Embed Size (px)
Citation preview

Non-invasive
Imaging of Carotid Artery
Atherosclerosis
최연현
성균관의대삼성서울병원영상의학과

Noninvasive Techniques
• US with Doppler
• CT
• MRI

Ultrasonography

Techniques of Carotid US
• US Anatomy (ICA vs ECA)
• Gray scale and color Doppler exam
• Transducer selection (4-7 vs 10-13 MHz)
• Artifacts
• New techniques

경동맥 협착의 Doppler 진단Criteria: Parameters
• ICA의 peak systolic velocity
• ICA의 end diastolic velocity
• ICA/CCA의 peak systolic velocity
ratio
• Proximal ICA(stenotic lesion)/distal
ICA peak systolic velocity ratio

Duplex Criteria:
Comparison of Recommended
Values
Study Severity PSV EDV VICA/VCCA Ratio
Moneta > 70% 325.0 130.0 4.0 (to 4.2)
Carpenter > 70% 210.0 70.0 3.0
Neale > 70% 270.0 110.0 NA
Hood > 70% 130.0 100.0 NA
Browman > 70% 175.0 NA NA
Moneta > 60% 260.0 70.0 3.2
Carpenter > 60% 170.0 40.0 2.0
Derdeyn > 60% 230.0 NA NA

Duplex Criteria:
for 50% and 70% Stenosis. (Robinson et al. AJR,1988)
Dm PSV EDV VICA/VCCA
Stenosis Ratio
50% > 150 >50 >2
70% > 230 >75 >3

경동맥 협착의Doppler 진단 Criteria
• CCA의 peak velocity는 근위부와원위부에서 측정할 때 차이(23 cm/sec 범위)
• Stenosis > 90-95%: PSV< 25 cm/sec


Pitfalls
• Hypertension or hypotension
• Severe stenosis of distal ICA
• Stenosis of contralateral ICA
• Tandem lesions
• Ulceration of plaque
• Vessel tortuosity

Intimomedial Thickness
Measurement

US quanfication of carotid
atheroma
• Manual or semi-automated method
• Thickness, area, and volume
measurement of plaques
• IMT measurement
• Objectiveness? (operator-dependent)


Carotid IMT and Brain
Infarction• Touboul et al. Circulation 2000;102:313
• 470 pts with brain infarction and 463 controls
• Mean IMT was higher in pts with brain infarction (0.797 mm vs 0.735 mm, p <0.0001)
• Odds ratio per SD increase (0.150) = 1.82 (95% conf. Level = 1.54~2.15)

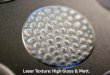
Enhanced CT

Maximum Intensity Projection

Noncalcified Coronary
Artery Plaque

Plaque Characterization:
ICUS vs CT
Schroeder Leber
Soft 14 26 HU 49 22 HU
Intermed 91 21 HU
Calcified 416 194 HU 391 156 HU
Schroeder et al. J Am Coll Cardiol 2001;37:1430
Leber et al. J Am Coll Cardiol. 2004;43:1241

Plaque Quantification
HanWonhee


MR Angiography: Techniques
• Noncontrast: time-of-flight, phase
contrast, true FISP (b-FFE, FIESTA)
• Longer time, motion artifact, flow sensitive
• Contrast-enhanced MRA
• High SI, quick, less artifacts, depiction of
vessel origins from the aortic arch

CE-MRA vs TOF MRA

Sonography
in Imaging Atheroma
• Fibrofatty, fibrocalcific, calcific type
• Inhomogeneous atheroma: calcifications,
cholesterol crystals, hemorrhage
• Plaque cap rupture: irregular surface, ulcer

US Assessment of Plaque
Composition

Ulcerated Plaques

Inhomogeneous Plaque

MRI for Carotid Atheroma
• Excellent tissue contrast (fat, fibrous
tissue, collagen, thrombus)
• Noninvasive
• More accurate and objective estimation
of stenosis degree than US

MRI Techniques
• T1-weighed spin echo imaging (precontrast axial, again with fat-saturation, postcontrast axial)
• Double inversion-recovery SE imaging (axial)
• T2-weighted spin echo imaging (axial)
• Proton-WI (axial)
• 3D Time-of-flight MRA (source and 3D images)
• Two 3-inch phased-array coils, bilateral application
• Field of view: 8x8 cm or 1010 cm
• Slice thickness = 2-3 mm, 256192 matrix, NEX = 1 or 2

