Embed Size (px)
Citation preview

1
Neurology Core Cases

NeurotransmittersAmino Acids
(Fast CNS neurotransmitters)Monoamines
(Diffuse neural pathways)Peptides
EXCITATORY: Glutamate + Aspartate
Ionotropic (AMPA,NMDA) and metabotropic receptors
Acetylcholine- fast NS in CNS. Peripheral effects via Muscarinic and Nicotinic receptors (NMJ)
Noradrenaline and Adrenaline (Act at adrenergic receptors)
Dopamine: Basal ganglia and limbic system
Serotonin: descending pain control pathways sleep and waking, aggresive behaviour
Histamine: H1 (SM in gut and bronchi) and H2 (acid and ↑HR) receptors
• Substance P•VIP•Enkephalin (opioid peptides)•Neuropeptide Y
INHIBITORY: GABA + Glycine
GABA A receptor- chloride channels with modulating sites for BZDs and barbiturates to enhance action.GABA B receptor: K+ channel
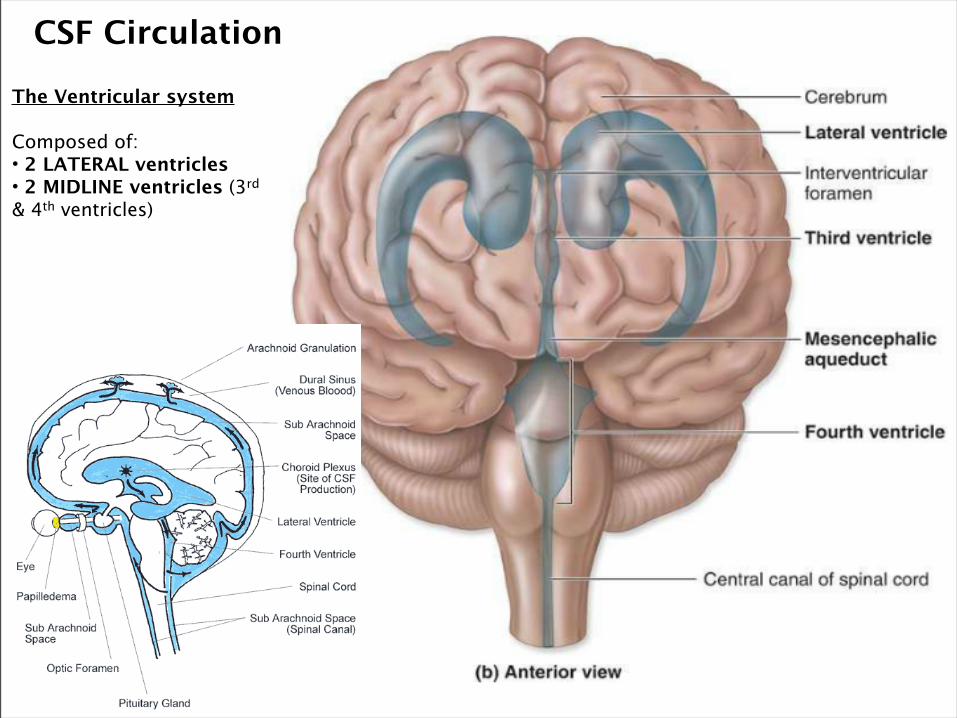
CSF Circulation
The Ventricular system
Composed of:• 2 LATERAL ventricles• 2 MIDLINE ventricles (3rd & 4th ventricles)
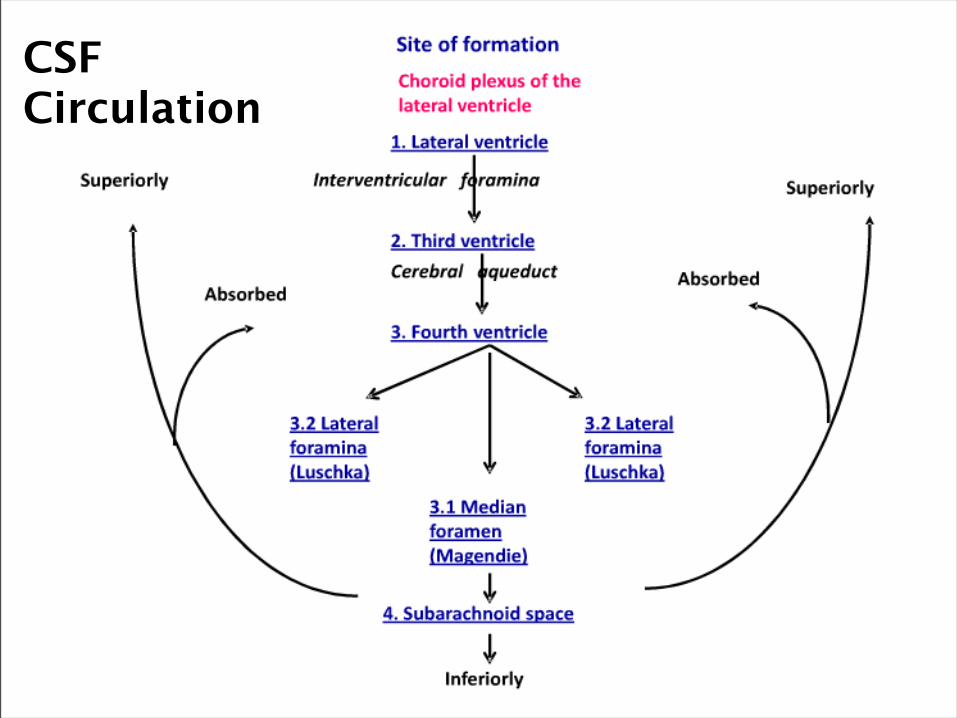
CSF Circulation

5
MeningesThree layers of the meninges:1) Dura Mater: Outermost. Means tough
mother. It acts to support the arachnoid space, and hold the dura sinuses.
2) Arachnoid Mater: Middle. Held on the under side
of the dura mater. Has connections into the dura mater to the dura sinuses to allow the drainage of CSF. The sunarachnoid space holds CSF and carries blood vessels of the brain.
3) Pia Mater: Inner most. Delicate & thin
layer which is impervious to water so keeps CSF in sub arach space. The pia mater is firmly adhered to the brain, following sulci. Inflammation of the pia mater causes meningitis.

Location of both motor & sensory spinal cord tracts


GCS
Best Eye Response Verbal response Motor response
E4 V5 M6
No eye opening No verbal response No motor response
Eye Opening to Pain Incomprehensible sound Extension to Pain
Eye Opening to Verbal Command
Inappropiate Words Flexion to Pain
Eye opening spontaneously
Confused Withdraws from Pain
Orientated Localises Pain
Obeys Command

Horner’s syndromeHorner's syndrome is a triad of features resulting from interruption of the sympathetic pathway
from the hypothalamus to the orbit, as follows:• ipsilateral miosis and partial ptosis• ipsilateral anhidria on the face• there is no enopthalmos, although the narrow palpebral aperture may suggest it
Despite the ptosis - normal range of lid movement in and up and down movement - supplied by the third nerve
Despite the miosis, the pupillary response to light and the near reflex are brisk and sustained but dilation of the Horner's pupil in response to darkness is diminished or absent
The degree of miosis is not related to the level of the lesion i.e. whether central, pre- or post- ganglionic
Aetiology: Horner's syndrome is a result of central or peripheral lesions:Central: vascular (PICA/ lateral medullary syndrome, basilar artery occlusion), demyelinating disease
(MS), syringomyelia or syringobulbia, tumours, cervical cord tumoursPre- and post- ganglionic lesions: apical pulmonary disease (Pancoast's syndrome), cervical rib,
mediastinal tumour, carotid aneurysm, thyroid enlargement - goitre, tumour, neck trauma - carotid arteriography, cervical sympathectomy, cervical lymphadenopathy, cervical sympathectomy, brachial plexus lesions (Klumpke's palsy)
10
Facial Nerve PalsyBell’s PalsyLMN lesion of the facial nerve. This means that there is no forehead sparing.Incidence is 20 per 100,000 from 10-40, but 59/100,000 >65. Incidence > in DM. 7% recurrence.Suggested link to herpes simplex.Sudden, usually unilateral weakness of facial muscles. Most cases are painless, some may develop
pain in ear. Loud sounds may be uncomfortable (stapedius affected), may lose sense of taste. Eyes may not close fully, and become dry.
Mx: Steroids can be started w/in 72 hours. Also Anti-virals could be started. Eye protection also important: eye pad, artificial tears, eye ointment for overnight use.
Prognosis: Symptoms usually start to improve after 2-3 weeks with full recovery in 2-3 months. In some weakness may remain.
Ramsey-Hunt SyndromeLMN lesion due to varicella zoster infection.Facial weakness associated with pain (prominent feature), vesicles seen in ispilateral ear, hard
palate, +/- anterior 2/3rds of tongue. It can also be associated with deafness & vertigo, and other cranial nerves can be affected.
Mx: Prompt treatment w/in 72 hours. Combined treatment of acyclovir and prednisolone.Prognosis: 75% complete facial recovery. Scarring of lesions may occur. Usually full hearing
returns.

