Embed Size (px)
Citation preview
Mark A. Carlson, MD
Department of SurgeryUniversity of Nebraska Medical Center
Omaha VA Medical CenterOmaha, Nebraska
USA
Next Generation Hemostatic Devices
UNMC Surgical Grand Rounds, March 10, 2010

Disclosures:None
Disclaimer:Not a trauma surgeon
Not a vascular surgeon
Content available: www.nebraskasurgicalresearch.com

Overview
• Currently available hemostatic aids & devices
• Description of Univ Nebr hemostasis research
• And, a completely unrelated topic in General Surgery

The Military Experience
• 15-20% of combat deaths are potentially preventable
• Rapid battlefield evacuation has resulted in more soldiers dying atmedical treatment facilities
• About half of the deaths from penetrating trauma are due to hemorrhage
• Hemorrhage is the #1 cause of preventable death
Impetus to improve treatment of exsanguinating hemorrhage

Clinical Problem:exsanguinating hemorrhage
Ann Surg 2007; 245: 986-991
J Trauma 2003; 54: S13-S19

Distinction:
*locally-applied (topical)* vs. systemic agents
NovoSeven(Novo Nordisk)Dry Fibrin Sealant Dressing
(American Red Cross)
Current Hemostatic Devices



The Ideal Hemostatic Device
1. *Efficacy*
2. Biocompatibility3. Safety4. Pliability5. Simplicity6. Stability7. Affordability8. Scalability9. FDA compatibility

State of the Art:Locally-Applied Hemostatic Devices
1. Occlusion/tamponade agents2. Scaffolding agents3. Chitin-based agents4. Mineral agents5. Thrombin-based agents6. Sealants7. Experimental treatments
Categories
…a Growth Industry

1. Occlusion & Tamponade Agents
limited to bone;local effects?
rapid; not dependenton patient; slowly
eliminated
occlusion &tamponade
alkylene oxidecopolymer
Ostene (Ceremed)
nonabsorbable;inhibits union;limited to bone
cheap; rapid; notdependent on patient
occlusion &tamponade
beeswax, paraffinBone wax (Ethicon)
disadvantagesadvantagesmechanismcompositionAgent
Indication: bleeding from cut surface of bone
Sternotomies

2. Scaffolding Agents
swelling brings risk ofcompression
biodegradable; pHneutrality; combinable
with thrombin
clotting scaffold;tamponade
gelatin foam(hydrolyzed collagen)
GelFoam (Pharmacia& Upjohn)
acidic degradation;possible long-term
complications
absorbable; pliable;versatile; antimicrobial
clotting scaffoldoxidized regeneratedcellulose (wood pulp)
Surgicel (Ethicon)
less effective withthrombocytopenia;handling issue with
powder form
biodegradable; pHneutrality; versatility;no effect by heparin;
no swelling
clotting scaffold;platelet activation
microfibrillar collagen(multiple formulations)
Avitene (Davol)Helistat (Integra)Instat (Ethicon)
disadvantagesadvantagesmechanismcompositionAgent
Indication: raw surface bleeding; small vessel/orifice bleeding
GelFoam in tumor bed Surgicel on liver bed

3. Chitin-based agents
HemCon(HemCon MedicalTechnologies)
modified Rapid DeploymentHemostat, mRDH (MarinePolymer Technologies)
TraumaStat (Ore-Medix)
allergy risk; relies onpatient’s clottingcascade; gauze-
based products arenonabsorbable
absorbable;antimicrobial;
versatile; stable;gauze-based productsare more efficaciousthan regular gauze
scaffolding agent;vasoconstrictor;
clotting activation
polymers ofN-acetyl-
glucosamine(chitin, chitosan)
Celox (Celox Medical)
disadvantagesadvantagesmechanismcompositionAgent
Indication: severe traumatic injuries; field use; elective procedures
HemCon Celox

