Embed Size (px)
Citation preview

Review Article
New Therapeutic Agents for Diabetes Mellitus:Implications for Anesthetic Management
Daniel Chen, MD*†
Stephanie L. Lee, MD, PhD‡
Robert A. Peterfreund, MD, PhD†
Multiple hormones and transmitter systems contribute to glucose homeostasisand the control of metabolism. Recently, the gastrointestinal peptide hormonesglucagon-like peptide 1 and amylin have been shown to significantly contribute tothis complex physiology. These advances provide the foundation for new treat-ments for diabetes mellitus. Therapies based on glucagon-like peptide 1 and amylinhave now been introduced into clinical practice. Rimonabant, the selective endo-cannabinoid receptor antagonist, had been used in European countries for thetreatment of obesity; it has recently been withdrawn for this indication. This drugexhibited therapeutic benefits for metabolic variables and for type 2 diabetesmellitus. Anesthesia providers caring for patients with diabetes mellitus will needto understand the implications of these new therapies in perioperative settings,particularly with respect to side effects and interactions.(Anesth Analg 2009;108:1803–10)
Diabetes mellitus (DM) is a condition with anabsolute (Type 1) or relative (Type 2) deficiency ofinsulin. Significant end-organ consequences of bothtypes of diabetes include renal, neurological, cardio-vascular, and peripheral vascular pathology that mayhave an impact on the perioperative course. Multiplehormones and neural systems control glucose ho-meostasis. The principle regulator of plasma glucoselevels is insulin, a polypeptide secreted by pancreatic� cells. The plasma glucose decreasing action of insu-lin has long been recognized and its effect is counter-regulated by epinephrine, growth hormone, cortisoland glucagon, a polypeptide secreted by pancreatic �cells. Conventional therapies for DM have recentlybeen reviewed.1–4 Table 1 presents a summary of themajor classes of medications used in the treatmentof DM.
Contemporary studies revealed that two new fami-lies of gastrointestinal (GI) hormones, represented bythe incretins and amylin, have significant effects onglucose homeostasis. In addition, antagonists of theendocannabinoid system acting at the CB1 receptor,
represented by rimonabant, were found to exert mul-tiple effects on food intake and metabolic variables,including glucose homeostasis. These advances pro-vide new opportunities for therapeutic approaches topatients with DM. Anesthesia providers will increas-ingly encounter patients treated with novel drugsbased on the enhanced understanding of glucosehomeostasis and the physiological control of metabo-lism. We aim to provide anesthesia clinicians with anintroduction to the rapidly evolving pharmacology ofmedical treatment for DM.
BIOLOGY OF INCRETINSIdentification of the members of the incretin family
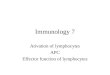
of endogenous gut hormones was based on the obser-vation that the insulin response to oral glucose loads ismore vigorous than from IV glucose loads producingthe same blood glucose levels. In human studies,when subjects achieve identical plasma glucose in-creases, oral glucose administration resulted in moreinsulin secretion than IV glucose administration (Fig.1).5–9 This indicated that previously unidentified fac-tors produced by the GI system influence blood glu-cose levels in combination with the known hormones,insulin and glucagon. The consequence of these gutfactors is called the “incretin” effect.
The incretin effect is mediated via GI hormones thatstimulate insulin secretion in response to glucoseincrease from an enteral carbohydrate load. GIP(glucose-dependent insulinotropic polypeptide) andglucagon-like peptide 1 (GLP-1, Fig. 2) are the firsttwo incretin hormones identified. Because much ofGIP’s insulinotropic effect is lost in diabetic patientsdue to resistance to its actions, its potential utility indiabetic therapy is low7,10 and therefore will not bediscussed further. Unlike GIP, GLP-1’s insulinotropic
From the *Department of Anesthesiology, Hospital for SpecialSurgery, New York, New York; †Department of Anesthesia andCritical Care, Massachusetts General Hospital, Harvard MedicalSchool; and ‡Section of Endocrinology, Diabetes and Nutrition,Boston Medical Center, Boston University School of Medicine,Boston, Massachusetts.
Accepted for publication October 30, 2008.Reprints will not be available from the author.Address correspondence to Robert A. Peterfreund, MD, PhD,
Department of Anesthesia and Critical Care, Jackson 439, Massa-chusetts General Hospital, 55 Fruit Street, Boston, MA 02114.Address e-mail to [email protected].
Copyright © 2009 International Anesthesia Research SocietyDOI: 10.1213/ane.0b013e31819dcc51
Vol. 108, No. 6, June 2009 1803

action persists in patients with DM.10 This makes it apotential target for diabetic therapy. Initial studiesidentified enteroendocrine L cells located in the distalileum and large intestine as the source of GLP-1. Onestudy also found enteroendocrine L cells located moreproximally in the duodenum and jejunum.11 The fastingblood GLP-1 level is approximately 5–10 pmol/L.Within minutes of food intake, the level increases to15–50 pmol/L.11 The rapid increase in blood levels ofGLP-1 suggests that the secretion of GLP-1 is not simplydue to detection of nutrients by the L cells in thedigestive tract; a faster endocrine/neural signalingsystem must also be involved.11
The peptide hormone GLP-1 reduces appetite,slows gastric emptying, reduces glucagon levels, en-hances glucose- stimulated insulin secretion, and in-creases insulin biosynthesis (Table 1).9,11,12 In animalmodels, GLP-1 has trophic actions to increase thenumbers of pancreatic � cells.13 GLP-1 works througha G protein coupled signal transduction system, andits receptors are found in pancreatic � and � cells, thecentral nervous system, and the GI tract. Through itsreceptors on � cells, GLP-1 enhances insulin exocyto-sis, but only in a glucose-dependent manner.7 GLP-1induces gene transcription in pancreatic � cells topromote insulin biosynthesis. In vitro studies demon-strate that GLP-1 influences � cell survival by promoting
Figure 1. Insulin secretion after IV or oral glucose load.Subjects received oral glucose (50 g glucose/400 mL) or anIV infusion of glucose to produce the same blood glucoselevels. As measured by plasma levels of C-peptide (a frag-ment of the insulin prohormone), oral glucose loading (solidcircles) resulted in a greater secretion of insulin comparedwith IV glucose loading (open circles) designed to achieveidentical plasma glucose concentrations. The difference be-tween insulin secretion profiles after oral versus IV loading isdefined as the incretin effect. Left, plasma glucose after oral orisoglycemic IV loading of glucose. Right, C-peptide levels inresponse to oral or IV glucose loading. Modified from Ref 5,with publisher’s permission from the Endocrine Society.
Table 1. Classes of Agents Regulating Glucose Levels
Class Route Mechanism of action Side effects Clinical agentsInsulin SQ, IV 1Glucose uptake Hypoglycemia Many preparationsGLP-1 SQ 1Insulin secretion (if
hyperglycemia)Nausea Exenatide
2Glucagon secretion2Appetite2Gastric emptying
Amylin SQ 2Postprandial glucagonsecretion
Hypoglycemia (withinsulin)
Nausea
Pramlintide
1Satiety2Gastric emptying
DPP-IV inhibitor Oral 2GLP-1 degradation Infection SitagliptinCannabinoid receptor
antagonistOral Weight loss 2Glucose Rimonabant
Multiple other effects Depression2Appetite
Sulfonylurea Oral 1Insulin secretion viabinding to specific receptoron � cells
HypoglycemiaHyponatremiaDrug-drug interactions
ChlorpropamideGlimepirideGlipizideGlyburideTolazamideTolbutamide
Meglitinide Oral 1Insulin secretion by bindingto ATP dependent K�
channels on � cells
Hypoglycemia RepaglinideNateglinide
Thiazolidinedione Oral Insulin sensitizer by bindingto PPAR � receptor
Edema, anemia, obesity,CHF, hepatotoxicity
RosiglitazonePioglitazone
Biguanide Oral 2Hepatic glucose output Lactic acidosis MetforminInsulin sensitizer Diarrhea
Alpha-glucosidaseinhibitor
Oral 2GI glucose absorption byinhibiting enzyme thatmetabolizes complexcarbohydrates
MalabsorptionFlatulenceDiarrhea
AcarboseMiglitol
Incretin-mimetics (GLP-1, DPP-IV inhibitors) and insulin sensitizers (thiazolidinediones, biguanides) in single agent therapy do not predispose to hypoglycemia even in the fasting state.CHF � congestive heart failure; SQ � subcutaneous; DPP-IV � dipeptidyl pepidase IV; GLP-1 � glucagon-like peptide 1.
1804 New Therapies for Diabetes Mellitus ANESTHESIA & ANALGESIA

proliferation and resistance to apoptosis.14 Through itsreceptors on � cells, GLP-1 inhibits glucagon secretionin a glucose-dependent manner and consequentlyreduces hepatic glucose production. The counter regu-latory release of glucagon in response to hypoglyce-mia remains active.15 Through actions on the centralnervous system, GLP-1 decreases appetite and foodintake with a resulting contribution to weight loss.12,15
GLP-1 also slows gastric emptying, thereby bluntingthe postprandial increase in blood glucose levels.6
A feature of the biology of GLP-1 is its rapiddegradation by the peptidase dipeptidyl peptidase IV(DPP-IV) (Fig. 2a).9,16 DPP-IV cleaves peptides at theiramino terminal where the penultimate amino acidresidue is proline or alanine.16 The presence of DPP-IVin the capillary bed of the gut mucosa facilitates rapidinactivation of GLP-1.17 DPP-IV is a ubiquitous,membrane-spanning, cell surface aminopeptidase. Itsextracellular domain can be cleaved and circulate inthe plasma, retaining full enzymatic strength. DPP-IVis also found in liver, lung, kidney, the intestinal brushborder, lymphocytes and endocrine cells. In additionto GLP-1, DPP-IV has numerous substrates, includingvasoactive intestinal polypeptide, gastrin-releasingpeptide, neuropeptide Y and growth hormone-releasing hormone.18,19 DPP-IV also has a role in theimmune system. It is found on lymphocytes as CD26,which has been implicated in cellular uptake of theHuman Immunodeficiency Virus.20 Other biologicaleffects of DPP-IV include actions on T cell activation,chemotaxis and possibly tumor transformation andinvasion.21
Compared with healthy individuals, patients withDM exhibit a blunted increase in blood GLP-1 levelsafter food intake.22 Consequently, experimental treat-ment for DM has evaluated treatment with the nativeGLP-1 peptide. However, since DPP-IV rapidly de-grades GLP-1, only a constant IV infusion of thepeptide is effective in sustaining therapeutic plasmalevels. Two pharmacological strategies are now clini-cally used to counter the effects of the DPP-IV pepti-dase (Table 2).7,8 One strategy uses injection of aGLP-1 analog resistant to DPP-IV. A second pharma-cological strategy targeting DPP-IV uses an inhibitorof this peptidase in order to increase levels of endog-enous GLP-1.
Specific AgentsThe naturally occurring peptide homolog of GLP-1,
exendin-4, resists degradation by DPP-IV. The syn-thetic form is known as exenatide; its commercialname is Byetta�. Exendin-4/exenatide is originallyderived from salivary secretions of the lizard Helo-derma suspectum (the Gila monster) and shares roughly50% of its amino acid sequence with mammalian
Figure 2. Structure of the peptide glucagon-like peptide 1(GLP-1) and analogs. a, Amino acid sequence of the mam-malian peptide GLP-1. Arrow at the amino terminus indi-cates site of cleavage by the ubiquitous peptidase, dipeptidylpeptidase IV (DPP-IV). DPP-IV preferentially cleaves pep-tides with proline (P) or alanine (A) in the second aminoterminal position. b, Amino acid sequence of the naturallyoccurring peptide exenatide. This peptide is resistant todegradation by DPP-IV because of the substitution of gly-cine (G) at the second amino terminal position (hatchedarrow). It exhibits a biological profile similar to the endog-enous mammalian peptide, GLP-1. c, Structure of the syn-thetic GLP-1 analog liraglutide. This peptide is covalentlymodified with a C16 fatty acid chain via the addition of aglutamic acid (E) to the native lysine (K) as indicated by thearrowhead. The modified peptide binds noncovalently toalbumin. This hinders degradation by DPP-IV. Incretinbiological activity is preserved.
Table 2. Pharmacologic Agents Acting via the Incretin and Amylin Pathways
Agent Mechanism of action Major side effects Time to onset (h) Duration of action (h)Exenatide
(Byetta�)Incretin-mimetic, increases
insulin secretion onlywith hyperglycemia
Risk of hypoglycemia whengiven with asulfonylurea; delay ingastric emptying, nausea,anorexia
�0.25 6–12
Sitagliptin(Januvia�)
Inhibitor of DPP-IV Upper respiratoryinfections, headache
Peak at 1–4 h Half life approximately12
Pramlintide(Symlin�)
Amylin analog,suppresses postprandialglucagon secretion
Hypoglycemia when givenwith insulin, delay ingastric emptying, nausea
�0.25 2–4
DPP-IV � dipeptidyl pepidase IV.
Vol. 108, No. 6, June 2009 © 2009 International Anesthesia Research Society 1805

GLP-1.23 However, a substitution of glycine for ala-nine in its amino terminal protects exenatide fromdegradation by DPP-IV (Fig. 2b).11 Exenatide has acirculating half-life variously reported between 60 and90 min to 2.5 h, with plasma concentrations lasting 4 to6 h or more after a single subcutaneous dose. Elimi-nation is primarily through the renal system, althoughpatients with mild to moderate renal impairment donot exhibit significantly altered clearance.23
Exenatide is currently approved for the treatmentof type 2 DM patients receiving concurrent metforminor sulfonylurea therapy.23 It has no role in therapy ofpatients with DM type 1. Exenatide is given as asubcutaneous injection of 5 to 10 �g twice daily.Clinical trials show a significant reduction in hemo-globin A1c levels over 30 wk (absolute reduction ofapproximately 0.6%–0.9% from baseline hemoglobinA1c of 8.2%–8.7%) and a modest amount of weightloss (2 kg over 30 wk).24
The most common adverse events were GI symp-toms, including nausea and, rarely, vomiting ordiarrhea.25 Patients receiving both exenatide and asulfonylurea exhibit an increased risk for mild to mod-erate hypoglycemic events. However, the risk was notincreased in patients receiving concurrent treatmentwith exenatide and metformin.25 Approximately, 40% to50% of patients receiving exenatide develop low titers ofa weak affinity antibody. However, the antibody forma-tion has not been associated with decreased effectivenessof exenatide or other adverse reactions.11
A long-acting exenatide preparation is currentlyunder development, a polylactide-glycolide micro-sphere suspension containing 3% exenatide peptide.In diabetic rats, this preparation produced dose-dependent control of serum glucose for up to 28 daysafter a single injection.11
Liraglutide is another GLP-1 analog. With aminoacid substitutions at positions 34 and 26, and a co-valently linked C16 fatty-acid group, liraglutide formsnoncovalent bonds with albumin, which confers resis-tance to DPP-IV-mediated degradation (Fig. 2c).11 It isnot yet released in the United States for clinical use.Like exenatide, liraglutide is given as a subcutaneousinjection. It has a half-life of 10–14 h and consequentlycan be given as a once-daily injection. Clinical trialswith liraglutide demonstrated significant reductionsin postprandial glucose levels.11 Reduced hemoglobinA1c levels (absolute reduction of approximately 0.8%from baseline hemoglobin A1c) suggest improvedlong-term glucose control.25 Liraglutide also preventsweight gain or induces modest weight loss.11 The mostcommon adverse event is nausea, which is generallymild and decreases over time.
Sitagliptin is a DPP-IV inhibitor, now commer-cially available in the United States. The trade nameis Januvia�. Other DPP-IV inhibitors, includingvildagliptin, are in clinical trials and may soon beapproved for routine use.18 Sitagliptin enhancesinsulin secretion and decreases glucagon secretion
in a glucose-dependent matter. However, unlikeexenatide and liraglutide, sitagliptin does not affectgastric emptying.26 It has a half-life of 12 h and istaken orally as a once or twice daily medication.Clinical trials have shown a significant reduction inhemoglobin A1c levels associated with sitagliptintherapy (absolute reduction of 0.8% from baselinehemoglobin A1c of 5.8%–10.4% over 3 mo).26 Unliketherapy with exenatide, there was no significantweight change associated with sitagliptin. In earlyclinical trials, sitagliptin seemed to be well tolerated,without significant GI symptoms or hypoglycemicevents.26 However, given widespread expression ofDPP-IV in many cell types, and multiple potentialsubstrates for this peptidase,8 additional clinical stud-ies are needed to assess the long-term safety of DPP-IVinhibitors.18
BIOLOGY OF AMYLINAmylin, another GI hormone, has been identified as
a potential therapeutic target in DM (Fig. 3a).8,27
Pancreatic � cells, the same cells that manufacture andsecrete insulin, produce the amylin peptide hormone.Consequently, patients lacking functional pancreatic �cells (individuals with type 1 DM or advanced type 2DM) are deficient in both insulin and amylin.27 Similarto GLP-1, food intake stimulates amylin secretion. Its24-h profile resembles that of insulin, with low fastingblood levels and a robust increase in response tomeals. The glucose-decreasing effect of amylin seems
Figure 3. Structure of amylin and the synthetic analogpramlintide. a, Amino acid sequence of the naturally occur-ring peptide hormone. Arrowhead indicates the disulfidebridge between two cysteines. b, Structure of the syntheticamylin analog pramlintide. Substitution with proline at posi-tions 25, 28, and 29 of the native peptide (arrows) conferssolubility without disrupting biological activity. Arrowheadindicates the disulfide bridge between two cysteines.
1806 New Therapies for Diabetes Mellitus ANESTHESIA & ANALGESIA

to be independent of, and additive to, the effects ofinsulin.28
Like GLP-1, the actions of amylin include suppres-sion of glucagon secretion in a glucose-dependentmanner and delayed gastric emptying (Table 1); how-ever, the mechanism(s) of action remain incompletelydefined. Amylin is also a satiety agent, with receptorsin the area postrema of the hindbrain.28 By suppress-ing glucagon secretion and delaying gastric emptying,amylin slows the inflow of glucose into the circulation.At the same time, insulin stimulates cellular uptake ofglucose to reduce postprandial blood glucose levels.Effort has been made to treat patients with diabetesusing the native amylin peptide. However, endoge-nous amylin aggregates and forms insoluble masses ofamyloid. Consequently, synthetic modifications arenecessary to produce a soluble amylin analog suitablefor clinical use.
Specific AgentPramlintide is a synthetic amylin analog with pro-
line substitutions at amino acid positions 25, 28, and29 (Fig. 3b).27 These structural changes improve solu-bility. Pramlintide is used as an adjunct to insulin forboth type 1 and type 2 DM patients. It is given as asubcutaneous injection two or three times daily. Pram-lintide has an onset of approximately 20 min andduration of action of about 2 to 4 h. Clinical trialsdemonstrated significant improvement of postpran-dial glucose levels and hemoglobin A1c levels (abso-lute reduction of 0.67% at 13 wk and 0.39% at 52 wk)associated with pramlintide treatment.24 Pramlintideseems to decrease postprandial triglyceride excur-sions.29 The most common adverse reaction associatedwith pramlintide therapy is nausea, which improvesover the course of treatment. By itself, pramlintide hasnot been shown to cause an increased risk of hypogly-cemia; however, any concurrent insulin dose needs tobe adjusted to prevent hypoglycemia.27
THE ENDOCANNABINOID SYSTEMA comprehensive overview of the astonishingly
complex endocannabinoid signaling system is beyondthe scope of this article. Detailed reviews are avail-able.30 Briefly, the identification of specific bindingsites for plant products led to the identification of twoG protein-coupled receptors, labeled CB1 and CB2.The CB1 receptor is widespread throughout the brainand peripheral tissues, whereas the CB2 receptor has amore restricted distribution. These receptors seem touse several different signal transduction pathways,depending on how the receptor is activated and thetissue where it is expressed. The diverse distributionof the CB1 receptor, in particular, explains the exten-sive array of biological activities associated with itsactivation or blockade which include effects on appe-tite and ingestive behavior, addictive behaviors,sleep/awake cycles, peripheral energy metabolism,pain and inflammation.
The isolation of specific receptors for exogenousagonists suggested the existence of endogenous li-gands for the two cannabinoid receptors. Severalcandidate ligands have been identified. These includeanandamide, derived by enzymatic hydrolysis fromthe membrane lipid precursor N-arachidonoyl phos-phatidylethanolamide, and 2-arachidonoylglycerol de-rived from diacylglycerol. Of compelling interest forthe administration of anesthesia, there is evidence thatpropofol acts, at least in part, via activation of CB1receptors.31 This effect may be mediated by the inhi-bition of anandamide breakdown.32 Schelling et al.,33
however, provided evidence that the inhaled gen-eral anesthetic sevoflurane has different effects onanandamide levels than does propofol, suggestingagent-specific interactions with the endocannabi-noid system.
Specific DrugRimonabant was available until recently in many
countries (trade name: Acomplia), primarily as a treat-ment for obesity, with an added benefit of improvingglucose homeostasis beyond what might be expectedfrom weight loss alone.34,35 Clinical trials with rimon-abant (such as the Rimonabant in Obesity trial) dem-onstrated sustained weight loss and a reduction inwaist circumference. In addition, metabolic profilesimproved for triglyceride levels, lipoprotein choles-terol levels, and insulin resistance. Consequently, con-siderable interest developed in this drug for themanagement of metabolic syndrome.34,36 This drughas multiple pharmacologic effects37 and a long ter-minal elimination half-life in animals (approximately7 h). A prominent finding is that treatment withrimonabant is associated with neuropsychiatric sideeffects.38 Out of concern for an enhanced risk ofdepression and suicide,39 rimonabant was not ap-proved in the United States40 and it has recently beenwithdrawn in Europe for the original indication ofobesity.
ANESTHETIC CONSIDERATIONSA literature search via the National Library of
Medicine tool PubMed does not produce publishedexamples of adverse effects, drug-drug interactions orclinical conundrums attributable to exenatide, pram-lintide, a DPP IV inhibitor, or rimonabant in patientsundergoing anesthesia or surgery. These drugs haveonly recently appeared in clinical practice, and only asubset of all treated patients may have required ananesthetic since the drugs were approved and re-leased. Consequently, the number of clinical situationsin which a potential adverse effect emerges may be toofew for the manifestation of an uncommon reaction.
Alternatively, adverse effects may have occurred,but went undetected in complex clinical scenarios inwhich patients suffering from multiple co-morbidconditions received several medications concurrently.
Vol. 108, No. 6, June 2009 © 2009 International Anesthesia Research Society 1807

Moreover, untoward effects in anesthetized or surgi-cal patients attributable to one of these newly releaseddrugs simply may not have been reported. As clinicalexperience with these new drugs increases, it is pos-sible that recognizable patterns will develop. There-fore, at this time it is only possible to suggest potentialanesthesia concerns based on the known physiologyand pharmacology of the novel therapies.
Nausea is the most common adverse reaction asso-ciated with medications active along the incretin andamylin pathways. Clinical trials have shown nauseaoccurring in as many as 57% of patients treated withexenatide.41 The incidence of vomiting is less frequent.However, vomiting still occurs in approximately 17%of the patients receiving exenatide.41 Nausea is gener-ally mild to moderate, and most prevalent in the first8 wk of treatment. The frequency and intensity ofnausea generally declines thereafter. The risk of nau-sea is dose-dependent and can be decreased bygradual dose titration. However, adverse GI effectsassociated with exenatide are still the most commoncauses for patients to withdraw from clinical trials.41
Clinical studies with DPP-IV inhibitors, such assitagliptin, have reported no increased GI adversereactions. They are overall well tolerated with lowabsolute rates of adverse effects.26 This lack of GIadverse reactions may be secondary to the fact thatDPP-IV inhibitors only moderately increase the levelsof endogenous incretin hormones. In contrast, admin-istration of incretin analogs, such as exenatide, in-creases incretin hormone activity to a much greaterextent. Similar reasoning explains the finding that,while incretin analogs cause significant weight loss inpatients, DPP-IV inhibitors usually do not producesignificant weight changes.
Nausea is the most common adverse effect ofpramlintide, the amylin analog. Nausea occurs morefrequently in the type 1 DM patient than in the type 2DM patient.27 It is usually mild to moderate in inten-sity, occurring most frequently in the early stage oftreatment, and commonly attenuates over time. Theincidence of nausea is approximately 47% in type 1diabetics and 27% in type 2 diabetics.42 The risk ofnausea depends on the dose of pramlintide and can bedecreased by gradual dose titration.
Prominent antinausea effects of cannabinoids maybe mediated, at least in part, by CB1 receptors. Thishas led to occasional use of cannabinoids for patientsreceiving cancer chemotherapy.30 In a meta-analysis ofstudies on the use of rimonabant in smoking cessation,nausea was one of the adverse effects emerging fromthe pooled data from the early trials.43
Although there are no published reports of unusualpostoperative nausea and vomiting (PONV) attrib-uted to rimonabant or to drugs active along theincretin and amylin pathways, it seems reasonable toexpect that patients treated with these medicationsmay experience more frequent, or more severe, PONVthan the average patient. Consequently, for elective
surgery requiring anesthesia, at this time it seemslogical to withhold these medications in the immedi-ate perioperative period to reduce the likelihood orintensity of PONV. In situations of urgent or emer-gency surgery, without an opportunity to halt theadministration of these novel drugs, it is possible thatpatients will exhibit exaggerated or refractory postop-erative nausea. Future clinical studies may eventuallyprovide evidence-based recommendations.
Delaying gastric emptying is one of the mecha-nisms by which incretin peptides and amylin decreasepostprandial glucose levels.6 By impeding gastricemptying, glucose inflow into the circulation slows.Consequently, the incretins and amylin allow insulinmore time to stimulate glucose uptake and regulateserum glucose levels. Both exenatide and pramlintidecause delayed gastric emptying. DPP-IV inhibitors,such as sitagliptin, however, have little or no effect ongastric emptying,26 probably attributable to the mod-est increases in GLP-1 levels caused by this class ofdrugs. Gastroparesis is a feature of advanced diabetes,and medications that slow gastric emptying mayexacerbate this problem.44 Although no publishedreports document an increased risk of aspiration as-sociated with the new diabetes therapies, patientsreceiving these medications are theoretically at agreater risk for this complication during the perioper-ative period, especially those patients with peripheralneuropathy and gastroparesis as manifestations oftheir diabetes. In urgent or emergent situations wherethere has been no opportunity to withhold the medi-cations, clinicians may find unexpectedly large vol-umes of gastric contents removed by gastric suction.The administration of drugs promoting gut motility,such as metoclopramide, might factor more promi-nently in overall management of the patient unlessthere are specific contraindications.
Hypoglycemia is a potential adverse effect of medi-cations active along the incretin and amylin pathways,particularly if used in conjunction with an insulinpreparation or a sulfonylurea. Because incretinanalogs only promote insulin secretion in a“glucose-dependent” manner and because thecounter-regulatory release of glucagon secondary tohypoglycemia is preserved with incretins, the risk ofhypoglycemia should be low. Clinical trials show thatsevere hypoglycemia requiring medical interventionis rare with incretin analogs, such as exenatide. In 1trial, only 5 of 2781 patients treated with exenatidehad hypoglycemia requiring medical assistance.45 Allfive patients also received an insulin secretagogue,such as a sulfonylurea. No patients receiving bothexenatide and an insulin sensitizer, such as met-formin, developed hypoglycemia requiring medicalassistance.
When clinical trials are combined and reviewedunder meta-analysis, the overall incidence of hypogly-cemia associated with exenatide is approximately
1808 New Therapies for Diabetes Mellitus ANESTHESIA & ANALGESIA

16%.41 Hypoglycemia occurs especially when ex-enatide is co-administrated with a sulfonylurea. Thisrisk is comparable with the risk of hypoglycemia forpatients receiving insulin for treatment of diabetes.The likelihood of hypoglycemia is greatest during theinitial treatment period and declines over time. Whencompared with incretin analogs, DPP-IV inhibitorscarry less risk of hypoglycemia. In meta-analysis, onlyapproximately 1.6% of patients had episodes of mildto moderate hypoglycemia, which was not statisticallydifferent from the control group.41
Clinical trials with the amylin analog pramlintideshowed no increase in the overall event rates forsevere hypoglycemia.46 However, in patients also re-ceiving insulin for their diabetes, the rate of hypogly-cemia increased during the initial 4 wk of therapywith pramlintide.46 The enhanced risk of hypoglyce-mia was transient and diminished with appropriate bloodglucose monitoring and adjustments of insulin dose.
The half-lives and clinical effects of sitagliptin,exenatide, and pramlintide are relatively short. Fur-thermore, no clinical reports suggest that medicationsactive along the incretin or amylin pathways causehypoglycemia in the perioperative period. However,in the absence of definitive evidence, the theoreticalrisk of hypoglycemia is another reason to withholdthese medications in advance of elective surgery. Thiswould be a particularly pertinent consideration forpatients receiving both a sulfonylurea or an insulinpreparation and exenatide. Suppression of glucagonrelease by exenatide would be a mechanism contrib-uting to hypoglycemia. Should longer-acting GLP-1analogs, such as liraglutide, enter into clinical use, theglucose-decreasing effects might extend into the sur-gical or anesthesia interval. Anesthesia providersroutinely monitor the blood glucose levels of theirpatients. Perhaps, however, particular vigilance forthe possibility of hypoglycemia is warranted, espe-cially in urgent/emergent surgical situations in whichthere is no opportunity to withhold the medications.In theory, patients treated with long-acting insulinpreparations or sulfonylureas along with exenatidewould be most vulnerable. Clinicians might con-sider more frequent monitoring in urgent or emer-gent situations.
Hypoglycemia does not seem to be a likely conse-quence of rimonabant therapy.35
OTHER EFFECTSDPP-IV is a ubiquitous aminopepetidase with mul-
tiple natural substrates and it plays a role in theimmune system. Consequently, it seems plausible thatinhibiting DPP-IV can potentially cause adverse reac-tions. Clinical trials have shown that DPP-IV inhibi-tors were very well tolerated with low rates of adverseeffects. In meta-analysis, there is a small increased riskof nasopharyngitis and urinary tract infection associ-ated with DPP-IV inhibitors.41 Clinical experience in
anesthetized patients receiving DPP-IV inhibitors islimited. Because multiple peptides are potential sub-strates for this enzyme,18 clinicians should be alert forunusual reactions, especially in urgent procedures inwhich the drug may not have been withheld.
The endocannabinoid system is involved in manycomplex behaviors and physiologic responses, in-cluding pain and sleep/awake cycles. In preclinicalstudies, as cited above, there appear to be interac-tions between the endocannabinoid system andanesthetics. Given the “pleiotropic” effects ofrimonabant,37 the exact consequences of clinicalinteractions between drugs acting on cannabinoidreceptors in the brain and periphery with sedatives,narcotics, and inhaled or injected general anesthet-ics remain to be determined.
SUMMARY AND RECOMMENDATIONSFood ingestion increases secretion of insulin, amy-
lin, and the incretin peptides. Insulin and amylinregulate postprandial hyperglycemia, while amylinalso suppresses glucagon secretion and slows foodintake and gastric emptying. GLP-1 amplifies glucose-stimulated insulin release, in addition to suppressingglucagon secretion, food intake, and gastric emptying.The new treatment options for DM acting along theincretin pathway and the amylin analog offer somepotential advantages for chronic treatment of DM bytargeting these physiologic mechanisms. However,the biological activities of these drugs may presentchallenges in the perioperative period. This is espe-cially true in the urgent or emergent clinical circum-stances in which there are no opportunities towithhold these medications.
As clinical experience accumulates with noveldrugs in anesthetized patients, it may become pos-sible to develop more definitive warnings and rec-ommendations. However, until this informationbecomes available, we suggest withholding GLP-1analogs, DPP-IV inhibitors, and pramlintide on theday of surgery. Patients can probably continue totake these drugs the day before surgery without anenhanced risk of hypoglycemia while fasting.With these drugs, there are potentially enhancedrisks of nausea, aspiration of gastric contents, andhypoglycemia.
As the newer treatments for DM become increasinglyprevalent in clinical practice, anesthesia providersshould maintain particular vigilance for unusual orexaggerated effects and responses during the perioper-ative period.
ACKNOWLEDGMENTSWe thank Drs. Enrico Cagliero, Steven Russell, and Jean
Kwo of Massachusetts General Hospital for providinginsightful suggestions during the drafting of this article.
Vol. 108, No. 6, June 2009 © 2009 International Anesthesia Research Society 1809

REFERENCES
1. Peterfreund RA, Lee SL. Anesthesia considerations for endo-crine surgery and patients with endocrine conditions. In: Long-necker D Brown D, Newman M, Zapol W, eds. Anesthesiology.New York: McGraw-Hill, 2007:1420–49
2. McAnulty GR, Robertshaw HJ, Hall GM. Anaesthetic man-agement of patients with diabetes mellitus. Br J Anaesth2000;85:80 –90
3. Robertshaw HJ, McAnulty GR, Hall GH. Strategies for manag-ing the diabetic patient. Best Pract Res Clin Anaesthesiol2004;18:631–43
4. Rhodes ET, Ferrari LR, Wolfsdorf JI. Perioperative managementof pediatric surgical patients with diabetes mellitus. AnesthAnalg 2005;101:986–99
5. Nauck MA, Homberger E, Siegel EG, Allen RC, Eaton RP, EbertR, Creutzfeldt W. Incretin effects of increasing glucose loads inman calculated from venous insulin and C-peptide responses.J Clin Endocrinol Metab 1986;63:492–8
6. Maggs D, MacDonald I, Nauck MA. Glucose homeostasis andthe gastrointestinal tract: insights into the treatment of diabetes.Diabetes Obes Metab 2008;10:18–33
7. Fujioka K. Pathophysiology of type 2 diabetes and the role ofincretin hormones and beta-cell dysfunction. JAAPA 2007;Suppl:3–8
8. Combettes M, Kargar C. Newly approved and promising an-tidiabetic agents. Therapie 2007;62:293–310
9. Ranganath LR. Incretins: pathophysiological and therapeuticimplications of glucose-dependent insulinotropic polypeptideand glucagon-like peptide-1. J Clin Pathol 2008;61:401–9
10. Nauck MA, Heimesaat MM, Orskov C, Holst JJ, Ebert R,Creutzfeldt W. Preserved incretin activity of glucagon-likepeptide 1 [7–36 amide] but not of synthetic human gastricinhibitory polypeptide in patients with type-2 diabetes mellitus.J Clin Invest 1993;91:301–7
11. Drucker DJ, Nauck MA. The incretin system: glucagon-likepeptide-1 receptor agonists and dipeptidyl peptidase-4 inhibi-tors in type 2 diabetes. Lancet 2006;368:1696–705
12. Holst JJ. The physiology of glucagon-like peptide 1. Physiol Rev2007;87:1409–39
13. Drucker DJ. The biology of incretin hormones. Cell Metab2006;3:153–65
14. Li Y, Hansotia T, Yusta B, Ris F, Halban PA, Drucker DJ.Glucagon-like peptide-1 receptor signaling modulates beta cellapoptosis. J Biol Chem 2003;278:471–8
15. Nauck MA, Heimesaat MM, Behle K, Holst JJ, Nauck MS, RitzelR, Hufner M, Schmiegel WH. Effects of glucagon-like peptide 1on counterregulatory hormone responses, cognitive functions,and insulin secretion during hyperinsulinemic, stepped hypo-glycemic clamp experiments in healthy volunteers. J Clin Endo-crinol Metab 2002;87:1239–46
16. Mentlein R, Gallwitz B, Schmidt WE. Dipeptidyl-peptidaseIV hydrolyses gastric inhibitory polypeptide, glucagon-likepeptide-1(7–36)amide, peptide histidine methionine and is re-sponsible for their degradation in human serum. Eur J Biochem1993;214:829–35
17. Hansen L, Deacon CF, Orskov C, Holst JJ. Glucagon-likepeptide-1-(7–36)amide is transformed to glucagon-like peptide-1-(9–36)amide by dipeptidyl peptidase IV in the capillariessupplying the L cells of the porcine intestine. Endocrinology1999;140:5356–63
18. Chahal H, Chowdhury TA. Gliptins: a new class of oral hypo-glycaemic agent. QJM 2007;100:671–7
19. Mentlein R. Dipeptidyl-peptidase IV (CD26)–role in the inacti-vation of regulatory peptides. Regul Pept 1999;85:9–24
20. Callebaut C, Krust B, Jacotot E, Hovanessian AG. T cell activa-tion antigen, CD26, as a cofactor for entry of HIV in CD4� cells.Science 1993;262:2045–50
21. Tanaka T, Umeki K, Yamamoto I, Sakamoto F, Noguchi S,Ohtaki S. CD26 (dipeptidyl peptidase IV/DPP IV) as a novelmolecular marker for differentiated thyroid carcinoma. Int JCancer 1995;64:326–31
22. Nathan DM, Schreiber E, Fogel H, Mojsov S, Habener JF.Insulinotropic action of glucagonlike peptide-I-(7–37) in dia-betic and nondiabetic subjects. Diabetes Care 1992;15:270–6
23. Yoo BK, Triller DM, Yoo DJ. Exenatide: a new option for thetreatment of type 2 diabetes. Ann Pharmacother 2006;40:1777–84
24. Hoogwerf BJ. Exenatide and pramlintide: new glucose-loweringagents for treating diabetes mellitus. Cleve Clin J Med2006;73:477–84
25. Salehi M, D’Alessio DA. New therapies for type 2 diabetesbased on glucagon-like peptide 1. Cleve Clin J Med 2006;73:382–9
26. Idris I, Donnelly R. Dipeptidyl peptidase-IV inhibitors: a majornew class of oral antidiabetic drug. Diabetes Obes Metab2007;9:153–65
27. Kruger DF, Gloster MA. Pramlintide for the treatment ofinsulin-requiring diabetes mellitus: rationale and review ofclinical data. Drugs 2004;64:1419–32
28. Schmitz O, Brock B, Rungby J. Amylin agonists: a novelapproach in the treatment of diabetes. Diabetes 2004;53 Suppl3:S233–S238
29. Weyer C, Gottlieb A, Kim DD, Lutz K, Schwartz S, Gutierrez M,Wang Y, Ruggles JA, Kolterman OG, Maggs DG. Pramlintidereduces postprandial glucose excursions when added to regularinsulin or insulin lispro in subjects with type 1 diabetes: adose-timing study. Diabetes Care 2003;26:3074–9
30. Pacher P, Batkai S, Kunos G. The endocannabinoid system as anemerging target of pharmacotherapy. Pharmacol Rev 2006;58:389–462
31. Guindon J, LoVerme J, Piomelli D, Beaulieu P. The antinocicep-tive effects of local injections of propofol in rats are mediated inpart by cannabinoid CB1 and CB2 receptors. Anesth Analg2007;104:1563–9
32. Patel S, Wohlfeil ER, Rademacher DJ, Carrier EJ, Perry LJ,Kundu A, Falck JR, Nithipatikom K, Campbell WB, HillardCJ. The general anesthetic propofol increases brainN-arachidonylethanolamine (anandamide) content and inhibitsfatty acid amide hydrolase. Br J Pharmacol 2003;139:1005–13
33. Schelling G, Hauer D, Azad SC, Schmoelz M, Chouker A,Schmidt M, Hornuss C, Rippberger M, Briegel J, Thiel M,Vogeser M. Effects of general anesthesia on anandamide bloodlevels in humans. Anesthesiology 2006;104:273–7
34. Nogueiras R, Rohner-Jeanrenaud F, Woods SC, Tschop MH.The endocannabinoid system and the control of glucose ho-meostasis. J Neuroendocrinol 2008;20 Suppl 1:147–51
35. Scheen AJ. Cannabinoid-1 receptor antagonists in type-2 diabe-tes. Best Pract Res Clin Endocrinol Metab 2007;21:535–53
36. Jensen MD. What is the potential role of cannabinoid-1 receptorblockade in glucose and lipid management? Am J Med2007;120:S25–S31
37. Bifulco M, Grimaldi C, Gazzerro P, Pisanti S, Santoro A.Rimonabant: just an antiobesity drug? Current evidence on itspleiotropic effects. Mol Pharmacol 2007;71:1445–56
38. Christensen R, Kristensen PK, Bartels EM, Bliddal H, Astrup A.Efficacy and safety of the weight-loss drug rimonabant: ameta-analysis of randomised trials. Lancet 2007;370:1706–13
39. Rimonabant: suicide and depression. Depression and suicidaltendencies are about twice as frequent with rimonabant as withplacebo. Prescrire Int 2007;16:250
40. Traynor K. Panel advises against rimonabant approval. Am JHealth Syst Pharm 2007;64:1460–1
41. Amori RE, Lau J, Pittas AG. Efficacy and safety of incretintherapy in type 2 diabetes: systematic review and meta-analysis.JAMA 2007;298:194–206
42. Whitehouse F, Kruger DF, Fineman M, Shen L, Ruggles JA,Maggs DG, Weyer C, Kolterman OG. A randomized study andopen-label extension evaluating the long-term efficacy of pram-lintide as an adjunct to insulin therapy in type 1 diabetes.Diabetes Care 2002;25:724–30
43. Cahill K, Ussher M. Cannabinoid type 1 receptor antagonists(rimonabant) for smoking cessation. Cochrane Database SystRev 2007:CD005353
44. Cure P, Pileggi A, Alejandro R. Exenatide and rare adverseevents. N Engl J Med 2008;358:1969–70; discussion 71–2
45. Kendall DM, Riddle MC, Rosenstock J, Zhuang D, Kim DD,Fineman MS, Baron AD. Effects of exenatide (exendin-4) onglycemic control over 30 weeks in patients with type 2 diabetestreated with metformin and a sulfonylurea. Diabetes Care2005;28:1083–91
46. Hollander PA, Levy P, Fineman MS, Maggs DG, Shen LZ,Strobel SA, Weyer C, Kolterman OG. Pramlintide as an adjunctto insulin therapy improves long-term glycemic and weightcontrol in patients with type 2 diabetes: a 1-year randomizedcontrolled trial. Diabetes Care 2003;26:784–90
1810 New Therapies for Diabetes Mellitus ANESTHESIA & ANALGESIA

