Embed Size (px)
DESCRIPTION
Neuropathic features and Neurological complications seen in CRF . Identifying them and treating them.
Citation preview
Neurological Complication of Chronic Renal FailurePresenter –Dr Prakash Harischandra
Moderator- Dr B.P ShelleyProf & HOD Neurology , YMC

• Neurological complications occur in almost all patients with severe CKD, potentially affecting all levels of the nervous system, from the CNS through to the PNS.
• Patients on dialysis tend to be weaker and less active, and to have reduced exercise capacity, when compared with healthy individuals Cognitive impairment, peripheral and autonomic neuropathy are also seen.

Overview
• Neurological Complications due to Uremic state or due to its treatment can manifest as symptoms
• Despite Rx, uremia, like uremic encephalopathy, atherosclerosis,neuropathy and myopathy , dialysis dementia, dysequilibrium syndrome, aggravation of atherosclerosis, cerebrovascular accidents are seen

overview
• hypertensive encephalopathy, Wernicke’s encephalopathy,
• hemorrhagic stroke, subdural hematoma, osmotic myelinolysis, opportunistic infections, intracranial hypertension and mononeuropathy.
• Transplantation, Immunosuppresion can give rise to newer infections


CNS EncephalopathyIn patients with renal failure, encephalopathy is common-may be caused by uremia, thiamine deficiency,dialysis, transplant rejection, hypertension, fluid and electrolyte disturbances or drug toxicity -It is often associated with headache, visual abnormalities, tremor, asterixis, multifocal myoclonus, chorea and seizures. These signs fluctuate from day to day or sometimes from hour to Hour-Uremic encephalopathy may accompany acute or chronic• renal failure, Sx worsen rapidly with deterioration. “uremic
twitch convulsive”syndrome can be seen• Hemodialysis Improves Sx . EEG is non diagnostic but when
done serially can give a prognostic value. Neuroimagin not Essential.
Cognitive Dysfunction
• Cognitive dysfunction increases in prevalence with CKD severity, potentially affecting up to 80% of patients
• Cognitive impairment in CKD not only increases the risk of mortality, but also has major implications for informed consent in relation to dialysis initiation and maintenance, and, ultimately, renal transplantation

Acute Cognitive impairment• In addition to chronic cognitive dysfunction and dementia, acute
disturbances of cognition are prevalent in CKD. In the early days of dialysis, these acute disturbances frequently took the form of the dialysis disequilibrium syndrome
• Acute disturbances in cognitive function typically relate to metabolic abnormalities that complicate the uremic state, including electrolyte disturbances (for example, hypercalcemia, hypophosphatemia and hyponatremia), acute fluid shifts during dialysis, which lead to cerebral hypoperfusion, and malignant hypertension
• global cognitive function varied markedly, with the greatest impairments being noted during the dialysis session, particularly with regard to memory, executive functioning and verbal fluency.
Chronic Cognitive Impairment & Dementia
• Moderate renal impairment that does not require dialysis is also associated with a significantly increased risk of dementia
• Cognitive tests demonstrate objective evidence of moderate to severe cognitive impairment in 70% of patients with CKD, with dysfunction most commonly noted in the domains of memory and executive function.
Dialysis Dementia
• Dialysis dementia is a term reserved to describe a syndrome of progressive dementia related to aluminum intoxication and first described several decades ago when aluminum contamination of dialysate fluid and the use of aluminum-containing binders were more prevalent; however, this disorder is now rare.

Pathophysiology of Cognitive Impairment
• high incidence of clinically silent cerebrovascular disease, MRI studies have shown that clinically silent white matter disease is present in 50% of patients with CKD, compared with 10% in the general population Traditional and non traditional vascular risk factors (inflammatory mediators)
• Modern techniques of water purification and the use of non- aluminum phosphorus binders have, however, made aluminum intoxication a rare complication of CKD
• Potential roles of secondary hyperparathyroidism and anemia as risk factors for cognitive impairment, Increased PTH – neurotoxic

Clinical evaluation of dementia
The MMSE is the best known cognitive test for dementia A score below 24 (out of a maximum score of 30) has a sensitivity and specificity of greater than 80% for dementia detection in the general population.Other cognitive tests that can be administered in 5 minutes or less, such as the clock drawing task, the Minicog (consisting of the clock drawing task plus uncued recall of three words), the Short Portable Mental Status Questionnaire, have similar performance characteristics in the general population

