Embed Size (px)
Citation preview

Next Generation EGFR Inhibitors
Tony Mok MD
Li Shu Fan Medical Foundation Professor of Clinical Oncology
Dept. of Clinical Oncology
The Chinese University of Hong Kong

EGFR TKIs
First Generation
-Gefitinib
-Erlotinib
-Icotinib
Second Generation
-Afatinib
-Dacomitinib
Third Generation Fourth Generation?

EGFR TKI
First Generation
-Gefitinib
-Erlotinib
-Icotinib
Second Generation
-Afatinib
-Dacomitinib
Third Generation Fourth Generation?

ATP Erlotinib Erlotinib +T790M
EGFR Exon 20 T790M

1st generation
gefitinib, erlotinib
2nd generation
Afatinib, dacomitinib
T790M
WT
L858R/
X19 del
IC5
0
Clinical
tolerable
dose

Cross D, et al. Cancer Discov. 2014;4:1046-1061.
3rd-generation EGFR TKI
Mutation selective + irreversible binding + EGFR WT sparing
(30–100× more potent against T790M and 100× less potent against EGFR WT)
Irreversible binding occurs due to covalent bond with C797.

Pyrimidine-based TKI
Zhou and Janne Nature 2009
0
20
40
60
80
100
1000
2000
3000
4000Gefitinib
CL-387,785
HKI-272
WZ3146
WZ4002
WZ8040
H1975
IC5
0 (
nM
)
0
20
40
60
80
100
1000
2000
3000
4000Gefitinib
CL-387,785
HKI-272
WZ3146
WZ4002
WZ8040
PC9 GR
IC5
0 (
nM
)

De
l19
/T7
90
M
0w Vehicle 2w
0w WZ4002 2w
L8
58
R/T
79
0M
0w WZ4002 2w
0w Vehicle 2w
0
50
100
150
200
250
Vehicle WZ-4002 Vehicle WZ-4002
Rela
tive T
um
or
Vo
lum
e %
p = 0.018p = 0.001
L858R/T790MDel19/T790M
Zhou et al. Nature 2009
0 3 7 10 14 17 21 24 280
200
400
600
800
1000
Vehicle
WZ4002
Erlotinib
Day
Tu
mo
r S
ize
(m
m3)
A431 Cells
EGFR WT & amplified

A New Generation of T790M inhibition
AZD9291
HM61713
CO1686
Avitinib

AZD9291
(Osimertinib)

AURA: Phase I dose expansion study
Escalation
Expansion
Phas
e I
Cohort 1
20 mg
Negative
Cohort 2
40 mg
Cohort 5
240 mg
Rolling six design
Cytology
Tablet
Negative
Cohort 3
80 mg
Negative
Cohort 4
160 mg
Positive Positive PositivePositive Positive
Biopsy Biopsy
First-line First-line
Patients with T790M positive advanced NSCLC
whose disease has progressed following either
one prior therapy with an EGFR-TKI or following
treatment with both EGFR-TKI and other
anticancer therapy

AURA: RR of osimertinib in T790M
positive patients
RR: 64%
Janne et al NEJM 372:1689, 2015

Impact of dose on RR

PFS in T790M +ive and –ive populations
Median
PFS at 9.6
months

AURA2: Phase II, open-label, single-arm study on osimertinib
*Mitsudomi et al WCLC 2015
Primary objective
To investigate the efficacy of AZD9291 by assessment of ORR (RECIST 1.1 BICR)
Patients with confirmed
EGFRm locally advanced or
metastatic NSCLC who have
progressed following prior
therapy with an approved
EGFR-TKI
Central T790M mutation
testing* of biopsy sample
collected following confirmed
disease progression
T790M
positive
(n=210)
T790M
negative
AZD9291 80 mg once daily
Not eligible for enrollment
Key inclusion criteria
•Aged ≥18 (≥20 in Japan)
•Confirmation of tumor EGFR mutation associated with EGFR-TKI
•At least one lesion suitable for accurate repeated measurements
•WHO performance status 0 or 1
•Acceptable organ function
•Stable brain metastases allowed