Anesthesiology 2005; 103:186–98 © 2005 American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc.
Practice Advisory for the Perioperative Management ofPatients with Cardiac Rhythm Management Devices:Pacemakers and Implantable Cardioverter–Defibrillators
A Report by the American Society of Anesthesiologists Task Force on PerioperativeManagement of Patients with Cardiac Rhythm Management Devices
PRACTICE advisories are systematically developed re-ports that are intended to assist decision making in areasof patient care. Advisories provide a synthesis and anal-ysis of expert opinion, clinical feasibility data, openforum commentary, and consensus surveys. Advisoriesare not intended as standards, guidelines, or absoluterequirements. They may be adopted, modified, or re-jected according to clinical needs and constraints.
The use of practice advisories cannot guarantee anyspecific outcome. Practice advisories summarize thestate of the literature and report opinions derived from asynthesis of task force members, expert consultants, openforums, and public commentary. Practice advisories are notsupported by scientific literature to the same degree asstandards or guidelines because of the lack of sufficientnumbers of adequately controlled studies. Practice adviso-ries are subject to periodic revision as warranted by theevolution of medical knowledge, technology, and practice.
Methodology
A. Definition of Cardiac Rhythm ManagementDevicesFor this Advisory, a cardiac rhythm management de-
vice (CRMD) refers to any permanently implanted car-diac pacemaker or any implantable cardioverter–defibril-lator (ICD). The term CRMD also refers to any cardiacresynchronization device. The term CRT refers to aCRMD that provides cardiac resynchronization therapyusing biventricular pacing techniques. Generic pace-maker and defibrillator codes are provided in appendix1. Note that every ICD includes both pacing and shocktherapies for the management of bradyarrhythmias andtachyarrhythmias.
B. Purposes of the AdvisoryThe purposes of this Advisory are to (1) facilitate safe
and effective perioperative management of the patientwith a CRMD and (2) reduce the incidence of adverseoutcomes. Perioperative management refers to the pre-operative, intraoperative, postoperative or recovery pe-riod in any setting where an anesthesia provider deliversanesthesia care. Adverse outcomes associated with aCRMD include (but are not limited to) damage to thedevice, inability of the device to deliver pacing orshocks, lead–tissue interface damage, changes in pacingbehavior, electrical reset to the backup pacing mode, orinappropriate ICD therapies.* Adverse clinical outcomesinclude (but are not limited to) hypotension, tachyarrhyth-mia or bradyarrhythmia, myocardial tissue damage, andmyocardial ischemia or infarction. Other related outcomesmay include extended hospital stay, delay or cancellation ofsurgery, readmission to manage device malfunction, oradditional hospital resource utilization and cost.
C. FocusThis Advisory focuses on the perioperative manage-
ment of patients who have a preexisting, permanentlyimplanted CRMD for treatment of bradyarrhythmia,tachyarrhythmia, or heart failure. Both inpatient andoutpatient procedures are addressed by this Advisory.This Advisory does not address the perioperative man-agement of any patient undergoing CRMD implantationor revision. It is not applicable to any patient (1) without
Additional material related to this article can be found on theANESTHESIOLOGY Web site. Go to http://www.anesthesiology.org, click on Enhancements Index, and then scroll down tofind the appropriate article and link. Supplementary materialcan also be accessed on the Web by clicking on the “Arti-clePlus” link either in the Table of Contents or in the HTMLversion of the article.
�
Developed by the American Society of Anesthesiologists Task Force on Peri-operative Management of Patients with Cardiac Rhythm Management Devices:James R. Zaidan, M.D., M.B.A. (Chair), Atlanta, Georgia; John L. Atlee, M.D.,Milwaukee, Wisconsin; Peter Belott, M.D., El Cajon, California; Kurt S. Briesa-cher, M.D., Atlanta, Georgia; Richard T. Connis, Ph.D., Woodinville, Washington;John D. Gallagher, M.D., Lebanon, New Hampshire; David Hayes, M.D., Roches-ter, Minnesota; Jane E. Hershey, M.D., Highland, Maryland; Neal Kay, M.D.,Birmingham, Alabama; David G. Nickinovich, Ph.D., Bellevue, Washington; MarcA. Rozner, Ph.D., M.D., Houston, Texas; Mark F. Trankina, M.D., Birmingham,Alabama. Submitted for publication December 28, 2004. Accepted for publica-tion December 28, 2004. Supported by the American Society of Anesthesiologistsunder the direction of James F. Arens, M.D., Chair, Committee on PracticeParameters. Approved by the House of Delegates on October 27, 2004. A list ofthe references used to develop this Advisory is available by writing to theAmerican Society of Anesthesiologists. This Advisory is endorsed by the Ameri-can Heart Association, the Heart Rhythm Society, and the Society of Cardiovas-cular Anesthesiologists.
Address reprint requests to the American Society of Anesthesiologists: 520 N.Northwest Highway, Park Ridge, Illinois 60068-2573. This Practice Advisory, aswell as all published ASA Practice Parameters, may be obtained at no costthrough the Journal Web site, www.anesthesiology.org.
* Inappropriate ICD therapy refers to the delivery of antitachycardia therapy(paced or shock) in the absence of a clinically indicated tachyarrhythmia. Inap-propriate ICD therapy can harm a patient by inducing ischemia, worsening thearrhythmia, or causing the patient to move during a delicate procedure.
Anesthesiology, V 103, No 1, Jul 2005 186

a permanently implanted pacemaker or ICD, (2) with atemporary CRMD, (3) with a noncardiac implantabledevice (e.g., neurologic or spinal cord stimulator), or (4)with an implantable mechanical cardiac assist device(e.g., ventricular assist device). This Advisory does notaddress any procedure where there are no known peri-operative CRMD concerns, such as diagnostic radiation(e.g., x-ray studies, fluoroscopy, or mammograms), com-puted tomography scans, or ultrasound.
D. ApplicationThis Advisory is intended for use by anesthesiologists
and all other individuals who deliver or who are respon-sible for anesthesia care. The Advisory may also serve asa resource for other physicians and healthcare profes-sionals who treat patients with CRMDs.
E. Task Force Members and ConsultantsThe American Society of Anesthesiologists (ASA) ap-
pointed a Task Force of 12 members to (1) review andassess currently available scientific literature, (2) obtainexpert consensus and public opinion, and (3) develop apractice advisory. The Task Force members consisted ofanesthesiologists and cardiologists in private and aca-demic practices from various geographic areas of theUnited States and two methodologists from the ASACommittee on Practice Parameters.
The Task Force used a six-step process. First, theyreached consensus on the criteria for evidence of effec-tive perioperative management of cardiac rhythm man-agement devices. Second, original published articlesfrom peer-reviewed journals relevant to these issueswere evaluated. Third, consultants who had expertise orinterest in CRMDs and who practiced or worked invarious settings (e.g., academic and private practice)were asked to (1) participate in opinion surveys on theeffectiveness of various perioperative management strat-egies and (2) review and comment on a draft of theAdvisory developed by the Task Force. Fourth, additionalopinions were solicited from random samples of activemembers of both the ASA and the Heart Rhythm Society(HRS).† Fifth, the Task Force held an open forum at anational anesthesia meeting and at a major cardiology meet-ing to solicit input on the key concepts of this Advisory.Sixth, all available information was used to build consensuswithin the Task Force on the Advisory.
The draft document was made available for review on theASA Web site, and input was invited via e-mail announce-ment to all ASA members. All submitted comments wereconsidered by the Task Force in preparing the final draft.
F. Availability and Strength of EvidencePractice advisories are developed by a protocol similar
to that of an ASA evidence-based practice guideline,including a systematic search and evaluation of the liter-ature. However, practice advisories lack the support of asufficient number of adequately controlled studies topermit aggregate analyses of data with rigorous statisticaltechniques such as meta-analysis. Nonetheless, litera-ture-based evidence from case reports and other descrip-tive studies is reported. This literature often permits theidentification of recurring patterns of clinical practice.
As with a practice guideline, formal survey informationwas collected from Consultants and members of the ASA.For this Advisory, surveys were also sent to members of theHRS. Additional information was obtained from open fo-rum presentations and other invited and public sources.The advisory statements contained in this document rep-resent a consensus of the current spectrum of clinicalopinion and literature-based findings.‡
Advisories
I. Preoperative EvaluationPerioperative treatment of CRMD patients is a com-
mon occurrence. It has been reported that more than500,000 individuals in the United States have perma-nently implanted pacemakers or ICDs with 115,000 newdevices implanted each year.1 Perioperative manage-ment of CRMD patients typically begins with a focusedpreoperative evaluation consisting of (1) establishingwhether a patient has a CRMD, (2) defining the type ofdevice, (3) determining whether a patient is CRMD de-pendent for antibradycardia pacing function, and (4)determining device function.
Although no controlled trials of the clinical impact ofperforming a focused preoperative evaluation for CRMDpatients were found, case reports suggest that incom-plete preoperative examination of patients with CRMDsmay lead to adverse outcomes (e.g., inhibited CRMDfunction, asystole).2–4 The majority of Consultants andrandom samples from the ASA and HRS membershipsagree that the above four preoperative evaluation activ-ities should be conducted.§
Advisory. The consensus of the Task Force is that afocused preoperative evaluation should include establish-ing whether a patient has a CRMD, defining the type ofdevice, determining whether a patient is CRMD dependentfor pacemaking function, and determining CRMD function.
Determining whether a patient has a CRMD should bebased on (1) a focused history including but not limitedto the patient interview, medical records review, reviewof available chest x-ray films, electrocardiogram, or anyavailable monitor or rhythm strip information and (2) afocused physical examination (checking for scars, pal-pating for device).
† Formerly North American Society of Pacing and Electrophysiology (NASPE).
‡ Refer to appendix 2 for a summary of the advisories.
§ Refer to appendix 3 for results of the Consultant, ASA membership, and HRSmembership surveys.
187PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

Defining the type of device is accomplished by (1)obtaining the manufacturer’s identification card from thepatient or other source, (2) ordering chest x-ray studies ifno other data are available,� or (3) referring to supplemen-tal resources (e.g., manufacturer’s databases, pacemakerclinic records, consultation with a cardiologist).
Cardiac rhythm management device dependency forpacemaking function may be determined by one or moreof the following: (1) a verbal history or an indication inthe medical record that the patient has experienced abradyarrhythmia that has caused syncope or other symp-toms requiring CRMD implantation, (2) a history of suc-cessful atrioventricular nodal ablation that resulted inCRMD placement, or (3) a CRMD evaluation that showsno evidence of spontaneous ventricular activity whenthe pacemaking function of the CRMD is programmed toVVI pacing mode at the lowest programmable rate.
Cardiac rhythm management device function is ideallyassessed by a comprehensive evaluation of the device.5
If a comprehensive evaluation is not possible, then, at aminimum, confirm whether pacing impulses arepresent and create a paced beat. Consultation with acardiologist or CRMD service may be necessary. Contact-ing the manufacturer for perioperative recommenda-tions may be a consideration.
II. Preoperative PreparationPreparation for patient safety and proper maintenance
of the device during a procedure includes (1) determin-ing whether electromagnetic interference (EMI) is likelyto occur during the planned procedure; (2) determiningwhether reprogramming the CRMD pacemaking func-tion to an asynchronous pacing mode or disabling anyspecial algorithms, including rate adaptive functions, isneeded; (3) suspending antitachyarrhythmia functions ifpresent; (4) advising the individual performing the proce-dure to consider use of a bipolar electrocautery system orultrasonic (harmonic) scalpel to minimize potential adverseeffects of EMI on the pulse generator or leads; (5) assuringthe availability of temporary pacing and defibrillationequipment; and (6) evaluating the possible effects of anes-
thetic techniques on CRMD function and patient–CRMDinteractions.
Numerous descriptive studies and case reports suggestthat the following procedures are likely to be associatedwith EMI: (1) electrocautery,6–11 (2) radio frequencyablation,12–20 (3) magnetic resonance imaging (MRI),21–31
and (4) radiation therapy.32–34 No studies were found thatreported EMI during electroconvulsive therapy (ECT).Some descriptive studies report the occurrence of EMIduring lithotripsy,35,36 whereas other descriptive studiesand case reports indicate no apparent EMI effects.37–39 Nocontrolled trials of the clinical impact of programming thepacemaking function to an asynchronous mode for a pro-cedure were found. Although some case reports suggestthat such reprogramming is beneficial during electrocau-tery,40–42 other reports indicate that EMI may continue toaffect reprogrammed pacemakers.43,44 The literature lackssufficient guidance regarding the potential perioperativeimpact of anesthetic techniques on CRMD function. Themajority of Consultants as well as the samples of ASA andHRS members agree that it should be determined whetherEMI is likely to occur before a planned procedure. Themajority of Consultants agree that a CRMD’s rate-adaptivetherapy should be turned off before a procedure, whereasthe ASA and HRS members are equivocal. The majority ofConsultants and HRS members disagree that all patients’CRMDs should be programmed to an asynchronous modebefore surgery, whereas the ASA members are equivocal. Inaddition, the majority of Consultants and HRS membersagree that pacemaker-dependent patients’ CRMDs shouldbe programmed to an asynchronous mode before surgery,whereas the ASA members are again equivocal. The major-ity of Consultants and ASA and HRS members agree that (1)suspending antitachyarrhythmia functions if present, (2)advising the individual performing the procedure to con-sider use of a bipolar electrocautery system to minimizepotential adverse effects of EMI on the pulse generator orleads, (3) assuring the availability of temporary pacing anddefibrillation equipment, and (4) evaluating the possibleeffects of anesthetic techniques on CRMD function andpatient–CRMD interactions are important steps in promot-ing patient safety and successfully treating patients withCRMDs. The Consultants and ASA members agree and theHRS members are equivocal regarding the consideration ofusing an ultrasonic scalpel.
Advisory. The Task Force agrees that planned proce-dures should include a determination as to whether EMI islikely to occur for either conventional pacemakers or ICDs.
If EMI is likely to occur, the conventional pacing func-tion of a CRMD should be altered by changing to anasynchronous pacing mode# in pacemaker-dependentpatients and suspending special algorithms, includingrate-adaptive functions. These alterations may be accom-plished by programming or applying a magnet whenapplicable.** However, the Task Force cautions againstthe use of the magnet over an ICD.†† In addition, an
� Most current CRMDs have an x-ray code that can be used to identify themanufacturer of the device.
# The VVT mode (with attention to the upper rate limit) might also beconsidered for a patient with ventricular ectopy where concern exists regardingR-on-T pacing during an asynchronous pacing mode. However, the upper pacingrate during VVT mode is manufacturer- and possibly generator-specific and canapproach 200 beats/min for many devices. Generally, VVT mode pacing wouldnot be a consideration except in very rare circumstances. Before using the VVTmode, a cardiologist and the generator manufacturer should be consulted todetermine the suitability of the upper pacing rate for any patient.
** A magnet correctly applied to a pacemaker often results in asynchronouspacemaker function at a predetermined rate without rate responsiveness. Themagnet rate and response varies by manufacturer. Magnet response can beaffected by programming and remaining battery life. The magnet rate may beexcessive for some patients. Some pacemakers may have no magnet response.
†† Magnet application to an ICD rarely alters bradycardia pacing rate andfunction. A magnet correctly applied to an ICD often results in suspension oftachyarrhythmia therapy. For most ICDs, there is no reliable means to detectappropriate magnet placement. Some ICDs may have no magnet response. SomeICDs can be permanently disabled by magnet application.
188 PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

ICD’s antitachyarrhythmia functions should be sus-pended, if present. For ICD patients who depend onpacing function for control of bradyarrhythmia, thesefunctions should be altered by programming as notedabove. Consultation with a cardiologist or pacemaker–ICD service may be necessary.
For all CRMDs, consider advising the individual per-forming the procedure to use a bipolar electrocauterysystem or an ultrasonic scalpel when applicable. Tem-porary pacing and defibrillation equipment should beimmediately available before, during, and after aprocedure.
Finally, the Task Force believes that anesthetic tech-niques do not influence CRMD function. However, an-esthetic-induced physiologic changes (i.e., cardiac rate,rhythm, or ischemia) in the patient may induce unex-pected CRMD responses or adversely affect the CRMD–patient interaction.
III. Intraoperative ManagementThe primary activities associated with intraoperative
management of a CRMD include (1) monitoring theoperation of the device; (2) preventing potential CRMDdysfunction; and (3) performing emergency defibrilla-tion, cardioversion, or heart rate support.
1. Monitoring. Intraoperative monitoring includescontinuous electrocardiography as well as monitoring ofthe peripheral pulse (e.g., palpation of the pulse, auscul-tation of heart sounds, monitoring of a tracing of intraar-terial pressure, ultrasound peripheral pulse monitoring,or pulse plethysmography or oximetry).45 Although nocontrolled trials were found that examine the clinicalimpact of electrocardiography or peripheral pulse mon-itoring for CRMD patients, case reports note the impor-tance of intraoperative electrocardiographic monitoringin the detection of pacemaker or cardiac dysfunction forthese patients.4,46–50 The majority of Consultants andASA and HRS members agree that (1) continuous elec-trocardiographic monitoring should be done for allCRMD patients and (2) continuous peripheral pulsemonitoring should be conducted.
Advisory. Electrocardiography and peripheral pulsemonitoring are important components of perioperativetreatment of patients with CRMDs. The Task Forceagrees that a patient’s electrocardiogram should be con-tinuously displayed, as required by ASA standards, fromthe beginning of anesthesia until the patient is trans-ferred out of the anesthetizing location, with additionalelectrocardiographic monitoring in the postoperativeperiod as indicated by the patient’s medical condi-tion.45,51 The Task Force believes that these standards
should apply to all CRMD patients receiving general orregional anesthesia, sedation, or monitored anesthesiacare. Continuous peripheral pulse monitoring should beperformed for all CRMD patients receiving general orregional anesthesia, sedation, or monitored anesthesiacare. If unanticipated device interactions are found, con-sider discontinuation of the procedure until the sourceof interference can be eliminated or managed.
2. Managing Potential Sources of EMI. Proceduresusing electrocautery, radiofrequency ablation, litho-tripsy, MRI, or radiation therapy may damage CRMDs orinterfere with CRMD function, potentially resulting insevere adverse outcomes. Sources of EMI are oftenunique to specific procedures, and the management ofeach of these potential EMI sources is reported sepa-rately below.
A. Electrocautery. Management of potential sources ofEMI associated with electrocautery includes (1) assuringthat the cautery tool and current return pad‡‡ are posi-tioned so that the current pathway does not passthrough or near the CRMD pulse generator and leads; (2)avoiding proximity of the cautery’s electrical field to thepulse generator or leads; (3) using short, intermittent,and irregular bursts at the lowest feasible energy levels;and (4) using a bipolar electrocautery system or an ul-trasonic (harmonic) scalpel, if possible.
Two case reports52,53 and one observational study54
suggest that EMI may occur despite positioning the cur-rent return pad as far as possible away from the gener-ator and leads. However, the majority of Consultants andASA and HRS members agree that the current return padshould be positioned so that the electrosurgical currentpathway does not pass through or near the CRMD pulsegenerator or leads.
One case report suggested that application of unipolarelectrocautery on the sternum resulted in completepacemaker inhibition.55 Although some manufacturerssuggest substituting bipolar for monopolar electrocau-tery to minimize CRMD interactions, no clinical litera-ture was found to support this recommendation. Themajority of Consultants and ASA and HRS members agreethat direct contact between the electrocautery systemand the CRMD pulse generator or its leads should beavoided.
Although no recent studies were found examining thebenefit of using short, intermittent bursts at the lowestfeasible energy levels, earlier literature§§ suggests thatshort, intermittent bursts may be useful in completingprocedures without no1table EMI interference.56–60 Themajority of Consultants and ASA and HRS members agreethat short, intermittent bursts should be performed.
Finally, case reports suggest that surgery for pace-maker patients may proceed uneventfully when bipolarelectrocautery systems42,43,46 or harmonic scalpels61,62 areused. The majority of Consultants and ASA and HRS mem-bers agree that bipolar electrocautery systems should be
‡‡ Although commonly referred to as the “grounding pad,” most operatingroom power supplies in the United States are ungrounded.
§§ See appendix 3 for an explanation of the term earlier literature.
189PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

used when possible. The majority of Consultants and ASAmembers agree that harmonic scalpels should be usedwhen possible, and HRS members are equivocal.
B. Radiofrequency Ablation. Management of potentialsources of EMI associated with radiofrequency ablationprimarily involves keeping the radiofrequency currentpath (electrode tip to current return pad) as far awayfrom the pulse generator and lead system as possible.One observational study reports 3 of 12 cases that re-sulted in a significant decrease in resistance on the pace-maker leads when radiofrequency ablation was used inproximity to the leads.63 One case report suggests thatpositioning of the radiofrequency ablation cluster elec-trode no closer than 5 cm from the pacer leads allowedthe procedure to continue uneventfully.40 The majorityof Consultants and ASA and HRS members agree that theindividual performing the procedure should avoid directcontact between the ablation catheter and the CRMDand leads and should keep the radiofrequency ablationcurrent path as far away from the pulse generator andlead system as possible.
C. Lithotripsy. Management of potential sources of EMIassociated with lithotripsy includes (1) avoiding focus ofthe lithotripsy beam near the pulse generator and (2)disabling atrial pacing if the lithotripsy system triggerson the R wave. The literature is silent regarding thebenefits of focusing the lithotripsy beam away from thepulse generator as well as the benefits of disabling atrialpacing during lithotripsy. The majority of Consultantsand ASA and HRS members agree that focusing the lith-otripsy beam near the pulse generator should beavoided, and all three groups are equivocal regardingwhether atrial pacing should be disabled before a pro-cedure if the lithotripsy system triggers on the R wave.
D. Magnetic Resonance Imaging. The literature is notsufficiently rigorous to examine the effects of specificmanagement activities related to CRMD patients receiv-ing MRI. Some descriptive studies and case reports sug-gest that MRI may be completed without notable EMIunder specific circumstances and with appropriate pa-tient qualification and monitoring.30,31,64–71 However,other literature generally suggests that MRI is contrain-dicated.21–29 The majority of Consultants and ASA andHRS members generally agree that MRI is contraindi-cated for all CRMD patients.
E. Radiation Therapy. The literature does not providesufficient guidance regarding specific management activ-ities related to CRMD patients undergoing radiation ther-apy. However, none of the Consultants or HRS membersand only 10% of the ASA members agree that radiation
therapy is contraindicated for all CRMD patients. Fifty-seven percent of the Consultants, 59% of the HRS mem-bers, and 37% of the ASA members agree that radiationtherapy is contraindicated for some but not all CRMDpatients, whereas 43% of the Consultants, 41% of theHRS members, and 53% of the ASA members agree thatradiation therapy is not contraindicated for any CRMDpatient.
F. Electroconvulsive Therapy. No clinical studies werefound that report EMI effects or permanent CRMD mal-function associated with ECT. One study reports twocases where patients’ ICDs were turned off before ECTbut does not report the effect of the therapy on ICDfunction.72 However, the author indicates that treatmentwith ECT might be associated with significant cardiacrisks. Transient electrocardiographic changes (e.g., in-creased P-wave amplitude, altered QRS shape, T-waveand ST-T abnormalities) may result from ECT, and addi-tional cardiac complications (e.g., arrhythmia or isch-emia) may occur in patients with preexisting cardiacdisease. Finally, physiologic stresses after ECT, such as aperiod of bradycardia and reduced blood pressure, fol-lowed by tachycardia and an increase in blood pressure,may account for cardiac failure in the extended postop-erative period (i.e., several hours or days after ECT)among patients with marginal cardiac function.
Advisory. The Task Force believes that EMI could beminimized during certain procedures using a variety ofintraoperative management techniques.
The Task Force agrees that the risk of intraoperativeinterference from electrocautery systems may be mini-mized by (1) positioning the cautery tool and currentreturn pad so that the current pathway does not passthrough or near the CRMD system� �; (2) avoiding prox-imity of the cautery’s electrical field to the pulse gener-ator and leads, including avoidance of waving the acti-vated electrode over the generator##; (3) using short,intermittent, and irregular bursts at the lowest feasibleenergy levels; and (4) using bipolar electrocautery sys-tems or ultrasonic (harmonic) scalpels if possible. Advis-ing or reminding the individual performing the proce-dure to implement these management techniquesshould be considered.
Risk of interference from radiofrequency ablation maybe reduced by avoiding direct contact between the ab-lation catheter and the pulse generator and leads and bykeeping the radiofrequency’s current path (electrode tipto current return pad) as far away from the pulse generatorand leads as possible. During all radiofrequency ablativeprocedures, consider discussing with the individual per-forming the procedure any concerns regarding the prox-imity of the ablation catheter to the CRMD leads.
During lithotripsy, the lithotripsy beam should not befocused near the pulse generator. If the lithotripsy sys-tem triggers on the R wave, atrial pacing might need tobe disabled before the procedure.
� � For some cases, the electrosurgical receiving plate will need to be placedon a site different from the thigh. For example, in head and neck cases, thereceiving plate can be placed on the posterior superior aspect of the shouldercontralateral to the generator position.
## An inhibitory effect could occur even when the active electrode of theelectrocautery is not touching the patient.
190 PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

The Task Force believes that MRI is generally contra-indicated for CRMD patients. If MRI must be performed,consult with the ordering physician, the patient’s pace-maker specialist or cardiologist, the diagnostic radiolo-gist, and the CRMD manufacturer.
The Task Force believes that radiation therapy can besafely performed for CRMD patients.*** The device mustbe outside the field of radiation. Therefore, some pulsegenerators will require surgical relocation before com-mencing radiation. Most manufacturers recommend ver-ification of pulse generator function during and at thecompletion of radiation. Problems may include pace-maker failure and runaway pacemaker.†††
Although transient or long-term myocardial and ner-vous system effects may be associated with ECT, theTask Force believes that such therapies may be admin-istered to CRMD patients without significant damage toa disabled CRMD. If ECT must be performed, consultwith the ordering physician and the patient’s cardiolo-gist to plan for the first and subsequent ECTs. All CRMDsshould undergo a comprehensive interrogation beforethe procedure(s). ICD functions should be disabled forshock therapy during ECT; however, be prepared totreat ventricular arrhythmias that occur secondary to thehemodynamic effects of ECT. CRMD-dependent patientsmay require a temporary pacing system to preserve car-diac rate and rhythm during shock therapy. Also, theCRMD may require programming to asynchronous activ-ity to avoid myopotential inhibition of the device inpacemaker-dependent patients.
3. Emergency Defibrillation or Cardioversion.During the perioperative period, emergency defibrilla-tion or cardioversion may become necessary for a CRMDpatient. In this case, the primary concern is to minimizethe current flowing through the pulse generator and leadsystem. Recent and earlier case reports suggest thatoptimal positioning of the defibrillation or cardioversionpads or paddles may be an important factor in the pre-vention of adverse CRMD-related outcomes.73–77 Themajority of Consultants and ASA and HRS members agreethat the defibrillation or cardioversion pads should bepositioned as far as possible from the pulse generator.The majority of Consultants and ASA and HRS membersalso agree that the anterior–posterior position should beused and that a clinically appropriate energy outputshould be used regardless of the type of CRMD.
Advisory. The Task Force believes that before at-tempting emergency defibrillation or cardioversion of apatient with an ICD and magnet-disabled therapies, all
sources of EMI should be terminated, and the magnetshould be removed to reenable antitachycardia therapies.The patient should then be observed for appropriateCRMD therapy. For patients with an ICD and antiarrhyth-mic therapies that have been disabled by programming,consider reenabling therapies through programming. If theabove activities do not restore ICD function, proceed withemergency external defibrillation or cardioversion.
Overriding the above discussion is the need to followexisting Advanced Cardiac Life Support and emergencyguidelines78 to provide rapid cardioversion or defibrilla-tion, and attention should be turned to providing thistherapy as quickly as possible.
If a life-threatening arrhythmia occurs, follow Ad-vanced Cardiac Life Support guidelines for energy leveland for paddle placement. If possible, attempt to mini-mize the current flowing through the pulse generatorand lead system by (1) positioning the defibrillation orcardioversion pads or paddles as far as possible from thepulse generator and (2) positioning defibrillation or car-dioversion pads or paddles perpendicular to the majoraxis of the CRMD pulse generator and leads to the extentpossible by placing them in an anterior–posterior loca-tion. A clinically appropriate energy output should al-ways be used regardless of the presence of a CRMD, andthe paddles should be positioned as best as can be donein an emergency.
IV. Postoperative ManagementPostoperative treatment of CRMD patients primarily
consists of interrogating and restoring CRMD function.Although no recent studies were found examining out-comes associated with interrogating or restoring CRMDfunction, an earlier case report indicates that postoper-ative evaluation resulted in the discovery and correctionof a pacemaker problem.79 The majority of Consultantsand ASA and HRS members agree that postoperativepatient treatment should include interrogating and re-storing CRMD function in the postanesthesia care unit orintensive care unit.
Advisory. The Task Force believes that cardiac rateand rhythm should be continuously monitored through-out the immediate postoperative period. Backup pacingcapability and cardioversion–defibrillation equipmentshould be immediately available at all times.
Postoperative interrogation and restoration of CRMDfunction are basic elements of postoperative manage-ment. The CRMD first should be interrogated to assesspostoperative device functions. If interrogation deter-mines that CRMD settings are inappropriate, the deviceshould be reprogrammed to appropriate settings. For anICD, all antitachyarrhythmic therapies should be re-stored. Consultation with a cardiologist or pacemaker–ICD service may be necessary.
*** Radiation shielding may not be feasible for some patients because of thesize and weight of the shield. This may be compensated for by relocating thegenerator.
††† Runaway pacemaker is a potentially catastrophic pulse generator mal-function characterized by the sudden onset of rapid, erratic pacing. Runawaypacemaker is the result of multiple internal component failure, and it is relativelyuncommon in modern devices. Circuitry in modern pacemakers (and ICDs)limits the runaway pacing rate to less than 210 beats/min.
191PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

Appendix 1: Generic Pacemaker andDefibrillator Codes
The generic pacemaker and defibrillator codes were developed asjoint projects by the North American Society of Pacing and Electro-
physiology (NASPE)‡‡‡ and the British Pacing and ElectrophysiologyGroup (BPEG).80,81 The five positions refer to the order of the pro-grammed settings on the CRMD (tables 1 and 2).
Table 1. Generic Pacemaker Code (NBG*): NASPE/BPEG Revised (2002)
Position I, PacingChamber(s)
Position II, SensingChamber(s)
Position III, Response(s) toSensing
Position IV,Programmability
Position V, MultisitePacing
O � none O � none O � none O � none O � noneA � atrium A � atrium I � inhibited R � rate modulation A � atriumV � ventricle V � ventricle T � triggered V � ventricleD � dual (A � V) D � dual (A � V) D � dual (T � I) D � dual (A � V)
Examples:
AAI � Atrial-only antibradycardia pacing. In the AAI mode, any failure of the atrium to produce an intrinsic event within the appropriate time window (determined by the lowerrate limit) results in an atrial pacing pulse emission. There is no ventricular sensing; thus, a premature ventricular event will not likely reset the pacing timer.
AOO � Asynchronous atrial-only pacing. In this mode, the pacing device emits a pacing pulse regardless of the underlying cardiac rhythm.
DDD � Dual-chamber antibradycardia pacing function in which every atrial event, within programmed limits, is followed by a ventricular event. The DDD modeimplies dual-chamber pacing with atrial tracking. In the absence of intrinsic activity in the atrium, it will be paced, and, after any sensed or paced atrialevent, an intrinsic ventricular event must occur before the expiration of the atrioventricular timer or the ventricle will be paced.
DDI � Dual-chamber behavior in which the atrial activity is tracked into the ventricle only when the atrial event is created by the antibradycardia pacing functionof the generator. In the DDI mode, the ventricle is paced only when no intrinsic ventricular activity is present.
DOO � Asynchronous atrioventricular sequential pacing without regard to the underlying cardiac rhythm.
VOO � Asynchronous ventricular-only pacing without regard to the underlying cardiac rhythm.
VVI � Ventricular-only antibradycardia pacing. In the VVI mode, any failure of the ventricle to produce an intrinsic event within the appropriate time window(determined by the lower rate limit) results in a ventricular pacing pulse emission. There is no atrial sensing; thus, there can be no atrioventricular synchronyin a patient with a VVI pacemaker and any intrinsic atrial activity.
* NBG: N refers to NASPE, B refers to BPEG, and G refers to generic.
Table 2. Generic Defibrillator Code (NBD): NASPE/BPEG
Position I, ShockChamber(s)
Position II,Antitachycardia
Pacing Chamber(s)Position III,
Tachycardia Detection
Position IV,*Antibradycardia
Pacing Chamber(s)
O � none O � none E � electrogram O � noneA � atrium A � atrium H � hemodynamic A � atriumV � ventricle V � ventricle V � ventricleD � dual (A � V) D � dual (A � V) D � dual (A � V)
* For robust identification, position IV is expanded into its complete NBG code. For example, a biventricular pacing–defibrillator with ventricular shock andantitachycardia pacing functionality would be identified as VVE-DDDRV, assuming that the pacing section was programmed DDDRV. Currently, no hemodynamicsensors have been approved for tachycardia detection (position III).
‡‡‡ Now called the Heart Rhythm Society (HRS).
192 PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

Appendix 2: Summary of Practice Advisory
Preoperative Evaluation● Establish whether a patient has a CRMD.
- Conduct a focused history (patient interview, medical records review, review of available chest x-ray films, electrocardiogram, or any available monitoror rhythm strip information).
- Conduct a focused physical examination (check for scars, palpate for device).● Define the type of CRMD.
- Obtain manufacturer’s identification card from patient or other source.- Order chest x-ray studies if no other data are available.- Refer to supplemental resources (e.g., manufacturer’s databases).
● Determine dependency on pacing function of the CRMD.- History of symptomatic bradyarrhythmia resulting in CRMD implantation.- History of successful atrioventricular nodal ablation.- Inadequate escape rhythm at lowest programmable pacing rate.
● Determine CRMD function.- Interrogate device (consultation with a cardiologist or pacemaker–ICD service may be necessary).- Determine whether the device will capture when it paces (i.e., produce a mechanical systole with a pacemaker impulse).- Consider contacting the manufacturer for perioperative recommendations.
Preoperative Preparation● Determine whether EMI is likely to occur during the planned procedure.● Determine whether reprogramming pacing function to asynchronous mode or disabling rate responsive function is advantageous.● Suspend antitachyarrhythmia functions if present.● Advise individual performing the procedure to consider use of a bipolar electrocautery system or ultrasonic (harmonic) scalpel.● Temporary pacing and defibrillation equipment should be immediately available.● Evaluate the possible effects of anesthetic techniques and of the procedure on CRMD function and patient CRMD interactions.
Intraoperative Management● Monitor operation of the CRMD.
- Conduct electrocardiographic monitoring per ASA standard.- Monitor peripheral pulse (e.g., manual pulse palpation, pulse oximeter plethysmogram, arterial line).
● Manage potential CRMD dysfunction due to EMI.- Electrocautery.
y Assure that the electrosurgical receiving plate is positioned so that the current pathway does not pass through or near the CRMD system. Forsome cases, the receiving plate might need to be placed on a site different from the thigh (e.g., the superior posterior aspect of the shouldercontralateral to the generator position for a head and neck case).
y Advise individual performing the procedure to avoid proximity of the cautery’s electrical field to the pulse generator or leads.y Advise individual performing the procedure to use short, intermittent, and irregular bursts at the lowest feasible energy levels.y Advise individual performing the procedure to reconsider the use of a bipolar electrocautery system or ultrasonic (harmonic) scalpel in place of a
monopolar electrocautery system, if possible.- Radiofrequency ablation.
y Advise individual performing the procedure to avoid direct contact between the ablation catheter and the pulse generator and leads.y Advise individual performing the procedure to keep the radiofrequency’s current path as far away from the pulse generator and lead system as possible.
- Lithotripsy.y Advise individual performing the procedure to avoid focusing the lithotripsy beam near the pulse generator.y If the lithotripsy system triggers on the R wave, consider preoperative disabling of atrial pacing.
- MRI.y MRI is generally contraindicated in patients with CRMDs.y If MRI must be performed, consult with the ordering physician, the patient’s cardiologist, the diagnostic radiologist, and the CRMD manufacturer.
- Radiation therapy.y Radiation therapy can be safely performed in patients who have CRMDs.y Surgically relocate the CRMD if the device will be in the field of radiation.
- Electroconvulsive therapy.y Consult with the ordering physician, the patient’s cardiologist, a CRMD service, or the CRMD manufacturer.
● Emergency defibrillation or cardioversion.- For a patient with an ICD and magnet-disabled therapies:
y Advise individual performing the procedure to terminate all sources of EMI while magnet is removed.y Remove the magnet to reenable antitachycardia therapies.y Observe the patient and the monitors for appropriate CRMD therapy.y If the above activities do not restore ICD function, proceed with emergency external defibrillation or cardioversion.
- For a patient with an ICD and programming-disabled therapies:y Advise individual performing the procedure to terminate all sources of EMI while magnet is removed.y Reenable therapies through programming if the programmer is immediately available and ready to be used.y Observe the patient and the monitors for appropriate CRMD therapy.y If the above activities do not restore ICD function, proceed with emergency external defibrillation or cardioversion.
- For external defibrillation:y Position defibrillation/cardioversion pads or paddles as far as possible from the pulse generator.y Position defibrillation/cardioversion pads or paddles perpendicular to the major axis of the CRMD to the extent possible by placing them in an
anterior–posterior location.y If it is technically impossible to place the pads or paddles in locations that help to protect the CRMD, defibrillate/cardiovert the patient in the
quickest possible way and be prepared to provide pacing through other routes.y Use a clinically appropriate energy output.
Postoperative Management● Continuously monitor cardiac rate and rhythm and have backup pacing and defibrillation equipment immediately available throughout the immediate
postoperative period.● Interrogate and restore CRMD function in the immediate postoperative period.
- Interrogate CRMD; consultation with a cardiologist or pacemaker–ICD service may be necessary.- Restore all antitachyarrhythmic therapies in ICDs.- Assure that all other settings of the CRMD are appropriate.
Refer to Table 3 for an example of a stepwise approach to the perioperative treatment of the patient with a CRMD.
ASA � American Society of Anesthesiologists; CRMD � cardiac rhythm management device; EMI � electromagnetic interference; ICD � implantablecardioverter–defibrillator; MRI � magnetic resonance imaging.
193PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

Table 3. Example of a Stepwise Approach to the Perioperative Treatment of the Patient with a CRMD
Perioperative Period Patient/CRMD Condition Intervention
Preoperative evaluation Patient has CRMD ● Focused history● Focused physical examination
Determine CRMD type (pacemaker,ICD, CRT)
● Manufacturer’s CRMD identification card● Chest x-ray studies (no data available)● Supplemental resources*
Determine whether patient is CRMD-dependent for pacing function
● Verbal history● Bradyarrhythmia symptoms● Atrioventricular node ablation● No spontaneous ventricular activity†
Determine CRMD function ● Comprehensive CRMD evaluation‡● Determine whether pacing pulses are present and create paced beats
Preoperative preparation EMI unlikely during procedure ● If EMI unlikely, special precautions are not needed
EMI likely: CRMD is pacemaker ● Reprogram to asynchronous mode when indicated● Suspend rate-adaptive functions§
EMI likely: CRMD is ICD ● Suspend antitachyarrhythmia functions● If patient is dependent on pacing function, alter pacing functions as above
EMI likely: all CRMD ● Use bipolar cautery; ultrasonic scalpel● Temporary pacing and external cardioversion–defibrillation available
Intraoperative physiologic changeslikely (e.g., bradycardia, ischemia)
● Plan for possible adverse CRMD–patient interaction
Intraoperativemanagement
Monitoring ● Electrocardiographic monitoring per ASA standard● Peripheral pulse monitoring
Electrocautery interference ● CT/CRP—no current through PG/leads● Avoid proximity of CT to PG/leads● Short bursts at lowest possible energy● Use bipolar cautery; ultrasonic scalpel
Radiofrequency catheter ablation ● Avoid contact of radiofrequency catheter with PG/leads● Radiofrequency current path far away from PG/leads● Discuss these concerns with operator
Lithotripsy ● Do not focus lithotripsy beam near PG● R wave triggers lithotripsy? Disable atrial pacing�
MRI ● Generally contraindicated● If required, consult ordering physician, cardiologist, radiologist, and
manufacturer
RT ● PG/leads must be outside of RT field● Possible surgical relocation of PG● Verify PG function during/after RT course
ECT ● Consult with ordering physician, patient’s cardiologist, a CRMD service, orCRMD manufacturer
Emergency defibrillation–cardioversion
ICD: magnet disabled ● Terminate all EMI sources● Remove magnet to reenable therapies● Observe for appropriate therapies
ICD: programming disabled ● Programming to reenable therapies or proceed directly with externalcardioversion–defibrillation
ICD: either of above ● Minimize current flow through PG/leads● PP as far as possible from PG● PP perpendicular to major axis PG/leads● To extent possible, PP in anterior–posterior location
Regardless of CRMD type ● Use clinically appropriate cardioversion/defibrillation energy
Postoperativemanagement
Immediate postoperative period ● Monitor cardiac R&R continuously● Backup pacing and cardioversion/defibrillation capability
Postoperative interrogation andrestoration of CRMD function
● Interrogation to assess function● Settings appropriate?#● Is CRMD an ICD?**● Use cardiology/pacemaker–ICD service if needed
* Manufacturer’s databases, pacemaker clinic records, cardiology consultation. † With cardiac rhythm management device (CRMD) programmed VVI at lowestprogrammable rate. ‡ Ideally CRMD function assessed by interrogation, with function altered by reprogramming if required. § Most times this will benecessary; when in doubt, assume so. � Atrial pacing spikes may be interpreted by the lithotriptor as R waves, possibly inciting the lithotriptor to deliver a shockduring a vulnerable period in the heart. # If necessary, reprogram appropriate settings. ** Restore all antitachycardia therapies.
CRP � current return pad; CRT � cardiac resynchronization therapy; CT � cautery tool; ECT � electroconvulsive therapy; EMI � electromagnetic interference;ICD � internal cardioverter–defibrillator; MRI � magnetic resonance imaging; PG � pulse generator; PP � external cardioversion–defibrillation pads or paddles;R&R � rhythm and rate; RT � radiation therapy.
194 PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

Appendix 3: Literature Review andConsensus-based Evidence
A. State of the LiteratureFor this Advisory, a literature review was used in combination with
opinions obtained from experts and other sources (e.g., professionalsociety members, open forums, Web-based postings) to provide guid-ance to practitioners regarding the perioperative treatment of patientswith CRMDs. Both the literature review and opinion data were basedon evidence linkages, consisting of directional statements about rela-tions between specific perioperative management activities and CRMDfunction or clinical outcomes.
A study or report that appears in the published literature is includedin the development of an advisory if the study (1) is related to one ofthe specified linkage statements, (2) reports a finding or set of findingsthat can be tallied or measured (e.g., articles that contain only opinionare not included), and (3) is the product of an original investigation orreport (i.e., review articles or follow-up studies that summarize previ-ous findings are not included). Because CRMDs represent a rapidlychanging technology, earlier literature (i.e., literature published before1990) was rarely included in the evaluation of evidence for this Prac-tice Advisory.
Although evidence linkages are designed to assess causality, few ofthe reviewed studies exhibited sufficiently acceptable quantitativemethods and analyses to provide a clear indication of causality. There-fore, the published literature could not be used as a source of quanti-tative support (required for the development of practice guidelines).However, many published studies were evaluated that provided theTask Force with important noncausal evidence. For example, descrip-tive literature (i.e., reports of frequency or incidence) is often useful inproviding an indication of the scope of a problem. Information regard-ing whether a particular adverse outcome is common or rare may haveconsiderable bearing on the practicality of an advisory. Case reportsare typically used as a forum for reporting and recognizing unusual oradverse outcomes and may suggest caution when devising an advisory.
For the literature review, potentially relevant studies were identifiedvia electronic and manual searches of the literature. The electronicsearch covered a 39-yr period from 1966 through 2004. The manualsearch covered a 45-yr period from 1961 through 2005. More than1,500 citations were initially identified, yielding a total of 411 nonover-lapping articles that addressed topics related to the evidence linkages.After review of the articles, 283 studies did not provide direct evidenceand were subsequently eliminated. A total of 128 articles (from 39journals) contained direct linkage-related evidence. No evidence link-age contained enough studies with well-defined experimental designsand statistical information to conduct a quantitative analysis (i.e.,meta-analysis).
Interobserver agreement among Task Force members and two meth-odologists was established by interrater reliability testing. Agreementlevels using a � statistic for two-rater agreement pairs were as follows:(1) type of study design, � � 0.72–0.90; (2) type of analysis, � �0.80–0.90; (3) evidence linkage assignment, � � 0.84–1.00; and (4)literature inclusion for database, � � 0.70–1.00. Three-rater chance-corrected agreement values were (1) study design, Sav � 0.81, Var(Sav) � 0.010; (2) type of analysis, Sav � 0.86, Var (Sav) � 0.009; (3)linkage assignment, Sav � 0.82, Var (Sav) � 0.005; and (4) literaturedatabase inclusion, Sav � 0.78, Var (Sav) � 0.031. These valuesrepresent moderate to high levels of agreement.
Future studies should focus on prospective methodologies, whenpossible, that use traditional hypothesis testing techniques. Use of thefollowing methodologic procedures for assessing the impact of peri-operative management of CRMDs is recommended: (1) comparisonstudies (i.e., one technique vs. another) when clinically feasible; (2)randomization; and (3) full reporting of sample size, effect size esti-mates, test scores, measures of variability, and P values.
B. Consensus-based EvidenceConsensus was obtained from multiple sources, including (1) survey
opinion from Consultants who were selected based on their knowl-edge or expertise in perioperative management of CRMDs, (2) surveyopinions from randomly selected samples of active members of theAmerican Society of Anesthesiologists and active members of the HRS,(3) testimony from attendees of two publicly held open forums at anational anesthesia meeting and at a major cardiology meeting,§ § §(4) Internet commentary, and (5) Task Force opinion and interpreta-tion. The survey rate of return was 56% (n � 23 of 41) for Consultants,15% (n � 89 of 600) for the ASA membership, and 15% (n � 44 of 300)for the HRS membership. Survey results are presented in the text of thedocument and in table 4.
The ASA Consultants were also asked to indicate which, if any, of theevidence linkages would change their clinical practices if the Advisorywas instituted. The rate of return was 39% (n � 16 of 41). The percentof responding Consultants expecting no change associated with eachlinkage were as follows: preoperative evaluation—67%; preoperativepatient preparation—67%; intraoperative monitoring of CRMDs—67%; emergency defibrillation or cardioversion—87%; postoperativemonitoring of CRMDs—73%; postoperative interrogation and restora-tion of CRMD function—60%; intraoperative management of EMI dur-ing: electrocautery—73%, radiofrequency ablation—73%, lithotripsy—80%, MRI—80%, radiation therapy—80%, and electroconvulsivetherapy—73%. Forty percent of the respondents indicated that theAdvisory would have no effect on the amount of time spent on a typicalcase. Nine respondents (60%) indicated that there would be an in-crease in the amount of time they would spend on a typical case withthe implementation of this Advisory. The amount of increased timeanticipated by these respondents ranged from 5 to 30 min.
§ § § International Anesthesia Research Society; 78th Clinical and ScientificCongress, Tampa, Florida, March 28, 2004, and NASPE Heart Rhythm SocietyAnnual Meeting, San Francisco, California, May 20, 2004.
195PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