Visual impairmentLesion location Causes Visual defect
Optic nerve lesion MS, tumour, B12 deficiency, toxins, Vascular (Giant cell arteritis, Amaurosis fugax, HTN, diabetes), Trauma, papilloedema
Ipsilateral Monocular visual loss
Optic chiasm Pituitary adenoma, craniopharyngioma, 2° neoplasms, aneurysms
Bitemporal hemianopia
Optic radiation + optic tract
Tumours, stroke, infection Parietal – inferior quadrantanopia (pie on the floor)Temporal- superior quadrantanopia(pie in the sky)
Occipital cortex Macular sparing (dual blood supply from MCA and PCA)


Labyrinthitis Commonest cause of acute vertigo associated with Sever vertigo, hearing loss (always, but do not have fullness of ear as in meniere’s, and possibly tinnitus, sweating, nausea, vomiting, pallor and occasional diarrhoea. Viral origin, so usually preceded by URTI. PCs: Nystagmus + sensorineural deafness.Self-limiting: couple of weeks, treat w/ anti-emetics.
Benign paroxysmal positional vertigo (BPPV)
Brief recurrent attacks of vertigo provoked by certain changes in head position with respect to gravity most. Common provocation moves are: rolling over in bed, bending over, looking upward.Attacks are sudden w/ movement but usually abate after 30 seconds if head still.Associated with nausea, not usually vom. Hearing & tinnitus not involved. Can be confirmed by Halpike Test. Rx: Epley’s manoeuvre, short term use of anti-emetics, avoid vestibular suppresants
Menieres disease
Progressive dilation of the membranous labyrinth by fluid changes causing, a mixture of all of: vertigo, hearing loss & tinnitus.Core symptoms: Paroxysmal attacks (minutes to hours: usually hours) of disabling vertigo, hearing impairment, tinnitus and feeling of fullness in ears. Acute episodes may occur in clusters 6-11/year, with remission lasting months. Most progress uni->bilateral. 4% have drop attacks: sudden fall w/out LOC or vertigo.Rx: Acute: Anti-emetics, Prophylaxis: Vestibular sedatives (betahistine/ cinnarizine/antiemetics). Advise: reduce salt, avoid caffeine, chocolate, alcohol, tobacco.
Acoustic neuroma / Vestibular Schwannoma (benign)
Cerebellopontine angle (CPA) lesionAssociated with neurofibromatosis type IIOften involvement with CN V + VIIPCs: Unilateral sensorineural deafness (90%), vertigo+ tinnitus (70%), headacheIx: MRI. Rx: Surgery/ radiotherapy
Vertigo

HeadachesRule out ENT, ocular, teeth, sinus problemsDrugs: Analgesics, nitrates, caffeine...• Acute (vascular)- extradural, subdural, subarachnoid, intracerebral (intra-parenchymal),
intraventicular, first onset migraine, coital/exertional headache• Subacute- Giant cell arteritis, tumour, meningits/encephalitis, venous sinus thrombosis• Chronic- Tension, Migraine, Raised ICP, Cluster, Trigeminal Neuralgia,
Migraine•With aura – classical (30%) / Without- common (70%)Triggers: Hunger, sleep deprivation, exercise, + stress Hormones, OCP + (during periods). Foods: caffeine, alcohol, cheese, chocolateS&S Prodrome (mood/behaviour change/ yawning, hunger, cravings, fatigue) Aura typically
visual (flashes, spots, zigzags of light) or sensory disturbances (numbness+ tingling of limbs)Headache: Severe, unilateral throbbing/ pulsating– often lasts <24 hours but can last days. AFs: N+V, photophobia, phonophobia, mood change, lethargy
Ix: Aimed at ruling out other causes. May include FBC, ESR, CT/MRI, LPMx: Rx: 5HT agonists (triptans), NSAIDs, paracetamol, codeine + antiemetics.
Prophylaxis: β- blockers, valproate, TCAs.Advice: Regular meals, sleep, caffeine restriction, stress reduction, avoid triggers, symptom diary, restBeware of analgesia overuse headaches (OTC meds)
Cluster HeadachesFeatureless, never severe, squeezing (band round head). Worse with nervous tension. Rx: stress management, Amitryptilline (CI’d in restless legs and poor sleepers)

Trigeminal Autonomic Cephalgias (TACS)Short acting headaches with Autonomic disturbances→ lacrimation, rhinorrhoea, miosis, ptosis, eyelid oedemaCluster Men- middle early aged + smoke
Recurrent attacks of unilateral pain, centred around the orbit, Autonomic features: red runny eye, ptosis, very severe (15/10 pain), Agitation, distressed, horrible. Wake from sleep- same time!Duration 20mins-4hours/ frequency 1X3 per day. Abrupt offsetAcute management: 100% Oxygen (7-15 L/min for 20 mins) Sumatriptan (sc)Intermediate: Prednisolone <3 weeksLong term: Verapamil, occipital nerve blocks
Paroxysmal hemicranias
Short, very frequent attacks of unilateral pain, (2-3mins) marked cranial autonomic features, Excellent response to indomethacin. Associated with TGN
SUNCT / SUNA Short-lived unilateral headache with conjunctival injection and tearing.V. Rare: Even more brief(5-240secs) and frequent (upto 200/day) than paroxysmal hemicranias. Triggered by cutaneous stimuli (touching, cold wind) Can be misdiagnosed as TGN, more likely to affect forehead than TGN and leads to bloodshot eye. Rx lamotrigine
Hemicrania continua
Similar to cluster headache but rarer, shorter lasting and more frequent. 5-20minutes between 20 and 40/per day. Diagnosis by indomethacin trial which resolves it.
Trigeminal Neuralgia:
Electric shock pain very severe lasting from a few seconds to several minutes. Pain usually on one side of cheek or face but can also involve eyes, lips, nose, or ears.Triggers: Vibration, skin contact (shaving, washing), brushing teeth, rating, wind.Mx: Carbamazapine (first line), gabapentin w/ baclofen or clonazepam, lamotrigine.Surgery: relieve pressure on trigeminal nerve (usually blood vessels).
TMJ Dysfunction(Not TACS but similar pain)
3 cardinal features: facial pain, reduced mouth opening, joint noise. Pain typically around TMJ (below tragus) but can radiate to head, neck & ear.Mx: Conservative: Rest, bite guards, accupuncture, physio. NSAIDs, amitryptaline.Surgery: Intra-articular inject. Max fax involvement if conservative failed.

Raised ICP headacheCauses •Haematomas: Extradural, subdural, intracerebral.
•Neoplasams: Mets, Glioma, Mets.•Abscess.•CSF disturbance: obstructive hydrocephalus, communicating hydrocephalus.•Cerebral Venous Thrombosis.•Diffuse Brain Oedema: encephalitis, meningitis, diffuse head injury, subarach, Reye’s.•Idiopathic Intracranial Hypertension.
S&S: Generalised acheAggravated by bending, coughing, straining (stoop+ poop)- all ↑ICPWorse in morning (may awaken patient)Severity gradually progressesTypical Triad of: Headache, papilloedema, vomiting.
Acutely Severe Raised ICP: Cushing’s Triad: Widening pulse pressure (Hypertension), bradycardia & irregular breathing (Cheyne-Stokes Breathing).
Often accompanied by vomiting, visual obscurations and progressive focal neuro signs
Mx: Risk of herniation ie coning, do not do LP.
Must do MRI/ CT to assess brain shift

Subarachnoid haemorrhageSpontaneous arterial bleed into the subarachnoid space from an aneurysm.Causes: Saccular “Berry” aneurysms (70%). AV malformations (10%) Not definedAneurysm originally thought to be congenital, but now thought also to be due to atherosclerosis & HTN.Link between Berry aneurysm & Polycystic Kidney Disease.Epidem: 6% of population. 6-12/100,000/year. Mean age 50. 10-15% don’t reach hospital.S&S: •Severe headache/ worst ever /instant onset/ “Hit round head with baseball bat”. May only last
one second. Patient may accuse someone of hitting them around the head. Only symptom in 1/3 of patients. However usually last 1-2 weeks.•LOC (transient or prolonged). Seizure in 7% but highly suggestive if occurs.•N+V (due to raised ICP).
Patient may have sentinel bleeds. 10-15% of pts. Headache, dizziness, orbital pain, diplopia.
Signs of meningism after 3-12 hours, drowsiness/coma, focal signs
Hx: Warning signs/headaches. FHx, HTN, smoking, anticoagulantsIx: CT scan
LP if inconclusive and no contraindications (xanthochromia)CT angiography if still inconclusive
Mx: Immediate: Regular obs, bed rest+ fluid replacement,antiemetics+ laxatives (avoid straining), analgesia (codeine), Nimodipine (↓ vasospasm), transfer to neurosurgical unit
Surgery: Coiling+ clipping Prognosis: 10-15% don’t make hospital.
60% die in first 30 days.Rebleed carries mortality of 50-80%.Severe morbidity afterwards. Needs extensive rehabilitation & psychological support.

Subdural haemorrhage (SDH)Collection of blood that collects in the subdural space (between the dura mater and the arachnoid mater. This can be causes by:-Bleeding from damaged cortical artery-Bleeding from underlying parenchymal injury-Tearing of bridging veins from cortex to one of draining venous sinuses.The bleed, depending on the time of symptoms from underlying cause can be:-Acute: Almost instantaneous from direct blunt head trauma.-Subacute:3-7 days after after the initial injury.-Chronic: 2-3 weeks after the initial injury.
Risk Factors:
Alchoholics, elderly (due to brain atrophy), anticoagulant therapy, infants (shaken baby syndrome: always suspect abuse).
Hx Acute: Trauma, Headache, ↓ conscious level. May be lucid period of couple of hours before the patient begins to deteriorate.Chronic: Headache, anorexia, N&V, confusion, cognitive impairment, focal neurological signs: limb weakness, speech difficulty, psychiatric symptoms.
Ix: CT head: Crescent /sickle shaped mass- concave over brain surface Blood white on CT.MRI-brain has high sensitivity especially for isodense or small SDHsXR for skull fracture
Mx: ABC...Depends on size: •Conservative may allow spontaneous resorption. •Surgical- burrholes/ craniotomy
Comps: •↑ ICP, cerebral oedema, seizures
Extradural haemorrhage: traumatic tear to middle meningeal artery. Usually younger patients with a temporal or parietal skull fracture (battle signs). Biconvex on imaging

19
Extradural haemorrhage (EDH)Bleed into the space between the skull and the dura mater.Most often due a fracture of the temporal or parietal bone causing damage to the middle cerebral artery. Most commonly due to trauma in the temporal region. Only 20% of extradural haematomas occur outside of the the temporal region.Can also occur in the spinal cord where it called an epidural haematoma.
Hx Usually history of trauma which caused LOC.Classically this is followed by a lucid interval after which the patient deteriorates. Extradural haematoma can cause a very rapid deterioration to death in minutes.
Associated w/: Headache, N&V, seizures, Cushing Reflex (bradycardia, wide pulse pressure & irregular breathing), evidence of skull fracture: CSF otorrhoea, rhinorrhea, panda eyes, decreased GCS, unequal pupils, facial nerve injury, weakness of limbs, focal neuro signs.
Ix: Plain X-ray: may show skull fracture. Cervical Spine X-ray: rule out other C-spine injury.CT: haematoma causes convex haematoma (unlike concave for sub-dural).LP: avoided.
Mx: Full ATLS management.Alert patient can be treated conservatively but with close observations for deterioration.If raised ICP: mannitol. Burr holes may be required to reduce pressure.
Comps: Prognosis excellent in children but decreases with age.Can cause permanent neurological deficit.

