Embed Size (px)
Citation preview

New Insulin Possibilities in Diabetes Care
Anders Carlson, MD
Medical Director, International Diabetes Center
Director HealthPartners Diabetes Program
Assistant Professor, University of Minnesota Medical School

Disclosures
• Dr. Carlson disclosures:
– Advisory Board/Consultant: Sanofi, Merck
– Speaker’s Bureau: Dexcom
– Research Support: Medtronic, Novo Nordisk, Johnson & Johnson, Hygieia, Sanofi

Objectives
• Review available new and concentrated insulins • Clinical perspective of the use of concentrated insulin • Summary of DEVOTE trial • New and future insulin therapeutic options and technologies

Sulfonylurea (Glimepiride or GlipizideXL)
Risk of hypoglycemia Weight gain
Rapid glucose lowering Long history of use
Lowest cost
GLP-1 Agonist (Albiglutide, Dulaglutide, Exenatide, Exenatide XR,
Liraglutide, or Lixisenatide) No hypoglycemia; weight loss GI side effects – nausea; pen; Higher cost; liraglutide ↓ CV events in pts. with CVD
Titrate to clinically effective dose Advance if not at target within 3 months
Two-Drug Therapy (Metformin plus…)
© 2017 International Diabetes Center at Park Nicollet internationaldiabetescenter.com 1-888-637-2675
Advance if not at target within 3 months Titrate to clinically effective dose
Multi-Drug Therapy (Maintain metformin and add…)
Self-Management • Refer for diabetes education
• Monitor BG, titrate medications
Medical Nutrition and Activity Therapy • Refer to Registered Dietitian • Walk 30 min., 5 days/wk, plus some resistance training
Glycemic Targets Premeal 70-130 mg/dL (Individualized) Postmeal <180 mg/dL
A1C <7% (Individualized) Minimize Hypoglycemia
Emotional Health • Psychosocial support / motivation • Assess for anxiety and/or depression
Advance/initiate drug treatment if not at target
Metformin If not tolerated or if contraindicated select initial
therapy from TWO-DRUG THERAPY below
At Presentation and Ongoing
A1C 6.5-8.9%
A1C 9-11.9%
Premixed Insulin*
Insulin Therapy
A1C ≥12% and/or
BG ≥350 mg/dL
(Insulin recommended if patient clinically
unstable or need for rapid glucose control)
IDC Type 2 Diabetes Glycemic Control Algorithm
Advance if not at target within 3 months Titrate to clinically effective dose
DPP-4 Inhibitor
No hypoglycemia; weight neutral Well tolerated Higher cost CV neutral; saxagliptin ↑ hosp. for HF
(Alogliptin, Linagliptin Saxagliptin or Sitagliptin)
SGLT2 Inhibitor (Canagliflozin, Dapagliflozin, or
Empagliflozin) No hypoglycemia; weight loss UTI, Mycotic Infections, Hypotension, DKA (rare) Higher cost; empagliflozin
↓CV death in pts. with CVD
Background Insulin + Mealtime Insulin* (1, 2 or All Meals) or
Background Insulin + GLP-1 Agonist
*Recommend adding or maintaining metformin; discontinue sulfonylurea; discontinue or reduce dose of thiazolidinedione; consider maintaining DPP-4 inhibitor, GLP-1 agonist, or SGLT2 inhibitor if patient experienced positive response to medication
or
Background Insulin (Basaglar, Degludec, Detemir, or Glargine
[U100 and U300]) Lowers FPG; risk of hypoglycemia and weight gain; consider stopping SU; stop or reduce TZD; use NPH if cost is an issue
SGLT2 Inhibitor Lowers FPG and PPG No added risk of hypoglycemia Weight loss May be used off label with GLP-1 Agonist
GLP-1 Agonist Lowers FPG and PPG No added risk of hypoglycemia Weight loss Stop DPP-4 Inhibitor May be used off label with SGLT2 Inhibitor

Case
• 66 year old male, with type 2 diabetes for over 20 years
• BMI 49, has met with RD/CDE but refuses follow up
• Eats several large meals/day, and requires very high doses of insulin
• Currently, on glargine (lantus) 80 units BID and lispro (Humalog) 30 units TID with meals, plus metformin
• No known CV disease, but has hyperlipidemia (high LDL and TGs)
• Renal function normal
• BGs high most of the day, in the 150-250+ mg/dl (8.3-13.9 mmol/l) range, A1c usually 8.5-9.5%

ARS Question: What is the next best step for this patient to control his diabetes?
A. Strongly encourage him to go back to diabetes education
B. Increase basal insulin glargine to 100 units BID
C. Start DDP4 sitaglipitin (Januvia) 100 mg daily
D. Change glargine and lispro over to U-500R insulin, twice daily before meals
E. Change to a V-Go insulin pump

Concentrated Insulins
• Historically, insulin has been U-100
– 100 units per ml
• Types of concentrated insulin:
–U-500 Regular
–Glargine U-300 (Toujeo)
–Degludec U-200 (Tresiba)
–Humalog U-200 (the only rapid acting)

Candidates for concentrated insulin
Lane et al. Endocr Pract 2009;15(1):71-9.
• Type 2 DM with obesity and/or severe insulin resistance
• Patients with insulin requirements > 200 units per day (reduces volume and/or number of shots per day)
• Post-operative or post-transplant state
• High-dose glucocorticoids
• Insulin resistant syndromes
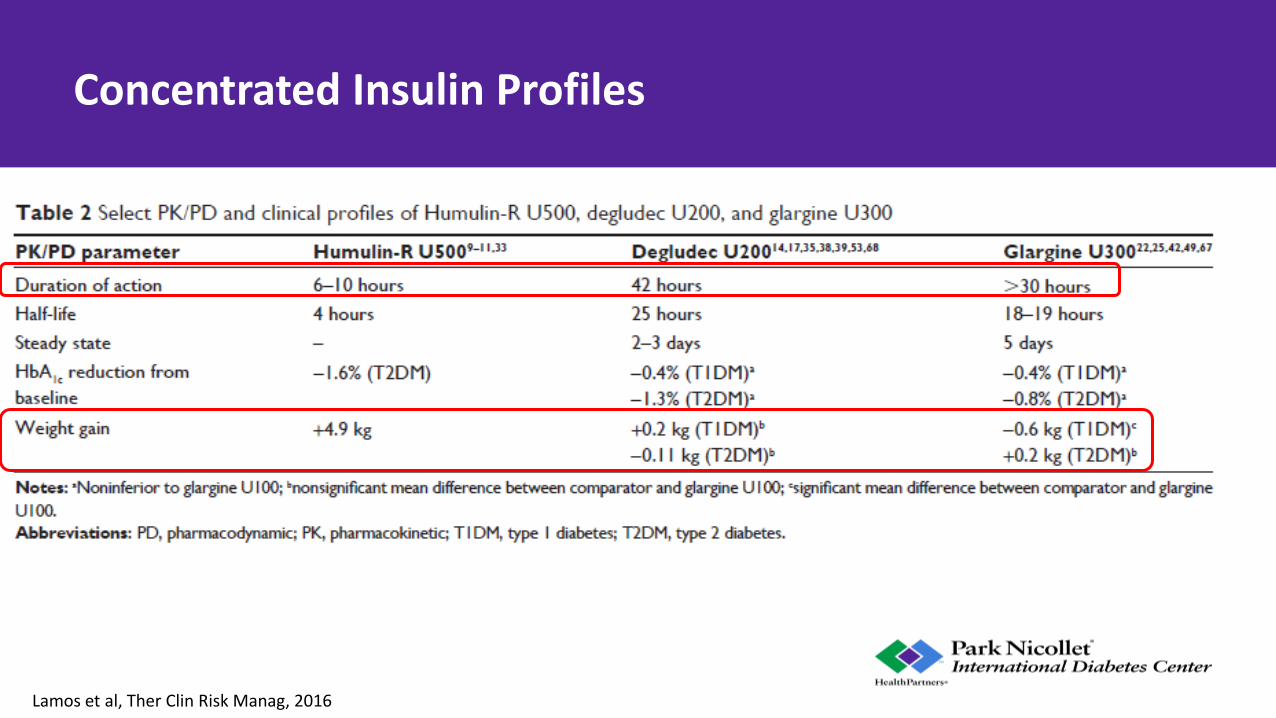
Concentrated Insulin Profiles
Lamos et al, Ther Clin Risk Manag, 2016