NOTE: Investigator-assessed ORR was also 71% (95% CI 64, 77)
Data cut-off: May 1, 2015. Population: evaluable for response set (n=199). *Represents imputed values: if it is known that the patient has died, has new lesions or progression of non-target lesions, has withdrawn due to disease progression, and
has no evaluable target lesion (before or at progression) assessments, best change will be imputed as 20%; †ORR defined as the number (%) of patients with at least one visit response of complete response or partial response that was confirmed
at least 4 weeks later; ‡Response required confirmation after 4 weeks; §Stable disease ≥6 weeks included the RECIST visit window (±7 days) CI, confidence interval; DCR, disease control rate (complete response + partial response + stable disease)
Tumor response by independent central review
Confirmed objective response Total
ORR† 71% (95% CI 64, 77)
Complete response,‡ n (%)
Partial response,‡ n (%)
Stable disease ≥6 weeks,§ n (%)
Progressive disease, n (%)
2 (1)
139 (70)
41 (21)
15 (8)
DCR92%
(95% CI 87, 95)
Best percentage change from baseline in target lesion – all patients
Complete response
Partial response
Stable disease
Progressive disease
Not evaluable
100
80
60
20
-20
-40
-60
-80
-100
40
0
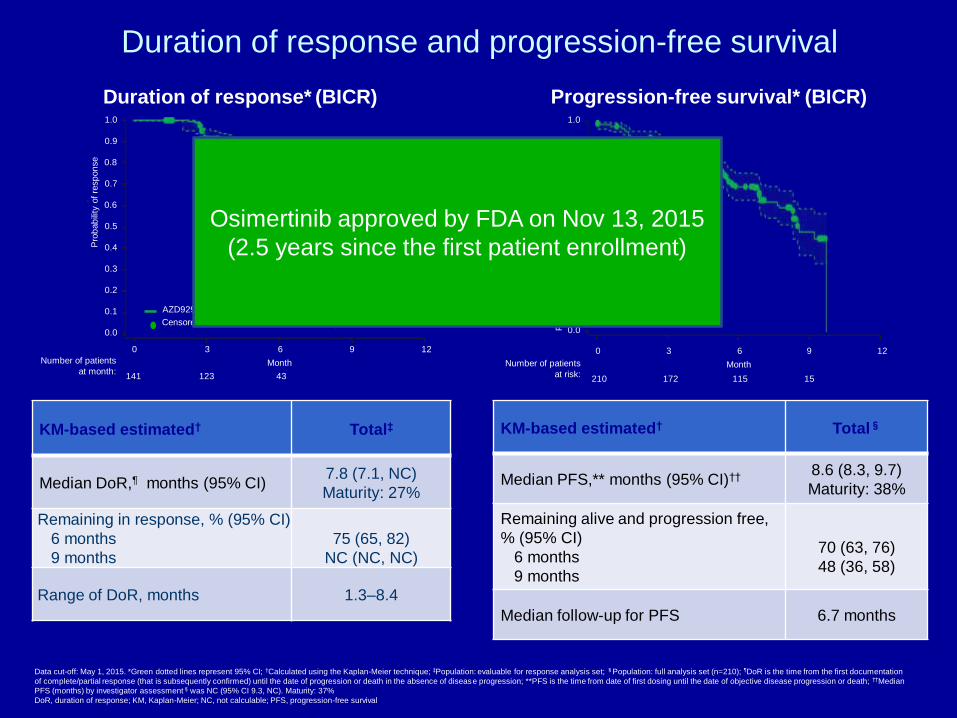
Duration of response and progression-free survival
Data cut-off: May 1, 2015. *Green dotted lines represent 95% CI; †Calculated using the Kaplan-Meier technique; ‡Population: evaluable for response analysis set; §Population: full analysis set (n=210); ¶DoR is the time from the first documentation
of complete/partial response (that is subsequently confirmed) until the date of progression or death in the absence of disease progression; **PFS is the time from date of first dosing until the date of objective disease progression or death; ††Median
PFS (months) by investigator assessment§was NC (95% CI 9.3, NC). Maturity: 37%
DoR, duration of response; KM, Kaplan-Meier; NC, not calculable; PFS, progression-free survival
KM-based estimated† Total§
Median PFS,** months (95% CI)†† 8.6 (8.3, 9.7)
Maturity: 38%
Remaining alive and progression free,
% (95% CI)
6 months
9 months
70 (63, 76)
48 (36, 58)
Median follow-up for PFS 6.7 months
Progression-free survival* (BICR)
KM-based estimated† Total‡
Median DoR,¶ months (95% CI)7.8 (7.1, NC)
Maturity: 27%
Remaining in response, % (95% CI)
6 months
9 months
75 (65, 82)
NC (NC, NC)
Range of DoR, months 1.3–8.4
Duration of response* (BICR)
Number of patients
at risk:
1.0
0.9
0.8
0.7
0.5
0.4
0.3
0.2
0.0Pro
bab
ility
of
pro
gre
ssio
n-f
ree s
urv
ival
129630
Month
0.6
0.1AZD9291 80 mg
210 172 115 15
Censored observations
1.0
0.9
0.8
0.7
0.5
0.4
0.3
0.2
0.0
Pro
bab
ility
of
resp
on
se
129630
Month
0.6
0.1
Number of patients
at month:
AZD9291 80 mg
141 123 43
Censored observations
Osimertinib approved by FDA on Nov 13, 2015
(2.5 years since the first patient enrollment)

