Embed Size (px)
Citation preview

Nocturia in older people: A review of causes, consequences,assessment and management
A. ALI ,1 J . SNAPE2
SpR Geriatric Medicine,1 Consultant Geriatrician,2 King’s Mill Hospital, Mansfield Road, Sutton in Ashfield, Notts
SUMMARY
Nocturia is common in older people and it may be bother-
some for both patients and carers. It is most commonly
related to bladder storage difficulties and nocturnal polyuria.
The former results most frequently from an uninhibited
overactive bladder. The latter occurs as a consequence of
age-associated changes in the circadian rhythm of urine
excretion. The management of an overactive bladder includes
both behavioural and drug treatment. The management
options for nocturnal polyuria include an afternoon diuretic
and desmopressin, but caution is required, particularly with
the latter, as it can cause significant hyponatraemia.
Keywords: Nocturia; nocturnal polyuria; bladder storage
problems
� 2004 Blackwell Publishing Ltd
INTRODUCT ION
The purpose of this article is to explore the causes and impact
of nocturia in older patients and their carers, to discuss its
assessment and diagnosis and to go on to look at the manage-
ment of some of the conditions which lead to nocturia. The
standardisation subcommittee of the International Con-
tinence Society has recently agreed to the standardisation of
terminology in relation to nocturia (1) (Figure 1).
We will concentrate on nocturnal polyuria (NP) and bladder
storage problems, briefly mentioning other conditions that
might appear in the differential diagnosis of nocturia.
DEF IN IT IONS
Nocturia
Nocturia is the complaint that a patient has to wake at night
to void, on one or more occasions (1). It particularly affects
older individuals (2,3). Four per cent of children aged 7–15
years were reported as suffering from regular nocturia (4)
whereas in men and women aged 50–59 years the prevalence
was 66 and 58%, respectively (5). In those over 80 years 91%
of men and 72% of women reported nocturia (5).
Nocturia needs to be distinguished from nocturnal enuresis
(which is not considered here) where voiding occurs during
sleep. The first morning void is not included as a night time
void, as it is the natural expulsion of urine produced during the
night (1). Patients with nocturia may or may not be bothered
by it, and this will determine whether or not they seek help.
Nocturnal Polyuria
NP is defined as the production of an abnormally large
volume of urine during sleep. This includes all urine pro-
duced after going to bed plus the first morning void. If the
24-h urine volume is normal, the output during sleep can be
expressed as a percentage of the total (1). Healthy adults aged
21–35 years excrete about 14% of their total urine at night
(6) whereas older people pass about 34% (7). About 25%
of nursing home residents in one study were passing more
than 50% of their total daily output at night (8).
Therefore, younger people producing more than 20% of
their urine during sleep and older individuals who produce
more than 33% of their daily total during the same time are
defined as suffering from NP (1). The causes of NP will be
considered below.
Bladder Storage Problems
Patients with reduced structural bladder capacity (e.g. due to
fibrosis, previous radiation therapy or carcinoma in situ) orwith reduced functional bladder capacity including those
with uninhibited overactive bladder or with significant post-
void residuals among others, may have bladder storage
problems which tend to present with frequency, urgency, urge
incontinence and nocturia. They may have several episodes of
nocturia but the volumes passed were small (9). The diagnosis
can be clarified by using a frequency/volume (F/V) chart.
Correspondence to:Dr J. Snape, MB, FRCP, Consultant Geriatrician, King’s Mill
Hospital, Mansfield Road, Sutton in Ashfield, Notts, NG17 4JL
Tel.: 144 (1623) 785100
Fax: 144 (1623) 785230
Email: [email protected]
ª 2004 Blackwell Publishing Ltd Int J Clin Pract, April 2004, 58, 4, 366–373
REVIEW

Polyuria
Patients with urine output exceeding 40ml/kg body weight/
24 h are suffering from polyuria. They may present with
nocturia. The polyuria should be further investigated to see
whether it is due to water diuresis (e.g. diabetes insipidus or
excessive fluid intake) or a solute diuresis (e.g. diabetes mellitus).
Sleep Disorders
Some patients may seem to have bladder storage problems
when the F/V chart is studied, but their real problem is one of
the sleep disorders (e.g. insomnia, obstructive sleep apnoea or
periodic leg syndrome).
Patients who are constantly waking up at night for other
reasons may feel the need to void on each occasion and void a
small volume. Further investigations in a sleep laboratory may
be necessary.
Consequences of Nocturia to Patient and Care Given
Nocturia is one of the commonest causes of sleep interruption
and lack of sleep. It is associated with unrefreshing sleep and
daytime fatigue. Concentration, co-ordination, problem-solving
skills and creativity are reduced. There may be mood alteration
and muscle stiffness (10). Lack of sleep has also been associated
with reduced natural killer cell numbers and cytokine levels in the
blood – the result of which is an increased incidence of infection
(11). Nocturia is also a risk factor of falls and fractures; the risk
increases proportionally to the frequency of nocturia (12).