U-500 insulin
• U-500 = 5 times concentrated (500 units/ml)
• Requires clear education for the patient
• In vial form Need an insulin syringe (U-100 or U-500 syringe) – Prescription should be very clear to avoid confusion, which is a major limitation of U-
500
– For example, a prescription should read: U-500 concentrated insulin, Inject 100 units (drawn to 20 units or 0.2 ml on a U-100 syringe) TID with meals
• It is now available as a pre-calibrated pen device – So, a 50 unit dose will be dispensed as 0.1 mL, 100 units is 0.2 ml, etc.

Amparo de la Peña et al. Dia Care 2011;34:2496-2501
U-500 profile
• U-500 profile is similar to regular insulin, with a longer “tail”
• Usually dosed 2-3 times/day with meals
• Acts as both mealtime and basal insulin
Regular
U-500

Dosing considerations with U-500 insulin
• U-500 insulin: – If A1c ≤8% or average glucose <183 mg/dl (10 mmol/l), use 80% TDD
– Otherwise use 100% of TDD
– Dose 60% pre-breakfast, 40% pre-dinner
– Alternatively, can do 40% breakfast, 30% lunch and 30% dinner
– Titrate weekly (or at your discretion)
– 2 pens per box
Hood et al, Endo Prac, 2015
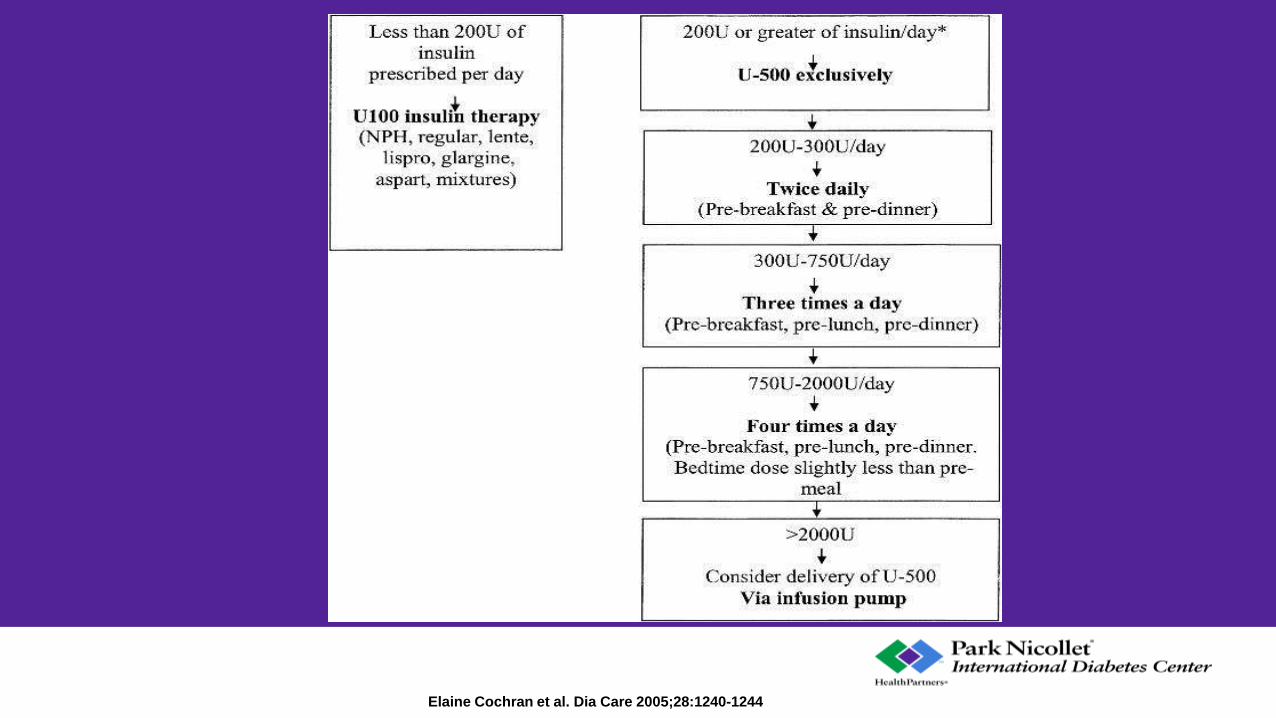
Elaine Cochran et al. Dia Care 2005;28:1240-1244
NOT FOR PROMOTIONAL USE
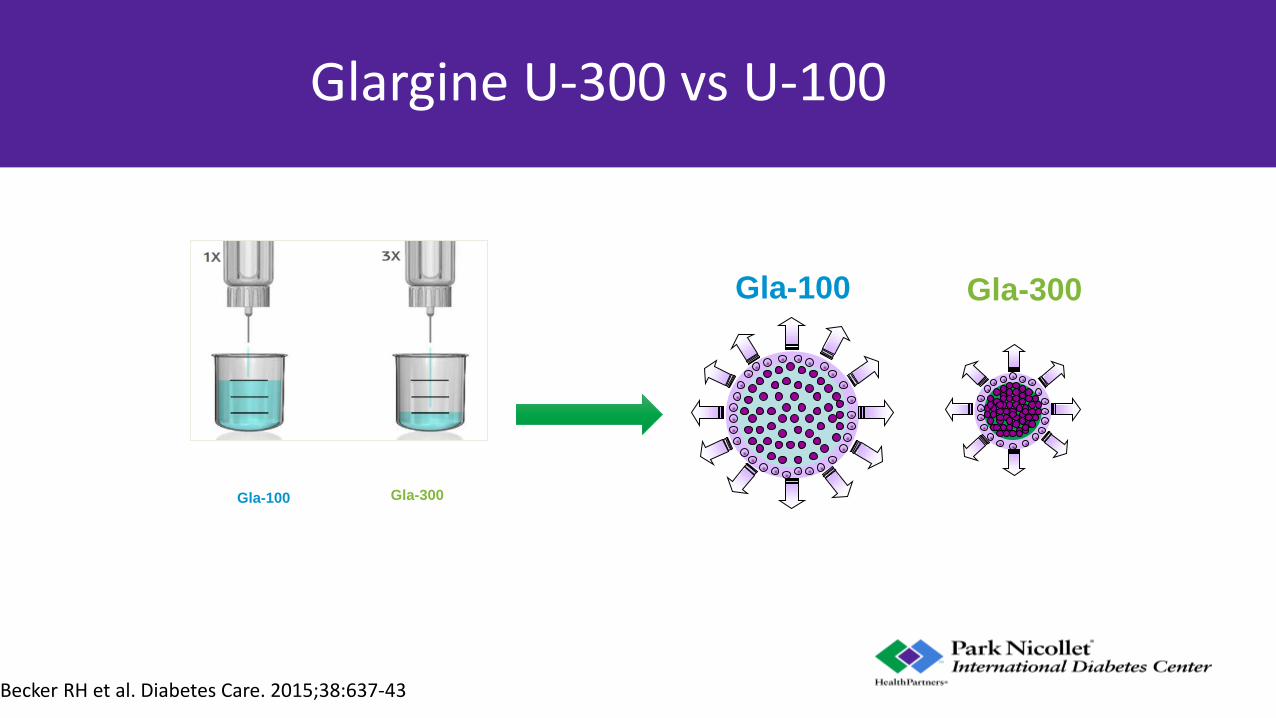
Glargine U-300 vs U-100
Becker RH et al. Diabetes Care. 2015;38:637-43
14
Gla-300 Gla-100
Gla-300 Gla-100
NOT FOR PROMOTIONAL USE
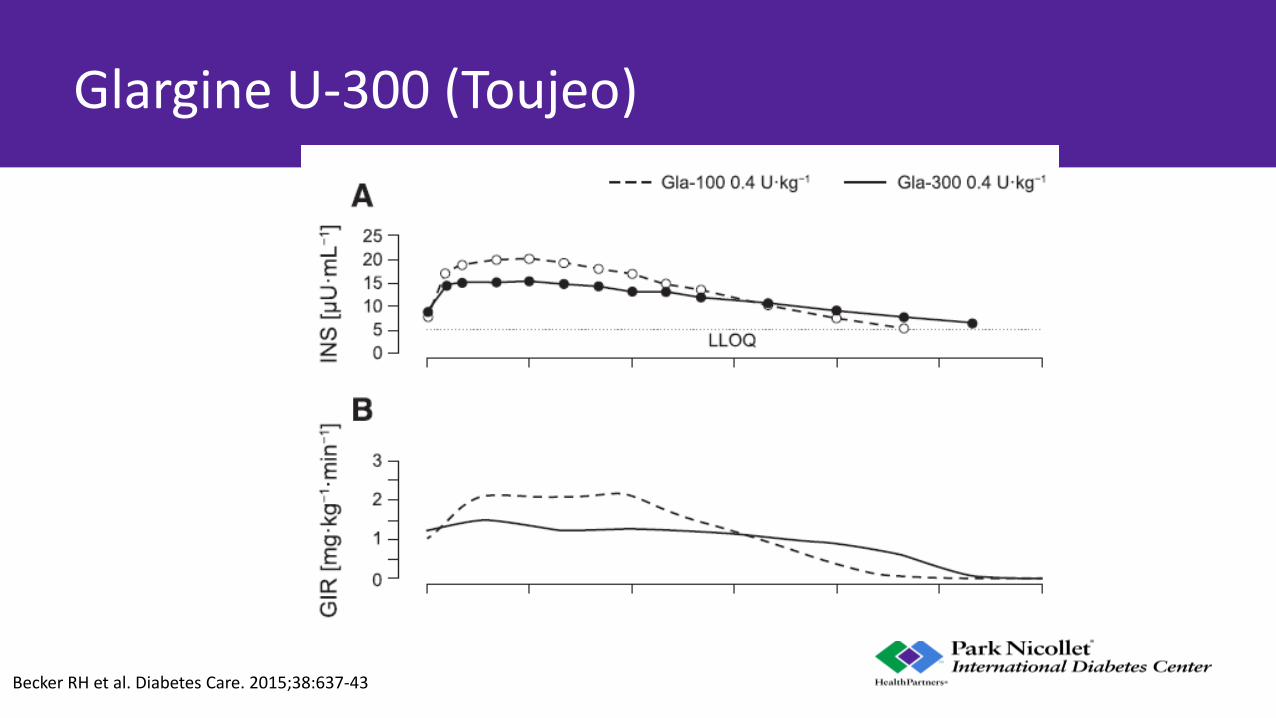
Glargine U-300 (Toujeo)
Becker RH et al. Diabetes Care. 2015;38:637-43

