Embed Size (px)
Citation preview

MULLIN INDEPENDENT SCHOOL DISTRICT
www. Mullinisd.net
NEW STUDENT REGISTRATION – FALL 2016-2017
Parkview Lubbock Parkview Levelland
Please provide MISD with a copy of the following:
Birth Certificate
Immunization Records
Social Security Card
Last Report Card or Withdrawal Form
Parent/Guardian valid Photo ID
Kindergarten student must turn 5 on or before September 1, 2016
Pre-Kindergarten student must turn 4 on or before September 1, 2016
(Please attach copies to the email with signed enrollment forms)

If this student has previously attended Mullin ISD, list the two most recent schools. School name(s) Grade(s) School year(s)
Brothers and sisters (aged 4 to 19):
Last name First name Date of birth Grade School
False or misleading information on this form is a misdemeanor offense. I hereby acknowledge that the above information is true.
MULLIN INDEPENDENT SCHOOL DISRTICT
Student Registration Form / Student Entrance Sheet (Please print)
SCHOOL USE ONLYEntry Date:
_____/_____/_____
Campus #:
ID #:
Grade:
Requested Records:
Registrar's Name:
Contact Form Attached
Student Information Student’s name (as legally recorded) First Name: Middle Name: Last Name:
Student’s date of birth: Gender:
o Male o Female
Student’s social security number:
Address (as legally recorded): City: Zip code:
Doctor’s name: Doctor’s phone number:
Country of birth: If not USA, grade and date entered U.S. schools:
Grade: ______ Date: _____/_____/_____
Special Information
This student is currently being served in: o Special Education o 504 o Bilingual/ESL o GT o Dyslexia
This student previously has been served in: o Special Education o 504 o Bilingual/ESL o GT o Dyslexia
Has this student ever been retained? o No o Yes If yes, what grades? _____________________________________________
Last school attended by student: School district:
Date completed: Parent’s / legal guardian’s name (printed):
Parent’s / legal guardian’s signature:
Grade:
State:
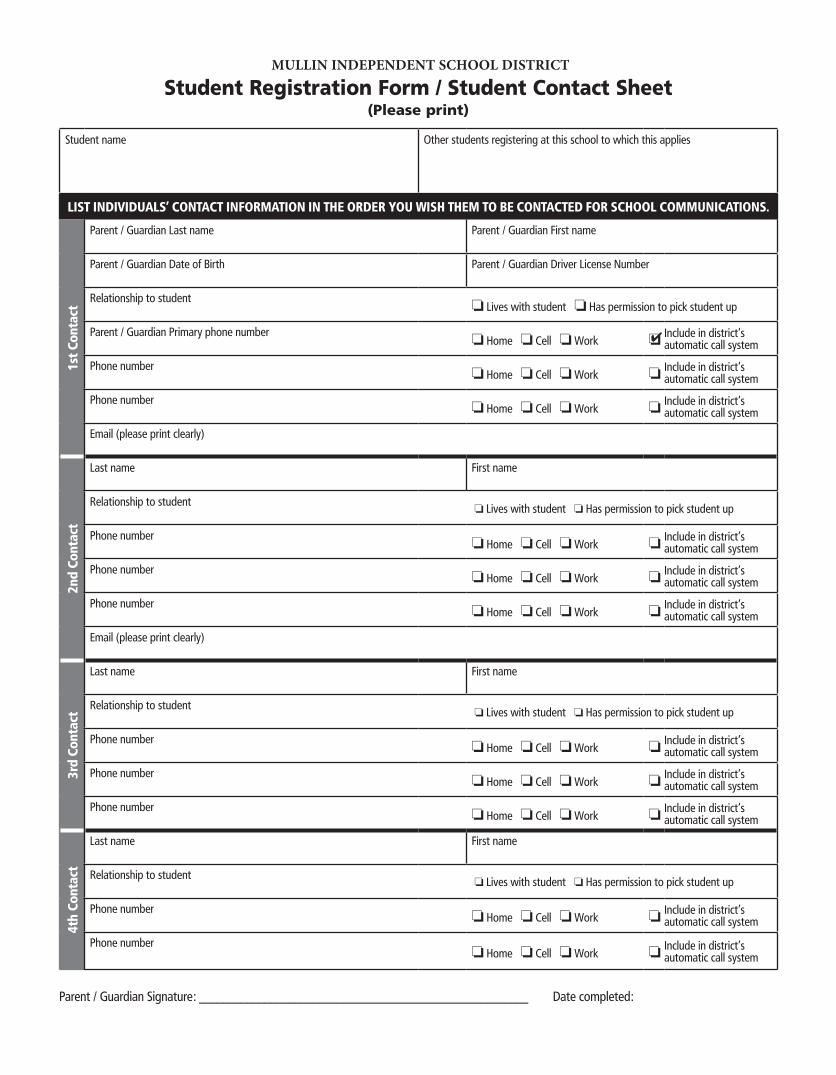
MULLIN INDEPENDENT SCHOOL DISTRICT
Student Registration Form / Student Contact Sheet (Please print)
Date completed:Parent / Guardian Signature: _______________________________________________________
Student name Other students registering at this school to which this applies
LIST INDIVIDUALS’ CONTACT INFORMATION IN THE ORDER YOU WISH THEM TO BE CONTACTED FOR SCHOOL COMMUNICATIONS.