Cerebrovascular Event (or CVA)Disruption of blood supply to the brain, causing rapidly developing signs of focal or global disturbance of cerebral functions lasting greater than 24 hours.TIA: similar clinical picture except symptoms abate w/in 24 hours.
Epidem: 150,00 people have stroke/year. 53,000 die from stroke/year. 20,000 TIAs.
Causes-Emboli from distant vessel & subsequent brain infarction (rupture of Atherosclerotic plaque, AF, MI, endocarditis etc); -Thrombosis: Internal carotid, vertebral or intracranial-Haemorrhage (HTN/trauma) Also includes SAH (5% of CVAs).
Also (< common): venous infarction, carotid/vertebral artery dissection, air/fat emboli, MS, tumours compressing vessels, vasculitis/arteritis (consider SLE,RA, Sjogrens in younger patients) neuro-syphilis.
Signs & Symptoms:
Cerebral hemisphere infarcts (50%) may cause contra-lateral hemiplegia (initially flaccid, later spastic); contra-lateral sensory loss; homomymous hemianopia; dysphasia. Brainstem infarct (25%): wide range of effects inc quadriplegia; gaze/vision disturbances; locked-in syndrome (aware, can’t respond). Lacunar infarct (25%): small infarct around basal ganglia, internal capsule, thalamus & pons – may cause pure motor, pure sensory, mixed signs or ataxia, intact cognition/ consciousness. Haemorrhagic stroke: severe headache (often occipital); vomiting; collapse +/- seizures; coma. Cerebellar haemorrhage can cause acute hydrocephalus. Dysphagia affects lost of stroke patients.
Ix: CT/MRI imaging – initial choice of investigation to distinguish btw haemorragic/infarct strokes. CT angiogramRoutine Blood: FBC (polycythaemia+ infection), ESR/CRP (inflammatory disease), Urinalysis/glucose, Fasting lipids, blood cultures (endocarditis), Autoantibodies (vasculitis), coag screen.Carotid Doppler: degree of carotid artery stenosis (>70% = endarectomy)Others: Lumbar puncture, CXR (neoplasm/HF), ECG (AF/MI),Echo (AF/endocarditis) MR angiography

NICE Stroke ManagementSuspected Stroke
Screen in community using FAST
Establish diagnosis using ROSIER
Maintain optimal Homeostasis:-Oxygen >95%-BM: 4-11 mmol/L-BP control <185/110, & only if hypertensive crisis.-Nutritional Support.
Immediate Brain Scan? (w/in 1 hour)-Indications for thrombolysis
-on anticoag therapy-Depressed GCS-Papilloedema
-Severe Headache, neckstiffness, fever
Yes No
Brain Scan w/in 24 hours.Thrombolysis indicated
Thrombolysis w/ Alteplase
w/in 4.5 hours
Direct admission to stroke unit.
YesNo
If haemorrhagic:-reverse anti-coag: Vit K/
protamine-Refer to neurosurgeons
Give Aspirin.Maintain optimal haemostasis as above.
OT/Physio/SALT input, early mobilization.
If thrombotic: give Aspirin 300mg with clopidogrel or dipyridamole at earliest opportunity.If venous sinus thrombosis give Aspirin, Heparin & Warfarin.If haemorrhagic see below.
22
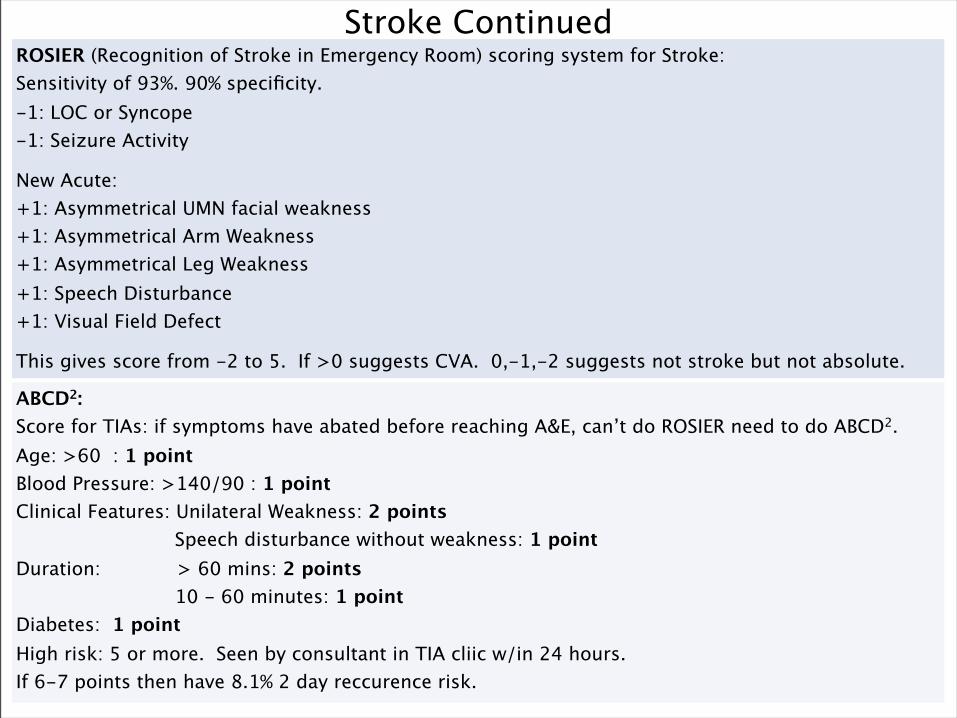
Stroke ContinuedROSIER (Recognition of Stroke in Emergency Room) scoring system for Stroke:Sensitivity of 93%. 90% specificity.-1: LOC or Syncope-1: Seizure Activity
New Acute:+1: Asymmetrical UMN facial weakness+1: Asymmetrical Arm Weakness+1: Asymmetrical Leg Weakness+1: Speech Disturbance+1: Visual Field Defect
This gives score from -2 to 5. If >0 suggests CVA. 0,-1,-2 suggests not stroke but not absolute.
ABCD2:Score for TIAs: if symptoms have abated before reaching A&E, can’t do ROSIER need to do ABCD2.Age: >60 : 1 pointBlood Pressure: >140/90 : 1 pointClinical Features: Unilateral Weakness: 2 points Speech disturbance without weakness: 1 pointDuration: > 60 mins: 2 points 10 - 60 minutes: 1 pointDiabetes: 1 pointHigh risk: 5 or more. Seen by consultant in TIA cliic w/in 24 hours.If 6-7 points then have 8.1% 2 day reccurence risk.

23
Intracranial Venous Thrombosis (Sinus Thrombosis)Thrombosis of intracranial veins or dural venous sinuses can lead to infarction or haemorrhage.The dural venous sinuses are present in the dura mater. They receive blood from the internal & external veins of the head & CSF from the sub-arch space. They all ultimately drain into the internal jugular vein. There blockage causes congestion and occlusion along their stem which can cause infarction or haemorrhage.May present very similar to a stroke or sub-arach, and can be difficult to diagnose. The thrombus causes congestion and obstruction leading to decreased perfusion and infarction.Main two types: Sagittal Sinus Thrombosis (47%), Transverse Sinus Thrombosis (35%).Also Canvernous Sinus Thrombosis which can spread from facial pustules or folliculitis.
Aetiology: -Infection: with spread from, most commonly the frontal sinuses. (staph most common).-Trauma or neurosurgical procedures.-Pregnancy & puerperium recognized association due to pro-thrombotic state.-Hypercoaguable states: anti-phospholipid, thrombophillia, anti-thrombin III deficiency.-Dehydration: due to increased coagulability.-Disseminated malignancy: due to increased coagulability.-Crohn’s & Ulcerative Colitis (also steroids used in treatment).-Vascular Disease: SLE, Wegner’s, Behcet’s.
Epidem: 1-2% of strokes. Affects wide demographic of patients w/ rfs. Women 20-35.
S&S: -Headache is common. Can be episodic and precede event by weeks. Also could be thunderclap, like sub-arach. May be only symptom.-Seizures and/or status epilepticus is common (very rare in arterial stroke).-Impaired or loss of consciousness is common.-Foc neuro S&S: hemiparesis, weakness of lower limbs, aphasia, ataxia, chorea, hemianopia.-Papilloedema -Cranial Nerves: Vestibular neuropathy, pulsatile tinnitus, unilateral deafness, diplopia, facial weakness, obstruction of vision.Sagittal Sinus Thrombus: Headache, vomiting, seizures, decreased vision, papilloedema.Transverse Sinus Thrombus: Headache +/- mastoid pain, focal S&S, seizures, papilloedema.Cortical Vein Thrmobus: Stroke like S&S develop over days or suddenly thunderclap, seizures, encephalopathy.

24
Intracranial Venous Thrombosis cont.Ix: Diagnosis with CT/MRI (venogram). Area of infarction not compatible with arterial occlusion.
Shows absence of sinuses post occlusion.Tests for underlying cause: FBC (platelets), Clotting, auto-antibodies.
Mx: Seek expert advice.Seizures: anticonvulsants.Thrombolysis: evidence still not conclusive. Best results when adminersted with catheter into sinus.Anticoagulation: Good evidence for heparin & warfarin.Surgery: rarely used. Thrombolectomy if rapid neurological deterioration.
Comps: Good prognosis if treated well. Mortality can range from 5-30%.2x increased success with use of anticoagulation.