NOT FOR PROMOTIONAL USE
Gla-300 Glargine: EDITION trials
1. Riddle MC et al. Diabetes Care. 2014;37:2755-62; 2. Yki-Järvinen H et al. Diabetes Care. 2014;37:3235-43; 3. Bolli GB et al. Diabetes Obes Metab. 2015;17:386-94; 4. Terauchi Y et al. Diabetes Obes Metab. 2016;18:366-74 (main article and Supplementary Table 2); 5. Home PD et al. Diabetes Care. 2015;38:2217-25;6. Data on file, EDITION 4 CSR (6 months) pg 88; 7. Matsuhisa M et al. Diabetes Obes Metab. 2016;18:375-83 (main article and Supplementary Table 1)
-0.83
-0.57
-1.42
-0.45 -0.40 -0.30
-0.83
-0.56
-1.46
-0.55 -0.44 -0.43
-1.5
-1.0
-0.5
0.0
LSM
Hb
A1
C c
han
ge f
rom
b
asel
ine,
%
EDITION 3 EDITION JP 2 EDITION 1 EDITION 2 EDITION 4 EDITION JP
0.00% (-0.11 to 0.11)
-0.01% (-0.14 to 0.12)
0.04% (-0.09 to 0.17)
0.10% (-0.08 to 0.27)
0.04% (-0.10 to 0.19)
0.13% (-0.03 to 0.29)
16
Primary endpoint: non-inferiority in HbA1C change with Gla-300 vs Gla-100 at Month 6
Gla-100
Gla-300
T2DM
T1DM
LSM difference (95%CI)

Rate of nocturnal (00:00–05:59 h) confirmed (≤70 mg/dL *≤3.9 mmol/L]) or severe hypoglycemia in T2DM studies at Month 6
• 1. Adapted from Riddle MC et al. Diabetes Care. 2014;37:2755-62;
• 2. Yki-Järvinen H et al. Diabetes Care. 2014;37:3235-43;
• 3. Bolli GB et al. Diabetes Obes Metab 2015;17:386-394 (main article and Supplementary Figure 3);
• 4. Terauchi Y et al. Diabetes Obes Metab. 2016;18:366-74
a

Dosing considerations with long-acting U-300 glargine insulin
• U-300 glargine (Toujeo) in some cases need dose increase of 10-20% above the previous basal insulin dose
– Not always observed in clinical practice
– If converting to U-300 glargine and patient is tightly controlled, then may not need a dose increase
– If converting from U-300 glargine to U-100 glargine, and patient tightly controlled, then you may want to lower dose 10-20%
• Can dose +/- 3 hours from dosing time
• 3 pens per box

Degludec (Tresiba) U-100 or U-200
Tambascia and Eliaschewitz, Diab Met Synd, 2015

Degludec PK/PD
• U100 and U200 degludec appear similar
• Fairly consistent AUC over 24 hour period

BEGIN Program
• Metanalysis of the 7 BEGIN trials (3a)
• Non-inferior HbA1c (treat to target)
• Greater reduction in FPG
• Reduced risk for nocturnal hypoglycemia
Russell Jones et al. Nutrition, Metabolism & Cardiovascular Diseases 2015;25:898-905

Degludec vs. U-300 glargine?
• Single center, randomized, blinded crossover study in 48 pts with T1D
• Euglycemic clamps done on day 8
Bailey et al, abstract presented at ADA 77th Sci Sessions, June 10 2017, 985-P


