Embed Size (px)
Citation preview

AMKHICAN JOURNAL OK OPTOMETRY & PHYSIOLOGICAL OPTICSCopyright © 1977 American Academy of Optometry
Volume 54, No. 2, February 1977Printed in U.S.A.
Neuro-optometry: An EvolvingSpecialty Clinic*
Lawrence Stark,-f- A, Terry Bahill,^: Kenneth J. Ciuffreda,§ Robert V. Kenyon,||and Stephen Phillips:):
School of Optometry and Department of Electrical Engineering and Computer Science [L. S , ] ,University of California, Berkley, California
ABSTRACTNeuro-optometry is evolving as an optometricclinical specialty focusing on neurologicaldysfunctions of the visual system. Initially, wefocused upon abnormalities of ocularmovements, and our investigations have nowbroadened to include static and dynamicmeasurements of eye movements,accommodation, and the pupilWe feel the clinic serves three fundamentalpurposes: (1) to provide service to the patient,(2) to perform clinical research, and (3) tobroaden the scope of the students' clinicalexperience. Operation of the clinic, technicalmethods of measurement, the testing protocol,and examples of interesting clinical recordingsare described.
Neuro-optometry is now evolving in direc-tions that depend upon the utilization of thisspecialty clinic in our School of Optometry, We,ourselves, are concentrating on the motor func-tion aspect of neuro-optometry which includesversional eye movements of all types: fixation,optokinetic nystagmus, eye tracking, readingeye movements, and "scanpaths" or free view-ing of pictures. We are also studying vergenceeye movements and the interaction betweenvergence and versional eye movements. Fur-thermore, the triadic response (accommoda-tion, pupillary, and vergence eye movementresponses to near and far targets) is another
This work was partially supported by PHS Train-ing Grant #5T01 EY00076-04 to A. T. B., K. J. C., R.V. K,, and S. P., and an Auxiliary to the AmericanOptometric Association Research Grant to K. J. C.
* Submitted May 3, 1976.t Neurologist, M.D., Member of Faculty.$ Bioengineer, Ph.D.§ Optometrist, O.D.IIBioengineer, M. S.
area of our focused attention, and we are makingdynamic studies of all these in our Neuro-optometry Clinic.
Sensory functions, such as visual fields orvisually evoked responses (VER), are alsoclearly of great importance and, in fact, arebeing developed by other faculty members inour school. Another area of increasing impor-tance in neuro-optometry is the fundoscopicstudy of the nerve fiber layer in the retina,including the remarkable anatomical region ofthe optic nerve head. Although the importanceof this has been emphasized, for example, byProfessor William Hoyt who was advocatedusing a green light in the ophthalmoscope forbetter viewing of the retinal nerve fiber layer(William F. Hoyt, personal communication), wehave not yet introduced this as a procedure inour Neuro-optometry Clinic but are consideringa clinical photographic study in-this direction.
RATIONALEThe rationale for our Neuro-optometry Clinic
with its emphasis on motor dysfunctions is pri-marily one of service to our patients. Clinicalservice means to us that each patient will bestudied for the direct benefit of the patient. Hisoptometrist or physician will obtain an objectiverecord of the oculomotor disability to refer to inthe chart and the best quantitative evaluation ofhis disorder to correlate with the clinical evalua-tion. Eye movement recordings are now an on-going clinical testing procedure in this clinic andin many hospitals. Electro-oculography (EOG),photoelectric eye movement recordings, andelectromyography (EMG) techniques are not"human experimentation" in the acceptedsense of these terms. The Committees onHuman Experimentation at both the Universityof California, Berkeley, and the University ofCalifornia, San Francisco, have carefully re-viewed our procedures and have agreed with us
85

86 AM J OPTOM & PHYSIOL OPTICS Vol. 54, No. 2
concerning our rationale of clinical service to theindividual patient. Based upon this informa-tion, they have allowed us to carry out theseprocedures without requiring the explicit con-sent of the patient, since all procedures per-formed on the patient are for his direct benefitas part of his normal optometric or medicalcare. The data will be collected as a conse-quence of established (in California) medicalprocedures as ordered by the patient's optome-trist or attending physician. Such procedures
.are nonintrusive and present no risk to the pa-tient as defined by the Department of Health,Education and Welfare.
In addition, we expect to do clinical researchwhich depends upon detailed analysis of the eyemovement records using our on-line laboratorydigital computer and other bioengineering andneurological analysis techniques, such as con-trol systems models of the human eye move-ment system. The purpose of this work is to use"nature's experiments to refine such math-
'
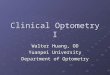
FIG. 1. A, eye movement monitor with binocular photocell sensors mounted on a modified ophthalmic frame inplace on patient. Circular photocells positioned approximately 12 mm from the eye and perpendicular to theglobe measure amount of infrared light reflected from the nasal or temporal limbus, respectively. B,patient's head supported by headrest and chinrest. The target is a small spot of light moving on a large,translucent screen 57 cm away (on left). Infrared light source (lower left) is a tungsten lamp with a Kodak No. 2darkroom safelight filter.

