Embed Size (px)
DESCRIPTION
Repairing the brain after a patient has suffered from Traumatic Brain Injury
Citation preview

Neural Grafting: Repairing the Brain andSpinal Cord
October 1990
OTA-BA-462NTIS order #PB91-114249

Recommended Citation:
U.S. Congress, Office of Technology Assessment, Neural Grafting: Repairing the Brain andSpinal Cord, OTA-BA-462 (Washington, DC: U.S. Government Printing Office, September1990.
For sale by the Superintendent of DocumentsU.S. Government Printing Office, Washington, DC 20402-9325
(order form can be found in the back of this report)

Foreword
Extraordinary developments in the neuroscience in recent years have shown promise ofnew advances for treating diseases of the nervous system and for increased generalunderstanding of the human mind. Paralleling these developments has been a growingcongressional interest in their policy implications. The designation of the 1990s by the101stCongress as the “Decade of the Brain” is one indication of this interest, as was the requestfor OTA to undertake a series of reports under an assessment of “New Developments inNeuroscience.” Requesting committees are the House Committees on Energy and Commerce;Science, Space, and Technology; Appropriations; Veterans Affairs; and the SenateSubcommittee on Science, Technology, and Space of the Committee on Commerce, Science,and Transportation.
This special report, the second of our neuroscience series, discusses the field of neuralgrafting into the brain and spinal cord to treat neurological disorders. It describes thetechnology of neural grafting, the neurological conditions that it may be used to treat, and thepatient populations that are affected. Also, the legal and ethical issues raised by thedevelopment of neural grafting techniques are discussed. The report includes a range ofoptions for congressional action related to the Federal funding of transplantation researchusing human fetal tissue, the adequacy of existing Federal laws and regulations regarding theuse of human fetal tissue, and the role of the Federal Government in guiding the developmentand promoting the safety and efficacy of neural grafting procedures.
The first publication in OTA’s assessment of “New Developments in Neuroscience”was Neurotoxicity: Identifying and Controlling Poisons of the Nervous System, published inApril 1990. OTA was assisted in preparing the present study by a panel of advisers, aworkshop group, and reviewers selected for their expertise and diverse points of view on theissues covered by the assessment. OTA gratefully acknowledges the contribution of each ofthese individuals. As with all OTA reports, responsibility for the content of the report is OTA’Salone.
K YA . - # A .JOHN H. GIBBONSu D i r e c t o r
. . .Ill
New Developments in Neuroscience Advisory PanelPeter S. Spencer, Chair
Center for Research, Occupational, and Environmental ToxicologyOregon Health Sciences University
Portland, OR
Robert H. BlankSocial Science Research InstituteNorthern Illinois UniversityDeKalb, IL
James F. ChildressDepartment of Religious StudiesUniversity of VirginiaCharlottesville, VA
Fred H. GageDepartment of NeuroscienceUniversity of California-San DiegoLa Jolla, CA
Bernice GrafsteinDepartment of PhysiologyCornell UniversityNew York, NY
Ronald KartzinelVice President for CNS DevelopmentCIBA-GEIGY CorporationSummit, NJ
Laurane G. MendelssohnManager of Personnel ResearchLilly Research LaboratoriesIndianapolis, IN
Franklin E. MirerDirector, Health and Safety DepartmentUnited Auto WorkersDetroit, MI
Albert S. MoraczewskiRegional DirectorPope John XXIII Medical, Moral, Research,
and Education CenterHouston, TX
Herbert ParolesDepartment of PsychiatryColumbia UniversityNew York NY
Richard M. RestakPhysicianNeurological Associates, P.C.Washington, DC
Alan KrautExecutive DirectorAmerican Psychological SocietyWashington, DC
Neural Grafts Study PanelRoy A. E. BakaySection of NeurosurgeryThe Emory ClinicAtlanta, GA
Nancy Buc (ad hoc)PartnerWeil, Gotshal & MangesWashington, DC
Mary B. MahowaldCenter for Clinical Medical EthicsUniversity of ChicagoChicago, 11
Jerry SilverDepartment of Developmental GeneticsCase Western Reserve Univ.Cleveland, OH
Robert P. Gale John R. Sladek, Jr.Division of Hematology and Oncology Department of Neurobiology and AnatomyUniversity of California-Los Angeles University of RochesterLos Angeles, CA Rochester, NY
Patricia King (ad hoc) H.Fred VossGeorgetown University Program Director
Law Center Biotrack, Inc.Washington, DC Mountain View, CA
NOTE: OTA appreciates and is grateful for the valuable assistance and thoughtful critiques provided by the advisory and study panelmembers. The panels do not, however, necessarily approve, disapprove, or endorse this report. OTA assumes full responsibilityfor the report and the accuracy of its contents.
i v

OTA Project Staff-Neural Grafting: Repairing the Brain and Spinal Cord
Roger C. Herdman, Assistant Director, OTA, Health and Life Sciences Division
Gretchen S. Kolsrud, Biological Applications Program Managerl
OTA Project Staff
David R. Liskowsky, Project Director
Timothy P. Condon, Project Director2
Monica Bhattacharyya, Research Assistant
Joyce Anne Brentley, Legal Analyst
Laura Lee Hall, Analyst
Wendy S. Pachter, Legal Analyst
Claire L. Pouncey, Research Assistant
E. Blair Wardenburg, Research Analyst3
Gladys B. White, Analyst 4
Patricia Anderson, NIH Detailees
Support Staff
Cecile Parker, Office Administrator
Linda Rayford-Journiette, Administrative Secretary
Jene Lewis, Secretary
Sharon Oatman, Administrative Assistant6
Contractors
Blair Burns Potter (editor), Bethesda, MDJulie Phillips (indexer), Oakton, VA
Lori Andrews, American Bar FoundationAlan Fine, Dalhousie University
Thomas B. Freeman, University of South FloridaKaren Gervais, University of Minnesota Center for Biomedical Ethics
William F. Hickey, Washington UniversityRonald D. McKay, Massachusetts Institute of Technology
Rosa Lynn Pinkus, University of PittsburghAli H. Rajput, University of Saskatchewan
Imou@ September 19892mou@ August 1989.3~ou@ August 1989.4 Through June 1989.5 Through October 1989.6 Through February 1989.

ContentsPage
Chapter 1: Summary, Policy Issues, and Options for Congressional Action . . . . . . . . . . 3
Chapter 2: Introduction ... ... ... ... ... ... ... ... .*. ... .*. ... .$. .*. .$. . **@"$"""""""" 19
Chapter 3: Neuroscience Primer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Chapter 4: General Features of Neural Grafting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
Chapter 5: Applications of Neural Grafting Into the Brain and Spinal Cord . . . . . . . . . . 61
Chapter 6: Relevant Neurological Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
Chapter 7: Legal and Regulatory Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113
Chapter 8: Ethical Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 149
Appendix A: DHHS Moratorium on Human Fetal Tissue Transplantation Research . . 171
Appendix B: Participants in the Workshop on New Developments in Spinal CordInjury: Acute Interventions and Neural Grafts . . . . . . . . . . . . . . . . . . . . . . . . 174
Appendix C: Decade of the Brain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 175
Appendix D: Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 177
Appendix E: List of Contractor Documents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 180
Appendix F: Acronyms and Glossary of Terms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .187

Chapter 1
Summary, Policy Issues, andIssues for Congressional Action

CONTENTSPage
GENERAL FEATURES OF THE NERVOUS SYSTEM ANDGRAFTING . . . .’. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
NEURAL. . . . . . . . . . . . . . . . . . . . . . . . . 4
Therapeutic Strategies ... ... ... ... ... ... ..*. . o..........*..*....***.*.*+..******* 4
Materials for Neural Grafting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Determinants of Successful Neural Grafting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Potential Risks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
APPLICATIONS OF NEURAL GRAFTING INTO THE BRAIN ANDSPINAL CORD . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
RELEVANT NEUROLOGICAL DISORDERS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7LEGAL AND REGULATORY ISSUES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Protection of Neural Graft Recipients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Protection of Donors of Fetal Tissue . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Government Oversight . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
ETHICAL ISSUES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9POLICY ISSUES AND OPTIONS FOR CONGRESSIONAL ACTION . . . . . . . . . . . . . . . 11
Figure Page
1-1. Components of the Nervous System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Figures
1-2. Methods Used To Graft Genetically Modified Cells . ......,..........*.**,..*,,. 61-3. National Institutes of Health 1989 Estimates of Costs of Neurological Disorders . . 7
TablesTable Page1-1. Prevalence of Neurological Disorders in the United States . . . . . . . . . . . . . . . . . . . . . . 31-2. Federal Funding of Neural Grafting Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4

Chapter 1
Summary, Policy Issues, and Options for Congressional Action
Tens of millions of Americans suffer from someform of neurological disorder. Some of thesedisorders are minor and are easily treated withmedication or rest. Others are marked by severe,debilitating symptoms and result in pain, suffering,and sometimes death. Some neurological disordersmay be treatable by neural grafting—i.e., thetransplantation of tissue into the brain and spinalcord (table l-l). Although few neural graftingprocedures have been carried out to date, the numbercould increase in the future.
Neural grafting has long been used in basicresearch to study the nervous system. In fact, muchneural grafting continues to be used as a tool forunderstanding the development of the nervoussystem and its response to injury. In addition to itsuse as a research tool, however, neural grafting isbeing examined as a possible therapy for neurologi-cal disorders. In the clinical arena, neural graftingconsists of the surgical transfer of tissue fromvarious sources into specific areas of the nervoussystem that have been affected by a disease or injury.This report focuses on the field of neural graftinginto the brain and spinal cord to treat neurologi-cal disease and injury.
Current treatments for neurological disordersinclude drugs, surgery, physical therapy, and behav-ioral interventions. These treatments may improvesignificantly as advances in the field of neuroscienceprovide a better understanding of the causes and
Table l-l—Prevalence of Neurological Disordersin the United States
Neurological disorder Prevalence
Alzheimer’s disease . . . . . . . . . . . . . . . . 1 to 5 millionStroke . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.8 millionEpilepsy . . . . . . . . . . . . . . . . . . . . . . . . . . 1.5 millionParkinson’s disease . . . . . . . . . . . . . . . . 500,000 to 650,000Multiple sclerosis . . . . . . . . . . . . . . . . . . . 250,000Spinal cord injury. . . . . . . . . . . . . . . . . . . 180,000Brain injury. . . . . . . . . . . . . . . . . . . . . . . . 70,000 to 90,000’Huntington’s disease . . . . . . . . . . . . . . . . 25,000Amyotrophic lateral sclerosis . . . . . . . . . 15,000a Estimate of persons permanently disabled from head injury.
NOTE: Prevalence is defined as the total number of cases of a diseaseestimated to be in existence in the United States at any given time.
SOURCE: Office of Technology Assessment, 1990.
mechanisms of neurological injury and disease. Formost neurological disorders, current treatments donot provide a cure, but rather relief of symptoms. Itis possible that neural grafting could provide a curein some cases where current treatments cannot (e.g.,injury) or could bring about sustained relief fromsymptoms where existing therapies either fail or losetheir effectiveness (e.g., certain diseases, such asParkinson’s). Because of this potential, transplanta-tion of tissue into the central nervous system (CNS)may become a significant therapeutic alternative inthe future.
Currently, grafting of tissue into the CNS totreat neurological disorders is highly experimen-tal. Neural grafting has advanced to clinical humanresearch only for the treatment of Parkinson’sdisease; for other applications, basic research iscontinuing. (Federal funding of neural graftingresearch is presented in table 1-2.) While severalstrategies for the use of neural grafting haveemerged, much additional basic research is neededto determine in what ways and to what extent neuralgrafting may be beneficial. It has the potential fortreating damage to the brain and spinal cord, therebybenefiting millions of Americans with impairedneurological functions. Realizing the benefits ofneural grafting will depend on a better under-standing of both the potential uses of neuralgrafts and the mechanisms underlying neurologi-cal disorders.
This report is about the technology of neuralgrafting, the neurological disorders that it may beused to treat, the patient populations that might beaffected, and the issues raised by the development ofthis technology. Two considerations related to thedevelopment of neural grafting are:
. sources of materials for transplantation, and
● protection of human subjects in research.
In particular, concerns have been raised aboutwhether or under what circumstances to use humanfetal tissue as a graft material and when to movefrom the laboratory to clinical research.
–3–

4 ● Neural Grafting: Repairing the Brain and Spinal Cord
Table 1-2—Federal Funding of Neural Grafting Research (in millions of dollars)
Agency 1987 1988 1989 1990a
National institutes of Health:National institute of Neurological Disorders
and Stroke . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4.1 6.5 7.3 7.5National Eye institute . . . . . . . . . . . . . . . . . . . . . . . . 1.2 1.4 1.6 1.6National institute on Aging . . . . . . . . . . . . . . . . . . . . . 1.1 1.1 1.6 2.1National institute of Child Health and
Human Development . . . . . . . . . . . . . . . . . . . . . . . — 0.2 0.4 0.4Alcohol, Drug Abuse, and Mental Health
Administration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.3 0.3 0.5 0.4Department of Veterans Affairs. . . . . . . . . . . . . . . . . . . 0.4 0.5 0.5 0.5National Science Foundationa . . . . . . . . . . . . . . . . . . . . 0.2 0.2 0.2 0.2a Estimated.SOURCE: Office of Technology Assessment, 1990.
GENERAL FEATURES OFTHE NERVOUS SYSTEM
AND NEURAL GRAFTING
The fundamentals of neural grafting are basedon an understanding of how the nervous systemgrows and develops, how it responds to injuryand disease, and the mechanisms underlyingneurological disorders. The nervous system isdivided into the CNS and the peripheral nervoussystem (PNS) (figure l-l). The brain and spinalcord, which make up the CNS, are complex struc-tures that control and regulate all of the activities andfunctions of the body. Cells of the brain and spinalcord are much more flexible in their ability to growand form interconnections during development thanin the fully formed CNS. Also, PNS elements canregrow following an injury, even in an adult,whereas regrowth in the CNS is extremely limited.Neural grafting takes what is known about thesephenomena and the mechanisms underlying neuro-logical disorders and tries to harness them to repairthe injured or diseased nervous system.
Neural grafting differs from organ transplan-tation, wherein an entire diseased or injured organ,such as the heart or kidney, is replaced with a healthyone. Although neural grafting may entail replacinga diseased portion of the brain, animal experimentssuggest that it may also serve a number of otherfunctions and may use tissues from a variety ofsources. Thus, neural grafting is a generic termthat includes many different treatment goals andmaterials.
Therapeutic Strategies
How a neural graft improves CNS function withinthe graft recipient is not completely understood. Infact, neural grafts display a wide range of potentialcapabilities. These diverse functions lead research-ers to predict that neural grafts may be employedto accomplish different treatment goals in differ-ent neuropathological disorders. Continued re-search is necessary to determine precisely howneural grafts function and how those functions canbenefit a graft recipient. Three possible functions ofneural grafts have been identified:
●
●
●
They may provide a continuous supply ofchemical substances that have been depleted byinjury or disease in affected regions of the brainor spinal cord.They may introduce new substances or cellsthat promote neuron survival, neuron regrowth,or both.They may replace nerve cells in the CNS thatwere lost to injury or disease.
Materials for Neural Grafting
Several types of biological materials maybe usedfor neural grafting, each of which raises uniquetechnical issues. The most important determinant ofa particular material’s usefulness is its ability toimprove CNS function with minimal risk to therecipient.
Tissue from the fetal CNS, because of its abilityto develop and integrate readily within a hostorganism, has been extensively studied. Manyscientists consider fetal CNS tissue to be the mosteffective material currently available for neuralgrafting. However, ethical, social, and political

Chapter 1--Summary, Policy Issues, and Options for Congressional Action ● 5
Photo credit: C. Freed, Department of Medicine and Pharmacology,University of Colorado
A portion of the dissected human fetal centralnervous system.
issues surrounding its use have been raised in theUnited States and propel the search for alternativematerials. Other materials that are being examinedinclude PNS tissue; peripheral autonomic neurons;tissue from outside the nervous system; and isolated,cultured, or genetically engineered cells (figure 1-2).
Determinants of Successful Neural Grafting
To survive grafting, cells must endure mechanicaland metabolic disruption during preparation forgrafting, and they must incorporate into the foreign,and potentially hostile, environment of the host. Thesurgical technique and specific material used forneural grafting are important determinants of suc-cess. Immature tissue can survive grafting morereadily than its mature counterpart. The ability ofgrafted materials to avoid immunological rejectionby the host and to obtain ready access to nutritionalsupport and a supply of oxygen by becomingincorporated with the host blood supply are majordeterminants of graft survival.
Potential Risks
As with any surgical intervention, neural graft-ing presents risks to the recipient. Unfortunately,many of the risks attributed to neural grafting areeither poorly understood or simply speculative.Before neural grafting can become routine in hu-mans, the risks must be carefully delineated, mini-mized, and measured against expected benefits.Problems may result from complications associatedwith the neurosurgery itself or immunological rejec-tion of the graft. Concerns that grafts could induceunwanted psychological effects, be a means for
Figure l-l-Components of the Nervous System
Z@R%. brain
PNS Y/y ~ ,7,
\*/
< :.. . -:..x....: . .. .. .. .., .:. . . .. . . .. . .. . . . . . *.>?,. .. . .-,.. . . .
1
..: . -.. +..,.: ‘~,,,.*=—
@ii
t:. . ‘ ““’ spinali~.>. -. . .. .. . . . . <,. . . . . cord. . . : “..,. . 6 - .. .spiner
‘ W4W? spine
The nervous system is composed of the central (CNS) andperipheral nervous systems (PNS).SOURCE: C. Romero-Sierra, fVeuroanatorny, A Conceptual Approach
(New York, NY: Churchill Livingstone, 1986).
transmitting bacterial and viral infections, or growexcessively once implanted have also been raised.
APPLICATIONS OF NEURALGRAFTING INTO THE BRAIN AND
SPINAL CORDThe technology of grafting into the brain and
spinal cord to restore functions lost throughdisease or injury is still very much in the initialstages of development. Research in animals hasindicated that neural grafting may provide beneficialtherapeutic effects in some neurological conditions,notably Parkinson’s disease. But in every case,including Parkinson’s disease, there is still muchinformation that needs to be collected before neuralgrafting can be adapted for general use in humans.Research currently being conducted in this field is

6. Neural Grafting: Repairing the Brain and Spinal Cord
Figure 1-2—Methods Used To Graft GeneticallyModified Cells
//Grow cells
t
1° cells \
Culture cells
-
J~\EE/ $Biochemical Genetic
characterizationSelect modified cells
modification
SOURCE: F. Gage, Department of Neuroscience, School of Medicine,University of California, San Diego.
aimed at learning more about basic mechanismsinvolved in grafting tissues into the CNS and theactions and effects neural grafts can exert there.
Scientists use many different kinds of experi-ments with animals to obtain this information. Theneed for animal models that mimic a given neurolog-ical disorder in humans is as important in the field ofneural grafting as it is in most other areas of clinicalresearch. The closer an animal model is to the humancondition of interest (in terms of the neurologicaldamage induced and the behavioral effects thatdamage produces), the easier it is to extend observa-tions from the model to a human disorder. Virtuallyall scientists in the field of neural grafting believe itis essential to develop good animal models for usein neural grafting experiments.
Neural grafting has been used to treat somepatients with Parkinson’s disease; however, thisclinical use of neural grafting, begun in the early1980s, has generated controversy in the scientificand medical communities. The tissue used hascome from two sources: the recipient’s adrenal glandand the fetal CNS. In both cases, there is someconcern that the treatment has been used prema-turely. In the case of adrenal grafting, many observ-ers believe that there has been a rush to proceed withhuman trials without having first collected adequatedata from animal experiments. In the case of fetaltissue grafts, while there is a larger base of animaldata to draw on, there is still concern that widespreadimplementation of human fetal tissue grafting could
Photo credit: J.R. Slade~ Jr.
A picture of a graft of monkey fetal tissue implanted into thebrain of an adult monkey.
proceed before adequate information has been de-rived from experimental studies.
As of 1990, between 300 and 400 persons withParkinson’s disease had received neural graftsworldwide, with about 100 of them having receivedfetal tissue grafts. In the United States, approxi-mately 130 patients have been treated with adrenaltissue, while fewer than 10 have had fetal tissueimplants. The use of fetal tissue for implantation islimited in the United States to privately fundedventures because the Secretary of Health and HumanServices has imposed a moratorium on Federalfunding of research involving the transplantation ofhuman fetal tissue obtained from induced abortionsinto human subjects.
The question of whether clinical experimentsusing grafting procedures to treat Parkinson’s dis-ease patients should continue before additional dataare gathered from animal experiments is unan-

Chapter 1--Summary, Policy Issues, and Options for Congressional Action ● 7
swered. In the case of adrenal grafts, many personsin the medical and scientific communities haveretreated from the rush of enthusiasm that accompa-nied their initial use. In the case of fetal tissue grafts,many believe that questions can best be answeredwith additional animal research, coupled with lim-ited human experimentation.
The use of neural grafts for other neurologicaldisorders is still at the stage of animal experimen-tation. Much basic research is being conducted toexamine what role grafts might play in a variety ofneurological conditions. For neurodegenerative dis-eases (e.g., Huntington’s disease, Alzheimer’s dis-ease, and motor neuron disease), the ability of graftsto provide lost neurotransmitters, replace lost cells,and stimulate growth in the diseased brain is beingstudied. Neural grafts are being used in animalmodels of brain and spinal cord injury in hopes ofreversing functional deficits by inducing regrowth orreplacing damaged areas. In conditions such asepilepsy, neuroendocrine defects, and demyeli-nating diseases (i.e., multiple sclerosis), the abilityof grafts to supply specific chemicals to control orreverse the effects of these disorders is beingexamined.
Neural grafting holds the promise of newtreatments for neurological disorders, but a finaldetermination of its usefulness must await moreinformation about the mechanisms underlyingneurological disorders, graft functions, and howthose functions relate to various neurologicaldisorders.
RELEVANT NEUROLOGICALDISORDERS
Since neural grafting is in the very early stages ofdevelopment, predicting its ultimate utility is specu-lative at best. However, since current animal re-search intimates that neural grafting may be appliedto the study and treatment of diverse neurologicaldisorders, this technology may have a significantimpact on medicine and society.
Neurological disorders are a significant cause ofillness, disability, and death in the United States.They cost, by conservative estimates from theNational Institutes of Health, more than $100 billionper year in medical expenses and lost income (figure1-3). Not all neurological disorders are amenable totreatment by neural grafting. The Office of
Figure 1-3-National Institutes of Health 1989Estimates of Costs of Neurological Disorders
Alzheimer’s disease
Stroke
CNS injury
Epilepsy
Movement disorders”
Multiple sclerosis
Amyotrophlc lateralsclerosis t 1 1 1 1
0 10 20 30 40 50 60Billions of dollars
● Parkinson’s and Huntington’s diseases.NOTE: Costs are per year, including medical care, lost income, etc.SOURCE: National institutes of Health.
Technology Assessment identifies those disordersthat may one day be treatable with graftingtechnology. A disorder was considered treatableif current understanding of its nature and causesuggests that neural grafting may be a beneficialtreatment approach or if results from animalexperiments offer support for this possibility.
These neurological disorders afflict persons of allages. Adolescents and young adults are most likelyto suffer from epilepsy, head or spinal cord injury, ormultiple sclerosis; Huntington’s disease andamyotrophic lateral sclerosis first appear in middleage; stroke, Alzheimer’s disease, and Parkinson’sdisease afflict primarily the elderly.
Preventive measures can reduce the incidence ofCNS injury, but the causes of the other diseases areunknown. While in every case the pathologicalhallmarks of the disorder can be described, there isno cure for the nerve cell death and abnormalfunctioning that cause mortality and morbidity.Research involving genetic analysis, molecular biol-ogy, and new drug development, as well as neuralgrafting, continues to advance our understanding ofthe various disorders and possible treatments forthem.
LEGAL AND REGULATORYISSUES
To the extent that Federal funds are used tosupport research involving neural grafts or to pay for

8 ● Neural Grafting: Repairing the Brain and Spinal Cord
the clinical use of such procedures, Federal regula-tions govern the conduct of that research. Even ifFederal funds are not used, the Federal Governmenthas powers under the interstate commerce clause toregulate neural grafting research. This power is thebasis for the establishment of the Food and DrugAdministration (FDA), the prohibition on paymentto organ donors for transplantation, and the regula-tion of medical laboratories engaged in interstatecommerce. The Federal Government may, under thePublic Health Service Act, regulate intrastate activi-ties as necessary to prevent transmission or spread ofcommunicable diseases. However, questions havebeen raised about the extent to which these mecha-nisms address neural grafting procedures. Someexisting Federal policies governing experimentationand organ transplantation could affect tissue trans-plants, but they were developed before the recentextensive debate on fetal tissue transplantation.
Protection of Neural Graft Recipients
Department of Health and Human Services(DHHS) regulations apply to all research withhuman subjects that is conducted or funded byDHHS [45 CFR 46.101]; in addition, DHHSregulations are used widely as guidelines by otherinstitutions, regardless of whether they receiveFederal funding. These regulations specific thatresearch protocols be reviewed and approved by anInstitutional Review Board (IRB), that selection ofsubjects be equitable, and that informed consent beobtained from each subject. IRB review is alsonecessary for any product for which marketingapproval is sought from the FDA. Informed consentis defined by Federal regulations which specify whatinformation must be provided to the research sub-ject. Other Federal regulations pertain to research onparticularly vulnerable groups, including the men-tally disabled, and provide guidelines for IRBapproval and informed consent related to researchinvolving these subjects. Such regulations may alsopertain to those experimental neural transplantsubjects who are mentally impaired. In researchprograms where there is no Federal involvementor influence, government oversight will dependon whether there are State statutes, although fewStates have statutes that address human experi-mentation in any detail.
Decisions regarding the safety and efficacy ofneural grafting materials are likely to come withinFDA jurisdiction. However, FDA’s role in regulat-
ing neural grafting materials is complicated bythe fact that there are several different types ofmaterials, each of which raises slightly differentquestions. In addition, neural grafting materialsrepresent developing technologies that have not yetbeen directly addressed by the FDA. The FDA hasjurisdiction over the manufacture and distribution ofmaterials that meet statutory definitions of drugs,devices, or biologics. Safety considerations and theFDA’s current regulation of similar products makeit likely that the agency will seek to regulate mostneural grafting materials. Questionable jurisdictionunder the Public Health Service Act could limitFDA’s ability to regulate these materials, since it isunclear whether neural tissue grafts, cell lines, andproducts of biotechnology to be used as neural graftsare analogous to the articles listed as biologics in thestatute. Other legal issues include questions of FDAjurisdiction when a neural graft is produced andperformed intrastate and jurisdiction in relation tothe practice of medicine.
Unlike the intricate system of regulation to ensurethe safety and efficacy of articles intended for use inthe diagnosis, treatment, or prevention of disease inhumans, there is no direct Federal regulation of newsurgical procedures developed for the same pur-poses. New surgical procedures are usually subjectto IRB review and are regulated indirectly bythird-party payers, including Federal insurers suchas the Health Care Financing Administration, theDepartment of Veterans Affairs, and the Departmentof Defense, which decide whether or not to reim-burse. Other forms of indirect regulation includehospital standards set by the Joint Commission onAccreditation of Healthcare Organizations, profes-sional standards of practice, State licensing laws,and medical malpractice cases. This system ofindirect regulation will preside over the develop-ment and introduction of neural grafting proce-dures using materials that fall outside the juris-diction of the other Federal regulatory mecha-nisms.
Protection of Donors of Fetal Tissue
Since fetal tissue is one of the possible sources ofneural grafts, Federal regulations and State lawsgoverning the donation and use of embryos and fetaltissue in research may apply. Federal regulations[45 CFR 46.201-211] lay out specific guidelinesfor research conducted on living fetuses. Underthese regulations, certain types of fetal research are

Chapter I-Summary, Policy Issues, and Options for Congressional Action ● 9
allowed, with constraints based on obtaining paren-tal consent and minimizing risk to the pregnantwoman and the fetus. They defer to State laws onthe subject of research on fetal cadavers.
The overwhelming majority of State legislatureshave yet to address the issues associated withexperimental neural grafting using fetal tissue. OnlyMissouri and Pennsylvania have enacted legislationdirected specifically toward fetal tissue transplants.Although other States have not specifically ad-dressed the question of neural tissue grafts fromfetuses, the general fetal research laws pertaining toresearch on living fetuses, in effect in 25 States, maycome to bear on it. Of these 25 States, 14 haveprovisions regulating research with fetal cadavers.In addition, 16 of the State fetal research statutesprohibit the sale of fetal tissue, 7 of them for anypurpose and 9 for research purposes. The mostsignificant factor in regulating research on dead orlive fetuses and in determiningg the extent ofrestriction imposed appears to be whether theresearch concerns a fetus that has been or is to beintentionally aborted. Most of the State fetal re-search statutes were passed as part of abortionlegislation.
Government Oversight
Issues and questions raised by the introductionand development of neural grafting procedurescould make other government regulatory mecha-nisms relevant. For example, issues and legalquestions regarding restrictions imposed on researchcould be raised. Not all regulations on research areconstitutional. Laws restricting research may bestruck down as too vague or as violating the equalprotection clause of the Constitution. Laws applyingto experimentation on fetuses or in the context ofabortion may violate the constitutional right toprivacy. Some legal commentators posit that there isa constitutional right to undertake or participate inresearch; however, even if undertaking and partic-ipating in research were constitutionally protected,certain restrictions to further health and safety couldbe permissible.
Regulations regarding the disposition of ca-davers, particular fetal remains, may be ofrelevance. Most State statutes specify when fetaldeaths must be registered and how fetal remains areto be disposed of. These statutes are important notonly because they provide penalties for unauthor-
ized uses of dead bodies, but also because theydetermine what must be done with fetal remainsonce their research or clinical value has beenexhausted and what reports must be filed.
The Uniform Anatomical Gift Act (UAGA) isof special significance because it is the onlyuniform body of law that might be used toregulate fetal tissue implants. Adopted in all 50States, the UAGA regulates the donation anddistribution of cadaveric organs. While it includesfetuses and their tissues, some States exclude theseprovisions from their version of the UAGA. Be-cause this Act was drafted before neural graftingtechnology became known, it was not designed toaddress the specific and unique problems thatfetal grafts raise, and some of its provisions maynot be appropriate for this use.
The possibility that women might be paid for fetaltissue for transplants has raised particular concernwithin some groups. The National Organ Trans-plant Act (NOTA) bans the sale of certain listedorgans (including certain fetal organs and theirsubparts) [42 U.S.C. 274(e)] and provides that theSecretary of Health and Human Services may listadditional organs. Since the brain, spinal cord,and other components of the nervous system arenot listed as organs, payment for use of fetalnervous system tissue for transplantation will notbe banned until the Secretary so designates. Apartfrom NOTA, the procurement of fetal tissue isregulated by State statutes.
ETHICAL ISSUESNeural grafting technology is a complex subject
for ethical discussion because of the scope of theissues it raises. Some ethical issues raised by neuralgrafting are not unique to this technology, as theyconcern the allocation of limited resources and thetension between the Federal Government’s commit-ment to promote the public health by fundingbiomedical research and its responsibility to respondto public concern about certain research and itspossible applications.
Public funding of biomedical technology involvesbroad analyses of economic benefits and costs, aswell as possible social benefits and ethical conse-quences of the new technology. Knowledge ofeconomic consequences is necessary for financialplanning, but it is also integral to ethical decision-making, since the allocation of public funds raises

10 ● Neural Grafting: Repairing the Brain and Spinal Cord
questions about justice and equity. Some peoplebelieve that justice requires the expenditure of fundsin areas where they can benefit the greatest numberof persons. To resolve some of these questions, itmight be helpful to evaluate neural grafting inrelation to treatments for other diseases, keeping inmind the priorities set and the amount of researchfunded. In order to make decisions about fundingneural grafting research, it will be necessary toestimate the efficacy of the technology, the numberof people now affected by the neurological disorder,and the number likely to be affected in the future.
The use of various grafting materials and the risksof surgery to recipients of grafts also raise ethicalissues. The most ethically problematic issue is theuse of fetal tissue. Fetal tissue from spontaneousabortion or ectopic pregnancy has been suggested asan acceptable source of graft material since thistissue is free of association with elective abortion.There is some question as to whether the physiolog-ical anomaly that caused the pregnancy to end wouldalso cause increased risk to the graft recipient afterimplantation. While using fetal tissue from thera-peutic or spontaneous abortions may avoid associa-tion of neural grafting with elective abortion, it maynot be a practical source of graft material.
Tissue obtained from electively aborted fetuses iscurrently believed to be the most promising neuralgraft material, but it is also the most controversial.The primary impediment to resolving this ethicalissue has been the lack of consensus about the moralrelevance of elective abortion to any subsequent useof the tissue. The positions taken on the morality offetal tissue grafting, however, do not necessarilyreflect a person’s beliefs about the morality ofabortion. Both supporters and opponents ofabortion rights have articulated reasons forsupporting fetal tissue grafting research, andboth have identified reasons for not doing so.Although personal opinions on fetal tissue trans-plantation tend to be consistent with personalopinions on elective abortion.
Arguments for and against the use of electivelyaborted fetal tissue for neural grafting stem fromissues raised by current research and issues that maybe raised if neural grafting is accepted as standardmedical practice in the future. These include ques-tions of whether the grafting procedure deniesrespect for fetal life by using the fetus as a means toan end. There has also been discussion of whether
groups besides fetuses, such as women and societyat large, maybe adversely affected by a policy thatendorses fetal tissue grafting. Some claims havebeen made about the consequences of neural graftingin the future, such as the effect this research mayhave on the number of elective abortions performedin the United States. Currently, there is no evidenceto support or refute the contention that fetal tissuegrafting research would cause an increase in thenumber of abortions performed.
The use of small amounts of fetal tissue to startcell lines that can be propagated in a laboratory mayallay some concerns about the consequences ofusing electively aborted fetal tissue for neuralgrafting. Such use complicates the issue of consent,however, because questions are raised aboutwhether the tissue donor has property rights. Forexample, although it maybe deemed appropriate fora woman who aborts to consent to the use of fetaltissue in a cell line, it may not be consideredappropriate for her to profit financially from it.While questions regarding the ownership of tissuesused for commercially profitable cell lines are beingaddressed by the courts, discussion has been limitedto the ownership of adult tissues. Questions pertain-ing to ownership of fetal tissue remain unanswered.
Controversy also exists about whether the womanwho elects to have the abortion is the appropriateperson to give consent for fetal tissue donation and,if so, when consent should be solicited. Both theregulations for the protection of research subjectsand those for the donation of body parts have beensuggested as models for fetal tissue donation, butthese regulations do not explicitly cover the dona-tion of fetal tissue for transplantation research.
The ethical issues related to neural graft recipientsrekindle discussions about the treatment of researchsubjects and the meaning of informed consent.While these issues are not unique to neural grafting,they may warrant special attention for this technol-ogy. Existing regulations may not adequately pro-tect recipients from the risks unique to this surgery.The possibility of doing a sufficient risk-benefitanalysis has been challenged on the grounds that notenough research has been done to know what thebenefits of neural grafting are likely to be. Obtaininginformed consent may be difficult, both because therisks and benefits cannot be realistically estimated atthis time and because persons with neurologicaldisorders may also have cognitive limitations.

Chapter I-Summary, Policy Issues, and Options for Congressional Action ● 11
POLICY ISSUES AND OPTIONSFOR CONGRESSIONAL ACTIONThree policy issues related to neural grafting were
identified during the course of this assessment:
Federal funding of human fetal tissue trans-plantation research,the adequacy of existing Federal laws andregulations regarding the use of human fetaltissue, andthe role of the Federal Government in guidingthe development and promoting the safety andefficacy of neural grafting procedures.
Associated with each policy issue are severaloptions for congressional action, ranging fromtaking no action to making substantial changes.Some of the options involve direct legislative action.Others involve the executive branch, but withcongressional oversight or direction. The order inwhich the options are presented do not imply anypriority. Moreover, the options are not, for the mostpart, mutually exclusive; adopting one does notnecessarily disqualify others within the same cate-gory or in any other category. A careful combinationof options might produce the most desirable effects.It is also important to keep in mind that changes inone area may have repercussions in other areas.
ISSUE 1: Should the Federal Government fundhuman fetal tissue transplantation research?
A number of grafting materials are being studiedfor their usefulness in ameliorating the symptoms ofneurological disorders. Neural tissue from humanfetuses is a promising source of neural graftingmaterial; however, the Department of Health andHuman Services (DHHS) has imposed a moratoriumon the use of Federal funds to support researchinvolving the implantation of human fetal tissuefrom induced abortions into human patients. Firstimposed in March 1988, the moratorium was ex-tended indefinitely in November 1989.
Option 1: Take no action.
If Congress takes no action, it appears that themoratorium will stand indefinitely, resulting in alack of Federal funds for both neural grafting andother areas of research using human fetal tissue anda consequent lack of Federal involvement in theconduct of such research.
Photo
As a result of the moratorium, research involvingthe implantation of human fetal tissue from inducedabortions into human patients can only be funded byprivate sources. Since the inception of the morato-rium, a few privately funded efforts to examine fetalneural grafts for the treatment of Parkinson’s diseasehave been undertaken in the United States. The lackof Federal support for these neural grafting studieshas limited the scope of Parkinson’s disease researchin the United States.
As basic research continues, neural graftingtechniques using human fetal tissue may be devel-oped to treat other neurological disorders. Thetransition from animal to human studies may bedifficult without Federal funding. Lack of Federalfunds for clinical studies could retard the develop-ment of these techniques in the United States,leaving progress to be made by other countries,where this research is continuing. Some observerssuggest that the moratorium has had the secondaryeffect of discouraging basic research in neuralgrafting, resulting in the channeling of investigatorsinto other areas of biomedical research.

12 ● Neural Grafting: Repairing the Brain and Spinal Cord
Privately funded clinical research is regulatedunder applicable State laws. Although Federalregulations, including review of research protocolsby a local Institutional Review Board (IRB), areoften voluntarily used to guide privately fundedresearch, there is no requirement that they be used.Thus, in the absence of Federal funding, fetal tissuetransplantation research can proceed without theoversight required for federally funded biomedicalresearch. This oversight includes the peer reviewprocess established by funding agencies such as theNational Institutes of Health (NIH) or the Alcohol,Drug Abuse, and Mental Health Administration(ADAMHA), and without the steering function of
these agencies to ensure efficient, standardizedcollection of data.
Option 2: Commission a study to assess the impacton society of the lack of Federal funding forhuman fetal tissue transplantation research.
Congress could commission a study by a govern-mental or nongovernmental agency, such as theNational Academy of Sciences, to assess the impli-cations for society of the lack of support by theFederal Government of fetal tissue transplantationresearch. Public debate has highlighted a number ofareas that could be affected by Federal support ofthis research, including the manner and timing of theprocurement of fetal tissue; the possible commer-cialization of fetal tissue; the conditions for in-formed consent for donation of the tissue; the effectthat the use of fetal tissue could have on theincidence of abortion; and the implications that thelack of Federal funding could have for the acquisi-tion of new biomedical information and the develop-ment of new treatments for some neurologicaldisorders. To date, there has been no comprehensivestudy of what effects Federal funding might have onthese areas. The results of such a study could be usedto guide policy decisions and develop guidelines forFederal funding of fetal tissue transplantation re-search.
Option 3: Enact legislation to permit Federalfunding of human fetal tissue transplantationresearch.
Congress could reinstate Federal funding ofhuman fetal tissue transplantation research andintroduce guidelines for its implementation throughdirect legislative mandate. Guidelines could bebased on the recommendations of the NIH’s HumanFetal Tissue Transplantation Research Panel, which
was convened under the direction of the AssistantSecretary for Health in 1988. The DHHS EthicsAdvisory Board, which was disbanded in 1980,could also be reconvened to propose guidelines.
Such legislation would most likely result inincreased research in neural grafting in the UnitedStates. Increased research could clarify the role thatneural grafts might play in some neurologicaldisorders and could result in the development of newtherapies for those disorders.
On the other hand, some observers have expressedthe concern that if Congress takes this action andresearch in this area were to increase, a number ofdetrimental effects could ensue. Arguments made bysupporters of the moratorium include concerns thatFederal funding of human fetal tissue transplanta-tion research might encourage induced abortion; thatthe number of induced abortions in the United Statesmight increase; and that, in the absence of carefullycrafted guidelines, negative effects related to thedonation, procurement, distribution, and transplan-tation of fetal tissue could occur.
ISSUE 2: Do existing Federal laws and regula-tions governing organ transplantation ade-quately address concerns raised by humanfetal tissue transplantation?
Concerns over the possible commercialization offetal tissue and the lack of regulation of its use havebeen raised in public debates about human fetaltissue transplantation. Neither DHHS regulations forthe protection of human subjects [45 CFR 46] northe National Organ Transplant Act (NOTA) explic-itly addresses the use of cadaveric fetal tissue inneural grafting, although either could be amended todo SO.
The DHHS regulations for the protection ofhuman subjects apply to research supported orconducted by DHHS, although they are oftenvoluntarily followed for privately funded research.These regulations impose specific conditions onresearch involving living fetuses or their tissues.With respect to research involving fetal cadavers orthe use of cadaveric fetal tissue, the regulations statethat research must be conducted according to Stateand local laws. The extent to which other provisionsof the DHHS regulations apply to research usingtissue obtained from a fetal cadaver is unclear.NOTA bans the sale of certain organs (includingfetal organs and their subparts) and provides that the

Chapter 1--Summary, Policy Issues, and Options for Congressional Action ● 13
Secretary of Health and Human Services may listother organs. The brain, spinal cord, and othercomponents of the nervous system are not listed asorgans covered by NOTA.
The Uniform Anatomical Gift Act (UAGA),which was drafted by the Commissioners on Uni-form State Laws and adopted in all 50 States, is theonly other body of law that might be used to regulatethe use of cadaveric fetal tissue for neural grafts. Itprovides guidelines for the donation and receipt ofcadavers for research, education, therapy, andtransplantation. The UAGA specifically includesstillborn infants and fetal cadavers, although someStates have excluded fetuses from their provisions ofthe law. However, some observers feel that there areprovisions of the UAGA that do not take intoaccount concerns raised by fetal tissue donation. TheUAGA allows the next of kin, starting with eitherparent and following a fixed order of priority, todonate fetal tissue and allows the donor of the tissueto designate a recipient. It also allows consent fordonation to be sought immediately before death. Ifthis last provision were applied in the case of fetaltissue, it might allow consent to be obtained from apregnant woman before an abortion. The ethics ofdesignating a recipient and obtaining consent fordonation before an abortion are controversial. Thequestion of who has the right to donate tissue froman elective abortion has also been raised. Thus theappropriateness of some of the provisions of theUAGA for the regulation of the donation of fetaltissue for transplantation is in question.
Option 1: Take no action.
In the absence of congressional action, no directFederal regulatory framework pertaining to the useof cadaveric fetal tissue for transplantation wouldexist. While some aspects of fetal tissue transplanta-tion would continue to be covered under the UAGAand other State laws, such regulations differ fromState to State. No specific regulations would pertainto the use of cadaveric fetal tissue for transplantationresearch supported by DHHS, and payment for fetalbrain, spinal cord, or other components of thenervous system will not be banned by Federal law,although it might be banned by State laws.
Option 2: Establish a congressional commission torecommend Federal policy on human fetal tissuetransplants.
Congress could establish a commission to exam-ine the comprehensiveness of existing legislationand regulations surrounding the use of human fetaltissue for transplantation. Such a commission couldsuggest guidelines for regulating the donation,procurement, distribution, and use of fetal tissue fortransplantation. Findings could be used to directfurther Federal regulatory and legislative action or toamend the UAGA.
Option 3: Encourage the National Conference ofCommissioners on Uniform State Laws to amendthe Uniform Anatomical Gift Act.
Congress could encourage the Conference,through a letter of request by a Committee or throughlegislation, to amend the UAGA to take into accountthe issues raised by the donation of cadaveric fetaltissue. While the Conference is under no obligationto respond to congressional initiatives, taking thisaction would indicate Congress’ concern about theappropriateness of some of the provisions of theUAGA for dealing with fetal tissue donation.
Option 4: Direct the Secretary of Health andHuman Services to amend the current Depart-ment of Health and Human Services regulationsregarding the protection of human subjects.
Congress could direct the Secretary of Health andHuman Services to amend existing regulations toaddress specifically the use of cadaveric human fetaltissue for transplantation research. Such regulationscould guide the procurement, distribution, and use offetal tissue. If Congress takes this action, it wouldresult in the establishment of uniform, specificregulations for the use of tissue from fetal cadaversin federally funded research.
Option 5: Mandate that the brain and nervoussystem tissue be added to the list of organscovered by the National Organ Transplant Act.
NOTA lists certain organs (including those froma fetus) that cannot be bought or sold and providesthat the Secretary of Health and Human Servicesmay add other organs to the list. The brain, spinalcord, and other components of the nervous systemare not now on that list. Congress could add them,either by amending NOTA directly or by directingthe Secretary of Health and Human Services to doso. Taking this action would result in a Federalinjunction against the buying or selling of tissuefrom the fetal nervous system and would thus ban

14 ● Neural Grafting: Repairing the Brain and Spinal Cord
the commercialization of fetal nervous tissue for usein neural grafting procedures.
ISSUE 3: Should the Federal Government takefurther action to guide the development andpromote the safety and efficacy of neuralgrafting procedures?
The development of new medical and surgicalprocedures, such as neural grafting, generally pro-ceeds through a series of stages. First, basic researchis conducted using animal models and other experi-mental designs. Based on the results of these studies,researchers may proceed to clinical research, prior tointroduction of the procedure as standard therapy.However, unlike the elaborate Federal regulatoryframework that guides the development and intro-duction of new drugs and medical devices to ensuretheir safety and efficacy, there is little direct Federaloversight of the development and introduction ofnew medical and surgical procedures.
Because of the diverse nature of neural graftingmaterials, it is unclear where in the Federal regula-tory framework neural grafting procedures will fall.In addition, concerns have been raised about thecriteria that have been used to move neural graftingfrom the laboratory to clinical research.
Option I: Take no action.
If Congress takes no action, the Food and DrugAdministration (FDA) could seek to regulate thedevelopment of those neural grafting procedures thatuse materials which fall under its jurisdiction. Therewill be little or no Federal regulation of neuralgrafting materials that do not come under FDAoversight. In such cases, and in the absence ofcongressional action, decisions concerning when thetransition from animal to human studies shouldoccur, how human research should be carried out,and when a neural grafting procedure ceases to beexperimental will be made through traditional mech-anisms for the development of new surgical proce-dures.
The decision to move from animal to humanstudies, as was made for the use of neural grafts forthe treatment of Parkinson’s disease, is generallymade by individual researchers or institutions. Forfederally supported studies, research protocols aresubject to the peer review process conducted byFederal funding agencies and to DHHS regulationsfor the protection of human subjects. These regula-
tions require that research proposals be approved bythe local IRB; however, IRBs have no specificcriteria for moving from animal studies to humantrials. While nonfederally funded studies may besubmitted to local IRB scrutiny and may undergo apeer review process, there is no requirement thatthey do so. If Congress takes no action, the decisionof when a neural grafting procedure is ready toproceed from animal to human experimentation willbe made in this way. Some observers believe thatthis framework did not provide adequate guidance inthe case of neural grafting for the treatment ofParkinson’s disease, resulting in a premature moveto clinical trials. Others believe that additionaloversight would be unduly burdensome and couldstifle scientific progress.
In clinical research, the designs of the studies andthe protocols followed are determined by the re-searchers involved. Coordination of efforts, to en-hance the efficient collection and analysis of data (ashas been attempted in some trials of neural graftingfor the treatment of Parkinson’s disease), is some-times undertaken voluntarily by professional socie-ties, private organizations, or agreements betweenresearch groups. Federal funding agencies can im-pose criteria for the conduct of research and thusensure more efficient data collection and analysis. Inthe absence of congressional action, the develop-ment of neural grafting procedures in humans mayproceed in a fashion that does not optimize thecoordination of research efforts, which could resultin an inefficient collection of the data necessary tomake a determination about the safety and efficacyof procedures.
Data collected during clinical trials guide thetransition from research to standard therapy. Neuralgrafting procedures have not yet reached this stage,but it is possible that they may. Clinical use andavailability of a procedure are indirectly regulatedby third-party payers, professional societies, Statelicensing laws, and medical malpractice claims.There is no direct Federal oversight of this process;however, the Federal Government regulates it indi-rectly in its role as an insurer of medical care. TheHealth Care Financing Administration (HCFA)determines when sufficient information is availableto warrant Medicare or Medicaid coverage; HCFAmay also establish criteria that must be met byfacilities providing the procedure. The Departmentof Defense, through the CHAMPUS insuranceprogram, and the Department of Veterans Affairs are

Chapter 1--Summary, Policy Issues, and Options for Congressional Action . 15
also third-party payers. The decisions of theseFederal agencies often influence private third-partypayers’ decisions to reimburse for a new medical orsurgical procedure and the medical community’sdecision to provide it.
The Agency for Health Care Policy and Research(AHCPR), established within DHHS to promoteresearch on selected surgical and medical proce-dures in order to assess their appropriateness,necessity, and effectiveness, could also play a role inthis process. If directed to do so, the AHCPR couldserve as a Federal mechanism for assessing neuralgrafting procedures. In the absence of congressionalaction, AHCPR may or may not choose to studyneural grafting procedures.
Option 2: Direct that the National Institutes ofHealth establish guidelines for neural graftingresearch protocols with humans.
Congress could direct the Secretary of Health andHuman Services, through NIH, to provide IRBs andpeer review boards with guidelines concerningproposed grafting research projects using humansubjects. Such guidelines could provide informationabout the status of the procedure, what animalresearch has been conducted, and whether sufficientdata have been collected to warrant the transitionfrom animal to human studies. These guidelinescould be used to direct decisions regarding federallyfunded research proposals and provide guidance fordecisions about nonfederally funded studies.
Option 3: Direct the Secretary of Health andHuman Services to coordinate federally fundedhuman neural grafting trials in order to optimizethe collection of data.
Congress could direct the Secretary of Health andHuman Services, through NIH and ADAMHA, tocoordinate federally funded human neural graftingtrials. Such coordination could take a number offorms, such as designating specific centers to carryout experimental trials using uniform protocols andprocedures or requiring federally funded studies tofollow specified guidelines concerning experimen-tal design and the collection of data. By taking thisaction, Congress could ensure that federally fundedexperimental trials to determine the safety andefficacy of neural grafting procedures would pro-ceed in the most efficient manner.
Option 4: Mandate that the Agency for Health CarePolicy and Research monitor the development ofneural grafting procedures.
The AHCPR, through the Medical TreatmentEffectiveness Program, assesses the medical effec-tiveness and patient outcomes associated with se-lected medical and surgical procedures. Congresscould direct AHCPR to assess the development ofneural grafting procedures and develop guidelinesfor the use of these procedures.

Chapter 2
Introduction
CONTENTSPage
DISORDERS . .......,?*..........*..*,*,.....,.* 20NATURE OF NEUROLOGICALInjury ... .*. ... ... ... ... ... ... ... ... ... ... ... ..*. ... .*. ... **+** c**+* *a. **G****. 20Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . *.***.. . . . . . . . .*. . . . ,*. 20
APPROACHES TO TREATMENT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21HISTORICAL PERSPECTIVE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21FEDERAL INTERESTS . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22THE OTA STUDY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24CHAPTER 2 REFERENCES ... ..*. ..*. ... ... ... ... ... ..*. +.. ..*** e.**. ..*** .. t**** 24
FigureFigure Page2-1. Annual publications on Grafting Into the Nervous System . . . . . . . . . . . . . . . . . . . . . . 22
TablesTable Page2-1. Tissue and Organ Transplants in the United States, 1989 . . . . . . . . . . . . . . . . . . . . . . . 192-2. Landmarks for Neural Grafting in Mammalian Central Nervous Systems 232-3. Federal Funding of Neural Grafting Research
. . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24

Chapter 2
Introduction
Tens of millions of Americans suffer from someform of neurological disorder. Some of thesedisorders are minor and are easily treated withmedication or rest. Others are marked by severe,debilitating symptoms and result in pain, suffering,and sometimes death. These conditions includedementias, such as Alzheimer’s disease; movementdisorders, such as Parkinson’s disease; damagecaused by stroke or injuries to the brain or spinalcord; and epilepsy. Some of these neurologicaldisorders may be treatable by neural grafting—i.e., the transplantation of tissue into the brainand spinal cord.
In 1989, over 500,000 Americans received tissueor organ transplants. The vast majority of theseoperations involved transplantation of bone, cornea,kidney, liver, heart, pancreas, lung, and bone mar-row (table 2-l). A small number of procedures,however, involved neural grafts. Although fewneural grafting procedures have been carried out todate, the number could increase in the future.
The use of neural grafting in the laboratory isnot new. It has long been used in basic research tostudy the nervous system. In fact, much neuralgrafting continues to be used as a tool for under-standing the development of the nervous system andits response to injury. In addition to its use as aresearch tool, however, neural grafting is beingexamined as a possible therapy for neurologicaldisorders.
In the clinical arena, neural grafting consists of thesurgical transfer of tissue from various sources intospecific areas of the nervous system that have beenaffected by disease or injury. The ability of neuralgrafts to repair injured nerves in the peripheralnervous system has been studied fairly extensively.Examination of the potential therapeutic effects ofneural grafts within the central nervous system(CNS) (i.e., the brain and spinal cord) is a morerecent field of study. This report focuses on thefield of neural grafting into the brain and spinal
Table 2-l—Tissue and Organ Transplants inthe United States, 1989
Material transplanted Number
Bone or bone fragment . . . . . . . . 450,000 (approximate)a
Cornea . . . . . . . . . . . . . . . . . . . . . 36,900’Kidney . . . . . . . . . . . . . . . . . . . . . . 8,886Bone marrow . . . . . . . . . . . . . . . . 2,500 (approximate)Liver . . . . . . . . . . . . . . . . . . . . . . . . 2,160Heart . . . . . . . . . . . . . . . . . . . . . . . 1,673Pancreas . . . . . . . . . . . . . . . . . . . 412Lung . . . . . . . . . . . . . . . . . . . . . . . 89Heart and lung . . . . . . . . . . . . . . . 70Neural . . . . . . . . . . . . . . . . . . . . . . <30a 1998~SOURCE: United Network for Organ Sharing; American Association of
~ssue Banks; Eye Bank Association of America; North Ameri-can Autologous Transplant Registry; International Bone MarrowTransplant Registry; Office of Technology Assessment, 1990.
cord to treat neurological disorders. It is aboutthe technology of neural grafting, the neurologi-cal disorders that neural grafts may be used totreat, the patient populations that might beaffected, and the legal and ethical issues raised bythe development of this technology.
Although therapeutic neural grafting into the CNSof humans is relatively new, several strategies for itsuse have emerged. These strategies can be groupedas follows:
● grafts to replace lost chemicals of the nervoussystem;
● grafts to stimulate growth and promote survivalof cells in the nervous system; and
. grafts to replace lost structures in the nervoussystem.
Much additional basic research is needed todetermine in what ways and to what extent neuralgrafting may be beneficial. It has the potential fortreating damage to the brain and spinal cord, therebybenefiting millions of Americans with impairedneurological functions. Realizing the benefits ofneural grafting will depend on a better understand-ing of both the potential uses of neural grafts and themechanisms underlying neurological disorders.
–19-

20 ● Neural Grafting: Repairing the Brain and Spinal Cord
NATURE OF NEUROLOGICALDISORDERS
Injury
Injury to the CNS can result from mechanicaldamage to the brain or spinal cord (e.g., skullfracture, concussion, wounds from projectiles,broken backs) or a disruption in the normal flowof blood to the brain (e.g., stroke). It can result inshort- or long-term impairment. Blunt injury to thehead, for example, can result in immediate butshort-term unconsciousness that has no lastingeffect. Blunt injury to the head can also cause severetrauma to the brain (swelling, decreased blood flow,lack of oxygen, and massive cell death), resulting inpermanent paralysis, loss of the sense of touch orability to feel pain, loss of cognitive function, ordeath. Severe trauma, such as that which can occurin automobile collisions or sports injuries, can causeprofound and often permanent damage to the spinalcord. Such damage usually results in paralysis andsevere physical disability. The ability of graftedmaterial to replace tissue lost through injury and topromote recovery following an injury is a major areaof investigation.
Disease
The brain and spinal cord are complex and fragileorgans susceptible to a number of diseases. Amongthem are neurodegenerative disorders, demyeli-nating disorders, and epilepsy.
Neurodegenerative Disorders
Neurodegenerative disorders are a class ofneurological diseases marked by the loss ofspecific nerve cell population(s) in the brain orspinal cord. In most cases, the cell loss is a gradualprogression that continues indefinitely. Neurode-generative disorders include Parkinson’s disease,Huntington’s disease, Alzheimer’s disease, andamyotrophic lateral sclerosis (Lou Gehrig’s dis-ease). The nature of the functional loss or impair-ment associated with a neurodegenerative disorderis directly related to the population of neuronsaffected. In Parkinson’s disease, for example, theloss of dopamine-producing cells in the substantialnigra results in such motor symptoms as tremors andrigiditv. while in Alzheimer’s disease loss of acetyl-
choline-producing cells in the forebrain results incognitive deficits such as memory loss and confu-sion. Although the cause of the selective loss of cellpopulations in neurodegenerative disorders remainsunknown, it is possible that multiple factors areresponsible. It is also possible that the ultimatemechanism of cell death in these disorders may besimilar, although the stimuli that trigger the mecha-nism could be quite different in each.
Neural grafting might play a number of roles intreating neurodegenerative disorders or their symp-toms. Neural grafts could replenish chemicals thathave been depleted by cell loss, replace the lost cellswith new ones that could reestablish contacts withother brain cells, or furnish growth factors that couldprotect threatened cells or stimulate new growthfrom other cells. All of these potential applicationsare being studied in animal models and otherexperimental paradigms to determine their feasi-bility.
Photo credit: National Institutes of Health
A patient undergoing a brain scan.

Chapter Introduction ● 2 1
Demyelinating Disorders
Demyelinating disorders are marked by loss ofthe fatty material (myelin) that surrounds manyaxons in the brain and spinal cord. When a cellloses this myelin sheath, its ability to send messagesis impaired. Myelin loss can be caused by certaintypes of injuries and by disease. One of the mostcommon demyelinating diseases is multiple sclero-sis. The ability of grafted myelin-producing cells toreplace myelin lost as a result of disease or injury iscurrently being explored.
Epilepsy
Epilepsy is a disruption of the normal electricalactivity of the brain. It can occur in a specific,confined area of the brain, or it can involve the entirebrain. The seizures normally associated with epi-lepsy result from an episode of abnormal electricalactivity in the brain. Epilepsy can occur spontane-ously or as a result of disease or injury to the brain.Neural grafts are being examined in animal researchfor their ability to curtail the number and severity ofepileptic seizures.
APPROACHES TO TREATMENTCurrent treatments for neurological disorders
include drugs, surgery, physical therapy, and behav-ioral interventions. For most disorders, currenttreatments do not provide a cure, but rather relief ofsymptoms. Nevertheless, treatments are likely toimprove significantly as advances in the field ofneuroscience provide a better understanding of thecauses and mechanisms of neurological injury anddisease. It is possible that neural grafting couldprovide a cure in some cases where current treat-ments cannot (e.g., injury) or could bring aboutsustained relief from symptoms where existingtherapies either fail or lose their effectiveness (e.g.,certain diseases, such as Parkinson’s disease).
Currently, grafting of tissue into the nervoussystem to treat neurological disorders is highlyexperimental. It is just beginning to emerge into theclinical arena, and there is a great need for basicresearch to determine the scope of its effectivenessin a variety of disorders. To date, neural grafting hasonly been used to treat a relatively small number ofpatients. However, because of its potential toreplace damaged nerve cells, restore chemicalslost through injury to nerve cells, and stimulatenerve cell growth and regeneration, grafting of
tissue into the CNS may become a significanttherapeutic alternative in the future.
HISTORICAL PERSPECTIVEThe first report of attempted tissue transplantation
into the brain is attributed to W.G. Thompson, anAmerican scientist. Thompson published a briefaccount of his animal experiments in 1890 (3). Anumber of reports followed over the next 20 years,but it was not until 1917 that E. Dunn frostdemonstrated that CNS tissue transplanted fromnewborn rodents into adult rodents could surviveover an extended period of time, provided thetransplanted tissue was in an immature, developingstate. During the following 50 years, only occasionalreports on transplantation into the CNS appeared. Inthe last 20 years, however, there has been anexplosion of experimental work in this area(figure 2-l). Some historical landmarks in neuralgrafting into the mammalian CNS are presented intable 2-2.
The vast majority of neural grafting experi-ments to date have been conducted on animalmodels (e.g., rodents and nonhuman primates).The first grafting experiments on humans wereundertaken in 1982 in Sweden in an attempt totreat Parkinson’s disease (2). The Swedish groupimplanted dopamine-producing cells into the brainsof Parkinson’s disease patients whose medicationwas no longer effective. The cells came from eachpatient’s own adrenal gland in order to minimize thechances of rejection by the body’s immune system.It was theorized that replacing the lost dopamine inthe brain would ameliorate some of the characteristicsymptoms of Parkinson’s disease. From 1982 to1984, neural transplants were performed on fourpatients. The patients, however, did not show anysignificant, long-term improvement (7).
In 1986, a neurosurgical team from Mexico Cityannounced substantial amelioration of most of theclinical signs of Parkinson’s disease after transplant-ing adrenal tissue to the patient’s brain (10). Basedon the success reported by this group, many othergroups attempted the procedure, and by mid-1989over 300 patients in at least six countries (Swe-den, Mexico, United States, Cuba, Spain, andChina) had received adrenal cell transplants,with mixed results.
Since many researchers failed to achieve the levelof success reported by the Mexican group, a number

22 ● Neural Grafting: Repairing the Brain and Spinal Cord
Figure 2-l—Annual Publications on Grafting Into the Nervous System
200
150
100
50
U.J.AuA
1890 1900 1910 1920 1930 1940 1950 1960 1970 1980 1988
YearSOURCE: Adapted from J.R. Sladek, Jr., and D.M. Gash (eds.h Neura/ Tramdants: fkdomnent and/%nction (New.
Yo~, NY: Plenum Press, 1984)..,
of the transplant groups in the United Statessuspended neural grafting with adrenal cells. Somegroups raised questions about the efficacy of thisapproach in humans, the amount of animal experi-mentation done prior to use of the procedure onParkinson’s patients, and the magnitude of effectseen in these animal studies (12). However, reportsof limited success in treating Parkinson’s patientswith neural grafting of adrenal cells continue toappear in the scientific literature (1,5,6).
In 1988, grafting of human fetal CNS tissueinto the brain was announced by the sameMexican and Swedish research groups that hadpreviously performed adrenal cell transplants inParkinson’s patients (9,11). Subsequently, severalcenters around the world—in the People’s Republicof China, Cuba, Spain, Great Britain, and the UnitedS t a t e s - b e g a n performing these procedures. FetalCNS tissue was chosen for grafting because devel-oping tissue is more likely to become integrated inthe brain and restore lost or damaged nervous systemfunctions than mature CNS tissue. Despite the moreextensive animal research preceding this move tohuman experiments, concerns were still raised aboutthe efficacy and experimental nature of this treat-ment for Parkinson’s disease. The use of humanfetal tissue from elective abortions has also raisedethical questions. Recently, some beneficial effects
from human fetal tissue grafts have been reported ina limited number of Parkinson’s disease patients(4,8).
In a few instances, neural grafting has beenattempted inpatients suffering from other neurolog-ical disorders. (See ch. 5 for a complete descriptionof the history of neural grafting in Parkinson’sdisease and its use to date in other disorders.)
FEDERAL INTERESTSAs is often the case in the biomedical sciences, the
development of neural grafting has raised scientific,legal, and ethical issues, including:
● protection of human subjects in research, and● sources of tissue for transplantation.
The role of the Federal Government in theresearch, development, and regulation of neuralgrafting is questioned by some parties.
A continuing question in biomedical researchis when to move from the laboratory to theclinical arena. How much animal experimentationshould be conducted before performing new orinnovative procedures on humans? What kind ofanimal experimentation should be conducted? Howshould the results be assessed? What mechanismsand safeguards exist to guide the development of

Chapter Introduction ● 2 3
Table 2-2—Landmarks for Neural Grafting in Mammalian Central Nervous Systems
Year Researcher Accomplishment
18901898
1907
1909
19111917
1921
1924
1940
1957
1979
1982
1985,1986
1987
W.G. Thompson (U. S.A.) . . . . . . . . . . . . . . . . . .
J. Forssman (Sweden) . . . .’.. . . . . . . . . . . . . . .
G. Del Conte (Italy) . . . . . . . . . . . . . . . . . . . . . . .
W. Ranson (U. S.A.) . . . . . . . . . . . . . . . . . . . . . .F. Tello (Spain) . . . . . . . . . . . . . . . . . . . . . . . . . .
E. Dunn (U.S.A.) . . . . . . . . . . . . . . . . . . . . . . . . .Y. Shirai (Japan) . . . . . . . . . . . . . . . . . . . . . . . . .
G. Faldino (ltaly) . . . . . . . . . . . . . . . . . . . . . . . . .
W.E. LeGros Clark (U.K.) . . . . . . . . . . . . . . . . . .
B. Flerko and J. Szentagothai (Hungary) . . . . .
A. Bjorklund and U. Stenevi (Sweden)M.J. Perlow et al. (U.S.A.) . . . . . . . . . . . . . . . . . .
E.O. Backlund et al. (Sweden) . . . . . . . . . . . . . .
R.A.E. Bakay et al. (U.S.A.)D.E. Redmond et aL (U.S.A.) . . . . . . . . . . . . . . .
O. Lindvall et al. (Sweden)l. Madrazo et al. (Mexico); . . . . . . . . . . . . . . . . .
Attempt to graft adult CNS tissue into brain
Neurotrophic effects of grafted CNS tissue
Attempt to graft embryonic tissues into brain
Successful grafting of spinal ganglia into brain
Successful grafting of peripheral nerve into brain
Successful grafting of neonatal CNS tissue into adult brainDemonstration of brain as an immunologically privileged site
Successful grafting of fetal CNS tissue into anterior eye chamber
Successful grafting of fetal CNS tissue into neonatal brain
Successful intraventricular grafting of endocrine tissue
Functional recovery after grafting dopamine-producing cells into the brainHuman neural graft with adrenal chromaffin cells (autograft)
Reversal of experimentally induced Parkinson’s disease in nonhumanprimates
Human fetal tissue graft (allograft)
NOTE: All experimental work performed in animals unless otherwise indicated.SOURCE: Ada@ed from A. Bi&klund and U. Stenevi (eds.), “lntracerebral Grafting: A Historical Pers@ctive,” Neural Grafting in the Mamm~ian CNS
(Amsterdam: Elsev~er Science Publishers, 1985).’
new treatments from conception and evolution in theclinical research environment to accepted medicalpractice?
In its efforts to protect the public health, theFederal Government regulates one important aspectof medical care, namely, the development, testing,and marketing of drugs, biologics, and medicaldevices. Are similar regulatory schemes necessaryor desirable to protect patients’ welfare in clinicaltrials of medical and surgical procedures? Is thepresent system of Institutional Review Boards,under the auspices of the Department of Health andHuman Services, adequate to safeguard patients incases of experimental surgical procedures? Whendoes an experimental surgical or medical procedure,such as neural grafting, become standard therapy?
Related to these questions is the issue of the typeand function of the material to be grafted. There aremany possible sources of material for neuralgrafts. One is cultured and genetically manipulatedcells. Because of the nature and possible functions ofthese materials (e.g., as drug delivery systems),regulation would probably fall under the jurisdictionof the Food and Drug Administration (FDA).Another possible source of material is unmanipu-lated tissue from other organs or fetal tissue. These
substances may not be regulated by the FDA, sincethey do not fall under its jurisdiction and their use asneural grafting material may be considered thepractice of medicine. Thus, depending on whatmaterial is used, there may or may not be directFederal oversight of neural grafting technologies.
An issue of particular concern is the procure-ment and use of human fetal tissue for neuralgrafting procedures. Because of its unique charac-teristics, human fetal tissue is a widely used sourceof neural grafting material. Although many scien-tists believe that it may ultimately be superseded insome proposed applications by other sources ofmaterial (e.g., cell lines, genetically manipulatedcells), they also believe that this is not likely to occurin the near future. Most scientists feel that, atpresent, continued study of fetal tissue is neededto discern the mechanisms that underlie theability of the nervous system to heal and toevaluate what role fetal tissue grafts can play inthat process.
Many of the same concerns that have been voicedabout organ transplantation in general pertain to theuse of human fetal tissue for neural grafting. Theseinclude:

24 ● Neural Grafting: Repairing the Brain and Spinal Cord
Table 2-3-Federal Funding of Neural Grafting Research (in millions of dollars)
Agency 1987 1988 1989 1990’
National Institutes of Health:National Institute of Neurological Disorders
and Stroke . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4.1 6.5 7.3 7.5National Eye Institute . . . . . . . . . . . . . . . . . . . . . . . . 1.2 1.4 1.6 1.6National Institute on Aging . . . . . . . . . . . . . . . . . . . . . 1.1 1.1 1.6 2.1National Institute of Child Health and
Human Development . . . . . . . . . . . . . . . . . . . . . . . — 0.2 0.4 0.4Alcohol, Drug Abuse, and Mental Health
Administration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.3 0.3 0.5 0.4Department of Veterans Affairs . . . . . . . . . . . . . . . . . . . 0.4 0.5 0.5 0.5National Science Foundationa . . . . . . . . . . . . . . . . . . . . 0.2 0.2 0.2 0.2aEstimated.SOURCE: Office of Technology Assessment, 1990.
buying and selling of organs for transplanta-tion, and
legal authority for consent to donate organs ortissues.
Use of fetal tissue raises some additional sensitiveand controversial questions. Are the issues sur-rounding abortion relevant to the use of fetal remainsfor research and medical therapy? Should themoratorium on Federal funding of abortion have anybearing on Federal funding of research employingfetal tissue for transplantation? Should cadavericfetal tissue (i.e., tissue from dead fetuses) bediscarded when this material could provide a therapyfor neurological disorders? Are there potentialabuses in the acquisition and use of fetal tissue forwhich safeguards should be developed?
In 1988, the Assistant Secretary for Health placeda moratorium on all federally funded therapeutictransplantation research that used human fetal tissuefrom induced abortions. This moratorium was ex-tended indefinitely in 1989. As a result of thisaction, no Federal funds can be used to supportthe transplantation of human fetal tissue ob-tained from an induced abortion into a patient.
Of continuing interest to Congress is the level offunding for both basic and clinical research and thedevelopment of new technologies (table 2-3). It hasbeen suggested that neural grafting has the potentialto treat millions of Americans with certain neurolog-ical disorders. However, questions about the pre-cise benefits of this technology, the particulardisorders that may be affected, and the timeframe for applying these technologies as humantherapies remain to be answered.
THE OTA STUDYThis report to Congress examines the develop-
ment of neural grafting into the central nervoussystem, i.e., the procedures and materials involvedin the transplantation of tissue to the brain and spinalcord for the treatment of neurological disorders.Although other advances in neuroscience have greatpotential in treating neurological disorders, thoseadvances are beyond the scope of this report.
In the six chapters that follow, OTA examines theimpact neural grafting is likely to have on thetreatment of neurological disorders and the legal,regulatory, and ethical issues these new proceduresraise. In addition, OTA examines the role ofCongress and the Federal Government in addressingthese public policy issues.
Chapters 3,4, and 5 describe basic principles ofneuroscience, general principles and concepts ofneural grafting, and the research that has beenconducted thus far on neural grafting as a treatmentfor neurological disorders. Chapter 6 identities someof the disorders that may be amenable to treatmentby neural grafting procedures, and chapters 7 and 8discuss the legal, regulatory, and ethical issuesassociated with neural grafting.
1.
2.
CHAPTER 2 REFERENCESApuzzo, M. L.J., Neal, J.H., Waters, C.H., et al.,“Utilization of Unilateral and Bilateral Stereotacti-cally Placed AdrenomedWary-Striata.l Autografts inParki.nsonian Humans: Rationale, Techniques, andObservations,” Neurosurgery 26:746-757, 1990.Baclclund, E. O., Granberg, P. O., Hamberger, B., etal., “Transplantation of Adrenal Medulkuy Tissue toStriatum in Parkinsonisrn, First Clinical Trials,”Journal of Neurosurgery 62:169-173, 1985.

