanced disease 2: patient assessment andmanagement.NursingTimes.Vol.106.No.44.pp.12-14.
Bausewein, C., Booth, S., Gysels, M. and Higginson, I.J. (2008) Non-pharmacologicalinterventions for breathlessness in advanced stages of malignant and non-malignantdiseases.CochraneDatabaseofSystematicReviews:CD005623.
Bausewein,C.,Booth,S.,Gysels,M.,Kuhnbach,R.andHigginson,I.J.(2010)Effectivenessofahand-heldfanforbreathlessness:arandomisedphase2trial.BMCPalliativeCare.Vol.9.No. 22. Retrieved from: http://bmcpalliatcare.biomedcentral.com/articles/10.1186/1472-684X-9-22.(Lastaccessed18thOctober2016.)
Booth, S. andWade, R. (2003)Oxygen or air for palliation of breathlessness in advancedcancer.JournaloftheRoyalSocietyofMedicine.Vol.96.No.5.pp.215-218.
Booth,S.,Moffat,C.,Burkin,J.,Galbraith,S.andBausewein,C.(2011)Nonpharmacologicalinterventions forbreathlessness.CurrentOpinion inSupportiveandPalliativeCare.Vol.5.pp.77-86.
Brewis,R.A.L.(1995).RespiratoryMedicine.2ndeds.London:Saunders.
Chapman, S.J., Robinson, G., Stradling, J.R. and West, S. (2005) Oxford Handbook ofRespiratoryMedicine.NewYork:OxfordUniversityPress.
Corner, J., PlantH.,A’Hern,R. andBailey,C. (1996)Nonpharmacological intervention forbreathlessnessinLungcancer.PalliativeMedicine.Vol.10.No.4.pp.299-305.
Dellon, E.P., Shores, M.D., Nelson, K.I., et al. (2010) Family caregivers perspectives onsymptomsandtreatmentsforpatientsdyingfromcomplicationsofcysticfibrosis.JournalofPainandSymptomManagement.Vol.40.No.6.pp.829-837.
Facchiano, L., Hoffman, S.C. and Nunez, D.E. (2011) A literature review on breathingretrainingasaselfmanagementstrategyoperationalizedthroughRosswurmandLarrabee’sevidence based practicemodel. Journal of the American Academy of Nurse Practitioners.Vol.23.No.8.pp.421-426.
Galbraith, S., Perkins, P., Lynch, A. and Booth, S. (2010) Does the use of a handheld fanimprove chronic dyspnea? A randomised controlled Ccrossover trial. Journal of Pain andSymptomManagement.Vol.39.No.5.pp.831-838.
Hately, J., Laurence, V., Scott, A., Baker, R. and Thomas, P. (2003) Breathlessness clinicswithin specialist palliative care settings can improve the quality of life and functionalcapacityofpatientswithlungcancer.PalliativeMedicine.Vol.17.pp.410-417.
Holland,A.E.,Hill,C.J., Jones,A.Y.etal. (2012)Breathingexercises forchronicobstructivepulmonarydisease.CochraneDatabaseofSystematicReviews.10;CD008250.
17
Kamal,A.H.,Maguire,J.M.,Wheeler,J.L.,Currow,D.C.andAbernethy,A.P.(2012)Dyspneareviewforthepalliativecareprofessional:treatmentgoalsandtherapeuticoptions.JournalofPalliativeMedicine.Vol.15.No.1.pp.106-114.
Laviolette,L.andLaveneziana,P.(2014)Dyspnoea:amultidimensionalandmultidisciplinaryapproach.EuropeanRespiratoryJournal.Vol.43.No.6.pp.1750-1762.
Louie, S.W. (2004) The effects of guided imagery relaxation in people with COPD.OccupationalTherapyInternational.Vol.11.No.3.pp.145-159.
MiglioreNorweg,A.,Whiteson,J.,etal.(2005)Theeffectivenessofdifferentcombinationsofpulmonaryrehabilitationprogrammecomponents.Arandomisedcontrolledtrial.Chest.Vol.128.No.2.pp.663-672.
Moore,S.,Corner,J.,Haviland,J.etal.(2002)Nurseledfollowupandconventionalmedicalfollowupinmanagementofpatientswithlungcancer:randomisedtrial.BMJ.Vol.325.No.7373.pp.1145-1147.