25
Localising the Lesion in StrokeTwo main blood supplies to the brain:-The anterior circulation: supplied by the internal carotids-The Posterior Circulation: supplied by the vetrebral-basilar system.These anastamose to from the circle of willis which is made from three main arteries.-Anterior Circulation: Anterior & Middle Cerebral Arteries.-Posterior Circulation: Posterior Cerebral Artery.
Anterior Cerebral Artery:Supplies: Frontal & medial part of the cerebrum. Motor & Sensory: Weak, numb contra-lateral leg, foot drop +/- milder arm symptoms (think of
homunculus distribution). Face is spared. Bilateral infarction can cause akinetic mutism (damage to cingulate gyri).
Cognitive Changes: Expressive aphasia, apraxia on affected side. Confusion, Amnesia, Personality: flat, apathy, short attention span, slowness, deterioration in intellect.
Middle Cerebral Artery:Supplies: Lateral aspect of each hemisphere.Motor & Sensory: Contralateral hemiparesis, hemisensory loss (esp face & arm), contralateral
homonymous hemianopia.Cognitive Changes: Rapid progression to LOC. Dysphasia, w/ dominant hemisphere lesions
(usually left), or visu-spatial disturbance w/ non-dominant lesions. Dysgraphia, Dyslexia.
Posterior Cerebral Artery:Supplies: Posterior region of both hemispheres.Motor & Sensory: If Thalamus involved: diffuse sensory loss, mild hemiparesis, intention tremor.
If brainstem involved: Pupillary dysfunction, nystagmus, loss of conjugate gaze.Vision Changes: Homonymous hemianopia, cortical blindness, lack of depth perception, visual
hallucinations, memory deficit, dyslexia.

26
Localising the Lesion in StrokeVertebrobasilar Circulation Damage:Supplies: Cerebellum, Occipital Lobes & Brain Stem. Depending on lesion can cause a range of symptoms.If major artery in vertebrobasilar system then causes death or massive disability. Blockage usually
occurs in the smaller arteries and cause a number of different clinical pictures.General (any or combination of 3 main groups): -Vision: hemianopia, cortical blindness, diplopia.-Cerebellar: vertigo, nystagmus, ataxia, dysarthria, dysphasia.-Motor & Sensory: hemi or quadraplegia, unilateral or bilateral sensory symptoms.Others: hiccups, N&V, distrubance or LOC, Headache, incontinence.
Lateral Medullary Syndrome: Occlusion of one of vertebral arteries or PICA.Causes: Infarction of lateral medulla, and the inferior cerebellar surface.S&S: Vertigo, vomiting, dysphagia, nystagmus, ipsilateral ataxia, soft palate paralysis, ipsilateral
Horner’s.
Locked in Syndrome: Due to damage of the ventral pons from pontine artery occlusion.S&S: Patient unable to move but fully aware.
Cerebellar Infarction:in-coordination, clumsiness, intention tremor, ataxia, dysarthria, scanning speech.
Intranuclear Ophtlamaplegia:Horizontal gaze palsy.

27
Speech Problems:Speech area is in the dominant side which is usually the left hemisphere.It is in the left hemisphere in 99% of right handed people and 70% of left handed people.Therefore it is unusual to get a speech problem and left sided sensory or motor problems (as they are
on opposite sides).
-Dysarthria:Impaired ability to produce words. This is a motor problem, not a conceptual problem.Caused by: UMN lesions of cerebrum or LMN of brainstem, basal ganglia or cerebellum.
-Dysphasia:Impaired ability to understand or construct spoken word.
Receptive Dysphasia: Sensory or Wernicke’s Aphasia:Primarily a problem of comprehension. Speech is fluent but lacks content and is meaningless.
Patient’s lack awareness of their speech problem. Expressive Dysphasia: Production or Broca’s Aphasia:Primarily a problem of speech production. Speech is not fluent but generally has good semantic
content. Patients typically have slow halting speech, tip of the tongue feelings. Patient’s have awareness of their speech problem.
Wernicke’s Area: Located in the posterior Superior Temporal Gyrus.Broca’s Area: Located in the inferior frontal gyrus.Connected by: Arcuate fasciculus.

> 2 seizures. Seizure (Ictus): Paroxysmal synchronised cortical electrical discharges • Partial (simple and complex) – are focal- often temporal lobe, frontal lobe, occipital lobe• Partial becoming generalised• Generalised: Clonic, tonic, Tonic-clonic, absence- typical (petit mal) & atypical, myoclonic, atonic
Aetiology: •Idiopathic (Majority)-presumed to be genetic•Vascular (haemorrhage, infarct), most commonly seen in venous sinus thrombosis.•Drugs (Alcohol abuse /BZD withdrawal)•Tumour, •Trauma•Metabolic imbalances hypo/hypernatraemia, hypoglycaemia, hypomagnesaemia, hypocalcaemia, uraemia, hypoxia and porphyria. •Infection(Meningitis, encephalitis, neurosyphilis). • Malignant hypertensionImbalance between inhibitory and excitatory currents (Na+/K+) and neurotransmission(glutamate, GABA). Precipitants include anything that promotes excitation of cortex (flashing lights, drugs, sleep deprivation, metabolic) but often cryptogenic. Non Compliance
S&S: -Aura (may help localisation)- limb/oral automatisms, altered emotion, jamais vu, deja vu may suggest temporal lobe (also speech, smell, taste+ memory). Abnormal behaviour may suggest Frontal lobe-Onset, Duration, Consciousness, Memory, Tongue biting (side of tongue), incontinence, limb jerking (synchronous?), trauma, -Post-ictal phase: Confusion/ drowsy, residual focal neurological deficit (Todd’s paralysis) Pupil dilatation, ↑ HR/BP, cyanosis, ↓ O2 + pH, ↑ prolactin will help differentiate a true seizure from a pseudoseizure (psychogenic)
Epilepsy
Ix:
Bloods: FBC, U+E, LFT,CRP, glucose/thiamine,B12/folate, Ca2+, Mg2+, septic screen, TFTsCK + prolactin (transient↑ shortly after true seizure),Toxicology screen, ABGs, Anticonvulsant levelsEEG, Other: MRI/CT (Tumour, bleed etc) , LP (infection)
Mx: Long term AEDs: start after 2 seizures. Monotherapy preferred. When changing/stopping drugs, be slow and cautious (rebound seizures).Generalised: Valproate/lamotriginePartial: Carbamazepine/ lamotrigineAbsence in children: Ethosuximide
Patient info: Withdrawal and compliance. If of child bearing age, implications for pregnancy, breast feeding, effectiveness of OCP (Multiple drug interactions/ enzyme inducer), teratogenicity (seek specialist advice).
DVLA: Seizure free for 1 year to drive. Nocturnal seizures (free from daytime for 3 yrs). Single precipitating cause (3-6 months off driving). Changing/stopping meds (6 months off from last dose)
Status epilepticus: Resuscitate (ABC), Check glucose, Thiamine if alcoholism or malnutrition suspected to avoid precipitating Wernicke’s encephalopathy)IV lorazepam or IV/PR diazepam (repeat at 15mins if necessary)→IV phenytoin, valproate → Consider GA
Surgery: Tumour removal. Also Vagus nerve stimulation(VNS)
Comps: Trauma with seizuresAEDs: Phenytoin- gingivial hypertrophy, carbamazepine (agranulocytosis), lamotrigine (Stevens-Johnson syndrome)
Epilepsy

Seizures vs syncopeSYNCOPE TONIC-CLONIC SEIZURE
BEFORE •Usually upright position (standing)•Prodromal symptoms: (cerebral hypoperfusion) light-headedness, nausea, tinnitus, dimming vision, pallor, sweating•Triggers: Fear, pain, postural, micturition, coughing. CV arrhythmia, outflow problem. Can also have incontience
•Can occur in any position at any time•Preceding aura symptoms•Sudden onset•Urinary/faecal incontinence•Tongue biting (side of tongue)
DURING •FALL.•FLOPPY.•TWITCH (brief).•PALE/CLAMMY.•Hypotension+ bradycardia
RIGID + CYANOSED (TONIC).CLONIC JERKING- > 1 MIN.
AFTER Relatively rapid recovery: quickly orientated.
Post-ictal confusion, drowsiness, headache
Other ∆∆ of transient LOC: Vertebrobasilar insufficency ( other brainstem symptoms- vertigo, diplopia), hypoglycaemia, hyperventilation, narcolepsy/cataplexy

GCSE vs PNESGCSE PNES
MOVEMENTS SymmetricalStiff/ rigid
Small amplitude
Flailing, high amplitude, back arching, thrusting.
Stop- start
RESPIRATORY DISTRESS
Cyanosis Pink
LOC Unconscious May respond (RTOE)

Parkinson’s DiseaseA-kinetic rigid syndrome (diminished movement w/ an increased tone).Substantia nigra through dopamine has an inhibitory effect on other movement areas so damage and removal of the inhibition causes constant activity so: rigidity & reduce movement as already contracted so not much movement possible from this base line.80% of neurons in subtsantia nigra need to be lost to have Parkinsonian symptoms.
Aetiology: Cause unknown. Twin studies conflicting. Some ev of exogenous toxins (herb/pesticides, heroin).Parkinson’s Disease (Primary Parkinson's): Idiopathic (also Juvenile Parkinson’s).2o Parkinsonism: Drugs (anti-psychotics & anti-emetics (meteroclopramide/ domperidone), Vascular Parkinsonism, Infectious Parkinsonism, Trauma, Neoplastic, Hydrocephalus.
Parkinson Plus: Multi-System Atrophy, Progressive Supra-Nuclear Palsy (Autonomic Dysfunction).
S&S Classical Triad:1) Tremor: Coarse resting tremor (pill rolling), decreased on movement, increased by distraction.2) Rigidity: Stiffness of limbs, felt throughout movement, equally on flexors & extensors. Rigidity is usually asymmetric.Lead-Pipe: Rigidity alone.Cog-wheel: Rigidity mixed with tremor giving it a shaky quality.3) Bradykinesia: Slowing & poverty of movement. Limbs & face (mask like), Causes festinate gait.
Other features:-Loss of postural reflexes. Inc, falls, stooping shuffling gait, feet close together, poor arm swing.-Speech: Monotonous, hypophonic, dysarthria.-Micrographia, -Constipation & Urinary Incontinence common.-Psychiatry: Dementia common in later disease. Depression also common.-O/E: Sensory examination is normal & power is usually preserved.