Chapter 2--Introduction ● 25
3.
4.
5.
6.
7,
Bjorklund, A., and Stenevi, U. (eds.), “IntracerebralNeural Grafting: A Historical Perspective,” NeuralGrafting in the Mammalian CNS (Amsterdam:Elsevier Science Publishers, 1985).Freed, C.R,, Breeze, R.E., Rosenberg, N.L., et al.,“Transplantation of Human Fetal Dopamine Cellsfor Parkinson’s Disease, Results at 1 Year,” Archivesof Neurology 47:505-512, 1990.Goetz, C.G., Tanner, C.M., Pem, M.D., et al.,“Adrenal Medullary Transplant to the Striatum ofPatients With Advanced Parkinson’s Disease: l-YearMotor and Psychomotor Data,” Neurology 4Q273-276, 1990.Lieberman, A., Ransohoff, J., Berczeller, P., et al.,“Adrenal Medullary Transplants as a Treatment forAdvanced Parkinson’s Disease,” Acta NeurologicalScandinavia 126:189-1%, 1989.Lindvall, O., “Transplantation Into the HumanBrain: Present Status and Future Possibilities,”Journal ofNeurology, Neurosurgery, and Psychiatryspecial supp.:39-54, 1989.
8.
9.
10.
11.
12.
Lindvall, O., Brundin, P., Widner, H., et al., “Graftsof Fetal Dopamine Neurons Survive and ImproveMotor Function in Parkinson’s Disease,” Science247:574-577, 1990.Lindvall, O., Rehncrona, S., Gustavii, B., et al.,“Fetal Doparnine-Rich Mesencephalic Grafts inParkinson’s Disease” [letter], Lancet 2:1483-1484,1988.Madrazo, I., Drucker-Colin, R., Diaz, V., et al.,“open Microsurgical Autograft of Adrenal Medullato the Right Caudate Nucleus in Two Patients WithIntractable Parkinson’s Disease,” New EnglandJournal of Medicine 316:831-834, 1987.Madrazo, I., km, V., Torres, C., et al., “Transplan-tation of Fetal Substantial Nigra and Adrenal Medullato the Caudate Nucleus in Two Patients WithParkinson’s Disease” [letter], New England JournuZof Medicine 318:51, 1988.Sladek, J.R., Jr., and Gash, D.M., “Nerve-CellGrafting in Parkinson’s Disease,’ Journal of Neuro-surgery 68:337-351, 1988.

Chapter 3
Neuroscience Primer

CONTENTSPage
ORGANIZATION OF THE NERVOUS SYSTEM . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Cellular Components . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Central Nervous System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Peripheral Nervous System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Autonomic Nervous System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ●
N E U R A L COMMUNICATION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .GROWTH AND DEVELOPMENT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .*RESPONSE TO INJURY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .*.CHAPTER 3 REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
292930323232333436
BoxBox Page3-A. Neurotrophic and Neurotropic Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
FiguresFigure Page3-1. Components of the Nervous System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3-2. The Neuron . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3-3. Glial Cells . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3-4. The Central Nervous System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3-5. The Spinal Cord . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3-6. The Synapse . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3-7 A Neuron and Its Synapses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3-8. The Development of the Human Brain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3-9. The Response of a Neuron in the Peripheral Nervous System to Injury . . . . . . . . . .
293030313232333435

Chapter 3
Neuroscience Primer
This chapter describes the major anatomicalcomponents of the nervous system, some of the basicprocesses underlying neural growth, development,and communication, and the response of the nervoussystem to injury. A grasp of these basic concepts ofneuroscience is helpful to understanding neuralgrafting. Additional information is available from anumber of sources (1,3,4).
ORGANIZATION OF THENERVOUS SYSTEM
The nervous system can be divided into twoparts: the central nervous system (CNS) and theperipheral nervous system (PNS) (figure 3-l). TheCNS is made up of the brain and spinal cord. ThePNS is composed of all the nerves, nerve cells, andspecialized sensory receptors that lie outside theCNS. Sensory information about the outside worldis brought into the CNS via the nerves and sensoryreceptors in the PNS; activation and regulation ofactivity in muscles, glands, and organs are conveyedby the motor, or outflow, component of the PNS.Most information processing, decisionmaking, andcoordination of activities is under the control of theCNS.
Cellular Components
There are two major classes of cells in thenervous system: neurons, or nerve cells, and glia,or glial cells.
Neurons
All information processing in the nervous systemis done by networks of neurons that communicatewith each other. Neurons consist of a cell body withlong extensions, much like branches of a tree, calleddendrites. Also projecting out of the cell body is asingle fiber called the axon, which can extend forgreat distances (figure 3-2). All nerves in the bodyare actually the bundled axons of many neuronsconveying information to and from the CNS. Theend of the axon is also branched.
Glial Cells
Glial cells support neurons by carrying on impor-tant chemical and physiological reactions and pro-ducing a variety of substances that are needed for
normal neurological functioning. There are a num-ber of different types of glial cells in the PNS andCNS--astrocytes, microglia, Schwann cells, andoligodendrocytes (figure 3-3). Schwann cells (in thePNS) and oligodendrocytes (in the CNS) producemyelin, a fatty insulating material that forms asheath around axons and speeds the conduction ofelectrical impulses. Both of these types of cells playa crucial role in nerve cell regeneration: Schwanncells support regrowth of peripheral nerves, whilerecent evidence suggests that oligodendrocytes in-hibit the regrowth of damaged axons in the CNS.The other glial cells help regulate the biochemicalenvironment within the nervous system, provide
Figure 3-l-Components of the Nervous System
cranialnerves
/ \PNS ‘–
‘Pina’ m“nerves
CNS
/spinalcord
The nervous system is composed of the central (CNS) andperipheral nervous systems (PNS).SOURCE: C. Romero-Sierra, A/euroanatorny, A Conoeptua/ Approach
(New York, NY: Churchill Livingstone, 1986).
–29–

30 ● Neural Grafting: Repairing the Brain and Spinal Cord
Figure 3-2—The Neuron
Two neurons in synaptic contact.SOURCE: R. Restak, The Brain (New York, NY: Bantam Books, 1984).
structural support for the neurons, and supply certainsubstances that are essential for the nervous systemto work properly.
Central Nervous System
The Brain
One useful way of visualizing the brain is as amushroom. The cap of the mushroom is the cerebralcortex, and the stem of the mushroom is the rest ofthe brain, which is made up of hundreds of nuclei(figure 3-4). A nucleus is a group of cells that sharethe same anatomical region and, to varying degrees,the same function. Information is conveyed through-out the brain and spinal cord along the axonsextending from nuclei. For any given function, suchas vision, a number of nuclei and areas of thecerebral cortex must act together in a coordinatedand synchronized reamer so that information can beaccurately analyzed.
The anatomy of the brain and the intricacy of theconnections among nuclei are exceedingly complex.Information from every area of the nervous systemabout many different functions is constantly beingcombined, compared, contrasted, and coordinated.The brain determines the relevance of each bit ofinformation, fits it in with all other informationavailable, and decides what actions should or shouldnot be taken to regulate bodily functions and to
Figure 3-3-Glial Cells
B.
u.
Types of glial cells include: A) astrocytes, B) microglia, C)oliogdendrocytes, D) Schwann cells (surrounding an axon).SOURCE: Adapted from J.A. Kiernan, Introduction to Human Neuros-
cience (Philadelphia, PA: J.B. Lippincott, 1987).
permit successful interaction with the externalenvironment. The result is everything that makes uplife and existence as human beings perceive it—from the maintenance of heart rate to falling in love;from finding food to contemplating the nature of theuniverse. All of these arise from the biologicalevents that make up the activity of the human brain.

Chapter 3-Neuroscience Primer ● 31
Figure 3-4—The Central Nervous System
cortex
- - l
,1
. .. . . ,: ...,7.- --- I
Spinal cord
11I
The brain (cerebral cortex, upper brain, brain stem) and the spinalcord.SOURCE: Adapted from R. Restak, The Mind (New York, NY: Bantam
BOOkS, 1988).
The bottom of the stem of the mushroom is thebrain stem, which regulates essential bodily func-tions. Heart rate, blood pressure, and respiratoryactivity are all controlled by nuclei in the brain stem.Higher up the stem of the mushroom is the upperbrain, containing other structures, such as thehypothalamus and the thalamus. Each of these is acollection of nuclei with specific functions. The
thalamic nuclei are primarily involved in analyzingand relaying sensory and motor information. Somehypothalamic nuclei control behaviors such aseating, “drinking, and sexual activity; others helpwith regulating the activity of the endocrine system.Still further up the stem of the mushroom are thebasal ganglia, nuclei that help mediate movement.Also in this area are some of the nuclei of the limbicsystem, which is involved in emotional behaviors,and the hippocampus, a limbic nucleus that is alsoone of the nuclei crucial to learning and memory.These are only a sampling of the many nuclei locatedin the stem of the mushroom.
Overlying the stem is the cerebral cortex, theevolutionary newest part of the brain and its mostadvanced decisionmaking portion. The cerebralcortex consists of layers of neurons and their axons,which communicate with each other and with otherregions of the brain. Roughly divided into four lobeson each side, the cerebral cortex receives sensoryinformation and analyzes, deciphers, and puts it intocontext based on previous experience. Combiningnew input with experience, the cerebral cortexdecides what actions should be taken and institutesthose actions by activating the proper motor andendocrine networks. It is at the level of the cerebralcortex that differences among species become mostnotable. Warm-blooded animals have a more highlydeveloped cerebral cortex than cold-blooded ani-mals. The cortex is most fully developed in humans,with highly developed frontal lobes and specializedareas to subserve the development and use oflanguage. The frontal lobes are thought to be the seatof higher order thinking, which gives humans theability to engage in abstract thought and to developphilosophical concepts of morality, self, and place inthe universe.
The Spinal Cord
Extending downward ii-em the base of the stem ofthe mushroom is the spinal cord. The spinal cord iscomposed of a central core of cells surrounded bypathways of axons. Leaving and entering the spinalcord are the nerves that bring sensory informationinto the CNS and convey motor and other activatinginformation out into the periphery (figure 3-5). Thespinal cord is divided into 31 segments that aredemarcated by collections of nerves called nerveroots. The spinal segments and their nerve rootsserve the organs of the body and correspondingregions of muscles and skin in the limbs and along

32 ● Neural Grafting: Repairing the Brain and Spinal Cord
Figure 3-5-The Spinal Cord
Axons
Cell
Ventral root \.’<~ Nerve root
The spinal cord is made up of a central core of cell bodies,surrounded by axons. The nerve roots convey information into(dorsal root) and out of (ventral root) the spinal cord.SOURCE: Adapted from A.C. Guyton, Basic Neuroscience: Anatomy and
Physio/ogy(Philadelphia, PA: W.B. Saunders, 1987).
the trunk of the body. There is communicationamong segments and between the segments and thebrain. Some basic functions, such as motor reflexes,are organized and directed from within the spinalcord. The spinal cord also contains a column ofspecialized cells that help control the autonomicfunctions of the body (see later discussion of theautonomic nervous system). All the areas within thespinal cord that control bodily activities are modu-lated by the brain.
Peripheral Nervous System
The PNS is made up of all the sensory nervescoming into, and motor nerves leaving, the spinalcord via the nerve roots. These include the nerves ofthe autonomic nervous system. In addition, the PNSincludes some sensory and motor nerves that enterand exit from the brain stem.
Autonomic Nervous System
The autonomic nervous system is made up of theportions of the CNS and PNS that are concerned withthe control of visceral functions. These functionsinclude heart rate, blood pressure, digestion, andreflexive sexual activities. Within the CNS, theneurons of the autonomic nervous system are in thebrain stem and the spinal cord; in the PNS, theneurons occur in specialized groups, known asganglia. The ganglia are found in columns on either
Figure 3-6-The Synapse
00
00~o
Axon 0 0 000
terminal
‘“’’” Body of neuron
The anatomy of a synapse.SOURCE: Adapted from A.C. Guyton, Basic Neuroscience; Anatomy and
Physiology (Philadelphia, PA: W.B. Saunders, 1987).
side of the spinal cord or in close association with theorgans they serve (2).
NEURAL COMMUNICATIONInformation in the nervous system is conveyed by
chains of neurons. It usually travels through a neuronin one direction-horn the dendrites, through thecell body, and along the axon. The end of the axonof one neuron interacts with the next neuron in thechain. Information in the nervous system is codedas an electrical-chemical message that is sentfrom one neuron to the next. The point where theaxon of one neuron connects with a dendrite or cellbody of another neuron is called a synapse (figure3-6). The two neurons never actually touch eachother; instead, there is a small space between themcalled the synaptic space. Because the end of theaxon and the dendrites of a neuron are branched, theaxon of any one neuron can form synapses withthousands of other neurons and thus can sendmessages to and receive messages from thousands ofother neurons (figure 3-7).
When a neuron generates a nerve impulse, or‘‘ fires,’ an electrical message is sent along the axontoward the synapse. When the electrical messagegets to the synapse, it causes the release of achemical, called a neurotransmitter, from the axoninto the synaptic space. The neurotransmitter acts asa messenger, moving across the synaptic space andbinding to the membrane of the next neuron. The

Chapter 3--Neuroscience Primer ● 33
Figure 3-7-A Neuron and Its Synapses
The terminals of many axons can make synapses with thedendrites or cell body of one neuron.SOURCE: R. Restak, The Mind(New York, NY: Bantam Books, 1988).
binding of the neurotransmitter to the membranethen initiates, facilitates, or hinders an electricalmessage in that neuron. The time it takes for thisprocess to occur, from the initiation of a message inone neuron to the release and binding of theneurotransmitter and the initiation of a message inthe next neuron, is measured in thousandths of asecond.
There are many different kinds of neurotransmit-ters. Whether and when a neuron will release aneurotransmitter is determined by the combinedaction of all its synapses, with their excitatory andinhibitory neurotransmitters, at any one time.
GROWTH AND DEVELOPMENTIn humans, the first signs of the developing
nervous system appear in the third week of embry-onic development (figure 3-8). The cells destined toform the brain and other parts of the nervous systemthen go through a period of proliferation, duringwhich time they multiply. At the same time, the cellsmigrate to their proper positions in the developingbrain. Following this period of proliferation andmigration, the cells stop dividing and differentiateinto the various types of neurons and glial cells thatmake up the nervous system. At this time, thenumber of neurons becomes fixed; for the rest of theperson’s life, no new neurons are thought to be
produced. Most glial cells, on the other hand,maintain the capacity to replicate.
The mechanisms by which neurons migrate to theproper location and axons find their way to theproper target site and form synapses are not fullyunderstood. The process of axonal growth is thoughtto include an initial, genetically predetermined mapof axonal pathways. The growing axons are guidedto their final destinations by chemicals calledneurotrophic (nourishing) and neurotropic (guid-ing) factors (see box 3-A). Neurotrophic factorspromote axonal growth and neuronal survival, andneurotropic factors provide a surface, or substrate,for the axon to grow along to its target. These factorsact as signposts to guide the growing axons andprovide chemical addresses for them to reach. Whichchemical address, or target site, an axon will searchfor is believed to be genetically programmed withineach neuron.
Once the cells are in position, differentiationoccurs: the dendrites and axons of the neurons beginto grow and establish the proper synaptic contacts.In the case of some axons this can mean elongationover considerable distances, while in other cases allof the synaptic contacts of a neuron can occur withina few millimeters of the cell. The ultimate wiringof the brain, made up of billions of synapses andconnections, is extremely complex. Although inhumans most axons reach their target sites beforebirth, the final configuration of the synaptic contactsis not completed until well after birth.
There are many more neurons in the developingnervous system than there are in the mature nervoussystem. It has been estimated that about half of thecells initially generated die. Death is caused bycompetition between the growing neurons for avail-able synaptic sites and a matching of the number ofneurons to the needs of the developing nervoussystem. This process results in the survival of thoseneurons that have grown properly. There are about200 billion neurons in the mature human brain.
Although the general pattern of synapses estab-lished once an axon reaches its target is bothgenetically predetermined and under the control ofchemical factors, the final, precise synaptic patternof an axon can also be shaped by other factors. Theseinclude the amount and kind of activity that occur inthe pathway in response to outside stimulation. Thisflexibility in synapse formation in response to

34 ● Neural Grafting: Repairing the Brain and Spinal Cord
Figure 3-8-The Development of the Human Brain
6R&@@
25 days 35 days 40 days 50 days 100 days
Q. . . . . . . .. . . . .. .. . , .. .. .’, ’ ...,, -# . . . . . .. . . .!.... ,.,. .. . . :.. ,.:., .,, . ,, ..:
,.,..,,” . : . . . . . . . . .
. . ,, : ..;.”:’ .”:. . . ‘.’..,’., , ,.. ,: ;, -;2;:..:!”-.. ;?::./” : ,, -
, . ..;:”..”.””: . . ,x ““””””’” ‘K’.. ?“”:”
Five months
L’Eight months
\ L \Six months Seven months
The human brain shown in its developmental sequence, starting at 25 days and progressing through birth.SOURCE: R. Restak, The Brain (New York, NY: Bantarn Books, 1984).
environmental stimuli is maintained throughout lifeand may play a role in learning and memory.
RESPONSE TO INJURYThe CNS and PNS respond differently to injury.
When a peripheral nerve is damaged, the axonsof the damaged neurons can regrow; but whendamage occurs in the CNS, axonal regrowth islimited. Research on animals has shown that thisdifference is due not to differences in peripheral and
central neurons (in fact, many peripheral nerves arisefrom cell bodies in the CNS), but to variations in theenvironment surrounding the axons in the CNS andPNS.
The key element in axon regrowth in the PNS isthe presence of Schwann cells and the growth factorsthey secrete. Schwann cells normally surround eachaxon, supplying its fatty myelin sheath. When aperipheral nerve is damaged and dies, the bundledaxons die and leave behind the Schwann cells that

Chapter 3--Neuroscience Primer ● 35
Figure 3-9—The Response of a Neuron in the Peripheral Nervous System to Injury
A) The normal neuron and part of the axon; B) the axon is injured and the section away from the cell body dies; C) the end of the injuredaxon begins to grow into the remaining Schwann cells.SOURCE: RerXinted bv ~ermission from “Reactions of Neuronsto ldw,” Pri~@/= of~euro=ief=, pd ~.. E-R. Kandel and J.H. *hwartz (*.) (N’SWyOkJ. .
NY: Elsevie~ !3cience Publishers, 1985), p. 191. - -
had surrounded them. When the nerve regenerates,its axons grow within the column of remainingSchwann cells to the sense organ or muscle to whichthey were originally connected (figure 3-9).Schwann cells release neurotrophic and neurotropicfactors that promote elongation and provide apathway for the regenerating axons.
When the CNS is damaged, there is someregrowth that is limited to a small area around thewound. A process called synaptic sprouting occurs,whereby fibers from nearby, undamaged axons formnew branches and make new synapses to replacesome of the lost ones. However, unlike Schwanncells, the myelin-producing oligodendrocytes of theCNS do not promote regrowth of the damagedaxons. In fact, recent studies have shown that
oligodendrocytes actively block regeneration. Fur-thermore, following an injury, another type of glialcell, the astrocyte, forms a scar at the site of thewound and blocks regrowth. Why there are mecha-nisms in the CNS that actively block healing is notknown. It is thought that once all the wiring of thebrain is established, the growth-promoting mecha-nisms that were present during development are nolonger needed, and these inhibitory mechanismstake over to prevent any further growth that couldshort-circuit the completed brain. By learning moreabout the differences in the environments thatallow regeneration in the PNS and block it in theCNS, scientists may ultimately be able to controlthe processes involved and enable CNS damageto be repaired.

36 ● Neural Grafting: Repairing the Brain and Spinal Cord
Box 3-A—Neurotrophic and Neurotropic Factors
During the last few years, neuroscientist have learned that the development, maintenance of function, andresponse to injury of neurons are influenced by chemicals called neurotrophic and neurotropic factors. Thesesubstances are produced by some neurons and glial cells and can affect the nervous system in two ways. Some aresecreted by a cell into the spaces between cells in the nervous system; they can then be absorbed by neurons to initiatean intracellular process, such as growth of an axon. Other factors can act externally to guide the growing axon alonga particular path to its region of synaptic contact. A chemical that stimulates growth or development is called aneurotrophic agent, while one that helps guide a growing neuron is called a neurotropic agent.
Only a few substances have been positively identified as neurotrophic or neurotropic factors. Of them, nervegrowth factor (NGF) has been the most extensively studied NGF is a protein that is known to promote growth inspecific areas of the peripheral nervous system and to play a role in the development of vertebrate sensory systems.What role NGF plays in the central nervous system (CNS) is not well understood. It seems that NGF has a selectiveeffect on certain populations of cells in the brain that use acetylcholine as their neurotransmitter. NGF promotesgrowth and development of these cells in the fetal brain and, when extra amounts are administered in experimentalconditions, can promote growth and prevent cell death following an injury in the adult brain. It has also been shownthat NGF can facilitate the incorporation of some neural grafts. The observation that NGF seems to exert this effectonly on certain cells in the brain suggests that there maybe different neurotrophic factors for different groups of braincells. Thus far, other substances that have been identified as having possible neurotrophic or neurotropic effectsinclude ciliary neurotrophic factor, brain-derived neurotrophic factor, neurotrophin-3, glia-derived nexin, fibroblastgrowth factors, insulin and insulin-like growth factors, epidermal growth factor, S100 protein, and laminin. What rolethese play in CNS regeneration is unclear at this point.
Neurotrophic and neurotropic factors are known to be present in the developing CNS and to play an importantrole in the formation of neuronal circuitry. Much less is known about their role in the mature CNS. When an injuryoccurs in the brain, there is an increase in neurotrophic activity at the site of the wound. This activity seems to promotethe limited amount of healing and cell survival that is seen following some injuries. It is also thought that some ofthese factors are important for maintaining normal function and structural integrity in the adult brain. It has beenobserved that some neurons die in the absence of neurotrophic factors. It is possible that some of the factors associatedwith growth and development are either no longer present or are somehow inactivated within the adult CNS.Introducing missing factors or stimulating deactivated ones in the CNS by implanting tissues that produceneurotrophic and neurotropic factors may reestablish the environment needed for growth.
SOURCE: Office of Technology Assessment, 1990.
CHAPTER 3 REFERENCES tion, Apr. 25, 1990.
1. Adelman, G. (cd.), Encyclopedia of Neuroscience, 3. Ferry, G., “Getting Wired Up," New Scientist, Mar. 4,1989, pp. 1-4.vols. I and II (Cambridge, MA: Birkhauser Boston,
1987). 4. Kandel, E. R., and Schwartz, J. H., Principles of Neu-2. Coquelin, A., professor, Texas Tech University Health roscience (New York, NY: Elsevier Science Publish-
Sciences Center, Lubbock, TX, personal communica- ing, 1985).

Chapter 4
General Features ofNeural Grafting

CONTENTSPage
THERAPEUTIC STRATEGIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Source of Depleted Chemical Substances . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Promotion of Neuron Growth and Survival . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Replacement of Lost Structures in the Brain and Spinal Cord . . . . . . . . . . . . . . . . . . . . . . . 41
MATERIALS FOR NEURAL GRAFTING . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42Fetal Central Nervous System Tissue . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42Peripheral Nerve Tissue . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43Peripheral Autonomic Tissue . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44Tissue From Outside the Nervous System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45Isolated, Cultured, or Genetically Engineered Cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
DETERMINANTS OF SUCCESSFUL NEURAL GRAFTING . . . . . . . . . . . . . . . . . . . . ...49Developmental State of the Graft Material . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49Immune System Response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49Blood Vessel Formation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51The Age of the Host . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
POTENTIAL RISKS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52Immune System Reaction or Suppression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52Unwanted Psychological Effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52Effects of the Surgical Procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52Excessive Growth of Graft Material . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52Infection and Other Effects on the Host CNS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
SUMMARY AND CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53CHAPTER 4 REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
Box4-A. The Deep Freeze: Cryopreservation
BoxPage
of Fetal CNS Tissue . . . . . . . . . . . . . . . . . . . . . . . 46
FiguresFigure Page4-1. Injured Nerve Cells With and Without Growth Factor Treatment . . . . . . . . . . . . . . . 414-2. Fetal Central Nervous System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 444-3. Transplanted Fetal Nerve Cell . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 454-4. Peripheral Nerve Graft . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 454-5. Genetic Engineering of Graft Tissue . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 484-6. Blood-Brain Barrier in Transplanted Tissue . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 504-7. Blood Vessel Growth in Transplant . . . . . . . . . . . “. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51

Chapter 4
General Features of Neural Grafting
Neural grafting has been hailed as.. one of themost promising approaches to have come fromexperimental neurobiology as a potential therapy fora variety of disorders involving damage to thecentral nervous system” (41). It has also triggered adebate among physicians and medical researchersabout when a medical procedure should be advancedfrom a research tool in animals to a treatment inhumans. The use of neural grafting to treat patientssuffering from Parkinson’s disease has led to bothdramatic claims of success and more cautiousstatements of results. A proposal for neural graftingresearch prompted the Executive Branch of the U.S.Government to forbid Federal support of transplan-tation procedures employing human fetal tissuefrom induced abortions. All of this controversy begsa clear answer to the question, What is neuralgrafting?
The term neural grafting, as used in thisreport, refers to the transplantation of tissue intothe brain or spinal cord. Neural grafting differsfrom organ transplantation, wherein an entire dis-eased or injured organ, such as the heart or kidney,is replaced with a healthy one. Although neuralgrafting may entail replacing a diseased portion ofthe brain, animal experiments suggest that it mayalso serve as a drug delivery system, providingchemical substances to the central nervous system(CNS) of the graft recipient, or that it may be usedto promote recovery of the host’s injured brain orspinal cord. In addition, a neural graft may bederived from various types of tissues, including fetalCNS tissue, peripheral nervous tissue, cells fromother organs, or cell lines sustained in the laboratory.Thus, neural grafting is a generic term thatembraces many different treatment goals andmaterials.
This chapter focuses on the salient features ofneural grafting and issues related to its potential useto treat the diseased or injured CNS. Unless other-wise specified, data discussed in this chapter arederived from animal studies. Despite the publicitythat has recently attended neural grafting attempts inpatients suffering from Parkinson’s disease, theclinical usefulness of this approach is not certain. Inthe case of Parkinson’s disease, optimal methods forusing neural grafting are still under investigation. In
general, the development of innovative techniques,including the use of genetically engineered cells,relies on extensive basic research. Furthermore,many questions concerning the functional effects ofneural grafts, as well as the problems presented bytheir use, are unanswered. Neural grafting may,however, lead to promising treatments for neurolog-ical disorders, which often resist therapeutic inter-vention. Issues addressed in this chapter include:
What therapeutic strategies are possiblethrough neural grafting?What tissues and cells can be used for neuralgrafting?What factors influence the successful survivaland function of neural grafts?What potential risks are presented by neuralgrafting?
THERAPEUTIC STRATEGIESHow a neural graft improves CNS function within
the recipient is not completely understood. A neuralgraft may simply provide a depleted chemicalsubstance to the brain or it may permit othertherapeutic strategies as well (5,33,61). In fact,neural grafts display a wide range of capabilities.These diverse functions lead researchers to pre-dict that neural grafts will be employed toaccomplish different treatment goals in differentneuropathological disorders. Continued researchis necessary to determine precisely how neural graftsfunction and how those functions can benefit a graftrecipient (37). In this section, potential therapeuticstrategies are discussed. Neural grafts may:
● provide a source of depleted chemical sub-stances,
● stimulate neuron growth and promote survivalof neurons, and
● replace lost structures in the brain and spinalcord.
Source of Depleted Chemical Substances
Neural grafts may supply chemical substancesthat have been depleted in the CNS by injury ordisease.
The loss of neurons within the brain or spinal cordcan severely impair memory, the control of muscle
-39-

40 ● Neural Grafting: Repairing the Brain and Spinal Cord
movement, and other functions performed by thenervous system. Impaired CNS function may resultfrom a depletion of the chemical substances nor-mally produced by the degenerating or missingneurons. Conventional drug therapy can be em-ployed to replenish the supply of a depleted chemi-cal in the brain. However, several factors can makedrug therapy problematic. For example, someadministered substances are prevented from enteringthe CNS by the blood-brain barrier, which excludesmany cells and molecules in the blood from the CNS(11,74).
The current limited success in treating CNSdisorders via drug therapy may be circumvented bythe use of neural grafts. Cells that synthesize andsecrete a neurotransmitter (a messenger moleculeused by neurons in communication) or other chemi-cal substance may be implanted in the CNS; it isthought such implants may provide a continuoussupply of chemicals directly to the depleted regionof the brain or spinal cord.
It is postulated that neural grafts supply chemicalsubstances in one of two ways (5). If the graft iscomposed of cells that do not form connections(synapses) with the host neurons, it may simplysynthesize and release a steady and diffuse supply ofchemical substances to adjacent regions of the CNS,acting as a localized pump, or drug delivery system.If synapses are forged between graft and hostneurons, integrating the graft into a neuron network,the release of chemicals may be more carefullyregulated by the host neurons. In this case, ratherthan indiscriminately spewing chemicals near thegraft site, the grafted neurons may discharge thechemicals in a more controlled fashion at synapsesabutting host neurons.
Promotion of Neuron Growth and Survival
Neural grafts may introduce new substances orcells that promote and guide host neuron re-growth, prevent host neuron death, or both.
The complex network of nerve fibers within themature brain and spinal cord attests to the tremen-dous neuron outgrowth and synapse formation thatoccurs during development. Developing neuronsmay form long fibers and establish contact with asmany as 1,000 other neurons. While mature neuronsdo enjoy some regenerative potential, the ability toextend long fibers appears to be masked or inhibitedin the mature CNS. Anything more than modest
Photo credit: Laura Lee Hall
Injured nerve ceils.
injury of mature neurons often proves fatal to them.In general, glial cells inhibit neuron regrowthfollowing injury (20,76,84). Injured neurons may bepermanently disconnected from their targets withinthe CNS, they may degenerate and die, or both.Furthermore, neurons that die are not replaced, sincethey lack the ability to reproduce themselves.
Experimental evidence suggests that the degener-ative consequences of neuronal injury in the maturebrain and spinal cord can be prevented, or at leastameliorated, if a growth-promoting environment,such as that found in the developing brain, isprovided. In other words, recovery of injured neu-rons within the mature CNS may be enhanced bycells or chemical factors that promote neuronregrowth, neuron survival, or both (figure 4-l). It is

Chapter 4-General Features of Neural Grafting ● 41
speculated that neural grafts may be used in thiscapacity, stimulating neuron functions such as nervefiber and synapse growth or preventing neuron death(21).
A neural graft may lead to the recovery of injuredneurons in several ways. Grafted cells may synthe-size and release growth-promoting factors near theinjured neurons, preventing neuron death and pro-moting neuron regrowth. Neural grafts may also beused to form a bridge between a group of neuronsand their target within the CNS, bypassing theunfavorable environment of the mature CNS. Thesegraft materials may enhance neuron outgrowth andprovide a terrain over which it is directed. Neuralgrafts may also serve to reduce scar formation withinthe injured CNS or neutralize the growth-inhibitingeffect of the mature CNS (85,90). Other graftactivities, such as the removal of toxic substances,may also be possible (34).
A neural graft used to promote regrowth andrecovery of the host’s own brain or spinal cord tissuemay be required only temporarily, thus makinglong-term graft survival, which may be difficult toachieve, unnecessary.
Replacement of Lost Structures inthe Brain and Spinal Cord
A neural graft may be used to replace nervecells in the CNS that were lost to injury or disease.
Normal aging, injury, disease, or lack of oxygencan precipitate the death of nerve cells within theCNS. Since neurons generally are not replacedwithin the brain and spinal cord of adult mammals,their death leads to a permanent decrease in thenumber of neurons in the brain and creates a missinglink in neuronal networks. This loss of neurons anddisruption of neuronal networks may result in the
Figure 4-1—injured Nerve Cells With and Without Growth Factor Treatment
N(5F +NGFr
A f
v, ‘bs
? ‘ J!@” --””’* .-. ~ %4.
5
#,*,-
Photograph of brain section; nerve cells are darkly stained. Injured nerve cells on side D received nerve growth factor (NGF) and thereforesurvived injury. Injured nerve cells on side B, in the absence of NGF, degenerated.SOURCE: S. Varon, “Neuronal Growth Factors,” Neura/Fbgeneratkm and Transpkmtation, Frontiers of C/inica/Neuroscience, vol. 6, F.J. Seil (cd.) (New York,
NY: Alan R. Lies, 1989).

42 ● Neural Grafting: Repairing the Brain and Spinal Cord
permanent impairment of a CNS function. Anothertherapeutic use for neural grafts may be the replace-ment of degenerated neurons.
Replacement of neurons and the reconstitution ofneuronal networks within the adult CNS seem aremote possibility, considering the intricate interac-tions that occur between neurons within the nervoussystem. A single neuron may receive thousands ofcontacts from different regions of the brain. Despitethis complexity, grafted fetal neurons demonstrate aremarkable ability to integrate into the mature CNSof a recipient. Grafts of fetal neurons can send nervefibers into the host CNS and form synapses with hostneurons, often in an appropriate and recognizablepattern. Grafted fetal neurons may also receivesynaptic input from the host.
Complete and literal replacement of a group ofneurons is probably impossible. For example, whenneurons that normally project long distances withinthe CNS degenerate, replacement neural grafts aregenerally implanted near the target in the host CNSrather than in the original site of nerve cell degener-ation. In this situation, juxtaposition of graft and hostCNS target can be important for their interaction(41). Although the graft will probably not receive thefull range of normal inputs from other CNS regions,it may be sufficiently integrated into host neuronalnetworks to restore a useful degree of function.
MATERIALS FORNEURAL GRAFTING
Several types of biological materials may beused for neural grafting. The first and perhapsmost important determinant of a particular mate-rial’s usefulness is its ability to improve CNSfunction with minimal risk to the recipient. Theavailability and source of the graft material will alsosignificantly influence its application in humans.Currently, several sources of tissue for neuralgrafting in humans seem possible, including humanfetuses, cells maintained in cultures, or tissue fromgraft recipients themselves. Nonhuman species alsorepresent a potential source of neural graftingmaterial, although they may present serious func-tional and immunological problems (30,52,67,70).Each of these sources presents unique technicalissues and questions about availability. In addition,the type and source of material used are central to the
ethical and legal questions surrounding neural graft-ing (see chs. 7 and 8). In this section, general featuresof the following potential neural grafting materialsare discussed:
●
●
●
●
●
tissue from the fetal central nervous system;tissue from the peripheral nervous system;peripheral autonomic neurons;tissue from outside the nervous system; andisolated, cultured, or genetically engineeredcells.
Fetal Central Nervous System Tissue
Animal experiments have shown that fetal tissue, l
unlike mature CNS tissue, readily develops andintegrates within a host organism following grafting.A majority of neural grafting research in animals hasmade use of tissue from the fetal brain and spinalcord. In pioneering experiments, fetal CNS tissueoften displayed a considerable capacity for survivalwithin the CNS of the graft recipient (for reviews see7,35,89). During the 1960s and 1970s, technologicaladvances heralded a new era of neural grafting withfetal CNS tissue. Reliable methods for distinguish-ing surviving graft tissue within the host weredeveloped, as were improved surgical methods forinserting the graft material. When fetal CNS tissuewas transplanted into the CNS of young animals, itmatured and interacted with the host brain for asubstantial period of time. Subsequent studies re-vealed that fetal CNS tissue could also be success-fully grafted into the mature brain. In fact, thegrafted fetal CNS tissue was shown not only tosurvive and develop in the host, but to integrate intothe host brain in a predictable manner.
Research further established that grafted fetalnervous tissue often produced functional im-provements in animals with neurological deficits.For example, in several studies grafted neurons wereseen to increase brain hormone production inanimals that demonstrated a deficiency of hormones(38,40,58). The absence of the hormones impairedthe brain’s regulation of kidney or reproductiveorgan function. When the appropriate fetal nervecells from the same species were introduced into theCNS of the impaired animals, they produced thedeficient hormones and restored control of kidney orreproductive function. More recent studies, directedtoward the analysis of biological rhythms, have
lh thi5 c~pter, when referring to hums, the fetal stage is considered the period from the end of the eighth week after fertilization UIW Mh.

Chapter 4--General Features of Neural Grafting ● 43
shown that fetal tissue from a region of the braincalled the suprachiasmatic nucleus could be graftedand subsequently control daily cycles of behavior inhamsters (73).
Animal models for parkinsonism were employedto evaluate the effectiveness of grafted fetal nervoustissue (6,72). In rodents and nonhuman primates,chemicals were used to destroy the nerve cells thatdegenerate in humans suffering from Parkinson’sdisease. The chemically induced nerve cell death ismanifested as abnormal rotatory movement in ro-dents and as abnormal body movements (similar tothose seen in humans with Parkinson’s disease) innonhuman primates. When fetal neurons are graftedto replace the destroyed cells, the movement disor-der is partially reversed. The success of this tech-nique led to its adaptation for studies in humanssuffering from Parkinson’s disease. Ongoing clini-cal trials are examining the effectiveness of neuralgrafting with human fetal tissue for the treatment ofpersons with Parkinson’s disease (see ch. 5).
Many different animal models of neurologicaldeficits are being used to study the effects ofgrafted fetal CNS tissue. Results suggest thatneural grafting with fetal neurons may one day bedeveloped to treat several neurological disorders(see ch. 6).
The number of fetal nerve cells needed forneural grafting may be of critical importance,especially when the graft recipient’s brain isrelatively large, as is the adult human ’s. While toomany grafted fetal neurons pose the threat ofexcessive growth and overenlargement within theCNS of the host, too few cells (a more commonoccurrence) may fail to improve CNS functionsignificantly. For example, the amelioration ofsymptoms of Parkinson’s disease reported in asingle patient following neural grafting requiredCNS tissue from four human fetuses (62). Invaria-bly, some neurons are lost while collecting the fetaltissue. In addition, identification of the region of thefetal brain required for grafting is difficult; thedesired fetal brain region transplanted into humanswith Parkinson’s disease is approximately 1 milli-meter long (less than 4/100 of an inch) (figure 4-2).Human fetal CNS tissue for neural grafting isderived from first-trimester elective abortions,which are commonly performed via vacuum aspira-tion; this results in fragmented fetal tissue, thetransplantable components of which maybe difficult
to identify (18). Some researchers have estimatedthat human fetal tissue for neural grafting inParkinson’s disease is correctly identified in only 10to 50 percent of aborted tissue analyzed (27,61).Furthermore, only 5 to 10 percent of the transplantedneurons may survive the grafting procedure. Im-proving graft retrieval and survival could diminishthe amount of fetal tissue necessary for transplanta-tion.
Like other tissue used for neural grafting, fetalCNS tissue presents some risks (see discussion ofrisks later in this chapter). However, many scien-tists consider fetal CNS tissue to be the mosteffective material currently available for neuralgrafting (46,93). Fetal CNS cells appear to be lessvulnerable than adult cells to damage from, forexample, lack of oxygen, which is encounteredduring the transplantation process. Also, cells withinfetal CNS tissue can readily mature and integratewithin the host; mature CNS tissue has lost thesecapabilities. Of all the graft materials available at thepresent time, fetal CNS tissue is most capable ofreconstituting nerve cell structure and functionwithin the host CNS. In addition, fetal CNS tissuemay enjoy at least a temporary immunologicaladvantage (see later discussion) and, like otherpotential graft materials, is amenable to long-termstorage via cryopreservation (figure 4-3) (box 4-A).Despite the usefulness of fetal tissue for neuralgrafting, ethical, social, and political issues havecreated a barrier to its use in the United Statesand propel the search for alternative neuralgrafting materials.
Peripheral Nerve Tissue
The permanent deficit in function that frequentlyresults from injury to the mature CNS reflects, inpart, the stymied regrowth of neurons within theCNS. In contrast, axons in the peripheral nervoussystem (PNS), which lies outside the brain andspinal cord, can regrow following injury. Compo-nents of the PNS, including Schwann cells, a type ofglial cell that produces the insulating myelin sheatharound axons, promote axon growth (19).
Investigators have attempted to harness thegrowth-promoting capacity of peripheral nervesby grafting segments of peripheral nerve into theCNS. Early animal experiments showed that a pieceof peripheral nerve placed into a lesion in the CNSwould bridge the lesion, allowing host nerve fibers

44 ● Neural Grafting: Repairing the Brain and Spinal Cord
Figure 4-2—Fetal Central Nervous System
A portion of the dissected human fetal central nervous system.SOURCE: Curt Freed, Department of Medicine and Pharmacology, University of Colorado,
to penetrate and completely traverse the graft (22)(figure 4-4). Nerve fibers that regenerate through agrafted peripheral nerve penetrate only a shortdistance on reentry into the host CNS. However,even this shallow penetration back into the hostbrain permits some reconnection with target neu-rons. Thus, some recovery of function may beobtained by using this approach (55). This approachmay be limited to certain regions of the CNS due togeometric constraints on nerve graft placement. Forexample, it may be impossible to interconnectdeeply embedded regions of the brain with a nervegraft without damaging the surrounding brain tissue.
Most of these animal experiments have involvedautografts; that is, the graft material has come fromthe animal itself. An autograft provides two advan-tages: rejection of the graft by the host immune
system is avoided, and the graft recipient serves asa readily available source of material.
Peripheral Autonomic Tissue
Some neurons are located outside the brain andspinal cord and interact directly with various organs,regulating body temperature, metabolism, and thebody’s response to stress. These peripheral neuronsare part of the autonomic nervous system, and theysynthesize neurotransmitters and other chemicalsubstances that are similar to those found in theCNS. In addition, mature peripheral autonomicneurons can survive injury and redevelop nervefibers. Because this class of neurons is easilyaccessible and exhibits a great potential for re-growth, several investigators have examined theusefulness of peripheral autonomic neurons forneural grafting. Autonomic neurons have been

Chapter 4--General Features of Neural Grafting ● 45
Figure 4-3-Transplanted Fetal Nerve Cell
Photograph of a fetal nerve cell following cryopreservation andtransplantation.SOURCE: D.E. Redmond, Jr., F. Naftolin, T.J. Collier et al., “Culture and
Transplantation of Human Fetal Mesencephalic Tissue IntoMonkeys,” &“errce 242:788-771, 1988.
grafted into the mature brain in a few animalexperiments, and in some cases these grafted neu-rons survived and led to improvement in functionwithin the injured CNS (54, 83).
Tissue From Outside the Nervous System
Some nonneuronal cells located outside the cen-tral and peripheral nervous systems share a commonheritage with nervous tissue; i.e., they develop fromthe same type of embryonic precursor cell as nervoussystem cells. These cells (sometimes referred to asparaneurons) produce neurotransmitters and can bestimulated to extend nerve fibers. Included in thiscategory are some cells in the adrenal gland, as wellas other, smaller collections of cells in the body (e.g.,carotid body cells, which monitor the concentrationof oxygen in the blood). Because such cells resembleneurons, they have been considered potential candi-dates for neural grafting. Cells from the adrenalgland have been studied extensively.
The adrenal glands are located above each kidney,and they produce various hormones. The innermostregion of the adrenal gland is the adrenal medulla.One type of adrenal medullary cell, the chromaffincell, is derived from precursor cells that alsogenerate neurons in the autonomic nervous system.
Figure 4-4—Peripheral Nerve Graft
Diagram of graft from the PNS, permitting CNS nerve fiberregrowth to target.SOURCE: A.J. Aguayo, “Regeneration of Axons From the Injured Central
Nervous System of Adult Mammals,” Encyclopedia of fVeuro-science, vol. 11, G. Adelman (cd.) (Boston, MA: Birkhi?mser,1987).
Chromaffin cells produce neurotransmitters chemi-cally related to those made in the nervous system.One of the neurotransmitters produced by- chro-maffin cells is dopamine, the chemical that isdeficient in the brain of persons with Parkinson’sdisease.
The finding that fetal neurons which producedopamine could reverse parkinsonian symptoms inanimals suggested the use of adrenal medulla cellsfor neural grafting (6,72). In the latter case, animalscould provide their own chromaffin cells for graft-ing, thus eliminating concerns about a source oftissue and possible rejection of the graft. Theadrenal medulla grafts were shown to reversesome of the abnormal body movements in animalmodels of parkinsonism (see ch. 5).
A few recent experiments have employed anothernonneuronal tissue, human amnion membrane ma-trix (HAMM), taken directly from the discardedhuman placenta, as a neural graft material (23,32).When positioned in an animal’s brain, HAMMappears to serve as a bridge that supports neuronoutgrowth. HAMM does not contain cells; rather, itcontains a chemical substance that promotes andguides neuron regrowth. It does not seem to provokerejection of the graft by the host immune system, andit is available in abundance. Although more researchis necessary to evaluate the usefulness of HAMM inneural grafting, these experiments suggest thatmanmade materials, coated with a growth-promoting chemical, may ultimately be devel-oped and used in neural grafting.

46 ● Neural Grafiing: Repairing the Brain and spinal Cord
Box 4-A—The Deep Freeze: Cryopreservation of Fetal CNS Tissue
Neural grafting with fetal CNS tissue is constrained by the need for rapid implantation of freshly collectedtissue into the graft recipient. The viability of fetal CNS tissue diminishes within hours of procurement. Extendingthe interval between tissue collection and implantation would greatly ease the logistics of neural grafting and allowassessment of tissue contamination, vitality, and genetic compatibility with the intended recipient. Cryopreserva-tion, or freezing of cells and tissue at very low temperatures, can be used to extend the time between tissue collectionand neural grafting. This technique is routinely used for the storage of continuous cell lines and other types of cells.In fact, cryopreservation of fetal CNS tissue has a long history.
Prior to cryopreservation, cells or tissue are typically treated with a cryoprotectant, a chemical that limits tissuedamage during the freezing process. The cryoprotected material is then either abruptly or more gradually loweredto -l%” C, the temperature of liquid nitrogen. Once at this temperature, cells or tissue can be stored for a long time;frozen cells can also be transported readily between clinical centers.
Fetal CNS tissue from several species, including humans, has been examined following cryopreservation. Ingeneral, cryopreserved fetal CNS tissue demonstrated a significant reduction in viability when thawed. Recently,however, improved cryopreservation of human fetal tissue has been reported, resulting ’in 95 percent viability ofthawed fetal neurons. Furthermore, cryopreserved human fetal tissue has been shown to survive following graftinginto monkeys and humans.
SOURCES: T.J. Collier, D.E. Redmond, Jr., CD. Sladek et al., “Intracerebral Grafting and Culture of Cryopreserved Primate DopamineNeurons,” Brain Research 436:363-366, 1987; T.J. Collier, C.D. Sladek, M. J. Gallagher et al., “Cryopreservation of Fetal Rat andNon-human Primate Mesencephalic Neurons: Viability in Culture and Neural Transplantation,” Progress in Brain Research, vol.78, Transplantation Info the Mammlian CNS, D.M. Gash and J.R. Sladek, Jr. (eds.) (Amsterdam.: Elsevier Science Publishers,1988); D.E. Redmond, Jr., “Fetal Tissue Transplantation: Animal and Human Studies,’ paper presented at the AmericanAssociation for the Advancement of Science annual meeting, New Orleans, LA, 1990, D.E. Redmond, Jr., F. Naftolin, T.J. Collieret al., “Culture and Transplantation of Human Fetal Mesencephalic Tissue Into Monkey s,” Science 242:768-771, 1988; D.E.Redmond, Jr., D. Spencer, F. Naftolin et al., “Cryopreserved Human Fetal Neural Tissue Remains Viable 4 Months AfterTransplantation Into Human Caudate Nucleus,’ paper presented at the Society for Neuroscience 19th annual meeting, Phoenix,Arizona, 1989; V. Silani, A. Pizzuti, O. Strada et al., ‘‘Human Neuronal Cell Viability Demonstrated in Culture AfterCryopreservation,” Brain Research 473:169-174, 1988; T. Sorensen, S. Jensen, A. Moller et al., “Intracephalic Transplants ofFreeze-stored Rat Hippocampal Tissue, ’ Journal of Comparative Neurology 252:468-482, 1986.
Isolated, Cultured, or Genetically Cell SuspensionsEngineered Cells
The graft materials discussed thus far have beendistinct types of tissue harvested directly from adonor organism. Technical developments that per-mit the separation of individual cells from a solidblock of tissue, the maintenance of living cells in thelaboratory, and the manipulation of genes withincells may expand the types and forms of materialsavailable for neural grafting. The methods describedin this section can be applied to many cell types. Inthis report, however, the cells derived from eachtissue source via the methods described are treatedas a separate neural grafting material because eachgives rise to unique technological issues. The formsof neural graft materials presented in this section
Neural grafting can involve the placement ofsmall, solid pieces of tissue into the brain (8,61);however, solid pieces of tissue cannot be implantedand sustained in all locations within the CNS. Inorder to overcome this limitation, procedures havebeen developed in which solid tissue is dispersedinto individual cells or, more often, aggregates ofcells prior to grafting (8,16). Dispersed cells in asupporting fluid are known as a cell suspension. Useof cell suspensions for grafting involves: 1) removalof the required tissue from a donor organism, 2)dissociation of the tissue into individual cells orsmall aggregates of cells, 3) suspension of theindividual cells or aggregates in a supporting fluid,and 4) injection of the suspension into the host CNS.
include: Cell suspensions from several types of tissue havebeen used for neural grafting in animals (71).
● cell suspensions,Experiments have shown that fetal neurons
● cells in culture, and grafted in the form of a cell suspension are● genetically engineered cells. capable of long-term survival and interaction

Chapter 4--General Features of Neural Grafting ● 47
with the host CNS and can restore function in adamaged region of the brain (8). In fact, neuronsuspension grafts may provide more rapid andcomplete integration into the host brain than solidgrafts. Another advantage of using cells in suspen-sion rather than solid tissue for neural grafting is theease with which suspensions can be manipulated. Asolid piece of tissue contains a heterogeneouspopulation of cells, the number and viability ofwhich cannot be determined. In contrast, cell num-ber and viability can be monitored more accuratelyin suspensions, and it may be possible to isolate asingle type of cell for transplantation (16,63). Also,neural grafting with a cell suspension may provokea less severe immune system response than solidtissue grafts.
Cells in Culture
Once solid tissue is dissociated into a suspensionof cells, the living cells can be maintained in thelaboratory for several weeks or months in culture.For primary culture, cells are taken directly from anorganism and grown in vitro (literally, in glass).Culturing cells prior to grafting them increasesthe opportunity for manipulating the cells andthus may increase the versatility of neural graft-ing.
A vast amount of information concerning the invitro culturing of different groups of nerve cells,each with its specific requirements, has emergedfrom basic neuroscience research (9), including arecent report of successful culturing of humanneurons (78). Primary cultures of nerve cells, whichare generally derived from embryonic or fetal tissue,have demonstrated the ability to survive implanta-tion in the host CNS, to integrate into the host brain,and to promote recovery following an induced injury(15,39,51). In general, culturing fetal neurons dimin-ishes their survival in the host following grafting.
The use of primary cultures of glial cells for neuralgrafting has also been studied. For example, neuralgrafts of astrocytes from the developing brain canreduce scar formation following CNS injury inanimal experiments (90) and promote recovery ofbrain function (56). Schwann cells and oligodendro-cytes, both myelin-producing glial cells, have alsobeen grown in primary cultures and used for neuralgrafting. Cultured Schwann cells and oligodendro-cytes have been implanted into the CNS of myelin-deficient rats, resulting in the formation of myelinwithin the host CNS (31,45).
Photo credit: National Institute of Neurological Disorders andSfroke, Bethesda, MD, 1990
Nerve cells in culture.
Most cells survive for only a limited period inprimary culture, either replicating a freed number oftimes or not at all. However, some cells can continueto replicate and thus can potentially survive indefi-nitely. These continually self-propagating cells mayarise spontaneously, may be derived from tumors, ormay be created via genetic engineering. Sustained,self-propagating cells in culture are known ascontinuous cell lines (CCLs). Because CCLs canproduce a large number of cells and are in a senseimmortal, they have been extremely useful in anumber of areas of research.
Several CCLs have been studied extensively asmodel systems for neuron development and func-tion, including PC12 and neuroblastoma cells. Theseneuronal CCLs, originally derived from tumors, canbe induced to stop replicating and to developfeatures of adult neurons (e.g., formation of longnerve fibers and secretion of neurotransmitters).Experiments have shown that neuronal CCLs

48 ● Neural Grafting: Repairing the Brain and Spinal Cord
can be successfully grafted into the CNS and mayattenuate functional problems produced by le-sions in the CNS (29,36,48,57).
Because CCLs are capable of continuous self-replication, they could provide an inexhaustiblesource of donor tissue for neural grafting; how-ever, this very trait presents a critical obstacle totheir use. As is true of all replicating cells, theirpotential for uncontrolled growth in the host CNSmay lead to tumor formation. Tumor formationhas been observed in some, but not all, animalexperiments using CCLs for neural grafting(29,53,57). In order to eliminate the threat of tumorformation, strategies for chemically controlling theoccurrence and arrest of cell replication are beingevaluated (2,57). Although CCLs may offer anattractive option for neural grafting in the future,more research is necessary to characterize andcontrol cell replication in tissue culture and in thegraft recipient.
Genetically Engineered Cells
Research is demonstrating that cells may bedesigned to synthesize a specific chemical sub-stance or to perform a specific function beforebeing implanted into a recipient. This customizedapproach to neural grafting is made possible by theuse of genetic engineering techniques. Geneticengineering permits the insertion of new genes intoa cell. Genes code for proteins, which carry out manycell functions, and different genes direct the synthe-sis, or expression, of different sets of proteins. Cellsderived from fetal CNS tissue, the prospective host,primary cell cultures, or a CCL can be geneticallyengineered.
Genetic engineering techniques have been ap-plied to tissue from the CNS. In one approach,immature precursor cells from the developing CNSof rats, which are capable of developing into maturebrain cells, were isolated and maintained in primarycell culture (42,66). There they replicated for a finiteperiod and then matured. Genetic engineering meth-ods were designed to permit the immature precursorcells to replicate indefinitely in the laboratory, butthen subsequently to mature and to stop replicatingwhen transplanted into a host brain or spinal cord.Using this approach, specific CCLs from the brainand spinal cord may be developed for use in neuralgrafting (10). The hope is that specific ‘‘immortal”precursors for each type of cell within the brain andspinal cord can be isolated and made available to
Figure 4-5-Genetic Engineering of Graft Tissue
/ 1° cells \Grow cells Culture ceils
s4
!’,IL==J,Biochemical
@iiiiia@&iiiia Geneticcharacterization
Select modified cellsmodification
Diagram of methods used to graft genetically modified cells.SOURCE: Fred H. Gage, Department of Neuroscience, School of Medi-
cine, University of California, San Diego.
replace diseased or injured cells through neuralgrafting.
Two types of nonneuronal cells have been usedfor genetic engineering and neural grafting: astro-cytes and fibroblasts (cells found in connectivetissue) (figure 4-5). Early research demonstrated thatgenetically engineered cells can survive and func-tion within the host CNS (34). In more recentexperiments, fibroblasts have been genetically engi-neered to synthesize: 1) an enzyme important for theproduction of the brain chemical L-dopa, which is aprecursor of the brain chemical dopamine; a n d 2 )nerve growth factor (NGF) (25,79,97). When usedfor neural grafting, these genetically engineeredcells enhanced survival and growth of neurons,improved CNS function, or both.
The use of genetically engineered fibroblasts,which are easily derived from the skin, as neuralgraft material has all the advantages of autografts: aready source of tissue and no worry about immunesystem rejection of the graft. Although the use ofnonneuronal cells precludes the graft from formingsynapses with host neurons, genetically engineerednonneuronal cells may be able to function as a drugdelivery system in the host. Fibroblasts, like otherreplicating cells, do present some risk of excessivereplication within the host. However, since fibro-blasts are primary cells, not derived from a CCL,their multiplication is inhibited by contact with othercells, minimizing the threat of tumor formation.

Chapter 4--General Features of Neural Grafting ● 49
Many important questions remain concerningthe grafting of genetically modified cells into thehuman brain. Perhaps most important, the genescontrolling various cell functions within the CNS(e.g., neurotransmitter synthesis and growth factorproduction) must be identified. Once the genescontrolling CNS function and disease are identified,they must be isolated and made available for geneticengineering. Providing multiple genes to cells forneural grafting and controlling their expression arelong-term goals requiring extensive research. Never-theless, current research represents an encouragingstart toward many of these revolutionary therapeuticstrategies.
DETERMINANTS OFSUCCESSFUL NEURAL
GRAFTINGTo survive grafting, cells must endure mechanical
and metabolic disruption during their preparation forgrafting, and they must incorporate into the foreign,and potentially hostile, environment of the host. Thesurgical technique and tissue used for neural graftingare important determinants of success. Severaladditional characteristics may figure prominently inthe survival of a neural graft, including:
. the developmental state of the graft material,● the host’s immune system response,. blood vessel formation into the graft, and. the age of the host.
Developmental State of the Graft Material
In general, immature tissue can survive graft-ing more readily than its mature counterpart.Several characteristics of immature tissue, espe-cially fetal tissue, make it well-suited for grafting(l). In general, cells from fetal tissue replicaterapidly and can differentiate into functioning maturecells. Nutritional support provided by blood vesselsfrom the host is easily accepted and probablypromoted by fetal tissue. Fetal tissue is amenable tocell culture and storage techniques, thereby expand-ing its flexibility for use in grafting. These features,which make fetal tissue especially suitable forgrafting, are diminished or lost with maturity.
Early experiments in neural grafting of tissuefrom the adult brain and spinal cord indicated thatthis tissue survives poorly in the host CNS (7,35,89).In contrast, tissue from the CNS of a fetus or
newborn exhibits great potential for survival anddevelopment following neural grafting. Neuralgrafting experiments in which cell suspensions areused demonstrate an even greater reliance on the useof fetal nervous tissue (8).
Although CNS tissue in later stages of develop-ment has been used with some success for neuralgrafting in rodents and nonhuman primates, survivalis greatest when fetal CNS tissue is used (17,86).Apparently, immature neurons, which have not yetgrown long and elaborate fiber-like extensions, areless vulnerable to the mechanical disruption associ-ated with tissue collection. In addition, immaturecells may be more resistant to other stresses’ associ-ated with the grafting procedure, such as a temporaryreduction in oxygen supply. Because neuronsthroughout the CNS develop and mature asynchro-nously, different groups of neurons reach the opti-mal developmental stage for neural grafting atdifferent fetal ages. The developmental stage of theCNS tissue used for grafting may present immunol-ogical considerations. Grafts of fetal CNS tissue failto provoke an immediate immune response, prob-ably because the cells and molecules that triggergraft rejection by the host immune system have notyet developed within fetal tissue. Fetal CNS tissuedoes possess the capability of expressing im-munoreactive molecules on maturity, hence it couldprovoke a delayed immune system response.
The optimum donor age of non-CNS tissues forneural grafting has not been as extensively evalu-ated. Adrenal medulla transplants in rats demon-strate greater functional effects when derived fromyounger rather than older animals (28). Thus,optimal success in adrenal grafting maybe obtainedby using young, and perhaps even fetal, adrenalmedulla tissue. Grafted nerve cells from the auto-nomic nervous system do not survive well whenderived from the fetus; however, mature autonomicnerve cells regenerate briskly when transplanted(82).
Immune System Response
Mammals have evolved an immune system toprotect them from disease-causing agents encoun-tered in the environment. This system is a finelytuned collection of tissues, organs, cells, and mole-cules that seek out, identify, destroy, and rememberforeign cells and molecules. An individual’s im-mune system vigilance against cells and mole-

50 ● Neural Grafting: Repairing the Brain and Spinal Cord
cules that do not originate within itself presents amajor obstacle for organ or tissue transplanta-tion. In order for a graft to survive for an extendedperiod of time in the host, the host’s immune systemmust be contravened or suppressed.
Rejection of a graft can be prevented by usingtissue from the host’s own body. As noted earlier,such a graft is called an autograft. Graft materialfrom an identical twin-an isograft--should behaveimmunologically like an autograft. After these twotypes of grafts, compatibility is increasingly rare.Either an allograft--tissue transferred between dif-ferent members of the same species--or a xe-nograft--tissue transferred between individuals ofdifferent species-can lead to graft rejection. Hostrejection of grafted tissue may be prevented byreducing the genetic disparity between the donorand the host and by using drugs that suppress theaction of the immune system.
It has long been thought that the CNS enjoysrelative isolation from the immune system becauseit permits the entry of few cells from the immunesystem that recognize foreign cells or molecules (forreview, see 69,94). This isolation has given rise tothe concept of immunological privilege; i.e., theCNS is not subjected to the same degree of scrutinyby immune system components as the rest of thebody. However, although allografts within the CNSseem to survive frequently without inducing rejec-tion, xenografts in the CNS do provoke graftrejection (69). These data and others demonstratethat the immune system can penetrate the CNS andlead to graft rejection, thus casting doubt on thedegree to which immunological privilege operates inthe CNS.
Many immune system components are excludedfrom the CNS by the blood-brain barrier, an impor-tant agent of immunological privilege (figure 4-6).Injury, surgery, or infection can disturb the blood-brain barrier, allowing cells and molecules from theimmune system to enter the CNS and cells from theCNS to enter the bloodstream. While there is debateabout whether the blood-brain barrier is permanentlydisrupted by the implantation of tissue in the CNS(12,81), it is undoubtedly disrupted for at least a fewdays (13). The type of grafting material used alsoappears to affect the development of the blood-brainbarrier within the graft (13,83).
Figure 4-6—Blood-Brain Barrier inTransplanted Tissue
Blood vessel surrounded by brain tissue shown in photograph.Inset B displays the source of the blood-brain barrier, i.e., the tightadhesion of endothelial cells, which line blood vessels.SOURCE: Richard D. Broadwell, Division of Neurological Surgery, Univer-
sity of Maryland School of Medicine.
A second feature of the CNS which was believedto isolate grafts and hinder graft rejection is the lackof extensive lymphatic drainage. Lymphatic drain-age returns fluids, molecules, foreign particles, andcells from various tissues in the body through thelymphatic system back to the immune and circula-tory systems. It is through this drainage that graftedcells capable of triggering rejection reach the host’simmune system. The CNS had been thought not toexperience lymphatic drainage; however, somestudies have suggested that molecules and cells canleave the CNS and enter the lymphatic system. Thusthe CNS may indeed experience some lymphaticdrainage and therefore be capable of provokingrejection (96).
The use of CNS tissue as a grafting material oftenfails to provoke rejection by the immune system, atleast in the short term. Cells within the CNSnormally lack, or express very few, immunoreactivemolecules, i.e., molecules that trigger rejection by

Chapter 4-General Features of Neural Grafting .51
the host’s immune system (88,98).2 Also, tissuefrom ‘the CNS was thought not to contain cells thatenter the immune system and trigger an immuneresponse (47). Unfortunately, recent experimentssuggest that the CNS can be provoked to produceimmunoreactive molecules and that the CNS doespossess cells which may reach the immune systemand initiate graft rejection (3,50,92,98).
Another cell type that can provoke an immuneresponse is endothelial cells (49,65), which form theinner walls of blood vessels and are commonlyfound in grafts of solid pieces of tissue. This causeof graft rejection can be eliminated by using neuralgrafts composed of a single type of cell, as in cellcultures or purified suspensions of cells, which donot contain blood vessels or endothelial cells.
The fact that many types of neural graftssurvive in the host CNS suggests that the brainand spinal cord do enjoy some immunologicalprivilege. However, research indicates that somegrafts can be identified and destroyed by thehost’s immune system. Further experiments andanalyses are required to delineate the precise rela-tionship between the immune system and the CNS,as well as the immune system’s response to neuralgrafts.
Blood Vessel Formation
The neural graft’s ability to obtain readyaccess to nutritional support and a supply ofoxygen from the host is critical for its survival.The failure of many early neural grafts may reflectinadequate incorporation of the grafted tissue intothe host blood supply (8). Solid tissue grafts into theCNS may not receive an adequate blood supply formore than 1 week (13).
Several approaches to neural grafting have beendeveloped to accelerate the provision of nutritionalsupport to the graft. One entails placing the graftnear a CNS surface that is naturally rich in bloodvessels. The brain ventricles were a favored site forgraft placement in animal experiments for thisreason (82). Ventricles are cavities within the brainthat contain cerebrospinal fluid (CSF). CSF mayprovide immediate nutritional support to the solidgraft, and regions rich in blood vessels within theventricles provide long-term support. Another ap-
Figure 4-7—Blood Vessel Growth in Transplant
t‘. .% i $
*%%4
Darkly stained blood vessels invading neural graft tissue in brain.SOURCE: Richard D. Broadwell, Division of Neurological Surgery, Univer-
sity of Maryland School of Medicine.
preach is to create a rich vascular surface within thebrain (91). Under normal conditions, new bloodvessels are very rarely formed in the brain. However,when a cavity is produced surgically in the CNS,new blood vessel growth is stimulated and the cavitywalls become heavily invested with blood vessels.Placing a graft within the cavity often results in agood supply of blood vessels to the grafted tissue.Greater blood vessel growth is produced by graftplacement than by a wound alone (59). The choiceof grafting material may also influence blood vesselformation: blood vessels can grow into suspensionsof cells more readily than into solid pieces of tissue,and fetal tissue seems to stimulate blood vesseldevelopment better than adult tissue (figure 4-7)(77). Finally, certain drugs may be used to enhanceblood vessel development within a graft (26).
It has been debated whether blood vessels withina neural graft are derived from the donor or the host.The relative contribution of each may depend on thetype of tissue transplanted, whether it is transplantedas a solid piece or in a cell suspension, and theamount of tissue damage sustained by the recipientduring placement of the graft (13,24,60,69,83).Blood vessels within the graft may or may not fullydevelop a blood-brain barrier, depending on the typeof tissue utilized (13,14,68,80,95). Both of theseobservations, the presence of donor cells in the graftblood vessels and the formation of the blood-brainbarrier, have important implications for graft rejec-
~e presence of specific molecules, including the major histocompatibility complex, or MHC antigens, is an important determinant of a tissue’simrnunogenicity. Detection and measurement of these molecules can be diffkult (71).

