Embed Size (px)
Citation preview
The next meeting of the NHS Stockport Clinical Commissioning Group Governing Body will be held at Regent House, Stockport at 9am on 28 March 2018
Agenda item Report Action Indicative Timings Lead
1 Apologies Verbal
To receive and note 9.00 J Crombleholme
2 Declarations of Interest
Verbal To receive and note
3 Approval of the draft Minutes of the meeting held on 28 January 2018
Attached To receive and approve
J Crombleholme
4 Actions Arising
Attached To comment and note
9.05 J Crombleholme
5 Notification of Items for Any Other Business
Verbal
To note and consider
9.10 J Crombleholme
6 Patient Story Video 9.10 J Crombleholme
7 Corporate Performance Reports a) Finance Report b) Performance Report
Written Reports
To receive, assure and note.
9.25 M Chidgey G Mullins
8 Stockport Together Highlight Report
Written Reports
To consider 9.40 T Ryley
9 Locality Chairs’ Update
Verbal
To receive and note 9.55 Locality Chairs
10 Report of the Chair
Verbal Report
To receive and note 10.05 J Crombleholme
11 Report of the Chief Operating Officer to include the following:
• CQC System Visit • Q4 Assurance Visit
Written Report
To discuss and note (To Follow)
10.10 G Mullins
NHS Stockport Clinical Commissioning Group Governing Body Part 1
A G E N D A
Chair: Ms J Crombleholme Enquiries to: Laura Latham 07827 239332 [email protected]
001

12 Refresh and update of 2018/19 operational plan
Written Report
To approve outline plans (To Follow)
10.30 TR / MC
13 Reports from Committees
• Quality Report • Finance and
Performance Committee • Primary Care
Commissioning Committee
Written reports
To note the content of the reports and approve the recommendations of the Remuneration Committee
11.15
A Rolfe V Owen Smith J Crombleholme
15 Any Other Business
Verbal 11.25
J Crombleholme
Date, Time and Venue of Next meeting The next NHS Stockport Clinical Commissioning Group Governing Body meeting will be held on 30 May 2018 Potential agenda items should be notified to [email protected] by 1 May 2018.
002

1
NHS STOCKPORT CLINICAL COMMISSIONING GROUP MINUTES OF THE GOVERNING BODY
MEETING HELD AT REGENT HOUSE,
STOCKPORT ON WEDNESDAY 31 JANUARY 2018
PART 1
PRESENT
Mrs J Crombleholme Lay Member (Chair) Mrs G Mullins Chief Operating Officer Mr M Chidgey Chief Finance Officer Mrs A Rolfe Executive Nurse Dr J Higgins Locality Chair: Heatons and Tame Valley Dr D Kendall Secondary Care Consultant Ms C Morgan Lay Member for Primary Care Mr J Greenough Lay Member for Finance and Audit Dr V Owen Smith Clinical Director Public Health Dr R Gill Chief Clinical Officer Dr Lydia Hardern Locality Chair: Stepping Hill and Victoria Dr A Johnson Locality Chair: Marple and Werneth Dr S Woodworth Interim Medical Director
IN ATTENDANCE Mr T Ryley Director of Strategy and Performance Dr D Jones Director of Service Reform Mrs L Latham Associate Director Corporate Governance Mrs S Carroll Healthwatch Stockport Cllr T McGee Stockport Metropolitan Borough Council 68/17 APOLOGIES Apologies were received from Dr P Carne. 69/17 DECLARATIONS OF INTEREST Dr S Woodworth declared a pecuniary interest with regard to Item 16 Report of the Remuneration Committee on the basis that he was the interim post holder to which the remuneration would be negotiated. The Chair confirmed that he should leave the meeting and not take part in the discussion. Dr J Higgins, Dr R Gill, D L Hardern and D A Johnson declared an interest with regard to Item 9 Approval of Stockport Together plans. The nature of the interest being that they were partners in GP Practices in Stockport and the plans included investment in the GP Federation and also into General Practice. They also declared an interest with regard to Item 10 Mental Health Investment Plan. The nature of the interest being that they were partners in GP Practices in Stockport and the plans included investment into General Practice. Dr V Owen Smith declared that she was employed by Stockport Metropolitan Borough Council. Dr J Higgins declared an interest with regard to Item 9 Approval of Stockport Together Plans. The nature of the interest being that his practice was one of the designed sites for delivering Enhanced Case
003

2
Management. 70/17 APPROVAL OF THE DRAFT MINUTES OF THE GOVERNING BODY MEETING HELD ON 29 NOVEMBER 2018 The minutes of the meeting held on 29 November 2018 were approved as a correct record. 71/17 ACTIONS ARISING 29 11 2017 – Patient Story – Action completed and to be removed from the log. 29 11 2017 – Chief Clinical Officers’ Report – Action completed and to be removed from the log. 29 11 2017 – Finance Report – Action being progressed as part of the national planning guidance so to be removed from the log and reported to Governing Body as part of future plans. 72/17 ANY OTHER BUSINESS There were no items on this occasion. 73/17 PATIENT STORY The Governing Body heard from a patient who had accessed the GP Seven Day Service and also from a nurse working as part of the pilot site at Heaton Moor Medical Centre. The patient confirmed that accessing a Saturday morning appointment had proved very convenient for her and had meant that she’d not needed to take leave from work. Sister Taylor from the Practice confirmed that the service was working well and awareness amongst patients had recently increased. She noted that IT issues had been rectified and that clinicians working at weekends had commented that clinics had operated smoothly and they’d been able to deliver high quality care to patients. In particular she highlighted positive feedback from working age patients who found weekday appointments less easy to access. The Governing Body commented on the following elements of the story:
• Appointments were bookable in advance and on the day which was important. • Important at weekends to have access to range of clinical skills within clinics and not just GPs. • The importance to understand the impact on clinicians as part of Seven Day working in terms of
work life balance. • Importance of ensuring further roll out of the system was accessible for patients in terms of travel to
GP Hub sites. • The need to ensure real time data capture about the Seven Day Service which would be progressed
through the GP Federation.
Resolved: That Governing Body:
1. Note the Patient Story and express thanks to the patient and Sister Taylor for sharing their experiences.
74/17 CORPORATE PERFORMANCE REPORTS (a) Finance
M Chidgey provided an overview of the CCG’s financial position as at December 2017 and noting the forecast outturn position for 2017/18. He confirmed the CCG’s CIP position, including some significant elements achieved which were non-recurrent. He highlighted the CCG’s net risk of £0.64m which was outside the forecast and highlighted the impact of national price increases due to drugs in short supply. He drew Governing Body’s attention to the recommendation relating to the CCG’s relocation to Stopford House as was cross referenced to the Chief Operating Officer’s report.
004

3
In response to discussion the following key elements were highlighted by Members:
• The technical accounting position for brought forward surpluses and the NHS England position. • The significant work undertaken by the Medicines Optimisation Team in terms of CIP achievement
and of GPs in prescribing medication which was effective firstly for patients in terms of treatment but also cost effective.
• Potential financial risk for NHS Stockport Foundation Trust of cancelled electives in 2017/18 as patient numbers would be likely to increase in 2018/19.
• The national impact of drugs in short supply which could not be planned for.
Resolved: That Governing Body:
• Notes the year-to-date position is in line with plan. • Notes that an outturn breakeven position is forecast to be delivered. • Notes that net risks totalling £0.64m are not reflected within the forecast. • Notes that the position includes provision in full of the 0.5% non-recurrent uncommitted reserve as
required by NHS England business rules. • Notes that the Mental Health financial performance target is forecast to be achieved. • Note that a recurrent deficit of £3.10m is currently forecast to be carried forward into 18/19 and the
risks associated with this. • Approves the agreement of a 10 year lease for relocation of NHS Stockport CCG to 4th Floor
Stopford House at an estimated total cost of £1.60m and note that this value was still subject to ongoing negotiations.
(b) Performance M Chidgey provided an overview of current performance noting that a future schedule of reporting to Governing Body had been proposed within the report. In particular he highlighted the current position relating to Urgent Care Performance including the actions being taken by Commissioners in response which included partnership work in terms of pathways and resilient and safe services. New services being put into place to support improvements in Urgent Care performance were noted. The Governing Body also considered continued improvements in mental health performance and high performance in terms of the delivery of cancer standards. As part of discussion and questioning, the following elements were highlighted by the Governing Body:
• Modelling and understanding of any potential impact of the newly formed Manchester University Hospital Trust on performance in Stockport including patient choice.
• The reporting and investigation processes for validated 12 hour breaches at NHS Stockport Foundation Trust and the role of the CCG’s Quality Committee in considering the outcome.
• G Mullins noted that the CCG had received a letter from Healthwatch on this matter and would respond in due course. A Rolfe confirmed that herself and the Director of Nursing from the Trust would be happy to meet with Healthwatch representatives to discuss issues highlighted in further detail.
• Concern about the impact on outcomes for those patients waiting longer than 12 hours was noted. • The need to understand the ambulance performance position as aligned to existing measures to
consider all contributory factors. R Gill confirmed that the CCG was actively working with Greater Manchester Health and Social Care Partnership and with the Trust and local partners to provide commissioner leadership and support as part of a Locality response to continued urgent care performance issues. He noted that improvements in patient safety had been demonstrated but that urgent care remained the priority for all partners in Stockport. Resolved: That Governing Body:
(i) Notes the format and timing of performance reporting in transitioning to a quarterly integrated performance report.
005

