Embed Size (px)
Citation preview

Vol. 5. 47-52. Ja,iuars#{149}1996 Cancer Epidemiology, Biomarkers & Prevention 47
Nitrite, N-Nitroso Compounds, and Other Analytes in Physiological
Fluids in Relation to Precancerous Gastric Lesions’
w-c. You,2 L. Zhang, C-S. Yang, Y-S. Chang, H. Issaq,S. D. Fox, W. E. Utermahlen, L. Zhao, L. Keefer,W-D. Liu, W-H. Chow, J-L. Ma, R. Kneller,M. Y. K. Ho, J. F. Fraumeni, Jr.,3 G-W. Xu, andW. J. Blot
Beijing Institute for Cancer Research and School of Oncology. Beijing
Medical University. Beijing 10(8)34 lW-C. Y.. L. Zhang. L. Zhao, G-W. Xl,
Weifang Medical Institute. Weifang. Shandong 261041 IY-S. C., J-L.Ml, and
Linqu Public Health. Linqu County. Shandong 262600 IW-D. LI, China:
Lalxrators for Cancer Research, Rutgers University. Piscataway. New Jersey
08855 [C-S. Y.[: PRIIDynCorp lB. I.. S. D. F.. W. E. U.l and Laboratory of
Comparative Carcinogenesis [L. K.. M. Y. K. H.[. National Cancer Institute-
Frederick Cancer Research and Development Center. Frederick. Maryland
21702: National Cancer Institute. Bethesda, Maryland 20892 [W-C. Y..W-H. C.. R. K.. J. F. F.[: International Epidemiology Institute, Ltd., Rockville,
Maryland 20850 [W. J. B.[
Abstract
Levels of gastric juice nitrite, several urinary N-nitrosocompounds, and other analytes were examined amongnearly 600 residents in an area of Shandong, China,where precancerous gastric lesions are common and ratesof stomach cancer are among the world’s highest. Gastricjuice nitrite levels were considerably higher among thosewith gastric juice pH values above 2.4 versus below 2.4.Nitrite xsas detected more often and at higher levelsamong persons with later stage gastric lesions, especiallywhen gastric pH was high. Of those with intestinalmetaplasia, 17.5% had detectable levels of gastric nitrite,while this analyte was detected in only 7.2% of those withless advanced lesions. Relative to those with undetectablenitrite, the odds of intestinal metaplasia increased from1.5 (95% confidence interval 0.6-4.1) to 4.1 (95%
confidence interval = 1.8-9.3) among those with low andhigh nitrite concentrations, respectively. Urinaryacetaldehyde and formaldehyde levels also tended to behigher among those with more advanced pathology,particularly dysplasia. However, urinary excretion levelsof total N-nitroso compounds and several nitrosaminoacids differed little among those with chronic atrophicgastritis and intestinal metaplasia and dysplasia,consistent with findings from recent studies in the UnitedKingdom, France, and Colombia. The data from this
Received 6/1/95: revised 8/25/95: accepted 9/5/95.The costs of publication of this article were defrayed in part by the payment of
page charges. This article must therefore be hereby marked advertisement in
accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
I This study was supported in part by National Cancer Institute contracts NOI-
CP- I 5620. NO I -CP-0563 I . NO I -CP-2 I (8)9. and NO I -CP-3304 I.
2 To whom requests for reprints (China) should be addressed. at Beijing Institute
for Cancer Research and School of Oncology. Beijing Medical University.
Beijing 1(88)34. China.
‘ To who,i: requests for reprints (all other countries) should be addressed. at
National Citcer Institute, EPN Ro�m 543, Bethesda, MD 20892.
high-risk population suggest that elevated levels of gastricnitrite, especially in a high pH environment, areassociated with advanced precancerous gastric lesions,although specific N-nitroso compounds were notimplicated.
Introduction
NOC,4 especially nitrosamides such as N-methyl-N’-nitro-N-
nitrosoguanidine, have long been suspected as gastric carcino-gens, perhaps affecting early stages of the carcinogenic process(1, 2). This hypothesis has stimulated several investigations ofintragastric nitrosation in individuals with precancerous gastric
lesions, but results have been mixed (3-10). In an epidemio-logical study in Linqu, a rural area in China’s Shandong prov-ince with one of the world’s highest rates of stomach cancer, wefound several factors related to nitrosation to be associated with
risk of this cancer ( 1 1 ). In particular, risk was elevated amongthose who consumed sour pancakes, in which mutagenic activ-ity and NOC have been detected, and was lower among thosewith high intakes of allium vegetables. a-carotene, and vitaminC, which may inhibit the formation of NOC. Additional studyhas indicated that the prevalence of precancerous gastric lesions
in this area is exceptionally high. with one-half of the residentsages 35-64 years diagnosed with IM and 20% with gastricdysplasia ( 12). Herein we report results of a quantitative anal-ysis of gastric juice nitrite and urinary NOC excretion amongpersons with precancerous lesions.
Materials and Methods
Individuals in the present study participated in a gastroscopicscreening survey during 1989-1990 in 14 villages in Linqu
County. Details are described in an earlier report (1 2). In brief,a total of 3433 adults, representing 83% of eligible residents
ages 35-64 years, received a physical and endoscopic exami-nation. The gastric mucosa was observed visually by a gastro-enterologist, and seven biopsies were taken from the followingstandard locations: two from the body; one from the angulus;and four from the antrum of the stomach. In two of the villages.an eighth biopsy was taken from within 2 cm of the cardia alongthe lesser curvature.
Biopsy diagnoses were based on criteria proposed by theChinese Gastric Pathology Association after review by expertson stomach pathology in both China and the United States (13).Each slide was reviewed by three senior pathologists at theBeijing Institute for Cancer Research (Beijing, China), and aconsensus diagnosis was made. The presence or absence of 5G.