February 1977 Neuro-optometry: An Evolving Specialty—Stark et al. 87
ematical descriptions of the neurological controlsystem," This clinical research does not incon-venience the patients, since it is carried out inlarge part after the patient has left the labora-tory and, indeed, after the clinical report hasbeen sent to the referring doctor. The results ofour clinical research will appear as case studies3:
1. A. T, Bahill et al. on "Dynamic and StaticViolations of Hering's Law of Equal Inner-vation"
2. K. Ciuffreda et al. on "Reading Eye Move-ments: Case Reports"
3. R. Kenyon et al. on "Absence of DisparityVergence Eye Movements"
4. S. Phillips et al, on "Dynamic Abnormal-ities in Accommodation" '
These are examples of the output of ourNeuro-optometry Clinic,
Our philosophy is that there is really nodifference between applied and basic research.Our neuro-optometry studies can contribute inan applied clinical research fashion by helpingto define the history of a motor abnormality,including its recession, following treatment; inoptometry, treatment may include vision train-ing or corrective lenses. At the same time we aredoing basic research, because this informationmay yield new insights into the underlyingneurological mechanisms controlling eye move-ments which may lead to improved basic bioen-gineering models of these controlled processes, avery basic research goal indeed.
A final rationale for our Neuro-optometryClinic is an innovation in the professionalinstruction in the School of Optometry. A newlyestablished section of Optometry 483A,B,C,the Neuro-optometry Clinic, will enable ouroptometry students to come in contact withpatient examinations in our clinic, so that theycan become acquainted with this evolving spe-cialty area of optometry. In addition, the objec-tive recordings and quantitative studies of thesepatients will enable the students to becomeconversant with this important area of interac-tion between clinical medicine and clinicaloptometry.
°A. Terry Bahill, Kenneth J. Ciuffreda, Robert V.Kenyon, and Lawrence Stark, Dynamic and staticviolations of Hering's law of equal innervation, Am. J.Optom., 53 (12): 798-808, 1976; Kenneth J. Ciuffreda,A. Terry Bahill, Robert V, Kenyon, and LawrenceStark, Eye movements during reading: case reports,Am. J. Optom., 53 (8): 389-395, 1976; Robert V,Kenyon, Kenneth J. Ciuffreda, and Lawrence Stark,Absence of disparity vergence eye movements, inpreparation; S. Phillips and L. Stark, Dynamic ab-normalities in accommodation, in preparation; L.Thai, S. Phillips, and L. Stark, Isolated paralysis of ac-commodation in a young woman, Am. J. Optom., inpreparation.
CLINIC OPERATION
The mode of operation of our clinic over thepast year has been to encourage and acceptdirect referrals from the ongoing clinics in theSchool of Optometry. Our referrals have comefrom a number of other specialty clinics:orthoptics, strabismus, pathology, and the gen-eral refraction clinic, as well as a scattering ofreferrals from outside practitioners. As the otherclinical instructors on the faculty and the 3rdand 4th-year students, who directly manage thepatients, become more familiar with our serv-ices and potentialities, we may develop otherand more vigorous patterns of referral proce-dures. The clinic director, Dr, Kenneth Poise,has provided us with several opportunities todiscuss our Neuro-optometry Clinic and some ofour findings at meetings of the clinical staff,and we have found this interactive feedback tobe of benefit to us in many ways, in addition toour primary point of informing others about ourclinic.
The output to the referring optometrist orphysician from our clinic, at present, is in theform of a written report summarizing thepatient findings, based on our studies of theobjective recordings and our attempts to corre-late these findings with the patient's generalclinical findings and laboratory findings fromother clinics, such as the VER clinic. It is hopedalso that as students take our specialty pro-gram, part of their work would be preparingclinical case discussions based upon the patientstudies that occurred during their tenure in theclinic.
FIG, 2. Plot of eye position versus voltage showinglinear operating range of photocell monitor.

AM J OPTOM & PKYS10L OPTICS Vol. 54, No. 2
TABLE 1. Overview of eye movement recording methods
Method Published in" Parameterrecorded
Estimatedbandwidth
(Hz)
Track-ing
rangewith±5%line-arity(de-
grees)
Noise orresolution Comments
Esti-mated
cost($)
exclud-ing
stripchart
record-er andampli-fiers
Non-contact methods for measuring eye movements
Photography ofcorneal reflection
Photoelectric
After-image tech-niques
Movie camera
Stanford ResearchInstitute eyetracker
TV type camera
Mirror for reflectedeye image
Psych, Rev., 1901(Dodge)
Exp. Neurol., 1975(BahSll et al.)