52 ● Neural Grafting: Repairing the Brain and Spinal Cord
tion. (See the earlier discussion of immune systemresponse.)
The Age of the Host
In general, the younger the graft recipient, themore likely the graft is to survive and integratewithin the host brain. A younger host animal,especially a newborn, maybe better able to supportgrafted material because it can more vigorously formblood vessels (8). Furthermore, an adult recipientrejects neural grafts more rapidly than an immaturerecipient (64). The age of the host, however, is lesscritical to graft survival than the age of the donor,immunological response, and extent of blood vesselformation.
POTENTIAL RISKSA major goal of neural grafting is to improve CNS
function following disease or trauma. As with anysurgical intervention, however, neural grafting pre-sents risks to the recipient. Problems may resultfrom:
● immune system reaction or suppression,. unwanted psychological effects,. the surgical procedure itself,● excessive growth of graft material, or● infection or other effects on the host CNS.
Unfortunately, many of the risks attributed to neuralgrafting are either poorly understood or simplyspeculative. Before any routine application ofneural grafting in humans, the risks must becarefully delineated, minimized, and measuredagainst expected benefits.
Immune System Reaction or Suppression
The transplantation of tissue from one individ-ual to another presents the risk of graft rejection.The foreign tissue triggers a cascade of events in thegraft recipient, culminating in destruction of thegraft. In general, allografts implanted in the CNS donot appear to suffer immediate rejection by thehost’s immune system, although rejection in thelong term may be possible.
When tissue transplantation is performed outsidethe CNS, drugs that suppress the immune system areemployed to prevent rejection and promote survivalof the graft. Immunosuppression poses serious risksto the graft recipient, including increased suscepti-bility to infection and the development of some
forms of cancer (87). Uncertainty about immunesystem reactions in the CNS complicates attempts tobalance the risks of immunosuppression againstthose of neural graft rejection. Studies of fetal CNStissue grafting in humans with Parkinson’s diseasehave both applied and abstained from applyingimmunosuppression therapy (27,62,75).
Unwanted Psychological Effects
Implantation of tissue into the human brainraises the possibility of unwanted psychologicaleffects. Assessment of adrenal medulla grafts inhumans with Parkinson’s disease indicates thatsome psychological changes consistently accom-pany this procedure, including hallucinations, con-fusion, and somnolence (43,44). These psychologi-cal responses proved, in general, to be transient.How such changes are produced is unknown, butthey may reflect either trauma to the brain from thesurgical procedure itself or the effects of chemicalsubstances released by the grafted adrenal tissue.Similar effects have not been reported in the fewParkinson’s patients who have received fetal CNStissue grafts.
Effects of the Surgical Procedure
Aside from its suspected role in producing tempo-rary psychological changes in the recipient, thesurgical procedure used to insert a neural graftpresents other serious risks. Graft placement in thebrain, especially the more invasive surgical pro-cedures (see ch. 5), can cause serious damage, suchas excessive bleeding or injury to brain tissue.Injury may result in the loss of CNS function orexacerbate the recipient’s immune response to thegrafted tissue (41). In addition, surgery disrupts theblood-brain barrier for at least a week; even the lessinvasive method of graft insertion probably disruptsthe blood-brain barrier for 1 to 3 days (14,94). TheCNS’s protected environment may thus be losttemporarily near the graft site, posing a risk to thegraft recipient.
Excessive Growth of Graft Material
Fetal CNS tissue, some nonneuronal tissues,and continuous cell lines can continue to replicatein the CNS of the graft recipient, presenting therisk of excessive graft enlargement. Brain tissuecan be compressed and permanently damaged by anexpanding mass of tissue. In addition, an enlargingneural graft placed in the brain ventricles can

Chapter 4--General Features of Neural Grafting ● 53
obstruct the flow of CSF, which can dangerouslyincrease pressure in the brain. The number of cellsused for neural grafting is thus an important consid-eration; the number chosen must reflect a balancebetween the risk of overenlargement and the morecommon problem of inadequate cell survival. Asdiscussed earlier, some replicating cells pose theadded threat of tumor formation.
Infection and Other Effects on the Host CNS
Transplanted cells can transmit bacterial andviral infections, placing the graft recipient at risk forsuch diseases as hepatitis, AIDS, or herpes simplexencephalitis. Several actions can reduce this risk.The likelihood of a potential donor carrying aninfectious agent can be assessed. The potential donoror graft material can be screened for infectiousagents. In addition, graft material can be treated withdrugs, such as antibiotics, to destroy susceptibleinfectious agents prior to implantation.
Materials used for neural grafting may disruptor alter CNS function in the recipient. Forexample, non-CNS tissue, such as cells from theadrenal medulla or fibroblasts, may prevent thereestablishment of the blood-brain barrier near thegraft (13,59,83). The implantation of certain fetalCNS tissue has been shown to produce seizures insome experimental animals (33). In addition, injec-tion of brain tissue into the abdomen of animals hasled to experimental allergic encephalomyelitis(EAE) (4), a potentially fatal inflammatory diseaseof the CNS in which immune cells attack compo-nents of nerves. Although EAE has not beenreported in neural grafting experiments in animals,it represents a serious risk, especially in the case ofxenografts. Finally, the graft may be susceptible tothe pathological processes that underlie the neuro-logical disorder being treated. Since many neurolog-ical disorders are of unknown etiology, it is difficultto assess the likelihood of this risk factor.
SUMMARY AND CONCLUSIONSNeural grafting involves many therapeutic goals,
materials, and procedures. Tissue or cells may betransplanted to the brain and spinal cord in order todeliver chemical substances, to promote neuronalgrowth and survival following injury, or to replacelost nerve cells. Numerous materials have been usedfor neural grafts, including fetal CNS tissue, periph-eral nerve tissue, and tissue from outside the nervoussystem. In addition, several types of tissue have been
manipulated, using cell culture and molecular bio-logical techniques, in preparation for neural grafting.While genetically engineered cells present an excit-ing possibility for the future of neural grafting, atpresent fetal CNS tissue is demonstrably the mosteffective graft material available. The developmen-tal stage of the grafted material, the host’s immuneresponse, vascular support within the host, and theage of the host also influence graft survival andfunction. Depending on the material chosen and thesurgical procedures employed, neural grafting tech-nology does present some risk to the host.
The potential use of neural grafting for the routinetreatment of the diseased or injured CNS requiresmuch more research, even for Parkinson’s disease,where the technology is most highly developed atpresent. Research is necessary to evaluate andoptimize transplant procedures. Other neural graft-ing approaches, including the use of geneticallyengineered cells, will require even more extensivebasic research. Factors that determine the long-termsurvival and function of a neural graft, especially theimmune system reactions, must be probed moredeeply. The influence of the disease process on thegrafted material must also be addressed. Perhapsmost important, a more complete understanding ofthe basis of disease and malfunction within the CNSis required for the development of treatments such asneural grafting.
CHAPTER 4 REFERENCES1.
2.
3.
4.
5.
6.
Auerbach, R., “Qualities of Fetal Cells and Tissues,”Report of the Human Fetal Tissue TransplantationResearch Panel, vol. II (Bethesda, MD: NationalInstitutes of Health, 1988).Barnes, D., “Serum-free Animal Cell Culture,”Biotechniques 5;534-541, 1987.Bartlett, P.F., Kerr, R. S. C., and Bailey, K.A.,“Expression of MHC Antigens in the Central Nerv-ous System,” Transplantation Proceedings 21:3163-3165, 1989.Bauer, H.J., “Umstrittene MS-Therapie,” Nerve-narzt 54:400-405, 1983.Bjorkhmd, A., Lindvall, O., Isacson, O., et al.,“Mechanisms of Action of Intracerebral NeuralImplants: Studies on Nigral and Striatal Grafts to theLesioned Striatum, ” Trends in Neuroscience10:509-516, 1987.Bjorkhmd, A., and Stenevi, U., “Reconstruction ofthe Nigrostriatal Dopamine Pathway by IntracerebralNigral Transplants,” Brain Research 177:555-560,1979.

54 ● Neural Grafting: Repairing the Brain and Spinal Cord
7. Bjorklund, A., and Stenevi, U., “IntracerebralG raft-ing: A Historical Perspective,” Neural Grafting inthe Mammalian CNS, A. Bjorklund and U. Stenevi(eds.) (Amsterdam: Elsevier Science Publishers,1985).
8. Bjorldund, A., Stenevi, U., Schmidt, R.H., et al.,“Intracerebral Grafting of Neuronal Cell Suspen-sions, I: Introduction and General Methods ofPreparation,” Acta Physiologic Scandinavia supp.522:1-7, 1983.
9. Bottenstein, J.E., “Growth and Differentiation ofNeural Cells in Defined Media,” Cell Culture in theNeuroscience, J.E. Bottenstein and G. Sato (eds.)(New York, NY: Plenum Press, 1985).
10. Bredesen, D.E., Hisanaga, K., and Sharp, F.R.,“Neural Transplantation Using Temperature-Sensitive Immortalized Neural Cells: A PreliminaryReport,” Annuls of Neurology 27:205-207, 1990.
11. Bnghtman, M.W., and Reese, T. S., “JunctionsBetween Intimately Opposed Cell Membranes inVertebrate Brains,” Journal of Cell Biology 40%48-677,1969.
12. Broadwell, R.D., “Absence of a Blood-Brain BarrierWithin Transplanted Brain Tissue,” Science 241:473, 1988.
13. Broadwell, R.D., Charlton, H.M., Ebert, P., et al.,“Allografts of CNS Tissue Possess a Blood-BrainBarrier, II: Angiogenesis in Solid Tissue and CellSuspension Grafts,” Experimental Neurology, sub-mitted.
14. Broadwell, R.D., Charlton, H.M., Ganong, W.F., etd., “Allografts of CNS Tissue Possess a Blood-Brain Barrier, I: Grafts of Medial Preoptic Area inHypogonadal Mice,’ Experimental Neurology 105:135-151, 1989.
15. Brundin, P., Barbin, G., Isacson, O., etal., “Survivalof Intracerebrally Grafted Rat Dopamine NeuronsPreviously Cultured In Vitro,” Neuroscience Letters61:79-84, 1985.
16. Brundin, P., Isacson, O., and Bjorklund, A., “Moni-toring of Cell Viability in Suspensions of EmbryonicCNS Tissue and Its Use as a Criterion for Intracere-bral Graft Survival,” Brain Research 331:251-259,1985.
17. Brundin, P., Isacson, O., Gage, F. H., et al.,“Intracerebral Grafts of Neuronal Cell Suspen-sions,” Neural Grafiing in the Mammalian CNS, A.Bjorlchmd and U. Stenevi (eds.) (Amsterdam: Else-vier Science Publishers, 1985).
18. Brundin, P., Nilsson, O.G., Strecker, R.E., et al.,“Behavioral Effects of Human Fetal DopamineNeurons Grafted in a Rat Model of Parkinson’sDisease,” ExperimentalBrain Research 65:235-240,1986.
19. Bunge, R.P., “The Cell of Schwann,” Diseases ofthe Nervous System: Clinical Neurobiology, A.K.
Asbury, G.M. McKhann, and W.I. McDonald (eds.)(Philadelphia, PA: W.B. Saunders, 1986).
20. Caroni, P., Savio, T, and Schwab, M.E., “CentralNervous System Regeneration: Oligodendrocytesand Myelin as Non-permissive Substrates for NeuriteGrowth,’ Progress in Brain Research, vol. 78,Transplantation Into the Mammalian CNS, D.M.Gash and J.R. Sladek, Jr. (eds.) (Amsterdam: ElsevierScience Publishers, 1988).
21. Cotman, C.W., and Kesslak, J.P., “The Role ofTrophic Factors in Behavioral Recovery and Integra-tion of Transplants,” Progress in Brain Research,VOL 78, Transplantation Into the Mammalian CNS,D.M. Gash and J.R. Sladek, Jr. (eds.) (Amsterdam:Elsevier Science Publishers, 1988).
22. David, S., and Aguayo, A.J., “Peripheral NerveTransplantation Techniques to Study Axonal Regen-eration From the CNS of Adult Mammals,” NeuralGrafting in the Mammalian CNS, A. Bjorklund andU. Stenevi (eds.) (Amsterdam: Elsevier SciencePublishers, 1985).
23. Davis, G.E., Blaker, S.N., Engvall, E., etal., “HumanAmnion Membrane Serves as a Substratum forGrowing Axons In Vitro and In Vivo,” Science236:1106-1109, 1987.
24. Dusart, 1., Nothias, F., Roudier, F., et al., “Vascular-ization of Fetal Cell Suspension Grafts in theExcitotoxically Lesioned Adult Rat Thalamus,”Developmental Brain Research 48:215-228, 1989.
25. Ernfors, P., Ebendal, T., Olson, L., et al., “A CellLine Producing Recombinant Nerve Growth FactorEvokes Growth Responses in Intrinsic and GraftedCentral Cholinergic Neurons,” Proceedings of theNational Academy of Sciences, (J.SA 86:47564760,1989.
26. Finger, S., and Dunnett, S. B., “Nimodipine En-hances Growth and Vascularization of NeuralGrafts,” Experimental Neurology 104: 1-9, 1989.
27. Freed, C., “FetalMesencephalicI replants forParkin-son’s Disease,” presentation at the Office of Tech-nology Assessment, U.S. Congress, Washington,DC, December 1989.
28. Freed, W.J., Cannon-Spoor, H.E., and Krauthamer,E., “Factors Influencing the Efficacy of AdrenalMedulla and Embryonic Substantial Nigra Grafts,”Neural Grafting in the Mammalian CNS, A.Bjorklund and U. Stenevi (eds.) (Amsterdam:Elsevier Science Publishers, 1985).
29. Freed, W.J., Patel-Vaidya, U., and Geller, H.M.,“Properties of PC12 Pheochromocytoma CellsTransplanted to the Adult Rat Brain,” ExperimentalBrain Research 63:557-566, 1986.
30. Freeman, T.B., Wojak, J. C., Brandeis, L., et al.,“Cross-species Intracerebral Grafting of EmbryonicSwine Doparninergic Neurons,” Progress in BrainResearch, VOL 78, Transplantation Into the Mammal-

Chapter 4--General Features of Neural Grafting ● 55
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44,
ian CNS, D.M. Gash and J.R. Sladek, Jr. (eds.)(Amsterdam: Elsevier Science Publishers, 1988).Friedman, E., Nilaver, G., ca.rmel, P., et al., “Myeli-nation by Transplanted Fetal and Neonatal Oligoden-drocytes in a Dysmyelinating Mutant,” Brain Re-search 378:142-146, 1986.Gage, F.H., Blaker, S.N., Davis, G.E., et al., “HumanAmnion Membrane Matrix as a Substratum forAxonal Regeneration in the Central Nervous Sys-tem,” Experimental Brain Research 72:371-380,1988.Gage, F.H., and Buzsaki, G., ‘CNS Grafting: Poten-tial Mechanisms of Action,” Neural Regenerationand Transplantation, F. Seil (cd.) (New York, NY:Alan R. Liss, 1989).Gage, F.H., Wolff, J.A., Rosenberg, M. B., et al.,“Grafting Genetically Modified Cells to the Brain:Possibilities for the Future,” Neuroscience 23:795-807, 1987.Gash, D.M., “Neural Transplants in Mammals, AHistorical Overview,” Neural Transplants: Devel-opment and Function, J.R. Slade~ Jr., and D.M.Gash (eds.) (New York, NY: Plenum Press, 1984).Gash, D.M., Netter, M.F.D., Okawara, S.H., et al.,“Amitotic Neuroblastoma Cells Used for NeuralImplants in Monkeys,” Science 233:1420-1422,1986.Gash, D.M., and Sladek, J.R., Jr., “NeuralTransplan-tation: Problems and Prospects-Where Do We GoFrom Here?” Mayo Clinics Proceedings 64:363-367, 1989.Gash, D.M., Sladek, J.R., Jr., and Sladek, C.D.,“Functional Development of Grafted VasopressinNeurons,” Science 210:1367-1369, 1980.Gibbs, R. B., Pixley, S.K.R., and Cotman, C.W.,“Transplantation of Septal Neurons Maintained inImg-Term Culture,’ Brain Research 382:409415,1986.Gibson, M.J., Krieger, D.T., Charlton, H.M., et al.,“Mating and Pregnancy Can Occur in GeneticallyHypogonadal Mice With Preoptic Area BrainGrafts,” Science 225:949-951, 1984.Gill, TJ., and Lund, R.D., “Implantation of TissueInto the Brain,” Journal of the American MedicalAssociation 261:2674-2676, 1989.Giotta, G.J., Heitzmann, J., and Cohn, M., “Proper-ties of Two Temperature-Sensitive Rous SarcomaVirus Transformed Cerebella Cell Lines,” BrainResearch 202:445-448, 1980.Goetz, C.G., Olanow, C.W., Keller, W. C., et al.,“Multicenter Study of Autologous Adrenal Medul-lary Transplantation to the Corpus Striatum inPatients With Advanced Parkinson’s Disease,’ NewEngland Journal of Medicine 320:337-341, 1989.Goetz, C.G., Tanner, C.M., Penn, R.D., et al.,“Adrenal Medullary Transplant to the Striatum of
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56,
57.
Patients With Advanced Parkinson’s Disease: l-YearMotor and Psychomotor Data, Neurology 40:273-276, 1990.Gumpel, M., Baumann, N., Raoul, M., et al., “Sur-vival and Differentiation of Oligodendrocytes FromNeural Tissue Transplanted in New-Born MouseBrain,” Neuroscience Letters 37:307-311, 1983.Hansen, J.T., and Sladek, J.R., Jr., “Fetal Research,”Science 246:775-779, 1989.Hart, D. N.J., and Fabre, J.W., “Demonstration andCharacterization of Ia-positive Dendritic Cells in theInterstitial Connective Tissue of Rat Heart and OtherTissues, But Not Brain,” Journal of ExperimentalMedicine 154:347-361, 1981.Hefti, F., Hartikka, J., and Schlumpf, M., “Implanta-tion of PC12 Cells Into the Corpus Striatum of RatsWith ksions of the Dopaminergic NigrostriatalNeurons,” Brain Research 348:283-288, 1985.Hickey, W. F., and Kimura, H., “Perivascular Micro-glial Cells Are Bone Marrow-Derived and PresentAntigen In Vivo,” Science 239:290-292, 1988.Hickey, W.F., Osborn, J.P., and Kirby, W.M.,“Expression of Ia Molecules by Astrocytes Duringfwute EAE in the Lewis Rat,” Cellular Immunology91:528-533, 1985.Hisanaga, K., Tsukui, H., Takei, N., et al., “Trans-plantation of Fetal and Early Postnatal Rat SeptalCholinergic Neurons Cultured in Serum-free andSerum-containing Medium With Nerve Growth Fac-tor,” Brain Research 475:349-355, 1988.Huffaker, T.K., Boss, B.D., Morgan, A. S., et al.,“Xenogmfting of Fetal Pig Ventral MesencephalonCorrects Motor Asymmetry in the Rat Model ofParkinson’s Disease,’ Experimental Brain Research77:329-336, 1989.Jaeger, C. B., ‘‘Immunocytochemical Study of PC12Cells Grafted to the Brain of Immature Rats,”Experimental Brain Research 59:615-624, 1985.Kamo, H., Kim, S.U., McGeer, P.L., et al., “Func-tional Recovery in a Rat Model of Parkinson’sDisease Following Transplantation of CulturedHuman Sympathetic Neurons,” Brain Research 397:372-376, 1986.Keirstead, S.A., Rasmins&, M., Fukuda, Y., et al.,“Electrophysiologic Responses in Hamster SuperiorColliculus Evoked by Regenerating Retinal Axons,”Science 246:255-257, 1989.Kesslak, J.P., Nieto-Sampedro, M., Globus, J., et al.,“Transplants of Purified Astrocytes Promote Behav-ioral Recovery After Frontal Cortex Ablation,”Experimental Neurology 92:377-390, 1986.Kordower, J.H., Netter, M.F.D., Yeh, H., et al., “AnIn Vivo and In Vitro Assessment of DifferentiatedNeuroblastoma Cells as a Source of Donor Tissue forTransplantation,” Annals of the New York Acaakmyof Sciences 495:606-621, 1987.

56 ● Neural Grafting: Repairing the Brain and Spinal Cord
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
Krieger, D.T, Perlow, M.J., Gibson, M. J., et al.,“Brain Grafts Reverse Hypogonadism of Gonado-tropin Releasing Hormone Deficiency,” Nature298:468471, 1982.Krum, J.M., and Rosenstein, J. M., “Patterns ofAngiogenesis in Neural Transplant Models: I. Auto-nomic Tissue Transplants,’ Journal of ComparativeNeurology 258:420434, 1987.Krum, J.M., and Rosenstein, J. M., “Patterns ofAngiogenesis in Neural Transplant Models: II. FetalNeocortical Transplants,” Journal of ComparativeNeurology 271:331-345, 1988.Lindvall, O., “Transplantation Into the HumanBrain: Present Status and Future Possibilities,”Journal of Neurology, Neurosurgery, and PsychiatrySUPP.: 39-54, 1989.Lindvall, O., Brundin, P., Widner, H., et al., ‘‘Graftsof Fetal Dopamine Neurons Survive and ImproveMotor Function in Parkinson’s Disease, ” Science247:574-577, 1990.bpez-bzano, J.J., Gash, D.M., Leary, J.F., et al.,“Survival and Integration of Transplanted Hypotha-lamic Cells in the Rat CNS After Sorting by Flowcytometry,” Cell and Tissue Transplantation Intothe Adult Brain, E.C. Azmitia and A. Bjorklund(eds.) (New York, NY: New York Academy ofSciences, 1987).Lund, R. D., Rae, K., Hankin, M., et al., “III:Transplantation of Retina and Visual Cortex to RatBrains of Different Ages: Maturation Patterns andImmunological Consequences, ” Annals of the NewYork Academy of Sciences 495:227-241, 1987.McCarron, R. M., Kempski, O., Spatz, M., et al.,“Presentation of Myelin Basic Protein by MurineCerebral Vascular Endothelial Cells,” Journal ofImmunology 134:3100-3103, 1985.McKay, R., Frederiksen, K., Jat, P. J., et al., “Recon-structing the Brain From Immortal Cell Lines, ’Progress in Brain Research, VOL 78, TransplantationInto the Mammalian CNS, D.M. Gash and J.R.Sladek, Jr. (eds.) (Amsterdam: Elsevier SciencePublishers, 1988).Mason, D. W., Charlton, H. M., Jones, A. J., et al.,“The Fate of Allogeneic and Xenogeneic NeuronalTissue Transplanted Into the Third Ventricles ofRodents,” Neuroscience 19:685-694, 1986.Naradzay, J.F., and Rosenstein, J. M., “VascularMorphology and Permeability in Fetal CNS Grafts tothe Renal Capsule, ” Experimental Neurology104:284-291, 1989.Nicholas, M. K., and Arnason, B. G. W., “Immuno-logic Considerations in Transplantation to the Cen-tral Nervous System,” Neural Regeneration andTransplantation, F.J. Seil (cd.) (New York, NY: AlanR. Liss, 1989).
70.
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
Olson, L., Stromberg, I., Bygdeman, M., et al.,“Human Fetal Tissues Grafted to Rodent Hosts:Structural and Functional Observations of Brain,Adrenal and Heart Tissues in Oculo,” ExperimentalBrain Research 67:163-178, 1987.Patel-Vaidya, U., Wells, M.R., and Freed, W. J.,“Survival of Dissociated Adrenal Chromaffin Cellsof Rat and Monkey Transplanted Into Rat Brain,”Cell and Tissue Research 240:281-285, 1985.Perlow, M. J., Freed, W. J., Hoffer, B. J., et al., “BrainGrafts Reduce Motor Abnormalities Produced byDestruction of Nigro-Striatal Dopamine System,”Science 204:643-647, 1979.Ralph, M.R., Foster, K. G., Davis, F. C., et al.,‘‘Transplanted Suprachiasmatic Nucleus DeterminesCircadian Period,” Science 247: 975-978, 1990.Rapaport, S.1., Blood-Brain Barrier in Physiologyand Medicine (New York, NY: Raven Press, 1976).Redmond, D. E., Jr., “Fetal Tissue Transplantation:Animal and Human Studies,’ paper presented at theAmerican Association for the Advancement of Sci-ence annual meeting, New Orleans, LA, 1990.Reier, P. J., Eng, L. F., and Jakeman, L., “ReactiveAstrocyte and Axonal Outgrowth in the Injured CNS:Is Gliosis Really an Impediment to Regeneration?”Neural Regeneration and Transplantation, F.J. Seil(cd.) (New York, NY: Alan R. Liss, 1989).Risau, W., “Developing Brain Produces Angiogene-sis Factor,’ Proceedings of the National Academy ofSciences, U.S.A. 83:3855-3859, 1986.Ronnett, G.V., Hester, L. D., Nye, J. S., et al., “HumanCortical Neuronal Cell Line: Establishment From aPatient With Unilateral Megalencephaly,” Science248:603-605, 1990.Rosenberg, M, B., Friedmann, T., Robertson, R. C., etal., “Grafting Genetically Modified Cells to theDamaged Brain: Restorative Effects of NGF Expres-sion,” Science 242:509-516, 1988.Rosenstein, J. M., “Neocortical Transplants in theMammalian Brain Lack a Blood-Brain Barrier toMacromolecules,’ Science 235:772-774, 1987.Rosenstein, J. M., ‘‘Absence of a Blood-Brain BarrierWithin Transplanted Brain Tissue?” Science241:473-474, 1988.Rosenstein, J. M., and Brightman, M. W., “IntactCerebral Ventricle as a Site for Tissue Transplanta-tion,” Nature 276:83-85, 1978.Rosenstein, J. M., and Brightman, M. W., “Circum-venting the Blood-Brain Barrier With AutonomicGanglion Transplants,’ Science 221:879-881, 1983.Savio, T., and Schwab, M.E., “Rat CNS WhiteMatter, But Not Gray Matter, Is Nonpermissive forNeuronal Cell Adhesion and Fiber Outgrowth,”Journal of Neuroscience 9:1126-1133, 1989.Schnell, L., and Schwab, M.E., “Axonal Regenera-tion in the Rat Spinal Cord Produced by an Antibody

Chapter 4--General Features of Neural Grafting ● 57
86.
87.
88.
89.
90.
91.
92.
Against Myelin-Associated Neurite Growth Inhib-itors,” Nature 343:269-272, 1990.Seiger, A., and Olson, L., “Quantitation of FiberGrowth in Transplanted Central Monoamine Neu-rons,” Cell and Tissue Research 179:285-316, 1977.Shevach, E.M., “The Effects of Cyclosporin-A onthe Immune System,” Annual Review of Immunol-0~ 3:397424, 1985.Skoskiewicz, M.J., Colvin, R. C., Scheenberger, E.E.,et al., “Widespread and Selective Distribution ofMajor Histocompatibility Complex Determined An-tigens In Vivo by Interferon,’ JournaZ of Experimen-tal Medicine 152:1645-1664, 1985.Sladek, J.R., Jr., and Gash, D.M., “Nerve-cellGrafting in Parkinson’s Disease,’ JourruzZ of Neuro-surgery 68:337-351, 1988.Smith, G. M., and Silver, J., “Transplantation ofImmature and Mature Astrocytes and Their Effect onScar Formation in the ksioned Central NervousSystem,” Progress in Brain Research, vol. 78,Transplantation Into the Mammalian CNS, D.M.Gash and J.R. Sladek, Jr. (eds.) (Amsterdam: ElsevierScience publishers, 1988).Stenevi, U., Kromer, L.F., Gage, F.H., et al., “SolidNeural Grafts in Intracerebral Transplantation Cavi-ties,” Neural Grafting in the Mammalian CNS, A.Bjorklund and U. Stenevi (eds.) (Amsterdam:Elsevier Science Publishers, 1985).Ting, J.P.Y., Nixon, D.R., Weiner, L.P., et al., ‘BrainIa Antigens Have a Bone Marrow Origin,” Immuno-
93.
94.
95.
%.
97.
98.
genetics 17:295-301, 1983.
Weiss, R., “Bypassing the Ban,” Science News136:378-379, 1989.
Widner, H., and Brundin, P., “Immunological As-pects of Grafting in the Mammalian Central NervousSystem, A Review and Speculative Synthesis,”Brain Research Reviews 13:287-324, 1988.
Widner, H., Brund.in, P., Bjorklund, A., et al.,“Immunological Aspects of Neural Grafting in theMammalian Central Nervous System,” Progress inBrain Research, vol. 78, Transplantation Itio theMamrnulian CNS, D.M. Gash and J.R. Sladek, Jr.(eds.) (Amsterdam: Elsevier Science Publishers,1988).Widner, H., Johansson, B.B., Moller, G., et al.,“QualitativeDemonstration of aLink Between BrainParenchyma and the Lymphatic System After Intra-cerebral Antigen Deposition,” Journal of CerebralBlood Flow Metabolism 5:88-89, 1985.
Wolff, J.A., Fisher, L.J., Xu, L., et al., “GraftingFibroblasts Genetically Modified To Produce L-dopain a Rat Model of Parkinson’s Disease,’ Proceedingsof the National Academy of Sciences, U.S.A.86:9011-9014, 1989.
Wong, G. H.W., Bartlett, P. F., and Clark-kwis, I.,“Interferon Induces the Expression of H-2 and IaAntigens on Brain Cells,” Journal of Neuroimmu-?’W1OQ 7:255-278, 1985.

Chapter 5
Applications of Neural Grafting Intothe Brain and Spinal Cord

CONTENTSPage
NEURODEGENERATIVE DISORDERS . . . . . . .A.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Parkinson’s Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Huntington’s Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Alzheimer’s Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Motor Neuron Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CENTRAL NERVOUS SYSTEM INJURY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Spinal Cord Injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Brain Injury and Stroke . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
EPILEPSY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .NEUROENDOCRINE DEFICITS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .DEMYELINATING DISORDERS: MULTIPLE SCLEROSIS . . . . . . . . . . . . . . . . . . . . . . . .SUMMARY AND CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .CHAPTER 5 REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
61617374757575818282838484
Page. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
Box5-A. MPTP, a Key to Parkinson’s5-B. The Use of Registries To Collect Data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70
FiguresFigure .5-1. The Substantial Nigra and the Striatum . . . . . .5-2. Monkey Brain Exposed to MPTP . . . . . . . . . . .5-3. Adrenal Medulla Neural Graft for Parkinson’s5-4. Grafting Genetically Modified Fibroblasts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 675-5. Stereotactic Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 685-6. Brain Activity in an Alzheimer’s Disease and a Normal Brain . . . . . . . . . . . . . . . . . . 745-7. Possible Actions of Neural Grafts in Spinal Cord Injury . . . . . . . . . . . . . . . . . . . . . . . . 77
Page. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63Disease . . . . . . . . . . . . . . . . . . . . . . . . . 65

Chapter 5
Applications of Neural Grafting Into the Brain and Spinal Cord
The technology of grafting into the brain andspinal cord to restore functions lost through diseaseor injury is still in the initial stages of development.Research in animals has indicated that neuralgrafting may provide beneficial therapeutic effectsin some neurological disorders, notably Parkinson’sdisease. But in every case, including Parkinson’sdisease, there is still much information that needs tobe collected before neural grafting can be adaptedfor general use in humans. The research currentlybeing conducted in this field is aimed at learningmore about basic mechanisms involved in graftingtissues into the central nervous system (CNS) andthe actions and effects neural grafts can exert there.Information is being sought in three broad areas:
the conditions necessary for graft survival andincorporation into the host,the functional role grafted material can play inalleviating deficits caused by disease or injury,andthe mechanisms by which grafts produce anyfunctional recovery that is observed..
Scientists use many different kinds of experi-ments with animals to obtain this information. Someexperiments are designed to gain information aboutbasic mechanisms related to brain development, thebrain’s response to injury, and the regenerativecapabilities of nervous tissue. Others examine theability of grafts to ameliorate or reverse experimen-tally induced deficits. Still others use animal modelsthat either replicate or share features of humandisorders in order to determine whether graftingcould result in improved function. Thus, experi-mental work in the field of neural graftingprovides information about basic brain mecha-nisms as well as the role grafts can play inneurological disorders.
The need for animal models that mimic a givenneurological disorder in humans is as important inthe field of neural grafting as it is in most other areasof clinical research. Animal models of a disease orinjury can be either homologous (sharing a commonorigin with the human condition) or analogous(sharing similar organ damage, though not necessar-ily via the same disease mechanism). Currently,there are very few homologous models of human
neurological disease. The closer an animal model isto the human condition under study (in terms of theneurological damage induced and the resultingbehavioral effects), the easier it is to extend observa-tions from the model to a human disorder. Virtuallyall scientists in the field of neural grafting believe itis essential to develop good animal models for usein grafting experiments.
Theoretically, the applications of neural graftingtechnologies into the brain and spinal cord couldencompass many types of neurological disorders.The possible therapeutic applications of neuralgrafting range from the highly speculative to theactually implemented. This chapter provides anoverview of some of the possible applications ofneural grafting into the brain and spinal cord, theresearch that has been conducted so far, and thecurrent status of each. In addition, the possiblemechanism of therapeutic action of neural grafts foreach condition is discussed. The neurological disor-ders are presented according to type, with anemphasis on those that have been studied mostextensively.
NEURODEGENERATIVEDISORDERS
Parkinson’s Disease
The clinical use of neural grafting in the treatmentof Parkinson’s disease, begun in the early 1980s, hasgenerated controversy in the scientific and medicalcommunities. While more is known about neuralgrafting in Parkinson's disease than in any otherneurological disorder, the efficacy of grafting inhumans is unclear, and ethical concerns areunresolved. The concern about the discrepancybetween the base level of knowledge and the actualclinical use of these procedures, even under experi-mental conditions, has increased public awarenessof this controversy. This section provides a summaryof the animal research and clinical use of neuralgrafting in persons with Parkinson’s disease.
Parkinson’s disease is well suited to the applica-tion of neural transplantation because the diseaseresults from the degeneration of a discrete popula-tion of neurons located in an area of the brain called
-61-

62 ● Neural Grafting: Repairing the Brain and Spinal Cord
Figure 5-l—The Substantial Nigra and the Striatum
“’’’’””’X———W
Substantial
The cells of the substantial nigra send their axons to the striatum.This pathway degenerates in Parkinson’s disease.SOURCE: R. Restak, The Brain (New York, NY: Bantarn Books, 1984).
the substantial nigra. These neurons produce dopa-mine, a neurotransmitter, and form synapses withneurons in another area of the brain, the striatum(figure 5-l). The neurons in the striatum are notdestroyed in Parkinson’s disease (67); however, thedepletion of dopamine in the striatum, caused by theloss of cells in the substantial nigra, is associated withthe symptoms of tremor, rigidity, difficulty instanding, and slowness of movement that are charac-teristic of Parkinson’s disease. Neural grafting inParkinson’s disease has been aimed at correcting theloss of the dopamine-producing pathway betweenthe substantial nigra and the striatum by eitherreplacing the dying cells or supplying additionaldopamine . To do this, neural grafting materialsfrom two main sources have been used: 1) tissuefrom the adrenal gland and 2) tissue from thefetal CNS. A graft that would survive indefinitelycould produce continuous relief from symptoms, butevidence suggests that the degeneration of thedopamine -producing neurons in the substantial nigrawould continue. All research to date has beenaimed at the ability of grafts to provide relieffrom symptoms and reduced disability, not cessa-tion or reversal of the degenerative process.
The most obvious site for transplantation ofdopamine -producing cells in Parkinson’s disease
would seem to be the locus of the degenerating cells,i.e., the substantial nigra. While cells placed in thissite might receive some inputs from neurons in otherareas of the brain that normally send fibers to thesubstantial nigra, axons from the grafted cells wouldhave to grow several centimeters through the brainto connect with their targets in the striatum. Unfortu-nately, nerve fibers do not readily grow over suchdistances in the adult brain, and it has been shownthat dopamine-producing grafts implanted into theexperimentally damaged substantial nigra of rodentshave no effect on the parkinsonian symptoms suchdamage causes (40).
Instead, dopamine-producing cells have beengrafted (either as a cell suspension or as solid pieces)to sites close to their targets in the striatum, in orderto facilitate formation of synapses. In fact, it isunclear whether the formation of synapses is actu-ally necessary to produce an effect—it is possiblethat some of the effects of dopamine produced in the
.*
%%1$-,%
. . \1 @.~.,.*W
$ . .* ,* \ ~.,+$ ~%.w. ~’ ~ ,’, %. . .%% - Q *.-,.* ., *.~.:? .% -3$. . ...;3 ‘ . ~“ >k> ,+
. .* , ;$%< “b’
~;’ .,s . . ~~ %’ :ky ‘.$’ ‘
.4.$J A $ . . .Photo credit: J.R. Sladek, Jr., University of Rochester Medical Center
Picture of a graft of monkey fetal tissue implanted into anadult monkey.

Chapter 5--Applications of Neural Grafting Into the Brain and Spinal Cord ● 63
striatum by grafts may result simply from the diffuserelease of chemicals in the area and thus do notrequire specific, point-to-point synaptic connectionsand precisely timed release.
Animal Research
Fetal Tissue—The first indication that graftsmight be effective in the treatment of Parkinson’sdisease was observed in experiments conducted in1979 (19,1 19). These experiments used rats in whichthe pathway between the substantial nigra and thestriatum had been destroyed by the neurotoxin6-OHDA, l thus chemically affecting the same sitethat is thought to be central to the clinical signs ofParkinson’s disease. Grafts of dopamine-producingneural tissue from rat fetuses, implanted into thestriatum, were able to reduce some deficits causedby the wound (40,41); however, the extent and typeof function that was restored depended on where inthe striatum the graft was placed (40,41).
Since these initial experiments, many others usingthe same animal model have shown that implantedfetal tissue sends out fibers and makes contact withthe host tissue, receives inputs from the host tissue,and performs typical neuronal functions within thehost (3,20,54,55,103,131,139,141, 153).
Although some of the functional recovery pro-duced by neural grafting may be due to thenonspecific release of dopamine into the host brain,studies have shown that much of the observedrecovery is related to the extent to which theimplanted tissue becomes incorporated within thehost brain--i.e., the degree to which the graft sendsconnections to, and receives connections from, thehost brain. This finding indicates that more than justa diffuse release of dopamine into the striatum isinvolved. In fact, when the graft is removed, thecorrective effects disappear, suggesting that they aredue to a direct action of the graft and not to an effectunrelated to it (17,42).
Dopamine-producing fetal tissue has also beenstudied in the MPTP model of parkinsonism (figure5-2).2 While it takes only days for MPTP to producethe symptoms of parkinsonism in laboratory ani-
Figure 5-2—Monkey Brain Exposed to MPTP
The brain of a monkey that was exposed to MPTP on one side.‘The substantial nigra on the unexposed side (right) is normal(black band). On the MPTP exposed side (left) the cells of thesubstantial nigra are destroyed.SOURCE: R.A.E. Bakay, Section of Neurological Surgery, The Emory
Clinic.
reals, as compared to years for the disease itself inhumans, most scientists still regard this as the bestanimal model of the disease (see box 5-A). Also,since MPTP is particularly effective in monkeys, ithas provided scientists with an important primatemodel of parkinsonism. (Data derived from experi-ments using monkeys are more easily extrapolatedto humans than are data from nonprimate animalmodels.) As with the 6-OHDA experiments, it wasshown that grafted dopamine-producing fetal neuraltissue can become incorporated into the striatum oftreated monkeys and result in significant, long--lasting reductions in movement abnormalities, in-cluding tremor, rigidity, and slowness of movement(7,8,31,49,124,135). Recently, this effect of fetaltissue grafts in monkeys has been linked to theability of the grafts to stimulate new growth fromundamaged neurons (10).
In Summary, a number of different studies havedemonstrated that dopamine-producing fetal tis-sue can counteract some of the effects producedin the 6-OHDA and MPTP animal models ofparkinsonism. In particular, some of the results seenfollowing grafting in nonhuman primates treatedwith MPTP have been promising. However, in
l~s tiogoW anim~ model is produced by the neurotoxin 6-hydroxydop amine (6-OHDA), which selectively destroys doparni.m+producingneurons. In this model the 6-OHDA is injected directly into the substantial nigra. While the lesion produced by this injection destroys the same neuronsthat are lost in Parldnson’s disease, the action of the chemical and the temporal course of the neuron destruction do not mimic what occurs in the disease.Also, the functional deficits produced, while in some respects simiku to those produced by Parkinson’s disease, are not exactly the same.2- (1-Me~yl.~phenyl.l-z.3-6-te&~y&opfi~e) is a chemical that, when administered, causes a syndrome ShikU tO pMhSOn’S dis-.
Thus, the drug is said to result in parkinsonism rather than Parkinson’s disease (see box 5-A).

64 ● Neural Grafting: Repairing the Brain and Spinal Cord
Box 5-A—MPTP, a Key to Parkinson’s Disease
On a July morning in 1982, a patient was brought into the emergency room of a hospital in Santa Cruz,California. He was stooped over and displayed the symptoms of rigidity and inability to initiate movement typicallyseen in persons in their sixties or seventies who have been suffering from Parkinson’s disease for many years. Theclinical picture was that of classic, late-stage Parkinson’s disease. However, this patient was 24 years 014 and hissymptoms had developed virtually overnight. With this startling patient began one of the most interesting andimportant chapters in the history of Parkinson’s disease research and treatment.
A closer examination of this patient and five others who came to hospital emergency rooms in the northernCalifornia area at about the same time revealed that they were all heroin addicts who had injected some homemadenarcotics that contained an impurity. The impurity was determined to be the chemical 1-methy1-4-phenyl-1,2,3,6-tetrahydropyridine, or MPTP. It was thought that the MPTP might have caused brain damage that mimickedParkinson’s disease, resulting in identical symptoms, This hypothesis was lent further credence by an autopsy reporton another individual who had been exposed to MPTP. The report noted that the man’s brain looked like that ofsomeone who had suffered from Parkinson’s disease for years: The dopamine-containing neurons in the substantialnigra, which are lost in Parkinson’s disease, were destroyed. It was also found that when given L-dopa, the mostcommon medicine for treating Parkinson’s disease, the patients exposed to MPTP improved dramatically. However,the effectiveness of the L-dopa began to wear off after 2 to 3 years, just as it does in most Parkinson’s patients after5 to 10 years.
Immediately after the identification of MPTP as the agent responsible, scientists began to study the compoundto find out how it causes this model of parkinsonism. They found that MPTP can enter the bloodstream throughdirect injection, inhalation, or contact with the skin. Inside the brain, an enzyme called monoamine oxidase B(MAO-B) breaks down MPTP into other chemicals, including an electrically charged molecule calledmethylpyridine (MPP+). The MPP+ molecules are taken up selectively by dopamine-producing neurons. It isthought that, once inside these dopamine neurons, the MPP+ may cause another chemical reaction to take place.This reaction produces toxic substances, such as peroxides, and other charged particles, called free radicals. Theproduction of these substances destroys the cell. It was also found that if the breakdown of MPTP to MPP+ isprevented by blocking the activity of MAO-B, MPTP has no effect.
This understanding of the chemistry of MPTP has led to a new understanding of what might be occurring inpersons with Parkinson’s disease. It is possible that the same sorts of toxin-producing chemical reactions that MPTPcauses in the brain occur in Parkinson’s patients, What causes the chemical reactions to take place in the diseaseis unclear, but it may be some disruption in the normal biochemical activity of the dopamine-producing neurons.Indeed, it has been known for some time that MAO-B is also involved with the normal breakdown of dopaminein these cells. It is possible that this normal process gets disrupted somehow and that when the dopamine is brokendown, peroxides and free radicals are produced. Based on these new MPTP data, a drug called deprenyl, which isknown to block the action of MAO-B, was studied. It has been shown, at least in one study, that deprenyl appearsto have a retarding effect on the progression of the disease. While this finding needs to be confirmed, it indicateshow the information gained from the MPTP model of parkinsonism is giving scientists and doctors valuable newinformation about the disease,
Another theory that has been proposed as a result of the discovery of MPTP is that Parkinson’s disease mightbe caused by environmental exposure to MPTP or a chemical like it. While this is a possibility, no strong evidenceof any link between the incidence of Parkinson’s disease and exposure to MPTP in the environment has been foundto date.
Interestingly, it has been found that MPTP does not affect all species. While it produces symptoms ofparkinsonism in humans, nonhuman primates, and mice, it has little or no effect in rats, cats, rabbits, and a numberof other species. The reason for this is not clear, but it is thought to be due to differences in the blood-brain barrier.
The discovery of MPTP has greatly advanced the understanding of Parkinson’s disease. Not only has itprovided important new insights into the possible mechanism that causes the disease, but it has given scientists animportant and extremely useful new tool to study Parkinson’s disease. The nonhuman primate MPTP model hasbeen and will continue to be one of the best experimental tools for detegrafting to treat Parkinson’s disease.
rmining the efficacy of the use of neural
SOURCE: Office of Technology Assesstment, 1990.

Chapter 5-applications of Neural Grafting Into the Brain and Spinal Cord ● 65
Figure 5-3—Adrenal Medulla Neural Graft for Parkinson’s Disease
Tissue from a patient’s adrenal gland, which lies atop the kidney(1), is implanted into the striatum (2).SOURCE: Newsweek Apr. 14, 19S6, I.B. Ohls.son.
addition to the need to replicate and expand thesefindings, there is a need to answer the followingquestions by means of additional animal studies:
. Where in the striatum should material begrafted to achieve maximum effect?
● How long do the effects of the graft last?
Adrenal Medullary Tissue—There is consider-able interest in finding alternative sources of dopam-ine-producing grafting material, for two reasons.First, there are ethical, legal, and technical obstaclesto procurement of human fetal tissue for transplanta-tion. Second, the use of autografts (tissue from theperson’s own body) eliminates possible immuno-logical rejection of the graft. While other types oftissue for autografts have been studied [sympatheticganglia, carotid body glomus cells, (15,83)], tissuefrom the medulla of the adrenal gland has attractedthe greatest interest. In animal experiments, theadrenal tissue is collected from donor animals; inhumans with Parkinson’s disease, the patient’s ownadrenal tissue can be used for the graft (figure 5-3).
The efficacy of adrenal tissue is more uncertainthan that of fetal CNS tissue. Questions have been
raised about how effective adrenal tissue is inproducing fictional recovery, what mechanisminduces functional effects, and whether any ob-served functional effect is actually due to a directeffect of the graft or to some other factor.
Implantation of adrenal medullary tissue canameliorate some of the deficits created in the6-OHDA model in rodents; however, the range offunctions recovered is narrower than when fetaltissue is used (52,96). The beneficial effects arethought to result from either a nonspecific, diffuserelease of dopamine by the adrenal cells (53) or anincrease in the number of new dopamine fibers nearthe graft site (112). The latter presumably reflectsthe degree to which the grafted adrenal medulla cellsare converted into neuron-like cells that produce
dopamine.
The number of adrenal cells that survive implanta-tion is very low in both rodents (15) and monkeys(1 1,75,108). If the cells do not survive, the chance offunctional recovery is small and any long-term

66 ● Neural Grafting: Repairing the Brain and Spinal Cord
Photo credit: R.A.E. Bakay, The Emory Clinid
Section of a monkey brain showing a surviving graft ofadrenal medulla tissue that was implanted along with other
tissues that produce neurotrophic substances.
recovery that does occur is probably due to someeffect unrelated to continued graft function. Adrenalcell survival is enhanced when neurotrophic factors,including nerve growth factor (NGF), are added tothe graft site (16,88,140). In monkeys, increasedfictional recovery is observed when adrenal cellsare grafted along with cells that produce neurotro-phic factors (88), although it has been observed inrats that the same level of functional recovery occurswhen NGF is given in conjunction with eitheradrenal grafts or grafts of nondopamine-producingmaterial (121). This suggests that the functionalrecovery observed in the latter case resulted, in part,from activation of the brain’s injury responsemechanisms due to surgical injury (including releaseof growth factors) and the nonspecific action of NGFto promote axon growth.
Another issue surrounding adrenal tissue grafts isthe influence of donor age on graft efficacy. Graftsfrom younger rats are more effective than those fromolder rats in promoting functional recovery follow-ing destruction of dopamine-producing cells with6-OHDA (51). Also, older tissue is less likely toundergo the conversion from adrenal medulla cellst o dopamine-producing neurons (9). This may bedue to a lack of growth-promoting factors, perhapsNGF, in the older tissue. When NGF is administeredto rats in conjunction with grafts of older adrenaltissue, more conversion of cells to dopamine-producing neurons is seen and a greater improve-ment in movement occurs (140). Since many Parkin-son’s disease patients are elderly, donor age may be
one reason for the limited effect of adrenal autograftsused in these patients (see later discussion).
The data collected on adrenal grafts in the MPTPnonhuman primate model of parkinsonism agreewith the data obtained in 6-OHDA experiments withrats. As noted previously, only limited survival ofgrafted tissue following implantation has beenobserved (11,75). This raises the question of what isresponsible for the functional recovery that has beenseen. New dopamine fibers growing in the host brain(47) and functional improvement (11) have beenobserved in both grafted animals and animals thathad the surgery performed without tissue implanta-tion. This suggests that the surgical procedure itselfhas some effect. As was true of the rats, the degreeof functional recovery in nonhuman primates is lesswith adrenal medullary tissue than with fetal CNStissue (100).
In summary, the ability of adrenal medullarytissue to ameliorate the deficits caused in animalmodels of parkinsonism is unclear. Questions thatneed to be answered include:
●
●
●
Are the functional improvements that havebeen observed the result of the adrenal graft orthe surgical procedure?If adrenal grafts do have a beneficial effect,what is the range of deficits that can beimproved?What role can concomitant application ofgrowth-promoting factors play in the survivaland efficacy of adrenal grafts?
Genetically Engineered Cells-Genetically en-gineered cells have been shown to survive graftinginto the CNS (58). The ability of geneticallymanipulated cells to decrease the abnormal behaviorcaused by administration of 6-OHDA to rats hasrecently been investigated (151). Certain skin cells,called fibroblasts, were taken from rats and geneti-cally modified to produce the enzyme tyrosinehydroxylase (TH), which is required for the produc-tion of dopamine (figure 5-4). It was hoped thatinserting these cells into the 6-OHDA rats wouldcause the animals to produce dopamine and thusreduce their abnormal behavior. The grafts of thegenetically engineered cells did reduce abnormalbehavior, by about 40 percent.
Although this important study indicates thatgenetically altered cells might be an effectivegrafting material, it was noted that the extent of

Chapter 5--Applications of Neural Grafting Into the Brain and Spinal Cord ● 67
Figure 5-4-Grafting Genetically ModifiedFibroblasts
/’” + u 1° cells or;:j cell line
~ GraftBehavioral 4
b
testing Culture cells
mk==>fBiochemical
- - Geneticcharacterization
Select modified cellsmodification
The process of grafting genetically engineered fibroblasts con-sists of: 1) culturing the fibroblasts, 2) genetically modifying them,3) selecting which cells to use, 4) testing them, 5) grafting into thebrain, and 6) behavioral testing of the animal to determine theeffect of the graft.SOURCE: F. Gage, Department of Neuroscience, University of California,
San Diego.
recovery was less than that which has been observedwhen fetal CNS tissue is used. One possible reasonfor this difference is that the manipulated cells do notproduce as much dopamine as normal fetal braincells. Nonetheless, since the use of geneticallymanipulated cells lines would circumvent the prob-lems associated with fetal tissue and the immuno-logical considerations connected with other sources,continued exploration of their use is an importantarea of research.
Human Application
Human trials of neural grafting in persons withParkinson’s disease have used both adrenal and fetalCNS tissue. In both cases, some observers have heldthat the trials were premature (137). In the case ofadrenal grafting, many observers believe that therehas been a rush to proceed with human trials withouthaving first collected adequate data from animalexperiments; in the case of fetal tissue grafts, whilethere is a larger base of animal data to draw on, thereis still concern that widespread implementation ofhuman fetal tissue grafting could proceed beforeadequate information has been derived from animalexperiments. This question may place scientists whoare doing the research at odds with patients anddoctors, who must deal with the realities of devastat-ing illness on a daily basis. The participants in thisdebate include scientists performing basic research,
desperately ill patients who are willing to undergovirtually anything that might help them, and clini-cians, who are motivated by the altruistic desire tohelp their patients and, perhaps, by the ambition tobe on the cutting edge of a new and exciting field.
As of 1990, between 300 and 400 persons withParkinson's disease had received neural graftsworldwide. About 100 of them have been implantedwith fetal CNS tissue, the remainder with adrenaltissue. In the United States, approximately 130patients have been treated with adrenal tissue, whilefewer than 10 have had fetal tissue implants. The useof fetal tissue for implantation in this country islimited to privately funded ventures because of themoratorium on Federal funding for such research(see app. A).
Surgical Procedures--Implantation of adrenal orfetal tissue into the brain can be done using either astereotactic or an open surgical approach. In astereotactic procedure, the tissue is implanted bymeans of a long needle inserted into the brainthrough a small hole made in the skull; thisprocedure is guided by various computer-assistedimaging procedures and brain scans (figure 5-5). Inan open surgical procedure, the area where the graftis to be placed is exposed so it can be seen by theneurosurgeon. This procedure, therefore, is moreinvasive than the stereotactic procedure. In addition,a patient undergoing an adrenal transplant must alsoundergo surgery to remove one of his or her adrenalglands for implantation.
Most stereotactic procedures are performed underlocal anesthesia, although general anesthesia issometimes used. Implantation of tissue using astereotactic procedure usually takes 1 to 1 1/2 hours.Following surgery, patients are often observed in aneurological intensive care unit overnight in casesurgical complications develop. Provided there areno complications, the patient could recover from theoperation within 24 to 48 hours and be fit fordischarge a few days after that. In the case ofexperimental procedures, however, it is likely thatthe patient would be kept in the hospital longer, forobservation and for comprehensive testing.
While an open approach is more invasive, itprovides more flexibility in the way graft tissue canbe implanted. A general anesthetic is given, and aportion of the skull is removed. For grafting inParkinson’s disease patients, the surface of thestriatum is exposed by incising the overlying brain

68 ● Neural Grafting: Repairing the Brain and Spinal Cord
Figure 5-5-Stereotactic Surgery
Photo credit: The Emory Clinic
Adrenal medulla graft surgery.
tion may make it possible to retrieve the adrenaltissue, preserve it, and then wait until the patient hasrecovered from the abdominal surgery before per-forming the grafting procedure.
An X-ray of a patient in a streotactic apparatus.SOURCE: Spiegel, Encyclopedia of Neuroscience, vol. G.
(cd.) (New York, NY: Boston, 1987).
tissue; a cavity is made on the surface of the striatum,and the graft tissue is placed into that cavity.Sometimes the graft is held in place by surgicalstaples or by a covering of a specially treatedmaterial. The piece of bone that was removed fromthe skull is replaced, and the scalp wound is closed.This operation generally takes 3 to 4 hours. Thepatient is usually returned to the neurologicalintensive care unit for observation. In general,recovery from the operation takes several weeks.
When adrenal medullary tissue is used for graft-ing, one of the patients two adrenal glands has to beremoved. This procedure is called an adrenalectomy.Since the adrenal gland lies atop the kidney, itsremoval requires abdominal surgery. Access to theadrenal gland is obtained through an incision ineither the abdomen or the side of the patient.Normally, an adrenalectomy is performed by asurgeon working in tandem with a neurosurgeon,who is simultaneously preparing for the implanta-tion. In the future, techniques such as cryopreserva-
Thus far, the majority of patients who havereceived adrenal grafts have had both the adrenalec-tomy and the brain surgery done at the same time.The procedure is quite debilitating, and recoverytakes a long time, often weeks. Patients may alsoexperience the surgical complications that canaccompany abdominal surgery and neurosurgery.Based on the results presented by different groups inthe United States that have done adrenal grafts, themortality rate and the rate of complications haveeach been estimated at 5 to 10 percent (100).
Adrenal Medulla Grafts—Based on the earlysuccess obtained in rodent experiments using adre-nal tissue, the first grafts of adrenal medullary tissuein humans were performed on two Parkinson’spatients in Sweden in 1982; both patients had beenexperiencing severe fluctuations in the managementof their disease by medications (the so-called on-offphenomenon ) (5). In a subsequent study, twoadditional patients were operated on (97). In all fourpatients, a stereotactic technique was used to trans-plant medullary tissue from the patient’s ownadrenal gland into the striatum on one side of thebrain. These patients showed minor improvementsin motor function that lasted for about 2 months. By
to and unpredictable shifts between periods in which the symptoms of Parkinson’s waler (on), they (off). This occurs regardless of when patients aregiven.It is thoughtthat the phenomenon results from the continued progression of the disease. Most patients will eventually experience dose-related fluctuations in theirsymptoms, but the on-off phenomenon is more rare.

Chapter 5-applications of Neural Grafting Into the Brain and Spinal Cord . 69
6 months, no positive effects remained. No adverseeffects of the procedure were reported. Long-termfollowup of these patients has not shown anyinfluence of the transplant on the course of thedisease (96). In the face of these modest effects andthe simultaneous development of the MPTP primatemodel of parkinsonism, it was widely consideredthat further animal research was needed beforeattempting additional grafts in patients.
In 1986, however, a group in Mexico conductedsimilar grafting experiments on patients with Park-inson’s disease. These experiments differed fromthose done by the Swedish group in that the adrenalgrafts were performed using an open surgicalprocedure and the tissue was placed into the brain ina slightly different fashion. Furthermore, the pa-tients were generally younger and in a less advancedstage of the disease. In 1987, the Mexican groupreported dramatic and persistent improvements inthe first two patients (102). The surgeons placedseveral fragments of adrenal tissue into a singlecavity on the surface of the striatum on one side ofthe brain and anchored them with miniature staples.Improvements in muscle movements were seenalmost immediately after recovery from surgery,with continued improvement over the next 10months. In a second report, in 1988, the outcomes forthe Mexican group’s first 11 grafting patients weredescribed (38). All patients (ages 35 to 65) were saidto have improved in gait and writing capability;tremor and rigidity were lessened and movementwas improved in most cases; and medication couldbe reduced in all. The Mexican group has nowperformed the operation on more than 40 Parkin-son’s disease patients. Four of the patients havesubsequently died (the relation of death to thesurgery is not clear); no postmortem confirmation ofsurviving adrenal cells has been reported.
Despite the discrepancies between the Mexicanand Swedish results, the 1987 Mexican report led toa torrent of adrenal medullary operations on Parkin-son’s patients around the world. Approximately 300operations using adrenal medulla autografts havebeen carried out worldwide. In many of theseoperations, the neurosurgeons attempted to followthe procedure of the Mexican group, with only minormodifications. A detailed observation of 19 patientsover a period of 6 months in Chicago, Tampa, andKansas City has been published (69,1 18). A modestreduction in these patients’ off periods (whensymptoms are most severe) was found, but the
patients were still disabled by the disease. Also, thegrafting procedure did not permit dosages of theirmedications to be decreased. Frequent medicalcomplications were associated with the procedure. Afollowup study of 7 of the 19 original patientsreported that, 12 months after their operations, theoverall amount of on time was increased and theseverity of symptoms during off time was decreased(71).
Other studies, including one involving a group of18 patients treated in Nashville (1) and severalinvolving smaller groups of patients (2,94,95,117,148), have been published or presented inabstract form at scientific meetings. They havereported variable results with the use of adrenalgrafts. In an effort to establish a centralized reposi-tory for the data collected from these procedures,two registries have been established (see box 5-B).The results collected by each of these registries havebeen published (6,70), with the data from somecenters included in both reports. One registryindicated that there was “a rather diffuse responsewith a general trend for improvement, but mostlymodest improvement” (6) 1 year following surgery,and the other reported a statistically significantdecrease in disability, as indicated by an increase inon time and less severe symptoms during off periods1 year after surgery (70). Neither registry found thatit was possible to decrease the medication patientsreceived, and both reported a number of postopera-tive complications. The complications, which insome cases were transitory (lasting less than 3months) but in others persisted for as long as a year,included respiratory problems, pneumonia, urinarytract infections, and a number of transitory psychiat-ric problems, including hallucinations or delusions,sleepiness, and confusion.
Data from both registries clearly show that thereare fewer complications associated with removal ofthe adrenal gland through the patient’s side asopposed to the abdominal cavity and by stereotacticplacement of the tissue into the brain versus an openneurosurgical approach. Older, more severely af-fected patients were more likely to have adverseeffects and less likely to benefit from the procedure,leading to the conclusion that, based on the datacollected thus far, the ideal patient ‘‘. . . would beless than 55 years of age and only moderatelydisabled” (6). The mortality rate according to thedata collected by one of the registries was 10percent, though not all the deaths were thought to

70 ● Neural Grafting: Repairing the Brain and Spinal Cord
Box 5-B—The Use of Registries To Collect Data
In 1987, in an attempt to docum ent the activity occurring in the field of adrenal-neural grafting, the AmericanAssociation of Neurological Surgeons (AANS), in collaboration with the National Institute of NeurologicalDisorders and Stroke (NINDS), established the General Registry of Adrenal-Fetal Transplantation (GRAFT’). Likethe National Heart Transplant Registry established in the early 1980s to track the work being done in hearttransplantation, the idea behind GRAFT is to provide a central clearinghouse where researchers in the field can sendtheir data so that sufficient information can be collected to evaluate the various methodologies being used.Following the report from Mexico of successful adrenal grafting in persons with Parkinson’s disease, a number ofcenters began trying to replicate the results. These studies usually involved small numbers of patients and usedvarious modifications in the surgical technique. It was thought that, by pooling data from the various sources, anongoing analysis could be performed . . of the evolving transplantation experience to document the potential riskfactors and to guide future studies” (Bakay et al., in press).
At about the same time that GRAFT was established, the United Parkinson Foundation (UPF) announcedformation of its own registry. In order to avoid duplication and competition between the two groups, it was decidedthat the focus of the two registries would be different. GRAFT would focus on safety, efficacy, and surgical issuesby collecting data from as many centers as were willing to participate. The UPF registry would collect data froma smaller, more uniform group of investigators. Due to different methods of data acquisition, the UPF would be ableto make a more quantitative evaluation of efficacy, as opposed to GRAFT, which would have to rely on qualitativemeasures of efficacy. As a result of this arrangement, some research teams have contributed data to both registries.
As of mid-1990, the GRAFT registry had collected data on 135 patients from 24 centers. Most are from theUnited States, with two centers each from Canada and South America and one from Europe and Mexico. Thedatabase includes preoperative information on demography, medical history, and prior treatment of parkinsonism,as well as qualitative evaluation of patients’ responses to the procedure and complications at 3, 6, and 12 monthsafter the operation. Followup information more than 1 year later is currently being collected.
The UPF registry has collected information on 61 patients from 13 centers in the United States and Canada.The same kind of demographic information was collected, but the pre- and post-operative data were collected ina more uniform manner: All the centers were asked to analyze the patients and their responses to the surgicalprocedure using the same rating scale. This made it possible to compare and evaluate the data from all the centersmore easily. These data were collected 12 months tier the operation,
The l-year data from both registries have been published and both registries are continuing to collectinformation. Registries are an effective way of collecting and comparing information derived from a variety ofsources in order to evaluate progress in the development of a surgical procedure. Their success depends on thewillingness of investigators to supply their data and in some cases to comply with requests to collect data usingstandardized methods. When these criteria are met, data from registries are invaluable guides for futureinvestigations.
SOURCES: R.A.E. Balmy, G.S. Allen, M.L.J. Apuzzo et al., “Preliminary Report on Adrenal Medullary Grafting From the AmericanAssociation of Neurological Surgeons GRAFT Project,” Progress in Brain Research, in press; C.G. Goetz, G.T. Stebbins, H.L.Klawans et al., “United Parkinson Foundation Neurotransplantation Registry Multicenter United States and Canada DatabasePresurgical and 12-Month Followup,” Proceedings of the Third International Congress of Neurotransplantaion: Cambridge(Amsterdam: Elsevier Science Publishers, 1989).
have been due to the surgical procedure (70). The beginning in 1986. The Chinese group used aoverall level of improvement and number of compli-cations observed led to this summary of the datacollected by both groups:
This strongly suggests that there is an effect fromthe transplantation, although the effect inmost casesis not very dramatic. The mild-to-moderate improve-ment would be more enthusiastically received if thesurgical morbidity were less (6).
The original Swedish results also inspired a seriesof adrenal medullary autografts in Beijing, China,
stereotactic technique similar to that of the Swedishgroup, but it used a larger total mass of implantedtissue and administered antiparkinson drugs after theoperation. Substantial improvements in movementand lessening of rigidity and tremor were observedin the first four patients for at least 6 months aftersurgery. To date, this group has operated on at least10 patients, with claims of varying degrees ofimprovement in all cases (84). However, somescientists believe that it is difficult to interpret andcompare the results of this study and others (60,143)

Chapter Applications of Neural Grafting Into the Brain and Spinal Cord ● 71
due to differences in the methods used for assessingbenefit to patients and in the medical treatment theyreceived pre- and post-operatively.
Adrenal medullary autografts have also beenperformed in the United States in a small number ofpatients with progressive supranuclear palsy (PSP),a neurodegenerative disorder marked by loss ofneurons at various locations in the brain, includingthe substantial nigra. PSP, though much less commonthan Parkinson’s disease, has many of the samesymptoms, including difficulty in moving and stand-ing up. The disease is invariably fatal and there areno satisfactory pharmacological therapies. One re-port (87) described three patients with PSP who hadtissue from one of their adrenal glands grafted intothe striatum. Only one of the three patients showeda small degree of improvement, mostly in his abilityto stand. The authors conclude from these data that‘‘adrenal medullary transplantation has only limitedefficacy in progressive supranuclear palsy.’
To date, the success reported by the Mexicangroup in 1987 has been difficult to replicate. Thereason for this is unclear. Questions about diagnosticand other criteria used for inclusion of patients, themethods used to measure the severity of the diseasepreoperatively, the handling of the patients’ medica-tions, and the methods used to quantify the improve-ments in movement that were observed have beenraised about the Mexican study.
Based on the available data, the efficacy ofadrenal medulla autografts is unclear. The rela-tive effectiveness of the various open and stereotac-tic procedures used, their modes of action, and theexistence of surviving, functional adrenal medullarycells have not yet been conclusively established. Theefficacy of adrenal grafts has yet to be demonstratedin experiments using nonhuman primates, and thehuman clinical data are inconsistent, with severalstudies suggesting that there may be only minimal,perhaps transitory, improvement. Judging from ani-mal experiments and the small amount of post-mortem human data available, the ability of adrenaltissue to survive in the brain seems to be limited(80,120). Survival may be improved by concurrentadministration of growth-promoting factors, but thisneeds to be explored further in the laboratory. Ifadrenal tissue does not survive, it is unclear whetherany observed improvement is the result of the graftor of nonspecific effects. The observation made inmany of the clinical trials that improvement was
Photo credit: The Emory
Dissecting tissue to be used as a graft.
seen on both sides of the body when the graft wasplaced in only one side of the brain also suggests ageneral effect, perhaps circulation of graft-relatedfactors in the cerebrospinal fluid, rather than a directaction of the graft. Additional animal experimenta-tion can provide more information and help answerthese questions. Regarding the use of the procedurein humans, the adrenalectomy and open neurosurgi-cal procedures most widely used are associated withrisk of severe complications in older, more pro-foundly afflicted patients. Also, the best age fordonor tissue and a clarification of which Parkinson’spatients are most likely to benefit fromthe procedureneeds to be delineated.
Fetal Neural Tissue-Only about 100 personsworldwide have received grafts of fetal CNS tissuefor the treatment of Parkinson’s disease. Clinicaltrials with such tissue are going on in Sweden,England, Mexico, the People’s Republic of China,Czechoslovakia, Spain, and Cuba. Approximately10 patients have undergone the procedure in theUnited States. While the results of some of theseprocedures have been reported at various scientificand medical meetings, there are very few published

72 ● Neural Grafting: Repairing the Brain and Spinal Cord
Some of the most thoroughly documented re-search has been conducted in Sweden, where twopatients underwent this procedure in 1987 (100).
Dopamine-producing tissue from four human fe-tuses, 7 to 9 weeks (postconception) of age, wasimplanted as a cell suspension, stereotactically, onone side of the brain in each patient. Both patientsreceived drugs to keep the graft from being rejected.Up to 6 months after the operation, although bothpatients showed some minor improvement in howquickly they could move and how well they re-sponded to a single dose of antiparkinson drugs, thescientists reported that “. . . no major therapeuticeffect from the operation was observed” (96). Thissame research group reported a greater degree ofimprovement in another patient, for whom they useddifferent methods of handling and implanting thefetal tissue and thus may have increased the abilityof the graft to survive (99). This patient exhibited alessening of his symptoms and an increased re-sponse to his medications for the 6 months he wasobserved after the surgery.
Other positive results have been reported fromgroups in Mexico and England, but these reportshave not been in the form of published papers inscientific journals providing information on how theprocedure was performed, what criteria were usedfor assessing patients pre- and post-operatively, andgiving all the details necessary to analyze the results.
In the United States, observations of a patient whowas operated on in Colorado in November 1988were reported 15 months after the operation (50). Inthis case, drugs to prevent graft rejection were notused. Some improvement in movement and motorcoordination was observed in this patient, and thepatient has reported increased ease in doing dailytasks (cutting food, brushing teeth, and so on). Also,the patient’s medication could be decreased withoutany adverse effects. While the investigators in-volved state that the patient is not cured, they believethat the implants can reduce disability, smooth outmedication-related fluctuations in symptoms, andincrease mobility.
The limited data collected to date suggest thatfetal CNS grafts may have a beneficial effect incontrolling some of the symptoms of Parkinson’sdisease. However, more information must be de-rived before an ultimate determination of the effi-cacy of this procedure can be made. How long the
grafted tissue survives, the optimal placement oftissue in the striatum, and the time course for seeingan improvement are unknown. Additional animalresearch can answer these questions. Then thedetails of how much tissue is needed to achieve aworthwhile therapeutic effect and the susceptibilityof the grafted tissue to immunological rejection andto the underlying destructive mechanism of Parkin-son’s disease can be derived from human experi-mentation. As stated by the Swedish research group:
Although our findings support the idea that neuralgrafting can be developed into an effective therapyin Parkinson’s disease, further work is necessary tooptimize the transplantation procedure. . . (99).
What Is the Next Step?
Whether clinical neural grafting experimentsshould continue before additional data are gatheredfrom animal experiments is still a subject ofscientific debate (93). In the case of adrenal tissuegrafts, the lack of replication of successes and thelack of a solid basis in animal experimentation havemade many persons in the medical and scientificcommunities retreat from the rush of enthusiasm thataccompanied the initial reports.
The effectiveness of fetal tissue grafting in animalmodels and the initial reports of some success withits use in humans indicate that fetal tissue graftingmay have a more solid scientific basis than adrenalgrafting. The question that now arises is how toproceed from here. Many persons in the scientificand medical communities feel that the questionsconcerning fetal CNS tissue grafting can best beanswered with additional basic animal research,coupled with limited human experimentation. Thenexpanded human trials could proceed to determinewhether fetal CNS grafts area genuinely efficacioustreatment for persons with Parkinson’s disease. Thisevaluation has been expressed in the followingstatement by two prominent scientists:
. . . too many questions remain unanswered aboutthe use of embryonic nerve cells to propose anythingmore than limited fetal grafting in humans as arequisite next step. Although scientifically it seemslogical to proceed, considerable information isneeded before therapeutic success might be pre-dicted . . . . We are still at a stage at which basicscientific studies are needed to elucidate importantdetails. . . (60).

Chapter 5-Applications of Neural Grafting Into the Brain and Spinal Cord ● 73
When clinical experiments do proceed, it will benecessary to standardize their designs, the criteriaused for assessing pre- and post-operative levels ofdisability, and the methods of reporting results. Forthe most part, this has not been done in the clinicalexperiments carried out so far, making it difficult tointerpret and compare studies.
Beyond the scientific issues, the legal and ethicalcontroversies that surround the use of fetal tissuecould impede the initiation of clinical trials. In theUnited States, the Federal ban on funding oftransplants using human fetal tissue from inducedabortions will limit clinical research (see app. A).
Huntington’s Disease
Huntington’s disease is a genetic disorder, themajor pathological hallmark of which is a loss ofneurons in the striatum. Symptoms of the diseaseinclude abnormal movements, especially of the faceand extremities, and a progressive deterioration inmental ability. Unlike Parkinson’s disease, whereonly one population of cells dies, Huntington’sdisease involves the destruction of several popula-tions of neurons, generally located in the striatum,that contain different neurotransmitters. An animalmodel in which chemicals known as excitotoxins areused to destroy the cells in the striatum4 has beenemployed to see whether implantation of fetalstriatal tissue could reverse some of the deficitscaused by the injury. This animal model exhibitssome of the same characteristics as persons sufferingfrom Huntington’s disease (e.g., abnormal move-ments, inability to respond to sensory stimuli, anddeficits in learning and memory). In most of theseexperiments, grafts have been inserted in hopesof replacing the lost striatal neurons rather thansupplying a single neurotransmitter, as in theParkinson’s disease research.
Studies have shown that rat fetal striatal tissue cansurvive following implantation into the striatum ofadult rats that have been injected with excitotoxins(114). These grafts have also been shown to decreasesome of the abnormal movement (36,66,81,129) andlearning and memory deficits (35) produced in thismodel; however it has been reported that theanimals’ behavior is not returned to normal (114).
The mechanism by which the fetal tissue grafts actis not entirely clear. There are two possibilities.First, the grafted tissue may grow into the host brain,forming synapses and thus directly and actively playa role in the function of the striatum. Experimentalevidence to support this includes the need for anintact, undamaged graft (66) at a specific region ofthe striatum in order to achieve a functional effect(82) (indicating the importance of graft integrationinto the host), coupled with the observation of aninteraction between host and grafted tissues(128,147). The second possibility is that the graftedtissue could be exerting a growth-promoting effectthat causes the undamaged parts of the host striatumto grow and assume some of the fictional activityof the damaged parts. Experimental evidence sup-porting this idea includes the conflicting observa-tions that integration does not occur (101,146) but afunctional effect may nevertheless take place (113)and that fetal grafts may be able to protect againstexcitotoxins (145) [although this has not beenconclusively proven (11 l)]. Although the majorityof the evidence indicates that grafts do integrate intothe host, the data preclude an unequivocal statement.The possible role of fetal striatal tissue in thetreatment of Huntington’s disease must awaitfurther elucidation of both the graft’s mechanismof action and the underlying mechanism of thedisease itself.
There has been one report, not published in aresearch journal, that grafting of rat adrenal medullatissue into the rat striatum can protect neuronsagainst the destructive action of excitotoxins (132).Since one theory holds that excitotoxins may beinvolved in Huntington’s disease, adrenal tissuecould possibly play a role in treating this disorder.Despite the lack of conclusive evidence to supportthis hypothesis, a patient with Huntington’s diseasehas received an adrenal medulla autograft (132). Itwas reported that the patient received no beneficialeffect from the procedure. At this time, there is noevidence to support the idea that adrenal tissue canameliorate any of the symptoms associated withHuntington’s disease: the role of excitotoxins in thedisorder has yet to be clarified, and the effect ofadrenal tissue on the action of excitotoxins has yetto be proven.
4~ this model, ~xcitoto~ -C aci~ ibotefic a@ qfio~c acid) ~ ~j~ted &EC~y tito the s~m. These toxhls SdIdilte Sites 011 LleWOIIS
that are normally activated by certain neurotransmitters; however, these acids activate the cells so much (hence the name “exCitO”) that they kill tiecells. Whether these excitotoxins are actually involved in Huntington’s disease in humans is unclear.

