-
DOI: 10.1542/peds.2011-0643; originally published online March
5, 2012;Pediatrics
Laurel K. LeslieIp, Jane W. Newburger, Susan K. Parsons, Thomas
A. Trikalinos, John B. Wong and Angie Mae Rodday, John K. Triedman,
Mark E. Alexander, Joshua T. Cohen, Stanley
in Asymptomatic Children: A Meta-analysisElectrocardiogram
Screening for Disorders That Cause Sudden Cardiac Death
http://pediatrics.aappublications.org/content/early/2012/02/29/peds.2011-0643
located on the World Wide Web at: The online version of this
article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005.
Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois,
60007. Copyright © 2012 by the American Academy published, and
trademarked by the American Academy of Pediatrics, 141 Northwest
Pointpublication, it has been published continuously since 1948.
PEDIATRICS is owned, PEDIATRICS is the official journal of the
American Academy of Pediatrics. A monthly
at University of Missouri-Columbia on March 6,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/content/early/2012/02/29/peds.2011-0643http://pediatrics.aappublications.org/
-
Electrocardiogram Screening for Disorders ThatCause Sudden
Cardiac Death in AsymptomaticChildren: A Meta-analysis
abstractBACKGROUND AND OBJECTIVES: Pediatric sudden cardiac
death (SCD)occurs in an estimated 0.8 to 6.2 per 100 000 children
annually.Screening for cardiac disorders causing SCD in
asymptomatic chil-dren has public appeal because of its apparent
potential to averttragedy; however, performance of the
electrocardiogram (ECG) as ascreening tool is unknown. We estimated
(1) phenotypic (ECG- or echo-cardiogram [ECHO]-based) prevalence of
selected pediatric disordersassociated with SCD, and (2)
sensitivity, specificity, and predictive valueof ECG, alone or with
ECHO.
METHODS: We systematically reviewed literature on hypertrophic
car-diomyopathy (HCM), long QT syndrome (LQTS), and
Wolff-Parkinson-White syndrome, the 3 most common disorders
associated with SCDand detectable by ECG.
RESULTS: We identified and screened 6954 abstracts, yielding
396articles, and extracted data from 30. Summary phenotypic
prevalencesper 100 000 asymptomatic children were 45 (95%
confidence interval[CI]: 10–79) for HCM, 7 (95% CI: 0–14) for LQTS,
and 136 (95% CI: 55–218) for Wolff-Parkinson-White. The areas under
the receiver operatingcharacteristic curves for ECG were 0.91 for
detecting HCM and 0.92 forLQTS. The negative predictive value of
detecting either HCM or LQTS byusing ECG was high; however, the
positive predictive value varied bydifferent sensitivity and
specificity cut-points and the true prevalence ofthe
conditions.
CONCLUSIONS: Results provide an evidence base for evaluating
pedi-atric screening for these disorders. ECG, alone or with ECHO,
was a sen-sitive test for mass screening and negative predictive
value was high,but positive predictive value and false-positive
rates varied. Pediatrics2012;129:1–12
AUTHORS: Angie Mae Rodday, MS,a John K. Triedman, MD,b,c
Mark E. Alexander, MD,b,c Joshua T. Cohen, PhD,a,d Stanley
Ip,MD,a,d Jane W. Newburger, MD, MPH,b,c Susan K. Parsons,
MD,MRP,a,d Thomas A. Trikalinos, MD, PhD,a,d John B. Wong,
MD,a,d
and Laurel K. Leslie, MD, MPHa,d
aTufts Medical Center, Boston, Massachusetts;
bChildren’sHospital Boston, Boston, Massachusetts; cHarvard
MedicalSchool, Boston, Massachusetts; and dTufts University School
ofMedicine, Boston, Massachusetts
KEY WORDSsudden cardiac death, ECG screening,
hypertrophiccardiomyopathy, long QT syndrome,
Wolff-Parkinson-Whitesyndrome
ABBREVIATIONSAUC—area under the HSROC curveCI—confidence
intervalECG—electrocardiogramECHO—echocardiogramHCM—hypertrophic
cardiomyopathyHSROC—hierarchical summary receiver operating
characteristicLQTS—long QT syndromeNPV—negative predictive
valuePPV—positive predictive valueSCD—sudden cardiac
deathWPW—Wolff-Parkinson-White syndrome
www.pediatrics.org/cgi/doi/10.1542/peds.2011-0643
doi:10.1542/peds.2011-0643
Accepted for publication Nov 22, 2011
Address correspondence to Laurel K. Leslie, MD, MPH,
800Washington St, #345, Boston, MA 02111.
E-mail:[email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online,
1098-4275).
Copyright © 2012 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: Dr Triedman is a consultant forBiosense
Webster, Inc, and has received a speaker’s honorariafrom St Jude
Medical; the other authors have indicated theyhave no financial
relationships relevant to this article todisclose.
FUNDING: Supported by grant 1RC1HL100546-01 from theNational
Heart, Lung, and Blood Institute. Consultation from theTufts
Clinical and Translational Science Institute was supportedby grant
RR025752 from the National Center for ResearchResources. Funded by
the National Institutes of Health (NIH).
PEDIATRICS Volume 129, Number 4, April 2012 1
REVIEW ARTICLE
at University of Missouri-Columbia on March 6,
2012pediatrics.aappublications.orgDownloaded from
mailto:[email protected]://pediatrics.aappublications.org/
-
Although sudden cardiac death (SCD) inchildren and adolescents
(hereafter“children”) is rare (0.8–6.2 per 100 000annual
incidence1,2), the sudden deathof a child is tragic and has
widespreadrepercussions. Concern about SCD hasraised calls for
screening in primarycare or school-based settings for allchildren;
others have recommendedscreening for subgroups of childrenstarting
stimulants or participatingin competitive athletics, both of
whichincrease heart rate and may theoreti-cally precipitate
SCD.1,3,4
Population-based screening programsthat identify children at
risk for SCDhave broad public appeal, as commonsense suggests that
presymptomaticdiagnosis saves lives, and the societalcost is
presumed to be the cost of thescreening test itself. Japan is the
solecountry with published data on massscreening of school-aged
children, in-cluding a targeted cardiac history andphysical and
electrocardiogram (ECG).5
No data regarding mass pediatricscreening and associated costs
areavailable in the United States.6
In 2008, the American Heart Associationreleased a statement7
broadly inter-preted as recommending an ECG beforeinitiating
stimulants for children withattention-deficit/hyperactivity
disorder,estimated at 4% to 12% of children.8
The American Academy of Pediatricslater released a statement, in
collabo-ration with the American Heart Asso-ciation, recommending
that childrenwith attention-deficit/hyperactivity dis-order be
assessed with a targeted his-tory and cardiac examination but
thatfurther evaluation, including an ECG, beobtained only if
indicated.9 A recentdecision analysis recommended thatchildren
participating in competitivesports undergo mass screening.3
Sev-eral studies have described screeningprograms for athletes.
Italy uses pre-participation screening, includingECGs, for athletes
aged 12 to 351 and
some American universities use pre-participation screening and
ECGs forcollege athletes. Because 10 millionpeople in the United
States may beclassified as “young competitiveathletes,”10 calls for
screening havefar-reaching implications.
Screening programs are most effectiveif (1) preclinical
prevalence is suffi-ciently high in the screened population,(2) a
highly discriminatory screeningtest is available, (3) the disease
or dis-order is serious, and (4) treatmentwhile asymptomatic
decreases mor-bidity and mortality more than treat-ment after
symptoms develop.11 Thesecriteria enable evaluation of the
effi-ciency of ECG to detect the disordersthat may cause SCD in
asymptomaticchildren.