4
(ii) Notes the performance issues highlighted to the Governing Body, in particular the continued levels of urgent care performance.
(iii) Confirms that future reports will include data on ambulance performance. 75/17 STOCKPORT TOGETHER HIGHLIGHT REPORT T Ryley provided an update on the recent activity of the Stockport Together Transformation Programme and drew the Governing Body’s attention to five principal risks of workforce, system leadership changes, digital funding, benefits realisation, and competing expectations. He noted that a significant amount of work was underway to develop and test new ways of working which would be embedded in contracts subject to Commissioner approval of the next steps. Governing Body noted that implementation and service mobilisation timescales were behind plan but that plans had been re-assessed following the approval out the Outline Business Cases in July 2017. The positive feedback from the LCO Peer Visit to Stockport was noted. In response to questioning, M Chidgey confirmed that the approach to planning and contracting would be based on an outcomes framework linked to a population segmentation approach and work will be undertaken with Providers to test an initial series of segments. Resolved: That Governing Body note the update report. 76/17 APPROVAL OF STOCKPORT TOGETHER PLANS J Crombleholme provided the context for the Governing Body’s discussion noting that it was a significant milestone in the CCG and wider system’s transformation plans. She explained that the approach to decision making would be based on considering the following key elements:
• The consultation process followed • Information and evidence arising • Risks • Decision
Public questions would be taken ahead of the decision in order for them to be actively considered by Governing Body Members. It was noted that recommendations arising from the discussion would be captured as part of the Board’s formal decision. T Ryley provided an overview of the previous endorsement of Outline Business Cases in July 2017 and the reasons for transforming health and care in Stockport including the duty to address health inequalities, provide high quality integrated health and care services for the population of Stockport and reduce the financial gap. He noted that the public consultation had been accompanied by a series of Equality Impact Assessments (EIAs) which would continue to remain under review throughout proposed implementation. The output of the public consultation had been analysed independently and published as provided ahead of a Commissioner response. He noted that bed reductions had been highlighted as an area of concern but balanced against a wider context of improving the delivery of care for the population of Stockport. The actions and recommendations arising from the public consultation would be actively pursued as part of implementation and beyond. In discussing in detail the process followed as part of the public consultation the following elements were highlighted by the Governing Body:
• The importance of ensuring that the output of locality based consultation conversations was captured continually alongside review of EIAs and the provision of services within neighbourhoods to meet population needs whilst ensuring equality of service access for the population.
• Lack of evidence of patient choice within the consultation output and the reason for this in terms of statistical requirements.
• Language within the EIAs which refers to men working and should be amended to ensure equality and the importance of highlighting as part of continued review the digital divide.
006

5
• Importance of ensuring staff training on embedding equality and diversity understanding across the system was provided and in particular ensuring service design responded appropriately to those groups with protected characteristics.
• T Ryley confirmed that as part of the consultation and preceding Listening Exercise a range of methods had been used to capture views and feedback from those residents living in areas less traditionally willing to engage.
• The importance of aligning all the actions from EIAs into a single plan was highlighted. • Ongoing engagement with service users and their families would continue through to
implementation, in particular focusing on actions arising from the EIAs. A representative from the Consultation Institute who had acted as independent analysts for the consultation output addressed the Governing Body to confirm the process for analysis which had been followed and confirmed the approach taken in working with the CCG including the responsiveness of the organisation in providing the evidence collated and in receiving openly the output arising. He confirmed that the Programme Director had commented only on issues of factual accuracy ahead of publishing the report and not on the independently analysed content. The Governing Body then moved on to consider the additional evidence arising from the consultation and highlighted the following issues:
• Requirement to consider children and families as part of the partnership strategy in Stockport. • Future consideration of the tests which would be applied by Providers ahead of any bed closures • Importance of ensuring that the approach to carers is embedded as part of communications
approach to and delivery and implementation of new services. • Continued development of public understanding of the role of neighbourhoods in delivering health
and care services in Stockport. • Public health spend as part of the Stockport Together approach. • T Ryley confirmed that the analysts had separated out feedback from informed stakeholders and the
wider population. • Role of ensuring appropriate community and intermediate tier beds were available to support the
delivery
Governing Body discussed in detail the risks as at outlined to them and highlighted the following issues:
• The importance of ensuring the work reduces the risk of a growing gap in health inequalities in Stockport and future management of public health monies at a time of reducing spend remains in view.
• Future and continued focus on prevention. • The risks posed to patients and the system in not sharing data and the importance of ensuring the
7th Caldicott Principle outlining the duty to share is explicitly communicated across the system and commonly understood.
• The requirement for a comprehensive approach to system workforce planning given the scale of risk posed in this area and as aligned to the need for a Provider Organisational Development Plan to address known risks arising from culture and leadership matters.
• Future risks around access to adult social care services potentially arising from increases in rates for chargeable services need to be understood.
• Focus should remain at system and individual organisational level on mobilisation as aligned to benefits delivery.
• M Chidgey explained in response to questioning that individual organisational CIPs would need to be delivered.
• Effective management of implementation was highlighted as a risk, in particular relating to pace and embedding of change.
A question was raised by a Member of the public regarding the decision to conclude the MCP procurement. G Mullins confirmed that focus for the system was in delivering the new models of care and the future aspiration to move to a single integrated provider ACO remained. Governing Body concluded the discussion by considering in detail the recommendations contained within the report and in particular the elements regarding statutory partners and wider determinants of health. It was noted that further work had been undertaken to embed mental health as part of the approach to neighbourhood design and delivery in response to previous Governing Body recommendations.
007

6
J Crombleholme provided a summary of the Governing Body’s consideration and the full list of caveats and recommendations as outlined below.
Resolved: That Governing Body:
1. Endorsed following detailed consideration and scrutiny the feedback from the public consultation, the updated Equality Impact Assessments (EIAs), the views of the Adult Social Care and Health Scrutiny Committee and the proposed response.
2. Agreed that the following elements be captured as part of the revised documentation, plans and thematic recommendations to be included in the approach to implementation:
• Public Involvement to include reference to carers, patients and citizens and a systematic
approach to be progressed against agreed standards. • Equality Impact Assessment Action (EIA) Plans to be combined into a single plan following a
review of language to ensure consistency of terminology and understanding. • Reference in the EIAs to be made to the digital divide and those with learning disabilities and
LGBT groups. • Consideration to be given to measures to be applied to the Equality Impact Assessment Actions • Confirmation that the assurance will be received in future about the embedding of the approach
to equality as part of implementation beyond the training staff will require as part of their roles. • That reference to statutory partners including housing associations be made more explicit in
addition to the Third Sector. • That the future approach to health and care services for children be articulated as part of the
wider implementation context. • Commissioners to provide leadership and expertise to support the development of a robust and
comprehensive approach to system workforce strategy and plans. • Organisational Development Strategy to include references and understanding of organisational
culture and the link to leadership. • Designated capacity be put in place to lead the workforce and organisational development work. • Reference to be included to Caldicott Principle 7 as part of the integration and sharing of data. • The Health and Care Integration Board to consider how strategic and operational risks linked to
implementation are managed in a changing and complex environment. • Decision making by all partners regarding Financial and Operational Planning to consider
system impact and potential implications for delivery of system transformation and performance improvements.
• Governing Body to receive detail about the tests to be applied prior to closure of any beds at NHS Stockport Foundation Trust ahead of any decisions being made by Providers.
3. Approved the recommendation at 4.5.2 to approve the approach described in the previously
endorsed outline business cases and proceed to implementation subject to the recommendations set out in Section 5 of the report namely that:
• We review how, as commissioners and providers, we further engage and involve local people –
those who use health and social care services as well as those who do not. We accept that, in the past, consultation outreach has sometimes appeared start/stop. Going forward, we will act on comments made by consultees which suggest we should involve local people in a more consistent, regular, and sustained way.
• From January 2018, Commissioners will consider a method of engagement that involves collaborative working amongst stakeholders. It will build on comments received during this consultation about how we avoid complexity in our communications, promoting innovation and opportunity within our health and care system.
• Through more effective engagement techniques, we will specifically build-in checks and balances to ensure there is an equal and fair representation for people who often do not have their voices heard.
• We will review how we present financial information, and the need to provide greater clarity around how funding is directed (on what services), and how this compares to previous years. We would hope that greater familiarity of issues, through more regular and consistent
008

7
‘involvement’, creates better understanding of those issues amongst patients and our wider stakeholder groups.
• We continue to work closely with the new Citizens Representation Panel to ensure closer working with our operational leads and move closer to a culture of ‘shared leadership’ in decision making.
• We proactively build on the networks and contacts already achieved and established through this consultation. This will enable us to build greater involvement of local people in decision making about their health and social care services – particularly those less able to access services, for example visually impaired, deaf and disabled people.
• Work with GPs and the new ‘Neighbourhood model’ structures to establish local networks that create meaningful and early involvement of local people in decision making. We will establish channels of communication and engagement that will regularly update patients and the public on progress – some of these channels will include Patient Participation Groups, collaborative working between patients and clinicians and greater use of digital media to support information flow to both patients and the public.
4. Approve the adoption of the series of recommendations regarding implementation in light of the
consultation feedback as set out in Section 5.1.2 of the report and outlined above.
5. Approve the proposals to review progress as described in Section 6.1.2 of the report that the Health and Care Integrated Commissioning Board (HCICB) will consider in public a report on progress in addressing the recommendations as set out in Section 5 of the report and the Equality Impact Assessment Plans. This report would be presented in September 2018 and reviewed again in July 2019.
77/17 MENTAL HEALTH INVESTMENT PLAN M Chidgey provided an overview of the investment plan and expressed thanks to Dr N Hussain and G Evans who had led the work on behalf of the CCG. He drew attention to the detailed investment plan for the period 17/18 – 20/21 and noted that of the total £9.1m investment, £6.1m would be invested in national ‘must dos’ and the remaining £3m into local priorities as aligned to system plans. The 4 themes within the plan were highlighted and the risks of not proceeding immediately were approximately £600k of schemes were considered by the Governing Body including the importance of setting the investment plan within the wider context of the Stockport Together Business Cases. The significance of the investment plan in working towards Parity of Esteem was noted. Governing Body members highlighted the importance of mental health investments being made on the basis of the neighbourhood model. J Greenough sought clarity about the basis for the development of the investment plan including the involvement of GPs and wider patient and stakeholder groups. *Dr L Harden left the meeting. Resolved: That Governing Body: (i) Notes the content of the Mental Health Investment Plan (ii) Approves the investment plan as a high priority for inclusion within the 2018/19 CCG plan. (iii)Notes that the scope of this plan excludes both the CQC action plan and PCFT underlying financial position. 78/17 LOCALITY CHAIRS REPORT On behalf of Locality Chairs J Higgins presented the report which focused on work being actioned relating to member feedback on the crisis report, flu and long term condition management. V Owen Smith noted the high immunisation rates in Stockport which included being second nationally for Reception and Years 2 and 3 aged children. G Mullins noted that the member view of the changes to the crisis response service were being considered by commissioners.
009