Treatise on Physio-logical Optics,1866 (Helmholtz)
Arch. Ophthal-mol., 1966(Higginsand Daroff)
J.Opt. Soc. Am.,1973(Cornsweetand Crane)
lEEEBiol. Med.,1974 (Merchantetal.)
Ann. Ocul. (Javal),1879
Eye position
Eye position
Eye position
Eye posit ion
Eye position
Eye position
Eye position
100
500
32
10
15
40
20
100
60
/ 12
60
60
0.5°
Less than bio-logical noisewhich is~1 min arc
0.5°
< biological
1°
One of the 1stpublished rec-ords of eyemovementsand one of thebest
Used in 2 Cali-fornia clinics;bandwidth usu-ally 70-100 Hzwhen used withstrip chart re-corder
No permanentrecord
Time-consumingdata analysis
Newer version haslarger band-width but ar-tifacts at endofsaccades
Also made byWhittakerCorp. and Ham-amasu Co,
No permanentrecord
Contacting methods for measuring eye movements
300
None
30,000
50,000
Elect ro-oculography(EOG)
Contact lens withmirror attached
Contact lens withcoil attached
Vision Res,, 1970(Weber & Daroff)
Science, 1973(Steinmanet al.)
Vision Res., 1975(Collewjn)
Sine eye position
Eye position
Sine eye position
25
60
50; could beincreased to1 KHz
80
10
40
1,5°
<biological
<biological
No head re-straint neces-sary; outputvaries withambient light;large amountof drift
Also used byYarbus, Riggs,Cornsweet,Ditchburn, andFender
Developed byRobinson(IEEE Biol.Med., 1963)
25
3,000
10,000

February 1977 Neuro-optometry: An Evolving Specialty—Stark et al 89
TABLE 1—Continued
Method
Plaster "contactlens" with leverattached
Published in
Am. J. Psych,,1898 (Delabarre)
Parameterrecorded
Eye position
Estimatedbandwidth
(Hz)
30
Track-ing
rangewith±5%line-arityIAo(ue-
grees)
15
Noise orresolution
~0.5°
Comments
Cocaine must beused to rendercornea insensi-tive; mentionedfor histor-ical purposesonly
Esti-mated
cost($)
exclud-ing
stripchart
record-er andampli-
fiers
10
"1. Bahill, A. T., and L. Stark. Dynamic overshoot in saccadic eye movements is caused by neurologic control signal reversals,Exp. Neurol., 48: 107-122, 1975.
2. Cornsweet, T. N., and H. D. Crane, Accurate two-dimensional eye tracker using first and fourth Purkinje images, J, Opt,Soc. Am., 63: 921-928, 1973.
3. Delabarre, E. L., A method for recording eye movements, Am, J. Psyehol., 9: 572-574,1898.4. Dodge, R., and T. S. Cline, The angle velocity of eye movements, Psyehol. Rev., 8: 145-157, 1901.5. Collewijn, H., F. van der Mark, and T. C. Jansen, Precise recording of human eye movements, Vision Res., 15: 447-450,
1975.6. Steinman, R. F., G. M. Haddad, A. A. Skavenski, and D. Wyman, Miniature eye movements. Science, 181: 810-819,1973.7. Higgins, D. C., and R. B. Daroff, Overshoot and oscillation in ocular dysmetria. Arch. OphthaK, 75: 742-745, 1966.8. Weber, R. B., and R. B. Daroff, The metrics of horizontal saccadic eye movements in normal humans, Vision Res., 11: 921-
928, 1971.9. Helmholtz, H. von, Helmholtz's Treatise of Physiological Optics, edited by J, P. Southhall. Vol. 3, pp. 108-112, Dover
Publication, 1925 (originally published in 1866).10. Javal, E., Essai sur la physiologie de la lecture, Ann. Ocul., 82: 240-274,1879.11. Robinson, D. A., A method of measuring eye movement using a scleral search coil in a magnetic field, IEEE Trans. Bio.
Med., BME-10: 137-145, 1963.12. Merchant, J., R. Morrissette, and J. L. Porterfield, Remote measurement of eye direction allowing subject motion over one
cubic foot of space, IEEE Trans. Bio. Med., BME-21: 309-317,1974.