1st C
onta
ct
Parent / Guardian Last name Parent / Guardian First name
Parent / Guardian Date of Birth Parent / Guardian Driver License Number
Relationship to studento Lives with student o Has permission to pick student up
Parent / Guardian Primary phone numbero Home o Cell o Work o
Include in district’sautomatic call system
Phone numbero Home o Cell o Work o
Include in district’sautomatic call system
Phone numbero Home o Cell o Work o
Include in district’sautomatic call system
Email (please print clearly)
2nd
Cont
act
Last name First name
Relationship to studento Lives with student o Has permission to pick student up
Phone numbero Home o Cell o Work o
Include in district’sautomatic call system
Phone numbero Home o Cell o Work o
Include in district’sautomatic call system
Phone numbero Home o Cell o Work o
Include in district’sautomatic call system
Email (please print clearly)
3rd
Cont
act
Last name First name
Relationship to studento Lives with student o Has permission to pick student up
Phone numbero Home o Cell o Work o
Include in district’sautomatic call system
Phone numbero Home o Cell o Work o
Include in district’sautomatic call system
Phone numbero Home o Cell o Work o
Include in district’sautomatic call system
4th
Cont
act
Last name First name
Relationship to studento Lives with student o Has permission to pick student up
Phone numbero Home o Cell o Work o
Include in district’sautomatic call system
Phone numbero Home o Cell o Work o
Include in district’sautomatic call system

Mullin ISD 167902 District Name Texas Education Agency County District No.
Division of Equal Education Opportunity Application for Transfer
SY: 2016-2017
Authority for Data Collection: Texas Education Code 21:061; Civil Action 5281, Section A Planned Use of Data: To complete the report required by Federal Court Order Civil Action 5281.
Instructions: This form must be used for all student transfers, with the State of Texas, including hardship. For questions please see campus Registrar. The Superintendent of the receiving district must circle approved or disapproved and sign the transfer form. For further information, contact the Division of Equal Education Opportunity at (512) 463.96713
District Student Attended Prior Year
Campus Assigned in Receiveing District
District Name Campus Number
Office UseParent/Guardian must complete information below.
Students Name Date of BirthEthnic Code Co. Dist. No. Campus
Student's School of Residence
Grade
Parent or guardian must complete this section: I have been informed of the receiving district’s policy concerning tuition charges, if any, for a transferred student whose grade is taught in the student’s district of residence; and I accept responsibility for the payment of tuition.
Signature: _____________________________Print Name: ____________________________
Street Address: _______________________________________________________________
City, State, Zip ________________________________________________________________
The receiving Campus Principal must complete this section:
The above transfer(s) was Approved on this ______ day of ______ ______________, 20 ________ Disapproved
Typed Name of Receiving
Campus Principal Date Telephone Signature
Mullin ISD does not discriminate on the basis of race, religion, color, national origin, sex, or disability in providing education services, activities, and programs including vocational programs in accordance with Title VI of the Civil Rights Act of 1964, as amended. Title IX of the Educational Amendment of 1972, and Section 504 of the Rehabilitation act of 1973, as amended
One copy should be retained at both districts for audit purposes. DO NOT MAIL TO THE TEXAS EUCUATION AGENCY.
