Embed Size (px)
Citation preview

NEW METHODS IN DIAGNOSIS AND MANAGEMENT OF AKI
Stefano Picca, MD Department of Pediatrics, Dialysis Unit
“Bambino Gesù” Pediatric Research Hospital, IRCCS
ROMA, Italy
Third IPNA-ESPN Master for Junior Classes Leuven (Belgium), October 28-30th, 2016

1. Diagnosis: biomarkers and new AKI classifications
2. Treatment: methods and timing
OUTLINE

TIME WINDOWS FOR AKI MANAGEMENT
Modified from Sutton, 2002
-sCreatinine increase OR -Urine Output decrease
• AKI diagnosis traditionally dependent on changes in SCr • sCr as a marker of AKI: limitations of time, body habitus, sex, age, steady-state
measurement, patient condition • diagnosis of AKI is often delayed with barrier to effective early intervention
AKI in children: the diagnosis problem
research of novel AKI biomarkers research of new AKI classifications

Period Acute Myocardial Infarction
1960s LDH
1970s CPK, myoglobin
1980s CK-MB
1990s Troponin T
2000s Troponin I
Multiple Therapies 50% ↓ Mortality
Supportive Care High Mortality
Need early biomarkers of AKI for improved understanding, early treatment and better outcomes
Biomarkers: AMI versus AKI
Acute Kidney Injury
Serum creatinine
Serum creatinine
Serum creatinine
Serum creatinine
Serum creatinine
Courtesy of P. Devarajan

AKI biomarker = a sensitive and specific early marker of renal injury ( “kidney troponin”)