Management of Cognitive Impairment
• Improvements in cognition in relation to baseline values were demonstrated 6 months after transplantation
• Improvements in both neuropsychological tests, such as the Mini-Mental State Examination, and neurophysiological markers of cognitive function, as measured using evoked potential latencies and EEG rhythms
• Although kidney transplantation is optimal therapy for most patients with ESRD, many patients with chronic cognitive impairment may not be eligible for transplantation Intensification of the dialysis regimen remains a potential management strategy

CNS - Encephalopathy
is a common problem that may be caused by uremia, thiamine deficiency, dialysis, transplant rejection, hypertension, fluid and electrolytedisturbances or drug toxicity . Seen both in ARF & CRF , Sx more Pronounced in ARF.EEG findings in uremic encephalopathy are non-specificbut correlate with clinical symptoms and therefore may be of diagnostic value especially if serial studies are performed.

EEG in uremic excessive encephalopathy showing showing generalised slowing with an excess of delta and theta waves and
bilateral spikes.• EEG from a patient with uraemic encephalopathy.The recording is predominantly δ
(4-8 Hz) and θ (4 Hz)wave activity, with no normal α (>8-13 Hz) or β (>13 Hz)waves
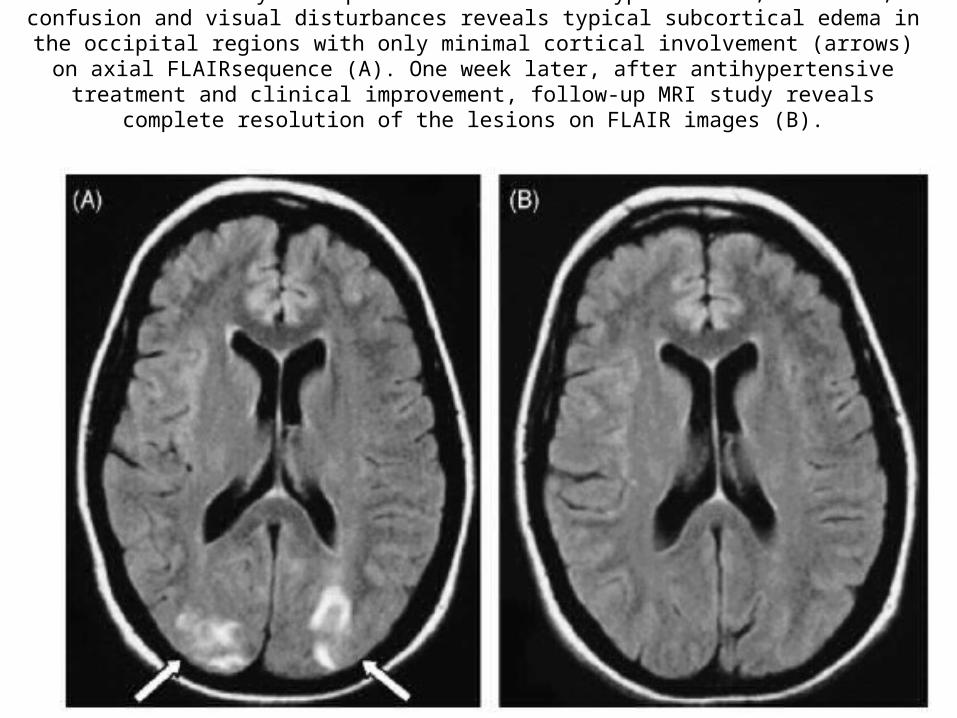
Initial MRI study in a patient with severe hypertension, headache, confusion and visual disturbances reveals typical subcortical edema in the occipital regions with only minimal cortical involvement (arrows) on axial FLAIRsequence (A). One week later, after antihypertensive treatment and clinical improvement,
follow-up MRI study reveals complete resolution of the lesions on FLAIR images (B).