Several rare disorders cause pediatricSCD, but not all have ECG
findings.12 Themost common disorders detectable byECG are
hypertrophic cardiomyopathy(HCM), long QT syndrome (LQTS),
andWolff-Parkinson-White syndrome (WPW).Their estimated prevalence
rates arelow in otherwise healthy, asymptomaticchildren; moreover,
the value of the ECGas a “highly discriminatory” test is notwell
established. The ECG should se-lectively identify disorders
respon-sible for SCD in all affected patients(ie, sensitivity) and
rule out these dis-orders in healthy children (ie,
specificity).Together, low prevalence and imperfectsensitivity and
specificity estimatescould result in inefficient
screeningstrategies with unanticipated societaland economic
costs.
We undertook a systematic review andmeta-analysisof the
literatureof these3disorders that cause SCD. Our first aimwas to
summarize how often ECG- orechocardiogram (ECHO)-based
testing(phenotypic prevalence) suggests HCM,LQTS,
orWPWamongasymptomatic andundiagnosed children who could
beidentified by mass screening. We fo-cused onphenotypic
prevalence, rather
than genetic prevalence, because ge-netic testing is currently
impractical inmass screening programs and is lim-ited to diagnosis
or risk stratification.Our second aim was to examine thereported
sensitivity and specificity ofthe ECG, alone or with ECHO, to
detectthese disorders and calculate predictivevalues. Together,
this information onphenotypic (ECG- or ECHO-based) prev-alence,
sensitivity, specificity, and pre-dictive value form an evidence
base thatwill facilitate further evaluation of theefficiency and
downstream implicationsof ECG screening programs for SCD.
METHODS
We focused on HCM, LQTS, and WPWbecause they are the most
commondisorders potentially detectable by ECGamong children.
Because ECG findingsin HCM are age sensitive (ie, may not
bedetected until late adolescence or
earlyadulthood)andcanbenonspecific, thusrequiring an ECHO for
diagnostic guid-ance, we chose to include articles thatexamined
test characteristics of ECGalone, ECHO alone, or ECG
combinedwithECHO (ECG/ECHO).
Literature Searches
We performed a systematic review andsearched the Medline
database (1950to December 2010) for studies report-ing on HCM,
LQTS, WPW, and SCD or onECG and/or ECHO detection of
thesedisorders. We combined keywords andMedical Subject Heading
terms forhypertrophic cardiomyopathy, longQT syndrome,
Wolff-Parkinson-Whitesyndrome, sudden cardiac death,
elec-trocardiography, echocardiography, sen-sitivity, and
specificity. The search waslimited to English-language
publica-tions of primary studies in humanswith no geographic
restrictions. Sixreviewers screened titles and ab-stracts to
identify relevant studiesand then examined full-text articlesfor
eligibility.
2 RODDAY et al at University of Missouri-Columbia on March 6,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
Eligibility Criteria
To summarize how often ECG- or ECHO-based testing (phenotypic
prevalence)suggests HCM, LQTS, or WPW in asymp-tomatic children or
young adults (3–25years old), we included cross-sectionalor cohort
studies from the general pop-ulation that used ECG or ECHO
diagnosticcriteria for each disorder consistentwith clinical
standards. Studies in whichthemean age was.2 SDs from 25 yearswere
excluded, including a recent studyfocused on neonates.13 We also
excludedstudies of highly selected subgroups thatwere not
representative of the generalpopulation. For example, “elite”
athleteswho competed in competitive regional,national, or
international events wereexcluded, but studies of normally
activehigh school athletes were included.Studies that used sampling
techniquesthat might result in a nonrepresentativesample (eg,
convenience sampling,studies requiring informed consent
fromparticipants) were excluded. Studiesassessing the frequency of
genetic var-iations related to HCM, LQTS, or WPWwere excluded,
given our focus on ECGscreening in asymptomatic and pre-viously
undiagnosed children.
For our second aimwe included studieswithdataon thesensitivity
or specificityof ECG (with orwithout ECHO) to identifychildren who
would have a diagnosis ofHCM, LQTS, or WPWaccording to
clinicalcriteria. Specifically, wedeemed that anadequate reference
(“gold”) standardfor HCM is ECHO, genotyping, or a well-documented
HCM diagnosis. For LQTS,we accepted as reference standardtesting
for pathogenic variations (eg,the KCNQ1, KCNH2, and SCN5A genes)
ora combination of personal and familyhistory, clinical follow-up,
and ECG. ForWPW, ECG is the reference standard, sosensitivity and
specificity informationwere not collected. Based on thesecriteria,
studies with incorporation bi-as (where the index test
comprisespart of the reference standard against
which it is measured) were eligible. Weincluded studies in which
only those withpositive ECG and/or ECHO were verifiedwith the
reference standard (verificationbias, which may overestimate
sensitivityand underestimate the specificity of theindex test). For
those studies that hadmultiple alternative sets of ECG and/orECHO
criteria, we selected the mostwidely used or most sensitive
criteriato avoid duplication of information.
Data Extraction
Four reviewers extracted data with atleast 2 independently
extracting or re-viewing each article. All 4 reviewers
dis-cussedandresolvedanydiscrepanciesbyconsensus. From studies
informing onphenotypic (ECG- or ECHO-based) preva-lence, we
extracted information on studypopulation (description, country),
studydesign (prospective, retrospective),sampling technique
(representative ornot), age of the study sample, samplesize,
diagnostic criteria, and number ofparticipants with each
disorder.
From studies on the sensitivity andspecificity of ECG and/or
ECHO to identifyHCMorLQTS,weextracted informationonstudy population
(description, country),age of the study sample, type of test
(ECGand/or ECHO), diagnostic criterion andthresholds for the test,
reference stan-dard definition, true-positive, false-negative,
false-positive, true-negative,and presence of verification bias. If
thestudy provided only sensitivity andspecificity, we used this
information tocalculate thetrue-positive,
false-negative,false-positive, and true-negative values.
Analysis
Because of the complexities of ourmethods, we briefly discuss
analysesin the following paragraphs and pro-vide detailed
Supplemental Informa-tion that discusses characteristics
ofscreening tests in general (eg, sensi-tivity, specificity,
predictive value) andanalytic methods used (eg, creation of
hierarchical summary receiver oper-ating characteristic [HSROC]
curve).
Analysis of Phenotypic Prevalence
Phenotypic (ECG- or ECHO-based) preva-lence (per 100 000)
estimates and 95%confidence intervals (CIs) for HCM, LQTS,and WPW
were calculated by using theexact binomial distribution. We
obtainedsummary estimates of phenotypicprevalence by using random
effectsmeta-analysis of logit-transformedphenotypic prevalence.14
To assess theextent to which variation in the reportedoutcomes may
be a result of chancealone, we used Cochran Q to test
forheterogeneity (significant when P ,.10) and quantified its
magnitude interms of I2,15 which ranges between0% and 100% and
expresses the pro-portion of between-study variabilityattributable
to heterogeneity ratherthan chance. We considered I2
valuesexceeding 75% suggestive of substantialheterogeneity. These
calculations wereperformed by using Stata, version 11(StataCorp LP,
College Station, TX).
Analysis of Sensitivity andSpecificity
For each disorder, we summarized therelationship between
sensitivity (ie, theprobability of having a positive testamong
those with the disorder) andspecificity (ie, the probability of
havinganegative test among thosewithout thedisorder) of ECG and/or
ECHO with anextension of the HSROC model.16–18 Foreach disorder and
screening tool com-bination, we plotted the HSROC curve
forindividual studies and the HSROC curvefor the summary of the
reviewed stud-ies. These curves allow visual compari-son between
individual studies and thesummary curve. Points along the sum-mary
curves incorporate different di-agnostic criteria and do not
corresponddirectly to specific observed study cutpoints for ECG
and/or ECHO. Restrictingthe range to that observed in the data,the
area under the posterior estimate
REVIEW ARTICLE
PEDIATRICS Volume 129, Number 4, April 2012 3 at University of
Missouri-Columbia on March 6,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/lookup/suppl/doi:10.1542/peds.2011-0643/-/DCSupplementalhttp://pediatrics.aappublications.org/lookup/suppl/doi:10.1542/peds.2011-0643/-/DCSupplementalhttp://pediatrics.aappublications.org/
-
of the HSROC curve (AUC) calculatedby numeric integration
indicates testperformance. An AUC of 1.0 representsa perfect test,
whereas an AUC of 0.5represents a test that performs nobetter than
chance.