Atheromatous Core• Mostly composed of cholesterol and
cholesterol esters in solid (crystal)
and smectic (liquid-crystaline) state
• Short T2 of core due to
– Micellar structure of lipoproteins
– Denaturation by oxidation
– Exchange btw CEs and water
molecules
T2WI

Regions with Fibers
• Collagen, elastin, proteoglycan
• “Moderately” high SI areas on T2WI

MRI Appearance of Plaque Components on
Various Imaging Sequences
Plaque
Components
T2WI T1WI T1WI,
Fat-
Suppr.
Proton
WI
TOF CE on
Post-
Contrast
Recent
Hemorrhage
Variable H-to-M H Variable H No
Lipid-rich
Necrotic Core
Variable
(L)
H M-to-H H M No
Fibrous Tissue Variable M M H M-to-L Yes
Calcification L L L L L No
Tissue contrast is relative to SI of muscle

Stable Plaque
T2WI Pathology

T1WI Proton-WI T2WI
FISSURE
TOF
Lipid-rich Plaque

LeeSG
Fibrous Cap on MRI

Intact plaque cap with intraplaque
hemorrhage (fibrin)
Cap
Fibrin
TOF T1FS

Pre Post
Contrast-enhancement in fibrous
component

• Increased neovasculature within plaque may contribute to plaque instability.
• Contrast-enhancement represents neovasculature in the histopathology (sensitivity 76%, specificity 79% by Yuan).
• Contrast-enhancement improves differentiation of tissue types (fibrous tissue, necrotic core, calcifications).

Plaque Characterization by
Contrast-enhancement
Pre Post
Chinyongil

MRI Accuracy
• Ex vivo T2WI: Accurate for fibrocalcific
plaques (90% sensitivity, 100%
specificity) -Serfaty et al
• In vivo multispectral MRI for lipid-rich
cores and intraplaque hemorrahge:
overall accuracy 87%, sensitivity 85%,
specificity 92% -Yuan et al

Fibrous Cap Rupture at MRI
and Recent TIA or Stroke (Yuan, Circulation 2002)
%
Symptomatic
Likelihood to
have
TIA/stroke
Odds Ratio
Intact thick FC
(n = 11)
9 1X
Intact thin FC
(n = 12)
50 10X
(95% CI =
1.0, 104)
6
Ruptured FC
(n = 30)
70 23X
(95% CI = 3,
210)
18

Lipid lowering drugs
Direct effects on
• Endothelial cell function
• Inflamm. cell activity
• VSMC proliferation
• Platelet aggregation
• Thrombus formation

Effects of Lipid-Lowering Therapy onCarotid Plaques at MRI
• Significant reduction in vessel wall thickness and area at 12 m and after (Corti, 2001)
• Pts with 10-y intensive therapy had a smaller core lipid area and lipid composition than control group (Zhao 2001)

Changes in Carotid Plaques after Statin
Therapy: MRI Evaluation
• 45 pts with 30-70% stenosis
• PreTx (Simbastatin 20 mg) and F-up MRI (19 ± 7.5 m)
• Decreased mean total chol., LDL, & CRP compared with control group:
Total Chol = 188 ± 26 vs 158 ± 50, p<.001
LDL = 125 ± 23 vs 110± 42, p <.001
CRP = 0.41 ± 0.59 vs 0.10 ± 1.3, p<0.01

Results
• Stabilization of plaque components on
MRI in 16% (7/45)
• Decreased plaque thickness:
4.2 mm± 1.0 vs 3.4 mm ± 1.3, p
< 0.001

Increased Fibrotic Component on
T2WI at 20 m f-up
YoonJY

Improved Wall Thickness, at 1 y
(0.5 mm)
YoonYCh

Contrast Agents for MR
Imaging of Atherosclerosis
• Ultrasmall superparamagnetic particles
of iron oxide (USPIO)
• Fibrin-specific polypeptide (EPIX)
• Plaque detection by Gadofluorine
(Schering)

USPIO in
Watanabe Hyperlipidemic Rabbits (5 ds)
USPIO USPIO No USPIO
Watanabe Control Watanabe

Gadofluorine M
Courtesy of Dr Whal Lee, SNUH

Fibrin-specific polypeptide
(20 h post EP-1873, EPIX)
Botnar, Circulation 2004

Summary
• Noninvasive imaging studies may eliminate the need of DSA in assessment of stenosis degree.
• CT angiography and high-resolution MRI/MRA can be useful in further evaluation of intracranial/extracranial carotid arteries and coronary arteries in selected patients
• High-resolution MRI can identify vulnerable carotid plaques and allows early intervention on unstable plaques.