Embed Size (px)
Citation preview

Nivolumab improved survival vs dacarbazine in patients with
untreated advanced melanomaGeorgina V. Long,1 Victoria Atkinson,2 Paolo A. Ascierto,3 Benjamin Brady,4 Caroline Dutriaux,5 Michele Maio,6Laurent Mortier,7 Jessica C. Hassel,8 Piotr Rutkowski,9 Catriona McNeil,10 Ewa Kalinka‐Warzocha,11 Kerry J. Savage,12 Micaela Hernberg,13 Celeste Lebbé,14 Julie Charles,15 Catalin Mihalcioiu,16 Vanna Chiarion‐Sileni,17Cornelia Mauch,18 Henrik Schmidt,19 Dirk Schadendorf,20 Helen Gogas,21 Christine Horak,22 Brian Sharkey,23
Ian M. Waxman,22 Caroline Robert241Melanoma Institute Australia, University of Sydney, and Mater Hospital, Sydney, Australia; 2Princess Alexandra Hospital, Wooloongabba & Gallipoli Medical Research Foundation, Greenslopes Private Hospital Queensland, Australia; 3Istituto Nazionale Tumori Fondazione Pascale, Naples, Italy; 4Cabrini Health, Melbourne, Australia; 5Hôpital Saint André CHU, Bordeaux, France; 6University Hospital of Siena, Siena, Italy; 7Hôpital Claude Huriez, Lille, France; 8University Hospital Heidelberg & National Center for Tumor Diseases, Heidelberg; 9Maria Sklodowska‐Curie Memorial Cancer Center & Institute of Oncology, Warsaw, Poland; 10Chris O'Brien Lifehouse, The
Melanoma Institute Australia & Royal Prince Alfred Hospital, Camperdown; 11Wojewodzki Szpital Specjalistyczny im. M. Kopernika, Lodz, Poland; 12British Columbia Cancer Agency, Vancouver, Canada, Canada; 13Department of Oncology, Helsinki University Central Hospital, Helsinki, Finland; 14APHP Dermatology and CIC Hôpital Saint Louis Paris
7 University, INSERM 976, Paris, France; 15Grenoble University Hospital Grenoble France ‐ INSERM U823, Joseph Fourier University, Grenoble, France; 16Royal Victoria Hospital, Alberta, Canada; 17Oncology Institute of Veneto IRCCS, Padua, Italy; 18Department of Dermatology, University Hospital Cologne and CIO Köln Bonn, Germany;
19Department of Oncology, Aarhus University Hospital, Aarhus, Denmark; 20Department of Dermatology, University of Essen, Essen, Germany; 21University of Athens Medical School, Laiko General Hospital, Athens, Greece; 22Bristol‐Myers Squibb, Lawrenceville, NJ, U.S.A.; 23Bristol‐Myers Squibb, Wallingford, CT, U.S.A.; 24Gustave, Roussy and
INSERM U981, Villejuif‐Paris‐Sud, France

Disclosures• Employment or Leadership Position: None • Consultant/Advisory Role: Bristol‐Myers Squibb,
Roche‐Genentech, Merck Sharp & Dohme, Glaxo Smith‐Kline, Ventana, Novartis, Amgen
• Stock Ownership: None • Honoraria: Bristol‐Myers Squibb, Roche‐Genentech,
Glaxo Smith‐Kline• Research Funding: Bristol‐Myers Squibb, Roche‐Genentech,
Merck Sharp & Dohme, Ventana• Expert Testimony: None• Other Remuneration: None

BackgroundUnmet need in metastatic melanoma • > 50% patients have BRAF wild‐type tumor1
• Only ipilimumab has OS benefit in this group of patients2,3
Nivolumab• A fully human anti‐PD‐1 monoclonal antibody4 with clinical benefit5–8
Phase 1 Study 0035,6
1‐Year 2‐Year 3‐Year 4‐Year
OS 63% 48% 42% 32%
Phase 3 Study CheckMate‐0377,8
Nivolumab3 mg/kg Q2W
Investigator’s Choice of
Chemotherapy
ORR 32% 11%
1. Long et al. J Clin Oncol 2011; 2. Hodi et al. N Engl J Med 2010; 3. Robert et al. N Engl J Med 2011; 4. Wang et al. Cancer Immunol Res 2014;5. McDermott et al. ESMO 2014; 6. Hodi et al. SMR 2014; 7. Weber et al. ESMO 2014; 8. D’Angelo et al. SMR 2014.