AURA2 (n=210)
Osimertinib 80 mg
QD
T790M
positiveT790M
negative
Central T790M mutation testing* of biopsy
sample collected following confirmed
disease progression
Patients with confirmed EGFRm locally
advanced or metastatic NSCLC who have
progressed following prior therapy with an
approved EGFR-TKI
Pooled analysis of AURA 1+2
Escalation
Expansion
Ph
ase
I
AURA Phase II Extension (n=201)
Osimertinib 80 mg QD
T790M
cohorts
Cohort 1
20 mg
Negative
Cohort 2
40 mg
Cohort 5
240 mg
Rolling six design
Cytology
Tablet
Negative
Cohort 3
80 mg
Negative
Cohort 4
160 mg
Positive Positive PositivePositive Positive
Biopsy Biopsy
First-line First-line
AURA Ph I/II AURA2 Ph II
Not eligible
for enrollment
Patients with T790M positive advanced NSCLC whose disease has
progressed following either one prior therapy with an EGFR-TKI or
following treatment with both EGFR-TKI and other anticancer therapy
AURA Ph I data cut-off 4 January, 2016; AURA pooled Ph II data cut-off 1 November, 2015.
*The EGFR T790M mutation status of the patient’s tumour was prospectively determined by the designated central laboratory using the
cobas™ EGFR Mutation Test (Roche Molecular Systems) by biopsy taken after confirmation of disease progression on the most recent treatment regimen.
Data from cohorts in grayed out boxes are not included in the analyses reported here.
QD, once daily
Pooled Phase IIRR and PFS on 411 patients with T790M mutation

Largest cohort (n=411) of T790M +ive
population on osimertinib 80mg
Yang et al ELCC 2016
Median PFS: 11 months

AURA 3 Study Design
P
T790M+
(n=470)
T790M- Not eligible for enrolment
AZD9291 (80 mg p.o.
qd) (n=407)
Platinum-based doublet
chemotherapy* every
3 weeks (n=203)
Central
testing of
~ 1540
biopsy
samples
Randomise ~470 patients 2:1
*Pemetrexed 500 mg/m2 + carboplatin AUC5 or
Pemetrexed 500 mg/m2 + cisplatin 75 mg/m2AUC5, area under the plasma concentration–time curve 5 mg/mL−1 per minute;
EGFRm+, EGFR mutation-positive; EGFR-TKI, EGFR tyrosine kinase inhibitor;
NSCLC, non-small cell lung cancer; p.o., orally; qd, once daily;
T790M+, T790M mutation-positive; T790M-, T790M mutation-negative
Primary endpoint:
PFS
PI: T Mok YL Wu

Best timing for osimertinib?
Dx of EGFR
mutation
positive lung
cancer
(+/- T790M)
Presence of
T790M in
plasma
cfDNA
Clinical
progression
and T790M
+ive
Supported by
AURA 1/2/3
To be supported
by FLAURA? ?
EGFR TKI

Potential study concept:
Osimertinib for molecular progression
Monthly
cfDNA for
T790M for
patient on
first line TKI
Continue
the same
TKI till
radiologic
progression
Osimertinib
Plasma positive for
T790M without
radiologic
progression
osimertinib
Time to osimertinib Failure (TTF)
Time to osimertinib Failure (TTF)
Primary
endpoint:
TTF or OS