4 The abbreviations used are: NOC, N-nitroso compounds: IM. intestinal meta-
plasia; SG, superficial gastritis; CAG, chronic atrophic gastritis: NPRO. N-
nitrosoproline; NMTCA, N-nitroso-2-methyl-thiazolidine 4-carboxylic acid:NTCA. N-nitrosothiazolidine 4-carboxylic acid: OR. odds ratio: Cl. confidence
interval.
on April 9, 2019. © 1996 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

48 Nitrosation as a Risk Factor in Gastric Lesions
CAG, lM, or dysplasia was recorded for each biopsy, and eachsubject was given an overall diagnosis based on the most severe
histology. Almost always IM occurred in the presence of CAG,
and dysplasia almost always occurred in the presence of IM in
the same or a different biopsy (12).During the physical examination, fasting gastric juice and
overnight urine specimens were collected from approximately600 subjects selected at random, representing nearly 20% of theparticipants in this survey. A l500-ml plastic jar was providedfor each participant for overnight urine collection. An aliquot of
50 ml of urine from each subject was transferred to a centrifugetube, spiked with 25 �.d of an aqueous internal standard solutionof 0.15 mM in N-methyl-N-nitroso-�-a1anine and 1.5 mM in
piperidine 2-carboxylic acid, and immediately frozen onalcohol-dry ice. Fasting gastric juice was collected through aplastic tube from the individuals during the endoscopic exam-
ination. The pH was measured by using a pH meter (DigitalCo.) immediately after the collection of gastric juice. The urineand gastric juice specimens were stored at -20#{176}Cand then
moved into a -70#{176}Cfreezer within 2 or 3 days. The urine andgastric juice specimens, packed with dry ice, were shipped tothe National Cancer Institute’s Frederick Cancer Research andDevelopment Center (Frederick. MD) for analysis of NOC and
other substances.The nitrosamino acids, NPRO, c’is- and trans-NMTCA,
and NTCA, were quantified by the method of Ohshima andBartsch ( 14), adapted as follows. Fifteen ml of urine weremixed with S g of sodium chloride and 2 ml of 20% ammoniumsulfamate in 1 .8 M sulfuric acid. The resulting solution was
extracted three times with 25 ml of 10% methanol in dichlo-
romethane. The combined extracts were dried over anhydroussodium sulfate, evaporated to dryness. dissolved in 0.5 ml of
diethyl ether, and derivatized by treatment with a diazometh-ane-ether solution. The latter was prepared by dropping a so-
lution of N-methyl-N-nitroso-p-toluenesulfonamide (Dia.zald;Aldrich Chemical Co., Milwaukee, WI) in diethyl ether into awarm, stirring mixture of S g of potassium hydroxide with 20ml of 50% aqueous ethanol and distilling out the diazomethane-ether solution, 2 ml of which were added to the sample. The
ether was evaporated, and the residue was dissolved in 0. 1 mlofdichloromethane. The resulting solution was analyzed by gaschromatography on a capillary column coated with a l-�m
layer of DB-FFAP (J & W Scientific. Folsom, CA) held at 75#{176}Cfor 2 mm and then programmed at 10#{176}C/mmto 200#{176}C,whereit was held for 10 mm. Helium flow rate was 10 ml/min.Temperature of the injector was 250#{176}C,whereas that of thetransfer line connecting the column to the nitrosamine-specificchemiluminescence detector (TEA Model 610 Nitrogen ana-lyzer; Thermedics, Inc., Woburn, MA) was 225#{176}C.The inte-grals of the peaks, the retention times of which correspond tothose of separately injected authentic NPRO, NTCA, and cis-
and trans-NMTCA standards were compared to that of theinternal standard, N-methyl-N-nitroso-�-alanine, to infer theconcentration of each analyte in the urine. Standard curves
prepared by analyzing spiked urines revealed that response waslinear to >20 ng/ml for each compound, with detection limitsof 0.1-0.2 ng/ml each. Detection of N-nitrosopiperidine 2-
carboxylic acid was taken as evidence for artifactual N-nitro-
sation after the sample was collected; < 1 % of the samplescontained detectable N-nitrosopiperidine 2-carhoxylic acid, andthe highest value seen was 2 ng/ml.
Nitrate was determined by ion chromatography. Urine(500 p.1) or gastric juice ( 1(X) Ml) was diluted to 3 ml withdeionized water. The resulting mixture was first passed througha Burdick and Jackson (Baxter Healthcare Corp., Muskegon,
MI) Solid Phase System 200-mg Octadecyl (C18) column, thenthrough an Alltech Associates (Deerfield. IL) IC-Ag� cartridge
column for cleanup. The first milliliter of the eluate was dis-
carded, and 50 �l of the subsequent eluate was injected onto a
Dionex (Sunnyvale, CA) lonPac ASS column in a Dionex ionchromatography apparatus. By using a mobile phase preparedby dissolving 240 mg of sodium carbonate and 470 mg ofsodium bicarbonate in 1 liter of deionized water (flow rate 1.5ml/min), the nitrate signal was quantified by integrating theconductivity detector response and comparing the result tothose obtained for separately injected standard nitrate solutions.
Nitrite was assayed using the colorimetric Griess reagent( 15). A solution of 10 g of sulfanilamide/liter of 5% phosphoricacid was mixed with an equal volume of a second solutioncontaining 1 g of N-(l-naphthyl) ethylenediamine dihydrochlo-ride/liter of water. Two ml of the resulting solution were mixedwith urine or gastric juice (diluted as necessary to I ml) in a
disposable cuvette, and the absorbance at 546 nm was measured5 mm later. Absorbance was converted to nitrite concentration
via a calibration curve prepared from standard solutions con-taming authentic nitrite at concentrations of 0. 1-5 p�g/ml.
Total NOC values were determined by the method ofJanini et al. (16). Aliquots (1 ml) of urine or gastric juice werepassed through a 0.45-sm nylon filter, treated with 250 p.1 of20% aqueous sulfamic acid, and filtered through a 0.2-�tmnylon filter. A S0-pJ aliquot of the resulting solution was
introduced into a Nitrolite photolysis unit (Thermedics, Inc.),where it was irradiated with a mercury vapor lamp. Photolyt-ically released nitric oxide was swept through two cold traps
(the first held near 0#{176}Cand the second �-80#{176}C) into the
chemiluminescence chamber of a Model 502A Thermal EnergyAnalyzer (Thermedics, Inc.) by flushing the photolysis unitwith helium at the rate of 20 mllmin. The integral of the nitricoxide signal was compared to those of N-nitrosopiperidine
4-carboxylic acid standards to provide a measure of the totalNOC concentration in the sample.
Formaldehyde and acetaldehyde were analyzed by themethod of Farrelly (17). Briefly, urine was diluted as necessaryto 1 ml and mixed with 1.25 mg of 2,4-dinitrophenylhydrazine
dissolved in 0.5 ml of 6 M hydrochloric acid. The resultingsolution was extracted with S ml of isooctane that had been
purified by distillation from a pot containing 2,4-dinitrophenyl-hydrazine. The isooctane layer was extracted in turn with 1 mlof acetonitrile that had also been distilled from 2,4-dinitrophe-nylhydrazine. Aliquots of the acetonitrile extract were analyzedby high-pressure liquid chromatography on a Hewlett PackardModel 1090 chromatograph (Rockville, MD) equipped with a250 mm X 4.6-mm column of Hypersil ODS (Hewlett Pack-
ard). The flow rate for the mobile phase (55:45 of acetonitrile:water) was 1 ml/min, with detection at 340 nm. Peak areas werecompared to those of standards of known composition to obtainthe concentrations of the aldehydes in urine and gastric juice.