Zhao, I. and Yates, P. (2008) Non-pharmacological interventions for breathlessnessmanagementinpatientswithlungcancer:asystematicreview.PalliativeMedicine.Vol.22.pp.693-670.
18
Appendix1
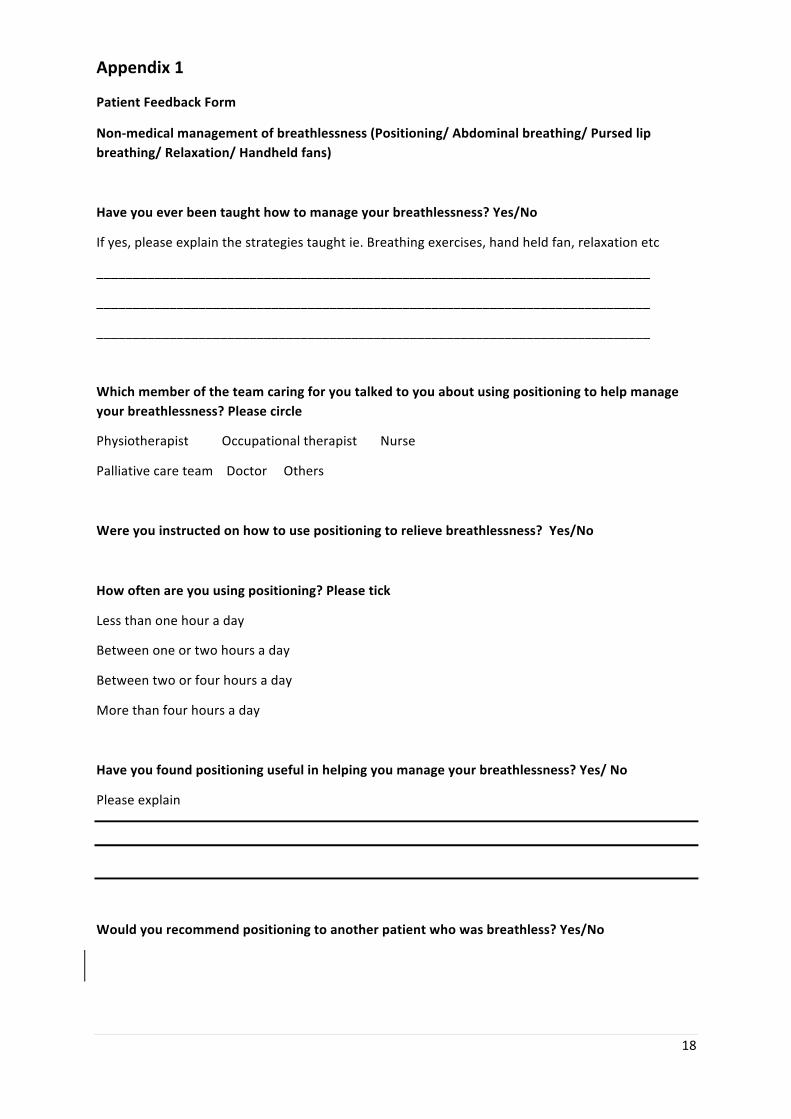
PatientFeedbackForm
Non-medicalmanagementofbreathlessness(Positioning/Abdominalbreathing/Pursedlipbreathing/Relaxation/Handheldfans)
Haveyoueverbeentaughthowtomanageyourbreathlessness?Yes/No
Ifyes,pleaseexplainthestrategiestaughtie.Breathingexercises,handheldfan,relaxationetc
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
Whichmemberoftheteamcaringforyoutalkedtoyouaboutusingpositioningtohelpmanageyourbreathlessness?Pleasecircle
PhysiotherapistOccupationaltherapistNurse
PalliativecareteamDoctorOthers
Wereyouinstructedonhowtousepositioningtorelievebreathlessness?Yes/No
Howoftenareyouusingpositioning?Pleasetick
Lessthanonehouraday
Betweenoneortwohoursaday
Betweentwoorfourhoursaday
Morethanfourhoursaday
Haveyoufoundpositioningusefulinhelpingyoumanageyourbreathlessness?Yes/No
Pleaseexplain
Wouldyourecommendpositioningtoanotherpatientwhowasbreathless?Yes/No
19
Appendix2
Patientvotingfortop5interventions
20
21
Appendix3
Staffeventvotingresults
22
Appendix4
Votingformforpatientstochoosetheirtop5interventions
23
Appendix5
Posterdisplayedonwardswiththetoolkit