8
Resolved: That the report be noted. 79/17 REPORT OF THE CHIEF OPERATING OFFICER G Mullins introduced the report and the following updates on key elements were provided:
• Working Well Project. • Re-location of CCG Offices to Stopford House. • Stockport Town Ambassador.
With regard to the CCG office relocation, she informed Governing Body that the approach was aligned to the agreed strategy regarding strategic integrated commissioning and the terms of a lease for the floor space was being negotiated with the Council. T Ryley confirmed that scoping work had been undertaken regarding meeting room access and the financial case for moving would make a modest saving for the CCG and would ensure public sector monies remained in the public sector. Resolved: That Governing Body: 1. The CCG Governing Body are asked to note the report and confirm their endorsement of Stockport’s engagement in the Working Well Early Help Programme. 2. Request that the Chief Operating report to the Governing Body any material changes to lease terms. 3. Delegate authority to the Chief Operating Officer to enter into a 10 year lease for the 4th Floor Stopford House subject to the final negotiated lease cost remaining value for money.
80/17 CHIEF CLINICAL OFFICERS REPORT R Gill introduced the report and D Jones provided a brief over view of the work being progressed relating to Healthier Together. In addition to the business case work being continued and refinement of the financial position, improved bowel cancer rates were noted and pathway work was noted to be progressing well with design characteristics now signed off. Resolved: That the report was noted. 81/17 SAFEGUARDING ANNUAL REPORT J Parker provided an overview of the report for the 2016/17 year. She highlighted in particular the work which had been undertaken to ensure the CCG met its statutory safeguarding requirements and ensures the compliance of its providers with CCG Safeguarding standards. She noted that the Quality Committee provided ongoing assurance regarding safeguarding activity and provided an overview of the issues highlighted regarding assurance from GP Practices as regards safeguarding standards. Areas of work which remained under progression were noted to be:
• Meeting the needs of Looked After Children, including those placed out of area. • Additional capacity had been secured for safeguarding adults. • Commitment to learning from safeguarding reviews • Progress in embedding the PREVENT agenda.
In response to questioning C Morgan expressed concern that the CCG had reported in 2016/17 that statutory duties had not been met and noted that she wished this to be formally recorded within the minutes. J Parker acknowledged the concern noting that work was being undertaken with small providers to ensure assurance regarding safeguarding was routinely provided to the CCG and a joint Quality Team between the CCG and Council had been established. She noted that the CCG would anticipate reporting full compliance in 2017/18 and the matter was being monitored by Quality Committee. Resolved: That the Governing Body:
010

9
• Notes the Annual report • Acknowledges that the CCG is not fully meeting its safeguarding responsibilities and accepts the
level of assurance provided and the residual risk. • Acknowledges the gaps / risks in the system and the actions in place to address them. • Notes that C Morgan and J Greenough would meet with J Parker to review the work which had been
undertaken in 2017/18 and would inform the Annual Report. 82/17 REPORTS FROM COMMITTEES
(a) Finance and Performance
V Owen Smith provided an overview of the recent work of the Committee including the focus on risks associated with delivery of CIP, performance against plan and financial cost pressures arising from NICE guidance and new medication. Resolved: That the report be noted.
(b) Primary Care Commissioning Committee
J Crombleholme provided an overview of the recent work of the Committee including the ongoing negotiation with the GP Federation regarding the contract for the delivery of 7 Day Services. Governing Body was informed of the Committee’s approval of catch up scheme for pneumococcal vaccinations to be put in place for Winter 2017 in line with Urgent Care Plan and schemes to reduce Winter Pressures and approval of an application for an estates and technology transformation fund application for Bramhall Park Medical Practice. She noted that the Committee also approved the lifting of contract notices at Bredbury Medical Centre. Resolved: That the report be noted.
(c) Remuneration Committee
J Greenough provided an overview of the recent work of the Committee which included the discussions regarding the remuneration for the Medical Director position. Resolved: That Governing Body:
• Approves the range within which the Chief Clinical Officer can negotiate an agreed salary with the appointee to the Medical Role was £130,000 - £140,000.
011
Actions arising from Governing Body Part 1 Meetings
NUMBER ACTION MINUTE DUE DATE OWNER AND UPDATE
1
Patient Story Note the Patient Story and express thanks to the patient and Sister Taylor for sharing their experiences.
73/17
February 2018
L Latham
2
Performance Report Confirms that future reports will include data on ambulance performance.
74/17
March 2018
M Chidgey
3
Safeguarding Annual Report Notes that C Morgan and J Greenough would meet with J Parker to review the work which had been undertaken in 2017/18 and would inform the Annual Report.
81/18
April 2018
C Morgan, J Greenough and J Parker
NHS Stockport Clinical Commissioning Group 31 January 2018
012

013

Finance Report for the period ending 28th February 2018 – Month 11
NHS Stockport Clinical Commissioning Group will allow
people to access health services that empower them to live healthier, longer and more independent lives.
Tel: 0161 426 9900 Fax: 0161 426 5999 Text Relay: 18001 + 0161 426 9900 Website: www.stockportccg.org
NHS Stockport Clinical Commissioning Group 7th Floor Regent House Heaton Lane Stockport SK4 1BS
014
2
Executive Summary
What decisions do you require of the Governing Body?
(i) Note the year-to-date position is in line with plan. (ii) Note that an outturn breakeven position is forecast to be delivered. (iii) Note a NIL net risk position is now being reported. (iv) Note that the position includes provision in full of the 0.5% non-recurrent
uncommitted reserve as required by NHS England business rules. (v) Note that the Mental Health financial performance target is forecast to be
achieved. (vi) Note that a recurrent deficit of c£3.10m is currently forecast to be carried
forward into 18/19 and the consequent impact on the CIP target for 2018/19.
Please detail the key points of this report The YTD and forecast outturn positions are in line with the planned in year surplus of £1.32m. As a result of activity levels being above planned levels, non-delivery of recurrent CIP and an increase in the number of CHC placements a £3.10m forecast recurrent deficit will be carried forward into 2018/19. What are the likely impacts and/or implications? Non-delivery of NHS England business rules and performance targets would result in increased scrutiny and would impact on the CCG’s assurance rating. How does this link to the Annual Business Plan? As per 2017/18 Financial Plan. What are the potential conflicts of interest? N/A Where has this report been previously discussed? This report is being presented for the first time. Clinical Executive Sponsor: Ranjit Gill Presented by: Mark Chidgey Meeting Date: 28 March 2018 Agenda item: 7 a Reason for being in Part 2 (if applicable) N/A
015
3
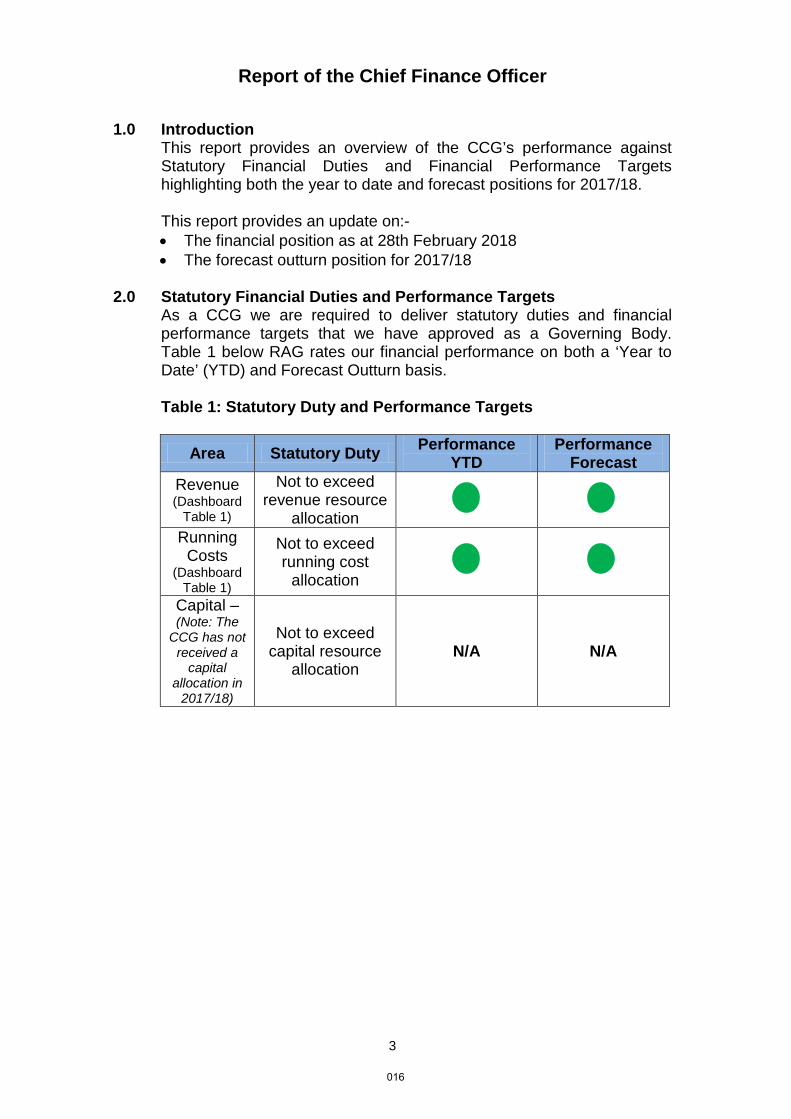
Report of the Chief Finance Officer
1.0 Introduction This report provides an overview of the CCG’s performance against
Statutory Financial Duties and Financial Performance Targets highlighting both the year to date and forecast positions for 2017/18.
This report provides an update on:-
• The financial position as at 28th February 2018 • The forecast outturn position for 2017/18
2.0 Statutory Financial Duties and Performance Targets As a CCG we are required to deliver statutory duties and financial
performance targets that we have approved as a Governing Body. Table 1 below RAG rates our financial performance on both a ‘Year to Date’ (YTD) and Forecast Outturn basis.
Table 1: Statutory Duty and Performance Targets
Area Statutory Duty Performance YTD
Performance Forecast
Revenue (Dashboard
Table 1)
Not to exceed revenue resource
allocation
Running Costs
(Dashboard Table 1)
Not to exceed running cost
allocation
Capital – (Note: The
CCG has not received a
capital allocation in
2017/18)
Not to exceed capital resource
allocation N/A N/A
016
4
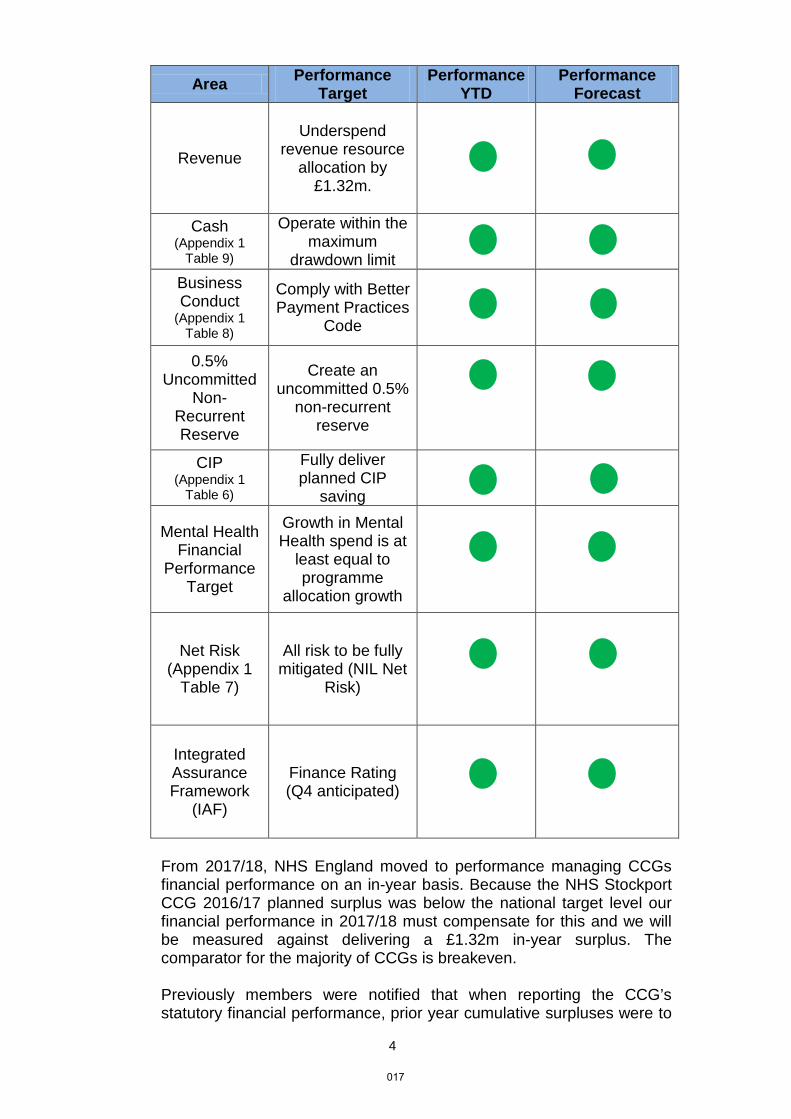
Area Performance Target
Performance YTD
Performance Forecast
Revenue
Underspend
revenue resource allocation by
£1.32m.
Cash (Appendix 1
Table 9)
Operate within the maximum
drawdown limit
Business Conduct
(Appendix 1 Table 8)
Comply with Better Payment Practices
Code
0.5% Uncommitted
Non-Recurrent Reserve
Create an uncommitted 0.5%
non-recurrent reserve
CIP (Appendix 1
Table 6)
Fully deliver planned CIP
saving
Mental Health Financial
Performance Target
Growth in Mental Health spend is at
least equal to programme
allocation growth
Net Risk (Appendix 1
Table 7)
All risk to be fully mitigated (NIL Net
Risk)
Integrated Assurance Framework
(IAF)
Finance Rating (Q4 anticipated)
From 2017/18, NHS England moved to performance managing CCGs financial performance on an in-year basis. Because the NHS Stockport CCG 2016/17 planned surplus was below the national target level our financial performance in 2017/18 must compensate for this and we will be measured against delivering a £1.32m in-year surplus. The comparator for the majority of CCGs is breakeven. Previously members were notified that when reporting the CCG’s statutory financial performance, prior year cumulative surpluses were to
017