Table 4. Consultant and Membership Survey Responses: Percent Agreement/Disagreement*
Survey Item
Consultants ASA Members HRS Members
n % Agree/Disagree n % Agree/Disagree n % Agree/Disagree
1. To perform a preoperative evaluation:Establish whether a patient has a CRMD. 23 100/0 89 100/0 44 100/0Define the type of device. 23 100/0 87 95/0 44 100/0Determine whether a patient is CRMD dependent for
pacemaking function.23 96/0 89 96/0 44 96/4
Determine CRMD function. 23 96/0 89 88/3 44 71/112. To prepare a CRMD patient for a procedure:
Determine whether EMI is likely to occur. 23 96/4 89 91/2 44 96/2Turn pacemaking rate-adaptive therapy off. 23 52/35 89 35/35 44 34/34Program pacemaking function to asynchronous mode:
All CRMD patients. 22 0/82 88 21/48 43 9/84Pacemaker-dependent patients only. 22 73/23 83 47/27 43 54/28
Suspend antitachyarrhythmia functions. 21 86/5 87 54/21 43 63/21Consider using a bipolar electrocautery system (when
applicable).22 91/0 86 90/2 44 77/14
Consider using an ultrasonic (harmonic) scalpel (whenapplicable).
22 68/18 88 63/3 44 34/9
Assure the availability of temporary pacing anddefibrillation equipment.
22 100/0 87 95/1 44 89/7
Consider the possible effects of anesthetic agents ortechniques on CRMD function.
22 64/18 86 779 44 66/21
3. Intraoperative monitoring should include:Continuous electrocardiography. 23 100/0 88 100/0 44 100/0Continuous peripheral pulse monitoring. 23 96/0 88 86/11 44 61/18
4. For procedures using electrocautery:Position the electrosurgical receiving plate so current
pathway does not pass through or near the generator orleads.
23 100/0 88 97/0 44 96/0
Avoid proximity of the cautery’s electrical field to thepulse generator or leads.
23 100/0 87 100/0 44 96/2
Use short, intermittent, and irregular bursts at the lowestfeasible energy levels.
23 96/0 87 83/2 44 91/7
Use a bipolar electrocautery system (when applicable). 23 91/0 88 94/1 44 84/2Use an ultrasonic (harmonic) scalpel (when applicable). 23 57/13 88 65/1 44 41/9
5. For radiofrequency ablation:Avoid direct contact between the ablation catheter and
the CRMD and leads.23 83/0 87 76/0 44 91/2
Keep the current path (electrode tip to return plate) as faraway from the pulse generator and lead system aspossible.
23 87/0 87 78/0 44 89/5
6. For lithotripsy:Avoid focusing the lithotripsy beam near the pulse
generator.23 91/0 86 78/1 44 86/0
If the lithotripsy system triggers on the R wave, disableatrial pacing before procedure.
23 39/26 86 38/13 44 39/9
7. For MRI:†
MRI is contraindicated for all CRMD patients. 21 81 79 80 44 55MRI is contraindicated for some but not all CRMD
patients.21 19 79 18 44 39
MRI is not contraindicated for any CRMD patient. 21 0 79 2 44 68. For RT:†
RT is contraindicated for all CRMD patients. 21 0 73 10 44 0RT is contraindicated for some but not all CRMD patients. 21 57 73 37 44 59RT is not contraindicated for any CRMD patient. 21 43 73 53 44 41
9. For emergency defibrillation or cardioversion:Position the defibrillation or cardioversion pads as far as
possible from the pulse generator.23 83/0 87 69/13 44 91/7
Use an anterior–posterior position. 23 74/9 84 61/6 44 68/25Use a clinically appropriate energy output regardless of
the device.23 100/0 87 87/0 44 100/0
10. To treat CRMD patients postoperatively:Interrogate and restore CRMD function in the PACU or
ICU.23 96/4 88 98/1 44 77/21
* The percentages of respondents who agreed/disagreed with each item are presented. The percentages of respondents who were uncertain are notpresented. † Respondents were asked to select one of the three choices. Therefore, the numbers represent percent agreement only.
ASA � American Society of Anesthesiologists; CRMD � cardiac rhythm management device; EMI � electromagnetic interference; HRS � Heart Rhythm Society;ICU � intensive care unit; MRI � magnetic resonance imaging; PACU � postanesthesia care unit; RT � radiation therapy.
196 PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

References � � �1. Barold S, Zites D: Cardiac pacemakers and antiarrhythmic devices, Heart
Disease, 5th edition. Edited by Braunwald E. Philadelphia, WB Saunders, 1997, pp705–41
2. Mychaskiw G, Eichhorn JH: Interaction of an implanted pacemaker with atransesophageal atrial pacemaker: Report of a case. J Clin Anesth 1999; 11:669–71
3. Purday JP, Towey RM: Apparent pacemaker failure caused by activation ofventricular threshold test by a magnetic instrument mat during general anaes-thesia. Br J Anaesth 1992; 69:645–6
4. Kellow NH: Pacemaker failure during transurethral resection of the pros-tate. Anesthesia 1993; 48:136–8
5. Bernstein AD, Irwin ME, Parsonnet V, Wilkoff BL, Black WR, BuckinghamTA, Maloney JD, Reynolds DD, Saksena S, Singer I, Nickelson DE, Schurig L:Report of the NASPE policy conference on antibradycardia pacemaker follow-up:Effectiveness, needs and resources. Pacing Clin Electrophysiol 1994; 17:1714–29
6. Ahern TS, Luckett C, Ehrlich S, Pena EA: Use of bipolar electrocautery inpatients with implantable cardioverter-defibrillators: No reason to inactivatedetection or therapies. PACE 1999; 22:776
7. Bailey AG, Lacey SR: Intraoperative pacemaker failure in an infant. Can JAnaesth 1991; 38:912–3
8. El-Gamal HM, Dufresne RG, Saddler K: Electrosurgery, pacemakers andICDs: A survey of precautions and complications experienced by cutaneoussurgeons. Dermatol Surg 2001; 27:385–90
9. Rozner MA: Review of electrical interference in implanted cardiac devices.PACE 2003; 26:923–5
10. Wilson JH, Lattner S, Jacob R, Stewart R: Electrocautery does not interferewith the function of the automatic implantable cardioverter defibrillator. AnnThorac Surg 1991; 51:225–6
11. Wong DT, Middleton W: Electrocautery-induced tachycardia in a rate-responsive pacemaker. ANESTHESIOLOGY 2001; 94:10–1
12. Chang AC, McAreavey D, Tripodi D, Fananapazir L: Radiofrequency cath-eter atrioventricular node ablation in patients with permanent cardiac pacingsystems. Pacing Clin Electrophysiol 1994; 17:65–9
13. Chin MC, Rosenqvist M, Lee MA, Griffin JC, Langberg JJ: The effect ofradiofrequency catheter ablation on permanent pacemakers: An experimentalstudy. Pacing Clin Electrophysiol 1990; 13:23–9
14. de Chillou C, Sadoul N Beurrier D, Bizeau O, Aliot E, Dodinot B: Effects ofradiofrequency catheter ablation on the behavior of permanent pacemakers.Pacing Clin Electrophysiol 1996; 19:680
15. Ellenbogen KA, Wood MA, Stambler BS: Acute effects of radiofrequencyablation of atrial arrhythmias on implanted permanent pacing systems. PacingClin Electrophysiol 1996; 19:1287–95
16. Pfeiffer D, Tebbenjohanns J, Schumacher B, Jung W, Luderitz B: Pace-maker function during radiofrequency ablation. Pacing Clin Electrophysiol 1995;18:1037–44
17. Pfeiffer D, Tebbenjohanns J, Schumacher B, Jung W, Manz M, Luderitz B:Pacemaker behaviour during radiofrequency current delivery. J Am Coll Cardiol1994; 23(suppl A):324A
18. Moore S, Firstenberg M, Simmons TW, Trohman R: The interaction be-tween radiofrequency ablation and permanent pacemakers. Circulation 1992;86(suppl 1):I-449
19. Trohman RG, Simmons TW, Moore SL, Firstenberg MS, Williams D, Ma-loney JD: Catheter ablation of atrioventricular junction using radiofrequencyenergy and a bilateral cardiac approach. Am J Cardiol 1992; 70:1438–43
20. Wolfe DA, McCutcheon MJ, Plumb VJ, Kay N: Radiofrequency current mayinduce exit block in chronically implanted ventricular leads. Pacing Clin Electro-physiol 1995; 18:919
21. Achenbach S, Moshage W, Diem B, Bieberle T, Schibgilla V, Bachmann K:Effects of magnetic resonance imaging on cardiac pacemakers and electrodes.Am Heart J 1997; 134:467–73
22. Fontaine JM, Mohamed FB, Gottlieb, Callans DJ, Marchlinski FE: Rapidventricular pacing in a pacemaker patient undergoing magnetic resonance im-aging. Pacing Clin Electrophysiol 1998; 21:1336–9
23. Garcia-Bolao I, Albaladejo V, Benito A, Alegria E, Zubieta JL: Magneticresonance imaging in a patientv with a dual-chamber pacemaker. Acta Cardiol1998; 53:33–5
24. Gimbel JR, Johnson D, Levine PA, Wilkoff BL: Safe performance of mag-netic resonance imaging on five patients with permanent cardiac pacemakers.Pacing Clin Electrophysiol 1996; 19:913–9
25. Gimbel JR, Lorig RJ, Wilkoff BL: Safe magnetic resonance imaging ofpacemaker patients. J Am Coll Cardiol 1995; 25:11A
26. Hayes DL, Holmes DR Jr, Gray JE: Effect of 1.5 Tesla nuclear magneticresonance imaging scanner on implanted permanent pacemakers. J Am CollCardiol 1987; 10:782–6
27. Luechinger R, Duru F, Scheidegger MB, Boesiger P, Candinas R: Force and
torque effects of a 1.5-Tesla MRI scanner on cardiac pacemakers and ICDs. PacingClin Electrophysiol 2001; 24:199–205
28. Pavlicek W, Geisinger M, Castle L, Borkowski GP, Meaney TF, Bream BL,Gallagher JH: The effects of nuclear magnetic resonance on patients with cardiacpacemakers. Radiology 1993; 147:149–53
29. Vahlhaus C, Sommer T, Lewalter T, Schimpf R, Schumacher B, Jung W,Luderitz B: Interference with cardiac pacemakers by magnetic resonance imag-ing: Are there irreversible changes at 0.5 Tesla? Pacing Clin Electrophysiol 2001;24:489–95
30. Martin ET, Coman JA, Shellock FG, Pulling CC, Fair R, Jenkins K: Magneticresonance imaging and cardiac pacemaker safety at 1.5-Telsa. J Am Coll Cardiol2004; 43:1315–24
31. Rozner MA, Burton AW, Kumar AJ: Pacemaker complication during MRI.J Am Coll Cardiol 2005; 45:161–2
32. Raitt MH, Stalzer KJ, Laramore GE, Bardy GH, Dolack GL, Poole JE,Kudenchuk PJ: Runaway pacemaker during high-energy neutron radiation ther-apy. Chest 1994; 106:955–7
33. Rodriguez F, Filimonov A, Henning A, Coughlin C, Greenberg M: Radia-tion-induced effects in multiprogrammable pacemakers and implantable defibril-lators. Pacing Clin Electrophysiol 1991; 14:2143–53
34. Hurkmans CW, Scheepers E, Springorum BG, De Ruiter GS, Uiterwaal HA:Influence of therapeutic irradiation on the latest generation of pacemakers. HeartRhythm 2004; 1(suppl):S53–4
35. Drach GW, Weber C, Donovan JM: Treatment of pacemaker patients withextracorporeal shock wave lithotripsy: Experience from 2 continents. J Urol1990; 143:895–6
36. Vassolas G, Roth RA, Venditti FJ Jr: Effect of extracorporeal shock wavelithotripsy on implantable cardioverter defibrillator. Pacing Clin Electrophysiol1993; 16:1245–8
37. Theiss M, Wirth MP, Frohmuller HG: Extracorporeal shock wave litho-tripsy in patients with cardiac pacemakers. J Urol 1990; 143:479–80
38. Vaidyanathan S, Hirst R, Parsons KF, Singh G, Soni BM, Oo T, Zaidi A, WattJW, Sett P: Bilateral extracorporeal shock wave lithotripsy in a spinal cord injurypatient with a cardiac pacemaker. Spinal Cord 2001; 39:286–9
39. Venditti FJ Jr, Martin D, Long AL, Roth RA: Renal extracorporeal shockwave lithotripsy performed in patient with implantable cardioverter defibrillator.Pacing Clin Electrophysiol 1991; 14:1323–5
40. Hayes DL, Charboneau JW, Lewis BD, Asirvatham SJ, Dupuy DE, LexvoldNY: Radiofrequency treatment of hepatic neoplasms in patients with permanentpacemakers. Mayo Clin Proc 2001; 76:950–2
41. O’Donoghue JK: Inhibition of a demand pacemaker by electrosurgery.Chest 1973; 64:664–6
42. Smith CL, Frawley G, Hamar A: Diathermy and the telectronics “META”pacemaker. Anaesth Intensive Care 1993; 21:452–4
43. Kleinman B, Hamilton J, Heriman R, Olshansky B, Justus D, Desai R:Apparent failure of a precordial magnet and pacemaker programmer to converta DDD pacemaker to VOO mode during the use of the electrosurgical unit.ANESTHESIOLOGY 1997; 86:247–50
44. Mangar D, Atlas GM, Kane PB: Electrocautery-induced pacemaker malfunc-tion during surgery. Can J Anaesth 1991; 38:616–8
45. American Society of Anesthesiologists: Standards for basic anesthetic mon-itoring, In ASA Standards, Guidelines and Statements. Chicago, American Societyof Anesthesiologists, October 2004
46. Baller MR, Kirsner KM: Anesthetic implications of implanted pacemakers:A case study. AANA J 1995; 63:209–16
47. Celentano WJ, Jahr JS, Nossaman BD: Extracorporeal shock wave litho-tripsy in a patient with a pacemaker. Anesth Analg 1992; 74:770–2
48. Chew EW, Troughear RH, Kuchar DL, Thorburn CW: Inappropriate ratechange in minute ventilation rate responsive pacemakers due to interference bycardiac monitors. Pacing Clin Electrophysiol 1997; 20:276–82
49. Rubin JM, Miller ED: Intraoperative pacemaker malfunction during totalhip arthroplasty. Anesth Analg 1995; 80:410–2
50. Samain E, Marty J, Souron V, Rosencher N, Eyrolle L: Intraoperativepacemaker malfunction during a shoulder arthroscopy. ANESTHESIOLOGY 2000;93:306–7
51. Society of Anesthesiologists: Standards for postanesthesia care, In ASAStandards, Guidelines and Statements. Chicago, American Society of Anesthesi-ologists, October 2004
52. O’Donoghue JK: Inhibition of a demand pacemaker by electrosurgery.Chest 1973; 64:664–6
53. Rubin JM, Miller ED: Intraoperative pacemaker malfunction during totalhip arthroplasty. Anesth Analg 1995; 80:410–2
54. Heller LI: Surgical electrocautery and the runaway pacemaker syndrome.Pacing Clin Electrophysiol 1990; 13:1084–5
55. Mychaskiw G, Eichhorn JH: Interaction of an implanted pacemaker with atransesophageal atrial pacemaker: Report of a case. J Clin Anesth 1999; 11:669–71
56. Batra YK, Bali IM: Effect of coagulating and cutting current on a demandpacemaker during transurethral resection of the prostate: A case report. CanAnaesth Soc J 1978; 25:65–6
57. Erdman S, Levinsky L, Servadio C, Stoupel E, Levy MJ: Safety precautionsin the management of patients with pacemakers when electrocautery operationsare performed. Surg Gynecol Obstet 1988; 167:311–4
� � � The references listed here do not represent a complete bibliography of theliterature reviewed. A complete bibliography is available by writing to theAmerican Society of Anesthesiologists or by accessing the ANESTHESIOLOGY Website: http://www.anesthesiology.org.
197PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

58. Dresner DL, Lebowitz PW: Atrioventricular sequential pacemaker inhibi-tion by transurethral electrosurgery. ANESTHESIOLOGY 1988; 68:599–601
59. Lerner SM: Suppression of a demand pacemaker by transurethral electro-cautery. Anesth Analg 1973; 52:703–6
60. Wajszczuk WJ, Mowry FM, Dugan NL: Deactivation of a demand pace-maker by transurethral electrocautery. N Eng J Med 1969; 280:34–5
61. Epstein MR, Mayer JE Jr, Duncan BW: Use of an ultrasonic scalpel as analternative to electrocautery in patients with pacemakers. Ann Thorac Surg 1998;65:1802–4
62. Ozeren M, Dogan OV, Duzgun C, Yucel E: Use of an ultrasonic scalpel inthe open-heart reoperation of a patient with pacemaker. Eur J Cardiothorac Surg2002; 21:761–2
63. Val-Majias JE, Diehl T, Quesada LC: Long-term effects of RF ablation onpacemakers leads. Pacing Clin Electrophysiol 1996; 19:635
64. Alagona P, Toole JC, Maniscalco BS: Nuclear magnetic resonance imagingin a patient with a pacemaker. Pacing Clin Electrophysiol 1989; 12:619
65. Inbar S, Larson J, Burt T, Mafee M, Ezri MD: Case report: nuclear magneticresonance imaging in a patient with a pacemaker. Am J Med Sci 1993; 305:174–5
66. Lauck G, Sommer T, Wolke S, Luderitz B, Manz M: Magnetic resonanceimaging in patients with implanted permanent pacemakers. Pacing Clin Electro-physiol 1995; 18(suppl):1168
67. Lauck G, von Smekal A, Wolke S, Seelos KC, Jung W, Manz M, Luderitz B:Effects of nuclear magnetic resonance imaging on cardiac pacemakers. PacingClin Electrophysiol 1995; 18:1549–55
68. Roguin A, Zviman MM, Meininger GR, Rodrigues ER, Dickfeld TM,Bluemke DA, Lardo A, Berger RD, Calkins H, Halperin HR: Modern pacemakerand implantable cardioverter/defibrillator systems can be magnetic resonanceimaging safe. Circulation 2004; 110:475–82
69. Shellock FG, O’Neil M, Ivans V, Kelly D, O’Connor M, Toay L, Crues JV:Cardiac pacemakers and implantable cardioverter defibrillators are unaffected byoperation of an extremity MR imaging system. Am J Roentgenol 1999; 172:165–70
70. Sommer T, Valhaus C, Lauck G, von Smekal A, Reinke M, Hofer U, Block
W, Traber F, Schneider C, Gieseke J, Jung W, Schild H: MR imaging and cardiacpacemakers: In vitro evaluation and in vivo studies in 51 patients at 0.5 T.Radiology 2000; 215:869–79
71. von Smekal A, Wolke S, Seelos KC, Hermans J, Lauch G, David P, Reiser M,Biersack HJ: Cardiac pacemaker in magnetic resonance studies: Influence of thestatic magnetic field on hardware components. Eur Heart J 1993; 14:335
72. Goldberg RJ, Badger JM: Major depressive disorder in patients with theimplantable cardioverter defibrillator: Two cases treated with ECT. Psychosomat-ics 1993; 34:273–7
73. Alyward P, Blood R, Tonkin A: Complications of defibrillation with per-manent pacemaker in situ. Pacing Clin Electrophysiol 1979; 2:462–4
74. Das G, Eaton J: Pacemaker malfunction following transthoracic counter-shock. Pacing Clin Electrophysiol 1981; 4:487–90
75. Gould L, Patel S, Gomes GI, Chokshi AB: Pacemaker failure followingexternal defibrillation. Pacing Clin Electrophysiol 1981; 4:575–7
76. Palac RT, Hwang MH, Klodnycky ML, Loeb HS: Delayed pulse generatormalfunction after DC countershock. Pacing Clin Electrophysiol 1981; 4:163–7
77. Zullo M: Function of ventricular pacemakers during resuscitation. PacingClin Electrophysiol 1990; 13:736–44
78. ACLS Provider Manual. Edited by Cummins RO. Dallas, American HeartAssociation, 2003
79. Levine PA, Balady GJ, Lazar HL, Belott PH, Roberts AJ: Electrocautery andpacemakers: Management of the paced patient subject to electrocautery. AnnThorac Surg 1986; 41:313–7
80. Bernstein AD, Daubert JC, Fletcher RD, Hayes DL, Luderitz B, ReynoldsDW, Schoenfeld MH, Sutton R: The revised NASPE/BPEG generic code forantibradycardia, adaptive-rate, and multisite pacing. North American Society ofPacing and Electrophysiology/British Pacing and Electrophysiology Group. Pac-ing Clin Electrophysiol 2002; 25:260–4
81. Bernstein AD, Camm AJ, Fisher JD, Fletcher RD, Mead RH, Nathan AW,Parsonnet V, Rickards AF, Smyth NP, Sutton R: North American Society of Pacingand Electrophysiology policy statement: The NASPE/BPEG defibrillator code.Pacing Clin Electrophysiol 1993; 16:1776–80
198 PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

Anesthesiology 2008; 108:786–801 Copyright © 2008, the American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc.
Practice Advisory for the Prevention and Management ofOperating Room Fires
A Report by the American Society of Anesthesiologists Task Force on OperatingRoom Fires*
This article has been selected for the ANESTHESIOLOGY
CME Program. After reading the article, go to http://www.asahq.org/journal-cme to take the test and apply for Cate-gory 1 credit. Complete instructions may be found in theCME section at the back of this issue.
PRACTICE advisories are systematically developed re-ports that are intended to assist decision making in areasof patient care. Advisories are based on a synthesis ofscientific literature and analysis of expert opinion, clin-ical feasibility data, open forum commentary, and con-sensus surveys. Advisories developed by the AmericanSociety of Anesthesiologists (ASA) are not intended asstandards, guidelines, or absolute requirements. Theymay be adopted, modified, or rejected according to clin-ical needs and constraints.
The use of practice advisories cannot guarantee any spe-cific outcome. Practice advisories summarize the state ofthe literature and report opinions obtained from expertconsultants and ASA members. Practice advisories are notsupported by scientific literature to the same degree asstandards or guidelines because of the lack of sufficientnumbers of adequately controlled studies. Practice adviso-
ries are subject to periodic revision as warranted by theevolution of medical knowledge, technology, and practice.
The incidence of operating room (OR) fires is difficultto determine, due in part to the lack of a mandatorynational reporting system for OR fires.1–3 Some estimatessuggest that between 50 and 200 OR fires occur in theUnited States every year, with as many as 20% of re-ported fires resulting in serious injury or death.4,5
Fire requires the presence of three components,known as the “fire triad”: (1) an oxidizer, (2) an ignitionsource, and (3) fuel.
● Oxidizers used in the OR are oxygen and nitrous oxide.An oxidizer-enriched atmosphere increases the likeli-hood and intensity of combustion. An oxidizer-enrichedatmosphere commonly exists within closed or semi-closed breathing systems, including the patient’s airway.It can also be created locally when the configuration ofthe drapes and open oxygen sources (e.g., masks, nasalcannula) promote the trapping or pooling of oxygen or amixture of oxygen and nitrous oxide.
KEY CONCEPT: An oxidizer-enriched atmosphere occurs whenthere is any increase in oxygen concentration above room air level,and/or the presence of any concentration of nitrous oxide.
● Ignition sources include, but are not limited to, elec-trosurgical or electrocautery devices, lasers, heatedprobes, drills and burrs, argon beam coagulators, fiber-optic light cables, and defibrillator paddles or pads.
● Fuel sources include, but are not limited to, trachealtubes; sponges; drapes; gauze; alcohol-containing solu-tions (e.g., certain prepping solutions); solutions contain-ing other volatile compounds, such as ether or acetone;oxygen masks; nasal cannulae; the patient’s hair; dress-ings; ointments; gowns; gastrointestinal tract gases; blan-kets; suction catheters; flexible endoscopes; fiberopticcable coverings; gloves; and packaging materials.†
Methodology
A. Definition of OR Fires, High-risk Procedures, andOR Fire DrillsFor this Advisory, operating room fires are defined as
fires that occur on or near patients who are under anes-thesia care, including surgical fires, airway fires, and fireswithin the airway circuit. A surgical fire is defined as afire that occurs on or in a patient. An airway fire is aspecific type of surgical fire that occurs in a patient’s
Additional material related to this article can be found on the ANES-THESIOLOGY Web site. Go to http://www.anesthesiology.org, click onEnhancements Index, and then scroll down to find the appropriatearticle and link. Supplementary material can also be accessed on theWeb by clicking on the “ArticlePlus” link either in the Table ofContents or at the top of the HTML version of the article.
�
* Developed by the American Society of Anesthesiologists Task Force onOperating Room Fires: Robert A. Caplan, M.D. (Chair), Seattle, Washington;Steven J. Barker, Ph.D., M.D., Tucson, Arizona; Richard T. Connis, Ph.D., Wood-inville, Washington; Charles Cowles, M.D., Deer Park, Texas; Albert L. de Rich-emond, M.S., P.E., Plymouth Meeting, Pennsylvania; Jan Ehrenwerth, M.D., Mad-ison, Connecticut; David G. Nickinovich, Ph.D., Bellevue, Washington; DonnaPritchard, R.N., Brooklyn, New York; David Roberson, M.D., Boston, Massachu-setts; Gerald L. Wolf, M.D. (Honorary), Brooklyn, New York.
Submitted for publication November 6, 2007. Accepted for publication No-vember 6, 2007. Supported by the American Society of Anesthesiologists underthe direction of James F. Arens, M.D., Chair, Committee on Standards andPractice Parameters. Approved by the House of Delegates on October 17, 2007.A complete list of references used to develop this Advisory is available by writingto the American Society of Anesthesiologists.
This Practice Advisory has been endorsed by the American Academy ofOtolaryngology–Head and Neck Surgery.
Address correspondence to the American Society of Anesthesiologists: 520N. Northwest Highway, Park Ridge, Illinois 60068-2573. This Practice Advi-sory, as well as all published American Society of Anesthesiologists PracticeParameters, may be obtained at no cost through the Journal Web site,www.anesthesiology.org.
† Some of these items only burn in an oxidizer-enriched atmosphere.
Anesthesiology, V 108, No 5, May 2008 786

airway. Airway fires may or may not include fire in theattached breathing circuit.
A high-risk procedure is defined as one in which anignition source (e.g., electrosurgery) may come in prox-imity to an oxidizer-enriched atmosphere (e.g., supple-mental oxygen and/or nitrous oxide), thereby increasingthe risk of fire. Examples of high-risk procedures in-clude, but are not limited to, tonsillectomy, tracheos-tomy, removal of laryngeal papillomas, cataract or othereye surgery, burr hole surgery, or removal of lesions onthe head, neck, or face.
An OR fire drill is defined as a formal and periodicrehearsal of the OR team’s planned response to a fire. Inthis Advisory, the OR fire drill is characterized as a“formal and periodic rehearsal” to indicate that it takesplace during dedicated education time, not during pa-tient care. In other words, an OR fire drill is not thesame as a discussion or plan about fire management thattakes place during direct patient care.
B. PurposeThe purposes of this Advisory are to (1) identify situ-
ations conducive to fire, (2) prevent the occurrence ofOR fires, (3) reduce adverse outcomes associated withOR fires, and (4) identify the elements of a fire responseprotocol. Adverse outcomes associated with OR firesmay include major or minor burns, inhalation injuries,infection, disfigurement, and death. Related adverse out-comes may include psychological trauma, prolongedhospitalization, delay or cancellation of surgery, addi-tional hospital resource utilization, and liability.
C. FocusThis Advisory focuses on a specific care setting and
subset of fires. The specific care setting is any OR orprocedure area where anesthesia care is provided. Thespecific subset is fires that occur on the patient, in theairway, or in the breathing circuit. This Advisory doesnot address fires away from the patient (e.g., in a trashcan), institutional preplanning for fire, or the responsesof fire personnel.
D. ApplicationThis Advisory is intended for use by anesthesiologists
or other individuals working under the supervision of ananesthesiologist. Because prevention of OR fires requiresclose collaboration and prompt coordination betweenanesthesiologists, surgeons, and nurses, some responsi-bilities are shared among the disciplines. When sharedresponsibilities are described in this Advisory, the intentis to give the anesthesiologist a starting point for partic-
ipating in the allocation and understanding of sharedresponsibilities. The Advisory may also serve as a re-source for other physicians and healthcare professionals(e.g., technicians, safety officers, hospital administrators,biomedical engineers, industry representatives).
E. Task Force Members and ConsultantsThe ASA appointed a Task Force of nine members.
These individuals included four anesthesiologists in pri-vate and academic practice from various geographicareas of the United States, an otolaryngologist, a periop-erative registered nurse, a professional engineer/fire in-vestigator, and two consulting methodologists from theASA Committee on Standards and Practice Parameters.Two Task Force members are former firefighters.
The Task Force developed the Advisory by means of aseven-step process. First, they reached consensus on thecriteria for evidence. Second, a systematic review andevaluation was performed on original, published, peer-reviewed and other research studies related to OR fires.Third, a panel of expert consultants was asked to (1)participate in opinion surveys on the effectiveness ofvarious strategies for fire prevention, detection, andmanagement and (2) review and comment on a draft ofthe Advisory developed by the Task Force. Fourth, opin-ions about the Advisory were solicited from a randomsample of active members of the ASA. Fifth, the TaskForce held an open forum at a major national meeting‡to solicit input on its draft recommendations. Sixth, theconsultants were surveyed to assess their opinions onthe feasibility of implementing this Advisory. Seventh, allavailable information was used to build consensuswithin the Task Force to formulate the advisory state-ments (appendix 1).
F. Availability and Strength of EvidencePreparation of this Advisory followed a rigorous meth-
odological process (appendix 2). Evidence was obtainedfrom two principal sources: scientific evidence and opin-ion-based evidence.
Scientific Evidence. Study findings from publishedscientific literature were aggregated and are reported insummary form by evidence category, as described be-low. All literature (e.g., randomized controlled trials,observational studies, case reports) relevant to eachtopic was considered when evaluating the findings.However, for reporting purposes in this document, onlythe highest level of evidence (i.e., level 1, 2, or 3) withineach category is included in the summary.
Category A: Supportive Literature. Randomized con-trolled trials report statistically significant (P � 0.01)differences between clinical interventions for a specifiedclinical outcome.
Level 1: The literature contains multiple randomizedcontrolled trials, and the aggregated findings are sup-ported by meta-analysis.§
‡ Society for Ambulatory Anesthesia, 22nd Annual Meeting, San Diego, Cali-fornia, May 5, 2007.
§ All meta-analyses are conducted by the ASA methodology group. Meta-analyses from other sources are reviewed but not included.
787PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

Level 2: The literature contains multiple randomizedcontrolled trials, but there is an insufficient number ofstudies to conduct a viable meta-analysis for the pur-pose of this Advisory.
Level 3: The literature contains a single randomizedcontrolled trial.
Category B: Suggestive Literature. Information fromobservational studies permits inference of beneficial orharmful relationships among clinical interventions andclinical outcomes.
Level 1: The literature contains observational compari-sons (e.g., cohort, case–control research designs) oftwo or more clinical interventions or conditions andindicates statistically significant differences betweenclinical interventions for a specified clinical outcome.
Level 2: The literature contains noncomparative obser-vational studies with associative (e.g., relative risk,correlation) or descriptive statistics.
Level 3: The literature contains case reports.
Category C: Equivocal Literature. The literature can-not determine whether there are beneficial or harmfulrelationships among clinical interventions and clinicaloutcomes.
Level 1: Meta-analysis did not find significant differencesamong groups or conditions.
Level 2: There is an insufficient number of studies toconduct meta-analysis and (1) randomized controlledtrials have not found significant differences amonggroups or conditions or (2) randomized controlledtrials report inconsistent findings.
Level 3: Observational studies report inconsistent find-ings or do not permit inference of beneficial or harm-ful relationships.
Category D: Insufficient Evidence from Literature.The lack of scientific evidence in the literature is de-scribed by the following terms.
Silent: No identified studies address the specified rela-tionships among interventions and outcomes.
Inadequate: The available literature cannot be used toassess relationships among clinical interventions andclinical outcomes. The literature either does not meetthe criteria for content as defined in the “Focus” of theAdvisory or it does not permit a clear interpretation offindings due to methodologic concerns (e.g., con-founding in study design or implementation).
Opinion-based Evidence. All opinion-based evi-dence relevant to each topic (e.g., survey data, open-forum testimony, Web-based comments, letters, editori-
als) is considered in the development of this Advisory.However, only the findings obtained from formal surveysare reported.
Opinion surveys were developed by the Task Force toaddress each clinical intervention identified in the doc-ument. Identical surveys were distributed to two groupsof respondents: expert consultants and ASA members.
Category A: Expert Opinion. Survey responses fromTask Force–appointed expert consultants are reported insummary form in the text. A complete listing of consul-tant survey responses is reported in appendix 2.
Category B: Membership Opinion. Survey responsesfrom a random sample of members of the ASA and, whenappropriate, responses from members of other organiza-tions with expertise in the selected topics of interest arereported in summary form in the text. A complete listing ofASA member survey responses is reported in appendix 2.
Survey responses are recorded using a five-point scaleand summarized based on median values.�
Strongly Agree: Median score of 5 (at least 50% of theresponses are 5)
Agree: Median score of 4 (at least 50% of the responsesare 4 or 4 and 5)
Equivocal: Median score of 3 (at least 50% of the re-sponses are 3, or no other response category or com-bination of similar categories contains at least 50% ofthe responses)
Disagree: Median score of 2 (at least 50% of responsesare 2 or 1 and 2)
Strongly Disagree: Median score of 1 (at least 50% ofresponses are 1)
Category C: Informal Opinion. Open-forum testi-mony, Web-based comments, letters, and editorials areall informally evaluated and discussed during the devel-opment of the Advisory. When warranted, the TaskForce may add educational information or cautionarynotes based on this information.
Advisories
I. EducationOperating room fire safety education includes, but is
not limited to, knowledge of institutional fire safety pro-tocols and participation in institutional fire safety educa-tion. Case reports indicate that lack of education canresult in severe injury and death from uncontrolled ORfires.6,7 [Category B3 evidence.]
The consultants and ASA members strongly agree thatevery anesthesiologist should have knowledge of institu-tional fire safety protocols for the OR, and should par-ticipate in OR fire safety education. The consultants andASA members strongly agree that OR fire safety educa-tion for the anesthesiologist should emphasize the riskcreated by an oxidizer-enriched atmosphere.
� When an even number of responses are obtained, the median value isdetermined by a calculating the arithmetic mean of the two middle values. Tiesare calculated by a predetermined formula.
788 PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

Advisory Statements. All anesthesiologists shouldhave fire safety education, specifically for OR fires, withemphasis on the risk created by an oxidizer-enrichedatmosphere.
II. OR Fire DrillsA case report indicates that OR fire drills and simula-
tion training can result in improved staff response to afire.8 [Category B3 evidence.]
The consultants strongly agree and ASA membersagree that all anesthesiologists should periodically par-ticipate in OR fire drills with the entire OR team. Theconsultants and ASA members strongly agree that partic-ipation should take place during dedicated educationaltime, not during patient care.
Advisory Statements. Anesthesiologists should peri-odically participate in OR fire drills with the entire ORteam. This formal rehearsal should take place duringdedicated educational time, not during patient care.
III. PreparationPreparation for OR fires includes (1) determining
whether or not a high-risk situation exists and (2) a teamdiscussion of the strategy for the prevention and man-agement of an OR fire in a high-risk situation. The liter-ature is silent regarding whether a preoperative determi-nation of a high-risk situation or a team discussion of ORfire strategy reduces the incidence or severity of an ORfire. [Category D evidence.]
The consultants strongly agree and ASA membersagree that anesthesiologists should participate with theentire OR team in assessing the risk of an OR fire for eachcase and determining whether a high-risk situation ex-ists. The consultants strongly agree and ASA membersagree that all team members should jointly agree on howa fire will be prevented and managed for each particularprocedure. The consultants and ASA members stronglyagree that a protocol for the prevention and manage-ment of fires should be posted in each location where aprocedure is performed.
Advisory Statements. For every case, the anesthesi-ologist should participate with the entire OR team (e.g.,during the surgical pause) in determining whether ahigh-risk situation exists. If a high-risk situation exists, allteam members—including the anesthesiologist—shouldtake a joint and active role in agreeing on how a fire willbe prevented and managed. Each team member shouldbe assigned a specific fire management task to performin the event of a fire (e.g., removing the tracheal tube,stopping the flow of airway gases). Each team membershould understand that his or her preassigned taskshould be performed immediately if a fire occurs, with-out waiting for another team member to take action.When a team member has completed a preassigned task,he or she should help other team members performtasks that are not yet complete.
In every OR and procedure area where a fire triad canexist (i.e., an oxidizer-enriched atmosphere, an ignitionsource, and fuel), an easily visible protocol for the pre-vention and management of fires should be displayed(fig. 1).
Equipment for managing a fire should be readily avail-able in every procedural area where a fire triad mayexist. Table 1 provides an example of fire managementequipment that should be in or near the OR or proce-dural area.
IV. PreventionPrevention of OR fires includes (1) minimizing or
avoiding an oxidizer-enriched atmosphere near the sur-gical site, (2) safely managing ignition sources, and (3)safely managing fuels.
Comparative studies indicate that a wide range of mate-rial ignites more readily in an oxygen-enriched atmospherethan in room air.9–13 [Category B1 evidence.] One compar-ative study with awake volunteer subjects showed that theconfiguration of surgical drapes can result in oxygenbuildup, increasing the risk of fire.14 [Category B1 evi-dence.] This study also indicated that replacing oxygenwith compressed air or discontinuing supplemental oxy-gen for a period of time reduces oxygen buildup withoutsignificantly reducing oxygen saturation levels. Similarly, arandomized controlled trial comparing supplemental oxy-gen and compressed air in sedated patients undergoingcataract surgery found no differences in oxygen satura-tion.15 [Category C2 evidence.]
Observational studies and case reports indicate that elec-trocautery or electrosurgical devices and lasers are com-mon sources of ignition for many OR fires, particularlywhen used in an oxidizer-enriched atmosphere.16–68 [Cat-egory B2–3 evidence.]
Case reports indicate that alcohol-based skin-preppingagents generate volatile vapors that ignite easily. Thesereports suggest that insufficient drying time after appli-cation of alcohol-based skin-prepping agents is a cause offires on patients.23,69–73 [Category B3 evidence.] Com-parative studies show that conventional tracheal tubes,when exposed to a laser beam, are more likely to igniteor melt than laser-resistant tracheal tubes.74–84 [Cate-gory B1 evidence.] Case reports indicate that drysponges and gauze are common sources of fu-el.7,19,33,43,45,55,64,83–87 Comparative studies demonstratethat the flammability of sponges, cottonoids, or packingmaterial is reduced when wet rather than dry or partiallydry.88–91 [Category B1 evidence.]
For all procedures, the consultants and ASA membersstrongly agree that flammable skin prepping solutionsshould be dry before draping. They strongly agree thatsurgical drapes should be configured to prevent oxygenfrom accumulating under the drapes or from flowinginto the surgical site. They strongly agree that sponges
789PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

Fig. 1. Operating room fires algorithm. CO2 � carbon dioxide; OR � operating room.
790 PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

should be moistened when used near an ignition source,particularly when used in or near the airway.
For high-risk procedures (i.e., proximity of an ignitionsource and an oxidizer-enriched atmosphere), the con-sultants and ASA members strongly agree that anesthesi-ologists should collaborate with the procedure team forthe purpose of preventing and managing a fire. Theystrongly agree that the surgeon should be notified when-ever an ignition source is in proximity to an oxidizer-enriched atmosphere or when the concentration of ox-idizer has increased. They strongly agree that thefraction of inspired oxygen (FIO2) delivered to the pa-tient should be kept as low as clinically feasible when anignition source is in proximity to an oxygen-enrichedatmosphere. They strongly agree that the reduction ofFIO2 delivered to the patient should be guided by moni-toring patient oxygenation (e.g., pulse oximetry). TaskForce members agree that the reduction of FIO2 shouldbe monitored, if feasible, by measuring inspired, ex-pired, and/or delivered oxygen concentration. Theystrongly agree that the use of nitrous oxide should beavoided in settings that are considered high risk for fire.The consultants strongly agree and ASA members agreethat oxygen or nitrous oxide buildup may be minimizedby either insufflating with medical air or scavenging theoperating field with suction.
For laser surgery, consultants and ASA membersstrongly agree that laser resistant tracheal tubes shouldbe used, and that the tube choice should be appropriatefor the procedure and laser. They both strongly agreethat the tracheal cuff of the laser tube should be filledwith saline rather than air, when feasible. The consult-ants strongly agree and the ASA members agree thatsaline in tracheal tube cuff should be tinted with meth-ylene blue to act as a marker for cuff puncture by a laser.
Surgery inside the airway can bring an ignition sourceinto proximity with an oxidizer-enriched atmosphere,thereby creating a high-risk situation. For cases involvingsurgery inside the airway, consultants and ASA membersboth agree that a cuffed tracheal tube should be usedinstead of an uncuffed tracheal tube when medicallyappropriate. Because an elevated FIO2 is often necessary
during tracheostomy, the Task Force strongly agrees thatsurgeons should be advised not to enter the trachea withan ignition source such as an electrosurgical device. If anelectrosurgical device must be used, the anesthesiologistshould request that the surgeon provide adequate warn-ing to allow the concentration of oxidizer to be mini-mized before the trachea is entered. Consultants andASA members were asked to report the time that theybelieve is needed to reduce oxygen or nitrous oxideconcentration to a safe level before using an ignitionsource. For patients being ventilated with a trachealtube, consultants report a range of time of less than 1min to 5 min (mean � 1.8 min), and ASA members reporta range of time of less than 1 min to 10 min (mean �2.9 min). For patients wearing a facemask or nasal can-nula, both the consultants and ASA members report arange of time of less than 1 min to 5 min (mean � 1.7min for consultants, and mean � 2.3 min for ASA mem-bers). The consultants and ASA members both agree thatthe oropharynx should be scavenged with suction dur-ing oral procedures.
Surgery around the face, head, or neck can bring anignition source into proximity with an oxidizer-enrichedatmosphere, thereby creating a high-risk situation. Whenmonitored anesthesia care is considered for surgeryaround the face, head, or neck, the Task Force stronglyagrees that two specific factors should be considered:(1) the required depth of sedation and (2) oxygen de-pendence. The Task Force agrees that a sealed gas deliv-ery device (e.g., cuffed tracheal tube or laryngeal mask)should be considered if moderate or deep sedation isrequired or used, or if the patient exhibits oxygendependence. If neither factor is present, an open gasdelivery device (e.g., facemask or nasal cannula) may beconsidered. If an open gas delivery system is used, theTask Force agrees that before an ignition source is acti-vated around the face, head, or neck, the surgeon shouldgive the adequate notice that the ignition source will beactivated. The anesthesiologist should (1) stop the deliv-ery of supplemental oxygen or reduce the delivery to theminimum required to avoid hypoxia, and (2) wait a fewminutes between decreasing the flow of supplementaloxygen and approving the activation of the ignitionsource. In the unlikely event of nitrous oxide deliverywith an open system (e.g., facemask or nasal cannula),the Task Force agrees that the anesthesiologist should(1) stop the delivery of nitrous oxide, and (2) wait a fewminutes between stopping the nitrous oxide and approv-ing the activation of the ignition source.
Advisory Statements. To the extent that is medicallyappropriate, the following basic principles should beapplied to the management of oxidizers, ignitionsources, and fuels:
● The anesthesiologist should collaborate with all mem-bers of the procedure team throughout the procedure
Table 1. Operating Room Fire Equipment and Supplies ThatShould Be Immediately Available*
Several containers of sterile salineA CO2 fire extinguisherReplacement tracheal tubes, guides, facemasksRigid laryngoscope blades; this may include a rigid fiberoptic laryngoscopeReplacement airway breathing circuits and linesReplacement drapes, sponges
* Some facilities or locations may benefit from assembling a portable cartcontaining equipment and supplies that expedite the immediate response toan operating room fire. The contents of such a cart will vary depending onlocal conditions and resources. If the items needed for an immediate re-sponse to an operating room fire are already available, there may be no addedbenefit to assembling a portable cart.
CO2 � carbon dioxide.
791PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

to minimize the presence of an oxidizer-enriched at-mosphere in proximity to an ignition source.
● Surgical drapes should be configured to minimize theaccumulation of oxidizers (oxygen and nitrous oxide)under the drapes and from flowing into the surgical site.
● Flammable skin prepping solutions should be dry be-fore draping.
● Gauze and sponges should be moistened when used inproximity to an ignition source.
For high-risk procedures, the anesthesiologist shouldnotify the surgeon whenever there is a potential for anignition source to be in proximity to an oxidizer-en-riched atmosphere or when there is an increase in oxi-dizer concentration at the surgical site. Any reduction insupplied oxygen to the patient should be assessed bymonitoring (1) pulse oximetry and, if feasible, (2) in-spired, exhaled, and/or delivered oxygen concentration.
For laser procedures, a laser-resistant tracheal tubeshould be used, and the tube should be chosen to beresistant to the laser used for the procedure (e.g., carbondioxide [CO2], Nd:YAG, Ar, Er:YAG, KTP). The trachealcuff of the laser tube should be filled with saline andcolored with an indicator dye such as methylene blue.Before activating a laser, the surgeon should give theanesthesiologist adequate notice that the ignition sourceis about to be activated. The anesthesiologist should (1)reduce the delivered oxygen concentration to the mini-mum required to avoid hypoxia, (2) stop the use ofnitrous oxide, and (3) wait a few minutes after reducingthe oxidizer-enriched atmosphere before approving ac-tivation of the laser.
For cases involving an ignition source and surgeryinside the airway, cuffed tracheal tubes should be usedwhen clinically appropriate. The anesthesiologist shouldadvise the surgeon against entering the trachea with anignition source (e.g., electrosurgery unit). Before activat-ing an ignition source inside the airway, the surgeonshould give the anesthesiologist adequate notice that theignition source is about to be activated. The anesthesi-ologist should (1) reduce the delivered oxygen concen-tration to the minimum required to avoid hypoxia, (2)stop the use of nitrous oxide, and (3) wait a few minutesafter reducing the oxidizer-enriched atmosphere beforeapproving the activation of the ignition source. In somecases (e.g., surgery in the oropharynx), scavenging withsuction may be used to reduce oxidizer enrichment inthe operative field.
For cases involving moderate or deep sedation, anignition source, and surgery around the face, head, orneck, the anesthesiologist and surgeon should develop aplan that accounts for the level of sedation and thepatient’s need for supplemental oxygen.
● If moderate or deep sedation is required or used, or ifthe patient exhibits oxygen dependence, the anesthe-siologist and surgeon should consider a sealed gas
delivery device (e.g., cuffed tracheal tube or laryngealmask).
● If moderate or deep sedation is not required, and thepatient does not exhibit oxygen dependence, an opengas delivery device (e.g., facemask or nasal cannula)may be considered. Before activating an ignitionsource around the face, head, or neck, the surgeonshould give the anesthesiologist adequate notice thatthe ignition source is about to be activated. The anes-thesiologist should (1) stop the delivery of supplemen-tal oxygen or reduce the delivered oxygen concentra-tion to the minimum required to avoid hypoxia, and(2) wait a few minutes after reducing the oxidizer-enriched atmosphere before approving the activationof the ignition source.
V. Management of OR FiresManagement of OR fires includes (1) recognizing the
early signs of fire, (2) halting the procedure, (3) makingappropriate attempts to extinguish the fire, (4) followingan evacuation protocol when medically appropriate, and(5) delivering postfire care to the patient.
Case reports indicate that early signs of a fire mayinclude a flame or flash, unusual sounds, odors, smoke,or heat.22–24,41,42,46,53,62,73,92 [Category B3 evidence.]One case report indicates that removing the trachealtube and stopping the flow of oxygen can minimizepatient injury.53 [Category B3 evidence.] One case re-port demonstrated that pouring saline into the patient’stracheal tube was effective in extinguishing the fire.93
[Category B3 evidence.] One case of a patient deathfrom an OR fire indicated that fire extinguishers wereavailable but not used by the OR staff on the patient.7
When early warning signs of a fire are noted, theconsultants and ASA members strongly agree that thereshould be an immediate halt to the procedure. When afire is definitely present, the consultants and ASA mem-bers strongly agree that there should be an immediateannouncement of fire, followed by an immediate halt tothe procedure.
For a fire in the airway or breathing circuit, theconsultants and ASA members strongly agree that, asquickly as possible, the tracheal tube should be removedand all flammable and burning materials should be re-moved from the airway. The consultants strongly agreeand ASA members agree that the delivery of all airwaygases should stop, and they both agree that saline shouldbe poured into the patient’s airway to extinguish anyresidual embers and cool the tissues.
For a fire elsewhere on or in the patient, the consult-ants agree and ASA members are equivocal regardingwhether the delivery of all airway gases should stop.They both strongly agree that all burning and flammablematerials (including all drapes) should be removed fromthe patient, and that all burning materials in, on, or
792 PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

around the patient should be extinguished (e.g., withsaline, water, or a fire extinguisher).
Seventy-one percent of the consultants and 77% of theASA members indicated that the preferred means forsafely responding to an OR fire is for each team memberto immediately perform a fire management task in apredetermined sequence. Twenty-nine percent of theconsultants and 23% of the ASA members indicated thatthe preferred means of safely responding to an OR fire isfor each team member to immediately perform a preas-signed task, without waiting for others to act. The TaskForce believes that a predetermined sequence of taskscan be attempted when a fire occurs, but that teammembers should not wait for each other if there areimpediments to following the predetermined sequenceof tasks in a rapid manner. The Task Force agrees thata team member who has completed a preassigned taskmay assist another team member whose task is not yetcomplete.
If the first attempt to extinguish the fire in, on, oraround the patient is not successful, the consultants andASA members both agree that a CO2 fire extinguishershould be used. If fire persists after use of a CO2 fireextinguisher, consultants and ASA members bothstrongly agree that the fire alarm should be activated andthe patient should be evacuated, if feasible. The consult-ants and ASA members both agree that the door to theroom should be closed and not reopened. The consult-ants strongly agree and the ASA members agree that themedical gas supply to the room should be turned offafter evacuation.
The consultants and ASA members strongly agree thatafter a fire has been extinguished, the patient’s statusshould be assessed and a plan should be devised forongoing care of the patient. When an airway or breath-ing circuit fire has been extinguished, consultants andASA members both agree that ventilation should be re-established, avoiding supplemental oxygen and nitrousoxide, if possible. Both the consultants and ASA mem-bers strongly agree that the tracheal tube should beexamined to assess whether fragments have been leftbehind in the airway. The consultants strongly agree andthe ASA members agree that rigid bronchoscopy shouldbe considered to assess thermal injury, look for trachealtube fragments, and aid in the removal of residual mate-rials. If the fire did not involve the airway and the patient
was not intubated before the fire, the consultants andASA members both strongly agree that the patient shouldbe assessed for injury related to smoke inhalation.
Advisory Statements. When an early warning sign isnoted, halt the procedure and call for an evaluation offire. Early signs of a fire may include unusual sounds (e.g.,a “pop,” “snap,” or “foomp”), unusual odors, unex-pected smoke, unexpected heat, unexpected movementof drapes, discoloration of drapes or breathing circuit,unexpected patient movement or complaint, and unex-pected flash or flame.
When a fire is definitely present, immediately an-nounce the fire, halt the procedure, and initiate firemanagement tasks.
Team members should perform their preassigned firemanagement tasks as quickly as possible. Before theprocedure, the team may identify a predetermined orderfor performing the tasks. If a team member cannot rap-idly perform his or her task in the predetermined order,other team members should perform their tasks withoutwaiting. When a team member has completed a preas-signed task, he or she should help other members per-form tasks that are not yet complete.
The following lists are shown in an order that the teammay wish to consider in its discussion of a predeter-mined sequence.
For a fire in the airway or breathing circuit, as fast aspossible:#
● Remove the tracheal tube.● Stop the flow of all airway gases.● Remove all flammable and burning materials from the
airway.● Pour saline or water into the patient’s airway.
For a fire elsewhere on or in the patient, as fast aspossible:
● Stop the flow of all airway gases.● Remove all drapes, flammable, and burning materials
from the patient.● Extinguish all burning materials in, on and around the
patient (e.g., with saline, water, or smothering).
If the airway or breathing circuit fire is extinguished:
● Reestablish ventilation by mask, avoiding supplemen-tal oxygen and nitrous oxide, if possible.
● Extinguish and examine the tracheal tube to assesswhether fragments were left in the airway. Considerbronchoscopy (preferably rigid) to look for trachealtube fragments, assess injury, and remove residual de-bris.
● Assess the patient’s status and devise a plan for ongo-ing care.
If the fire elsewhere on or in the patient isextinguished:
# Some experts and educators recommend an initial step that involves twosimultaneous actions: removal of the tracheal tube and stopping the flow ofmedical gases (e.g., by disconnecting the breathing circuit at the Y-piece or theinspiratory gas limb). The intent is to prevent a “blowtorch” effect caused bycontinued gas flow through a burning tracheal tube. This “blowtorch” effect canspread fire to other locations on or near the patient, and may cause additionalburns on the patient or other members of the OR team. The Task Force hascarefully considered this concern and agrees that these simultaneous actionsrepresent an ideal response. However, the Task Force is concerned that, in actualpractice, the simultaneous actions may be difficult to accomplish or may result indelay when one team member waits for another. Therefore, the Task Forcerecommends that the actions take place as fast as possible.
793PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