74 ● Neural Grafting: Repairing the Brain and Spinal Cord
Figure 5-6-Brain Activity in an Alzheimer’s Diseaseand a Normal Brain
Brain scans showing the activity (white areas) in a normal brain(control) and the brain of an Alzheimer’s disease patient (AD). Thescan of the Alzheimer’s disease patient shows that many areas inthe brain are not functioning properly.SOURCE: R. York, NY: Bantam Books, 19S8).
Alzheimer’s Disease
Unlike Parkinson’s or Huntington’s diseases, inwhich there is either a loss of a specific populationof neurons or localization of cell destruction in oneregion of the brain, Alzheimer’s disease involves amuch more diffuse loss of neurons and affects anumber of different groups of cells (figure 5-6).Cells in the front of the brain that contain theneurotransmitter acetylcholine and cells in themiddle of the brain that contain norepinephrine areparticularly affected in Alzheimer’s disease. Theacetylcholine-containing areas are involved withmemory and learning, while the norepinephrine-containing regions are thought to be associated withcontrolling moods. Destruction of these areas resultsin the dementia and depression that are characteristicof Alzheimer’s disease. Due to the diffuse natureof the damage in Alzheimer’s disease, it isthought that if neural grafts have a role, it maybeto supply growth-promoting substances or tosupply lost neurotransmitters rather than toreplace lost structures.
At present there is no fully satisfactory animalmodel of the symptoms of Alzheimer’s disease. Theclosest is aged monkeys, which can exhibit some ofthe memory and cognitive deficits or abnormalchanges in brain cells, or both, seen in persons withAlzheimer’s disease (122). To date no neural graft-ing experiments have been conducted on suchmonkeys; however, experimentation has been con-ducted on aged rats and rats that have had injuriesmade in the same areas of the brain that are destroyedin Alzheimer’s disease. These animals exhibit someof the same types of memory and learning problemsseen in humans with the disease, even though theydo not truly mimic Alzheimer’s disease.
To create animal models, wounds are made insome of the same areas of the front or middle part ofthe brain that are destroyed in Alzheimer’s diseaseor in the pathways that connect these areas to otherparts of the brain.s The result is that the animals havedifficulty learning and remembering certain tasks,such as running through a maze. When rat fetaltissue is grafted into wounded adult rats near theareas to which the acetylcholine fibers project, thegrafts take hold and there is a partial improvement inthe rats’ ability to learn and remember specific tasks(42,43,48,86,150). This occurs if the fetal tissueimplanted is taken from areas in the fetal brain thatcorrespond to the wounded areas in the adults.Similar results have been observed in adult ratswhen either grafts of fetal tissue from mice (32) orcultured cells that naturally produce acetylcholine(89) were implanted.
The ability of acetylcholine-producing grafts toreverse memory deficits caused by the ingestion ofalcohol has also been examined(4). Large quantitiesof alcohol cause brain damage in rats, as in humans,especially in the regions of the cortex and hippocam-pus containing acetylcholine; this damage causesmemory and learning deficits. When acetylcholine-producing tissue from the front part of the brain isimplanted into either the cortex or the hippocampusof rats given alcohol, the deficits decreased. Thisdoes not occur when other tissue, not containingacetylcholine, is grafted. It is postulated that thepositive effects are due to the increased supply ofacetylcholine into the cortex and hippocampus.
in front part of the brain send their fibers to the and specific the and these cortical areas are very important in mediating learning and memory. The neurons in the middleof the brain also connect to cortical areas. The wounds result in the loss of these or pathways and the cells giving rise tothem.

Chapter 5--Applications of Neural Grafting Into the Brain and Spinal Cord ● 75
Aged rats are also known to have more difficultylearning certain types of tasks than younger animals.Implantation of acetylcholine-producing fetal tissueinto the hippocampus (56,57) or norepinephrine-containing fetal tissue into ‘the middle of the brain(30) improves the performance of some aged rats oncertain learning and memory tests.
It is thought that the grafts in these studies exertedtheir effect by releasing acetylcholine or norep-inephrine into the brain. While the research con-ducted to date has provided invaluable informationabout the ability of neural grafts to decrease experi-mentally induced deficits in cognitive performanceand deficits in learning and memory in aged rats, theextrapolation of that information to patients withAlzheimer’s disease is problematic. These modelsshare, at best, only a few characteristics of thedisease. In addition, when injuries are produced inexperiments, they are very specific to the area that isdamaged, whereas in Alzheimer’s disease the dam-age is not restricted to a single group of neurons.
Since acetylcholine-producing cells are one of themajor populations of cells affected in Alzheimer’sdisease and nerve growth factor (NGF) is known toact on acetylcholine neurons, investigators havestudied the ability of NGF to protect these cells. Theimplantation of cells that have been geneticallyengineered to produce NGF has been shown toprevent the acetylcholine neurons in the front part ofthe brain from dying following destruction of thepathway that connects them to the hippocampus(127) and other areas of the brain (45). In addition,the protected cells apparently started to grow newfibers in the direction of the implanted NGF-producing cells. Whether NGF can affect the pro-gression of Alzheimer’s disease is a question beinginvestigated extensively.
A number of important points must be ad-dressed before the potential value of graftingtherapy in Alzheimer’s disease can be deter-mined. A better understanding of the mechanismsunderlying the disease is needed in order to deter-mine the types of graft tissue likely to have thebroadest possible effect on the disease. Also, devel-opment of a valid animal model of the disease or itssymptoms is necessary.
Motor Neuron Disease
Motor neuron disease (MND) is a family ofdisorders marked by degeneration of neurons lo-cated in the spinal cord and brain that are involvedwith regulating movement. Probably the best knownMND is amyotrophic lateral sclerosis (LOU Gehrig’sdisease).
As in some other neurodegenerative disorders,such as Parkinson’s and Huntington’s diseases, thehallmark of MND is a selective loss of certainpopulations of cells. Since Parkinson’s and Hunting-ton’s diseases are thought to be candidates forsymptom amelioration by neural grafting, it can bespeculated that persons with MND may also benefitfrom this procedure. The same strategy of replacingthe lost cell populations with grafts may be applica-ble. The ability of fetal spinal motor neurons tobecome incorporated into the spinal cord of an adulthas been demonstrated in rats (134) and mice (37).To date, no research on the ability of neural grafts torestore functional deficits caused by induced injuriesto these cell populations has been conducted.Whether MND would be at all amenable to thistherapeutic strategy is purely conjectural. The factthat the populations of cells lost in MND aredistributed throughout the spinal cord and the brainmay be a hindrance to the effective use of implants.It is also possible that the mechanisms involved inthe development and progression of MND are suchthat graft technologies would not be suitable.
CENTRAL NERVOUS SYSTEMINJURY
Spinal Cord Injury
Injury to the spinal cord occurs most often whenthe bones of the spinal column (vertebrae) arepushed into the soft neural tissue of the spinal cord,bruising or tearing it. This ensues when a strong,rapid, mechanical force is applied to the back orneck, as can occur in automobile collisions orsporting injuries. Incidents such as these are theleading cause of spinal cord injury. Damage to thespinal cord can also be caused by a projectile or knifewound. In such cases the amount of tissue damagedis directly related to the strength of the force applied.A third cause of damage to the spinal cord isdisruption of its blood supply or gradual compres-sion (caused by various types of intruding bodies,such as tumors or blood clots).
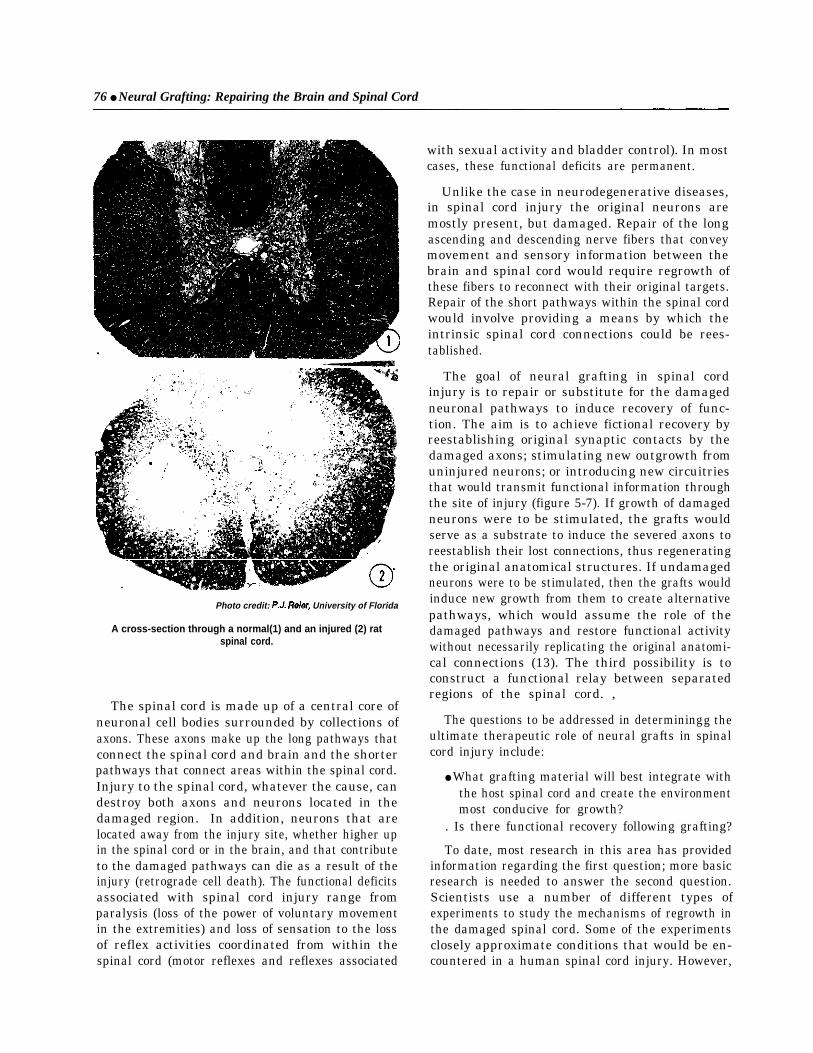
76 ● Neural Grafting: Repairing the Brain and Spinal Cord
Photo credit: University of Florida
A cross-section through a normal(1) and an injured (2) ratspinal cord.
The spinal cord is made up of a central core ofneuronal cell bodies surrounded by collections ofaxons. These axons make up the long pathways thatconnect the spinal cord and brain and the shorterpathways that connect areas within the spinal cord.Injury to the spinal cord, whatever the cause, candestroy both axons and neurons located in thedamaged region. In addition, neurons that arelocated away from the injury site, whether higher upin the spinal cord or in the brain, and that contributeto the damaged pathways can die as a result of theinjury (retrograde cell death). The functional deficitsassociated with spinal cord injury range fromparalysis (loss of the power of voluntary movementin the extremities) and loss of sensation to the lossof reflex activities coordinated from within thespinal cord (motor reflexes and reflexes associated
with sexual activity and bladder control). In mostcases, these functional deficits are permanent.
Unlike the case in neurodegenerative diseases,in spinal cord injury the original neurons aremostly present, but damaged. Repair of the longascending and descending nerve fibers that conveymovement and sensory information between thebrain and spinal cord would require regrowth ofthese fibers to reconnect with their original targets.Repair of the short pathways within the spinal cordwould involve providing a means by which theintrinsic spinal cord connections could be rees-tablished.
The goal of neural grafting in spinal cordinjury is to repair or substitute for the damagedneuronal pathways to induce recovery of func-tion. The aim is to achieve fictional recovery byreestablishing original synaptic contacts by thedamaged axons; stimulating new outgrowth fromuninjured neurons; or introducing new circuitriesthat would transmit functional information throughthe site of injury (figure 5-7). If growth of damagedneurons were to be stimulated, the grafts wouldserve as a substrate to induce the severed axons toreestablish their lost connections, thus regeneratingthe original anatomical structures. If undamagedneurons were to be stimulated, then the grafts wouldinduce new growth from them to create alternativepathways, which would assume the role of thedamaged pathways and restore functional activitywithout necessarily replicating the original anatomi-cal connections (13). The third possibility is toconstruct a functional relay between separatedregions of the spinal cord. ,
The questions to be addressed in determiningg theultimate therapeutic role of neural grafts in spinalcord injury include:
● What grafting material will best integrate withthe host spinal cord and create the environmentmost conducive for growth?
. Is there functional recovery following grafting?
To date, most research in this area has providedinformation regarding the first question; more basicresearch is needed to answer the second question.Scientists use a number of different types ofexperiments to study the mechanisms of regrowth inthe damaged spinal cord. Some of the experimentsclosely approximate conditions that would be en-countered in a human spinal cord injury. However,

Chapter 5--Applications of Neural Grafting Into the Brain and Spinal Cord ● 77
Figure 5-7-Possible Actions of Neural Grafts in Spinal Cord Injury
A.
o
0 <0 —— —..— <—— —.. 4
—————— –<
<
Graft
c.
{
v ---- —.\ -<‘ -. - .L
I \ ‘<‘<
<
Graft
D.
o <() <– –
‘ – – – – – –
~~o – – –– — ‘–-< ~
o -~ ~Graft
Theoretically, neural grafts could repair the damage caused by an injury to the spinal cord (A) in three ways: B) stimulate regrowth fromdamaged axons; C) stimulate new growth from uninjured axons; D) provide a relay that would transmit information through the site of injury.SOURCE: Office of Technology Assessment, 1990.

78 ● Neural Grafting: Repairing the Brain and Spinal Cord
since different types of injuries can result in a widerange of insults to the spinal cord (the damage donein an automobile collision may be quite differentfrom what occurs in a diving injury), no single modelcan be used to study spinal cord injury. Thedevelopment of analogous animal models is acrucial step in exploring the usefulness of neuralgrafts in spinal cord injury.
What Makes a Good Graft?
Several sources of grafting materials have beenexamined in animal experiments. These includeadult peripheral nerve and fetal CNS tissue, either inpieces or as cell suspensions. In general, autograftsand allografts have been used in these experiments.The use of tissue from other species has not beenwide ly examined; however, there is some evidencesuggesting that such tissue is not as suitable as theothers (142).
Peripheral Nerves—Nerves from the peripheralnervous system (PNS) are used to bridge a wound.They enable axons to cross the wound, reenter the farside of the spinal cord, and reinnervate their originaltargets. Over the past decade, some success has beenachieved in implanting segments of peripheralnerves into the spinal cords of animals with experi-mentally induced injuries; these grafts have survivedand become incorporated into the host spinal cord(126,130). The grafts support growth from thedamaged tissue, but the extent to which the elongat-ing axons can emerge from the graft and extend backinto the host tissue is extremely limited (34,126).
While the ability of peripheral nerve grafts toinduce growth in the injured spinal cord of experi-mental animals has been confined, the ability ofthese grafts to restore function has yet to bedemonstrated.
Fetal Spinal Cord Tissue—Another major sourceof grafting material in many animal experiments hasbeen fetal spinal cord tissue, usually from the samespecies. Given its ability to support growth, fetaltissue could act as a bridge across a wound or as arelay station between the severed axons and theirtarget sites on the other side of the wound byproviding a system of intervening neurons. Researchinto the use of this tissue does not have as long ahistory as that into peripheral nerve grafts. Experi-ments have shown that fetal tissue can create anenvironment that supports limited growth in thedamaged adult spinal cord. Also fetal tissue can
sometimes limit the scarring that occurs followingan injury (and that can act as a barrier to growth) (77)and prevent retrograde cell death (26).
One interesting model has demonstrated theeffectiveness of fetal spinal cord grafts in promotinggrowth at the boundary of the central and peripheralnervous systems. The fibers conveying sensoryinformation from the body (e.g., sensing when thebladder is full) into the spinal cord are called dorsalroots. These fibers travel in both the peripheral andcentral nervous systems and traverse the boundarybetween the CNS and PNS when they enter thespinal cord (see figure 3-5). In spinal cord injuriesthe dorsal roots are sometimes torn. When damaged,these fibers will regenerate in the periphery untilthey reach the PNS-CNS boundary at the spinal cordand then stop growing. This phenomenon clearlydemonstrates the ability of fibers to regrow in theperipheral but not in the central nervous system.Animal experiments have shown that if fetal spinalcord tissue is placed where the dorsal root enters thespinal cord, the severed root will continue to growinto the implant (133,144) and in some cases, to alimited extent, through it and into the host spinalcord (78). Fetal grafts, then, can support regenera-tion of these specialized peripheral-central fiberswithin the CNS and, to a certain degree, overcomethe barriers present at the PNS-CNS boundary.
Fetal spinal cord implants can also support growthof CNS axons in an animal that is still growing anddeveloping (24,25). In the newborn rat, axons fromthe brainstem are still growing into the spinal cord.If the spinal cord of a newborn rat is cut, the growingaxons cannot reach their targets, and in many casesthe neurons in the brain that send fibers into thespinal cord die. When fetal spinal cord tissue isplaced into wounds made in the spinal cords ofnewborn rats, the tissue supports the continueddevelopment of the growing spinal cord and pre-vents neuron death in the brain. Although thesestudies clearly show that fetal spinal cord grafts canfacilitate survival and regrowth of CNS axons in theimmature, growing spinal cord, they do not indicatewhether fetal spinal cord grafts would have anyeffect in the fully formed, adult spinal cord.
The ability of fetal spinal cord grafts to becomeintegrated into the adult spinal cord in rats has beendemonstrated (77,125). Fibers from the host spinalcord can grow into the grafts; however, the out-growth from fetal grafts, whether by spinal axons

Chapter 5--Applications of Neural Grafting Into the Brain and Spinal Cord . 79
Photo credit: B. Georgetown University
A cross-section through a rat spinal cord with a neural graftof rat fetal tissue.
transversing the graft or by neurons from within thegraft sending their axons into the host spinal cord, isvery limited. This again demonstrates the inabilityof axons to grow in the environment provided by themature CNS.
Neurotrophic and Neurotropic Factors—Themechanism by which peripheral nerves or fetaltissue induces growth of damaged axons in thespinal cord is thought to involve certain chemicalfactors (see box 3-A). Neural grafting into the spinalcord may owe its success thus far to the insertion oftissues that contain the correct mix of these chemi-cals at the injury site, establishing the properbiochemical environment to support regrowth of thedamaged axons and to allow reestablishment of lostsynaptic contacts. Providing the proper chemicalmessengers to turn the various components of theregeneration system on and off may be a crucialelement in the repair process. As more is learnedabout neurotrophic and neurotropic factors and theprocesses by which these substances regulategrowth in the nervous system, abetter understandingof exactly what is necessary to produce healing canbe determined.
Fetal Brain Tissue—Another grafting strategythat is being investigated involves the use of tissuefrom areas in the fetal brain that are known toregulate activity in the spinal cord. When the spinalcord is injured, descending fibers (originating in thebrain and containing a specific class of neurotrans-mitters called catecholamines) are damaged. It isknown that these fibers modulate the activity of localcenters in the spinal cord which control certain
Photo credit: B. Georgetown University
A rat being tested for the effects of a spinal cord injury. Therat has difficulty walking across the grid (arrow).
patterns of movement. There has been some investi-gation of whether these grafts could replace the lostcatecholamines and regulate activity in the affectedregions of the spinal cord. Grafts of fetal tissue fromthe relevant areas of the brain, implanted either assolid pieces (115,1 16) or in a cell suspension(18,123), become integrated into the host spinal cordand send fibers containing the catecholamines intothe surrounding tissue.
Is There Functional Recovery?
The most important question regarding thesetechniques as they relate to possible clinical applica-tions is whether there is any functional recoveryfrom an injury after grafting. None of the studiespreviously discussed examined whether the graftsrestored functions that were lost as a result of theinjury. Most research to date has been aimed atdetermining and establishing the conditions mostconducive to a successful implant and the degree towhich the graft can integrate with surrounding hosttissue. As a result, information regarding functionalrecovery following grafting is meager.
One study showed that grafting fetal rat spinalcord tissue into a small wound made in the spinalcords of adult rats decreased the difficulty inwalking that the animals normally would haveshown following such an injury (14). Significantly,

80 . Neural Grafting: Repairing the Brain and Spinal Cord
when the spinal cords of the animals that hadreceived grafts were examined, it was seen that therehad been very little regrowth of the severed fibers.The authors of the study concluded that the benefi-cial effects were probably” due to the growth-promoting factors in the grafts stimulating newgrowth from surviving neurons. They speculate thatthe surviving neurons assumed control of the lostfunctions by establishing new pathways that by-passed the injured area.
Injection of a cell suspension of rat fetal brainstem cells into the spinal cord can enhance legreflexes in rats in which catecholamine-containingneurons have been destroyed (27). The catecholam-ine-containing cells in the suspension integrate intothe spinal cord and establish new synaptic contactswith the spinal cord cells. It was hypothesized thatsome of the restoration of the leg reflexes was due tothe development of new catecholamine synapses,not regeneration of damaged cells.
In neither of these studies was the functionalrecovery observed thought to be due to regrowth ofthe damaged neuronal pathways at the site of thewound. In the first study, neurotrophic factors werethought to be involved, while in the second, theenhancement of reflexes was due partly to anincrease in catecholamine synapses and partly toother, unknown factors.
Some investigators have found evidence of recov-ery of function related to reconstruction of theneuronal pathways at the siteofawound(91). Graftsof fetal spinal cord tissue placed into the growingspinal cords of newborn rats lessen the deficits inwalking that occur when the spinal cords of theseanimals are injured. Since neural grafts in newbornsallow the growing spinal cord to assume a nearlynormal circuitry, it has been proposed that therecovery of function is due to this rewiring of thespinal cord at the site of the injury by the still-growing spinal cord.
Questions That Need To Be Answered
Neural grafts may be able to ameliorate deficitscaused by spinal cord injury; however, it isdifficult to predict if and when these technologieswill enter the clinical research arena. Animalexperimentation in this area is yielding a wealth ofinformation concerning basic biological mecha-nisms involved in growth and development of thenervous system, how it responds to injury, and the
feasibility of grafting tissues into the site of a spinalcord injury. A number of questions remain to beanswered before it can be known what clinicalapplication, if any, this research will have.
Can Grafted Biologic Material Exert a HealingEffect on the Damaged Spinal Cord?—Implicit inthis question is the notion that the spinal cord has nocapacity to heal-once it is damaged, it is damagedforever. Evidence to date shows that this is false. Thenormal response of the spinal cord to injury indicatesthat it has some regenerative capacity. If thiscapacity, coupled with the mechanisms controllinggrowth in the immature spinal cord, can be har-nessed and manipulated, then some form of healingcan be achieved.
Can the Healing Effects of a Graft RestoreFunction?--The ability of grafted material to be-come incorporated into the damaged spinal cordserves no clinical purpose in itself. The ultimateclinical goal of grafting is to restore function. Therequirements for restoration may differ from func-tion to function. For simple functions, such asawareness of when the bladder is full, it may bepossible to restore the necessary sensory input byreconnecting the dorsal root sensory nerves thatconvey this information to an intact area of the spinalcord. The graft would enable the sensory fibers tocross the PNS-CNS boundary and would allow themessage that the bladder is full to enter the nervoussystem. While this may not restore complete motorcontrol, the patient would be able to tell when it wastime to empty the bladder.
In the case of more complex functions under thecontrol of the spinal cord circuitry (blood pressureand temperature regulation, sexual reflex activity,bladder control, motor reflexes), reestablishment offunction may require bridging the wound to recon-nect the spinal cord control centers back into thereflex pathways or to reinstate the higher levelcontrol of these centers. The small degree ofoutgrowth from grafts that has been observed inmany experiments may be sufficient for bridgingspinal cord wounds. If the control centers them-selves are damaged, then grafts would have toprovide new cells to reform them. This wouldrequire a more complex interaction than just bridg-ing an injury site. Restoration of the motor andsensory deficits that result in paralysis would requirean even more comprehensive mending process, onethat would initiate regeneration or generation of

Chapter 5--Applications of Neural Grafting Into the Brain and Spinal Cord ● 81
pathways that could mediate the activity necessaryfor these functions.
The more complex and coordinated a function is,the more complex the type of repair needed toreinstate it. Exactly how much repair is necessary torestore a given function is not known. It is knownfrom animal models that, even if only a smallpercentage of fibers is spared at the time of injury,there can be marked recovery of function. It may bethat reestablishment of only a small proportion ofconnections, either by direct reconstruction or bystimulation of new pathways, may be sufficient forsignificant fictional recovery. In order to realizethis recovery, it may be necessary to follow thereconstructive surgery with extensive rehabilitativetherapy.
What Characteristics of the Graft Are Necessaryfor Functional Recovery?—The processes set inmotion by implantation of neural tissue must beunderstood before this technology can be used as atherapeutic tool. At the present time, grafting intothe spinal cord is analogous to inserting a “blackbox.’ Very little information is available as to whatcauses the observed morphological changes andfunctional effects. Is an integrated, solid piece oftissue necessary to supply the proper mixture ofneurotrophic factors to the right location and in theright form to induce growth? Or is it sufficient justto supply the growth-promoting factors alone? Is amixture of the two needed? Do these needs differdepending on what type of functional recovery isdesired? The answers to these questions are stillbeing sought.
What Are the Possible Unwanted Effects ofGrafting Into the Spinal Cord?—It is possible thatinserting tissue into the spinal cord or stimulatinggrowth from the damaged host tissue could causeabnormal pathways and connections to be formed.This could result in unwanted effects, notably thedevelopment of abnormal motor functions, such asmuscle spasticity and increased reflex actions, orpain or other discomforting sensations (e.g., burn-ing, tingling).
Brain Injury and Stroke
Since grafts may serve to replace lost ordamaged tissue or to stimulate growth fromdamaged areas, it is possible that neural graftscould restore functional losses caused by injuryto the brain. Animal experiments have demon-
Photo credit: R.A.E. Bakay, The Emory Clinic
Preparing a cell suspension for grafting.
strated that fetal tissue can survive and becomeincorporated into a wound made in the brain of anadult (e.g.,33,72,110). This includes tissue damagecaused by inducing a stroke in the experimentalanimal (usually rats) (104,109). The stroke is causedby clamping one of the vessels that supplies blood tothe brain, thus mimicking what happens in humanssuffering a stroke. The area of the brain that loses itsblood supply dies. When rat fetal tissue correspond-ing to the damaged area is placed in the wound, thegraft integrates into the host brain and becomesincorporated into the host blood supply. The cells inthe graft send signals like normal neurons, indicatingthat the graft is active. The grafts survive best whenthey are implanted at least 1 week after the stroke, aphenomenon that is observed when wounds aremade in either the brain or spinal cord. Neither thestroke studies nor the others previously mentionedexamined whether the grafts reversed any functionaldeficits caused by the wounds.
Studies of other kinds of brain injury in rats haveshown that implantation of rat fetal tissue intowounds made in the cerebral cortex can helpalleviate the deficits caused by the wounds(46,92,152). Grafting of fetal tissue into thesemodels results in functional improvement, but onlyif the tissue implanted is from regions of the fetalbrain that correspond to the areas destroyed in theadult.

82 . Neural Grafting: Repairing the Brain and Spinal Cord
The mechanism by which grafts exert their effectsin these animal models of brain injury is unclear.Recovery may be due either to integration of thegrafted material into the host brain or to effects notrelated to integration or even graft survival. It hasbeen observed that the beneficial effect occurs foronly a short time after implantation of the tissue (44)and that the same degree of functional recovery isseen whether a fetal graft, a suspension of glial cells,or a piece of sponge that has been sitting in thewound of another animal is placed into the wound(85). This indicates that part of the remedial effectmay result from the presence of neurotrophic factorsproduced when the wound was made or secreted bycells other than neurons contained in the graft. Thesefactors could stimulate growth from the injured hostbrain. Thus, both incorporation of the graft into thehost and the effects of growth-promoting factorscould play a role in recovery of function. Someinvestigators have stated:
It appears. . . that transplants can facilitate func-tional recovery by more than one mechanism,including promotion of survival and reactive synap-togenesis [synapse formation] of host neurons,stabilization of the damaged environment and re-placement of neurons (85).
The ability of grafts to reverse functional deficitscaused by brain injury is still unclear. If a functionaleffect can be produced, the underlying mechanism ofthat effect is uncertain and the requirements for thegrafted material are unknown. Additional basicresearch is needed to answer these questions andto define the ultimate role of grafts in braininjury.
EPILEPSYSome success has been achieved in using neural
grafts to block the occurrence of epileptic seizures ina very specific animal model of epilepsy called the“kindled” model. It is thought that the kindledmodel of epilepsy is analogous to temporal lobeepilepsy (68), which is the most frequent form of thedisease in adult humans. In this model, an area of thebrain called the locus ceruleus (LC), which inhibitsthe ability to induce seizures, is destroyed in rats.Investigators can therefore induce seizures in the
hippocampus of these animals more easily than innormal, intact rats.6 A graft of fetal rat LC tissueplaced in the hippocampus, however, can formconnections with the cells in the hippocampus andinhibit the induction of seizures (12,98). Thus, theLC graftS mimic, to a certain degree, the normalaction of the intact LC in this model. LC tissue graftshave also been shown to inhibit seizures in anotherrat model of epilepsy that uses a combination ofsurgery and drugs to induce seizures (28).
While these studies show that LC grafts caninhibit the induction of seizures in these models, therelationship to naturally occurring seizures in per-sons with epilepsy is unclear. There is no evidenceto date that LC grafts can inhibitor otherwise affectnaturally occurring seizures.
The ability of grafts of other types of fetal braintissue to suppress naturally occurring seizures hasbeen examined in rats that have a genetic predisposi-tion to seizures. The severity of seizures in these ratscan be decreased if either of the neurotransmittersnoradrenaline or gamma-aminobutyric acid(GABA) is injected into certain areas of the brain;however, grafts of tissue rich in these neurotransmit-ters, implanted into the proper areas of the brain, didnot appreciably reduce the intensity of the rats’seizures (138).
Experiments conducted to date indicate thatgrafts can affect the induction of seizures. How-ever, additional animal research is needed todetermine what role grafts could play in reducingnaturally occurring epileptic seizures.
NEUROENDOCRINE DEFICITSThe ability of grafts to supply chemicals makes
them well suited to reduce deficits caused by aloss or imbalance of normal hormone levels.Neurons in an area of the brain called the hypothala-mus regulate the release of hormones from thepituitary gland (which lies under the hypothalamus)into the bloodstream. In addition, some hormonesare made by neurons in the hypothalamus itself andare released directly into blood vessels. Once in theblood vessels, the hormones travel throughout thebody.
GSe~es ~ induc~ @ el~~~ly sthnu.lating a portion of the brain called the limbic syste~ which includes the hippocarnpus. The dech’idstimulation is given in small, progressive steps which make the Limbic system so sensitive tbat even a mild electrical shock will induce a generalizedseizure. Thus, the seizure is said to have been kindled. The locus cen,deus is thought to inhibit the kindling phenomenon by sending noradrenaline fibersto the hippocarnpus. Kindling takes place more quickly and easily when these fibers are destroyed.

Chapter 5--Applications of Neural Grafting Into the Brain and Spinal Cord ● 83
If the area of the hypothalamus that secretes thehormone vasopressin (VP) directly into the blood-stream is destroyed in rats, the resulting low levelsof VP cause water loss in the urine and producedehydration. The same phenomenon is observed ina mutant strain of rat that has a congenital absenceof VP-producing neurons. If VP-producing neuronsare grafted into either of these animal models, thegrafts become incorporated into the host and secreteVP into the circulatory system (59,105,136). Graftsof VP-producing cells can also ameliorate some ofthe deficits in fluid regulation seen in these animals(61,106). Finally, these grafts can prevent the deathof hypothalamic neurons that normally occurs whena wound is made, perhaps by the release ofgrowth-promoting factors (107).
Another model that has been used in this line ofresearch is a special strain of mice with a geneticabnormality that keeps them from producing thehormone GnRH (gonadotrophin-releasinghormone). GnRH, which is released from cells in thehypothalamus, causes cells in the pituitary gland torelease hormones that control sexual maturation.Mice of either sex with this genetic abnormalityhave immature reproductive organs and are sterile.The implantation of fetal grafts of hypothalamictissue from normal, GnRH-producing mice into thehypothalamus of adult mice with this dysfunctioncan correct many of the reproductive deficienciesthat occur in these animals (22,29,62-65,90). Thegrafts result in increased levels of pituitaryhormones, maturation of sexual organs, and initia-tion of sexual behavior.
Neural grafts have been shown to restore sexualpotency and sexual behavior in aged, impotent malerats (79). The sexual behavior of such rats before andafter fetal hypothalamic tissue was implanted intothe hypothalamus was observed. Before the im-plants, the animals did not engage in sexual behaviorwhen exposed to receptive females. After the grafts,the sexual behavior of most of the rats was restored,resulting in increased sexual activity and impregna-tion of the females.
The ability of neural grafts to reverse deficits andimbalances in hormone levels due to neurologicaldamage or abnormalities has been repeatedly shownin a number of animal models. Since analogousclinical conditions in humans are rare, and whenthey occur are treated with drugs, the ultimate
Anatomy in Basic Neuroohemistry,4th G. Siegel, B. R. and P. (New York,
NY: Raven Press, 29.
A photograph through a microscope showing a Schwanncell (N) and the it produces (black ring)
surrounding an axon (A).
role of neural grafts in human clinical neuroen-docrine conditions is yet to be elucidated.
DEMYELINATING DISORDERS:MULTIPLE SCLEROSIS
Demyelinating disorders disrupt nervous systemactivity by causing a breakdown in the insulatingsheath that surrounds many axons. Loss of themyelin sheath interferes with the normal transmis-sion of signals between neurons, causing messagesto travel more slowly than normal. Specialized glialcells (oligodendrocytes in the CNS, Schwann cellsin the PNS) produce the myelin covering of neurons.Within the CNS, demyelinating diseases attackeither the oligodendrocytes or the myelin theyproduce.
A number of disorders can affect myelin in theCNS. While most are rare, one, multiple sclerosis(MS), is more common. MS destroys patches of

84 . Neural Grafting: Repairing the Brain and Spinal Cord
myelin in an erratic and random fashion throughoutthe CNS. The cause of MS is unknown.
Demyelination can also occur in certain types ofspinal cord injuries. Injuries caused by a compres-sive force on the spinal cord often result in an areaof demyelinated axons surrounding a core of deadtissue (149). The ability of grafts to restore themyelin covering of the appropriate axons could aidin the recovery of lost functions.
The therapeutic strategy underlying the use ofneural grafts in patients with MS or otherdemyelinating conditions would be to provide asource of myelin that could become incorporatedinto the affected area and restore the lost myelinsheath. Any graft tied at replenishing lost myelinwould have to include either oligodendrocytes orSchwann cells. Since these cells, when implantedinto the CNS, can migrate some distance from thesite of insertion, it is thought that they may be usablein treating disorders that result in patchy areas ofdemyelinated axons.
Over the past decade, animal experiments haveshown that it is possible to replace lost myelin byinjecting the appropriate cells into regions in whichexperimentally induced demyelinating lesions havebeen produced. This has been demonstrated usingsuspensions of Schwann cells from peripheralnerves (21,22,39,76), cell suspensions of CNS tissue(23), and fragments of CNS tissue (73,74). Addi-tional animal experimentation is needed to deter-mine whether these grafting procedures canrestore functional deficits caused by demyelina-tion. Also, it is unknown whether implanted myelin-producing cells would be susceptible to the underly-ing disease process that caused the original demyeli-nation.
SUMMARY AND CONCLUSIONSThe possible therapeutic uses of neural grafting
into the brain and spinal cord are varied and diverse,encompassing a wide range of neurological deficits.Of these, the application of neural grafting inpersons with Parkinson’s disease is the most ad-vanced. But in Parkinson’s disease, as well as allother applications, no definitive statement about theactual usefulness of neural grafting as a therapeuticprocedure can be made at this time. The data fromthe basic research that has been conducted thus farprovide tantalizing hints of the potential usefulnessof neural grafting procedures, but additional animal
experimentation needs to be conducted to clarifythat potential. To increase the applicability of animaldata to human disorders, animal models of thevarious neurological disorders under study need tobe developed. Neural grafting holds the promise ofnew therapeutic interventions for neurological disor-ders, but a final determination of its usefulness mustawait the accumulation of more information aboutthe mechanisms underlying neurological diseaseand injury, graft functions, and how those functionsrelate to various neurological disorders.
1.
2.
3.
4.
5.
6.
7.
8.
9.
CHAPTER 5 REFERENCESAllen, G. S., Burns, R. S., lldipan, N.B., et al.,‘ ‘Adrenal Medullary Transplantation to the CaudateNucleus in Parkinson’s Disease,” Archives ofNeurology 46:487-497, 1989.Apuzzo, M.L.J., Neal, J.H., Waters, C.H., et al.,‘‘Utilization of Unilateral and Bilateral Stereotacti-cally Placed Adrenomedullary-Striatal Autograflsin Parkinsonian Humans: Rationale, Techniques,and Observations, ’ Neurosurgery 26:746-757,1990.Arbuthnott, G., Dunnett, S.B., and MacIx@ N.,‘ ‘Electrophysiological Properties of Single Units inDopamine-Rich Mesencephalic Transplants in RatBrain,” Neuroscience Letters 57:205-210, 1985.Arendt, T, Allen, Y, Sinden, J., et al., “Choliner-gic-Rich Brain Transplants Reverse Alcohol-Induced Memory Deficits,” Nature 332:448450,1988.Backlund, E. O., Granberg, P. O., Hamberger, B., etal., “Transplantation of Adrenal Medullary Tissueto Striatum in Parkinsonism, First Clinical Trials,”Journal of Neurosurgery 62:169-173, 1985.Bakay, R.A.E., Allen, G. S., Apuzzo, M.L.J., et al.,“Preliminary Report on Adrenal Medullary Graft-ing From the American Association of NeurologicalSurgeons GRAFT Project,” Progress in BrainResearch, in press.Bakay, R.A.E., Barrow, D. I., Fiandaca, M. S., et al.,“Biochemical and Behavioral Correction of MFI’PParkinson-Like Syndrome by Fetal CellTransplantation,’ Annals of the New York Academyof Sciences 495:623-638, 1987.Bakay, R.A.E., Fiandaca, M. S., Barrow, D.L., et al.,“Preliminary Report on the Use of Fetal TissueTransplantation To Correct ~P-Induced Parkin-son-like Syndrome in Primates, ’ AppZiedNeurophysiolology 48:358-361, 1985.Bakay, R.A.E., and Herring, C.J., “Central NervousSystem Grafting in the Treatment of Parkinson-ism, ” Stereotactic and Functional Neurosurgery53:1-20, 1989.

Chapter 5-applications of Neural Grafting Into the Brain and Spinal Cord ● 85
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
Bankiewicz, K. S., Plunkett, R.J., Jacobowitz, D.M.,et al., “TheEffect of Fetal Mesencephalon Implantson Primate MPTP-Induced Parkinsonism,’ Journalof Neurosurgery 72:231-244, 1990.Bankiewicz, K.S., Plunkett, R.J., Kopin, I.J., et al.,“Transient Behavioral Recovery in Hemiparkin-sonian Primates After Adrenal Medullary Allo-grafts,” Progress in Brain Research, vol. 78,Transplantation Into the Mammalian CNS, D.M.Gash and J.R. Sladek, Jr. (eds.) (Amsterdam:Elsevier Science Publishers, 1988).Barry, D.I., Kilmadze, I., Brundin, P., et al.,“Grafted Noradrenergic Neurons Suppress SeizureDevelopment in Kindling-Induced Epilepsy,’ Pro-ceedings of the National Aca&my of Sciences,U.SA. 84:8712-8715, 1987.Bernstein, J.J., “Successful Spinal Cord Regenera-tion: Known Biological Strategies,’ Current Issuesin Neural Regeneration Research, P. Reier, R.Bunge, and F. Seil (eds.) (New York, NY: Alan R.Liss, 1988).Bernstein, J.J., and Goldberg, W.J., “Fetal SpinalCord Homografts Ameliorate the Severity of h-sion-induced Hind Limb Behavioral Deficits,”Experimental Neurology 98:633-644, 1987.Bing, G., Netter, M.F.D., Hansen, J.T., et al.,“Comparison of Adrenal Medullary, Carotid Bodyand PC12 Cell Grafts in 6-OHDA Lesioned Rats,”Brain Research Bulletin 20:399-406, 1988.Bing, G., Netter, M.F.D., Hansen, J.T., et al.,“Enhanced Survival and Function of Grafted Adre-nal Medullary Cells When Cografted With TrophicProducing Arnitotic C6 Glioma Cells,” Neuros-cience, in press.Bjorklund, A., Dunnett, S.B., Stenevi, U., et al.,“Reinnervation of the Denervated Striatum bySubstantial Nigra Transplants: Functional Conse-quences as Revealed by Pharmacological and Sen-sorimotor Testing,” Brain Research 199:307-333,1980.Bjorklund, A., Nomes, H., and Gage, F.H., “CellSuspension Grafts of Noradrenergic Imcus Coerul-eus Neurons in Rat Hippocampus and Spinal Cord:Reinnervation and Transmitter lhrnover,” Neuro-science 18:685-698, 1986.Bjorklund, A., and Stenevi, U., “Reconstruction ofthe Nigrostriatal Doparnine Pathway by Intracere-bral Nigral Transplants, “ Brain Research 177:555-560,1979.Bjorklund, A., Stenevi, U., Schmidt, R.H., et al.,“Intracerebral Grafting of Neuronal Cell Suspen-sions, II: Survival and Growth of Nigral CellSuspensions Implanted in Different Brain Sites,”Acta Physiologic Scandinavia 522(supp.):9-18,1983.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
Blakemore, W.F., “Remyelination of CNS Axonsby Schwann Cells Transplanted From the SciaticNerve,” Nature 266:68-69, 1977.Blakemore, W.F., and Crang, A.J., “The Use ofCultured Autologous Schwann Cells to Remyelin-ate Areas of Persistent Demyelination in the CentralNervous System,” Journal of Neurological Sci-ences 70:207-223, 1985.Blakemore, W.F., and Crang, A.J., “ExtensiveOligodendrocyte Remyelination Following Injec-tion of Cultured Central Nervous System Cells IntoDemyelinating Lesions in the Adult Central Nerv-ous System,” Developmental Neuroscience 10:1-11, 1988.Bregman, B. S., “Development of Serotonin Im-munoreactivity in the Rat Spinal Cord and ItsPlasticity After Neonatal Spinal Cord Lesions,”Developmental Brain Research 431:245-263, 1987.Bregman, B. S., “Spinal Cord Transplants Permitthe Growth of Serotonergic Axons Across the Siteof Neonatal Spinal Cord Transection,” Develop-mental Brain Research 431:265-279, 1987.Bregman, B. S., and Reier, P.J., “Neural TissueTransplants Rescue Axotomized Rubrospinal CellsFrom Retrograde Death,” Journal of ComparativeNeurology 24486-95, 1986.Buchanan, J.T., and Nomes, H.O., ‘‘Transplants ofEmbryonic Brainstem Containing the ImcusCoeruleus Into Spinal Cord Enhance the HindlimbFlexion Reflex in Adults,” Brain Research381:225-236, 1986.Buzsaki, G., Ponomareff, G., Bayardo, F., et al.,“Suppression and Induction of Epileptic Activityby Neuronal Grafts,” Proceedings of the NationalAcademy of Sciences, U.SA. 85:9327-9330, 1988.Charlton, H.M., ‘‘Neural Grafts and Restoration ofPituitary and Gonadal Function in Hypogonadal(HPG) Mice,” Annals of Endocrinology 48:378-384,1987.Collier, T.J., Gash, D.M., and Sladek, J.R., Jr.,“Transplantation of Norepinephrine Neurons IntoAged Rats Improves Performance of a LearnedTask,” Brain Research 448:77-87, 1988.Collier, TJ., Redmond, D.E., Jr., Roth, R.H., et al.,“Reversal of Experimental Parkinsonism in Afri-can Green Monkeys Following Fetal DopamineNeuron Transplantation,” Progress in Parkz”nson’sResearch, F.F. Hefti and W.J. Weiner (eds.) (NewYork NY: Plenum Press, 1989).Daniloff, J.K., Bodony, R.P., hw, W.C., et al.,“Cross-Species Septal Transplants: Restoration ofConditioned Learning Behavior,” Brain Research346:176-180, 1985.Das, G.D., Hallas, B.H., and Das, K.G., “Tmnsplan-tation of Brain Tissue in the Brain of the Rat, I:Growth Characteristics of Cortical Transplants

86 ● Neural Grafting: Repairing the Brain and Spinal Cord
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
From Embryos of Different Ages,” Acta Anatomica158:135-145, 1980.David, S., and Aguayo, A.J., “Axonal ElongationInto Peripheral Nervous System ‘Bridges’ AfterCentral Nervous System Injury in Adult Rats,”Science 214:932-933, 1981.Deckel, A.W., Moran, T.H., Coyle, J.Y., et al.,“Anatomical predictors of Behavioral RecoveryFollowing Fetal Transplants,” Brain Research 365:249-258, 1986.Deckel, A.W., Robinson, R.G., Coyle, J.T., et al.,‘‘Reversal of I.mng-Term Imcomotor Abnormalitiesin the Kainic Acid Model of Huntington’s Diseaseby 18-Day Fetal Striatal Implants,” EuropeanJournal of Pharmacology 93:287-288, 1983.Demierre, B., Martinou, J.-C., and Kate, A. C.,“Embryonic Motoneurons Grafted Into the AdultCNS Can Differentiate and Migrate,” Brain Re-search 510:355-359, 1990.Drucker-Colin, R., Madrazo, I., Ostros&Solis, F.,et al., “AdrenalMedullaryT issue Transplants in theCaudate Nucleus of Parkinson’s Patients,” Pro-gress in Brain Research, vol. 78, TransplantationInto the Mammalian CNS, D.M. Gash and J.R.Sladek, Jr. (eds.) (Amsterdam: Elsevier SciencePublishers, 1988).Duncan, I.D., Aguayo, A.J., Bunge, R.P., et al.,“Transplantation of Rat Schwann Cells Grown inTissue Culture Into the Mouse Spinal Cord,”Journal of Neurological Science 49:241-252, 1981.Dunnett, S.B., Bjorklund, A., Schmidt, R.H., et al.,“Intracerebral Grafting of Neuronal Cell Suspen-sions, IV: Behavioral Recovery in Rats WithUnilateral 6-OHDA I.xxions Following Im-plantation of Nigral Cell Suspensions in DifferentForebrain Sites,” Acta Physiologic Scan&”navia522(supp.):29-37, 1983.Dunnett, S. B., Bjorklund, A., Stenevi, U., et al.,“Grafts of Embryonic Substantial Nigra Reinner-vating the Ventrolateral Striatum AmeliorateSensorimotor Impairments and Akinesia in RatsWith 6-OHDA bsions of the Nigrostriatal Path-way,” Brain Research 229:209-217, 1981.Dunnett, S.B., Hernandez,T.D., Summerfield, A., etal., “Graft-Derived Recovery From 6-OHDA Le-sions: Specificity of Ventral Mesencephalic GraftTissues,” Experimental Brain Research 71:411-424, 1988.Dunnett, S.B., Low, W. C., Iverson, S.D., et al.,‘‘SeptalTransplants Restore Maze barning in RatsWith Fornix-Fimbria ksion,” Brain Research251:335-348, 1982.Dunnett, S.B., Ryan, C.N., I_evin, P.D., et al.,“Functional Consequences of Embryonic Neo-cortex Transplanted to Rats With Prefrontal Cortex
45.
46.
47.
48.
49
50.
51.
52.
53.
54.
55.
Lesions,” Behavioral Neuroscience 101:489-503,1987.Emfors, P., Ebendal, T., Olson, L., et al., “A CellLine Producing Recombinant Nerve Growth FactorEvokes Growth Responses in Intrinsic and GraftedCentral Cholinergic Neurons,” Proceedings of theNational Academy of Sciences, U.S.A. 86:4756-4760,1989.Escobar, M., Femandez, J., Guevara-Agular, R., etal., “Fetal Brain Grafts Induce Recovery of Learn-ing Deficits and Connectivity in Rats With Gusta-tory Neocortex bsion,” Brain Research 478:368-374, 1989.Fiandaca, M. S., Kordower, J.H., Hansen, J.11, et al.,“Adrenal MeduWry Autografts Into the BasalGanglia of Cebus Monkeys: Injury-RelatedRegeneration,” Experimental Neurology 102:76-91,1988.Fine, A., Dunnett, S.B., Bjorklund, A., et al.,“Cholinergic Ventral Forebrain Grafts Into theNeocortex Improve Passive Avoidance Memory ina Rat Model of Alzheimer’s Disease,’ Proceedingsof the National Academy of Sciences, U.S.A.82:5227-5230, 1985.Fine, A., Hunt, S. P., Oertel, W. H., et al.,‘‘Transplantation of Embryonic Marmoset Dopam-inergic Neurons to the Corpus Striatum of Marmo-sets Rendered Parkinsonian by l-Methyl+Phenyl-l,2,3,6-Tetrahydropyridine,” Progress in BrainResearch 78:479-489, 1988.Freed, C.P., Breeze, R.E., Rosenberg, N.L., et al.,“Transplantation of Human Fetal Doparnine Cellsfor Parkinson’s Disease: Results at 1 Year,” Ar-chives of Neurology 47:505-512, 1990.Freed, W.J., Cannon-Spoor, H.E., and Krauthamer,E., “Factors Influencing the Efficacy of AdrenalMedulla and Embryonic Substantial Nigra Grafts,”Neural Grafi”ng in the Mammalian CNS, A. Bj&k-lund and U. Stenevi (eds.) (Amsterdam: ElsevierScience Publishers, 1985).Freed, W.J., Cannon-Spoor, H.E., and Krauthamer,E., “~trastiata.1 Adrenal Medulla Grafts in Rats,Long-Term Survival and Behavioral Effects,”Journal of Neurosurgery 65:664-670, 1986.Freed, W.J., Morihisa, J.M,, Spoor, E., et al.,“Transplanted Adrenal Chromaffin Cells in RatBrain Reduce Lesion-Induced Rotational Behav-ior,” Nature 292:351-352, 1981.Freed, W.J., Perlow, M.J., Karoum, F., et al.,“Restoration of Dopaminergic Function by Graft-ing of Fetal Substantial Nigra to the CaudateNucleus: Long-Term Behavioral, Biochemical, andHistochemical Studies,” Annals of Neurology8:510-519, 1980.Freund, T.F., Bolam, J.P., Bjorklund, A., et al.,‘‘Efferent Synaptic Connections of Grafted Dopam-

Chapter 5--Applications of Neural Grafting Into the Brain and Spinal Cord ● 87
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
inergic Neurons Reinnervating the Host Neostri-aturn: A Tyrosine Hydroxylase Irnrnunocytochemi-cal Study,” Journal of Neuroscience 5:603-616,1985.Gage, F.H., and Bjorklund, A., “Cholinergic SeptalGrafts Into the Hippocampa.1 Formation ImproveSpatial Ixarning and Memory in Aged Rats byAtropine-Sensitive Mechanism, ” Journal ofNeuroscience 6:2837-2847, 1986.Gage, F.H., Bjorklund, A., Stenevi, U., et al.,“Intra-Hippocampal Septal Grafts AmeliorateLearning Impairments in Aged Rats,” Science 225:533-536, 1984.Gage, F.H., Wollf, J.A., Rosenberg, M. B., et al.,“Implantation of Genetically Engineered Cells tothe Brain,” Progress in Brain Research 78:651-658,1988.Gash, D. M., and Sladek, J.R., Jr., “Functional andNon-Functional Transplants: Studies With GraftedHypothalamic and Preoptic Neurons,” Trends inNeuroscience 76:391-394, 1984.Gash, D. M., and Sladek, J. R., Jr., “NeuralTransplantation: Problems and Prospects-WhereDo We Go From Here?’ Mayo Clinic Proceedings64:363-367, 1989.Gash, D.M., Sladek, J.R., Jr., and Sladek, C.D.,“Functional Development of Grafted VasopressinNeurons,” Science 210:1367-1369, 1980.Gibson, M.J., Charlton, H.M., Perlow, E.A., et al.,“PreopticAreaBrain Grafts in Hypogonadal (HPG)Female Mice Abolish Effects of Congenital Hy-pothalamic Gonadotropin-Releasing Hormone(GnRH) Deficiency, “ Endocrinology 114:949-951,1984.Gibson, M.J., Krieger, D.T., and Charlton, H.M., etal., “Mating and Pregnancy Can Occur in Geneti-cally Hypogonadal Mice With Preoptic Area BrainGrafts,” Science 225:949-951, 1984.Gibson, M.J., Moscovitz, H. C., Kokoris, G.J., et al.,“Female Sexual Behavior in Hypogonadal MiceWith GnRH-Containing Brain Grafts,” Hormonesand Behavior 21:211-222, 1987.Gibson, M.J., Silverman, A.J., Kokoris, G.J., et al.,‘‘GnRH Cell Brain Grafts. Correction ofHypogonadism in Mutant Mice,” Annals of theNew York Academy of Sciences 495:296-305, 1988.Giordano, M., Houser, S.H., and Sanberg, P.R.,“Intraparenchymal Fetal Striatal Transplants andRecovery in Kainic Acid hsioned Rats,” BrainResearch 446:183-188, 1988.Girault, J.A., Raisman-Vozari, R., Agid, Y., et al.,“Striata.1 Phosphoproteins in Parkinson’s Diseaseand Progressive Supranuclear Palsy,” Proceedingsof the National Academy of Sciences, U.S.A.86:2493-2497, 1989.
68.
69.
70.
71.
72.
73.
74.
75.
76.
77.
78.
79.
Girgis, M., “Kindling as a Model of LirnbicEpilepsy,” Neuroscience 6:1695-1706, 1981.Goetz, C.G., Olanow, C.W., Keller, W.C., et al.,“Multicenter Study of Autologous Adrenal Medul-lary Transplantation to the Corpus Striatum inPatients With Advanced Parkinson’s Disease,”New England Journal of Medicine 320:337-341,1989.Goetz, C. G., Stebbins, G.T., Klawans, H.L., et al.,“United Parkinson Foundation Neurotransplanta-tion Registry Multicenter United States and CanadaDatabase Presurgical and 12-Month Followup,”Proceedings of the Third International Congress ofNeurotransplantation: Cambridge (Amsterdam:Elsevier Science Publishers, 1989).Goetz, C.G., Tanner, C.M., Pem, M.D., et al.,‘‘Adrenal Medullary Transplant to the Striatum ofPatients With Advanced Parkinson’s Disease: 1Year Motor and Psychomotor Data,” NeuroZogy40:273-276, 1990.Gonzalez, M.F., and Sharp, F.R., “Fetal FrontalCortex Transplanted to Injured Motor/Sensory Cor-tex of Adult Rats,” Journal of Neuroscience7:2991-3001, 1987.Gout, O., Gansmuller, A., Baumann, N., et al.,‘‘Remyelination by Transplanted Oligodendrocytesof a Demyelinated bsion in the Spinal Cord of theAdult Shiverer Mouse,” Neuroscience titters 87:195-199, 1988.Gumpel, M., Baumann, N., Raoul, M., et al.,“Survival and Differentiation of OligodendrocytesFrom Neural Tissue Transplanted in New-BornMouse Brain,” Neuroscience Letters 37:307-311,1983.Hansen, J.T., Kordower, J.H., Fiandaca, M. S., et al.,“Adrenal Medullary Autografts Into the BasalGanglia of Cebus Monkeys: Graft Viability andFine Structure,” Experimental Neurology 102:65-75, 1988.Harrison, B.M., “Remyelination by Cells Intro-duced Into a Stable Demyelinating Ixxion in theCentral Nervous System,’ Journal of NeurologicalScience 46:63-81, 1980.Houle, J.D., and Reier, P. J., “Transplantation ofFetal Spinal Cord Tissue Into the ChronicallyInjured Adult Rat Spinal Cord,” Journal of Com-parative Neurology 269:535-547, 1988.Houle, J.D., and Reier, P.J., “Regrowth of CaIci-tonin Gene-Related Peptide (CGRP) Immunoreac-tive Axons From the Chronically Injured Rat SpinalCord Into Fetal Spinal Cord Tissue Transplants,”Neuroscience titters 103:253-258, 1989.Huang, H. H., Kissane, J. Q., and Hawarylewicz,E.J., “Restoration of Sexual Function and Fertilityby Fetal Hypothalamic Transplants in Impotent

88 ● Neural Grafting: Repairing the Brain and Spinal Cord
Aged Male Rats,” Neurobiology of Aging 8:465-472,1987,
80. Hurtig, H., Joyce, J., Sladek, J.R., Jr., et al.,“Postmortem Analysis of Adrenal-Medulla-to-Caudate Autograft in a Patient With Parkinson’sDisease,” Annals of Neurology 25:607-614, 1989.
81. Isacson, O., Brund.in, P., andKelly, P., “FunctionalNeuronal Replacement by Grafted Striatal Neuronsin the Ibotenic Acid-Lesioned Rat Striatum,” Na-ture 311:458460, 1984.
82. Isacson, O., Dunnett, S.B., and Bjorklund, A.,“Graft Induced Behavioral Recovery in an AnimalModel of Huntington’s Disease,” Proceedings ofthe National Academy of Sciences, U.S.A. 83:2728-2732, 1986.
83. Itakura, T., Kamei, I., Nakai, K., et al., “Autotrans-plantation of the Superior Cervical Ganglion Intothe Brain,” Journal of Neurosurgery 68:955-959,1988.
84. Jiao, S., Ding, Y, Zhang, W., et al., letter, NewEngland Journal of Medicine 321:325, 1989
85. Kess~J.P., Nieto-Sampedro, M., Globus, J., etal.,“Transplants of Purified Astrocytes PromoteBehavioral Recovery After Frontal Cortex Abla-tion,” Experimental Neurology 92:377-390, 1986.
86. Kirnble, D.P., Bremiller, R., and Stichrod, G.,“Fetal Brain Implants Improve Maze Performancein HippocampaH.esioned Rats,” Brain Research363:358-363, 1986.
87. Keller, W. C., Morantz, R., Veter-Overfield, B., etal., “Autologous Adrenal Medullary Transplant inProgressive Supranuclear Palsy,” Neurology39:1066-1068, 1989.
88. Kordower, J.H., Fiandaca, M. S., Netter, M.F.D., etal., “Peripheral Nerve Provides NGF-like TrophicSupport for Grafted Rhesus Adrenal ChromaffinCells,” Journal of Neurosurgery, in press.
89. Kordower, J.H., Netter, M.F., and Gash, D.M.,“Neuroblastoma Cells in Neural Transplants: ANeuroanatomical and Behavioral Analysis,” BrainResearch 417:85-98, 1987.
90. Krieger, D.T., Perlow, M.J., Gibson, M.J., et al.,“Brain Grafts Reverse Hypogonadism of Gona-dotropin-Releasing Hormone Deficiency,’ Nature298:468-471, 1982.
91. Kunkel-Bagden, E., and Bregman, B. S., “SpinalCord Transplants Enhance the Development andRecovery of Reflex and Locomotor Function AfterNeonatal Spinal Cord Lesions,” ExperimentalBrain Research, in press.
92. Labbe, R., Firl, A., Mufson, E.J., etal., “FetalB rainTransplant Reduction of Cognitive Deficit in RatsWith Frontal Cortex Imion,” Science 221:470-472, 1983.
93. Landau, W.M., “Clinical Neuromythology VII—Artificial Intelligence: The Brain Transplant Cure
for Parkinsonism,” Neurology 40:733-740, 1990.94. Lieberman, A.N., Ransohoff, J., Berczeller, P., et
al., “AdrenalMedullary Transplants as a Treatmentfor Advanced Parkinson’s Disease,” Acta NeuroZ-ogica Scati”navia 126:189-196, 1989.
95. Liebennan, A.N., Ransohoff, J., and Koslow, M.,“Adrenal Medullary to Caudate Nucleus Trans-plant as an Effective Treatment for AdvancedParkinson’s Disease,” Neurology 38(supp. 1):142,1988.
96. Lindvall, O., “Transplantation Into the HumanBrain: Present Status and Future Possibilities,”Journal of Neurology, Neurosurgery and Psychia-try supp.:39-54, 1989.
97. Lindvall, O., Backlund, E.O., and Farde, L.,“Transplantation in Parkinson’s Disease: TwoCases of Adrenal Medullary Grafts to the Pu-tamen,” Annals of Neurology 22:457-468, 1987.
98. Lindvall, O., Barry, D.L, Kikvadze, L, et al., “Intra-cerebral Grafting of Fetal Noradrenergic ImcusCoeruleus Neurons: Evidence for Seizure Suppres-sion in the Kindling Model of Epilepsy,” Progressin Brain Research 78:79-86, 1988.
99. Lindvall, O., Brundin, P., Widner, H., eta.l., “Graflsof Fetal Dopamine Neurons Survive and ImproveMotor Function in Parkinson’s Disease,” Science247:574-577, 1990.
100. Lindvall, O., Rechncrona, S., Brundin, P., et al.,‘‘Human Fetal Dopamine Neurons Grafted Ihto theStnatum in Two Patients With Severe Parkinson’sDisease: A Detailed Account of Methodology anda 6-Month Followup,” Archives of Neurology46:615-631, 1989.
101. McAllister, J.P., Kaplan, L., and Reynolds, M.A.,‘‘Morphology and Connectivity of Fetal NeostriatalTissue Transplanted Into the Neostriatum of AdultHost,” Anatomical Record, 1984, p. 107A.
102. Madrazo, I., Drucker-Colin, R., Diaz, V., et al.,“Open Microsurgical Autograft of Adrenal Me-dulla to the Right Caudate Nucleus in Two PatientsWith Intractable Parkinson’s Disease,” New Eng-land Journal of Medicine 316:831-834, 1987.
103. Mahalik, TJ., Finger, TE., Stromberg, I., et al.,“Substantial Nigra Transplants Into DenervatedStriatum of the Rat: Ultrastructure of Graft and HostInterconnections,” Journal of Comparative Neu-rology 240:60-70, 1985.
104. Mampalam, T.J., Gonzalez, M. F., and Weinstein,P., “Neuronal Changes in Fetal Cortex Trans-planted to Ischemic Adult Rat Cortex,” JournaZ ofNeurosurgery 69:904-912, 1988.
105. Marciano, F.F., and Gash, D.M., “Structural andFunctional Relationships of Grafted VasopressinNeurons,” Brain Research 370:338-342, 1986.
106. Marciano, F.F., Gash, D.M., and Sladek, J.R., Jr.,“Transplanted Vasopressin Neurons: Structural

Chapter 5--Applications of Neural Grafting Into the Brain and Spinal Cord ● 89
107.
108.
109.
110.
111.
112.
113.
114.
115.
116.
117.
and Functional Correlates,” Neural Grafting in theMammalian CNS, A. Bjorklund and U. Stenevi(eds.) (Amsterdam: Elsevier Science Publishers,1985).Marciano, F.F., Wiegard, S.J., Sladek, J. R., Jr., etal., ‘Fetal Hypothalamic Transplants Promote Sur-vival and Functional Regeneration of AxotomizedAdult Supraoptic Magnocellular Neurons,” BrainResearch 483:135-142, 1989.Morihisa, J.M., Nakamura, R.K., Freed, W.J., et al.,“Adrenal Medulla Grafts Survive and ExhibitCatecholarnine-Specific Fluorescence in the Pri-mate Brain,’ Experimental Neurology 84:643-653,1984.Mudrick, L.A., Leung, P.P., Baimbndge, K.G., etal., “Neuronal Transplants Used in the Repair ofAcute Ischernic Injury in the Central NervousSystem,” Progress in Brain Research 78:87-93,1988.Mufson, E.J., Labbe, R., and Stein, D. G., “Mor-phologic Features of Embryonic Neocortex Graftsin Adult Rats Following Frontal Cortical Abla-tion,” Brain Research 401:162-167, 1987.Nash, D.R., Kaplan, S.M., Norman, A.B., et al.,“An Evaluation of the Possible Protective Effectsof Neonatal Striatal Transplants on Kainic Acid-Induced bsions,” paper presented at the annualmeeting of the Society for Neuroscience, Toronto,NOV. 18, 1988.Nishino, H., One, T., Shibata, R., et al., “AdrenalMedullary Cells Transmute Into DopaminergicNeurons in Dopamine-Depleted Rat Caudate andAmeliorate Motor Disturbances,” Brain Research445:325-337, 1988.Norman, A. B., Calderon, S.F., Giordano, M., et al.,“Striatal Tissue Transplants Attenuate Apomor-phine-Induced Rotational Behavior in Rats WithUnilateral Kainic Acid Lesions,” NeuropharmacoZ-0~ 27:333-336, 1988.Norman, A. B., Lehman, M.N., and Sanberg, P.R.,‘‘Functional Effects of Fetid Striatal Transplants,”Brain Research Bulletin 22:163-172, 1989.Nornes, H., Bjorklund, A., and Stenevi, U., “Rein-nervation of the Denervated Adult Spinal Cord ofRats by Intraspinal Transplants of Embryonic BrainStem Neurons,” Cell and Tissue Research 230:15-35, 1983.Nygren, L. G., Olson, L., and Seiger, A., “Monoam-inergic Reinnervation of the Transected Spinal Cordby Homologous Fetal Brain Grafts,” Brain Re-search 129:227-235, 1977.Olanow, C.W., Cahill, D., and Cox, C., “Autolo-gous Transplantation of Adrenal Medulla to Cau-date Nucleus in Parkinson’s Disease,” Neurology38(supp. 1):142, 1988.
118.
119.
120.
121.
122.
123.
124.
125.
126.
127.
128.
129.
130.
131.
Penn, R.D., Goetz, C.G., Tanner, C.M., et al., “TheAdrenal Medullary Transplant Operation for Park-inson’s Disease: Clinical Observations in FivePatients,” Neurosurgery 22:999-1004, 1988.Perlow, M.J., Freed, W.J., Hoffer, B.J., et al.,“Brain Grafts Reduce Motor Abnormalities Pro-duced by Destruction of the Nigrostriatal DoparnineSystem, “ Science 204%43-647, 1979.Peterson, D.I., Price, M.L., and Small, C. S., “Au-topsy Findings in a Patient That Had an Adrenal-to-Brain Transplant for Parkinson’s Disease,’ NeuroZ-Ogy 39:235-238, 1989.Pezzoli, G., Fahn, S., Dwork, A., et al., “Non-Chromaffin Tissue Plus Nerve Growth FactorReduces Experimental Parkinsonism in AgedRats,” Brain Research 459:398-403, 1988.Price, D.L., Troncoso, J. C., Whitehouse, P.J., et al.,“Approaches to Neurodegenerative Diseases,”Diseases of the Nervous System: Clinical Neuro-biology, A.K. Asbury, G.M. McKhann, and W.I.McDonald (eds.) (Philadelphia, PA: W.B. Saun-ders, 1986).Privat, A., Mansour, H., Pavy, A., et al., “Trans-plantation of Dissociated Fetal Serotonin NeuronsInto the Transected Spinal Cord of Adult Rats,”Neuroscience Letters 66:61-66, 1986.Redmond, D.E., Slade~ J.R., Jr., Roth, R.H., et al.,‘‘Fetal Neuronal Grafts in Monkeys Given Methyl-phenyl-tetrahydropyridine,” Lancet 1:1125-1127,1986.Reier, P.J., Bregman, B. S., and Wujek, J.R., “In-traspinal Transplantation of Embryonic Spinal CordTissue in Neonatal and Adult Rats,” Journal ofComparative Neurology 247:275-296, 1986.Richardson, P. M., McGuiness, U. M., and Aguayo,A.J., “PeripheralNerve Autografts to the Rat SpinalCord: Studies With Axonal Tracing Methods,”Brain Research 237:147-162, 1982.Rosenberg, M. B., Friedmam, T., Robertson, R. C.,et al., “Grafting Genetically Modified Cells to theDarnaged Brain: Restorative Effects of NGF Ex-pression,” Science 242:1575-1578, 1988.Rutherford, A., Garcia-Munoz, M., Dunnett, S. B., etal., “Electrophysiological Demonstration of HostCortical Inputs to Striatal Grafts,” NeuroscienceLetters 83:275-281, 1987.Sanberg, P.R., Henault, M.A., and Deckel, A.W.,“Locomotor Hyperactivity: Effects of MultipleStriatal Transplants in an Animal Model of Hunt-ington’s Disease,’ Pharmacology, Biochemistry,and Behavior 25:297-300, 1986.Sceats, D.J., Friedman, W.A., Sypert, G.W., et al.,‘‘Regeneration in Peripheral Nerve Grafts to the CatSpinal Cord, “ Brain Research 362:149-156, 1986.Schmidt, R.H., Ingvar, M., Lindvall, O., et al.,“Functional Activity of Substantial Nigra Grafts

90 ● Neural Grafting: Repairing the Brain and Spinal Cord
132.
133.
134.
135.
136.
137.
138.
139.
140.
141.
142.
Reinnervating the Striatum: Neuro-transmitter Me-tabolism and C-2-deoxy-D-Glucose Autoradio-graphy,” Journal of Neurochemistry 38:737-748,1982.Science News, “Experimental Cell Grafts for Hunt-ington’s,” Science N~s 133:268, 1988.Siegal, J.D., Kliot, M., Smith, G.M., et al., “InducedRegeneration of Cur Dorsal Root Fibers Into AdultRat Spinal Cord,” paper presented at the annualmeeting of the Society for Neuroscience, Toronto,NOV. 18, 1988.Sieradzan, K., and Vrbova, G., “Replacement ofMissing Motoneurons by Embryonic Grafts in theRat Spinal Cord,’ Neuroscience 31:1 15-136,1989.Sladek, J. R., Jr., Redmond, D.E., Jr., Collier, T. J., etal., “Fetal Dopamine Neural Grafts: ExtendedReversal of Methyl-phenyl-tetrahydropyridine-Induced Parkinsonism in Monkeys,” Progress inBrain Research 78:497-506, 1988.Sladek, J.R., Jr., Scholer, M.F.D., Netter, D. M., etal., “Immuno-histochemical Analysis of Vaso-pressin Neurons Transplanted Into the BrattleboroRat,’ Annals of the New York Academy of Sciences394:102-114, 1982.Sladek, J.R., Jr., and Sholson, I., “Neural Trans-plantation: A Call for Patience Rather Than Pa-tients,” Science 240:1386-1388, 1988.Stevens, J.R., Phillips, I., and Freed, W.J., “Cere-bralTransplants for Seizures: preliminary Results,”Epilepsia 29:731-737, 1988.Strecker, R.E., Sharp, T, Brundin, P.; et al.,‘‘Autoregulation of Dopamine Release and Metab-olism by Intrastriatal Nigral Grafts as Revealed byIntracerebral Dialysis,’ Neuroscience 22:169-178,1987.Stromberg, I., Herrera-Marschitz, M., Ungerstedt,U., et al., “Chronic Implants of Chromaffin TissueInto the Doparnine-Denervated St.riatum: Effects ofNGF on Graft Survival, Fiber Outgrowth andRotational Behavior,” Experimental Brain Re-search 60:335-349, 1985.Stromberg, I., Johnson, S., Hoffer, B., et al.,‘‘Reinnervation of Doparnine-Denervated Striatumby Substantial Nigra Transplants: Immunohisto-chemica.1 and Electrophysiological Correlates, ”Neuroscience 14:981-990, 1985.Tang, Y, and Bernstein, J. J., “Rapid Rejection ofFetal Chick Neocortical Xenografts Into the Spinal
143.
144.
145.
146.
147.
148.
149.
150.
151.
152.
153.
Cord of Adult Rats,” Neuroscience Letters 36:389-392, 1986.Tanner, C.M., Watts, R.L., Bakay, R.A.R., et al.,letter, New England Journal of Medicine 321:325,1989.Tessler, A., Himes, B.T., Houle, J., et al., “Regener-ation of Adult Dorsal Roots Into Transplants ofEmbryonic Spinal Cord,” Journal of ComparativeNeurology 270:537-548, 1988.‘IMipan, N., Huang, S., Whetsell, W.O., et al.,“Neonatal Striatal Grafts Prevent Lethal SyndromeProduced by Bilateral Intra-Striatal Injection ofKainic Acid,” Brain Research 377:163-167, 1986.Walker, P.D., and McAllister, J.P., “Minimal Con-nectivity Between Neostriatal Transplants and theHost Brain,” Brain Research 425:34-44, 1987.Walsh, J.P., Zhou, F. C., Hull, C.D., et al., “Physio-logical and Morphological Characterization of Stri-atal Neurons Transplanted Into the Adult RatStriatum,” Synapse 2:37-44, 1988.Watts, R.L., Balmy, R.A.E., Iuvone, P.M., et al.,“Autologous Adrenal-Caudate Transplantation inPatients With Parkinson’s Disease,” Neurology38(supp. 1):143, 1988.Waxman, S.G., “Demyelination in Spinal CordInjuries,” Journal of Neurological Sciences 91:1-14, 1989.Weiner, S.A., Dunnett, S. B., Salamone, J.D., et al.,“Transplantation of Embryonic Ventral ForebrainGrafts to the Neocortex of Rats With BilateralUsions of Nucleus Basalis Magnocellularis Ame-liorates a Ision-Induced Deficit in Spatial Mem-ory,” Brain Research 463:192-197, 1988.Wolff, J.A., Fisher, L. J., Xu, L.T., et al., “GraftingFibroblasts Genetically Modified To Produce L-dopa in a Rat Model of Parkinson’s Disease,”Proceedings of the National Aca&my of Sciences,U.SJL 86:9011-9014, 1989.Yirmiya, R., Zhou, F. C., and Holder, M.D., “PartialRecovery of Gustatory Function After Neural Tis-sue Transplantation to the Lesioned GustatoryNeocortex,” Brain Research Bulletin 20:619-625,1988.Zetterstrom, T, Brundin, P., Gage, F.H., et al., “InVivo Measurement of Spontaneous Release Metab-olism of Dopamine From Intrastriatal Nigral GraflsUsing Intracerebral Dialysis,” Brain Research 362:344-349, 1986.

