Embed Size (px)
Citation preview

Vol. 2, 1867-1871, November 1996 Clinical Cancer Research 1867
3 The abbreviation used is: EPO, eosinophil peroxidase.
New Marker for Blood Vessels in Human Ovarian and Endometrial
Cancers’
Michael Samoszuk,2 Fritz Lin, Paul Rim, and
Gary Strathearn
Pathology Department, University of California-Irvine, Irvine,
California 92697-4800 lM. S., F. L., P. Ri, and Isotope Products
Laboratories, Burbank, California 91504 [G. S.]
ABSTRACT
Angiogenesis plays a critical role in tumor biology and
may someday be a target for novel therapeutic interventions.
To date, however, relatively few markers have been identi-
fled that can specifically distinguish between microvessels in
benign versus malignant lesions. Here we report that thecationic heme-protein eosinophil peroxidase (EPO) was lo-
calized by in situ immunohistochemistry on the vascular
endothelial cells and/or connective tissue stroma in 16 of 16cases of human endometrial carcinoma and in 12 of 15 cases
of ovarian carcinoma. Similar deposits of EPO were notdetected in normal endometrial tissues or ovaries from fivehealthy subjects, in adjacent uninvolved tissues from fourtumor-bearing subjects, or in any normal organs from five
other subjects. These findings imply that eosinophil degran-ulation is a significant and previously unappreciated corn-ponent of the interaction between ovarian and endornetrialcancers and the host. Moreover, the abundant and highly
specific nature of the EPO deposition near and within the
microvessels of these cancers suggests that eosinophil de-
granulation is a new marker for tumor blood vessels that
potentially could be exploited to treat these important types
of cancers that currently lack highly effective therapies.
INTRODUCTION
A novel approach to the treatment of solid tumors would be
to target toxic drugs to the microvasculature of the tumor rather
than to the tumor cells themselves ( 1). As summarized by
Thorpe (2), such an approach could have several advantages.
For example, tumor vascular endothelial cells are directly ac-
cessible to drugs in the blood, whereas tumor cells are mostly
inaccessible, especially to large drugs such as monoclonal an-
tibodies. In addition, such an approach might be applicable to a
wide variety of solid tumors because all of them require a blood
supply for their survival and growth. Furthermore, the endothe-
hal cells within tumors are nonmalignant, thereby making it
unlikely that drug-resistant mutants would develop. Finally, this
approach has inherent amplification properties because many
Received 4/1 5/96; revised 6/20/96; accepted 8/16/96.
I Supported by Grant R01CA69079 from the National Cancer Institute.2 To whom requests for reprints should be addressed, at Pathology
Department. Medical Sciences D-440, University of California-Irvine,Irvine, CA 92697-4800. Phone: (714) 824-2323; Fax: (714) 824-2160.
tumor cells rely on each microvessel for nutrients and oxygen-
ation. Therefore, even partial damage to the blood vessels within
tumors might result in relatively massive destruction of tumor
cells.
The ideal target molecule for such a therapeutic approach
would be expressed at high density on the surface of vascular
endothelial cells in solid cancers and be absent on endothelial
cells in normal tissues. To date, several promising candidate
molecules with these properties have been identified in humans,
including tissue factor in breast cancer (3, 4), endoglin (5),
endosialin (6), an endoglin-like molecule (7), a fibronectin
isoform (8), receptors (9) for vascular endothelial cell growth
factor, and vascular endothelial growth factor itself (10).
Using a murine monoclonal antibody called EOS, we have
been studying the deposition ofEPO,3 a markedly cationic heme
protein, in human lymphomas (1 1, 12) and in breast cancers
(13). Normally, EPO is exclusively confined to the intracellular
granules within intact eosinophils. In a variety of pathological
conditions, however, eosinophils release their granule contents,
which then bind avidly to the anionic surfaces of adjacent cells.
Here we describe immunohistochemical evidence of a similar
degranulation phenomenon occurring in the microvasculature of
human ovarian and endometrial cancers.