Phase 3 CheckMate‐066: Study Design
Treat untilprogression* or unacceptabletoxicity
Primary endpoint: • OS
Secondary endpoints:• PFS• ORR• PD‐L1 correlates
R1:1
Nivolumab3 mg/kg IV Q2W
+Placebo IV Q3W
N=210 (206 treated)
Placebo IV Q2W
+Dacarbazine
1000 mg/m2 IV Q3W
N=208 (205 treated)
Double‐blind
Eligible patients with unresectable stage IIIor IV melanoma(N=418)
• BRAF wild‐type• Treatment‐naïve
Stratified by:
• PD‐L1 status(≥ 5% cell‐surfacestaining cutoff)
• M‐stage
*Patients may be treated beyond initial RECIST v1.1‐defined progression if considered by the investigator to be experiencing clinical benefit and tolerating study drug.

Data Monitoring Committee Review
• An ad hoc review determined clear survival benefit and recommended on 10 June 2014:– Unblind the study– Allow patients assigned to dacarbazine who had ended study treatment to receive nivolumab
• Results presented here are based on a clinical cutoff date of 24 June 2014,* prior to any patient from the dacarbazine arm receiving nivolumab
*Database lock was on 5 August 2014.

Baseline CharacteristicsNivolumab(N = 210)
Dacarbazine(N = 208)
AgeMedian (range) 64 (18–86) 66 (26–87)
GenderMale 58% 60%
ECOG Performance Status0 71% 58%1 29% 40%
M‐stageM0/M1a/M1b 39% 39%M1c 61% 61%
Baseline lactate dehydrogenase levels≤ Upper limit of normal range 62% 64%> Upper limit of normal range 38% 36%
PD‐L1 statusPositive (≥ 5% tumor cell‐surface staining) 35% 36%Negative/indeterminate 65% 64%

Primary Endpoint: Overall Survival
0 3 6 9 12 15 18
Patients whodied, n/N
Median OS mo (95% CI)
Nivolumab 50/210 NR
Dacarbazine 96/208 10.8 (9.3–12.1)
NR = not reached.Based on 5 August 2014 database lock.
100
90
80
70
60
0
50
40
30
20
10
HR 0.42 (99.79% CI, 0.25–0.73; P < 0.0001)(Boundary for statistical significance 0.0021)
Nivolumab (N = 210)
Dacarbazine (N = 208)
Months
Patie
nts Surviving (%
)
1‐yr OS 73%
1‐yr OS 42%
210208
185177
150123
10582
4522
83
00
Patients at RiskNivolumabDacarbazine
Follow‐up since randomization: 5.2–16.7 months

