Embed Size (px)
Citation preview

HISTORY
60-year-old man.
CHIEF COMPLAINT: Progressive shortness of breath of six
months duration.
PRESENT ILLNESS: At age 56 he had an acute myocardial infarction
complicated by pulmonary edema. He was clinically stable on digitalis and
diuretics until age 58 when he had an acute right femoral artery embolism with
successful embolectomy. For the last six months he has had progressive
orthopnea and dyspnea on minimal exertion in spite of therapy.
Question: What diagnoses are suggested by this history?
48-1

48-2
Answer: With a history of myocardial infarction, atherosclerotic heart
disease is by far the the most likely basic diagnosis. To explain the embolism
and failure, some complication such as left ventricular remodeling, progressive
ischemia, arrhythmia or ventricular aneurysm must be considered.
PHYSICAL SIGNS a. GENERAL APPEARANCE – 60-year-old man who appears mildly
dyspneic at rest.
b. VENOUS PULSE - The CVP is estimated to be 7 cm H2O.
Question: How do you interpret the venous pulse?
PHONO
LOWER LEFT
STERNAL
EDGE
JUGULAR
VENOUS
PULSE
S1 S2

48-3
Answer: The estimated central venous pressure is at the upper limits of
normal and the venous wave form is normal with a dominant “a” wave due to
atrial contraction.
c. ARTERIAL PULSE - (BP = 150/90 mm Hg)
Question: How do you interpret the arterial pulse?
ECG
CAROTID
UPPER RIGHT
STERNAL EDGE
S1 S2

48-4
Answer: The arterial pulse is normal in upstroke, peak, and downstroke.
d. PRECORDIAL MOVEMENT
Question: How do you interpret the patient’s precordial movement?
ANTERIOR AXILLARY
LINE 6TH and 7TH ICS
ECG

Answer: The apical impulse is inferolaterally displaced due to left
ventricular enlargement. In this case, there is a sustained systolic impulse due
to a true “anatomic” fibrotic ventricular aneurysm. Similar bedside findings may
be present with a “physiologic” aneurysm (that is, an ischemic dyskinetic
muscle that moves outward as the rest of the ventricular muscle contracts) or
with primary myocardial disease (cardiomyopathy).
In addition, a presystolic impulse, corresponding to an S4, is present due to
atrial contraction into a poorly compliant left ventricle.
Proceed
48-5

48-6
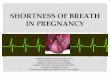
e. CARDIAC AUSCULTATION
Question: What is the likely cause of the systolic murmur at the apex?
APEXCARDIOGRAM
ECG
APEX
100 CPS
S2 S1

48-7
Answer: The murmur is likely due to mitral regurgitation from papillary
muscle dysfunction associated with outward bulging of the ventricular wall.
This is also well heard posterolateral to the mitral area over the enlarged left
ventricle. A diagram of the ventricle during maximum ejection explains the
mechanism as shown below:
Question: What is the significance of the third heart sound ?
NORMAL PATIENT
AORTA AORTA LA LA
LV LV
PP PP AP
AP
LA = left atrium AP = anterior papillary muscle
LV = left ventricle PP = posterior papillary muscle

48-8
Answer: The third heart sound reflects passive filling of the poorly
compliant left ventricle.
e. CARDIAC AUSCULTATION (continued)
Question: Based on information available by history and physical
examination, why is the second sound split in expiration?
EXPIRATION INSPIRATION
2L
ECG 2 1 1
A2 P2 A2 P2
1
0.1 sec

Answer: The second sound is paradoxically split due to the delay in aortic
valve closure associated with a prolonged pre-ejection period caused by left
ventricular dysfunction. The second sounds fuse in inspiration when the usual
prolongation of the right ventricular ejection occurs.
f. PULMONARY AUSCULTATION
Question: How do you interpret the acoustic events in the pulmonary lung
fields?
Proceed
48-9

48-10
Answer: In all lung fields, there are inspiratory and expiratory crackles,
reflecting chronic severe congestive failure.
ELECTROCARDOGRAM
(At time of first admission 4 years ago)
Question: How do you interpret this ECG?
I II III aVR aVL aVF
V1 V2 V3 V4 V5 V6

48-11
Answer: The ECG shows a left atrial abnormality and an extensive acute
anteroinferior infarction with Q waves, ST elevation and T inversion. This
implies anatomically that the entire apex of the heart is involved.
ELECTROCARDIOGRAM
(This admission)
Question: How do you interpret this ECG?
I II III aVR aVL aVF
V1 V2 V3 V4 V5 V6

Answer: The ECG shows persistence of ST-T elevation changes four years
after the infarction. Persistence of such changes for more than one month
suggests a ventricular aneurysm.
CHEST X RAY
Questions: 1. How do you interpret this chest X ray?
2. Based on the history, physical examination, ECG and chest X ray, what is
your diagnostic impression and plan to further evaluate this patient?
48-12

Answers:
1. The chest X ray shows a large left ventricular aneurysm (solid arrows)
and signs of interstitial pulmonary edema (broken arrows).
2. The history, physical examination, ECG and chest X rays are essentially
diagnostic of ventricular aneurysm. The patient has had two of
the major complications of this disease: peripheral arterial embolism and
congestive failure.
Question: What further study is indicated?
48-13

48-14
Answer: A two-dimensional echocardiogram will help define left ventricular
anatomy, function, and the presence of a clot.
LABORATORY- ECHOCARDIOGRAM
Proceed
APICAL FOUR CHAMBER
RV = right ventricle
RA = right atrium
LV = left ventricle
LA = left atrium