The combination of postural hypotension resulting in
impaired balance and nocturnal awakenings for frequent visits
to the toilet increases the risk of falls-related injury. Urgency
at night also increases the risk (13). Nocturia, in general,
causes poor health in older people. There is increased need
for emergency care, independent of the presence of heart
disease, asthma and renal problems. Older people who voided
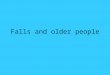
N O C T U R I A
Patient desires treatment Patient does not desire treatment
Screen
Lifestyle advice
Further investigations
Polyuria Nocturnal polyuria Apparent bladderstorage problems
Primary sleep disorders
Examples of causes related to bladder storage problems:
Detrusor overactivityReduced functional bladder capacity (e.g. significantpost void (PV) residualBladder outlet obstruction with PV residual
Figure 1 Algorithm for assessment of
patients with nocturia [adapted and
reproduced with the permission of the
International Continence Society (1)]
NOCTURIA IN OLDER PEOPLE 367
ª 2004 Blackwell Publishing Ltd Int J Clin Pract, April 2004, 58, 4, 366–373

three or more times at night had a greater mortality over a
54-month period (14). Heart disease (e.g. cardiac failure and
hypertension) and autonomic dysfunction may be respon-
sible, it was suggested.
In a Dutch study, older women with poor health were more
likely to suffer with nocturia.
Nocturia can also be a very bothersome symptom and have a
deleterious effect on everyday activities (15). Although not every-
body who reports nocturia, considers it problematic, some con-
sider it to be a part of normal ageing. Currently, there is no
dedicated instrument to measure the prevalence and impact of
nocturia in terms of quality of life, although there are several
valid and reliable questionnaires that include nocturia (16,17).
Seventy per cent of care givers have cited sleep-related problems
(nocturia being the most frequent complaint) of older relatives as
a major reason for deciding to institutionalise them (18).
FACTORS WHICH AFFECT URINE PRODUCT ION
IN THE AGED
Circadian Urine Production
A circadian rhythm of urine production is usually established
by 5 years of age. Seven-year olds produce 2–3 times the
amount of urine during the day than they do at night (19).
In adults, 25% or less of the daily urine output occurs during
the hours of sleep (20). After 60 years, a shift to more
nocturnal urine production occurs, and with increasing age,
the ratio of day to night time urine flow falls until the
latter equals or exceeds the former (7) The total 24-h urine
excretion, however, does not change with age (21).
Arginine Vasopressin
Arginine vasopressin (AVP) (otherwise anti-diuretic hor-
mone) is the main hormone responsible for the regulation
of urine production. Ageing does not affect the nuclei of the
hypothalamus either in terms of cell loss or synthetic ability.
There remains some confusion about the effect of ageing on
daytime blood AVP levels. Some studies have suggested an
increase in daytime basal plasma level of AVP in older people
(22,23,24), whereas others indicated that basal levels were not
affected by age (25,26). Further studies have reported lower
daytime plasma AVP concentrations in healthy older subjects
when compared with young subjects (27). During the hours
of sleep, however, it seems clear that there is a circadian
rhythm of AVP with peak concentration occurring at night
(28). It appears to be related to the wake/sleep cycle rather
than the time of day (29). With ageing, there is a blunting of
the nocturnal AVP secretions, so that, levels of hormone are
similar during the day and night (21,30). Impairment of
nocturnal AVP release accompanying with NP has been
demonstrated in multiple system atrophy (MSA) (31) and
Alzheimer’s disease (32).
Asplund (33) found that there was a difference between
older men and older women with a two-fold higher plasma
AVP in the former. This finding has so far not been
confirmed (24,25).
Atrial Natriuretic Hormone
Atrial natriuretic hormone (ANH) [previously known as atrial
natriuretic peptide (ANP)] through its action on the kidney
results in natriuresis and consequent diuresis. ANH levels have
been shown to increase with age (34) fivefold higher in older
nursing home residents compared to younger controls (35).
ANH has been shown to interact with the renin-angiotensin-
aldosterone system, high levels suppressing renal renin
secretion, plasma renin activity and thus plasma aldosterone
via plasma angiotensin II (36). A slow intravenous infusion of
ANH, causing minimal increase (within the physiological
range) in ANH, inhibits angiotensin II-provoked aldosterone
release (37). ANH, moreover, seems to suppress aldosterone
secretion directly (38). ANH also opposes AVP action in the
kidney and inhibits central AVP release (55). Therefore,
ANH, through its impairment of renal sodium conservation
and concomitant water loss (via the direct natriuretic effect
and through its suppression of aldosterone) and also
through its effect on AVP, may contribute to age-related
changes in urine excretion. Subclinical heart failure may also
be contributing to elevated ANH levels, resulting in nocturnal
diuresis. This was suggested by a study of patients present-
ing to a urology clinic. It was found that patients with NP
had a significantly higher level of ANH compared to controls,
and that they had significant cardiomegaly on chest X-ray
(39).