Chapter 6Relevant Neurological Disorders

CONTENTSPage
NEURODEGENERATIVE DISORDERS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . 94Parkinson’s Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94Huntington’s Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97Alzheimer’s Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ● . . . . . . . . . . . . . . . . . . . . . . . . . . 98Motor Neuron Disease: Amyotrophic Lateral Sclerosis . . . . . . . . . . . . . . . . . . . . . . . . . . . 99
CENTRAL NERVOUS SYSTEM INJURY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100Spinal Cord Injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100Brain Injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101Stroke . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
EPILEPSY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104DEMYELINATING DISORDERS: MULTIPLE SCLEROSIS . . . . . . . . . . . . . . . . . . s . . . 105SUMMARY AND CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 107CHAPTER 6 REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 107
BoxesBox Page6-A. Cycads and Amyotrophic Lateral Sclerosis, Parkinson’s Disease,
and Dementia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 966-B. Neurological Disorders and the Veteran . . . . . . . . . . . * . . . . . . *,, *, . . . + * * .+*,**..* 102
FiguresFigure Page6-1. National Institutes of Health 1989 Estimates of Costs of
Neurological Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 946-2. Types of Head Injury Causing Death . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1036-3. Geographical Differences in Death Rate Due to Multiple Sclerosis . . . . . . . . . . . . . . 106
TablesTable Page6-1. Incidence of Neurological Disorders in the United States . . . . . . . . . . . . . . . . . . . . . . 936-2. Prevalence of Neurological Disorders in the United States . . . . . . . . . . . . . . . . . . . . . 936-3. Drugs Used for the Treatment of Parkinson’s Disease . . . . . . . . . . . . . . . . . . . . . . . . . . 976-4. Drugs Being Developed for the Treatment of Alzheimer’s Disease . . . . . . . . . . . . . . 996-5. Department of Veterans Affairs, Spinal Cord Injury Centers, Fiscal Year 1989 . . 1026-6. Types of Epileptic Seizures ... **. *,, .*. **. ... .,*. ... ... ... ... ..*. .**. +. ***,*4 105

Chapter 6
Relevant Neurological Disorders
Reports of neural grafts relieving symptoms ofParkinson’s disease have captured the attention ofthe medical profession and public policymakers.Much of their excitement derives from the somberfact that Parkinson’s disease is a progressivelydebilitating illness, the symptoms of which can beonly imperfectly controlled. In fact, many centralnervous system (CNS) injuries and diseases aremarked by severe, unrelenting symptoms that defycure and exact a great toll in personal suffering andsocietal costs. Since current animal researchintimates that neural grafting may be applicableto the study and treatment of diverse neurologicaldisorders, this technology may ultimately have asignificant impact on medicine and society.
Exactly how far-reaching a therapeutic interven-tion is neural grafting likely to become? Its use as amedical treatment is most advanced in Parkinson’sdisease, but even there its ultimate therapeutic valueis far from established. The study of neural graftingfor the treatment of other neurological disorders isfaced with important barriers, including inadequateanimal models and incomplete knowledge about thebasic mechanisms underlying many CNS diseasesand injuries. (See ch. 5 for details.) Despite thesereasons for caution, it is notable that animal researchemploying neural grafting has in many cases im-proved structural or functional deficits in the CNS.These results are preliminary and their ultimateapplication is unknown, but the amount and diver-sity of neural grafting research suggests wide-ranging potential applications.
Neurological disorders are a significant cause ofillness, disability, and death in the United States.They cost, by conservative estimates from theNational Institutes of Health, more than $100 billionper year in medical expenses and lost income (tables6-1 and 6-2; figure 6-l). Not all neurologicaldisorders are amenable to treatment by neuralgrafting. In this chapter, the Office of TechnologyAssessment (OTA) identifies those disorders thatmay one day be treatable with grafting technology.The
●
criteria for selection were:
current understanding of the nature and cause ofthe condition suggests that neural grafting maybe a beneficial treatment approach, and
Table 6-1—incidence of Neurological Disordersin the United States
Neurological disorder Incidence
Stroke . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 500,000Brain injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 500,000Alzheimer’s disease . . . . . . . . . . . . . . . . . . . . . . 130,000Epilepsy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 125,000Parkinson’s disease . . . . . . . . . . . . . . . . . . . . . . 50,000Spinal cord injury . . . . . . . . . . . . . . . . . . . . . . . . 10,000Multiple sclerosis . . . . . . . . . . . . . . . . . . . . . . . . 8,800Amyotrophic lateral sclerosis . . . . . . . . . . . . . . . 5,000Huntington’s disease . . . . . . . . . . . . . . . . . . . . . 850
NOTE: Incidence is defined as the number of new cases of a diseaseestimated to occur each year in the United States. Sources forestimates are the same as those in the text.
SOURCE: Office of Technology Assessment, 1990.
Table 6-2—Prevalence of Neurological Disordersin the United States
Neurological disorder Prevalence
Alzheimer’s disease . . . . . . . . . . . . . . . .Stroke . . . . . . . . . . . . . . . . . . . . . . . . . . . .Epilepsy . . . . . . . . . . . . . . . . . . . . . . . . . .Parkinson’s disease . . . . . . . . . . . . . . . .Multiple sclerosis . . . . . . . . . . . . . . . . . . .Spinal cord injury . . . . . . . . . . . . . . . . . . .Brain injury. . . . . . . . . . . . . . . . . . . . . . . .Huntington’s disease . . . . . . . . . . . . . . . .Amyotrophic lateral sclerosis . . . . . . . . .
1 to 5 million2.8 million1.5 million
500,000 to 650,000250,000180,000
70,000 to 90,000’25,00015,000
a Estimate of persons permanently disabled from head injury.
NOTE: Prevalence is defined as the total number of cases of a diseaseestimated to be in existence in the United States at any given time.Sources for estimates are the same as those in the text.
SOURCE: Office of Technology Assessment, 1990.
● results from animal experiments indicate thepossibility of therapeutic value.
Although it is reasonable to underscore thepotential of neural grafting for the treatment ofpatients suffering from the neurological disorderschosen, neural grafting as a general therapeuticapproach is in the very early stages of develop-ment, and predictions of its ultimate utility arespeculative at best. Furthermore, only a subset ofpatients suffering from a particular disorder maybenefit from neural grafting. For example, in experi-ments, grafting with adrenal medulla tissue appearsto be more successful if the tissue is derived from ayounger rather than an older animal (15). A briefreview of the current understanding of, treatment
-93–

94 ● Neural Grafting: Repairing the Brain and Spinal Cord
Figure 8-l-National Institutes of Health 1989Estimates of Costs of Neurological Disorders
Alzheimer’s disease
Stroke
CNS injury
Epilepsy
Movement disorders.
Multiple sclerosis
Amyotrophic lateralsclerosis ~ -–– - — ~–- .- .—. -7. – ~
o 10 20 30 40 50 60Billions of dollars
*Parkinson’s and Huntington’s diseases.NOTE: Costs are per year, including medical care, lost income, etc.SOURCE: National Institutes of Health, 1990.
approaches to, and epidemiological data1 on each ofthe designated disorders is presented, exemplifyingsome of the factors that drive neural graftingresearch. (A detailed description of the neuralgrafting research related to each of the listeddisorders is presented in ch. 5.)
The epidemiology of the neurological disordersincluded in this chapter warrants special discussion.In some instances, epidemiological data are inade-quate, despite the extensive national health andmortality data collected by the Federal Government(16). This lack of data may reflect several factors.Some disorders are difficult to diagnose. Some arerare and thus elude medical data collection systems.Epidemiological studies can also be confounded byambiguous criteria for diagnosing a disorder orvariations in health care among communities. Manystudies were conducted using populations that arenot necessarily representative of the United States;for example, information has been derived fromlocal community studies or surveys in which institu-tionalized persons were not included. Despite theseconcerns and others, the epidemiological data usedin this chapter testify to the significant impact theseneurological disorders have on society.
NEURODEGENERATIVEDISORDERS
Parkinson’s Disease
In 1817 Dr. James Parkinson described sixpatients with marked shaking and impaired mobility(46). He called this condition “shaking palsy.”Other physicians noted similar cases and named thedisease after Parkinson. The predominant pathologi-cal change observed in persons with Parkinson’sdisease is death of nerve cells in a region of the braincalled the substantial nigra. In the healthy brain,nerve cells in the substantial nigra communicate withnerve cells located in the striatum, using thechemical transmitter dopamine. Death of substantialnigra nerve cells and the resulting dopamine deple-tion lead to the symptoms characteristic of thedisease--tremor, slowing of movement, and rigid-ity.
Parkinsonism represents not just one disease, buta collection of illnesses. Some manifestations ofparkinsonism are secondary to known causes (e.g.,drugs and other toxic chemicals, rare brain tumors,and recurrent head injuries, such as those sustainedby professional boxers) (32). The most commonform of parkinsonism, however, is that marked by aprogressive loss of nerve cells in the substantial nigradue to unknown causes. This subgroup of parkinson-ism is called idiopathic Parkinson’s disease, or justParkinson’s disease, and it accounts for 80 to 90percent of parkinsonism cases. In the followingsection, when discussing the scope of parkinsonism,all forms of the disease will be considered; whenexamining potential causes of the disorder, the focuswill be on Parkinson’s disease.
While it is not known what causes the nerve celldeath in Parkinson’s disease, there is now considera-ble evidence that the disease process begins anumber of years before the clinical features becomevisible (33, 39, 41). Nerve cell death in the substantialnigra proceeds slowly and does not produce anysymptoms until a critical number of cells (80 percentor more) has died.
The onset of symptoms of Parkinson’s disease isso imperceptible that patients usually require assis-
l~pi&fiO1@,~ &b are presented as incidence, the number of new cmes W eurring during a specified period of time (usually 1 year) within adesignated are% incidence rate, incidenee per unit of Population prevalence, the total number of cases in existence at a speci.fkd time in a designatedarea; pnwaZence rate, prevalence per unit of populatio~ and mortality rate, the number of deaths attributable to a disorder during a speci.fhxl period oftime within a designated area per unit of population.

Chapter 6--Relevant Neurological Disorders ● 95
Photo credit: B. Pansky, Medical College of Ohio
Right: picture of the brain of a Parkinson’s disease patient showing significant reduction in nervecells as compared to the adjacent picture, showing the same region of the brain in a
normal
tance from friends and relatives to recall its firstmanifestation. Parkinson’s disease is extremely rarein persons under age 20, but the incidence andprevalence rates increase with age. In a study of 806Parkinson’s patients, the median age of onset wasfound to be 63 (i.e., half the patients had symptomsby their 63rd birthday), and the majority (56 percent)of patients evidenced symptoms before age 65. Themean duration of illness (onset to death) varied from8 to 14 years (40).
The most crucial element in determiningg the causeof Parkinson’s disease is identifying the source ofthe nerve cell damage. Although the disease is morecommon among older persons, there is little evi-dence that it is related to arteriosclerosis, tumor,brain injury, or nutritional problems often associatedwith aging. Other possible causes may be geneticfactors, altered immune system function, or infec-tion. In general, however, there is a lack of evidencethat any of these factors plays a role in Parkinson’sdisease.
Since it is known that certain toxic substances inthe environment can produce parkinsonism, there isgreat interest in examining the role of exogenoustoxins in Parkinson’s disease (box 6-A). Because of
individual.
the ubiquitous nature of Parkinson’s disease, manysubstances have been suggested as possible causa-tive agents. For example, nine metals-aluminum,arsenic, calcium, copper, iron, manganese, magne-sium, mercury, and zinc-have been correlated withParkinson’s disease (10). As yet, however, metaltoxicity as a cause of Parkinson’s disease does nothave a sound scientific basis.
In 1979, it was discovered that a syntheticnarcotic, l-methyl-4-phenyl-l,2,3,6-tetrahydropyri-dine (MPTP), can cause parkinsonism in humans (9)(see box 5-A). Subsequent observations suggestedthat Parkinson’s disease may be caused by a toxicsubstance related to MPTP (14). Drugs that inhibitMPTP’s toxic effect are currently under investiga-tion for treating Parkinson’s disease.
The standard treatment for Parkinson’s diseasehas been drug therapy aimed at increasing dopaminein the brain (50). Dopamine is not readily absorbedinto the brain, so administration of dopamine itselfis not efficacious. However, levodopa (L-dopa), theprecursor of dopamine, is a very effective treatment.When L-dopa is taken, it is absorbed into the brainfrom the blood and is converted into dopamine bythe remaining substantial nigra nerve cells, amelio-

96 Neural Grafting: Repairing the Brain and Spinal Cord
Box 6-A--Cycads and Amyotrophic Lateral Sclerosis, Parkinson’s Disease, and Dementia
Amyotrophic lateral sclerosis-Parkinson’s disease-dementia (ALS-P-D) syndrome has been known among theChamorro natives of the Mariana Islands in the Pacific Ocean for more than 150 years and came to the attentionof U.S. scientists soon after World War II. It is characterized by parkinsonism and prominent dementia, oramyotrophic lateral sclerosis (Lou Gehrig’s disease), or a combination of the three. Gradually, the incidence of thedisorder declined, and that decline coincided with a change in lifestyle of the native population, including reducedingestion of the seed from the endogenous plant known as Cycas circinalis. The cycad seed is known to containhighly potent neurotoxic substances. During World War II, cycad seeds were the major source of flour and medicinein certain parts of the Mariana Islands. The subsequent high incidence of ALS-P-D syndrome has been attributedto the increased use of cycad for food or medicine.
Monkeys fed the amino acid derived from the cycad seed (known as Beta-N-methyl amino-L-alanine, BMAA)develop motor neuron and parkinsonian symptoms and behavioral changes. Another neurotoxic syndrome in man,lathyrism, is known to be caused by an amino acid that is structurally similar to BMAA. These observations arestrong indications that a cycad neurotoxic substance acting like BMAA is the cause of ALS-P-D syndrome,Although this syndrome is distinct from Parkinson’s disease, studies of ALS-P-D syndrome provide valuable cluesto the etiology of amyotrophic lateral sclerosis, Parkinson’s disease, and Alzheimer’s disease.
SOURCES: P.S. Spencer, P.B. Nunn, and J. Hugon, “Guam Amyotrophic Lateral Sclerosis-Parkinsonism-Dementia Linked to a Plant ExcitantNeurotoxin,” Science 237: 517-522, 1987; J.C. Steele and T. Guzman, “ O b s e r v a t i o n s A b o u t Amyotrophic Lateral Sclerosis and
the Parkinso nism-Dementia Complex of Guam With Regard to Epidemiology and Etiology, ” Canadian Journal of NeurologicalSciences 14:358-362, 1987.
rating many of the motor symptoms of the disease. delayed the onset of serious disability and treatment,Usually L-dopa is given in conjunction with anotherdrug, carbidopa, which increases the amount ofL-dopa that can enter the brain, thus making the drugeven more effective. Unfortunately L-dopa, thestandard therapy for Parkinson’s disease, doesnot have any effect on the progression of thedisease, and nerve cell death continues unabated.As a result, in most patients L-dopa therapy losesits effectiveness as the disease progresses, andsymptoms become more and more difficult tocontrol.
Other drugs are used to treat persons withParkinson’s disease as well (table 6-3). All of thesework by counteracting the effects of decreaseddopamine in the striatum (50). Like L-dopa, thesedrugs lessen the symptoms of Parkinson’s diseasewithout affecting the underlying mechanism thatcauses the nerve cell death. They, too, tend to losetheir effectiveness as the disease progresses. Neuralgrafting as a treatment in Parkinson’s disease iscurrently under investigation in animals andhumans. Strategies for the use of neural graftinginclude the replacement of degenerating neuronsand the provision of dopamine.
Recently, a drug that actually slows the progres-sion of Parkinson’s disease has been developed (47).In a group of patients with early, untreated Parkin-son’s disease, administration of the drug deprenyl
compared to a group of patients who did not receivethe drug. This finding is not only extremely impor-tant for the treatment of Parkinson’s disease, it alsorepresents the first time a drug has been shown tohave a retarding effect on any neurodegenerativedisorder. As more is learned about how deprenylworks, it may shed new light on the mechanisms thatproduce other progressive degenerative disorderssuch as Alzheimer’s disease and Huntington’sdisease.
Currently, data on the national prevalence andincidence of parkinsonism are limited. Availabledata are based on community studies and research-ers’ estimates. The reported prevalence rates ofparkinsonism vary widely, from 4 to 187 cases per100,000 persons (40). This vast difference undoubt-edly reflects the variability in the completeness ofcase findings and the varying standards of healthcare indifferent areas, which determine survival andhence prevalence rate. The number of persons withparkinsonism in the United States has beenestimated at 500,000 to 650,000 (37).
The reported annual incidence rates of parkinson-ism also vary widely, from 5 to 24 cases per 100,000persons (40). Data collected from a survey con-ducted in Rochester, Minnesota, indicated that theannual incidence rate of parkinsonism is 20.5 casesper 100,000 population (adjusted to the 1970 U.S.

Chapter &Relevant Neurological Disorders ● 97
Table 6-3-Drugs Used for the Treatment ofParkinson’s Disease
Drug Action
Levodopa (L-dopa) . . . . . Increases dopamine levelsAmantadine . . . . . . . . . . . Increases release of dopamineBromocriptine . . . . . . . . . Stimulates dopamine receptorsTrihexyphenidyl . . . . . . . . Decreases acetylcholine activityBenztropine . . . . . . . . . . . Decreases acetylcholine activityDeprenyl . . . . . . . . . . . . . . Slows progression of cell deatha
aUnder investigation.SOURCE: Office of T*nology Assessment, 1990.
population) (51). Study of the same communityindicates that Parkinson’s disease accounts for 85.5percent of all cases of parkinsonism and thatdrug-induced cases (due to antipsychotic drugs usedto treat certain mental disorders, and generallyreversible) are now the second most common formof parkinsonism (51). The number of personsdiagnosed with parkinsonism before age 50 seems tobe increasing (2).
Huntington's Disease
Huntington's disease (HD) is an incurable,inherited disorder. Onset is commonly between theages of 30 and 50 (7). It is heralded by personalityand behavioral changes and involuntary movements(12). As HD progresses, the involuntary movements,consisting of uncontrollable writhing and jerking, orchorea, become more frequent and exaggerated,eventually rendering the patient bedridden andincapable of per-forming everyday activities. Somepatients, especially with the juvenile form of thedisease, also experience slowed movement andrigidity. As the disease progresses, the patient’smemory and mental abilities decline. Patients maybecome emotionally deranged; all eventually lapseinto dementia. HD leads to a steady decline in health,and death usually occurs 14 to 19 years after onsetof the disease.
The brains of persons with HD appear shrunken atautopsy (12). There is extensive nerve cell death incertain regions of the brain, including the striatumand the cerebral cortex. The abnormal movementassociated with HD is attributed to loss of nerve cellsin the striatum; dementia is attributed to loss in otherregions. The nerve cell loss associated with HDresults in a profound decrease in certain brainchemicals, including GABA (gamma-aminobutyricacid) and acetylcholine. How nerve cell death isproduced in HD remains a mystery.
A single defective gene appears to be responsiblefor HD (29). Because HD is an autosomal dominantcondition, any child of a parent with HD has a 50percent risk of inheriting the gene and succumbingto the disease. Advances in molecular genetics havepinpointed the location of the HD gene to chromo-some 4 (23, 29). Although the gene itself has notbeen identified, knowledge of its location hasimportant practical implications-a person or fetuscarrying the HD gene may be identified prior toonset of the disease. Researchers are attempting todetermine the gene’s function and eventually todevelop an effective treatment for HD.
There is at present no cure for HD (12).Attempts to replace deficient brain chemicals havebeen unsuccessful. Treatment is aimed at minimiz-ing the abnormal movements and mental problemsassociated with the disease. In their normal state,nerve cells that degenerate in HD may suppress theactivity of other, dopamine-producing nerve cells.Destruction of the former may lead to excessive anduncontrolled dopamine production, causing the in-voluntary movements typical of HD. Drug therapyaimed at blocking the action of dopamine is em-ployed to suppress the involuntary movements. Thistherapy produces undesirable side-effects, however,including sedation, depression, and severe limitationof movement. Drugs are also used to help control themental changes associated with HD. None of thesedrug therapies is adequate for the treatment of HD,and none prevents the progression of the disease.Since the symptoms of HD are produced by thedeath of specific groups of nerve cells, the limitedanimal research into the treatment of HD byneural grafting is based on the possibility ofreplacing degenerated cells or replenishing cer-tain brain chemicals.
Huntington’s disease is a relatively rare disorder.Epidemiological assessment is complicated by thefact that it is extremely rare in many regions butunusually frequent in others (37). Its worldwideprevalence rate is estimated to be five cases per100,000 persons (37). Its incidence rate is estimatedto be 3.4 cases per 1 million persons each year. Incertain regions of the world, notably the LakeMaracaibo region of Venezuela, the prevalence rateis extremely high, affecting up to 700 people per100,000 persons. Between 1968 and 1974, it wasestimated that HD accounted for 1.15 deaths per 1million persons in the United States per year (37).Although there are no reliable national data on

9/I ● Neural Grafting: Repairing the Brain and Spinal Cord
the prevalence of HD, it is estimated that 25,000Americans now suffer from this disorder (7, 29,52). Another 125,000 Americans are thought to be atrisk of developing the disease.
Alzheimer's Disease
Alzheimer’s disease (AD) is an incurable disorderthat robs its victims of their intellect and eventuallyof their physical health. Its onset is insidious.Typically, its first symptom-loss of memory forrecent events—is ignored or attributed to othercauses, such as stress, a drug side-effect, or thegeneral forgetfulness of old age. As the diseaseprogresses, memory loss worsens and can no longerbe ignored or dismissed. A cascade of other behav-ioral symptoms ensues, including confusion, irrita-bility, combativeness, restlessness, and fearfulness.Problems with language occur, as do difficulties inexecuting purposeful movements. Ultimately, theAD patient will be completely helpless—incontinent, bedridden, and unable to speak or eat.Postmortem examination of the brains of ADpatients reveals a loss of nerve cells in specificregions, including the basal forebrain, amygdala,hippocampus, locus ceruleus, and parts of thecerebral cortex. The nerve cell loss is associated withreduced quantities of certain brain chemicals, partic-ularly acetylcholine. Reduced noradrenaline andother chemicals in the brain have also been reported(8, 19, 24).
At the present time, a definitive diagnosis of ADis achieved only after the patient’s death; it is basedon the presence of abnormal structures in the brain:neurofibrillary tangles and neuritic plaques. Neu-rofibrillary tangles are accumulations of twistedprotein filaments inside nerve cells, and neuriticplaques are abnormal clusters of degenerating nervecell fibers, other brain cells, and amyloid protein (seelater discussion) found in the areas between neurons(49). More recent developments have linked thedetection of a protein, called Alzheimer’s disease-associated protein (ADAP), in postmortem braintissue with AD (17). Chemical tests for ADAP maylead to the development of a diagnostic test for AD.
The cause or causes of Alzheimer’s disease arenot known. Genetic effects, environmental effects,and disrupted chemical processes in the brain haveall been examined as possible factors in the disease(30, 62, 69). Recently, attention has been focused ona protein called beta-amyloid, which is a key
~oto credit: R. Rest&, The Mind (New York NY: Bantam Books, 1988)
Picture of microscopic changes, including neurofibrillarytangles and neuritic plaques, that occur in the brain when
afflicted with Alzheimer’s disease.
component of neuritic plaques (56). It may be thatsome defect in beta-amyloid synthesis leads to theformation of neuritic plaques and nerve cell degener-ation seen in AD (58). Aluminum or aluminumbinding is also under consideration as a possiblecause of AD (69). Growth factors, specifically nervegrowth factor (NGF), may also play a role in thedevelopment of AD. NGF has been shown to protectacetylcholine-producing nerve cells from experi-mentally induced damage in laboratory animals (27,67).
Pharmacological treatment of AD has met withlittle success, and there is no cure for AD (table6-4). As discussed earlier, AD patients suffer from adeficit of several brain chemicals, particularly ace-tylcholine. Since acetylcholine has been demon-strated to be involved in learning and memory,restoration or augmentation of acetylcholine in ADvictims may lead to improvements in their memoryand other cognitive abilities. In addition, drugs thatact on other chemical systems implicated in AD mayalso lead to fictional improvements. None of thesedrugs would have an effect on the cause of thedisease, and none would halt its progression. As aresult of this fact and the lack of uniform success inalleviating AD symptoms with such drugs, othertreatments for AD are being explored.
As mentioned earlier, NGF has been shown toprevent the degeneration of acetylcholine-producingnerve cells after injury, and it appears to improvememory in a rat model of cognitive impairment withage (13). These and other findings have led research-

Chapter 6--Relevant Neurological Disorders ● 99
Table 6-4-Drugs Being Developed for the Treatmentof Alzheimer’s Disease
Drug Action
Velnacrine maleate . . . . .Physostigmine . . . . . . . . .Tetrahydroaminoacridine
(THA) . . . . . . . . . . . . . .Suronacrine maleate. . . .Milacemide . . . . . . . . . . . .Captopril . . . . . . . . . . . . . .Acetyl-L-carnitine . . . . . .
Nimodipine . . . . . . . . . . . .Idebenone . . . . . . . . . . . .
Inhibits cholinesteraseInhibits cholinesterase
Inhibits cholinesteraseAmplifies noradrenaline actionStimulates glycine activityInhibits angiotensin activityEnhances activity of nerve growth
factorBlocks calcium channelEnhances cerebral metabolism
SOURCE: J.F. Beary, “Alzheimer’s Medicines: Sixteen Medicines inTesting,” American Journal of Alzheimer’s Care and RelatedDisorders & Research (January/February): 4-6, 1990.
ers to suggest that administration of NGF may slowthe progression of the major symptoms of AD andcould be efficacious in treating persons with thedisease (48). The potential use of neural grafts totreat AD has been explored mainly in experi-ments involving rodents and is based largely onthe ability of neural grafts to provide growthfactors, such as NGF.
The collection of accurate statistics on theincidence and prevalence of AD is hampered bythe inability to diagnose AD definitively during apatient’s lifetime. AD is given as the clinicaldiagnosis when other causes of a progressive demen-tia have been eliminated (e.g., cardiovascular dis-ease, stroke, head injury, or adverse reaction todrugs). Although improvements have been made inthe ability to diagnose AD clinically (30), it remainsextremely difficult to diagnose the disease defini-tively early in its course.
Alzheimer’s disease is the primary cause ofdementia in the United States. Few national statisticsare available on the prevalence and incidence of ADper se; most available data relate to dementingdisorders as a whole. A 1987 OTA report (62)estimated that the prevalence of severe dementiain the United States is 1.5 million persons. Mild ormoderate dementia was estimated to occur inanother 1 to 5 million persons. AD is estimated toaccount for about 66 percent of all cases of dementia.
Much of the incidence and prevalence dataavailable specifically for AD are based on studiesthat differ from each other in diagnostic criteria andprocedures and in the populations analyzed. Inci-
dence rates per year have been estimated at 123.3cases per 100,000 persons over the age 29; theage-adjusted rate was calculated to be 51.6 personsper 100,000 persons per year (54). Prevalence ratesof AD have been estimated from recent communitystudies; AD was found among 2.0 to 10.3 percent ofthose over the age of 65, with an estimated 3 to 5million persons in the United States afflicted withAD (11, 31). Estimates of the total yearly costs ofAD range from $30 billion to $80 billion (28, 62).
Motor Neuron Disease: AmyotrophicLateral Sclerosis
Motor neuron diseases destroy the nerve cells thatcontrol muscle movement, resulting in impairedmuscle function. The most well-known motor neu-ron disease is amyotrophic lateral sclerosis (ALS),or Lou Gehrig’s disease. ALS is an incurableneurological disease. The average age of patients atthe time of diagnosis is 56 (44). Initial symptoms caninclude difficulty in performing fine tasks, weak-ened leg muscles, or difficulty in speech andswallowing. There is progressive loss of musclecontrol, and ultimately patients are unable to move,except to blink; they cannot speak, eat, or breathewithout assistance, yet the mind and senses are leftintact. The median survival time following onset ofALS is 23.8 months (37). Fewer than 20 percent ofALS patients survive 5 years or more.
Paralysis in ALS is produced by the selectivedeath of nerve cells in the brain and spinal cord thatcontrol muscle movement (43, 72). No single causeof ALS has been widely accepted. Five to 10 percentof ALS is familial, and research is being directedtoward uncovering its genetic underpinnings. Ge-netic factors were initially thought to be responsiblefor the high incidence of ALS observed in Guam.More recent studies, however, indicate that anenvironmental factor may have produced the highincidence of ALS in Guam (box 6-A) and may beresponsible for the increase in ALS mortality rate inthe United States (38). An infectious cause of ALShas also been considered (43). Disrupted immunesystem function, leading to autoimmunity, is anothersuspected cause of ALS, and clinical trials are nowunder way to evaluate the effectiveness of immuno-suppression in treating the disease.
Early diagnosis of ALS can be difficult, since it isnot associated with any specific chemical marker(44). Abnormal muscle function is generally detect-

100 Neural Grafting: Repairing the Brain and Spinal Cord
able at the time of diagnosis, however, and concen-trations of a chemical associated with muscleatrophy may be elevated in the blood. At present,there is no treatment or cure for ALS. Medicalintervention is directed at the management ofsymptoms. Drugs may be employed to limit musclespasticity and cramping and hypersalivation. Coun-seling and rehabilitation services are employed tohelp ALS patients adapt to their disability. In thefinal stages of the disease, a feeding tube orrespirator may be used to maintain the patient.Neural grafting with motor neurons has beenreported in a few animal experiments, althoughmany difficulties characterize this approach tothe treatment of ALS.
Difficulty in early diagnosis of ALS and somedisagreement over nomenclature have complicatedepidemiological studies of this disease (37). A recentstudy indicates that the mortality rate from motorneuron disease increased among the elderly between1962 and 1984 (38). In 1987, 3,381 deaths in theUnited States were attributed to motor neurondisease (64). The number of people suffering fromALS in the United States can only be estimated,since there are no national data on the incidenceand prevalence of this disease. The incidence ofALS is estimated from medical records in Rochester,Minnesota, between the years of 1925 and 1977; onaverage, two cases per 100,000 persons were diag-nosed each year (37, 72). Extrapolation from thesedata indicates that 5,000 new cases of ALS arediagnosed in the United States each year. It isestimated that approximately 15,000 Americanssuffer from ALS at any given time. Since theincidence of ALS increases with age, the number ofcases is expected to increase as the population ages.
CENTRAL NERVOUS SYSTEMINJURY
Spinal Cord Injury
Spinal cord injury is any damage to the spinal cordthat results in paralysis or loss of sensation in variousparts of the body, or both. The magnitude offictional loss following injury to the spinal cord isdirectly related to the extent of the damage andwhere in the spinal cord the injury occurs. Damageto the spinal cord can be caused by a sudden impact(from a motor vehicle collision or sporting injury),gradual compression of the spinal cord tissue (from
a tumor, blood clot, or herniated disk), or aninterruption in the blood supply to the spinal cord.
Spinal cord injury caused by sudden impactusually results from a forceful blow on the bones ofthe spine, causing them to strike the soft nervoussystem tissue of the spinal cord and injure it. Thevictim exhibits loss of movement and sensationbelow the level of the injury. This is partly due to theinitial shock of the injury. The injury also sets inmotion a chain of microscopic events that leads todegenerative changes. This secondary response maybe the most important cause of the permanentdamage associated with spinal cord injury.
Unlike sudden-onset trauma, injury due to gradualcompression is the result of a relatively slowdeformation of the tissue by an intruding body.While permanent loss of function can result fromspinal cord compression, the functional loss is oftenreversed once the compressing body is removed.
Disruption of the blood supply to the spinal cordfor a prolonged period of time can result in cell deathand permanent damage. Any sort of blockage ofblood vessels, such as a blood clot, or damage to themajor arteries supplying the spinal cord can cut offthe blood supply.
Whatever the cause, damage to the spinal corddisrupts the nerve cell networks and the brain’scontrol over body functions. Injuries to the upperregions of the spinal cord affect most of the body andare often life-threatening because control of breath-ing may be disrupted. Patients with an injury to theupper portion of the spinal cord generally must bemaintained on a respirator for the rest of their lives.Quadriplegic, or paralysis and loss of sensation fromthe shoulders down, results from damage to theupper spinal cord. Paraplegia, or loss of movementand sensation from the waist down, results fromdamage to the middle or lower portions of the spinalcord. Other results of injury to the spinal cordinclude muscle problems such as spasticity; sensoryconditions where the patient can experience painfrom the slightest touch; abnormal blood pressureand temperature regulation; disturbances of sexualfunction; loss of voluntary bladder control, whichcan lead to bladder infections; and loss of voluntarybowel function.
As many as 30 percent of persons die within 24hours of a spinal cord injury (36). The nature of thetraumatic event and the amount of force that caused

Chapter 6--Relevant Neurological Disorders . 101
the injury are important factors related to survivalduring the first 24 hours. For example, one studyshowed that the 24-hour survival rate was 97 percentfor recreational injuries and 60 percent for motorvehicle crashes (36). If a patient survives the initialspinal cord trauma, his or her chance of long-termsurvival is high. It has been estimated that 86 percentof patients who survive the first 24 hours followinga spinal cord injury are still alive 10 years later (60).
In the event of an injury to the spinal cord, thereare two phases at which therapeutic interventionscan be directed-the acute phase and the chronicphase. Interventions during the acute phase areaimed at prevention of damage, while treatmentduring the chronic phase is directed toward improve-ment of function.
During the acute phase, 8 to 12 hours immediatelyfollowing a spinal cord injury, surgical interventionmay be necessary to prevent further damage to thespinal cord. In addition, attempts may be made toslow or confine further nerve cell death and degener-ation in response to the spinal cord injury. Since ithas been shown in animal experiments that only asmall fraction of nerve cells has to be saved to retainsome degree of function, any tissue spared couldsignificantly improve subsequent rehabilitation. Anumber of drugs are being considered for use in thissituation, including antioxidants, calcium channelantagonists, naloxone, thyrotropin-releasinghormone, and corticosteroids. Dramatic results havebeen reported when the corticosteroid methylpredni-solone was administered shortly after an injury to thespinal cord (42). This treatment significantly de-creases the ultimate extent of injury in patients andlessens the disability they exhibit following theinjury. The continued development of drugs andprocedures that prevent, or at least contain, this acutedegenerative process is an important and promisingarea of research.
The chronic phase of treatment, aimed at rehabili-tation and improving function, continues throughoutthe life of the patient. Some newer techniquesinclude electrical stimulation of muscles and variousbiofeedback procedures. Advances in microelec-tronics have paved the way for the development ofneural prosthetic devices to activate and coordinateactivity in the injured spinal cord. All of thesetherapies are aimed at maximizing the rehabilitationprocess following an injury to the spinal cord: Noneis directed at repairing the damaged spinal cord.
Several strategies for the use of neural grafts torepair spinal cord injury have been proposed andtested in animal experiments, including thepromotion of regrowth, the bridging of theinjured region, and the replacement of nerve cellsin the spinal cord.
Since the vast majority of spinal cord injuries iscaused by trauma, prevention is an important strat-egy in reducing incidence. Motor vehicle crasheshave been reported to account for 48 percent ofspinal cord injuries, followed by falls (20 percent),acts of violence (15 percent), and sports injuries (14percent) (60). Older adolescents and young adultshave the highest rate of spinal cord injury, both in theUnited States and in other countries (34).
The incidence of spinal cord injury may beunderestimated because injuries resulting in imme-diate death may not be reported. The averageage-adjusted mortality rate for spinal cord injury wasestimated at 2.9 per 100,000 persons in OlmstedCounty, Minnesota, from 1935 to 1981 (20). Theincidence rate in that population was 8.34 per100,000 males, and 2.77 per 100,000 females (21).The estimated prevalence rate was 47.3 per 100,000persons (20). A recent survey of a nationwidesample of institutionalized and noninstitutional-ized persons estimated the prevalence rate ofspinal cord injury to be 72.1 cases per 100,000persons or a prevalence of approximately 180,000persons in the United States (25) (box 6-B).Medical intervention, rehabilitation services, andlost income due to spinal cord injury have beenestimated to cost more than $2 to $8 billion annually.
Brain Injury
Traumatic brain injury has been labeled the silentepidemic (66); brain injury is the major cause ofdeath and disability among children and youngadults in the United States (66). Since so many ofthe people who sustain brain injury are young, thecost to society, including medical and rehabilitationexpenses, support services, and lost income, is great,estimated at nearly $25 billion each year (66).
Motor vehicle collisions, violent assaults, andfalls are the main causes of head trauma and braininjury. The consequences of head trauma dependupon the amount and type of damage sustained bythe brain (53). When head injury produces a mildconcussion, there are usually few overt symptoms,although the brain may sustain structural damage

102 . Neural Grafting: Repairing the Brain and Spinal Cord
Box 6-13-Neurological Disorders and the Veteran
There are approximately 27 million veterans in the United States. Their medical needs are handled through the172 medical centers and 227 outpatient clinics of the Department of Veterans Affairs (VA). In fiscal year 1989,71,995 patients were discharged from the medical centers after having been treated for a variety of neurologicaldisorders. These included cerebrovascular disease (18,850 patients), dementia and organic brain syndrome (13,406),epilepsy (13,950), neuromuscular diseases (7,&17), diseases of the basal ganglia (3,096), and demyelinating diseasesand diseases of the spinal cord (2,755).
Spinal cord injury (SCI), caused principally by battlefield trauma during wartime and vehicular and divinginjuries during peacetime, is of special concern to the VA, which maintains 20 SCI centers throughout the UnitedStates (table 6-5). The number of veterans with an SCI has been put at 45,000. During fiscal year 1987,18,300 suchpatients were treated at VA centers; 64 percent of their injuries were service-related. Among this patient population,50 percent were over the age of 55, and just about all (98.9 percent) were men. Forty-one percent of the men servedduring World War II, veterans from the Korean conflict made up 22 percent of the patient population, and 30 percentwere from the Vietnam and post-Vietnam eras. Within this VA population of SCI patients, 53 percent wereparaplegic and 47 percent were quadriplegic. For fiscal year 1988, $90.8 million was allocated for direct medicalcare by these SCI centers.
SOURCES: L. Lehman, acting director, Neurology, Dep artment of Veterans Affairs, Washington, DC, personal communication% April 1990;T. Stripling, Paralyzed Veterans of America, personal communication, July 1990; Department of Veterans Affairs, Spinal CordInjury Service, Washington DC, 1990.
Table 6-5-Department of Veterans Affairs, temporary loss of consciousness, seizures, paralysis,Spinal Cord Injury Centers, Fiscal Year 1989 loss of memory, permanent loss of responsiveness,
Operating Inpatients Outpatientor death.
beds - treated visits
Augusta, GA. . . . . . . . . 60 546 342 Immediate and expert medical attention may beBrockton/
West Roxbury, MA .Bronx, NY. . . . . . . . . . .Castle Point, NY . . . . .Cleveland, OH . . . . . . .East Orange, NJ . . . . .Hampton, NY . . . . . . . .Hines, IL . . . . . . . . . . . .Houston, TX . . . . . . . . .Long Beach, CA.. . . . .Memphis, TN . . . . . . . .Miami, FL . . . . . . . . . . .Milwaukee, WI . . . . . . .Palo Alto, CA . . . . . . . .Richmond, VA . . . . . . .San Diego, CA. . . . . . .San Juan, PR . . . . . . .Seattle, WA . . . . . . . . .Sepulveda, CAa . . . . . .St. Louis, MO . . . . . . . .Tampa, FL . . . . . . . . . .
Total . . . . . . . . . . . . . . .
1158043802564
13526
197120365630
1205
2037NA4270
548182259271135134522159980690207506277785
89197330NA351448
1,361 7,616
2011,766
972338191
941,6601,327
15,3163,381
3752,2051,378
9964,1951,0861,6131,096
4962,588
41,184
able to prevent death and limit complications thatfollow serious injury of the brain; rehabilitation mayenhance and foster intact neurological functions.The death of nerve cells in the brain, however,cannot be reversed by any medical intervention atthis time. The irreversible nature of brain injuryemphasizes the importance of strategies aimed atpreventing and reducing the severity of traumaticbrain injury. The basis for neural grafting as atherapeutic approach in brain injury is thepossible replacement of degenerated nerve cells.This strategy has been examined in animalexperiments.
The system for determining the incidence andprevalence of brain injury in the United Stateshas been decried as inadequate (35, 59). Many
Outpatient center.SOURCE: Department of Veterans Affairs, Spinal Cord Injury Service,
Washington, DC, 1990.
with long-lasting effects. More serious head traumacan lead to diffuse injury throughout the brain, brainswelling, extensive bleeding, or direct damage ofnerve cells. The sequelae of such damage depend onwhich areas of the brain are injured and may include
factors contribute to the difficulty of tracking suchinjuries. There is no single registry of all victims ofbrain injuries. Sufferers of brain injury are widelydispersed throughout the health care system; forexample, 50 percent of the fatal cases of brain injurynever enter the hospital, where many statistics arecollected. And universal nomenclature for defininghead and brain injuries is lacking. The InteragencyHead Injury Task Force (66), convened in response

Chapter 6--Relevant Neurological Disorders ● 103
Figure 6-2-Types of Head Injury Causing Death
1 00
80
60
40
20
l-t
Transport
I
20
0- Olmsted Co U S San Diego Co Bronx, No Central San Diego Chicago
Minn. California N Y Virginia California area
Graph illustrates regional differences in death rates followinghead injury due to transport (vehicle collisions), assault and useof firearms, falls, and sporting injuries.SOURCE: J.F. Kraus, “Epidemiology of Head Injury,” Head h’@y, P.R.
Cooper (cd.) (Baltimore, MD: Williams & Wilkins, 1987).
to congressional concerns about the seriousness oftraumatic brain injury, affirmed the need for epi-demiologica1 investigation.
Each year in the United States, 75,000 to 100,000persons die from head injuries (66) (figure 6-2). Astudy of deaths associated with brain injury in theUnited States between 1979 and 1986, based on datafrom the National Center for Health Statistics, foundan annual rate of 16.9 deaths per 100,000 persons, orapproximately 42,250 people each year (59). Acommunity-based study in Olmsted County, Minne-sota, between 1965 and 1974, estimated that braininjuries are responsible for 32 deaths per 100,000persons among males and 9 deaths per 100,000persons among females (3; see also 35). Currently,there are no national data on the prevalence of braininjury. Estimates of the incidence rate of braininjury, mostly derived from community studies,indicate that 200 persons per 1003000 populationper year, or 500,000 persons per year in all, sufferfrom injury to the brain that is serious enough torequire hospital admission (35). There are no dataon how many people sustain permanent loss offunction due to head injuries. It has been calculatedthat 70,000 to 90,000 people each year arepermanently disabled as a result of head injury(35).
Stroke
Most strokes are caused by cerebrovascular dis-ease. They result in a sudden, specific neurologicaldeficit, the severity of which varies depending on
Photo credit: R. Restak, The Mind (New Yoti, NY: Bantam Books, 1988)
Picture of CAT scan of brain following a stroke.Arrow indicates region of damage.
where in the brain the lesion occurred. Functionalproblems can include coma, paralysis, or inability tospeak. A severe stroke can result in death.
There are two broad categories of conditionsunder the heading of stroke. Ischemia, or decreasedblood flow, is most commonly caused by blockageof a blood vessel in the brain and produces 82percent of strokes (45, 61). Bleeding into the braintissue or spaces around the brain causes 18 percentof strokes and is largely attributable to rupture ofblood vessels and less often to high blood pressure.Both ischemic stroke and intracranial hemorrhageinterrupt normal blood flow to brain tissue and causea shortage of oxygen and nutrients.
Currently, the brain damage produced by astroke cannot be reversed. Therapeutic interven-tions are aimed at reducing any further damage in thebrain and preventing a reoccurrence (71). Medical

104 . Neural Grafting: Repairing the Brain and Spinal Cord
therapy to reverse and prevent blood vessel blockageincludes aspirin and other drugs that prevent ordisrupt the formation of blood clots. Drugs thatinhibit blood vessel spasm may also be useful. Drugsor surgery may be necessary to reduce bleeding orexcess fluid in the brain. Rehabilitation therapy isadvised in order to maximize functional recoveryfollowing a stroke. Recovery depends on manyfactors, including the site and size of the stroke andthe degree of brain damage incurred.
Recent experimental data suggest that much of thebrain damage induced by strokes may ultimately bepreventable. The immediate nerve cell death pro-duced by an interrupted blood supply appears to berather modest; subsequent changes in the brain, suchas changes in the blood vessels and the release ofexcess excitatory chemicals, may be more destruc-tive. Experiments in animal models of stroke indi-cate that blocking the action of excess excitatorychemicals in the brain can reduce nerve cell death(45). Since nerve cell death causes the disabilitythat follows stroke, replacement of the nerve cellswith a neural graft is considered a potentialmedical therapy in some cases. Some animalexperimentation has been carried out investigat-ing this possibility.
The nomenclature for stroke has varied considera-bly during the last century, complicating epidemio-logical analysis. Furthermore, stroke is sometimesoverdiagnosed (37). Despite these problems, it isapparent that stroke is the third leading cause ofdeath in the United States, after heart disease andcancer. It is estimated that stroke costs $10 billioneach year in direct medical expenses and lostincome. In 1987, approximately 150,000 deathsnationwide were due to stroke, representing anage-adjusted mortality rate of 30.0 per 100,000persons, or 7.1 percent of all deaths (66). Withincreasing age, the incidence of stroke, as well asdeath due to stroke, increases; however, the nation-wide incidence of and mortality rate from stroke aredeclining, perhaps due to improved control ofhypertension, diabetes, and cardiac disease, as wellas a reduction in cigarette smoking (61, 71).
Mortality statistics do not present the entiremedical picture of stroke, since strokes are notalways fatal. There are 500,000 new stroke victimsin the United States annually (45). Among personsunder age 54, the yearly incidence rate of stroke is 17per 100,000 persons (37). Among persons over age
65, the annual incidence of stroke is more than 500per 100,000 persons.
A national survey conducted by the NationalInstitutes of Health found that as of 1976,1.7 millionpeople still living had a history of hospitalization forstroke (65). The most recent national data availablefrom the National Health Interview Survey indicateda prevalence rate in the United States of 1,120 casesper 100,000 persons (66).
EPILEPSYAn epileptic seizure may suddenly render an
individual unconscious and lead to violent bodymovements, or it may simply cause a brief loss ofconsciousness or repetitive and sometimes subtlemovements such as chewing. The occurrence of aseizure does not necessarily lead to a diagnosis ofepilepsy, since seizures may result from infections,head injury, and tumors. In general, a diagnosis ofepilepsy is made if repeated seizures occur in apatient due to CNS dysfunction.
Approximately one-half of those who suffer fromepilepsy experience their first seizure before age 20(18). Seizures are classified as generalized or partial,depending on the nature of the onset of abnormalbrain function (table 6-6). Electrical recording ofbrain activity during a seizure and clinical symptomsare used to delineate the different classes of seizure.Generalized seizures involve large regions of thebrain and are often characterized by loss of con-sciousness and symmetrical involvement of themuscles of the body. A partial seizure reflectsabnormal activity beginning in a single area of thebrain and usually results in more restricted disturb-ances.
The electrical impulses that are normally used bynerve cells to communicate and to send informationthroughout the body go awry in epilepsy. Nerve cellsdisplay excessive excitability and dispatch electricalimpulses at a manic rate. At the same time,metabolism in the brain is profoundly altered. Nervecells may be unable to regulate properly the entry ofcharged molecules, thus rendering them more excit-able. In addition, research indicates that abnormalinput from other nerve cells may lead to enhancedexcitability.
Management of epileptic disorders is complex(18). The first step involves accurate diagnosis anddetermination of the cause of the seizures. A careful

Chapter 6--Relevant Neurological Disorders ● 105
Table 6-6—Types of Epileptic Seizures
. Partial (seizures that begin in a discrete region of the brain)— simple partial (no loss of consciousness)— complex partial (impaired consciousness)— partial seizures that spread throughout the brain
. Generalized (seizures that begin throughout the brain)● Unclassified
SOURCE: Office of Technology Assessment, 1990.
medical history and sometimes intensive monitoringare necessary to diagnose the origin of seizures; inmost cases, however, the cause of seizures is notfound. The second step is to design a drug therapy.Anticonvulsant drugs can completely eliminate or atleast significantly curtail the occurrence of seizuresamong 75 percent of persons with epilepsy; how-ever, none of the drugs currently available can cureepilepsy, and all have side-effects. Anticonvulsantdrugs may act by blocking the entry of chargedmolecules into nerve cells or by increasing the actionof the inhibitory brain neurotransmitter GABA.Constant assessment and monitoring of the dosageand combination of drugs to control a patient’sepilepsy are generally necessary. Another treatmentfor some cases of epilepsy involves surgical removalof the hyperexcitable nerve cells. Initial animalexperiments have shown that neural grafting caninhibit seizures, suggesting that this approachmay one day provide a useful therapy for somecases of epilepsy (5).
There are a number of sources of epidemiologica1data about epilepsy. Estimates of the prevalence andincidence of epilepsy vary with the definition of thedisorder (a single seizure v. chronic seizures). Thesource of the data, whether from medical records orsurveys, also adds variability to the estimates. Thereis no doubt, however, that epilepsy is a commondisorder. Five to 10 percent of the population willsuffer at least one epileptic seizure (26). Theprevalence rate of epilepsy in 1974 in Rochester,Minnesota, was 650 cases per 100,000 persons;when extrapolated nationwide, these data indicatethat there are approximately 1.5 million cases ofepilepsy in the United States (37). Approximately40 to 60 new cases per 100,000 persons arediagnosed each year (37).
DEMYELINATING DISORDERS:MULTIPLE SCLEROSIS
Multiple sclerosis (MS) is a chronic neurologicaldisease characterized by an array of symptoms,
Photo credit: National Institutes of Health
Picture of measurement of brain activity using anelectroencephalograph, or EEG. Measurement is used to
detect epilepsy.
depending on wherein the CNS lesions occur (57).Initial symptoms of MS may include muscle weak-ness; numbness and tingling, especially in the armsand legs; loss of coordination and balance; dizzi-ness; slurred speech; fatigue; and loss of bowel orbladder control. Optic neuritis, which can result inblurred or double vision or disturbances of colorvision, may bean early symptom of the disease. Theonset of MS usually occurs between the ages of 20and 40 (70). The course of the disease is unpredicta-ble; typically, symptoms emerge, go away com-pletely, and then reemerge. Less frequently, symp-toms worsen steadily without remission.
The relapsing-remitting symptoms of MS areassociated with widespread lesions of myelinsheaths in the CNS. Myelin surrounds many nervefibers in the nervous system, insulating them andthus permitting the rapid conduction of electricalimpulses. When the myelin sheath is destroyed, theconduction of electrical nerve impulses is retarded,producing the characteristic symptoms of MS. It isnot known what causes the destruction of myelin inMS. Some data suggest that an infectious agent,particularly a virus, acquired between the ages of 5and 15 maybe involved, although no such agent hasbeen isolated, despite extensive research (6, 70).Unequal geographic distribution of MS seems tosupport the idea of an infectious or environmentalcause (37). The disease rarely occurs near theequator, and its incidence increases with latitude inthe Northern and Southern hemispheres (figure 6-3).Furthermore, migration before the age of 15 to ageographic area with a different incidence of MS

106 ● Neural Grafting: Repairing the Brain and Spinal Cord
Figure 6-3-Geographical Differences in Death Rate Due to Multiple Sclerosis
Deaths per 100,000 persons, by state of residence at death. Death rates are significantly higher in thenorthern versus the southern regions of the United States.SOURCE: J.F. Kurtzke and L.T. Kurland, “The Epidemiology of Necrologic Disease,” C/inica/ Neurology, R.J. Joynt
(cd.) (Philadelphia, PA: J.B. Lippincott, 1989).
changes an individual’s risk of MS to that of thenative population. While the immediate cause of MSis likely to be found in the environment, susceptibil-ity is probably genetically determined.
Other data indicate that disrupted immune func-tion may underlie MS. Some genes related toimmune system function are associated with MS(55). Furthermore, immune system cells that re-spond to components of myelin have been identifiedin individuals with MS (1, 68). It is postulated thata virus may initiate this immune response ingenetically susceptible individuals.
Diagnosis of MS presents some difficulties; itrests upon the characteristic symptoms, direct view-ing of demyelination within the CNS using MRI(magnetic resonance imaging), and the absence ofany other explanation. There is no cure for MS atpresent. Therapy is directed at shortening the timeduring which symptoms are present and alleviatingdisabling symptoms such as muscle spasms or pain.When symptoms of MS flare up, ACTH (adrenocor-ticotropic hormone) or methylprednisolone is oftenadministered. Such long-term measures, which in-hibit immune system function, have not proven to
prevent new or more disabling bouts with MS, andthey cause serious side-effects. A few animalexperiments have suggested that myelin-producing cells can be introduced into the CNS toseek out and myelinate nerve fibers; this researchsuggests a potential role for neural grafting in MS(22).
A national survey conducted in the 1970s indi-cated that approximately 10,000 persons are diag-nosed with MS annually (4). According to thatsurvey, there were 123,000 MS patients in theUnited States in 1976, a prevalence rate of 58 casesper 100,000 persons. More current national preva-lence data, from the National Health InterviewSurvey, estimate that 151,000 persons suffer fromMS, a prevalence rate of 70 cases per 100,000persons (63). The incidence and prevalence of MSwere also estimated from medical records in Olm-sted County, Minnesota, between 1905 and 1984(70). The prevalence rate of MS increased during thelast 10 years of the study, averaging 175 cases per100,000 persons. Extrapolated nationwide and ac-counting for the geographical gradient of MS, thesedata suggest that approximately 250,000 people inthe United States suffer from MS. This observed

Chapter 6--Relevant Neurological Disorders . 107
increase in MS was attributed largely to improveddiagnosis, although an increase in survival oroccurrence of the disease may have also contributed.Two-thirds of the MS patients were ambulatory andable to work.
SUMMARY AND CONCLUSIONSNeurological disorders that may one day prove
amenable to treatment with neural grafting are listedin this chapter. It is impossible to assert definitivelythe future applications of neural grafting at this earlystage in its development. However, the wide array ofanimal research currently probing the many differentuses and actions of neural grafting suggests that thistechnology may ultimately have several applica-tions. Furthermore, as new discoveries unveil thechemical and structural alterations associated withother brain disorders, additional applications ofneural grafting may become apparent.
While precise epidemiological data are oftenunavailable, it is clear that the neurological disorderslisted in this chapter area significant cause of illness,disability, and death in the United States. For manyof these disorders, there is no known cause and noadequate therapy. For none is there a cure for thenerve ceil death or other underlying pathology thatcauses mortality and morbidity. Research effortsinvolving genetic analysis, molecular biology, andnew drugs, as well as neural grafting, continue toimprove investigators’ understanding of the disor-ders and to suggest treatments.
CHAPTER 6 REFERENCES1.
2.
3.
4.
5.
6,
Allegretto, M., Nicklas, J.A., Srirarn, S., et al.,“T-Cells Responsive to Myelin Basic Protein inPatients With Multiple Sclerosis,” Science 247:718-721, 1990.American Parkinson’s Disease Association, quar-terly newsletter, winter 1989-90.Annegers, J.F., Grabow, J.D., Kurland, L.T, et al.,“The Incidence, Causes, and Secular Trends of HeadTrauma in Olrnsted County, MN, 1935-1974,”Neurology 30:912-919, 1980.Baum, H.M., and Rothschild, B.B., “The Incidenceand Prevalence of Reported Multiple Sclerosis,”Annals of Neurology 10:420-428, 1981.Buzsaki, G., Ponomareff, G., Bayardo, F., et al.,“Suppression and Induction of Epileptic Activity byNeuronal Grafts,” Proceedings of the NationalAcademy of Sciences, U.S.A. 85:9327-9330, 1988.Calder, V., Owen, S., Watson, C., et al., “MS: AI_malized Immune Disease of the Central Nervous
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
System,” Immunology Toduy 10:99-103, 1989.Conneally, P.M., “Huntington’s Disease: Geneticsand Epidemiology,” American Journal of HumanGenetics 36:506-526, 1984.Davies, P., Katzman, R., and Terry, R.D., “ReducedSomatostatin-like Immunoreactivity in Cerebral Cor-tex From Cases of Alzheimer’s Disease SenileDementia,” Nature 288:279-180, 1980.Davis, G. C., Williams, A. C., Markey, S.P., et al.,“Chronic Parkinsonism Secondary to IntravenousInjection of Meperidine-analog Synthesis,” Psychi-atric Research 1:249-254, 1979.Dreosti, I.E., and Smith, R.M., Neurobiology ofTrace Elements (Clifton, NJ: Humana Press, 1983),vols. 1 and 2.Evans, D.A., Funkenstein, H.H., Albert, M. S., et al.,“Prevalence of Alzheimer’s Disease in a CommunityPopulation of Older Persons Higher Than PreviouslyReported,’ Journal of the American Medical Associ-ation 262:2551-2556, 1989.Fahn, S., “Huntington’s Disease and Other Forms ofChorea,” Merritt’s Textbook of Neurology, L.P.Rowland (wI.) (Philadelphia, PA: ha & Febiger,1989).Fischer, W., Wictorin, K., Bjorklund, A., et al.,“Amelioration of Cholinergic Neuron Atrophy andSpatial Memory Impairment in Aged Rats by NerveGrowth Factor,” Nature 329:65-68, 1987.Fomo, L. S., Langston, J.W., DeLanney, L.E., et al.,“hcus Ceruleus I_esions and Eosinophilic Inclu-sions in MPTP-Treated Monkeys,” Annals of Neu-rology 20:449-455, 1986.Freed, W.J., Cannon-Spoor, H.E., and Krautharner,E., “Factors Influencing the Efficacy of AdrenalMedulla and Embryonic Substantial Nigra Grafts,”Neural Grafting in the Mammalian CNS, A.Bjorklund and U. Stenevi (eds.) (Amsterdam:Elsevier Science Publishers, 1985).Gable, C. B., “A Compendium of Public Health DataSources,’ American Journal of Epidemiology131:381-394, 1990.Ghanbari, H.A., Miller, B.E., Haigler, H.J., et al.,“Biochemical Assay of Alzheimer’s Disease-Associated Protein(s) in Human Brain Tissue,”Journal of the American Medical Association263:2907-2910, 1990.Goldensohn, E.S., Glaser, G.H., and Goldberg, M.A.,“Epilepsy,” Merritt’s Textbook of Neurology, L.P.Rowland (cd.) (Philadelphia, PA: ka & Febiger,1989).Greenwald, B.S., and Davis, K.L., “ExperimentalPharmacology of Alzheimer’s Disease,” The De-mentias, R. Mayeux and W.G. Rosen (eds.) (NewYork NY: Raven Press, 1983).Griffii, M.R., O’Fallen, W.M., Opitz, J.L., et al.,“Mortality, Survival and Prevalence: Traumatic

108 . Neural Grafting: Repairing the Brain and Spinal Cord
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
Spinal Cord Injury in Olmsted County, MN, 1935-1981,” Journal of Chronic Disorders 38:643-653,1985.Griffin, M.R., Opitz, J.L., Kurland, L.T, et al.,“Traumatic Spinal Cord Injury in Olmsted County,MN, 1935 -1981,” American Journal of Epi&miol-0~ 121:884-895, 1985.Gumpel, M., Baumann, N., Raoul, M., et al., “Sur-vival and Differentiation of Oligodendrocytes FromNeural Tissue Transplanted in New-Born MouseBrain,” Neuroscience Letters 37:307-311, 1983.Gusella, J.F., Wexler, N. S., Conneally, M.P., et al.,“A Polymorphic DNA Marker Linked to Hunting-ton’s Disease,” Nature 306:234-238, 1983.Haroutunian, V., Kanof, P.D., Tsuboyama, G.A., etal., “Animal Models of Alzheimer’s Disease: Behav-ior, Pha.rmacology, Transplants,’ Canadian Journalof Neurological Science 13:385-393, 1986.Harvey, C., Rothschild, B., Asmann, A.J., et al.,“Estimates of Spinal Cord Injury Prevalence: ASurvey-based Approach,” paper presented at theannual meeting of the American Spinal Cord InjuryAssociation, Orlando, FL, May 1990.Hauser, W. A., and Hesdorffer, D. C., Epilepsy: Fre-quency, Causes, and Consequences (Landover, MD:Epilepsy Foundation of America, 1990).Hefti, F., “Nerve Growth Factor Promotes Survivalof Septal Cholinergic Neurons After FimbrialTransections,’ Journal of Neuroscience 6:2155-2161, 1986.Huang, L.F., and Hu, ‘EW., “Economic Costs ofSenile Dementia in the United States,” paper pre-pared for the National Institute on Aging, Washing-ton, DC, 1984.Jenkins, J.B., and Conneally, P.M., “The Paradigmof Huntington’s Disease,” American Journal ofHuman Genetics 45:169-175, 1989.Katzman, R., “Alzheimer’s Disease,” New EnglandJournal of Medicine 314:964-973, 1986.Kokmen, E., Chandra, V., and Schoenberg, B.S.,“Trends in Incidence of Dementing Illness inRochester, MN, in Three Quinquennial Periods,1960-1974,” Neurology 38:975-980, 1989.Keller, W.C. (cd.), “Classification of Parkinson-ism,’ Handbook of Parkinson’s Disease (New YorkNY: Marcel Dekker, 1987).Keller, W., O’Hara, R., Weiner, W., et al., “Relation-ship of Aging to Parkinson’s Disease,’ Advances inNeurology, M.D. Y& and K.J. Bergmann (eds.)(New York, NY: Raven Press, 1987).Kraus, J.F., “Epidemiologic Aspects of Acute SpinalCord Injury: A Review of Xncidence, Prevalence,Causes, and Outcome,” Central Nervous SystemTrauma Status Report 1985, D.P. Becker and J.T.Povlishock (eds.) (Bethesda, MD: National Institutesof Health, 1985).
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
Kraus, J.F., “Epidemiology of Head Injury,” HeadZnjury, P.R. Cooper (cd.) (Baltimore, MD: Williams& Wilkins, 1987).Kraus, J.F., Franti, C.E., Borhani, N.O., et al.,“Survival With an Acute Spinal-Cord Injury,”Journal of Chronic Disorders 32:269-283, 1979.Kurtzke, J.F., and Kurland, L.T, “TheEpidemiologyof Necrologic Disease,” Clinical Neurology, R.J.Joynt (cd.) (Philadelphia, PA: J.B. Lippincott, 1989).Lilienfeld, D.E., Chan, E., Ehland, J., et al., “Increas-ing Mortality From Motor Neuron Disease in theUnited States During the Past Two Decades, ’’Lancet1:710-713, 1989.Marsden, C.D., “Basal Ganglia Disease,” Lancet2:1141-1146, 1982.Marttila, R.J., “Epidemiology,” Handbook of Park-inson’s Disease, W.C. Keller (cd.) mew York, NY:Marcel Dekker, 1987).Marttila, R.J., and Rinne, U.K., “Clues From Epi-demiology of Parkinson’s Disease,” Advances inNeurology, M.D. Yahr and K.J. Bergmann (eds.)(New Yorlq NY: Raven Press, 1986).hlarwic~ C., “Administering MethylprednisolonePromptly Appears To Mitigate Cord-Injury Paraly-sis,” Journal of the American Medical Association263:2150-2151, 1990.Mitsumoto, H., Hanson, M.R., and Chad, D.A.,“Amyotrophic Lateral Sclerosis; Recent Advancesin Pathogenesis and Therapeutic Trials,’ Archives ofNeurology 45:189-202, 1988.Munsat, T.L., “Adult Motor Neuron Diseases,”Merritt’s Textbook ofNeurology, L.P. Rowland (cd.)(Philadelphia, PA: Lea & Febiger, 1989).Nadeau, S. E., “Stroke,” Medical Clinics NorthAmerica 73:1351-1369, 1989.Parkinson, J., “An Essay on the Shaking Palsy,”James Parkinson (1755-1824): A Bicentenary Vol-ume of Papers Dealing With Parkinson’s Disease,W.H. McMenemey, F.M.R. Walshe, and J.G. Green-field (eds.) (bndon: Sherwood Neely & Jones, 1817;reprinted London: MacMillan, 1955).Parkinson Study Group, “Effect of Deprenyl on theProgression of Disability in Early Parkinson’s Dis-ease,’ New England Journal of Medicine 321:1364-1371, 1989.Phelps, C.H., Gage, F.H., Growdon, J.H., et al.,“Potential Use of Nerve Growth Factor To TreatAlzheimer’s Disease,” Neurobiology of Aging10:205-207, 1989.Price, D.L., “New Perspectives on Alzheimer’sDisease,” Annual Review of Neuroscience 9:489-512, 1986.Price, D.L., Troncoso, J. C., Whitehouse, P.J., et al.,“Approaches to Neurodegenerative Disease,” Dis-eases of the Nervous System, Clinical Neurobiology,

Chapter 6--Relevant Neurological Disorders ● 109
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
A.K. Asbury, G.M. McKhann, and W.I. McDonald(eds.) (Philadelphia, PA: W.B. Saunders, 1986).Rajput, A.H., Offord, K.P., Beard, C.M., et al.,“Epidemiology of Parkinsonism: Incidence, Classi-fication and Mortality,” Annals of Neurology16;278-282, 1984.Roberts, L., “Huntington’s Gene: So Near, Yet SoFar,” Science 247:624-627, 1990.Rowland, L.P., and Sciarra, D., “Head Injury,”Merritt’s Textbook ofNeurology, L.P. Rowland (cd.)(Philadelphia, PA: ba & Febiger, 1989).Schoenberg, B. S., Kokeman, E., and Okazaki, H.,“Alzheimer’s Disease and Other Illnesses in aDefined United States Population: Incidence Ratesand Clinical Features,’ Annals of Neurology 22:724-729, 1987.Seboun, E., Robinson, M.A., Doolittle, TH., et al.,“A Susceptibility Locus for Multiple Sclerosis IsLinked to the T-Cell Receptor Beta Chain Com-plex, “ Cell 57:1095-1100, 1989.Selkoe, D.J., “Deciphering Alzheimer’s Disease:The Amyloid precursor Protein Yields New Clues,”Science 248:1058-1060, 1990.Sibley, W.A., Poser, C.M., and Alter, M., “MultipleSclerosis,” Merritt’s Textbook of Neurology, L.P.Rowland (cd.) (Philadelphia, PA: ka & Febiger,1989).Sisodia, S. S., Koo, E.H., Beyreuther, K., et al.,“Evidence That Beta-Amyloid Protein in Alz-heimer’s Disease Is Not Derived by Normal Process-ing,” Science 248:492-495, 1990.Sosin, D.M., Sacks, J.J., and Smith, S.M., “Headhjury-Associated Deaths in the United States From1979 to 1986,” Journal of the American MedicalAssociation 262:2251-2255, 1989.Stover, S.L., and Fine, P.R. (eds.), Spinal Cord Injuryand Facts (Birmingham, AL: University of Alabamaat Birmingham, Spinal Rehabilitation Center, 1986).Tmle, J.F., “Etiology and Pathogenesis,” Merritt’sTextbook of Neurology, L.P. Rowland (cd.) (Phila-delphia, PA: Lea & Febiger, 1989).U.S. Congress, Office of Technology Assessment,Losing a Million Minds: Confronting the Tragedy ofAlzheimer’s Disease and Other Dementias, OTA-BA-323 (Washington, DC: U.S. Government Print-ing Office, April 1987).
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
U.S. Department of Health and Human Services,Public Health Service, Centers for Disease Control,National Center for Health Statistics’ computerdatabase (Hyattsville, MD: National Center forHealth Statistics, 1988).
U.S. Department of Health and Human Services,Public Health Service, Centers for Disease Control,National Center for Health Statistics’ computerdatabase (Hyattsville, MD: National Center forHealth Statistics, 1990).U.S. Department of Health and Human Services,Public Health Service, National Institutes of Health,National Institute of Neurological and Communica-tive Disorders and Stroke, National Survey of Stroke,NIH-83-2069 (Bethesda, MD: National Institutes ofHealth, 1983).U.S. Department of Health and Human Services,Public Health Service, National Institutes of Health,National Institute of Neurological Disorders andStroke, Interagency Head Injury Task Force Report(Bethesda, MD: National Institutes of Health, 1989).
Williams, L.R., Varon, S., Peterson, G.M., et al.,“Continuous Infusion of Nerve Growth FactorPrevents Basal Forebrain Neuronal Death AfterFimbria Fornix Transection,” Proceedings of theNational Academy of Sciences, U.S.A. 83:9231-9235,1986.
Wucherpfennig, K.W., ot~ K, Endo, N., et al.,“Shared Human T-Cell Receptor V-Beta Usage toIrnmunodominant Regions of Myelin Basic Pro-tein,” Science 248:1016-1019, 1990.
Wurtman, R.J., “Alzheimer’s Disease,” ScientificAmerican 252(January):62-74, 120, 1985.Wynn, D.R., Rodriguez, M., O’Fallen, W.M., et al.,“Update on the Epidemiology of Multiple Sclero-sis,” Mayo Clinic Proceedings 64:808-817, 1989.
Yatsu, F.M., “Treatment and Prevention of Stroke,”Merritt’s Textbook ofNeurology, L.P. Rowland (cd.)(Philadelphia, PA: Lea & Febiger, 1989).Yoshida, S., Mulder, D.W., Kurland, L.’I, et al.,“Followup Study on Amyotrophic Lateral Sclerosisin Rochester, MN, 1925 Through 1984,” Neuroepi-demiology 5:61-70, 1986.