DEVOTE trial
• Randomized, double blinded, active controlled
• Treat-to-target
• Event driven
• Primary outcome: cardiovascular safety of degludec compared to glargine U100
• Secondary outcome: efficacy and safety of degludec in patients with type 2 diabetes at high risk of cardiovascular events
June 12, 2017

DEVOTE: trial design
• 7637 patients randomized across 20 countries
• Interim analysis after 150 MACE events accrued
• End of treatment = 633 MACE events accrued
• 30 day follow up
• Inclusion: T2D, on ≥1 oral/injectable medication
• HbA1c ≥7.0% or <7% plus basal insulin ≥20 units/day
• High CVD risk: cardiovascular or chronic kidney disease and aged ≥50 or risk factors for cardiovascular disease and aged ≥60
Avg age = 65 years 62% male HbA1c 8.4% 85% established CV or CKD and age ≥50

Marso SP et al. N Engl J Med 2017. DOI: 10.1056/NEJMoa1615692
Kaplan–Meier Analysis of the Composite Primary Outcome.

Time to first 3-point MACE sensitivity analyses

• Non-inferiority of insulin degludec versus glargine U100 was confirmed for time to first event of 3-point MACE
– The estimated hazard ratio was 0.91 [95% CI: 0.78; 1.06]
• The estimated hazard ratio was consistent across:
– 4-point MACE
– Individual components of MACE: non-fatal stroke, non-fatal MI, CV death and unstable angina requiring hospitalization
– All-cause death
Summary of the cardiovascular outcomes
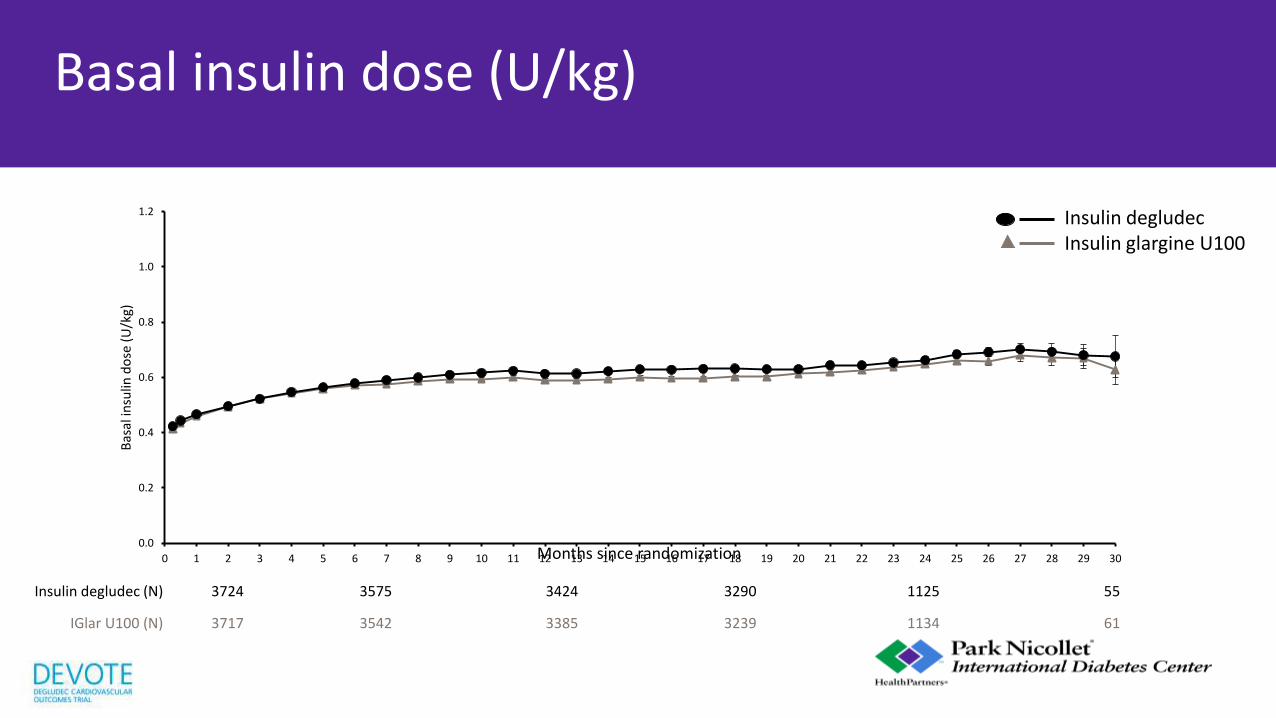
Basal insulin dose (U/kg)
0.0
0.2
0.4
0.6
0.8
1.0
1.2
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
Bas
al in
sulin
do
se (
U/k
g)
Insulin degludec (N) 3724 3575 3424 3290 1125 55
IGlar U100 (N) 3717 3542 3385 3239 1134 61
Months since randomization
Insulin degludec Insulin glargine U100

Similar mean HbA1c
-0.86 -0.84
-1.0
-0.5
0.0
%
Observed mean change from baseline at month 24
Insulin degludec IGlar U100
Post hoc ETD: 0.01% [95% CI: -0.05; 0.07]
6.5
7.0
7.5
8.0
8.5
9.0
0 3 6 9 12 15 18 21 24 27 30
Hb
A1
c (%
)
75
69
64
59
53
0
Hb
A1
c (mm
ol/m
ol)
Insulin degludec (N) 3774 3656 3608 3535 3525 2458 3344
IGlar U100 (N) 3776 3640 3562 3516 3500 2424 3277
0.0
Months since randomization
ET
Insulin degludec IGlar U100
7.55%
7.50%

Incidence of severe hypoglycemia
Full analysis set; The incidence of events is analyzed using a logistic regression model adjusted for treatment group
Time from randomization (months)
Insulin degludec (N=3818) IGlar U100 (N=3819)
N % N %
EAC-confirmed episodes 187 4.9 252 6.6
0
2
4
6
8
10
0 3 6 9 12 15 18 21 24 27 30
Pati
ents
wit
h a
n e
ven
t (%
)
Odds ratio: 0.73 [0.60; 0.89]95% CI
p<0.001
IGlar U100 Insulin degludec

Rates of nocturnal severe hypoglycemia
0
1
2
3
4
5
0 3 6 9 12 15 18 21 24 27 30
Mea
n n
um
ber
of
even
ts/1
00
PYO
Time from randomization (months)
Insulin degludec (N=3818) IGlar U100 (N=3819) N % E R N % E R
EAC-confirmed episodes 37 1.0 48 0.64 73 1.9 106 1.39
Rate ratio: 0.47 [0.31; 0.73]95% CI
p<0.001
IGlar U100 Insulin degludec