For each summary curve, we identified2 illustrative examples to
demonstratehowchanges in sensitivity andspecificityresulted in
different predictive values,numberneeded toscreen,
false-positives,and false-negatives. We selected 2 pointson the
HSROC curve: (1) the point with“maximal accuracy” (ie, maximizing
thesum of the sensitivity and specificity),thereby giving equal
weight to ruling inpeople with disease (sensitivity) andruling out
those without disease (speci-ficity); and (2) the point with
“maximalspecificity” where specificity was near 1and the
corresponding sensitivity,thereby giving more weight to rulingout
those without the disease (speci-ficity). We did not select a point
on thecurve where sensitivity was maximizedbecause the
corresponding specificitywas low (0.001). By using the 2
illus-trative points, we calculated 5 param-eters: (1) positive
predictive value (PPV,ie, the probability of having the disor-der
given a positive test), (2) negativepredictive value (NPV, ie, the
probabilityof not having the disorder given a neg-ative test), (3)
number needed toscreen to detect 1 case, (4) number
offalse-positives when detecting 1 case,and (5) number of
false-negatives per100 000 children screened. To explorethe effect
of alternative prevalencerates, we repeated these calculationsby
using oft-cited prevalences of 200per 100 000 for HCM,19 50 per 100
000for LQTS,13 and 200 per 100 000 for WPW(See Supplemental
Information, Sup-plemental Figures 4-8, and Supple-mental Tables
1-3 for more informationon screening trade-offs in general.).20
Sensitivity Analysis
To determine whether alternativeassumptions substantially
affected the
meta-analysis results, we performedextensive sensitivity
analyses.21 For keyquestions related to phenotypic (ECG-or
ECHO-based) prevalence, we re-peated the analyses excluding
studieswhere (1) diagnostic criteria were notspecified, (2)
reported phenotypic prev-alence exceeded the range of
often-citedprevalence rates, or (3) phenotypicprevalence was based
on previouslydiagnosed cases and not asymptom-atic cases. For key
questions address-ing the ability of ECG- or ECHO-basedtesting to
diagnose people with theconditions of interest, we repeated
theanalyses by excluding studies that didnot apply the reference
standard toparticipants with a nonsuggestive ECGand/or ECHO (ie,
verification bias).
For additional sensitivity analyses, weback-calculated disease
prevalencewhen applying a non-ECG referencestandard to define
disease. A positivescreening ECG (eg, a result suggestingLQTS) can
be either a true-positive (thepersonhasLQTS)ora false-positive
(thepersondoes not andwill not have LQTS).Thus, the frequency of
“suggestiveECGs” is not the same as the preva-lence of the disease.
One can back-calculate the prevalence of LQTS froman acceptable
alternative non-ECG ref-
erence standard to diagnose LQTS (eg,genetic testing for
deleterious mutationsin LQTS genes13), and from the pro-portion of
positive ECG tests in a pop-ulation. We performed such analysesonly
for LQTS, as an example to con-textualize our discussion comments.
Asdescribed in the Supplemental In-formation, we extended the
Bayesianmethod of Joseph and colleagues.22
RESULTS
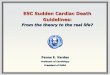
From 6954 titles and abstracts screenedforeligibility,we
retrieved andevaluatedthe full text in 396 articles, with
30meetingeligibility criteria (Fig 1).1,19,23–50
Characteristics of ReviewedStudies
In the 11 primary studies1,19,23–31 thatreported phenotypic
(ECG- or ECHO-based) prevalence findings, studypopulations ranged
from general tosubgroups of high school athletes andmilitary
conscripts. Studies were con-ducted in North America, Europe,
andAsia and had sample sizes rangingfrom 1369 to 1 336 377 (Table
1).
Twenty primary studies28,32–50 reportedsensitivity and
specificity estimates byusing ECG to detect LQTS and/or HCM,
FIGURE 1Literature search strategy.
4 RODDAY et al at University of Missouri-Columbia on March 6,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/lookup/suppl/doi:10.1542/peds.2011-0643/-/DCSupplementalhttp://pediatrics.aappublications.org/lookup/suppl/doi:10.1542/peds.2011-0643/-/DCSupplementalhttp://pediatrics.aappublications.org/
-
ECHO to detect HCM, or ECG/ECHO todetect HCM. Populations in
these stud-ies were mainly disease probands andtheir relatives. The
studies were con-ducted in North America, Europe, andAsia and had
sample sizes ranging from23 to 2770 (Table 2).
Hypertrophic Cardiomyopathy
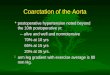
Based on 7 studies,1,19,24,25,27–29 HCMphenotypic (ECG- or
ECHO-based)prevalence ranged from 0 to 170per 100 000 (Fig 2) with
a summaryphenotypic prevalence rate of 45 per100 000 (95% CI:
10–79) but with sub-stantial variation between studies (I2 =91%, P
, .001). Inclusion of the studywith a phenotypic prevalence
estimateof zero29 helped inform the upperbounds of the estimate.
Although 1study27 did not specify diagnostic cri-teria, we included
it because its exclu-sion had no effect on phenotypicprevalence
(remained at 45 per 100000) and this study was based on
awell-established screening program inJapan. When adding 2
nonrepresenta-tive studies23,26 for sensitivity analysis,the
summary phenotypic prevalencerate decreased to 13 per 100 000
(95%CI: 7–19) with substantial heterogene-ity (I2 = 92%, P , .001).
Turning toscreening for HCM, Fig 3 illustratesa set of HSROC curves
for detectionby ECG (10 studies),28,32–40 ECHO(6
studies),33–35,37,40,41 and ECG/ECHO (4 studies).33–35,40 Based
onthe summary HSROC curves, the AUCvalues were high.
To provide clinical context for inter-preting these results, we
used thesummary phenotypic prevalence esti-mate for HCM and the 2
previouslydescribed illustrative points (the max-imal accuracy
point and the maximalspecificity point) on the HSROC
curvesfordetection of HCMbyusing ECG, ECHO,and ECG/ECHO (Table 3).