Chapter 7Legal and Regulatory Issues

CONTENTSPage
PROTECTION OF NEURAL GRAFT RECIPIENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113Coverage by Department of Health and Human Services Regulations
Governing Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113Coverage by State Laws and Regulations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113Role of Institutional Review Boards . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 116FDA Regulation of Neural Grafting Materials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 122Regulation of New Surgical Procedures ... ..*. ... ... ... *.. ... ... ,++*. *,** *e **o,** 127
PROTECTION OF DONORS OF FETAL TISSUE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 129Development of Federal Policy on Fetal Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 130Federal Regulations Governing Fetal Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 131State Laws Governing Embryonic and Fetal Research . . . . . . . . . . . . . . . . . . . . . . . . . . . . 132Payment in Connection With Fetal Experimentation . .....,.....,....,*...*..**.* 136Interstate Transfer of a Fetus ... ... ,.. ... ... ... ... ..*, ,., .*** ee*, **, **** **+ **,$* 137
GOVERNMENT OVERSIGHT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 137Potential Constitutional Challenges to Restrictions on Research . . . . . . . . . . . . . . . . . . . 137Fetal Remains Laws ... ... ... ... ... ... ... ..+ +, ... Q,oe*** *, *e**,*,,****.*,***.*** 138Uniform Anatomical Gift Act . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 139Compensation for Fetal Tissue in a Nonresearch Setting . * . . * ., . * . . * . . * . . ..,+*..., 140
SUMMARY AND CONCLUSIONS ... ... ... ... ... ... *.. ... .., .*. ... ... O **O*+,*** 143CHAPTER 7 REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 143
BoxBox Page7-A. The Genesis of Medical Research Ethics . .........,.*..........*.*.....,**,* 114
FigureFigure Page7-1. An Institutional Review Board Approval Process . . . . . . . . . . . . . . . . . . . . . . . . . . . . 118
TablesTable Page7-1. State Regulations Pertaining to the Protection of Human Subjects in
Experimentation ... ... ... ... ... ... ... ... ... e.. ... .ce**m* **** . *m.+.**.*****, 1157-2. State Regulations Pertaining to the Use and Procurement of Fetal Tissue
for Grafting Research ... ... ... ... ... ... ... ..*. ... ... ..** ... **** *.. v**.***** 133

Chapter 7
Legal and Regulatory Issues
Basic legal tenets govern experimentation andbiomedical research on human beings (see box 7-A).This chapter addresses the legal issues raised byneural grafting, including protection of recipients,protection of donors, informed consent, and Federaland State regulation.
PROTECTION OF NEURALGRAFT RECIPIENTS
Recipients of neural grafts may often be indi-viduals needing special protection. Both the Fed-eral and State Governments have recognized thisneed and have sought to provide protection throughstatutes and regulations. The relevant Federal andState legislation is outlined below.
Coverage by Department of Health andHuman Services Regulations Governing
Research
Department of Health and Human Services(DHHS) regulations apply to all research withhuman subjects that is conducted or funded byDHHS [45 CFR 46.101]. These Federal regulationshave potentially widespread application. The Fed-eral budget for the National Institutes of Health(NIH) alone represents over one-third of all moneyspent on health-related research in the United States(63). In addition, the reach of these Federal regula-tions extends well beyond federally funded research,since the regulations are used widely as guidelinesin institutions that do not receive Federal funding(19).
The DHHS regulations apply to both therapeuticand nontherapeutic research and define research as“a systematic investigation designed to develop orcontribute to generalizable knowledge” [45 CFR46.101-46.409; 21 CFR 50.1-50.48; 45 CFR 46.102(e)]. Some types of research are exempt from Federalregulations under certain conditions, for exampleeducational research and research involving surveyor interview procedures [45 CFR 46.10 l(b)(l) and(3)].
All Federally funded human research projectsmust be reviewed and approved by an Institu-tional Review Board (IRB) [45 CFR 46.103(b)].IRBs are required to conduct continuing review,
which can include third-party observation [45 CFR46.109(e)]. The intervals of continuing review arecontingent on the degree of risk involved in theexperiment but must not be less than once per year.The regulations also provide that risks of theproposed research must be minimized and mustbe reasonable in relation to anticipated benefits[45 CFR 46.ill(a)(l), (2)], and they provide forexpedited review of research that involves minimalrisk [45 CFR 46.1 IO@)]. “Minimal risk” meansthat the risks of harm anticipated in the proposedresearch are not greater than those encounteredin daily life or during the performance of routinephysical or psychological tests [45 CFR46.102(g)]. Research activities involving no morethan minimal risk include, for example, collection ofhair and nail clippings, recording of data that do notinvolve invasion of the subject’s privacy [46 FR8392], and minor changes in approved procedures[45 CFR 46.110(b)].
Federal regulations require that selection ofsubjects be equitable [45 CFR 46.ill(a)(3)] andthat informed consent be obtained from eachsubject [45 CFR 46.116]. The regulations stipulatethe basic elements that must be included in informedconsent and require that such consent be docu-mented and provided in language the subject canunderstand. They further provide that neither theresearcher, the institution, nor the sponsor may bereleased from liability through the subject’s oral orwritten consent. DHHS regulations specificallyaddress research involving fetuses, pregnantwomen, and human in vitro fertilization [45 CFR46.201]. Moreover, separate provisions are includedfor research with children [45 CFR 46.401 (a)].
Coverage by State Laws and Regulations
In research programs where there is no Federalinvolvement or influence, government oversightwill depend on whether there are State statutes.Where DHHS and Food and Drug Administration(FDA) regulations overlap State statutes, the Federalregulations are not intended to preempt applicableState or local laws [45 CFR 46.10 l(g); 21 CFR50.25(c)]. Few States have statutes that addresshuman experimentation specifically. At least sixaddress human research as part of patients’ rights
–113–

114 ● Neural Grafting: Repairing the Brain and Spinal Cord
Box 7-A—The Genesis of Medical Research Ethics
Many legal principles in the area of medical research ethics have been developed in response to abuses ofresearch subjects in Nazi Germany. Examples of unethical research in the United States further stimulated publicdiscussion and policy considerations. The most well-known examples of research abuses in the United States arethe Willowbrook hepatitis study and the Tuskegee syphilis study. In the 1960s, institutionalized mentally disabledchildren at Willowbrook Institution were infected with live hepatitis virus in an effort to develop a vaccine. Thescientists justified their procedures by noting that hepatitis ran rampant through the institution and that all of thechildren would eventually contract the disease. From 1932 to 1972, scientists conducting a U.S. Public HealthService study of 400 black men suffering from syphilis deliberately withheld treatment from them in order to studythe effects of allowing the disease to take its course, even though penicillin had been found to be an effectivetreatment. At least 28 of perhaps as many as 107 men died as a result of this study.
In the trials of Nazi physicians, the court set forth standards that should be met before and during research. TheNazi physicians tried to defend themselves by pointing out abuses in research that had occurred elsewhere, includingthose in the United States, However, this defense did not succeed, and 15 of the 23 physicians were found guiltyof war crimes and crimes against humanity. Those standards, subsequently adopted by the United Nations GeneralAssembly, are known as the Nuremberg Code. The tenets of the code significantly influenced subsequent State laws.For example, the preamble to the California human experimentation law states that the law was necessary since theNuremberg Code was not codified and thus is unenforceable [Cal. Health & Safety Code 24171(b)]. Federalregulations in the United States dealing with research were likewise influenced.
The Nuremberg Code provides guidelines for ensuring that participation in research is voluntary and that therisks of research are minimized It provides that:
. certain basic research and animal research must be done before human research is undertaken;
. the research must be well designed;● the research must be undertaken only by scientifically qualified individuals;. the potential results must justify the risk involved in the performance of the research; and. those results must not be procurable by other means of study.
The central principle of the Nuremberg Code is that participation in research must be voluntary, informed, anduncoerced and that subjects have the right to bring the experimentation to an end. The code also requires that risksbe minimized through appropriate design and conduct of the research as well as adequate preparation and facilitiesto protect the subjects. Research is forbidden if there is an a priori reason to believe that death or disabling injurywill occur (although the code does allow an exception if the scientists also serve as subjects), and ongoing researchmust be stopped if there is reason to believe that its continuation will lead to the injury, disability, or death of thesubjects.
In applying the ethical principles enunciated in the Nuremberg Code to the issue of neural grafting, the questionof whether there has been sufficient animal research may arise. Fetal grafts in rodents and in monkeys have beenstudied, but some experts in the field believe that more animal research is necessary. They also believe that certainadditional information is needed about the nervous system. They argue that eventually, however, human subjectsmust be involved.SOURCES: Office of Technology Assessment, 1990; based on L. Andrews, Medical Genetics: A Legal Frontier (Chicago, IL: American Bar
Foundation, 1987); B. Barber, “The Ethcis of Expeerimentation with Human Subjects,” Scientific American 234(February): 25-31,1976; A.M. Capron,"Human Experimentation," BioLaw l0:217-229, 1986; T. Gill and R Lund., “Implantation of Tissue into theBrain: An Immunologic Perspective, ‘‘ Journal of the American Medical Association 261 :2674-2676, 1989; S. GoIby, “Experimentsat the Willowbrook State School,’ Lancet 1:749, 1971; R. Greenwald, M. Ryan, and J. Mulvihill, Human Subjects Research: AHandbook for Institutional Review Boards (New York, NY: Plenum Press, 1982); J. Jones, Bad Blood: The Tuskegee SyphilisExperiment (New York, NY: Free Press, 1981).
statutes. Some States have statutes protecting partic- that list the requisite elements of informed consent.ular groups of research subjects (e.g., the mentally Some statutes simply prohibit human experimenta-disabled), while others have a professional ethics tion that involves any significant risk of physical orstatute that mandates obtaining patients’ consent to psychological harm. Often, the statutes use the termsexperimentation. The provisions range from a sim- “human research” and “human experimentation”ple statement that individuals have the right to refuse interchangeably. Table 7-1 lists State regulationsto participate in experimental research to statutes covering human subjects in experimentation.

Chapter 7-Legal and Regulatory Issues ● 115
Table 7-l-State Regulations Pertaining to the Protection of Human Subjects in Experimentation
Alaska regulates human experimentation with the mentally ill;limits experiments to those that pose no hazardous risk.
Arizona requires informed consent before a person may partici-pate in a research project as a human subject. Regulateshuman experimentation with the developmentally disabled.
Arkansas regulates human experimentation with the mentally ill;provides that patients have the right to refuse to participate.
California has a comprehensive statute regulating experimenta-tion involving novel therapy and research on human subjects.Requires Institutional Review Board (IRB) approval and in-formed consent for any research involving human subjects;requirements for informed consent include an explanation ofprocedures, possible side-effects, information about alternativetherapy, and subject’s right to withdraw consent at any timeduring the experiment. Regulates human experimentation withthe mentally ill; informed consent of the patient or guardian isrequired, and the research must be intended to benefit thementally ill subject. A grievance mechanism is provided shouldthe experiment go awry.
Colorado requires informed consent before a person mayanticipate in a research project as a human subject. Regulateshuman experimentation with residents of facilities for the
developmentally disabled; informed consent of the patient orguardian is required.
Connecticut provides that prospective subjects in human experi-mentation have the right to refuse to participate.
District of Columbia requires informed consent before a personmay participate in a research project as a human subject.
FEFEmentally retarded; informed consent of the patient or guardianand review board approval are required.
Delaware regulates human experimentation with the mentallydisabled; informed consent of the patient and IRB approval arerequired. The requirement for informed consent may be waivedin cases where an attempt to obtain informed consent from thepatient has failed, no other therapy exists or the patient has notresponded to accepted therapies, the research would be in thebest interests of the patient, and the waiver has been approvedby the IRB and the patient’s legal guardian or next of kin.
Florida requires informed consent before a person may partici-ate in a research project as a human subject. Regulateshuman experimentation with the developmentally disabled;
informed consent of the patient or guardian is required.Physician may request court approval when unwilling to act ondevelopmentally disabled patient’s consent and the guardian isunknown or cannot be located.
Hawaii regulates human experimentation with the mentallydisabled; states that patients have the right to refuse toparticipate.
Illinois regulates human experimentation with the mentally ill anddevelopmentally disabled; informed consent of the patient orguardian is required.
Kansas requires informed consent for participation in researchProjects. Regulates human experimentation with mentally illinpatients; requires informed consent of the patient and his orher guardian.
Maine requires informed consent before a person may participatein a research project as a human subject. Regulates humanexperimentation with the mentally retarded; informed consentof the patient or guardian is required.
Massachusetts provides that prospective subjects in humanexperimentation have the right to refuse to participate.
Michigan provides that respective subjects in human experi-Rmentation have the rig t to refuse to participate.
Minnesota requires informed consent for participation in researchprojects.
Missouri requires IRB approval for research with the mentallydisabled, informed consent of the patient or guardian, and that
fthe research be intended to benefit the mentally ill subject.Montana requires State review board approval and informed
Nevada provides that prospective subjects in human experimen-Ktation have the right to refuse to participate.
New Hampshire requires IRB approval for any research involvinghuman subjects.
New Jersey regulates experimentation with the mentally ill andmentally retarded; provides that mentally disabled patientshave the right to refuse to participate and requires that theresearch be intended to benefit the mentally ill subject. Courtapproval is mandatory if the disabled patient is declaredincompetent.
New Mexico regulates human experimentation with the develop-mentally disabled and the mentally ill; requires informedconsent of the patient or guardian.
New York has a comprehensive statute regulating experimenta-tion with novel therapy on humans and research on healthyhuman subjects. Requires IRB approval of any research withhuman subjects; requirements for informed consent include anexplanation of procedures, possible side-effects, alternativetherapies, and subject’s right to withdraw consent at any time
lduring the experiment. Ma es specific mention of these rightswith respect to the mentally ill.
North Carolina regulates human experimentation with the men-tally ill, the retarded, and substance abusers; requires informedconsent of the patient or guardian.
North Dakota requires informed consent for participation inresearch projects. Regulates human experimentation with thementally ill and developmentally disabled; requires informedconsent of the patient or guardian and that research be in thebest interests of the patient. A court order is mandatory forpsychosurgery, sterilization, medical/behavioral research, orpharmaceutical research on resident of a facility for thedevelopmentally disabled.
Ohio regulates human experimentation with the mentally ill;requires informed consent of the patient or guardian. A court
dersor r equired for unusually hazardous treatment proceduresif the patient is legally incompetent or involuntarily committed toa mental institution.
Oregon requires informed consent for participation in researchprojects.
dRho e Island requires informed consent for participation inresearch projects.
South Carolina regulates human experimentation with thementally ill and the developmentally disabled; states thatmentally disabled patients have the right to refuse to participate.
South Dakota requires State review board and informed consentof the patient or guardian before the mentally ill may participatein research.
Texas provides that prospective subjects in human experimenta-Rtion have the right to refuse to participate.
Vermont provides that prospective subjects in human experimen-tation have the right to refuse to participate.
Vlrginia has a comprehensive statute regulating experimentationwith novel therapy on humans and research on healthysubjects. Requires IRB approval of any research with humansubjects; requirements for informed consent include an expla-nation of procedures, possible side-effects, alternative thera-pies, and subject’s right to withdraw consent at any time duringthe experiment. Specifically regulates human experimentationwith the mentally ill; experiments are limited to those that poseno hazardous risk.
Washington requires informed consent for participation in re-search projects.
Wisconsin regulates human experimentation with the develop-mentally disabled, mentally ill, and substance abusers; requiresinformed consent of the patient and his or her guardian and IRBapproval.
Wyoming requires informed consent for participation in researchProjects. Regulates human experimentation with the mentallyill; informed consent of the patient or guardian is required.
consent for research with the mentally disabled.SOURCE: Office of Technology Assessment, 1990.

116 ● Neural Grafting: Repairing the Brain and Spinal Cord
Only three States have enacted comprehensivelegislation that applies specifically to medical re-search with human subjects-California, New York,and Virginia [Cal. Health & Safety Code 24170-24179.5; N.Y. Public Health Law 2440-2446; Va.Code 37.1-234-37.1-241]. The statutes of bothCalifornia and New York affirm that human experi-mentation is vital for the benefit of humankind butrequire that it be undertaken with due respect for therights of individuals to determine what is done withtheir bodies. The New York and Virginia statutesprovide that researchers conducting experimentationin compliance with Federal regulations concerningprotection of human subjects are not subject to theState requirement. California provides that research-ers conducting investigations within institutionsreceiving Federal funding and who obtain informedconsent as required by Federal regulations areexempt from all State requirements except theprovisions requiring that the subject receive a list ofsubjects’ rights and a list of any penalties that mayattach for violation. The list of subjects’ rights doesnot include information beyond that required in theFederal regulations. As noted earlier, compliancewith Federal regulations does not render State orlocal laws inapplicable [45 CFR 46.10 l(g)]. There-fore, in States that do not make provisions for theoverriding applicability of Federal regulations, re-searchers must observe both Federal regulations andany State or local statutes or regulations.
All three of the comprehensive State statutesappear to regulate experimentation involving noveltherapy on patients as well as research on healthysubjects. Each defines human experimentation (re-search). Virginia defines “human research” as anymedical research that departs from establishedmethods using human subjects who might be ex-posed to possible injury as a consequence of theirparticipation. This appears to encompass therapeuticexperimentation. California and New York define“human experimentation” as experiments that arenot necessary for treatment nor of direct benefit tothe subject. Although these statutes appear to beaimed primarily at experimentation on healthysubjects, both include as an element of informedconsent a requirement that the individual receiveinformation concerning appropriate alternative pro-cedures. As this information would not be relevantto the subject of purely nontherapeutic experimenta-ion, it could be argued that these statutes also applyto therapeutic experimentation.
Although Federal regulations and the statutes ofCalifornia, New York, and Virginia specificallyaddress the elements of informed consent, someStates merely provide that informed consent beobtained. In all, statutes of 24 jurisdictions containprovisions requiring some kind of informed consentbefore a person may participate in a research projectas a human subject. Of these statutes, 11 apply toresearch with the mentally disabled. Eleven of theinformed consent statutes do not specify whatinformation must be provided. Many States havegeneral medical consent statutes that would apply torecipients of neural grafts. Of the remaining statutes,10 provide only that the prospective subject has aright to refuse to participate in human experimenta-tion. Four of these statutes apply only to researchwith the mentally disabled.
The California human experimentation statuteprovides fines and terms of imprisonment for anyonewho violates its requirements. Liability extends topersons who are primarily responsible for conduct-ing medical experiments and representatives oremployees of pharmaceutical companies who aredirectly responsible for contracting with the sub-jects.
Role of Institutional Review Boards
There has been concern that research proposals bereviewed in advance by groups uninvolved with theresearch project itself. This has led to the formationof IRBs to assess the ethical ramifications ofproposed research. IRB approval is necessary beforea project can receive Federal funding [45 CFR46. 103(b)]. Federal regulations and some State lawsprovide for advance review of research proposals byIRBs. This mechanism arose out of concern forthe rights of human subjects who participate inmedical research (5,53) and the fear that relyingon the investigator’s sense of professional respon-sibility was an insufficient safeguard of thesubject’s rights (45). There is an inherent conflictbetween the researcher’s goals in undertakingthe experiment (which may lead to acquisition ofknowledge, enhanced professional status, or com-mercial gain) and the patient’s rights (53). Be-cause of this conflict, it was thought necessary toensure that proposed research is reviewed by animpartial body. When functioning properly, IRBsprevent premature experimentation with humansubjects (by monitoring whether appropriatelaboratory and animal research has been con-

Chapter 7--Legal and Regulatory Issues . 117
Photo credit: Gregory Robertson, Howard University
An Institutional Review Board voting on approval of a protocol involving human subjects in research.
ducted to support the scientific design and safetyof the study) and ensure that the subject has givenfully informed consent.
Currently, the Federal Government requires thatany product for which marketing approval is soughtfrom FDA and all research involving human subjectsthat is conducted or funded by DHHS be reviewedand approved by an IRB [45 CFR 46.101-46.409; 21CFR 56.107, 56.108]. Similarly, four States—California, New Hampshire, New York, and Vir-ginia-require IRB review of any research involvinghuman subjects. Seven States and the District ofColumbia provide for IRB approval of any researchwith the mentally disabled.
Federal regulations and New York and Virginiastatutes set forth duties of an IRB, which includeevaluating risks and benefits to the prospectivesubject and ensuring that risks are outweighed bypotential benefits to the subject or by the importanceof the knowledge to be gained. An IRB must take thefollowing factors into consideration in decidingwhether or not to authorize human research:
●
●
●
●
●
●
the adequacy of the researcher’s description ofthe potential benefits and risks involved;the adequacy of the methodology of the re-search;whether any nontherapeutic research presents ahazardous risk to human subjects;whether risks to human subjects are out-weighed by potential benefits to the subjects;the adequacy of the informed consent form; andwhether the informed consent is to be obtainedby adequate and appropriate methods.
IRBs are also charged with deciding whether thepersons proposing to conduct human research arequalified and competent, and they must periodicallyinvestigate each project to ensure that it is beingcarried out according to the original proposal [N.Y.Public Health Law 2444; Va. Code 37.1-236].Figure 7-1 illustrates the procedure for obtainingIRB approval for projects involving human subjectsat one research institution.
In any IRB review, the fundamental ethicalguidelines for determining whether a therapy

118 ● Neural Grafting: Repairing the Brain and Spinal Cord
Figure 7-l—An Institutional Review Board Approval ProcessI 1 I I
Principal Investigator/ Department Chairman,Project Director + > Dean/Director
I t 1
AI
Correspondence Applications for review
reflectingBoard action
Correspondence to IRB
v r II v
I
Executive Secretaryand
Support Staff of the IRB(Assistant Dean for Research,
College of Medicine)
Pharmacy and Therapeutics
4 — — – — — – — – —+ Committee, Howard UniversityHospital
1\ \ \ \
Agenda, \ \\
Critiques and minutes, \ Hospital Director
recommendations proposals for \Howard University Hospital
review \\
E---” ‘ ‘xInstitutional Review Board --——— Medical Director
Howard University Hospital
These interactions shall occur as the need arises, such as projects involving drugs (PTC); inpatients. . Howard University Hospital (Hospital and Medical Directors); adverse reaction (Medical Director,Hospital Director, and Vice President for Health Affairs); annual reports (Vice President for HealthAffairs).
Procedure for obtaining Institutional Review Board approval currently in use at one research institution.SOURCE: Howard University, Institutional Review Board, Washington, DC.
may be experimentally used on humans is to holdeach person fundamentally entitled to respect asan individual (70) and to proceed only if there isa favorable ratio of benefits to risks (l). Specifi-cally, this standard requires a thorough assessmentof the probable outcome (in both its helpful andharmful aspects), which is weighed against theresults of not using the proposed treatment. Forexample, if a patient has a fatal disease and there areno known mitigating treatments, a therapy previ-ously untested in humans that was not likely to causeserious or lethal harm to the patient might beapproved for experimental use in the patient.
Only the Federal regulations [45 CFR 46.109; 21CFR 56.108] and the statutes of Delaware, NewYork, Missouri, and Virginia set forth the composi-tion of an IRB. Under Federal law each IRB mustinclude:
. at least five members with varyinggrounds (including racial and culturalgrounds);
. a combination of men and women;
back-back-
. a member from a nonscientific discipline, suchas a lawyer or an ethicist; and
. a member who is not otherwise affiliated withthe institution [45 CFR 46.107].
Problems may arise if members of the IRB areassociated with the institution. Such individuals maynot be able to be completely objective because oftheir identification with the researcher, their loyaltyto the institution, and the fact that any possiblesuccess may accrue indirectly to associated reviewboard members (45). One way to avoid this problemwould be to require that the IRB include as membersonly individuals who have no connection with theresearch institution. Some commentators argue thatthis proposal may promote unwarranted publicinterference with medical research (45) and thatmembership on an IRB could become a politicalappointment, which might threaten the academicfreedom of researchers (56). However, it has beensuggested that the possibility of political interfer-ence should be outweighed by the necessity forobjective input. The principle underlying IRBs isthat protection of the rights of human researchsubjects overrides the absolute freedom of the

Chapter 7&gal and Regulatory Issues . 119
researcher to perform unrestricted experimenta-tion (56).
Requirements for Informed Consent
The doctrine of informed consent is based onthe right of every individual to participate indecisions about his or her own medical care (17).Informed consent means the ‘knowing” consent ofa person or, if the person is not competent to consent,his or her legally authorized representative (24). Anindividual cannot consent to be an experimentalsubject without understanding what that may entail.Adequate informed consent requires that the re-searcher transmit to the prospective subject, inlanguage the subject can understand, any informa-tion that might influence the subject’s decision toparticipate or not participate (24).
Potential problems with attempting to convey allupdated information to subjects have been noted(69). Studies are statistically designed to havesufficient power to acceptor reject a given hypothe-sis; however, unplanned interim analyses may beinvalid and may not provide sufficient, reliableinformation. Early disclosure of benefits (or lack ofbenefits) may be unfair to patients recruited early inthe study. Such patients consent to participatewithout any preliminary data. Patients acquired afterthe study has been under way may be at a distinctadvantage if they are provided with benefits gleanedfrom data (or lack of data) derived from the earlierpatients. However, it would be reasonable to updatethe informed consent by providing informationconcerning new risks or alternative therapies (69).
Some of the likely recipients of experimentalneural grafts, persons with Alzheimer’s disease, forexample, may have impaired mental functioning,which may or may not affect their ability to giveinformed consent. Thus, it is likely that somesubjects in this field may be incapable of givingconsent for themselves (11,64,65). Various guide-lines have been suggested for research on subjectswho are incapable of consenting. There is generalagreement that such individuals should be allowedto participate in therapeutic research the intent ofwhich is to provide a health benefit to them. Withrespect to nontherapeutic research, some commenta-tors suggest that it should not be undertaken onpeople who cannot personally give valid, informedconsent (49). Others suggest that it should be
permissible to undertake important, nontherapeuticresearch on incompetent individuals, provided thereis proxy consent and there are minimal or no risks(32).
Discussion of research in the four decades sinceadoption of the Nuremberg Code has highlightedsome additional ethical concerns. The concern thatselection of subjects for research be equitable hasbeen incorporated into the Federal regulations [45CFR 46.ill(a)(3)]. For example, a particular classor race of persons should not serve as subjects forresearch that primarily benefits persons of anotherclass or race. Some commentators suggest that thisshould be particularly true in the case of subjectsincapable of consenting (e.g., research on an incom-petent, elderly subject should benefit other elderlypeople).
The adequacy of consent for experimentaltherapy raises more questions than that forproven treatment because less is known about theefficacy and risks involved in an experimentalprocedure. Although no absolute guarantee ex-ists that an established treatment will be effectiveand will cause no harm, even fewer and possiblyno guarantees exist when the proposed therapy isexperimental. Therefore, a prospective subjectmust be made aware that little is known about thepossible risks and consequences involved in partici-pation in the experiment (15). As the New Yorkhuman experimentation law provides, “Everyhuman being has the right to be protected against thepossible conduct of medical or psychological re-search on his body without his voluntary informedconsent” [N.Y. Public Health Law 2440].
Federal regulations and laws in California, NewYork, and Virginia provide that the informationgiven for proper informed consent must include thefollowing:
●
●
●
●
●
an explanation of the procedures, drugs, ordevices to be used in the experiment;a description of any possible risks and discom-forts that might be expected;an explanation of possible benefits;
a disclosure of appropriate alternative proce-dures, drugs, or devices;
an offer to answer questions that the prospec-tive subject may have concerning the experi-ment and its effect; and

120 ● Neural Grafting: Repairing the Brain and Spinal Cord
Photo credit: Gregory Robertson, Howard University
Clinical investigator counsels patient prior to obtaininginformed consent for her participation in human subjects
research protocol.
. an instruction that the individual’s consent toparticipate in the experiment maybe withdrawnat any time, without prejudice [Cal. Health &Safety Code 24172; N.Y. Public Health Law2441; Va. Code 37.10234; 45 CFR 46.116].
There is virtually no disagreement concerning therequirement of these elements for informed consent.Federal regulations require, in addition, that in-formed consent include a statement describing theextent to which the confidentiality of the subject willbe maintained, the expected duration of the subject’sparticipation, and an explanation as to whether anymedical treatments or compensation are available inthe event of injury.
When the subject is also a patient, it is importantthat a realistic assessment of the expected results ofthe therapy be provided. Patients may tend tooverestimate the benefits they will experience withan experimental treatment. To counter that tendency,it may be useful to provide information, whenapplicable, about the extent of previous research onthe experimental treatment in animals and humans.
Informed consent must also include a statement ofwhether any alternative treatments exist. The subjectshould be told if the use of the experimentaltreatment will foreclose any of those alternatives. Anexample of this would be when the subject’s diseasewill have advanced too far after he or she hasreceived experimental therapy to treat it with tradi-tional therapy (30).
The use of aborted fetal tissue for neuraltransplantation raises a unique issue about con-sent. The recipient should be told the source of the
tissue-that it was from an aborted fetus-since thatinformation may be material to the recipient’sdecision whether or not to consent to the transplant(57). Another commentator goes further, stating thatdisclosure should be made concerning all animalsused in preclinical studies (10).
There are concerns about what should happen ifthe human subject is harmed in the study. Accordingto Federal regulations and California law, the subjectshould be given an explanation of the availability ofmedical therapy in case of injury incurred as a resultof the experiment [45 CFR 46.116(a)(6); 21 CFR50.25(a)(6); Cal. Health & Safety Code 24172(f)]. Ifcompensation for research injuries is not providedfor, the prospective subject should be so informed.If a subject has not been specifically informed thathe or she bears the financial cost of potentialphysical injury, the informed consent is, arguably,not complete (53).
Research subjects must also be given an assurancethat they are free to refuse to participate or towithdraw their consent at any time and to discon-tinue participation in the project without penalty orloss of benefits to which they are otherwise entitled[45 CFR 46.116(a)(8); 21 CFR 50.25(a)(8)]. Allethical codes stipulate that subjects must be able towithdraw from an experimental project at any time,without prejudice or penalty (30). The right towithdraw is derived from the premise that thesubject is doing something for the benefit of othersand that such acts are generally not obligatory (30).
If researchers do not provide adequate informa-tion to a subject before the study is undertaken, theycan be sued for damages if harm results (26). Inaddition, physician-researchers who do not obtaininformed consent may be disciplined for unprofes-sional conduct. In the Jewish Chronic DiseaseHospital case, 22 debilitated patients were injectedwith live cancer cells without first having given theirinformed consent (45). The Attorney General ofNew York brought an action against the principalinvestigators to the Board of Regents DisciplineCommittee, which found the doctors guilty of fraud,deceit, and unprofessional conduct. The doctorswere punished, not because they performedexperiments that resulted in harm to the patients,but because they did not obtain informed consentbefore proceeding. California law also providespenalties for violation of the informed consentprovision, including damages up to $1,000 for

Chapter 7--Legal and Regulatory Issues . 121
negligent failure to obtain informed consent, dam-ages up to $5,000 for willful failure to obtaininformed consent, and damages up to $10,000 andup to 1 year in jail for willful failure to obtaininformed consent that exposes the subject to sub-stantial physical or psychological risk. Additionalprotections are provided regarding drug companies.A representative or employee of a pharmaceuticalcompany who knows of substantial physical orpsychological risks of an experiment and does notdisclose them can be imprisoned for up to a year andfreed up to $10,000 [Cal. Health & Safety Code24176(a)].
Handling of Grievances and NonreleaseFrom Liability
The California statute provides a grievance mech-anism for patients when an experiment goes awry. Itrequires that the subject be given the ‘‘name,address, and phone number of an impartial third-party, not associated with the experiment, to whomthe subject may address complaints about theexperiment” [Cal. Health & Safety Code 24173(c)(lo)].
Like the Federal regulations [45 CFR 46.116; 21CFR 50.20], the statutes in California, New York,and Virginia provide that any attempted or purportedwaiver of an individual’s legal rights is void. TheNew York and Virginia statutes state that it isimpermissible to release any individual, institution,or agency and any agents thereof from liability fornegligence [Cal. Health & Safety Code 24176; N.Y.Public Health Code 2442; Va. Code 37.1-235].
Protections for Particularly Vulnerable Subjects
Some statutes and regulations cover research onparticularly vulnerable groups, for example childrenor the mentally disabled. Statutes concerning re-search on the mentally disabled may be relevant toexperimental neural grafts into subjects with disor-ders that affect their mental functioning. Federalregulations provide that IRBs shall add appropriateadditional safeguards if the potential subjects sufferfrom acute or severe physical or mental illness [45CFR 46.ill(b)]. Although the regulations do notdescribe what these additional protections might be,NIH has introduced guidelines covering intramuralresearch (20). The guidelines include a procedure forobtaining proxy consent as well as additionaloversight for research that involves more thanminimal risk. The guidelines prohibit research of
more than minimal risk if the patient is incapable ofchoosing a proxy decisionmaker and has no next ofkin to seek court-appointed guardianship.
Twenty-five States and the District of Columbiaspecifically regulate experimentation on the men-tally disabled (see table 7-l). Other States regulateexperimentation on residents of nursing homes [Mo.Ann. Stat. 198.088(l)(b)(c); Or. Rev. Stat. 441.385].The abundance of State legislation reflects a generalconcern that institutionalized persons are frequentlyused as experimental subjects because they are“administratively convenient” to the researcher(30) and that they are often taken advantage of,either because of their mental deficiencies or theirguardians’ lack of interest in their welfare (2). ThatState laws tend to pay close attention to the issue ofinformed consent for mentally ill patients is due toconcerns not only about voluntariness, but alsoabout the capacity of these persons to comprehendinformation (76).
Of the 25 jurisdictions that provide statutoryguidelines for experimentation on the mentallydisabled, 14 States and the District of Columbiarequire that informed consent of the patient orpatient’s guardian be obtained. Kansas and Wiscon-sin require informed consent of both the mentallydisabled person and the guardian [Kan. Stat. Ann.59-2929(6); Wise. Stat. Ann. 51.61]. Five Statesprovide only that mentally disabled patients have theright to refuse to participate in experimentationprojects.
In some States, the permissibility of research onmentally disabled individuals turns on both itspurpose and its level of risk. At least two States,Alaska and Virginia, limit experimentation on thementally deficient to that which poses no hazardousrisks. These statutes authorize an administrator todetermine what procedures are both experimentaland risky. Four States, California, Missouri, NewJersey, and North Dakota, require that the researchbe intended to benefit the mentally ill subject. Asimilar approach, with more stringent provisions, istaken by the Delaware statute, which prohibits theparticipation in experimental research of mentally illpersons who are incapable of giving voluntaryconsent-except under the following circumstances[Del. Code Ann. Tit. 16,5172, 5175]:
. an attempt to obtain informed consent from thepatient has failed;

122 ● Neural Grafting: Repairing the Brain and Spinal Cord
no other therapy exists or the patient has notresponded to accepted therapies;the research would be in the best interests of thepatient; andthe waiver has been approved by the IRB andthe patient’s legal guardian or next of kin.
proposed waiver must then be approved by acourt, which may deny approval for any reason itdeems appropriate.
Other statutes specify a particular review mecha-nism that must be followed. Six States require priorreview and approval of any research projects by anIRB, while three jurisdictions require review andapproval by State boards before experiments areconducted on mentally disabled persons. Florida,New Jersey, North Dakota, and Ohio require somesort of judicial determination of the necessity of anexperimental procedure before it maybe used on anincompetent person. Florida, New Jersey, and NorthDakota require that the patient be physically presentat such a judicial hearing, represented by counsel,and provided the right and opportunity to confrontand cross-examine witnesses. These three Statesalso place the burden of proof on the party allegingthe necessity of the treatment.
FDA Regulation of Neural Grafting Materials
Neural grafting presents a number of issues forwould-be recipients. A potential patient might beconcerned about what material is to be grafted intohis or her brain and whether that material is safe andeffective. These issues are likely to come within thejurisdiction of the FDA. Any description of theFDA’s role in regulating the safety and efficacy ofneural grafting materials is complicated by the factthat there are several different types of materials,each of which raises slightly different questions. Inaddition, neural grafting materials (and materialsthat could potentially be used for neural grafts)represent developing technologies that have not yetbeen directly addressed by the FDA. A finalcomplicating factor is the developing nature of FDApolicies for the regulation of biological products thatmay be analogous to neural grafting materials andthe resulting lack of published regulations or deci-sions in this area.
The FDA is responsible for regulating the distri-bution of drugs and devices under the Federal Food,Drug, and Cosmetic Act (FFDCA) [21 U.S.C. 321 etseq.] and has been delegated authority to regulate the
commercial distribution of biologics under thePublic Health Service Act (PHSA) [42 U.S.C. 262].In addition, the Coordinated Framework for theRegulation of Biotechnology [49 FR 50856; 50 FR47174; 51 FR 23302] delegated authority for theregulation of human drugs, medical devices, andbiologics produced by biotechnology to the FDA. Asdescribed in chapter 4, materials used in neuralgrafting are varied and may come from varioussources. Neural grafting ranges from implantingtissue obtained from the patient’s own body toimplanting genetically engineered cells from a cellline developed and maintained in a laboratory. Therisks inherent in using each type of material have yetto be assessed by the FDA, but it is possible tooutline the issues that the agency is likely toconsider, based on its statutory mandate, existingregulations, and decisions with respect to similarmaterials.
Neural grafting materials present challenges at thecutting edge of developing FDA policy becausethese materials are sometimes analogous to tissuetransplants and sometimes to products of geneticengineering. The principal questions regarding neu-ral grafting materials are:
● Is the FDA likely to regulate the manufactureand distribution of the product?
● If the answer to the first question is yes, will theproduct be regulated as a drug, device, orbiologic?
FDA jurisdiction with respect to drugs, devices,and biologics is described below. Areas in which thelaw is unclear as it may apply to neural graftingmaterials are described, and issues in the potentialregulation of specific types of neural grafts arepresented.
FDA Jurisdiction
Drug—The FFDCA defines “drug” in part as“articles intended for use in the diagnosis, cure,mitigation, treatment, or prevention of disease inman. . .’ and ‘articles (other than food) intended toaffect the structure or any function of the body ofman . . . but does not include devices or their com-ponents, parts, or accessories” [21 U.S.C. 321(g)(l)]. The classification of a product is thus based inpart on the use intended by the manufacturer. Aproduct may not be classified as both a drug and adevice, but it maybe regulated as both a drug and abiologic. The Supreme Court has sustained the

Chapter 7--Legal and Regulatory Issues ● 123
Photo crsdit: Food and Drug Administration
FDA’s authority to interpret the FFDCA’S defini-tions broadly, in view of the broad public healthobjectives of the legislation (60).
Device—The term “device” is defined in theFFDCA as “an instrument, apparatus, implement,machine, contrivance, implant, in vitro reagent, orother similar or related article. . . which is . . . in-tended for use in the diagnosis of disease or otherconditions, or in the cure, mitigation, treatment, orprevention of disease” or which is “intended toaffect the structure or any function of the body” and“which does not achieve any of its principalintended purposes through chemical actions withinor on the body” and “which is not dependent onbeing metabolized for the achievement of any of itsprincipal intended purposes” [21 U.S.C. 321(h)].
The items listed as devices in the statute implythat Congress intended the term to refer to man-made products. Aside from implants and in vitroreagents, the items in the list are synthetic productsthat are generally made of materials such as metal orplastic. The legislative intent underlying the defini-tion of device is probably limited to artificialimplants (66). Some products that may otherwise fitthe definition of drugs or biologics are regulated asdevices because they are considered accessories toor components of a device. A product may beclassified as both a biologic and a device.
Biologic—The law that authorizes Federalregulation of biological products for human use wasenacted in 1902 and was revised in 1944 as part ofthe recodification of the PHSA, (now codified at 42U.S.C. 262) (39). The PHSA establishes require-ments for ‘‘any virus, therapeutic serum, toxin,
32-801 0 - 90 - 5 : QL 3
antitoxin, vaccine, blood, blood component or deriv-ative, allergenic product, or analogous prod-uct . . . applicable to the prevention, treatment, orcure of diseases or injuries of man” [42 U.S.C. 262].At present, the scope of the term “analogousproduct” is unclear. It has not been extensivelyreviewed by the courts (71), nor did Congress clarifythe term in 1970, when, in response to conflictingpositions by the courts on whether blood was ananalogous product, it amended the PHSA to specifi-cally include blood, blood components or deriva-tives, and allergenic products [Public Law 91-515].It is therefore unclear whether courts woulduphold FDA regulation of neural grafting materi-als under the PHSA without the enactment ofspecific language to add such materials to thestatute.
The initial question, then, in determiningg whetherthe FDA has jurisdiction to regulate neural graftingmaterials is whether a particular material meets thedefinition of a drug, device, or biologic. All biol-ogics are considered either drugs or devices as wellas biologics (71). However, an article proposed foruse as a neural graft cannot simultaneously be botha drug and a device. The question of how tocategorize neural grafting materials will be consid-ered further later in this chapter.
FDA Regulation of Safety and Efficacy
The FDA regulates product safety and efficacyin a number of ways. Under the FFDCA, a drug ordevice is deemed to be adulterated if it consists of afilthy substance or if it has been prepared underunsanitary conditions such that it may have been
contaminated with filth or rendered injurious tohealth. Drugs and devices are considered adulteratedif the methods used in manufacturing, storing, orpacking them do not conform to current goodmanufacturing practice or if the container is made ofa substance that may render the contents injurious tohealth. Drugs are also adulterated if their strength,purity, or quality is less than is represented [21U.S.C. 351].
A drug or device is misbranded [21 U.S.C. 352] ifits labeling is false or misleading or if adequatedirections for use or adequate warnings againstunsafe use are omitted from the label. Any drug ordevice is misbranded if it is dangerous to healthwhen used in the dosage or manner or with thefrequency or duration described in the labeling.

124 . Neural Grafting: Repairing the Brain and Spinal Cord
Owners or operators of establishments for themanufacture, preparation, propagation, compound-ing, or processing of drugs or devices must registerall places of business with the FDA [21 U.S.C. 360]in order to facilitate inspection and enforcement ofFDA regulations. Several types of operations areexempted from the registration requirement. Theseinclude pharmacies dispensing prescription drugs ordevices on prescriptions of licensed practitionersprescribing for patients in the course of professionalpractice [21 U.S.C. 360(g)(l)], practitioners li-censed by law to administer drugs or devices andwho manufacture these items solely for use in theirprofessional practices [21 U.S.C. 360 (g)(2)], andpersons who make the products solely for use inresearch, teaching, or chemical analysis and not forsale [21 U.S.C. 360 (g)(3)].
Premarket approval of a new drug application(NDA) is required for new drugs [21 U.S.C. 355]. A“new drug” is one that is not generally recognizedby qualified experts as safe and effective for useunder the conditions prescribed in the labeling [21U.S.C. 321(p)(l)]. An application for premarketapproval (PMA) is required for some devices [21U.S.C. 360(e)], but all manufacturers of devices arerequired to at least notify the FDA 90 days beforeintroducing a device into the market [21 U.S.C. 360(k)].
An exemption from premarket approval may beobtained for shipment of products intended solelyfor investigational use by filing an investigationalnew product application. This submission is eitheran investigational new drug application (IND) [21U.S.C. 355(i); 21 CFR Part 312)] or an investiga-tional device exemption [21 U.S.C. 360(j)(g); 21CFR Part 812]. The FDA reviews the submission toprotect the safety of investigational subjects and toensure that the research design is adequate for thepurpose of testing safety and effectiveness in theevent that an NDA or PMA is filed. The study mustbe approved by an IRB in each institution or area inwhich the drug or device will be tested.
The FDA requires manufacturers of approveddrugs and devices to make prompt reports of adverseevents and periodic reports on safety and effective-ness [21 CFR 314.80, 314.81, and part 803] after theproducts have been distributed for use.
Biologics are subject to all of the FFDCArequirements listed above except the premarketapprovals. Instead of an NDA or PMA, both
biologics and the establishments that produce themmust be licensed (product and establishment li-censes are required prior to marketing). In addition,biologics are regulated for false labeling under thePHSA [42 U.S.C. 262(b)].
The FDA can enforce its requirements in a varietyof ways. Administrative mechanisms includeinspections to monitor compliance, revocation ofapproved marketing applications (NDA, PMA, orproduct licenses), and recalls. Judicial actions thatmay be sought by the FDA include seizures ofadulterated, misbranded, or unapproved drugs ordevices (including biologic), injunctions againstshipping, and criminal prosecutions (71).
Possible Limits on the FDA’sRegulatory Authority
Two legal concepts, interstate commerce andthe practice of medicine, may limit the FDA’sjurisdiction over some types of neural graftingmaterials. Arguments on both sides of each conceptare summarized here, although the courts havegenerally allowed the FDA broad authority to carryout its statutory mandates. The success of thearguments outlined below will depend, however, onthe facts and circumstances of the cases in whichthey may arise.
Interstate Commerce-One argument againstFederal regulation is that if the material is producedand distributed within a State, the interstate nexusrequired for Federal regulation does not exist. Forexample, cells obtained from one patient that arecultured and then grafted into the brain of anotherpatient within the same hospital do not appear to beinvolved in interstate commerce.
The FDA has successfully mounted several argu-ments that enabled it to regulate products that werenot shipped interstate. First, some of the statutoryrequirements for drugs, devices, and biologics do notrequire the showing of an explicit interstate nexus.Examples of these are registration of producers ofdrugs and devices [21 U.S.C. 360] and regulation offalse labeling of biologics [42 U.S.C. 262(b)] (61).In addition, the Medical Device Amendments of1976 [Public Law 94-295] authorize seizure ofmisbranded or adulterated devices without proof ofinterstate commerce (39).
A second argument used successfully by the FDAhas been that if a component of the drug travels ininterstate commerce, the interstate nexus has been

Chapter 7--Legal and Regulatory Issues ● 125
satisfied. An analogous argument could be madeabout the solutions in which tissues are preserved orthe petri dishes or media in which cells are cultured.
Finally, section 361 of the PHSA [42 U.S.C. 264]authorizes the Surgeon General, with the approval ofthe secretary of DHHS, to make and enforceregulations to prevent the transmission or spread ofcommunicable diseases. This authority has beendelegated to the Commissioner of the FDA forfictions related to FDA-regulated products [21CFR 5.10 (a)(4)]. The power of the FDA to ban theintrastate sale of small turtles in order to prevent theinterstate spread of Salmonella was upheld pursuantto this provision in State of Louisiana v. Mathews(58). The FDA also relied on section 361 as aprimary source of statutory authority to regulateblood in intrastate commerce in order to prevent thespread of syphilis, hepatitis B, and HIV (71).
Practice of Medicine--Traditionally, the FDAhas not interfered with the practice of medicine. TheFDA does not regulate the use by physicians ofapproved drugs for unapproved purposes (62,72),and physicians practicing medicine are specificallyexempted from the registration requirement imposedby the FFDCA [21 U.S.C. 360(g)(l)(2)]. The newtechnologies involved in neural grafting presentdifficult questions of what constitutes the practiceof medicine, whether there are circumstancesunder which the FDA would decide to regulatewhat might be called the practice of medicine,and the circumstances, if any, under which FDAjurisdiction to do so would be upheld.
The traditional exemptions serve several pur-poses. Approved drugs are presumably safe whenreasonable doses are prescribed and contraindica-tions are observed. In fact, the freedom of physiciansto prescribe as they see fit can lead to the discoveryof important new uses for existing products. TheU.S. District Court in United States v. Evers,concerned about regulation of the intrastate practiceof medicine, stated that restricting the medicalprofession (here a licensed physician) from using adrug for a purpose not contraindicated on the labelwould exceed the powers of Congress (62). Thecourt opined that malpractice claims provide appro-priate protection for the patient. Another reason forthe traditional exemption of the practice of medicinemight be the difficulty of trying to regulate thepractices of individuals relative to the ease ofregulating manufacturers, who are likely to be
shipping large quantities of products in interstatecommerce. Finally, the fact that the practice ofmedicine usually overlaps the issue of intrastatecommerce (because physicians have generally prac-ticed on patients within their States) may haveinfluenced the position of the FDA with respect toindividual practitioners.
Neural grafting materials and other tissues orproducts of biotechnology raise new questionsabout FDA regulation and the boundaries of thepractice of medicine. What is the boundarybetween product and process? For example,should the safety and efficacy of neural graftingbe seen as a function of the quality of the graftingmaterial, the storage of the material (e.g., tissuebanking), or the grafting process? Is the graftingprocess the practice of medicine? If so, will theFDA regulate the process?
In practice, the decision to regulate will probablydepend on the perceived dangers of the product. Forexample, concern about HIV infection throughblood products led to an innovative process for theregulation of blood banks. At the Federal level,blood is regulated as a service rather than a product.This has the effect of decreasing the liability ofblood banks and hospitals from strict liability for adangerous material to malpractice liability for negli-gence. Some persons believe that tissue banksshould be similarly regulated.
Genetically engineered materials present the op-tion of customized biologics, or therapeutics tailoredto each individual patient (34). This is a verydifferent situation from that of traditional biologics,such as vaccines, which were produced in largequantities and distributed to large portions of thehealthy population in order to prevent disease. Cells,for example, might be genetically engineered in alaboratory at the same hospital where they will begrafted into the patient. Is this the practice ofmedicine? The label “practice of medicine” doesnot necessarily preclude FDA regulation. Rather, itindicates a gray area in which the FDA may findenforcement difficult and physicians may protestregulation. Products of biotechnology such as genet-ically engineered cells present safety hazards unlikethose of traditional drugs or biologics. Manufactur-ing problems include difficulty in product character-ization and potency, nonreproducible products,difficulty with product stability, and the presence ofadventitious agents and contaminants (intrinsic and

126 . Neural Grafting: Repairing the Brain and Spinal Cord
acquired). Scientific problems include the absenceof feasible animal models for preclinical testing forsafety, efficacy, or both (38).
The problems outlined above present both areason for the FDA to be concerned about thesafety of neural grafting materials derived frombiotechnology and a challenge to its presentregulatory scheme. The development of theseproducts and their use by physicians may present achallenge to the traditional exemption of the practiceof medicine from FDA regulation.
Regulation of Neural Grafting Materials
The principal questions with respect to FDAregulation of materials used in neural grafting are:
● Will FDA regulate the material?. If so, how will the material be categorized
(drug, device, or biologic)?
The decision as to whether the FDA willregulate neural grafting materials dependslargely on whether the FDA determines that theproduct fits within the statutory definition ofdrug, device, or biologic. Another consideration iswhether the FDA has reason to be concerned aboutthe safety of the material. Finally, the question ofwhether or not the product is intended for commer-cial distribution may be relevant. The terms of thePHSA are “sale, barter or exchange” [42 U.S.C.262], which may allow for regulation even wherecommerce is not involved. As described earlier, theCommissioner of the FDA is empowered to promul-gate regulations to prevent the transmission orspread of communicable diseases, without regard tointerstate commerce [21 U.S.C. 264].
The second question is how neural graftingmaterials will be categorized. At present, there areno published regulations to help answer this ques-tion. The FDA has issued “Points to Consider” formanufacturers of exvivo-activated mononuclear leu-kocytes and for cell lines used to produce biologics.Points to Consider do not have the force of law, nordo they represent formal FDA policy, but they doindicate the current thinkin“ g of scientists at the FDA.Points to Consider for somatic cell therapy are likelyto be relevant to neural grafting materials, but theyhave not yet been approved for distribution by theFDA. Tissue products and products of biotech-nology are regulated on a case-by-case basis in orderto allow flexibility with respect to new technologies.
Decisions about whether a given product is a drug,device, or biologic and which administrative centerat the FDA will regulate it depend on the intendeduse of the product, who in the agency has therequisite expertise, and what analogous products areregulated in each center. This means that thesituation will change as similar materials are regu-lated, making it impossible to predict with confi-dence how neural grafting materials will be regu-lated by the time they are actually considered by theFDA. As more tissue and biotechnology productsare developed and regulated by the FDA, however,the agency could develop consistent regulations, asit did for blood products. As mentioned earlier, it isunclear whether a court would find neural graftingmaterials ‘analogous’ to blood products and there-fore subject to regulation under the PHSA withoutthe enactment of more specific statutory language.
There are many different types and sources ofneural grafting materials (see ch. 4). The followingclassification scheme will be used here to describethe issues the FDA is likely to consider in decidingwhether and how to regulate these materials:
●
●
●
●
autografts of tissue,allografts of tissue or cultured cells,autografts of genetically engineered cells, andgenetically engineered cells distributed to pa-tients.
The discussion which follows is subject to thecaveat that there are no formal regulations specifi-cally describing the role of the FDA with respect tothese materials. Considerations that are salient todaycould become less important by the time the FDA isactually confronted with the need to regulate neuralgrafting materials.
Autografts of Tissue—This refers to tissue ob-tained from the patient’s own body (e.g., the adrenalmedulla) and grafted into his or her brain. Thismaterial is least likely to be regulated by the FDAbecause there is minimal manipulation of the tissue,there is no increased risk of transmission of commu-nicable disease, and the procedure is within thetraditional practice of medicine. The FDA does not,for example, currently regulate bone marrow auto-grafts.
Allografts of Tissue or Cultured Cells—Thesource of this same-species graft material could be,for example, fetal tissue or cells from anotherperson. This category is a gray area in which it is

Chapter 7-Legal and Regulatory Issues ● 127
unclear what the FDA will decide. The FDA islikely to want to regulate for safety purposes (e.g., toprevent the spread of communicable diseases such asHIV infection). The considerations here could beanalogous to those surrounding blood banks, leadingto regulation of tissue banking and distribution.
The FDA has recently decided to regulate im-plants of dura mater, the tough, outer membranecovering the brain and spinal cord, because ofconcern about the possible transfer of Creutzfeldt-Jacob disease or human retroviruses. Dura mater isregulated as a device because it does not achieve anyof its principal intended purposes through chemicalactions within or on the body or through metabolism.To the extent that tissue grafts for mitigation ofParkinson’s disease are intended to act by releasing
dopamine, they are more likely to be regulated asdrugs than as devices. Tissue grafts used to patchinjured neural systems may be more analogous todura mater and therefore regulated as devices.Similarly, certain cell lines that are cultured in vitroand used for skin transplantation and in wound andburn therapy are regulated as medical devices (74).This suggests that cell lines used as neural graftingmaterial for the purpose of mechanically bridgingthe traumatized or injured central nervous systemcould be regulated as devices. It is most likely,however, that such cell lines would be consideredbiologics, because the neural bridging function isdependent on the biological activity of the cells (75).
Cells that are cultured, modified, or otherwiseexpanded in vitro are regarded by the FDA asbiological drugs and are believed to be subject toregulation under the PHSA (74). The regulatorystatus of in vitro-cultured cells that are not shippedin interstate commerce is not clear, but in mostinstances such cells are administered with investiga-tional biologics, necessitating an IND application(74). If an investigator were to produce cells withoutadditional investigational agents, the role of theFDA in regulating the therapy under the INDregulations would be less clear (73).
Autografts of Genetically Engineered Cells—Cells that are prepared by a patient’s personalphysician for infusion back into the same patientmay be considered “practice of medicine” andtherefore may not be subject to FDA regulation (74).However, safety issues arise in therapies that make
use of genetically engineered cells because of theunknown effects of the foreign genetic material onthe patient and persons in contact with the patient(74). In addition, cells may synthesize a drug orbiologic. The FDA might therefore choose to assertjurisdiction despite the practice of medicine issue. Aclinical trial begun under an IND at NIH recently seta precedent for FDA regulation of an autograft ofgenetically engineered cells. The FDA is concernedthat when using a virus there is a small chance ofrecombination with a virus already existing in thebody (25).
Genetically Engineered Cells Distributed toPatients-This category includes cells from animalsor humans other than the patient which are engi-neered and then grafted into the patient. Given thesafety considerations and the precedent estab-lished for autologous grafts of engineered cellsdescribed above, it is likely that the FDA wouldseek to regulate engineered cells in wider distri-bution.
Regulation of New Surgical Procedures
The previous section described briefly the com-plex regulatory scheme developed by Congress andthe FDA as it might apply to neural graftingmaterials. That intricate system of regulation toensure the safety and efficacy of articles intended foruse in the diagnosis, treatment, or prevention ofdisease in humans contrasts sharply with the absenceof any direct Federal regulation of new surgicalprocedures developed for the same purposes.1
Whether considering biomedical articles or proce-dures, the problem is whereto draw the line betweensafety and efficacy, on the one hand, and encourage-ment of biomedical innovation, on the other.
This section describes the implications of theabsence of direct Federal oversight for the develop-ment of neural grafting procedures. Indirect mecha-nisms for regulating new surgical procedures areoutlined, and a mechanism for potential Federalinvolvement in the assessment of safety and efficacyof new surgical procedures is described. The intentis to describe the current situation and ways in whichit could be modified, if that is deemed desirable.
While Congress and the FDA have recognizedthe need for careful consideration before movingfrom animal studies to controlled clinical trials
l~s swtion is con~rned with new surgical procedures that are not part of federally funded research.

128 ● Neural Grafting: Repairing the Brain and Spinal Cord
involving gradually increasing numbers of pa-tients for assessment of new products, there is noanalogous regulation of the move from animalstudies to human trials for surgical procedures.An IRB will only approve protocols that demon-strate some hope of benefit to the subject and theabsence of long-term negative effects, but there areno specific criteria for moving from animalstudies to human research.
Of the neural grafting procedures, only techniquesmeant to alleviate the symptoms of Parkinson’sdisease have progressed to human trials. Grafts oftissue from a patient’s adrenal medulla have beenperformed for Parkinson’s disease patients in Swe-den, Mexico, China, Canada, England, Spain, Portu-gal, Cuba, Colombia, Chile, and the United States.Implants of human fetal tissue have been per-formedin Sweden, Mexico, England, Spain, Cuba, China,and the United States (18). A few studies have beendone privately in the United States despite the ban onfederally funded transplantation research that usesfetal tissue obtained from induced abortions. Al-though these trials are already under way, debatecontinues as to whether the results of animal studiesjustify them. Some believe that animal research hasalready produced sufficient information to justifylimited human trials. In the words of one scientist,‘‘animal research is the key to initial understandingand refining techniques, but never solves all theproblems” (4).
Persons who question the wisdom of advancing tohuman neural grafting trials at this stage of researchquestion whether the animal (and the few human)trials that have been done provide evidence of theabsence of long-term adverse immunological effectsor the presence of beneficial effects. Others argueagainst progressing with human trials on the groundsthat no one has been able to identify the etiology ofParkinson’s disease and it is therefore not knownwhether the same disease processes that caused theinitial neuron degeneration could also producedegeneration of grafted neurons (23). A neurologistwho has used the procedure and identified adverseside-effects stated: ‘‘This is an area in which we’vedone too much too fast” (40). A neurobiologistadvised even greater caution: “I’m not convincedthe procedure is ready for humans. . . if we moveahead too soon, the results can be overinterpreted”(40).
While well-controlled human research usingmethods such as randomized clinical trials is essen-tial to the development of new drugs, the feasibilityand utility of such methods for evaluating theefficacy of new surgical procedures is controversial.Some surgeons argue that surgical procedures differfrom drugs in ways that render the results ofrandomized clinical trials of surgical proceduresuseless, if not harmful, to the development ofsurgical treatments (8, 9, 68). The outcomes ofsurgical procedures, according to this view, are sodependent on the skill and experience of theindividual surgeon and the circumstances of theindividual patient that research which generalizesacross patients and physicians will be meaningless.Other physicians and surgeons believe that con-trolled clinical trials are important for determiningwhether an innovative surgical therapy is of value (6,31) and when an accepted surgical procedure ofunproved value should be discontinued (21).
The absence of well-controlled clinical studiesand of standards for deciding when to move fromanimal to clinical studies may lead to severalproblems. First, physician-investigators may beencouraged to take large risks in order to be amongthe first to perform new surgical procedures. Thisencouragement takes the form of publicity, funding,and professional attention for bold new efforts tosave lives. While the surgeon may risk his or herprofessional reputation, the greater risks are to thepatient, who may not be able to give truly informedconsent because of the combination of chronic orterminal illness and lack of information aboutbenefits and risks of the new surgical procedure. Thephysician and patient may believe that any proce-dure is better than certain death or prolonged, severedisability, even if the benefits and risks of theprocedure are unknown. This logic was used tojustify liver transplantation in 1983, before therewere adequate data supporting its efficacy (51). Inthe absence of well-controlled clinical trials, proce-dures may be widely accepted clinically even if theyare not actually effective.
A study of the introduction of four new surgicalprocedures found that, with the exception of oneprocedure which was evaluated through the FDAdrug approval process, the procedures were intro-duced without controlled clinical trials or well-designed observational studies (12). This means thatthe procedures which were performed did notcontribute to an overall evaluation of their efficacy

Chapter 7&gal and Regulatory Issues ● 129
and that future patients will not have adequateinformation on which to base their decisions abouttreatment. In addition, when effectiveness is still inquestion, tension is likely to develop about theextremely high costs of some new surgical proce-dures (51).
A three-stage procedure for the evaluation of newsurgical procedures has been suggested (12). First,the physician-investigator should develop the newprocedure and define diagnostic criteria to evaluateit. The second stage would be collaborative clinicaltrials in which formal research protocols are fol-lowed and quantitative evidence is collected andanalyzed according to predetermined statistical cri-teria. Finally, after efficacy is established, theprocedure could be released for more general use.
Indirect Regulation of New Surgical Procedures
New surgical procedures are regulated indi-rectly by third-party payers, which decidewhether or not to reimburse for them. The numberof patients who undergo a procedure is determinedin part by the extent to which coverage is providedby insurers. Federal insurers of medical care includethe Health Care Financing Administration, Depart-ment of Veterans Affairs, and the Department ofDefense. Safety and efficacy determinations aresometimes part of the process by which insurersdecide whether a surgical procedure is experimentalor accepted treatment and, ultimately, whether theywill cover the procedure. Discussion of the means bywhich each Federal and private insurer assessessafety and efficacy in the course of deciding thestatus and coverage of procedures is beyond thescope of this report. The very different processes bywhich decisions were made about the status of liver,kidney, and heart transplantation have been de-scribed (51).
Other forms of indirect regulation of surgicalpractice include hospital standards set by the JointCommission on Accreditation of Healthcare Organi-zations, professional standards of practice fromspecialty societies, State licensing laws, and medicalmalpractice claims. IRBs exert the most directcontrol over research on new surgical procedures.While research protocols are often submitted tolocal IRBs, there is no Federal requirement thatthis be done unless the research receives Federalfunding or takes place as part of an FDAapplication. In addition, IRBs will have difficulty
evaluating a protocol in the absence of risk-benefitinformation.
Potential Federal Role
Concern about rising health-care costs and thesafety and efficacy of new medical procedures hasled to increasing congressional interest in theevaluation of such procedures. While direct regu-lation of the practice of medicine may strain theregulatory authority of the FDA, the FederalGovernment could play a role in the evaluation ofnew procedures and could promulgate standardsof practice for purposes of consumer informationand decisionmaking by physicians and third-party payers.
Neural grafting may eventually be considered asa treatment for some debilitating neurological disor-ders that affect large numbers of vulnerable patientswith chronic or terminal illnesses. It is essential,therefore, that the clinical development and use ofthe procedures be based on well-controlled researchon safety and efficacy rather than on desperate hopesof cures for these patients. The methods of assessingthe safety and efficacy of liver transplants prior to1984 (51) are a model of what to avoid in assessingnew surgical procedures.
The newly created Agency for Health Care Policyand Research [Budget Reconciliation Act of 1989,Public Law 101-239, sec. 6103] is charged withpromoting research on selected surgical proceduresin order to assess their appropriateness, necessity,and effectiveness. This agency could be chargedwith assessing the development of clinical neuralgrafting procedures, still in their infancy, to ensurethat the use of these procedures develops in accor-dance with data from well-controlled studies, ratherthan in response to factors external to the actualefficacy of the procedures.
PROTECTION OF DONORS OFFETAL TISSUE
Since embryos and fetuses are among the pro-posed sources of tissue for neural grafts (23), Federalregulations and State laws governing embryo andfetal research may apply. Some of these laws appearto be sufficiently restrictive to forbid experimentaltransplants using fetal tissue in certain States.However, if neural grafting becomes standard medi-cal therapy, current embryo and fetal research lawswould no longer prohibit the procedure. In legal

130 ● Neural Grafting: Repairing the Brain and Spinal Cord
contexts, the term ‘‘embryo’ has been used to referto the conceptus from fertilization until the end ofthe eighth week, and the term ‘fetus” has been usedto refer to the conceptus in all stages of development.
The use of fetuses as a source of tissue forneural grafts raises complicated issues. In mostinstances, the tissue will come from fetal cadavers,although the tissue itself may still be living. Abor-tuses of between 8 and 12 weeks’ gestation arepresently considered appropriate sources of tissuefor grafting. However, there may also be instances inwhich physicians intend to remove tissue from live,nonviable fetuses (fetuses incapable of survivingoutside the womb). Moreover, some experimentalinterventions might involve the pregnant womanand her living, in utero fetus; for example, a womanmight be asked to undergo an alternative abortionprocedure in order to better preserve fetal tissue orto postpone the abortion until the fetus is moredeveloped (36). Different laws will apply, depend-ing on whether the fetus is dead, alive ex utero, oralive in utero and depending on whether the experi-ment presents risks to the pregnant woman as well.
Photo credit: National Institutes of
Further issues are raised regarding maternalconsent. These center on whether a pregnant womanshould have the right to prohibit or authorize the useof her fetus for experimentation. Some laws addressthis issue, as well as the role of the father in theconsent process. An additional issue addressed byfetal research laws is whether women should beallowed to receive payment for fetal tissue. Somelaws banning compensation would extend to pay-ment of third-party intermediaries as well.
Development of Federal Policy onFetal Research
Federal activity with respect to the issue of fetalresearch has been extensive. In 1974 Congresspassed the National Research Act [Public Law93-348]. This legislation established the NationalCommission for the Protection of Human Subjectsof Biomedical and Behavioral Research, whose firstcharge was to investigate the scientific, legal, andethical aspects of fetal research. The statute prohib-ited all federally funded nontherapeutic research onfetuses prior or subsequent to an abortion until the

Chapter 7--Legal and Regulatory Issues . 131
Commission made its recommendations and regula-tions were adopted. In 1975 the Commission madeits recommendations (46), and in 1976 the Depart-ment of Health, Education, and Welfare (now theDepartment of Health and Human Services) adoptedregulations for the Federal funding of fetal research[45 CFR 46.201-211]. Under these regulations,which for the most part comport with the recommen-dations of the Commission, certain types of fetalresearch are allowed, with constraints based onobtaining parental consent and minimizing risk tothe pregnant woman and the fetus.
In 1985, Congress again acted on the issue of fetalresearch. It passed a law forbidding Federal conductor finding of research on viable ex utero fetuses [42U.S.C. 289]; however, there is an exception fortherapeutic research and for research that ‘will poseno added risk of suffering, injury, or death to thefetus and the purpose of which is the development ofimportant biomedical knowledge which cannot beobtained by other means” [42 U.S.C. 289g(a)]. Italso provides that, for research on living fetuses inutero, Federal regulations must require the standardof risk to be the same for fetuses that will be abortedas for fetuses that will be carried to term. Simultane-ously, Congress passed legislation creating a Bi-omedical Ethics Board, composed of six members ofthe Senate and six members of the House ofRepresentatives, with an outside advisory commit-tee [42 U.S.C. 275]. Fetal research was the first orderof business for the group. Under existing Federalregulations, the Secretary of DHHS may authorizeresearch that does not comply with the regulations ininstances of great need and great potential benefit[45 CFR 46.211]. A recent statute, however, sus-pends that authority until the Biomedical EthicsAdvisory Committee (BEAC) conducts a study ofthe “nature, advisability, and biomedical and ethicalimplications of exercising any waiver of the riskprovisions of the existing Federal regulations onfetal research” [42 U.S.C. 289g(c)]. As of autumn1989, the activities of the BEAC had been sus-pended, and it seems that no report on fetal researchwill be undertaken.
Federal attention again turned to the issue of fetaltissue transplantation research in 1988. The Directorof NIH requested permission to fund projects usingfetal tissue for transplantation. On March 22, 1988,the Assistant Secretary for Health denied the requeston the grounds that the use of fetal grafts raisedethical and legal issues that should be addressed by
an advisory panel and imposed a moratorium onFederal funding of human fetal tissue transplanta-tion research using tissue from induced abortions.Such an advisory panel was convened and subse-quently published its recommendations in the Re-port of the Human Fetal Tissue TransplantationResearch Panel (67). The panel recommendedlifting the moratorium and emphasized that com-mercialization should be prohibited and that theabortion procedure should be separated from theprocedure using fetal tissue. (See app. A for adiscussion of the DHHS moratorium on fetal tissuetransplantation research.)
Federal Regulations GoverningFetal Research
Federal regulations define the term “fetus” as aconceptus after implantation. They defer to State andlocal laws on the subject of research with fetalcadavers [45 CFR 46.210]; however, there is somedispute about whether another section of the statute,which does not specifically apply to dead fetuses,should be read to apply in the context of research (3).That section provides that “[n]o inducements,monetary or otherwise, may be offered to terminatepregnancy for purposes of the [research] activity”[45 CFR 46.206(b)]. Even if this section on induce-ments were read into the Federal law about researchon fetal cadavers, it would not necessarily precludeexperimentation involving neural grafts from abor-tuses. Although some commentators have allegedthat the possibility of donating fetal tissue forexperimental transplantation might lead women toundergo abortion (3) and thus is an inducement,others have suggested that there is little evidencethat women would do so if there were prohibitionson payment for fetal tissue and on donation of tissueto a relative (54). These persons have noted thatinforming women who are ambivalent concerningabortion about the chance to donate tissue would notbe an inducement unless it were specifically aimedat convincing the woman to abort, particularly if novaluable consideration is offered (54). Moreover,there is support for the position that the term“inducement” means valuable consideration andthat the possibility of participating in research,without compensation, would not be consideredvaluable consideration (54).
With respect to research on live fetuses, Federalregulations provide that appropriate studies must bedone on animal fetuses before human studies are