Sodium ion concentrations were measured with the aid ofa Perkin Elmer Cetus Model 5000 Atomic Absorption unit(Norwalk, CT) at 589 nm, with power set to 7 mA. Urine was
diluted l04-fold with deionized water before analysis, and so-dium ion levels were read from a response curve prepared byplotting concentration versus response for various dilutions of
the 1000 ppm Fisher Scientific Co. (Pittsburgh, PA) standardsolution.
Proline and arginine were determined by the method ofEinarsson et al. (18). Four-hundred �l of urine (diluted 1:100)
were mixed with 100 jil of 1 M boric acid (adjusted to pH 6.2with 5 M sodium hydroxide) and 500 �l of S msi 9-fluorenyl-methylchloroformate in acetone. After 40 s of reaction, the
on April 9, 2019. © 1996 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Cancer Epidemiology, Biomarkers & Prevention 49
Table I Correlatio n coeffici ents#{176}among gas tric juice nitrite, the uri nary corn pounds. an d serum micronutrients
Gastric
NO,
Urinary Serum
NO� Total NOC NPRO trans-NMTCA cis-NMTCA NTCA CH2O CH3CHO Arginine Proline Na4Vitamin a-carotene
NO� 1(8) -0.01 0.87k 005 0.10” 0.12” 0.4l� -0.01 0.01 0.04 -0.()4 0.15” 0.01 -0.05
NO, 1.00 0.05 0.13” 0.07 0.06 0.19” 0.01 0.02 0.04 0.18” 0.34k 0.15” 0.11
Total NOC 1.00 0.18” O.32� 0.36” 0.49” 0.02 0.01 0.04 0.10 0.18” -0.05 -0.09
NPRO 1.00 0.l3� 0.1 1” 0.3l� -0.02 0.01 0.04 0.07 0.08’ -0.04 0.05
tra,is-NMTCA 1.00 0.98k O.28� -0.01 -0.02 0.03 -0.05 0.10” -0.08 0.01
cis-NMTCA 1.00 0.29” -0.02 -0.01 0.02 -0.04 0.07 -0.1 I’ 0.02
NTCA 1.00 0.02 0.1 1b -0.02 0.09 0.17” -0.04 0.08
CH2O 1.00 0.12” -O.�4 -0.05 0.10” -0.08 0.09
CH1CHO 1.00 -0.03 0.03 0.07 -0.09 0.05
Arginine 1.00 0.l4� 0.2l� -0.05 -0.12
Proline l.O() 0.27” 0.04 0.04
Na ‘ I .00 0. 12� -0.01
VitaminC 1.00 -0.07
fl-carotene I .00
,‘ Correlations computed among persons with detectable levels of each pair of compounds.
“P < 0.01.,. P < 0.05.
resulting solution was extracted twice with 3 ml of4: 1 pentane:
ethyl acetate. The aqueous phase was analyzed on the samehigh-pressure liquid chromatographic system described abovefor the aldehyde analysis, except that the column was 20-cmlong, and detection was by fluorescence at 340 nm with exci-tation at 260 nm. The mobile phase for the first 12 mm afterinjection was 50:40: 10 acetic acid buffer:methanol:acetonitrile
and 50:50 acetic acid buffer:acetonitrile thereafter. The acetic
acid buffer was prepared by adding 3 ml of acetic acid and 1 mlof triethylamine to 1 liter of distilled water and adjusting the pHto 4.2 with sodium hydroxide. Flow rate was 0.8 mi/mm.Quantitation was accomplished via a calibration curve.
Creatinine (19) was determined by mixing 40 �l of urine,400 p.1 of 1 M sodium hydroxide, and 2 ml of saturated aqueouspicric acid solution and then diluting it 10 mm later with waterto I 0 ml. The absorbance at 530 nm was measured I S mm afterdilution and compared to a standard curve to obtain the creat-mine concentration.
In the gastric juice samples, nitrite, total NOC, and nitro-samino acids were measured, but only nitrite levels are pre-sented because levels of the NOC were very low or undetect-able in the large majority of samples. Serum levels of ascorbic
acid and �3-carotene, assayed by high-pressure liquid chromato-graphic methods, were also available for most of these individ-
uals (20).Spearman correlation coefficients were calculated as mea-
sures of association between pairs of analytes. Geometricmeans and SDs were calculated for each compound, the distri-butions of which tended to be skewed. The means were deter-
mined for strata defined by sex, age, gastric juice pH, cigarettesmoking status (determined during standardized interviews thataccompanied the screening examinations), and gastric mucosahistology. Most analyses examined two histology categories,the first combining SG and CAG and the second being IM withor without accompanying dysplasia. There were no individualswith normal mucosa in every biopsy, and only about 2% pre-sented with normal mucosa or SG on every biopsy. Thus, the
category of normal mucosa/SG could not be used as a referencegroup. Instead, ORs were computed as measures of associationbetween the compounds and risk of IM with or without accom-panying dysplasia relative to the risk of SG/CAG, adjusting forsex, age, and smoking status (risk factors for IM/dysplasia; Ref.
2 1 ) in logistic regression models (22). We also calculated ORsseparately for dysplasia and for IM without dysplasia. but
because these ORs tended to be similar we do not report them,except for several analytes where the patterns for dysplasiadiffered from those for IM.