• Glycemic control (insulin degludec vs. IGlar U100):
– End of treatment mean HbA1c values 7.55% vs. 7.50%
– Change in FPG levels -39.9 mg/dL vs. -34.9 mg/dL
• 27% fewer patients experienced severe hypoglycemia with insulin degludec
• 40% rate reduction of severe hypoglycemia
• 53% rate reduction of nocturnal severe hypoglycemia
Summary of glycemic control and severe hypoglycemia
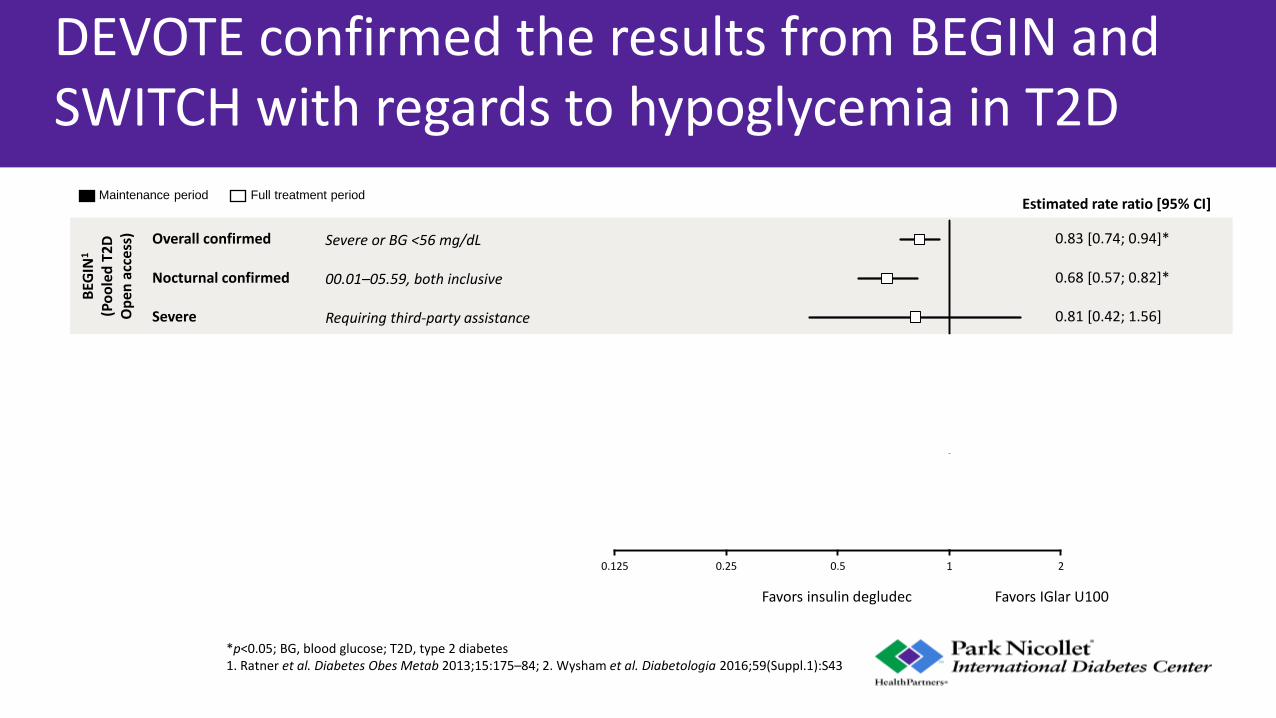
DEVOTE confirmed the results from BEGIN and SWITCH with regards to hypoglycemia in T2D
*p<0.05; BG, blood glucose; T2D, type 2 diabetes 1. Ratner et al. Diabetes Obes Metab 2013;15:175–84; 2. Wysham et al. Diabetologia 2016;59(Suppl.1):S43
Maintenance period Full treatment period
0.68 [0.57; 0.82]*
Estimated rate ratio [95% CI]
0.83 [0.74; 0.94]* Overall confirmed
Nocturnal confirmed
0.81 [0.42; 1.56] Severe
0.58 [0.46; 0.74]*
0.60 [0.48; 0.76]*
0.47 [0.31; 0.73]*
0.54 [0.21; 1.42]
0.70 [0.61; 0.80]* Overall confirmed
Nocturnal confirmed
Severe
SWIT
CH
22
(Do
ub
le
blin
d)
DEV
OTE
(D
ou
ble
b
lind
)
Severe
Nocturnal severe
0.125 0.25 0.5 1 2
Favors IGlar U100 Favors insulin degludec
BEG
IN1
(Po
ole
d T
2D
O
pen
acc
ess)
Severe or BG <56 mg/dL
00.01–05.59, both inclusive
Requiring third-party assistance
Severe or BG <56 mg/dL with symptoms
Severe or BG <56 mg/dL with symptoms, 00.01–05.59, both inclusive
Requiring third-party assistance and adjudicated
Requiring third-party assistance and adjudicated
00.01–05.59, both inclusive, requiring third-party assistance and adjudicated