County District No. of Residence
LVL High School - 110902 001LVL Middle - 110902 041LVL INT. - 110902 042LVL South ELEM - 110902 105

Exhibit 1A Ethnicity 2016-17 Texas Education Agency
Texas Public School Student/Staff Ethnicity and Race Data Questionnaire
The United States Department of Education (USDE) requires all state and local education institutions to collect data on ethnicity and race for students and staff. This information is used for state and federal accountability reporting as well as for reporting to the Office of Civil Rights (OCR) and the Equal Employment Opportunity Commission (EEOC). School district staff and parents or guardians of students enrolling in school are requested to provide this information. If you decline to provide this information, please be aware that the USDE requires school districts to use observer identification as a last resort for collecting the data for federal reporting. Please answer both parts of the following questions on the student’s or staff member’s ethnicity and race. United States Federal Register (71 FR 44866)
Part 1. Ethnicity: Is the person Hispanic/Latino? (Choose only one)
Hispanic/Latino - A person of Cuban, Mexican, Puerto Rican, South or Central American, or other Spanish culture or origin, regardless of race.
Not Hispanic/Latino Part 2. Race: What is the person’s race? (Choose one or more)
American Indian or Alaska Native - A person having origins in any of the original peoples of North and South America (including Central America), and who maintains a tribal affiliation or community attachment.
Asian - A person having origins in any of the original peoples of the Far East, Southeast Asia, or the Indian subcontinent including, for example, Cambodia, China, India, Japan, Korea, Malaysia, Pakistan, the Philippine Islands, Thailand, and Vietnam.
Black or African American - A person having origins in any of the black racial groups of Africa.
Native Hawaiian or Other Pacific Islander - A person having origins in any of the original peoples of Hawaii, Guam, Samoa, or other Pacific Islands.
White - A person having origins in any of the original peoples of Europe, the Middle East, or North Africa.
________________________________ Student/Staff Name (please print)
________________________________ (Parent/Guardian)/(Staff) Signature
________________________________
Student/Staff Identification Number
________________________________ Date
This space reserved for Local school observer – upon completion and entering data in student software system, file this form in student’s permanent folder. Ethnicity – choose only one:
_____ Hispanic / Latino
_____ Not Hispanic/Latino
Race – choose one or more: _____ American Indian or Alaska Native _____ Asian _____ Black or African American _____ Native Hawaiian or Other Pacific Islander _____ White
Observer signature: Campus and Date:
Texas Education Agency
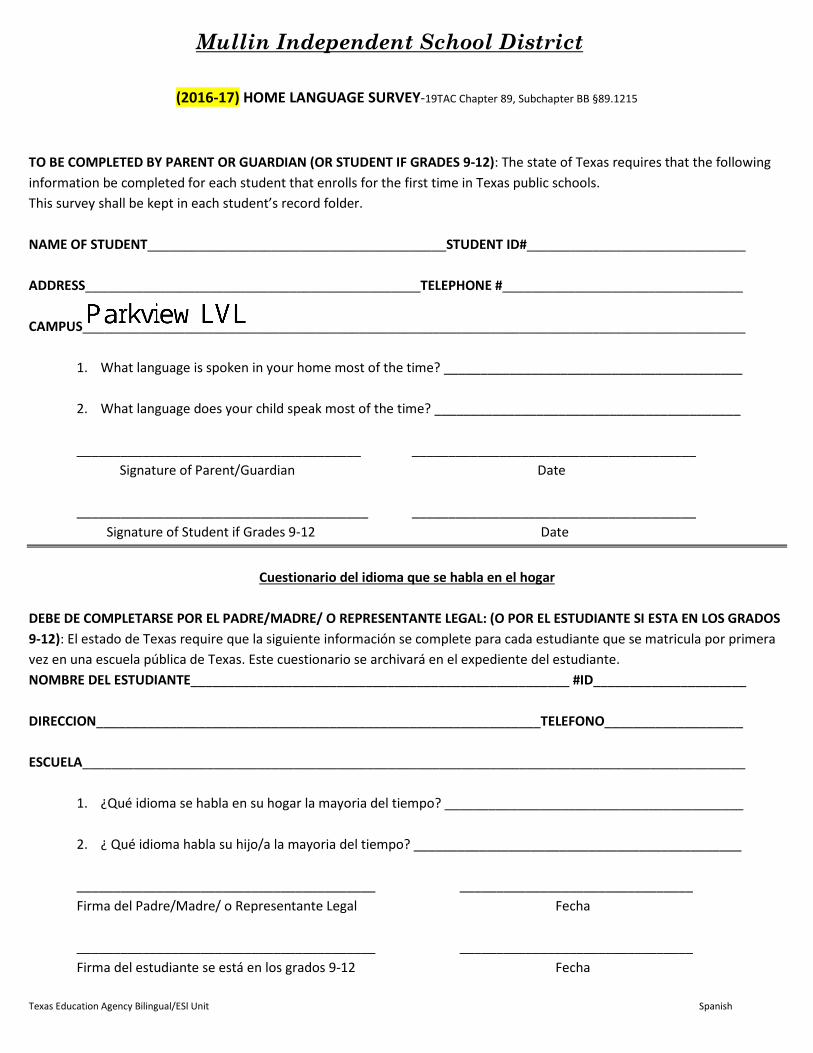
Mullin Independent School District
(2016-17) HOME LANGUAGE SURVEY-19TAC Chapter 89, Subchapter BB §89.1215
TO BE COMPLETED BY PARENT OR GUARDIAN (OR STUDENT IF GRADES 9-12): The state of Texas requires that the following information be completed for each student that enrolls for the first time in Texas public schools. This survey shall be kept in each student’s record folder.