Results
Data were available on individual gastric juice, urinary, orserum compounds for up to 583 persons (3 12 males and 271
females). Among these study subjects, none had all normalbiopsies, 8 had SG as the most severe histological diagnosis,
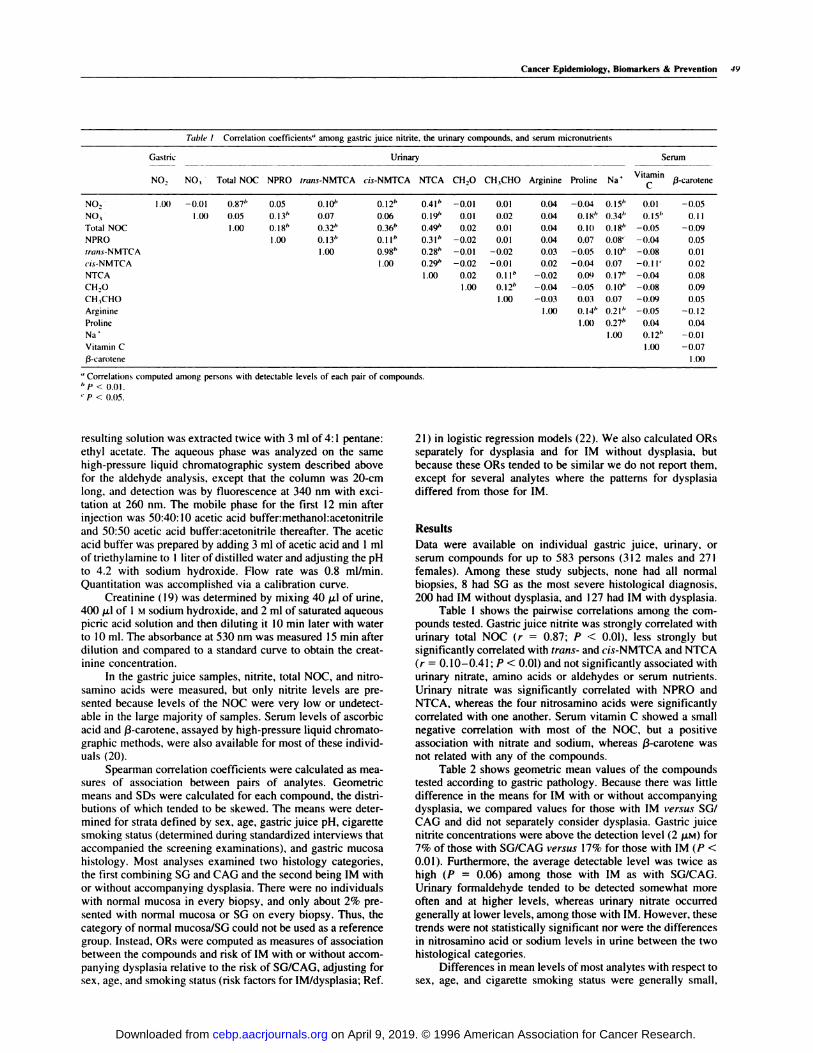
200 had IM without dysplasia, and I 27 had IM with dysplasia.Table 1 shows the pairwise correlations among the com-
pounds tested. Gastric juice nitrite was strongly correlated withurinary total NOC (r = 0.87; P < 0.01), less strongly butsignificantly correlated with tnans- and cis-NMTCA and NTCA
(n 0. 10-0.41 ; P < 0.01) and not significantly associated withurinary nitrate, amino acids or aldehydes or serum nutrients.
Urinary nitrate was significantly correlated with NPRO andNTCA, whereas the four nitrosamino acids were significantly
correlated with one another. Serum vitamin C showed a smallnegative correlation with most of the NOC, but a positive
association with nitrate and sodium, whereas a-carotene wasnot related with any of the compounds.
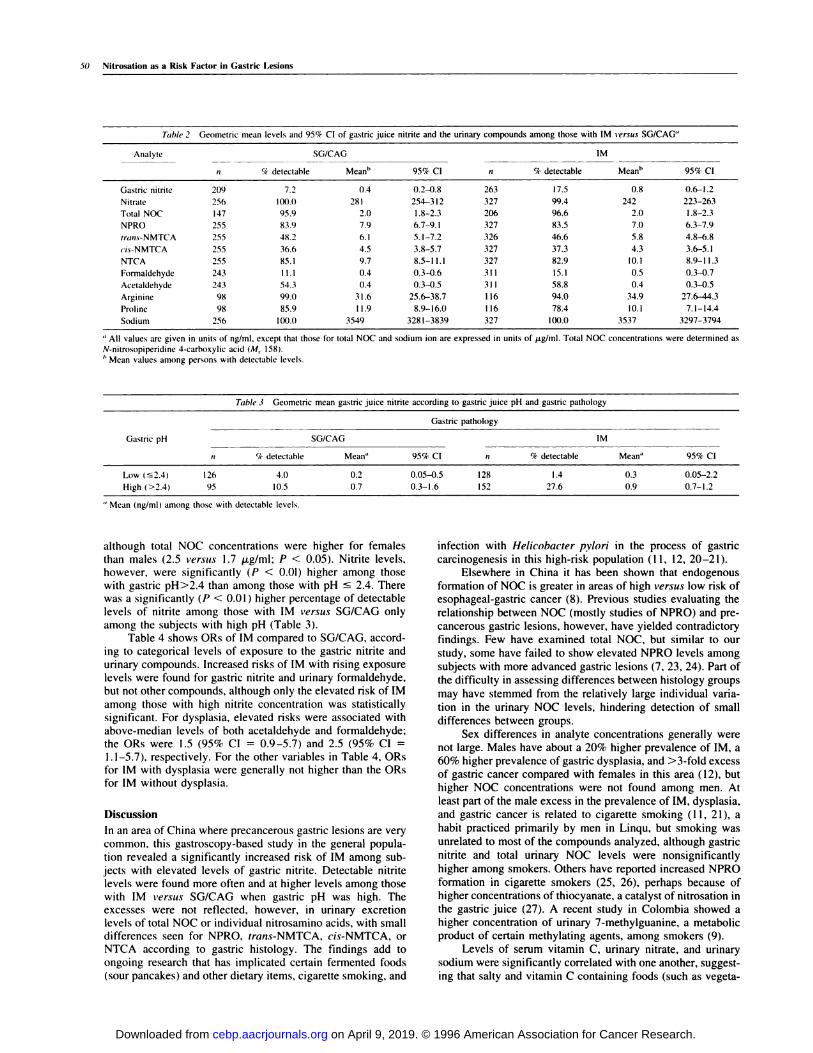
Table 2 shows geometric mean values of the compoundstested according to gastric pathology. Because there was littledifference in the means for IM with or without accompanyingdysplasia, we compared values for those with IM vensus SG/
CAG and did not separately consider dysplasia. Gastric juicenitrite concentrations were above the detection level (2 ,.LM) for7% of those with SG/CAG versus 17% for those with IM (P <
0.01). Furthermore, the average detectable level was twice ashigh (P = 0.06) among those with IM as with SG/CAG.
Urinary formaldehyde tended to be detected somewhat moreoften and at higher levels, whereas urinary nitrate occurred
generally at lower levels, among those with IM. However, thesetrends were not statistically significant nor were the differencesin nitrosamino acid or sodium levels in urine between the twohistological categories.