Another study looked at ANP levels in geriatric patients
with nocturia and nursing home residents with nocturnal
incontinence. Whilst ANP levels were elevated, NP was not
associated with higher levels. The study concluded that ANP
levels were unlikely to be a primary cause of nocturia but they
may contribute (along with other factors such as low AVP
levels) to the problem in some older patients (40).
RENAL FACTORS AND AGE
Water Loss
There is a fall in renal-concentrating ability with age. A fall in
maximum urine osmolality with age occurred in a study when
hospitalised males (aged 23–72 years) underwent 24 h of fluid
deprivation (40). Similarly healthy males aged 40–101 years
demonstrated a fall in urine-specific gravity from 1.03 at
40 years to 1.023 at 89 years when exposed to 24-h water
deprivation (41). This decline in renal-concentrating ability
was felt to be related to impaired renal tubular responsiveness
to AVP (40). In effect, this represents a mild form of acquired
nephrogenic diabetes insipidus.
368 NOCTURIA IN OLDER PEOPLE
ª 2004 Blackwell Publishing Ltd Int J Clin Pract, April 2004, 58, 4, 366–373

Sodium Loss
Normal ageing is associated with increased renal sodium loss.
The ability of the aged kidney to conserve sodium in response to
salt restriction is impaired (42). Natriuresis in older people is
associated with an osmotic diuresis which is more evident when
in the recumbent position. The ability of the kidney to conserve
sodium is partly dependent on the renin-angiotensin-aldosterone
system, which is affected by ageing. Renin secretion in
response to stimuli, such as low-dietary sodium and upright
posture, falls with age. This results in reduced aldosterone
secretion and therefore reduced renal sodium conservation
(43,44,45).
Age and Urine Storage
Community-based studies suggest that with normal ageing,
bladder capacity and bladder compliance fall as do urinary
flow rates and maximal urethral closure pressure. Frequency
of inhibited detrusor contractions and post-void residual
increase (46,47,48). These factors interfere with the bladder’s
ability to store urine successfully. In the presence of signifi-
cant lower urinary tract problems in old age, such as detrusor
overactivity (of whatever cause), this reservoir function may
be further impaired leading to frequency, urgency, urge
incontinence and nocturia. In men, the progressive enlarge-
ment of the prostate with age greatly influences the behaviour
of the bladder and urinary outflow tract contributing to lower
urinary tract symptoms including nocturia (49).
ASSESSMENT OF NOCTURIA
Several different urinary and extra urinary problems can lead to
nocturia. Its assessment is laid out in the algorithm (Figure 1).
The initial assessment should include a complete history, detail-
ing lower urinary tract symptoms (e.g. urgency may suggest an
overactive bladder; nocturia, hesitancy, poor stream and a feel-
ing of incomplete emptying in a male would indicate the
possibility of prostatic hyperplasia). A detailed medical history
including a known history of conditions, such as Parkinson’s
disease, multiple sclerosis, Alzheimer’s disease, diabetes mellitus,
congestive cardiac failure and obstructive sleep apnoea, is
important. The presence of chronic neurological conditions
may indicate an overactive bladder secondary to loss of central
inhibition of the detrusor muscle. It may also, in more advanced
conditions, suggest the presence of a hypotonic bladder.
In multiple system atrophy and Alzheimer’s disease,
reduced nocturnal AVP secretion can cause NP. Diabetes
may indicate polyuria secondary to poor glycaemic control
or hypotonic bladder due to autonomic neuropathy. Oedema
as a consequence of, for example, congestive cardiac failure or
hepatic disease, can provoke nocturia by the mobilisation of
large quantities of fluid at night when the patient is supine
(56). Obstructive sleep apnoea is a condition which results in
NP, thought to be a consequence of raised ANH levels at
night (21), hence, symptoms of this condition should be
sought. A review of symptoms may provide clues as to other
conditions leading to nocturia (e.g. constipation). A history of
previous surgical or gynaecological attention should be
sought. Drug history is important: diuretics in the evening
may cause nocturia, anti-cholinergics may cause retention and
overflow and lithium may cause nephrogenic diabetes insipi-
dus. The patient’s attitude to their problem (is it bother-
some?) is also vital when considering management. Details
of sleep pattern should be sought. A complete physical exam-
ination is mandatory and may provide evidence of congestive
cardiac failure, urinary retention, faecal impaction, neuro-
logical deficits or other conditions that may provide clues as
to the cause of nocturia.
Laboratory evaluation should include urinalysis, urine cul-
ture and sensitivity, blood urea, electrolytes, calcium and
glucose. These tests may indicate the presence of a urinary
tract infection (UTI) or a cause of polyuria that may explain
nocturia. Treatment of a UTI is only likely to be helpful if the
patient has symptoms and signs of infection. A chest X-ray,
ECG and echocardiogram may indicate overt or incipient
heart failure, which could be implicated as a cause of nocturia.