5
be included. NHS England has now issued guidance which sets out that the reporting of CCG’s statutory financial performance will align with the reporting of the CCG’s in-year financial performance and exclude prior year cumulative surpluses.
As required by the 2017/18 NHS Planning Guidance, the CCG has created a 0.5% (1.0% in 2016/17) uncommitted reserve. It is anticipated that the CCG will be required to release this reserve in M12 and as a result the reported surplus will increase by £2.00m to £3.32m.
3.0 Financial Position as at 28th February 2018 – Month 11
The financial position as at month 11 is summarised in Table 2 below with further detail provided in Appendix 1 to this report.
Table 2: Summary of Financial Position at Month 11
Plan Actual (Favourable) / Adverse Variance
(Surplus) / Deficit
(Surplus) / Deficit
£000s £000s £000s Month 11 YTD (1,208) (1,208) 0 Year End Forecast (1,318) (1,318) 0
The CCG has reported a YTD surplus of £1.21m and a forecast outturn surplus of £1.32m in line with plan. The forecast outturn includes CIP delivery of £17.64m (101.1%), against a plan of £17.45m of which £2.23m has been achieved by deploying the full CCG contingency against CIP delivery.
4.0 Programme Expenditure
Acute Acute contract spend is £3.54m higher than year to date plan and forecast to overspend by £3.86m. This is due both to increases in activity which, whilst they are below national growth forecasts of c2.5%, are above the local planned growth forecasts of 0%. In addition to this volume increase there is also a significant element of the variance which relates to price changes driven by the impact of HRG4+. Community Health The forecast overspend of £0.30m in Community Health is due to an increase in community neuro-rehabilitation placements. Continuing Care The forecast overspend of £1.07m is primarily due to an increase in the number of placements which aligns with changes to CHC process to reduce pressure on the acute system, in particular to reduce the number of Delayed Transfers of Care (DTOC). In addition, 4 high cost children’s
018

6
packages have been agreed which have a total cost of £0.38m per annum. Mental Health The Mental Health YTD over spend of £0.18m and forecast outturn over spend of £0.20m reflects funding costs associated with older people mental health services. The CCG is committed to implement all planned Mental Health schemes and investments in line with our local investment strategy. Where schemes planned for 17/18 have not yet been fully implemented then the full level of resources will be available in 18/19.
Prescribing The prescribing budget has been set at £48.10m which is equal to the 2016/17 outturn and in therefore consistent with the Stockport Together economic case. The current prescribing forecast of £49.09m therefore reflects an over spend of £0.99m but includes significant unplanned charges for concessional pricing for drugs which are in short supply (£2.32m) and Category M (generic drugs) price reduction benefits which, as part of a national financial risk reserve, are to be retained by NHS England (£0.48m). Without these externally set charges the Prescribing budget would be contributing an additional £1.81m to CIP.
Primary Care The forecast outturn includes an overspend of £0.34m which incorporates a cost pressure as a result of the 2016/17 QOF achievement being higher than anticipated as well as a higher QOF achievement estimate in 2017/18. The forecast outturn also includes an overspend of £0.24m due to an increase in claims for sickness and parental leave cover. These cost pressures have been offset by lower than planned increases in patient list sizes £0.30m, recovery of business rate overpayments and underspends within local enhanced services £0.19m.
5.0 Running Costs (Corporate)
The YTD underspend of £0.62m and forecast outturn underspend of £0.57m reflect pay underspend due to staff vacancies (£0.50m) and non-pay underspends (£0.12m).
6.0 Cost Improvement Programme (CIP)
Year to date £16.36m (93.7%) of the £17.45m CIP plan has been delivered, of which £2.23m has been achieved by deploying the CCG contingency in full against CIP delivery. It is forecast that £17.64m (101.1%) will be delivered by year end.
7.0 Recurrent (Underlying) Position Due to the planned level of Stockport Together benefits not being realised (i.e. activity levels being above planned levels), non-delivery of recurrent CIP and an increase in the number of CHC placements a £3.10m (Appendix 1 Table 1) forecast recurrent deficit will be carried forward into 2018/19.
019

7
This recurrent deficit places a significant additional pressure for the CCG achieving NHSE business rules in 2018/19. Failure to achieve the business rules would have a significant impact initially on the CCGs assessment rating but more fundamentally on the CCGs ability to implement the commissioning strategy, in particular where service change is dependent upon investment.
8.0 Recommendations These are set out on the front sheet of this report. Mark Chidgey Chief Finance Officer March 2018
Documentation Statutory and Local Policy Requirement
Cover sheet completed Y Change in Financial Spend: Finance Section below completed Y
Page numbers N Service Changes: Public Consultation Completed and Reported in Document n/a
Paragraph numbers in place Y Service Changes: Approved Equality Impact Assessment Included as Appendix n/a
2 Page Executive summary in place (Docs 6 pages or more in length) n/a Patient Level Data Impacted: Privacy Impact
Assessment included as Appendix n/a
All text single space Arial 12. Headings Arial Bold 12 or above, no underlining Y Change in Service Supplier: Procurement &
Tendering Rationale approved and Included n/a
Any form of change: Risk Assessment Completed and included n/a
Any impact on staff: Consultation and EIA undertaken and demonstrable in document n/a
020