Differences in mean levels of most analytes with respect tosex, age, and cigarette smoking status were generally small,
on April 9, 2019. © 1996 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
50 Nitrosation as a Risk Factor in Gastric Lesions
Table 2 Geometric mean levels and 9 5% CI of gastric juic e nitrite and the uri nary compoun ds among those wi th IM sersus SG/CAG”
Analyie SG/CAG IM
it Ck detectable Mean5 95% CI n % detectable Mean5 95% CI
Gastric nitrite 209 7.2 0.4 0.2-0.8 263 17.5 0.8 0.6-1.2
Nitrate 256 lOO.() 281 254-312 327 99.4 242 223-263
Total NOC 147 95.9 2.0 1.8-2.3 206 96.6 2.0 1.8-2.3
NPRO 255 83.9 7.9 6.7-9.1 327 83.5 7.0 6.3-7.9
tna,i.v-NMTCA 255 48.2 6.1 5.1-7.2 326 46.6 5.8 4.8-6.8
cis-NMTCA 255 36.6 4.5 3.8-5.7 327 37.3 4.3 3.6-5.1
NTCA 255 85.1 9.7 8.5-11.1 327 82.9 10.1 8.9-11.3
Formaldehyde 243 1 1.1 0.4 0.3-0.6 31 1 15.1 0.5 0.3-0.7
Acetaldehyde 243 54.3 0.4 0.3-0.5 31 1 58.8 0.4 0.3-0.5
Arginine 98 99.0 31.6 25.6-38.7 116 94.0 34.9 27.6-44.3
Proline 98 85.9 11.9 8.9-16.0 116 78.4 10.1 7.1-14.4
Sodium 256 100.0 3549 3281-3839 327 100.0 3537 3297-3794
“ All values are given in units of ng/ml. except that those for total NOC and sodium ion are expressed in units of 44/mI. Total NOC concentrations were determined as
N-nitrosopiperidine 4-carhoxylic acid (M, I 58).I, Mean values among persons with detectable levels.
Table 3 Geometri c mean gastric juice n itrite according to gastric juice p H and gastric pathology
Gastric pH
Gastric pathology
SG/CAG IM
Ii (4. detectable Mean” 95% CI n % detectable Mean 95% CI
Low �S2.4)
High (>2.4)
126
95
4.0
10.5
0.2
0.7
0.05-0.5 128
0.3-1.6 152
1.4
27.6
0.3
0.9
0.05-2.2
0.7-1.2
“ Mean (ng/ml) among those with detectable levels.
although total NOC concentrations were higher for femalesthan males (2.5 versus 1.7 �g/ml: P < 0.05). Nitrite levels,however, were significantly (P < 0.01) higher among thosewith gastric pH>2.4 than among those with pH � 2.4. Therewas a significantly (P < 0.01) higher percentage of detectable
levels of nitrite among those with IM versus SG/CAG onlyamong the subjects with high pH (Table 3).
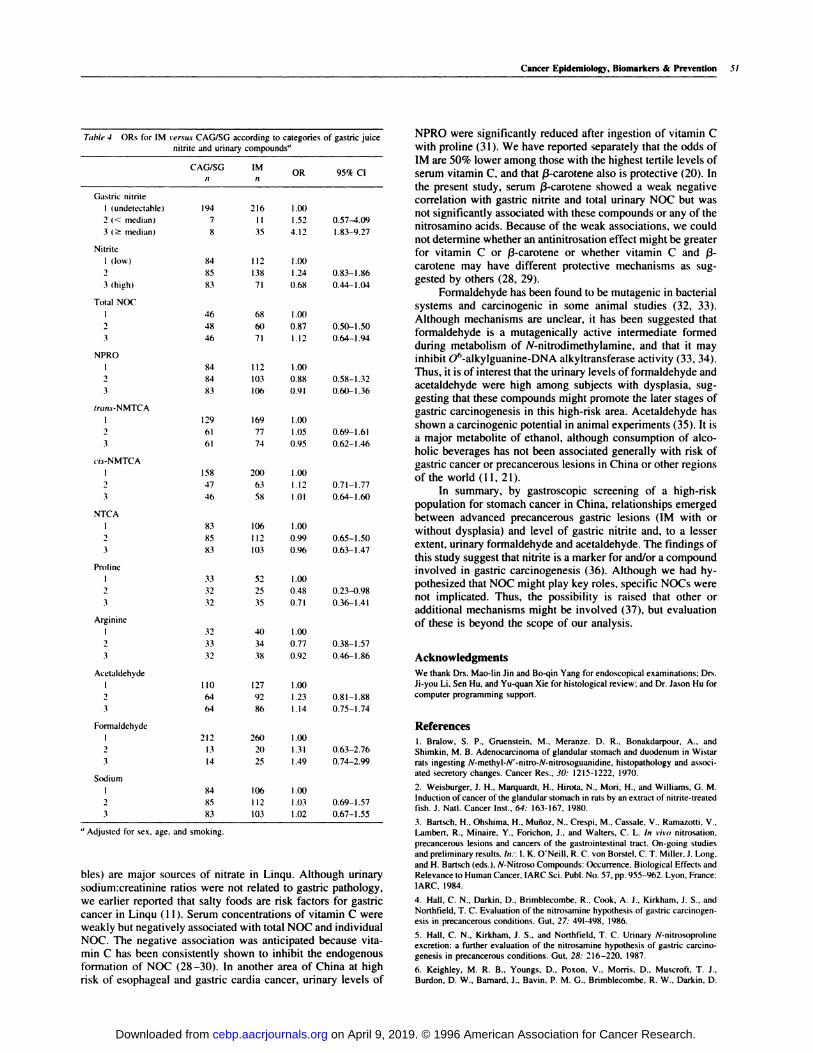
Table 4 shows ORs of IM compared to SG/CAG, accord-ing to categorical levels of exposure to the gastric nitrite andurinary compounds. Increased risks of IM with rising exposurelevels were found for gastric nitrite and urinary formaldehyde,but not other compounds, although only the elevated risk of IM
among those with high nitrite concentration was statisticallysignificant. For dysplasia, elevated risks were associated with
above-median levels of both acetaidehyde and formaldehyde;the ORs were 1.5 (95% CI = 0.9-5.7) and 2.5 (95% CI =
1.1-5.7), respectively. For the other variables in Table 4, ORsfor IM with dysplasia were generally not higher than the ORsfor IM without dysplasia.