Further evaluation crucially includes the F/V chart, which
should include of the voided urine (volume and time) over at
least 72 h (50). The chart should also include information on
the volume and type of fluid ingested, the bed time and time
of rising and subjective idea of each night’s sleep (good or
bad). The F/V chart is likely to identify patients with NP.
Measurement of post-void residual volume by non-invasive
ultrasound scan will identify patients with urinary retention
caused either by outlet obstruction or by neurogenic bladder.
Measures of quality of life (see above) may be appropriate in a
research setting. Serum ANP and AVP levels are not routinely
used in clinical practice. Patients with bladder storage problems
causing nocturia may also be identified from the F/V chart,
although some patients may require further urodynamic assess-
ment (e.g. filling and voiding cystometry). If a sleep disorder is
suspected, a nocturnal polysomnography should be considered.
Polyuria is defined as a 24-h voided volume in excess of
2800ml (i.e.> 40ml/kg in a 70 kg person). The F/V chart
should identify excessive fluid intake. Fasting blood glucose
and a fluid deprivation test should diagnose diabetes mellitus
or diabetes insipidus. Serum calcium and blood urea and
creatinine should identify hypercalcaemia and renal failure
(other possible causes of polyuria).
MANAGEMENT OF NOCTURIA
Lifestyle Advice
General lifestyle advice, such as reducing alcohol and caffeine
intake and limiting food/liquid intake after 7:00 PM, can be a
successful strategy in some patients. While it is recognised
NOCTURIA IN OLDER PEOPLE 369
ª 2004 Blackwell Publishing Ltd Int J Clin Pract, April 2004, 58, 4, 366–373

that in nursing homes, the sleep of residents is very disrupted
by noise, light and nursing practices (51) and that improving
sleep quality may improve nocturia, (52) attempts to try and
improve the sleep of residents by strategies to reduce noise
and light or by introducing a physical activity programme
have so far failed (53,54).
An interesting finding was that older people who were
treated with hypnotic excreted a smaller volume of urine at
night than those not so treated (52). It seemed that not only
spontaneous sleep but also sleep induced by medication
reduces nocturnal urine output. It has also been suggested
that the use of daytime compression stockings may be useful
in oedematous patients with NP and also afternoon nap (9),
but further research is needed.
Nocturnal Polyuria
Apart from lifestyle changes, three areas have been considered
for the pharmacological management of NP. Firstly, forcing
more urine output during the day in the hope that nocturnal
production would fall as a consequence. It has been observed
that nursing home patients taking diuretics had smaller noc-
turnal volumes than non-diuretic-taking controls (8). Diure-
tics taken 6 h before bedtime have been shown in two trials to
reduce nocturnal urine volume in some patients (57,58).
The mechanism may be diuretic induced reduction in the
intravascular volume and reduced renal blood flow. Improve-
ment in incipient cardiac failure resulting in decreased ANH
secretions is another possibility. Clearly, the risks of dehydra-
tion in older people when using such treatment should be
remembered.
Secondly, blocking or lowering nocturnal ANH production
has been suggested (59), but apart from the use of afternoon
diuretics, we found no studies in man that attempted to lower
ANH levels or block ANH receptors. However, it has been
proposed that NP and essential hypertension share a defect in
the nitric oxide pathway leading to resetting of the pressure-
natriuresis relation in the kidney, sodium retention and
compensatory nocturnal natriuresis (60). These authors pre-
dict that concentrations of urodilatin (a natriuretic peptide
produced by the kidney, which may be more important than
ANH in regulating sodium excretion) (61) and ANH will be
increased in patients with NP. Moreover, while they feel that
giving diuretics in the daytime in this situation to alleviate
sodium overload is a logical approach, measures to increase
the production of nitric oxide (such as dietary supplements
of L-arginine) may be more effective. They point out that
anti-hypertensive agents have not been systematically assessed
in the treatment of NP.
The third approach to reducing NP is the administration
of AVP before sleep, to restore the normal nocturnal rise.
Desmopressin has been used in a number of small studies in
different clinical settings. In a double blind placebo-
controlled crossover study of 25 women with nocturia
aged 41–76 years, 20 mg of desmopressin was given intra-
nasally to the treatment group. Two weeks of treatment
resulted in a significant fall in nocturnal urine output from
a mean of 438–267ml. Also, nocturnal frequency fell from
3.2 to 1.9 episodes (62).
Asplund and Aberg looked at short-term (2 weeks) and
long-term (2 months) use of desmopressin given intranasally
in 20 women with nocturnal diuresis (mean age 71 years) and
observed a significant decrease in nocturnal urine production,
which was sustained (63,64).