8
TABLE 1 TABLE 2
TABLE 3 TABLE 4 TABLE 5
TABLE 6
TABLE 7 - not required for month 11 TABLE 8
TABLE 9
Month 11 Financial Dashboard Appendix 1
Month 11 Financial Position - as at 28 February 2018
Budget Actual Var Var Budget Actual Var Var
£000s £000s £000s % £000s £000s £000s % £000s £000s £000s
Revenue Resource Limit (RRL)
Confirmed (415,151) (415,151) 0 0.0% (453,579) (453,579) 0 0.0% (445,422) (445,422) 0
Total RRL (415,151) (415,151) 0 0.0% (453,579) (453,579) 0 0.0% (445,422) (445,422) 0Net Expenditure
Acute 222,724 226,328 3,604 1.6% 242,954 246,811 3,857 1.6% 240,818 245,877 5,059Mental Health 31,120 31,571 451 1.4% 34,221 34,421 200 0.6% 33,721 34,385 664Community Health 35,187 35,490 303 0.9% 38,386 38,686 300 0.8% 38,386 38,695 309Continuing Care 14,043 14,978 935 6.7% 15,320 16,385 1,065 7.0% 15,320 16,411 1,091Primary Care 45,874 45,689 (185) (0.4%) 50,547 50,132 (415) (0.8%) 49,711 49,666 (45)Other 10,142 9,909 (233) (2.3%) 12,160 9,894 (2,266) (18.6%) 4,085 4,216 131
Sub Total Healthcare Contracts 359,090 363,965 4,875 1.4% 393,588 396,329 2,741 0.7% 382,041 389,250 7,209
Prescribing 44,094 44,975 881 2.0% 48,103 49,091 988 2.1% 48,103 48,103 0Running Costs (Corporate) 5,568 5,003 (565) (10.1%) 6,086 5,461 (625) (10.3%) 6,086 6,086 0Reserves (Ref: Reserves Summary) 5,191 0 (5,191) 0.0% 4,484 1,380 (3,104) (69.2%) 4,158 5,075 917
Total Net Expenditure and Reserves 413,943 413,943 0 0.0% 452,261 452,261 0 0.0% 58,347 59,264 917
TOTAL (SURPLUS) / DEFICIT (1,208) (1,208) 0 0.0% (1,318) (1,318) 0 0.0% (5,034) 3,092 8,126
Recurrent Budget
Recurrent Commitment
Recurrent Variance
(Favourable) / Adverse
YTD (Mth 11) Forecast 17/18
RAG RATING
RAG Rating Key:
G Potential risk of overspend: less than or equal to £0
A Potential risk of overspend: between £0 and £250k
R Potential risk of overspend: Over £250k
Acute Contract Performance
Annual Budget
Budget ActualYTD Variance - Overspend /
(Underspend)
Forecast Outturn
Forecast Variance -
Overspend / (Underspend)
£'000 £'000 £'000 £'000 £'000 £'000Stockport Foundation Trust 151,426 138,807 138,934 127 151,447 21Manchester University NHS Foundation Trust 23,840 19,863 20,903 1,040 25,015 1,175University Hospitals of South Manchester FT 13,765 13,765 14,355 590 14,351 586Central Manchester University Hospitals FT 10,071 10,071 10,009 (62) 10,009 (62)Salford Royal FT 6,976 6,394 6,832 438 7,500 524The Christie NHS Foundation Trust 3,546 3,250 3,354 104 3,658 112East Cheshire NHS Trust 2,118 1,942 2,158 216 2,357 239Tameside & Glossop Integrated Care FT 1,275 1,169 1,114 (55) 1,216 (59)AQPs/IS 13,786 12,637 13,350 713 14,567 781Other 16,151 14,826 15,319 493 16,691 540Total Acute 242,954 222,724 226,328 3,604 246,811 3,857
Year to Date Forecast
Major Acute Commissioning contracts & AQP/IS
Month 11 - as at 28 February 2018
Forecast Reserves Summary
Reserves Commitments Forecast BalsHeld Mth 11 Year End
Amounts Held in CCG Reserves £000s £000s £000s Investments 7,596 3,134 (4,462) Contingency 0 0 0 In-Year Allocations 684 413 (271) Savings & Efficiency (3,796) (2,167) 1,629Total Reserves 4,484 1,380 (3,104)
Statutory Surplus Forecast £000s2017-18 Allocation (453,579)Less: 2017-18 Expenditure 452,261 In-Year Surplus (1,318)Add: Brought forward 2016-17 Surplus Allocation 0Forecast Statutory (Surplus) / Deficit (1,318)
Public Sector Payment Policy (PSPP) - Measure of Compliance
Number £000s
Non-NHS PayablesTotal Non-NHS Trade Invoices Paid in the Year 11,888 100,701Total Non-NHS Trade Invoices Paid Within Target 11,528 99,910Percentage of Non-NHS Trade Invoices Paid Within Target 96.97 99.21NHS PayablesTotal NHS Trade Invoices Paid in the Year 2,712 261,282Total NHS Trade Invoices Paid Within Target 2,606 260,107Percentage of NHS Trade Invoices Paid Within Target 96.09 99.55Total NHS and Non NHS PayablesTotal NHS Trade Invoices Paid in the Year 14,600 361,983Total NHS Trade Invoices Paid Within Target 14,134 360,017Percentage of NHS Trade Invoices Paid Within Target 96.81 99.46
The Public Sector Payment Policy target requires CCG's to aim to pay 95% of all valid invoices by the due date or within 30 days of receipt of a valid invoice, whichever is later.
February YTD
We will continue to monitor our performance against the 95% 'Public Sector Payment Policy' (PSPP) target of invoices paid within 30 days of invoice. Performance is measured based on both numbers of invoices and £ value.
Cashflow Summary - Month 11 £000sCash Limit for the Year 451,177 Cash drawn down YTD 410,144 Remaining cash 41,033
Actual cash drawn down (%) 90.9%Expected cash drawn down (%) 91.7%
Jan 16 - Dec 16 (£000s)
Jan 17 - Dec 17 (£000s)
Change (£000s)Change in Spend (%)
Change in No. Items (%)
Cardiovascular System 6,528 7,262 734 11.2% -0.4%Appliances 1,526 1,659 133 8.7% 15.3%Stoma Appliances 1,657 1,771 114 6.9% 5.4%Nutrition And Blood 2,893 2,958 65 2.3% 3.2%Immunological Products & Vaccines 603 639 36 6.0% 7.2%
Top Five Increases in Prescribing Spend by Drug Type
021

022

Performance Update Report March 2018
NHS Stockport Clinical Commissioning Group will allow
people to access health services that empower them to live healthier, longer and more independent lives.
Tel: 0161 426 9900 Fax: 0161 426 5999 Text Relay: 18001 + 0161 426 9900 Website: www.stockportccg.org
NHS Stockport Clinical Commissioning Group 7th Floor Regent House Heaton Lane Stockport SK4 1BS
023
Executive Summary
What decisions do you require of the Governing Body? Governing Body is asked to:
(i) Note the format and timing of performance reporting in transitioning to a quarterly integrated performance report.
(ii) Note the performance issues highlighted to the Governing Body, in particular the continued levels of urgent care performance.
Please detail the key points of this report Urgent Care performance remains the key performance area for improvement. What are the likely impacts and/or implications? These are identified in the report. How does this link to the Annual Business Plan? The CCG’s Annual Business Plan is based upon achievement of national standards. What are the potential conflicts of interest? There are no potential conflicts of interest
Where has this report been previously discussed? n/a Clinical Executive Sponsor: Dr Ranjit Gill Presented by: Mark Chidgey Meeting Date: 28 March 2018 Agenda item: 7 b Reason for being in Part 2 (if applicable) Compliance Checklist:
Documentation Statutory and Local Policy Requirement
Cover sheet completed Y / N Change in Financial Spend: Finance Section below completed
To follow
Page numbers Y / N Service Changes: Public Consultation Completed and Reported in Document
n/a
Paragraph numbers in place Y / N Service Changes: Approved Equality Impact Assessment Included as Appendix
n/a
2 Page Executive summary in place (Docs 6 pages or more in length)
n/a Patient Level Data Impacted: Privacy Impact Assessment included as Appendix
Y / N
All text single space Arial 12. Headings Arial Bold 12 or above, no underlining Y / N Change in Service Supplier: Procurement &
Tendering Rationale approved and Included Y / Na
Any form of change: Risk Assessment Completed and included
n/a
024

Any impact on staff: Consultation and EIA undertaken and demonstrable in document
Y / N
025

4000
5000
6000
7000
8000
9000
10000
2016
-04
2016
-05
2016
-06
2016
-07
2016
-08
2016
-09
2016
-10
2016
-11
2016
-12
2017
-01
2017
-02
2017
-03
2017
-04
2017
-05
2017
-06
2017
-07
2017
-08
2017
-09
2017
-10
2017
-11
2017
-12
2018
-01
A&E Attendances (adjusted for calendar days) (Stockport CCG patients, all providers) April 2016 to January 2018
A&E Attendances Average UCL LCL
Issues highlighted to Governing Body 4 hour and 12 hour Urgent Care performance
Performance against the 4 Hour ED waiting time standard has continued to be significantly challenged. The graphs below show performance for the year, and this highlights the continued under-performance against the standard. When we compare our performance to Greater Manchester, our levels of performance are below those of other systems.
Whilst demand is 2.1% higher than last year, we can see that this is within normal/expected levels of variation. Control chart methodology shows that there has not seen a step change in the demand our population places on A&E departments.
Whilst performance is clearly a challenge, there is a small positive improvement in performance evident from March 2017 from 80% to 83%. The winter months have seen below average performance this year, as was the case last year. If our Urgent Care plans are effective, we would now hope to see a further improvement in performance over the summer months, this will need to be both sustained and increased.
026

We see a very similar pattern when we look at Stepping Hill as a whole. Whilst attendances this year are 2.5% up on last year, this all falls within expected and natural variation. A significant element of the 2.5% increase we see is due to below average levels of demand over the winter last year returning to average levels this year.
Again, we see an improvement in performance at Stepping Hill as of March 17 from average performance of 77% to 80%. The run of improved performance from Dec 16 to May 17 is most likely a combination of seasonality and the implementation of the system wide Urgent Care plan.
4000
5000
6000
7000
8000
9000
10000
2016
-04
2016
-05
2016
-06
2016
-07
2016
-08
2016
-09
2016
-10
2016
-11
2016
-12
2017
-01
2017
-02
2017
-03
2017
-04
2017
-05
2017
-06
2017
-07
2017
-08
2017
-09
2017
-10
2017
-11
2017
-12
2018
-01
2018
-02
A&E Attendances (adjusted for calendar days) (Stockport Foundation Trust, all commissioners) Apr 2016 to Feb 2018
A&E Attendances Average UCL LCL
Below average winter demand last year
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
2016
-04
2016
-05
2016
-06
2016
-07
2016
-08
2016
-09
2016
-10
2016
-11
2016
-12
2017
-01
2017
-02
2017
-03
2017
-04
2017
-05
2017
-06
2017
-07
2017
-08
2017
-09
2017
-10
2017
-11
2017
-12
2018
-01
2018
-02
A&E 4 hour performance (Stockport Foundation Trust, all commissioners) Apr 2016 to Feb 2018
Average UCL LCL Target 4hr A&E Performance
Returning to average this year
027