33
Drugs in ParkinsonismDopaminergic Agonists (Levadopa)Effective against bradykinesia & Rigidty. Usually large doses required: as 1% crosses BBB.L-Dopa metabloized to dopamine by dopa carboxylase in liver and peripheries. Less effective against festinate gate and postural instability.
Side Effects: N&V, confusion, chorea.Chronic Side Effects: Increasing lack of efficacy, Freezing, On/Off syndrome.Does not alter progression of disease.
CarbidopaCarboxylase inhibitor added to Levadopa to reduce peripheral breakdown of drug.Helps to prevent peripheral side effects of N&V.
MAO-B Inhibitor (Selegiline)Inhibits central (inside of BBB) catabolism of dopamine.Helps to smooth out response to L-Dopa.Can also be used to delay need for starting L-Dopa.
Side Effects: Inflammation of mouth, abnormal movements, constipation, depression.
COMT Inhibitors (Tolcapone & Entacapone).Reduces breakdown of COMT which breaks down of L-Dopa in the peripheries and centrally.Can only be used with carbidopa or levadopa, not effective alone.Increases peak levels of L-Dopa. Can reduce need for L-Dopa by 20-30%.
Dopamine Receptor Agonists (Ropinirole, Cabergoline, Pramipexol)Active against D1 & D2 receptors.Often used as a primary treatment before Levadopa.May have better effects against dyskinesia compared to L-Dopa.
Side Effects: Drowsiness, postural hypotension, GI Side effects, Constipation.
Huntington’s ChoreaHereditary condition caused by an expanded trinucleotide repeat (CAG) on chromosome 4 that
codes for protein Huntingtin. ↑ function of gene
Autosomal dominant inheritance- 50% inheritance riskDelayed onset Peak age 40years
Clinical features• Progressive cognitive and behavioural personality changes.• Movement disorders- chorea!! Pathology• Neuronal loss in the caudate nucleus, as well as areas such as the cerebral cortex.• Reduction in GABA & ACh neurotransmission (inhibitory). Treatment• No effective treatment. Phenothiazines: stop chorea by inducing parkinsonism.
Develop in middle age, leading to death in 12-15 years.

35
Tremor-Rest Tremor: Abolished on movement. Cause: Parkinsonism-Intention Tremor: Irregular, large amplitude, worse at end of purposeful tasks. Cause: Cerebellar
damage-Postural Tremor: Absent at rest. Present on maintained posture (arms outstretched). May persist
(but is not worse) on movement. Causes Benign Essential Tremor.-Re-emergent Tremor: Postural tremor developing after a delay of 10 seconds. Causes: Parkis.
Benign Essential Tremor:Very Common. Inherited (AD). Usually worse in upper limbs. Head & Neck sometimes affected. Worse
on intention. Exacerbated by stress, made better by alcohol.Mx: often unnecessary. B-blockers may help, or anxiolytics/antidepressants.
Physiological Tremor:Can occur in any state of normality or can be exagerated by hyperthyroidism, anxiety, hypoglycaemia,
caffiene excess, fever or medication induced.Usually associated w/ certain postures. Usually bi-lateral, symmetrical, and non-progressive. Should
be absence of other motor symptoms.Drugs: Salbutamol, B-blockers, Lithium.
Movement Disorders
ChoreaNon-rhythmic jerky movements, semi-purposeful movements flitting from one place to another e.g.
facial grimacing, raising shoulders, flexing fingers.Causes: Huntington's Chorea. Sydenham’s Chorea (post Strep), drugs (L-Dopa/neuroleptics),
hypocalcaemia, thyrotoxicosis, SLE, Wilson’s.
Hemi-ballismusLarge amplitude, flinging, hemi-chorea, affecting proximal muscles contralateral to a vascular lesion
of subthalamic nucleus. Recovers spontaneously after a few months.
AkathasiaFeeling of inner discomfort and restlessness, may be confused with anxiety. W/ or w/out movement
disorder.
36
Movement DisordersAthetosisSlow sinuous confluent, purposeless movements (esp digits, hands, face, tongue), often difficult to
distinguish from chorea. Causes: Commonest Cerebral Palsy
MyoclonusSudden involuntary focal or general jerks from cord, brainstem or cerebral cortex.Causes: Metabolic (Asterixis: liver/kidney failure, hyponatraemia, hypercapnia, gabapentin),
neurodegenerative, CJD, myoclonic epilepsy.Mx: Treat underlying cause. May be helped by valproate or clonazepam.
DystoniaProlonged contractions causing abnormal posture or repetitive movements. -Idiopathic generalized dystonia: childhood onset, starts in one leg than spreads to that side of the
body over 5-10 years. Difficult to treat but try anticholinergic or deep brain stimulation.-Focal Dystonia: Typically in adults: idiopathic. Rarely generalize. Worsened by stress. Patients may
develop a gesture to help to try to stop dystonia e.g. touching jaw. Mx: Botulinum injections usually effective.-Writer’s Cramp: Patient able to do other things but get bad contractions when writing. Association: OCD. Mx: B-blockers, valproate ineffective. Breath holding techniques, hand cooling and botulinum
effective.-Acute Dystonia: may occur on starting drugs: neuroleptics, antim-emetics (metoclopramide,
cyclizine), head pulled back, spasm, and eyes drawn up. Mx: Effective treatment with anti-cholinergics.
Tardive SyndromeDelayed onset movement disorders, which cause significant distress and disability and may be
permananet.

37
Tardive SyndromeDelayed onset movement disorders, which cause significant distress and disability and may be
permanent.-Tardive Dyskinesia: Chewing movements in face.-Tardive Dystonia: Sustained stereotyped muscle contractions of a twisting or turning character.-Tardive akathisia: Unpleasant inner sense of restlessness or unease +/- purposeful movements.-Others: Tardive myoclonus, tardive tourettism, Tardive Tremor.
Mx: Slowly remove neuroleptics. If still problem consider: terabenazine.Neuroleptics less likely to cause tardive syndromes: Quietapine, olanzapine, clozapine.
Movement Disorders
Drug Induced Movement DisordersNeuroleptics are drugs that cause a blockade of D2 receptor. This blockade causes extra-pyramidal
side effects by preventing natural blockade on movement groups which is carried out by dopamine.
This causes inappropiate activation of these muscle groups for certain periods of time, causing:-Parkinsonism-Akathasia (Most common cause of non-compliance).-Chorea-Athatosis-Dystonia-Tardive Dyskinesia
Drugs include typical antipsychotics (chlopromazine, haloperidol), also atypical antispychotics. Also anti-emetics (metoclopramide, cylcizine).
Mx: Stop neuroleptic drugs and start anti-cholinergic (choline is stimulatory to muscle groups from extrapyramidal system).
38
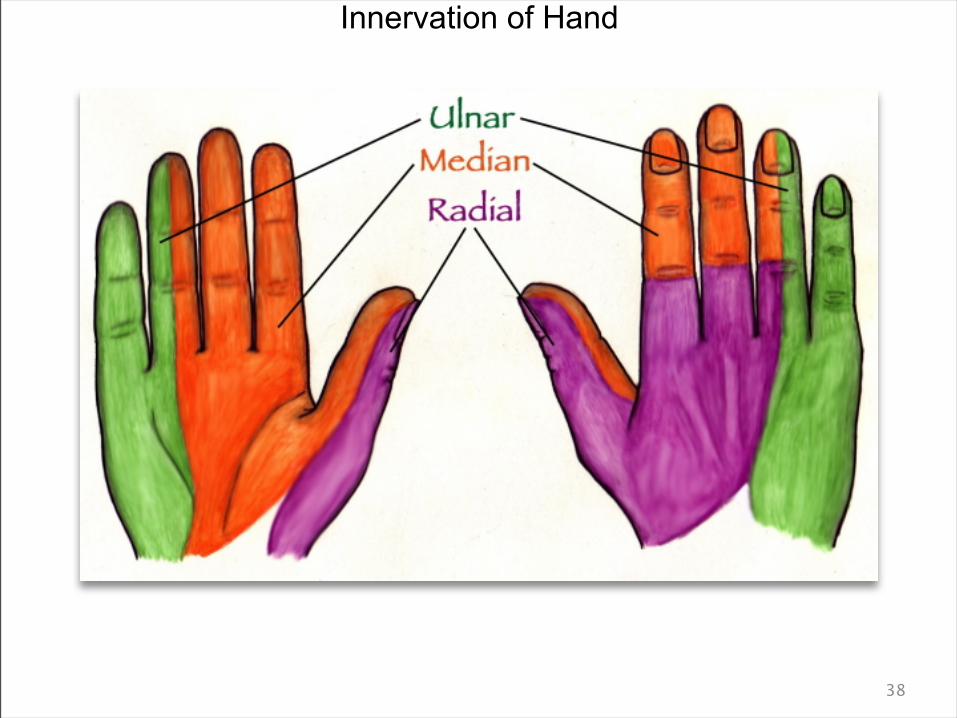
Innervation of Hand
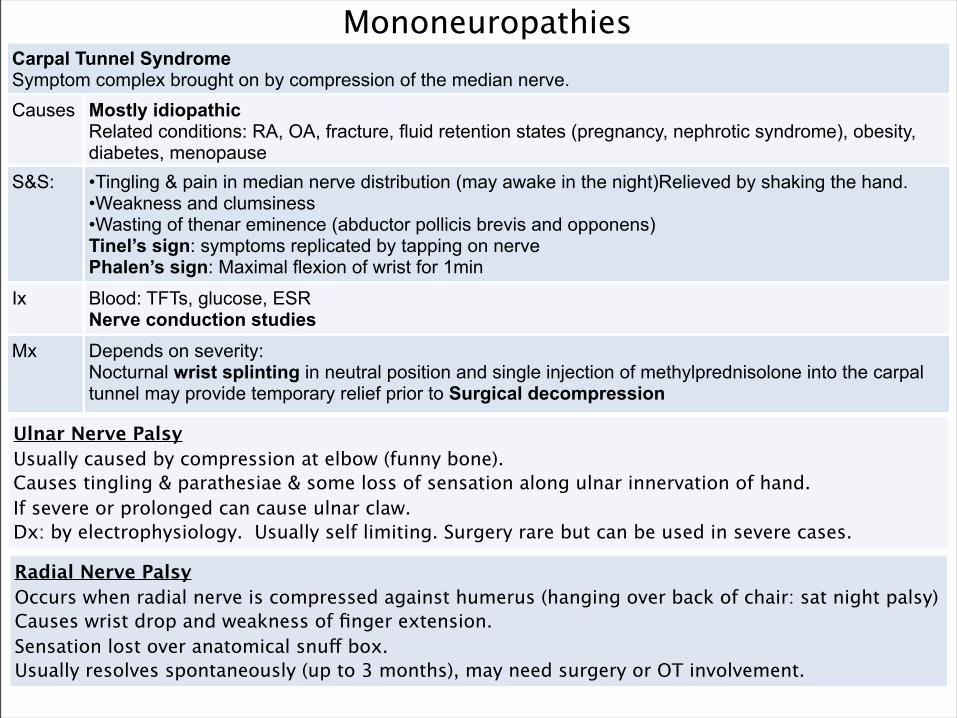
MononeuropathiesCarpal Tunnel Syndrome Symptom complex brought on by compression of the median nerve.Causes Mostly idiopathic
Related conditions: RA, OA, fracture, fluid retention states (pregnancy, nephrotic syndrome), obesity, diabetes, menopause
S&S: •Tingling & pain in median nerve distribution (may awake in the night)Relieved by shaking the hand.•Weakness and clumsiness•Wasting of thenar eminence (abductor pollicis brevis and opponens)Tinel’s sign: symptoms replicated by tapping on nervePhalen’s sign: Maximal flexion of wrist for 1min
Ix Blood: TFTs, glucose, ESRNerve conduction studies
Mx Depends on severity: Nocturnal wrist splinting in neutral position and single injection of methylprednisolone into the carpal tunnel may provide temporary relief prior to Surgical decompression
Ulnar Nerve PalsyUsually caused by compression at elbow (funny bone).Causes tingling & parathesiae & some loss of sensation along ulnar innervation of hand.If severe or prolonged can cause ulnar claw.Dx: by electrophysiology. Usually self limiting. Surgery rare but can be used in severe cases.
Radial Nerve PalsyOccurs when radial nerve is compressed against humerus (hanging over back of chair: sat night palsy)Causes wrist drop and weakness of finger extension. Sensation lost over anatomical snuff box. Usually resolves spontaneously (up to 3 months), may need surgery or OT involvement.