More recent studies have looked at the use and safety of
oral desmopressin in older subjects with NP. Asplund, in
1999, reported on a double blind randomised crossover trial
of 2 weeks of oral desmopressin vs. placebo in a group of
mixed gender with NP (mean age 67.7 years). It showed
significantly reduced nocturnal diuresis and number of
nocturnal voids. Also, longer uninterrupted sleep was demon-
strated. No serious adverse effects were observed (in particular
no significant hyponatraemia) (65). In a study reported in
2002, 30 patients (mean age 75.4 years) with nocturia on
three or more occasions or NP refractory to medication were
treated with 0.1mg desmopressin at bedtime for 4 weeks.
Twenty patients reported a good response with significantly
reduced nocturnal frequency (mean of 5.2 vs. 2.24 times/
night) and urine volume (mean of 956 vs. 528ml). Five
patients had side-effects including one with hyponatraemia
(66).
The benefits of desmopressin in geriatric patients with NP
and other problems such as dementia remain a concern. In a
placebo-controlled study, Seiler et al. treated nine patients
(mean age 82 years) who had dementia and nocturnal incon-
tinence, with intranasal desmopressin 10–40 mg daily. He
observed a significant reduction of urine volume from 10 to
50% of the original total. Also, long-term treatment with
10 mg daily restored the night time continence without
adverse effects (67).
There remains concern, however, about the possibility of
serious hyponatraemia occurring in association with the use of
desmopressin in older patients (60).
In a study, seven of 20 older men treated with 20–40 mgintranasal desmopressin for 2–4 weeks suffered adverse effects
(including profound hyponatraemia) (68). The British
National Formulary advise ‘considerable caution’ in prescrib-
ing desmopressin to patients with cardiovascular disease or
hypertension and recommends it be avoided in elderly
patients with nocturia (69).
BLADDER STORAGE PROBLEMS
Bladder storage problems may be caused by such conditions
as detrusor overactivity (from whatever cause), reduced
structural bladder capacity, reduced functional bladder
370 NOCTURIA IN OLDER PEOPLE
ª 2004 Blackwell Publishing Ltd Int J Clin Pract, April 2004, 58, 4, 366–373

capacity with increased post-void residual and bladder
outlet obstruction. These problems may present with
nocturia and appropriate management may improve the
nocturia.
Habit retraining, timed voiding and prompted voiding
are the techniques that may be employed in patients with
overactive bladder during the daytime and have beneficial
effects on night-time symptoms (70). Anti-cholinergic drugs
such as oxybutynin and tolterodine are effective in increasing
functional bladder capacity and reducing symptoms (includ-
ing nocturia) in patients with overactive bladders (71). Both
drugs have extended release preparations that seem to have
benefits in terms of efficiency and fewer side-effects.
Imipramine, a tricyclic anti-depressant, has long been
known to have anti-cholinergic effects, which can benefit
patients with overactive detrusor (72), as well as alpha-
adrenergic stimulant effects, which can be beneficial in
patients with stress or mixed continence.
But also Hunsballe et al. (73) described an anti-diuretic
effect of this drug, which they felt, resulted from increased
sensitivity of the renal collecting ducts to AVP or from
decreased solute excretion.
Patients with bladder outlet obstruction secondary to
benign prostatic hypertrophy (BPH) are more likely to have
both NP and polyuria as a cause of nocturia (9). Some
symptomatic benefits may be derived from alpha-adrenergic
blocking drugs in patients with BPH. However, orthostatic
hypotension is a common side-effect of these drugs, and in
combination with nocturia, the risks of night-time falls
is high. Patients should be warned. Tamsulosin is a more
selective alpha blocker which is less likely to cause postural
hypotension (74). Five alpha reductase inhibitors can also be
helpful, but they take several months to produce clinical
effects – working better on larger glands (75).
Patients with reduced functional bladder capacity and
increased post-void residual, once inappropriate medication
has been stopped (e.g. those with detrusor hyperreflexia and
impaired contractility) (76) and also in those with hypotonic
bladder (e.g. due to diabetic autonomic neuropathy) may
benefit from clean intermittent catherisation (77). This may
be particularly useful in reducing nocturia when performed
just before bedtime. Cholinergic drugs (e.g. bethanechol) in
this situation tend to be disappointing.
POLYURIA
The cause of polyuria (e.g. diabetes mellitus, diabetes insipidus
– pituitary or renal origin or primary polydipsia) should be
established and appropriate treatment instigated. No further
details will be included here, but treatment of the cause of
polyuria is likely to improve nocturia. Of course, more than
one cause of nocturia may coexist in the same patient.
CONCLUS ION
Terminology in relation to nocturia has recently been
standardised (1). This common symptom of older people causes
problems not only for patients but also for their carers. Careful
assessment should allow a cause for the nocturia to be identified.
As a result of an age-related fall in renal concentrating ability,
sodium conservation and secretion of renin-angiotensin-
aldosterone, together with impairment of the circadian rhythm
of AVP secretion and increased output of ANH, there is an
age-associated change in the circadian rhythm of urine excre-
tion leading to NP.
The most common causes for bladder storage problems in
old age are an uninhibited overactive bladder, bladder outflow
obstruction and infection; and for polyuria, it is diabetes
mellitus. Sleep disorders may need to be considered.