Regardless ofwhether an ECG, ECHO, or ECG/ECHO wasused, both
illustrative points yielded anTA
BLE1
ArticlesReportingPhenotypic(ECG-or
ECHO
-based)Prevalence
ofHCM,LQTS,andWPW
Author
PopulationandSource
Location
StudyDesign
SamplingTechnique
Age,y
SampleSize
DiagnosticCriteria
HCM,n
=9
Arola(1997)
23a
Medicalchartreviewwithinhospitals
Finland
RCRepresentative
Range:0–20
1336377
Interventricular
septum
orLV
wall
thickness$2SD
ofnorm
alColivicchi(2004)24
Pre-participationathleticscreening
Italy
PCRepresentative
Mean=
16.2SD=2.4
7568
LVwallthickness
$13
mm
Corrado(1998)
25Pre-participationathleticscreening
Italy
PCRepresentative
Mean=
19SD=5
33735
LVwallthickness
$13
mm
Corrado(2006)
1Pre-participationathleticscreening
Italy
PCRepresentative
Range:12–35
42386
LVwallthickness
$13
mm
Maron
(1995)
19Epidem
iology
studywith
subjects
selected
from
generalpopulation
USA
PCRepresentative
Range:23–35
4111
LVwallthickness
$15
mm
Maron
(1999)
26a
Diagnostictestingrequestedby
primaryphysicianinruralcom
munity
USA
PCRepresentative
Range:16–87
15137
LVwallthickness
.13
mm
Niimura(1989)
27Screeningof“presumablyhealthy”
nursery
schoolandjunior
high
schoolchildren
Japan
PCRepresentative
Ranges:3–5,12–14
930939
Notspecified
Nistri(2003)
28Screeningofmilitary
recruits(m
ales
only)
before
mandatory
military
service
Italy
RCRepresentative
Mean=
19SD=2
34910
LVwallthickness
$15
mm
Zou(2004)
29Epidem
iology
studyinrandom
sample
ofgeneralpopulation
China
PCRepresentative
Range:18–29
1369
LVwallthickness
$13
mm
LQTS,n
=4
Chiu(2008)
30Citywidesurvey
ofgeneralpopulation
Taiwan
PCRepresentative
Range:6–20
430391
QTc.450ms
Corrado(2006)
1Pre-participationathleticscreening
Italy
PCRepresentative
Range:12–35
42386
Male:QTc.440ms,Female:QTc.460ms
Kobza(2009)
31a
Screeningofmilitary
recruits(m
ostly
male)
before
mandatory
military
service
Switzerland
PCRepresentative
Mean=
19.2SD=1.4
40917
Male:QTc.450ms,Female:QTc.460ms
Niimura(1989)
27Screeningof“presumablyhealthy”
nursery
schoolandjunior
high
schoolchildren
Japan
PCRepresentative
Ranges:3–5,12–14
930939
Notspecified
WPW
,n=3
Chiu(2008)
30Citywidesurvey
ofgeneralpopulation
Taiwan
PCRepresentative
Range:6–20
430391
PRinterval,120ms;slurredupstroke
oftheQR
Scomplex;QRS
.120ms
Corrado(1998)
25Pre-participationathleticscreening
Italy
PCRepresentative
Mean=
19SD=5
33735
PRinterval,0.12
s;QR
S$0.12
sCorrado(2006)
1Pre-participationathleticscreening
Italy
PCRepresentative
Range:12–35
42386
PRinterval,0.12
s;QR
S$0.12
s
LV,leftventricular;PC,prospectivecohort;QTc,corrected
QTinterval;RC,retrospectivecohort.
aThesestudieswereincluded
insensitivityanalysisonly.
REVIEW ARTICLE
PEDIATRICS Volume 129, Number 4, April 2012 5 at University of
Missouri-Columbia on March 6,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
TABLE2
ArticlesReportingSensitivity
andSpecificity
forScreeningECGand/or
ECHO
todetect
HCM
andLQTS
Disorder
&Screening
Test
Author
(year)
Sample
Location
Age,y
ScreeningTestCriteria
Definitionof
Reference
(“Gold”)Standard
Verification
Bias
Sample
Size
HCM,n=11
ECG,n=
10Autore
(1988)
32First-degreerelatives
ofpatientswith
HCM
Italy
Mean=
36SD=20
LVhypertrophy;abnorm
alQwaves;negativeTwaves;
atrialfibrillation;leftor
rightb
undlebranch
block
ECHO
No72
Charron(1997)
33Genotypedprobands
and
first-degreerelatives
France
Range:18–29
Qwaves;LVhypertrophy,repolarizationalterations;
isolated
leftatrialenlargem
ent;shortP
Rinterval;
microvoltage;m
inor
Qwaves;bundle-branch
blockor
hemiblock
Genotyping
No58
Charron(1998)
34ChildrenofHCMgenotyped
families
France
,18
Qwaves;voltage;repolarizationalterations;abnormal
PRinterval,leftand/orrightatrialenlargement;
atrialfibrillation;abnorm
alQR
Saxis;increased
QRSduration;increasedventricularactivationtim
e;Twaves;R/S
ratio,rSr’aspect;bundlebranch
blockor
hemiblock;m
icrovoltage
Genotyping
No35
Charron(2003)
35Genotypedprobands
and
first-degreerelatives
France
Mean=
37.7SD=17.9
abnorm
alQwaves;T-waveinversion;LV
hypertrophy
Genotyping
No109
Dipchand
(1999)
36Childrenwith
HCMandhealthy
controls
Canada
Median=
3,Range:
0–19
Qwaves;R
waves;S
waves;T
waves;QTc
interval;voltage
ECHO
,LV
angiography
Yes
73
Fragola(1993)
37First-degreerelatives
ofpatientswith
HCM
Italy
Mean=
34SD=19
LVandRV
hypertrophy;atrialenlargem
ent;rhythm
disturbances;atrioventricularandintraventricular
conduction;ST-Tdisplacement;Qwaves;R
waves;QRS
ECHO
No116
Konno(2004)
38Genotypedrelatives
ofpatientswith
HCM
Japan
,30
Qwave;LV
hypertrophy;ST-segmentd
epression;
T-waveinversion
Genotyping
No45
Nistri(2003)
28Screeningofmilitary
recruits(m
ales
only)
Italy
$17
LVwallthickness;Q
waves;ST-Twaves
ECHO
No2770
Potter
(2010)
39Patientswith
HCM
andhealthycontrols
UK,Sweden,US
Mean=
48.7SD=14.0
RR,PR,P-wave,QR
SandQT
andJT
intervals;P,QR
S,andT-waveam
plitudes;frontalplane
QRS
andT-waveaxes;and
ST-segmentlevels
ECHO
Yes
181
Ryan
(1995)
40Probands
andrelatives
UK,Poland
Mean=
47SD=19
Rwaves;S
waves;Q
waves;ST-Twaves
Genotyping
orclinicaldiagnosis
No506
ECHO
,n=6
Charron(1997)
33Genotypedprobands
andfirst-degreerelatives
France
Range:18–29
MWT
Genotyping
No58
Charron(1998)
34ChildrenofHCMgenotyped
families
France
,18
MWT;intraventricular
septum
/posterior
wall;left
atrium
diam
eter;systolic
anterior
motionofmitral
valve;mid-systolic
aorticclosure;gradient
.30
mmHg;
mitralvalveregurgitation;E/Awaveratio
Genotyping
No35
Charron(2003)
35Genotypedprobands
and
first-degreerelatives
France
Mean=
37.7SD=17.9
MWTinanterior
septum
orposteriorwall;MWT
inposteriorseptum
orfree
wall;systolicanterior
motionofthemitralvalve,redundantleaflets
Genotyping
No109
Fragola(1993)
37First-degreerelatives
ofpatientswith
HCM
Italy
Mean=
34SD=19
Increasedinterventricular
septalthickness;posterior
wallthickness
ECHO
No122
Ho(2002)
41Genotypedrelatives
ofpatientswith
HCM
andhealthycontrols
USA
Mean=
35.6SD=12.6
LVejectionfraction;earlydiastolic
myocardialvelocities
Genotyping
No72
6 RODDAY et al at University of Missouri-Columbia on March 6,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
NPV that was near 100%, but PPV,number needed to screen,
false-positives, and false-negatives differedsubstantially. At the
maximal accuracypoint, the PPVs fell below 1% comparedwith PPVs
from 2% to 21% at the max-imal specificity point. The
maximalaccuracy point led to fewer false-negatives (16%) and a
lower numberneeded to screen to detect 1 case ofHCM (2600). In
contrast, the maximalspecificity point led to 40% to
96%false-negative rates and 4000 to 57 000needed to screen to
detect 1 case ofHCM. Last, the maximal accuracy pointled to more
false-positives per trueHCM case detected (400 vs 4–57) thanthe
maximal specificity point. By usingthe often-cited prevalence of
200 per100 00019 (4 times our estimate) re-sulted in similar NPV, a
fourfold in-crease in PPV and false-negatives per100 000 screened,
and a decrease inthe number needed to screen to detect1 case and
number of false-positiveswhen detecting 1 case.