4. Mineral agents
foreign body; relies onpatient; *Army halted
use in 2009
field use; simple; noexothermia
tamponade; sealant;scaffold
clay (silicate) -basedgranules (bentonite,
kaolin, smectite)
WoundStat(TraumaCure)
exothermic reaction;foreign body reaction& fibrosis; relies on
patient’s clotting
field use; simple;newer bandage forms
available withprehydration
absorbent; increaseslocal concentration of
patient's clottingfactors
mineral zeolite(microporous
aluminosilicate
QuickClot, CombatGauze (Z-Medica)
disadvantagesadvantagesmechanismcompositionAgent
Indication: severe traumatic injuries; field use
clay(aka dirt)

"The risk inherent in WS (WoundStat) use outweighs its benefits asa back-up hemostatic agent to combat gauze.
"CG (combat gauze) remains the recommended hemostatic agentfor current combat operations."
All Army Activity Message, 17 April 2009:
WoundStat
J Trauma 2010; 68: 269-278

5. Thrombin agents
requires patientclotting factors;plasma-derived
human plasma-derived thrombin
Evithrom (Ethicon)
requires patientclotting factors
human recombinantthrombin
Recothrom(Zymogenetics)
requires patientclotting factors;plasma-derived;risk of swellingcomplications
swelling + scaffoldeffect
activated thrombin +scaffold
human plasma-derived thrombin +
gelatin
FloSeal (Baxter)
requires patientclotting factors;
allergenic
simple to useactivated thrombin
bovine thrombinThrombin JMI (KingPharmaceuticals)
disadvantagesadvantagesmechanismcompositionAgent
Indication: treatment of raw surface ooze; low pressure/small orificebleeding (scaffold combinations)

6. Sealants
scaffold; fibrin sealant;platelet gel
possible swelling riskcross-links to tissue;rapid effect; minimal
inflammation
wound attachment;sealant
polyethylene glycolpolymers
Coseal (Baxter)
not dependent onpatient’s clottingtrue fibrin sealant
human plasma-derived fibrinogen
and thrombin +plasminogen inhibitor
Crosseal (Ethicon)
plasma-derived; notuseful in the field norfor arterial bleeding;very little Factor XIIIhuman plasma-
derived fibrinogenand thrombin
Evicel (Ethicon)
Tisseel (Baxter)
complex preparationincludes harvest of
patient plasma
combines fibrinsealant & platelet
activities
microfibrillar collagen+ plasma-derivedthrombin + patient’splasma
Vitagel (Orthovita)
risk of local nervecomplications
cross-links to tissue;rapid effect; not
affected bytemperature or liquid
wound attachment;sealant; clot scaffold
glutaraldehyde-crosslinked albumin
BioGlue (CryoLife)
disadvantagesadvantagesmechanismcompositionAgent
Indication: sealing of raw surface ooze and/or small orifice bleeding; tissue “welding”

7. Experimental Treatments
plasma-derived;minimal Factor XIII
activity
collagen sponge +fibrinogen +
thrombin
Tachosil (Nycomed)
complexmost likely the fastest& strongest clotting;no dependence onpatient factors; fully
recombinant;absorbable; pliable;
versatile; optimizable
formation of cross-linked human clot in
an absorbablescaffold
recombinanthuman fibrinogen,
thrombin, andFactor XIII; ±
polylactide mesh
Recombinant HemostaticDevices
(University of Nebraska)
expensive; brittlehandling; plasma-derived; minimal
Factor XIII activity
little dependence onhuman factors;
anecdotal battlefieldsuccess stories
(DFSD); absorbable
formation of humanclot in an absorbable
scaffold
freeze driedfibrinogen +thrombin on
polyglactin mesh
Dry Fibrin SealantDressing, DFSD
(American Red Cross)
disadvantagesadvantagesmechanismcompositionAgent
Indication: varied, including exsanguinatingtrauma in the field
DFSDTachosil
(on vascular graft)

8. Others
1. Hemostase (CryoLife): plant protein; scaffold/activation mechanism
2. Haempatch (Venomics): prothrombinase (Factor Xa mimetic) fromsnake venom in a collagen scaffold (compare to FloSeal, thrombin-soaked GelFoam)
3. Amylopectin powder (Hemostasis LLC)
4. Arista AH; TraumaDex (Medafor): microporous polysaccharide spheres