METHODS
A brief summary of our methods with someillustrative material is presented in order topermit the reader to get a more detailed view ofthe services that the Neuro-optometry Cliniccan provide for the patient. In order to measureeye movements, either versional or vergence, weuse spectacle frames with photocells mountedclose to the eye, but not interfering with eitherthe patient's eye movements or ability toblink,1-a The pictures in Fig, 1 show a patientwearing these eye movement monitors. Whenthe photo cells are properly positioned and thecircuitry is balanced and calibrated exactly asshown in Fig. 2, quite accurate eye movementrecordings can be obtained. Appendices A andB give further details on this methodology, andan overview of eye movement recordingmethods is presented in Table 1. The binocularreading eye movements shown in Fig. 3 are anexample of some of the interesting results of ourclinical studies.
In order to measure accommodation dynami-
cally, we use a third Purkinje image instrumentwhich was developed by O'Neill and Stark3 andby Phillips et al,4 (Fig. 4). The instrument ismounted within a slit-lamp biomicroscope.Because it measures the position of the anteriorsurface of the lens, it gives only a parametricmeasure of accommodation; thus, to calibrate,we use a Fincham coincidence optometer basedon the Scheiner principle (1619), The Finchmanoptometer is also used to record static measure-ments of accommodation (Fig. 5). Here we see-the contrast between the response of the normalsubject and the response of a patient with diffi-culty in accommodative facility. Dynamic re-sponses taken with our Purkinje image instru-ment are shown in Fig. 6. We hope to studythe influence of "accommodative rock" visiontraining procedures in influencing facility diffi-culties in a selected group of patients in co-operation with J. David Grisham, O.D., Assist-ant Clinical Professor in charge of the Orthop-tics Clinic, and James Ronan, O.D., ClinicalInstructor.
Pupillometry has expanded recently to be an

90 AM J OPTOM & PHYSIOL OPTICS Vol. 54, No. 2
FiG, 3. Binocular reading eye movements of an amblyopic patient showing (from top to bottom) right eyevelocity, left eye position, right eye position, and timing trace with 1 sec markers, Upward deflections inposition traces indicate leftward eye movements; position calibration bars represent 10 degrees. Velocity calibra-tion bar represents 480 degrees per sec. With the reading card at 50 cm, corrective lenses were not worn; the pa-tient reported seeing reading material clearly. Evident are several regressive movements, glissadic over-shooting in the amblyopic eye, and long fixation pauses. The patient's reading rate was reduced to 170 words perminute. Uncorrected visual acuity and refractive error were +0.75-2.00 x 90, 20/38 and -0,50 x 17, 20/20, re-spectively, for left and right eyes.
FIG. 4. Essential elements of dynamic optometer,a modified slit-lamp with photomultiplier attached tosecondary arm. The instrument measures the amountof light reflected from the anterior lens surface duringaccommodation, correlating with instantaneous ac-
exciting area of dynamic study; the TV pupil-lometer designed by Stark and Troelstra5'9 isshown in Fig. 7. Its mode of operation is (1) toobtain a video image of the subject's magnifiediris and pupil, (2) to use image-processingelectronics to define the pupil-iris border, (3) to
commodative state. Reflected light (infrared) wasamplified by photomultiplier system and signals wererecorded. Targets at 100 cm (1.0 D) and 20 cm (5.0D), shown on adjustable jacks, are alternately pre-sented with temporal randomization to the patient,who is instructed to keep the appropriate target inclear focus. Head stabilization and accurate fixationare a prerequisite for obtaining precise measurementsfree from movement artifacts. A bite bar may be uti-lized to minimize head movements; eye movementmonitors may be added to determine magnitude of anyocular movement that might have taken place duringan experimental run. The eye not being tested isoccluded.

ACCCWWDATIOH
RESPONSE
(D)
8 —
7 —
6 —
5 -
It -
3 -
2 -
a -
ACCOhMODATION STIMULUS (D)
FIG. 5. Two accommodative stimulus-response curves measured with Fincham optometer. Response (O)shows focusing ability of a normal 25-year-old patient. Note that from 0 to 7 D of accommodative stimulus, thepatient follows the target quite well and manifests typical "lazy lag of accommodation," Beyond 7 D ofaccommodative stimulus, the patient approaches the "presbyopic zone" (latent zone), and the plateau gives ameasure of accommodative amplitude. In contrast is the response (P) of another 25-year-old patient whocomplained of focusing difficulties at near and clearly exhibits an impaired focusing ability. At the time oftesting, the patient was wearing poorly fitting soft contact lenses and had slightly reduced and variable visualacuity.