2 4 6 8 12 24 36 48 60 72 84 96 108 120
Post CPB Time (hours)
Urine N
GA
L (
ng
/ml)
No AKI
(n=51)
AKI
(n=20)
Serum Creatinine Rise
Detection of Urinary NGAL by ELISA
Urine NGAL is upregulated 15-fold within 2 hours after CPB in patients who later develop ARF
Mishra J et al: Lancet 2005
15 14 13 12 11 10 9 8 7 6 5 4 3 2 1 0
25
50
75
100
125
150
175
200
225
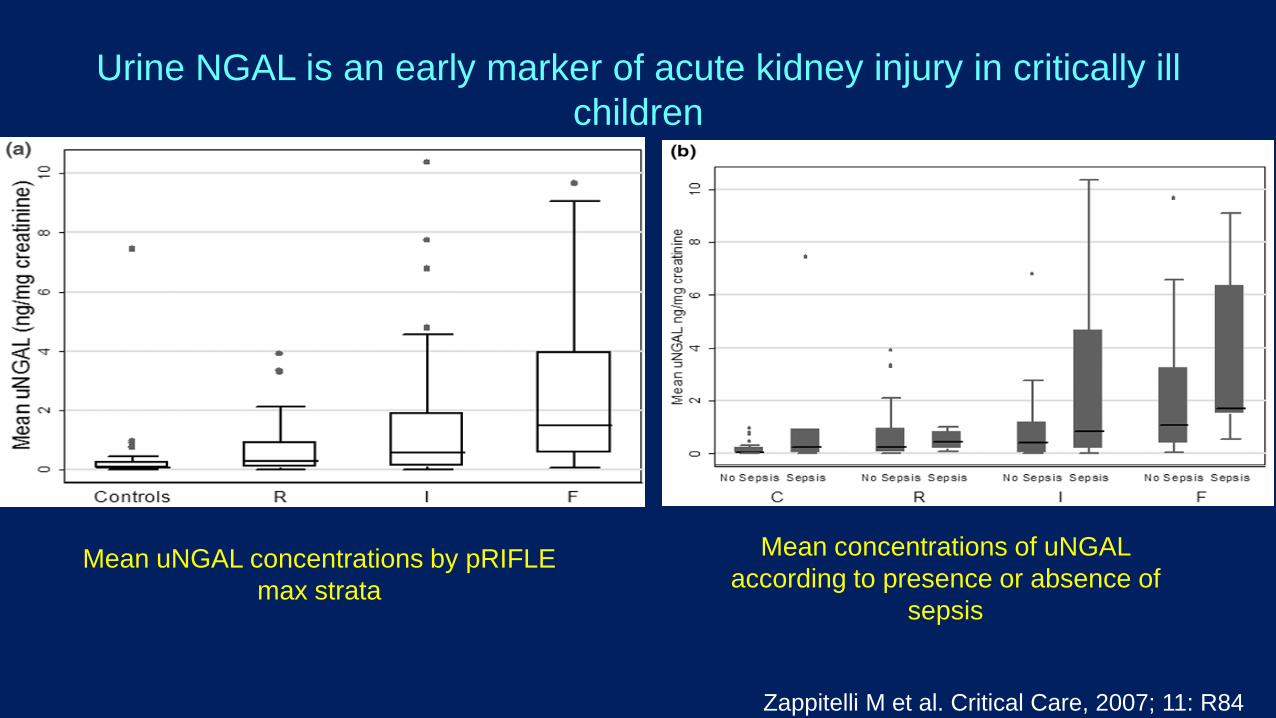
Zappitelli M et al. Critical Care, 2007; 11: R84
Urine NGAL is an early marker of acute kidney injury in critically ill
children
Mean uNGAL concentrations by pRIFLE
max strata
Mean concentrations of uNGAL
according to presence or absence of
sepsis
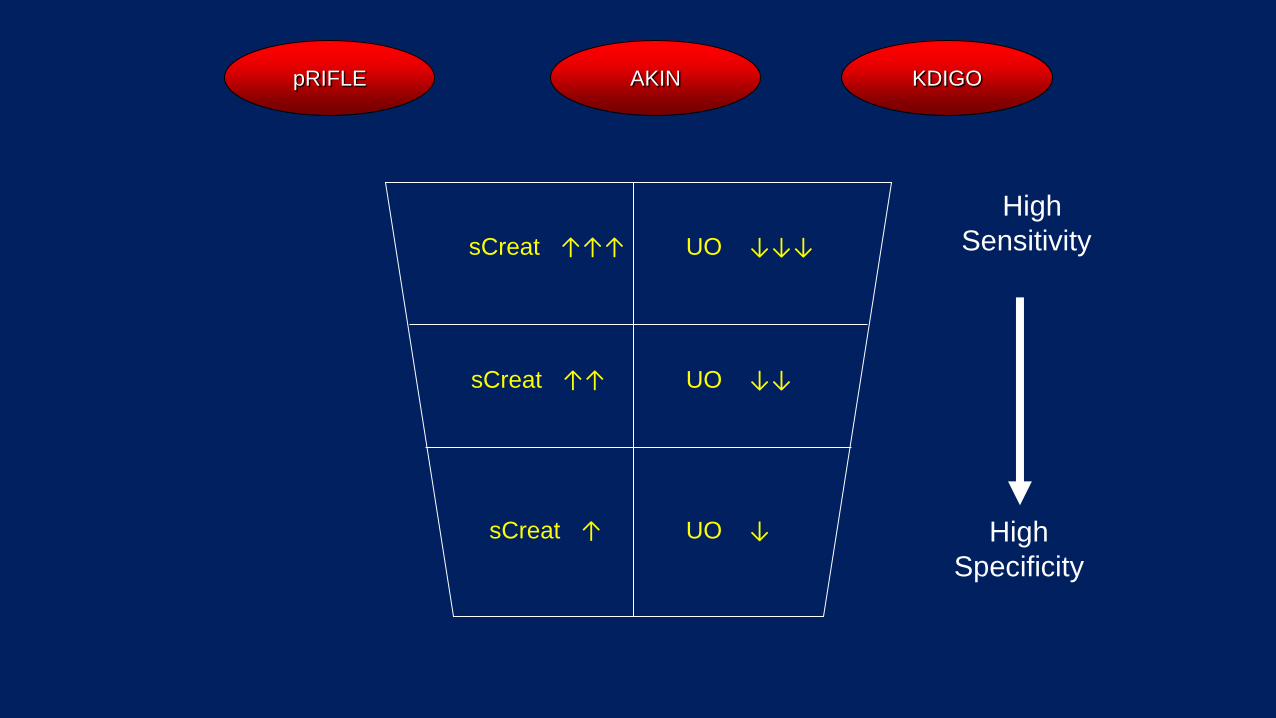
High
Specificity
High
Sensitivity sCreat ↑↑↑
sCreat ↑↑
sCreat ↑
UO ↓↓↓
UO ↓↓
UO ↓
pRIFLE AKIN KDIGO