Hemostasis Research at the University of Nebraska:
Recombinant clotting factors in a variety of formulations

Why is our research “Next Generation”?
1. Recombinant source of all clotting proteins2. Factor XIII3. Biodegradable, nanoengineered matrix4. Treatment can be optimized/configured
1. Efficacy2. Biocompatibility3. Safety4. Pliability5. Simplicity6. Stability7. Affordability8. Scalability9. FDA compatibility
and
10. Versatility
Ideal hemostatic device:


fibrinogen (Factor I)
fibrin monomer
fibrin polymer
fibrin clot
thrombin(Factor II)
Factor XIII(crosslinking factor)
Some have access to this
Everyone has access to this
*Only NU has access to this*
RECOMBINANT VERSION:
Simplified Coagulation Cascade

Expression of Human Proteins in Animal Vectors
Bos taurus
Sus scrofa domesticus
Pichia pastorisN
ational Geographic 1999; 196, N
o. 4
Nature Biotechnol 1997; 15: 971-975
insert gene + mammary specific-promoter into embryo
screen offspring for gene insertion
harvest milk, extract/purify protein product
fibrinogen, thrombin, Factors VII, VIII, IX, XIII,and more

Thromboelastography (TEG)
0 600 1200 1800
seconds
80
60
40
20
0
ampl
itude
(mm
)
normal human blood
high [fibrinogen] + IIa + XIIIa
low [fibrinogen] + IIa + XIIIa
in vitro performance ofrecombinant clotting factors
(clot “strength,”not adherence)
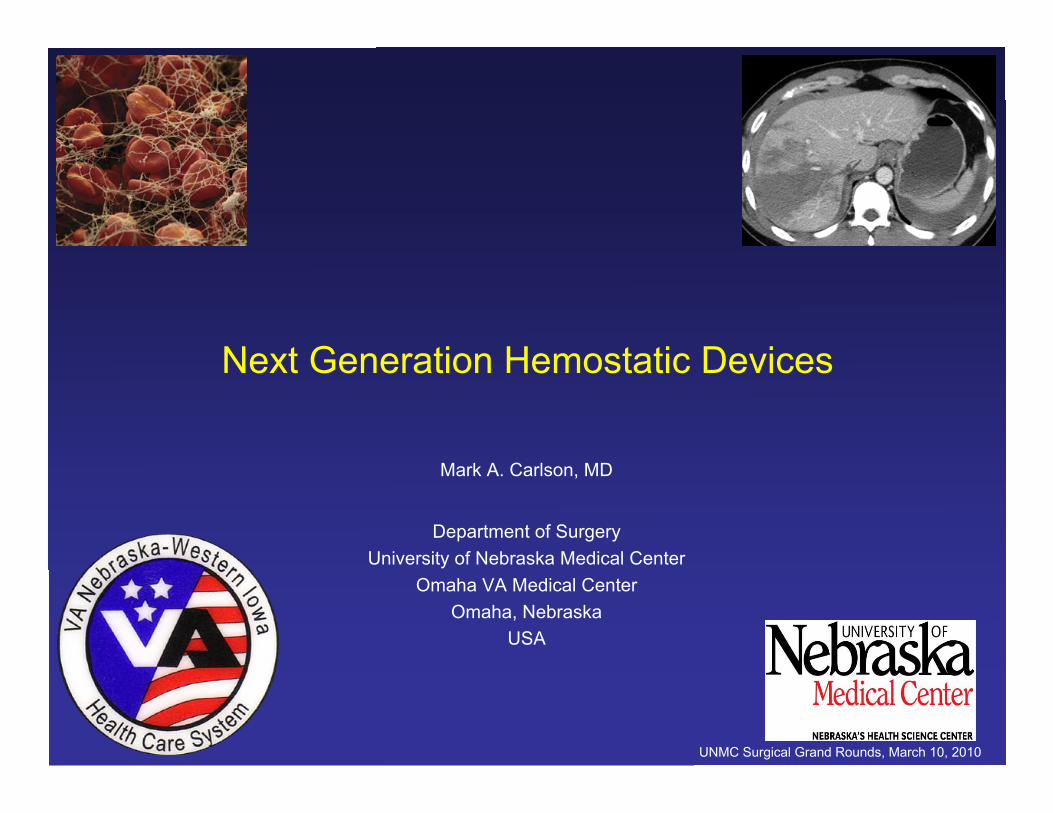
Polylactic acid (PLA) polymer
(or gelatin, chitosan, elastin, composites, etc.)
macroporous
microporousmass production at LNK Chemsolutions (Lincoln, NE)
Absorbable Scaffold