Rociletinib (CO-1686)

Phase I/II dose escalation study
T790M positive T790M negative
Sequist et al NEJM 2015
Confirmed RR by central
review in 46 pts = 59%
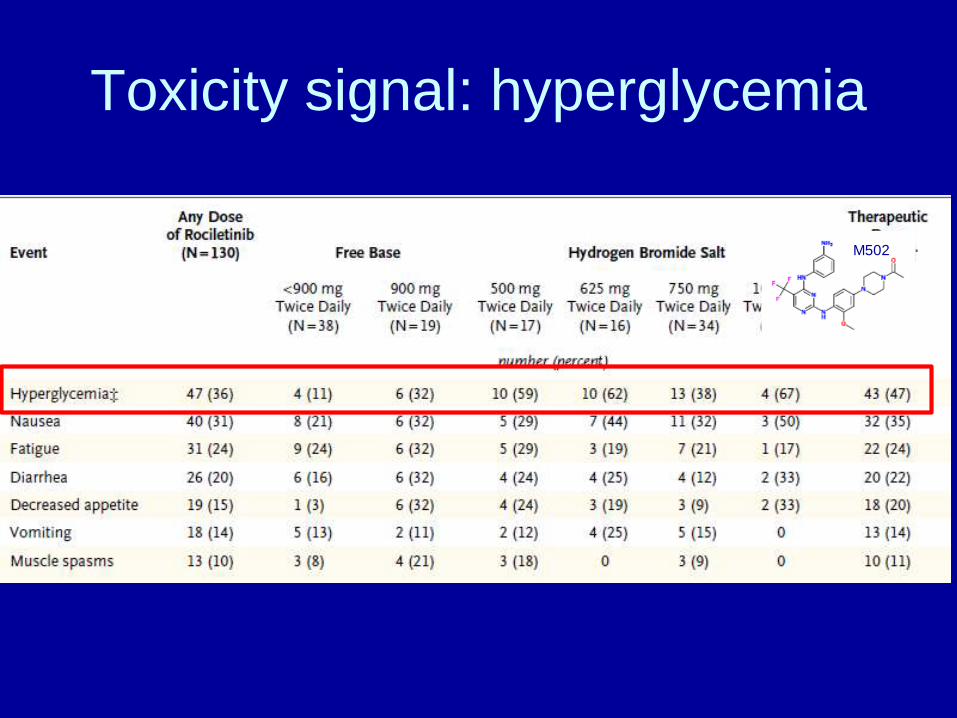
Toxicity signal: hyperglycemia
M502

625mg BID
500mg BID
TIGER-X: Phase 1/2 Trial of RociletinibKey eligibility criteria
• Advanced or recurrent NSCLC with a documented activating EGFR mutation
• Prior treatment with EGFR-directed therapy
• Recent biopsy available or willing to undergo a new on-study biopsy; plasma samples collected
• Phase 2 only
– Disease progression while on treatment with EGFR-directed therapy
– T790M-positive biopsy at the time of entering study
– Treated stable CNS metastases are allowed
26
Phase 1 (Dose Escalation) Phase 2 Expansion Cohorts
CO-1686 Treatment
750mg BID
2nd-line patients
PD upon 1 immediate prior TKI
>2nd-line patients
PD upon ≥2 TKI or chemotherapy
21-day cycles; escalate to MTD
Key outcome measures
• Safety
• Tolerability
• PK profile
• ORR

Best Response to Rociletinib (All Doses) in 256 Centrally Confirmed Tissue T790M+ Patients
100
80
60
40
20
0
−20
−40
−60
−80
−100
SL
D C
han
ge f
rom
Baseli
ne (
%)
500mg 625mg 750mg1000
mgTotal
N 50 124 78 4 256
ORR (%) 60 54 46 75 53
DCR (%) 90 84 82 100 85
27
+ Ongoing
500mg BID HBr
625mg BID HBr
750mg BID HBr
1000mg BID HBr
SLD, sum of longest diameters
*3 patients currently have no evaluable baseline lesions per database and are omitted from this analysis
Nov 2015:
FDA denied the fast track
application
May 2016:
Cessation of future
development of Rociletinib

Olmutinib
(HM61713)