Discussion
In an area of China where precancerous gastric lesions are very
common. this gastroscopy-based study in the general popula-tion revealed a significantly increased risk of IM among sub-jects with elevated levels of gastric nitrite. Detectable nitritelevels were found more often and at higher levels among thosewith IM t’ensus SG/CAG when gastric pH was high. Theexcesses were not reflected, however, in urinary excretionlevels of total NOC or individual nitrosamino acids, with smalldifferences seen for NPRO, tnans-NMTCA, cis-NMTCA, orNTCA according to gastric histology. The findings add toongoing research that has implicated certain fermented foods
(sour pancakes) and other dietary items, cigarette smoking, and
infection with Helicobacten pylon in the process of gastric
carcinogenesis in this high-risk population (11, 12, 20-21).Elsewhere in China it has been shown that endogenous
formation of NOC is greater in areas of high versus low risk ofesophageal-gastric cancer (8). Previous studies evaluating therelationship between NOC (mostly studies of NPRO) and pre-
cancerous gastric lesions, however, have yielded contradictoryfindings. Few have examined total NOC, but similar to our
study, some have failed to show elevated NPRO levels amongsubjects with more advanced gastric lesions (7, 23, 24). Part of
the difficulty in assessing differences between histology groups
may have stemmed from the relatively large individual varia-
tion in the urinary NOC levels, hindering detection of small
differences between groups.Sex differences in analyte concentrations generally were
not large. Males have about a 20% higher prevalence of IM, a60% higher prevalence of gastric dysplasia, and >3-fold excessof gastric cancer compared with females in this area (12), but
higher NOC concentrations were not found among men. Atleast part of the male excess in the prevalence of IM, dysplasia,
and gastric cancer is related to cigarette smoking (1 1, 21), a
habit practiced primarily by men in Linqu, but smoking was
unrelated to most of the compounds analyzed, although gastric
nitrite and total urinary NOC levels were nonsignificantly
higher among smokers. Others have reported increased NPRO
formation in cigarette smokers (25, 26), perhaps because ofhigher concentrations of thiocyanate, a catalyst of nitrosation inthe gastric juice (27). A recent study in Colombia showed a
higher concentration of urinary 7-methylguanine, a metabolic
product of certain methylating agents, among smokers (9).
Levels of serum vitamin C, urinary nitrate, and urinarysodium were significantly correlated with one another, suggest-ing that salty and vitamin C containing foods (such as vegeta-
on April 9, 2019. © 1996 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Gastric nitrite
I (undetectable)
2 (< median)
3 (� median)
Nitrite
I (low)
3 (high)
Total NOC
NPRO
irwis-NMTCA
#{231}isNMTCA
NTCA
Proline
Arginine
Acetaldehyde
194 216 1.00
7 II 1.52
8 35 4.12
84 112 1.00
85 138 1.24
83 71 0.68
46 68 1.00
48 6() 0.87
46 71 1.12
84 112 1.00
84 103 0.88
83 lOb 0.91
129 169 1.00
61 77 1.05
61 74 0.95
158 200 1.00
47 63 1.12
46 58 1.01
83 106 1.00
85 112 0.99
83 103 0.96
33 52 1.00
32 25 0.48
32 35 0.71
32 40 1.00
33 34 0.77
32 38 0.92
0.57-4.09
I .83-9.27
0.83- I .86
0.44-I .04
0.50-ISO
0.64-I .94
0.58-I .32
0.60-I .36
0.69-I .61
0.62-I .46
0.7 1-1.77
0.64-I .60
0.6�-1.S0
0.63-I .47
0.23-0.98
0.36-1.41
0.38-1.S7
0.46-1.86
0.81-I .88
0.75-I .74
0.63-2.76
0.74-2.99
0.69-I .57
0.67-I .55
260 1.00
20 1.31
25 1.49
106 1.00
112 1.03
103 1.02
Cancer Epidemiology, Biomarkers & Prevention 51
Table 4 ORs for IM rersu.s CAG/SG according to ca tegories of gastric juicenitrite and urinary compounds”
CAG/SG IMOR 95% Cl
Formaldehyde
I 212
2 13
3 14
Sodium
I 84
2 85
3 83
“ Adjusted for sex, age. and smoking.
110 127 1.00
64 92 1.23
64 86 1.14
bies) are major sources of nitrate in Linqu. Although urinarysodium:creatinine ratios were not related to gastric pathology,
we earlier reported that salty foods are risk factors for gastriccancer in Linqu ( 1 1 ). Serum concentrations of vitamin C wereweakly but negatively associated with total NOC and individualNOC. The negative association was anticipated because vita-mm C has been consistently shown to inhibit the endogenousformation of NOC (28-30). In another area of China at highrisk of esophageal and gastric cardia cancer, urinary levels of
NPRO were significantly reduced after ingestion of vitamin Cwith proline (31). We have reported separately that the odds ofIM are 50% lower among those with the highest tertile levels of
serum vitamin C, and that p3-carotene also is protective (20). In
the present study, serum (3-carotene showed a weak negativecorrelation with gastric nitrite and total urinary NOC but wasnot significantly associated with these compounds or any of thenitrosamino acids. Because of the weak associations, we couldnot determine whether an antinitrosation effect might be greaterfor vitamin C or a-carotene or whether vitamin C and �3-carotene may have different protective mechanisms as sug-
gested by others (28, 29).Formaldehyde has been found to be mutagenic in bacterial
systems and carcinogenic in some animal studies (32, 33).
Although mechanisms are unclear, it has been suggested thatformaldehyde is a mutagenically active intermediate formedduring metabolism of N-nitrodimethylamine, and that it mayinhibit 06-alkylguanine-DNA alkyitransferase activity (33, 34).
Thus, it is of interest that the urinary levels of formaldehyde andacetaidehyde were high among subjects with dysplasia, sug-gesting that these compounds might promote the later stages of
gastric carcinogenesis in this high-risk area. Acetaldehyde hasshown a carcinogenic potential in animal experiments (35). It isa major metabolite of ethanol, although consumption of alco-
holic beverages has not been associated generally with risk ofgastric cancer or precancerous lesions in China or other regionsof the world (1 1, 21).
In summary, by gastroscopic screening of a high-risk
population for stomach cancer in China, relationships emergedbetween advanced precancerous gastric lesions (lM with orwithout dysplasia) and level of gastric nitrite and, to a lesserextent, urinary formaldehyde and acetaldehyde. The findings of
this study suggest that nitrite is a marker for and/or a compoundinvolved in gastric carcinogenesis (36). Although we had hy-pothesized that NOC might play key roles, specific NOCs werenot implicated. Thus, the possibility is raised that other oradditional mechanisms might be involved (37), but evaluationof these is beyond the scope of our analysis.