MATERIALS AND METHODS
Reagents. Immunohistochemical staining of cryostat
sections of human ovarian and endometrial cancers was care-
fully performed, controlled, and evaluated using the same pro-
cedures and monoclonal antibodies that we recently used to
study human breast cancers ( I 3). In brief, an IgG 2a murine
monocbonal antibody called SF25.5 that binds to human EPO
was derived as described elsewhere ( I I ). This antibody is highly
specific for EPO and does not bind to any other cell types, to
myeloperoxidase, or to normal endometrium or ovaries when
radiolabeled and administered to human subjects ( I 2). Also
included in this study was a mouse monoclonal IgG-negative
control antibody (Dako Corp., Carpinteria, CA) diluted to the
same working concentration as the anti-EPO antibody (5 �ig/ml
PBS with 1% FCS). To visualize the architecture ofthe vascular
endothelium, separate serial sections of the tumors were also
stained with anti-CD34 (a vascular endothelial marker) mono-
clonal antibody (Becton Dickinson, San Jose, CA), using the
same conditions as were used with the other antibodies.
Tissue Specimens. In this study, we examined all of the
cryopreserved, primary ovarian and endometrial carcinomas
(listed in Table 1) that were available in the University of
California, Irvine, Cancer Center Human Tumor Bank (Orange,
CA). All of these cases were well-characterized by routine light

1868 Eosinophil Peroxidase in Tumor Blood Vessels
Table 1 Immunohi stochemical s tudies of human endometrial and ovarian can cers with EPO antibody
Diagnosis
No. of
cases
Degree of EPO deposition Location of EPO deposits
Extensive Present Absent Stroma Vasculature Tumor
Endometrial cancer
Endometrial adenocarcinoma
Adenosquamous carcinoma
Ovarian cancer
Clear cell carcinoma
Endometroid carcinoma
Mucinous carcinoma
Serous carcinoma
Serous papillary adenocarcinoma
15
I
5
4
1
4
I
14 1 0
1 0 0
4 0 1
2 2 0
0 0 1
3 0 1
1 0 0
15 13
1 1
4 2
4 3
0 0
3 21 1
4
0
2
0
0
0
1
microscopy of H&E-strained sections and by other special stud-
ies as appropriate. Normal endometrium, ovary, and other tis-
sues were obtained from autopsies of five nontumor-bearing
subjects. This study was approved by the Institutional Human
Subjects Review Board at the University of California, Irvine.
Immunohistology and Cytochemistry. The tumor and
control tissues were frozen in Histo-Prep embedding medium
(Fisher Chemical, Fair Lawn, NJ), sectioned at 2-6 p.m thick-
ness on a microtome, air dried on a glass slide, and fixed in
acetone for 1 mm. The cryostat sections were then submitted for
two separate assays. The first assay was a cytochemical proce-
dure for directly and specifically detecting EPO (I 1) using a
chromogenic substrate for EPO (aminoethyl carbazole) and 0.01
M potassium cyanide (which inhibits myeloperoxidase but notEPO). For optimal sensitivity, this procedure needed to be
performed within 24 h after tissue sectioning. These slides were
counterstained with hematoxylin prior to mounting.
The immunohistochemical procedure for detecting EPO
and CD34 in tissue sections used an avidin-biotin glucose oxi-
dase detection procedure (Vector Laboratories, Burlingame,
CA) to detect bound primary antibody and was followed by a
nuclear fast red counterstain. This detection method was se-
lected to avoid interference by endogenous peroxidase activity
that was present within the tissues.
The negative controls for each case consisted of tissue
sections that were incubated without the primary antibody or
with the irrelevant mouse monoclonal antibody at the same
concentration as SF25.5. A positive control was also included
and consisted of a cytopreparation of purified human eosino-
phils incubated with the SF25.5 antibody.
Each stained slide was reviewed by two observers. For
purposes of tabulation, EPO activity in each slide was classified
as extensive (present in every X250 microscopic field), present
(detectable in the tissue but not present in every field), or absent
(none visible). In addition, the microanatomic location (stromal,
peripheral, within tumors, within blood vessels, and others) of
the EPO was noted in each case.