Management of Encephalopathy
• After other causes of delirium have been ruled out, prompt treatment of uremic encephalopathy with initiation or intensification of renal replacement therapy is indicated.
• Resolution of symptoms typically occurs within days.• Correction of anemia (i.e., hemoglobin <10 g/dL) may
also be of benefit.• Dietary protein restriction is another adjunctive
measure used to delay the development of uremic symptoms,

Dialysis disequilibrium syndrome
• Attributable to the dialysis procedure itself and is seen during or shortly after the first several dialysis treatments.
• It is most likely to occur in pediatric or elderly patients, patients with severe azotemia, and patients undergoing high-efficiency hemodialysis
• However, it has also been reported in patients undergoing peritoneal dialysis and maintenance hemodialysis
• Dialysis dysequilibrium is characterized by symptoms of headache, visual disturbance, nausea, or agitation and in severe cases, delirium, lethargy, seizures, and even coma.

Stroke
• Compared with the general population, stroke event rates and stroke mortality rates are increased six- to 10- fold among patients on dialysis
• Like the general population, ischemic stroke is more common than hemorrhagic stroke
• Posterior circulation strokes involving the vertebrobasilar system occur more commonly in patients on dialysis than in the general population

Stroke Risk in ESRD• Kidney transplantation is associated with 30% lower risk for stroke or TIA
compared with patients remaining on the transplant wait list, allograft failure increases the risk for stroke or TIA by 150%
• Traditional risk factors with Proteinuria was associated with a 50% to 70% increased risk for stroke (meta- analysis of stroke cohort studies involving more than 140,000)
• Dialysis related factor • Intradialytic hypotension • Overcorrection of anemia, especially in the setting of ultrafiltration, may
lead to vascular stasis and thrombosis – requires anticoagulation • Imaging Non Contrast CT . gadolinium-enhanced MR angiography must be
carefully weighed against the potential benefits of the imaging procedure, Safety, efficacy, and practicality of thrombolytic therapy in the setting of CKD and ESRD remain unclear
Osmotic myelinolysis• Normally in central basis pontis, but extrapontine regions including
the midbrain, thalamus, basal nuclei and cerebellum can be affected as well.
• Clinically –progressive Quadriplegia, Dysarthria, dysphagia, Altered Consciousness, Vertical Gaze palsy
• Parkinsonism-Basal Ganglia or ataxia - cerebellum affected.• MRI, T2-show hyperintense patchy areas of demyelinationUsually Fatal, If survives, maximum recovery may require several months. Rx is supportive only. • postulated that glial cell edema, which is caused by fluctuating
osmotic forces, results in compression of fiber tracts and induces demyelination and eventually cell death
.

Movement disorders and restless legs syndrome• Can be seen due to Encephalopathy,Drugs or Structural lesions.• Asterixis or “flapping tremor” due to cortical dysfunction which mimic drop
attacks.• Typical movement disorder in uremic encephalopathy is the uremic “twitch-
convulsive” syndrome that consists of intense asterixis and myoclonic jerks that are accompanied by fasciculations, muscle twitches and seizures
• Thiamine deficency can casue basal ganglia degenration, movement disorder – Chorea.
• Rx induced Movmnt disorders seen in post Renal transplant Patients . Tacrolimus like drugs causing EPS Sx.
• RLS is also seen commonly, 20% of patients• dialysis does not substantially improve uremic restless legs syndrome, but cool
dialysate fluid (36.5C) Rx with levodopa, dopamine agonists, benzodiazepines, gabapentin, clonidine or opioids
• improvement of RLS symptoms after kidney transplantation has been described • The etiology is uncertain, but the association with peripheral neuropathy and CRF
is well known.

Opportunistic Infections
• Nocardia asteroides, Mycobacterium tuberculosis and Listeria monocytogenes
• Cryptococcus neoformans, Aspergillus fumigatus, Candida, Pneumocystis carinii, Histoplasma, Mucor and Paracoccidioides species
• Reactivation of latent viral infection with herpes simplex, cytomegalovirus and JC Polyomavirus are not uncommon
• severe , rapid progressive dementia, ataxia, visualdisturbances and other focal neurologic deficits, generally-vegetative state within 6 months

Neoplasms• Immunosuppresive states predisposition to opportunistic infection• De Novo Neoplasia• malignant meningioma, primary central nervous system lymphoma• Immunosuppressive therapy after renal transplantation , increased
risk of lymphoproliferative disease.• majority of post-transplantation (PTLD) are of B-cell origin and
contain EBV. poor clinical outcome • CNS involvement was predominant prior to the use of cyclosporine,
currently thoracic, and abdominal are common. • Radiotherapy is often applied for locations in the central nervous
system. Acyclovir,• surgical excision, several combinations of chemotherapeutic agents • monoclonal antilymphoma immunotherapy• With the increased incidence of urogenital, gastrointestinal,
hematologic and endocrine neoplasia expect a higher risk of brain metastasis