Total mortality
Cardiovascular mortality
Major cardiovascular event
1.8 [1.5; 2.2] 0.000
2.2 [2.0; 2.4] 0.000
2.3 [1.1; 5.0] 0.026
Hazard ratio [95% CI] p-value
253,390
11,011
61,434
1.0 0.1 10.0
Hazard ratio
Systematic review: association of hypoglycemia with outcomes
Adapted from Yeh et al. Acta Diabetol 2016;53:377–92
Number of patients
Dosing considerations with long-acting degludec insulin
• Dose 1:1 from previous basal dose
• Recommended titration is every 3-4 days
• Even though 42 hr duration, recommended dosing is daily
• Can have flexible dosing (dosing within 8 hours of previous dose not recommended)
• U-200 is 3 pens/box, U-100 is 5 pens/box
• FDA also approved degludec-aspart pre-mixed pen (Ryzodeg) but currently not available in the US
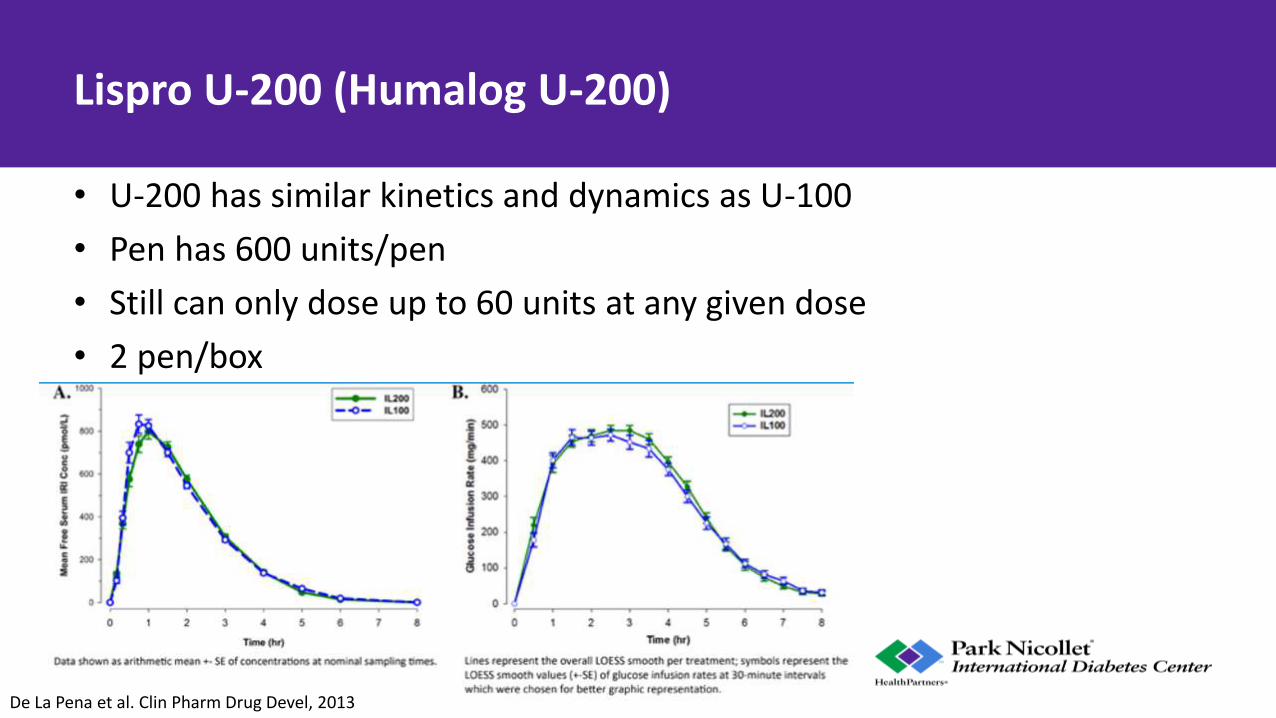
Lispro U-200 (Humalog U-200)
• U-200 has similar kinetics and dynamics as U-100
• Pen has 600 units/pen
• Still can only dose up to 60 units at any given dose
• 2 pen/box
De La Pena et al. Clin Pharm Drug Devel, 2013
Hypoglycemia
• U-300 glargine: – In T1D: -31% nocturnal hypoglycemia
– In T2D: -16% nocturnal hypoglycemia (also less severe hypo at any time of day)
• U-200 degludec metanalysis data: – In T1D: -25% nocturnal hypoglycemia
– In T2D: -32% nocturnal hypoglycemia
• U-500: – Limited studies, no clear data
– Intuitively, U-500 is risk for hypoglycemia
Lamos et al, Ther Clin Risk Manag, 2016
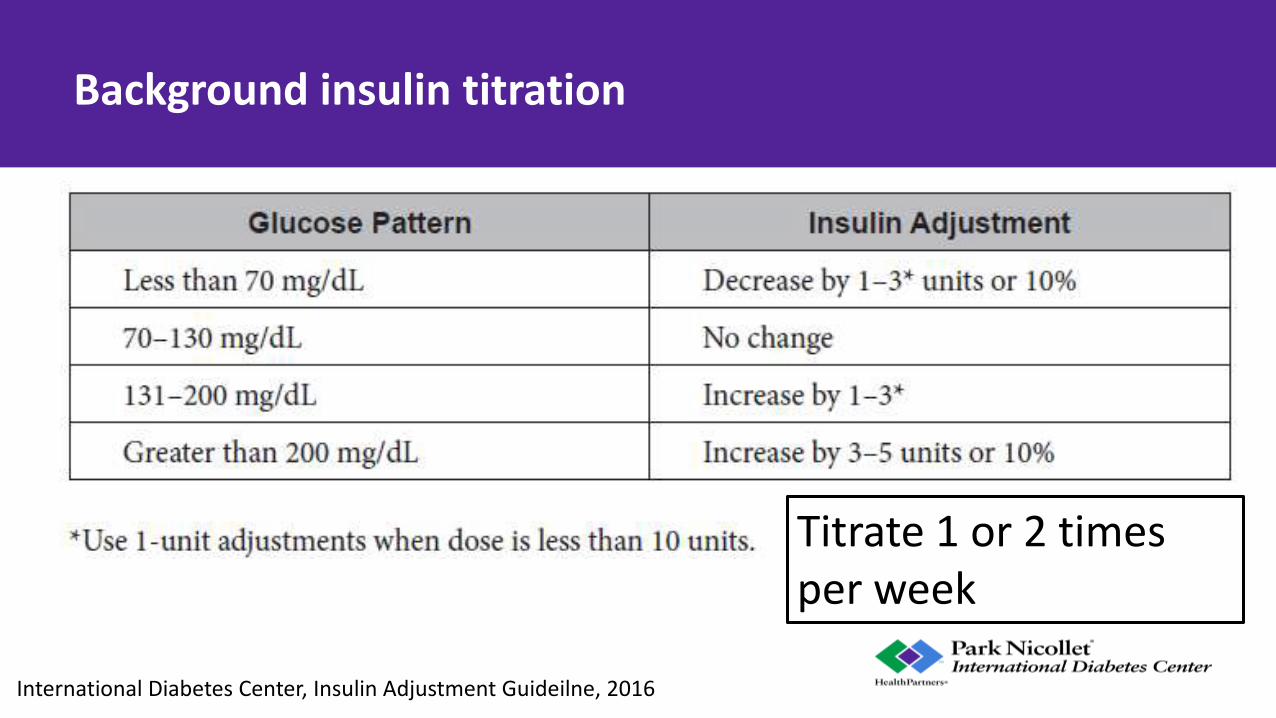
Background insulin titration
Titrate 1 or 2 times per week
International Diabetes Center, Insulin Adjustment Guideilne, 2016

What about “biosimilar” insulin?
• They are ”highly” similar to an already FDA-approved biological product
• Must have the same mechanism of action, route of administration, dosage form, and strength as the reference product
• They are not “generic”
• Biosimilars may have allowable differences because they are made from living organisms
• Biosimilars have no clinically meaningful differences in safety, purity, and potency

Basaglar (Eli Lilly) proved it was sufficiently similar to Lantus (Sanofi) to rely on past data about Lantus through new FDA expedited approval pathway Also had to do their own trials using Basaglar to show safety and efficacy

What about “biosimilar” insulin?
Heinemann and Hompesch, J Diab Sci Tech, 2014

Dosing Basaglar
• 1 to 1 conversion: It is a new brand name glargine, not generic
• Patients should monitor glucose more closely as they start
• Many clinics have standing orders to replace without new prescription
• May be an issue for patients only using glargine vials (Basaglar does not come in vials, only pens)

“Biosimilar” Lispro
• “Follow-on” Lispro
• 27 pts with T1D
• Insulin via pump
• 8 week cross-over design
• No difference in adverse effects, reactions, or hypoglycemia
Thrasher et al, ADA 77th Sci Sessions, June 2017, San Diego, CA, 1042-P
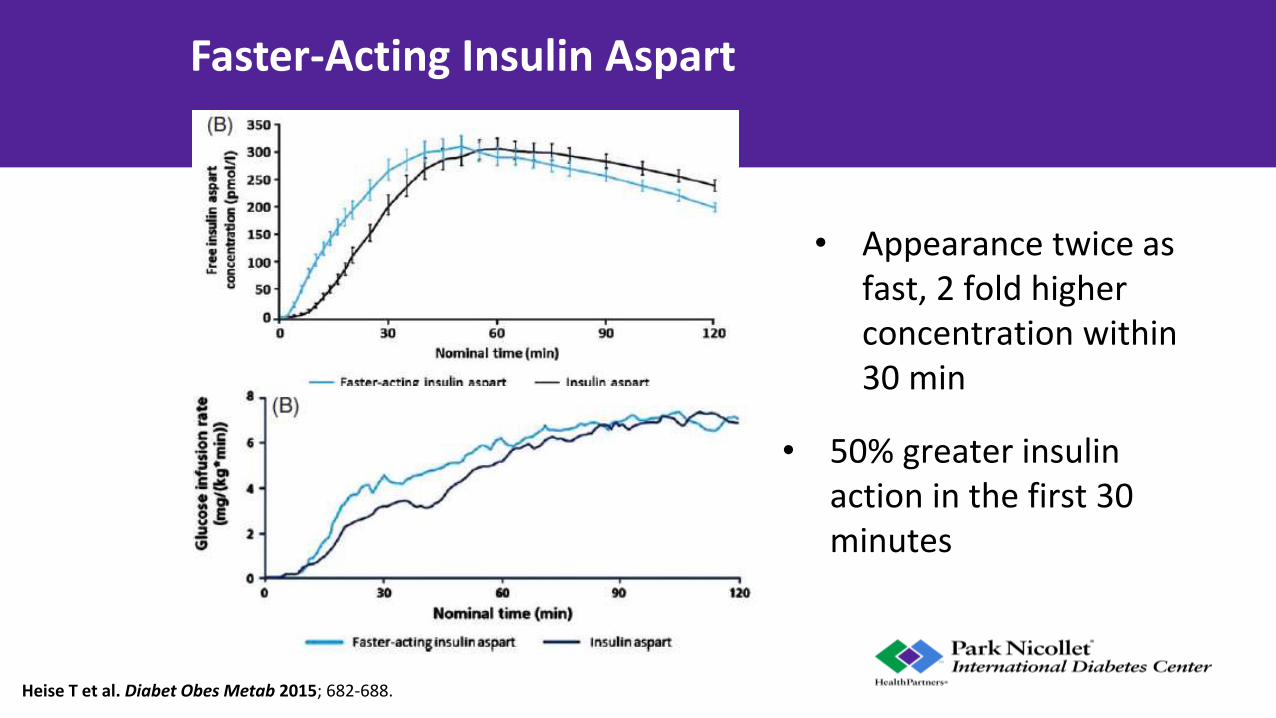
Faster-Acting Insulin Aspart
• 50% greater insulin action in the first 30 minutes
• Appearance twice as fast, 2 fold higher concentration within 30 min
Heise T et al. Diabet Obes Metab 2015; 682-688.