40
MononeuropathiesSciatica Damage to one of 5 nerve roots forming the sacrolumbar plexus (radiculopathy) or lower down to the nerve itself.Causes Spinal disc herniation (other causes of radiculopathy: spinal stenosis, inflammation of disc).
Cauda Equina SyndromePiriformis Disease. 15% of pop sciatic nerve runs through piriformis muscle rather than under it. Swelling of piriformis due to trauma or spasms, compresses the sciatic nerve.
S&S: Pain in lower back, buttock and other parts of leg. Made worse by cold exposure.Associated w/ pain & parathesiae numbness & muscle weakness down course of nerve.Typically unilateral.Symptoms made worse by straight leg lift.
Ix Blood: TFTs, glucose, ESRNerve conduction studies
Mx Depends on cause:-Disc Herniation 90% will recover spontaneously. Surgery if other causes of radiculopathy.-Conservative Mx in pirformis disease (anti-inflammatories & rest).
Common Peroneal Nerve PalsyCompression of nerve at fibular head.Causes: prolonged squatting or leg crossing, tight cast, prolonged bed rest, trauma to side of knee.Causes foot drop and weakness of eversion of foot.Sensory loss to anterolateral border of shin & dorsum of foot.Tibial Nerve PalsyCan be damaged by trauma to ankle or tarsal tunnel syndrome (compression in tarsal tunnel). OA.Tibial nerve damage causes: inability to stand on tip toes (plantar flexion), tingling and pain in sole of
foot. Symptoms may be worse at night. Pain may radiate into calf. Pain may be worse when in extreme dorsiflexion.
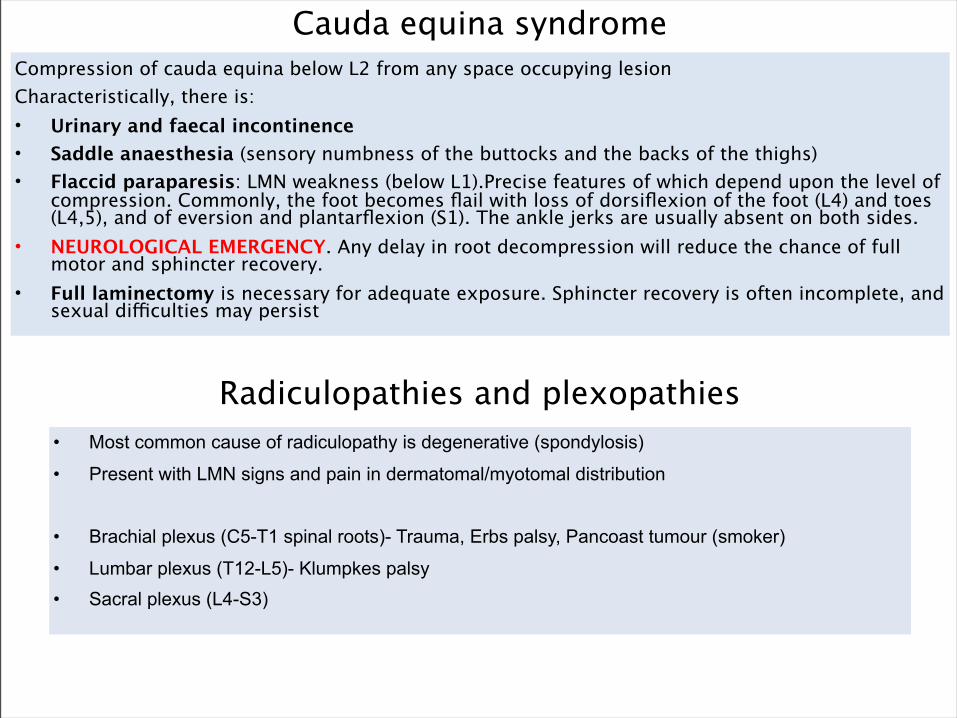
Cauda equina syndromeCompression of cauda equina below L2 from any space occupying lesionCharacteristically, there is:• Urinary and faecal incontinence• Saddle anaesthesia (sensory numbness of the buttocks and the backs of the thighs)• Flaccid paraparesis: LMN weakness (below L1).Precise features of which depend upon the level of
compression. Commonly, the foot becomes flail with loss of dorsiflexion of the foot (L4) and toes (L4,5), and of eversion and plantarflexion (S1). The ankle jerks are usually absent on both sides.
• NEUROLOGICAL EMERGENCY. Any delay in root decompression will reduce the chance of full motor and sphincter recovery.
• Full laminectomy is necessary for adequate exposure. Sphincter recovery is often incomplete, and sexual difficulties may persist
Radiculopathies and plexopathies• Most common cause of radiculopathy is degenerative (spondylosis)
• Present with LMN signs and pain in dermatomal/myotomal distribution
• Brachial plexus (C5-T1 spinal roots)- Trauma, Erbs palsy, Pancoast tumour (smoker)
• Lumbar plexus (T12-L5)- Klumpkes palsy• Sacral plexus (L4-S3)

42
Definition: Organic cause of global deterioration of higher functioning including memory loss (especially short term), cognitive deficits causing impairment in social or occupational functioning. Deterioration follows a progressive decline, without clouding or loss of consciousness.
Epidemiology: 1% in 65-74 years. 10% in >75 years. 25% in >85 years. Presentation: Memory: leaves keys, forgets names, forgets locations. Long-term
memory normally well preserved with loss of short term memory. Behaviour: Change in activities. Personality: Change from calm to anxious, placid to aggressive. Mood change: anhedonia, lethargy, low mood. Also can have specific deficits: Deterioration of language (aphasia), perception & comprehension (apraxia). Inability to recognize objects (agnosia), disturbance in executive functioning: abstract thought, plan, initiate, sequence and stop complex tasks.
Investigations: Aimed at addressing underlying cause. Bloods, CT/MRI. LP. A score of 23/30 or less is generally diagnostic of dementia.
Management: Aimed at support of patient and family. MDT care package: giving dignity and choice to pt and family. Specific care pathway: ways to make life easier e.g. getting pt involved in cleaning/cooking if she has been house wife all life.
Dementia

43
Management:(Medical)
Acetylcholinesterase inhibitors: used for treatment of mild cognitive & behaviour problems. Also slows progression of Alzheimer’s. NMDA antagonists used if AChI are contraindicated or non-tolerated for treatment of severe Alzheimer’s. Management of behaviour problems: olanzapine, risperidone, sodium valporate, carbmazapine, or short acting benzos.
Prognosis: Prognosis is poor. Progressive disease. Death from Alzheimer’s is usually w/in 10 years of diagnosis. Vascular dementia has shorter prognosis, with risk of massive stroke. Death is usually due to bronchopulmonary pneumonia.
Dementia
Alzheimer’s Disease (65%)Generalized atrophy of the brain. Associated with widening of sulci and ventricles. Caused by extracellular B-amyloid plaques and intracellular neurofibrillary tangles. Associated with increasing age, family history, Down’s Syndrome & head Injury. Onset usually >65 years and is relentlessly progressive.Key Features: Short term memory loss, difficulty learning new tasks/information, Dysphasia, dyspraxia, agnosia. Early impairment of sense of smell. Persecutory delusions common.Treatment is mainly with acetylcholinesterase inhibitors which slow the progression.

44
Vascular DementiaMultiple white matter infarcts with cystic tissue around infarcted areas. Reactive gliosis: demyelination of white cell tracts as a consequence. Associated with normal risk factors of CV disease.Causes an acute onset and a stepwise loss of cognition with further infarcts. In between can see periods of recovery but overall follows a similar progressive pathway as in Alzheimer’s. Key features: memory loss, personality change, signs of other vascular disease.Can also get a mixed Vascular and Alzheimer’s dementia.
Lewy Body DementiaDementia caused by eosinophillic intracellular inclusion bodies in the neurons of the brainstem and neocortex. Heavily associated with Parkinson’s disease.Causes fluctuating levels of awareness and cognition which can vary significantly from day to day.Key Features: Will often see mild Parkinsonian symptoms and associated falls are common. Visual hallucinations and delusions are common. Attentional and visuospatial problems more pronounced, while short term memory is more preserved. Associated with intermittent loss of consciousness, REM & sleep disorder.Management: avoid neuroleptic and anti-parkinson drugs (may speed up progression), acetylcholinesterase inhibitors may protect some cognitive function.