Acknowledgments
We thank Drs. Mao-Iin un and Bo-qin Yang for endoscopical examinations: Drs.Ji-you Li. Sen Hu. and Yu-quan Xie for histological review: and Dr. Jason Hu for
computer programming support.
References
I . Bralow, S. P., Gruenstein, M., Meranze. D. R., Bonakdarpour, A., and
Shimkin, M. B. Adenocarcinoma of glandular stomach and duodenum in Wistar
rats ingesting N-methyl-N’-nitro-N-nitrosoguanidine, histopathology and associ-
ated secretory changes. Cancer Res., 30: 1215-1222, 1970.
2. Weisburger, J. H., Marquardt. H., Hirota, N.. Mon. H.. and Williams, G. M.
Induction of cancer of the glandular stomach in rats by an extract of nitrite-treatedfish. J. Natl. Cancer Inst., 64: 163-167, 1980.
3. Bartsch, H., Ohshima, H., Mufioz. N., Crespi. M.. Cassale. V., Ramazotti. V..
Lambert. R., Minaire, Y.. Forichon, J.. and �Valters, C. L. In viva nitrosation,
precancerous lesions and cancers of the gastrointestinal tract. On-going studies
and preliminary results. In:: I. K. O’Neill. R. C. von Borstel, C. T. Miller. J. Long.
and H. Bartsch (eds.), N-Nitroso Compounds: occurrence, Biological Effects andRelevance to Human Cancer, IARC Sci. PubI. No. 57, pp. 955-962. Lyon. France:
IARC. 1984.
4. Hall, C. N., Darkin, D., Brimblecombe, R., Cook, A. J., Kirkham, J. S., and
Northfield, T. C. Evaluation of the nitrosamine hypothesis of gastric carcinogen-
esis in precancerous conditions. Gut. 27: 491-498, 1986.
5. Hall, C. N., Kirkham, J. S., and Northfield, T. C. Urinary N.nitrosoproline
excretion: a further evaluation of the nitrosamine hypothesis of gastric carcino-genesis in precancerous conditions. Gut. 28: 216-220, 1987.
6. Keighley, M. R. B., Youngs. D.. Poxon. V., Morris, D.. Muscroft, T. J..
Burdon, D. W., Barnard. J.. Bavin, P. M. G.. Brimblecombe, R. W., Darkin. D.
on April 9, 2019. © 1996 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

52 Nitrosation as a Risk Factor in Gastric Lesions
W., Moore, P. J.. and Viney. N. Intragastric N-nitrosation is unlikely to be
responsible for gastric carcinoma developing after operations for duodenal ulcer.
Gut, 25: 238-245. 1984.
7. Kyrtopoulos. S. A.. Daskalakis, G.. Legakis. N. I., Konidaris, N., Psarrou, E..
Bonatsos, G., Golematis, B., Lakiotis, G., Bliouras, N.. and Outram, J. R. Studies
in gastric carcinogenesis. II. Absence of elevated concentrations of N-nitrosocompounds in the gastric juice of Greek hypochlorhydric individuals. Carcino-
genesis (Land.), 6: 1 135-1 140. 1985.
8. Lu, S. H., Yang. W. X.. Guo, L. P.. Li. F. M., Wang. G. J.. Zhang. J. S.. andLi. P. Z. Determination of N-nitrosamines in gastric juice and urine and a
comparison of endogenous formation of N-nitrosoproline and its inhibition in
subjects from high- and low-risk areas for oesophageal cancer. In: H. Bartsch, I.K. O’Neill, and R. Schulte-Hermann (eds.), Relevance of N-Nitroso Compoundsto Human Cancer: Exposures and Mechanisms. IARC Sci. Publ. No. 84, pp.
538-543. Lyon. France: IARC, 1987.
9. Stillwell. W. G., Glogowski. J.. Xu, H-X., Wishnok, J. S.. Zavala, D., Montes,
G., Correa, P., and Tannenbaum, S. R. Urinary excretion of nitrate, N-nitroso-
proline. 3-methyladenine. and 7-methylguanine in a Colombian population athigh risk for stomach cancer. Cancer Res., 51: 190-194, 1991.
10. Crespi. M.. Ohshima, H., Ramazotti, V., Mu#{241}oz,N., Grassi, A., Casale, V..
Leclerc. H.. Calmels, S., Cattoen, C., Kaldor, J., and Bartsch, H. Intragastricnitrosation and precancerous lesions of the gastrointestinal tract: testing of an
etiological hypothesis. In: H. Bartsch. I. K. O’Neill, and R. Schulte-Hermann(eds.), Relevance of N-Nitroso Compounds to Human Cancer: Exposures and
Mechanisms, pp. 51 1-517, IARC Sci. PubI. No. 84. Lyon, France: IARC, 1987.
I I. You, W-C., Blot, W. J.. Chang. Y-S., Ershow, A. G., Yang. Z-T.. An, Q..Henderson. B.. Xu, G-W., Fraumeni, J. F., Jr., and Wang. T-G. Diet and high riskof stomach cancer in Shandong. China. Cancer Res., 48: 3518-3523. 1988.
12. You, W-C., Blot, W. J., Li, J-Y., Chang. Y-S.. Jin, M-L.. Kneller. R., Zhang.
L., Han, Z-X., Zeng. X-R., Liu, W-D., Zhao, L., Correa, P., Fraumeni, J. F., Jr.,
and Xu. G-W. Precancerous gastric lesions in a population at high risk of stomach
cancer. Cancer Res., 53: 1317-1321, 1993.
13. Chinese Association ofGastric Cancer. Classification and Diagnostic Criteria
for the Histologic Gastric and Duodenal Biopsy Specimens. Liaoning. China:
Liaoning Publishing House, I 981.
14. Ohshima, H., and Bartsch, H. Quantitative estimation of endogenous nitro-
sation by humans by monitoring N-nitrosoproline excreted in the urine. Cancer
Res.. 4/: 3658-3662, 1981.
15. Green, L. C.. Wagner. D. A., Glogowski. J.. Skipper. P. L.. Wishnok, J. S..
and Tannenbaum, S. R. Analysis of nitrate. nitrite. and (#{176}N)nitrate in biological
fluids. Anal. Biochem., /26: 131-138, 1982.