RESULTS
The results of our immunohistochemical staining with the
EOS monoclonal antibody are summarized in Table 1. A strik-
ing and consistent finding was the highly specific and obvious
localization of finely granular EPO deposits in a linear pattern,
apparently along and within the microvasculature within the
tumors (Fig. 1, a-d). The distribution of staining was luminal
and abluminal and was most intense at the edges of the tumors.
There was no apparent localization to regions of necrosis. A
similar linear distribution of staining was seen in parallel sec-
tions of the same tissues that were stained with the CD34
monoclonal antibody (Fig. le), but the CD34 staining was
homogeneous and not granular or abluminal. Adjacent unin-
volved normal tissue was available from four of our tumor-
bearing patients, and there was no apparent staining for EPO in
these specimens. There was also no tissue staining when a
negative control monoclonal antibody was substituted for the
EOS monoclonal antibody (Fig. lJ).
At the stromal interface between tumor and peripheral
connective tissue, there were extensive fibrillar deposits of EPO
(Fig. 2a) that were remarkably similar to those that we have
described previously in Hodgkin’s disease and in some human
breast cancers (I I, 13), and faint granular staining frequently
extended into the adjacent tumor cells. An identical wavy pat-
tern of staining in stroma at the tumor edges was also seen when
the tissues were stained with CD34 antibody (Fig. 2b), but the
adjacent tumor cells had no granular staining. Normal endome-
tria and ovarian tissues obtained from autopsies of five nontu-
mor-bearing subjects were devoid of similar EPO deposits when
stained identically with the EOS antibody, as were five speci-
mens of normal heart, liver, spleen, lung, kidney, skin, muscle,
and stomach tissues.
In routinely stained tissue sections, intact eosinophils could
be identified only in about one-half of our study cases and were
easily overlooked unless diligently sought. Eosinophils in our
study cases were most evident at the edges of the tumor, in the
connective tissue stroma adjacent to blood vessels (Fig. 3a), and
extending into the fibrovascular cores between nests of tumor
cells (Fig. 3b). This distribution closely paralleled the distribu-
tion seen with immunochemical staining for EPO. Cytochemical
staining of tumor sections for EPO also confirmed the specific
presence of EPO and eosinophils within the same locations of
the tumors (Fig. 3c).
DISCUSSION
Our in situ immunohistochemical and cytochemical study
has demonstrated that eosinophil degranulation and deposition
of EPO occur within and near the blood vessels and connective
tissues of a significant proportion of human ovarian and endo-
metrial cancers. This deposition of EPO occurred in a distribu-

T
;--: - --�
I , #��‘ � .-�
�-, t� ;r’�� �Irq�’�
1’ --�‘�
,I
�.�-
- -
,4�-;
. - - - - ‘4 - ... .4
-S �4�_� . --- � -.. �
,��. - � . � -
b
q� ‘� � : -
-t� .f-�
�., c..
‘.7,,,, � .�‘-� .: - � #{149}. ,
� � �
,�_ ‘i,- ,,.
- - 4-_:
f
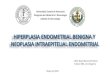
Fig. 1 Eosinophil peroxidase deposits in endometrial and ovarian cancers. In a-d. small blood vessels (marked by arrows) from four different tumorscontained luminal and abluminal blue granules, indicating the immunohistochemical detection of EPO. Similar deposition of EPO was generally
absent or decreased in the adjacent adenocarcinoma tumor cells (T) but usually extended into the fibrovascular stroma (S) between tumor cells (d).
A similar linear distribution ofpurple staining was observed when parallel sections were stained with a monoclonal antibody to CD34 (an endothelialcell marker), but the staining appeared to be exclusively luminal and homogeneous rather than granular (e). By contrast, incubation of the tumor
sections with a negative control monoclonal antibody produced no staining of tumor, blood vessels, or stroma (f). There was also no staining in normaltissues or in adjacent uninvolved tissues from four tumor-bearing subjects. All immunohistochemical photomicrographs are at an original
magnification of X250. Nuclear fast red counterstain and nitroblue tetrazolium substrate chromogen.
tion that was similar to the distribution of intact eosinophils seen blood vessels or tumor cells. This observation is significant
in routinely stained sections of one-half of the tumors that were because it implies that occult eosinophil degranulation is an
diligently examined. Thus, in view of the cytochemical and important and previously unsuspected part of the biological
histological confirmation, we conclude that eosinophils were the interaction between ovarian and endometrial cancers and the
source of the EPO rather than ectopic production of EPO by host.