Secondary Endpoint: PFSDeath or diseaseprogression, n/N
Median PFS mo (95% CI)
Nivolumab 108/210 5.1 (3.5–10.8)
Dacarbazine 163/208 2.2 (2.1–2.4)
HR 0.43 (95% CI, 0.34–0.56; P < 0.0001)
Patie
nts With
out P
rogression
(%)
Dacarbazine (N = 208)
Nivolumab (N = 210)
6‐mo PFS 48%
6‐mo PFS 19%
100
90
80
70
60
0
50
40
30
20
10
0 3 6 9 12 15 18Months
Patients at RiskNivolumabDacarbazine
210208
11674
8228
5712
120
10
00
Based on 5 August 2014 database lock.
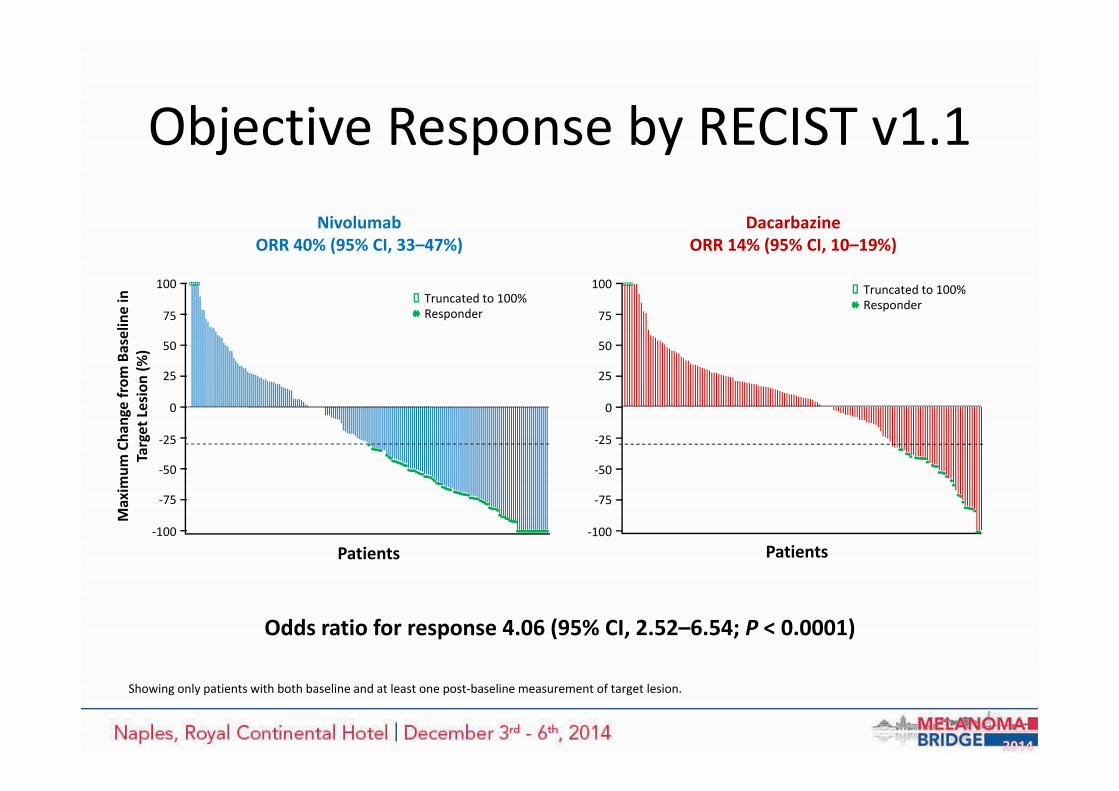
Objective Response by RECIST v1.1
Odds ratio for response 4.06 (95% CI, 2.52–6.54; P < 0.0001)
ResponderTruncated to 100%
Maxim
um Cha
nge from
Baseline in
Target Lesion (%
)
Patients
DacarbazineORR 14% (95% CI, 10–19%)
100
75
50
25
0
‐25
‐50
‐75
‐100
Nivolumab ORR 40% (95% CI, 33–47%)
Patients
100
75
50
25
0
‐25
‐50
‐75
‐100
Showing only patients with both baseline and at least one post‐baseline measurement of target lesion.
ResponderTruncated to 100%

Best Overall Response
Nivolumab(N = 210)
Dacarbazine(N = 208)
ORR, % (95% CI) 40% (33–47%) 14% (10–19%)
Best overall response
Complete response 8% 1%
Partial response 32% 13%
Stable disease 17% 22%
Progressive disease 33% 49%
Unable to determine 11% 15%
Based on 5 August 2014 database lock.

Time to and Durability of Response
Nivolumab Dacarbazine
Time to response, median (range), mo
2.1 (1.6–7.6)
2.1 (1.8–3.6)
Duration of response, median (range), mo NR 6.0
(3.0–NR)
Ongoing response among respondersa 72/84 (86%) 15/29 (52%)
aAt the time of the last follow‐up; NR=Not reached
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 54 57 60 63 66 69 72 75 78
Time (Week)
Nivolum
ab(84/210)
Dacarba
zine
(29/208)
Patie
nts
(no. of respo
nders/no
. ran
domize
d)
On treatmentOff treatmentFirst responseOngoing responseDeath

Patients Treated BeyondRECIST v1.1 Progression
Patients with RECIST v1.1 progression, but achieved or maintained a ≥ 30% reduction in the target lesion tumor burden• Nivolumab = 17 (8% of all 210 randomized) • Dacarbazine = 8 (4% of all 208 randomized)
Nivolumab Group, n = 54 Dacarbazine Group, n = 49
Chan
ge from
Baseline in
Target Lesion Size (%
)
Time Since Treatment Initiation (Weeks) Time Since Treatment Initiation (Weeks)
100
75
50
25
0
‐25
‐50
‐75
‐1000 6 12 18 24 30 36 42 48 54 60 66
100
75
50
25
0
‐25
‐50
‐75
‐1000 6 12 18 24 30 36 42 48 54 60 66
1st occurrence of new lesionPatient still on treatment
Complete or partial response% change truncated to 100%