● Assess the patient’s status and devise a plan for ongo-ing care of the patient.
● Assess for smoke inhalation injury if the patient wasnot intubated.
If the fire is not extinguished after the first attempt(e.g., after performing the preassigned tasks):
● Use a CO2 fire extinguisher in, on, or around the patient.● If the fire persists after use of the CO2 fire extinguisher:
- Activate the fire alarm.- Evacuate the patient if feasible, following institu-
tional protocols.- Close the door to the room to contain the fire, and
do not reopen it or attempt to reenter the room.- Turn off the medical gas supply to the room.
Follow local regulatory reporting requirements (e.g.,report fires to your local fire department and state de-partment of health). Treat every fire as an adverse event,following your institutional protocol.
References
1. Barnes AM, Frantz RA: Do oxygen-enriched atmospheres exist beneathsurgical drapes and contribute to fire hazard potential in the operating room?AANA J 2000; 68:153–61
2. McCranie J: Fire safety in the operating room. Todays OR Nurse 1994;16:33–7
3. Milliken RA, Bizzarri A: Flammable surgical drapes. Anesth Analg 1985;64:54–7
4. Wolf GL: Danger from OR fires still a serious problem: ASA Panel reportsrisks. J Clin Monit Comput 2000; 16:237–8
5. Surgical fire safety. Health Devices 2006; 35:45–666. Use of wrong gas in laparoscopic insufflator causes fire. Health Devices
1994; 23:456–77. Stouffer DJ: Fires during surgery: Two fatal incidents in Los Angeles. J Burn
Care Rehabil 1992; 13:114–78. Halstead MA: Fire drill in the operating room: Role playing as a learning tool.
AORN J 1993; 58:697–7069. Laser ignition of surgical drapes. Health Devices 1992; 21:15–610. Surgical drapes. Health Devices 1986; 15:111–3611. Epstein RH, Brummett RR Jr, Lask GP: Incendiary potential of the flash-
lamp pumped 585-nm tunable dye laser. Anesth Analg 1990; 71:171–512. Wolf GL, Sidebotham GW, Lazard JLP, Charchaflieh JG: Laser ignition of
surgical drape materials in air, 50% oxygen, and 95% oxygen. ANESTHESIOLOGY
2004; 100:1167–7113. Treyve E, Yarington CT Jr, Thompson GE: Incendiary characteristics of
endotracheal tubes with the CO2 laser. Ann Otol Rhinol Laryngol 1981; 90:328–30
14. Greco RJ, Gonzalez R, Johnson P, Scolieri M, Rekhopf PG, Heckler F:Potential dangers of oxygen supplementation during facial surgery. Plast Recon-str Surg 1995; 95:978–84
15. Neatrour GP, Lederman IR: Reducing fire hazard during ophthalmic sur-gery by using compressed air. Ophthalmic Surg 1989; 20:430–2
16. Aly A, McIlwain M, Duncavage JA: Electrosurgery-induced endotrachealtube ignition during tracheotomy. Ann Otol Rhinol Laryngol 1991; 100:31–3
17. Airway fires during surgery. PA-PSRS Patient Safety Advisory 2007; 4:1–418. Case history number 82: “Nonflammable” fires in the operating room.
Anesth Analg 1975; 54:152–419. Surgical fire case summaries. Health Devices 1992; 21:31–420. Ashcraft KE, Golladay ES, Guinee WS: A surgical field flash fire during the
separation of dicephalus dipus conjoined twins. ANESTHESIOLOGY 1981; 55:457–821. Awan MS, Ahmed I: Endotracheal tube fire during tracheostomy: A case
report. Ear Nose Throat J 2002; 81:90–222. Bailey MK, Bromley HR, Allison JG, Conroy JM, Krzyzaniak W: Electrocau-
tery-induced airway fire during tracheostomy. Anesth Analg 1990; 71:702–423. Barker SJ, Polson JS: Fire in the operating room: A case report and
laboratory study. Anesth Analg 2001; 93:960–524. Baur DA, Butler RC: Electrocautery-ignited endotracheal tube fire: Case
report. Br J Oral Maxillofac Surg 1999; 37:142–325. Bennett JA, Agree M: Fire in the chest. Anesth Analg 1994; 78:406
26. Boyd CH: A fire in the mouth: A hazard of the use of antistatic endotrachealtubes. Anaesthesia 1969; 24:441–6
27. Burgess GE III, LeJeune FE Jr: Endotracheal tube ignition during lasersurgery of the larynx. Arch Otolaryngol 1979; 105:561–2
28. Casey KR, Fairfax WR, Smith SJ, Dixon JA: Intratracheal fire ignited by theNd-YAG laser during treatment of tracheal stenosis. Chest 1983; 84:295–6
29. Chang BW, Petty P, Manson PN: Patient fire safety in the operating room.Plast Reconstr Surg 1994; 93:519–21
30. Cozine K, Rosenbaum LM, Askanazi J, Rosenbaum SH: Laser-inducedendotracheal tube fire. ANESTHESIOLOGY 1981; 55:583–5
31. Datta TD: Flash fire hazard with eye ointment. Anesth Analg 1984; 63:700–1
32. Dini GM, Casagrande W: Misfortune during a blepharoplasty. Plast Recon-str Surg 2006; 117:325–6
33. Eade GG: Hazard of nasal oxygen during aesthetic facial operations. PlastReconstr Surg 1986; 78:539
34. Galapo S, Wolf GL, Sidebotham GW, Cohen D: Laser ignition of surgicaldrapes in an oxygen enriched atmosphere (abstract). ANESTHESIOLOGY 1998; 89:A580
35. Gunatilake DE: Case report: Fatal intraperitoneal explosion during elec-trocoagulation via laparoscopy. Int J Gynaecol Obstet 1978; 15:353–7
36. Handa KK, Bhalla AP, Arora A: Fire during the use of Nd-Yag laser. IntJ Pediatr Otorhinolaryngol 2001; 60:239–42
37. Hirshman CA, Smith J: Indirect ignition of the endotracheal tube duringcarbon dioxide laser surgery. Arch Otolaryngol 1980; 106:639–41
38. Howard BK, Leach JL: Prevention of flash fires during facial surgeryperformed under local anesthesia. Ann Otol Rhinol Laryngol 1997; 106:248–51
39. Katz JA, Campbell L: Fire during thoracotomy: A need to control theinspired oxygen concentration. Anesth Analg 2005; 101:612
40. Keller C, Elliott W, Hubbell RN: Endotracheal tube safety during electro-dissection tonsillectomy. Arch Otolaryngol Head Neck Surg 1992; 118:643–5
41. Krawtz S, Mehta AC, Wiedemann HP, DeBoer G, Schoepf KD, Tomasze-wski MZ: Nd-YAG laser-induced endobronchial burn: Management and long-termfollow-up. Chest 1989; 95:916–8
42. Lach E: The hazards of using supplemental oxygen. Plast Reconstr Surg1996; 98:566–7
43. Lai A, Ng KP: Fire during thoracic surgery. Anaesth Intensive Care 2001;29:301–3
44. Le Clair J, Gartner S, Halma G: Endotracheal tube cuff ignited by electro-cautery during tracheostomy. AANA J 1990; 58:259–61
45. Lederman IR: Fire hazard during ophthalmic surgery. Ophthalmic Surg1985; 16:577–8
46. Lew EO, Mittleman RE, Murray D: Endotracheal tube ignition by electro-cautery during tracheostomy: Case report with autopsy findings. J Forensic Sci1991; 36:1586–91
47. Lypson ML, Stephens S, Colletti L: Preventing surgical fires: Who needs tobe educated? Jt Comm J Qual Patient Saf 2005; 31:522–7
48. Magruder GB, Guber D: Fire prevention during surgery. Arch Ophthalmol1970; 84:237
49. Mandych A, Mickelson S, Amis R: Operating room fire. Arch OtolaryngolHead Neck Surg 1990; 116:1452
50. Marsh B, Riley RH: Double-lumen tube fire during tracheostomy. ANESTHE-SIOLOGY 1992; 76:480–1
51. Martin L, Dolman P: Fire! Can J Anaesth 1999; 46:90952. Meyers A: Complications of CO2 laser surgery of the larynx. Ann Otol
Rhinol Laryngol 1981; 90:132–453. Michels AM, Stott S: Explosion of tracheal tube during tracheostomy.
Anaesthesia 1994; 49:110454. Ng JM, Hartigan PM: Airway fire during tracheostomy: Should we extu-
bate? ANESTHESIOLOGY 2003; 98:130355. Ortega RA: A rare cause of fire in the operating room. ANESTHESIOLOGY 1998;
89:160856. Pashayan AG, Gravenstein JS: Airway fires during surgery with the carbon
dioxide laser. ANESTHESIOLOGY 1989; 71:47857. Paugh DH, White KW: Fire in the operating room during tracheotomy: A
case report. AANA J 2005; 73:97–10058. Reyes RJ, Smith AA, Mascaro JR, Windle BH: Supplemental oxygen: Ensur-
ing its safe delivery during facial surgery. Plast Reconstr Surg 1995; 95:924–859. Robinson JS, Thompson JM, Wood AW: Fire and explosion hazards in
operating theatres: A reply and new evidence. Br J Anaesth 1979; 51:90860. Rogers ML, Nickalls RW, Brackenbury ET, Salama FD, Beattie MG, Perks
AG: Airway fire during tracheostomy: Prevention strategies for surgeons andanaesthetists. Ann R Coll Surg Engl 2001; 83:376–80
61. Santos P, Ayuso A, Luis M, Martinez G, Sala X: Airway ignition during CO2
laser laryngeal surgery and high frequency jet ventilation. Eur J Anaesth 2000;17:204–7
62. Schettler WH: Operating room flash fire. Anesth Analg 1974; 53:288–963. Simpson JI, Wolf GL: Endotracheal tube fire ignited by pharyngeal elec-
trocautery. ANESTHESIOLOGY 1986; 65:76–764. Singla AK, Campagna JA, Wright CD, Sandberg WS: Surgical field fire
during a repair of bronchoesophageal fistula. Anesth Analg 2005; 100:1062–465. Thompson JW, Colin W, Snowden T, Hengesteg A, Stocks RM, Watson SP:
Fire in the operating room during tracheostomy. South Med J 1998; 91:243–7
794 PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

66. Varcoe RL, MacGowan KM, Cass AJ: Airway fire during tracheostomy. ANZJ Surg 2004; 74:507–8
67. Waldorf HA, Kauvar NB, Geronemus RG, Leffel DJ: Remote fire with thepulsed dye laser: Risk and prevention. J Am Acad Dermatol 1996; 34:503–6
68. Wegrzynowicz ES, Jensen NF, Pearson KS, Wachtel RE, Scamman FL:Airway fire during jet ventilation for laser excision of vocal cord papillomata.ANESTHESIOLOGY 1992; 76:468–9
69. Fire hazard created by the misuse of DuraPrep solution. Health Devices1998;27:400–2
70. Hurt TL, Schweich PJ: Do not get burned: Preventing iatrogenic fires andburns in the emergency department. Pediatr Emerg Care 2003; 19:255–9
71. Prasad R, Quezado Z, St. Andre A: Fires in the operating room andintensive care unit: Awareness is the key to prevention. Anesth Analg 2006;102:172–4
72. Shah SC: Operating room flash fire. Anesth Analg 1974; 53:28873. Tooher R, Maddern GJ, Simpson J: Surgical fires and alcohol-based skin
preparations. ANZ J Surg 2004; 74:382–574. Laser contact tips and tracheal tubes. Health Devices 1992; 21:1875. Ossoff RH, Duncavage JA, Eisenman TS, Duncavage JA, Karlan MS: Com-
parison of tracheal damage from laser-ignited endotracheal tube fires. Ann OtolRhinol Laryngol 1983; 92:333–6
76. Patel KF, Hicks JN: Prevention of fire hazards associated with use ofcarbon dioxide lasers. Anesth Analg 1981; 60:885–8
77. Simpson JI, Schiff GA, Wolf GL: The effect of helium on endotracheal tubeflammability. ANESTHESIOLOGY 1990; 73:538–40
78. Sosis MB, Braverman B: Evaluation of foil coverings for protecting plasticendotracheal tubes from the potassium-titanyl-phosphate laser. Anesth Analg1993; 77:589–91
79. Sosis MB, Braverman B: Prevention of cautery-induced airway fires withspecial endotracheal tubes. Anesth Analg 1993; 77:846–7
80. Sosis MB, Braverman B, Caldarelli DD: Evaluation of a new laser-resistantfabric and copper foil-wrapped endotracheal tube. Laryngoscope 1996; 106:842–4
81. Sosis MB, Caldarelli D: Evaluation of a new ceramic endotracheal tube forlaser airway surgery. Otolaryngol Head Neck Surg 1992; 107:601–2
82. Sosis MB, Dillon FX: A comparison of CO2 laser ignition of the Xomed,plastic, and rubber endotracheal tubes. Anesth Analg 1993; 76:391–3
83. Sosis MB, Heller S: Evaluation of five metallic tapes for protection ofendotracheal tubes during CO2 laser surgery. Anesth Analg 1989; 68:392–3
84. Sosis MB: Which is the safest endotracheal tube for use with the CO2 laser?A comparative study. J Clin Anesth 1992; 4:217–9
85. Gupte SR: Gauze fire in the oral cavity: A case report. Anesth Analg 1972;51:645–6
86. Healy GB, Strong MS, Shapshay S, Vaughan C, Jako G: Complications ofCO2 laser surgery of the aerodigestive tract: Experience of 4416 cases. Otolar-yngol Head Neck Surg 1984; 92:13–8
87. Tysinger JW Jr: Weck-Cel sponges and Steri-Drapes burn. Ophthalmic Surg1986; 17:174.
88. Do pledgets protect the tracheal tube cuff from lasers? Health Devices1992;21:17
89. Axelrod EH, Kusnetz AB, Rosenberg MK: Operating room fires initiated byhot wire cautery. ANESTHESIOLOGY 1993; 79:1123–6
90. Macdonald MR, Wong A, Walker P, Crysdale WS: Electrocautery-inducedignition of tonsillar packing. J Otolaryngol 1994; 23:426–9
91. Rohrich RJ, Gyimesi IM, Clark P, Burns AJ: CO2 laser safety considerationsin facial skin resurfacing. Plast Reconstr Surg 1997; 100:1285–90
92. Anderson EF: A potential ignition source in the operating room. AnesthAnalg 1976; 55:217–8
93. Chee WK, Benumof JL: Airway fire during tracheostomy: Extubation maybe contraindicated. ANESTHESIOLOGY 1998; 89:1576–8
Appendix 1: Primary Findings of theAdvisory Task Force
I. Education
● All anesthesiologists should have fire safety education, specifically forOR fires, with emphasis on the risk created by an oxidizer-enrichedatmosphere.
II. OR Fire Drills
● Anesthesiologists should periodically participate in OR fire drills,with the entire OR team. This formal rehearsal should take placeduring dedicated educational time, not during patient care.
III. Preparation
● For every case, the anesthesiologist should participate with the entireOR team (e.g., during the surgical pause) in assessing and determin-ing whether a high-risk situation exists.
● If a high-risk situation exists, all team members—including the anes-thesiologist—should take a joint and active role in agreeing on howa fire will be prevented and managed.
● Each team member should be assigned a specific fire managementtask to perform in the event of a fire (e.g., removing the tracheal tube,turning off the airway gases).
● Each team member should understand that his or her preassignedtask should be performed immediately if a fire occurs, withoutwaiting for another team member to take action.
● When a team member has completed a preassigned task, he or sheshould help other team members perform tasks that are not yetcomplete.
● In every OR and procedure area where a fire triad can exist (i.e., anoxidizer-enriched atmosphere, an ignition source, and fuel), an easilyvisible protocol for the prevention and management of fires shouldbe displayed.
● Equipment for managing a fire should be readily available in everyprocedural location where a fire triad may exist.
IV. Prevention
● The anesthesiologist should collaborate with all members of the proce-dure team throughout the procedure to minimize the presence of anoxidizer-enriched atmosphere in proximity to an ignition source.
● For all procedures:- Surgical drapes should be configured to minimize the accumula-
tion of oxidizers (oxygen and nitrous oxide) under the drapes andfrom flowing into the surgical site.
- Flammable skin prepping solutions should be dry before draping.- Gauze and sponges should be moistened before use in proximity to
an ignition source.
● For high-risk procedures:- The anesthesiologist should notify the surgeon whenever there is
a potential for an ignition source to be in proximity to an oxidizer-enriched atmosphere or when there is an increase in oxidizerconcentration at the surgical site.
- Any reduction in supplied oxygen to the patient should be assessedby monitoring (1) pulse oximetry and, if feasible, (2) inspired,exhaled, and/or delivered oxygen concentration.
● For laser procedures:- A laser-resistant tracheal tube should be used.
▪ The laser-resistant tracheal tube used should be chosen to beresistant to the laser used for the procedure (e.g., CO2, Nd:YAG,Ar, Er:YAG, KTP).
- The tracheal cuff of the laser tube should be filled with saline andcolored with an indicator dye such as methylene blue.
- Before activating a laser:▪ The surgeon should give the anesthesiologist adequate notice
that the laser is about to be activated.▪ The anesthesiologist should:
� Reduce the delivered oxygen concentration to the minimumrequired to avoid hypoxia.
� Stop the use of nitrous oxide.� Wait a few minutes after reducing the oxidizer-enriched atmo-
sphere before approving activation of the laser.
● For cases involving an ignition source and surgery inside the airway:- Cuffed tracheal tubes should be used when clinically appropriate.- The anesthesiologist should advise the surgeon against entering the
trachea with an ignition source (e.g., electrosurgery unit).- Before activating an ignition source inside the airway:
795PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

▪ The surgeon should give the anesthesiologist adequate noticethat the ignition source is about to be activated.
▪ The anesthesiologist should:� Reduce the delivered oxygen concentration to the minimum
required to avoid hypoxia.� Stop the use of nitrous oxide.� Wait a few minutes after reducing the oxidizer-enriched atmo-
sphere before approving the activation of the ignition source.- In some cases (e.g., surgery in the oropharynx), scavenging with
suction may be used to reduce oxidizer enrichment in the opera-tive field.
● For cases involving moderate or deep sedation, an ignition source,and surgery around the face, head, or neck:- The anesthesiologist and surgeon should develop a plan that accounts
for the level of sedation and the patient’s need for supplementaloxygen.▪ If moderate or deep sedation is required or used, or if the patient
exhibits oxygen dependence, the anesthesiologist and surgeonshould consider a sealed gas delivery device (e.g., cuffed trachealtube or laryngeal mask).
▪ If moderate or deep sedation is not required, and the patientdoes not exhibit oxygen dependence, an open gas deliverydevice (e.g., facemask or nasal cannula) may be considered.
- Before activating an ignition source around the face, head, or neck:▪ The surgeon should give the anesthesiologist adequate notice
that the ignition source is about to be activated.▪ The anesthesiologist should:
� Stop the delivery of supplemental oxygen or reduce the deliv-ered oxygen concentration to the minimum required to avoidhypoxia.
� Wait a few minutes after reducing the oxidizer-enriched atmo-sphere before approving the activation of the ignition source.
V. Management of OR Fires
● When an early warning sign is noted, halt the procedure and call foran evaluation of fire.
● When a fire is definitely present, immediately announce the fire, haltthe procedure, and initiate fire management tasks.
● Team members should perform their preassigned fire managementtasks as quickly as possible.- Before the procedure, the team may identify a predetermined
order for performing the tasks.- If a team member cannot rapidly perform his or her task in the
predetermined order, other team members should perform theirtasks without waiting.
- When a team member has completed a preassigned task, he or sheshould help other members perform tasks that are not yet com-plete.
● For a fire in the airway or breathing circuit, as fast as possible:- Remove the tracheal tube.- Stop the flow of all airway gases.- Remove all flammable and burning materials from the airway.- Pour saline or water into the patient’s airway.
● For a fire elsewhere on or in the patient, as fast as possible:- Stop the flow of all airway gases.- Remove all drapes, flammable, and burning materials from the
patient.- Extinguish all burning materials in, on, and around the patient (e.g.,
with saline, water, or smothering).
● If the airway or breathing circuit fire is extinguished:
- Reestablish ventilation by mask, avoiding supplemental oxygenand nitrous oxide, if possible.
- Extinguish and examine the tracheal tube to assess whether frag-ments were left in the airway.▪ Consider bronchoscopy (preferably rigid) to look for tracheal
tube fragments, assess injury, and remove residual debris.- Assess the patient’s status and devise a plan for ongoing care.
● If the fire elsewhere on or in the patient is extinguished:- Assess the patient’s status and devise a plan for ongoing care of the
patient.- Assess for smoke inhalation injury if the patient was not intubated.
● If the fire is not extinguished after the first attempt (e.g., afterperforming the preassigned tasks):- Use a CO2 fire extinguisher in, on, or around the patient.- If the fire persists after use of the CO2 fire extinguisher:
▪ Activate the fire alarm.▪ Evacuate the patient if feasible, following institutional protocols.▪ Close the door to the room to contain the fire and do not reopen
it or attempt to reenter the room.▪ Turn off the medical gas supply to the room.
● Follow local regulatory reporting requirements (e.g., report fires toyour local fire department and state department of health).
● Treat every fire as an adverse event, following your institutionalprotocol.
Appendix 2: Methods and Analyses
A. State of the LiteratureFor this Advisory, a literature review was used in combination with
opinions obtained from experts and other sources (e.g., professionalsociety members, open forums, Web-based postings) to provide guid-ance to practitioners regarding OR fire prevention and management.Both the literature review and opinion data were based on evidencelinkages, or statements regarding potential relationships between fireprevention and management interventions and OR fire outcomes.**The evidence linkage interventions are listed below.
I. Education
1. Fire safety education, with an emphasis on an oxidizer-enrichedatmosphere
II. OR Fire Drills
2. Periodic participation in OR fire drills
III. Preparation
3. Display of an easily visible protocol for the prevention and man-agement of fires
4. Preoperative determination of a high-risk situation5. OR team discussion of OR fire strategy
IV. Prevention
6. Surgical drape configuration to minimize the accumulation ofoxidizers
7. Drying of flammable skin prepping solutions8. Moistening of sponges and gauze when used in proximity to an
ignition source9. Reducing the concentration of supplied oxygen for high-risk pro-
cedures10. Avoidance of nitrous oxide for high-risk procedures
** Unless otherwise specified, outcomes for the listed interventions refer to theoccurrence of fire or adverse sequela.
796 PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

11. Cuffed versus uncuffed tracheal tubes for cases in or around theairway
12. Insufflating with medical air during cases in or around the airway13. Scavenging with suction during cases in or around the airway14. Laser-resistant versus non–laser-resistant tracheal tubes during la-
ser surgery15. Filling the tracheal cuff of the laser tube with saline colored with
an indicator dye
V. Management
16. Early signs of a fire include a flame or flash, unusual sounds, odors,smoke, or heat (observational)
17. Removing the tracheal tube and stopping the flow of oxygen tominimize patient injury after an airway or breathing circuit fire
18. Pouring saline into the patient’s tracheal tube to extinguish anairway fire
For the literature review, potentially relevant studies were identifiedvia electronic and manual searches of the literature. The literaturesearch covered a 56-yr period from 1952 through 2007. More than 400citations were initially identified, yielding a total of 340 articles thataddressed topics related to the evidence linkages and met our criteriafor inclusion. After review of the articles, 240 studies did not providedirect evidence and were subsequently eliminated. A total of 100articles contained direct linkage-related evidence.†† No evidence link-age contained enough studies with well-defined experimental designsand statistical information to conduct a quantitative analysis (i.e., meta-analysis).
Interobserver agreement among Task Force members and two meth-odologists was established by interrater reliability testing. Agreementlevels using a � statistic for two-rater agreement pairs were as follows:
(1) type of study design, � � 0.63–0.82; (2) type of analysis, � �0.40–0.87; (3) evidence linkage assignment, � � 0.84–1.00; and (4)literature inclusion for database, � � 0.69–1.00. Three-rater chance-corrected agreement values were (1) study design, Sav � 0.69, Var(Sav) � 0.013; (2) type of analysis, Sav � 0.57, Var (Sav) � 0.031; (3)linkage assignment, Sav � 0.89, Var (Sav) � 0.004; and (4) literaturedatabase inclusion, Sav � 0.79, Var (Sav) � 0.025. These valuesrepresent moderate to high levels of agreement.
B. Consensus-based EvidenceConsensus was obtained from multiple sources, including (1) survey
opinion from consultants who were selected based on their knowledgeor expertise in OR fire prevention and management, (2) survey opin-ions solicited from active members of the ASA, (3) testimony fromattendees of a publicly held open forum at a national anesthesiameeting, (4) Internet commentary, and (5) Task Force opinion andinterpretation. The survey rate of return was 52% (n � 38 of 73) for theconsultants, and 64 surveys were received from active ASA members.Results of the surveys are reported in tables 2 and 3 and in the text ofthe Advisory.
The consultants were asked to indicate which, if any, of the evi-dence linkages would change their clinical practices if the Advisorywas instituted. The rate of return was 18% (n � 13 of 73). The percentof responding consultants expecting a change in their practice associ-ated with each linkage topic was as follows: (1) education, 77%; (2) ORfire drills, 69%; (3) team discussion of fire strategy, 69%; (4) minimizingor avoiding an oxidizer-enriched atmosphere near the surgical site,38%; (5) managing ignition sources, 38%; (6) managing fuels, 31%; (7)identification of a high-risk procedure, 85%; (8) management of ahigh-risk procedure, 31%; and (9) OR fire management, 77%. Eighty-five percent of the respondents indicated that the Advisory wouldhave no effect on the amount of time spent on a typical case, and15% indicated that there would be an increase of 1–5 min in theamount of time spent on a typical case with the implementation ofthis Advisory.
†† A complete list of references used to develop this Advisory is available onthe ANESTHESIOLOGY Web site, www.anesthesiology.org, or by writing to theAmerican Society of Anesthesiologists.
797PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

Table 2. Consultant Survey Responses
n‡StronglyAgree Agree Uncertain Disagree
StronglyDisagree
Education1a. Every anesthesiologist should have knowledge of institutional
fire safety protocols for the OR38 92.1* 7.9 0.0 0.0 0.0
1b. Every anesthesiologist should participate in OR fire safetyeducation
38 81.6* 15.8 2.6 0.0 0.0
1c. OR fire safety education for the anesthesiologist shouldemphasize the risk of an oxidizer-enriched atmosphere
38 81.6* 18.4 0.0 0.0 0.0
OR fire drills2a. All anesthesiologists should periodically participate in OR fire
drills with the entire OR team38 60.5* 31.6 5.3 2.6 0.0
2b. Participation in an OR fire drill should take place duringdedicated educational time, not during patient care
38 50.0* 34.2 5.3 10.5 0.0
Preparation3. Anesthesiologists should participate with the entire OR team in
assessing the risk of an OR fire for each case, and determiningwhether a high-risk situation exists
38 57.9* 29.0 2.6 10.5 0.0
4. All team members should agree on how an OR fire will beprevented and managed for each particular procedure
38 60.5* 29.0 7.9 2.6 0.0
5. Hospitals and procedure units should post a protocol for theprevention and management of fires in each location where aprocedure is performed
38 50.0* 26.3 18.4 5.3 0.0
Prevention for all procedures6. Flammable skin prepping solutions should be dry before
draping38 86.8* 13.2 0.0 0.0 0.0
7. Surgical drapes should be configured to prevent oxygen fromaccumulating under the drapes or from flowing into the surgicalsite
38 76.3* 18.4 2.6 2.6 0.0
8. Sponges should be moistened, particularly when used in ornear the airway
38 63.2* 15.8 21.0 0.0 0.0
Prevention for high-risk† procedures9. Anesthesiologists should collaborate with the procedure team
for the purpose of preventing and managing a fire38 84.2* 15.8 0.0 0.0 0.0
10. The surgeon should be notified of an increase in or thepresence of an oxidizer-enriched atmosphere in which anignition source will be used
38 84.2* 15.8 0.0 0.0 0.0
11a. Oxygen levels should be kept as low as clinically feasible whilethe ignition source is in proximity to the oxygen-enrichedatmosphere
38 81.6* 13.2 2.6 0.0 2.6
11b. The reduction of FIO2 should be guided by monitoring patientoxygenation
38 86.8* 7.9 5.3 0.0 0.0
12. The use of nitrous oxide should be avoided in settings that areconsidered high risk for OR fire
38 52.6* 26.3 15.8 5.3 0.0
13. Oxygen or nitrous oxide buildup may be minimized by eitherinsufflating with room air or scavenging the operating field withsuction
38 50.0* 36.8 10.5 2.6 0.0
Prevention during cases in or around the airway14. Cuffed tracheal tubes should be used instead of uncuffed
tracheal tubes38 39.5 31.6* 23.7 5.2 0.0
15. The oropharynx should be scavenged with suction during oralprocedures
38 42.1 23.7* 28.9 5.3 0.0
16. The sufficient amount of time needed to reduce oxygen ornitrous oxide concentrations to a safe level before using anignition source in the airway:
Mean � 1.76 min,Range � 0.25–5 min
17. The sufficient amount of time needed to reduce oxygen ornitrous oxide concentrations to a safe level before using anignition source for patients wearing a facemask or nasalcannula:
Mean � 1.67 min,Range � 0.15–5 min
Prevention during laser surgery18. Laser-resistant tracheal tubes appropriate to the procedure and
laser should be used38 68.4* 29.0 2.6 0.0 0.0
19a. Tracheal tube cuffs should be filled with saline rather than air,when feasible
38 71.1* 26.3 2.6 0.0 0.0
(continued)
798 PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

Table 2. Continued
n‡StronglyAgree Agree Uncertain Disagree
StronglyDisagree
19b. Saline in tracheal tube cuffs should be tinted with methyleneblue to act as a marker for cuff puncture by a laser
38 50.0* 39.5 10.5 0.0 0.0
Management of OR fires20. When early warning signs of a fire are noted, the procedure
should be halted immediately38 78.9* 15.8 5.3 0.0 0.0
21. When a fire is definitely present, the fire should be immediatelyannounced and the procedure should halt
38 92.1* 7.9 0.0 0.0 0.0
22. For a fire in the airway or breathing circuit:a. The tracheal tube should be removed as quickly as possible 38 78.9* 13.2 7.9 0.0 0.0b. All flammable and burning materials should be removed from
the airway as quickly as possible38 94.7* 5.3 0.0 0.0 0.0
c. The delivery of all airway gases should stop 38 73.7* 18.4 5.3 2.6 0.0d. Saline should be poured into the patient’s airway to
extinguish any residual embers and cool the tissues38 47.4 21.0* 21.0 7.9 2.6
23. For a fire elsewhere on or in the patient:a. The delivery of all airway gases should stop 38 47.4 13.1* 23.7 15.8 0.0b. All burning and flammable materials (including all drapes)
should be removed from the patient38 89.5* 10.5 0.0 0.0 0.0
c. All burning materials in, on and around the patient should beextinguished (e.g., with saline, water, or a fire extinguisher)
38 86.8* 13.2 0.0 0.0 0.0
24. The preferred means of safely responding to an OR fire is:a. For each team member to immediately respond without
waiting for others to actAgree � 29%
b. To immediately initiate a predetermined sequence ofresponses
Agree � 71%
25. If the first attempt to extinguish the fire is not successful, a CO2
fire extinguisher should be used38 39.5 39.5* 13.1 7.9 0.0
26. If the fire persists after use of a CO2 fire extinguisher:a. The fire alarm should be activated 38 79.0* 10.5 10.5 0.0 0.0b. The patient should be evacuated, if feasible 38 60.5* 34.2 5.3 0.0 0.0c. The door to the room should be closed and not reopened 38 47.4 23.7* 26.3 2.6 0.0d. The medical gas supply to the room should be turned off 38 60.5* 18.4 21.1 0.0 0.0
27. After a fire has been extinguished, the patient’s status should beassessed and a plan devised for ongoing care of the patient
38 84.2* 10.5 2.6 0.0 2.6
28. When the airway or breathing circuit fire has been extinguished:a. Ventilation should be reestablished, avoiding supplemental
oxygen and nitrous oxide, if possible38 47.4 31.6* 10.5 10.5 0.0
b. The tracheal tube should be examined to assess whetherfragments may be left behind in the airway
38 81.6* 18.4 0.0 0.0 0.0
c. Rigid bronchoscopy should be considered to assess thermalinjury and look for tracheal tube fragments and other residualmaterials
38 68.4* 23.7 5.3 0.0 2.6
29. If the fire did not involve the airway and the patient was notintubated before the fire, the patient should be assessed forinjury related to smoke inhalation
38 60.5* 36.8 2.7 0.0 0.0
* Median response falls within this designated response category. † A high-risk procedure is defined as one in which an ignition source may be in proximity toan oxidizer-enriched atmosphere. ‡ n is the number of consultants who responded to each item. All other numbers in the table represent the percentage ofconsultants who selected the designated response category.
CO2 � carbon dioxide; FIO2 � fraction of inspired oxygen; OR � operating room.
799PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

Table 3. ASA Member Survey Responses
n‡StronglyAgree Agree Uncertain Disagree
StronglyDisagree
Education1a. Every anesthesiologist should have knowledge of institutional
fire safety protocols for the OR142 74.6* 24.7 0.7 0.0 0.0
1b. Every anesthesiologist should participate in OR fire safetyeducation
142 55.6* 38.7 5.6 0.0 0.0
1c. OR fire safety education for the anesthesiologist shouldemphasize the risk of an oxidizer-enriched atmosphere
142 73.9* 22.5 3.5 0.0 0.0
OR fire drills2a. All anesthesiologists should periodically participate in OR fire
drills with the entire OR team142 42.3 40.1* 12.0 5.6 0.0
2b. Participation in an OR fire drill should take place duringdedicated educational time, not during patient care
142 54.9* 31.0 10.6 2.1 1.4
Preparation3. Anesthesiologists should participate with the entire OR team in
assessing the risk of an OR fire for each case, and determiningwhether a high-risk situation exists
142 38.7 45.8* 8.5 3.5 3.5
4. All team members should agree on how an OR fire will beprevented and managed for each particular procedure
142 39.4 38.0* 13.4 7.8 1.4
5. Hospitals and procedure units should post a protocol for theprevention and management of fires in each location where aprocedure is performed
142 51.4* 36.6 8.5 2.8 0.7
Prevention for all procedures6. Flammable skin prepping solutions should be dry before
draping142 68.3* 21.8 9.2 0.7 0.0
7. Surgical drapes should be configured to prevent oxygen fromaccumulating under the drapes or from flowing into the surgicalsite
142 64.8* 28.2 6.3 0.7 0.0
8. Sponges should be moistened, particularly when used in ornear the airway
142 63.4* 30.3 5.6 0.7 0.0
Prevention for high-risk† procedures9. Anesthesiologists should collaborate with the procedure team
for the purpose of preventing and managing a fire142 67.6* 31.0 1.4 0.0 0.0
10. The surgeon should be notified of an increase in or thepresence of an oxidizer-enriched atmosphere in which anignition source will be used
142 66.2* 29.6 3.5 0.7 0.0
11a. Oxygen levels should be kept as low as clinically feasible whilethe ignition source is in proximity to the oxygen-enrichedatmosphere
142 70.4* 26.1 2.1 1.4 0.0
11b. The reduction of FIO2 should be guided by monitoring patientoxygenation
142 71.8* 24.7 2.8 0.7 0.0
12. The use of nitrous oxide should be avoided in settings that areconsidered high risk for OR fire
142 50.0* 36.6 9.2 3.5 0.7
13. Oxygen or nitrous oxide buildup may be minimized by eitherinsufflating with room air or scavenging the operating field withsuction
142 32.4 43.0* 21.8 2.8 0.0
Prevention during cases in or around the airway14. Cuffed tracheal tubes should be used instead of uncuffed
tracheal tubes142 35.9 43.0* 16.2 4.9 0.0
15. The oropharynx should be scavenged with suction during oralprocedures
142 22.5 27.5* 44.4 5.6 0.0
16. The sufficient amount of time needed to reduce oxygen ornitrous oxide concentrations to a safe level before using anignition source in the airway:
Mean � 3.3 min,Range � 0.08–10
min17. The sufficient amount of time needed to reduce oxygen or
nitrous oxide concentrations to a safe level before using anignition source for patients wearing a facemask or nasalcannula:
Mean � 2.8 min,Range � 0.0–10 min
Prevention during laser surgery18. Laser-resistant tracheal tubes appropriate to the procedure and
laser should be used142 61.3* 35.9 2.8 0.0 0.0
19a. Tracheal tube cuffs should be filled with saline rather than air,when feasible
142 61.3* 33.1 4.9 0.7 0.0
(continued)
800 PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

Table 3. Continued
n‡StronglyAgree Agree Uncertain Disagree
StronglyDisagree
19b. Saline in tracheal tube cuffs should be tinted with methyleneblue to act as a marker for cuff puncture by a laser
142 44.4 37.3* 14.1 3.5 0.7
Management of OR fires20. When early warning signs of a fire are noted, the procedure
should be halted immediately142 78.2* 19.0 2.8 0.0 0.0
21. When a fire is definitely present, the fire should be immediatelyannounced and the procedure should halt
142 85.9* 12.7 1.4 0.0 0.0
22. For a fire in the airway or breathing circuit:a. The tracheal tube should be removed as quickly as possible 142 59.2* 26.1 8.4 4.2 2.1b. All flammable and burning materials should be removed from
the airway as quickly as possible142 73.9* 22.5 2.8 0.0 0.7
c. The delivery of all airway gases should stop 142 46.5 20.4* 16.9 14.1 2.1d. Saline should be poured into the patient’s airway to
extinguish any residual embers and cool the tissues142 33.1 29.6* 28.9 7.0 1.4
23. For a fire elsewhere on or in the patient:a. The delivery of all airway gases should stop 142 14.8 14.8 26.8* 39.4 4.2b. All burning and flammable materials (including all drapes)
should be removed from the patient142 74.7* 22.5 2.8 0.0 0.0
c. All burning materials in, on and around the patient should beextinguished (e.g., with saline, water, or a fire extinguisher)
142 73.2* 26.1 0.7 0.0 0.0
24. The preferred means of safely responding to an OR fire is:a. For each team member to immediately respond without
waiting for others to actAgree � 20%
b. To immediately initiate a predetermined sequence ofresponses
Agree � 80%
25. If the first attempt to extinguish the fire is not successful, a CO2
fire extinguisher should be used142 19.7 43.7* 36.6 0.0 0.0
26. If the fire persists after use of a CO2 fire extinguisher:a. The fire alarm should be activated 142 58.5* 37.3 4.2 0.0 0.0b. The patient should be evacuated, if feasible 142 52.1* 36.6 9.9 1.4 0.0c. The door to the room should be closed and not reopened 142 30.0 28.2* 26.1 6.3 1.4d. The medical gas supply to the room should be turned off 142 39.4 30.3* 20.4 7.0 2.8
27. After a fire has been extinguished, the patient’s status should beassessed and a plan devised for ongoing care of the patient
142 78.2* 20.4 0.7 0.0 0.7
28. When the airway or breathing circuit fire has been extinguished:a. Ventilation should be reestablished, avoiding supplemental
oxygen and nitrous oxide, if possible142 23.9 38.7* 11.3 21.8 4.2
b. The tracheal tube should be examined to assess whetherfragments may be left behind in the airway
142 60.6* 38.0 1.4 0.0 0.0
c. Rigid bronchoscopy should be considered to assess thermalinjury and look for tracheal tube fragments and other residualmaterials
142 43.7 39.4* 14.8 2.1 0.0
29. If the fire did not involve the airway and the patient was notintubated before the fire, the patient should be assessed forinjury related to smoke inhalation
142 52.1* 42.3 4.2 1.4 0.0
* Median response falls within this designated response category. † A high-risk procedure is defined as one in which an ignition source may be in proximityto an oxidizer-enriched atmosphere. ‡ n is the number of ASA members who responded to each item. All other numbers in the table represent the percentageof ASA members who selected the designated response category.
CO2 � carbon dioxide; FIO2 � fraction of inspired oxygen; OR � operating room.
801PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