ACCOMMODATIONSTIMULUS(D)
ACCOMMODATIONRESPONSEO.S,(D)
ACCOMMODATIONRESPONSEO.D.(D) 1
I 1 sec
FIG. 6. Dynamic accommodative responses to 4-D step changes of stimulus in a 24-year-old patient whocomplained of blurred vision and tired eyes after reading or sewing for short periods of time. Both eyes showed alatency of about 750 msec, nearly twice the normal value of about 380 msec. When blur stimulus was presentedto the left eye, response amplitude in diopters was within normal limits and without noticeable accommodativedrift. When the same stimulus was presented to the right eye, initial response amplitude was normal butaccurate focus was not maintained; accommodative response rapidly declined to about 2 D. With continuedtesting, the patient became slightly fatigued and produced a more variable accommodative response to thesame accommodative stimulus. Near the end of testing, with the patient quite fatigued, accommodativeresponse gradually decreased in amplitude; both eyes eventually developed an accommodative spasm centeredon 3 D. (Note: static accommodation measurements were within normal limits for age; the Fincham optometermeasured an accommodative amplitude of 7.4 D in the right eye and 8.0 D in the left eye; with the Prince rulepush-up method vising a slowly moving target, measured accommodative amplitude was 9.0 D in each eye.)Each eye was tested separately, and the 2 responses were not recorded simultaneously.
91

92 AM J OPTOM & PHYSIOL OPTICS Vol. 54, No. 2
FIG. 7. TV Infrared Pupillometer. On the right arehead and chin rest and fixation cross, while on theleft are infrared-sensitive television camera, zoomlens, and infrared light source adjacent to the lens.Stimulus is a bright light, seen in Maxwellian view,located within modified slit-lamp illumination hous-ing. Instrument, camera position, and infrared lightsource are adjusted to obtain a sharp image of the irison the TV monitor, then the light stimulus is properlypositioned. The entire alignment procedure takes 2min; the clinician is now ready to make accuraterecordings of pupillary responses to light, presented ineither a pulse or sinusoidal manner, or to step-accom-modative stimuli.
mark this border with a white crescent so thatthe experimenter can be certain that the instru-ment is functioning (as shown in Fig. 8), and (4)finally, to count the number of TV lines in thepupil image. This count is seen as the dynamicresponse trace shown in Fig. 9. In this figure, thenormal dynamic pupil response is contrastedwith the slowed, deficient pupil response of apatient following recent ocular trauma.
PROTOCOL
The testing protocol for the Neuro-optometryClinic was initially based on earlier experiencein various hospital clinics for neuro-ophthal-mology. From the protocol (Table 2), one seesthat the usual aspects of eye movements, suchas fixation, saccadic tracking and smooth pur-suit, vergence, reading eye movements, dynam-ic and static accommodation, and dynamicpupillary responses, are all part of our test. It isimportant to note that the calibration proce-dure appears first not only because we begin bycalibrating, but also to emphasize the impor-tance of calibration throughout the procedure.Several aspects of the protocol, such as optoki-netic nystagmus, and vestibular testing, havenot yet been implemented. The accommodationand pupillary tests are sufficiently complex thatthey are performed at a separate appointmentto the clinic.
Once a general overview of the patient'sabnormalities is obtained by utilizing the stan-dard protocol of Table 2, it is then possible to dofurther testing in accordance with a number ofspecial expanded protocols pointing toward spe-
FIG. 8. Patient's pupil and iris displayed on TV monitor. The white crescent seen at the left half of the pupilmargin indicates that correct pupillary diameter measurements are being electronically processed; the lightspot is the first Purkinje image of light source and does not contaminate pupil diameter measurements; thereference scale in mm is over the monitor screen. Besides using the TV monitor in alignment procedures, amagnified view of the pupil helps verify the record on the strip chart.

February 1977 Neuro-optometry: An Evolving Specialty—Stark et al. 93
PUPIL
DIAMtTkH(IUT.)
3 -
1» -
FIG. 9. Light-pupillary response of patient who received a powerful blow to the eye with a baseball 1 weekbefore examination. The left eye exhibited normal pupillary dynamics, with pupillary constriction followed bypupillary dilation, i.e., pupillary escape, during prolonged light stimulation. In contrast, the traumatized righteye had a semidilated pupil (5 mm) and displayed a greatly reduced pupillary response to light, indicating neuro-muscular and/or motor fiber damage (N III). Each eye was studied separately, and the 2 records are not simul-taneous.