Management of nocturia should include general lifestyle advice
and specific treatment for causes of polyuria (e.g. diet, oral
hypoglycaemic drugs or insulin in the case of diabetes mellitus).
Bladder storage problems should be defined and treated
appropriately (e.g. habit retraining and anti-cholinergic
drugs in inhibited overactive detrusor muscle).
In the case of NP treatment, options are limited. Both for
an afternoon diuretic and night-time desmopressin, there is
some evidence of benefit, but the trials that have been carried
out are small and short-term and considerable caution is still
required when using the latter in older patients, because of the
danger of significant hyponatraemia.
REFERENCES
1 Van-Kerrebroeck P, Abrams P, Chaibin D et al. The standard-
isation of terminology in nocturia. Neurourol Urodyn 2002; 21:
179–83.
2 Malmsten UG, Milsom I, Molander U, Norlen LJ. Urinary
incontinence and lower urinary tract symptoms in men aged
45–99 years. J Urol 1997; 158: 1733–7.
3 Swithinbank LV, Donovan J, James MC, Yang Q, Abrams P.
Female urinary symptoms: Age prevalence in a community
dwelling population using a validated questionnaire. Neurourol
Urodyn 1998; 77: 805–12.
4 Mattson. UI and nocturia in healthy school children. Acta
Paediatr 1994; 83: 950–4.
5 Middlekoop HA, Smilde van del Doel DA, Neren AK et al.
Subjective sleep characteristics of 1485 males and females aged
50 6 93. J Gerontol A Biol Sci Med Sci 1996; 51: 108–15.
6 Robertson GL, Rittig S, Kovacs L et al. Pathophysiology and
treatment of enuresis in adults. Scand J Urol Nephrol Suppl 1999;
202: 36–9.
7 Kirkland JL, Lye M, Levy DW, Bannerjee AK. Patterns of urine
flow and electrolyte excretion in healthy elderly patients. BMJ
1983; 287: 1665–7.
8 Ouslander J, Schnelle J, Simmons S, Bates JB, Zeitlin M. The
dark side of incontinence: Night time incontinence in nursing
home residents. J Am Geriatr Soc 1993; 41: 371–6.
NOCTURIA IN OLDER PEOPLE 371
ª 2004 Blackwell Publishing Ltd Int J Clin Pract, April 2004, 58, 4, 366–373

9 Weiss JP, Blaiwas JG, Stember DS, Brooks MM. Nocturia in adults:
Etiology and classification. Neurourol Urodyn 1998; 17: 467–72.
10 Hetta J. The impact of sleep deprivation caused by nocturia.
BJU Int 1999; 84 (Suppl. 1): 27–8.
11 Irwin M, McClintick J, Costlow C, Fortner M, White J,
Gillin JC. Partial night sleep reduces natural killer and cellular
immune responses in humans. FASEB J 1996; 10: 643–53.
12 Stewart RB, Moore MT, May FE et al. Nocturia: a risk factor for
falls in the elderly. J Am Geriatr Soc 1992; 40: 1217.
13 Brown JS, Vittinghoff E, Wyman JF et al. Urinary incontinence:
Does it increase risks for falls and fractures? J Am Geriatr Soc
2000; 48 (7): 721–5.
14 Asplund R. Mortality in the elderly in relation to nocturnal
micturition. BJU Int 1999; 84: 297–301.
15 Van Dijk L, Kooij D, Schellevis F. Nocturia and quality of life in
the Dutch adult population. Neurourol Urodyn 2002; 21: 313–4.
16 Donovan JL, Abrams P, Peters TJ et al. The ICS-BPH study:
The psychometric validity and reliability of the ICS male
questionnaire. Br J Urol 1996; 77: 554–62.
17 Jackson S, Donovan JL, Brookes S et al. The Bristol female lower
urinary tract symptoms questionnaire: Development and psycho-
metric testing. Br J Urol 1996; 77: 805–12.
18 Pollak CP, Perlick D. Sleep problems and institutionalisation of
the elderly. J Geriatr Psychiatry Neurol 1991; 4: 204–10.
19 Rittig S, Knudsen UB, Norgaard JP et al. Abnormal diurnal
rhythm of vasopressin and urinary output with enuresis. Am J
Physiol 1989; 256: F664–F671.
20 Miller M. Fluid and electrolyte homeostasis in the elderly:
Physiological changes of ageing and clinical consequence.
Baillieres Clin Endocrinol Metab 1997; 11: 367–87.
21 Asplund R. The nocturnal polyuria syndrome (NPS). Gen
Pharmacol 1995; 26: 1203–9.
22 Frolkis VV, Golovchenko SF, Medved VI, Frolkis RA.
Vasopressin and cardiovascular system in ageing. Gerontology
1982; 28: 290–302.
23 Crawford GA, Johnson AG, Gyory AZ, Kelly D. Change in
arginine vasopressin concentration with age. Clin Chem 1993;
39: 2023.