Review Article
New Therapeutic Agents for Diabetes Mellitus:Implications for Anesthetic Management
Daniel Chen, MD*†
Stephanie L. Lee, MD, PhD‡
Robert A. Peterfreund, MD, PhD†
Multiple hormones and transmitter systems contribute to glucose homeostasisand the control of metabolism. Recently, the gastrointestinal peptide hormonesglucagon-like peptide 1 and amylin have been shown to significantly contribute tothis complex physiology. These advances provide the foundation for new treat-ments for diabetes mellitus. Therapies based on glucagon-like peptide 1 and amylinhave now been introduced into clinical practice. Rimonabant, the selective endo-cannabinoid receptor antagonist, had been used in European countries for thetreatment of obesity; it has recently been withdrawn for this indication. This drugexhibited therapeutic benefits for metabolic variables and for type 2 diabetesmellitus. Anesthesia providers caring for patients with diabetes mellitus will needto understand the implications of these new therapies in perioperative settings,particularly with respect to side effects and interactions.(Anesth Analg 2009;108:1803–10)
Diabetes mellitus (DM) is a condition with anabsolute (Type 1) or relative (Type 2) deficiency ofinsulin. Significant end-organ consequences of bothtypes of diabetes include renal, neurological, cardio-vascular, and peripheral vascular pathology that mayhave an impact on the perioperative course. Multiplehormones and neural systems control glucose ho-meostasis. The principle regulator of plasma glucoselevels is insulin, a polypeptide secreted by pancreatic� cells. The plasma glucose decreasing action of insu-lin has long been recognized and its effect is counter-regulated by epinephrine, growth hormone, cortisoland glucagon, a polypeptide secreted by pancreatic �cells. Conventional therapies for DM have recentlybeen reviewed.1–4 Table 1 presents a summary of themajor classes of medications used in the treatmentof DM.
Contemporary studies revealed that two new fami-lies of gastrointestinal (GI) hormones, represented bythe incretins and amylin, have significant effects onglucose homeostasis. In addition, antagonists of theendocannabinoid system acting at the CB1 receptor,
represented by rimonabant, were found to exert mul-tiple effects on food intake and metabolic variables,including glucose homeostasis. These advances pro-vide new opportunities for therapeutic approaches topatients with DM. Anesthesia providers will increas-ingly encounter patients treated with novel drugsbased on the enhanced understanding of glucosehomeostasis and the physiological control of metabo-lism. We aim to provide anesthesia clinicians with anintroduction to the rapidly evolving pharmacology ofmedical treatment for DM.
BIOLOGY OF INCRETINSIdentification of the members of the incretin family
of endogenous gut hormones was based on the obser-vation that the insulin response to oral glucose loads ismore vigorous than from IV glucose loads producingthe same blood glucose levels. In human studies,when subjects achieve identical plasma glucose in-creases, oral glucose administration resulted in moreinsulin secretion than IV glucose administration (Fig.1).5–9 This indicated that previously unidentified fac-tors produced by the GI system influence blood glu-cose levels in combination with the known hormones,insulin and glucagon. The consequence of these gutfactors is called the “incretin” effect.
The incretin effect is mediated via GI hormones thatstimulate insulin secretion in response to glucoseincrease from an enteral carbohydrate load. GIP(glucose-dependent insulinotropic polypeptide) andglucagon-like peptide 1 (GLP-1, Fig. 2) are the firsttwo incretin hormones identified. Because much ofGIP’s insulinotropic effect is lost in diabetic patientsdue to resistance to its actions, its potential utility indiabetic therapy is low7,10 and therefore will not bediscussed further. Unlike GIP, GLP-1’s insulinotropic
From the *Department of Anesthesiology, Hospital for SpecialSurgery, New York, New York; †Department of Anesthesia andCritical Care, Massachusetts General Hospital, Harvard MedicalSchool; and ‡Section of Endocrinology, Diabetes and Nutrition,Boston Medical Center, Boston University School of Medicine,Boston, Massachusetts.
Accepted for publication October 30, 2008.Reprints will not be available from the author.Address correspondence to Robert A. Peterfreund, MD, PhD,
Department of Anesthesia and Critical Care, Jackson 439, Massa-chusetts General Hospital, 55 Fruit Street, Boston, MA 02114.Address e-mail to [email protected].
Copyright © 2009 International Anesthesia Research SocietyDOI: 10.1213/ane.0b013e31819dcc51
Vol. 108, No. 6, June 2009 1803

action persists in patients with DM.10 This makes it apotential target for diabetic therapy. Initial studiesidentified enteroendocrine L cells located in the distalileum and large intestine as the source of GLP-1. Onestudy also found enteroendocrine L cells located moreproximally in the duodenum and jejunum.11 The fastingblood GLP-1 level is approximately 5–10 pmol/L.Within minutes of food intake, the level increases to15–50 pmol/L.11 The rapid increase in blood levels ofGLP-1 suggests that the secretion of GLP-1 is not simplydue to detection of nutrients by the L cells in thedigestive tract; a faster endocrine/neural signalingsystem must also be involved.11
The peptide hormone GLP-1 reduces appetite,slows gastric emptying, reduces glucagon levels, en-hances glucose- stimulated insulin secretion, and in-creases insulin biosynthesis (Table 1).9,11,12 In animalmodels, GLP-1 has trophic actions to increase thenumbers of pancreatic � cells.13 GLP-1 works througha G protein coupled signal transduction system, andits receptors are found in pancreatic � and � cells, thecentral nervous system, and the GI tract. Through itsreceptors on � cells, GLP-1 enhances insulin exocyto-sis, but only in a glucose-dependent manner.7 GLP-1induces gene transcription in pancreatic � cells topromote insulin biosynthesis. In vitro studies demon-strate that GLP-1 influences � cell survival by promoting
Figure 1. Insulin secretion after IV or oral glucose load.Subjects received oral glucose (50 g glucose/400 mL) or anIV infusion of glucose to produce the same blood glucoselevels. As measured by plasma levels of C-peptide (a frag-ment of the insulin prohormone), oral glucose loading (solidcircles) resulted in a greater secretion of insulin comparedwith IV glucose loading (open circles) designed to achieveidentical plasma glucose concentrations. The difference be-tween insulin secretion profiles after oral versus IV loading isdefined as the incretin effect. Left, plasma glucose after oral orisoglycemic IV loading of glucose. Right, C-peptide levels inresponse to oral or IV glucose loading. Modified from Ref 5,with publisher’s permission from the Endocrine Society.
Table 1. Classes of Agents Regulating Glucose Levels
Class Route Mechanism of action Side effects Clinical agentsInsulin SQ, IV 1Glucose uptake Hypoglycemia Many preparationsGLP-1 SQ 1Insulin secretion (if
hyperglycemia)Nausea Exenatide
2Glucagon secretion2Appetite2Gastric emptying
Amylin SQ 2Postprandial glucagonsecretion
Hypoglycemia (withinsulin)
Nausea
Pramlintide
1Satiety2Gastric emptying
DPP-IV inhibitor Oral 2GLP-1 degradation Infection SitagliptinCannabinoid receptor
antagonistOral Weight loss 2Glucose Rimonabant
Multiple other effects Depression2Appetite
Sulfonylurea Oral 1Insulin secretion viabinding to specific receptoron � cells
HypoglycemiaHyponatremiaDrug-drug interactions
ChlorpropamideGlimepirideGlipizideGlyburideTolazamideTolbutamide
Meglitinide Oral 1Insulin secretion by bindingto ATP dependent K�
channels on � cells
Hypoglycemia RepaglinideNateglinide
Thiazolidinedione Oral Insulin sensitizer by bindingto PPAR � receptor
Edema, anemia, obesity,CHF, hepatotoxicity
RosiglitazonePioglitazone
Biguanide Oral 2Hepatic glucose output Lactic acidosis MetforminInsulin sensitizer Diarrhea
Alpha-glucosidaseinhibitor
Oral 2GI glucose absorption byinhibiting enzyme thatmetabolizes complexcarbohydrates
MalabsorptionFlatulenceDiarrhea
AcarboseMiglitol
Incretin-mimetics (GLP-1, DPP-IV inhibitors) and insulin sensitizers (thiazolidinediones, biguanides) in single agent therapy do not predispose to hypoglycemia even in the fasting state.CHF � congestive heart failure; SQ � subcutaneous; DPP-IV � dipeptidyl pepidase IV; GLP-1 � glucagon-like peptide 1.
1804 New Therapies for Diabetes Mellitus ANESTHESIA & ANALGESIA

proliferation and resistance to apoptosis.14 Through itsreceptors on � cells, GLP-1 inhibits glucagon secretionin a glucose-dependent manner and consequentlyreduces hepatic glucose production. The counter regu-latory release of glucagon in response to hypoglyce-mia remains active.15 Through actions on the centralnervous system, GLP-1 decreases appetite and foodintake with a resulting contribution to weight loss.12,15
GLP-1 also slows gastric emptying, thereby bluntingthe postprandial increase in blood glucose levels.6
A feature of the biology of GLP-1 is its rapiddegradation by the peptidase dipeptidyl peptidase IV(DPP-IV) (Fig. 2a).9,16 DPP-IV cleaves peptides at theiramino terminal where the penultimate amino acidresidue is proline or alanine.16 The presence of DPP-IVin the capillary bed of the gut mucosa facilitates rapidinactivation of GLP-1.17 DPP-IV is a ubiquitous,membrane-spanning, cell surface aminopeptidase. Itsextracellular domain can be cleaved and circulate inthe plasma, retaining full enzymatic strength. DPP-IVis also found in liver, lung, kidney, the intestinal brushborder, lymphocytes and endocrine cells. In additionto GLP-1, DPP-IV has numerous substrates, includingvasoactive intestinal polypeptide, gastrin-releasingpeptide, neuropeptide Y and growth hormone-releasing hormone.18,19 DPP-IV also has a role in theimmune system. It is found on lymphocytes as CD26,which has been implicated in cellular uptake of theHuman Immunodeficiency Virus.20 Other biologicaleffects of DPP-IV include actions on T cell activation,chemotaxis and possibly tumor transformation andinvasion.21
Compared with healthy individuals, patients withDM exhibit a blunted increase in blood GLP-1 levelsafter food intake.22 Consequently, experimental treat-ment for DM has evaluated treatment with the nativeGLP-1 peptide. However, since DPP-IV rapidly de-grades GLP-1, only a constant IV infusion of thepeptide is effective in sustaining therapeutic plasmalevels. Two pharmacological strategies are now clini-cally used to counter the effects of the DPP-IV pepti-dase (Table 2).7,8 One strategy uses injection of aGLP-1 analog resistant to DPP-IV. A second pharma-cological strategy targeting DPP-IV uses an inhibitorof this peptidase in order to increase levels of endog-enous GLP-1.
Specific AgentsThe naturally occurring peptide homolog of GLP-1,
exendin-4, resists degradation by DPP-IV. The syn-thetic form is known as exenatide; its commercialname is Byetta�. Exendin-4/exenatide is originallyderived from salivary secretions of the lizard Helo-derma suspectum (the Gila monster) and shares roughly50% of its amino acid sequence with mammalian
Figure 2. Structure of the peptide glucagon-like peptide 1(GLP-1) and analogs. a, Amino acid sequence of the mam-malian peptide GLP-1. Arrow at the amino terminus indi-cates site of cleavage by the ubiquitous peptidase, dipeptidylpeptidase IV (DPP-IV). DPP-IV preferentially cleaves pep-tides with proline (P) or alanine (A) in the second aminoterminal position. b, Amino acid sequence of the naturallyoccurring peptide exenatide. This peptide is resistant todegradation by DPP-IV because of the substitution of gly-cine (G) at the second amino terminal position (hatchedarrow). It exhibits a biological profile similar to the endog-enous mammalian peptide, GLP-1. c, Structure of the syn-thetic GLP-1 analog liraglutide. This peptide is covalentlymodified with a C16 fatty acid chain via the addition of aglutamic acid (E) to the native lysine (K) as indicated by thearrowhead. The modified peptide binds noncovalently toalbumin. This hinders degradation by DPP-IV. Incretinbiological activity is preserved.
Table 2. Pharmacologic Agents Acting via the Incretin and Amylin Pathways
Agent Mechanism of action Major side effects Time to onset (h) Duration of action (h)Exenatide
(Byetta�)Incretin-mimetic, increases
insulin secretion onlywith hyperglycemia
Risk of hypoglycemia whengiven with asulfonylurea; delay ingastric emptying, nausea,anorexia
�0.25 6–12
Sitagliptin(Januvia�)
Inhibitor of DPP-IV Upper respiratoryinfections, headache
Peak at 1–4 h Half life approximately12
Pramlintide(Symlin�)
Amylin analog,suppresses postprandialglucagon secretion
Hypoglycemia when givenwith insulin, delay ingastric emptying, nausea
�0.25 2–4
DPP-IV � dipeptidyl pepidase IV.
Vol. 108, No. 6, June 2009 © 2009 International Anesthesia Research Society 1805

GLP-1.23 However, a substitution of glycine for ala-nine in its amino terminal protects exenatide fromdegradation by DPP-IV (Fig. 2b).11 Exenatide has acirculating half-life variously reported between 60 and90 min to 2.5 h, with plasma concentrations lasting 4 to6 h or more after a single subcutaneous dose. Elimi-nation is primarily through the renal system, althoughpatients with mild to moderate renal impairment donot exhibit significantly altered clearance.23
Exenatide is currently approved for the treatmentof type 2 DM patients receiving concurrent metforminor sulfonylurea therapy.23 It has no role in therapy ofpatients with DM type 1. Exenatide is given as asubcutaneous injection of 5 to 10 �g twice daily.Clinical trials show a significant reduction in hemo-globin A1c levels over 30 wk (absolute reduction ofapproximately 0.6%–0.9% from baseline hemoglobinA1c of 8.2%–8.7%) and a modest amount of weightloss (2 kg over 30 wk).24
The most common adverse events were GI symp-toms, including nausea and, rarely, vomiting ordiarrhea.25 Patients receiving both exenatide and asulfonylurea exhibit an increased risk for mild to mod-erate hypoglycemic events. However, the risk was notincreased in patients receiving concurrent treatmentwith exenatide and metformin.25 Approximately, 40% to50% of patients receiving exenatide develop low titers ofa weak affinity antibody. However, the antibody forma-tion has not been associated with decreased effectivenessof exenatide or other adverse reactions.11
A long-acting exenatide preparation is currentlyunder development, a polylactide-glycolide micro-sphere suspension containing 3% exenatide peptide.In diabetic rats, this preparation produced dose-dependent control of serum glucose for up to 28 daysafter a single injection.11
Liraglutide is another GLP-1 analog. With aminoacid substitutions at positions 34 and 26, and a co-valently linked C16 fatty-acid group, liraglutide formsnoncovalent bonds with albumin, which confers resis-tance to DPP-IV-mediated degradation (Fig. 2c).11 It isnot yet released in the United States for clinical use.Like exenatide, liraglutide is given as a subcutaneousinjection. It has a half-life of 10–14 h and consequentlycan be given as a once-daily injection. Clinical trialswith liraglutide demonstrated significant reductionsin postprandial glucose levels.11 Reduced hemoglobinA1c levels (absolute reduction of approximately 0.8%from baseline hemoglobin A1c) suggest improvedlong-term glucose control.25 Liraglutide also preventsweight gain or induces modest weight loss.11 The mostcommon adverse event is nausea, which is generallymild and decreases over time.
Sitagliptin is a DPP-IV inhibitor, now commer-cially available in the United States. The trade nameis Januvia�. Other DPP-IV inhibitors, includingvildagliptin, are in clinical trials and may soon beapproved for routine use.18 Sitagliptin enhancesinsulin secretion and decreases glucagon secretion
in a glucose-dependent matter. However, unlikeexenatide and liraglutide, sitagliptin does not affectgastric emptying.26 It has a half-life of 12 h and istaken orally as a once or twice daily medication.Clinical trials have shown a significant reduction inhemoglobin A1c levels associated with sitagliptintherapy (absolute reduction of 0.8% from baselinehemoglobin A1c of 5.8%–10.4% over 3 mo).26 Unliketherapy with exenatide, there was no significantweight change associated with sitagliptin. In earlyclinical trials, sitagliptin seemed to be well tolerated,without significant GI symptoms or hypoglycemicevents.26 However, given widespread expression ofDPP-IV in many cell types, and multiple potentialsubstrates for this peptidase,8 additional clinical stud-ies are needed to assess the long-term safety of DPP-IVinhibitors.18
BIOLOGY OF AMYLINAmylin, another GI hormone, has been identified as
a potential therapeutic target in DM (Fig. 3a).8,27
Pancreatic � cells, the same cells that manufacture andsecrete insulin, produce the amylin peptide hormone.Consequently, patients lacking functional pancreatic �cells (individuals with type 1 DM or advanced type 2DM) are deficient in both insulin and amylin.27 Similarto GLP-1, food intake stimulates amylin secretion. Its24-h profile resembles that of insulin, with low fastingblood levels and a robust increase in response tomeals. The glucose-decreasing effect of amylin seems
Figure 3. Structure of amylin and the synthetic analogpramlintide. a, Amino acid sequence of the naturally occur-ring peptide hormone. Arrowhead indicates the disulfidebridge between two cysteines. b, Structure of the syntheticamylin analog pramlintide. Substitution with proline at posi-tions 25, 28, and 29 of the native peptide (arrows) conferssolubility without disrupting biological activity. Arrowheadindicates the disulfide bridge between two cysteines.
1806 New Therapies for Diabetes Mellitus ANESTHESIA & ANALGESIA

to be independent of, and additive to, the effects ofinsulin.28
Like GLP-1, the actions of amylin include suppres-sion of glucagon secretion in a glucose-dependentmanner and delayed gastric emptying (Table 1); how-ever, the mechanism(s) of action remain incompletelydefined. Amylin is also a satiety agent, with receptorsin the area postrema of the hindbrain.28 By suppress-ing glucagon secretion and delaying gastric emptying,amylin slows the inflow of glucose into the circulation.At the same time, insulin stimulates cellular uptake ofglucose to reduce postprandial blood glucose levels.Effort has been made to treat patients with diabetesusing the native amylin peptide. However, endoge-nous amylin aggregates and forms insoluble masses ofamyloid. Consequently, synthetic modifications arenecessary to produce a soluble amylin analog suitablefor clinical use.
Specific AgentPramlintide is a synthetic amylin analog with pro-
line substitutions at amino acid positions 25, 28, and29 (Fig. 3b).27 These structural changes improve solu-bility. Pramlintide is used as an adjunct to insulin forboth type 1 and type 2 DM patients. It is given as asubcutaneous injection two or three times daily. Pram-lintide has an onset of approximately 20 min andduration of action of about 2 to 4 h. Clinical trialsdemonstrated significant improvement of postpran-dial glucose levels and hemoglobin A1c levels (abso-lute reduction of 0.67% at 13 wk and 0.39% at 52 wk)associated with pramlintide treatment.24 Pramlintideseems to decrease postprandial triglyceride excur-sions.29 The most common adverse reaction associatedwith pramlintide therapy is nausea, which improvesover the course of treatment. By itself, pramlintide hasnot been shown to cause an increased risk of hypogly-cemia; however, any concurrent insulin dose needs tobe adjusted to prevent hypoglycemia.27
THE ENDOCANNABINOID SYSTEMA comprehensive overview of the astonishingly
complex endocannabinoid signaling system is beyondthe scope of this article. Detailed reviews are avail-able.30 Briefly, the identification of specific bindingsites for plant products led to the identification of twoG protein-coupled receptors, labeled CB1 and CB2.The CB1 receptor is widespread throughout the brainand peripheral tissues, whereas the CB2 receptor has amore restricted distribution. These receptors seem touse several different signal transduction pathways,depending on how the receptor is activated and thetissue where it is expressed. The diverse distributionof the CB1 receptor, in particular, explains the exten-sive array of biological activities associated with itsactivation or blockade which include effects on appe-tite and ingestive behavior, addictive behaviors,sleep/awake cycles, peripheral energy metabolism,pain and inflammation.
The isolation of specific receptors for exogenousagonists suggested the existence of endogenous li-gands for the two cannabinoid receptors. Severalcandidate ligands have been identified. These includeanandamide, derived by enzymatic hydrolysis fromthe membrane lipid precursor N-arachidonoyl phos-phatidylethanolamide, and 2-arachidonoylglycerol de-rived from diacylglycerol. Of compelling interest forthe administration of anesthesia, there is evidence thatpropofol acts, at least in part, via activation of CB1receptors.31 This effect may be mediated by the inhi-bition of anandamide breakdown.32 Schelling et al.,33
however, provided evidence that the inhaled gen-eral anesthetic sevoflurane has different effects onanandamide levels than does propofol, suggestingagent-specific interactions with the endocannabi-noid system.
Specific DrugRimonabant was available until recently in many
countries (trade name: Acomplia), primarily as a treat-ment for obesity, with an added benefit of improvingglucose homeostasis beyond what might be expectedfrom weight loss alone.34,35 Clinical trials with rimon-abant (such as the Rimonabant in Obesity trial) dem-onstrated sustained weight loss and a reduction inwaist circumference. In addition, metabolic profilesimproved for triglyceride levels, lipoprotein choles-terol levels, and insulin resistance. Consequently, con-siderable interest developed in this drug for themanagement of metabolic syndrome.34,36 This drughas multiple pharmacologic effects37 and a long ter-minal elimination half-life in animals (approximately7 h). A prominent finding is that treatment withrimonabant is associated with neuropsychiatric sideeffects.38 Out of concern for an enhanced risk ofdepression and suicide,39 rimonabant was not ap-proved in the United States40 and it has recently beenwithdrawn in Europe for the original indication ofobesity.
ANESTHETIC CONSIDERATIONSA literature search via the National Library of
Medicine tool PubMed does not produce publishedexamples of adverse effects, drug-drug interactions orclinical conundrums attributable to exenatide, pram-lintide, a DPP IV inhibitor, or rimonabant in patientsundergoing anesthesia or surgery. These drugs haveonly recently appeared in clinical practice, and only asubset of all treated patients may have required ananesthetic since the drugs were approved and re-leased. Consequently, the number of clinical situationsin which a potential adverse effect emerges may be toofew for the manifestation of an uncommon reaction.
Alternatively, adverse effects may have occurred,but went undetected in complex clinical scenarios inwhich patients suffering from multiple co-morbidconditions received several medications concurrently.
Vol. 108, No. 6, June 2009 © 2009 International Anesthesia Research Society 1807

Moreover, untoward effects in anesthetized or surgi-cal patients attributable to one of these newly releaseddrugs simply may not have been reported. As clinicalexperience with these new drugs increases, it is pos-sible that recognizable patterns will develop. There-fore, at this time it is only possible to suggest potentialanesthesia concerns based on the known physiologyand pharmacology of the novel therapies.
Nausea is the most common adverse reaction asso-ciated with medications active along the incretin andamylin pathways. Clinical trials have shown nauseaoccurring in as many as 57% of patients treated withexenatide.41 The incidence of vomiting is less frequent.However, vomiting still occurs in approximately 17%of the patients receiving exenatide.41 Nausea is gener-ally mild to moderate, and most prevalent in the first8 wk of treatment. The frequency and intensity ofnausea generally declines thereafter. The risk of nau-sea is dose-dependent and can be decreased bygradual dose titration. However, adverse GI effectsassociated with exenatide are still the most commoncauses for patients to withdraw from clinical trials.41
Clinical studies with DPP-IV inhibitors, such assitagliptin, have reported no increased GI adversereactions. They are overall well tolerated with lowabsolute rates of adverse effects.26 This lack of GIadverse reactions may be secondary to the fact thatDPP-IV inhibitors only moderately increase the levelsof endogenous incretin hormones. In contrast, admin-istration of incretin analogs, such as exenatide, in-creases incretin hormone activity to a much greaterextent. Similar reasoning explains the finding that,while incretin analogs cause significant weight loss inpatients, DPP-IV inhibitors usually do not producesignificant weight changes.
Nausea is the most common adverse effect ofpramlintide, the amylin analog. Nausea occurs morefrequently in the type 1 DM patient than in the type 2DM patient.27 It is usually mild to moderate in inten-sity, occurring most frequently in the early stage oftreatment, and commonly attenuates over time. Theincidence of nausea is approximately 47% in type 1diabetics and 27% in type 2 diabetics.42 The risk ofnausea depends on the dose of pramlintide and can bedecreased by gradual dose titration.
Prominent antinausea effects of cannabinoids maybe mediated, at least in part, by CB1 receptors. Thishas led to occasional use of cannabinoids for patientsreceiving cancer chemotherapy.30 In a meta-analysis ofstudies on the use of rimonabant in smoking cessation,nausea was one of the adverse effects emerging fromthe pooled data from the early trials.43
Although there are no published reports of unusualpostoperative nausea and vomiting (PONV) attrib-uted to rimonabant or to drugs active along theincretin and amylin pathways, it seems reasonable toexpect that patients treated with these medicationsmay experience more frequent, or more severe, PONVthan the average patient. Consequently, for elective
surgery requiring anesthesia, at this time it seemslogical to withhold these medications in the immedi-ate perioperative period to reduce the likelihood orintensity of PONV. In situations of urgent or emer-gency surgery, without an opportunity to halt theadministration of these novel drugs, it is possible thatpatients will exhibit exaggerated or refractory postop-erative nausea. Future clinical studies may eventuallyprovide evidence-based recommendations.
Delaying gastric emptying is one of the mecha-nisms by which incretin peptides and amylin decreasepostprandial glucose levels.6 By impeding gastricemptying, glucose inflow into the circulation slows.Consequently, the incretins and amylin allow insulinmore time to stimulate glucose uptake and regulateserum glucose levels. Both exenatide and pramlintidecause delayed gastric emptying. DPP-IV inhibitors,such as sitagliptin, however, have little or no effect ongastric emptying,26 probably attributable to the mod-est increases in GLP-1 levels caused by this class ofdrugs. Gastroparesis is a feature of advanced diabetes,and medications that slow gastric emptying mayexacerbate this problem.44 Although no publishedreports document an increased risk of aspiration as-sociated with the new diabetes therapies, patientsreceiving these medications are theoretically at agreater risk for this complication during the perioper-ative period, especially those patients with peripheralneuropathy and gastroparesis as manifestations oftheir diabetes. In urgent or emergent situations wherethere has been no opportunity to withhold the medi-cations, clinicians may find unexpectedly large vol-umes of gastric contents removed by gastric suction.The administration of drugs promoting gut motility,such as metoclopramide, might factor more promi-nently in overall management of the patient unlessthere are specific contraindications.
Hypoglycemia is a potential adverse effect of medi-cations active along the incretin and amylin pathways,particularly if used in conjunction with an insulinpreparation or a sulfonylurea. Because incretinanalogs only promote insulin secretion in a“glucose-dependent” manner and because thecounter-regulatory release of glucagon secondary tohypoglycemia is preserved with incretins, the risk ofhypoglycemia should be low. Clinical trials show thatsevere hypoglycemia requiring medical interventionis rare with incretin analogs, such as exenatide. In 1trial, only 5 of 2781 patients treated with exenatidehad hypoglycemia requiring medical assistance.45 Allfive patients also received an insulin secretagogue,such as a sulfonylurea. No patients receiving bothexenatide and an insulin sensitizer, such as met-formin, developed hypoglycemia requiring medicalassistance.
When clinical trials are combined and reviewedunder meta-analysis, the overall incidence of hypogly-cemia associated with exenatide is approximately
1808 New Therapies for Diabetes Mellitus ANESTHESIA & ANALGESIA

16%.41 Hypoglycemia occurs especially when ex-enatide is co-administrated with a sulfonylurea. Thisrisk is comparable with the risk of hypoglycemia forpatients receiving insulin for treatment of diabetes.The likelihood of hypoglycemia is greatest during theinitial treatment period and declines over time. Whencompared with incretin analogs, DPP-IV inhibitorscarry less risk of hypoglycemia. In meta-analysis, onlyapproximately 1.6% of patients had episodes of mildto moderate hypoglycemia, which was not statisticallydifferent from the control group.41
Clinical trials with the amylin analog pramlintideshowed no increase in the overall event rates forsevere hypoglycemia.46 However, in patients also re-ceiving insulin for their diabetes, the rate of hypogly-cemia increased during the initial 4 wk of therapywith pramlintide.46 The enhanced risk of hypoglyce-mia was transient and diminished with appropriate bloodglucose monitoring and adjustments of insulin dose.
The half-lives and clinical effects of sitagliptin,exenatide, and pramlintide are relatively short. Fur-thermore, no clinical reports suggest that medicationsactive along the incretin or amylin pathways causehypoglycemia in the perioperative period. However,in the absence of definitive evidence, the theoreticalrisk of hypoglycemia is another reason to withholdthese medications in advance of elective surgery. Thiswould be a particularly pertinent consideration forpatients receiving both a sulfonylurea or an insulinpreparation and exenatide. Suppression of glucagonrelease by exenatide would be a mechanism contrib-uting to hypoglycemia. Should longer-acting GLP-1analogs, such as liraglutide, enter into clinical use, theglucose-decreasing effects might extend into the sur-gical or anesthesia interval. Anesthesia providersroutinely monitor the blood glucose levels of theirpatients. Perhaps, however, particular vigilance forthe possibility of hypoglycemia is warranted, espe-cially in urgent/emergent surgical situations in whichthere is no opportunity to withhold the medications.In theory, patients treated with long-acting insulinpreparations or sulfonylureas along with exenatidewould be most vulnerable. Clinicians might con-sider more frequent monitoring in urgent or emer-gent situations.
Hypoglycemia does not seem to be a likely conse-quence of rimonabant therapy.35
OTHER EFFECTSDPP-IV is a ubiquitous aminopepetidase with mul-
tiple natural substrates and it plays a role in theimmune system. Consequently, it seems plausible thatinhibiting DPP-IV can potentially cause adverse reac-tions. Clinical trials have shown that DPP-IV inhibi-tors were very well tolerated with low rates of adverseeffects. In meta-analysis, there is a small increased riskof nasopharyngitis and urinary tract infection associ-ated with DPP-IV inhibitors.41 Clinical experience in
anesthetized patients receiving DPP-IV inhibitors islimited. Because multiple peptides are potential sub-strates for this enzyme,18 clinicians should be alert forunusual reactions, especially in urgent procedures inwhich the drug may not have been withheld.
The endocannabinoid system is involved in manycomplex behaviors and physiologic responses, in-cluding pain and sleep/awake cycles. In preclinicalstudies, as cited above, there appear to be interac-tions between the endocannabinoid system andanesthetics. Given the “pleiotropic” effects ofrimonabant,37 the exact consequences of clinicalinteractions between drugs acting on cannabinoidreceptors in the brain and periphery with sedatives,narcotics, and inhaled or injected general anesthet-ics remain to be determined.
SUMMARY AND RECOMMENDATIONSFood ingestion increases secretion of insulin, amy-
lin, and the incretin peptides. Insulin and amylinregulate postprandial hyperglycemia, while amylinalso suppresses glucagon secretion and slows foodintake and gastric emptying. GLP-1 amplifies glucose-stimulated insulin release, in addition to suppressingglucagon secretion, food intake, and gastric emptying.The new treatment options for DM acting along theincretin pathway and the amylin analog offer somepotential advantages for chronic treatment of DM bytargeting these physiologic mechanisms. However,the biological activities of these drugs may presentchallenges in the perioperative period. This is espe-cially true in the urgent or emergent clinical circum-stances in which there are no opportunities towithhold these medications.
As clinical experience accumulates with noveldrugs in anesthetized patients, it may become pos-sible to develop more definitive warnings and rec-ommendations. However, until this informationbecomes available, we suggest withholding GLP-1analogs, DPP-IV inhibitors, and pramlintide on theday of surgery. Patients can probably continue totake these drugs the day before surgery without anenhanced risk of hypoglycemia while fasting.With these drugs, there are potentially enhancedrisks of nausea, aspiration of gastric contents, andhypoglycemia.
As the newer treatments for DM become increasinglyprevalent in clinical practice, anesthesia providersshould maintain particular vigilance for unusual orexaggerated effects and responses during the perioper-ative period.
ACKNOWLEDGMENTSWe thank Drs. Enrico Cagliero, Steven Russell, and Jean
Kwo of Massachusetts General Hospital for providinginsightful suggestions during the drafting of this article.
Vol. 108, No. 6, June 2009 © 2009 International Anesthesia Research Society 1809

REFERENCES
1. Peterfreund RA, Lee SL. Anesthesia considerations for endo-crine surgery and patients with endocrine conditions. In: Long-necker D Brown D, Newman M, Zapol W, eds. Anesthesiology.New York: McGraw-Hill, 2007:1420–49
2. McAnulty GR, Robertshaw HJ, Hall GM. Anaesthetic man-agement of patients with diabetes mellitus. Br J Anaesth2000;85:80 –90
3. Robertshaw HJ, McAnulty GR, Hall GH. Strategies for manag-ing the diabetic patient. Best Pract Res Clin Anaesthesiol2004;18:631–43
4. Rhodes ET, Ferrari LR, Wolfsdorf JI. Perioperative managementof pediatric surgical patients with diabetes mellitus. AnesthAnalg 2005;101:986–99
5. Nauck MA, Homberger E, Siegel EG, Allen RC, Eaton RP, EbertR, Creutzfeldt W. Incretin effects of increasing glucose loads inman calculated from venous insulin and C-peptide responses.J Clin Endocrinol Metab 1986;63:492–8
6. Maggs D, MacDonald I, Nauck MA. Glucose homeostasis andthe gastrointestinal tract: insights into the treatment of diabetes.Diabetes Obes Metab 2008;10:18–33
7. Fujioka K. Pathophysiology of type 2 diabetes and the role ofincretin hormones and beta-cell dysfunction. JAAPA 2007;Suppl:3–8
8. Combettes M, Kargar C. Newly approved and promising an-tidiabetic agents. Therapie 2007;62:293–310
9. Ranganath LR. Incretins: pathophysiological and therapeuticimplications of glucose-dependent insulinotropic polypeptideand glucagon-like peptide-1. J Clin Pathol 2008;61:401–9
10. Nauck MA, Heimesaat MM, Orskov C, Holst JJ, Ebert R,Creutzfeldt W. Preserved incretin activity of glucagon-likepeptide 1 [7–36 amide] but not of synthetic human gastricinhibitory polypeptide in patients with type-2 diabetes mellitus.J Clin Invest 1993;91:301–7
11. Drucker DJ, Nauck MA. The incretin system: glucagon-likepeptide-1 receptor agonists and dipeptidyl peptidase-4 inhibi-tors in type 2 diabetes. Lancet 2006;368:1696–705
12. Holst JJ. The physiology of glucagon-like peptide 1. Physiol Rev2007;87:1409–39
13. Drucker DJ. The biology of incretin hormones. Cell Metab2006;3:153–65
14. Li Y, Hansotia T, Yusta B, Ris F, Halban PA, Drucker DJ.Glucagon-like peptide-1 receptor signaling modulates beta cellapoptosis. J Biol Chem 2003;278:471–8
15. Nauck MA, Heimesaat MM, Behle K, Holst JJ, Nauck MS, RitzelR, Hufner M, Schmiegel WH. Effects of glucagon-like peptide 1on counterregulatory hormone responses, cognitive functions,and insulin secretion during hyperinsulinemic, stepped hypo-glycemic clamp experiments in healthy volunteers. J Clin Endo-crinol Metab 2002;87:1239–46
16. Mentlein R, Gallwitz B, Schmidt WE. Dipeptidyl-peptidaseIV hydrolyses gastric inhibitory polypeptide, glucagon-likepeptide-1(7–36)amide, peptide histidine methionine and is re-sponsible for their degradation in human serum. Eur J Biochem1993;214:829–35
17. Hansen L, Deacon CF, Orskov C, Holst JJ. Glucagon-likepeptide-1-(7–36)amide is transformed to glucagon-like peptide-1-(9–36)amide by dipeptidyl peptidase IV in the capillariessupplying the L cells of the porcine intestine. Endocrinology1999;140:5356–63
18. Chahal H, Chowdhury TA. Gliptins: a new class of oral hypo-glycaemic agent. QJM 2007;100:671–7
19. Mentlein R. Dipeptidyl-peptidase IV (CD26)–role in the inacti-vation of regulatory peptides. Regul Pept 1999;85:9–24
20. Callebaut C, Krust B, Jacotot E, Hovanessian AG. T cell activa-tion antigen, CD26, as a cofactor for entry of HIV in CD4� cells.Science 1993;262:2045–50
21. Tanaka T, Umeki K, Yamamoto I, Sakamoto F, Noguchi S,Ohtaki S. CD26 (dipeptidyl peptidase IV/DPP IV) as a novelmolecular marker for differentiated thyroid carcinoma. Int JCancer 1995;64:326–31
22. Nathan DM, Schreiber E, Fogel H, Mojsov S, Habener JF.Insulinotropic action of glucagonlike peptide-I-(7–37) in dia-betic and nondiabetic subjects. Diabetes Care 1992;15:270–6
23. Yoo BK, Triller DM, Yoo DJ. Exenatide: a new option for thetreatment of type 2 diabetes. Ann Pharmacother 2006;40:1777–84
24. Hoogwerf BJ. Exenatide and pramlintide: new glucose-loweringagents for treating diabetes mellitus. Cleve Clin J Med2006;73:477–84
25. Salehi M, D’Alessio DA. New therapies for type 2 diabetesbased on glucagon-like peptide 1. Cleve Clin J Med 2006;73:382–9
26. Idris I, Donnelly R. Dipeptidyl peptidase-IV inhibitors: a majornew class of oral antidiabetic drug. Diabetes Obes Metab2007;9:153–65
27. Kruger DF, Gloster MA. Pramlintide for the treatment ofinsulin-requiring diabetes mellitus: rationale and review ofclinical data. Drugs 2004;64:1419–32
28. Schmitz O, Brock B, Rungby J. Amylin agonists: a novelapproach in the treatment of diabetes. Diabetes 2004;53 Suppl3:S233–S238
29. Weyer C, Gottlieb A, Kim DD, Lutz K, Schwartz S, Gutierrez M,Wang Y, Ruggles JA, Kolterman OG, Maggs DG. Pramlintidereduces postprandial glucose excursions when added to regularinsulin or insulin lispro in subjects with type 1 diabetes: adose-timing study. Diabetes Care 2003;26:3074–9
30. Pacher P, Batkai S, Kunos G. The endocannabinoid system as anemerging target of pharmacotherapy. Pharmacol Rev 2006;58:389–462
31. Guindon J, LoVerme J, Piomelli D, Beaulieu P. The antinocicep-tive effects of local injections of propofol in rats are mediated inpart by cannabinoid CB1 and CB2 receptors. Anesth Analg2007;104:1563–9
32. Patel S, Wohlfeil ER, Rademacher DJ, Carrier EJ, Perry LJ,Kundu A, Falck JR, Nithipatikom K, Campbell WB, HillardCJ. The general anesthetic propofol increases brainN-arachidonylethanolamine (anandamide) content and inhibitsfatty acid amide hydrolase. Br J Pharmacol 2003;139:1005–13
33. Schelling G, Hauer D, Azad SC, Schmoelz M, Chouker A,Schmidt M, Hornuss C, Rippberger M, Briegel J, Thiel M,Vogeser M. Effects of general anesthesia on anandamide bloodlevels in humans. Anesthesiology 2006;104:273–7
34. Nogueiras R, Rohner-Jeanrenaud F, Woods SC, Tschop MH.The endocannabinoid system and the control of glucose ho-meostasis. J Neuroendocrinol 2008;20 Suppl 1:147–51
35. Scheen AJ. Cannabinoid-1 receptor antagonists in type-2 diabe-tes. Best Pract Res Clin Endocrinol Metab 2007;21:535–53
36. Jensen MD. What is the potential role of cannabinoid-1 receptorblockade in glucose and lipid management? Am J Med2007;120:S25–S31
37. Bifulco M, Grimaldi C, Gazzerro P, Pisanti S, Santoro A.Rimonabant: just an antiobesity drug? Current evidence on itspleiotropic effects. Mol Pharmacol 2007;71:1445–56
38. Christensen R, Kristensen PK, Bartels EM, Bliddal H, Astrup A.Efficacy and safety of the weight-loss drug rimonabant: ameta-analysis of randomised trials. Lancet 2007;370:1706–13
39. Rimonabant: suicide and depression. Depression and suicidaltendencies are about twice as frequent with rimonabant as withplacebo. Prescrire Int 2007;16:250
40. Traynor K. Panel advises against rimonabant approval. Am JHealth Syst Pharm 2007;64:1460–1
41. Amori RE, Lau J, Pittas AG. Efficacy and safety of incretintherapy in type 2 diabetes: systematic review and meta-analysis.JAMA 2007;298:194–206
42. Whitehouse F, Kruger DF, Fineman M, Shen L, Ruggles JA,Maggs DG, Weyer C, Kolterman OG. A randomized study andopen-label extension evaluating the long-term efficacy of pram-lintide as an adjunct to insulin therapy in type 1 diabetes.Diabetes Care 2002;25:724–30
43. Cahill K, Ussher M. Cannabinoid type 1 receptor antagonists(rimonabant) for smoking cessation. Cochrane Database SystRev 2007:CD005353
44. Cure P, Pileggi A, Alejandro R. Exenatide and rare adverseevents. N Engl J Med 2008;358:1969–70; discussion 71–2
45. Kendall DM, Riddle MC, Rosenstock J, Zhuang D, Kim DD,Fineman MS, Baron AD. Effects of exenatide (exendin-4) onglycemic control over 30 weeks in patients with type 2 diabetestreated with metformin and a sulfonylurea. Diabetes Care2005;28:1083–91
46. Hollander PA, Levy P, Fineman MS, Maggs DG, Shen LZ,Strobel SA, Weyer C, Kolterman OG. Pramlintide as an adjunctto insulin therapy improves long-term glycemic and weightcontrol in patients with type 2 diabetes: a 1-year randomizedcontrolled trial. Diabetes Care 2003;26:784–90
1810 New Therapies for Diabetes Mellitus ANESTHESIA & ANALGESIA