132 ● Neural Grafting: Repairing the Brain and Spinal Cord
carried out [45 CFR 46.206(a)(2)]. When researchinvolving live human fetuses is undertaken, theconsent of the pregnant woman and prospectivefather are required (unless the prospective father’sidentity or whereabouts are not reasonably ascertain-able, he is not reasonably available, or the pregnancyresulted from rape) [45 CFR 46.208(b), 46.209(d)].Some persons criticize the requirement that theprospective father’s consent be obtained (54). Toprotect the pregnant woman and the fetus, theresearch must not alter a pregnancy terminationprocedure in a way that would cause greater thanminimal risk to either [45 CFR 46.206(a)(3) (4)].
To protect the fetus, the researchers must not havea role in either the determination of what procedureis used to terminate the pregnancy or the assessmentof whether the fetus is viable [45 CFR 46.206(a)(3)].In utero fetal research may be undertaken if theresearch is designed to be therapeutic to the particu-lar fetus and places the fetus at the minimum risknecessary to meet its health needs [45 CFR46.208(a)(l)]. It may also be undertaken if theresearch imposes minimal risks and ‘the purpose ofthe activity is the development of important knowl-edge which cannot be obtained by other means” [45CFR 46.208(a)(2)].
Where it is unclear whether an ex utero fetus isviable, that fetus may not be the subject of researchunless the purpose of the research is to enhance itschances of survival or the research subjects the fetusto no additional risk and its purpose is to developimportant, otherwise unobtainable biomedicalknowledge. Research on a living, nonviable, exutero fetus may be undertaken if the vital functionsof the fetus will not be artificially maintained,experimental activities terminating the heartbeat orrespiration will not be employed, and the purpose ofthe research is the development of important,otherwise unobtainable biomedical knowledge [45CFR 46.209(b)].
State Laws Governing Embryonic andFetal Research
The overwhelming majority of State legislatureshave yet to address the issues associated withexperimental neural grafting using fetal tissue. OnlyMissouri and Pennsylvania have enacted legislationdirected specifically at fetal tissue transplants. TheMissouri law makes it a crime for any physician toperform an abortion knowing that the woman is
seeking it for the purpose of donating the fetal tissuefor implantation, or for anyone to offer considerationfor the conception of a fetus which will be abortedand used for transplantation. In Pennsylvania nofetal tissue or organs maybe obtained for transplantpurposes without the written consent of the pregnantwoman. No payment of any kind maybe offered, andconsent is valid only if obtained after the decision toabort has been made. All persons who participate inthe procurement, use, or transplantation of fetaltissue or organs, including the recipients, must beinformed of the source of the tissue or organs (e.g.,stillbirth, miscarriage, ectopic pregnancy, abortion,or other means). The person giving consent to theprocurement or use of fetal tissue or organs may notdesignate the recipient. Violation of these provisionsmay result in civil penalties.
A proposed law in California takes a similarapproach (59). While allowing the donation of afetus for “medical research or therapeutic applica-tion,” this law incorporates many guidelines firstsuggested in 1987 in a forum on fetal tissuetransplants convened by Case Western ReserveUniversity School of Medicine (35) and suggestedby the Human Fetal Tissue Transplantation Re-search Panel in its report (67). The proposed lawprohibits consideration as an inducement to undergoan abortion for the purpose of donating the tissue, thenaming of a specific recipient, and doctors “partici-pating in the procedures resulting in the loss of afetus” from participating in any research usingtissue from that fetus.
Although other States have not specifically ad-dressed the question of neural tissue grafts fromfetuses, the general fetal research laws in effect in 25States may bear on it. Table 7-2 lists and describesState regulations. State laws governing fetal re-search are not as precise as Federal law. Somecontain no definition of fetus, death, or research.Indeed, “the uncertainties surrounding the reach ofsuch State regulatory regimes may both create adangerous chilling effect on even peripheral re-search, and leave the regimes exposed to constitu-tional attack” (59).
Only one State, New Mexico, has adopted a lawpatterned on Federal regulations pertaining to fetalresearch. Other States have enacted a variety ofregulatory approaches, with the permissibility offetal research depending, in part, on the followingfactors:

Chapter 7--Legal and Regulatory Issues ● 133
Table 7-2-State Regulations Pertaining to the Use and Procurement of Fetal Tissue for Grafting Research
Arizona regulates research using fetal cadavers and live ex uterofetuses; prohibits research with fetal cadavers (except forpathological examinations and autopsies) obtained through aplanned abortion; prohibits experimentation on live ex uterofetuses.
Arkansas requires maternal consent for research using fetalcadavers obtained through planned abortions; bans nonther-apeutic research involving live ex utero fetuses. Prohibits thesale of tissue from fetal cadavers.
California regulates research using live ex utero fetuses and fetalcadavers obtained through planned abortions; prohibits non-therapeutic research with live ex utero fetuses. Prohibitscontribution of organs for valuable consideration, but excludesfrom “valuable consideration” the costs of removing, transport-ing, inspecting, preserving, and reimplanting the organ ortissue; prohibits sales and purchases of an organ or tissue whenthe organ or tissue is to be removed after the death, as well asthe use of an organ known to have been transferred for valuableconsideration; prohibits the sale of unclaimed bodies.
Connecticut has no regulations directly addressing experimenta-tion with fetal tissue. Prohibits contribution of organs forvaluable consideration, but excludes from “valuable considera-tion” the costs of removing, transporting, inspecting, preserv-ing, and reimplanting the organ or tissue, as well as the donor’sexpenses of travel, housing, and lost wages; prohibits traffick-ing in dead bodies.
District of Columbia has no regulations directly addressing useof fetal tissue. Prohibits offering valuable consideration fororgans; nothing is excluded from definition of valuable consid-eration.
Delaware has no regulations directly addressing experimentationwith fetal tissue. Prohibits organ donor from receiving compen-sation for disposition of his or her own body; however, paymentto mother for fetal tissue is not prohibited.
Florida bans nontherapeutic research on live in utero and live exutero fetuses when done in connection with a planned abortion.Bans the selling, purchasing, or transferring of a human embryofor valuable consideration. Prohibits the offering of valuableconsideration for organs, but excludes from “valuable consider-ation” the expenses of removal and use of organ (this statutewould require regulatory action to cover brain tissue); prohibitsthe purchase and sale of unclaimed bodies.
Georgia has no regulations directly addressing experimentationwith fetal tissue. Prohibits buying or selling a human fetus orfetal part; this prohibition does not apply to donations under theUniform Anatomical Gift Act (UAGA), reimbursement of a livingdonor’s actual expenses, or payment of costs associated withcollecting, storing, and implanting a donated part; prohibits thepurchase and sale of bodies.
Hawaii has no regulations directly addressing experimentationwith fetal tissue. Prohibits contribution of organs for valuableconsideration, but excludes from “valuable consideration” thecosts of removing, transporting, inspecting, preserving, andreimplanting the organ or tissue; prohibits sales and purchasesof an organ or tissue when the organ or tissue is to be removedafter the death; prohibits sale of dead bodies.
Idaho has no regulations directly addressing experimentationwith fetal tissue. Prohibits contribution of organs for valuableconsideration, but excludes from “valuable consideration” thecosts of removing, transporting, inspecting, preserving, andreimplanting the organ or tissue; prohibits sales and purchasesof an organ or tissue when the organ or tissue is to be removedafter the death.
Illinois prohibits research with fetal cadavers except for autop-Asies and pathological examinations) obtained through planned
abortions [the Federal District Court recently ruled that this lawis unconstitutional]; with fetus not obtained from a plannedabortion, research can be undertaken on its tissues or cells withthe consent of one parent. Prohibits sale of fetal tissue for anypurpose; prohibits contribution of organs for valuable consider-ation, but excludes from “valuable consideration” the costs ofremoving, transporting, inspecting, preserving, and reim-planting the organ or tissue.
Indiana regulates research with fetal cadavers and live ex uterofetuses; prohibits research with fetal cadavers (except forautopsies and pathological examinations) obtained through aplanned abortion; with fetal cadavers not obtained from aplanned abortion, research can be undertaken on tissues orcells with the consent of one parent; prohibits research with liveex utero fetuses.
Kentucky bans research using live ex utero fetuses. Prohibitsdonation of live fetus for experimentation; prohibits sale oftissue from live or viable fetuses for research purposes.Prohibits sale or purchase of a child for adoption or any other
Louisiana prohibits farming in vitro fertilized fetuses for researchor for any use other than to create a pregnancy. Prohibits saleof in vitro fertilized embryos prior to implantation; prohibitspurchases and sales of all bodies and parts for valuableconsideration.
Maine prohibits research on live ex utero and live in utero fetuses.Prohibits sale or donation of fetal tissue from live fetuses forresearch.
Massachusetts regulates research using fetal cadavers, live exutero fetuses, and live in utero fetuses; requires mother’sconsent for research with fetal cadavers; bans research on liveex utero fetuses and live in utero fetuses which is nontherapeu-tic for the fetus when the fetus is to be the subject of a plannedabortion except for diagnostic and remedial measures topreserve the life or health of the mother) ;when fetus is not to bethe subject of a planned abortion, study of in utero fetuses isallowed, providing the procedures do not substantially jeopard-ize the life or health of the fetus. Prohibits donation of a fetus forexperimentation; prohibits the performance of an abortion incases where “part or all of the consideration for said perform-ance is that fetal remains may be used for experimentation”;prohibits sale of fetal tissue for research; prohibits purchase andsale of bodies.
Michigan regulates research using fetal cadavers, live ex uterofetuses, and live in utero fetuses; requires mother’s consent forresearch with fetal cadavers; bans research on live ex uterofetuses and live in utero fetuses which is nontherapeutic for thefetus when the fetus is to be the subject of a planned abortion(except for diagnostic and remedial measures to protect the lifeof the mother); when fetus is not to be the subject of a plannedabortion, study of in utero fetuses is allowed, providing the procedures do not substantially “jeopardize the life or health of
f the fetus. Prohibits donation o a fetus for experimentation;prohibits the performance of an abortion in cases where” art
for ail of the consideration for said performance is that etalremains may be used for experimentation”; prohibits contribu-tion of organs for valuable consideration, but excludes from“valuable consideration” the expenses of removal of the organ,use of the organ, and donor’s losses and expenses (this statutewould require regulatory action to cover brain tissue).
Minnesota prohibits nontherapeutic research using live ex uteroand live in utero fetuses. Prohibits sale of tissue from livefetuses for any purpose. Prohibits sale of living conceptuses ornonrenewable organs, but allows the buying and selling of a cellculture line from a nonliving conceptus.
Missouri prohibits nontherapeutic research using live ex utero orlive in utero fetuses obtained through a planned abortion.Prohibits physicians from performing an abortion knowing thatthe woman will donate tissue for implantation; prohibits mone-tary inducement to conceive with the intention of aborting thepregnancy and using the tissue for experimentation or tissueimplantation; prohibits knowingly offering or receiving valuableconsideration for organs or tissues of an aborted fetus otherthan payments for burial, other final dispositions, and pathologi-cal examination.
Montana bans nontherapeutic research on live ex utero fetuses.Nebraska bans research using live ex utero fetuses obtained
through a planned abortion (except for diagnostic and remedialmeasures to preserve the health of the mother). Prohibits saleof tissue from live or viable fetuses for research when fetaltissue is obtained through a planned abortion.
Continued on next page

134 ● Neural Grafting: Repairing the Brain and Spinal Cord
Table 7-2—State Regulations Pertaining to the Use and Procurement of Fetal Tissuefor Grafting Research-Continued
Nevada prohibits anyone from using or making available theremains of an aborted embryo or fetus for commercial pur-poses; prohibits contribution of organs for valuable considera-tion, but excludes from “valuable consideration” expensesassociated with removal and use of donated organ as well asexpenses incurred by the donor.
New Mexico prohibits nontherapeutic research or research thatposes a greater than minimal risk to the fetus on live ex uteroand live in utero fetuses. Prohibits monetary inducement toconceive in order to subject fetus or live-born infant to clinicalresearch activity; prohibits sale of unclaimed bodies.
New York has no regulations directly addressing experimentationwith fetal tissue. Prohibits contribution of organs for valuableconsideration but excludes from “valuable consideration” thecosts of removing, transporting, inspecting, preserving, andreimplanting the organ or tissue, as well as travel expenses andlost wages of donor (this statute would require regulatory actionto cover brain tissue).
North Dakota regulates research with fetal cadavers, live ex uterofetuses, and live in utero fetuses; prohibits research using fetalcadavers obtained through a planned abortion; fetal cadaversnot obtained through a planned abortion allowed with maternalconsent; bans nontherapeutic research using live ex utero andlive in utero fetuses except to preserve mother’s health.
fProhibits donation of fetus or experimentation; prohibits theperformance of abortions done to obtain material forexperimentation; prohibits the sale of live fetuses; prohibits theSal’ re by anyone but the mother of fetal cadavers or research;
prohibits the contribution of organs for valuable consideration,but excludes from valuable consideration” the costs of remov-
ing, transporting, inspecting, preserving, and reimplanting theorgan or tissue; prohibits sales and purchases of an organ ortissue when the organ or tissue is to be removed after death.
Ohio regulates research with fetal cadavers and live ex uterofetuses; prohibits research with fetal cadavers obtained fromabortions except for autopsies and pathological examinations;bans research on live ex utero fetuses. Prohibits the sale of fetaltissue.
Oklahoma regulates research with fetal cadavers, live ex uterofetuses, and live in utero fetuses; prohibits research with fetalcadavers obtained from abortions except for autopsies and
pathological examinations; bans nontherapeutic research onlive ex utero fetuses and live in utero fetuses. Prohibits the saleof fetal tissue for any purpose.
Pennsylvania regulates research with fetal cadavers, live exutero fetuses, and live in utero fetuses; requires mother’sconsent for research or human transplantation using fetalcadavers (no payment allowed in return for consent, consentmust be obtained after the decision to abort, and the mothermay not designate the recipient of any transplanted tissue);bans nontherapeutic research using live ex utero and live inutero fetuses. Prohibits sale of fetal tissue from fetusesobtained through an abortion; prohibits contribution of organsfor valuable consideration, but excludes from valuable consid-eration” the costs of removal and use of organ.
SOURCE: Office of Technology Assessment, 1990.
whether the fetus is dead or alive;whether the research involves a fetus prior to,during, or subsequent to an induced abortion;whether the pregnant woman consented to theresearch;whether the fetus is in the womb or outside thewomb; andwhether the fetus has reached a point or hasacquired characteristics that would warranttreating it as a person, or has acquired somecharacteristic, such as the capability of experi-
Rhode Island regulates research with fetal cadavers, live ex uterofetuses, and live in utero fetuses; requires mother’s consent forresearch with fetal cadavers; bans research on live ex uterofetuses and live in utero fetuses which is nontherapeutic for thefetus when the fetus is to be the subject of a planned abortion(except for diagnostic and remedial measures to preserve the
hlife or health of the mother); prohibits abortion if main motivationis procurement of tissue for research; prohibits donation of fetusfor experimentation. Prohibits sale of fetal tissue for experimen-tation.
South Carolina has no regulations directly addressing experi-mentation with fetal tissue. Prohibits purchase and sale of deadbodies.
South Dakota requires consent for research with fetal cadavers,live ex utero fetuses, and live in utero fetuses.
Tennessee requires mother’s consent for research with fetalcadavers obtained through a planned abortion; maternal con-sent required for research using live ex utero fetuses. Prohibitssale of tissue from live fetuses for any purpose; prohibits receiptof compensation for an aborted fetus by anyone except themother.
Texas has no regulations directly addressing experimentationwith fetal tissue. Prohibits knowing and intentional transfers offetal tissue for valuable consideration, but excludes from“valuable consideration” fees to physicians, reimbursement tobenefit ultimate receiver, and donor’s travel, housing, and lostwages; prohibits sale of organs for valuable consideration, butexcludes from “valuable consideration” costs for removing,transporting, inspecting, preserving, and reimplanting the or anor tissue and for expenses incurred by the donor; prohibitspurchase and sale of bodies.
Utah prohibits research using live in utero fetuses. Prohibits salesand
f “purchases of unborn children.
Virgin a has no regulations directly addressing experimentationwith fetal tissue. Prohibits contribution of organs for valuableconsideration, but excludes from “valuable consideration” thecosts of removing, transporting, inspecting, preserving, andreimplanting the organ or tissue.
West Virginia has no regulations directly addressing experimen-tation with fetal tissue, Prohibits contribution of organs forvaluable consideration, but excludes from “valuable considera-tion” the costs of removing, transporting, inspecting, preserv-ing, and reimplanting the organ or tissue, as well as the donor'stravel expenses and lost wages.
Wisconsin has no regulations directly addressing experimenta-tion with fetal tissue. Prohibits contribution of organs forvaluable consideration, but excludes from “valuable considera-tion” the costs of removing, transporting, inspecting, preserv-ing, and reimplanting the organ or tissue (this statute wouldrequire regulatory action to cover brain tissue).
Wyoming bans experimentation using live ex utero fetuses;prohibits donation of live or viable fetus for experimentation.Prohibits sale of fetal tissue for experimentation from a live orviable fetus obtained through a planned abortion.
encing pain, that would give it an importantclaim to protection (this factor is often ex-pressed in terms of the fetus’ viability ornonviability).
Many States’ fetal research laws do not apply toresearch that is potentially therapeutic to the fetus;this exception is not applicable in the case of neuralgrafting, since the procedure is not being done forthe benefit of the fetus. Nine States underscore their

Chapter 7--Legal and Regulatory Issues ● 135
ban on experimentation on fetuses by prohibitinganyone from donating a fetus for experimentation.
Research on Fetal Cadavers
Under State law, research involving fetal cadaversand living tissues from fetal cadavers is regulatedunder the Uniform Anatomical Gift Act (47), whichhas been adopted by all 50 States and the District ofColumbia. However, some States have excludedfetuses from their provisions of the law. Researchwith fetal cadavers is also regulated in some Statesby fetal research statutes. According to the provi-sions of the UAGA, either parent may donate all orany part of a fetus “after or immediately before [its]death,’ provided that the other parent does notoppose the gift. Under the UAGA, a ‘‘decedent’ isdefined to include “a stillborn infant or fetus.” TheAct covers the donation of all or any portions of thehuman body for purposes that include both educa-tional and therapeutic benefits. Thus, if abortion andorgan donation are both legal, this should also covertissue donation (55).
Of the 25 States that have more specific lawsgoverning fetal research, 14 have provisions regulat-ing research with fetal cadavers (table 7-2). Theselaws deviate from the provisions of the UAGA eitherin their consent requirements or prohibitions theyplace on the uses of fetal tissue. Eight of these lawsrequire the pregnant woman’s consent for researchbut make no provision for consent or objection bythe father. The California statute that allows researchwith fetal tissue is silent on the issue of parentalconsent. The remaining five States diverge from theUAGA, prohibiting any research with fetal cadaversexcept for pathological examinations o r a u t o p s i e s .The divergences of these 14 laws from the provi-sions of the UAGA are perhaps attributable tolawmakers’ interests in regulating abortion andrelated practices. Of the 14, eight apply only toresearch with abortuses. Of the five statutes thatprohibit any research except for pathological exami-nations, four apply exclusively to abortuses, and oneputs more restrictions on research with fetal cadav-ers resulting from an induced abortion (table 7-2).
Research on Live Fetuses
There may be instances in which an experimentalprotocol requires that some action be undertaken ona dying or about-to-be-aborted fetus in order tobetter prepare the fetus for use as a donor of tissue.There are significant questions about whether such
actions should be permitted. For example, somecommentators argue that no research should bepermitted on fetuses that are about to be abortedwhich would not be permissible on fetuses thatwould be carried to term (46). In addition, there areState statutory constraints on research on livefetuses. Federal regulations provide that, even incases of federally funded fetal research, the Statelaws are applicable [46 CFR 46.201(b)].
State laws governing research on live fetusesseverely constrain research that is not therapeutic tothe fetus itself (thus covering neural grafting re-search, which is not therapeutic to the fetus). Of the24 State fetal research laws that regulate research onlive ex utero fetuses (see table 7-2),21 would appearto prohibit research involving neural grafting, eitherbecause the procedure is not therapeutic to the fetusor because all experimentation on such fetuses isprohibited. Of these 21 statutes, 5 permit diagnosticand remedial measures to preserve the life or healthof the pregnant woman, perhaps leading to theincongruous result that the pregnant woman maydonate fetal tissue to herself but to no one else. Whileit has been argued that an ex utero fetus is nottechnically a fetus (36), two of the remaining statuteswould appear to permit research involving a live exutero fetus, provided the pregnant woman hasconsented. The final statute prohibits only thefarming of in vitro-fertilized embryos for researchpurposes and any use of such embryos other than tocreate a pregnancy.
Of the 14 States regulating research on live inutero fetuses, 13 would appear to prohibit neuralgrafting research, either because it is not therapeuticto the fetus itself or because all experimentation onsuch fetuses is prohibited. One State, South Dakota,would apparently permit it, as long as the pregnantwoman consented.
Distinction Based on Whether the Research IsDone in Connection With an Abortion
The most significant factor in regulating researchon dead or live fetuses and in determining the extentof restriction imposed appears to be whether theresearch concerns a fetus that has been or is to beobtained through an induced abortion. Most of theState fetal research statutes were passed as part ofabortion legislation. Twelve of the 25 laws apply toresearch only where it concerns a fetus prior to orsubsequent to an induced abortion (see table 7-2). Ofthe 13 that apply to fetuses more generally, 5 impose

136 . Neural Grafting: Repairing the Brain and Spinal Cord
more stringent restrictions on fetal research inconjunction with an abortion.
Another approach that has been used to ensurethat fetal research does not encourage abortion is toprohibit the performance of an abortion where someor all of the consideration for the abortion is thedonation of fetal remains for experimental use.
In the past, important scientific gains were madethrough experimentation in the context of an in-duced abortion. For example, prenatal diagnostictechniques have been developed in pregnant patientsabout to undergo abortions (27). The most appropri-ate tissue for neural grafting will probably comefrom elective, rather than spontaneous, abortions.Tissue from spontaneously aborted fetuses may notbe appropriate for neural grafting since a fetalpathology may have lead to the miscarriage andsince the fetus may have died in utero and deterio-rated before being miscarried. Some persons arguethat research involving fetuses from induced abor-tions, whether the fetus be living or dead, is morallyimpermissible on the grounds that it constitutescooperation with an immoral practice. The point wasmade in the following way:
If one objects to most abortions being performedin our society as immoral, is it morally proper toderive experimental profit from the products of suchan abortion system? Is the progress achieved throughsuch experimentation not likely to blunt the sensitiv-ities of Americans to the immorality (injustice) of theprocedure that made such advance possible, andthereby entrench attitudes injurious and unjust tonascent life? This is, in my judgment, a serious moralobjection to experimentation on the products of mostinduced abortions (whether the fetus be living ordead, prior to abortion or post abortional) (32).
Many State fetal research laws regulate re-search only where it involves a fetus that is thesubject of an abortion, and some impose a stricterstandard on research involving fetuses to be abortedthan on research involving fetuses to be carried toterm. Against this view it is possible to argue that,even if abortion represents a moral wrong in somepeople’s minds, the use of dead abortuses for certaintypes of research is not only morally legitimate butobligatory. It has been argued that research withfetuses to be aborted is morally justified, providedthe research is aimed at deriving information poten-tially beneficial to other fetuses. This would beunlikely in the case of fetal tissue transplants toParkinson’s patients (7). One neurosurgeon has
argued that there is a moral obligation to do goodwhere possible; since the fetal cadaver is beyondhelp or hope, to waste its tissues is a moral wrong(50). It has been stated that, by allowing researchintended to benefit future fetuses, “what we havedone is add a moral good to a morally tragicsituation” (28). On the other hand, it has beenargued that this practice is comparable to the use ofdata obtained by Nazi researchers (44).
Payment in Connection WithFetal Experimentation
One of the greatest concerns regarding neuralgrafting-and the concern that State legislatures arelikely to address first-is the possibility that theneed for fetal tissue may encourage women toconceive for the sole purpose of donating tissue torelatives or selling it for profit. This could lead to theexploitation of women and intended recipients (33).Currently, 16 State fetal research statutes prohibitthe sale of fetal tissue, 7 of them for any purpose and9 for research purposes (see table 7-2). Some of thesestatutes apply only to induced abortions and thuswould not preclude the sale of a miscarried fetus fortissue transplantation. The penalties attached tosome of these laws are very stiff. Selling a viableabortus for experimentation in Wyoming, for exam-ple, subjects a person to a fine of not less than$10,000 and imprisonment of 1 to 14 years [Wyo.Stat. 35-6-115]. Several States have nonuniformUAGA provisions that prohibit transfer of organs ortissues, including fetal organs and tissues, for value.Moreover, some State laws would forbid the sale offetuses even when they are not being used forresearch purposes, thus covering payment for neuralgrafting in the clinical setting.
Biotechnology companies create cell lines fromfetal tissue, a fact which raises the possibility that awoman may donate fetal tissue to a company whichmay then exploit it commercially (57). The issue ofcommercial exploitation of cell lines was examinedin a recent California case (42) (see ch. 8 fordiscussion). The court held that an individual has aprotectable monetary interest in products made fromhis or her genetic material. The fact that a corpora-tion might profit from fetal tissue whereas thewoman who donated it is prevented from receivingconsideration for it seems to violate the principle ofthis case. However, on appeal the California Su-preme Court held that the plaintiff did not have aproperty right to his tissues and cells but did have a

Chapter 7--Legal and Regulatory Issues ● 137
right to informed consent for any use by others of histissues and cells (43).
It is possible that, because a cell line is new tissueproduced from the genetic material of, but notoriginally apart of, the aborted fetus, laws proscrib-ing the sale of fetal tissue may not apply to cell lines.In fact, a Minnesota law prohibits the sale of livingconceptuses or nonrenewable organs but does allow‘‘the buying and selling of a cell culture line or linestaken from a non-living human conceptus . . .“[Minn. Stat. Ann. 145.1627(3)]. In contrast, Ne-vada’s broadly worded statute making it a crime foranyone to use or “make available. . . the remains ofan aborted embryo or fetus for any commercialpurpose” could conceivably outlaw the productionof cell lines from fetal tissue [Nev. Rev. Stat. Ann.451.015]. Moreover, it could outlaw cell line trans-plants.
Interstate Transfer of a Fetus
Some State statutes also contain restrictions onthe interstate transfer of fetal tissues. An Indianalaw, for example, forbids transporting a fetus froman induced abortion to another State “for experi-mental purposes” [Ind. Code Ann. 35-l-58.5-6].
In Arkansas, there is a ban on ‘possession” of theorgan, tissue, or material of an aborted fetus [Ark.Stat. Ann. 20-17-802(d)]. However, the Arkansasstatute expressly exempts from its provisions physi-cians and the instructional and research programs ofinstitutions of higher education [Ark. Stat. Ann.20-17-80 (e)].
GOVERNMENT OVERSIGHTIssues and questions raised by the introduction
and development of neural grafting procedurescould make other government regulatory mecha-nisms relevant. For example, special concerns sur-rounding neural tissue transplants may requiregovernment oversight to protect the interests of theparties involved. Also, fetal rights is a relatively newarea of the law, and many of the existing lawsdesigned to protect human subjects in biomedicalresearch do not cover fetal issues. Some of theanticipated problems are discussed below.
Potential Constitutional Challenges toRestrictions on Research
Not all regulations on research are constitutional.Laws restricting research may be struck down as too
vague or as violating the equal protection clause ofthe Constitution. Those applying to experimentationon fetuses or in the context of abortion may violatethe right to privacy (48). In addition, some legalcommentators posit that there is a constitutionalright to undertake or participate in research. Even ifundertaking and participating in research wereconstitutionally protected, however, certain restric-tions to further health and safety would be constitu-tionally permissible.
Laws governing research must meet certain stan-dards of clarity in order to be constitutional. ALouisiana law prohibiting nontherapeutic experi-mentation on fetuses was declared unconstitutionalby a Federal appeals court, because the term‘‘experimentation’ was so vague that it did not giveresearchers adequate notice about what kind ofconduct was banned. The court said that the term‘‘experimentation’ was impermissible vague be-cause physicians do not and cannot distinguishclearly between medical experimentation and medi-cal tests. It noted that “even medical treatment canbe reasonably described as both a test and anexperiment,” for example, “whenever the results ofthe treatment are observed, recorded, and introducedinto the database that one or more physicians use inseeking better therapeutic methods” (37).
Although there is no specifically enumerated rightto research in the Constitution, some commentatorsassert that support for such a right could be derivedfrom the 14th amendment right to personal libertyand the first amendment right to free speech (52).Arguably, the right to participate as a researchsubject is protected by the 14th amendment’s rightto privacy, since an individual’s decision to use hisor her body in an experiment designed to furthermedical knowledge or to be of personal benefit is aprivate matter (52). This right to research consists ofthe freedom to pursue knowledge and the freedom tochoose the means to achieve that knowledge (52).On the other hand, it has been argued that meanshave their own morality (44). The Supreme Courthas stated that the right to liberty guaranteed by the14th amendment encompassed freedom to “acquireuseful knowledge . . . and generally to enjoy thoseprivileges long recognized at common law asessential to the orderly pursuit of happiness by freemen” (41). This language, arguably, applies notonly to the researcher’s right to scientific inquiry,but also to an individual’s right to participate as aresearch subject (52). It could be interpreted as

138 ● Neural Grafting: Repairing the Brain and Spinal Cord
supporting an individual’s right to help acquireknowledge by participating as an experimentalsubject (52).
Some arguments hinge on the first amendment’sprotection of free speech, which, it can be argued,includes a right to learn new information. However,one must distinguish the freedom to pursue knowl-edge from the right to choose the method forachieving that knowledge. Although it is argued thatgovernment may not prohibit research in an attemptto prevent the development of new knowledge, itmay restrict or prohibit the means used by research-ers if the means intrude on interests in which thestate has a legitimate concern (52). Therefore, boththe Federal and State governments may regulate theresearcher’s methods in order to protect the rights ofresearch subjects and community safety (52). Re-search may be restricted, for example, to protect thesubject’s right to autonomy and welfare by requiringinformed, free, and competent consent; however, thestate cannot arbitrarily regulate research solelybecause it deems the knowledge sought to bedistasteful or subject to harmful use (52).
Fetal Remains Laws
Every jurisdiction makes some provision for theregistration of deaths (usually by death certificate)and the disposition of dead bodies. Most States havea vital statistics statute governing death registrationand issuance of permits for transporting or disposingof dead bodies. In most States, dead bodies must bedisposed of in an authorized manner within aspecified period of time, usually 72 hours afterdeath. Any disposition of a dead body usuallyrequires a permit, which is generally issued onlyafter a death certificate has been filed. Most of thesestatutes also specify when fetal deaths must beregistered and how to dispose of fetal remains. Inaddition, some States make separate provision forreporting fetal deaths and disposing of fetal remains.These statutes are important, not only because theyprovide penalties for unauthorized uses of deadbodies, but also because they determine what mustbe done with fetal remains once their research orclinical value has been exhausted and what reportsmust be filed.
The two most common sources of authority forconducting research are research statutes and theUAGA. In addition, many States establish anadministrative agency to distribute unclaimed dead
bodies for scientific and educational purposes. Sincethese statutes typically require a lengthy holdingperiod or embalming of the body, they do notprovide useful authority for the use of fetal tissue inneural grafts. Moreover, anyone who conducts fetaltissue research that is not authorized by one of thesestatutes may be charged with corpse abuse orunauthorized dissection. The most common corpseabuse statute follows the Model Penal Code 250.10and prohibits any use of a corpse that would offend“family sensibilities.”
Most jurisdictions exempt fetuses in early stagesof development from death certification and regis-tration requirements. These States define “fetaldeaths” or “stillbirths” requiring registration interms of a minimum gestational period, a minimalweight, or both. Eight States apparently require fetaldeath certificates regardless of the age or weight ofthe fetus. Of the statutes that require fetal deathcertificates, at least five exempt deaths resultingfrom induced abortions. Finally, 13 States do notrequire death certificates for fetuses of any particularage or weight but do require at least some fetaldeaths to be reported. Three of the statutes requiringsome report of fetal deaths make special provisionfor reporting deaths resulting from induced abor-tions.
Some States require disposition permits regard-less of the age or weight of the fetus, while at leastsix States directly exempt fetuses in early stages ofdevelopment from permit requirements. Eighteenother States apparently obtain the same resultindirectly, by anticipating that disposition permitswill be issued only on the filing of a death certificate,but exempting fetuses in early stages of develop-ment from death certification requirements. In a fewStates, whether a permit is required depends on thekind of disposition planned rather than on anycharacteristic of the fetus.
The most common kinds of dispositions of fetalremains are burial, cremation, and entombment.Kentucky apparently allows only burial of fetalremains [Ky. Rev. Stat. 213.160]. At least 16 statutesanticipate that a health-care institution will disposeof fetal remains and require the institution to reportthese dispositions. Finally, seven States that providefor fetal death certificates or death reports explicitlyexclude fetuses in early stages of development fromdisposition requirements, make no specific provi-

Chapter 7--Legal and Regulatory Issues ● 139
sion for fetal remains, or authorize an administrativeagency to decide what disposition is appropriate.
At least seven of the statutes governing thegeneral disposition of dead bodies make someprovision for parental consent to the disposition offetal remains, while five statutes require parentalconsent for any disposition of a dead fetus, regard-less of gestational age. One of the five statutesrequires the pregnant woman’s but not the partner’sconsent when the pregnant woman is unmarried,while the two remaining statutes require consent ofa parent only in certain circumstances.
The reamer in which fetal remains are disposed ofis also covered under the statutes of some States. TheCalifornia penal statute clearly does not affect neuralgrafts; it merely prohibits disposition of fetal re-mains in sites open to public view [Cal. Penal Code643]. The California Health and Safety Code re-quires that fetal remains be incinerated at theconclusion of research, but this provision does notapply to educational institutions [Cal. Health &Safety Code 25957(a)]. The Arkansas statute re-quires physicians performing abortions to ensurethat fetal remains are disposed of in a similar mannerto other human tissue [Ark. Stat. Ann. 20-17-802(a)], namely, ‘‘incineration, cremation, burial, orother sanitary means prescribed by the State healthdepartment” [Ark. Stat. Ann. 20-17-801(a)]. Thelaws of Florida, Georgia, Minnesota, and NorthDakota allow any manner of disposition approvedby the State health department. The Florida statutealso requires the health department to promulgaterules consistent with the disposition of other humantissues [Fla. Stat. Ann. 390.012(2)]. Whether neuralgrafts are allowed in these States depends on whatregulations are currently in force. Finally, theMassachusetts statute requires fetal remains to bedisposed of at the parent’s direction, whether byburial, entombment, cremation, or, if the hospital orattending physician is to dispose of the remains, byany method that does not create a public healthhazard [Mass. Ann. Laws ch. 11,202]. In addition,the statute requires the hospital or attending physi-cian to inform parents of their right to directdisposition and of any hospital policy governingdisposition of fetal remains.
The fetal remains laws in some States have beensubject to successful constitutional challenges. Arecent Supreme Court case held that an ordinancerequiring fetal remains to be disposed of in a humane
UNIFORM DONOR CARDof
Print or type name of donorIn the hope that I may help others, I hereby make this anatomicalgift, if medically acceptable, to take effect upon my death. The wordsand marks below indicate my desires
I give (a) — any needed organs or parts( b ) — only the following organs or parts
Specify the organ(s) or part(s)for the purposes of transplantation, therapy, medical research oreducation,
( c ) — my body for anatomical study if needed
Limitations orspecial wishes, if any
08-21-81 100M/81
Signature of Donor Date of Birth of Donor
Date Signed City & State
Witness Witness
This iS a legal document under the Uniform Anatomical Gift Act orsimilar laws
For further information consult your physician or
National Kidney Foundation of the NationalCapital Area, Inc.
2233 Wisconsin Ave., NW, Suite 320Washington, DC 20007
Photo credit: Office of Technology Assessment
An organ donation card.
and sanitary manner was impermissible vague (16).In addition, laws that specifically required a womanto decide, in advance of an abortion, whether theaborted fetus was to be buried, cremated, or disposedof at the hospital’s discretion have been struck downas unconstitutionally interfering with the woman’sright to privacy (29).
Uniform Anatomical Gift Act
The Uniform Anatomical Gift Act (47) is the onlyuniform body of law that might regulate acquisitionor donation of fetal tissue implants. Forty-sevenStates and the District of Columbia presently con-form to some form of the 1968 version of the UAGA.California, Connecticut, and Hawaii have adopted anew version of the UAGA, approved by the NationalConference of Commissioners on Uniform StateLaws in 1987. In fact, in the 25 States that lack fetaltissue research statutes, the UAGA is the primarylegislation that would affect this technology (57).
Specifically, the UAGA affects fetal tissue im-plants by including “a stillborn infant or fetus’ in

140 . Neural Grafting: Repairing the Brain and Spinal Cord
the definition of “decedent” and by stating that“parts” includes “tissues” (47); however, not allStates have included a fetal tissue provision in theirversion of the UAGA. According to the 1987 versionof the Act, either parent may consent to the donationof fetal tissue; in reality, the consent of both parentsis necessary because if either objects, a donor whoknows of the objection may not accept the gift (47).The UAGA would appear to allow the parents of anaborted or stillborn fetus to designate a recipient,even though this practice would be in direct opposi-tion to the recommendations of the Report of theHuman Fetal Tissue Transplantation ResearchPanel (67). The panel expressed concern that such apractice might encourage abortions in order todonate fetal tissue for the treatment of relatives.Furthermore, because of the genetic nature ofdiseases such as diabetes and Huntington’s disease,the effectiveness of the treatment might actually bejeopardized by implanting fetal cells which possessthe same defect that the procedure is supposed toameliorate (67). The UAGA and the NIH reportdiffer on several points because the UAGA waswritten before the NIH report and before fetaltransplants were thought to have so many possibleapplications (13).
In adopting the UAGA, many States addedsections designed to facilitate and regulate thedonation of tissue. The most common nonuniformprovisions found in State laws either require hospi-tals to adopt an organ procurement protocol, whichis designed to facilitate the procurement of donortissue while recognizing the sensitivity of therelatives who must consent to the donation, orsimply require hospital personnel to request therelative of a suitable decedent to make the dece-dent’s organs available for donation (see table 7-2).In either case, physicians wishing to obtain fetaltissue would be required to request parental consentin a professional and sensitive manner. Those lawswhich require that consent be obtained wouldrequire doctors to inform all abortion patients of thepossibility of donation for transplants, preferablyafter the abortion decision had been made. If theconsent were sought prior to the decision to abort, itmight conceivably influence the decision. For thisreason, the Human Fetal Tissue TransplantationResearch Panel recommends that the decision toobtain an abortion precede any request to donatetissue for implantation (67). These two proce-dures probably should be handled by two sepa-
rate advisers, the supervising physician and theresearcher (55).
In 1987 the National Conference of Commission-ers on Uniform State Laws approved a new modelUAGA, which has been adopted by at least sevenStates. The new version retains provisions allowingthe next of kin to designate the fetal tissue recipientand incorporates changes designed to increase thenumber of organ donations, particularly throughrequired request policies. Organ procurement pro-fessionals have traditionally gone to great lengths toassure the public that organ donation will notcompromise the patient’s medical care in any way.Accordingly, the family is approached about possi-ble donation only after the patient has been declareddead by the physician. Following these guidelines,parents can be approached about possible donationonly after the abortion and after the fetus has beendeclared dead. Language in the new version of theUAGA, however, suggests it may be permissible toseek consent before the abortion. The new versionallows consent to be sought after or immediatelybefore death (14).
The laws of at least eight States would protectrecipients of fetal tissue by requiring that all donorsbe tested for HIV. An additional two States, whilenot requiring HIV testing of donors, have estab-lished standards that decrease the likelihood ofAIDS-infected tissues being made available fordonation.
Overall, the UAGA and its various manifestationsprovide some guidelines in the area of fetal tissuetransplants. Because this Act was drafted beforeneural grafting technology became known, it isobviously not designed to address the specific andunique problems that these implants raise.
Compensation for Fetal Tissue in aNonresearch Setting
There is much concern about the possibility thatwomen will be paid for fetal tissue for transplanta-tions. One commentator points to ‘‘the fear thatpermitting the commercialization of the fetal tissuetransplantation system will result in the exploitationof the women who bear tissue for profit and of thecritically-ill patients who want to acquire it” (59).The NIH panel recommended that sale of fetal tissuenot be allowed, for two reasons:

Chapter 7&gal and Regulatory Issues ● 141
. so as not to influence a woman’s decision toabort; and
. so as not to induce an abortion facility to baseits choice of abortion procedure on the profita-bility of the fetal tissue to be retrieved (22).
The prohibition on payment to organ donors gener-ally prohibits payment to women for fetal tissue. Inaddition, a variety of State statutes also have thesame prohibition (table 7-2).
The National Organ Transplant Act, passed underCongress’ commerce clause authority, bans the saleof certain listed organs (including certain fetalorgans and their subparts) [42 U.S.C. 274(e)] andprovides that the Secretary of DHHS list additionalorgans under the ban. Since the brain is not listed asone of the organs, payment for use of fetal braintissue for transplantation will not be banned until theSecretary so designates.
In addition to the 16 State fetal research statutesthat prohibit the sale of fetal tissues for purposesincluding research, seven State laws forbid the saleof fetuses or fetal material (see table 7-2). TheFlorida statute places a flat ban on selling, purchas-ing, or transferring a human embryo for valuableconsideration and on offering or advertising to do so[Fla. Stat. Ann. 837.05(1)]. Nevada prohibits anycommercial use of an aborted fetus or fetal materialresulting from an abortion [Nev. Stat. Ann.451.015]. Missouri prohibits knowingly offering orreceiving any valuable consideration for the organsor tissues of an abortus, except payments for burialor other final disposition and for pathologicalexaminations [Mo. Ann. Stat. 188.036(5)]. Utahprohibits sales and purchases of, or offers to buy orsell, unborn children [Utah Code Ann. 76-7-311].The Georgia statute prohibits buying or selling ahuman fetus or fetal part [Ga. Code Ann. 48-401 etseq.], but the prohibition does not apply to donationsunder the UAGA, reimbursement of a living donor’sactual expenses, or payment of costs associated withcollecting, storing, and implanting a donated part[Ga. Code Am. 26-9957(b)]. Similarly, the Texasstatute prohibits knowing and intentional transfersof fetal tissue for valuable consideration but ex-cludes from ‘‘valuable consideration’ fees paid tophysicians, hospitals, and clinics for services ren-dered in the usual course of medical practice,reimbursement of legal or medical fees incurred tobenefit the ultimate receiver of the tissue, and thedonor’s travel and housing expenses and lost wages
[Tex. Penal Code 48.02]. Finally, in an unusualprovision, Kentucky prohibits selling or purchasinga child for adoption or any other purpose [Ky. Rev.Stat. Ann. 199.590(2)]. Since the statute specificallyexcludes from its coverage in vitro fertilization inwhich the genetic donors are a married couple andthe fertilized ovum is to be implanted in the wife, theKentucky legislators seem to have intended ‘child”to include the human organism from conception and“any purpose” to include medical and scientificprocedures. Thus, this statute could be used toprohibit any agreement to pay the pregnant womanfor fetal tissue made while the fetus is still alive.
At least 18 jurisdictions have laws forbiddingpayment to organ donors. Ten of the statutes arenonuniform UAGA provisions. The DelawareUAGA provision clearly does not prohibit paymentto the pregnant woman for fetal tissue: it applies onlyto payments to a donor for disposition of his or herown body [Del. Code Ann. tit. 16, 2713(f)]. Whetherthe nine remaining UAGA provisions prohibitpayment to the pregnant woman depends on twofactors—whether any or all of the payment can beconsidered reasonable costs associated with the useof the tissue, and when the tissue will be removed.
The nonuniform provisions of nine States prohibitthe purchase or sale of organs or tissue for valuableconsideration but exclude from the definition of“valuable consideration’ the costs of removing,transporting, inspecting, preserving, and reim-planting the organ or tissue. Three States excludefrom “valuable consideration” “ the expenses oftravel, housing, and lost wages” incurred by the“donor.” This suggests that the pregnant womancannot be reimbursed for nonmedical losses andexpenses without specific statutory authority. More-over, under the UAGA, the term “donor” appliesonly to ‘an individual who makes a gift of all or partof his body” (47). In the case of fetuses, thepregnant woman is not a donor, but someoneauthorized to consent to the gift of a decedent’sremains. Thus, the pregnant woman may not be paidfor agreeing to transfer the fetal remains, even underState laws (47).
Under the nonuniform provisions of four States,California, Hawaii, Idaho, and North Dakota, pay-ment to the pregnant woman may be banned foranother reason. These States prohibit sales andpurchases of organs and tissues for valuable consid-eration when the organ or tissue is to be removed

142 ● Neural Grafting: Repairing the Brain and Spinal Cord
after the decedent’s death. Unless the fetal tissue isto be removed while the fetus is still alive (whichmay be forbidden under the State’s fetal research orother statute), payment to the pregnant woman isforbidden under these anatomical gift act provisions.The California Anatomical Gift Act is supplementedby a penal provision that prohibits a person fromknowingly acquiring, receiving, selling, or promot-ing the transfer or otherwise transferring any organfor transplantation for valuable consideration. It alsoprohibits the use of an organ known to have beentransferred for valuable consideration. The law isdirected against brokering organs rather than thedirect sale by a donor to a recipient.
Of the eight statutes remaining that prohibit thesale of organs but are not part of the State UAGA,one clearly does not prohibit payments to thepregnant woman. The Tennessee statute prohibitsonly transfers of organs for valuable considerationthat “affect commerce” [Tern. Code Ann. 68-30-401] and is presumably aimed at brokers. The law ofthe District of Columbia clearly prohibits suchpayments, and it excludes nothing of value from thedefinition of valuable consideration [D.C. CodeAnn. 6-260(b)]. The remaining statutes are similar tothe nonuniform anatomical gift act provisions previ-ously discussed. Six allow reimbursement of reason-able expenses associated with the removal, preserva-tion, and use of the donated organ, and four make anadditional allowance for the donor’s losses andexpenses.
The Federal and State laws prohibiting paymentto organ donors would ban more than just a cashpayment to women. They would also cover paymentof a woman’s abortion expenses in order that she
may donate fetal tissue (54). The reach of some Statelaws may also extend to payment to agencies thatretrieve and process the fetal tissue. These agencieswould not be able to “sell’ tissue to physicians orpatients; however, they would be able to recovertheir costs and overhead for obtaining the tissue. Forexample, the New York and West Virginia statutesexclude from the definition of ‘valuable considera-tion” reimbursement of expenses incurred by non-profit agencies and corporations in offering servicesrelated to the location, maintenance, and distributionof the donated organ [N.Y. Public Health Law 4307;W.Va. Code 16-19-7(a)].
Most of the statutes prohibiting transfers oforgans for value define organ quite broadly andwould cover most types of tissues and organs to betransplanted from fetuses. Other statutes are morelimited in the body parts they cover and wouldrequire regulatory agency action to cover braintissue. The Florida statute bans the sale of thekidney, liver, heart, lung, pancreas, bone, skin, orany other organ or tissue specified by rules adoptedby the Department of Health and RehabilitativeServices [Fla. Stat. Ann. 873.01(3)(a)]. The NewYork statute begins with a larger list of items andthen provides for regulatory expansion. It defines“human organ’ as ‘the human kidney, liver, heart,lung, bone marrow, and any other human organ ortissue as maybe designated by the commissioner butshall exclude blood” [N.Y Public Health Law4307]. To the New York list, Wisconsin adds thepancreas, cornea, eye, bone, skin, and any otherorgan specified by the department except blood,blood products, and semen [Wisc. Stat. Ann.146.345]. Michigan has by far the most comprehen-sive list: “human kidney, liver, heart, lung, pan-creas, bone marrow, cornea, eye, bone, skin, carti-lage, dura mater, ligaments, tendons, fascia, pitui-tary gland, and middle ear structures, and any otherhuman organ specified by rule promulgated by thed e p a r t m e n t ’ [ M i c h . C o m p . L a w s A n n .333. 10204(3)(a)].
Finally, 10 States prohibit “trafficking” in deadbodies—that is, transferring dead bodies for valua-ble consideration (see table 7-2). These statutes arearguably drafted broadly enough to prohibit eitherpayment to or receipt of payment by the pregnantwoman for the use of fetal remains. Only one statuteexplicitly covers all bodies and bodily parts [La.Rev. Stat. Ann. 17:2280]. The remaining eithercover bodies but do not refer to parts or limit theircoverage to unclaimed bodies (those that have notbeen claimed for burial). The majority of States banboth purchases and sales of dead bodies, but threeStates prohibit only sales, and one State morebroadly proscribes “delivering or receiving forspeculation or pecuniary profit.” In addition, fivestatutes prohibit transporting dead bodies out ofState.

Chapter 7--Legal and Regulatory Issues . 143
SUMMARY AND CONCLUSIONS
The use of neural grafts raises many legal issues,despite the fact that this procedure is showing somepromise in the treatment of several disorders. Thereare grounds for Federal action in this area. To theextent that Federal funds are used to support researchinvolving neural grafting or to pay for the clinicaluse of such procedures, Federal regulations mayestablish mandatory policies governing the conductof such research. Even if Federal funds are not used,the Federal Government has powers under thecommerce clause to regulate this activity. Thispower has served as the basis for the establishmentof the FDA, the prohibition on payment to organdonors for transplantation involving interstate com-merce, and the regulation of medical laboratoriesengaged in interstate commerce.
It is difficult to predict how the FDA will chooseto regulate the various tissues and products ofbiotechnology that may be used in neural grafting.Questions of safety and the FDA’s current regulationof similar products make it likely that the agencywill seek to regulate most neural grafting materials.
Questionable jurisdiction under the Public HealthService Act may limit the ability of the FDA toregulate these materials, since it is unclear whetherneural tissue grafts, cell lines, and products ofbiotechnology to be used as neural grafting materialsare analogous to the other articles listed as biologicsin the statute. Other legal issues include questions ofFDA jurisdiction in relation to when a neural graft isproduced and performed intrastate and in relation tothe practice of medicine.
Some existing Federal policies governing experi-mentation and organ transplantation could affecttissue transplants. However, the Federal regulationson fetal research and the Federal law on transplanta-tion were developed before the extensive, recentdebate on fetal tissue transplantation. It might beappropriate to amend existing policies to addressmore directly the concerns raised by neural grafting.In particular, Federal regulations and law might bemodified to provide that a woman not be paidvaluable consideration for fetal tissue for transplan-tation and not be allowed to designate a donor.Federal regulations might also be amended to ensurethat health-care professionals undertaking counsel-ing and persons involved in abortion procedures are
not also involved in the harvest and transplantationof fetal tissue.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
CHAPTER 7 REFERENCESAnderson, W., and Fletcher, J., “Gene Therapy inHumans: When Is It Ethicalto Begin? ’’New EnglandJournal of Medicine 303:1293-1297, 1980.Annas, G., Glantz, L., and Katz, B., InformedConsent to Human Experimentation: The Subject’sDilemma (Cambridge, MA: Ballinger, 1977).Areen, J., “Statement on kgal Regulation of FetalTissue Transplant,” Report of the Human FetalTissue Transplantation Research Panel (Bethesda,MD: National Institutes of Health, 1988).Bakay, R., neuroscientist, Emory University, Atlanta,GA, personal communication, December 1989.Barber, B., “The Ethics of Experimentation withHuman Subjects,” Scientific American 234 (Febru-ary): 25-31, 1976.Barnett, H., Sackett, D., Taylor, D., et al., “Are theResults of the Extracranial-Intracranial Bypass TrialGeneralizable?” New England Journal of Medicine316:820-824, 1987.Blank, R., Program for Biosocial Research, SocialScience Research Institute, Northern Illinois Univer-sity, DeKalb, IL, personal communication, Dec. 18,1989.Bonche~ L., “Are Randomized Trials Appropriatefor Evaluating New Operations?” New EnglandJournal of Medicine 301;4445, 1979.Bonche~ L., letter, New England Journal of Medi-cine 301:1181-1183, 1979.Buc, N., Weil, Gotshal & Manges, Washington DC,personal communication, Dec. 18,1989.Buchanan, A., and Brock, D.W., “Deciding forOthers,” Milbank Quarterly 64:17-94, 1986.Bunker, J., Hin.kley, D., and McDermott, W., “Surgi-cal Innovation and Its Evaluation,” Science 200:937-941, 1978.Carr, S., legislative analyst, Office of GovernmentalRelations, Association of American Medical Col-leges, Washington, DC, personal communication,April 1990.Center for Biomedical Ethics, The Use of HumanFetal Tissue: Scientific, Ethical, and Policy Con-cerns (Minneapolis, MN: University of Minnesota,1990).Christoffel, T, Health and the Luw: A Handbook forHealth Professionals (New York, NY: Free Press,1982).City of Akron v. Akron Center for ReproductiveHealth, Inc., 462 U.S. 416 (1983).Curran, W., “Forward,” Consent to Treatment: APractical Guide, F. Rozovsly (cd.) (Boston, MA:Little, Brown, 1984).

144 . Neural Grafting: Repairing the Brain and Spinal Cord
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.30.
31.
32.
33.
Fazzini, E., “Neural Transplants in Parkinson’sDisease,” paper presented at the International Sym-posium, Centrol Ramon y Cajal, Madrid, May 19-20,1989.Fletcher, J., “Moral Problems and Ethical Issues inProspective Human Gene Therapy,” University ofVirginia Law Review 69:515-546, 1983.Fletcher, J., Dornmel, J., and Cowell, D., “Consentto Research With Impaired Human Subjects,” IRB:A Review ofHuman Subjects Research 7 (November-December) :l-6, 1985.Fowler, N., letter, New England Journal of Medicine,301:1181, 1979.Fox, J., “Overview,” Report of the Human FetalTissue Transplantation Research Panel (Bethesda,MD: National Institutes of Health, 1988).Gill, T, and Lund, R., “Grafting into the Brain,”testimony before the Human Fetal Tissue Transplan-tation Research Panel, National Institutes of Health,Bethesda, MD, Sept. 14, 1988.Greenwald, R., Ryan, M., and Mulvihill, J., HumanSubjects Research: A Handbook for InstitutionalReview Boards (New York, NY: Plenum Press,1982).Gunter, K., Division of Biological InvestigationalNew Drugs, Center for Biologics Evaluation andResearch, Food and Drug Administration, personalcommunication, Feb. 26, 1990.Halushka v. University of Saskatchewan, 53 D.L.R.2d 436 (Sask. 1968).Jackson, L., “Prenatal Genetic Diagnosis by Chori-onic Villus Sampling (CVS),” Seminars in Perina-tology 9:209-218, 1985.Lappe, M., “Balancing Obligations to the LivingHuman Fetus with the Needs for Experimentation,”U.S. Department of Health, Education, and Welfare,National Commission for the Protection of HumanSubjects of Biomedical and Behavioral Research,Research on the Fetus, DHEWPub. No. (OS) 76-127(Washington, DC: U.S. Government Printing Office,1975).Leigh v. Olsen, 497 F. Supp. 1340 (C.D.N.D. 1980).kvine, R., Ethics and Regulation of Clinical Re-search (Baltimore, MD: Urban & Schwarzenberg,1981).Imh, L, letter, New England Journal of Medicine301:1182, 1979.McCormic~ R., “Experimentation on the Fetus:Policy Proposals,” U.S. Department of Health,Education, and Welfare, National Commission forthe Protection of Human Subjects of Biomedical andBehavioral Research, Research on the Fetus DHEWPub. No. (OS) 76-127 (Washington, DC: U.S.Government Printing Office, 1975).McCoy v. Georgia Baptist Hospital, 167 Ga. App.495,306 S.E.2d 746 (1983).
34.
35.
36.
37.
38.
39.
40.
41.42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
Mackler, B., ‘‘Regulatory Issues Concerning Organsand Tissues,” paper presented at the Annual Educa-tional Conference of the Food and Drug LawInstitute, Washington, DC, Dec. 13, 1989.Mahowald, M.B., Areen, J., Hoffer, B.J., et al.,“Transplantation of Neural Tissue horn Fetuses,”Science 235:4794, 1987.Mahowald, M.B., Silver, J., and Ratcheson, R.A.,“The Ethical Options in Transplaning Fetal Tissue,’Hastings Center Report 17(February):9-15, 1987.Margaret S. v. Edwards, 794 F.2d 994 (5th Cir.1986).Merchant, B., and Hybritech, X., “Emerging Issueson Product Safety Evaluation,” paper presented atthe Annual Educational Conference of the Food andDrug Law Institute, Washington, DC, Dec. 13,1989.Merrill, R.A., and Hutt, P.B., Food and Drug Lzw:Cases and Materials (Mineola, NY: FoundationhtXS, 1980).Men, B. “Neurobiologists Join Neurosurgeons inUrging Restraint in Parkinson’s Surgery,” JournaZofthe American Medical Association 216:2929, 1989.Meyer v. Nebraska, 262 U.S. 390 (1923).Moore v. Regents of the University of Cal~ornia, 202Cal. App.3d 1230, 249 Cal. Rptr. 494 (1988), reh.granted, 252 Cal. Rptr. 816,763 P.2d 479, 1988.Moore v. Regents of the University of Cal#ornia,Supreme Court of the State of Californi~ CaseNumber S006987, July 9, 1990.Moraczewski, A. S., Regional Director, Pope JohnXXIII Medical, Moral, Research, and EducationCenter, Houston, TX, personal communication, Dec.18, 1989.Mulford, R., “Experimentation on Human Beings,”Stanford L.uw Review 20:99-117, 1967.National Commission for the Protection of HumanSubjects of Biomedical and Behavioral Research,U.S. Department of Health, Education, and Welfare,Research on the Fetus: Report and Recommenda-tions, DHEW Pub. No. (OS) 76-127 (Washington,DC: U.S. Government Printing Office, 1975).National Conference of Commissioners on UniformState Laws, Uniform Anatomical Gift Act, annualconference, Chicago, IL, 1987.Note, “State Prohibition of Fetal Experimentationand the Fundamental Right to Privacy,” ColumbiaLaw Review 88:1073-1097, 1988.Ramsey, P., The Patient as Person: Explorations inMedicaZ Ethics (New Haven, CT: Yale UniversityPress, 1970), pp. 11-19.Redmond, D. E., neurosurgeon, NeurobehavioralLaboratory, Yale University School of Medicine,New Haven, ~, personal communication, May1990.Rettig, R. A., “The Politics of Organ Transplantation:A Parable of Our Time,” Organ Transplantation

Chapter 7-Legal and Regulator Issues . 145
52.
53.
54.
55.
56.
5’7.
58.
59.
60.
61.
62,
63.
64.
65.
Policy: Issues and Prospects, J.F. Blumstein andF.A. Sloan (eds.) (Durham, NC: Duke UniversityPress, 1989), pp. 191-227.Robertson, J., “Compensating Injured ResearchSubjects: II, The Law,” Hastings Center Report6(December):29-31, 1976.Robertson, J., “The Law of Institutional ReviewBoards,” University of California at La AngelesLaw Review 26:484-549, 1979.Robertson, J., “Fetal Tissue Transplants,” Wash-ington University Luw Quarterly 66:443498, 1988.Rosner, J., Executive Director, United ParkinsonFoundation, Chicago, IL, personal communication,May 1990.Schwartz, R., “Institutional Review of MedicalResearch,” Journal of Legal Medicine 4:143-166,1983.Sheehan, A., “Fetal Tissue Implants: An ExplosiveTechnology Needs National Action,” DickinsonLuw Review 92:895-916, 1988.State of Louisiana v. Mathews, 427 F. Supp. 174(D.C. La. 1977).Terry, N., “Politics and Privacy: Refhing the Ethicaland Legal Issues in Fetal Tissue Transplantation,”Washington University Law Quarterly 66:523-551,1988.United States v. An Article of Drug. . . Bacto-Unidisk, 394 U.S. 784 (1968), reh. denied, 395 U.S.954 (1%9).United States v. Calise, 217 F. Supp. 705 (D. C.N.Y.1962).United States v. Evers, 453 F. Supp. 1141 (D.C. Ala.1978).U.S. Congress, Office of Technology Assessment,Human Gene Therapy, OTA-BP-BA-32 (Washing-ton, DC: U.S. Government Printing Office, Decem-ber 1984).U.S. Congress, Office of Technology Assessment,Losing a Million Minds: Con@onting the Tragedy ofAlzheimer’s Disease and Other Dementias, OTA-BA-323 (Washington, DC: U.S. Government Print-ing Office, April 1987).U.S. Congress, Office of Technology Assessment,Life-Sustaining Technologies and the Elderly, OTA-BA-306 (Washington, DC: U.S. Government Print-ing Office, July 1987).
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
76.
U.S. Department of Health and Human Services,Public Health Service, Food and Drug Administra-tion, testimony before the House Committee onScience and Technology, Subcommittee on Investi-gations and Oversight, Nov. 9, 1983.U.S. Department of Health and Human Services,Public Health Service, National Institutes of Health,Report of the Human Fetal Tissue TransplantationResearch Panel (Bethesda, MD: 1988).van der Linden, W., “Pitfalls in Randomized Surgi-cal Trials,” Surgery 87:258-262, 1980.White, R.M., Associate Professor of Medicine andOncology, Howard University Cancer Center, Wash-ington, DC, personal communication, June 12, 1990.Williamson, B., “Gene Therapy,” Nature 298:416-418, 1982.Wion, A., Associate Chief Counsel for Drugs andBiologics, Food and Drug Administration, “hgalIssues Concerning Federal Regulation of Tissues,”paper presented at the American Association ofTissue Banks-FDA colloquium, Washington, DC,Oct. 1, 1989.Wion, A., Associate Chief Counsel for Drugs andBiologics, Food and Drug Administration, “Regula-tory Issues Concerning Organs and Tissues,” paperpresented at the Annual Educational Conference ofthe Food and Drug Law Institute, Washington, DC,Dec. 13, 1989.Woodcock J., Director, Division of Biological Inves-tigational New Drugs, Center for Biologics Evalua-tion and Research, Food and Drug Administration,letter to R. Chin, Office of Technology Assessment,received Oct. 26, 1989.Woodcock, J., Director, Division of Biological Inves-tigational New Drugs, Center for Biologics Evalua-tion and Research, Food and Drug Administration,letter to Wendy Pachter, Office of TechnologyAssessment, received Dec. 14, 1989.Woodcock, J., Director, Division of Biological Inves-tigational New Drugs, Center for Biologics Evalua-tion and Research, Food and Drug Administration,personal communication, June 1990.Woody, K., “Legal and Ethical Concepts Involved inInformed Consent to Human Research,” CaliforniaWestern Law Review 18:50-79, 1981.

Chapter 8
Ethical Issues

CONTENTSPage
ISSUES RELATED TO RESEARCH FUNDING . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 149What kinds of diseases might be treated with this technology? . . . . . . . . . . . . . . . . . . . . . 150What impact do these diseases currently have on society and what threat do they
hold for the future?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 150What alternative surgical or medical treatments are available? . . . . . . . . . . . . . . . . . . . . . 150To what extent does the Federal Government’s commitment to funding biomedical
research extend to neural grafting research?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 151Would finding neural grafting require the government to redirect limited funds
from other areas of research?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 151ISSUES RELATED TO TISSUE SOURCE. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 151
Fetal Tissue.**. *.. ... ... ..*. . *.....................**..*.**...@*..**.***+*.*.* 151Cell Lines. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 159
ISSUES RELATED TO GRAFT RECIPIENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 161Risks to Research Subjects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 161Informed Consent. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 162
SUMMARY AND CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 163CHAPTER 8 REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 165
BoxesBox Page8-A. Just Distribution of Resources and the Funding of Heart Transplants . . . . . . . . . . . 1508-B. Moore v. Regents of the University of California . ....*.*.,..*.........***.,*** 160
FigureFigure Page8-1. Types of Abortion and Morally Relevant Differences Among Them . . . . . . . . . . . 153

Chapter 8
Ethical Issues
Neural grafting is a complex subject for ethicaldiscussion because of the scope of the issues itraises. Ethical arguments surrounding neural graft-ing are part of the continuing debates about themorality of abortion and genetic manipulation, andthey rekindle discussions about the treatment ofresearch subjects and the meaning of informedconsent. This chapter discusses ethical aspects of thevarious neural grafting technologies currently beingresearched.
Some ethical issues raised by neural grafting arenot unique to this technology. One such issue is theallocation of scarce Federal resources, since fundscommitted to neural grafting might be spent onalternative biomedical research or other areas alto-gether. Questions about funding can be addressedwith empirical evidence of the number of individu-als affected by diseases, the availability of alterna-tive treatments, and the economic costs that both thediseases and the treatments create for society.Another general ethical concern is the tensionbetween the Federal Government’s commitment topromoting the public health and funding biomedicalresearch, and its responsibility to respond to publicconcern about certain research and its possibleapplications.
The various grafting materials used also raiseethical issues. Human fetal tissue, in particular, hasgenerated extensive discussion in several forums. Amoratorium on federally funded fetal tissue trans-plantation research was declared in March 1988 bythe Secretary of Health and Human Services and wascontinued indefinitely in November 1989 (see app.A). As a result of this moratorium, a NationalInstitutes of Health (NIH) advisory panel wasconvened and in 1988 issued a report on the ethicsof fetal tissue transplantation (54). The panel’spolicy recommendations were accepted by a largemajority of its members and were accepted unani-mously by the NIH Director’s Advisory Committee.However, the points on which panel membersdisagreed were never resolved, and no action wastaken on the recommendations by the NIH Directoror the Assistant Secretary for Health.
As the technology develops, the use of continuouscell lines as a source of grafting material may also
create general concern. Advances in molecularbiology suggest it may be possible to developeffective brain and spinal cord grafts by geneticallymanipulating cells before transplantation. Geneticmanipulation of cells has generated considerablecontroversy since it was first introduced (49), but thesomatic cell alterations that would be used for neuralgrafting are less troublesome than germ cell genetherapy. On the other hand, as cell lines have beendeveloped, questions have been raised about owner-ship of tissues. Uncertainty about how to determinethe rightful ownership of cell lines could complicatethe use of this material considerably.
The treatment of patients who receive neuralgrafts is another area of ethical concern. Issues ofprotecting patients from undue risk and obtainingadequate informed consent are not unique to neuralgrafting, but they warrant special attention for thistechnology. At this stage of research, some personsquestion whether the risks to research subjects arecomparable to the expected benefits. It is alsoquestionable whether requirements for informedconsent can be met, given the vulnerability of somepersons with neurological disorders.
This chapter describes the ethical concerns thathave been raised about neural grafting. It identifiesissues and presents the various arguments surround-ing them in order to represent the spectrum ofattitudes expressed in public debate.
ISSUES RELATED TORESEARCH FUNDING
Public funding of biomedical technology involvesbroad analyses of the economic benefits and costs,as well as the social benefits and ethical conse-quences, a new technology might have. Knowledgeof economic consequences is necessary for financialplanning but it is also integral to ethical decision-making, since the allocation of public funds raisesquestions about justice and equity. Some personsbelieve that justice requires the expenditure of fundsin areas where they can benefit the greatest propor-tion of the population rather than a few disadvan-taged individuals. If neural grafting techniques arevery expensive to study or to provide as medical
–149-

150 . Neural Grafting: Repairing the Brain and Spinal Cord
Box 8-A—Just Distribution of Resources andthe Funding of Heart Transplants
“On February 1, 1980, the 12 lay trustees of theMassachusetts General Hospital announced theirdecision not to permit heart transplants at thatinstitution ‘at the present time. They noted that itwas difficult to turn away even one patient in needof a heart transplant, but they underlined theimportance of making such decisions ‘in terms ofthe greatest good for the greatest number. ’ In Juneof that same year, Patricia Harris, then secretary ofthe Department of Health and Human Services,withdrew an earlier tentative authorization forMedicare to pay for heart transplants because of theneed to evaluate the technology’s ‘social conse-quences,’ including its costs. In 1987, legislators inOregon made an equally dramatic change in theOregon Medicaid program (the State-Federal pro-gram that provides funds to cover medical needs forfinancially needy citizens in the State). Theydecided not to pay for most transplants in order touse their limited budget for other purposes, Inparticular, they noted that the money that wouldhave covered approximately 30 heart, liver, bonemarrow, and pancreas transplants would instead beused to provide regular prenatal care for 1,500pregnant women. The altered allocation was justi-fied by its proponents because it would save morelives. ’
The controversy about the funding of hearttransplants is an example of the generic ethical
d an expensive medicalissues that may surrountherapy. Neural grafting could provoke similarconsiderations.
SOURCE: T.L. Beauchamp and J.F. Childress, “The Principleof Justice,” Principles of Biomedical Ethics (NewYork, NY: Oxford University Press, 1989), pp.286-287.
therapy, budget restrictions could require that neuralgrafting activity be limited (see box 8-A).
Questions arise about whether the research andapplication of technologies such as neural graftingought to receive Federal support. Some criticsconsider it unjust to spend a great deal of money tobenefit a few persons or to develop a surgicaltechnique for a relatively uncommon conditionwhen the same funds might be used to developmedical treatments that would benefit many morepersons. In order to determine whether expenditureof public funds for neural grafting research consti-tutes just allocation of resources, some background
information is required. The following questions arenot ethical issues, but answers to them could help theFederal government decide whether to fund neuralgrafting.
What kinds of diseases might be treatedwith this technology?
It has been argued that the government ought tofund research that seeks to cure neurological disor-ders that affect large numbers of U.S. citizens (2).Neural grafting is a possible therapy for Parkinson’sdisease, Huntington’s disease, Alzheimer’s disease,spinal cord injury, and other neurological disorders,although whether neural grafting will be successfulin any of these remains to be seen (see ch. 5).
What impact do these diseases currently haveon society and what threat do they hold
for the future?
Neurological disorders exact a high financial tollfrom society, although measures of their costs andstatistics on the number of persons affected varyconsiderably (see ch. 6). Neural grafting has beensuggested as a possible therapy for some age-relateddiseases, e.g., Parkinson’s disease, Alzheimer’sdisease, and stroke. Should neural grafts proveeffective for such diseases and should the prevalenceof these diseases increase with an aging society, thedemand for neural grafts might increase as well.
What alternative surgical or medicaltreatments are available?
If neural grafting is more effective and lessexpensive than alternative treatments for neurologi-cal disorders, an ethical argument could be made forFederal support of neural grafting. For most neuro-logical disorders, however, including Parkinson’sdisease, Huntington’s disease, spinal cord injury,and Alzheimer’s disease, no cures are available andcontrol of symptoms is inadequate. Symptoms ofParkinson’s disease are often treated with L-dopa,but this drug is palliative (it treats only the symp-toms of the disease and not the cause), and itsbenefits diminish as the disease progresses. Somealternative treatments are available or in the processof being developed. For example, a new drug calleddeprenyl shows promise for slowing the progressionof Parkinson’s disease (see ch. 6), although it doesnot stop the progression or affect advanced stages ofthe disease (45). While neural grafting is a promising

Chapter 8-Ethical Issues ● 151
treatment for Parkinson’s disease at this time, it, too,may be only palliative (see ch. 5). Fair allocation ofhealth care resources may require that the financialcosts of neurological disorders now and in the futurebe estimated and compared to the costs of neuralgrafting and alternative treatments. However, fairallocation may also require that resources spent onneurological disorders reflect the impact of thesediseases on society.
To what extent does the Federal Government’scommitment to funding biomedical research
extend to neural grafting research?
Because neural grafting techniques are still beingstudied, the question at this point is whether thegovernment has an obligation to support neuralgrafting research. Given the government’s commit-ment to support basic scientific research and tofurther the health of the Nation, it might be expectedthat basic research which could aid in developingnew neural grafting technologies would be funded.This is, in fact, the case: Only research on theimplantation of human fetal tissue from induced1
abortions does not receive Federal funds (53,57).The moratorium on Federal funding for human fetaltissue grafting research was declared because spe-cific ethical issues surrounding this research cameinto conflict with the government’s general commit-ment to fund basic research. The ethical issuesrelated to fetal tissue grafting will be discussed laterin this chapter.
Would funding neural grafting require thegovernment to redirect limited funds from
other areas of research?
It has been suggested that, in order to fund neuralgrafting research, resources might be provided at theexpense of other projects that could lead to moreeffective or less controversial treatments for neuro-logical disorders (38) or increased “understandingof the fundamental biological principles underlyingthe normal function and dysfunction of the humannervous system” (11). In general, Congress allo-cates funds for biomedical research to Federalresearch agencies, but the distribution of those fundsto the institutes within the agencies and then toindividual investigators falls outside Congress’s
purview (12). Federal research grants are made onthe basis of merit, as determined through peer reviewof research protocols. Neural grafting researchreceives Federal funding when grant proposalsscientifically warrant that support. Withholdingresearch funds from neural grafting frees resourcesfor other projects, but there is no guarantee that thosefunds will be put toward other neurological research.
ISSUES RELATED TOTISSUE SOURCE
Questions about the propriety of federally fundedneural grafting research are not limited to resourceallocation-they also address the propriety of usingvarious graft materials. As discussed in chapter 4, anumber of neural grafting materials are used, someof which are more ethically problematic than others.Autografts and allografts using adult tissue arerelatively free of ethical controversy: For example,the primary ethical reasons for not doing adrenalmedullary autografts to treat Parkinson’s disease arelikely to be related to protection of the researchsubject rather than to the source of the graftingmaterial.
Fetal Tissue
Adult human neural tissue is not a suitablematerial for grafting, so scientists have turned tohuman fetal neural tissue. Fetal tissue is promisingfrom a scientific point of view, but it is also the mostethically controversial grafting material because it isusually obtained from abortions.
While use of aborted fetal tissue in research is notnew, the current ethical arguments surrounding itsuse and the Federal attitude toward funding suchresearch reflect a different level of concern than haspreviously been demonstrated. The use of humanfetal cells played an important role in the develop-ment of vaccines for polio and other childhooddiseases (20,48), and research on the transplantationof fetal thymus glands into infants with DiGeorge’ssyndrome was performed in the United States 20years ago (7,30). The National Commission for theProtection of Human Subjects of Biomedical andBehavioral Research (hereafter referred to as theNational Commission) scrutinized ethical issuesrelated to the use of fetal tissue in research and
l~e Department of He~~ and Human Services referred to “induced abortion” in the fetal tissue IIanSpk@XiOn mOrWOriUm (57). ~e~ tie
moratorium orFederal activity surrounding it is discussed in this chapter, “induced abortion” will be used. Where a distinction is made between differenttypes of induced abortio~ more specific terminology will be used.