Preclinical Studies
• Swine (~35 kg)
• Femoral arteriotomy (4-6 mm)
• Stellate liver injury, central region
• Major hepatic resection
Endpoints:a) hemostasisb) blood lossc) survivald) vessel patencye) long-term effects
B
C
FA
PLA
M L
prox
dist
PLAM
L
prox
dist
FAL
M
prox
dist
A
PLA
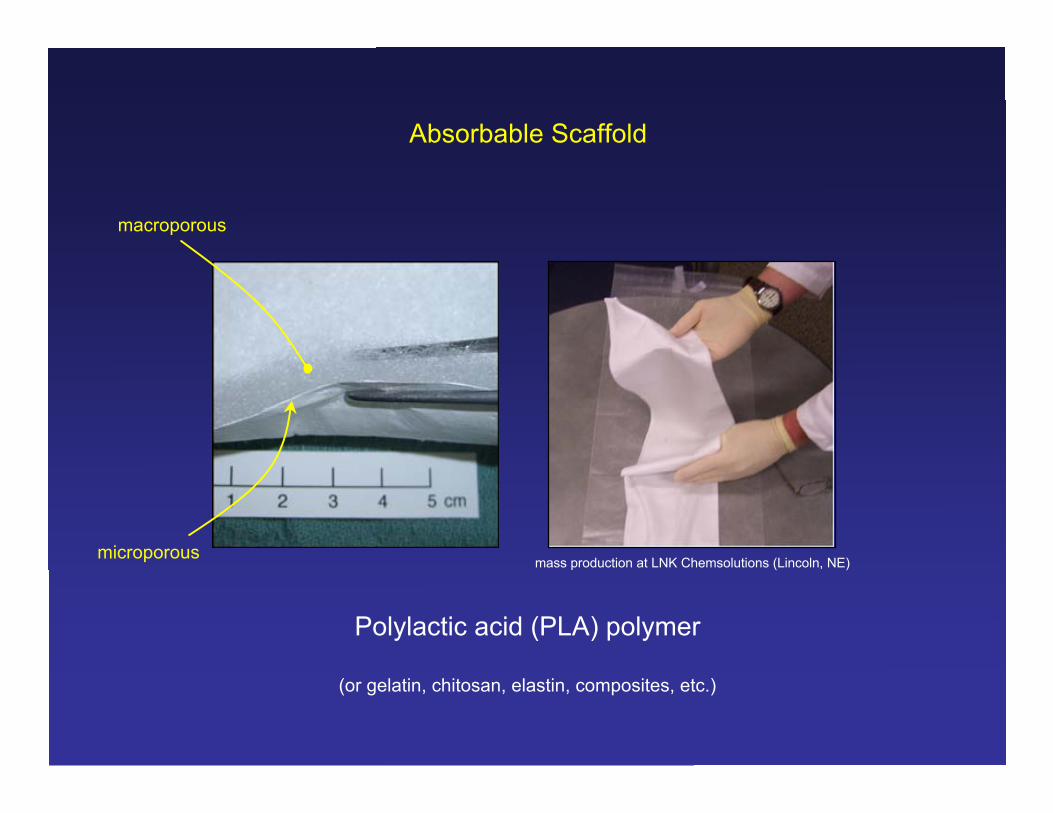
Figure 4: the swine femoral arteriotomy model.(A) The femoral artery (FA) is exposed through agroin incision (right side shown), and controlled withvessel loops. A 4 mm arteriotomy is made with apunch instrument between the loops. A dressing(microporous PLA in this image) then is applied,finger pressure is held for 5 min, and then the site isinspected for bleeding. (B) Hemostatic result afterapplication of microporous PLA in 2 plies, containingthrombin and recombinant Factor XIII in the inner ply,and recombinant fibrinogen in the outer ply. Dopplerflow was present in the distal artery. L = lateral; M =medial; prox = proximal; dist = distal. (C) Hemostaticresult after application of the macroporous (“woolly”)PLA in 2 layers with the same distribution of clottingfactors as in B. Doppler flow was present in the distalartery. (D) Appearance of a macroporous PLA ban-dage containing all 3 clotting factors post-removalfrom an arteriotomy site. Note formation of a prom-inent vessel groove (arrowheads) in the dressingmaterial. This used bandage was quite firm to thetouch.
D
Femoral Arteriotomy
Treatment of femoral arteriotomy with microporous PLAwet with recombinant fibrinogen, thrombin, and XIIIa
[go to video file “Vid1_microporous.mov”]