HM61713 = BI 1482694

Phase I/II study in patients with EGFR TKI
pre-treated NSCLC
1. Park K, et al Santa Monica 2016.
Dose escalation (N=66)1
75 mg
100 mg
150 mg
200 mg
250 mg
300 mg
400 mg
500 mg
650 mg
800 mg
1200 mg
Expansion Part 2 (N=76; ongoing)
Expansion Part 1 (N=83)1
T790M-positive (central test)
Progression on ≥1 prior EGFR TKI
T790M positive or negative
Progression on prior EGFR TKI
T790M-positive or negative
Progression on ≥2 prior therapies,
including EGFR TKI

ORR and tumor shrinkage in T790M+
patients (independent review)
PR (n=43)
SD (n=20)
PD (n=3)NE (n=3)
Confirmed PR (n=32)
–100
–50
0
40T
um
or
vo
lum
e c
ha
ng
e (%
)
• DoR is immature; in patients with confirmed OR, response duration ranged between 6 and 31
weeks at data cut-off
Evaluable patients (n=69)
OR (confirmed and unconfirmed), n (%) 43 (62)
Disease control, n (%)
Confirmed OR, n (%)
SD, n (%)
63 (91)
32 (46)
31 (45)
PD, n (%) 3 (4)
NE, n (%) 3 (4)
DoR, duration of response; OR, objective response; ORR, objective response rate; NE, not evaluable; PD, progressed disease; PR, partial
response; SD, stable disease

Most frequent treatment-related adverse
events at 800 mg QDBI1482694 (HM61713) 800 mg QD (n=76)
AE, n (%) All grades Grade 3
Diarrhea 42 (55) 0
Rash 29 (38) 4 (5)
Nausea 28 (37) 0
Pruritus 27 (36) 1 (1)
Dry skin 22 (29) 1 (1)
Palmar-plantar erythrodysesthesia syndrome 22 (29) 2 (3)
Decreased appetite 20 (26) 0
Skin exfoliation 16 (21) 0
Vomiting 12 (16) 2 (3)
Abdominal pain 11 (14) 0
ALT increased 11 (14) 2 (3)
Abdominal pain upper 10 (13) 0
Constipation 10 (13) 0
Pyrexia 9 (12) 0
AST increased 9 (12) 2 (3)
Platelet count decreased 9 (12) 0
Dyspepsia 8 (11) 0
Fatigue 8 (11) 0
AE, adverse event; ALT, alanine aminotransferase; AST, aspartate aminotransferase

LUX Lung Program

ELUXA Lung Program
• ELUXA 1: Phase II trial in ≥second-line patients with
EGFRT790M+ NSCLC
• ELUXA 2: Phase III trial of second-line BI 1482694 vs platinum-
doublet chemotherapy in patients with EGFRT790M+ NSCLC
• ELUXA 3: Phase III trial of first-line BI 1482694 vs afatinib
in EGFR M+ NSCLC
• ELUXA 4: Phase I/II trial of BI 1482694 in Japanese
patients with EGFRT790M+ NSCLC

EGF816

Phase I/II study design
Tan et al ASCO 2015

Tumor response (n=53)
Tan et al ASCO 2015

Skin rash

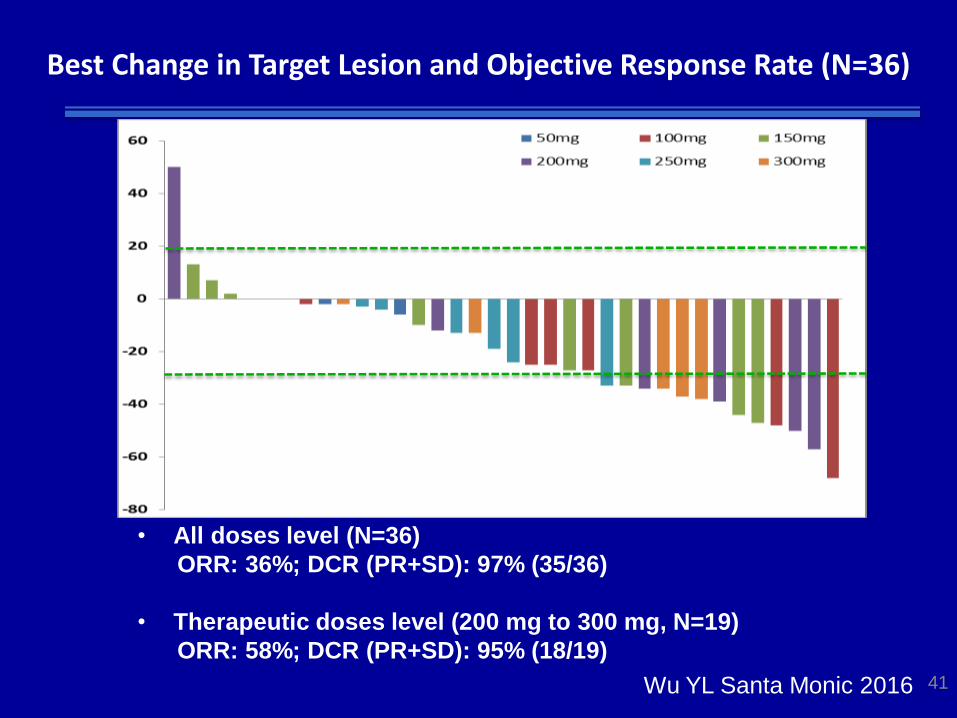
Avitinib (AC0010)