Clinical Cancer Research 1869
I #{149}
�
k 4�
.- I
‘ -� eal’, .\ . � .:..‘#{149}::�::‘��� �_jc�c�i-
� � , .
. ‘Ii:. �,Jc.4-��-: - ‘�; � .- 4
-.�. , ., .�
::.�. � �.:‘ .
:�, . .‘� . ‘.- -‘ �“ #{149},, -‘ :. - � - .
‘!�i � . ., - ,- -- . ‘ �:
� .‘,tI.�,’ � . .c:�:�,�&:‘� : �
� .., . ...
� � .* �. � �.. � �

I
��.
�‘4 �
t.,
�. $;:-.
�- -
S
�( �� “ci’ � 4’�:k , b�
��,:4I�4 �. . I, � #{149} � . .
#{149}‘Jt1�’ .� ‘ - ., - - ‘:‘�� “-,� A. #{149}2� #{149}
.
4�.,._. 4b�
0“4
-.
S‘. C
. � b
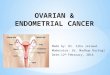
Fig. 3 Histological and cytochemical confirmation of eosinophils in en-
dometrial and ovarian cancers. When diligently sought in H&E-stained
sections, eosinophils (some of which are denoted by arrows) could be
identified in the fibrovascular stroma adjacent to and within blood vessels
(V), as seen in this case of endometrial carcinoma (a). The eosinophils were
readily recognizable by their intensely red, granular cytoplasm and charac-
teristic bi-lobed nuclei. Eosinophils (some of which are denoted by arrows)
could also be detected in a linear distribution in the fibrovascular regions
between some nests of tumor cells (b), duplicating the immunohistochem-
ical distribution of EPO. In a case of ovarian carcinoma, specific cytochem-
ical staining for EPO confirmed the presence of EPO and eosinophils (c),
which stained orange-brown when incubated with the chromogenic sub-
strate aminoethylcarbazole and potassium cyanide (an inhibitor of my-
eloperoxidase). a and b, H&E stain, X450. c, aminoethylcarbazole chro-mogenic substrate and hematoxylin counterstain, X 200.
practical implications for the management of women with ovar-
ian or endometrial cancer.
For example, we have previously shown (12) that iv.
1870 Eosinophil Peroxidase in Tumor Blood Vessels
4. A�
T #{149}-‘ �:: � -...�f- - -
:� ,�:.4j�-’. .
Fig. 2 EPO deposition at the edge of an ovarian adenocarcinoma. EPOwas detectable in wavy fibrillar deposits (a) at the interface between
tumor cells (1) and adjacent connective tissue stroma (S). Fainter
granules of EPO staining also extended into the adjacent tumor cells. A
similar wavy pattern of staining was observed when parallel sections
were stained with anti-CD34, but there was no granular staining within
the tumor itself (b).
. %
In specific, the strikingly localized deposition of EPO that
we observed in the connective tissues and microvasculature of
human gynecological cancers suggests the intriguing possibility
that the degranulating eosinophils somehow participated in the
neovascularization and extracellular matrix formation that were
present within and around these tumors. This possibility is
strengthened by the numerous previous reports that eosinophils
accumulate, activate, and degranulate in the connective tissues
and blood vessels during normal wound healing (14, 15), in
utero during the implantation period (16, 17), in hypervascular
nasal polyposis ( 1 8), and in association with the connective
tissue matrix of a variety of other cancers (19 -2 1 ). The neo-
vascularization and extracellular matrix formation that are ob-
served in all of these conditions have been attributed to trans-
forming growth factors a and �3, both of which are abundantly
produced by eosinophils (14, 15, 18-24).