Biochaperone Lispro: PK/PD
Onset of action: Biochaperone: 23 min (30.1) Lispro: 34 (44.5) P = 0.0003
v

Biochaperone Lispro in T2D
• 51 pts on MDI
• ↓20% in post-prandial glucose (avg)
• “faster-in, faster-out”
Heise et al, ADA 77th Sci Sessions, San Diego, CA, 2017, P-994
a

Insulin Lispro Containing Citrate and Treprostinil: Faster Absorption and Improved Postprandial Glucose Excursions vs. Humalog in Patients with T1DM
• 2.2 fold increase in insulin exposure in the first 30 min
• Reduced post-prandial excursion 44% compared to Humalog
• No difference in hypoglycemia
Kazda et al. ADA 77th Sci Sessions, San Diego, CA, 2017. 959-P

Inhaled insulin

U.S. Food and Drug Administration. (2014, June). Afrezza: Full prescribing information (Report No. 3533688).
Retrieved from https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/022472lbl.pdf

The future: Glucose Responsive Insulin (“Smart Insulin”)
Yu et al, PNAS, 2015
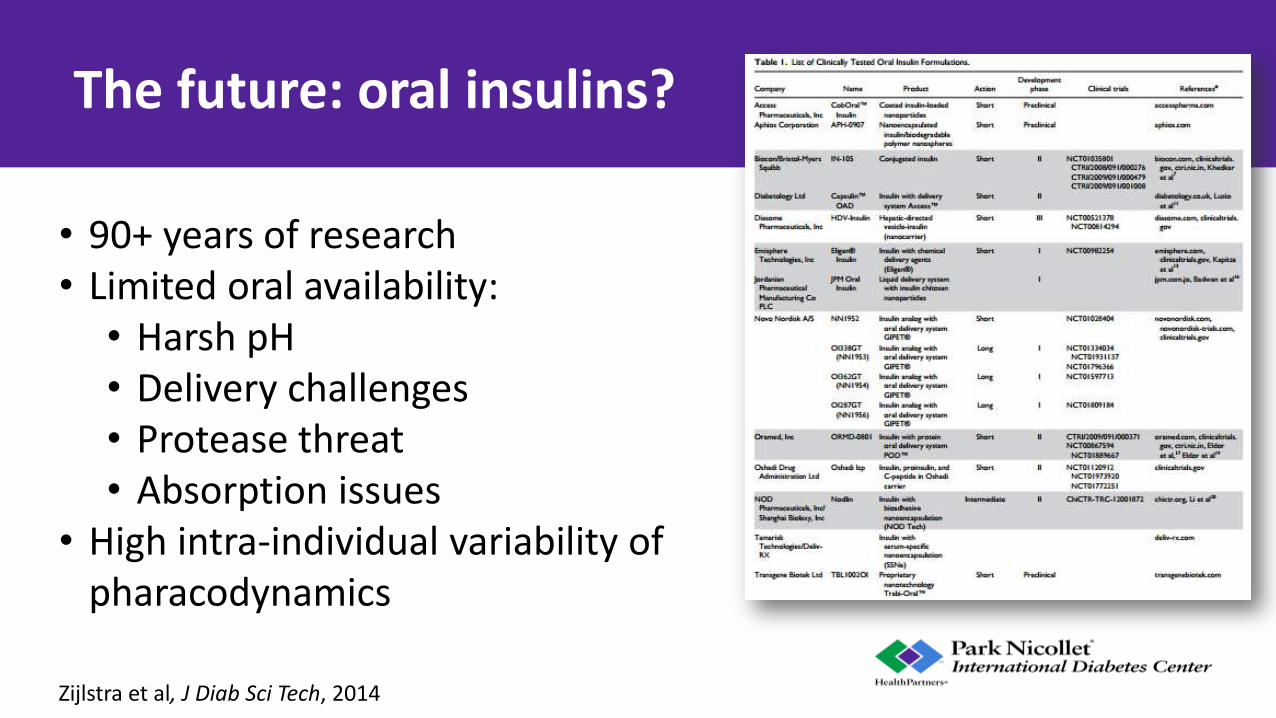
The future: oral insulins?
• 90+ years of research • Limited oral availability:
• Harsh pH • Delivery challenges • Protease threat • Absorption issues
• High intra-individual variability of pharacodynamics
Zijlstra et al, J Diab Sci Tech, 2014

Oral Insulins: recent clinical trial
• Oramed (ORMD-081)
• 179 T2D patients randomized, blinded
• Taken at night
• Treated 28 weeks with placebo vs oral insulin
• Compared CGM pre- and post-treatment
Kidron et al, ADA 77th Sci Sessions, San Diego CA, June 2017, P-989

Case 1
• 38 year old female with T1D for 18 years
• Reasonably well controlled, HbA1c usually 6.9-7.6% range
• Occasional, non-severe hypoglycemia
• No known diabetes complications
• Recently changed to hybrid closed loop automated insulin delivery device (Minimed 670G)
• Doing well, but often forgets to bolus before her meals



Case 1
• What future improvements in artificial pancreas technology could help her with her post-prandial glucose variability?
A. Improved CGM technology
B. Faster-acting insulin
C. Addition of dual hormone therapy in pump
D. Improved algorithms for closed loop insulin delivery
E. All of the above

MiniMed 630G/640G
• Similar to the 530G sensor augmented pump
• 300 unit reservoir
• Uses “Smart Guard” technology
• Automatically stops insulin for up to 2 hours when threshold reached
• Alerts up to 30 min before glucose hits upper/lower set limits, 640G can predict and suspend before lows
• Has new design
Hybrid Closed Loop (HCL)
• Insulin pump software automatically increases or decreases insulin delivery based on sensor glucose values
• Patients are still required to enter carbohydrate information for dose delivery prior to eating (“hybrid”)
• Success of HCL is dependent on insulin infusion site and sensor
• HCL works best on overnight/fasting glucose (possibly due to limits of current rapid acting insulins?)