NAME OF STUDENT_________________________________________STUDENT ID#______________________________
ADDRESS______________________________________________TELEPHONE #_________________________________
CAMPUS___________________________________________________________________________________________
1. What language is spoken in your home most of the time? _________________________________________
2. What language does your child speak most of the time? __________________________________________
_______________________________________ _______________________________________ Signature of Parent/Guardian Date
________________________________________ _______________________________________ Signature of Student if Grades 9-12 Date
Cuestionario del idioma que se habla en el hogar
DEBE DE COMPLETARSE POR EL PADRE/MADRE/ O REPRESENTANTE LEGAL: (O POR EL ESTUDIANTE SI ESTA EN LOS GRADOS 9-12): El estado de Texas require que la siguiente información se complete para cada estudiante que se matricula por primeravez en una escuela pública de Texas. Este cuestionario se archivará en el expediente del estudiante.NOMBRE DEL ESTUDIANTE____________________________________________________ #ID_____________________
DIRECCION_____________________________________________________________TELEFONO___________________
ESCUELA___________________________________________________________________________________________
1. ¿Qué idioma se habla en su hogar la mayoria del tiempo? _________________________________________
2. ¿ Qué idioma habla su hijo/a la mayoria del tiempo? _____________________________________________
_________________________________________ ________________________________ Firma del Padre/Madre/ o Representante Legal Fecha
_________________________________________ ________________________________ Firma del estudiante se está en los grados 9-12 Fecha
Texas Education Agency Bilingual/ESl Unit Spanish

For more information, please contact Migrant Service Coordinator: _____________________________________
SCHOOL DISTRICT PERSONNEL: THIS FORM CAN NOT BE ALTERED 11-15/FP
Working with fruits, vegetables, cotton, wheat, grain, agricultural farms, fields or vineyards
☐
Working in a fishery
☐
Working in a slaughter House-packaging and cutting meat
☐
Mullin ISD
Family Survey 2016-2017
In order to better serve your child/children, the school district would like to identify students who may qualify to receive additional educational services. The information provided will be kept confidential.
Please print and return form to school office:
Campus: __________________________________ Date: _________________ Student Name: _____________________________ Grade: ________ Father/Guardian: ___________________________ Mother/Guardian: __________________________ Father’s Place of Employment: ________________ Mother’s Place of Employment: _______________ Home Address: _____________________________ City: ____________________Zip: ______________ Home Phone: ______________________Cell Phone: _____________________Work Phone: ______________
Please answer the following questions:
1. Within the past 3 years have you moved from one city, state, or school district to another?
☐ Yes ☐ No
2. If yes, did you or your child move/leave in order to work (temporary or seasonal) in agriculture or fishing?(By checking yes, you are stating that you have worked in agricultural or fishing work within the last 36 months).
☐ Yes ☐ No
If you answered YES to question 2, please check all that apply.
Other similar work, please explain:
__________________________________
__________________________________
Working in a cannery
☐
Working on a dairy farm. Working on a ranch-feeding livestock, clearing fields, building fences
☐
Working in a plant, nursery or orchard, growing or harvesting trees or picking pecans
☐
Working on a poultry farm
☐

Student Emergency Information (2016-17)
Student Name: ____________________________________________ Sex: Male Female
DOB: ________________________________ AGE:_______________________ Grade:_______________
Parent/Guardian Info:
Mother’s Name:____________________________ Father’s Name:__________________________
Mother’s Phone #: __________________________ Father’s Phone #:_________________________
Alternate Phone #:__________________________ Alternate Phone #:________________________
If Medical Care is Necessary, Call:
Doctor:_______________________________________________________________________________ NAME CITY PHONE NUMBER
Hospital:______________________________________________________________________________ NAME CITY PHONE NUMBER
Does your child have insurance coverage? No Yes Medicaid? No Yes Name of Insurance Company: {optional}_______________________
In case of injury of sudden illness, __________________ will be called first. I hereby give authority to any hospital or doctor to render immediate aid as might be required at the time for my child’s health and safety. It is understood by me that the expense of this service will be accepted and paid for by me.