Intracranial hypotension
• Orthostatic headache, occasionally associated with neck stiffness, nausea, visual disturbances, dizziness, hearing loss or 6th Nerve palsy
• S/o Hypotension – due to reduced CSF . Subdural haematoma could mimic this . Imagin required. CSF pressured to be Measured.
• Can be due to CSF leak , Dehydration, Uremia
Intracranial Hypertension
• Could be primary or sec due to Steroids or Neiplasms• Raised ICH -headache, transient visual obscurations, &
diplopia due to unilateral or bilateral sixth nerve palsy• dizziness, nausea, vomiting, tinnitus.• papilledema and progressive optic atrophy with
accompanying constriction of the visual field, loss of colour vision and eventually blindness
• Rx Goal reduce ICH – Acetozolamide, furosemide, Steroids.Shunting can be done.

Neuropathy
Neuropathy• Peripheral neuropathy• Carpal tunnel syndrome• Autonomic neuropathy• Pruritis
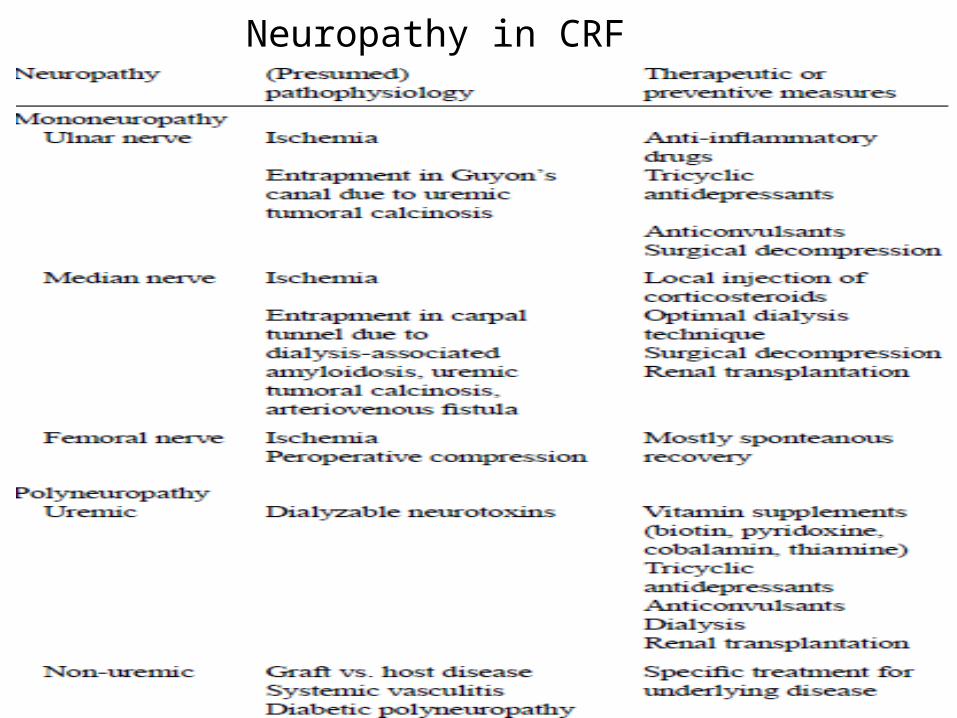
Neuropathy in CRF

Peripheral neuropathy
About 50 per cent of patients starting treatment had clinical evidence of a peripheral neuropathy in early days of dialysis Because of earlier initiation of dialysis these days, neuropathy is usually asymptomatic Nerve conduction abnormalities have been reported in up to 60% of patients receiving dialysis Abnormalities in motor nerve conduction velocity parallel the decline in GFR Uremic neuropathy is a distal, symmetric, mixed sensorimotor polyneuropathy.Loss of ankle vibration sensation and the ankle jerk are often the first manifestations, progressing to a burning sensation in the feet, followed by motor deficit, such as weakness of ankle dorsiflexion