The echocardiogram shows a dilated left ventricle with an apical thrombus
(clot). In the real-time study it is also apparent that the apex of the left
ventricle is dyskinetic (i.e., moves paradoxically) confirming the presence of
an aneurysm.
Question: What is the third major complication of a ventricular aneurysm?
48-15

48-16
Answer: Ventricular arrhythmias.
This patient demonstrated no significant arrhythmias. Because of refractory
congestive heart failure, cardiac catheterization was carried out.
LABORATORY- CATHETERIZATION DATA
The results of the coronary anatomy and hemodynamics follow.
LEFT VENTRICULAR ANGIOGRAM

Coronary angiography showed total obstruction of the left anterior descending
(LAD) and right coronary (RCA) arteries with poor distal runoff and without
collateral flow to the area.
The left ventricular end diastolic pressure was 18 mm Hg (normal <12 mm Hg).
The left atrial pressure curve showed prominent “v” waves. The cardiac index
was 2.0 (normal 2.5 - 3.5).
Questions: 1. How do you interpret the laboratory data?
2. How would you treat this patient?
48-17

Answers:
1. The left ventricular angiogram demonstrates the ventricular aneurysm (solid
arrows) and mitral regurgitation (broken arrows outline left atrium). The
latter is supported by prominent “v” waves in the left atrial pressure curve.
The elevated left ventricular end diastolic pressure and low cardiac index
reflect the patient’s left ventricular failure.
2. If the patient’s congestive failure does not respond to maximizing his
medical therapy (i.e., adding ACE-I, anticoagulation, etc.), ventricular
aneurysmectomy is indicated. An additional though more remote indication
is his history of peripheral arterial embolism.
Proceed
48-18

The patient underwent ventricular aneurysmectomy without complication. No
coronary bypass surgery was performed as the LAD and RCA were totally
occluded without distal runoff. The patient’s mitral regurgitation was no longer
present after surgery, as the cause of his papillary muscle dysfunction had
been treated. However, in similar cases, repair or replacement of the mitral
valve have been necessary.
The patient was discharged on aspirin, a beta-blocker, an ACE-inhibitor and a
statin. He was instructed to follow a low fat diet and an exercise program based
on outpatient stress testing.
Proceed for Summary
48-19

SUMMARY
Ventricular aneurysm is almost always a complication of atherosclerotic heart
disease in which myocardial infarction, as a result of remodeling, becomes
organized into a thin, fibrous, wide-mouthed, sac-like structure which bulges
out under the force of systolic pressure. Physiologically, areas of dyskinetic or
akinetic motion are seen angiographically (and may be palpated at the bedside)
in many patients with myocardial infarction or ischemia. Persistent ST
elevation is an indication of likely ventricular aneurysm.
Proceed
48-20

SUMMARY (continued)
True ventricular aneurysms must be differentiated from false aneurysms. False
aneurysms occur when myocardial infarctions rupture and the resulting
hematoma is contained by the pericardium and becomes organized. The
mouth of the aneurysm is characteristically small. Unlike true aneurysms, false
aneurysms may rupture. The typical gross pathology of a true ventricular
aneurysm follows.
48-21

48-22
Proceed for Case Review
MITRAL VALVE
POSTERIOR
LEAFLET
LEFT ATRIUM
POSTEROMEDIAL
PAPILLARY
MUSCLE
LEFT
VENTRICULAR
ANEURYSM
MURAL
THROMBUS
APEX OF
LEFT VENTRICLE
INTERVENTRICULAR
SEPTUM
RIGHT VENTRICLE
AORTA
RIGHT ATRIUM

48-23
To Review This Case of
Ventricular Aneurysm:
The HISTORY is typical, including previous infarction, embolism due to
mural thrombus formation, and congestive failure due to dyssynergic left
ventricular contraction. Another type of presentation not seen in this patient is
ventricular arrhythmia. Note that the patient had pulmonary edema at the time
of his initial infarct, which also suggests that the infarction was extensive.
PHYSICAL SIGNS
a. The GENERAL APPEARANCE shows the patient to be mildly
dyspneic at rest.
b. The JUGULAR VENOUS PULSE mean pressure is at the upper limits of
normal, and the wave form is normal.
Proceed

c. The CAROTID PULSE is normal. The patient’s borderline hypertension
may be due to congestive failure alone, as there is a reflex increase in
peripheral resistance when cardiac output is diminished.
d. PRECORDIAL MOVEMENT reveals an inferolaterally displaced,
enlarged and sustained apical impulse. In addition, presystolic expansion of
an S4 is present, reflecting poor ventricular distensibility.
e. CARDIAC AUSCULTATION reveals paradoxic splitting of the second
sound due to a prolonged pre-ejection period from pump dysfunction. A
third sound reflects poor ventricular compliance, and the palpable fourth
sound is confirmed. Finally there is a soft midsystolic murmur of mitral
insufficiency due to papillary muscle dysfunction associated with systolic
expansion of the aneurysm.
f. PULMONARY AUSCULTATION reveals inspiratory and expiratory
crackles in all lung fields, reflecting chronic severe congestive failure.
48-24

The ELECTROCARDIOGRAM shows an anteroseptal current of
injury present for four years that is typical of ventricular aneurysm.
The CHEST X RAY reveals a large left ventricular aneurysm and signs
of interstitial pulmonary edema. Occasionally the aneurysm is calcified and this
may be seen on the X ray.
LABORATORY STUDIES including echocardiography show an
apical aneurysm and mural thrombus. Cardiac catheterization and angiography
confirm poor left ventricular function, a left ventricular aneurysm, mitral
regurgitation and total occlusion of the left anterior descending and right
coronary arteries.
TREATMENT is aneurysmectomy, as the patient has refractory failure.
48-25