Mortality increases with
RIFLE strata
in every study
Courtesy of SL Goldstein

Stuart L. Goldstein, MD
On Behalf of the AWARE Investigators

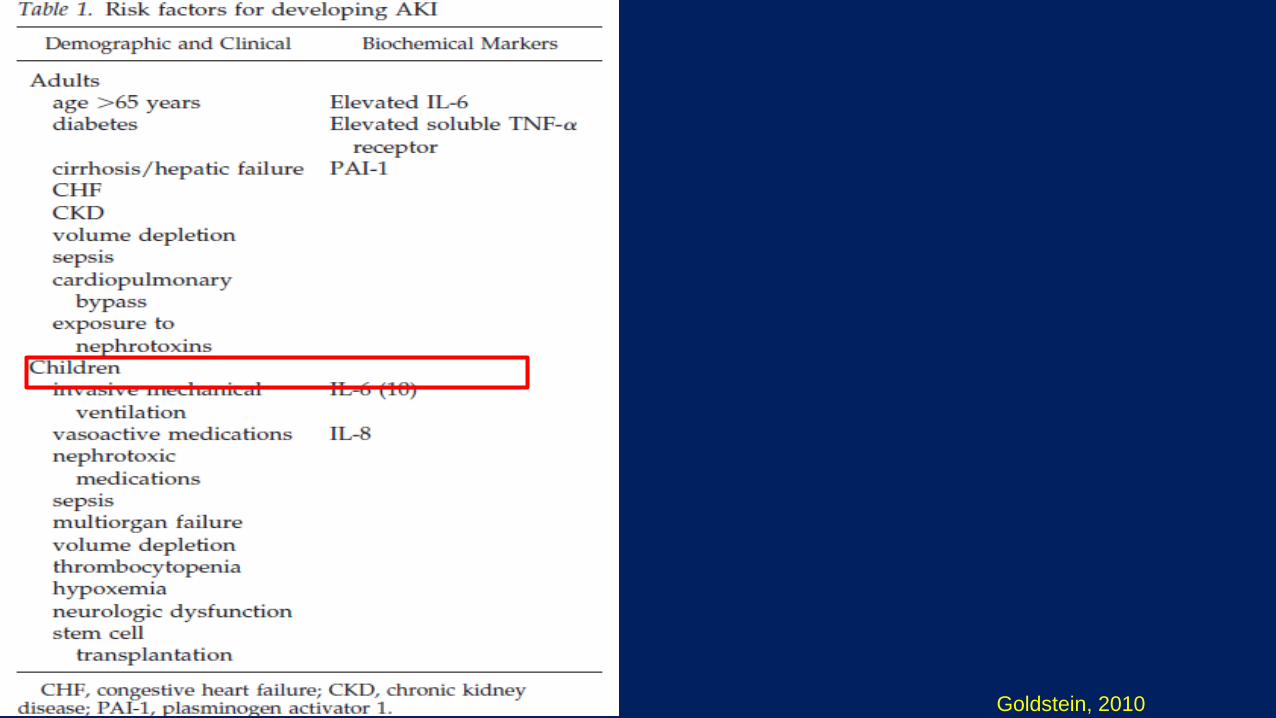
THE RENAL ANGINA APPROACH (1)
Basu, 2012; Goldstein, 2010

THE RENAL ANGINA APPROACH (2)
Basu, 2013

Sutherland SM, 2010
• n=297
•Data from ppCRRT
Registry
• ≤10% FO: 51.5%
• 10%-20% FO: 17.2%
• ≥20% FO: 31.3%
P= 0.07
P<.001 P<.001

ALL NEPHROLOGICAL NON NEPHROLOGICAL
DEAD
ALIVE
<5% <5% <5% 5-10% >10% >10% >10%
%FO %FO %FO
0%
20%
40%
60%
80%
100%
Surv
ival
0%
20%
40%
60%
80%
100%
0%
20%
40%
60%
80%
100%
5-10% 5-10%
n= 131
Overall survival: 45,8%

I want my p< 0,05 !!!!!
Hey, Dr. Dialysis what the hell do you want???
The ped-AKI Arena: Dr. Dialysis and Mr. Underlying Disease


Akcan-Arikan (2007), n=123: • 71% of patients who attained pRIFLE F AKI did not receive RRT.
• “pRIFLE criteria is overly sensitive for identifying severe AKI…” Mehta A (2010), n= 80: All pts needing RRT belonged to F group
• “pRIFLE important in determining RRT” Almaslamani T (2010), n= 95:
• “AKI acc. to RIFLE: only 37% of RRT… not a good predictor” Plotz FB (2008), n= 103:
• 6/103 required RRT: only 1 was pRIFLE F
TRANSLATING CLASSIFICATION INTO MANAGEMENT. IS IT POSSIBLE?

Duzova A, 2010

Let’s classify….. Hurry, he’s about to die….
AKI DEFINITION: FACING THE EXTREMES…

TIME WINDOWS FOR AKI MANAGEMENT
Nephroprotection?
Modified from Sutton, 2002
Fluids
Drugs
RRT
?

FENOLDOPAM AND NEPHROPROTECTION: MECHANISM
FENOLDOPAM MESYLATE
Short-acting selective DA-1 dopaminergic receptor agonist
INDUCES:
• Increased cAMP-PKA production in renal arteries smooth muscle:
arterial relaxation and
increased renal blood flow
• Increased cAMP concentration in tubular cells and inhibition of Na-H and Na-K ATPase: increased natriuresis
• Decreased aldosterone production:
increased natriuresis
M Ranucci Minerva Anestesiol 2010 Z Ricci Interact CardioVasc Thorac Surg 2008

n= 80 AKI (pRIFLE>0): 50% in group F 72% in group C (P = 0.08)

Factors involved in the decision for dialysis in AKI
“MODERN” • Fluid overload control • Inflammatory mediators removal with
CRRT • “Anticipation” (based on AKI staging,
clinical conditions, etc)
“TRADITIONAL” • Reliance on criteria for maintenance dialysis initiation (medically
refractory acidosis, hyperkalemia, threshold creatinine) simply wrong • Fluid restriction failure restriction hard to establish, often induces late indication to
dialysis • “Waiting” for renal function reprise undefined duration in often undefined AKI diagnosis

2 M. 5 yrs • BMT • Sepsis, SIRS, hypotension • 2 pressors • Fluid overload +10%. •UO 3.1 ml/kg/h with Lasix • sCreat 0.5 mg/dl
2 CLINICAL CASES
1 F. 14 mos • HUS • Diarrhea, dehydration • Anuria • rehydration • Fluid overload 15% • sCreat 1.3 mg/dl.
TREATMENT ?