TABLE 2, Testing protocol of Neuro-optometry Clinic
I, Calibration
1) _5° _2.5° 0° +2.5° 4-5" horizontal steps2) Triangular target movement (±5°) in the horizontal plane
.a. To check for linearity throughout the range of eye movements tested in the protocol3) _5° o° -4-5° vertical steps
a. To check for horizontal-vertical crosstalk
II. Static posit ion
1) Fixation; -5° -2.5° 0° +2.5" +5° horizontal steps2) Performed with right eye only, left eye only, and with both eyes
a. TO test for fixational instabilities, such as gaze or latent nystagmus or unusually large microsaccadesb. To determine whether a composite prism arrangement reduces the amplitude and/or frequency of
nystagmus (binocular conditions only)
III. Saccadic tracking
1) -5° to+5° and +5° to-5°2). 0°to + 5° and +5° to 0°3) -5° to 0° and 0° to -5°
a. To determine saccadic magnitude, latency, duration, and peak velocityb. To detect violations of Bering's Law to indicate pathological casesc. To determine the action of drugs or fatigue on saccadic decompositiond. To detect any abnormal types of overshoot or undershoote. To test for the presence of apraxiaf. To test for directional nonlinearities
IV. Smooth pursuit
1) Triangular target movement (=t5°) from 0.1 to 1.5 Hz or greatera. To detect saccades, the velocity is monitoredb. To measure smooth pursuit velocity range and decomposition with increasing target oscillationsc. To measure gain or stability margind. To determine smooth pursuit breakdown with auxiliary lenses producing retina] image blur and/or
magnification changes

February 1977
TABLE 3—Continued
Patientno. Age Referring
clinicOculomotor abnormality
27 Strabismus Fixational instability; poor sac-cadic and smooth pursuittracking when using ambly-opic eye alone
Neuro-optometry: An Evolving Specialty—Stark et aL 95
dyslexia. These cases may be further studiedand presented as single case reports, as articlesdescribing a diagnostic group, or as articles insome area of control, theoretical, or physiologi-cal oculomotor function.
33 22 Strabismus
16
23
38
12 Orthoptics
25 Strabismus
9 General
32 19 General
41 38 General
Poor oculomotor control ofamblyopic eye during all eyemovement tasks
Pseudo-INO; abnormal ver-gence responses
Reading eye movements showabnormally long fixationaldurations and numerous re-gressions
Reduced accommodative ampli-tude «5 D) in each eye; ex-cessive number of fixationsper unit text and hypometricsaccadic return-sweeps dur-ing reading
Accommodative spasm withfocus "fixed" for 33 cm andmore difficult to relax accom-modation than to increaseaccommodation
INO, but glissadic undershoot-ing of both eyes for adductingsaccades only, indicates earlyneurological involvement; re-cently diagnosed as havingmultiple sclerosis
cific disorders. We are developing these as ourexperience and the case load of our clinicwarrants. For example, in a patient with areading disorder, we might emphasize apraxiatests, laterality of control of saccades, interac-tion of vergence and version, scanpaths con-structed on viewing pictures, and the behaviorof the eyes in a number of actual reading tests,
PATIENT EXPERIENCE
Over the past 6 months (to July 1, 1975), wehave studied approximately 40 patients. Thepercentage of patients without clear oculomotorabnormalities was rather high in the earlyphases of our clinical operation. After establish-ing communication channels between the clini-cians, the senior students, and our own group,the percentage of abnormalities has beengreater than 80%. Table 3 lists 20 patients,giving their age, the referring clinic, and thetype of abnormality recorded. Our patient pop-ulation represents a number of interesting ocu-lomotor abnormalities and diagnostic cate-gories: nystagmus, abnormal vergence (strabis-mus), nonconjugate saccades, adductor lag, and "
SUMMARY
The Neuro-optometry Clinic exists as a cur-rent service in the School of Optometry on thecampus of the University of California, Berke-ley. Patients are being referred in order toobtain information which the optometrist orphysician can utilize for the patient's benefit.The clinic is active in teaching the students, theclinic staff, and, of course, ourselves with re-spect to the nature of the oculomotor dysfunc-tion definition of syndromes by objective re-cording, and this results in more precise diagno-sis and better patient management. In additionto these patient service and teaching functions,we conduct clinical and basic research. Forth-coming research reports explore such areas asdyslexia, Bering's Law violations, and dynamicaccommodation and vergence abnormalities.
We quote from the pioneer of eye movementrecording, Dr. Raymond Dodge,7 " . . . I havebeen able to examine the eye of patients. . . ,Some cases presented exceptions to the normalcompensatory eye movements, which might,perhaps, become of diagnostic value," and alsofrom our distinguished neuroophthalmologycolleague, Dr. William F, Hoyt (personal com-munication), from the University of California,San Francisco, "Photoelectrical eye movementrecording is serving the neuro-ophthalmologistas 'the X-ray' of eye movement disorders,"
ACKNOWLEDGMENTSWe thank Kenneth Poise, Clinic Director,
School of Optometry, University of California,Berkeley, for encouragement and partial finan-cial support for the Neuro-optometry Clinic; theclinical staff at the School of Optometry fortheir cooperation in patient referrals; andCynthia Cowee for assistance with the manu-script,
REFERENCES
1. Stark, Lawrence, Gerhard Vossius, and LaurenceR. Young, Predictive control of eye tracking move-ments, Inst. Radio Eng, Trans. Human FactorsElectronics, HFE-3: 52-57, 1962.