Within Q3, the acuity of patients presenting across the holiday period increased significantly over December with a number of flu patients attending requiring isolation, putting a greater pressure on patient flow through the hospital. During December and January an additional 30 medical beds were opened at SFT to provide additional capacity but placing additional pressure on workforce capacity to staff all areas safely . Additional capacity was commissioned by the CCG over the winter period and into January from Mastercall to support admission avoidance through the following schemes:
– 7 day access – ATT/GP Pathfinder capacity – IV Capacity
Supportive actions have continued to take place to promote performance improvement at Stockport Foundation Trust in January and February. Performance on the 4 Hour target continues to be a challenge with unvalidated performance predicted to be 73.8% in February. Cumulative annual performance of 80.0% for the period April 2017 to February 2018 compares to 77.2% for the period April 2016 to February 2017. 4 hour performance at all providers is slightly higher at 82% year to date. There were 52 patients who experienced a 12 hour trolley waits at Stockport Foundation Trust in January 18, raising the year to date figure to 64 patients. It is known that patients have been experiencing long waits prior to the recruitment of extra medical staff. The recruitment of the medical staff and the subsequent assessment of patients with clear treatment plans and decisions to admit has made the long waits safer but this situation is not acceptable. There is an expectation that further improvements will be made to reduce the incidence of the 12 hour waits. The Quality and Safety Team are working closely with SFT to ensure that there are thorough investigations of each of the circumstances and subsequent learning. A key theme of learning is the timing of bed availability throughout the day, which requires improved flow through the hospital.
Delayed Transfers Of Care There has been good progress in reducing the number of patients classified as DToC, although a point prevalence in medicine in February suggests Medically Optimised Awaiting Transfer (MOAT) patients to be as high as 90; equivalent to 55% of the specialty medicine bed base. A four week Multi Agency Discharge Event (MADE) commenced at the end of January to reduce delays and increase discharges. Implementation of the SAFER programme continues to be the approach for reducing delays from admission to discharge, by aiming to deliver timely appropriate care at the right time in the right place. The implementation is not consistent and a robust standardised approach is needed for the benefits of this programme to be realised. Longer term sustainability of performance will only be delivered by full delivery of the Urgent Care Improvement Plan and the service model changes outlined in the Stockport Together Business Cases.
028

Ambulance Ambulance response times remain a challenge with performance across all categories consistently below the national standard, particularly over the winter months. Response times to Category 2 (emergency) calls are particularly challenging with performance at ~40 minutes in Jan 18 against a standard of 18 minutes. There has been issue with patients experiencing delays in waiting for an ambulance response. The Executive Nurse has corresponded with the Chief Executive of North West Ambulance Service to advise that the delays are impacting in patient safety. The Executive Nurse has also escalated the issue to Blackpool CCG who are the lead commissioner and GMHSCP for wider discussion with the rest of GM CCGs at the GM Quality Board. Referral to Treatment Time for Planned Care (RTT) Maintaining RTT performance at SFT is at significant risk, primarily as a consequence of clinical resources being prioritised away from elective activity to support the urgent care pathway over the winter period. This is in line with national policy. A capacity and demand review has taken place to assess risks to performance and agree a planned response to improving performance.
The impact of the above on the number of patients waiting longer than 18 weeks at SFT is that this has increased from:-
• 268 in November to 472 as at the end of Feb 18 (admitted patients) • 1,322 in November to 1,811 at the end of Feb 2018 (non-admitted patients)
To achieve the 92% standard the combined number of patients waiting longer than 18 weeks should be no greater than 1,675.
52 Week Waits There were 2 reportable 52 week waits in January Diagnostic performance standard and cancelled operations Although within range for January, both diagnostic and cancelled operations standards have failed year to date. The diagnostic performance is a result of patients waiting at Manchester University Hospitals NHS Trust (formerly UHSM and CMFT) Clostridium difficile The 2017/18 Health Economy Target is no more than 86 cases, SFT have been allocated no more than 17 Lapses in Care (LIC) with 69 allocated as non acute cases. SFT cases investigated to determine LIC identified 3 LIC cases for 17/18 (April = 1, May = 2). Due to 9 cases in Dec (trajectory for month is 7), the health economy is currently 9 cases over our total trajectory for the year to date (trajectory of 64, actual of 73) In comparison to 2016/17 for the same period (77 cases), the health economy has reduced the incidence of CDT by 4 cases
029
MRSA We have had one acute MRSA bacteremia reported this year, a ‘transfer in’ from Manchester FT, and as a result the bacteremia has been assigned to SNHSFT. We have had two community MRSA bacteremia reported, one attributed to the Christie Hospital because the patient had not been receiving community services and the other was a Tameside patient. The CCG is currently negotiating with both providers regarding the acceptance of responsibility.
Mixed Sex Accommodation (MSA) The CQC, in its inspection of Pennine Care in 2016 reported that they were in breach of MSA regulations, these have been correctly reported from August 2017 Pennine Care Trust Board has received an options paper to move to single sex wards for both adults and older people to ensure patient safety and maintain dignity, and also to ensure compliance with CQC regulations. A full consultation exercise will need to be undertaken. CPA 7 day Follow up This target is measured quarterly with performance across Q3 at 95.6%. October underperformance: One patient not followed up within 7 days, Trust report every attempt was made to follow-up the service user, this continues. December underperformance: One patient not followed up within 7 days due to patient having influenza.
030

2016/2017 2017/2018
Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan
E.B.5 Patients should be admitted, transferred or discharged within 4hours of their arrival at an A&E department
95% 79.76% 80.75% 87.10% 87.57% 87.29% 85.79% 85.61% 85.04% 83.50% 82.92% 81.68% 80.72% 82.26%
E.B.S.5 No waits from decision to admit to admission (trolley waits) over 12 hours 0 0 0 0 0 0 0 4 0 0 0 8 52 64
ARP.01 Category 1 (life-threatening) calls - 90th centile appropriate response time 00:15:00 #N/A #N/A #N/A #N/A #N/A #N/A 00:15:59 00:16:21 0:15:36 00:16:14 00:18:37 00:16:44
ARP.02 Category 1 (life-threatening) calls – mean time taken for a response to arrive 00:07:00 #N/A #N/A #N/A #N/A #N/A #N/A 00:10:07 00:09:50 00:09:29 00:09:44 00:11:17 00:09:51
ARP.03 Category 2 (emergency) calls – 90th centile appropriate response time 00:40:00 #N/A #N/A #N/A #N/A #N/A #N/A 00:55:54 00:56:11 00:57:41 01:10:18 01:43:58 01:31:33
ARP.04 Category 2 (emergency) calls – mean time taken for an appropriate response to arrive
00:18:00 #N/A #N/A #N/A #N/A #N/A #N/A 00:24:20 00:25:04 00:25:55 00:30:34 00:44:49 00:39:59
ARP.05 Category 3 (urgent) calls – 90th centile appropriate response time 02:00:00 #N/A #N/A #N/A #N/A #N/A #N/A 01:37:27 01:58:21 02:01:58 02:02:02 02:54:47 03:14:16
ARP.06 Category 4 (non-urgent “assess, treat, transport” calls only) – 90th centile appropriate response time
03:00:00 #N/A #N/A #N/A #N/A #N/A #N/A 02:34:21 02:40:28 02:28:47 02:36:00 03:33:35 03:16:31
E.B.15.i Category A calls resulting in an emergency response arriving within 8minutes – Red 1
75% 64.71% 65.64% 70.08% 65.92% 62.50% 64.67% #N/A #N/A #N/A #N/A #N/A #N/A 65.75%
E.B.15.ii Category A calls resulting in an emergency response arriving within 8minutes – Red 2
75% 60.96% 63.44% 68.94% 64.43% 64.67% 64.17% #N/A #N/A #N/A #N/A #N/A #N/A 65.51%
E.B.16 Category A calls resulting in an ambulance arriving at the scene within 19 minutes
95% 88.38% 90.23% 92.54% 90.08% 89.39% 89.80% #N/A #N/A #N/A #N/A #N/A #N/A 90.43%
E.B.3 Patients on incomplete non-emergency pathways waiting no more than 18 weeks from referral
92% 92.76% 92.99% 92.47% 92.89% 92.52% 92.41% 91.97% 91.61% 91.83% 92.18% 91.63% 91.31% 92.08%
E.B.S.4 Zero tolerance of over 52 week waiters 0 1 0 3 4 1 0 2 1 2 3 3 2 21
E.B.4 Patients waiting for a diagnostic test should have been waiting no more than 6 weeks from referral
99% 99.19% 99.56% 99.15% 99.20% 98.84% 98.58% 97.97% 98.41% 99.07% 99.25% 98.93% 99.25% 98.87%
E.B.S.6 Urgent operations cancelled a second time 0 0 0 0 0 0 0 0 0 0 0 0 0 0
E.B.S.2 Number of patients not treated within 28 days of last minute elective cancellation. (Quarterly Measure)
0 #N/A 4 #N/A #N/A 6 #N/A #N/A 2 #N/A #N/A 1 #N/A 9
E.B.6 Maximum two-week wait for first outpatient appointment for patients referred urgently with suspected cancer by a GP
93% 97.22% 97.88% 97.17% 97.95% 97.05% 97.95% 98.83% 97.57% 97.20% 97.65% 95.99% 96.47% 97.40%
E.B.7 Maximum two-week wait for first outpatient appointment for patients referred urgently with breast symptoms (where cancer was not initially suspected)
93% 95.03% 94.80% 93.62% 96.84% 94.85% 98.57% 97.44% 94.92% 98.37% 97.89% 96.95% 99.23% 96.86%
E.B.8 Maximum one month (31-day) wait from diagnosis to first definitive treatment for all cancers
96% 96.32% 100.00% 99.15% 100.00% 98.45% 99.17% 98.54% 98.26% 99.25% 100.00% 98.33% 100.00% 99.14%
E.B.9 Maximum 31-day wait for subsequent treatment where that treatment is surgery 94% 96.77% 96.43% 95.83% 100.00% 100.00% 100.00% 100.00% 93.55% 100.00% 100.00% 100.00% 100.00% 98.91%
E.B.10 Maximum 31-day wait for subsequent treatment where that treatment is an anti-cancer drug regimen
98% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
E.B.11 Maximum 31-day wait for subsequent treatment where the treatment is a course of radiotherapy
94% 100.00% 100.00% 100.00% 100.00% 97.30% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 99.74%
E.B.12 Maximum two month (62-day) wait from urgent GP referral to first definitive treatment for cancer
85% 92.75% 89.04% 91.67% 77.05% 82.00% 90.91% 89.71% 87.50% 91.89% 84.29% 89.47% 84.48% 87.01%
E.B.13 Maximum 62-day wait from referral from an NHS screening service to first definitive treatment for all cancers
90% 83.33% 83.33% 100.00% 82.35% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 96.81%
E.B.14 Maximum 62-day wait for first definitive treatment following a consultant's decision to upgrade the priority of the patient
No National Standard 86.96% 92.59% 84.21% 85.00% 95.83% 69.23% 82.61% 90.91% 88.46% 80.00% 79.17% 84.62% 84.47%
E.A.S.4 HCAI measure (MRSA) 0 0 0 0 0 0 0 1 0 0 0 1 1 3
E.A.S.5 HCAI measure (Clostridium difficile infections) 0 9 9 13 5 8 10 10 7 6 4 9 7 79
E.B.S.1 Mixed Sex Accommodation Breaches 0 0 0 0 5 3 5 6 10 9 6 13 6 63
2017/18 YTD to January 18National StandardNHS Constitution Indicator
Cancer Waits
Healthcare Acquired Infections
Mixed Sex Accommodation Breaches
Code
A&E Waits
Ambulance (Performance at Ambulance Trust Level)
Referral To Treatment Waiting
Diagnostic test waiting times
Cancelled Operations
Performance at M10
031
032