In case of emergency, or if I cannot be contacted to pick up my child, I hereby authorize the following person(s) to be contacted to pick up my child:
__________________________________________________________________________________________________ Name Relationship to Child Phone #
__________________________________________________________________________________________________Name Relationship to Child Phone #
__________________________________________________________________________________________________ Name Relationship to Child Phone #
Medical conditions or heath concerns that may affect my child include the following :( please circle or fill in) Diabetes Asthma Nose Bleeds Headaches Menstrual Cramps Seasonal Allergies Other (please list): ___________________________________________________________________________________
I further understand it is my responsibility to provide any necessary medications and instructions for treating my child for the above conditions. All medications and instructions will be listed on the attached medication permission form.
___________________________________________ _______________________________ Parent Signature Date

Mullin Independent School District Military Connected | 16-17 SY
Student Name: _________________________________ School Name: _______________
Student ID: _______ Grade: ________ Date of Birth: _____________
Please return this form to your child’s campus ONLY if your child meets one of the criteria below
In 2009 The Texas Legislature adopted the Interstate Compact on Educational Opportunity for Military Students – Texas Education Code Chapter 162. This legislation requires schools to recognize and extend certain privileges to students who are military dependents and to assist military dependent students in the transition process of changing schools when their military parents are reassigned and forced to relocate.
Please check one box below to indicate if your child is a dependent of a member of:
For all students:
Not a military connected student
Active Duty: Army, Navy, Air Force, Marine Corps, or Coast Guard [This includes Missing in Action (MIA)]
Texas National Guard
Reserve Duty: Army, Navy, Air Force, Marine Corps, or Coast Guard
For Pre-Kindergarten students ONLY:
Pre-kindergarten student is a dependent of: 1) an active duty uniformed member of the Army, Navy, Air Force, Marine Corps, or Coast Guard, 2) activated/mobilized uniformed member of the Texas National Guard (Army, Air Guard, or State Guard), or 3) activated/mobilized members of the Reserve components of the Army, Navy, Marine Corps, Air Force, or Coast Guard; who are currently on active duty or who were injured or killed while serving on active duty.
______________________________ ______________________________ Printed Name of Parent/Guardian Date
______________________________ Parent/Guardian Signature
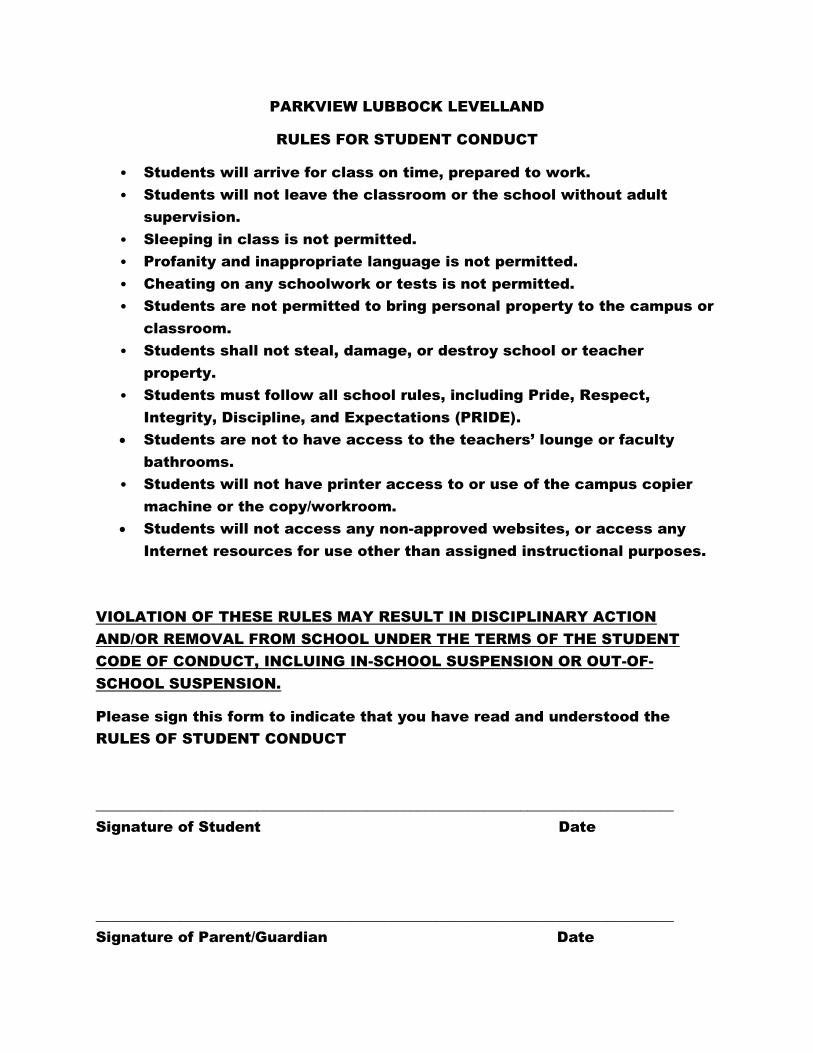
PARKVIEW LUBBOCK LEVELLAND
RULES FOR STUDENT CONDUCT
• Students will arrive for class on time, prepared to work.