Long QT Syndrome
Phenotypic (ECG-based) prevalencerates of the 3 studies
reporting on LQTSranged from1 to 12 per 100 000 (Fig 2),1,27,30
with a summary phenotypicprevalence rate of 7 per 100 000 (95%CI:
0–14) and substantial heterogeneity(I2 = 93%, P, .001). Although 1
study27
did not specify diagnostic criteria, weincluded it because its
exclusion in-creased phenotypic prevalence to only9 per 100 000 and
this study was basedon a well-established screening pro-gram in
Japan. The Kobza study31 wasexcluded because its prevalence
rate(550 per 100 000) exceeded often-citedprevalence rates of LQTS
(40–50 per100 000).13 When incorporating Kobza,the summary
prevalence increasedfivefold to 38 per 100 000 (95% CI: 19–58)and
heterogeneity increased (I2 = 99%, P, .001).42–50 The Bayesian
sensitivityanalysis giving the Schwartz13 priora low weight
(1/2500) resulted in similarTA
BLE2
Continued
Disorder
&Screening
Test
Author
(year)
Sample
Location
Age,y
ScreeningTestCriteria
Definitionof
Reference
(“Gold”)Standard
Verification
Bias
Sample
Size
Ryan
(1995)
40Probands
andrelatives
UK,Poland
Mean=
47SD=19
LVwallthickness
Genotyping
orclinicaldiagnosis
No506
ECG/ECHO
,n=
4Charron(1997)
33Genotypedprobands
andfirst-degreerelatives
France
Range:18–29
SeeaboveCharron1997
ECGandECHO
criteria
Genotyping
No58
Charron(1998)
34ChildrenofHCMgenotypedfamilies
France
,18
SeeaboveCharron1998
ECGandECHO
criteria
Genotyping
No35
Charron(2003)
35Genotypedprobands
andfirst-degreerelatives
France
Mean=
37.7SD=17.9
SeeaboveCharron2003
ECGandECHO
criteria
Genotyping
No109
Ryan
(1995)
40Probands
andrelatives
UK,Poland
Mean=
47SD=19
SeeaboveRyan
1995
ECGandECHO
criteria
Genotyping
orclinicaldiagnosis
No506
LQTS,n=9
ECG,n=
9Benhorin(1990)
42ParticipantsintheInternational
LQTS
Registry
andhealthy
controls
USA,Italy
Range:17–60
STsegm
ent;repolarizationarea;T
wavearea
symmetry
ECG:QTc.
440ms
Yes
352
Kaufman
(2001)
43Genotypedrelatives
ofpatientswith
LQTS
USA
#13
QTc
Genotyping
No38
Miller
(2001)
44Genotypedproband
andfirst-degreerelatives
USA
Range:2–85
QTc
Genotyping
No23
Moennig(2001)
45Genotypedprobands
andrelatives
Germ
any
Mean=
38Range:
31–50
QTc
Genotyping
No116
Neyroud(1998)
46Genotypedpatientswith
LQTS
andmatched
controls
France
Mean=
31SD=17
QTc
Genotyping
Yes
50
Swan
(1998)
47Genotypedprobands
andrelatives
Finland
Range:7–72
QTc
Genotyping
No73
Vincent(1992)48
Genotypedprobands
andrelatives
Notspecified
Range:1.5–39.0
QTc
Genotyping
No198
Viskin(2010)
49Patientswith
LQTS
andhealthycontrols
Notspecified
Mean=
32SD=15
QTc
LQTS
registry
orgenotyping
Yes
150
Wong(2010)
50Genotypedprobands
andrelatives
UKMean=
26SD=31
QTc
Genotyping
No159
ECG/ECHO
,ECG
combinedwith
ECHO
;LV,leftventricular;MWT,maximalwallthickness;QTc,corrected
QTinterval;RV,rightventricular.
REVIEW ARTICLE
PEDIATRICS Volume 129, Number 4, April 2012 7 at University of
Missouri-Columbia on March 6,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
phenotypic prevalence of 7 per 100 000(95% CI: 1–30), whereas
giving theSchwartz prior more weight increasedthe phenotypic
prevalence to 34 per100 000 (95% CI: 20–54). For detectingLQTS (9
studies), Fig 3 illustrates a set
of HSROC curves for ECG with a sum-mary AUC of 0.92.
To provide clinical context, we used thesummary phenotypic
prevalence esti-mate for LQTS and 2 illustrative points(the maximal
accuracy point and the
maximal specificity point) on theHSROCcurve for detection of
LQTS by using ECG(Table 3). For both points, the NPV wasnear 100%.
The PPV was very low(0.04% [1 in 2324]) at the maximal ac-curacy
point, but increased slightly atthe maximal specificity point
(0.7%[1 in 136]). With maximal accuracy, thenumber needed to screen
to detect 1case of LQTS with an ECG was morethan 16 000 with only
14% of those withLQTS missed (false-negatives), butmore than 2000
false-positives per LQTScase detected. With maximal specificity,the
number needed to screen to detect 1case increased to 135 000 and
91% ofthose with LQTS would be missed, butthere would be only 135
false-positives per LQTS case detected.By using the often-cited
prevalence of50 per 100 00013 (7 times our estimate)resulted in a
similar NPV, a sevenfoldincrease in PPV and false-negatives per100
000 screened, and a decrease innumber needed to screen to detect
1case and number of false-positives whendetecting 1 case.
WPW Syndrome
Three studies1,25,30 reported pheno-typic (ECG-based) prevalence
rates forWPW ranging from 68 to 222 per 100000 with a summary
phenotypic prev-alence rate of 136 per 100 000 (95% CI:55–218) (Fig
2) and substantial het-erogeneity (I2 = 95%, P , .001). Be-cause
ECG is considered the referencestandard and no studies
reportedestimates of sensitivity and specificityfor any other
screening tests to detectWPW, we assumed that its sensitivityand
specificity were one and the PPVand NPV estimates were perfect
andare not discussed further. By using theoften-cited prevalence
estimate of 200per 100 00020 did not substantially alterthe number
needed to screen.
DISCUSSION
Byusingpublished literature,we reporton phenotypic (ECG- or
ECHO-based)
FIGURE 2Forestplot of phenotypic (ECG- or ECHO-based)
prevalenceofHCM, LQTS, andWPW fromreviewedstudies.ES, effect
size.
FIGURE 3HSROC and AUC of reviewed studies for HCM and ECG, HCM
and ECHO, HCM and ECG/ECHO (ECG combinedwith ECHO), and LQTSandECG.
Solid black lines represent summaries of reviewed studiesandother
linesrepresent individual studies. The lines describe the
relationship between (average) sensitivity and(average) specificity
for varying diagnostic thresholds (eg, increasingly stringent ECGor
ECHOcriteria inthe 2 top panels, respectively). These lines
describe average test performance. It is generally
notstraightforward to correspond specific points on the curve to
specific cut points for ECG or ECHO. Thex-axis is restricted to the
range of the data.
8 RODDAY et al at University of Missouri-Columbia on March 6,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
prevalence ratesofHCM, LQTS, andWPWin asymptomatic children and
the testcharacteristics of ECG and/or ECHO indetecting
thesedisorders. Basedonourprespecified inclusion/exclusion
crite-ria and methodology, phenotypic prev-alence estimates
demonstrated widevariation across studies and werelower than those
in neonates (eg,Schwartz et al13) or studies examininggenotypic
prevalence. Consequently,we explored the effects of
alternativeprevalence estimates in our results.Although the AUC
ranged from 0.88 to0.92, indicating that ECG and/or ECHOare
statistically acceptable screeningtests for detecting the most
commondisorders that cause SCD, the low phe-notypic prevalence
substantially affectedthe predictive value.
Because these disorders have a verylow phenotypic prevalence,
choosinga point on the HSROC curve that max-imizes accuracy or
maximizes speci-ficity had little impact on NPV (nearly
100% NPV for HCM and LQTS); however,themaximal specificity point
resulted inimproved PPV (0.74% [1 in 136] to 21%)at the cost of
needing to screen moreindividuals to detect 1 case andmissingmore
diseased individuals because ofreduced sensitivity. With maximal
ac-curacy, the number needed to screen todetect 1 case fell and
fewer cases weremissed, but at the cost of lower PPV(0.04% [1 in
2324] to 0.26% [1 in 390])and more false-positives per
casedetected. These findings help defineboundaries of the
theoretical utility ofECG and/or ECHO as screening tests forthese
disorders, but are difficult tocomprehend in isolation. Unlike
“typi-cal” screening programs that valueruling in those who may
have the dis-ease (ie, sensitivity), these illustrativepoints
demonstrate that when pheno-typic prevalence is low,
prioritizingspecificity over sensitivity can improvePPV while not
affecting the NPV (similarto HIV screening51).