24 Johnson AG, Crawford GA, Kelly D, Nguyen TV, Gyory AZ.
Arginine vasopressin and osmolality in the elderly. J Am Geriatr
Soc 1994; 42: 399–404.
25 Bursztyn M, Bresnahan M, Gavras I, Gavras H. Effect of ageing
on vasopressin, catecholamines and alpha2-adrenergic receptors.
J Am Geriatr Soc 1990; 38: 628–32.
26 Helderman JH, Vestal RE, Rowe JW, Tobin JD, Andres R,
Robertson GL. The response of arginine vasopressin to intra-
venous ethanol and hypertonic saline in man. The impact of
ageing. J Gerontol 1978; 33: 39–47.
27 Faull CM, Holmes C, Baylis PH. Water balance in elderly
people: Is there a deficiency of vasopressin? Age Ageing 1993;
22: 114–20.
28 George CPL, Messerli FH, Genest J et al. Diurnal variations of
plasma vasopressin in man. J Clin Endocrinol Metab 1975; 41:
332–8.
29 Nadal M. Secretary rhythm of vasopressin in healthy subjects
with inversed sleep-wake cycle; evidence for the existence of an
intrinsic regulation. J Eur Endocrinol 1996; 134: 174–6.
30 Matthiesen TB, Rittig S, Norgaard JP, Pederson EB,
Djurhuus JC. Nocturnal polyuria and natriuresis in male
patients with nocturia and lower urinary tract symptoms.
J Urol 1996; 156: 1292–9.
31 Ozawa T, Oyanagi K, Tanaka H et al. Suprachiasmatic nucleus
in a patient with multiple system atrophy with abnormal
circadian rhythm of AVP secretions into plasma. J Neurol Sci
1998; 154: 116–21.
32 Ouslander JG, Nasr SZ, Miller M et al. AVP levels in nursing
home residents with night time urinary incontinence. JAGS
1998; 46: 1274–9.
33 Asplund R, Aberg H. Diurnal variations in the levels of AVP in
the elderly. J Intern Med 1991; 299: 131–4.
34 Cugini P, Lucia P, Dipelina L et al. Effect of ageing on ANP
plasma renin activity and plasma aldosterone. J Gerontol 1992;
47: B14–B19.
35 Ohasi M, Fujio N, Nawata H et al. High plasma concentration
of human ANP in aged men. J Clin Endocrinol Metab 1987; 64:
81–5.
36 Genest J, Larochelle P, Cusson JR et al. The atrial natriuretic
factor in hypertension; State of the art lecture. Hypertension
1988; (Suppl.1): 11; 13–7.
37 Cuneo RC, Espiner EA, Nicholls MG et al. Effect of physio-
logical levels of ANP on hormone secretion. J Clin Endocrinol
Metab 1987; 65: 765–22.
38 Clinkingbeard C, Sessions C, Shenker Y. The physiological
role of ANH in the regulation of salt and water metabolism.
J Clin Endocrinol Metab 1990; 70: 582–9.
39 Carter PG, McConnell AA, Abrams P. The significance of atrial
natriuretic peptide in nocturnal urinary symptoms in the elderly.
Proc Int Continence Soc 1992; 11: 420–1.
40 Ouslander JG, Johnson T, Nasr S et al. ANP levels in geriatric
patients with nocturia and nursing home residents with night
time incontinence. JAGS 1999; 47: 1439–44.
41 Miller JH, Slock NW. Age differences in the renal tubular
response to ADH. J Gerontol 1953; 8: 446–50.
42 Lewis WH, Alving AS. Changes with age in the renal function in
adult men. Am J Physiol 1938; 123: 500–15.
43 Epstein M, Hollenberg NK. Age as a determination of renal
sodium conservation in normal man. J Lab Clin Med 1976;
87: 411–7.
44 Bauer JH. Age related changes in the renin-aldosterone system.
Physiological effects and clinical implications. Drugs Aging 1993;
3: 238–45.
45 Tsunoda K, Abe K, Goto T et al. Effect of age on the
renin-angiotensin-aldosterone system in normal subjects. J Clin
Endocrinol Metab 1986; 62: 384–9.
46 Burgio KL, Engel BT, Locker JL. Normal patterns of diurnal
urination across 6 age decades. J Urol 1991; 145: 728–31.
47 Malone Lee JG, Wahedna I. Characterisation of detrusor
contractile function in relation to old age. Br J Urol 1993; 72:
873–80.
48 Bonde HV, Sejr D, Erdmann L et al. Residual urine in 75 year
old men and women. A normative population study. Scand J
Urol Nephrol 1996; 30: 89–91.
49 Holm NR, Horn T, Hald T. Detrusor in ageing and obstruc-
tion. Scand J Urol Nephrol 1995; 29: 45–9.