45
Frontotemporal Dementia (Pick’s Disease)Severe atrophy of the frontal and temporal lobes with, neuronal loss, gliosis, Pick cells (ballooned neurons) and Pick bodies (argentophillic inclusions). Insidious onset of symptoms, which is relentlessly progressive.Key Features: Frontal lobe psych problems: socially inappropriate behaviour, lack of concern and apathy, aggression. Speech and language problems occur early and progress rapidly. Memory problems are less severe than other aspects and preserved in early disease. Incontinence develops early and parkinsonian features may develop but not to the level of Lewy Body. Visuospatial abilities are usually well preserved.Management: little can be done. Stop CNS drugs (may speed up progression), consider thiamine or vitamin supplements.
Normal Pressure Hydrocephalus (up to 6%)Enlarged ventricles without raised ICP (although raised ICP in early stages of disease, drops of ventricles dilate). 50% of causes for enlarged ventricles unknown. Other common causes include: subarach, meningitis, head injury, CNS tumour. Key Features: Gradually progressive classical triad of symptoms: (1) Gait Disturbance: Due to compression of corona radiata by enlarged vents. Causes parkinson type picture: slow broad-based and shuffling movements but without significant rigidity or tremor. (2) Sphincter disturbance: Due to compression of sacral nerves leaving the brain. Most commonly urinary incontinence but can also effect anus. (3) Dementia: Due to distortion of the periventricular limbic system. Memory loss, inattention, bradyphrenia. Progression is less rapid than in Alzheimer’s. Management: Main: CSF shunt. Other medical treatments. Reversible cause.

Differentiating between the dementiasAlzheimers Usually onset after 65 years.
Relentlessly progressiveSTM loss, difficulty learning/retaining new info. Dysphasia, dyspraxia. Persecutory beliefs are common
Vascular Acute onset.Stepwise deterioration
Memory loss, personality change, Signs of vascular disease elsewhere (including RF’s)
Lewy body Average age- 68 years onset. Variable progression- better prognosis
Movement / Parkinsonian symptoms (bradykinesia more than tremor).Lewy bodies Show on PET scans. Sensitive to antipsychotics. Falls
Frontotemporal dementia eg Pick’s disease
Insidious pre-senile onset usually 50-60 years. Slow progression
Early personality changes. Coarsening of social behaviour, disinhibition, speech disturbance, apathy/ restlessness. Memory preserved in early years
Normal pressure hydrocephalus
After 70 years Dementia with frontal lobe dysfunction. Urinary incontinence. Gait distubance.
CJD Onset often before 65 years. Rapid progression- death within 2 years
Affects all higher cerebral functionsa. Dementia associated with neurological signs: pyramidal, extrapyramidal, cerebellar, aphasia
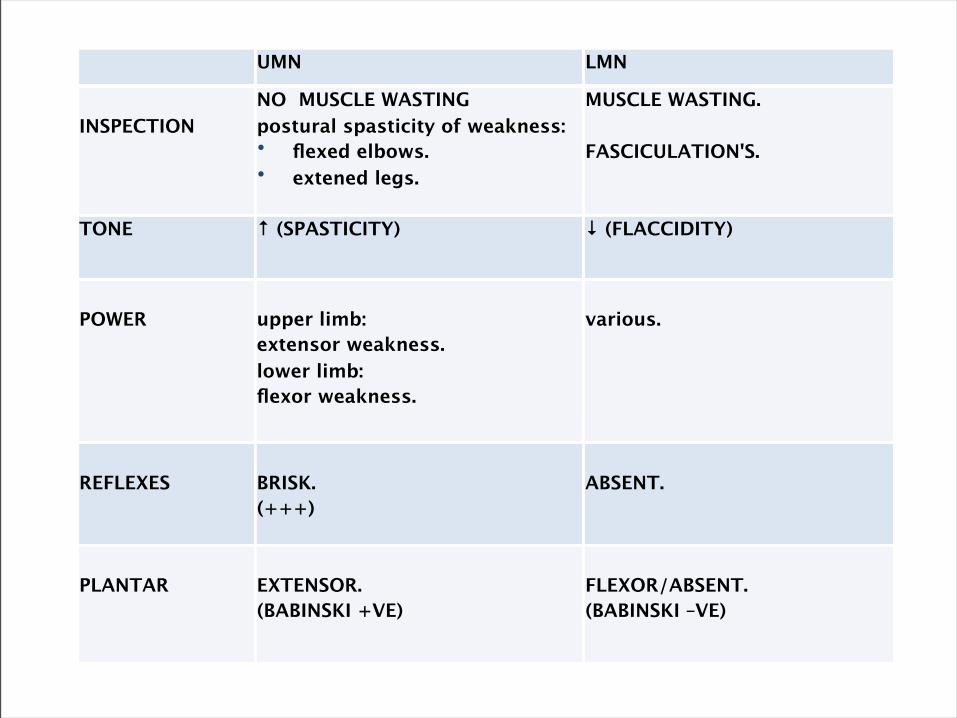
UMN LMN
INSPECTIONNO MUSCLE WASTINGpostural spasticity of weakness:• flexed elbows.• extened legs.
MUSCLE WASTING.
FASCICULATION'S.
TONE ↑ (SPASTICITY) ↓ (FLACCIDITY)
POWER upper limb:extensor weakness.lower limb:flexor weakness.
various.
REFLEXES BRISK.(+++)
ABSENT.
PLANTAR EXTENSOR.(BABINSKI +VE)
FLEXOR/ABSENT.(BABINSKI –VE)

Group of degenerative conditions which cause selective damage & loss of motor neurons.The disease affects both upper and motor lower neurons but with sparing of sensory neurons & sphincters.Also MND never affects eye movements.Motor Neuron damage occurs in: the motor cortex, cranial nerve nuclei & anterior horn cells.4 Clinical Patterns:1) Amytrophic Lateral Sclerosis (ALS): Most common form. Increased risk in post Gulf War vetrans. Affects motor cortex & anterior horn cells so UMN &LMN signs.2) Progressive Bulbar Palsy (2nd most common): Only affects cranial nerves IX-XII. Often progresses to ALS.3) Progressive Muscular Atrophy (3rd): Anterior Horn cell lesion only so only LMN signs. Distal-proximal muscle involvement. Better prognosis than ALS.4) Primary Lateral Sclerosis (4th): Damage primarily to motor cortex so mainly UMN signs with marked spastic leg weakness & pseudobulbar palsy.
Aetiology: Cause is unknown, but suggested viral trigger. Less than 10% familial.
Epidem: Annual Incidence of 2 cases/100,000. Prevalence 5-7/100,000. Peak >50. M:F 2:1.
Presentation ALS: Mixed UMN & LMN signs in one of three recognised patterns:-Limb onset (vast majority of cases).Upper Limb: dropping objects, difficulty manipulating objects (turning keys), wrist drop, weakness or cramping of hands, wasting & fasiculations.Lower Limb: Foot drop, gait disorder, heaviness of legs, falls, difficulty rising from sitting/climbing stairs, fatigue when walking.-Bulbar onset (20% of cases) Symptoms as listed next page.-Respiratory Onset (Least common). Dyspnoea & orthopnea due to hypoventilation at night.Main features: Fasiculating, wasted & weak area w/ brisk reflexes w/out sensory loss.
Ix: No particular investigation to diagnose MND.-Nerve Conduction Studies: normal nerve condution-EMG: Shows fibrillation & fasciculation (classical pattern).-CT/MRI, blood tests & muscle biopsy: rule out other pathologies.
Motor Neuron Disease

Mx: MDT: Neurologist, GP, Palliative Care, SALT, OT, Physio, Psychological Services.-Riluzole: Glutamate-release inhibitor): Costly, prolongs life by 2-4 months. Best effects seen by reducing tracheostomy-free time. Started by specialist. Quite well tolerated.-Drooling: anticholinergics: hyoscine or amitriptyline. -Muscle Cramps/Spasticity: Diazepam, baclofen, quinine.-Dysphagia: Blend food, NG tube, PEG feeding.-Joint Pains & Distress: Analgesic Ladder.-Depression: anti-depressants.-Non-invasive ventilation: Used over-night. Significant improvement. NICE recommends.
Comps: Respiratory failure, pneumonia, UTI, Cognitive Impairment (fronto-temporal dementia).Constipation, Spasticity & muscle cramps, depression, loss of speech, immobility.
Prognosis: Usually rapidly progressing & fatal. Median Survival: 3-5 years.90% die in sleep due to hypercapnia (patients worry about choking to death: doesn’t happen).Small group (10-20%) have early onset disease, which is slowly progressing.
Bulbar Symptoms: LMN damage to cranial nerves IX-XII.This means LMN signs of the tongue & muscles of talking & swallowing.This causes: flaccid, fasiculating tongue, normal/absent jaw jerk, slurred, quiet speech, which is hoarse/nasal.Difficulty eating, drooling, dysarthria, dysphonia, choking, pulmonary aspiration.Causes: MND, GBS, polio, MG, syringobulbia, brainstem tumours, central pontine myelonsis.
Pseudo-Bulbar Symptoms: UMN damage to cranial nerves IX-XII.Commoner than bulbar palsy. Due to bilateral lesions above mid-pons e.g. corticobulbar tracts.This causes: Slow tongue movements, slow deliberate speech, increased jaw jerk & pharyngeal & platal reflexes. Emotional Incontinence: mood incongruent weeping or laughing. (Also seen in MS, dementia & head injury).
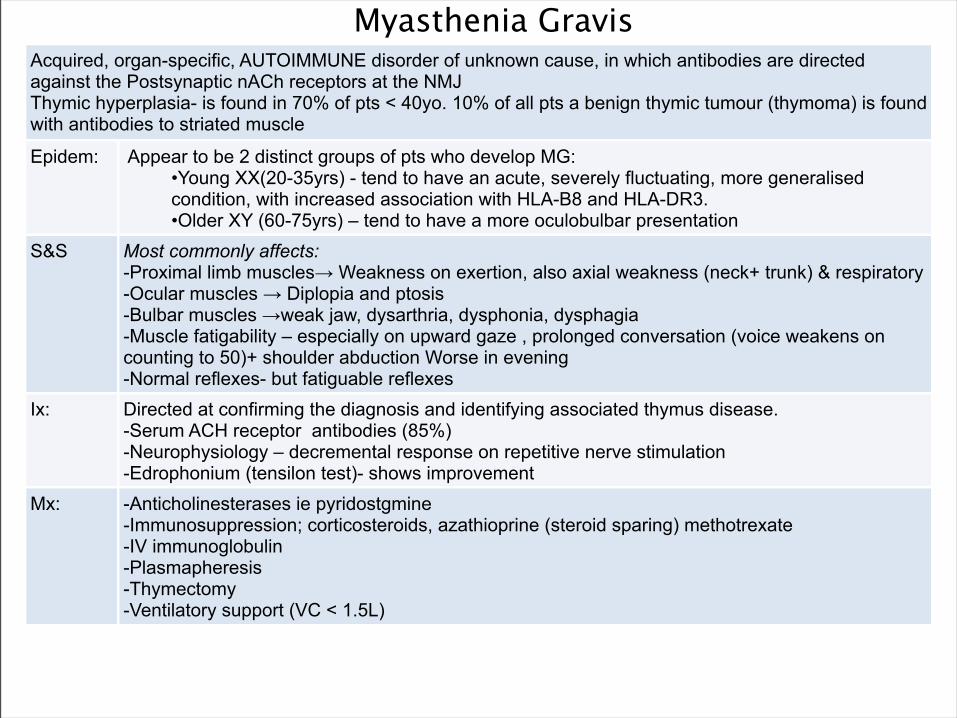
Myasthenia GravisAcquired, organ-specific, AUTOIMMUNE disorder of unknown cause, in which antibodies are directed against the Postsynaptic nACh receptors at the NMJThymic hyperplasia- is found in 70% of pts < 40yo. 10% of all pts a benign thymic tumour (thymoma) is found with antibodies to striated muscle
Epidem: Appear to be 2 distinct groups of pts who develop MG:•Young XX(20-35yrs) - tend to have an acute, severely fluctuating, more generalised condition, with increased association with HLA-B8 and HLA-DR3.•Older XY (60-75yrs) – tend to have a more oculobulbar presentation
S&S Most commonly affects:-Proximal limb muscles→ Weakness on exertion, also axial weakness (neck+ trunk) & respiratory -Ocular muscles → Diplopia and ptosis-Bulbar muscles →weak jaw, dysarthria, dysphonia, dysphagia-Muscle fatigability – especially on upward gaze , prolonged conversation (voice weakens on counting to 50)+ shoulder abduction Worse in evening-Normal reflexes- but fatiguable reflexes
Ix: Directed at confirming the diagnosis and identifying associated thymus disease.-Serum ACH receptor antibodies (85%)-Neurophysiology – decremental response on repetitive nerve stimulation-Edrophonium (tensilon test)- shows improvement
Mx: -Anticholinesterases ie pyridostgmine-Immunosuppression; corticosteroids, azathioprine (steroid sparing) methotrexate-IV immunoglobulin-Plasmapheresis-Thymectomy-Ventilatory support (VC < 1.5L)