The findings presented in this report also suggest that EPO
deposition from degranulating eosinophils is a new marker that
can specifically distinguish between microvessels in benign
tissues versus ovarian and endometrial cancers, a property that
is not shared by other tumor markers that have previously been
described in these cancers (25-27). Consequently, EPO depos-
ited within tumor blood vessels could eventually have important

Clinical Cancer Research 1871
administered, radiolabeled EOS antibody localized in a highly
specific manner to tumor sites in 18 patients with a variety of
lymphomas that contained EPO deposits that were similar to
those that we have now also described in ovarian and endome-
trial cancers. Therefore, intravascular EPO may be an ideal
target for a radioimmunoconjugate to be used in women with
ovarian or endometrial cancers. In addition, we have recently
demonstrated that EPO deposition in murine plasmacytomas
sensitized the tumors to killing in vivo by hydrogen peroxide-
generating, anionic Stealth liposomes (28). Based on the data in
this report, a similar experimental approach might also have
value for targeting and chemically killing the EPO-coated blood
vessels in human gynecological cancers that are resistant to
more conventional treatments.
Finally, it is of interest that eosinophils have sometimes
been thought to exert a beneficial antitumor effect in vivo (29).
In view of our findings, additional studies are now warranted to
determine if eosinophils can modulate the clinical course of
ovarian and endometrial cancer in humans.
REFERENCES
I . Burrows, F. J., and Thorpe, P. E. Vascular targeting: a new approachto the therapy of solid tumors. Pharmacol. Ther., 64: 155-174, 1994.
2. Thorpe, P. Antibody-directed targeting of tumor vasculature. Proc.
Am. Assoc. Cancer Res., 37: 668, 1996.
3. Contrino, J., Hair, G., Kreutzer, D. I., and Rides, F. R. in situ detectionof tissue factor in vascular endothelial cells: correlation with the malignant
phenotype of human breast tissue. Nat. Med., 2: 209-213, 1996.
4. Folkman, J. Tumor angiogenesis and tissue factor. Nat. Med., 2:
167-168, 1996.
5. Burrows, F. J., Derbyshire, E. J., Tazzari, P. L., Amlot, P., Gazdar.A. F., King, S. W., Letarte, M., Vitetta, E. S., and Thorpe, P. E.Up-regulation of endoglin on vascular endothelial cells in human solid
tumors: implications for diagnosis and therapy. Clin. Cancer Res., I:
1623-1634, 1995.
6. Rettig, W. J., Garinchesa, P., Healy, J. H., Su, S. L., Jaffe, E. A., and
Old, L. J. Identification of endosialin, a cell surface glycoprotein ofvascular endothelial cells in human cancer. Proc. Natl. Acad. Sci. USA,
89: 10832-10836, 1992.
7. Wang, J. M., Kumar, S., Pye, D., Vanagthoven, A. J., Krupinski, J.,
Hunter, R. D. A monoclonal antibody detects heterogeneity in vascular
endothelium of tumours and normal tissues. Int. J. Cancer, 54: 363-370,
1993.
8. Carnemolla, B., Balza, E., Siri, A., Zardi, L., Nicrotra, M. R., Bigotti,
A., and Natali, P. G. A tumor-associated fibronectin isoform generatedby alternative splicing of messenger RNA precursors. J. Cell Biol., 108:
1138-1148, 1989.
9. Plate, K. H., Breier, G., Welch, H. A., and Risau, W. Vascularendothelial growth factor is a potential tumour angiogenesis factor in
human gliomas in vivo. Nature (Lond.), 359: 845-848, 1992.
10. Dvorak. H. J., Sioussat, T. M., Brown, L. F., Berse, B., Nagy, J. A.,
Sotrel, A., and Manseau, E. J. Distribution of vascular permeabilityfactor (vascular endothelial growth factor) in tumors: concentration in
tumor blood vessels. J. Exp. Med., 174: 1275-1278, 1991.
1 1 . Samoszuk, M. K., Lukes, R. J., and Nathwani, B. Extensive depo-sition of eosinophil peroxidase in Hodgkin’s and non-Hodgkin’s lym-
phomas. Am. J. Pathol., 125: 426-429, 1986.