PD Peritoneal Dialysis •Continuous • Low cost, easy application •Good CV tolerance •No extracorporeal circuit •No anticoagulation •Low ultrafiltration
PD DEFINITION
Dialysate +
Filtrate
Diaysate

HD HemoDialysis •Intemittent •Poor CV tolerance •Anticoagulation •Quick depuration of small molecules and water •Highly specialized equipment and expertise
HD DEFINITION
Filtrate- Diaysate
Dialysate

CVVH (postdilution) Continuous VenoVenous Hemofiltration •Continuous •Good CV tolerance •Slow depuration of small molecules and water •Anticoagulation •Highly specialized equipment and expertise
CRRT DEFINITION
Filtrate
collecting
device
Replace-ment
fluid

Courtesy of Z. Ricci

Pediatric patients in the range of 2-10 kgs
(approximate BSA of 0.15–0.5 m2)
DESIGNED BY THE INTERNATIONAL RENAL RESEARCH INSTITUTE OF
VICENZA (2011)

OPBG EXPERIENCE
- 12 neonates
- About 32 sessions
- 50% times 0.075 m2
- Weight range 2.1-3.5 kg
- CVVH 100% pre
- Qb 5-14 ml/min
- Q rep 20-30 ml/kg/h
- NETQuf 10-20 ml/h
- Vasc access 6.5F, 4F
or two 20-24G cannulas
Courtesy of Z. Ricci

time
Solutes/
fluid
PD
HD
CRRT

1. Adana (Dr. Aysun Karabay BAYAZIT)
2. Ankara (Dr. Ali DUZOVA)
3. Berlin (Dr. Uwe QUERFELD)
4. Bern (Dr. Giacomo SIMONETTI)
5. Bologna (Dr. Francesca Mencarelli)
6. Budapest (Dr. Peter SALLAY)
7. Bordeaux (Dr. Jerome HARAMBAT)
8. Firenze (Dr. Marco MATERASSI)
9. Hamburg (Dr. Jun OH)
10. Heidelberg ( Dr. Claus SCHMITT)
11. Innsbruck (Dr. Gerard CORTINA)
12. Istanbul (Dr. Salim CALISKAN)
13. Istambul (Dr. Sevinc EMRE)
14. Izmir (Dr. Pelin ERTAN)
15. Izmir (Dr. Pelin MIR)
16. Izmir (Dr. Ebru YILMAZ)
17. London (Dr. Rukshana SHROFF)
Lyon (Dr. Bruno RANCHIN)
Dialysis Treatment of AKI in Europe:
The 4C Study Group Survey
19. Lodz (Dr. Marcin TKACZY)
20. Katowice (Dr. Maria SZCZEPANSKA)
21. Kaunas (Dr. Sarunas RUDAITIS)
22. Kocaeli (Dr. Zelal Ekinci)
23. Koln (Dr. Lutz WEBER)
24. Malatya (Dr. Yilmaz TABEL)
25. Marburg (Dr. Guenter KLAUS)
26. Milano (Dr. Gianluigi ARDISSINO)
27. Padova (Dr. Enrico VIDAL)
28. Porto (Dr. Helena PINTO)
29. Rome (Dr. Isabella GUZZO, Dr. Stefano PICCA)
30. Rostock (Dr. Hagen STAUDE)
31.Strasbourg (Dr. Michel FISCHBACH)
32. Vilnius (Dr. Augustina JANKAUSKIENE)
33. Warsaw (Dr. Ryszard GRENDA)
34. Wien (Dr. Klaus ARBEITER)
• 34 participating centers

CRRT
PD
HD
0%
10%
20%
30%
40%
50%
60%
1995 1999 2003 Warady et al, Pediatr Neph 2003, 15:11-3
0
10
20
30
40
50
60
70
% o
f tr
eate
d p
atients
Picca, European Survey 2013,
unpublished
European Survey of AKI
treatment with dialysis
in children
n= 903

author n Time to PD start Pts with negative fluid
balance
Survivors
Lowrie (2000) 17 NA 35% 24%
Fleming (1995) 21 2.5 days (1-6) after surgery 36% 38%
Golej (2002) 116 NA, but 43% of pts started on PD
when CVP>10 mmHg
53% 47%
Werner (1996) 23 2.6±0.6 days 100% 53%
Santos (2012) 23 4.8±16.8 hrs 100% 56.6%
Chien (2009) 7 1.2±0.4 days after AKI onset NA 57%
Dittrich (1999) 27 In the OR or first hrs in ICU 100% 73%
Sorof (1999) 20 22 hrs 100% 80%
PD AFTER HEART SURGERY IN CHILDREN:
FLUID BALANCE AND SURVIVAL THROUGH THE YEARS
Survival > 50% occurs only when all patients reach a negative fluid
balance with PD