Treatment of femoral arteriotomy with macroporous PLAwet with recombinant fibrinogen, thrombin, and XIIIa
[go to video file “Vid2_macroporous.mov”]

Blood-letting through femoral arteriotomy withflash of proximal clamp (MAP > 100 mm Hg)
[go to video file “Vid3_bloodletting.mov”]

liver injury clamp
Treatment of central liver injurywith soluble recombinant factors
(fibrinogen, thrombin, XIIIa)
IVC

treatment of central liver injury with liquid recombinant factors (fibrinogen, thrombin, XIIIa)
delivered with aerosol propulsion
[go to video file “Vid4_centralinjury.mov”]

Hemostasis of majorhepatic resections with
recombinant clotting factorsR L
d
gb

Major liver resection treated with recombinant fibrinogen, thrombin, and XIIIa
[go to video file “Vid5_majorresection.mov”]

Quantification of efficacy:
Aerosolized clotting factors& small hepatic wedge cuts
Hemostasis obtained with[fibrinogen] < 10% of that
contained in Tisseel

Application of recombinant factors with dual-reservoir aerosol gun

Small hepatic wedge excisions treated withaerosolized fibrinogen, thrombin, and XIIIa
[go to video file “Vid6_wedgeresection.mov”]

Planned Experiments in Swine
1. Trial of our hemostatic bandage vs. competitor bandage in swine femoralarteriotomy and/or aortotomy models
2. Trial of our fibrin sealant vs. competitor fibrin sealant in a swine liver resectionmodel (normothermic/noncoagulopathic)
3. Trial of our fibrin sealant vs. competitor fibrin sealant in a swine liver injurymodel (hypothermic/coagulopathic)
4. Investigational studies of recombinant factors as systemic adjunctivetreatment of coagulopathic hemorrhage (e.g., treatment of liver fracture incold/coagulopathic swine with intravenous recombinant fibrinogen)
5. Investigational studies of recombinant factors + absorbable scaffold fortreatment of incompressible hemorrhagic injuries

Opinions
Wait, Ground Rounds is not over yet….
1. Variety of topical hemostatic agents with reasonable efficacy
2. Treatment options for exsanguinating hemorrhage in the fieldhave improved, but still need to be better
3. Hemostatic devices composed of recombinant fibrinogen,thrombin, and Factor XIIIa have great potential




![NSR-MSxT2BLB SUGバックアップ編 F V03 - Elecom...1 2 セットアップガイド[バックアップ編] NSR-MS2T2BLB NSR-MS4T2BLB NSR-MS6T2BLB NSR-MS8T2BLB 3 ACLの保存と復元](https://img.dokumen.tips/doc/110x75/5e6d5b3e33c1d14c254dcc0e/nsr-msxt2blb-sugffffffc-f-v03-1-2-fffffffffffffc.jpg)