Embed Size (px)
Citation preview

Neutron Therapy Treatment For Advanced and Radioresistant Tumors
Fighting Cancer with Neutrons

Neutron Therapy at Fermilab
One of two (three ?) neutron therapy facilities in the US
Operated in partnership with NIU Located in the Linac Gallery Have been treating since 1976, not experimental Radioresistant – not well controlled by
conventional photon (x-ray) therapy Depends on the type of tissue that is cancerous Location & type

Neutron Therapy at Fermilab
Patients from both physician and self referral
Also referred to as “fast” neutron therapyFirst trials of neutron therapy in 1938 used
lower energy neutrons than what is used today.

FAST NEUTRON THERAPYFAST NEUTRON THERAPY
Why is it necessary?Why is it necessary?Why Fermilab?Why Fermilab?How is it done?How is it done?Clinical ResultsClinical Results

Why Radiation Therapy?
Why is it Necessary?

CancerStages & Treatment
Stages
Local Tumor
Regional Metastasis Locally advanced
Systemic Disease
Treatment
Surgery
Radiation Therapy
Chemotherapy

What is Radiation Therapy?(External Beam Therapy)
Radiation directed at the tumor from outside the body

Conventional photon (x-ray) therapy

What is Radiation Therapy?(External Beam Therapy)
Radiation directed at the tumor from outside the body
Two critical componentsWhere the energy is depositedThe type of damage produced

Where is the Energy Deposited?
0
20
40
60
80
100
0 5 10 15 20 25 30 35
) Depth in Phantom(cm
Dose, N
orm
alize
d t
o D
max )%
(
SAD = 190 cm
SSD = 180 cm
Photons
Neutrons
Protons

Neutrons

LargeLarge radioresistantradioresistant tumors are not well tumors are not well controlled by photon (or proton) therapycontrolled by photon (or proton) therapy
Resting cells are radioresistantResting cells are radioresistant Hypoxic (low oxygen) cells are Hypoxic (low oxygen) cells are
radioresistantradioresistant
Neutron therapy is less affected by cell cycle or oxygen content
Why are Neutrons Needed?

How Do Neutrons Overcome Resistance?The Type of Damage Produced
Cell killing mechanisms are complicatedDNA damageFree radicalsBystander effectInflammationGenetics
Focus on DNA damage through:Radiation QualityLinear Energy Transfer - LET

Radiation QualityRadiation Quality
Photons and Charged Particles Neutrons
Low LET High LET

2 nm 10 nm 30 nm 2 μm
Optimum LET100 eV/nm~3 ip
~200 nm
DNA DamageDNA Damage

LET ComparisonLET Comparison(Linear Energy Transfer)(Linear Energy Transfer)
Belli, et. al., Molecular Targets in Cellular Response to Ionizing Radiationand Implications in Space Radiation Protection, J. Radiat. Res.,43:Suppl.,S13-S19 (2002)
Photons & Protons
Neutrons

How can we turn LET,radiation quality,
and all the other complexities of cell killing
into something we can understand?

Survival of Clonogenic DU 145 Prostate Cancer Cells
0.000001
0.00001
0.0001
0.001
0.01
0.1
1
0 5 10 15 20 25 30
Dose in Gray
Photons in 2.00 Gyfractions
Neutrons in 1.75 GyFractions
Preliminary
Blazek, et al
Factor of 3
Relative Biological Effectiveness
Neutrons
Photons
Relative Biological Effectiveness- RBE -
is the reason for pursuingNeutron Therapy

So What is the Best Therapy?
LETLow High
DoseDistribution
Bragg
Exponential
Photons
Protons
Neutrons
Ions
$ $$
$$$ $$$$($)
Cost-effectiveHigh RBETherapy

Why Fermilab?
Robert Wilson – 1st director of Fermilab Article in Radiology in 1946 proposing protons
Paper by Louis Rosen of LASL Use of accelerators for other than physics research – PAC ‘71
Prof. Lester Skaggs – U of C & Argonne Cancer Hospital Organized discussions looking at p, ions, π –1971
Clinical results from Hammersmith Hosp With neutrons - RBE
September 7, 1976 – 1st patient treatment With neutrons
How is radiation therapy done?

Electron linear accelerator for photon therapy

Proton linear accelerator for neutron therapy

Proton linear accelerator for Neutron therapy

Proton linear accelerator for neutron therapy

Photon & Neutron CollimatorsPhoton & Neutron Collimators

Some Clinical Results
How good is Neutron Therapy?
It depends.

Before Neutron Therapy
ProstateTumor
Bladder(with contrast)
displaced
CT scan of prostate cancer