• Wasting of intrinsic hand muscles, with prominentbilateral atrophy of thenar muscles, in a patient withsevere neuropathy resulting from chronic kidneydisease
Pathophysiology of uraemic neuropathy
• Typically the large diameter axons in the distal nerve trunks supplying the legs are affected, with relative sparing of the unmyelinated and the small myelinated afferent neurons.Predominant defect is one of axonal loss with secondary demyelination Repeated episodes of demyelination followed by remyelination - onion like structures on nerve biopsies

• Thiamine Defcient • Clinical symptoms and nerve conduction
parameters improve rapidly following renal transplantation, often within days of surgery Rapidity of these changes suggests that toxin-mediated blockade of neural transmission has an important role in the neurological dysfunction associated with CKD.

Diagnosis of uremic neuropathy
• First step in the diagnosis of uremic neuropathy is to exclude other causes of neuropathy
• Serological testing should be undertaken to exclude vas-culitic neuropathy in those rapidly evolving weakness
• Nerve conduction studies (NCS) remain the gold standard in the diagnosis of uremic neuropathy.
• NCS demonstrate generalized neuropathy of the axonal type, with reductions in sensory amplitudes > motor amplitudes Sural sensory amplitude is the most sensitive indicator of uremic neuropathy
• Systemic diseases that contribute to ESRD and also affect nerve function
• Diabetes mellitus • Amyloidosis • SLE • Transplantation Provides a treatment option• Recovery seen in 3-6 months .

Carpal tunnel syndrome
• Attributable to dialysis-associated amyloidosis or ischemic mononeuropathy associated with an arteriovenous fistula.
• Pain is typically worse at night and during haemodialysis.
• Eventually weakness of thumb abduction occurs with wasting of the thenar eminence. CTS is more common in ,middle aged and older women , diabetics , patients with hypothyroidism ◦ patients on dialysis > 7 years

CTS in CRF
• Diagnosis of CTS can be confirmed by measuring a delay in median nerve conduction across the wrist, and also by ultrasound of the wrist demonstrating bone cysts and distortion of the flexor tendons Haemodialysis with a high flux polyacrylonitrile, or haemodiafiltration, have been reported to reduce the deposition of β2- microglobulin
Autonomic neuropathy• Autonomic dysfunction is a common and potentially life-threatening
complication of CKD, and can occur in the absence of length-dependent uremic neuropathy.
• More common in diabetics and elderly patients Cardiovascular autonomic dysfunction in CKD is associated with an increased risk of cardiac arrhythmia and sudden cardiac death
• Impotence remains the most common symptom of autonomic dysfunction in CKD Other common clinical features include bladder and bowel dysfunction, impaired sweating, and orthostatic intolerance
• Intradialytic hypotension, Renal transplantation leads to considerable improvement in autonomic function
• Sildenafil , midodrine can be used to alleviate Sx.
Uremic Myopathy
• Leads to proximal muscle weakness and wasting, predominantly in the muscles of the lower limbs Uremic myopathy typically develops with glomerular filtration rates of <25 ml/min,
• been associated with fatigability and reduced exercise capacity
• EMG and creatine kinase levels are generally normal, and the diagnosis is, therefore, made largely on clinical grounds.
• Muscle biopsy tends to demonstrate nonspecific features, including type II fiber atrophy with internalized nuclei and fiber