Anesthesiology 2005; 103:186–98 © 2005 American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc.
Practice Advisory for the Perioperative Management ofPatients with Cardiac Rhythm Management Devices:Pacemakers and Implantable Cardioverter–Defibrillators
A Report by the American Society of Anesthesiologists Task Force on PerioperativeManagement of Patients with Cardiac Rhythm Management Devices
PRACTICE advisories are systematically developed re-ports that are intended to assist decision making in areasof patient care. Advisories provide a synthesis and anal-ysis of expert opinion, clinical feasibility data, openforum commentary, and consensus surveys. Advisoriesare not intended as standards, guidelines, or absoluterequirements. They may be adopted, modified, or re-jected according to clinical needs and constraints.
The use of practice advisories cannot guarantee anyspecific outcome. Practice advisories summarize thestate of the literature and report opinions derived from asynthesis of task force members, expert consultants, openforums, and public commentary. Practice advisories are notsupported by scientific literature to the same degree asstandards or guidelines because of the lack of sufficientnumbers of adequately controlled studies. Practice adviso-ries are subject to periodic revision as warranted by theevolution of medical knowledge, technology, and practice.
Methodology
A. Definition of Cardiac Rhythm ManagementDevicesFor this Advisory, a cardiac rhythm management de-
vice (CRMD) refers to any permanently implanted car-diac pacemaker or any implantable cardioverter–defibril-lator (ICD). The term CRMD also refers to any cardiacresynchronization device. The term CRT refers to aCRMD that provides cardiac resynchronization therapyusing biventricular pacing techniques. Generic pace-maker and defibrillator codes are provided in appendix1. Note that every ICD includes both pacing and shocktherapies for the management of bradyarrhythmias andtachyarrhythmias.
B. Purposes of the AdvisoryThe purposes of this Advisory are to (1) facilitate safe
and effective perioperative management of the patientwith a CRMD and (2) reduce the incidence of adverseoutcomes. Perioperative management refers to the pre-operative, intraoperative, postoperative or recovery pe-riod in any setting where an anesthesia provider deliversanesthesia care. Adverse outcomes associated with aCRMD include (but are not limited to) damage to thedevice, inability of the device to deliver pacing orshocks, lead–tissue interface damage, changes in pacingbehavior, electrical reset to the backup pacing mode, orinappropriate ICD therapies.* Adverse clinical outcomesinclude (but are not limited to) hypotension, tachyarrhyth-mia or bradyarrhythmia, myocardial tissue damage, andmyocardial ischemia or infarction. Other related outcomesmay include extended hospital stay, delay or cancellation ofsurgery, readmission to manage device malfunction, oradditional hospital resource utilization and cost.
C. FocusThis Advisory focuses on the perioperative manage-
ment of patients who have a preexisting, permanentlyimplanted CRMD for treatment of bradyarrhythmia,tachyarrhythmia, or heart failure. Both inpatient andoutpatient procedures are addressed by this Advisory.This Advisory does not address the perioperative man-agement of any patient undergoing CRMD implantationor revision. It is not applicable to any patient (1) without
Additional material related to this article can be found on theANESTHESIOLOGY Web site. Go to http://www.anesthesiology.org, click on Enhancements Index, and then scroll down tofind the appropriate article and link. Supplementary materialcan also be accessed on the Web by clicking on the “Arti-clePlus” link either in the Table of Contents or in the HTMLversion of the article.
�
Developed by the American Society of Anesthesiologists Task Force on Peri-operative Management of Patients with Cardiac Rhythm Management Devices:James R. Zaidan, M.D., M.B.A. (Chair), Atlanta, Georgia; John L. Atlee, M.D.,Milwaukee, Wisconsin; Peter Belott, M.D., El Cajon, California; Kurt S. Briesa-cher, M.D., Atlanta, Georgia; Richard T. Connis, Ph.D., Woodinville, Washington;John D. Gallagher, M.D., Lebanon, New Hampshire; David Hayes, M.D., Roches-ter, Minnesota; Jane E. Hershey, M.D., Highland, Maryland; Neal Kay, M.D.,Birmingham, Alabama; David G. Nickinovich, Ph.D., Bellevue, Washington; MarcA. Rozner, Ph.D., M.D., Houston, Texas; Mark F. Trankina, M.D., Birmingham,Alabama. Submitted for publication December 28, 2004. Accepted for publica-tion December 28, 2004. Supported by the American Society of Anesthesiologistsunder the direction of James F. Arens, M.D., Chair, Committee on PracticeParameters. Approved by the House of Delegates on October 27, 2004. A list ofthe references used to develop this Advisory is available by writing to theAmerican Society of Anesthesiologists. This Advisory is endorsed by the Ameri-can Heart Association, the Heart Rhythm Society, and the Society of Cardiovas-cular Anesthesiologists.
Address reprint requests to the American Society of Anesthesiologists: 520 N.Northwest Highway, Park Ridge, Illinois 60068-2573. This Practice Advisory, aswell as all published ASA Practice Parameters, may be obtained at no costthrough the Journal Web site, www.anesthesiology.org.
* Inappropriate ICD therapy refers to the delivery of antitachycardia therapy(paced or shock) in the absence of a clinically indicated tachyarrhythmia. Inap-propriate ICD therapy can harm a patient by inducing ischemia, worsening thearrhythmia, or causing the patient to move during a delicate procedure.
Anesthesiology, V 103, No 1, Jul 2005 186

a permanently implanted pacemaker or ICD, (2) with atemporary CRMD, (3) with a noncardiac implantabledevice (e.g., neurologic or spinal cord stimulator), or (4)with an implantable mechanical cardiac assist device(e.g., ventricular assist device). This Advisory does notaddress any procedure where there are no known peri-operative CRMD concerns, such as diagnostic radiation(e.g., x-ray studies, fluoroscopy, or mammograms), com-puted tomography scans, or ultrasound.
D. ApplicationThis Advisory is intended for use by anesthesiologists
and all other individuals who deliver or who are respon-sible for anesthesia care. The Advisory may also serve asa resource for other physicians and healthcare profes-sionals who treat patients with CRMDs.
E. Task Force Members and ConsultantsThe American Society of Anesthesiologists (ASA) ap-
pointed a Task Force of 12 members to (1) review andassess currently available scientific literature, (2) obtainexpert consensus and public opinion, and (3) develop apractice advisory. The Task Force members consisted ofanesthesiologists and cardiologists in private and aca-demic practices from various geographic areas of theUnited States and two methodologists from the ASACommittee on Practice Parameters.
The Task Force used a six-step process. First, theyreached consensus on the criteria for evidence of effec-tive perioperative management of cardiac rhythm man-agement devices. Second, original published articlesfrom peer-reviewed journals relevant to these issueswere evaluated. Third, consultants who had expertise orinterest in CRMDs and who practiced or worked invarious settings (e.g., academic and private practice)were asked to (1) participate in opinion surveys on theeffectiveness of various perioperative management strat-egies and (2) review and comment on a draft of theAdvisory developed by the Task Force. Fourth, additionalopinions were solicited from random samples of activemembers of both the ASA and the Heart Rhythm Society(HRS).† Fifth, the Task Force held an open forum at anational anesthesia meeting and at a major cardiology meet-ing to solicit input on the key concepts of this Advisory.Sixth, all available information was used to build consensuswithin the Task Force on the Advisory.
The draft document was made available for review on theASA Web site, and input was invited via e-mail announce-ment to all ASA members. All submitted comments wereconsidered by the Task Force in preparing the final draft.
F. Availability and Strength of EvidencePractice advisories are developed by a protocol similar
to that of an ASA evidence-based practice guideline,including a systematic search and evaluation of the liter-ature. However, practice advisories lack the support of asufficient number of adequately controlled studies topermit aggregate analyses of data with rigorous statisticaltechniques such as meta-analysis. Nonetheless, litera-ture-based evidence from case reports and other descrip-tive studies is reported. This literature often permits theidentification of recurring patterns of clinical practice.
As with a practice guideline, formal survey informationwas collected from Consultants and members of the ASA.For this Advisory, surveys were also sent to members of theHRS. Additional information was obtained from open fo-rum presentations and other invited and public sources.The advisory statements contained in this document rep-resent a consensus of the current spectrum of clinicalopinion and literature-based findings.‡
Advisories
I. Preoperative EvaluationPerioperative treatment of CRMD patients is a com-
mon occurrence. It has been reported that more than500,000 individuals in the United States have perma-nently implanted pacemakers or ICDs with 115,000 newdevices implanted each year.1 Perioperative manage-ment of CRMD patients typically begins with a focusedpreoperative evaluation consisting of (1) establishingwhether a patient has a CRMD, (2) defining the type ofdevice, (3) determining whether a patient is CRMD de-pendent for antibradycardia pacing function, and (4)determining device function.
Although no controlled trials of the clinical impact ofperforming a focused preoperative evaluation for CRMDpatients were found, case reports suggest that incom-plete preoperative examination of patients with CRMDsmay lead to adverse outcomes (e.g., inhibited CRMDfunction, asystole).2–4 The majority of Consultants andrandom samples from the ASA and HRS membershipsagree that the above four preoperative evaluation activ-ities should be conducted.§
Advisory. The consensus of the Task Force is that afocused preoperative evaluation should include establish-ing whether a patient has a CRMD, defining the type ofdevice, determining whether a patient is CRMD dependentfor pacemaking function, and determining CRMD function.
Determining whether a patient has a CRMD should bebased on (1) a focused history including but not limitedto the patient interview, medical records review, reviewof available chest x-ray films, electrocardiogram, or anyavailable monitor or rhythm strip information and (2) afocused physical examination (checking for scars, pal-pating for device).
† Formerly North American Society of Pacing and Electrophysiology (NASPE).
‡ Refer to appendix 2 for a summary of the advisories.
§ Refer to appendix 3 for results of the Consultant, ASA membership, and HRSmembership surveys.
187PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

Defining the type of device is accomplished by (1)obtaining the manufacturer’s identification card from thepatient or other source, (2) ordering chest x-ray studies ifno other data are available,� or (3) referring to supplemen-tal resources (e.g., manufacturer’s databases, pacemakerclinic records, consultation with a cardiologist).
Cardiac rhythm management device dependency forpacemaking function may be determined by one or moreof the following: (1) a verbal history or an indication inthe medical record that the patient has experienced abradyarrhythmia that has caused syncope or other symp-toms requiring CRMD implantation, (2) a history of suc-cessful atrioventricular nodal ablation that resulted inCRMD placement, or (3) a CRMD evaluation that showsno evidence of spontaneous ventricular activity whenthe pacemaking function of the CRMD is programmed toVVI pacing mode at the lowest programmable rate.
Cardiac rhythm management device function is ideallyassessed by a comprehensive evaluation of the device.5
If a comprehensive evaluation is not possible, then, at aminimum, confirm whether pacing impulses arepresent and create a paced beat. Consultation with acardiologist or CRMD service may be necessary. Contact-ing the manufacturer for perioperative recommenda-tions may be a consideration.
II. Preoperative PreparationPreparation for patient safety and proper maintenance
of the device during a procedure includes (1) determin-ing whether electromagnetic interference (EMI) is likelyto occur during the planned procedure; (2) determiningwhether reprogramming the CRMD pacemaking func-tion to an asynchronous pacing mode or disabling anyspecial algorithms, including rate adaptive functions, isneeded; (3) suspending antitachyarrhythmia functions ifpresent; (4) advising the individual performing the proce-dure to consider use of a bipolar electrocautery system orultrasonic (harmonic) scalpel to minimize potential adverseeffects of EMI on the pulse generator or leads; (5) assuringthe availability of temporary pacing and defibrillationequipment; and (6) evaluating the possible effects of anes-
thetic techniques on CRMD function and patient–CRMDinteractions.
Numerous descriptive studies and case reports suggestthat the following procedures are likely to be associatedwith EMI: (1) electrocautery,6–11 (2) radio frequencyablation,12–20 (3) magnetic resonance imaging (MRI),21–31
and (4) radiation therapy.32–34 No studies were found thatreported EMI during electroconvulsive therapy (ECT).Some descriptive studies report the occurrence of EMIduring lithotripsy,35,36 whereas other descriptive studiesand case reports indicate no apparent EMI effects.37–39 Nocontrolled trials of the clinical impact of programming thepacemaking function to an asynchronous mode for a pro-cedure were found. Although some case reports suggestthat such reprogramming is beneficial during electrocau-tery,40–42 other reports indicate that EMI may continue toaffect reprogrammed pacemakers.43,44 The literature lackssufficient guidance regarding the potential perioperativeimpact of anesthetic techniques on CRMD function. Themajority of Consultants as well as the samples of ASA andHRS members agree that it should be determined whetherEMI is likely to occur before a planned procedure. Themajority of Consultants agree that a CRMD’s rate-adaptivetherapy should be turned off before a procedure, whereasthe ASA and HRS members are equivocal. The majority ofConsultants and HRS members disagree that all patients’CRMDs should be programmed to an asynchronous modebefore surgery, whereas the ASA members are equivocal. Inaddition, the majority of Consultants and HRS membersagree that pacemaker-dependent patients’ CRMDs shouldbe programmed to an asynchronous mode before surgery,whereas the ASA members are again equivocal. The major-ity of Consultants and ASA and HRS members agree that (1)suspending antitachyarrhythmia functions if present, (2)advising the individual performing the procedure to con-sider use of a bipolar electrocautery system to minimizepotential adverse effects of EMI on the pulse generator orleads, (3) assuring the availability of temporary pacing anddefibrillation equipment, and (4) evaluating the possibleeffects of anesthetic techniques on CRMD function andpatient–CRMD interactions are important steps in promot-ing patient safety and successfully treating patients withCRMDs. The Consultants and ASA members agree and theHRS members are equivocal regarding the consideration ofusing an ultrasonic scalpel.
Advisory. The Task Force agrees that planned proce-dures should include a determination as to whether EMI islikely to occur for either conventional pacemakers or ICDs.
If EMI is likely to occur, the conventional pacing func-tion of a CRMD should be altered by changing to anasynchronous pacing mode# in pacemaker-dependentpatients and suspending special algorithms, includingrate-adaptive functions. These alterations may be accom-plished by programming or applying a magnet whenapplicable.** However, the Task Force cautions againstthe use of the magnet over an ICD.†† In addition, an
� Most current CRMDs have an x-ray code that can be used to identify themanufacturer of the device.
# The VVT mode (with attention to the upper rate limit) might also beconsidered for a patient with ventricular ectopy where concern exists regardingR-on-T pacing during an asynchronous pacing mode. However, the upper pacingrate during VVT mode is manufacturer- and possibly generator-specific and canapproach 200 beats/min for many devices. Generally, VVT mode pacing wouldnot be a consideration except in very rare circumstances. Before using the VVTmode, a cardiologist and the generator manufacturer should be consulted todetermine the suitability of the upper pacing rate for any patient.
** A magnet correctly applied to a pacemaker often results in asynchronouspacemaker function at a predetermined rate without rate responsiveness. Themagnet rate and response varies by manufacturer. Magnet response can beaffected by programming and remaining battery life. The magnet rate may beexcessive for some patients. Some pacemakers may have no magnet response.
†† Magnet application to an ICD rarely alters bradycardia pacing rate andfunction. A magnet correctly applied to an ICD often results in suspension oftachyarrhythmia therapy. For most ICDs, there is no reliable means to detectappropriate magnet placement. Some ICDs may have no magnet response. SomeICDs can be permanently disabled by magnet application.
188 PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

ICD’s antitachyarrhythmia functions should be sus-pended, if present. For ICD patients who depend onpacing function for control of bradyarrhythmia, thesefunctions should be altered by programming as notedabove. Consultation with a cardiologist or pacemaker–ICD service may be necessary.
For all CRMDs, consider advising the individual per-forming the procedure to use a bipolar electrocauterysystem or an ultrasonic scalpel when applicable. Tem-porary pacing and defibrillation equipment should beimmediately available before, during, and after aprocedure.
Finally, the Task Force believes that anesthetic tech-niques do not influence CRMD function. However, an-esthetic-induced physiologic changes (i.e., cardiac rate,rhythm, or ischemia) in the patient may induce unex-pected CRMD responses or adversely affect the CRMD–patient interaction.
III. Intraoperative ManagementThe primary activities associated with intraoperative
management of a CRMD include (1) monitoring theoperation of the device; (2) preventing potential CRMDdysfunction; and (3) performing emergency defibrilla-tion, cardioversion, or heart rate support.
1. Monitoring. Intraoperative monitoring includescontinuous electrocardiography as well as monitoring ofthe peripheral pulse (e.g., palpation of the pulse, auscul-tation of heart sounds, monitoring of a tracing of intraar-terial pressure, ultrasound peripheral pulse monitoring,or pulse plethysmography or oximetry).45 Although nocontrolled trials were found that examine the clinicalimpact of electrocardiography or peripheral pulse mon-itoring for CRMD patients, case reports note the impor-tance of intraoperative electrocardiographic monitoringin the detection of pacemaker or cardiac dysfunction forthese patients.4,46–50 The majority of Consultants andASA and HRS members agree that (1) continuous elec-trocardiographic monitoring should be done for allCRMD patients and (2) continuous peripheral pulsemonitoring should be conducted.
Advisory. Electrocardiography and peripheral pulsemonitoring are important components of perioperativetreatment of patients with CRMDs. The Task Forceagrees that a patient’s electrocardiogram should be con-tinuously displayed, as required by ASA standards, fromthe beginning of anesthesia until the patient is trans-ferred out of the anesthetizing location, with additionalelectrocardiographic monitoring in the postoperativeperiod as indicated by the patient’s medical condi-tion.45,51 The Task Force believes that these standards
should apply to all CRMD patients receiving general orregional anesthesia, sedation, or monitored anesthesiacare. Continuous peripheral pulse monitoring should beperformed for all CRMD patients receiving general orregional anesthesia, sedation, or monitored anesthesiacare. If unanticipated device interactions are found, con-sider discontinuation of the procedure until the sourceof interference can be eliminated or managed.
2. Managing Potential Sources of EMI. Proceduresusing electrocautery, radiofrequency ablation, litho-tripsy, MRI, or radiation therapy may damage CRMDs orinterfere with CRMD function, potentially resulting insevere adverse outcomes. Sources of EMI are oftenunique to specific procedures, and the management ofeach of these potential EMI sources is reported sepa-rately below.
A. Electrocautery. Management of potential sources ofEMI associated with electrocautery includes (1) assuringthat the cautery tool and current return pad‡‡ are posi-tioned so that the current pathway does not passthrough or near the CRMD pulse generator and leads; (2)avoiding proximity of the cautery’s electrical field to thepulse generator or leads; (3) using short, intermittent,and irregular bursts at the lowest feasible energy levels;and (4) using a bipolar electrocautery system or an ul-trasonic (harmonic) scalpel, if possible.
Two case reports52,53 and one observational study54
suggest that EMI may occur despite positioning the cur-rent return pad as far as possible away from the gener-ator and leads. However, the majority of Consultants andASA and HRS members agree that the current return padshould be positioned so that the electrosurgical currentpathway does not pass through or near the CRMD pulsegenerator or leads.
One case report suggested that application of unipolarelectrocautery on the sternum resulted in completepacemaker inhibition.55 Although some manufacturerssuggest substituting bipolar for monopolar electrocau-tery to minimize CRMD interactions, no clinical litera-ture was found to support this recommendation. Themajority of Consultants and ASA and HRS members agreethat direct contact between the electrocautery systemand the CRMD pulse generator or its leads should beavoided.
Although no recent studies were found examining thebenefit of using short, intermittent bursts at the lowestfeasible energy levels, earlier literature§§ suggests thatshort, intermittent bursts may be useful in completingprocedures without no1table EMI interference.56–60 Themajority of Consultants and ASA and HRS members agreethat short, intermittent bursts should be performed.
Finally, case reports suggest that surgery for pace-maker patients may proceed uneventfully when bipolarelectrocautery systems42,43,46 or harmonic scalpels61,62 areused. The majority of Consultants and ASA and HRS mem-bers agree that bipolar electrocautery systems should be
‡‡ Although commonly referred to as the “grounding pad,” most operatingroom power supplies in the United States are ungrounded.
§§ See appendix 3 for an explanation of the term earlier literature.
189PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

used when possible. The majority of Consultants and ASAmembers agree that harmonic scalpels should be usedwhen possible, and HRS members are equivocal.
B. Radiofrequency Ablation. Management of potentialsources of EMI associated with radiofrequency ablationprimarily involves keeping the radiofrequency currentpath (electrode tip to current return pad) as far awayfrom the pulse generator and lead system as possible.One observational study reports 3 of 12 cases that re-sulted in a significant decrease in resistance on the pace-maker leads when radiofrequency ablation was used inproximity to the leads.63 One case report suggests thatpositioning of the radiofrequency ablation cluster elec-trode no closer than 5 cm from the pacer leads allowedthe procedure to continue uneventfully.40 The majorityof Consultants and ASA and HRS members agree that theindividual performing the procedure should avoid directcontact between the ablation catheter and the CRMDand leads and should keep the radiofrequency ablationcurrent path as far away from the pulse generator andlead system as possible.
C. Lithotripsy. Management of potential sources of EMIassociated with lithotripsy includes (1) avoiding focus ofthe lithotripsy beam near the pulse generator and (2)disabling atrial pacing if the lithotripsy system triggerson the R wave. The literature is silent regarding thebenefits of focusing the lithotripsy beam away from thepulse generator as well as the benefits of disabling atrialpacing during lithotripsy. The majority of Consultantsand ASA and HRS members agree that focusing the lith-otripsy beam near the pulse generator should beavoided, and all three groups are equivocal regardingwhether atrial pacing should be disabled before a pro-cedure if the lithotripsy system triggers on the R wave.
D. Magnetic Resonance Imaging. The literature is notsufficiently rigorous to examine the effects of specificmanagement activities related to CRMD patients receiv-ing MRI. Some descriptive studies and case reports sug-gest that MRI may be completed without notable EMIunder specific circumstances and with appropriate pa-tient qualification and monitoring.30,31,64–71 However,other literature generally suggests that MRI is contrain-dicated.21–29 The majority of Consultants and ASA andHRS members generally agree that MRI is contraindi-cated for all CRMD patients.
E. Radiation Therapy. The literature does not providesufficient guidance regarding specific management activ-ities related to CRMD patients undergoing radiation ther-apy. However, none of the Consultants or HRS membersand only 10% of the ASA members agree that radiation
therapy is contraindicated for all CRMD patients. Fifty-seven percent of the Consultants, 59% of the HRS mem-bers, and 37% of the ASA members agree that radiationtherapy is contraindicated for some but not all CRMDpatients, whereas 43% of the Consultants, 41% of theHRS members, and 53% of the ASA members agree thatradiation therapy is not contraindicated for any CRMDpatient.
F. Electroconvulsive Therapy. No clinical studies werefound that report EMI effects or permanent CRMD mal-function associated with ECT. One study reports twocases where patients’ ICDs were turned off before ECTbut does not report the effect of the therapy on ICDfunction.72 However, the author indicates that treatmentwith ECT might be associated with significant cardiacrisks. Transient electrocardiographic changes (e.g., in-creased P-wave amplitude, altered QRS shape, T-waveand ST-T abnormalities) may result from ECT, and addi-tional cardiac complications (e.g., arrhythmia or isch-emia) may occur in patients with preexisting cardiacdisease. Finally, physiologic stresses after ECT, such as aperiod of bradycardia and reduced blood pressure, fol-lowed by tachycardia and an increase in blood pressure,may account for cardiac failure in the extended postop-erative period (i.e., several hours or days after ECT)among patients with marginal cardiac function.
Advisory. The Task Force believes that EMI could beminimized during certain procedures using a variety ofintraoperative management techniques.
The Task Force agrees that the risk of intraoperativeinterference from electrocautery systems may be mini-mized by (1) positioning the cautery tool and currentreturn pad so that the current pathway does not passthrough or near the CRMD system� �; (2) avoiding prox-imity of the cautery’s electrical field to the pulse gener-ator and leads, including avoidance of waving the acti-vated electrode over the generator##; (3) using short,intermittent, and irregular bursts at the lowest feasibleenergy levels; and (4) using bipolar electrocautery sys-tems or ultrasonic (harmonic) scalpels if possible. Advis-ing or reminding the individual performing the proce-dure to implement these management techniquesshould be considered.
Risk of interference from radiofrequency ablation maybe reduced by avoiding direct contact between the ab-lation catheter and the pulse generator and leads and bykeeping the radiofrequency’s current path (electrode tipto current return pad) as far away from the pulse generatorand leads as possible. During all radiofrequency ablativeprocedures, consider discussing with the individual per-forming the procedure any concerns regarding the prox-imity of the ablation catheter to the CRMD leads.
During lithotripsy, the lithotripsy beam should not befocused near the pulse generator. If the lithotripsy sys-tem triggers on the R wave, atrial pacing might need tobe disabled before the procedure.
� � For some cases, the electrosurgical receiving plate will need to be placedon a site different from the thigh. For example, in head and neck cases, thereceiving plate can be placed on the posterior superior aspect of the shouldercontralateral to the generator position.
## An inhibitory effect could occur even when the active electrode of theelectrocautery is not touching the patient.
190 PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

The Task Force believes that MRI is generally contra-indicated for CRMD patients. If MRI must be performed,consult with the ordering physician, the patient’s pace-maker specialist or cardiologist, the diagnostic radiolo-gist, and the CRMD manufacturer.
The Task Force believes that radiation therapy can besafely performed for CRMD patients.*** The device mustbe outside the field of radiation. Therefore, some pulsegenerators will require surgical relocation before com-mencing radiation. Most manufacturers recommend ver-ification of pulse generator function during and at thecompletion of radiation. Problems may include pace-maker failure and runaway pacemaker.†††
Although transient or long-term myocardial and ner-vous system effects may be associated with ECT, theTask Force believes that such therapies may be admin-istered to CRMD patients without significant damage toa disabled CRMD. If ECT must be performed, consultwith the ordering physician and the patient’s cardiolo-gist to plan for the first and subsequent ECTs. All CRMDsshould undergo a comprehensive interrogation beforethe procedure(s). ICD functions should be disabled forshock therapy during ECT; however, be prepared totreat ventricular arrhythmias that occur secondary to thehemodynamic effects of ECT. CRMD-dependent patientsmay require a temporary pacing system to preserve car-diac rate and rhythm during shock therapy. Also, theCRMD may require programming to asynchronous activ-ity to avoid myopotential inhibition of the device inpacemaker-dependent patients.
3. Emergency Defibrillation or Cardioversion.During the perioperative period, emergency defibrilla-tion or cardioversion may become necessary for a CRMDpatient. In this case, the primary concern is to minimizethe current flowing through the pulse generator and leadsystem. Recent and earlier case reports suggest thatoptimal positioning of the defibrillation or cardioversionpads or paddles may be an important factor in the pre-vention of adverse CRMD-related outcomes.73–77 Themajority of Consultants and ASA and HRS members agreethat the defibrillation or cardioversion pads should bepositioned as far as possible from the pulse generator.The majority of Consultants and ASA and HRS membersalso agree that the anterior–posterior position should beused and that a clinically appropriate energy outputshould be used regardless of the type of CRMD.
Advisory. The Task Force believes that before at-tempting emergency defibrillation or cardioversion of apatient with an ICD and magnet-disabled therapies, all
sources of EMI should be terminated, and the magnetshould be removed to reenable antitachycardia therapies.The patient should then be observed for appropriateCRMD therapy. For patients with an ICD and antiarrhyth-mic therapies that have been disabled by programming,consider reenabling therapies through programming. If theabove activities do not restore ICD function, proceed withemergency external defibrillation or cardioversion.
Overriding the above discussion is the need to followexisting Advanced Cardiac Life Support and emergencyguidelines78 to provide rapid cardioversion or defibrilla-tion, and attention should be turned to providing thistherapy as quickly as possible.
If a life-threatening arrhythmia occurs, follow Ad-vanced Cardiac Life Support guidelines for energy leveland for paddle placement. If possible, attempt to mini-mize the current flowing through the pulse generatorand lead system by (1) positioning the defibrillation orcardioversion pads or paddles as far as possible from thepulse generator and (2) positioning defibrillation or car-dioversion pads or paddles perpendicular to the majoraxis of the CRMD pulse generator and leads to the extentpossible by placing them in an anterior–posterior loca-tion. A clinically appropriate energy output should al-ways be used regardless of the presence of a CRMD, andthe paddles should be positioned as best as can be donein an emergency.
IV. Postoperative ManagementPostoperative treatment of CRMD patients primarily
consists of interrogating and restoring CRMD function.Although no recent studies were found examining out-comes associated with interrogating or restoring CRMDfunction, an earlier case report indicates that postoper-ative evaluation resulted in the discovery and correctionof a pacemaker problem.79 The majority of Consultantsand ASA and HRS members agree that postoperativepatient treatment should include interrogating and re-storing CRMD function in the postanesthesia care unit orintensive care unit.
Advisory. The Task Force believes that cardiac rateand rhythm should be continuously monitored through-out the immediate postoperative period. Backup pacingcapability and cardioversion–defibrillation equipmentshould be immediately available at all times.
Postoperative interrogation and restoration of CRMDfunction are basic elements of postoperative manage-ment. The CRMD first should be interrogated to assesspostoperative device functions. If interrogation deter-mines that CRMD settings are inappropriate, the deviceshould be reprogrammed to appropriate settings. For anICD, all antitachyarrhythmic therapies should be re-stored. Consultation with a cardiologist or pacemaker–ICD service may be necessary.
*** Radiation shielding may not be feasible for some patients because of thesize and weight of the shield. This may be compensated for by relocating thegenerator.
††† Runaway pacemaker is a potentially catastrophic pulse generator mal-function characterized by the sudden onset of rapid, erratic pacing. Runawaypacemaker is the result of multiple internal component failure, and it is relativelyuncommon in modern devices. Circuitry in modern pacemakers (and ICDs)limits the runaway pacing rate to less than 210 beats/min.
191PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

Appendix 1: Generic Pacemaker andDefibrillator Codes
The generic pacemaker and defibrillator codes were developed asjoint projects by the North American Society of Pacing and Electro-
physiology (NASPE)‡‡‡ and the British Pacing and ElectrophysiologyGroup (BPEG).80,81 The five positions refer to the order of the pro-grammed settings on the CRMD (tables 1 and 2).
Table 1. Generic Pacemaker Code (NBG*): NASPE/BPEG Revised (2002)
Position I, PacingChamber(s)
Position II, SensingChamber(s)
Position III, Response(s) toSensing
Position IV,Programmability
Position V, MultisitePacing
O � none O � none O � none O � none O � noneA � atrium A � atrium I � inhibited R � rate modulation A � atriumV � ventricle V � ventricle T � triggered V � ventricleD � dual (A � V) D � dual (A � V) D � dual (T � I) D � dual (A � V)
Examples:
AAI � Atrial-only antibradycardia pacing. In the AAI mode, any failure of the atrium to produce an intrinsic event within the appropriate time window (determined by the lowerrate limit) results in an atrial pacing pulse emission. There is no ventricular sensing; thus, a premature ventricular event will not likely reset the pacing timer.
AOO � Asynchronous atrial-only pacing. In this mode, the pacing device emits a pacing pulse regardless of the underlying cardiac rhythm.
DDD � Dual-chamber antibradycardia pacing function in which every atrial event, within programmed limits, is followed by a ventricular event. The DDD modeimplies dual-chamber pacing with atrial tracking. In the absence of intrinsic activity in the atrium, it will be paced, and, after any sensed or paced atrialevent, an intrinsic ventricular event must occur before the expiration of the atrioventricular timer or the ventricle will be paced.
DDI � Dual-chamber behavior in which the atrial activity is tracked into the ventricle only when the atrial event is created by the antibradycardia pacing functionof the generator. In the DDI mode, the ventricle is paced only when no intrinsic ventricular activity is present.
DOO � Asynchronous atrioventricular sequential pacing without regard to the underlying cardiac rhythm.
VOO � Asynchronous ventricular-only pacing without regard to the underlying cardiac rhythm.
VVI � Ventricular-only antibradycardia pacing. In the VVI mode, any failure of the ventricle to produce an intrinsic event within the appropriate time window(determined by the lower rate limit) results in a ventricular pacing pulse emission. There is no atrial sensing; thus, there can be no atrioventricular synchronyin a patient with a VVI pacemaker and any intrinsic atrial activity.
* NBG: N refers to NASPE, B refers to BPEG, and G refers to generic.
Table 2. Generic Defibrillator Code (NBD): NASPE/BPEG
Position I, ShockChamber(s)
Position II,Antitachycardia
Pacing Chamber(s)Position III,
Tachycardia Detection
Position IV,*Antibradycardia
Pacing Chamber(s)
O � none O � none E � electrogram O � noneA � atrium A � atrium H � hemodynamic A � atriumV � ventricle V � ventricle V � ventricleD � dual (A � V) D � dual (A � V) D � dual (A � V)
* For robust identification, position IV is expanded into its complete NBG code. For example, a biventricular pacing–defibrillator with ventricular shock andantitachycardia pacing functionality would be identified as VVE-DDDRV, assuming that the pacing section was programmed DDDRV. Currently, no hemodynamicsensors have been approved for tachycardia detection (position III).
‡‡‡ Now called the Heart Rhythm Society (HRS).
192 PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

Appendix 2: Summary of Practice Advisory
Preoperative Evaluation● Establish whether a patient has a CRMD.
- Conduct a focused history (patient interview, medical records review, review of available chest x-ray films, electrocardiogram, or any available monitoror rhythm strip information).
- Conduct a focused physical examination (check for scars, palpate for device).● Define the type of CRMD.
- Obtain manufacturer’s identification card from patient or other source.- Order chest x-ray studies if no other data are available.- Refer to supplemental resources (e.g., manufacturer’s databases).
● Determine dependency on pacing function of the CRMD.- History of symptomatic bradyarrhythmia resulting in CRMD implantation.- History of successful atrioventricular nodal ablation.- Inadequate escape rhythm at lowest programmable pacing rate.
● Determine CRMD function.- Interrogate device (consultation with a cardiologist or pacemaker–ICD service may be necessary).- Determine whether the device will capture when it paces (i.e., produce a mechanical systole with a pacemaker impulse).- Consider contacting the manufacturer for perioperative recommendations.
Preoperative Preparation● Determine whether EMI is likely to occur during the planned procedure.● Determine whether reprogramming pacing function to asynchronous mode or disabling rate responsive function is advantageous.● Suspend antitachyarrhythmia functions if present.● Advise individual performing the procedure to consider use of a bipolar electrocautery system or ultrasonic (harmonic) scalpel.● Temporary pacing and defibrillation equipment should be immediately available.● Evaluate the possible effects of anesthetic techniques and of the procedure on CRMD function and patient CRMD interactions.
Intraoperative Management● Monitor operation of the CRMD.
- Conduct electrocardiographic monitoring per ASA standard.- Monitor peripheral pulse (e.g., manual pulse palpation, pulse oximeter plethysmogram, arterial line).
● Manage potential CRMD dysfunction due to EMI.- Electrocautery.
y Assure that the electrosurgical receiving plate is positioned so that the current pathway does not pass through or near the CRMD system. Forsome cases, the receiving plate might need to be placed on a site different from the thigh (e.g., the superior posterior aspect of the shouldercontralateral to the generator position for a head and neck case).
y Advise individual performing the procedure to avoid proximity of the cautery’s electrical field to the pulse generator or leads.y Advise individual performing the procedure to use short, intermittent, and irregular bursts at the lowest feasible energy levels.y Advise individual performing the procedure to reconsider the use of a bipolar electrocautery system or ultrasonic (harmonic) scalpel in place of a
monopolar electrocautery system, if possible.- Radiofrequency ablation.
y Advise individual performing the procedure to avoid direct contact between the ablation catheter and the pulse generator and leads.y Advise individual performing the procedure to keep the radiofrequency’s current path as far away from the pulse generator and lead system as possible.
- Lithotripsy.y Advise individual performing the procedure to avoid focusing the lithotripsy beam near the pulse generator.y If the lithotripsy system triggers on the R wave, consider preoperative disabling of atrial pacing.
- MRI.y MRI is generally contraindicated in patients with CRMDs.y If MRI must be performed, consult with the ordering physician, the patient’s cardiologist, the diagnostic radiologist, and the CRMD manufacturer.
- Radiation therapy.y Radiation therapy can be safely performed in patients who have CRMDs.y Surgically relocate the CRMD if the device will be in the field of radiation.
- Electroconvulsive therapy.y Consult with the ordering physician, the patient’s cardiologist, a CRMD service, or the CRMD manufacturer.
● Emergency defibrillation or cardioversion.- For a patient with an ICD and magnet-disabled therapies:
y Advise individual performing the procedure to terminate all sources of EMI while magnet is removed.y Remove the magnet to reenable antitachycardia therapies.y Observe the patient and the monitors for appropriate CRMD therapy.y If the above activities do not restore ICD function, proceed with emergency external defibrillation or cardioversion.
- For a patient with an ICD and programming-disabled therapies:y Advise individual performing the procedure to terminate all sources of EMI while magnet is removed.y Reenable therapies through programming if the programmer is immediately available and ready to be used.y Observe the patient and the monitors for appropriate CRMD therapy.y If the above activities do not restore ICD function, proceed with emergency external defibrillation or cardioversion.
- For external defibrillation:y Position defibrillation/cardioversion pads or paddles as far as possible from the pulse generator.y Position defibrillation/cardioversion pads or paddles perpendicular to the major axis of the CRMD to the extent possible by placing them in an
anterior–posterior location.y If it is technically impossible to place the pads or paddles in locations that help to protect the CRMD, defibrillate/cardiovert the patient in the
quickest possible way and be prepared to provide pacing through other routes.y Use a clinically appropriate energy output.
Postoperative Management● Continuously monitor cardiac rate and rhythm and have backup pacing and defibrillation equipment immediately available throughout the immediate
postoperative period.● Interrogate and restore CRMD function in the immediate postoperative period.
- Interrogate CRMD; consultation with a cardiologist or pacemaker–ICD service may be necessary.- Restore all antitachyarrhythmic therapies in ICDs.- Assure that all other settings of the CRMD are appropriate.
Refer to Table 3 for an example of a stepwise approach to the perioperative treatment of the patient with a CRMD.
ASA � American Society of Anesthesiologists; CRMD � cardiac rhythm management device; EMI � electromagnetic interference; ICD � implantablecardioverter–defibrillator; MRI � magnetic resonance imaging.
193PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

Table 3. Example of a Stepwise Approach to the Perioperative Treatment of the Patient with a CRMD
Perioperative Period Patient/CRMD Condition Intervention
Preoperative evaluation Patient has CRMD ● Focused history● Focused physical examination
Determine CRMD type (pacemaker,ICD, CRT)
● Manufacturer’s CRMD identification card● Chest x-ray studies (no data available)● Supplemental resources*
Determine whether patient is CRMD-dependent for pacing function
● Verbal history● Bradyarrhythmia symptoms● Atrioventricular node ablation● No spontaneous ventricular activity†
Determine CRMD function ● Comprehensive CRMD evaluation‡● Determine whether pacing pulses are present and create paced beats
Preoperative preparation EMI unlikely during procedure ● If EMI unlikely, special precautions are not needed
EMI likely: CRMD is pacemaker ● Reprogram to asynchronous mode when indicated● Suspend rate-adaptive functions§
EMI likely: CRMD is ICD ● Suspend antitachyarrhythmia functions● If patient is dependent on pacing function, alter pacing functions as above
EMI likely: all CRMD ● Use bipolar cautery; ultrasonic scalpel● Temporary pacing and external cardioversion–defibrillation available
Intraoperative physiologic changeslikely (e.g., bradycardia, ischemia)
● Plan for possible adverse CRMD–patient interaction
Intraoperativemanagement
Monitoring ● Electrocardiographic monitoring per ASA standard● Peripheral pulse monitoring
Electrocautery interference ● CT/CRP—no current through PG/leads● Avoid proximity of CT to PG/leads● Short bursts at lowest possible energy● Use bipolar cautery; ultrasonic scalpel
Radiofrequency catheter ablation ● Avoid contact of radiofrequency catheter with PG/leads● Radiofrequency current path far away from PG/leads● Discuss these concerns with operator
Lithotripsy ● Do not focus lithotripsy beam near PG● R wave triggers lithotripsy? Disable atrial pacing�
MRI ● Generally contraindicated● If required, consult ordering physician, cardiologist, radiologist, and
manufacturer
RT ● PG/leads must be outside of RT field● Possible surgical relocation of PG● Verify PG function during/after RT course
ECT ● Consult with ordering physician, patient’s cardiologist, a CRMD service, orCRMD manufacturer
Emergency defibrillation–cardioversion
ICD: magnet disabled ● Terminate all EMI sources● Remove magnet to reenable therapies● Observe for appropriate therapies
ICD: programming disabled ● Programming to reenable therapies or proceed directly with externalcardioversion–defibrillation
ICD: either of above ● Minimize current flow through PG/leads● PP as far as possible from PG● PP perpendicular to major axis PG/leads● To extent possible, PP in anterior–posterior location
Regardless of CRMD type ● Use clinically appropriate cardioversion/defibrillation energy
Postoperativemanagement
Immediate postoperative period ● Monitor cardiac R&R continuously● Backup pacing and cardioversion/defibrillation capability
Postoperative interrogation andrestoration of CRMD function
● Interrogation to assess function● Settings appropriate?#● Is CRMD an ICD?**● Use cardiology/pacemaker–ICD service if needed
* Manufacturer’s databases, pacemaker clinic records, cardiology consultation. † With cardiac rhythm management device (CRMD) programmed VVI at lowestprogrammable rate. ‡ Ideally CRMD function assessed by interrogation, with function altered by reprogramming if required. § Most times this will benecessary; when in doubt, assume so. � Atrial pacing spikes may be interpreted by the lithotriptor as R waves, possibly inciting the lithotriptor to deliver a shockduring a vulnerable period in the heart. # If necessary, reprogram appropriate settings. ** Restore all antitachycardia therapies.
CRP � current return pad; CRT � cardiac resynchronization therapy; CT � cautery tool; ECT � electroconvulsive therapy; EMI � electromagnetic interference;ICD � internal cardioverter–defibrillator; MRI � magnetic resonance imaging; PG � pulse generator; PP � external cardioversion–defibrillation pads or paddles;R&R � rhythm and rate; RT � radiation therapy.
194 PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

Appendix 3: Literature Review andConsensus-based Evidence
A. State of the LiteratureFor this Advisory, a literature review was used in combination with
opinions obtained from experts and other sources (e.g., professionalsociety members, open forums, Web-based postings) to provide guid-ance to practitioners regarding the perioperative treatment of patientswith CRMDs. Both the literature review and opinion data were basedon evidence linkages, consisting of directional statements about rela-tions between specific perioperative management activities and CRMDfunction or clinical outcomes.
A study or report that appears in the published literature is includedin the development of an advisory if the study (1) is related to one ofthe specified linkage statements, (2) reports a finding or set of findingsthat can be tallied or measured (e.g., articles that contain only opinionare not included), and (3) is the product of an original investigation orreport (i.e., review articles or follow-up studies that summarize previ-ous findings are not included). Because CRMDs represent a rapidlychanging technology, earlier literature (i.e., literature published before1990) was rarely included in the evaluation of evidence for this Prac-tice Advisory.
Although evidence linkages are designed to assess causality, few ofthe reviewed studies exhibited sufficiently acceptable quantitativemethods and analyses to provide a clear indication of causality. There-fore, the published literature could not be used as a source of quanti-tative support (required for the development of practice guidelines).However, many published studies were evaluated that provided theTask Force with important noncausal evidence. For example, descrip-tive literature (i.e., reports of frequency or incidence) is often useful inproviding an indication of the scope of a problem. Information regard-ing whether a particular adverse outcome is common or rare may haveconsiderable bearing on the practicality of an advisory. Case reportsare typically used as a forum for reporting and recognizing unusual oradverse outcomes and may suggest caution when devising an advisory.
For the literature review, potentially relevant studies were identifiedvia electronic and manual searches of the literature. The electronicsearch covered a 39-yr period from 1966 through 2004. The manualsearch covered a 45-yr period from 1961 through 2005. More than1,500 citations were initially identified, yielding a total of 411 nonover-lapping articles that addressed topics related to the evidence linkages.After review of the articles, 283 studies did not provide direct evidenceand were subsequently eliminated. A total of 128 articles (from 39journals) contained direct linkage-related evidence. No evidence link-age contained enough studies with well-defined experimental designsand statistical information to conduct a quantitative analysis (i.e.,meta-analysis).
Interobserver agreement among Task Force members and two meth-odologists was established by interrater reliability testing. Agreementlevels using a � statistic for two-rater agreement pairs were as follows:(1) type of study design, � � 0.72–0.90; (2) type of analysis, � �0.80–0.90; (3) evidence linkage assignment, � � 0.84–1.00; and (4)literature inclusion for database, � � 0.70–1.00. Three-rater chance-corrected agreement values were (1) study design, Sav � 0.81, Var(Sav) � 0.010; (2) type of analysis, Sav � 0.86, Var (Sav) � 0.009; (3)linkage assignment, Sav � 0.82, Var (Sav) � 0.005; and (4) literaturedatabase inclusion, Sav � 0.78, Var (Sav) � 0.031. These valuesrepresent moderate to high levels of agreement.
Future studies should focus on prospective methodologies, whenpossible, that use traditional hypothesis testing techniques. Use of thefollowing methodologic procedures for assessing the impact of peri-operative management of CRMDs is recommended: (1) comparisonstudies (i.e., one technique vs. another) when clinically feasible; (2)randomization; and (3) full reporting of sample size, effect size esti-mates, test scores, measures of variability, and P values.
B. Consensus-based EvidenceConsensus was obtained from multiple sources, including (1) survey
opinion from Consultants who were selected based on their knowl-edge or expertise in perioperative management of CRMDs, (2) surveyopinions from randomly selected samples of active members of theAmerican Society of Anesthesiologists and active members of the HRS,(3) testimony from attendees of two publicly held open forums at anational anesthesia meeting and at a major cardiology meeting,§ § §(4) Internet commentary, and (5) Task Force opinion and interpreta-tion. The survey rate of return was 56% (n � 23 of 41) for Consultants,15% (n � 89 of 600) for the ASA membership, and 15% (n � 44 of 300)for the HRS membership. Survey results are presented in the text of thedocument and in table 4.
The ASA Consultants were also asked to indicate which, if any, of theevidence linkages would change their clinical practices if the Advisorywas instituted. The rate of return was 39% (n � 16 of 41). The percentof responding Consultants expecting no change associated with eachlinkage were as follows: preoperative evaluation—67%; preoperativepatient preparation—67%; intraoperative monitoring of CRMDs—67%; emergency defibrillation or cardioversion—87%; postoperativemonitoring of CRMDs—73%; postoperative interrogation and restora-tion of CRMD function—60%; intraoperative management of EMI dur-ing: electrocautery—73%, radiofrequency ablation—73%, lithotripsy—80%, MRI—80%, radiation therapy—80%, and electroconvulsivetherapy—73%. Forty percent of the respondents indicated that theAdvisory would have no effect on the amount of time spent on a typicalcase. Nine respondents (60%) indicated that there would be an in-crease in the amount of time they would spend on a typical case withthe implementation of this Advisory. The amount of increased timeanticipated by these respondents ranged from 5 to 30 min.
§ § § International Anesthesia Research Society; 78th Clinical and ScientificCongress, Tampa, Florida, March 28, 2004, and NASPE Heart Rhythm SocietyAnnual Meeting, San Francisco, California, May 20, 2004.
195PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

Table 4. Consultant and Membership Survey Responses: Percent Agreement/Disagreement*
Survey Item
Consultants ASA Members HRS Members
n % Agree/Disagree n % Agree/Disagree n % Agree/Disagree
1. To perform a preoperative evaluation:Establish whether a patient has a CRMD. 23 100/0 89 100/0 44 100/0Define the type of device. 23 100/0 87 95/0 44 100/0Determine whether a patient is CRMD dependent for
pacemaking function.23 96/0 89 96/0 44 96/4
Determine CRMD function. 23 96/0 89 88/3 44 71/112. To prepare a CRMD patient for a procedure:
Determine whether EMI is likely to occur. 23 96/4 89 91/2 44 96/2Turn pacemaking rate-adaptive therapy off. 23 52/35 89 35/35 44 34/34Program pacemaking function to asynchronous mode:
All CRMD patients. 22 0/82 88 21/48 43 9/84Pacemaker-dependent patients only. 22 73/23 83 47/27 43 54/28
Suspend antitachyarrhythmia functions. 21 86/5 87 54/21 43 63/21Consider using a bipolar electrocautery system (when
applicable).22 91/0 86 90/2 44 77/14
Consider using an ultrasonic (harmonic) scalpel (whenapplicable).
22 68/18 88 63/3 44 34/9
Assure the availability of temporary pacing anddefibrillation equipment.
22 100/0 87 95/1 44 89/7
Consider the possible effects of anesthetic agents ortechniques on CRMD function.
22 64/18 86 779 44 66/21
3. Intraoperative monitoring should include:Continuous electrocardiography. 23 100/0 88 100/0 44 100/0Continuous peripheral pulse monitoring. 23 96/0 88 86/11 44 61/18
4. For procedures using electrocautery:Position the electrosurgical receiving plate so current
pathway does not pass through or near the generator orleads.
23 100/0 88 97/0 44 96/0
Avoid proximity of the cautery’s electrical field to thepulse generator or leads.
23 100/0 87 100/0 44 96/2
Use short, intermittent, and irregular bursts at the lowestfeasible energy levels.
23 96/0 87 83/2 44 91/7
Use a bipolar electrocautery system (when applicable). 23 91/0 88 94/1 44 84/2Use an ultrasonic (harmonic) scalpel (when applicable). 23 57/13 88 65/1 44 41/9
5. For radiofrequency ablation:Avoid direct contact between the ablation catheter and
the CRMD and leads.23 83/0 87 76/0 44 91/2
Keep the current path (electrode tip to return plate) as faraway from the pulse generator and lead system aspossible.
23 87/0 87 78/0 44 89/5
6. For lithotripsy:Avoid focusing the lithotripsy beam near the pulse
generator.23 91/0 86 78/1 44 86/0
If the lithotripsy system triggers on the R wave, disableatrial pacing before procedure.
23 39/26 86 38/13 44 39/9
7. For MRI:†
MRI is contraindicated for all CRMD patients. 21 81 79 80 44 55MRI is contraindicated for some but not all CRMD
patients.21 19 79 18 44 39
MRI is not contraindicated for any CRMD patient. 21 0 79 2 44 68. For RT:†
RT is contraindicated for all CRMD patients. 21 0 73 10 44 0RT is contraindicated for some but not all CRMD patients. 21 57 73 37 44 59RT is not contraindicated for any CRMD patient. 21 43 73 53 44 41
9. For emergency defibrillation or cardioversion:Position the defibrillation or cardioversion pads as far as
possible from the pulse generator.23 83/0 87 69/13 44 91/7
Use an anterior–posterior position. 23 74/9 84 61/6 44 68/25Use a clinically appropriate energy output regardless of
the device.23 100/0 87 87/0 44 100/0
10. To treat CRMD patients postoperatively:Interrogate and restore CRMD function in the PACU or
ICU.23 96/4 88 98/1 44 77/21
* The percentages of respondents who agreed/disagreed with each item are presented. The percentages of respondents who were uncertain are notpresented. † Respondents were asked to select one of the three choices. Therefore, the numbers represent percent agreement only.
ASA � American Society of Anesthesiologists; CRMD � cardiac rhythm management device; EMI � electromagnetic interference; HRS � Heart Rhythm Society;ICU � intensive care unit; MRI � magnetic resonance imaging; PACU � postanesthesia care unit; RT � radiation therapy.
196 PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