After 12.25 Gray of neutrons
Bladder(no contrast)
Normal position

Beginning Of Treatment End of Treatment
Soft Tissue Sarcoma
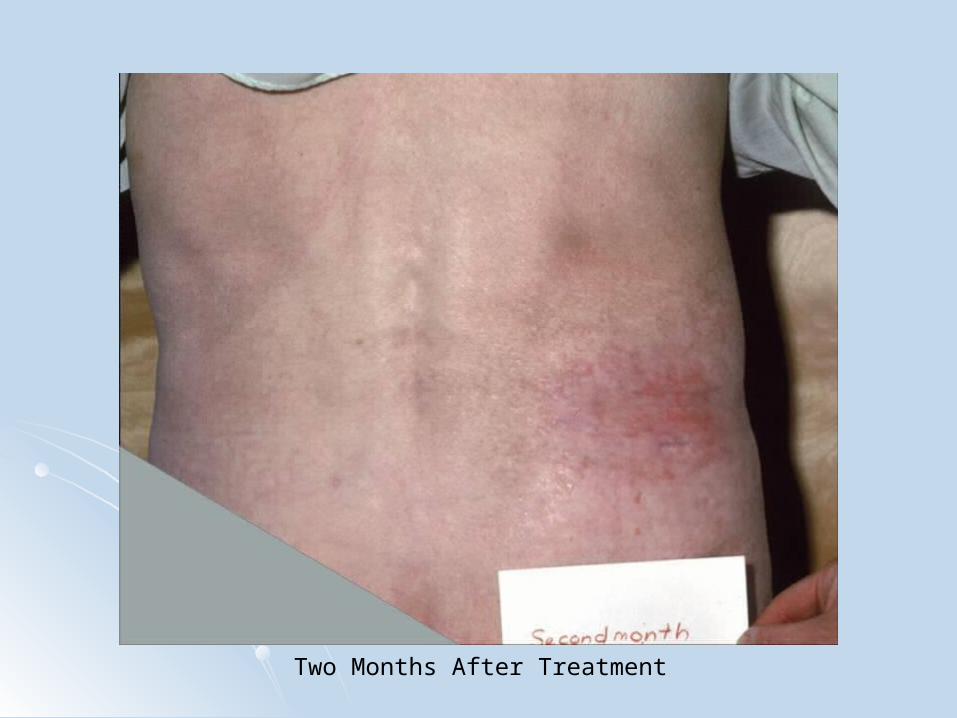
Two Months After Treatment

Squamous Cell Carcinoma

Results of Neutron Clinical TrialsResults of Neutron Clinical Trials Reference - Nuclear data for neutron therapy: Status and Reference - Nuclear data for neutron therapy: Status and
future needs - IAEA TECDOC 992 (1997)future needs - IAEA TECDOC 992 (1997)
““The proportion of patients suitable for neutrons ranges from 10-20%, but this is probably a lower limit…with high energy modern cyclotrons neutron therapy will be useful for a larger proportion of patients. ” (page 24) ” (page 24)
Tumors where fast neutrons are superior to conventional x-rays are: Salivary - locally extended, well differentiated Paranasal sinuses - adenocarcinoma, mucoepidermoid,
squamous, adenoid cystic Head and Neck - locally extended, metastatic Soft tissue, osteo, and chondrosarcomas Locally advanced prostate Inoperable/recurrent melanomas (page 23) (page 23)

Results of Neutron Clinical TrialsResults of Neutron Clinical Trials IAEA IAEA
TECDOC 992 (1997) - (continuedTECDOC 992 (1997) - (continued))
Tumors where more research is needed Inoperable Pancreatic Bladder Esophagus Recurrent or inoperable rectal Locally advanced uterine cervix Neutron boost for brain tumors (pp 13-19)(pp 13-19)

Review of the loco-regional rates for malignant Review of the loco-regional rates for malignant salivary gland tumors treated with radiation salivary gland tumors treated with radiation
therapy.therapy.
Fast Neutrons
Authors Number of Patients
Loco-regional control (%)
Saroja et al. (1987) 113 71 (63%)
Catterall and Errington (1987)
65 50 (77%)
Battermann and Mijnheer (1986)
32 21 (66%)
Griffin et al. (1988) 32 26 (81%)
Duncan et al. (1987) 22 12 (55%)
Tsunemoto et al. (1989) 21 13 (62%)
Maor et al. (1981) 9 6 (67%)
Ornitz et al. (1979) 8 3 (38%)
Eichhorn (1981) 5 3 (60%)
Skolyszewski (1982) 3 2 (67%)
Overall 310 207 (67%)
Low-LET Radiotherapy Photon and/or Electron beams
and/or Radioactive Implants
Authors Number of Patients
Loco-regional control (%)
Fitzpatrick and Theriault (1986)
50 6 (12%)
Vikramet et al. (1984) 49 2 (4%)
Borthne et al. (1986) 35 8 (23%)
Rafla (1977) 25 9 (36%)
Fu et al. (1977) 19 6 (32%)
Stewart et al. (1968) 19 9 (47%)
Dobrowsky et al. (1986) 17 7 (41%)
Shidnia et al. (1980) 16 6 (38%)
Elkon et al. (1978) 13 2 (15%)
Rossman (1975) 11 6 (54%)
Overall 254 61 (24%)
Table III. from IAEA-TECDOC-992, “Nuclear data for neutron therapy: Status and future needs,” December 1997, pg. 12.


Side EffectsTheraputic Window
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 5 10 15 20 25
Dose (Gy)
Tu
mo
r C
on
tro
l
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Co
mp
licati
on
Rate
tumor control
complication rate
Desired tumor control
Acceptable complication rate
Theraputic Window

Incidence of Life-Threatening or Fatal late normal Incidence of Life-Threatening or Fatal late normal tissue toxicity in the head and neck by prescribed tissue toxicity in the head and neck by prescribed
tumor dose.tumor dose.

An Important Point for PotentialHealth Care Consumers
Neutron Therapy is NOT a treatment of last resort. Healthy tissue can only tolerate a certain amount of
any type of radiation. A specific tumor site cannot be retreated if it has
already been treated with photons.
Patients from both physician and self referral We presently treat up to 20 patients per year
Very underutilized

How to find us
neutrontherapy.niu.edu
Or
neutrontherapy.org

Does Fermilab Still Have a Role?Not tied to a major Hospital
Good and BadLarge source to isocenter distanceContinuity in physician support Inventive environment
Presently developing upgrades
Until an optimized,dedicated facility is built,
Fermilab is (almost) the only game in town.

The End – Thank youThe End – Thank you
Marty Murphy