Multiple SclerosisAn autoimmune inflammatory disease with multiple areas of demyelination affecting white matter tracts in the CNS, leading to scarring. Episodes of demyelination are separated by time and space so the disease classically follows and relapsing and remitting pattern before eventually becoming progressive. Unknown Cause: thought to be a mix of genetics, environment, infection.-Relapsing & Remitting (90%): Lesions at different times with recovery inbetween.-Secondary Progressive (50% of relapsing remitting): Time between each episode becomes shorter until continuous. -Primary Progressive (10%): Little or no recovery from episodes with progressive disability from onset.
Epidem: More common in temperate regions. 60-100 cases/100,000.Peak usually 20-30. F>M.
S&S: -Fatigue-Eyes: Unilateral optic neuritis (central scotoma and pain on ocular movement- recovery over a few weeks) Intranuclear opthalmoplegia (failure of conjugate gaze- damage to MLF), Diplopia, Relative afferent pupillary defect (fails to constrict with light). Optic atrophy/ papillitis/ retrobulbarneuritis also-Skeletal Muscles: Numbness & tingling, Ataxia, Weakness (usually in legs) and spasticity→ paraparesis (recurrent & in different nerves)-Other Brainstem + cerebellar involvement:, Nystagmus, vertigo, dysarthria, dysphagia, intent tremor-Smooth muscles: (SC presentation)- Bladder- Frequency, urgency, incontinence•Worse in heat or exercise (Uthoff’s phenomenen).•Lhermitte’s sign: electrical sensation in spine on neck flexion.
Ix: -MRI- demyelination often in periventricular regions (lesions separated in time and place)-LP- high protein+ oligoclonal bands (CSF but not serum) -NCS and EPs (visual, somatosensory and brainstem auditory EP’s)- slow
Mx: NO CURE. Acute relapse: Methyprednisolone pulsedProphylaxis: Βeta-interferon –reduces relapse rate - may slow disability+ glatiramir.Palliation: baclofen, diazepam, botox, intermittent self catheterisation, anticholinergics

Guillain-Barre syndromeAcute inflammatory demyelinating polyneuropathyPost infective: Recent (within 3 weeks) respiratory infection (Mycoplasma pneumoniae) / diarrhoea (Campylobacter jejuni)Can also occur in autoimmune diseases (ie SLE)
S&S Prodromal malaise with headache, fever+ limb pains is surmounted by a progressive + ascending, symmetrical limb weakness/paralysisParaesthesia (distal)Can have bulbar involvement
Ix: •Nerve conduction studies/ EMG (↓ conduction velocities- often a later sign)•LP (↑ CSF protein after 2-3 week of illness)•Blood: Antibodies + virology (test for C. Jejuni)
Mx: Supportive: IV Immunoglobulins (IVIG) , PlasmapheresisTracheostomy/ Ventilation if respiratory muscles are involved/ VC <1 litrePhysiotherapy + NG feed
Prognosis VariableMortality 8%5% develop chronic disease (CIDP) which runs a relapsing+ remitting course
Miller- Fisher syndrome is a proximal variant

Duchenne’s Muscular Dystrophy (DMD)X-linked recessive disorder- 1/3rd of cases do arise by spontaneous mutationGene locus is Xp21 region of the X chromosomeAbsence of gene product (lack of protein dystrophin): Dystrophin is essential for stability of the cell membrane
S&S: No abnormality at birth, Usually evident by the 4th yearDifficulty in runningDifficulty in arising to an erect position from the floor – uses hands to climb up (Gower’s sign)Initially proximal limb weakness –with pseudohypertrophy of the calves (champagne bottles)Weakness eventually spreadsMyocardium is affectedSeverely disabled and wheel-chair bound by aged 10Death usually occurs by the age of 20 – usually due to respiratory failure or cardiomyopathy
IX: Diagnosis often on clinical grounds aloneCreatine phosphokinase (CK) is grossly elevated (x100-200 normal limits)Muscle biopsy characteristics: Variation in fibre size, Fibre necrosis, Regeneration of fibres, Replacement by fat, Immunochemical staining shows absence of dystrophinEMG – myopathic pattern
Mx: NO CUREPassive physiotherapy to prevent contracture in later lifeCarrier detectionAccurate carrier status and prenatal diagnosis – using cDNA probesGenetic advice – explaining inheritanceDetermination of foetal sex by amniocentesis (selective termination of male foetus’)
Becker’s Muscular Dystrophy (BMD): Also X-linked recessive disorder. Similar characteristics to DMD Much milder course- dystrophin is altered rather than absent.Presentation is not usually until later- Boys continue to walk in their teens and early adult lifeCramps associated with exercise are common. Cardiomyopathy is usually worse than the weakness

Inflammation of the meninges. Typically caused by an infective agent; bacteria, virus, fungiInfection can reach the meninges from direct spread eg sinuses, nasopharynx or inner ears, Cranial injury (skull fracture),congenital meningeal defects and the bloodstream.80% <16yrs. Uncommon in neonates but mortality is up to 50%
COMMON BACTERIA (varies with age)Neonatal→3months: GBS,E.coli and other coliforms eg. Klebsiella Listeria Monocytogenes. Older children and adults: Neisseria Meningitidis, Strep Pneumoniaie, Haemophilus influenzaeElderly: Strep Pneumoniaie, ListeriaVIRAL Enteroviruses, CMV, Coxsackie, Mumps, HSV, EBV, HIV, adenovirusesFUNGAL: Cryptococcus neoformans, CandidaAlso: TB ,Malignancy, Autoimmune
Rfs: Impaired immunity: young age, defects of complement system, splenic defect: Factors associated with low socioeconomic status: crowding , poverty, and close contact (droplet spread)
S&S: Headache, Photophobia, Neck stiffness, Fever +/- rigors (may be absent in ‘aseptic’ meningitis), Vomiting, Signs of shock , Focal neurological signs
Non-blanching petechial (purpuric rash)- Meningococcal sepsisLethargy/drowsiness/LOC/Coma/SeizuresOther signs of ↑ICP: papilloedema, ↑bp with↓pulseKERNIG’S SIGN: Child lying supine+hips and knees flexed, back pain on knee extensionBRUDZINSKI’s SIGN: Flexion of neck with patient supine causes knee and hip flexion
Ix: FULL SEPTIC SCREENBloods: ↑WBC, ↑CRP, U+E, LFTs, glucose, lactate, clotting studies, G+S, ABGsM,C+S : Blood , stool, throat swab, urineRapid antigen screenLP for CSF (accept where contraindicated)CT /MRI scanIf TB suspected (Mantoux test), CXR
Meningitis

Mx: •Bacterial= Medical emergency1. ABC, Oxygen, 2. Start antibiotics immediately if septicaemia is suspected (3rd generation cephalosporin ie
Cefotamime/ceftriaxone). Benzylpenicillin if in community3. Corticosteroid treatment: improvement in morbidity and LT complications by reducing
inflammation and immune response4. Supportive: analgesics + antipyretics
•Non-bacterial causes: •Fungal – amphotericin and fluclonazole•TB- rifampicin, isoniazid•Viral- self limiting + benign
•Contact Consultant in communicable disease control (CCDC) Notifiable disease, Contact prophylaxis, Later Immunisations (BCG, Men C vaccine +HiB)•Contact Prophylaxis: Rifampacin.
Meningitis
Glucose Protein WBC Cell Differential Opening Pressure
Bacterial: ⬌/⬇ ⬆ ⬆ Predominance of Neutrophils ⬆
Viral: ⬌ ⬌/moderate ⬆ ⬆ Early: NeutrophilsLate: Lymphocytes ⬌
Tuberculosis(+ve culture) ⬇ ⬌/moderate ⬆ Variable Predominance of
Lymphocytes Variable
Fungal+ve fungal culture ⬇ ⬆ Variable Predominance of
Lymphocytes Variable





