• Students will not leave the classroom or the school without adult
supervision.
• Sleeping in class is not permitted.
• Profanity and inappropriate language is not permitted.
• Cheating on any schoolwork or tests is not permitted.
• Students are not permitted to bring personal property to the campus or
classroom.
• Students shall not steal, damage, or destroy school or teacher
property.
• Students must follow all school rules, including Pride, Respect,
Integrity, Discipline, and Expectations (PRIDE).
Students are not to have access to the teachers’ lounge or faculty
bathrooms.
• Students will not have printer access to or use of the campus copier
machine or the copy/workroom.
Students will not access any non-approved websites, or access any
Internet resources for use other than assigned instructional purposes.
VIOLATION OF THESE RULES MAY RESULT IN DISCIPLINARY ACTION
AND/OR REMOVAL FROM SCHOOL UNDER THE TERMS OF THE STUDENT
CODE OF CONDUCT, INCLUING IN-SCHOOL SUSPENSION OR OUT-OF-
SCHOOL SUSPENSION.
Please sign this form to indicate that you have read and understood the
RULES OF STUDENT CONDUCT
_______________________________________________________________________________
Signature of Student Date
_______________________________________________________________________________
Signature of Parent/Guardian Date

Please understand that failure to return this release form within ten (10) school days from the
date of distribution will constitute approval of the above requests.
MULLIN INDEPENDENT SCHOOL DISTRICT
Student Media Consent and Directory Release Form
There are two different items that require your signature – photo consent and directory information. For each item, please sign consent or no consent. Please return this form to your child’s School Registrar. Thank you for your assistance.
According to Texas Law a district may video tape students for the following:
(1) Purpose of safety, including the maintenance of order and discipline in common areas of theschool or on school buses;
(2) A purpose related to a co-curricular or extra-curricular activity;(3) A purpose related to regular classroom instruction;or(4) Media coverage of the school.
Mullin ISD will be videotaping students for purposes listed immediately above.
I hereby give Mullin ISD permission for any additional videotaping/photographing for purposes of school related events: i.e. Yearbook, UIL, Ag, etc.
I further release and relieve MISD, its Board of Trustees, employees, and other representatives from any liabilities, known or unknown, arising out of the use of this material.
1) Photo Consent: I do consent and allow my child to be filmed, videotaped and/or photographed for use by my school, MISD/its partners andthe media. I also allow my child’s work product to be featured by MISD (this will include the school yearbook).
Child’s Name Parent’s Signature Date
No Photo Consent: I do NOT consent nor allow my child to be filmed, videotaped and/or photographed for use by my school, MISD/its partners and the media (this will include the school yearbook).
Child’s Name Parent’s Signature Date
2) Directory Information Consent:I do consent and allow the district to release directory information on my child. Directory information includes the student’s name, place and dateof birth, major course of study, participation in sports and other official school activities, height and weight if an athletic team member, date ofgraduation, dates of attendance (date of enrollment through date of withdrawal or graduation), degrees and awards.
Child’s Name Parent’s Signature Date
No Directory Information Consent: I do NOT consent nor allow the district to release directory information on my child.
Child’s Name Parent’s Signature Date





