We performed calculations to under-stand how these estimates
might applyto population-based ECG screening.First, assuming
independence, thecombined prevalence estimate of HCM,LQTS, and WPW
from our meta-analysisis 188 per 100 000. When maximizingaccuracy,
the NPV approaches 100%,indicating a low false-reassurancerate.
However, the PPV of using anECG to screen for any of the 3
disordersis 1%, indicating a high false-alarmrate (99% of children
with a positiveECG would not have any of the dis-orders).
Conversely, when maximizingspecificity, the NPV still
approaches100% (false-reassurance rate remainsnear 0%), but the PPV
is 41% (false-alarm rate decreases to 59%). Asensitivity analysis
using often-citedprevalence rates (40–50 per 100 000for LQTS,13 200
per 100 000 for HCM,19
100–200 per 100 000 for WPW20) showeda more favorable outlook
for screening(higher PPV, fewer need to screen to
TABLE 3 Implications of Screening ECG and/or ECHO on PPV, NPV,
Number Needed to Screen, False-Positives, and False-Negatives for
Illustrative Pointson the HSROC Curve
Prevalence per100 000
Sensitivity Specificity PPV NPV Number Neededto Screen toDetect
1 Case
Number ofFalse-Positives WhenDetecting 1 Case
Number ofFalse-Negatives per100 000 Screened
Illustrative point where sensitivity and specificity are equally
weighted (maximal accuracy) with prevalence from meta-analysisHCM
& ECG 45 0.847 0.848 0.0025 (1/400) 0.9999 2624 399 7HCM &
ECHO 45 0.851 0.851 0.0026 (1/390) 0.9999 2611 389 7HCM &
ECG/ECHO 45 0.837 0.837 0.0023 (1/434) 0.9999 2655 433 7LQTS &
ECG 7 0.861 0.860 0.0004 (1/2324) 0.9999 16 592 2323 1WPW & ECG
136 1.000 1.000 1.0000 1.0000 735 0 0Illustrative point where
specificity is given more weight (maximal specificity) with
prevalence from meta-analysisHCM & ECG 45 0.039 0.999 0.0173
(1/58) 0.9996 56 980 57 43HCM & ECHO 45 0.607 0.999 0.2146
(1/5) 0.9998 3661 4 18HCM & ECG/ECHO 45 0.514 0.999 0.1879
(1/5) 0.9998 4323 4 22LQTS & ECG 7 0.106 0.999 0.0074 (1/136)
0.9999 134 771 135 6WPW & ECG 136 1.000 1.000 1.0000 1.0000 735
0 0Illustrative point where sensitivity and specificity are equally
weighted (maximal accuracy) with oft-cited prevalenceHCM & ECG
20019 0.847 0.848 0.0110 (1/91) 0.9996 590 90 31HCM & ECHO
20019 0.851 0.851 0.0113 (1/88) 0.9996 588 87 30HCM & ECG/ECHO
20019 0.837 0.837 0.0102 (1/98) 0.9996 597 97 33LQTS & ECG 5013
0.861 0.860 0.0031 (1/326) 0.9999 2323 325 7WPW & ECG 20020
1.000 1.000 1.0000 1.0000 500 0 0Illustrative point where
specificity is given more weight (maximal specificity) with
oft-cited prevalenceHCM & ECG 20019 0.039 0.999 0.0725 (1/14)
0.9981 12 821 13 192HCM & ECHO 20019 0.607 0.999 0.5488(1/2)
0.9992 824 1 79HCM & ECG/ECHO 20019 0.514 0.999 0.5074 (1/2)
0.9990 973 1 97LQTS & ECG 5013 0.106 0.999 0.0504 (1/20) 0.9996
18 868 19 45WPW & ECG 20020 1.000 1.000 1.0000 1.0000 500 0
0
ECG/ECHO, ECG combined with ECHO.
REVIEW ARTICLE
PEDIATRICS Volume 129, Number 4, April 2012 9 at University of
Missouri-Columbia on March 6,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
detect 1 case, fewer false-positiveswhen detecting 1 case, but
more false-negatives per 100 000 screened).
Although these results suggest that ECGmay be considered for
mass screeningfrom a statistical perspective and fromthe US
Preventive Services Task Forcecriteria,52 it does not address
othercomponents of screening programs,including changes in
mortality, mor-bidity, cost, quality of life, and func-tioning that
need to be weighed.Because of the very low phenotypicprevalence and
inherent inaccuracy innearly all medical tests (including
pe-diatric cardiologists reviewing ECGs53),screening for rare
disorders will leadto many false-positive tests that
triggeradditional diagnostic evaluations and,possibly, unnecessary
therapies andphysical activity restrictions. In addi-tion,
false-positives may lead to un-warranted child and parent
anxiety;previous work suggests this anxietymay not dissipate
immediately follow-ing a cardiac evaluation and may in-fluence
lifelong lifestyle decisions.54
Concern has been raised about in-creased rates of diagnosed
heart dis-ease where diagnosis may not behelpful (resulting in
diagnosis of car-diac nondisease and overtreatment55).Some children
may ultimately be di-agnosed by other means (eg, familyhistory,
emergence of sublethal symp-toms, diagnostic testing for
unrelatedindications) even in the absence ofmass screening, and
earlier diagnosisof the disorder may not provide sur-vival benefit.
Among those childrendetected by screening, the safety, effi-cacy,
and acceptability of specifictherapies and recommendations
forprophylaxis of SCD in asymptomaticchildren is sometimes
uncertain and
often based on expert consensus asopposed to clinical
evidence.6
In addition, families need to be awarethat a negative ECG does
not definitivelyrule out risk for SCD. Other rare cardiacdisorders
cause SCD, such as anomalousorigin of the coronary artery,
arrhyth-mogenic right ventricular cardiomy-opathy,
catecholaminergic ventriculartachycardia, and Brugada syndrome.With
the exception of Brugada syndrome,which manifests in late
adolescence,these disorders are not typically di-agnosed by ECG.
Also, given that clinicaland ECG findings may not manifest inHCM
until adolescence, programs thatscreen young children may miss
thosegenetically predisposed to developingHCM, which may
necessitate repeatECGs during adolescence.
This study has several limitations. First,our search was
restricted to literaturecataloged by Medline. Medline indexesmost
biomedical articles, making itunlikely that we omitted
importantfindings. Second, our estimates mayreflect publication
bias, as it is con-ceivable that “unsuccessful” studies
ofdiagnostic or detection interventionsmay not have been published.
Thisphenomenon, if it took place, wouldinflate our test accuracy
estimates.Third, heterogeneity existed betweenstudies. Populations
varied by age andstudies varied in their screening ap-proach and
their diagnostic criteria.Fourth, our calculations omitted a
tar-geted history and physical. Althoughwe included medical
history, physicalexamination, and family history in oursearch, we
found insufficient data forfurther analyses. Published
studiessuggest that history and physical ex-amination have low
sensitivity,25 lowPPV,56 and limited value from a health
economics perspective.3,4 Fifth, we de-fined phenotypic
prevalence basedon results from ECG or ECHO (not ge-notyping)
because these were thescreening options considered in ouranalysis
and because genotyping hasonly recently become available and
isstill evolving. In estimating the sensi-tivity and specificity of
ECG and/orECHO, however, we allowed genotypi-cally identified
cohorts because ge-netic testing will likely play a moreprominent
role in screening and diag-nosing disorders that cause SCD. Byusing
genotyping as the referencestandard allows us to incorporatesome
variability in penetrance (leadingto false-positives), which will
likely beimportant for screening test inter-pretation. Finally,
this study is limitedby considering only 3 disorders, butthese are
the 3 most common dis-orders detectable by ECG and/or ECHO.