16. Janini, G. M., Fox. S. D., Citro. M. L., Musehik. G. M., and Issaq. H. J.Determination of total N-nitroso compounds in biological fluids by photolytic
denitrosation and thermal energy analysis. Anal. Instrum.. 2/: 1-9, 1993.
I 7. Farrelly. J. G. A new assay for the microsomal metabolism of nitrosamines.
Cancer Res.. 40: 3241-3244, 1980.
I 8. Einarsson. S., Josefsson, B., and Lagerkvist. S. Determination of amino acids
with 9-fluorenylmethyl chloroformate and reversed-phase high-performance liq-
uid chromatography. J. Chromatogr.. 282: 609-618. 1983.
19. Narayanan. S.. and Appleton. H. D. Creatinine: a review. Clin. Chem., 26:
1119-1126. 1980.
20. Zhang. L., Blot, W. J., You, W-C., Chang. Y-S.. Liu, X-Q., Kneller. R. W.,
Zhao. L., Liu, W-D., Li. J-Y., un, M-L.. Xu, G-W., Fraumeni, J. F., Jr., and Yang.C. S. Serum micronutrients in relation to pre-cancerous gastric lesions. Int. J.Cancer, 56: 650-654, 1994.
21. Kneller, R. W., You, W-C., Chang. Y-S.. Liu. W-D., Zhang, L.. Zhao, L., Xu,G-W., Fraumeni, J. F., Jr., and Blot, W. J. Cigarette smoking and other risk factors
for progression of precancerous stomach lesions. J. NatI. Cancer Inst., 84:
1261-1266, 1992.
22. Breslow, N. E., and Day, N. E. Statistical Methods in Cancer Research: TheAnalysis of Case-Control Studies, Vol. 1. IARC Sci. Publ. No. 32. Lyon, France:
IARC. 1980.
23. Cuello, C., Correa, P., Zarama, G., Lopez, J.. Murray. J.. and Gordillo, 0.Histopathology of gastric dysplasias: correlations with gastric juice chemistry.
Am. J. Surg. Pathol., 3: 491-500, 1979.
24. Pignatelli. B.. Malaveille, C.. Rogatko. A.. Hautefeuille. A., Thuillier, P..
Mu#{241}oz,N., Moulinier, B., Berger, F., Dc Montclos, H., Lambert, R., Correa, P.,Ruiz, B., Sobala, 0. M., Schorab, C. J., Axon A. T. R., and Bartsch, H. Mutagens.
N-nitroso compounds and their precursors in gastric juice from patients with and
without precancerous lesions of the stomach. Eur. J. Cancer. 29: 2031-2039.
1993.
25. Hoffmann, D., and Hecht, S. S. Nicotine-derived N-nitrosamines and tobac-co-related cancer: current status and future directions. Cancer Res., 45: 935-944,
1985.
26. Hoffmann, D., and Brunnemann, K. D. Endogenous formation of N-nitroso-
proline in cigarette smokers. Cancer Res., 43: 5570-5574, 1983.
27. Ruddell, W. S. J., Bone, E. S., Hill, M. J., Blendis, L. M., and Walters, C. L.Gastric-juice nitrite: a risk factor for cancer in the hypochlorhydric stomach?
Lancet, 2: 1037-1039, 1976.
28. Steinmetz, K. A., and Potter, J. D. Vegetables. fruit. and cancer. II. Mech-
anisms. Cancer Causes & Control, 2: 427-442, 1991.
29. Fiala, E. S., Reddy. B. S., and Weisburger, J. H. Naturally occurring anti-
carcinogenic substances in foodstuffs. Ann. Rev. Nutr., 5: 295-321. 1985.
30. Xu, 0. P., Song, P. J., and Reed. P. 1. Effects of fruit juices, processed
vegetable juice. orange peel and green tea on endogenous formation of N-
nitrosoproline in subjects from a high-risk area for gastric cancer in Moping
County. China. Eur. J. Cancer Prey., 2: 327-335, 1993.
31. Lu, S-H., Ohshima, H., Fu, H-M., Tian, Y., Li, F-M., Blettner, M.,Wahrendorf, J., and Bartsch, H. Urinary excretion of N-nitrosamino acids and
nitrate by inhabitants of high- and low-risk areas for esophageal cancer in
northern China: endogenous formation of nitrosoproline and its inhibition by
vitamin C. Cancer Res., 46: 1485-1491, 1986.
32. Tumer, L. The Mutagenic and Carcinogenic Potential of Formaldehyde.Technical Report No. 2. pp. 2-3 1 . Brussels. Belgium: ECETOC. I 981.
33. Pool, B. L., Frei, E., Plesch, W. J., Romruen, K., and Wiessler, M. Formal-
dehyde as a possible mutagenic metabolite of N-nitrodimethylamine and of otheragents which are suggested to yield non-alkylating species in vitro. Carcinogen-
esis (Lond.), 5: 809-814, 1984.
34. Harris, C. C. Biochemical and molecular effects of N-nitroso compounds in
human cultured cells: an overview. In: H. Bartsch, I. K. O’Neill, and R. Schulte-Hermann (eds.), Relevance of N-Nitroso Compounds to Human Cancer: Expo-
sures and Mechanisms, IARC Scientific Publications No. 84, pp. 20-25. Lyon.
France: IARC. 1987.
35. Feron, V. J., Kruysse. A.. and Woutersen. R. A. Respiratory tract tumours
in hamsters exposed to acetaldehyde vapour alone or simultaneously to
benzo(a)pyrene or dimethylnitrosamine. Eur. J. Cancer CIin. Oncol., 18:
13-31, 1982.
36. Correa. P. Human gastric carcinogenesis: a multistep and multifactorialprocess-First American Cancer Society Award lecture on cancer epidemiology
and prevention. Cancer Res., 52: 6735-6740, 1992.
37. Temir, S.. deRojas-Walker, T., Ji. H.. Wishnok, J. S.. and Tannenbaum, S. R.
DNA damage by nitric oxide (NO). Proc. Am. Assoc. Cancer Res.. 35: 155. 1994.
on April 9, 2019. © 1996 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
1996;5:47-52. Cancer Epidemiol Biomarkers Prev W C You, L Zhang, C S Yang, et al. physiological fluids in relation to precancerous gastric lesions.Nitrite, N-nitroso compounds, and other analytes in
Updated version
http://cebp.aacrjournals.org/content/5/1/47
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/5/1/47To request permission to re-use all or part of this article, use this link
on April 9, 2019. © 1996 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from





