References � � �1. Barold S, Zites D: Cardiac pacemakers and antiarrhythmic devices, Heart
Disease, 5th edition. Edited by Braunwald E. Philadelphia, WB Saunders, 1997, pp705–41
2. Mychaskiw G, Eichhorn JH: Interaction of an implanted pacemaker with atransesophageal atrial pacemaker: Report of a case. J Clin Anesth 1999; 11:669–71
3. Purday JP, Towey RM: Apparent pacemaker failure caused by activation ofventricular threshold test by a magnetic instrument mat during general anaes-thesia. Br J Anaesth 1992; 69:645–6
4. Kellow NH: Pacemaker failure during transurethral resection of the pros-tate. Anesthesia 1993; 48:136–8
5. Bernstein AD, Irwin ME, Parsonnet V, Wilkoff BL, Black WR, BuckinghamTA, Maloney JD, Reynolds DD, Saksena S, Singer I, Nickelson DE, Schurig L:Report of the NASPE policy conference on antibradycardia pacemaker follow-up:Effectiveness, needs and resources. Pacing Clin Electrophysiol 1994; 17:1714–29
6. Ahern TS, Luckett C, Ehrlich S, Pena EA: Use of bipolar electrocautery inpatients with implantable cardioverter-defibrillators: No reason to inactivatedetection or therapies. PACE 1999; 22:776
7. Bailey AG, Lacey SR: Intraoperative pacemaker failure in an infant. Can JAnaesth 1991; 38:912–3
8. El-Gamal HM, Dufresne RG, Saddler K: Electrosurgery, pacemakers andICDs: A survey of precautions and complications experienced by cutaneoussurgeons. Dermatol Surg 2001; 27:385–90
9. Rozner MA: Review of electrical interference in implanted cardiac devices.PACE 2003; 26:923–5
10. Wilson JH, Lattner S, Jacob R, Stewart R: Electrocautery does not interferewith the function of the automatic implantable cardioverter defibrillator. AnnThorac Surg 1991; 51:225–6
11. Wong DT, Middleton W: Electrocautery-induced tachycardia in a rate-responsive pacemaker. ANESTHESIOLOGY 2001; 94:10–1
12. Chang AC, McAreavey D, Tripodi D, Fananapazir L: Radiofrequency cath-eter atrioventricular node ablation in patients with permanent cardiac pacingsystems. Pacing Clin Electrophysiol 1994; 17:65–9
13. Chin MC, Rosenqvist M, Lee MA, Griffin JC, Langberg JJ: The effect ofradiofrequency catheter ablation on permanent pacemakers: An experimentalstudy. Pacing Clin Electrophysiol 1990; 13:23–9
14. de Chillou C, Sadoul N Beurrier D, Bizeau O, Aliot E, Dodinot B: Effects ofradiofrequency catheter ablation on the behavior of permanent pacemakers.Pacing Clin Electrophysiol 1996; 19:680
15. Ellenbogen KA, Wood MA, Stambler BS: Acute effects of radiofrequencyablation of atrial arrhythmias on implanted permanent pacing systems. PacingClin Electrophysiol 1996; 19:1287–95
16. Pfeiffer D, Tebbenjohanns J, Schumacher B, Jung W, Luderitz B: Pace-maker function during radiofrequency ablation. Pacing Clin Electrophysiol 1995;18:1037–44
17. Pfeiffer D, Tebbenjohanns J, Schumacher B, Jung W, Manz M, Luderitz B:Pacemaker behaviour during radiofrequency current delivery. J Am Coll Cardiol1994; 23(suppl A):324A
18. Moore S, Firstenberg M, Simmons TW, Trohman R: The interaction be-tween radiofrequency ablation and permanent pacemakers. Circulation 1992;86(suppl 1):I-449
19. Trohman RG, Simmons TW, Moore SL, Firstenberg MS, Williams D, Ma-loney JD: Catheter ablation of atrioventricular junction using radiofrequencyenergy and a bilateral cardiac approach. Am J Cardiol 1992; 70:1438–43
20. Wolfe DA, McCutcheon MJ, Plumb VJ, Kay N: Radiofrequency current mayinduce exit block in chronically implanted ventricular leads. Pacing Clin Electro-physiol 1995; 18:919
21. Achenbach S, Moshage W, Diem B, Bieberle T, Schibgilla V, Bachmann K:Effects of magnetic resonance imaging on cardiac pacemakers and electrodes.Am Heart J 1997; 134:467–73
22. Fontaine JM, Mohamed FB, Gottlieb, Callans DJ, Marchlinski FE: Rapidventricular pacing in a pacemaker patient undergoing magnetic resonance im-aging. Pacing Clin Electrophysiol 1998; 21:1336–9
23. Garcia-Bolao I, Albaladejo V, Benito A, Alegria E, Zubieta JL: Magneticresonance imaging in a patientv with a dual-chamber pacemaker. Acta Cardiol1998; 53:33–5
24. Gimbel JR, Johnson D, Levine PA, Wilkoff BL: Safe performance of mag-netic resonance imaging on five patients with permanent cardiac pacemakers.Pacing Clin Electrophysiol 1996; 19:913–9
25. Gimbel JR, Lorig RJ, Wilkoff BL: Safe magnetic resonance imaging ofpacemaker patients. J Am Coll Cardiol 1995; 25:11A
26. Hayes DL, Holmes DR Jr, Gray JE: Effect of 1.5 Tesla nuclear magneticresonance imaging scanner on implanted permanent pacemakers. J Am CollCardiol 1987; 10:782–6
27. Luechinger R, Duru F, Scheidegger MB, Boesiger P, Candinas R: Force and
torque effects of a 1.5-Tesla MRI scanner on cardiac pacemakers and ICDs. PacingClin Electrophysiol 2001; 24:199–205
28. Pavlicek W, Geisinger M, Castle L, Borkowski GP, Meaney TF, Bream BL,Gallagher JH: The effects of nuclear magnetic resonance on patients with cardiacpacemakers. Radiology 1993; 147:149–53
29. Vahlhaus C, Sommer T, Lewalter T, Schimpf R, Schumacher B, Jung W,Luderitz B: Interference with cardiac pacemakers by magnetic resonance imag-ing: Are there irreversible changes at 0.5 Tesla? Pacing Clin Electrophysiol 2001;24:489–95
30. Martin ET, Coman JA, Shellock FG, Pulling CC, Fair R, Jenkins K: Magneticresonance imaging and cardiac pacemaker safety at 1.5-Telsa. J Am Coll Cardiol2004; 43:1315–24
31. Rozner MA, Burton AW, Kumar AJ: Pacemaker complication during MRI.J Am Coll Cardiol 2005; 45:161–2
32. Raitt MH, Stalzer KJ, Laramore GE, Bardy GH, Dolack GL, Poole JE,Kudenchuk PJ: Runaway pacemaker during high-energy neutron radiation ther-apy. Chest 1994; 106:955–7
33. Rodriguez F, Filimonov A, Henning A, Coughlin C, Greenberg M: Radia-tion-induced effects in multiprogrammable pacemakers and implantable defibril-lators. Pacing Clin Electrophysiol 1991; 14:2143–53
34. Hurkmans CW, Scheepers E, Springorum BG, De Ruiter GS, Uiterwaal HA:Influence of therapeutic irradiation on the latest generation of pacemakers. HeartRhythm 2004; 1(suppl):S53–4
35. Drach GW, Weber C, Donovan JM: Treatment of pacemaker patients withextracorporeal shock wave lithotripsy: Experience from 2 continents. J Urol1990; 143:895–6
36. Vassolas G, Roth RA, Venditti FJ Jr: Effect of extracorporeal shock wavelithotripsy on implantable cardioverter defibrillator. Pacing Clin Electrophysiol1993; 16:1245–8
37. Theiss M, Wirth MP, Frohmuller HG: Extracorporeal shock wave litho-tripsy in patients with cardiac pacemakers. J Urol 1990; 143:479–80
38. Vaidyanathan S, Hirst R, Parsons KF, Singh G, Soni BM, Oo T, Zaidi A, WattJW, Sett P: Bilateral extracorporeal shock wave lithotripsy in a spinal cord injurypatient with a cardiac pacemaker. Spinal Cord 2001; 39:286–9
39. Venditti FJ Jr, Martin D, Long AL, Roth RA: Renal extracorporeal shockwave lithotripsy performed in patient with implantable cardioverter defibrillator.Pacing Clin Electrophysiol 1991; 14:1323–5
40. Hayes DL, Charboneau JW, Lewis BD, Asirvatham SJ, Dupuy DE, LexvoldNY: Radiofrequency treatment of hepatic neoplasms in patients with permanentpacemakers. Mayo Clin Proc 2001; 76:950–2
41. O’Donoghue JK: Inhibition of a demand pacemaker by electrosurgery.Chest 1973; 64:664–6
42. Smith CL, Frawley G, Hamar A: Diathermy and the telectronics “META”pacemaker. Anaesth Intensive Care 1993; 21:452–4
43. Kleinman B, Hamilton J, Heriman R, Olshansky B, Justus D, Desai R:Apparent failure of a precordial magnet and pacemaker programmer to converta DDD pacemaker to VOO mode during the use of the electrosurgical unit.ANESTHESIOLOGY 1997; 86:247–50
44. Mangar D, Atlas GM, Kane PB: Electrocautery-induced pacemaker malfunc-tion during surgery. Can J Anaesth 1991; 38:616–8
45. American Society of Anesthesiologists: Standards for basic anesthetic mon-itoring, In ASA Standards, Guidelines and Statements. Chicago, American Societyof Anesthesiologists, October 2004
46. Baller MR, Kirsner KM: Anesthetic implications of implanted pacemakers:A case study. AANA J 1995; 63:209–16
47. Celentano WJ, Jahr JS, Nossaman BD: Extracorporeal shock wave litho-tripsy in a patient with a pacemaker. Anesth Analg 1992; 74:770–2
48. Chew EW, Troughear RH, Kuchar DL, Thorburn CW: Inappropriate ratechange in minute ventilation rate responsive pacemakers due to interference bycardiac monitors. Pacing Clin Electrophysiol 1997; 20:276–82
49. Rubin JM, Miller ED: Intraoperative pacemaker malfunction during totalhip arthroplasty. Anesth Analg 1995; 80:410–2
50. Samain E, Marty J, Souron V, Rosencher N, Eyrolle L: Intraoperativepacemaker malfunction during a shoulder arthroscopy. ANESTHESIOLOGY 2000;93:306–7
51. Society of Anesthesiologists: Standards for postanesthesia care, In ASAStandards, Guidelines and Statements. Chicago, American Society of Anesthesi-ologists, October 2004
52. O’Donoghue JK: Inhibition of a demand pacemaker by electrosurgery.Chest 1973; 64:664–6
53. Rubin JM, Miller ED: Intraoperative pacemaker malfunction during totalhip arthroplasty. Anesth Analg 1995; 80:410–2
54. Heller LI: Surgical electrocautery and the runaway pacemaker syndrome.Pacing Clin Electrophysiol 1990; 13:1084–5
55. Mychaskiw G, Eichhorn JH: Interaction of an implanted pacemaker with atransesophageal atrial pacemaker: Report of a case. J Clin Anesth 1999; 11:669–71
56. Batra YK, Bali IM: Effect of coagulating and cutting current on a demandpacemaker during transurethral resection of the prostate: A case report. CanAnaesth Soc J 1978; 25:65–6
57. Erdman S, Levinsky L, Servadio C, Stoupel E, Levy MJ: Safety precautionsin the management of patients with pacemakers when electrocautery operationsare performed. Surg Gynecol Obstet 1988; 167:311–4
� � � The references listed here do not represent a complete bibliography of theliterature reviewed. A complete bibliography is available by writing to theAmerican Society of Anesthesiologists or by accessing the ANESTHESIOLOGY Website: http://www.anesthesiology.org.
197PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

58. Dresner DL, Lebowitz PW: Atrioventricular sequential pacemaker inhibi-tion by transurethral electrosurgery. ANESTHESIOLOGY 1988; 68:599–601
59. Lerner SM: Suppression of a demand pacemaker by transurethral electro-cautery. Anesth Analg 1973; 52:703–6
60. Wajszczuk WJ, Mowry FM, Dugan NL: Deactivation of a demand pace-maker by transurethral electrocautery. N Eng J Med 1969; 280:34–5
61. Epstein MR, Mayer JE Jr, Duncan BW: Use of an ultrasonic scalpel as analternative to electrocautery in patients with pacemakers. Ann Thorac Surg 1998;65:1802–4
62. Ozeren M, Dogan OV, Duzgun C, Yucel E: Use of an ultrasonic scalpel inthe open-heart reoperation of a patient with pacemaker. Eur J Cardiothorac Surg2002; 21:761–2
63. Val-Majias JE, Diehl T, Quesada LC: Long-term effects of RF ablation onpacemakers leads. Pacing Clin Electrophysiol 1996; 19:635
64. Alagona P, Toole JC, Maniscalco BS: Nuclear magnetic resonance imagingin a patient with a pacemaker. Pacing Clin Electrophysiol 1989; 12:619
65. Inbar S, Larson J, Burt T, Mafee M, Ezri MD: Case report: nuclear magneticresonance imaging in a patient with a pacemaker. Am J Med Sci 1993; 305:174–5
66. Lauck G, Sommer T, Wolke S, Luderitz B, Manz M: Magnetic resonanceimaging in patients with implanted permanent pacemakers. Pacing Clin Electro-physiol 1995; 18(suppl):1168
67. Lauck G, von Smekal A, Wolke S, Seelos KC, Jung W, Manz M, Luderitz B:Effects of nuclear magnetic resonance imaging on cardiac pacemakers. PacingClin Electrophysiol 1995; 18:1549–55
68. Roguin A, Zviman MM, Meininger GR, Rodrigues ER, Dickfeld TM,Bluemke DA, Lardo A, Berger RD, Calkins H, Halperin HR: Modern pacemakerand implantable cardioverter/defibrillator systems can be magnetic resonanceimaging safe. Circulation 2004; 110:475–82
69. Shellock FG, O’Neil M, Ivans V, Kelly D, O’Connor M, Toay L, Crues JV:Cardiac pacemakers and implantable cardioverter defibrillators are unaffected byoperation of an extremity MR imaging system. Am J Roentgenol 1999; 172:165–70
70. Sommer T, Valhaus C, Lauck G, von Smekal A, Reinke M, Hofer U, Block
W, Traber F, Schneider C, Gieseke J, Jung W, Schild H: MR imaging and cardiacpacemakers: In vitro evaluation and in vivo studies in 51 patients at 0.5 T.Radiology 2000; 215:869–79
71. von Smekal A, Wolke S, Seelos KC, Hermans J, Lauch G, David P, Reiser M,Biersack HJ: Cardiac pacemaker in magnetic resonance studies: Influence of thestatic magnetic field on hardware components. Eur Heart J 1993; 14:335
72. Goldberg RJ, Badger JM: Major depressive disorder in patients with theimplantable cardioverter defibrillator: Two cases treated with ECT. Psychosomat-ics 1993; 34:273–7
73. Alyward P, Blood R, Tonkin A: Complications of defibrillation with per-manent pacemaker in situ. Pacing Clin Electrophysiol 1979; 2:462–4
74. Das G, Eaton J: Pacemaker malfunction following transthoracic counter-shock. Pacing Clin Electrophysiol 1981; 4:487–90
75. Gould L, Patel S, Gomes GI, Chokshi AB: Pacemaker failure followingexternal defibrillation. Pacing Clin Electrophysiol 1981; 4:575–7
76. Palac RT, Hwang MH, Klodnycky ML, Loeb HS: Delayed pulse generatormalfunction after DC countershock. Pacing Clin Electrophysiol 1981; 4:163–7
77. Zullo M: Function of ventricular pacemakers during resuscitation. PacingClin Electrophysiol 1990; 13:736–44
78. ACLS Provider Manual. Edited by Cummins RO. Dallas, American HeartAssociation, 2003
79. Levine PA, Balady GJ, Lazar HL, Belott PH, Roberts AJ: Electrocautery andpacemakers: Management of the paced patient subject to electrocautery. AnnThorac Surg 1986; 41:313–7
80. Bernstein AD, Daubert JC, Fletcher RD, Hayes DL, Luderitz B, ReynoldsDW, Schoenfeld MH, Sutton R: The revised NASPE/BPEG generic code forantibradycardia, adaptive-rate, and multisite pacing. North American Society ofPacing and Electrophysiology/British Pacing and Electrophysiology Group. Pac-ing Clin Electrophysiol 2002; 25:260–4
81. Bernstein AD, Camm AJ, Fisher JD, Fletcher RD, Mead RH, Nathan AW,Parsonnet V, Rickards AF, Smyth NP, Sutton R: North American Society of Pacingand Electrophysiology policy statement: The NASPE/BPEG defibrillator code.Pacing Clin Electrophysiol 1993; 16:1776–80
198 PRACTICE ADVISORY
Anesthesiology, V 103, No 1, Jul 2005

Anesthesiology 2008; 108:786–801 Copyright © 2008, the American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc.
Practice Advisory for the Prevention and Management ofOperating Room Fires
A Report by the American Society of Anesthesiologists Task Force on OperatingRoom Fires*
This article has been selected for the ANESTHESIOLOGY
CME Program. After reading the article, go to http://www.asahq.org/journal-cme to take the test and apply for Cate-gory 1 credit. Complete instructions may be found in theCME section at the back of this issue.
PRACTICE advisories are systematically developed re-ports that are intended to assist decision making in areasof patient care. Advisories are based on a synthesis ofscientific literature and analysis of expert opinion, clin-ical feasibility data, open forum commentary, and con-sensus surveys. Advisories developed by the AmericanSociety of Anesthesiologists (ASA) are not intended asstandards, guidelines, or absolute requirements. Theymay be adopted, modified, or rejected according to clin-ical needs and constraints.
The use of practice advisories cannot guarantee any spe-cific outcome. Practice advisories summarize the state ofthe literature and report opinions obtained from expertconsultants and ASA members. Practice advisories are notsupported by scientific literature to the same degree asstandards or guidelines because of the lack of sufficientnumbers of adequately controlled studies. Practice adviso-
ries are subject to periodic revision as warranted by theevolution of medical knowledge, technology, and practice.
The incidence of operating room (OR) fires is difficultto determine, due in part to the lack of a mandatorynational reporting system for OR fires.1–3 Some estimatessuggest that between 50 and 200 OR fires occur in theUnited States every year, with as many as 20% of re-ported fires resulting in serious injury or death.4,5
Fire requires the presence of three components,known as the “fire triad”: (1) an oxidizer, (2) an ignitionsource, and (3) fuel.
● Oxidizers used in the OR are oxygen and nitrous oxide.An oxidizer-enriched atmosphere increases the likeli-hood and intensity of combustion. An oxidizer-enrichedatmosphere commonly exists within closed or semi-closed breathing systems, including the patient’s airway.It can also be created locally when the configuration ofthe drapes and open oxygen sources (e.g., masks, nasalcannula) promote the trapping or pooling of oxygen or amixture of oxygen and nitrous oxide.
KEY CONCEPT: An oxidizer-enriched atmosphere occurs whenthere is any increase in oxygen concentration above room air level,and/or the presence of any concentration of nitrous oxide.
● Ignition sources include, but are not limited to, elec-trosurgical or electrocautery devices, lasers, heatedprobes, drills and burrs, argon beam coagulators, fiber-optic light cables, and defibrillator paddles or pads.
● Fuel sources include, but are not limited to, trachealtubes; sponges; drapes; gauze; alcohol-containing solu-tions (e.g., certain prepping solutions); solutions contain-ing other volatile compounds, such as ether or acetone;oxygen masks; nasal cannulae; the patient’s hair; dress-ings; ointments; gowns; gastrointestinal tract gases; blan-kets; suction catheters; flexible endoscopes; fiberopticcable coverings; gloves; and packaging materials.†
Methodology
A. Definition of OR Fires, High-risk Procedures, andOR Fire DrillsFor this Advisory, operating room fires are defined as
fires that occur on or near patients who are under anes-thesia care, including surgical fires, airway fires, and fireswithin the airway circuit. A surgical fire is defined as afire that occurs on or in a patient. An airway fire is aspecific type of surgical fire that occurs in a patient’s
Additional material related to this article can be found on the ANES-THESIOLOGY Web site. Go to http://www.anesthesiology.org, click onEnhancements Index, and then scroll down to find the appropriatearticle and link. Supplementary material can also be accessed on theWeb by clicking on the “ArticlePlus” link either in the Table ofContents or at the top of the HTML version of the article.
�
* Developed by the American Society of Anesthesiologists Task Force onOperating Room Fires: Robert A. Caplan, M.D. (Chair), Seattle, Washington;Steven J. Barker, Ph.D., M.D., Tucson, Arizona; Richard T. Connis, Ph.D., Wood-inville, Washington; Charles Cowles, M.D., Deer Park, Texas; Albert L. de Rich-emond, M.S., P.E., Plymouth Meeting, Pennsylvania; Jan Ehrenwerth, M.D., Mad-ison, Connecticut; David G. Nickinovich, Ph.D., Bellevue, Washington; DonnaPritchard, R.N., Brooklyn, New York; David Roberson, M.D., Boston, Massachu-setts; Gerald L. Wolf, M.D. (Honorary), Brooklyn, New York.
Submitted for publication November 6, 2007. Accepted for publication No-vember 6, 2007. Supported by the American Society of Anesthesiologists underthe direction of James F. Arens, M.D., Chair, Committee on Standards andPractice Parameters. Approved by the House of Delegates on October 17, 2007.A complete list of references used to develop this Advisory is available by writingto the American Society of Anesthesiologists.
This Practice Advisory has been endorsed by the American Academy ofOtolaryngology–Head and Neck Surgery.
Address correspondence to the American Society of Anesthesiologists: 520N. Northwest Highway, Park Ridge, Illinois 60068-2573. This Practice Advi-sory, as well as all published American Society of Anesthesiologists PracticeParameters, may be obtained at no cost through the Journal Web site,www.anesthesiology.org.
† Some of these items only burn in an oxidizer-enriched atmosphere.
Anesthesiology, V 108, No 5, May 2008 786

airway. Airway fires may or may not include fire in theattached breathing circuit.
A high-risk procedure is defined as one in which anignition source (e.g., electrosurgery) may come in prox-imity to an oxidizer-enriched atmosphere (e.g., supple-mental oxygen and/or nitrous oxide), thereby increasingthe risk of fire. Examples of high-risk procedures in-clude, but are not limited to, tonsillectomy, tracheos-tomy, removal of laryngeal papillomas, cataract or othereye surgery, burr hole surgery, or removal of lesions onthe head, neck, or face.
An OR fire drill is defined as a formal and periodicrehearsal of the OR team’s planned response to a fire. Inthis Advisory, the OR fire drill is characterized as a“formal and periodic rehearsal” to indicate that it takesplace during dedicated education time, not during pa-tient care. In other words, an OR fire drill is not thesame as a discussion or plan about fire management thattakes place during direct patient care.
B. PurposeThe purposes of this Advisory are to (1) identify situ-
ations conducive to fire, (2) prevent the occurrence ofOR fires, (3) reduce adverse outcomes associated withOR fires, and (4) identify the elements of a fire responseprotocol. Adverse outcomes associated with OR firesmay include major or minor burns, inhalation injuries,infection, disfigurement, and death. Related adverse out-comes may include psychological trauma, prolongedhospitalization, delay or cancellation of surgery, addi-tional hospital resource utilization, and liability.
C. FocusThis Advisory focuses on a specific care setting and
subset of fires. The specific care setting is any OR orprocedure area where anesthesia care is provided. Thespecific subset is fires that occur on the patient, in theairway, or in the breathing circuit. This Advisory doesnot address fires away from the patient (e.g., in a trashcan), institutional preplanning for fire, or the responsesof fire personnel.
D. ApplicationThis Advisory is intended for use by anesthesiologists
or other individuals working under the supervision of ananesthesiologist. Because prevention of OR fires requiresclose collaboration and prompt coordination betweenanesthesiologists, surgeons, and nurses, some responsi-bilities are shared among the disciplines. When sharedresponsibilities are described in this Advisory, the intentis to give the anesthesiologist a starting point for partic-
ipating in the allocation and understanding of sharedresponsibilities. The Advisory may also serve as a re-source for other physicians and healthcare professionals(e.g., technicians, safety officers, hospital administrators,biomedical engineers, industry representatives).
E. Task Force Members and ConsultantsThe ASA appointed a Task Force of nine members.
These individuals included four anesthesiologists in pri-vate and academic practice from various geographicareas of the United States, an otolaryngologist, a periop-erative registered nurse, a professional engineer/fire in-vestigator, and two consulting methodologists from theASA Committee on Standards and Practice Parameters.Two Task Force members are former firefighters.
The Task Force developed the Advisory by means of aseven-step process. First, they reached consensus on thecriteria for evidence. Second, a systematic review andevaluation was performed on original, published, peer-reviewed and other research studies related to OR fires.Third, a panel of expert consultants was asked to (1)participate in opinion surveys on the effectiveness ofvarious strategies for fire prevention, detection, andmanagement and (2) review and comment on a draft ofthe Advisory developed by the Task Force. Fourth, opin-ions about the Advisory were solicited from a randomsample of active members of the ASA. Fifth, the TaskForce held an open forum at a major national meeting‡to solicit input on its draft recommendations. Sixth, theconsultants were surveyed to assess their opinions onthe feasibility of implementing this Advisory. Seventh, allavailable information was used to build consensuswithin the Task Force to formulate the advisory state-ments (appendix 1).
F. Availability and Strength of EvidencePreparation of this Advisory followed a rigorous meth-
odological process (appendix 2). Evidence was obtainedfrom two principal sources: scientific evidence and opin-ion-based evidence.
Scientific Evidence. Study findings from publishedscientific literature were aggregated and are reported insummary form by evidence category, as described be-low. All literature (e.g., randomized controlled trials,observational studies, case reports) relevant to eachtopic was considered when evaluating the findings.However, for reporting purposes in this document, onlythe highest level of evidence (i.e., level 1, 2, or 3) withineach category is included in the summary.
Category A: Supportive Literature. Randomized con-trolled trials report statistically significant (P � 0.01)differences between clinical interventions for a specifiedclinical outcome.
Level 1: The literature contains multiple randomizedcontrolled trials, and the aggregated findings are sup-ported by meta-analysis.§
‡ Society for Ambulatory Anesthesia, 22nd Annual Meeting, San Diego, Cali-fornia, May 5, 2007.
§ All meta-analyses are conducted by the ASA methodology group. Meta-analyses from other sources are reviewed but not included.
787PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

Level 2: The literature contains multiple randomizedcontrolled trials, but there is an insufficient number ofstudies to conduct a viable meta-analysis for the pur-pose of this Advisory.
Level 3: The literature contains a single randomizedcontrolled trial.
Category B: Suggestive Literature. Information fromobservational studies permits inference of beneficial orharmful relationships among clinical interventions andclinical outcomes.
Level 1: The literature contains observational compari-sons (e.g., cohort, case–control research designs) oftwo or more clinical interventions or conditions andindicates statistically significant differences betweenclinical interventions for a specified clinical outcome.
Level 2: The literature contains noncomparative obser-vational studies with associative (e.g., relative risk,correlation) or descriptive statistics.
Level 3: The literature contains case reports.
Category C: Equivocal Literature. The literature can-not determine whether there are beneficial or harmfulrelationships among clinical interventions and clinicaloutcomes.
Level 1: Meta-analysis did not find significant differencesamong groups or conditions.
Level 2: There is an insufficient number of studies toconduct meta-analysis and (1) randomized controlledtrials have not found significant differences amonggroups or conditions or (2) randomized controlledtrials report inconsistent findings.
Level 3: Observational studies report inconsistent find-ings or do not permit inference of beneficial or harm-ful relationships.
Category D: Insufficient Evidence from Literature.The lack of scientific evidence in the literature is de-scribed by the following terms.
Silent: No identified studies address the specified rela-tionships among interventions and outcomes.
Inadequate: The available literature cannot be used toassess relationships among clinical interventions andclinical outcomes. The literature either does not meetthe criteria for content as defined in the “Focus” of theAdvisory or it does not permit a clear interpretation offindings due to methodologic concerns (e.g., con-founding in study design or implementation).
Opinion-based Evidence. All opinion-based evi-dence relevant to each topic (e.g., survey data, open-forum testimony, Web-based comments, letters, editori-
als) is considered in the development of this Advisory.However, only the findings obtained from formal surveysare reported.
Opinion surveys were developed by the Task Force toaddress each clinical intervention identified in the doc-ument. Identical surveys were distributed to two groupsof respondents: expert consultants and ASA members.
Category A: Expert Opinion. Survey responses fromTask Force–appointed expert consultants are reported insummary form in the text. A complete listing of consul-tant survey responses is reported in appendix 2.
Category B: Membership Opinion. Survey responsesfrom a random sample of members of the ASA and, whenappropriate, responses from members of other organiza-tions with expertise in the selected topics of interest arereported in summary form in the text. A complete listing ofASA member survey responses is reported in appendix 2.
Survey responses are recorded using a five-point scaleand summarized based on median values.�
Strongly Agree: Median score of 5 (at least 50% of theresponses are 5)
Agree: Median score of 4 (at least 50% of the responsesare 4 or 4 and 5)
Equivocal: Median score of 3 (at least 50% of the re-sponses are 3, or no other response category or com-bination of similar categories contains at least 50% ofthe responses)
Disagree: Median score of 2 (at least 50% of responsesare 2 or 1 and 2)
Strongly Disagree: Median score of 1 (at least 50% ofresponses are 1)
Category C: Informal Opinion. Open-forum testi-mony, Web-based comments, letters, and editorials areall informally evaluated and discussed during the devel-opment of the Advisory. When warranted, the TaskForce may add educational information or cautionarynotes based on this information.
Advisories
I. EducationOperating room fire safety education includes, but is
not limited to, knowledge of institutional fire safety pro-tocols and participation in institutional fire safety educa-tion. Case reports indicate that lack of education canresult in severe injury and death from uncontrolled ORfires.6,7 [Category B3 evidence.]
The consultants and ASA members strongly agree thatevery anesthesiologist should have knowledge of institu-tional fire safety protocols for the OR, and should par-ticipate in OR fire safety education. The consultants andASA members strongly agree that OR fire safety educa-tion for the anesthesiologist should emphasize the riskcreated by an oxidizer-enriched atmosphere.
� When an even number of responses are obtained, the median value isdetermined by a calculating the arithmetic mean of the two middle values. Tiesare calculated by a predetermined formula.
788 PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

Advisory Statements. All anesthesiologists shouldhave fire safety education, specifically for OR fires, withemphasis on the risk created by an oxidizer-enrichedatmosphere.
II. OR Fire DrillsA case report indicates that OR fire drills and simula-
tion training can result in improved staff response to afire.8 [Category B3 evidence.]
The consultants strongly agree and ASA membersagree that all anesthesiologists should periodically par-ticipate in OR fire drills with the entire OR team. Theconsultants and ASA members strongly agree that partic-ipation should take place during dedicated educationaltime, not during patient care.
Advisory Statements. Anesthesiologists should peri-odically participate in OR fire drills with the entire ORteam. This formal rehearsal should take place duringdedicated educational time, not during patient care.
III. PreparationPreparation for OR fires includes (1) determining
whether or not a high-risk situation exists and (2) a teamdiscussion of the strategy for the prevention and man-agement of an OR fire in a high-risk situation. The liter-ature is silent regarding whether a preoperative determi-nation of a high-risk situation or a team discussion of ORfire strategy reduces the incidence or severity of an ORfire. [Category D evidence.]
The consultants strongly agree and ASA membersagree that anesthesiologists should participate with theentire OR team in assessing the risk of an OR fire for eachcase and determining whether a high-risk situation ex-ists. The consultants strongly agree and ASA membersagree that all team members should jointly agree on howa fire will be prevented and managed for each particularprocedure. The consultants and ASA members stronglyagree that a protocol for the prevention and manage-ment of fires should be posted in each location where aprocedure is performed.
Advisory Statements. For every case, the anesthesi-ologist should participate with the entire OR team (e.g.,during the surgical pause) in determining whether ahigh-risk situation exists. If a high-risk situation exists, allteam members—including the anesthesiologist—shouldtake a joint and active role in agreeing on how a fire willbe prevented and managed. Each team member shouldbe assigned a specific fire management task to performin the event of a fire (e.g., removing the tracheal tube,stopping the flow of airway gases). Each team membershould understand that his or her preassigned taskshould be performed immediately if a fire occurs, with-out waiting for another team member to take action.When a team member has completed a preassigned task,he or she should help other team members performtasks that are not yet complete.
In every OR and procedure area where a fire triad canexist (i.e., an oxidizer-enriched atmosphere, an ignitionsource, and fuel), an easily visible protocol for the pre-vention and management of fires should be displayed(fig. 1).
Equipment for managing a fire should be readily avail-able in every procedural area where a fire triad mayexist. Table 1 provides an example of fire managementequipment that should be in or near the OR or proce-dural area.
IV. PreventionPrevention of OR fires includes (1) minimizing or
avoiding an oxidizer-enriched atmosphere near the sur-gical site, (2) safely managing ignition sources, and (3)safely managing fuels.
Comparative studies indicate that a wide range of mate-rial ignites more readily in an oxygen-enriched atmospherethan in room air.9–13 [Category B1 evidence.] One compar-ative study with awake volunteer subjects showed that theconfiguration of surgical drapes can result in oxygenbuildup, increasing the risk of fire.14 [Category B1 evi-dence.] This study also indicated that replacing oxygenwith compressed air or discontinuing supplemental oxy-gen for a period of time reduces oxygen buildup withoutsignificantly reducing oxygen saturation levels. Similarly, arandomized controlled trial comparing supplemental oxy-gen and compressed air in sedated patients undergoingcataract surgery found no differences in oxygen satura-tion.15 [Category C2 evidence.]
Observational studies and case reports indicate that elec-trocautery or electrosurgical devices and lasers are com-mon sources of ignition for many OR fires, particularlywhen used in an oxidizer-enriched atmosphere.16–68 [Cat-egory B2–3 evidence.]
Case reports indicate that alcohol-based skin-preppingagents generate volatile vapors that ignite easily. Thesereports suggest that insufficient drying time after appli-cation of alcohol-based skin-prepping agents is a cause offires on patients.23,69–73 [Category B3 evidence.] Com-parative studies show that conventional tracheal tubes,when exposed to a laser beam, are more likely to igniteor melt than laser-resistant tracheal tubes.74–84 [Cate-gory B1 evidence.] Case reports indicate that drysponges and gauze are common sources of fu-el.7,19,33,43,45,55,64,83–87 Comparative studies demonstratethat the flammability of sponges, cottonoids, or packingmaterial is reduced when wet rather than dry or partiallydry.88–91 [Category B1 evidence.]
For all procedures, the consultants and ASA membersstrongly agree that flammable skin prepping solutionsshould be dry before draping. They strongly agree thatsurgical drapes should be configured to prevent oxygenfrom accumulating under the drapes or from flowinginto the surgical site. They strongly agree that sponges
789PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

Fig. 1. Operating room fires algorithm. CO2 � carbon dioxide; OR � operating room.
790 PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

should be moistened when used near an ignition source,particularly when used in or near the airway.
For high-risk procedures (i.e., proximity of an ignitionsource and an oxidizer-enriched atmosphere), the con-sultants and ASA members strongly agree that anesthesi-ologists should collaborate with the procedure team forthe purpose of preventing and managing a fire. Theystrongly agree that the surgeon should be notified when-ever an ignition source is in proximity to an oxidizer-enriched atmosphere or when the concentration of ox-idizer has increased. They strongly agree that thefraction of inspired oxygen (FIO2) delivered to the pa-tient should be kept as low as clinically feasible when anignition source is in proximity to an oxygen-enrichedatmosphere. They strongly agree that the reduction ofFIO2 delivered to the patient should be guided by moni-toring patient oxygenation (e.g., pulse oximetry). TaskForce members agree that the reduction of FIO2 shouldbe monitored, if feasible, by measuring inspired, ex-pired, and/or delivered oxygen concentration. Theystrongly agree that the use of nitrous oxide should beavoided in settings that are considered high risk for fire.The consultants strongly agree and ASA members agreethat oxygen or nitrous oxide buildup may be minimizedby either insufflating with medical air or scavenging theoperating field with suction.
For laser surgery, consultants and ASA membersstrongly agree that laser resistant tracheal tubes shouldbe used, and that the tube choice should be appropriatefor the procedure and laser. They both strongly agreethat the tracheal cuff of the laser tube should be filledwith saline rather than air, when feasible. The consult-ants strongly agree and the ASA members agree thatsaline in tracheal tube cuff should be tinted with meth-ylene blue to act as a marker for cuff puncture by a laser.
Surgery inside the airway can bring an ignition sourceinto proximity with an oxidizer-enriched atmosphere,thereby creating a high-risk situation. For cases involvingsurgery inside the airway, consultants and ASA membersboth agree that a cuffed tracheal tube should be usedinstead of an uncuffed tracheal tube when medicallyappropriate. Because an elevated FIO2 is often necessary
during tracheostomy, the Task Force strongly agrees thatsurgeons should be advised not to enter the trachea withan ignition source such as an electrosurgical device. If anelectrosurgical device must be used, the anesthesiologistshould request that the surgeon provide adequate warn-ing to allow the concentration of oxidizer to be mini-mized before the trachea is entered. Consultants andASA members were asked to report the time that theybelieve is needed to reduce oxygen or nitrous oxideconcentration to a safe level before using an ignitionsource. For patients being ventilated with a trachealtube, consultants report a range of time of less than 1min to 5 min (mean � 1.8 min), and ASA members reporta range of time of less than 1 min to 10 min (mean �2.9 min). For patients wearing a facemask or nasal can-nula, both the consultants and ASA members report arange of time of less than 1 min to 5 min (mean � 1.7min for consultants, and mean � 2.3 min for ASA mem-bers). The consultants and ASA members both agree thatthe oropharynx should be scavenged with suction dur-ing oral procedures.
Surgery around the face, head, or neck can bring anignition source into proximity with an oxidizer-enrichedatmosphere, thereby creating a high-risk situation. Whenmonitored anesthesia care is considered for surgeryaround the face, head, or neck, the Task Force stronglyagrees that two specific factors should be considered:(1) the required depth of sedation and (2) oxygen de-pendence. The Task Force agrees that a sealed gas deliv-ery device (e.g., cuffed tracheal tube or laryngeal mask)should be considered if moderate or deep sedation isrequired or used, or if the patient exhibits oxygendependence. If neither factor is present, an open gasdelivery device (e.g., facemask or nasal cannula) may beconsidered. If an open gas delivery system is used, theTask Force agrees that before an ignition source is acti-vated around the face, head, or neck, the surgeon shouldgive the adequate notice that the ignition source will beactivated. The anesthesiologist should (1) stop the deliv-ery of supplemental oxygen or reduce the delivery to theminimum required to avoid hypoxia, and (2) wait a fewminutes between decreasing the flow of supplementaloxygen and approving the activation of the ignitionsource. In the unlikely event of nitrous oxide deliverywith an open system (e.g., facemask or nasal cannula),the Task Force agrees that the anesthesiologist should(1) stop the delivery of nitrous oxide, and (2) wait a fewminutes between stopping the nitrous oxide and approv-ing the activation of the ignition source.
Advisory Statements. To the extent that is medicallyappropriate, the following basic principles should beapplied to the management of oxidizers, ignitionsources, and fuels:
● The anesthesiologist should collaborate with all mem-bers of the procedure team throughout the procedure
Table 1. Operating Room Fire Equipment and Supplies ThatShould Be Immediately Available*
Several containers of sterile salineA CO2 fire extinguisherReplacement tracheal tubes, guides, facemasksRigid laryngoscope blades; this may include a rigid fiberoptic laryngoscopeReplacement airway breathing circuits and linesReplacement drapes, sponges
* Some facilities or locations may benefit from assembling a portable cartcontaining equipment and supplies that expedite the immediate response toan operating room fire. The contents of such a cart will vary depending onlocal conditions and resources. If the items needed for an immediate re-sponse to an operating room fire are already available, there may be no addedbenefit to assembling a portable cart.
CO2 � carbon dioxide.
791PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

to minimize the presence of an oxidizer-enriched at-mosphere in proximity to an ignition source.
● Surgical drapes should be configured to minimize theaccumulation of oxidizers (oxygen and nitrous oxide)under the drapes and from flowing into the surgical site.
● Flammable skin prepping solutions should be dry be-fore draping.
● Gauze and sponges should be moistened when used inproximity to an ignition source.
For high-risk procedures, the anesthesiologist shouldnotify the surgeon whenever there is a potential for anignition source to be in proximity to an oxidizer-en-riched atmosphere or when there is an increase in oxi-dizer concentration at the surgical site. Any reduction insupplied oxygen to the patient should be assessed bymonitoring (1) pulse oximetry and, if feasible, (2) in-spired, exhaled, and/or delivered oxygen concentration.
For laser procedures, a laser-resistant tracheal tubeshould be used, and the tube should be chosen to beresistant to the laser used for the procedure (e.g., carbondioxide [CO2], Nd:YAG, Ar, Er:YAG, KTP). The trachealcuff of the laser tube should be filled with saline andcolored with an indicator dye such as methylene blue.Before activating a laser, the surgeon should give theanesthesiologist adequate notice that the ignition sourceis about to be activated. The anesthesiologist should (1)reduce the delivered oxygen concentration to the mini-mum required to avoid hypoxia, (2) stop the use ofnitrous oxide, and (3) wait a few minutes after reducingthe oxidizer-enriched atmosphere before approving ac-tivation of the laser.
For cases involving an ignition source and surgeryinside the airway, cuffed tracheal tubes should be usedwhen clinically appropriate. The anesthesiologist shouldadvise the surgeon against entering the trachea with anignition source (e.g., electrosurgery unit). Before activat-ing an ignition source inside the airway, the surgeonshould give the anesthesiologist adequate notice that theignition source is about to be activated. The anesthesi-ologist should (1) reduce the delivered oxygen concen-tration to the minimum required to avoid hypoxia, (2)stop the use of nitrous oxide, and (3) wait a few minutesafter reducing the oxidizer-enriched atmosphere beforeapproving the activation of the ignition source. In somecases (e.g., surgery in the oropharynx), scavenging withsuction may be used to reduce oxidizer enrichment inthe operative field.
For cases involving moderate or deep sedation, anignition source, and surgery around the face, head, orneck, the anesthesiologist and surgeon should develop aplan that accounts for the level of sedation and thepatient’s need for supplemental oxygen.
● If moderate or deep sedation is required or used, or ifthe patient exhibits oxygen dependence, the anesthe-siologist and surgeon should consider a sealed gas
delivery device (e.g., cuffed tracheal tube or laryngealmask).
● If moderate or deep sedation is not required, and thepatient does not exhibit oxygen dependence, an opengas delivery device (e.g., facemask or nasal cannula)may be considered. Before activating an ignitionsource around the face, head, or neck, the surgeonshould give the anesthesiologist adequate notice thatthe ignition source is about to be activated. The anes-thesiologist should (1) stop the delivery of supplemen-tal oxygen or reduce the delivered oxygen concentra-tion to the minimum required to avoid hypoxia, and(2) wait a few minutes after reducing the oxidizer-enriched atmosphere before approving the activationof the ignition source.
V. Management of OR FiresManagement of OR fires includes (1) recognizing the
early signs of fire, (2) halting the procedure, (3) makingappropriate attempts to extinguish the fire, (4) followingan evacuation protocol when medically appropriate, and(5) delivering postfire care to the patient.
Case reports indicate that early signs of a fire mayinclude a flame or flash, unusual sounds, odors, smoke,or heat.22–24,41,42,46,53,62,73,92 [Category B3 evidence.]One case report indicates that removing the trachealtube and stopping the flow of oxygen can minimizepatient injury.53 [Category B3 evidence.] One case re-port demonstrated that pouring saline into the patient’stracheal tube was effective in extinguishing the fire.93
[Category B3 evidence.] One case of a patient deathfrom an OR fire indicated that fire extinguishers wereavailable but not used by the OR staff on the patient.7
When early warning signs of a fire are noted, theconsultants and ASA members strongly agree that thereshould be an immediate halt to the procedure. When afire is definitely present, the consultants and ASA mem-bers strongly agree that there should be an immediateannouncement of fire, followed by an immediate halt tothe procedure.
For a fire in the airway or breathing circuit, theconsultants and ASA members strongly agree that, asquickly as possible, the tracheal tube should be removedand all flammable and burning materials should be re-moved from the airway. The consultants strongly agreeand ASA members agree that the delivery of all airwaygases should stop, and they both agree that saline shouldbe poured into the patient’s airway to extinguish anyresidual embers and cool the tissues.
For a fire elsewhere on or in the patient, the consult-ants agree and ASA members are equivocal regardingwhether the delivery of all airway gases should stop.They both strongly agree that all burning and flammablematerials (including all drapes) should be removed fromthe patient, and that all burning materials in, on, or
792 PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

around the patient should be extinguished (e.g., withsaline, water, or a fire extinguisher).
Seventy-one percent of the consultants and 77% of theASA members indicated that the preferred means forsafely responding to an OR fire is for each team memberto immediately perform a fire management task in apredetermined sequence. Twenty-nine percent of theconsultants and 23% of the ASA members indicated thatthe preferred means of safely responding to an OR fire isfor each team member to immediately perform a preas-signed task, without waiting for others to act. The TaskForce believes that a predetermined sequence of taskscan be attempted when a fire occurs, but that teammembers should not wait for each other if there areimpediments to following the predetermined sequenceof tasks in a rapid manner. The Task Force agrees thata team member who has completed a preassigned taskmay assist another team member whose task is not yetcomplete.
If the first attempt to extinguish the fire in, on, oraround the patient is not successful, the consultants andASA members both agree that a CO2 fire extinguishershould be used. If fire persists after use of a CO2 fireextinguisher, consultants and ASA members bothstrongly agree that the fire alarm should be activated andthe patient should be evacuated, if feasible. The consult-ants and ASA members both agree that the door to theroom should be closed and not reopened. The consult-ants strongly agree and the ASA members agree that themedical gas supply to the room should be turned offafter evacuation.
The consultants and ASA members strongly agree thatafter a fire has been extinguished, the patient’s statusshould be assessed and a plan should be devised forongoing care of the patient. When an airway or breath-ing circuit fire has been extinguished, consultants andASA members both agree that ventilation should be re-established, avoiding supplemental oxygen and nitrousoxide, if possible. Both the consultants and ASA mem-bers strongly agree that the tracheal tube should beexamined to assess whether fragments have been leftbehind in the airway. The consultants strongly agree andthe ASA members agree that rigid bronchoscopy shouldbe considered to assess thermal injury, look for trachealtube fragments, and aid in the removal of residual mate-rials. If the fire did not involve the airway and the patient
was not intubated before the fire, the consultants andASA members both strongly agree that the patient shouldbe assessed for injury related to smoke inhalation.
Advisory Statements. When an early warning sign isnoted, halt the procedure and call for an evaluation offire. Early signs of a fire may include unusual sounds (e.g.,a “pop,” “snap,” or “foomp”), unusual odors, unex-pected smoke, unexpected heat, unexpected movementof drapes, discoloration of drapes or breathing circuit,unexpected patient movement or complaint, and unex-pected flash or flame.
When a fire is definitely present, immediately an-nounce the fire, halt the procedure, and initiate firemanagement tasks.
Team members should perform their preassigned firemanagement tasks as quickly as possible. Before theprocedure, the team may identify a predetermined orderfor performing the tasks. If a team member cannot rap-idly perform his or her task in the predetermined order,other team members should perform their tasks withoutwaiting. When a team member has completed a preas-signed task, he or she should help other members per-form tasks that are not yet complete.
The following lists are shown in an order that the teammay wish to consider in its discussion of a predeter-mined sequence.
For a fire in the airway or breathing circuit, as fast aspossible:#
● Remove the tracheal tube.● Stop the flow of all airway gases.● Remove all flammable and burning materials from the
airway.● Pour saline or water into the patient’s airway.
For a fire elsewhere on or in the patient, as fast aspossible:
● Stop the flow of all airway gases.● Remove all drapes, flammable, and burning materials
from the patient.● Extinguish all burning materials in, on and around the
patient (e.g., with saline, water, or smothering).
If the airway or breathing circuit fire is extinguished:
● Reestablish ventilation by mask, avoiding supplemen-tal oxygen and nitrous oxide, if possible.
● Extinguish and examine the tracheal tube to assesswhether fragments were left in the airway. Considerbronchoscopy (preferably rigid) to look for trachealtube fragments, assess injury, and remove residual de-bris.
● Assess the patient’s status and devise a plan for ongo-ing care.
If the fire elsewhere on or in the patient isextinguished:
# Some experts and educators recommend an initial step that involves twosimultaneous actions: removal of the tracheal tube and stopping the flow ofmedical gases (e.g., by disconnecting the breathing circuit at the Y-piece or theinspiratory gas limb). The intent is to prevent a “blowtorch” effect caused bycontinued gas flow through a burning tracheal tube. This “blowtorch” effect canspread fire to other locations on or near the patient, and may cause additionalburns on the patient or other members of the OR team. The Task Force hascarefully considered this concern and agrees that these simultaneous actionsrepresent an ideal response. However, the Task Force is concerned that, in actualpractice, the simultaneous actions may be difficult to accomplish or may result indelay when one team member waits for another. Therefore, the Task Forcerecommends that the actions take place as fast as possible.
793PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