ORR by PD‐L1 Status*
*PD‐L1 positive: ≥ 5% tumor cell surface staining. PD‐L1 negative: < 5% tumor cell surface staining.Based on 5 August 2014 database lock.
0 10 20 30 40 50 60 70
PD‐L1+
PD‐L1‐
ORR (%) (95% CI)
Nivolumab (N=210)
Dacarbazine (N=208)
53% (41–64%)
11% (5–20%)
33% (25–42%)
16% (10–23%)
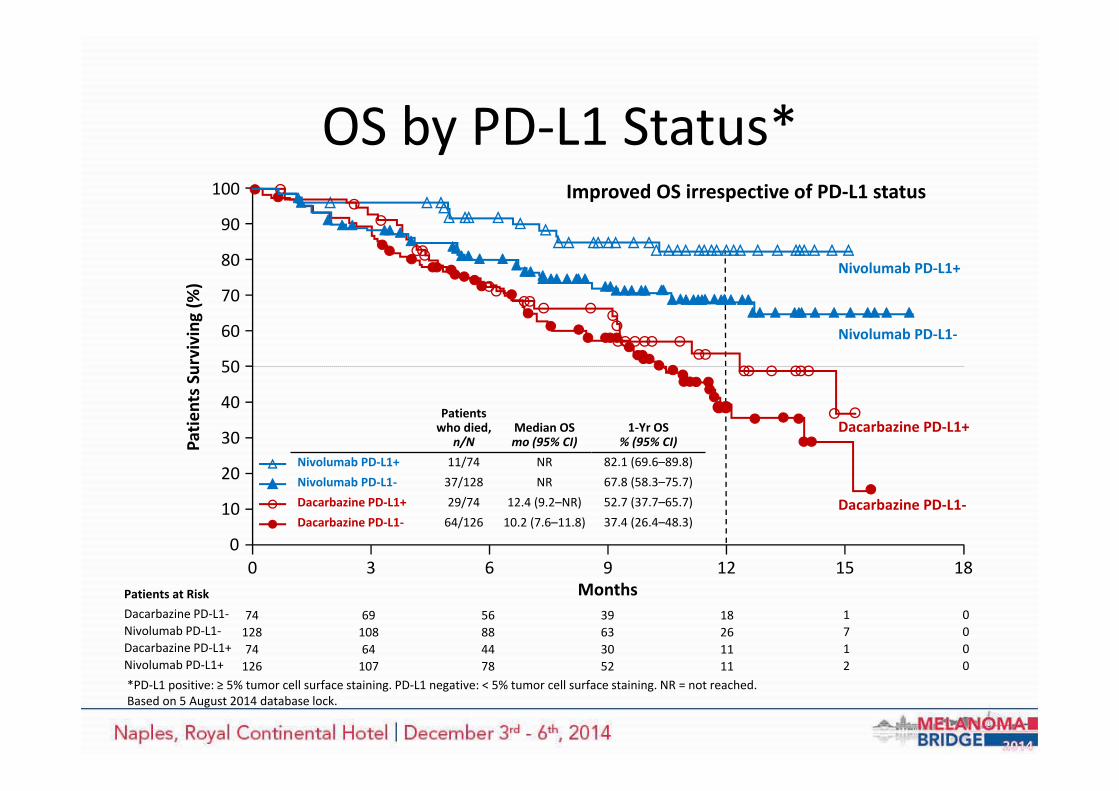
OS by PD‐L1 Status*Improved OS irrespective of PD‐L1 status100
90
80
70
60
0
50
40
30
20
10
0 3 6 9 12 15 18Months
Nivolumab PD‐L1+
Dacarbazine PD‐L1+
Nivolumab PD‐L1‐
Dacarbazine PD‐L1‐
Patients at RiskDacarbazine PD‐L1‐Nivolumab PD‐L1‐Dacarbazine PD‐L1+Nivolumab PD‐L1+
7412874126
6910864107
56884478
39633052
18261111
1712
0000
Patie
nts Surviving (%
)
1‐Yr OS% (95% CI)
82.1 (69.6–89.8)67.8 (58.3–75.7)52.7 (37.7–65.7)37.4 (26.4–48.3)
Patients who died,
n/NMedian OS mo (95% CI)
Nivolumab PD‐L1+ 11/74 NRNivolumab PD‐L1‐ 37/128 NRDacarbazine PD‐L1+ 29/74 12.4 (9.2–NR)Dacarbazine PD‐L1‐ 64/126 10.2 (7.6–11.8)
*PD‐L1 positive: ≥ 5% tumor cell surface staining. PD‐L1 negative: < 5% tumor cell surface staining. NR = not reached.Based on 5 August 2014 database lock.