1
Stockport Together Programme Director’s Report
NHS Stockport Clinical Commissioning Group will allow
people to access health services that empower them to
live healthier, longer and more independent lives.
Tel: 0161 426 9900 Fax: 0161 426 5999
Text Relay: 18001 + 0161 426 9900
Website: www.stockportccg.org
NHS Stockport Clinical Commissioning Group
7th Floor
Regent House
Heaton Lane
033
2
Executive Summary
What decisions do you require of the Governing Body?
No decisions are required of the Governing Body
This report is for consideration and note
Please detail the key points of this report
The report draws the Governing Body’s attention to three areas:
- The progress made in service delivery, IM&T and structural change including consultation in 2017-18
- The most significant issues facing the partnership in delivery of the model currently and progress in addressing these
- The next steps with a focus on the first quarter of 2018-19 What are the likely impacts and/or implications?
- Considerable contract work to embed changes from a commissioning perspective
- Slower than anticipated benefits realisation resulting in lower than originally planned activity changes as set out in the CCG operational plan
How does this link to the Annual Business Plan?
The Annual Business Plan includes delivery of improvements in the areas described and sets out the associated shifts in activity.
What are the potential conflicts of interest?
None
Where has this report been previously discussed?
Stockport Together Programme Board
Clinical Executive Sponsor: Gaynor Mullins
Presented by: Tim Ryley
Meeting Date: 28th March 2018
Agenda item: 8
034

3
Stockport Together Governing Body Report
1. Introduction The Stockport Together programme is coming to the end of the second year of its 5 year plan and the second year of the 3 year Greater Manchester Partnership Investment Agreement. The programme is designed to address many of the deep rooted causes behind the financial and performance challenges facing Health & Social Care in Stockport. The programme has a number of dimensions including structural change, a large scale and recurrent investment in new integrated services, and a new integrated outcome based approach to commissioning. Full realisation of our ambition also requires significant cultural change among leadership and staff across the system.
This report updates the Governing Body on:
- Progress made in this financial year - The main issues being addressed by the programme - The next steps in Quarter 1 of 2018-19.
2. Progress in 2017-18 During 2017-18 we have made significant progress in a number of areas: Service Delivery, IM&T, Structural change
2.a. Service Delivery The following services have gone live as a consequence of the plan during this financial year:
• Stockport Falls Service – Steady in Stockport • Psychological Medicines Service • Care Home Quality Team • Crisis Response • Active Recovery • Integrated Discharge Team • Enhanced Case Management
Work is still underway to ensure these are fully optimised as we bring together staff and process across the system. In a number of other areas service delivery is being rolled-out and it is anticipated will be completed in the first quarter of 2018-19, including
• GP 7 day services • GP Home Visiting services • Enhanced Medicines Management • Direct Access Physiotherapy
The one area where considerable further work will be required in 2018-19 is Outpatients.
035

4
2.b IM&T All GP Practices and the NHS Community Services are now on EMIS (EMIS is a sophisticated patient record system). EMIS remote access (RC) is in A&E to provide access to patient information to hospital clinicians and is being utilised to roll-out GP 7 day access and home visiting services.
The Stockport Health & Social Care record (SHSCR) version 3 has been implemented ensuring live feeds and thus real time data is now potentially available to all professionals working together to care for individuals. The GM Partnership has now adopted the same system across Greater Manchester and this will enable information sharing at a patient level under the right information governance arrangements across all GM health & social care providers. Further work is required in 2018-19 to deliver on all these opportunities.
2.c Structure At a system level we have the neighbourhood leadership established including GPs from the CCG Governing Body who have transferred to Viaduct Care.
The permanent SNC management team is now in place with Caroline Drysdale’s arrival and the Alliance Agreement is now formally signed by all providers.
We have undertaken a thorough public consultation exercise leading to approval of business cases by the joint commissioners allowing for changes to be made recurrent through contracts.
3. Issues The scale and complexity of the changes underway are significant. There are a number of issues currently being managed jointly by the Stockport Together Chief Executive’s Group.
Issue Escalated Progress Update 1. Pace of introducing Enhanced Case Management
The integration of social workers, community nursing and others utilising risk stratification and MDT’s is the largest single project within the programme to date and is also identified as the primary individual driver of non-elective benefit. Since November 2017 significant progress has been made - 150 staff have been trained to be enhanced case managers with another 122 booked in for March; 345 individuals have active Goal of Care plans with a further 1648 identified; 7 out of 8 neighbourhoods have the service.
2. Pace of introducing GP 7 day & Home Visiting Service
There have been delays in getting the Viaduct Care Contract in place. The Contract has now been agreed. Viaduct Care underwritten by the CCG has gone at risk and 2 hubs are already on line and all are on-track for May. Home visiting will go live in April 18.
3. Commissioning the Collaborative
There has been concern about the impact on benefits of this work area being behind due to challenges of starting a new
036

5
General Practice Model
organisation from scratch and associated contract delays. As noted above the contract is now agreed as organisational structures in place. In addition 5 CCG staff are now supporting Viaduct Care. It should be noted that other than prescribing Viaduct Care projects are not significant direct drivers of financial benefit delivery. The good news is that prescribing improvements whilst not yet at full mobilisation have already delivered next year’s benefit of £1.5m. Viaduct Care have been recruiting ahead of contract for the full range of services and it is expected that all services will be mobilised in the first quarter of 18-19 with 7 day and home visiting earlier.
4. Development of system level Workforce & OD strategies
There is a Workforce Strategy & Plan in place for Stockport Neighbourhood Care and workforce is now being tracked in an integrated way. However, there is not a yet a sufficiently robust workforce strategy for the wider system. The CCG Governing Body have noted as a condition of business case approval that a plan is put in place ahead of the CQC visit to address this and an individual of suitable calibre is appointed. This will also need to address wider OD. A draft proposal is being worked up.
5. Formal Staff Engagement
Work continues with staff side representatives to address concerns and a further series of staff engagement events is being undertaken. The challenges we are facing are indicative of the level of change we are now embedding as normal business.
7. Accessing Digital Funds
In a number of areas full mobilisation is now being compromised by IM&T systems and lack of mobile technology. This is in part (though not exclusively) due to delays in securing the digital fund component of the Investment Agreement. Over a three year period we had planned for £3.1m; to date the figure received is closer to £1.4m. To mitigate this where possible we have deployed other resources but mobile working in particular has been delayed. We are working with GMHCP with the intention of securing the remaining funding in 18-19.
8. Benefit Realisation Plan
The system in the Economic Business Case (and other cases) agreed a set of benefit realisation measures in 2017 and monitors these through routine systems. However, as we move into full mobilisation (and the need to realise benefits through cash releasing activity) it was agreed that this needed to be further developed. A piece of work has been undertaken and during March will be going through partnership governance starting with providers to ensure input and accuracy and will go to the Chief Executives’ Group in April. It is focussed on three tiers. Bottom Tier answers the question, “is this service mobilised?”. The next tier (2) answers the question, “is the service optimised and working as envisaged?”, and Tier 1 then asks whether the collective impact of optimised services is
037

6
delivering benefits both on the target cohorts and also on the wider system. Wherever possible all benefits are tracked at both neighbourhood and system level.
4. Next Steps During 2018-19 the emphasis will be on optimising the services already mobilised, completing mobilisation of those under development and in particular focussing on ensuring that service transformation supports urgent care delivery and making the planned changes to outpatients.
In the first quarter of next year the emphasis will be on:
• Optimisation of existing new service models • Completing mobilisation of collaborative general practice • Ensuring changes are being managed effectively through joint commissioning
arrangements • Adjusting the service model in light of learning from the CQC visit to Stockport • Renegotiation of the GM Investment Agreement • Taking forward integration of commissioning to create a single strategic
commissioning function (SCF)
038
Quality Report
Report of the Quality Committee – March 2018
NHS Stockport Clinical Commissioning Group will allow people to access health services that empower them to
live healthier, longer and more independent lives.
NHS Stockport Clinical Commissioning Group 7th Floor Regent House Heaton Lane Stockport SK4 1BS
Tel: 0161 426 9900 Fax: 0161 426 5999 Text Relay: 18001 + 0161 426 9900
Website: www.stockportccg.org
039
Page 2 of 4
Executive Summary
The Governing Body is requested to consider the issues discussed at Quality Board Please detail the key points of this report
Summary This report summaries
• The key issues arising from the Quality Committee in February 2018
• Quality Committee August Issues Log
Decisions - None
How does this link to the Annual Business Plan? Improving the quality of commissioned services is a key strategic aim within the CCG Annual Operational Plan.
What are the potential conflicts of interest? None Where has this report been previously discussed? Quality Committee Clinical Executive Sponsor: Dr Simon Woodworth Presented by: Anita Rolfe Meeting Date: 28 March 2018 Agenda item: 13 Reason for being in Part 2 (if applicable) Not applicable
040