● Assess the patient’s status and devise a plan for ongo-ing care of the patient.
● Assess for smoke inhalation injury if the patient wasnot intubated.
If the fire is not extinguished after the first attempt(e.g., after performing the preassigned tasks):
● Use a CO2 fire extinguisher in, on, or around the patient.● If the fire persists after use of the CO2 fire extinguisher:
- Activate the fire alarm.- Evacuate the patient if feasible, following institu-
tional protocols.- Close the door to the room to contain the fire, and
do not reopen it or attempt to reenter the room.- Turn off the medical gas supply to the room.
Follow local regulatory reporting requirements (e.g.,report fires to your local fire department and state de-partment of health). Treat every fire as an adverse event,following your institutional protocol.
References
1. Barnes AM, Frantz RA: Do oxygen-enriched atmospheres exist beneathsurgical drapes and contribute to fire hazard potential in the operating room?AANA J 2000; 68:153–61
2. McCranie J: Fire safety in the operating room. Todays OR Nurse 1994;16:33–7
3. Milliken RA, Bizzarri A: Flammable surgical drapes. Anesth Analg 1985;64:54–7
4. Wolf GL: Danger from OR fires still a serious problem: ASA Panel reportsrisks. J Clin Monit Comput 2000; 16:237–8
5. Surgical fire safety. Health Devices 2006; 35:45–666. Use of wrong gas in laparoscopic insufflator causes fire. Health Devices
1994; 23:456–77. Stouffer DJ: Fires during surgery: Two fatal incidents in Los Angeles. J Burn
Care Rehabil 1992; 13:114–78. Halstead MA: Fire drill in the operating room: Role playing as a learning tool.
AORN J 1993; 58:697–7069. Laser ignition of surgical drapes. Health Devices 1992; 21:15–610. Surgical drapes. Health Devices 1986; 15:111–3611. Epstein RH, Brummett RR Jr, Lask GP: Incendiary potential of the flash-
lamp pumped 585-nm tunable dye laser. Anesth Analg 1990; 71:171–512. Wolf GL, Sidebotham GW, Lazard JLP, Charchaflieh JG: Laser ignition of
surgical drape materials in air, 50% oxygen, and 95% oxygen. ANESTHESIOLOGY
2004; 100:1167–7113. Treyve E, Yarington CT Jr, Thompson GE: Incendiary characteristics of
endotracheal tubes with the CO2 laser. Ann Otol Rhinol Laryngol 1981; 90:328–30
14. Greco RJ, Gonzalez R, Johnson P, Scolieri M, Rekhopf PG, Heckler F:Potential dangers of oxygen supplementation during facial surgery. Plast Recon-str Surg 1995; 95:978–84
15. Neatrour GP, Lederman IR: Reducing fire hazard during ophthalmic sur-gery by using compressed air. Ophthalmic Surg 1989; 20:430–2
16. Aly A, McIlwain M, Duncavage JA: Electrosurgery-induced endotrachealtube ignition during tracheotomy. Ann Otol Rhinol Laryngol 1991; 100:31–3
17. Airway fires during surgery. PA-PSRS Patient Safety Advisory 2007; 4:1–418. Case history number 82: “Nonflammable” fires in the operating room.
Anesth Analg 1975; 54:152–419. Surgical fire case summaries. Health Devices 1992; 21:31–420. Ashcraft KE, Golladay ES, Guinee WS: A surgical field flash fire during the
separation of dicephalus dipus conjoined twins. ANESTHESIOLOGY 1981; 55:457–821. Awan MS, Ahmed I: Endotracheal tube fire during tracheostomy: A case
report. Ear Nose Throat J 2002; 81:90–222. Bailey MK, Bromley HR, Allison JG, Conroy JM, Krzyzaniak W: Electrocau-
tery-induced airway fire during tracheostomy. Anesth Analg 1990; 71:702–423. Barker SJ, Polson JS: Fire in the operating room: A case report and
laboratory study. Anesth Analg 2001; 93:960–524. Baur DA, Butler RC: Electrocautery-ignited endotracheal tube fire: Case
report. Br J Oral Maxillofac Surg 1999; 37:142–325. Bennett JA, Agree M: Fire in the chest. Anesth Analg 1994; 78:406
26. Boyd CH: A fire in the mouth: A hazard of the use of antistatic endotrachealtubes. Anaesthesia 1969; 24:441–6
27. Burgess GE III, LeJeune FE Jr: Endotracheal tube ignition during lasersurgery of the larynx. Arch Otolaryngol 1979; 105:561–2
28. Casey KR, Fairfax WR, Smith SJ, Dixon JA: Intratracheal fire ignited by theNd-YAG laser during treatment of tracheal stenosis. Chest 1983; 84:295–6
29. Chang BW, Petty P, Manson PN: Patient fire safety in the operating room.Plast Reconstr Surg 1994; 93:519–21
30. Cozine K, Rosenbaum LM, Askanazi J, Rosenbaum SH: Laser-inducedendotracheal tube fire. ANESTHESIOLOGY 1981; 55:583–5
31. Datta TD: Flash fire hazard with eye ointment. Anesth Analg 1984; 63:700–1
32. Dini GM, Casagrande W: Misfortune during a blepharoplasty. Plast Recon-str Surg 2006; 117:325–6
33. Eade GG: Hazard of nasal oxygen during aesthetic facial operations. PlastReconstr Surg 1986; 78:539
34. Galapo S, Wolf GL, Sidebotham GW, Cohen D: Laser ignition of surgicaldrapes in an oxygen enriched atmosphere (abstract). ANESTHESIOLOGY 1998; 89:A580
35. Gunatilake DE: Case report: Fatal intraperitoneal explosion during elec-trocoagulation via laparoscopy. Int J Gynaecol Obstet 1978; 15:353–7
36. Handa KK, Bhalla AP, Arora A: Fire during the use of Nd-Yag laser. IntJ Pediatr Otorhinolaryngol 2001; 60:239–42
37. Hirshman CA, Smith J: Indirect ignition of the endotracheal tube duringcarbon dioxide laser surgery. Arch Otolaryngol 1980; 106:639–41
38. Howard BK, Leach JL: Prevention of flash fires during facial surgeryperformed under local anesthesia. Ann Otol Rhinol Laryngol 1997; 106:248–51
39. Katz JA, Campbell L: Fire during thoracotomy: A need to control theinspired oxygen concentration. Anesth Analg 2005; 101:612
40. Keller C, Elliott W, Hubbell RN: Endotracheal tube safety during electro-dissection tonsillectomy. Arch Otolaryngol Head Neck Surg 1992; 118:643–5
41. Krawtz S, Mehta AC, Wiedemann HP, DeBoer G, Schoepf KD, Tomasze-wski MZ: Nd-YAG laser-induced endobronchial burn: Management and long-termfollow-up. Chest 1989; 95:916–8
42. Lach E: The hazards of using supplemental oxygen. Plast Reconstr Surg1996; 98:566–7
43. Lai A, Ng KP: Fire during thoracic surgery. Anaesth Intensive Care 2001;29:301–3
44. Le Clair J, Gartner S, Halma G: Endotracheal tube cuff ignited by electro-cautery during tracheostomy. AANA J 1990; 58:259–61
45. Lederman IR: Fire hazard during ophthalmic surgery. Ophthalmic Surg1985; 16:577–8
46. Lew EO, Mittleman RE, Murray D: Endotracheal tube ignition by electro-cautery during tracheostomy: Case report with autopsy findings. J Forensic Sci1991; 36:1586–91
47. Lypson ML, Stephens S, Colletti L: Preventing surgical fires: Who needs tobe educated? Jt Comm J Qual Patient Saf 2005; 31:522–7
48. Magruder GB, Guber D: Fire prevention during surgery. Arch Ophthalmol1970; 84:237
49. Mandych A, Mickelson S, Amis R: Operating room fire. Arch OtolaryngolHead Neck Surg 1990; 116:1452
50. Marsh B, Riley RH: Double-lumen tube fire during tracheostomy. ANESTHE-SIOLOGY 1992; 76:480–1
51. Martin L, Dolman P: Fire! Can J Anaesth 1999; 46:90952. Meyers A: Complications of CO2 laser surgery of the larynx. Ann Otol
Rhinol Laryngol 1981; 90:132–453. Michels AM, Stott S: Explosion of tracheal tube during tracheostomy.
Anaesthesia 1994; 49:110454. Ng JM, Hartigan PM: Airway fire during tracheostomy: Should we extu-
bate? ANESTHESIOLOGY 2003; 98:130355. Ortega RA: A rare cause of fire in the operating room. ANESTHESIOLOGY 1998;
89:160856. Pashayan AG, Gravenstein JS: Airway fires during surgery with the carbon
dioxide laser. ANESTHESIOLOGY 1989; 71:47857. Paugh DH, White KW: Fire in the operating room during tracheotomy: A
case report. AANA J 2005; 73:97–10058. Reyes RJ, Smith AA, Mascaro JR, Windle BH: Supplemental oxygen: Ensur-
ing its safe delivery during facial surgery. Plast Reconstr Surg 1995; 95:924–859. Robinson JS, Thompson JM, Wood AW: Fire and explosion hazards in
operating theatres: A reply and new evidence. Br J Anaesth 1979; 51:90860. Rogers ML, Nickalls RW, Brackenbury ET, Salama FD, Beattie MG, Perks
AG: Airway fire during tracheostomy: Prevention strategies for surgeons andanaesthetists. Ann R Coll Surg Engl 2001; 83:376–80
61. Santos P, Ayuso A, Luis M, Martinez G, Sala X: Airway ignition during CO2
laser laryngeal surgery and high frequency jet ventilation. Eur J Anaesth 2000;17:204–7
62. Schettler WH: Operating room flash fire. Anesth Analg 1974; 53:288–963. Simpson JI, Wolf GL: Endotracheal tube fire ignited by pharyngeal elec-
trocautery. ANESTHESIOLOGY 1986; 65:76–764. Singla AK, Campagna JA, Wright CD, Sandberg WS: Surgical field fire
during a repair of bronchoesophageal fistula. Anesth Analg 2005; 100:1062–465. Thompson JW, Colin W, Snowden T, Hengesteg A, Stocks RM, Watson SP:
Fire in the operating room during tracheostomy. South Med J 1998; 91:243–7
794 PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

66. Varcoe RL, MacGowan KM, Cass AJ: Airway fire during tracheostomy. ANZJ Surg 2004; 74:507–8
67. Waldorf HA, Kauvar NB, Geronemus RG, Leffel DJ: Remote fire with thepulsed dye laser: Risk and prevention. J Am Acad Dermatol 1996; 34:503–6
68. Wegrzynowicz ES, Jensen NF, Pearson KS, Wachtel RE, Scamman FL:Airway fire during jet ventilation for laser excision of vocal cord papillomata.ANESTHESIOLOGY 1992; 76:468–9
69. Fire hazard created by the misuse of DuraPrep solution. Health Devices1998;27:400–2
70. Hurt TL, Schweich PJ: Do not get burned: Preventing iatrogenic fires andburns in the emergency department. Pediatr Emerg Care 2003; 19:255–9
71. Prasad R, Quezado Z, St. Andre A: Fires in the operating room andintensive care unit: Awareness is the key to prevention. Anesth Analg 2006;102:172–4
72. Shah SC: Operating room flash fire. Anesth Analg 1974; 53:28873. Tooher R, Maddern GJ, Simpson J: Surgical fires and alcohol-based skin
preparations. ANZ J Surg 2004; 74:382–574. Laser contact tips and tracheal tubes. Health Devices 1992; 21:1875. Ossoff RH, Duncavage JA, Eisenman TS, Duncavage JA, Karlan MS: Com-
parison of tracheal damage from laser-ignited endotracheal tube fires. Ann OtolRhinol Laryngol 1983; 92:333–6
76. Patel KF, Hicks JN: Prevention of fire hazards associated with use ofcarbon dioxide lasers. Anesth Analg 1981; 60:885–8
77. Simpson JI, Schiff GA, Wolf GL: The effect of helium on endotracheal tubeflammability. ANESTHESIOLOGY 1990; 73:538–40
78. Sosis MB, Braverman B: Evaluation of foil coverings for protecting plasticendotracheal tubes from the potassium-titanyl-phosphate laser. Anesth Analg1993; 77:589–91
79. Sosis MB, Braverman B: Prevention of cautery-induced airway fires withspecial endotracheal tubes. Anesth Analg 1993; 77:846–7
80. Sosis MB, Braverman B, Caldarelli DD: Evaluation of a new laser-resistantfabric and copper foil-wrapped endotracheal tube. Laryngoscope 1996; 106:842–4
81. Sosis MB, Caldarelli D: Evaluation of a new ceramic endotracheal tube forlaser airway surgery. Otolaryngol Head Neck Surg 1992; 107:601–2
82. Sosis MB, Dillon FX: A comparison of CO2 laser ignition of the Xomed,plastic, and rubber endotracheal tubes. Anesth Analg 1993; 76:391–3
83. Sosis MB, Heller S: Evaluation of five metallic tapes for protection ofendotracheal tubes during CO2 laser surgery. Anesth Analg 1989; 68:392–3
84. Sosis MB: Which is the safest endotracheal tube for use with the CO2 laser?A comparative study. J Clin Anesth 1992; 4:217–9
85. Gupte SR: Gauze fire in the oral cavity: A case report. Anesth Analg 1972;51:645–6
86. Healy GB, Strong MS, Shapshay S, Vaughan C, Jako G: Complications ofCO2 laser surgery of the aerodigestive tract: Experience of 4416 cases. Otolar-yngol Head Neck Surg 1984; 92:13–8
87. Tysinger JW Jr: Weck-Cel sponges and Steri-Drapes burn. Ophthalmic Surg1986; 17:174.
88. Do pledgets protect the tracheal tube cuff from lasers? Health Devices1992;21:17
89. Axelrod EH, Kusnetz AB, Rosenberg MK: Operating room fires initiated byhot wire cautery. ANESTHESIOLOGY 1993; 79:1123–6
90. Macdonald MR, Wong A, Walker P, Crysdale WS: Electrocautery-inducedignition of tonsillar packing. J Otolaryngol 1994; 23:426–9
91. Rohrich RJ, Gyimesi IM, Clark P, Burns AJ: CO2 laser safety considerationsin facial skin resurfacing. Plast Reconstr Surg 1997; 100:1285–90
92. Anderson EF: A potential ignition source in the operating room. AnesthAnalg 1976; 55:217–8
93. Chee WK, Benumof JL: Airway fire during tracheostomy: Extubation maybe contraindicated. ANESTHESIOLOGY 1998; 89:1576–8
Appendix 1: Primary Findings of theAdvisory Task Force
I. Education
● All anesthesiologists should have fire safety education, specifically forOR fires, with emphasis on the risk created by an oxidizer-enrichedatmosphere.
II. OR Fire Drills
● Anesthesiologists should periodically participate in OR fire drills,with the entire OR team. This formal rehearsal should take placeduring dedicated educational time, not during patient care.
III. Preparation
● For every case, the anesthesiologist should participate with the entireOR team (e.g., during the surgical pause) in assessing and determin-ing whether a high-risk situation exists.
● If a high-risk situation exists, all team members—including the anes-thesiologist—should take a joint and active role in agreeing on howa fire will be prevented and managed.
● Each team member should be assigned a specific fire managementtask to perform in the event of a fire (e.g., removing the tracheal tube,turning off the airway gases).
● Each team member should understand that his or her preassignedtask should be performed immediately if a fire occurs, withoutwaiting for another team member to take action.
● When a team member has completed a preassigned task, he or sheshould help other team members perform tasks that are not yetcomplete.
● In every OR and procedure area where a fire triad can exist (i.e., anoxidizer-enriched atmosphere, an ignition source, and fuel), an easilyvisible protocol for the prevention and management of fires shouldbe displayed.
● Equipment for managing a fire should be readily available in everyprocedural location where a fire triad may exist.
IV. Prevention
● The anesthesiologist should collaborate with all members of the proce-dure team throughout the procedure to minimize the presence of anoxidizer-enriched atmosphere in proximity to an ignition source.
● For all procedures:- Surgical drapes should be configured to minimize the accumula-
tion of oxidizers (oxygen and nitrous oxide) under the drapes andfrom flowing into the surgical site.
- Flammable skin prepping solutions should be dry before draping.- Gauze and sponges should be moistened before use in proximity to
an ignition source.
● For high-risk procedures:- The anesthesiologist should notify the surgeon whenever there is
a potential for an ignition source to be in proximity to an oxidizer-enriched atmosphere or when there is an increase in oxidizerconcentration at the surgical site.
- Any reduction in supplied oxygen to the patient should be assessedby monitoring (1) pulse oximetry and, if feasible, (2) inspired,exhaled, and/or delivered oxygen concentration.
● For laser procedures:- A laser-resistant tracheal tube should be used.
▪ The laser-resistant tracheal tube used should be chosen to beresistant to the laser used for the procedure (e.g., CO2, Nd:YAG,Ar, Er:YAG, KTP).
- The tracheal cuff of the laser tube should be filled with saline andcolored with an indicator dye such as methylene blue.
- Before activating a laser:▪ The surgeon should give the anesthesiologist adequate notice
that the laser is about to be activated.▪ The anesthesiologist should:
� Reduce the delivered oxygen concentration to the minimumrequired to avoid hypoxia.
� Stop the use of nitrous oxide.� Wait a few minutes after reducing the oxidizer-enriched atmo-
sphere before approving activation of the laser.
● For cases involving an ignition source and surgery inside the airway:- Cuffed tracheal tubes should be used when clinically appropriate.- The anesthesiologist should advise the surgeon against entering the
trachea with an ignition source (e.g., electrosurgery unit).- Before activating an ignition source inside the airway:
795PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

▪ The surgeon should give the anesthesiologist adequate noticethat the ignition source is about to be activated.
▪ The anesthesiologist should:� Reduce the delivered oxygen concentration to the minimum
required to avoid hypoxia.� Stop the use of nitrous oxide.� Wait a few minutes after reducing the oxidizer-enriched atmo-
sphere before approving the activation of the ignition source.- In some cases (e.g., surgery in the oropharynx), scavenging with
suction may be used to reduce oxidizer enrichment in the opera-tive field.
● For cases involving moderate or deep sedation, an ignition source,and surgery around the face, head, or neck:- The anesthesiologist and surgeon should develop a plan that accounts
for the level of sedation and the patient’s need for supplementaloxygen.▪ If moderate or deep sedation is required or used, or if the patient
exhibits oxygen dependence, the anesthesiologist and surgeonshould consider a sealed gas delivery device (e.g., cuffed trachealtube or laryngeal mask).
▪ If moderate or deep sedation is not required, and the patientdoes not exhibit oxygen dependence, an open gas deliverydevice (e.g., facemask or nasal cannula) may be considered.
- Before activating an ignition source around the face, head, or neck:▪ The surgeon should give the anesthesiologist adequate notice
that the ignition source is about to be activated.▪ The anesthesiologist should:
� Stop the delivery of supplemental oxygen or reduce the deliv-ered oxygen concentration to the minimum required to avoidhypoxia.
� Wait a few minutes after reducing the oxidizer-enriched atmo-sphere before approving the activation of the ignition source.
V. Management of OR Fires
● When an early warning sign is noted, halt the procedure and call foran evaluation of fire.
● When a fire is definitely present, immediately announce the fire, haltthe procedure, and initiate fire management tasks.
● Team members should perform their preassigned fire managementtasks as quickly as possible.- Before the procedure, the team may identify a predetermined
order for performing the tasks.- If a team member cannot rapidly perform his or her task in the
predetermined order, other team members should perform theirtasks without waiting.
- When a team member has completed a preassigned task, he or sheshould help other members perform tasks that are not yet com-plete.
● For a fire in the airway or breathing circuit, as fast as possible:- Remove the tracheal tube.- Stop the flow of all airway gases.- Remove all flammable and burning materials from the airway.- Pour saline or water into the patient’s airway.
● For a fire elsewhere on or in the patient, as fast as possible:- Stop the flow of all airway gases.- Remove all drapes, flammable, and burning materials from the
patient.- Extinguish all burning materials in, on, and around the patient (e.g.,
with saline, water, or smothering).
● If the airway or breathing circuit fire is extinguished:
- Reestablish ventilation by mask, avoiding supplemental oxygenand nitrous oxide, if possible.
- Extinguish and examine the tracheal tube to assess whether frag-ments were left in the airway.▪ Consider bronchoscopy (preferably rigid) to look for tracheal
tube fragments, assess injury, and remove residual debris.- Assess the patient’s status and devise a plan for ongoing care.
● If the fire elsewhere on or in the patient is extinguished:- Assess the patient’s status and devise a plan for ongoing care of the
patient.- Assess for smoke inhalation injury if the patient was not intubated.
● If the fire is not extinguished after the first attempt (e.g., afterperforming the preassigned tasks):- Use a CO2 fire extinguisher in, on, or around the patient.- If the fire persists after use of the CO2 fire extinguisher:
▪ Activate the fire alarm.▪ Evacuate the patient if feasible, following institutional protocols.▪ Close the door to the room to contain the fire and do not reopen
it or attempt to reenter the room.▪ Turn off the medical gas supply to the room.
● Follow local regulatory reporting requirements (e.g., report fires toyour local fire department and state department of health).
● Treat every fire as an adverse event, following your institutionalprotocol.
Appendix 2: Methods and Analyses
A. State of the LiteratureFor this Advisory, a literature review was used in combination with
opinions obtained from experts and other sources (e.g., professionalsociety members, open forums, Web-based postings) to provide guid-ance to practitioners regarding OR fire prevention and management.Both the literature review and opinion data were based on evidencelinkages, or statements regarding potential relationships between fireprevention and management interventions and OR fire outcomes.**The evidence linkage interventions are listed below.
I. Education
1. Fire safety education, with an emphasis on an oxidizer-enrichedatmosphere
II. OR Fire Drills
2. Periodic participation in OR fire drills
III. Preparation
3. Display of an easily visible protocol for the prevention and man-agement of fires
4. Preoperative determination of a high-risk situation5. OR team discussion of OR fire strategy
IV. Prevention
6. Surgical drape configuration to minimize the accumulation ofoxidizers
7. Drying of flammable skin prepping solutions8. Moistening of sponges and gauze when used in proximity to an
ignition source9. Reducing the concentration of supplied oxygen for high-risk pro-
cedures10. Avoidance of nitrous oxide for high-risk procedures
** Unless otherwise specified, outcomes for the listed interventions refer to theoccurrence of fire or adverse sequela.
796 PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

11. Cuffed versus uncuffed tracheal tubes for cases in or around theairway
12. Insufflating with medical air during cases in or around the airway13. Scavenging with suction during cases in or around the airway14. Laser-resistant versus non–laser-resistant tracheal tubes during la-
ser surgery15. Filling the tracheal cuff of the laser tube with saline colored with
an indicator dye
V. Management
16. Early signs of a fire include a flame or flash, unusual sounds, odors,smoke, or heat (observational)
17. Removing the tracheal tube and stopping the flow of oxygen tominimize patient injury after an airway or breathing circuit fire
18. Pouring saline into the patient’s tracheal tube to extinguish anairway fire
For the literature review, potentially relevant studies were identifiedvia electronic and manual searches of the literature. The literaturesearch covered a 56-yr period from 1952 through 2007. More than 400citations were initially identified, yielding a total of 340 articles thataddressed topics related to the evidence linkages and met our criteriafor inclusion. After review of the articles, 240 studies did not providedirect evidence and were subsequently eliminated. A total of 100articles contained direct linkage-related evidence.†† No evidence link-age contained enough studies with well-defined experimental designsand statistical information to conduct a quantitative analysis (i.e., meta-analysis).
Interobserver agreement among Task Force members and two meth-odologists was established by interrater reliability testing. Agreementlevels using a � statistic for two-rater agreement pairs were as follows:
(1) type of study design, � � 0.63–0.82; (2) type of analysis, � �0.40–0.87; (3) evidence linkage assignment, � � 0.84–1.00; and (4)literature inclusion for database, � � 0.69–1.00. Three-rater chance-corrected agreement values were (1) study design, Sav � 0.69, Var(Sav) � 0.013; (2) type of analysis, Sav � 0.57, Var (Sav) � 0.031; (3)linkage assignment, Sav � 0.89, Var (Sav) � 0.004; and (4) literaturedatabase inclusion, Sav � 0.79, Var (Sav) � 0.025. These valuesrepresent moderate to high levels of agreement.
B. Consensus-based EvidenceConsensus was obtained from multiple sources, including (1) survey
opinion from consultants who were selected based on their knowledgeor expertise in OR fire prevention and management, (2) survey opin-ions solicited from active members of the ASA, (3) testimony fromattendees of a publicly held open forum at a national anesthesiameeting, (4) Internet commentary, and (5) Task Force opinion andinterpretation. The survey rate of return was 52% (n � 38 of 73) for theconsultants, and 64 surveys were received from active ASA members.Results of the surveys are reported in tables 2 and 3 and in the text ofthe Advisory.
The consultants were asked to indicate which, if any, of the evi-dence linkages would change their clinical practices if the Advisorywas instituted. The rate of return was 18% (n � 13 of 73). The percentof responding consultants expecting a change in their practice associ-ated with each linkage topic was as follows: (1) education, 77%; (2) ORfire drills, 69%; (3) team discussion of fire strategy, 69%; (4) minimizingor avoiding an oxidizer-enriched atmosphere near the surgical site,38%; (5) managing ignition sources, 38%; (6) managing fuels, 31%; (7)identification of a high-risk procedure, 85%; (8) management of ahigh-risk procedure, 31%; and (9) OR fire management, 77%. Eighty-five percent of the respondents indicated that the Advisory wouldhave no effect on the amount of time spent on a typical case, and15% indicated that there would be an increase of 1–5 min in theamount of time spent on a typical case with the implementation ofthis Advisory.
†† A complete list of references used to develop this Advisory is available onthe ANESTHESIOLOGY Web site, www.anesthesiology.org, or by writing to theAmerican Society of Anesthesiologists.
797PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

Table 2. Consultant Survey Responses
n‡StronglyAgree Agree Uncertain Disagree
StronglyDisagree
Education1a. Every anesthesiologist should have knowledge of institutional
fire safety protocols for the OR38 92.1* 7.9 0.0 0.0 0.0
1b. Every anesthesiologist should participate in OR fire safetyeducation
38 81.6* 15.8 2.6 0.0 0.0
1c. OR fire safety education for the anesthesiologist shouldemphasize the risk of an oxidizer-enriched atmosphere
38 81.6* 18.4 0.0 0.0 0.0
OR fire drills2a. All anesthesiologists should periodically participate in OR fire
drills with the entire OR team38 60.5* 31.6 5.3 2.6 0.0
2b. Participation in an OR fire drill should take place duringdedicated educational time, not during patient care
38 50.0* 34.2 5.3 10.5 0.0
Preparation3. Anesthesiologists should participate with the entire OR team in
assessing the risk of an OR fire for each case, and determiningwhether a high-risk situation exists
38 57.9* 29.0 2.6 10.5 0.0
4. All team members should agree on how an OR fire will beprevented and managed for each particular procedure
38 60.5* 29.0 7.9 2.6 0.0
5. Hospitals and procedure units should post a protocol for theprevention and management of fires in each location where aprocedure is performed
38 50.0* 26.3 18.4 5.3 0.0
Prevention for all procedures6. Flammable skin prepping solutions should be dry before
draping38 86.8* 13.2 0.0 0.0 0.0
7. Surgical drapes should be configured to prevent oxygen fromaccumulating under the drapes or from flowing into the surgicalsite
38 76.3* 18.4 2.6 2.6 0.0
8. Sponges should be moistened, particularly when used in ornear the airway
38 63.2* 15.8 21.0 0.0 0.0
Prevention for high-risk† procedures9. Anesthesiologists should collaborate with the procedure team
for the purpose of preventing and managing a fire38 84.2* 15.8 0.0 0.0 0.0
10. The surgeon should be notified of an increase in or thepresence of an oxidizer-enriched atmosphere in which anignition source will be used
38 84.2* 15.8 0.0 0.0 0.0
11a. Oxygen levels should be kept as low as clinically feasible whilethe ignition source is in proximity to the oxygen-enrichedatmosphere
38 81.6* 13.2 2.6 0.0 2.6
11b. The reduction of FIO2 should be guided by monitoring patientoxygenation
38 86.8* 7.9 5.3 0.0 0.0
12. The use of nitrous oxide should be avoided in settings that areconsidered high risk for OR fire
38 52.6* 26.3 15.8 5.3 0.0
13. Oxygen or nitrous oxide buildup may be minimized by eitherinsufflating with room air or scavenging the operating field withsuction
38 50.0* 36.8 10.5 2.6 0.0
Prevention during cases in or around the airway14. Cuffed tracheal tubes should be used instead of uncuffed
tracheal tubes38 39.5 31.6* 23.7 5.2 0.0
15. The oropharynx should be scavenged with suction during oralprocedures
38 42.1 23.7* 28.9 5.3 0.0
16. The sufficient amount of time needed to reduce oxygen ornitrous oxide concentrations to a safe level before using anignition source in the airway:
Mean � 1.76 min,Range � 0.25–5 min
17. The sufficient amount of time needed to reduce oxygen ornitrous oxide concentrations to a safe level before using anignition source for patients wearing a facemask or nasalcannula:
Mean � 1.67 min,Range � 0.15–5 min
Prevention during laser surgery18. Laser-resistant tracheal tubes appropriate to the procedure and
laser should be used38 68.4* 29.0 2.6 0.0 0.0
19a. Tracheal tube cuffs should be filled with saline rather than air,when feasible
38 71.1* 26.3 2.6 0.0 0.0
(continued)
798 PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

Table 2. Continued
n‡StronglyAgree Agree Uncertain Disagree
StronglyDisagree
19b. Saline in tracheal tube cuffs should be tinted with methyleneblue to act as a marker for cuff puncture by a laser
38 50.0* 39.5 10.5 0.0 0.0
Management of OR fires20. When early warning signs of a fire are noted, the procedure
should be halted immediately38 78.9* 15.8 5.3 0.0 0.0
21. When a fire is definitely present, the fire should be immediatelyannounced and the procedure should halt
38 92.1* 7.9 0.0 0.0 0.0
22. For a fire in the airway or breathing circuit:a. The tracheal tube should be removed as quickly as possible 38 78.9* 13.2 7.9 0.0 0.0b. All flammable and burning materials should be removed from
the airway as quickly as possible38 94.7* 5.3 0.0 0.0 0.0
c. The delivery of all airway gases should stop 38 73.7* 18.4 5.3 2.6 0.0d. Saline should be poured into the patient’s airway to
extinguish any residual embers and cool the tissues38 47.4 21.0* 21.0 7.9 2.6
23. For a fire elsewhere on or in the patient:a. The delivery of all airway gases should stop 38 47.4 13.1* 23.7 15.8 0.0b. All burning and flammable materials (including all drapes)
should be removed from the patient38 89.5* 10.5 0.0 0.0 0.0
c. All burning materials in, on and around the patient should beextinguished (e.g., with saline, water, or a fire extinguisher)
38 86.8* 13.2 0.0 0.0 0.0
24. The preferred means of safely responding to an OR fire is:a. For each team member to immediately respond without
waiting for others to actAgree � 29%
b. To immediately initiate a predetermined sequence ofresponses
Agree � 71%
25. If the first attempt to extinguish the fire is not successful, a CO2
fire extinguisher should be used38 39.5 39.5* 13.1 7.9 0.0
26. If the fire persists after use of a CO2 fire extinguisher:a. The fire alarm should be activated 38 79.0* 10.5 10.5 0.0 0.0b. The patient should be evacuated, if feasible 38 60.5* 34.2 5.3 0.0 0.0c. The door to the room should be closed and not reopened 38 47.4 23.7* 26.3 2.6 0.0d. The medical gas supply to the room should be turned off 38 60.5* 18.4 21.1 0.0 0.0
27. After a fire has been extinguished, the patient’s status should beassessed and a plan devised for ongoing care of the patient
38 84.2* 10.5 2.6 0.0 2.6
28. When the airway or breathing circuit fire has been extinguished:a. Ventilation should be reestablished, avoiding supplemental
oxygen and nitrous oxide, if possible38 47.4 31.6* 10.5 10.5 0.0
b. The tracheal tube should be examined to assess whetherfragments may be left behind in the airway
38 81.6* 18.4 0.0 0.0 0.0
c. Rigid bronchoscopy should be considered to assess thermalinjury and look for tracheal tube fragments and other residualmaterials
38 68.4* 23.7 5.3 0.0 2.6
29. If the fire did not involve the airway and the patient was notintubated before the fire, the patient should be assessed forinjury related to smoke inhalation
38 60.5* 36.8 2.7 0.0 0.0
* Median response falls within this designated response category. † A high-risk procedure is defined as one in which an ignition source may be in proximity toan oxidizer-enriched atmosphere. ‡ n is the number of consultants who responded to each item. All other numbers in the table represent the percentage ofconsultants who selected the designated response category.
CO2 � carbon dioxide; FIO2 � fraction of inspired oxygen; OR � operating room.
799PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

Table 3. ASA Member Survey Responses
n‡StronglyAgree Agree Uncertain Disagree
StronglyDisagree
Education1a. Every anesthesiologist should have knowledge of institutional
fire safety protocols for the OR142 74.6* 24.7 0.7 0.0 0.0
1b. Every anesthesiologist should participate in OR fire safetyeducation
142 55.6* 38.7 5.6 0.0 0.0
1c. OR fire safety education for the anesthesiologist shouldemphasize the risk of an oxidizer-enriched atmosphere
142 73.9* 22.5 3.5 0.0 0.0
OR fire drills2a. All anesthesiologists should periodically participate in OR fire
drills with the entire OR team142 42.3 40.1* 12.0 5.6 0.0
2b. Participation in an OR fire drill should take place duringdedicated educational time, not during patient care
142 54.9* 31.0 10.6 2.1 1.4
Preparation3. Anesthesiologists should participate with the entire OR team in
assessing the risk of an OR fire for each case, and determiningwhether a high-risk situation exists
142 38.7 45.8* 8.5 3.5 3.5
4. All team members should agree on how an OR fire will beprevented and managed for each particular procedure
142 39.4 38.0* 13.4 7.8 1.4
5. Hospitals and procedure units should post a protocol for theprevention and management of fires in each location where aprocedure is performed
142 51.4* 36.6 8.5 2.8 0.7
Prevention for all procedures6. Flammable skin prepping solutions should be dry before
draping142 68.3* 21.8 9.2 0.7 0.0
7. Surgical drapes should be configured to prevent oxygen fromaccumulating under the drapes or from flowing into the surgicalsite
142 64.8* 28.2 6.3 0.7 0.0
8. Sponges should be moistened, particularly when used in ornear the airway
142 63.4* 30.3 5.6 0.7 0.0
Prevention for high-risk† procedures9. Anesthesiologists should collaborate with the procedure team
for the purpose of preventing and managing a fire142 67.6* 31.0 1.4 0.0 0.0
10. The surgeon should be notified of an increase in or thepresence of an oxidizer-enriched atmosphere in which anignition source will be used
142 66.2* 29.6 3.5 0.7 0.0
11a. Oxygen levels should be kept as low as clinically feasible whilethe ignition source is in proximity to the oxygen-enrichedatmosphere
142 70.4* 26.1 2.1 1.4 0.0
11b. The reduction of FIO2 should be guided by monitoring patientoxygenation
142 71.8* 24.7 2.8 0.7 0.0
12. The use of nitrous oxide should be avoided in settings that areconsidered high risk for OR fire
142 50.0* 36.6 9.2 3.5 0.7
13. Oxygen or nitrous oxide buildup may be minimized by eitherinsufflating with room air or scavenging the operating field withsuction
142 32.4 43.0* 21.8 2.8 0.0
Prevention during cases in or around the airway14. Cuffed tracheal tubes should be used instead of uncuffed
tracheal tubes142 35.9 43.0* 16.2 4.9 0.0
15. The oropharynx should be scavenged with suction during oralprocedures
142 22.5 27.5* 44.4 5.6 0.0
16. The sufficient amount of time needed to reduce oxygen ornitrous oxide concentrations to a safe level before using anignition source in the airway:
Mean � 3.3 min,Range � 0.08–10
min17. The sufficient amount of time needed to reduce oxygen or
nitrous oxide concentrations to a safe level before using anignition source for patients wearing a facemask or nasalcannula:
Mean � 2.8 min,Range � 0.0–10 min
Prevention during laser surgery18. Laser-resistant tracheal tubes appropriate to the procedure and
laser should be used142 61.3* 35.9 2.8 0.0 0.0
19a. Tracheal tube cuffs should be filled with saline rather than air,when feasible
142 61.3* 33.1 4.9 0.7 0.0
(continued)
800 PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008

Table 3. Continued
n‡StronglyAgree Agree Uncertain Disagree
StronglyDisagree
19b. Saline in tracheal tube cuffs should be tinted with methyleneblue to act as a marker for cuff puncture by a laser
142 44.4 37.3* 14.1 3.5 0.7
Management of OR fires20. When early warning signs of a fire are noted, the procedure
should be halted immediately142 78.2* 19.0 2.8 0.0 0.0
21. When a fire is definitely present, the fire should be immediatelyannounced and the procedure should halt
142 85.9* 12.7 1.4 0.0 0.0
22. For a fire in the airway or breathing circuit:a. The tracheal tube should be removed as quickly as possible 142 59.2* 26.1 8.4 4.2 2.1b. All flammable and burning materials should be removed from
the airway as quickly as possible142 73.9* 22.5 2.8 0.0 0.7
c. The delivery of all airway gases should stop 142 46.5 20.4* 16.9 14.1 2.1d. Saline should be poured into the patient’s airway to
extinguish any residual embers and cool the tissues142 33.1 29.6* 28.9 7.0 1.4
23. For a fire elsewhere on or in the patient:a. The delivery of all airway gases should stop 142 14.8 14.8 26.8* 39.4 4.2b. All burning and flammable materials (including all drapes)
should be removed from the patient142 74.7* 22.5 2.8 0.0 0.0
c. All burning materials in, on and around the patient should beextinguished (e.g., with saline, water, or a fire extinguisher)
142 73.2* 26.1 0.7 0.0 0.0
24. The preferred means of safely responding to an OR fire is:a. For each team member to immediately respond without
waiting for others to actAgree � 20%
b. To immediately initiate a predetermined sequence ofresponses
Agree � 80%
25. If the first attempt to extinguish the fire is not successful, a CO2
fire extinguisher should be used142 19.7 43.7* 36.6 0.0 0.0
26. If the fire persists after use of a CO2 fire extinguisher:a. The fire alarm should be activated 142 58.5* 37.3 4.2 0.0 0.0b. The patient should be evacuated, if feasible 142 52.1* 36.6 9.9 1.4 0.0c. The door to the room should be closed and not reopened 142 30.0 28.2* 26.1 6.3 1.4d. The medical gas supply to the room should be turned off 142 39.4 30.3* 20.4 7.0 2.8
27. After a fire has been extinguished, the patient’s status should beassessed and a plan devised for ongoing care of the patient
142 78.2* 20.4 0.7 0.0 0.7
28. When the airway or breathing circuit fire has been extinguished:a. Ventilation should be reestablished, avoiding supplemental
oxygen and nitrous oxide, if possible142 23.9 38.7* 11.3 21.8 4.2
b. The tracheal tube should be examined to assess whetherfragments may be left behind in the airway
142 60.6* 38.0 1.4 0.0 0.0
c. Rigid bronchoscopy should be considered to assess thermalinjury and look for tracheal tube fragments and other residualmaterials
142 43.7 39.4* 14.8 2.1 0.0
29. If the fire did not involve the airway and the patient was notintubated before the fire, the patient should be assessed forinjury related to smoke inhalation
142 52.1* 42.3 4.2 1.4 0.0
* Median response falls within this designated response category. † A high-risk procedure is defined as one in which an ignition source may be in proximityto an oxidizer-enriched atmosphere. ‡ n is the number of ASA members who responded to each item. All other numbers in the table represent the percentageof ASA members who selected the designated response category.
CO2 � carbon dioxide; FIO2 � fraction of inspired oxygen; OR � operating room.
801PRACTICE ADVISORY
Anesthesiology, V 108, No 5, May 2008