Case 2
• 56 year old F, with T2D for 15 years
• On metformin ER 2000 mg/day, liraglutide 1.8 mg/day
• No issues doing injections of liraglutide
• Checks SMBG 1-2 times/day
• Works evening shifts 3 nights/week as nurse
• HbA1c gradually increasing, now 8.7%
• Fasting BG typically 140-180 mg/dl (7.8-10.0 mmol/l)
• Planning to start basal insulin

Case 2: Question
• Which of the following would be best for starting her on basal insulin?
A. Start NPH insulin 0.2 unit/kg at 10 pm daily
B. Start glargine U-100 10 units when she goes to sleep
C. Start degludec 10 units daily
D. Use lispro insulin in a V-Go insulin patch pump

Degludec flexibile dosing
Mathieu et al, BEGIN Flex T1, JCEM 2103

NOT FOR PROMOTIONAL USE
CGM in T1D Glargine U-300 vs U-100: morning or evening dosing
Adapted from Bergenstal RM et al. Diabetes Technol Ther 2015;17:A16–A17
65
Me
an (
SE)
glu
cose
, mg/
dL
0 2 4 6 8 10 14 16 18 20 22 24
Gla-100
Time, h
Morning Evening
0 2 4 6 8 10 12 14 16 18 20 22 24
Gla-300
Morning Evening
Morning injection
140
130
0 2 4 6 8 10 12 14 16 18 20 22 24
0 2 4 6 8 10 12 14 16 18 20 22 24
Evening injection
Time, h
150
160
170
200
180
190
140
130
150
160
170
200
180
190
140
130
150
160
170
200
180
190
140
130
150
160
170
200
180
190
Me
an (
SE)
glu
cose
, mg/
dL

V-Go: Disposable Insulin Delivery
V-Go website: www.go-vgo.com

V-Go Dosing
V-Go website: www.go-vgo.com

V-Go
• Lajara et al, Diabetes Ther, 2015
• Improved A1c
• Less insulin used
• No increased rates of hypoglycemia

OneTouch Via (Calibra Finesse)
• Insulin patch pump worn for 3 days
• Gives bolus insulin only
• Holds up to 200 units of rapid-acting insulin
• Boluses in 2 unit increments
• Can bolus through clothing
• 50 year old M, T2D for 10 years
• A1c in 9-11% range for years
• Wife has well-controlled T2D, he is main cook for family
• Does not like checking BG (1-2/day)
• Glargine U-300 : 140 units
• Lispro: 50 units w/ meals
• Past Med Hx:
– HTN, hyperlipidemia
• Non-smoker
• Early neuropathy
• Has been working hard on diet and lifestyle
• A1c now = 9.0%
Case 3

Case 3
Average BG: 177 mg/dl +/- 53 (9.5 mmol/l)

Case 3: Question
• What would be a good option for you do next for this patient?
A. Increase basal insulin
B. Strengthen his evening meal carb ratio
C. Get more data with a continuous glucose monitor device
D. Change to an insulin pump

Case 3
Diagnostic CGM done in clinic:

• High overnight but drops quite a bit
• Spike around 9AM and again around 10PM
• Fairly steady during the midday
• breakfast and dinner lispro, glargine u-300
• Limit evening snacking
Case 3


8.6%
7.6% 7.7%
8.6%
8.1% 8.2%
7.0
7.2
7.4
7.6
7.8
8.0
8.2
8.4
8.6
8.8
Me
an A
1c,
%
CGM
Usual care
Dexcom DIAMOND Study: A1c Reduction
P<.001 P<.001
Week 24 -0.6% (-0.8% to -0.3%)
Week 12 -0.5% (-0.7% to -0.3%)
Baseline Adjusted mean difference (95%
CI) Beck et al, JAMA, 2017
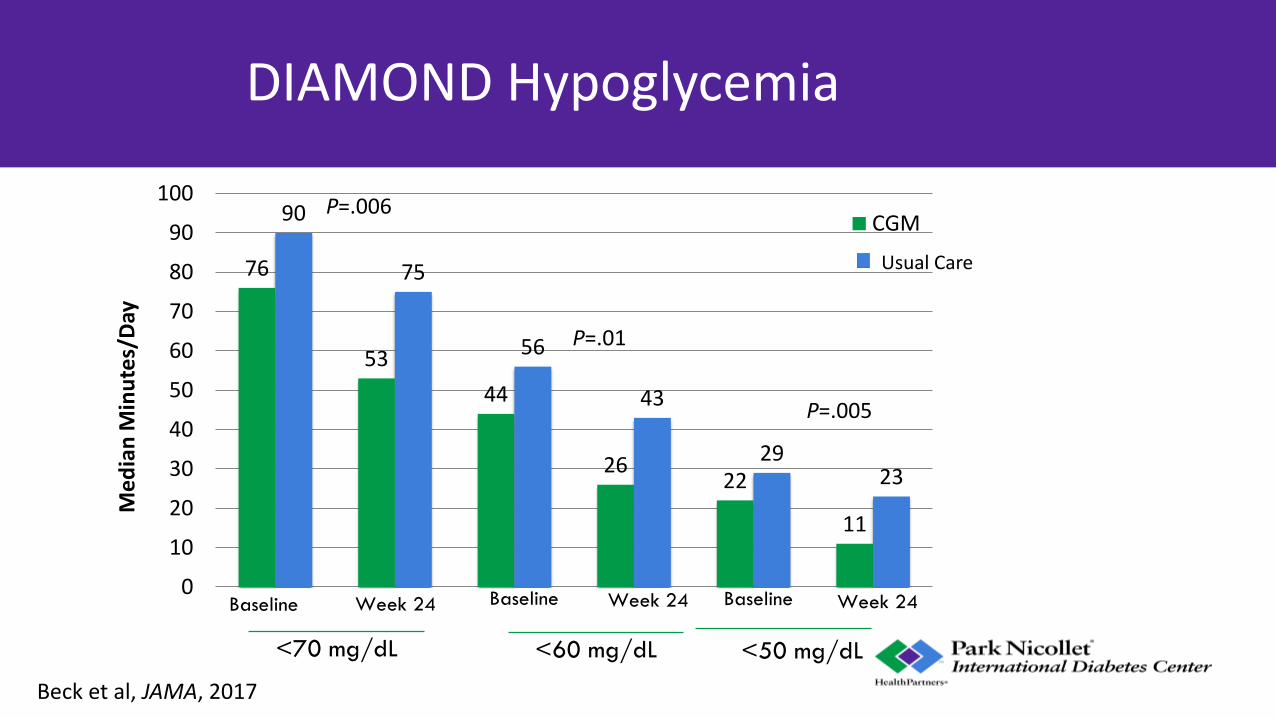
DIAMOND Hypoglycemia
76
53
44
26 22
11
90
75
56
43
29 23
0
10
20
30
40
50
60
70
80
90
100
Me
dia
n M
inu
tes/
Day
CGM
<70 mg/dL
Baseline Week 24 Baseline Week 24 Baseline Week 24
<60 mg/dL <50 mg/dL
P=.006
P=.01
P=.005
Usual Care
Beck et al, JAMA, 2017

Conclusions
• Concentrated insulins are an option for patients requiring high amounts of insulin
• New basal insulins have a smoother profile and less risk for overnight hypoglycemia
• Faster acting meal time insulins are in development
• The use of automated insulin delivery, CGM, and other pump devices can help better administer insulin

Thank you




