372 NOCTURIA IN OLDER PEOPLE
ª 2004 Blackwell Publishing Ltd Int J Clin Pract, April 2004, 58, 4, 366–373

50 Abrams PH. Frequency Volume charts: An indispensable part of
lower urinary tract assessment. Scand J Urol Nephrol Suppl 1996;
179: 47–53.
51 Schnelle JF, Ouslander JG, Simmons SF et al. The night time
environment, incontinence care and sleep disruption in nursing
homes. JAGS 1993; 41: 910–4.
52 Asplund R, Abert HE. Micturition habits of older people. Void-
ing frequency and urine volumes. Scand J Urol Nephrol 1992; 26:
345–9.
53 Schnelle JF, Alessi CA, Al-Samarrai NR et al. The nursing home
at night: Effects of an intervention on noise, light and sleep.
JAGS 1999; 47: 430–8.
54 Alessi CA, Schnelle JF, MacKae PG et al. Does physical activity
improve sleep in impaired nursing home residents? JAGS 1995;
43: 1098–102.
55 Standaert DG, Cechetto DF, Needleman P et al. Inhibition of
the firing of vasopressin neurons by atriopeptin. Nature 1987;
329: 151–3.
56 Burgio KL, Locker JL, Ives DG et al. Nocturnal enuresis in
community dwelling older patients. JAGS 1996; 44 (2): 139–43.
57 Reynard JM, Cannon A, Yang Q et al. A novel therapy for
nocturnal polyuria: a double blind randomised trial of frusemide
v placebo. Br J Urol 1998; 81: 215–8.
58 Pedersen PA, Johansen PB. Prophylactic treatment of adult
nocturia with bumetanide. Br J Urol 1998; 62 (2): 145–7.
59 Donahue JL, Lowethal DT. Nocturnal polyuria in the elderly
person. Am J Med Sci 1997; 314: 232–8.
60 McKeigue PM, Reynard JM. Relation of nocturnal polyuria of
the elderly to essential hypertension. Lancet 2000; 355: 486–8.
61 Dummer C, Franck W, Heer M et al. Postprandial natriuresis in
humans: Further evidence that uroldilation not ANP modulates
sodium excretion. Am J Physiol 1996; 270: F301–10.
62 Hilton P, Stanton SL. The use of DD AVP in nocturnal fre-
quency in the female. Br J Urol 1982; 54: 252–5.
63 Asplund R, Aberg H. Desmopressin in elderly women with
increased nocturnal diuresis. A short term study. Br J Urol
1993; 72: 42–5.
64 Asplund R, Aberg H. Desmopressin in elderly subjects with
increased nocturnal diuresis. A two months treatment study.
Scand J Urol Nephrol 1993; 27: 77–82.
65 Asplund R, Sundberg B, Bengtsson P. Oral desmopressin for
NP in elderly subjects: A double blind, placebo controlled
randomised exploratory study. BJU Int 1999; 83: 591–5.
66 Kuo H-C. Efficacy of desmopressin in treatment of refractory
nocturia in patients older than 65 years. Urol 2002; 59: 485–9.
67 Seiler WO, Stahelin HB, Hefti U. Desmopressin reduces night
urine volume in geriatric patients. Clin Invest 1992; 70: 619.
68 Cannon A, Carter PG, McConnell AA, Abrams P. Desmopressin
in the treatment of nocturnal polyuria in the male. Br J Urol
1999; 84: 20–4.
69 British National Formulary 44. London: BMA and Royal
Pharmaceutical Society of Great Britain, September 2000: P371.
70 Weiss JP, Blaivas JG. Nocturia. J Urol 2000; 163: 5–12.
71 Lackner TE. Pharmacologic management of urinary incon-
tinence. Am Long Term Care 2000; 8: 29–37.
72 Castleden CM, Duffin HM, Gulati RS. Double blind study of
imipramine and placebo for incontinence due to bladder
instability. Age Ageing 1986; 15: 299–303.
73 Hunsballe JM, Rittig S, Pedersen EB et al. Single dose imi-
pramine reduces nocturnal urine output in patients with nocturnal
enuresis and nocturnal polyuria. J Urol 1997; 158: 830–6.
74 Chapple CR, Baert L, Third P et al. Tamsulosin 0.4mg once
daily: Tolerability in older and younger patients with lower
urinary tract symptoms suggestive of BPH. Eur Urol 1997; 32
(4): 462–70.
75 Boyle P, Gould AL. Prostate volume predicts outcome of treat-
ment of BPH with finasteride: a meta-analysis of randomised
clinical trials. Urology 1996; 48: 398–405.
76 Resnick N, Yalla SV. Detrusor hyperreflexia with impaired con-
tractile function. JAMA 1987; 257: 3076–81.
77 Terpenning MS, Allada R, Kauffman CA. Intermittent urethral
catheterisation in the elderly. JAGS 1989; 37: 411–6.
Paper received May 2003, accepted August 2003
NOCTURIA IN OLDER PEOPLE 373
ª 2004 Blackwell Publishing Ltd Int J Clin Pract, April 2004, 58, 4, 366–373