Despite these limitations, this studyprovides an important
starting pointforevaluatingSCDscreeningprograms.Screening programs
may be gainingpopularity because of availability biasin risk
perception (ie, recent publicizedevents result in the
overestimatedlikelihood of a similar event occurring).Given our
results on the low phenotypic(ECG- or ECHO-based) prevalence
andthevariation in false-positiveratebasedon different
sensitivities and specific-ities, further cost- or
comparative-effectiveness analyses will be necessaryto determine
whether screening pro-grams to detect SCD in asymptomaticchildren
should be promoted as publichealth policy.
ACKNOWLEDGMENTWe thank Tully S. Saunders for his assis-tance in
manuscript preparation.
REFERENCES
1. Corrado D, Basso C, Pavei A, Michieli P,Schiavon M, Thiene G.
Trends in sudden
cardiovascular death in young competitiveathletes after
implementation of a pre-
participation screening program. JAMA.2006;296(13):1593–1601
10 RODDAY et al at University of Missouri-Columbia on March 6,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
2. Berger S, Utech L, Fran Hazinski M. Suddendeath in children
and adolescents. PediatrClin North Am. 2004;51(6):1653–1677,
ix–x
3. Wheeler MT, Heidenreich PA, Froelicher VF,Hlatky MA, Ashley
EA. Cost-effectiveness ofpreparticipation screening for
preventionof sudden cardiac death in young athletes.Ann Intern Med.
2010;152(5):276–286
4. Denchev P, Kaltman JR, Schoenbaum M,Vitiello B. Modeled
economic evaluation ofalternative strategies to reduce
suddencardiac death among children treated forattention
deficit/hyperactivity disorder. Cir-culation.
2010;121(11):1329–1337
5. Tanaka Y, Yoshinaga M, Anan R, et al. Use-fulness and cost
effectiveness of cardio-vascular screening of young adolescents.Med
Sci Sports Exerc. 2006;38(1):2–6
6. Kaltman JR, Thompson PD, Lantos J, et al.Screening for sudden
cardiac death in theyoung: report from a National Heart, Lung,and
Blood Institute working group. Circu-lation.
2011;123(17):1911–1918
7. Vetter VL, Elia J, Erickson C, et al; AmericanHeart
Association Council on Cardiovascu-lar Disease in the Young
Congenital Car-diac Defects Committee; American HeartAssociation
Council on Cardiovascular Nurs-ing. Cardiovascular monitoring of
childrenand adolescents with heart disease re-ceiving medications
for attention deficit/hyperactivity disorder [corrected]: a
scien-tific statement from the American HeartAssociation Council on
Cardiovascular Dis-ease in the Young Congenital Cardiac
DefectsCommittee and the Council on Cardiovascu-lar Nursing.
Circulation. 2008;117(18):2407–2423
8. Pastor PN, Reuben CA. Diagnosed attentiondeficit
hyperactivity disorder and learningdisability: United States, 2004
-2006. Na-tional Center for Health Statistics. VitalHealth Stat.
2008; 10(237)
9. Perrin JM, Friedman RA, Knilans TK; BlackBox Working Group;
Section on Cardiologyand Cardiac Surgery. Cardiovascular
mon-itoring and stimulant drugs for attention-deficit/hyperactivity
disorder. Pediatrics.2008;122(2):451–453
10. Maron BJ, Thompson PD, Ackerman MJ,et al; American Heart
Association Councilon Nutrition, Physical Activity, and
Metabo-lism. Recommendations and considerationsrelated to
preparticipation screening forcardiovascular abnormalities in
competitiveathletes: 2007 update: a scientific statementfrom the
American Heart Association Coun-cil on Nutrition, Physical
Activity, and Me-tabolism: endorsed by the American Collegeof
Cardiology Foundation. Circulation. 2007;115(12):1643–1655
11. Hennekens CH, Buring JE, Mayrent SL. Epi-demiology in
Medicine. 1st ed. Philadelphia,PA: Lippincott Williams &
Wilkins; 1987
12. Berger S, Dhala A, Friedberg DZ. Suddencardiac death in
infants, children, and ado-lescents. Pediatr Clin North Am.
1999;46(2):221–234
13. Schwartz PJ, Stramba-Badiale M, Crotti L, et al.Prevalence
of the congenital long-QT syn-drome. Circulation.
2009;120(18):1761–1767
14. DerSimonian R, Laird N. Meta-analysis inclinical trials.
Control Clin Trials. 1986;7(3):177–188
15. Higgins JP, Thompson SG. Quantifying het-erogeneity in a
meta-analysis. Stat Med.2002;21(11):1539–1558
16. Rutter CM, Gatsonis CA. A hierarchical re-gression approach
to meta-analysis of di-agnostic test accuracy evaluations. StatMed.
2001;20(19):2865–2884
17. Gatsonis C, Paliwal P. Meta-analysis of di-agnostic and
screening test accuracy eval-uations: methodologic primer. AJR Am
JRoentgenol. 2006;187(2):271–281
18. Dukic V, Gatsonis C. Meta-analysis of di-agnostic test
accuracy assessment studieswith varying number of thresholds.
Bio-metrics. 2003;59(4):936–946
19. Maron BJ, Gardin JM, Flack JM, Gidding SS,Kurosaki TT, Bild
DE. Prevalence of hypertro-phic cardiomyopathy in a general
populationof young adults. Echocardiographic analysisof 4111
subjects in the CARDIA Study. Cor-onary Artery Risk Development in
(Young)Adults. Circulation. 1995;92(4):785–789
20. Triedman JK. Management of asymptomaticWolff-Parkinson-White
syndrome. Heart. 2009;95(19):1628–1634
21. Higgins J, Green S, eds. Cochrane Handbookfor Systematic
Reviews of InterventionsVersion 5.0.2 [updated September 2009].
TheCochrane Collaboration. West Sussex, England:John Wiley &
Sons Ltd; 2009
22. Joseph L, Gyorkos TW, Coupal L. Bayesianestimation of
disease prevalence and theparameters of diagnostic tests in the
ab-sence of a gold standard. Am J Epidemiol.1995;141(3):263–272
23. Arola A, Jokinen E, Ruuskanen O, et al. Ep-idemiology of
idiopathic cardiomyopathiesin children and adolescents. A
nationwidestudy in Finland. Am J Epidemiol. 1997;146(5):385–393
24. Colivicchi F, Ammirati F, Santini M. Epide-miology and
prognostic implications ofsyncope in young competing athletes.
EurHeart J. 2004;25(19):1749–1753
25. Corrado D, Basso C, Schiavon M, Thiene G.Screening for
hypertrophic cardiomyopa-thy in young athletes. N Engl J Med.
1998;339(6):364–369
26. Maron BJ, Mathenge R, Casey SA, Poliac LC,Longe TF. Clinical
profile of hypertrophiccardiomyopathy identified de novo in
ruralcommunities. J Am Coll Cardiol. 1999;33(6):1590–1595
27. Niimura I, Maki T. Sudden cardiac death inchildhood. Jpn
Circ J. 1989;53(12):1571–1580
28. Nistri S, Thiene G, Basso C, Corrado D,Vitolo A, Maron BJ.
Screening for hyper-trophic cardiomyopathy in a young malemilitary
population. Am J Cardiol. 2003;91(8):1021–1023, A8
29. Zou Y, Song L, Wang Z, et al. Prevalence ofidiopathic
hypertrophic cardiomyopathy inChina: a population-based
echocardiographicanalysis of 8080 adults. Am J Med.