2. Bahill, A. Terry, Michael R. Clark, and LawrenceStark, Dynamic overshoot in saccadic eye move-ments is caused by neurological control signalreversals, Exp. Neurol., 48: 107-122, 1975.
3. O'Neill, William D., and Lawrence Stark, Triplefunction ocular monitor, J. Opt. Soc. Am., 58:570-573, 1968.
4. Phillips, Stephen, Douglas Shirachi, and LawrenceStark, Analysis of accommodative response times

94 AM J OPTOM & PHYS10L OPTICS
TABLE 2—Continued
Vol. 54, No. 2
V. Vergence
1) Targets placed at 50 and 25 cm for testing of divergence and convergence abilitya. To measure peak velocity, latency, and to detect abnormalities in the dynamics of the vergence response
for disparity vergence (symmetric, line of sight, general asymmetric) and accommodative vergence
VI. Optokinet ic nystagmus: nol yet implementedVII. Ve.stihular testing: not yet implemented
VI]]. Higher level control
1) Reading eye movements; 90-word text for children and 150-word text for adultsa. To detect abnormalities of fixational duration, small saccadic eye movements, large return-sweep
saccadic eye movements, fixation frequency (number of fixations per unit text), and reading rate (wordsper minute)
b. To detect any abnormal reading patterns, such as superimposed nystagmus or backwards reading eyemovements
2) Scanpaths: horizontal scanpaths onlya. To investigate patterns of information processing when looking at ordinary scenes and pictures
IX. Accommodation
1) Static accommodation measured with a Fincham coincidence optometer and Prince rule (push-uptechnique)a. To detect abnormal accommodative amplitude or accommodative response
2) Dynamic accommodation measured with infrared optometer; targets placed at 100 and at 20 cma. To check for abnormally long latencies, slow dynamics, the ability to sustain accommodation accurately,
and the effect of fatigue on the accommodative response
X. Pupil
1) Pupilliary responses measured with Stark TV pupillometera. To determine the characteristics of the dynamic pupillary response to accommodative stimulib. To determine the characteristics of the dynamic pupillary response to step and sinusoidal light stimulic. To check for static and dynamic abnormalities relating to neuropathology and ocular pathology
TABLE 3. Patient listing for Neuro-optometry Clinic
Patientno.
12
26
29
35
37
10
20
11
, ReferringAse clinic
21 Pathology
69 General
12 Orthoptics
12 General
8 General
13 Orthoptics
30 Orthoptics
5 General
Oculomotor abnormality
Oblique sawtooth nystagmus
Pendular nystagmus; nonconju-gate saccades f requen t lypresent
Jerk nystagmus
Pendular and jerk nystagmus;nonconjugate sarcades fre-quently present
Uni la te ra l vert ical pendularnystagmus due to t raumaresulting in a blind eye and apupil unresponsive to lights t imul i
Slow divergence ability butaccommodat ive dynamicsnormal
Abnormal vergence
Congenital un i la te ra l ptosis buteye movements normal
4 24 Orthoplics Abnormal vergence eye move-ments; abducting saccadesshowed glissadic overshootwhile adduct ing saccadesshowed glissadic undershoot;these saccadic dynamics aretypically found in patientswith internuclear ophthalmo-plegia (1NO); increased ac-commodative latency and ac-commodative drift
25 24 General Poor convergence eye move-ments; backward reading eyemovements (reverse stair-case); accommodation slow,reduced range and long laten-cies
22 22 Strabismus Abnormal vergence response;fixaiional instability withamvolyopic eye fixating
9 11 Orthoptics Poor saccadic and smooth pur-suit t racking; hypometricsaccades
34 54 Pathology Hypometric saccades; fixationinstability; abduction pseudo-1NO (recovered stroke vic-t im)

AMERICAN JOURNALOP OPTOMETRY& PHYSIOLOGICAL OPTICSVol. 54, No. 6, p. 402June 1977Copyright © 1977 AmericanAcademy of QptometryPrinted in U.SA,
OmissionsStark, L., A.T. Bahill, K. C. Ciuffreda, R. V. Kenyon, and S, Phillips,Neuro-optometry: An evolving specialty clinic, Am. J. Optom. &Physiol. Optics, 54 (2): 85-96, 1977.
The last portion of the references, ,theauthor's address, and the beginning of Ap-pendix A were inadvertently omitted frompage 96 of this paper. This information isprovided here.
REFERENCES
4. Phillips, Stephen, Douglas Shirachi, and Law-rence Stark, Analysis of accommodative re-sponse times using histogram information, Am.J. Optbm., 49: 389-401,1972.
5. Stark, Lawrence, and Arne Troelstra, UnitedStates Patent #3,533,683, Dynamic Pupillome-ter Using Television Camera Systems, 1970.