3-6 3-6 3-63-63-6
Phase I dose Escalation/Expansion (BID) in T790M+
NSCLC Patients (NCT02330367)
3-6
40
20 20 202020
41
Best Change in Target Lesion and Objective Response Rate (N=36)
• All doses level (N=36)
ORR: 36%; DCR (PR+SD): 97% (35/36)
• Therapeutic doses level (200 mg to 300 mg, N=19)
ORR: 58%; DCR (PR+SD): 95% (18/19)
Wu YL Santa Monic 2016

EGFR TKI
First Generation
-Gefitinib
-Erlotinib
-Icotinib
Second Generation
-Afatinib
-Dacomitinib
Third Generation Fourth Generation?

Erlotinib
OsimertinibT790M+
EGFR
activating
mutation
T790M-
T790M – plus
unknown
resistance
“Loss of T790M”
T790M+ plus
unknown
resistance
T790M+ plus
C797S
Evolution of resistance mechanisms in EGFR mutant lung
cancer following successive EGFR TKI therapy
= resistance mechanism due to
activation of bypass or downstream
signaling pathway
= EGFR C797S
= EGFR T790M
Oxnard et al. IASLC 2015, and Planchard et al. Ann Oncol 2015

EGFR C797S
Zhou et al. Nature, 2009; Thress et al, Nature Medicine, 2015; 2Oxnard et al. IASLC 2015; 3Song et al. JTO 2016
EGFR C797 – Covalent binding site of all mutant
selective EGFR Inhibitors
Normalize of All Cells
-6 -4 -2 0 20
50
100
150121 pt - GEF
121 pt - WZ
121 Res # 1- GEF
121 Res # 1 - WZ
[TKI] log (uM)
Rela
tive C
ell N
um
be
r %
Co
ntr
ol
Figure 1
A)
Actin
ERK
pERK
pEGFR
- + - + 1 uM WZ
121 Pt Res # 1 C)
D)
MGH121 Res # 1 MGH121 pt
Figure 1 – A WZ4002-resistant cell line acquires a C797S mutation and maintains EGFR activity in the
presence of TKI. A) MGH121 parental (pt) and MGH121 WZ4002 Resistant # 1 (Res # 1) cells were
treated with the indicated concentrations of the 1st generation EGFR TKI gefitinib (GEF) or the 3rd generation
EGFR TKI WZ4002 (WZ) for 72 hours. Cell viability was measured by CellTiter-Glo. Experiments were
performed in quadruplicate and error bars depict standard error of the mean. B) MGH121 pt and Resistant
# 2 cells were treated with the indicated concentrations of WZ4002 (nM) for 1 week and then stained with
crystal violet. C) Lysates from MGH121 pt and MGH121 Resistant # 1 cells treated with DMSO or 1μM