AKI RISK IDENTIFICATION AND MANAGEMENT
EASILY PREDICTABLE/ PREDICTABLE: Heart surgery,
initial sepsis, BMT, LT, nephrotoxicity, etc
HARDLY PREDICTABLE/ UNPREDICTABLE:
Late referral, ATN, metabolic diseases , etc
Classification/biomarkers most useful
pRIFLE-AKIN-KDIGO
Classification/biomarkers less useful
RRT
Most of the times =
Fluid overload
Preventive interventions possible
volume
diuretics
fenoldopam
RRT ?



“Is he so sick because he has a horrible disease or because someone (may be me…) waited too long?”

ACKNOWLEDGEMENTS
• Nephrology Unit: Isabella Guzzo, MD and Lara De Galasso, MD for OPBG CRRT database and EurAKId website
• CICU: Zaccaria Ricci, MD
• PICU: Matteo Di Nardo,MD; Emanuele Rossetti, MD
• NICU: Andrea Dotta, MD
• All ICUs nurses
• All Dialysis Unit nurses
• Tim Bunchman, Stu Goldstein, Claudio Ronco for precious advices and friendship through the years . Thanks!

Dialysis Unit, “Bambino Gesù” Pediatric Hospital
Roma, Italy.
Doctor:
S. Picca
Headnurse:
V. Bandinu
Nurses:
N. Avari
D. Ciullo
E. Iacoella
P. Iovine
P. Lozzi
L. Stefani
Nurse Coordinator:
M. D’Agostino


Available information mainly coming from one multicenter study (ppCRRT) utilizing
only one modality (CRRT) in one patient population (critical)
DIALYSIS in PEDIATRIC AKI:
ARE OUTCOME AND DIALYSIS MODE RELATED?
PROBLEMS AFFECTING STUDIES
Retrospectively:
•No standardized AKI definition
•Indication to the modality depending on local facilities/expertise
•Changing modalities in the same patient Prospectively:
•Paucity of patients
•Ethical issues for randomized studies
•Organization issues with ICUs
LACK of RANDOMIZED
STUDIES

Peritoneal vs Extracorporeal Dialysis in AKI: Pediatric Studies
AA (yr) n PD n CRRT n IHD Type
of study
Mortality P
Fleming (1995) 17 17 - retrospective 38% vs 37% NS
Bunchman
(2001)
59 61 106 retrospective 51% vs 60% vs 19% <0.01
Bandeira
(2005)
82 36 - retrospective - NS
Krause
(2011)
81 31 18 retrospective 52% vs 83% vs 8% <0.01
Retrospective Studies comparing different Dialysis Modalities are affected by
the attitude of addressing the patient to a specific modality according to the
severity of illness

AKI Definitions to 2002
• Over 30 definitions in published literature – Nearly all based on absolute or change in serum
creatinine concentration
• Few prospective pediatric studies – Retrospective studies assess AKI causes
– Control group without AKI not assessed to determine risk factors for AKI
Courtesy of SL Goldstein

?