Page 3 of 4
1.0 Quality Committee – February 2018 The Quality Committee is a sub-committee of Stockport CCG’s Governing Body. It highlights quality and safeguarding concerns to the Governing Body by the use of an issues log. The Quality Committee meeting in February 2018 reviewed a number of quality reports from a range of providers and areas, in line with the quality assurance framework managed by the quality and safeguarding teams. Highlight information for the Board to note: • Safe Staffing. Quality committee have reviewed safe staffing as part of a deep dive process
and acknowledge the challenges that are being experienced by all care providers across the Stockport system. Stockport providers are reflective of the national picture. Stockport NHS FT has invested a significant amount of senior nursing time and capacity into developing a recruitment and retention strategy and this is having a positive impact for them. Pennine Care NHS FT have been subject to a 5 CCG scrutiny of safe staffing levels, with further detail still needed to confirm future plans. Pennine Care is using significant amounts of bank and agency spend to support 1:1 observations of patients to maintain safety.
• Safeguarding Exception Report: An update on progress in meeting the assessment expectations for Looked After Children was received. The timeliness of initial health assessments remains a significant challenge however an action plan is in place to reduce the waiting list for the health assessments. There are currently 375 children placed in Stockport from outside of the borough. In line with the expectations from the GMHSCP Q3 assurance meeting with GMHSCP, there has been follow up action completed to engage with the GM LAC review. A GM summary report is expected in April 2018.
• Harm Free Care: Venous Thromboembolism (VTE) prevalence remains below the national expectation and is being monitored by the CCG Quality Lead. The CCG is above trajectory for C Difficile (C Diff) for the year to date. The CCG has strengthened its quality oversight with SNHSFT now that there is a specific lead nurse for quality in place, and a weekly review of all cases is now place.
• Maternity Care: There has been a delay in the reporting of the NHSSFT maternity dashboard for Quality Committee to consider. SNHSFT have been formally requested to ensure that the information is made available to the next CCG Quality and Performance contractual oversight committee for discussion.
• Continuing Health Care: The team continues to actively maintain the number of completed assessments in hospital at around 9%. In relation to the completion of process within of 28 days from date of referral to ratified outcome, the team is improving towards the 80% KPI, and is currently achieving around 73%.
• Stockport NHS Foundation Trust – The committee were updated on the FT’s progress to complete serious incident investigations, which has demonstrated fragile improvements that need time to embed thoroughly. The Trust has recently reported an issue with its policy and procedures governance following the migration from one IT system to another. There are a large number of policies showing as very overdue for revision. SNHSFT corporate nursing team is supporting the correction of the issue. An update on progress was required at the Quality and Performance Contractual meeting. Issues also remain with system and process for the management of appropriate application of NICE Guidance within the Trust.
• Urgent Care – Quality committee noted the significant efforts that are being applied across the system as well as the oversight that is provided from
- Urgent Care Cabinet - Urgent Care Delivery Board - Stockport Improvement Board
The increase in 12 hour breach incidents is an indication of a change in practice now that patients are being assessed and provided with a Decision to Admit rather than long waits in ED that are not recorded as such. The CCG quality assurance team continues to routinely visit Stepping Hill to view care being provided in line with the CQC action plan that is in
041

Page 4 of 4
place. The Director of Nursing at Stepping Hill is leading a number of patient experience changes that are expected to demonstrate improvements in care.
• Pennine Care NHS Foundation Trust –The 5 CCG Clinical Quality Leads Group, continues to oversee quality assurance and is attended by all commissioning CCG quality leads. PCNHSFT are focusing on ensuring that mixed sex accommodation expectations are met, as well as understanding safe staffing requirements more deeply.
• SEND – The development of SEND services continue with a focus on compliance with the expected SEND inspection that is likely to take place later in the year continues.
2.0 Quality Committee Issues Log: Issue 1: ED Performance. There is a recovery plan in place through February and March and a Home for Easter plan is underway. Remain on log: RED Issue 2: LAC health assessments. Issues with meeting the health assessment KPI, and follow up support regarding GM approach has been sought from GM. Remain on log: RED Issue 3: NICE Compliance - reporting and assurance process is not improving. Remain on log: RED Issue 4: Non completion of Diabetes Audit. Partial completion for 17/18, but will be compliant in 18/19. Remain on log: AMBER Issue 5: SNHSFT CQC Report. Improvements continue. Improvement Board remains in place Remain on log Remain on log: AMBER Issue 6: SEND reform. Progress impediments to be addressed by the planned workshop in April. Remain on log: AMBER Issue 7: Staffing at SNHSFT. The deep dive has provided further understanding and is managing the recruitment and retention of staff better. Removed from log Issue 8: Leadership capacity at Pennine Care NHS FT. Senior leadership recruitment has resolved this issue Removed from log Issue 9: Serious Incident Management. Remove from log, currently at zero overdue reports, and reporting regularly. Removed from log
042

Page 5 of 4
3.0 Quality Review: The next planned Quality Review will take place in March and will review Safeguarding systems and process. 4.0 Decisions for the Governing Body To note the issues presented. Compliance Checklist:
Documentation Statutory and Local Policy Requirement
Cover sheet completed
Y Change in Financial Spend: Finance Section
below completed N/A
Page numbers
Y Service Changes: Public Consultation
Completed and Reported in Document N/A
Paragraph numbers in place
Y
Service Changes: Approved Equality Impact Assessment Included as Appendix
N/A
2 Page Executive summary in place (Docs 6 pages or more in length)
N/A Patient Level Data Impacted: Privacy Impact Assessment included as Appendix
N/A
All text single space Arial 12. Headings Arial Bold 12 or above, no underlining
Y Change in Service Supplier: Procurement &
Tendering Rationale approved and Included N/A
Any form of change: Risk Assessment Completed and included
N/A
Any impact on staff: Consultation and EIA undertaken and demonstrable in document
N/A
Anita Rolfe Executive Nurse Stockport CCG March 2018
043

044

Report of the Finance and Performance Committee
NHS Stockport Clinical Commissioning Group will allow
people to access health services that empower them to live healthier, longer and more independent lives.
Tel: 0161 426 9900 Fax: 0161 426 5999 Text Relay: 18001 + 0161 426 9900 Website: www.stockportccg.org
NHS Stockport Clinical Commissioning Group 7th Floor Regent House Heaton Lane Stockport SK4 1BS
045
Executive Summary
What decisions do you require of the Governing Body? This report provides a summary of the meeting of the Finance and Performance Committees which took place on 14th March 2018. No decisions are required of the Governing Body.
Please detail the key points of this report
The report provides an overview of the discussions which took place at the meeting relating to the following matters:
• 17/18 CIP progress and financial position. • Prescribing benchmarked position. • Governance. • Compliance with the 18/19 planning process.
What are the likely impacts and/or implications? Non delivery of CIP would impact significantly on the CCG’s financial plans and the delivery of required efficiencies (both non-financial and financial). Compliance with NHSE requirements are an important requirement of the CCG assurance framework. How does this link to the Annual Business Plan?
CIP is an integral part of the CCG’s Operational Plan.
What are the potential conflicts of interest?
None
Where has this report been previously discussed? The issues covered by this report were considered at the Finance and Performance Committee meeting on 14th March 2018. Clinical Executive Sponsor: Ranjit Gill Presented by: Vicci Owen-Smith Meeting Date: 27th March 2018 Agenda item: Reason for being in Part 2 (if applicable)
Finance and Performance Committee Update for Governing Body
046

Meeting of the 14th March 2018
1.0 CIP and Financial Position
The committee reviewed risks associated with the forecast outturn surplus of £1.32m which is in line with the plan. It was noted that whilst CIP achievement for the year is likely to exceed 100% this includes the release of contingency. The committee also noted that a significant element of this was non-recurrent and this was a significant factor in the 18/19 plan including a significant deficit of £3.1m - £3.5m.
The committee reviewed the risks that remain to achieve the target year end surplus and it was confirmed that after implementation of agreed mitigation actions the net risk of £0.0m was achievable. The committee emphasised the importance of agreeing and implementing the 18/19 CIP plan and the risks of both unidentified CIP and continued reliance on non-recurrent achievement.
2.0 Prescribing Benchmarking Report
The committee received and scrutinised a benchmarking report of Stockport CCG prescribing expenditure alongside local and national comparators. The committee requested that additional information was brought to the committee in April in order to complete their assurance review.
3.0 Governance
It was confirmed that a new chair was required for the committee and that this would form part of a wider review of governance within the CCG.
4.0 Compliance with Planning Process The committee reviewed the draft plans that had been submitted and received confirmation that:-
• The CCG had submitted the required information in March and was on track to achieve the remaining planning milestones.
• Contract variations for price and activity variations would be agreed by the 23rd March deadline.
• The GM Investment Agreement activity targets would be reviewed with partner organisations during Q1 of 2018/19.
047

048

Report from Primary Care Commissioning Committee
NHS Stockport Clinical Commissioning Group will allow
people to access health services that empower them to live healthier, longer and more independent lives.
Tel: 0161 426 9900 Fax: 0161 426 5999 Text Relay: 18001 + 0161 426 9900 Website: www.stockportccg.org
NHS Stockport Clinical Commissioning Group 7th Floor Regent House Heaton Lane Stockport SK4 1BS
049

Executive Summary
What decisions do you require of the Governing Body? This report provides an overview of the considerations at the Primary Care Commissioning Committee at its meetings held on 25 January 2018. Please detail the key points of this report The Primary Care Commissioning Committee has been established by the CCG to exercise the management of the delegation functions and the exercise of the delegated powers from NHS England in relation to the commissioning of primary care medical services. The Committee held a Part 1 meeting on 25 January 2018 as part of its routine cycle to consider a range of issues which included consideration of the following matters: 1. Contract Merger Proposal – Eastholme Surgery and Heaton Moor Medical Group which
was supported on the basis of a supportive stakeholder consultation and the benefits for patients and the practice workforce. Approval was subject to agreement of IT costs and merger date.
2. Draft GMS Contract Review proposal which had been undertaken across Greater Manchester. The Committee agreed that the latest GMS Standard Contract (2017/18) be re-issued to Greater Manchester Contract Holders.
3. Viaduct Care Establishment and Contract Update – The Committee received an overview
of progress since the approval of the Commissioning Intentions which were subsequently issued to the Federation including the negotiation process which was currently underway. In particular the Committee considered the risks and mitigations.
4. Primary Care Quality in particular noting the service developments in safe guarding and
shared care drugs funding. The Committee also considered flu vaccination rates in Stockport and some continued concerns around data transfer from pharmacies to GPs.
What are the likely impacts and/or implications? The work of the Primary Care Commissioning Committee is integral to managing the delegated functions from NHS England and ensuring the continued high quality provision of primary care medical services in Stockport. How does this link to the Annual Business Plan? The work of the Committee supports the delivery of the Annual Business Plan and ensures the CCG complies with its statutory duties. What are the potential conflicts of interest? Conflicts of interest for members of the Primary Care Commissioning Committee continue to be managed in line with the NHS England Statutory guidance, in particular for those members of the Committee who are GPs. Where has this report been previously discussed?
050

The issues covered by this report were considered at the Primary Care Commissioning Committee on 25 January 2018. Some issues were also discussed by the Primary Care Quality Committee Clinical Executive Sponsor: Dr Ranjit Gill Presented by: Jane Crombleholme Meeting Date: 28 March 2018 Agenda item: 15
051

052





