WZ4002 for 6 hours were probed with the indicated antibodies. D) Chromatograms depicting the acquired
C797S mutation present in MGH121 Resistant # 2, but not MGH121 parental cells. The arrow is pointing to
the mutated base (G is WT-Cys, C is mt–Ser).
0
B)
10 30
100 300 1000
0 10 30
100 300 1000
MGH121 pt MGH121 Res # 1
G G C T G/C C C T C
Gly 796
Cys/Ser
797 Leu 798
G G C T G C C T C
Gly 796 Cys 797 Leu 798
EGFR
pS6
S6
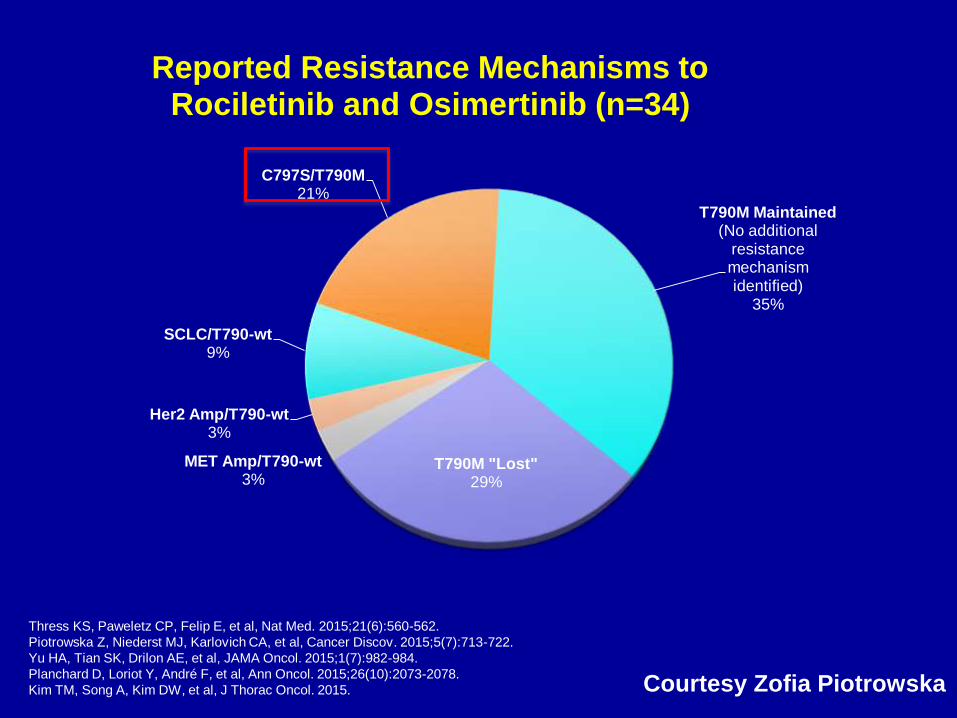
C797S/T790M21%
T790M Maintained (No additional
resistance mechanism identified)
35%
T790M "Lost"29%
MET Amp/T790-wt3%
Her2 Amp/T790-wt3%
SCLC/T790-wt9%
Reported Resistance Mechanisms to Rociletinib and Osimertinib (n=34)
Thress KS, Paweletz CP, Felip E, et al, Nat Med. 2015;21(6):560-562.
Piotrowska Z, Niederst MJ, Karlovich CA, et al, Cancer Discov. 2015;5(7):713-722.
Yu HA, Tian SK, Drilon AE, et al, JAMA Oncol. 2015;1(7):982-984.
Planchard D, Loriot Y, André F, et al, Ann Oncol. 2015;26(10):2073-2078.
Kim TM, Song A, Kim DW, et al, J Thorac Oncol. 2015. Courtesy Zofia Piotrowska

EGFR L798I
αD helix
PNAS, 1991, 88, 5317-5320 Jeabong Jang and Nathanael Gray

Chabon et al ASCO 2016

The first report of a potential
molecule targeting C797S

EGFR Allosteric Inhibitor:
EAI-045

Limited activity as an single agent
• EAI045 binds the C-
Helix, which can be
displaced by
dimerization of EGFR
• Prevention of
dimerization may
improve the potency
of EAI045 in C797S
mutation.

Summary• AZD9291 (Osimertinib)
– Approved therapy for T790M+ disease
– RR at 64%, PFS 9.6month
• CO1686 (Rociletinib)
– RR is not confirmed at the FDA submission
– Hyperglycemia from active metabolite
• HM61713 (Olmutinib)
– Enter into phase III study after a partnership with BI
• EGF816
– Phase I response rate at 75%
– Unusual maculopapular rash
• Fourth Generation?
– Targeting C797S
– Allosteric molecule EAI045

I am so confused!!





