OS in Pre‐defined Subgroups
*OS difference is not displayed if sample size is less than 10 subjects in any treatment group.LDH = lactate dehydrogenase; ULN = upper limit of normal range.
OS DifferenceNivolumab Dacarbazine Unstratified HR for death (95% CI)
N No. of death / No. randomized
All patients 418 50/210 96/208PD‐L1 status
Positive 148 11/74 29/74Negative/indeterminate 270 39/136 67/134
M‐stage at study entryM0/M1a/M1b 163 11/82 29/81M1c 255 39/128 67/127
History of brain metastasesYes* 15 1/7 2/8No 403 49/203 94/200
Baseline LDH≤ ULN 245 16/120 38/125> ULN 153 29/79 53/74
Nivolumab better Dacarbazine better
0 1 2

Adverse Event Overview
There were no deaths related to study drug toxicity in either arm
Nivolumab(N = 206)
Dacarbazine(N = 205)
Patients reporting, n (%)AnyGrade
Grade3–4
AnyGrade
Grade3–4
Drug‐related AE 153 (74) 24 (12) 155 (76) 36 (18)
Serious drug‐related AE 19 (9) 12 (6) 18 (9) 12 (6)
Drug‐related AE leading todiscontinuation 5 (2) 4 (2) 7 (3) 5 (2)

Treatment‐Related AEs Reportedin ≥ 10% of Patients
Patients reporting AE, n (%)
Nivolumab (N = 206)
Dacarbazine (N = 205)
Any GradeGrade 3–4 Any Grade
Grade 3–4
Any treatment‐related adverse event 153 (74) 24 (12) 155 (76) 36 (18)Fatigue 41 (20) 0 30 (15) 2 (1)Pruritus 35 (17) 1 (1) 11 (5) 0Nausea 34 (17) 0 85 (42) 0Diarrhea 33 (16) 2 (1) 32 (16) 1 (1)Rash 31 (15) 1 (1) 6 (3) 0Vitiligo 22 (11) 0 1 (1) 0Constipation 22 (11) 0 25 (12) 0Asthenia 21 (10) 0 25 (12) 1 (1)Vomiting 13 (6) 1 (1) 43 (21) 1 (1)Neutropenia 0 0 23 (11) 9 (4)Thrombocytopenia 0 0 21 (10) 10 (5)

Treatment‐Related Immune‐Mediated Adverse Events
Majority of all grade drug‐related immune‐mediated AEs resolved and were manageable using recommended guidelines
Patients reporting immune‐mediated AE (organ category), n (%)
Nivolumab (N = 206) Dacarbazine (N = 205)
Any Grade Grade 3–4 Any Grade Grade 3–4Skin 77 (37) 3 (2) 29 (14) 0
Pruritus 35 (17) 1 (1) 11 (5) 0Rash 31 (15) 1 (1) 6 (3) 0Vitiligo 22 (11) 0 1 (1) 0
Gastrointestinal 35 (17) 3 (2) 32 (16) 1 (1)Diarrhea 33 (16) 2 (1) 32 (16) 1 (1)
Endocrine 15 (7) 2 (1) 1 (1) 0Hypothyroidism 9 (4) 0 1 (1) 0Hyperthyroidism 7 (3) 0 0 0Hypophysitis 1 (1) 1 (1) 0 0
Hepatic 7 (3) 3 (2) 8 (4) 2 (1)Pulmonary 3 (2) 0 0 0
Pneumonitis 3 (2) 0 0 0Renal 4 (2) 1 (1) 1 (1) 0
Conclusions• In treatment‐naïve, BRAF wild‐type patients with metastatic melanoma,
nivolumab led to significant improvements over dacarbazine in– Overall survival– Progression‐free survival– Objective response rates
• The survival benefit of nivolumab vs dacarbazine was observed irrespective of tumor PD‐L1 status, and across all pre‐defined subgroups
• Safety profile of nivolumab was acceptable, manageable, and consistent with previous reports1‐4
• Nivolumab represents a potential new standard of care for patients with BRAF wild‐type advanced melanoma
1.Topalian et al. N Engl J Med 2012; 2. Topalian et al. J Clin Oncol 2014; 3. McDermott et al. ESMO 2014; 4. Weber et al. ESMO 2014.
Acknowledgments• The patients and their families
• Investigators and members of the clinical study teams in:
– Argentina, Australia, Canada, Chile, Denmark, Finland, Germany, Ireland, Italy, Israel, Mexico, Netherlands, New Zealand, Norway, Poland, Spain, Sweden, Switzerland, United Kingdom
• Dako for collaborative development of the automated PD‐L1 immunohistochemistry assay
• Study sponsored by Bristol‐Myers Squibb
• All authors contributed to and approved the presentation; writing and editorialassistance with preparation of the slides was provided by Wayne Peng and Karin McGlynn of StemScientific, funded by Bristol‐Myers Squibb






