6. Stark, Lawrence, and Arne Troelstra, UnitedStates Patent #3,533,684, Display of Measure-ment Adequacy Marker Systems for Pupillome-ters, 1970. ' ,:
7. Dodge, Raymond, Five types of eye movementsin 'the horizontal plane of the field of regard,Am. J. Physiol., 8 (4):'326, 1903.
AUTHOR'S ADDRESS:Lawrence StarkSchool of OptometryUniversity of CaliforniaBerkeley, California 94720
APPENDIX AResearchers starting to use the eye
movement glasses spend a good deal oftime and have trouble becoming ac-quainted with the glasses, becomingskilled in positioning them, and balancingthe electronic circuits. This is especiallytrue in clinical settings and in psychologi-cal studies where the student experimen-ters are unlikely to be skilled in electronicinstrumentation.
There are essentially 2 problems: (1) po-sitioning of the photocells and infraredlight sources, and (2) balancing the elec-tronic circuitry. Perhaps this could be ac-complished by using an automatic controlsystem and computer linearization.
402

96 AM J OPTOM & PHYSIOL OPTICS Vol. 54, No, 2
. (.ion. However, automatic calibration andcomputer linearization are of dubious value ifthey only serve to mask ineffective positioningof the photocells. It is always important to thinkabout photocell positioning and to adjust themfor the optimal response.
The balancing and calibration procedureincludes.3 steps. The 1st step is the independentdark current cancellation of all photocells whilethe subject is looking straight ahead (0°). The2nd step is to balance with a potentiometer andto use photocell positioning in an iterativemanner. Among the ways to check the balanceare to have the subject tract triangular wavesand balance for linearity of response, to havethe subject make vertical saccades and balancefor common mode rejection (with the horizontalset of photocells), and, finally, to have thesubject move plus or minus 5 degrees fromcenter (0°) and balance for equality of response.Lastly, the gain which should be independent ofthe balance, is adjusted so that there is a stand-ard output. For example, in the clinical set up,we have 1 volt equal 1 degree so that we canbecome accustomed to looking at eye move-ments on the same amplitude and time scale onthe pen recorder.
A different set of procedures might be devel-oped for vertical eye movements, especially ifthe photocells are arranged so that they suminstead of take differences.
Computer linearization has been developedby 2 groups working on scanpaths: 1 group at
• Stanford and 1 at Berkeley. In each, the subjectpositions his eyes over a grid of 9 or 25 dots in amatrix array. The computer measures the volt-age output of the photocells about 300 msecafter a particular point on the matrix has beenbrightened as a signal for the subject to directhis gaze at that point. Then the computerdevelops a linearization algorithm for differentpie-shaped sectors of the entire visual field. Byusing a table look-up, on-line linearization ofthe eye movement voltage measurements can beperformed as data are taken into the computer.
We have been considering automatic calibra-tion procedures for dark current cancellation ofboth photocells and for balancing the circuitrybased on the maneuvers described above. Whatis needed is a fairly complex measurement andcontrol device, probably a microcircuitry sys-tem which would adjust a resistance, such as aFET, whose resistance can be controlled byvoltage. This voltage, in turn, would be con-trolled by some test for zero dark current and forequality of response in the balancing procedure.The computer linearization technique could bedone in the first instance with a minicomputer,such as a PDP-8 or PDP-15,but it may beworthwhile to develop a microcomputer for thispurpose.
APPENDIX B
We have had extensive experience with 3types of photocells." 1) The FPT 100 photodiode and the FPT 101
phototransistor, each costing about 1 dollar,have been used in our classroom and clinicallaboratory. These have a large field of view and,because of that, are easier to position; however,they are noisier because they take in a good dealof eyelid movement.
2) The LS 400 photodiodes, which cost about8 dollars each, have a narrow field of view; thus,they are harder to position, but once wellpositioned, they have the lowests noise level andalso the least interference with vision due totheir small size. Indeed, Terry Bahill feels thathis LS-400 system is not at all limited byelectronic noise, and has found eye movementrecords where all the noise was biological noise.
3) A new type of infrared, light-emittingdiode and photodiode system has been on themarket for about a year. This is the OPT 125which costs about 6 dollars. It consists of a smallblack plastic triangular elment about 1 x 5 x 8mm, which includes the photodiode and theinfrared light-emitting diode in fixed positions.It is the hardest to align, since one must notonly carefully arrange it horizontally and verti-cally, but the distance is also critical, so thatthe reflecting surface (the limbus) is properlylocated in the field of view of the emitter andthe receiver. An advantage of the OPT 125 isthat the light source is mounted on the specta-cle frame, and thus, head movement effects areminimized. Another difficulty of the OPT isthat they sometimes tend to partially blockvision unless carefully positioned.