12. Samoszuk, M., Anderson, A. L., Ramzi, E., Wang, F., Braunstein,
P., Majmundar, H., and Slater, L. Radioimmunodetection of Hodgkin’s
disease and non-Hodgkin’s lymphomas with monoclonal antibody to
eosinophil peroxidase. J. Nucl. Med., 34: 1246-1253, 1993.
13. Samoszuk, M., Nguyen, V., Gluzman, I., and Pham, J. H. Occult
deposition of eosinophil peroxidase in a subset of human breast carci-
nomas. Am. J. Pathol., 148: 701-706, 1996.
14. Wong, D. T. Sequential expression of transforming growth factors
a and 13 1 by eosinophils during cutaneous wound healing in the
hamster. Am. J. Pathol., 143: 130-142, 1993.
15. Todd, R. The eosinophil as a cellular source of transforming growth
factor a in healing cutaneous wounds. Am. J. Pathol., 138: 1307-13 13,
1991.
16. Lea. R. G., Stewart, F., Allen, W. R., Ohno, I., and Clark, D. A.
Accumulation of chromotrope 2R positive cells in equine endometrium
during early pregnancy and expression of transforming growth factor-
�32. J. Reprod. Fertil., 103: 339-347, 1995.
17. McMaster, M. T., Newton, R. C., Dey, S. K., and Andrews, G. K.
Activation and distribution of inflammatory cells in mouse uterus during
the preimplantation period. J. Immunol., 148: 1699-1705, 1992.
18. Elovic, A., Wong, D. T., Weller, P. F., Matossian, K., and Galli,
S. J. Expression of transforming growth factors-a and �3 I messengerRNA and product by eosinophils in nasal polyps. J. Allergy Clin.Immunol., 93: 864-869, 1994.
19. Kadin, M., Butmarc, J., Elovic, A.. and Wong, D. Eosinophils are
the major source of transforming growth factor43 1 in nodular sclerosing
Hodgkin’s disease. Am. J. Pathol., 142: 1 1-16, 1993.
20. Ghiabi, M., Gallagher, G. T., and Wong, D. T. Eosinophils, tissue
eosinophilia, and eosinophil-derived transforming growth factor a in
hamster oral carcinogenesis. Cancer Res., 52: 389-393, 1992.
21. Wong, D. T. TGF-a and oral carcinogenesis. Eur. J. Cancer Part B,
Oral Oncol., 29B: 3-7, 1993.
22. Wong, D. 1. Eosinophils from patients with blood eosinophilia
express transforming growth factor �3l. Blood, 78: 2702-2707, 1991.
23. Ohno, I. Eosinophils in chronically inflamed human upper airway
tissue express transforming growth factor �3l gene. J. Clin. Invest., 89:
1662-1668, 1992.
24. Wong, D. T. Human eosinophils express transforming growth factor
a. J. Exp. Med., 172: 673-681, 1990.
25. Sonoda, K., Nakashima, M., Kaku, T., Kamura T., Nakano, H.,and Watanabe, T. A novel tumor-associated antigen expressed in
human uterine and ovarian carcinomas. Cancer (Phila.), 77: 1501-
1509, 1996.
26. Saffari, B, Jones, L. A., El-Naggar, A., Felix, J. C., George, J., and
Press, M. F. Amplification and overexpression of HER-2/neu (c-erbB2)
in endometrial cancers: correlation with overall survival. Cancer Res.,
55. 5693-5698, 1995.
27. Quadri, S. M., Malik, A. B., Tang, X., Patenia, R., Freedman, R. S.,
and Vriesendorp, H. M. Preclinical analysis of intraperitoneal adminis-
tration of � � ‘In-labeled human tumor reactive monoclonal 1gM AC6C3-
2B12. Cancer Res., 55 (Suppl.): 5736s-5742s, 1995.
28. Samoszuk, M.. Wimley, W. C., and Nguyen, V. Eradication of
interleukin-5 transfected J558L plasmacytoma in mice by hydrogen
peroxide-generating Stealth liposomes. Cancer Res. , 56: 87-90.
1996.
29. Tepper, R. I., Coffman, R. L., and Leder, P. An eosinophil-depen-
dent mechanism for the antitumor effect of interleukin-4. Science
(Washington DC), 257: 548-551, 1992.