PCCM 2006
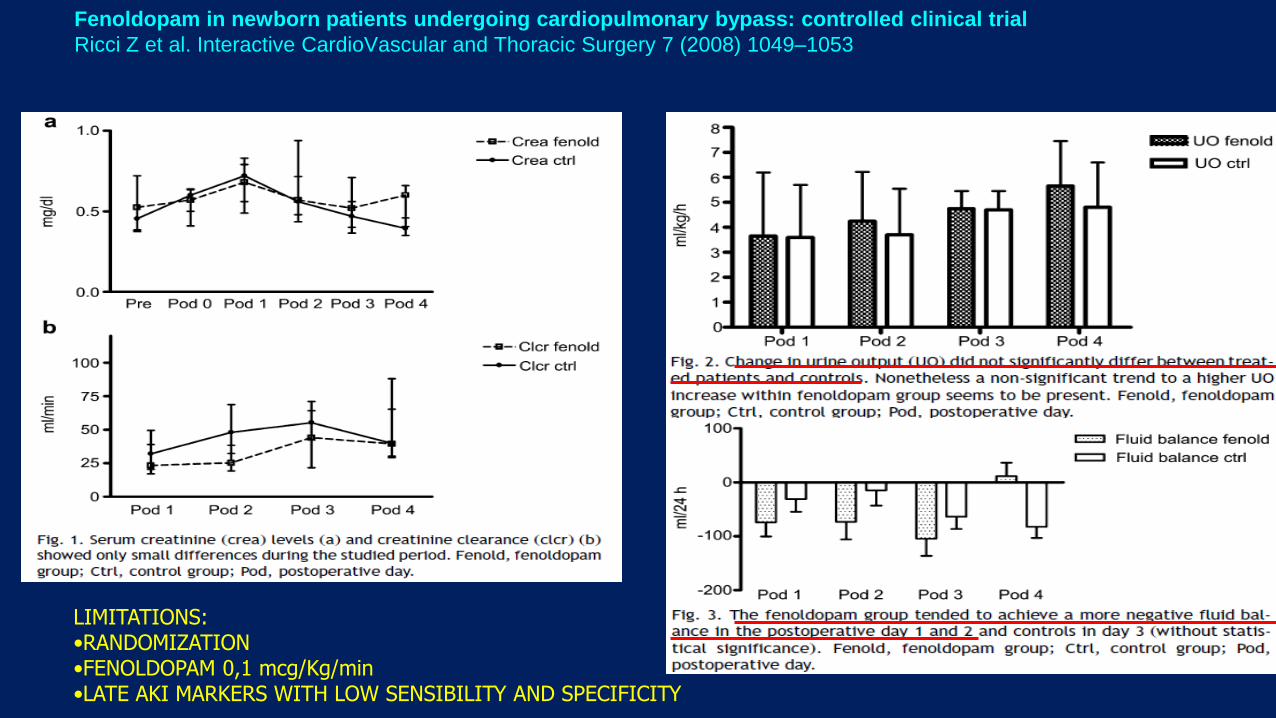
LIMITATIONS: •RANDOMIZATION •FENOLDOPAM 0,1 mcg/Kg/min •LATE AKI MARKERS WITH LOW SENSIBILITY AND SPECIFICITY
Fenoldopam in newborn patients undergoing cardiopulmonary bypass: controlled clinical trial
Ricci Z et al. Interactive CardioVascular and Thoracic Surgery 7 (2008) 1049–1053

Goldstein, 2010

KDIGO 2012

CHANGE IN THE EPIDEMIOLOGY OF AKI
Primary renal disease AKI as complication of
systemic diseases
Single organ failure
Renal ward/ Dialysis Unit
MODS
ICU
+
Courtesy of E. Vidal, modified

Day N
(% total) Nephrotoxins Diuretics
Cumulative
Fluid
Balance
% FO KDIGO 2-3
by Cr
KDIGO 2-3 by
UOP
1 4730
(90.4) 37.1% 14.7% 604
(200-1266)
3.6
(1.1-6.8) 7.8% 2.4%
2 2937
(56.1) 42.0% 23.9% 870
(289-1685)
5.4
(1.6-10) 10.1% 1.9%
3 2085
(39.9) 42.3% 30.9% 1050
(339-2042)
6.3
(1.9-8.4) 11.3% 2.3%
4 1563
(29.9) 39.4% 35.6% 1145
(353-2518)
7.5
(2.1-14.6) 14.0% 2.8%
5 1225
(23.4) 40.7% 38.8% 1299
(391-2502)
8.7
(2.7-16.5) 11.6% 3.2%
6 985
(18.8) 41.5% 40.4% 1454
(469-2794)
10
(3.1-18.9) 12.9% 2.4%
7 837

IN NEONATES
“Immature” newborn kidney
Torres de Melo Bezerra, NDT 2013
Low GFR
High Urine Output
To accomplish the physiologic extracellular post-natal fluid reduction (10% weight loss)
To manage the large water load coming from breast feeding