2004;116(1):14–18
30. Chiu SN, Wang JK, Wu MH, et al; Taipei Pe-diatric Cardiology
Working Group. Cardiacconduction disturbance detected in a
pediat-ric population. J Pediatr. 2008;152(1):85–89
31. Kobza R, Roos M, Niggli B, et al. Prevalenceof long and
short QT in a young populationof 41,767 predominantly male Swiss
con-scripts. Heart Rhythm. 2009;6(5):652–657
32. Autore C, Fragola PV, Picelli A, et al. Equivo-cal and
borderline myocardial hypertrophyin relatives of patients with
hypertrophiccardiomyopathy: possible implications ingenetics of the
disease. Cardiology. 1988;75(5):348–356
33. Charron P, Dubourg O, Desnos M, et al. Di-agnostic value of
electrocardiography andechocardiography for familial
hypertrophiccardiomyopathy in a genotyped adult pop-ulation.
Circulation. 1997;96(1):214–219
34. Charron P, Dubourg O, Desnos M, et al. Di-agnostic value of
electrocardiography andechocardiography for familial
hypertrophiccardiomyopathy in genotyped children. EurHeart J.
1998;19(9):1377–1382
35. Charron P, Forissier JF, Amara ME, et al.Accuracy of
European diagnostic criteriafor familial hypertrophic
cardiomyopathyin a genotyped population. Int J
Cardiol.2003;90(1):33–38, discussion 38–40
36. Dipchand AI, McCrindle BW, Gow RM, FreedomRM, Hamilton RM.
Accuracy of surface elec-trocardiograms for differentiating
childrenwith hypertrophic cardiomyopathy fromnormal children. Am J
Cardiol. 1999;83(4):628–630, A10
37. Fragola PV, Borzi M, Cannata D. The spec-trum of
echocardiographic and electrocardi-ographic abnormalities in
nonaffectedrelatives of patients with hypertrophic car-diomyopathy:
a transverse and longitudinalstudy. Cardiology.
1993;83(5-6):289–297
38. Konno T, Shimizu M, Ino H, et al. Diagnosticvalue of
abnormal Q waves for identificationof preclinical carriers of
hypertrophic
REVIEW ARTICLE
PEDIATRICS Volume 129, Number 4, April 2012 11 at University of
Missouri-Columbia on March 6,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
cardiomyopathy based on a moleculargenetic diagnosis. Eur Heart
J. 2004;25(3):246–251
39. Potter SL, Holmqvist F, Platonov PG, et al.Detection of
hypertrophic cardiomyopathyis improved when using advanced
ratherthan strictly conventional 12-lead electro-cardiogram. J
Electrocardiol. 2010;43(6):713–718
40. Ryan MP, Cleland JG, French JA, et al. Thestandard
electrocardiogram as a screen-ing test for hypertrophic
cardiomyopathy.Am J Cardiol. 1995;76(10):689–694
41. Ho CY, Sweitzer NK, McDonough B, et al.Assessment of
diastolic function withDoppler tissue imaging to predict genotypein
preclinical hypertrophic cardiomyopa-thy. Circulation.
2002;105(25):2992–2997
42. Benhorin J, Merri M, Alberti M, et al. LongQT syndrome. New
electrocardiographiccharacteristics. Circulation.
1990;82(2):521–527
43. Kaufman ES, Priori SG, Napolitano C, et
al.Electrocardiographic prediction of abnor-mal genotype in
congenital long QT syn-drome: experience in 101 related
familymembers. J Cardiovasc Electrophysiol. 2001;12(4):455–461
44. Miller MD, Porter CB , Ackerman MJ. Diagnos-tic accuracy of
screening electrocardiograms
in long QT syndrome I. Pediatrics. 2001;108(1):8–12
45. Moennig G, Schulze-Bahr E, Wedekind H,et al. Clinical value
of electrocardiographicparameters in genotyped individuals
withfamilial long QT syndrome. Pacing ClinElectrophysiol. 2001;24(4
pt 1):406–415
46. Neyroud N, Maison-Blanche P, Denjoy I, et al.Diagnostic
performance of QT intervalvariables from 24-h electrocardiography
inthe long QT syndrome. Eur Heart J. 1998;19(1):158–165
47. Swan H, Saarinen K, Kontula K, Toivonen L,Viitasalo M.
Evaluation of QT interval du-ration and dispersion and proposed
clin-ical criteria in diagnosis of long QTsyndrome in patients with
a geneticallyuniform type of LQT1. J Am Coll
Cardiol.1998;32(2):486–491
48. Vincent GM, Timothy KW, Leppert M, KeatingM. The spectrum of
symptoms and QTintervals in carriers of the gene for thelong-QT
syndrome. N Engl J Med. 1992;327(12):846–852
49. Viskin S, Postema PG, Bhuiyan ZA, et al.The response of the
QT interval to thebrief tachycardia provoked by standing:a bedside
test for diagnosing long QTsyndrome. J Am Coll Cardiol.
2010;55(18):1955–1961
50. Wong JA, Gula LJ, Klein GJ, Yee R, SkanesAC, Krahn AD.
Utility of treadmill testing inidentification and genotype
prediction inlong-QT syndrome. Circ Arrhythm Electro-physiol.
2010;3(2):120–125
51. Meyer KB, Pauker SG. Screening for HIV:can we afford the
false positive rate?N Engl J Med. 1987;317(4):238–241
52. Harris RP, Helfand M, Woolf SH, et al;Methods Work Group,
Third US PreventiveServices Task Force. Current methods ofthe US
Preventive Services Task Force:a review of the process. Am J Prev
Med.2001;20(suppl 3):21–35
53. Hill AC, Miyake CY, Grady S, Dubin AM. Ac-curacy of
interpretation of preparticipationscreening electrocardiograms. J
Pediatr.2011;159(5):783–788
54. Young PC. The morbidity of cardiac non-disease revisited. Is
there lingering con-cern associated with an innocent murmur?Am J
Dis Child. 1993;147(9):975–977
55. Bergman AB, Stamm SJ. The morbidity ofcardiac nondisease in
schoolchildren.N Engl J Med. 1967;276(18):1008–1013
56. Maron BJ, Shirani J, Poliac LC, Mathenge R,Roberts WC,
Mueller FO. Sudden death inyoung competitive athletes. Clinical,
de-mographic, and pathological profiles.
JAMA.1996;276(3):199–204
12 RODDAY et al at University of Missouri-Columbia on March 6,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/
-
DOI: 10.1542/peds.2011-0643; originally published online March
5, 2012;Pediatrics
Laurel K. LeslieIp, Jane W. Newburger, Susan K. Parsons, Thomas
A. Trikalinos, John B. Wong and Angie Mae Rodday, John K. Triedman,
Mark E. Alexander, Joshua T. Cohen, Stanley
in Asymptomatic Children: A Meta-analysisElectrocardiogram
Screening for Disorders That Cause Sudden Cardiac Death
ServicesUpdated Information &
/peds.2011-0643http://pediatrics.aappublications.org/content/early/2012/02/29including
high resolution figures, can be found at:
Supplementary Material
9/peds.2011-0643.DCSupplemental.htmlhttp://pediatrics.aappublications.org/content/suppl/2012/02/2Supplementary
material can be found at:
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables)
or in its entirety can be found online at: Information about
reproducing this article in parts (figures,
Reprints
http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN:
1098-4275.Grove Village, Illinois, 60007. Copyright © 2012 by the
American Academy of Pediatrics. All and trademarked by the American
Academy of Pediatrics, 141 Northwest Point Boulevard,
Elkpublication, it has been published continuously since 1948.
PEDIATRICS is owned, published, PEDIATRICS is the official journal
of the American Academy of Pediatrics. A monthly
at University of Missouri-Columbia on March 6,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/content/early/2012/02/29/peds.2011-0643http://pediatrics.aappublications.org/content/suppl/2012/02/29/peds.2011-0643.DCSupplemental.htmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/site/misc/reprints.xhtmlhttp://pediatrics.aappublications.org/