myopathy
• Possible etiologies include :- Hyperparathyroidism,
• Metabolic bone disease with vitamin D deficiency
• Impaired potassium regulation • Accumulation of uremic toxins • Carnitine deficiency, which can lead to
mitochondrial dysfunction ◦ Malnutrition
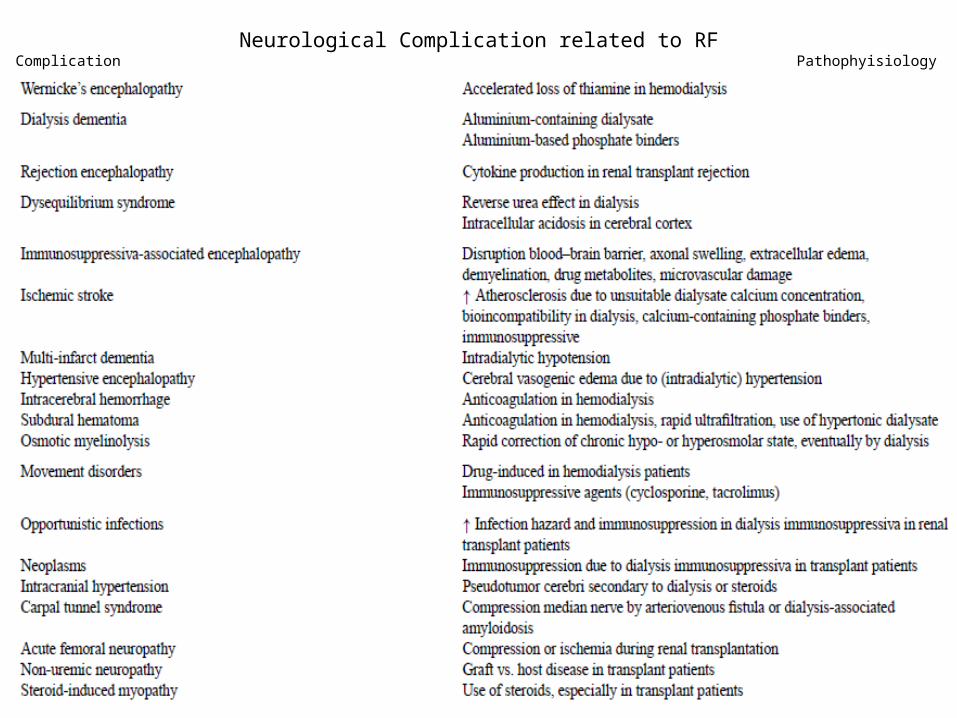
Neurological Complication related to RFComplication Pathophyisiology

Encephalopathy in Renal FailureType Pathophysio Rx
Summary • Presentation in acute delirius/ confusional state is common in
CKD patients and can have wide array of differential diagnosis.• Cognitive impairment is common in patients on dialysis,
typically manifesting as a vascular-type dementia with prominent deficits in executive function
• Renal transplantation improves cognitive function, peripheral neuropathy and autonomic neuropathy
• Stroke is a common factor adding to morbidity and mortality in these patients. Management strategies – unclear
• Uremic toxin mediated disturbances in resting axonal membrane potential leads to length-dependent neuropathy in CKD
• Polyneuropathy, Mononeuropathy, Autonomic neuropathy
Conclusion
• Neurological complications whether due to the uremic state or its treatment, contribute largely to the morbidity and mortality in patients with renal failure.
• Despite continuous therapeutic progress, most neurological complications of uremia
fail to fully respond to dialysis and many are elicited or aggravated by dialysis or renal transplantation.
Refrences• Neurologic complications in chronic renal failure: a retrospective study
Clin Pediatr (Phila).1990 Sep;29(9):510-4. Uysal S, Renda Y, Saatci U,Yalaz K
• Neurological Complications of Chronic Kidney Disease Arun V. Krishnan, PhD, FRACP; Matthew C. Kiernan, PhD, FRACP- Medscape
• Neurological complications in renal failure: a review R. Brounsa,b, P.P. De Deyna,b, Clinical Neurology and Neurosurgery 107 (2004) 1–16∗




![Delayed Recurrent Encapsulated Pneumocephalus: A Case ...complication and can occur delayed after neurological surgery [12]. The radiographic modality of choice is the CT scan. It](https://img.dokumen.tips/doc/110x75/60e24969f373e343c40946f9/delayed-recurrent-encapsulated-pneumocephalus-a-case-complication-and-can-occur.jpg)


![Successful recovery without any neurological complication ... · PDF fileneurological complication after intraoperative cardiopulmonary ... prone CPR [1], ... Extracorporeal CPR seemed](https://img.dokumen.tips/doc/110x75/5ab6fdce7f8b9ab7638e558a/successful-recovery-without-any-neurological-complication-complication-after.jpg)











![Dialysis Disequilibrium Syndrome: The Changes of ... Dialysis Disequilibrium Syndrome (DDS) is a rare but well-known serious complication of dialysis [1]. A clinical deteriorated neurological](https://img.dokumen.tips/doc/110x75/5fca506f1ef448245c25d799/dialysis-disequilibrium-syndrome-the-changes-of-dialysis-disequilibrium-syndrome.jpg)