nRIFLE
Ricci, Ronco, adapted from Torres de Melo Bezerra, NDT 2013

Jetton, Askenazi, adapted from Koralkar R, 2011
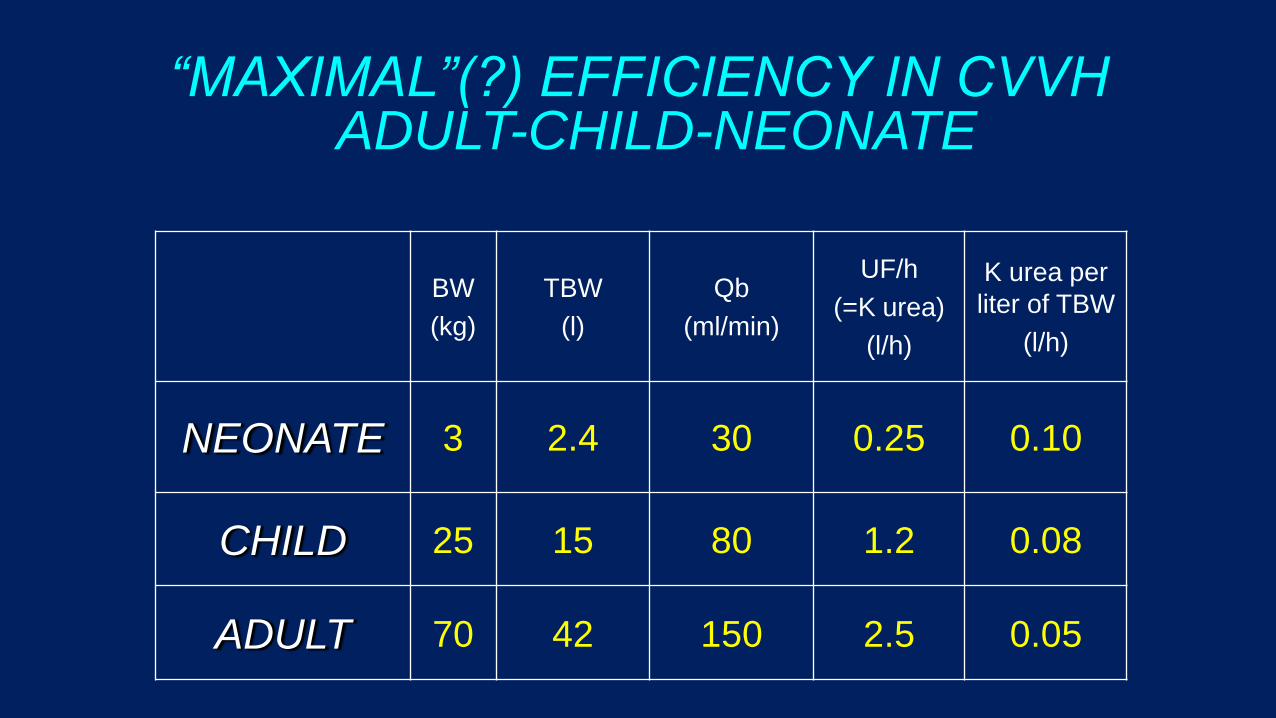
“MAXIMAL”(?) EFFICIENCY IN CVVH ADULT-CHILD-NEONATE
BW
(kg)
TBW
(l)
Qb
(ml/min)
UF/h
(=K urea)
(l/h)
K urea per
liter of TBW
(l/h)
NEONATE 3 2.4 30 0.25 0.10
CHILD 25 15 80 1.2 0.08
ADULT 70 42 150 2.5 0.05
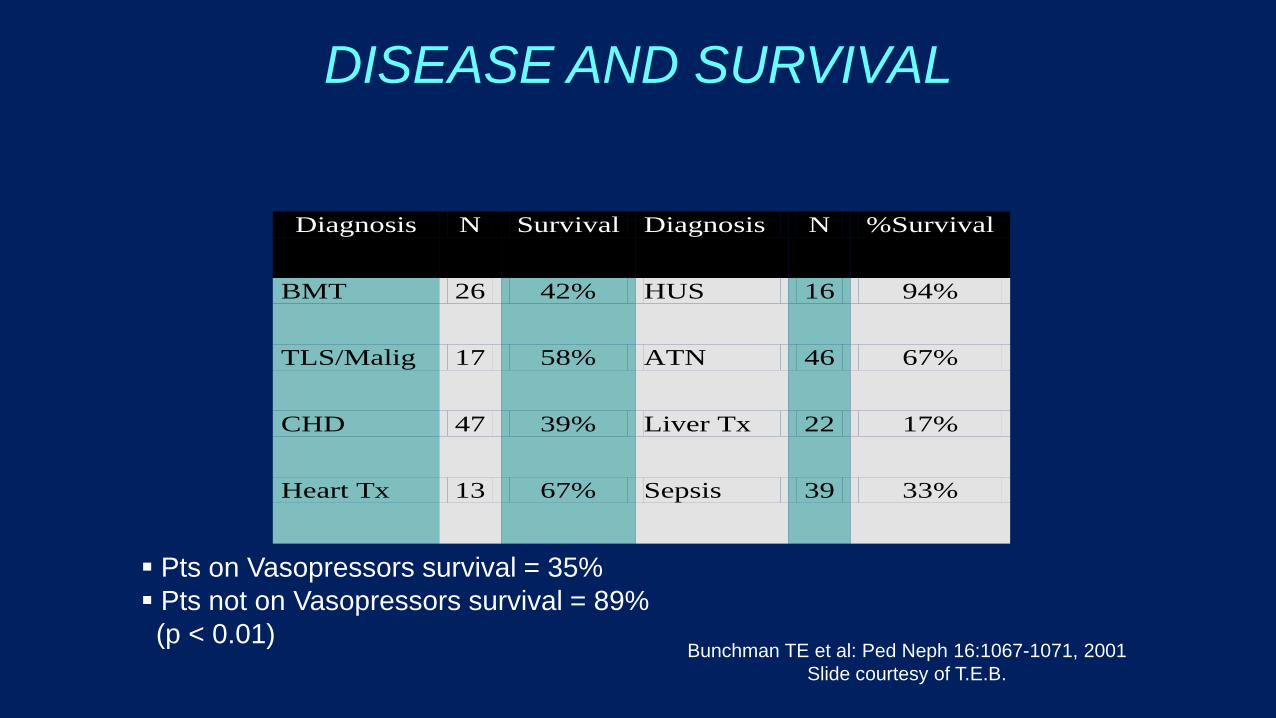
DISEASE AND SURVIVAL
Diagnosis N Survival Diagnosis N %Survival
BMT 26 42% HUS 16 94%
TLS/Malig 17 58% ATN 46 67%
CHD 47 39% Liver Tx 22 17%
Heart Tx 13 67% Sepsis 39 33%
Bunchman TE et al: Ped Neph 16:1067-1071, 2001
Slide courtesy of T.E.B.
Pts on Vasopressors survival = 35%
Pts not on Vasopressors survival = 89%
(p < 0.01)
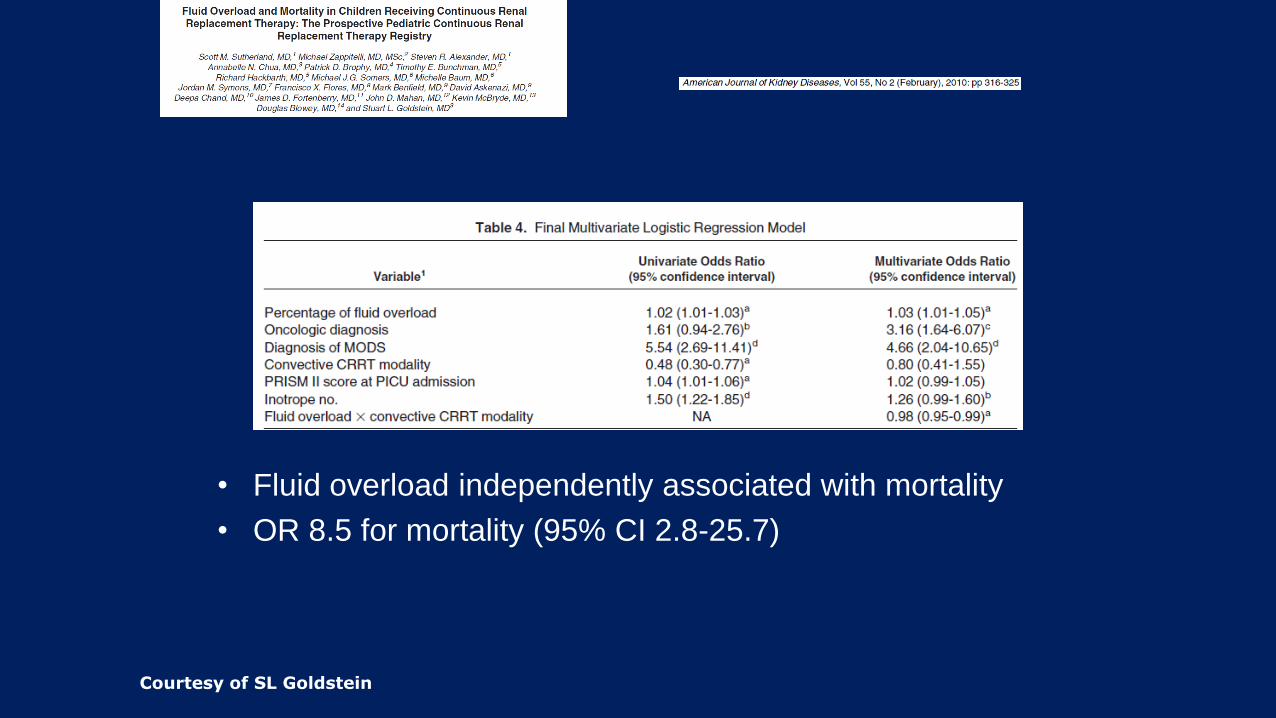
• Fluid overload independently associated with mortality
• OR 8.5 for mortality (95% CI 2.8-25.7)
Courtesy of SL Goldstein

CRRT O.R. 95% CI p
Days in PICU before CRRT 1,069 1,002 1,141 0,043
Fluid Overload 1,039 1,010 1,069 0,009
Fluid Overload>10% 2,993 1,431 6,258 0,004
N° pressors 1,878 1,332 2,648 0,000
Vasoactive score 1,082 1,034 1,132 0,001
Dopamine 1,278 0,982 1,663 0,068
AKI 2,974 1,346 6,572 0,007
MODS 9,644 4,051 22,958 0,000
Hypotension 4,488 1,858 10,842 0,001
Diuretics 2,623 1,271 5,412 0,009
CRRT
Qr 0,998 0,993 1,003 0,482
Qd 0,999 0,996 1,003 0,648
Qb 0,980 0,860 1,118 0,767
THE OPBG CRRT REGISTRY: RETROSPECTIVE DATA. UNIVARIATE ANALYSIS
Guzzo, 2013, unpublished

Need for dialysis
AKI definition pRIFLE
AKIN
KDIGO
sCreat or UO changes
OVER THE YEARS…





