152 . Neural Grafting: Repairing the Brain and Spinal Cord
developed the guidelines used to create the 1975Federal regulations for use of fetal tissue in research(52). The National Commission’s report and theregulations that developed from it [45 CFR 46]focused on research performed on living fetuses andpaid little attention to fetal cadavers. Both specifiedonly that research on cadaveric fetal tissue should“be conducted in accordance with commonly heldconvictions about respect for the dead, and inaccordance with State and local laws” (10). Nomoral distinction was made about the means of fetaldeath. As a result, research using aborted fetal tissuefor experimental purposes has been, and continues tobe, relatively uncontroversial. The moratorium onFederal funding of research involving transplanta-tion of human fetal tissue obtained from inducedabortions into humans is a recent exception (see app.A).
Fetal Research v. Fetal TissueTransplantation Research
What makes transplantation research differentfrom other research that uses cadaveric fetal tissue?Some persons perceive a significant ethical differ-ence. In fetal research,2 cadaveric fetal tissue is usedto develop a treatment; in fetal tissue transplantationresearch, fetal tissue is the treatment (43). Thesepersons question whether fetal tissue should be usedto benefit an individual recipient.
On the other hand, some persons perceive noethical difference between the transplantation ofcadaveric adult organs and tissues and those ofcadaveric fetuses. Unless the decedent has explicitlyrefused to donate body parts, adult cadaveric tissuesmay be donated by the next of kin as a gift and maybe removed for transplantation by a coroner ormedical examiner. Once these conditions are met,tissues may be used to benefit a single recipient. Inthis view, cadavers do not have protectable interests,and tissue from dead fetuses is no different thantissue from dead adults.
Procurement of Fetal Tissue
Most ethical objections to the use of fetal tissuefor neural grafting relate to tissue procured fromnontherapeutic induced abortions (to be referred tohereafter as elective abortions) (see figure 8-l).Many persons who object to the use of fetal tissue
from elective abortions have suggested that fetaltissue from spontaneous abortions (miscarriages)could be used for transplantation without ethicalobjection because fetal death is not intended. Thefirst human fetal nervous system grafts used tissuefrom spontaneous abortions (29), but since sponta-neous abortions are seldom anticipated and usuallytake place outside a hospital, it is difficult to collectthe tissue for grafting. Tissue from therapeuticinduced abortions for cervical cancer or ectopicpregnancy has also been suggested as an ethicallyunobjectionable alternative, since protection of thepregnant woman’s life, not the termination ofpregnancy, is the primary purpose of the abortion.There is some question, however, as to whether aphysiological anomaly that caused the pregnancy tobe terminated (as evidenced by spontaneous abor-tion, ectopic pregnancy, or cancer) would make thetissue inappropriate for grafting (10,39). Ectopicpregnancy is more likely to result from a physiolog-ical anomaly of the woman than a defect in the fetus(17), but without thorough genetic and physiologicaltesting, the use of tissue from spontaneous andtherapeutic induced abortions for neural graftingmight be considered unethical because of the risk tothe recipient if the graft material is infected with avirus or bacteria or has a genetic anomaly that couldaffect the recipient (3,10,39). While grafting fetaltissue from spontaneous abortions and therapeuticinduced abortions could avoid association of neuralgrafting with elective abortion, it may not be apractical source of graft material.
Some persons object to the use of electivelyaborted fetal tissue for grafting because procurementof the neural tissue might cause pain or even deathto the fetus. Research has indicated that neural tissuefrom electively aborted fetuses between 8 and 12weeks of development is the most clinically appro-priate for neural grafting (48). This early stage ofdevelopment makes it unlikely that a fetus would beviable after an abortion procedure (5). First-trimesterabortions are usually performed by vacuum aspira-tion, a procedure that seldom results in a live, or evenintact, fetus (10). Concern has been expressed,however, that elective abortions performed at a latergestational age might allow a fetus to survive theprocedure and that the separation of neural tissue forthe graft would not only cause great pain but could
me National Commission report and the Federal regulations for fetal research identify several types: activities &ted toward fetuses in utero assubjects, activities directed toward viable fetuses ex utero, activities directed toward nonviable fetuses ex utero, and activities involving the dead fetus,fetal material, or the placenta [45 CFR 46].

Chapter 8--Ethical Issues ● 153
Figure 8-l—Types of Abortion and Morally Relevant Differences Among Them
Without any qualification, the term “abortion” reveals nothing except that a pregnancy has ended.This termination is not usually considered morally bad in itself. Spontaneous abortions may beconsidered unfortunate but are not usually considered morally blameworthy. The abortions that usuallygenerate ethical controversy are those that are induced.
There are two types of induced abortions: therapeutic and nontherapeutic. Although some personsobject to any induced abortion on the grounds that the premature termination of fetal life constitutesmurder, others find that moral distinctions may be made, depending on the reason for the abortion.Conditions such as cancer of the cervix or uterus and ectopic pregnancy will usually lead to the deathof both the pregnant woman and the fetus if the pregnancy is not aborted. If the life of the woman isendangered by cervical cancer, the Roman Catholic Church teaches that “the treatment is not really anabortion, even though the fetus dies. The intent of the action is the removal of the life threateningrendition, and the death of the fetus is a foreseen but unintentional consequence.” Other persons arguethat when a fetus’s and a woman’s rights to life conflict, the woman’s life maybe saved at the expenseof the fetus’s. There are many other points of view on this question. Although there is some disagreementas to whether a pregnancy maybe terminated if bringing the pregnancy to term will result in the deathof the woman but the birth of a baby, therapeutic induced abortion is not as controversial asnontherapeutic induced (elective) abortion. Many reasons have been put forth for both the morality andthe immorality of nontherapeutic induced abortion.SOURCES: Adapted from M.B. Mahowald, “Neural Fetal Tissue Transplantation: Should We Do What We Can Do?”
Neuro/ogic C/inics 7:745-757, 1989; A. Moraczewski, regional director, Pope John XXIII Medical, Moral,Research, and Education Center, Houston, TX, personal communication, April 1990.
actually cause the death of the fetus (27). The use ofa living fetus for transplantation is a form ofvivisection, which is generally recognized to beunethical and which, moreover, is prohibited byFederal law: As long as the fetus is alive, its tissuesmay not be removed for any research or therapeuticprocedure [45 CFR 46]. The distinction between alive fetus and a dead fetus with living tissue isextremely important in this regard.
Arguments For and Against Human Fetal TissueTransplantation Research
Arguments for and against using electivelyaborted fetal tissue for neural grafting address theissues raised by research already under way and thefuture use of fetal tissue grafting on a large scale.These arguments raise four main questions:
. Is the means of fetal death ethically relevant toany subsequent use of the tissue?
. Is it ethical to use electively aborted fetal tissueas therapeutic treatment for another individual?
. What are the ethical implications of a publicpolicy that supports fetal tissue transplantation
research?● Whose consent, if any, is necessary for the use
of aborted fetal tissue for neural grafting?
Is the means of fetal death ethically relevant toany subsequent use of the tissue ?-While disputesover the morality of abortion have complicated andpoliticized discussions about the use of electivelyaborted fetal tissue for neural grafting, the ethicalrelevance of an elective abortion to the transplan-tation of fetal tissue is the true subject of publicdebate. Both opponents and supporters of elec-tive abortion rights have articulated a number ofreasons for supporting fetal tissue transplanta-tion research, and both have also identifiedreasons for not doing so.
The main argument supporting fetal tissue trans-plantation states that there is no relevant differencebetween the transplantation of cadaveric fetal tissue(i.e., tissue from a dead fetus) and any othercadaveric tissue. (This position has been taken byboth supporters and opponents of elective abortion.)The argument, which claims that it is not unethicalto use tissue from elective abortion, is based on the

154 ● Neural Grafting: Repairing the Brain and Spinal Cord
premise that by the time the fetus becomes a possiblesource of transplantation tissue it is already dead andthat the reamer of death is irrelevant to anysubsequent use. The NIH Human Fetal TissueTransplantation Research Panel compared the use oftissue from a dead fetus and the use of tissue fromaccident and murder victims. The persons fromwhom organs are obtained are already dead, andusing the organs in no way harms them, deprivesthem of respect, objectifies them, or uses them as ameans to another’s end. Neither does it indicateapproval of the death or the manner in which it wasbrought about. On the contrary, using organs andtissues from these victims is thought to allow somegood to come from their death and thus is morallypermissible.
Another argument suggests that there is a moralobligation to help others when it is possible to do soand thus it is unethical not to use tissue from electiveabortions. Some persons believe that since theaborted fetus is already dead and its tissue legallymay be used for research and medical treatments,and since fetal tissue grafts may benefit others,preventing use of that tissue is ethically reprehensi-ble. They believe that since the dead have nointerests to protect, using fetal tissue does not harmthe fetus physically or morally. They believe thatusing cadaveric fetal tissue for grafts that relievesuffering is morally good and thus perceive anethical imperative to use that tissue to help others.
Other persons disagree with the claim that themeans of fetal death is morally irrelevant to the useof the tissue for grafting and perceive a moralobligation not to use fetal tissue for transplantation.Many of these persons also strongly oppose abor-tion. One argument is that using electively abortedfetal tissue for neural grafting indicates indifferenceto the means of fetal death. Another argument saysthat using aborted fetal tissue for neural graftsconstitutes post facto complicity in murder (8).Those who hold this position argue that becauseabortion is murder, the procurement of fetal tissuefrom abortion clinics requires collaboration withmurderers. For example, since surgeons who per-form neural grafting must have access to fetal tissue,they must work hand-in-hand with abortionists toobtain the tissue while the cells are still alive. Unlikesurgeons who retrieve organs from murder oraccident victims, those who retrieve and transplantaborted fetal tissue participate retroactively in thekilling by obtaining the consent of the pregnant
woman for use of the tissue (in cases where this isdone), by collecting fetal tissue from those whoperform abortions, and in some cases by killingnonviable abortuses when separating neural tissuefor grafting.
Is it ethical to use tissue from an electivelyaborted fetus as therapeutic treatment for anotherindividual?—While transplantation of cadaverictissues has become a common practice and isregulated under the Uniform Anatomical Gift Act(UAGA) in all 50 States (see ch. 7), some personsobject to the use of fetal tissue for transplantationinto individual recipients on the principle that oneshould not treat the fetus as the means to another’send. They believe the “consideration of any class ofhuman subjects as no more than a commodity to beused for the benefit of others is wrong” (27). Theydo not believe that the alleviation of sufferingjustifies the use of aborted tissue. In their belief, nomatter how good an outcome might derive from fetaltissue transplantation, it does not justify the moraldevaluation of the fetus necessary for that outcometo occur.
Other persons question why the transplantation ofcadaveric fetal tissue should be treated differentlyfrom the transplantation of any other cadaverictissue. The use of cadaveric adult organs is rarelyregarded as indicative of disrespect, commodifica-tion, or devaluation (56). Why, then, should trans-plantation of cadaveric fetal tissue be considered amoral devaluation? Some persons believe transplan-tation of cadaveric tissue into individuals is moreacceptable than using it for general research, since‘‘it may do more good to heal than simply learn howto heal” (31).
What are the possible consequences of a publicpolicy that supports fetal tissue transplantationresearch?—Some persons are concerned that Fed-eral funding of fetal tissue transplantation researchwould lead to an increase in the number of abortionsperformed in the United States. The Department ofHealth and Human Services (DHHS) expressed thisconcern in continuing the human fetal tissue trans-plantation research moratorium in November 1989.These persons believe women may decide to abort ifthey believe fetal tissue could help another personand that women who are ambivalent about theirpregnancies will consider fetal tissue grafting ajustification for having an abortion (35). If fetaltissue grafting research shows promise for Parkin-

Chapter 8--Ethical Issues . 155
son’s disease or other disorders, they argue, thesupply of fetal tissue will not satisfy the demand.Elective abortion might implicitly or explicitly beencouraged in order to make more fetal tissueavailable. Some persons believe it would be ethi-cally unacceptable if the ability to donate fetal tissuefor grafting influenced even one woman’s decisionto have an abortion (35).
Other persons disagree that elective abortionwould have to be encouraged to make fetal tissueavailable for grafting. Some claim that the numberof elective abortions already being performed in theUnited States would provide adequate tissue even ifneural grafting became standard practice (13). As isthe case with kidneys, hearts, and other body tissuesthat are transplanted, the number of neural graftingprocedures performed could be limited to theamount of fetal tissue already available (30). Also,the development of continuous cell lines might makeit unnecessary in some cases to procure newlyaborted tissue. Fetal tissue might be used to start acell line without increasing the number of abortionsthat take place and might not therefore be ethicallyobjectionable to some persons (34). Currently, thereis no evidence to support or refute the contention thatfetal tissue grafting research would cause an increasein the number of abortions performed, either becauseof a need for grafting material or because womenperceive an altruistic justification for elective abor-tion.
Women’s groups in particular have objected to theclaim that the opportunity to donate fetal tissue fortransplantation after an elective abortion wouldaffect a woman’s decision to terminate a pregnancy,even if she did believe that this use of fetal tissuewould do good. Other persons argue that requiringanonymity between tissue donors and graft recipi-ents would make specified donation impossible inthe event that a woman wanted to provide neuralgrafting material for a specific recipient.
Whose consent, if any, is necessary for the use ofaborted fetal tissue for neural grafting?--Consentis generally required for participants in researchprotocols and for donors of tissue. It is not certain,however, what role consent would play in donatingfetal tissue for neural grafting research, and there isdebate about who should give it.
The donation of adult cadaveric tissue for trans-plantation, and fetal tissue in some States, is
32-801 0- 90 - 6 : QL 3
regulated under the UAGA (see ch. 7). As fetal tissuegrafting research progresses, the models for obtain-ing consent may have to be modified to include fetaltissue donation, or a new model may have to becreated. Those who believe fetal tissue transplanta-tion is analogous to the transplantation of othercadaveric tissue find it appropriate for the next ofkin, in this case the woman who has the abortion, togive consent to use fetal tissue for transplantation.However, some persons challenge the woman’sauthority to give this consent, since, according totheir view, she is also the cause of the fetus’s death.Consent for fetal tissue use in neural grafting fallsbetween existing regulations and practices.
Some persons hold that a woman’s prerogative todonate fetal tissue stems not from her legal status asnext of kin, but from a basic right to control her ownbody and its products. They believe that seekingconsent to examine or use fetal remains is consistentwith the treatment accorded any other tissue or organremoved during surgery, thus to deny a woman theopportunity to specify what should happen toaborted fetal tissue would be to deny her autonomy(10). Consent should be obtained out of respect forthe interests of the woman, who may want the tissueto be handled a certain way after the abortionprocedure. For example, some women may hope tobenefit another person by donating aborted fetaltissue for transplantation, while other women maywant to dispose of the tissue. Whatever the decisionand whatever the reason for it, these persons arguethat the decision should be the woman’s.
Some persons believe that fetal tissue is not thewoman’s to donate. They believe that no fetus isproperty merely because it is sustained by anotherperson’s body; more important, they believe thatafter the abortion has taken place and the fetus is nolonger part of the body, a woman’s claim to bodilyproperty carries even less weight (8,11). Thesepersons argue that the only reason to obtain theconsent of the pregnant woman would be for her toact as proxy for a fetus to be used in research [underthe Protection of Human Subjects Act [45 CFR 46].Proxy decisionmaking assumes the surrogate deci-
to act in the interests of thesionmaker’s commitmentincompetent. Since the woman clearly does notintend to protect the fetus, they believe it isinappropriate for her to act as the fetus’ proxy; sheshould have no say over what happens to the tissue(8).

156 ● Neural Grafting: Repairing the Brain and Spinal Cord
The donation of cadaveric tissue need not be seenstrictly in terms of property or proxy, however. Thedonation of adult cadaveric tissues by family mem-bers is done in the context of a gift-giving model thatneither recognizes property rights on the part of thefamily nor grants guardianship or proxy. The factthat the woman’s consent is obtained does notnecessarily mean she acts as proxy for the fetus,since her role would be to consent to tissue donation,not research participation. Some persons believefetal tissue donation is consistent with the acceptedgift-giving model for organ donation and constitutesan altruistic act women are morally free to take.Others, however, believe that electively aborted fetaltissue is an inappropriate gift (10).
It has also been suggested that no consent isneeded to use fetal tissue for grafting research. Sinceelectively aborted fetal tissue is normally discardedwithout any specification on the woman’s part, itmight be justifiable to consider the abortus aban-doned and to use it without consent. This methodmight avoid the obstacles created by views ofcompeting rights (the woman v. the fetus); however,refusing to acknowledge protectable interests on thepart of either the woman or the fetus could beinterpreted as exploitation. Although tissues andorgans from adult cadavers can be used for trans-plantation without the consent of family members,some women might prefer that the tissue not be usedfor transplantation. Using the fetal tissue without theconsent of the woman could create more problemsthan it solves.
If it is decided that it is ethically appropriate ornecessary to obtain the woman’s consent, thequestion of when to solicit consent is raised. Thereis some agreement that consent should be obtainedonly after the woman has conclusively decided toabort, in order to separate the decision to abort fromthe decision to donate fetal tissue (1,32,48,54). Itmay also be possible to obtain consent tier theelective abortion has been performed and the tissuehas been identified as suitable for transplantation,especially if the tissue is frozen before transplanta-tion, although this option is not entirely free ofethical problems (see box 4-A).
The protocol used in one privately funded fetaltissue transplantation trial solicited consent from thewoman after the abortion had been completed (16).The consent form specified that fetal tissue wasbeing solicited for research purposes, which could
include fetal tissue transplantation research. Thisapproach provides the woman an opportunity toprevent the use of the tissue for grafting, while notinfluencing her decision to maintain or terminate thepregnancy. Other investigators may choose not torequest consent immediately after abortion becauseit could be emotionally stressful for the woman (14),although some persons believe that there is nodifference between requesting consent for tissuefrom a woman who has just aborted a pregnancy andrequesting organ donation from the family of adeceased adult.
The consent forms used for other fetal tissueresearch may not be comprehensive enough toaddress all aspects of grafting. It is not clear whetherthe abortion consent forms which allow fetal tissueto be donated for research should include clausesspecifying that the tissue might be used for trans-plantation. A separate consent form for fetal tissuetransplantation might be appropriate.
Relationships Among the Questions-Attitudestoward consent for the donation of fetal tissue fortransplantation are likely to be consistent withbeliefs about the relevance of the means of fetaldeath to fetal tissue transplantation, the appropriate-ness of using cadaveric fetal tissue for therapeuticpurposes, and the ethical implications of publicpolicy that supports this research. The presentdiscussion delineates issues for the sake of illustrat-ing different aspects of the debate, but the argumentsof individuals and groups who discuss the ethics offetal tissue transplantation research are often morefluid.
For example, some persons who oppose fetaltissue transplantation research because they believesuch grafting is complicitous with murder readilylink three of the four questions discussed above.They feel that the means of fetal death is relevant tografting fetal tissue because elective abortion is theunjust killing of innocent human beings. A womanwho has an abortion therefore should not serve as itsproxy. Public support should not be given to fetaltissue transplantation research because it wouldconstitute public approbation for unjust killing (26).
Similarly, some persons who do not object to fetaltissue grafting research argue that the means of fetaldeath is irrelevant. They believe that once a fetus isdead, it has no interests to protect and maybe treatedin the same reamer as adult cadaveric tissue.Consent for its use should therefore be solicited from

Chapter 8--Ethical Issues ● 157
the next of kin, which in this case is likely to be thewoman who has the abortion. These persons feel thatpublic support of fetal tissue transplantation re-search would be consistent with other fetal tissueresearch and cadaveric organ donation and wouldhave no specific ethical implications.
Issues Surrounding Fetal Tissue Transplants asStandard Therapy
The preceding arguments have been presented inpublic debates about the ethical implications of fetaltissue transplantation research. Some of the potentialproblems can be illustrated dramatically by describ-ing the consequences should fetal tissue graftingbecome standard therapy. (“Standard therapy”describes procedures that are no longer regulated asresearch.)
Some persons have expressed concern that Fed-eral support of fetal tissue transplantation throughfunding or regulation of the procedure wouldlegitimize and institutionalize elective abortion.3
Others persons contend that since elective abortionis legal, and since the Federal Government profitsfrom it by taxing abortion clinics (3), it is alreadyboth legitimate and institutionalized. They arguethat claims that Federal support of neural graftingresearch would further institutionalize the practicecarry no weight. Fetal tissue from elective abortionswould be used after the abortion has already takenplace and would have no effect on law or policyconcerning abortion itself. Still other persons be-lieve that even though elective abortion is legal, itshould not be encouraged. If fetal tissue transplanta-tion is accepted as a medical treatment, they believeit maybe impossible to make abortion illegal again.Even some persons who support the freedom to havean abortion do not necessarily consider it a practicethey would like to see endorsed by a public policy;i.e., while abortion should be legal, it does not followthat fetal tissue should be used for neural grafting.
Another concern is that the use of electivelyaborted fetal tissue as standard therapy may lead tocommercial exploitation of fetuses. This concern hasalso been expressed in more extreme terms: Someargue that using aborted fetal tissue for neuralgrafting may make it a commercially desirablecommodity and lead to the establishment of a fetal
tissue industry. As in the development of reproduc-tive technologies and the increase of surrogatemotherhood, the growing demand for neural graftsmight cause the fetus to be increasingly perceivedonly as a potential source of grafting material. It hasbeen argued that the fetus should neither be endowedwith a financial value, as it would be in a commercialexchange, nor be conceived for the sole purpose ofusing its tissue for transplantation (1,13,48,54). In1988, the National Organ Transplant Act wasamended to prohibit the sale of certain fetal organsand tissues, although neural tissue is not specified[Public Law 100-607].
Precautions against this consequence have beensuggested. If it were likely that women could becoerced into conceiving and aborting in order toprovide fetal tissue to benefit others, profit restric-tions might create a disincentive. Payments towomen who abort, including compensation for thecost of the abortion procedure, might be prohibited,as might payments to doctors, clinics, or any otherparties involved in the abortion procedure. Tissuebanks used to distribute fetal tissue maybe prohib-ited from profiting from their role. To preventwomen from conceiving in order to provide tissuefor grafts, specification of tissue recipients, includ-ing the woman herself, might also be prohibited(1,32,48,54).
Concern has been expressed that women, as the‘‘producers’ of fetal tissue, could also be commer-cially exploited in order to obtain tissue in adequatequantities and of useful gestational age. There hasbeen some suggestion that women who are ambiva-lent about terminating their pregnancies may bevulnerable to coercion by a physician who wants thefetal tissue for research or for another patient. Thisthreat might be removed by requiring absoluteseparation of the doctors who perform abortions andthose who do transplantation. One way to accom-plish this might be to establish tissue banks for fetaltissue distribution, as is being done in Great Britain(44).
On the other hand, there have been strongobjections to the assumption that women havelimited abilities to make their own reproductivechoices and that they can be easily coerced. Similarconcerns have been raised about women who act as
3~@~tion is described by the center for Biom~ical Ethics (10) as the justifkation of an act or practice “in such a manner that Others become
more inclined to regard it as acceptable and to engage in it. ” Institutionalization may be seen to carry legitimation one step further, in that institutions(in this case the U.S. Government), by incorporating a practice, accept and engage in it, and in some cases profit fmncially from it.

158 . Neural Grafting: Repairing the Brain and Spinal Cord
surrogate mothers. The charge that the practice ofsurrogacy exploits women has been called paternal-istic because:
It questions women’s ability to know their owninterests and to enter into a contractual arrangementknowingly and competently. There may well be acoercive aspect to commercial surrogacy, sincemoney. . . can serve as a coercive inducement to dosomething a person might not otherwise do voluntar-ily. . . . What they are really saying is that those whoelect to enter surrogacy arrangements are incompe-tent to choose and stand in need of protection (28).
Many persons also have rejected the argument thatwomen need to be protected from solicitation of fetaltissue.
The question of whether a woman’s medical caremight be altered (either with or without her consent)in order to obtain tissue of an appropriate gestationalage and in the best possible condition for graftinghas also been raised (33). There is general agreementthat the means and timing of an abortion should bebased on the pregnant woman’s medical needs andnot on the future use of the fetal tissue (32,48,54). Onthe other hand, not all variations in medical treat-ment will cause harm to the woman. Requiring thatthe woman’s medical care always be placed first,that the timing and method of abortion not be altered,that separate doctors perform abortion and neuralgrafting procedures, and that only first-trimesterabortuses be used might ensure that obstetrical careis not compromised for the sake of neural grafting.
Some fear that using electively aborted fetal tissuefor grafting would gradually erode respect forhuman life. This argument can be seen in terms of aslippery slope, and what is perched at the top of theslope is our view of humanity. The concern is that,as society becomes accustomed to a new technologyand its social consequences, social effects whichnow seem extreme or immoral might becomeacceptable. The increments by which society movestoward policies that are now appalling to somepersons may pass unnoticed, and the result might bea society that by current standards is ethicallyunacceptable. A gradual acceptance of new develop-ments, however, does not necessarily mean thatethical standards erode. Another interpretation of thesame evidence might be that society learns fromexperience and that as current fears are provenunfounded or preventable, they are cast away.
When the practice of retrieving organs fromaccident and homicide victims first began in the1960s, many persons held similar fears aboutwhether transplanting those organs was morallyacceptable without the prior consent of either thedeceased or the deceased’s next of kin (21). Thisconcern was alleviated to a large extent as it becameclear that cadaveric tissue could be transplantedwithout violating most ethical standards for treat-ment of the dead [although some religious traditionscontinue to oppose the practice (40)]. Each Stateestablished standards for the use of cadaveric tissuethat respected not only the cadaver, but the familieswho were asked to make the decision to donate.Although familial consent for cadaveric organs isnot a legal necessity in all cases, it is customarilyobtained before organs are removed. This practicehas alleviated many fears about moral violationsagainst both the deceased and the living. Fetal tissueuse might be regulated in a similar manner.
There is some concern that, since there is nodistinct time when a procedure stops being researchand becomes standard therapy, fetal tissue graftingmight be put into widespread use despite ethicalobjections to it and without ethical norms to guide it(see ch. 7). If such research becomes standardtherapy, there may be no way to control or restrict itsuse, even if ethical reasons are found for doing so. Ifan experimental therapy, especially one funded withtax dollars, proves successful, it might be extremelydifficult to deny that treatment to a demandingpublic, whatever social and ethical consequences itmight have and whatever alternative treatmentsmight be forthcoming. It can also be argued that it isunfair to withhold a treatment from the taxpayerswho funded the research that developed it.
It is not necessarily the case, however, that fetaltissue grafting techniques will become standardtherapy (41). While it is reasonable to expect thatthey will, continuing research could reveal informa-tion about the etiologies of diseases and the mecha-nisms of neural repair that suggest better or lesscontroversial alternatives to fetal tissue. Fetal tissuetransplantation research may lay the groundwork forother therapies without ever being used widely itself.In that case, present concerns could prove un-founded.
At this stage of scientific research it is difficult topredict accurately what the consequences of wide-spread fetal tissue grafting are likely to be. By the

Chapter 8--Ethical Issues ● 159
time adequate research has been done and a proce-dure is proven effective, there maybe a more certainfactual basis for any ethical discussions. At the sametime, Federal standards for the procurement of tissueand regulation of technology transfer might preventmany of the anticipated consequences.
Cell Lines
Continuous cell lines (CCLs) promise self-perpetuating cells that can be propagated indefi-nitely. When the small number of cells used toinitiate a cell line are derived from a consentingparticipant, there are few ethical implications relatedto the tissue itself, although there may be questionsof ownership of the cell lines (50). CCLs derivedfrom fetal tissue may be one of the more scientifi-cally promising neural grafting materials, but ethicalissues arise from the fact that cadaveric fetal tissuemay be used to start them, and ownership of thetissue will be difficult to determine.
The use of CCLs could either perpetuate orresolve the debate about the use of electively abortedfetal tissue for transplantation, depending on whichof the arguments described in the previous sectionare accepted. Those who believe that electiveabortion is immoral and that any subsequent use ofthe tissue is also immoral are likely to object to fetaltissue CCLs for the same reason they object to fetaltissue transplantation (8).
Objections may be weaker, however, on the partof persons who object to fetal tissue transplantationon the grounds that it might promote abortion(11,34), decrease the value of human life, or use thefetus as the means to another’s end. Theoretically,only a few cells from a fetus would be needed for allfuture fetal tissue grafting. Thus, far less tissuewould be needed to start a CCL than would beneeded to provide a neural graft. If fetal tissue fromspontaneous or therapeutic abortions is thoroughlytested for any genetic anomalies or disease, suchtissue might be used for cell lines, ensuring that fetaltissue grafts will not increase the number of electiveabortions that take place. Using CCLs might alsomake it improbable that a woman would conceive inorder to provide aid to a specific recipient. Continu-ous fetal cell lines may make it possible to use fetaltissue for transplantation without leading to antici-pated undesirable consequences.
Ownership of Tissue Used in Cell Lines
The question of whether the person whose cellsare used to start a cell line has proprietary claim overthe line is another new and as yet unresolved issue.A California appellate court ruled in 1988 in Moorev. Regents of the University of California (37) thata plaintiff whose tumorous spleen was used to starta commercially profitable CCL without his permis-sion has property claims over his body tissues andany commercial products derived from them. TheCalifornia Supreme Court reversed this decision inJuly 1990-the majority, consenting, and dissentingopinions were all based on ethical concerns, al-though they reached different conclusions (see box8-B). Until this issue is decided by legislative actionor the U.S. Supreme Court, however, there are noclear legal rules for identifying property rights overbody parts.
The question of ownership of fetal CCLs adds tothe confusion. Claims that women have propertyrights over fetal tissue have been challenged indebates about abortion and consent for tissue dona-tion, and these claims may be more contentious ifbodily property becomes marketable.4 Because thedevelopment of CCLs can be very profitable,questions of ownership of body tissues and cell linesderived from them have become increasingly impor-tant.
As previously discussed, it has not been estab-lished whether the basis for requiring consent for theuse of aborted fetal tissue from the woman whoelects the abortion is an acknowledgement of herownership or her guardianship of fetal tissue, or evenwhether her consent is seen as appropriate at all. Iffetal tissue donation is an act of altruism, the samejustification used for other types of fetal tissueresearch may hold. It is arguable, however, thataltruism is not the motivation for a gesture that couldbe extremely profitable to the person who givesconsent. If the consent requirement is based on anassumption of ownership, consent provides a meansfor the donation of personal property. But should apregnant woman be considered a partial owner of thecell line, based on proprietary rights? Is it ethical toregard the woman as the owner of fetal tissue thatcan be used in a commercial undertaking? Is she
4,,htie M o o r e ~me, rheappelkkcomheld tit “O 00 even though full property rights are not recognized in a dead body, a limited property interesthas been found. . . . Eowever, w]e are not called upom nor are we attempting, to resolve the complex issues relating to the human fetus’’.

160 ● Neural Grafting: Repairing the Brain and Spinal Cord
Box 8-B—Moore v. Regents of the University of California
The case John Moore brought against the investigators who used his body tissues to start a commercialcontinuous cell line raises fundamental questions concerning a patient’s right to the control of his or her own bodyand whether the commercial exploitation of a patient’s cells by medical care providers, without the patient consent,gives rise to an action for damages.
In 1976, Moore sought medical treatment at the Medical Center of the University of California, Los Angeles,for a condition known as hairy-cell leukemia As a necessary part of the treatment for this disease , Moore’s spleenwas removed.
Without the patient’s knowledge or consent to donate his cells for research, the medical staff examined theexcised tissue and determined that Moore’s spleen cells had unique qualities. Through genetic engineering, theydeveloped from the spleen cells a cell line that is capable of producing pharmaceutical products of enormoustherapeutic and commercial value. The university patented the cell line, along with methods of producing manyproducts from it, The university also entered into a series of commercial agreements for rights to the cell line andits products with two corporations. The commercial value of the products was predicted to be approximately $3billion by 1990.
Moore sued the university and the corporations on several grounds, one of which was that “had he known whatwas taking place, he would not have consented to the splenectomy for these research and commercial activities;would have insisted on participating in control of the use of his blood and bodily substances; would not havepermitted these materials to be used by defendants solely for their independent research, commercial activity, andeconomic benefit; would have considered treatment at another medical facility where his wishes would have beencarried out; and would have sought participation in the economic benefit.
The first court dismissed the case. The appellate court found that:The Protection of Human Subjects in Medical Experimentation Act, adopted m 1978, expresses a strong public
policy that medical experimentation on human subjects "shall be undertaken with due respect to the preciousness ofhuman life and the right of individuals to determine what is done to their own bodies” [Cal. Health & Safety Code24171] [emphasis added]. . . . The essence of a property interest-the ultimate right of control--therefore exists withregard to one's own human body.
The California Supreme Court found in July 1990 that:Neither the Court of Appeals’ opinion, the parties' briefs, nor our research discloses a case holding that a person
retains a sufficient interest in excised cells to support a cause of action for conversion. . . . There are three reasonswhy it is inappropriate to impose liability for conversion based upon the allegations of Moore’s complaint. First, afair balancing of the relevant policy considerations counsels against extending the tort. Second, problems in this areaare better suited to legislative resolution. Third, the tort of conversion is not necessary to protect patients’ rights.
Rather than deciding on property rights over body tissues, the Supreme Court held:. . . that a physician who is seeking a patient’s consent for a medical procedure must, in order to satisfy his fiduciaryduty and to obtain the patient’s informed consent, disclose personal interests unrelated to the patient’s health, whetherresearch or economic, that may affect his medical judgment.
This decision applies only to California Without congressional action or a ruling by the U.S. Supreme Court, Statecourts and legislatures are free to decide for themselves whether an individual who donates body tissue should bethought to own it or be able to profit from its use in the development of cell lines and other biologics.
SOURCES: Moore v. Regents of tbe University of California, 202 Cal. App.3d 1230,249 Cal. Rptr. 494 (1988), reh. granted, 252 Cal. Rptr.816, 763 P.2d 479 (1988); Moore v. Regents of the University of California, Supreme Court of the State of California, case No.S006987, July 9, 1990.
entitled to profit from the fetal cell line, or would that any profit from products of her own body butconstitute exploitation of the fetus? allowing others to-profit may be exploitative of and
discriminatory against those women.It might be possible to prevent women who donate
fetal tissue from profiting from cell line develop- Waiving the consent requirement might be onement, but what about allowing investigators to profit way of avoiding these pitfalls. This would indicatefrom the cell line? This, too, could be perceived as that a woman does not have proprietary rights to theexploitation of the fetus. Also, denying the woman fetus and that a proxy donation is inappropriate in

Chapter 8--Ethical Issues . 161
this case. It might ensure that fetal tissue is notdonated purely for personal profit and eliminatecompetition for women to donate their fetuses inorder to profit. On the other hand, if consent is notobtained from women, this omission could be seenas denial of autonomy or exploitation. The recentMoore decision could make patients more reluctantto donate tissues and organs for research.
The question of ownership of fetal tissue used forCCLs will have to be addressed by State or Federallegislatures at some point. The fact that cell linedevelopment may be financially profitable compli-cates fetal tissue donation for scientific purposes. Ifa woman who undergoes an abortion donates fetaltissue for cell line development and profits from thecell line, it could be perceived as exploitation of thefetus. If she does not receive any payment from acommercially profitable cell line, but other personsdo profit from it, it could be perceived as exploita-tion of both her and the fetus. If consent is notobtained from the woman, it may constitute a denialof her autonomy. Finally, if one believes that theindividual from whom cells are obtained to start aCCL is the only one who should consent to this use,then consent should only be obtained from the fetus.Should fetal tissue cell lines be prohibited? Shouldthe scientists who develop cell lines be denied theopportunity to profit financially from them? Arethere justifications for using fetal tissue to startCCLs that make it unnecessary to decide whetherfetal tissue ought to be considered property? Thesequestions are only beginning to be addressed.
Genetic Manipulation of Cells Used for Grafting
Genetically modified cells have been used forneural grafting in animal experiments. The possibil-ity of using them in humans raises the question ofwhether it is ethical to manipulate genes that wouldbe passed on to future generations. As this debate hasdeveloped, it has become clear that somatic cell genetherapy (which modifies the DNA of certain differ-entiated cells in the body that cannot be passed tooffspring) is relatively uncontroversial; it is germcell gene therapy (which modifies undifferentiatedcells that may later become gametes and thus may bepassed to offspring) that creates concern (49).Genetic manipulation of CCLs for neural graftingwould constitute somatic cell gene therapy and thusremove any possibility of inheritance.
Many of the fears expressed about genetic manip-ulation have to do with possible eugenic misuses—
namely, the use of gene therapy to promote orexaggerate desired qualities in individuals ratherthan to correct anomalies that lead to illness. At thistime it is difficult to see how gene therapy could beperformed on cells for enhancement purposes: Notenough is known about the brain to design grafts thatwould improve particular physical or intellectualabilities. Instead, gene therapy might be used todesign grafts that could alleviate specific neurologi-cal disorders in a host—by producing neurotrophicfactors or neurotransmitters, for example. Graftscould be engineered to compensate for specificdeficiencies in the recipient.
ISSUES RELATED TO GRAFTRECIPIENTS
Neural grafting also presents ethical issues relatedto the graft recipients. These ethical questions existfor any new procedure, but they may be especiallypertinent to clinical (human) trials of neural grafting.
Federal law dictates that federally funded proto-cols must be sent to an Institutional Review Board(IRB) for approval of the legal and ethical featuresof protocol design [45 CFR 46], particularly featuresrelating to treatment of research subjects. Of theseven criteria for IRB approval of research, two maypose problems for neural grafting research. Theseare the requirements that risks to subjects bereasonably comparable to the expected benefits andthat the investigator obtain the subject’s informedconsent to participate in research.
Risks to Research Subjects
Risks to subjects are always difficult to determineat the beginning of clinical trials; it has beensuggested that the lack of knowledge about howgrafts work may make the risks associated withneural grafting particularly difficult to determine(27). The question that arises when anew therapy ispresented for experimentation on human subjects iswhether there is evidence that it promises significantbenefit to the patient and does not present undue risk.This risk-benefit analysis is performed by severalparties involved with the research protocol: theinvestigator, the IRB, and the prospective researchsubjects and their families.
Considerable debate surrounds the experimentaluse of fetal and adrenal tissue grafts to treat personswith Parkinson’s disease (see ch. 5). In fact, somepersons believe investigators had not gathered
.

162 . Neural Grafting: Repairing the Brain and Spinal Cord
enough data from animal studies to warrant pro-gressing to clinical trials (22,36) and, therefore, mayhave been unable to meet their responsibilities tovulnerable human research subjects. Some personsclaim that it is impossible for investigators orsubjects involved in neural grafting research tobalance risks and benefits unless they can estimaterealistically what those benefits and risks will be.That claim, however, may be made of all clinicalresearch (25). Some persons have argued that thepatient undergoing neural grafting for the treatmentof Parkinson’s disease may be risking more than isjustified if the graft is unsuccessful, if it is affectedby the same neurodegenerative processes that madethe graft necessary in the first place (19,27) [al-though it has been pointed out that the originaldegeneration in Parkinson’s disease takes place overthe course of several decades (5)], or if there is adelayed immunological response to the graft thatproves more harmful than the disease.
Information should be obtained from the leastpossible amount of research conducted during theshortest possible period of time (9). The number oftrials performed is another important considerationin protecting research subjects from unnecessaryrisks. Some observers suggest that controlled studiesand pooled results from different locations may bethe most efficient means of deriving data. Thissuggests single-protocol research pursued at multi-ple centers, formation of a comprehensive database,constant monitoring and interpreting of data, as wellas constant updating of information given to subjectsfor informed consent (18). On the other hand, ifneural grafting research on a particular disease isdeemed an important public health priority, it mightproceed more quickly and in accordance withdiverse research protocols. In order for the transitionto be made from clinical trials to therapeutic use inthis case, many more patients will have to be enlistedas subjects; the human costs, as well as the medicaland research costs, may be very high (18).
Informed Consent
One important ethical question is whether neuralgrafting protocols conform to standards of protec-tion for research subjects. Since informed consentrequires “[a] description of any reasonably foresee-able risks or discomforts to the subject [and] adescription of any benefits to the subject or to otherswhich may reasonably be expected from the re-search’ [45 CFR 46.116], each patient must conduct
e
a risk-benefit analysis of his or her own. This entailstwo kinds of information, the scientific and thepersonal (15). The first is made up of the objectivedata about the disease, alternative treatments, andsocial support systems and agencies; the secondencompasses the subjective data related to thepatient’s experience.
The objective data for this analysis must beprovided by the researcher. It should include theprognosis if the disease runs its course, the availabil-ity of alternative treatments, the fact that theprocedure is experimental, the extent of uncertaintyinvolved in the surgery, the intended and possiblelong-term outcomes of surgery, the availability ofsocial support systems and agencies to aid recovery,and a thorough description of what the surgery willinvolve, including the pain and suffering likely toaccompany the procedure and the immediate recov-ery from it, as well as risks of complications. Thehard data will vary depending on the disease, the ageof the patient, and the type of graft used.
The subjective data needed for a risk-benefitanalysis can only come from the patient, for theyinvolve the patient’s perception of his or her qualityof life. Quality of life is a concept that describes theexperience of the individual, what kind of life ispossible given the person’s condition, and whetherthat condition will allow the individual to have a lifethat he or she views as worth living (23). There maybe differences, however, between how a personperceives the quality of his or her own life, how anobserver assumes he or she perceives the quality ofhis or her life, and how an observer evaluates thequality of that person’s life (51). The severe physicaland emotional suffering associated with neurologi-cal disease and injury are frequently thought tocreate poor quality of life, but it is important thatpatients have the freedom and medical informationnecessary to make their own quality of life evalua-tions.
The same conditions that depreciate the quality oflife of individuals with neurological diseases andspinal cord injuries may make these persons espe-cially susceptible to coercion. While the possibilityof undue influence exists in any research situation,patients with neurological disorders may be espe-cially vulnerable to judgments about their quality oflife made by researchers or family members. Onereason is that patients who have an apparentlypermanent injury or an incurable disease may be

Chapter 8--Ethical Issues ● 163
tempted to try anything that might be of help. Inmany cases, there are few or no alternative treat-ments or support services for neurological disorders,and what treatments there are may have limitedefficacy. For some patients, this lack of alternativesconstitutes sufficient reason to participate in neuralgrafting research. A necessary condition for allresearch subjects, however, is that they be free tomake uncoerced, informed choices.
Some patients with neurological injuries or dis-ease may be incapable of performing the ethicalcost-benefit analyses necessary for truly informedconsent (6). In these cases, a patient may have to relyinstead on the judgment of a family member or legalguardian. The proxy decisionmaker should attemptto evaluate the quality of the patient’s life on thesame basis the patient would have used. Opencommunication about what investigators and pa-tients (or their proxies) perceive as the relevantfactors in the decision to participate in research isnecessary if a patient is to do a risk-benefit analysiswithout coercion. Given adequate scientific data bythe researcher, the patient or proxy can predict morerealistically what benefits the patient is likely to gainby undergoing neural grafting surgery.
Three factors make it difficult for investigators togive accurate information about the probable risksand benefits of neural grafting procedures. First, it isuncertain at this early stage of research what the risksand benefits of neural grafting are likely to be.Second, it maybe tempting for investigators to painta more positive picture than is warranted because oftheir own high expectations. Finally, researchersmay filter empirical evidence through their interpre-tations of the patient’s current or future quality oflife, rather than allowing patients to draw their ownconclusions (18). These factors apply to all clinicalresearch, but sensitivity to limitations may beespecially important for neural grafting research.The solicitation of informed consent from neurolog-ical patients or their families must be done with theirvulnerability in mind, making clear to the patient orfamily the degree of uncertainty for the experimentalprocedure. Although it is impossible in any researchsetting for a patient to be totally informed of risksand benefits, in the case of neural grafting it may beextremely important for patients to be aware of thescientific limitations at this time.
There may be reasons besides possible changes inquality of life for an individual to turn down the
opportunity to receive a neural graft. For somesubjects, neural grafting presents a chance formedical science to overcome disease; but for others,neural grafting may present a threat to personalidentity and sense of self, aspects of the human mindthat are, to some persons, the very essence ofhumanity (18). The ability to do neural graftingraises questions about whether the mind can beexplained in terms of the brain. It is difficult to knowwhat physical functions of the brain define aperson’s existence as a unique individual or areessential to the retention of his or her personalidentity across time. Consequently, some wouldargue, there is no way to predict the extent to whichneural grafting in the brain will or will not interferewith the functions of the mind that determineindividuality, personhood, or a sense of self. Theseare metaphysical questions rather than ethical ones,but they are important considerations for persons ina position to receive neural grafts.
SUMMARY AND CONCLUSIONSNeural grafting includes a variety of materials and
surgical procedures used to investigate and treat anumber of neurological disorders. As the graftingmaterials and techniques viny, so do the ethicalissues surrounding them. Whether the Federal Gov-ernment becomes involved in funding or regulatingfetal tissue grafting or not, research in fetal tissuetransplantation continues.
Some of the ethical issues surrounding neuralgrafting are common to any new area of biomedicalresearch or treatment. They include whether to usepublic funds to support neural grafting research orneural grafting as a standard medical treatment.They also include economic questions about how toestablish health-care priorities and how to allocateresources for research.
There are currently few alternative treatments forneurological disorders. Some persons feel that,because neural grafting is an exciting and possiblyprofitable area of research, it may get more supportthan alternatives and reduce the impetus to find lessexpensive, less risky, and less controversial treat-ments for neurological disorders (38). Decreasedsupport for neural grafting research, however, doesnot necessarily make funds available for researchinto other treatments for neurological disease andinjury (12). In order to resolve some of the questionsabout fair distribution of resources, it might be

164 Neural Grafting: Repairing the Brain and Spinal Cord
helpful to evaluate neural grafting in relation totreatments for other diseases and other treatments forneurological disorders, keeping in mind the priori-ties set and the amount of research funded. In orderto make decisions about funding neural graftingresearch, it will be necessary to estimate the efficacyof the technology, the number of people nowaffected by neurological disorders, and the numberof people likely to be affected in the future.
Ethical issues arising from the surgical proce-dures and the materials used in the neural graftingprocess also demand attention. Some of these issuesare analogous to issues that have been dealt withalready and are reflected in Federal regulations; e.g.,informed consent and the protection of researchsubjects were addressed in the 1970s. Existingregulations, however, may not adequately protectneural graft recipients from the risks unique to brainimplantation surgery. The possibility of doing asufficient risk-benefit analysis has been challengedon the grounds that not enough animal research hasbeen done to know what the benefits of neuralgrafting are likely to be. Obtaining informed consentfrom persons with neurological disease may bedifficult, both because the risks and benefits cannotbe realistically estimated at this time and because ofthe possible cognitive limitations of persons withsome neurological disorders.
On the other hand, there are several reasons whythe Federal Government should not involve itself insurgical development. Research risks to the subjectare almost always unknown in early clinical trials(24). Furthermore, much surgical innovation, in-cluding neural grafting, is therapeutic as well asexperimental (25) and, therefore, may be more likelyto hold the promise of benefit for the subject[although some commentators have called “thera-peutic research” an oxymoron (46)]. Neural graftinginvestigators should conduct research in a noncoer-cive manner consistent with the treatment of otherresearch subjects. While it is important for personsdeveloping new surgical techniques to be aware ofmoral considerations, ethical and practical argu-ments may be made for allowing, even encouraging,such innovation.
Thus far, the greatest ethical controversy sur-rounds the use of fetal tissue from elective abortionsfor neural grafting. Positions taken on the moralityof fetal tissue grafting, however, do not dependstrictly on a person’s beliefs about the morality of
elective abortion. Both supporters and opponents ofabortion have articulated reasons for denying fund-ing for fetal tissue grafting research, and both haveidentified reasons for providing it. Tissue fromspontaneous abortions, ectopic pregnancies (42),and fetal tissue cell lines have been suggested asethically acceptable alternatives.
Many different positions are taken regarding theethics of using fetal tissue obtained from electiveabortions for neural grafting. Some of these consid-erations include the implications of a public policythat either supports or restricts the use of abortedfetal tissue for grafting and the possible conse-quences of such a policy. It has been suggested thatusing electively aborted fetal tissue for neuralgrafting will both harm individual fetuses and denyfetuses respect. It has also been suggested thatgroups besides fetuses-e. g., women and society atlarge-may be adversely affected by a policy thatendorses fetal tissue transplantation. A number ofthe arguments against fetal tissue transplantation arebased on predictions about its future social effects.While it is important to anticipate potential prob-lems, it is impossible to know at this time whetherthe consequences predicted will come to pass.
Some persons believe that once a fetus is dead, itno longer has interests to protect and that it isinappropriate for the Federal Government to with-hold funding for research that may benefit manysufferers of neurological disorders. A number ofgroups in the United States and abroad haveproposed safeguards for protecting social values andvulnerable groups, while allowing biomedical sci-ence to move forward (32,48,54,55) (see app. A, boxA-2). It has been suggested that these protectionswould be most effective with Federal involvement inthe research process (4,47). Despite the similaritiesof the safeguards recognized by the various studygroups and the fact that both existing DHHSregulations and Federal laws already implementmany of the suggested guidelines (58), some personsremain skeptical about the feasibility of implement-ing these measures.
The solicitation of consent for the use of tissuefrom cadaveric fetuses presents another ethicalquestion. Controversy exists about whether thewoman who elects the abortion is the appropriateperson to give consent and when consent should besolicited. Both the regulations for the protection ofresearch subjects and those for the donation of

Chapter 8--Ethical Issues ● 165
cadaveric body parts can help in determiningg theappropriate donor of electively aborted fetal tissue,but these regulations do not explicitly cover thedonation of fetal tissue for transplantation research.
The use of fetal tissue to start continuous cell linesfurther complicates the issue of consent, becausequestions are raised about whether the donor oftissue used to start a CCL may profit financiallyfrom it. Although it maybe deemed appropriate fora woman who aborts to give her consent to use offetal tissue, it may not be considered appropriate forher to profit financially. While questions regardingthe ownership of tissues used for commerciallyprofitable cell lines are being addressed by thecourts, discussion has been limited to the ownershipof adult tissues. Questions pertaining to the propertreatment of fetal tissue remain unanswered.
CHAPTER 8 REFERENCES1.
2.
3.
4.
5.
6.
7.
8.
9.
American Medical Association, Council on Scien-tific Affairs and Council on Ethical and JudicialAffairs, “Medical Applications of Fetal TissueTransplantation,” Journal of the American MedicalAssociation 263:565-570, 1990.American Paralysis Association, testimony beforethe U.S. House of Representatives Committee onEnergy and Commerce, Subcommittee on Health andthe Environment, hearings on Human Fetal TissueTransplantation, Apr. 2, 1990.Annas, G.J., and Elias, S., “The Politics of Trans-plantation of Human Fetal Tissue,” New EnglandJournal of Medicine 320:1079-1082, 1989.Annas, G.J., and Elias, S., letter, New EnglandJournal of Medicine 321:1609, 1989.Bakay, R.A.E., associate professor of surgery, sec-tion of neurosurgery, Emory University School ofMedicine, Atlanta, GA, personal communication,December 1989.Blank, R., professor of sociology and associatedirector, program for Biosocial Research, NorthernIllinois University, DeKalb, IL, personal communi-cation, December 1989.Buckley, R.H., “Fetal Thymus Transplantation forthe Correction of Congenital Absence of the Thymus@iGeorge’s Syndrome),” testimony before theHumanFetal Tissue Transplantation Research Panel,National Institutes of Health, Bethesda, MD, Sept.14, 1988.Burtchaell, J.T., “University Policy on ExperimentalUse of Aborted Fetal Tissue,” IRB: A Review ofHumun Subjects Research 10:7-11, 1988.Caplan, A.L., testimony before the Human FetalTissue Transplantation Research Panel, NationalInstitutes of Health, Bethesda, MD, Sept. 15, 1988.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
Center for Biomedical Ethics, The Use of HumanFetal Tissue: Scientific, Ethical, and Policy Con-cerns (Minneapolis, MN: University of Minneso@1990).Crutchner, K.A., testimony before the House ofRepresentatives Committee on Energy and Com-merce, Subcommittee on Health and the Environ-ment, hearings on Human Fetal Tissue Transplanta-tion Research, Apr. 2, 1990.Davis, M., senior policy analyst, Office of HealthPlanning and Evaluation, Division of Policy Analy-sis, U.S. Department of Health and Human Services,personal communication, April 1990.Fine, A., “The Ethics of Fetal Tissue Transplants,”Hastings Center Report 18:5-8, 1988.Fine, A., associate professor, Department of Physiol-ogy and Biophysics, Dalhousie University School ofMedicine, Halifax, Nova Scotia, Canada, personalcommunication, April 1990.Forrow, L., Wartman, S.A., and Brock, D.W., “Sci-ence, Ethics, and the Making of Clinical Decisions:Implications for Risk Factor Intervention,” Journalof the American Med”cal Association 259:3161-3167, 1988.Freed, C., professor of medicine and pharmacology,University of Colorado, Denver, CO, personal com-munication, December 1989.Fung, C.H.K., and Lo, J.W., “Alternatives To UsingFetal Tissue From Induced Abortions” Petter],Journal of the American Medical Association 264:34, 1990.Gervais, K.G., “Neural Transplants and Nerve Re-generation Technologies: Ethical Issues,” preparedfor the OffIce of Technology Assessment, U.S.Congress, Washington, DC, 1989.Gill, T.J., and Lund, R.D., “Grafting Into the Brain,”testimony before the Human Fetal Tissue Transplan-tation Research Panel, National Institutes of Health,Bethesda, MD, Sept. 14, 1988.Hansen, J.T., and Sladek, J.R., Jr., “Fetal Research,”Science 246:775-779, 1989.Hastings Center Project on Organ Transplantation,Ethical, tigal and Policy Issues Pertaining to SolidOrgan Procurement (Hastings-on Hudson, NY: TheHastings Center, 1985).Landau, W.M., “Artificial Intelligence: The BrainTransplant Cure for Parkinsonism,” Neurology 40:733-740, 1990.Lappe, M., “Ethics at the Center of Life: ProtectingVulnerable Subjects,” Hastings Center Report 8:1 1-13, 1978.kbacqz, K., and Jensen, A.R., statement, U.S.Department of Health, Education, and Welfare,National Commission for the Protection of HumanSubjects of Biomedical and Behavioral Research,Research on the Fetus: Report and Recommendu-

166 . Neural Grafting: Repairing the Brain and Spinal Cord
25.
26.
27.
28.
29.
30.
31.
32,
33.
34.
35.
36.
37.
38.
tions, DHEW Pub. No. (0S)76-127 (Washington,DC: U.S. Government Printing Office, 1975).McCarthy, C.R., “RegulatoryAspects of the Distinc-tion Between Research and Medical Practice,” Z~:A Review of Human Subjects Research 6:7-8, 1984.McCarthy, D., Roman Catholic priest, Church ofSaint Antoninus, Cincinnati, OH, personal communi-cation, April 1990.McCullagh, P., The Foetus as Transplant Donor:Scientific, Social and Ethical Perspectives (Chi-chester, Australia: John Wiley & Sons, 1987).Macklin, R., “Is There Anything Wrong WithSurrogate Motherhood? An Ethical Analysis,” Law,Mealcine, and Health Care 16(SpringlSumrner) :57-64, 1988.Madrazo, I., Leon, V., Torres, C., et al., “Transplan-tation of Fetal Substantial Nigra and Adrenal Medullato the Caudate Nucleus in Two Patients WithParkinson’s Disease” [letter], New EnglandJournalof Medicine 318:51, 1988.Mahoney, M.J., “The Nature and Extent of ResearchInvolving Living Human Fetuses,’ U.S. Departmentof Health, Education, and Welfare, National Com-mission for the Protection of Human Subjects ofBiomedical and Behavioral Research, Research onthe Fetus: Appendix, DHEW Pub. No. (OS) 76-128(Washington, DC: U.S. Government Printing Office,1975).Mahowald, M.B., professor, Center for ClinicalMedical Ethics, University of Chicago, Chicago, IL,personal communication, May 1990.Mahowald, M.B., Areen, J., Hoffer, B.J., et al.,“Transplantation of Neural Tissue From Fetuses”fletter], Science 235:1307-1308, 1987.Mahowald, M.B., Silver, J., and Ratcheson, R.A.,“The Ethical Options in Transplanting Fetal Tis-sue,” Hastings Center Report 17:9-15, 1987.Mason, J.O., “Should the Fetal Tissue Transplanta-tion Research Ban Be Lifted?” Journal of NIHResearch 2:17-18, 1990.Mason, J. O., testimony before the U.S. House ofRespresentatives Committee on Energy and Com-merce, Subcommittee on Health and the Environ-ment, hearings on Human Fetal Tissue Transplanta-tion Research, Apr. 2, 1990.Men, B., “Neurologists Join Neurosurgeons inUrging Restraint in Parkinson’s Surgery,’ Journal ofthe American Medical Association 261:2929, 1989.Moore v. Regents of the University of C’al#ornia, 202Cal. App.3d 1230, 249 Cal. Rptr. 494 (1988), reh.granted, 252 Cal. Rptr. 816,763 P.2d 479 (1988).Moraczewski, A. S., regional director, Pope JohnXXIII Medical, Moral, Research, and EducationCenter, Houston, TX, personal communication, April1990.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
Murphy, J.B., “TheEthics of Research Using HumanFetal Tissue” [letter], New England Journal ofMedicine 321:1608, 1989.Murray, TH., “Who Owns the Body? On the Ethicsof Using Human Tissue for Commerical Purposes,”IRB: A Review of Human Subjects Research 8: 1-5,1986.Murray, TH., “Ethical Issues in Research on HumanFetal Tissue Transplantation,” testimony before theHuman Fetal Tissue Transplantation Research Panel,National Institutes of Health, Bethesda, MD, Sept.15, 1988.Nolan, K., “Genug ist Genug: A Fetus Is Not aKidney,” Hastings Center Report 18:13-19, 1988.Nolan, K., “Public Policy Considerations in the Useof Human Fetal Tissue,’ testimony before theHuman Fetal Tissue Transplantation Research Panel,National Institutes of Health, Bethesda, MD, Sept.14, 1988.Polkinghorne, J., Hoffenberg, R., Kennedy, I., et al.,Review of the Guidance on the Research Use ofFetuses and Fetal Material (Jmndon: Her Majesty’sStationery Office, July 1989).Redmond, D. E., neurosurgeon, NeurobehavioralLaboratory, Yde University School of Medicine,New Haven, CT, personal communication, April1990.Rolleston, F., and Miller, J,R., “Therapy or Re-search: A Need for Precision,” IRB: A Review ofHuman Subjects Research 3:1-3, 1981.Ryan, K., testimony before the U.S. House ofRepresentatives Committee on Energy and Com-merce, Subcommittee on Health and the Environ-ment, hearings on Human Fetal Tissue Transplanta-tion Research, Apr. 2, 1990.Stanford University Medical Center Committee onEthics, “Special Report: The Ethical Use of HumanFetal Tissue in Medicine,” New England Journal ofMedicine 320:1093-1096, 1989.U.S. Congress, Office of Technology Assessment,Human Gene Therapy4 Background Paper, OTA-BP-BA-32 (Washington, DC: U.S. GovernmentPrinting Office, December 1984).U.S. Congress, Office of Technology Assessment,New Developments in Biotechnology: Ownership ofTissues and Celldpecial Report, OTA-BA-337(Washington, DC: U.S. Government Printing Office,March 1987).U.S. Congress Office of Technology Assessment,L~e-Sustaining Technologies and the Elderly, OTA-BA-306 (Washington, DC: U.S. Government Print-ing Office, July 1987).U.S. Department of Health, Education, and Welfare,National Commission for the Protection of HumanSubjects of Biomedical and Behavioral Research,Research on the Fetus: Report and Recommend&

Chapter 8--Ethical Issues . 167
53.
54.
55.
tions DHEW Pub. No. (0S)76-127 (Washington, 56.DC: U.S. Government Printing Office, 1975).U.S. Department of Health and Human Services,statement by Imuis W. Sullivan, Secretary, Nov. 2,1989. 57.U.S. Department of Health and Human Services,Public Health Service, National Institutes of Health,Report of the Human Fetal Tissue TransplantationResearch Panel (Bethesda, MD: 1988).Walters, L., testimony before the U.S. House of 58,Representatives Committee on Energy and Com-merce, Subcommittee on Health and the Environ-ment, hearings on Human Fetal Tissue Transpkmta-tion Research, Apr. 2, 1990.
Wikler, D., professor of philosophy, University ofWisconsin, Madison, WI, personal communication,April 1990.
Windom, R.E., Assistant Secretary for Health, U.S.Department of Health and Human Services, memo-randum to J.B. Wyngaarden, Director, NationalInstitutes of Health, Mar. 22, 1988.
Wyngaarden, J.B., Director, National Institutes ofHealth, memorandum to Robert E. Windom, Assis-tant Secretary for Health, U.S. Department of Healthand Human Services, Jan. 19, 1989.
32-801 0- 90 - 7 : QL 3

Appendixes

Appendix A
DHHS Moratorium onHuman Fetal Tissue Transplantation Research
While human fetal tissue transplantation research is apromising and exciting area of scientific study at thistime, it has also created considerable controversy. Thepublic debate is in one sense a straightforward, althoughcomplicated, discussion about the ethics of public fundingof research that uses electively aborted human fetal tissue.for transplantation; however, the Federal Government’sresponse to the controversy has itself raised questions.
In March 1988, a moratorium was imposed on the useof human fetal tissue from induced abortions for trans-plantation until the ethical issues surrounding this usecould be adequately studied. Nineteen months after it wasinitiated, the moratorium was extended indefinitely by thenew Secretary of Health and Human Services. Added tothe ethical issues initially presented for discussion, theFederal Government’s actions in this matter have beenquestioned on legal and ethical bases (3). It may beinstructive to trace the events leading up to the morato-rium, the activities of the National Institutes of Health(NIH) Human Fetal Tissue Transplantation ResearchPanel, and the events following the panel’s report(l 1) andits acceptance by the NIH Director’s Advisory Commit-tee.
Events Preceding the Moratorium
Fetal tissue has long been used in research (2,4)-including research involving the transplantation of fetalthymus tissue into humans—and the ethical questions itraises have been addressed by an executive branchcommission and in Federal regulations [45 CFR 46].When fetal tissue began to be used for neural grafting inthe mid-1980s, however, some questioned whether theseregulations adequately address all the issues raised by thisresearch. In fiscal year 1987, NIH funded about $11.2million of nontherapeutic human fetal-tissue research(10). In 1987, a research protocol for implantation of fetalneural tissue from induced abortions into persons suffer-ing from Parkinson’s disease was proposed by a re-searcher at the National Institute of Neurological Disor-ders and Stroke (NINDS). The Institutional Review Boardat the NIH clinical center reviewed the scientific, legal,and ethical issues raised by the protocol and accepted itfor funding, yet the nature of the research was consideredsufficiently controversial by the director of NINDS to besubmitted for the approval of the Director of NIH. TheDirector voluntarily sought approval from the Depart-ment of Health and Human Services (DHHS) to reviewand approve the protocol. In response, the AssistantSecretary for Health issued a temporary moratorium on allfetal tissue transplantation research using tissue from
induced abortions until NIH could convene an advisorycommittee to examine the use of human fetal tissue frominduced abortions for transplantation and make recom-mendations for its use. The advisory committee was askedto address 10 questions (see box A-l).
Although the intramural NIH proposal stimulatedsignificant ethical debate, NIH funds had already beengranted that year for an extramural protocol to study theeffects of fetal pancreatic islet cells on juvenile diabetes.It is unclear why the intramural proposal received closerscrutiny than the extramural protocol.
One factor that may have impeded the decisionmakingprocesses within NIH is the lack of an authoritative bodywithin the Federal Government to address ethical issuesraised by biomedical research and treatment and to makepolicy decisions regarding them. The Ethics AdvisoryBoard (EAB) that had existed within DHHS to addressquestions of this sort was disbanded in 1980. While thescientific, ethical, and legal features of the Parkinson’sdisease protocol were approved by the NIH InstitutionalReview Board, the protocol was regarded as problematicfirst by the director of the Institute performing theresearch and then by the Director of NIH. The Director ofNIH was forced to turn to the Assistant Secretary forHealth for advice on appropriate action.
Although the conditions of the moratorium were notretroactive, the investigators who had received NIH fundsfor fetal pancreatic islet cell transplantation voluntarilysuspended their research because of the controversy.Since that time, only research funded by private institu-tions has continued. Although most privately funded fetaltissue transplantation has been stopped voluntarily, someinitiatives in this area have continued. In late 1988, at theUniversity of Colorado Health Sciences Center, physi-cians implanted fetal cells obtained from an inducedabortion into the brain of a 52-year-old Denver man whohad been suffering from Parkinson’s disease for 20 years(l). Also in late 1988, physicians at Yale Medical Schoolimplanted human fetal cells into the brain of a womansuffering from Parkinson’s disease, after first freezing thecells and testing their viability (6). The fetal cells used inthis surgery were donated by a woman who had had aninduced abortion in her first trimester (6).
The Report of the NIH Human Fetal TissueTransplantation Research Panel
In response to the questions presented by the AssistantSecretary for Health, the Human Fetal Tissue Transplan-
–171–

172 . Neural Grafting: Repairing the Brain and Spinal Cord
Box A-l--Questions Addressed to the NIH Human Fetal Tissue Transplantation Research Panel
● Is an induced abortion of moral relevance to the decision to use human fetal tissue for research? Would the answerto this question provide any insight on whether and how this research should proceed?
* Does the use of the fetal tissue in research encourage women to have an abortion that they might otherwise notundertake? If so, are there ways to minimize such encouragement?
. As a legal matter, does the very process of obtaining informed consent from the pregnant woman constitute aprohibited ‘‘inducement’ to terminate the pregnancy for the purposes of the research-thus precluding researchof this sort under HHS regulations?
● Is maternal consent a sufficient condition for the use of the tissue, or should additional consent be obtained? Ifso, what should be the substance and who should be the source(s) of the consent, and what procedures shouldbe implemented to obtain it?
● Should there be and could there be a prohibition on the donation of fetal tissue between family members, or friendsand acquaintances? Would a prohibition on donation between family members jeopardize the likelihood ofclinical success?
● If transplantation using fetal tissue ❆❒❏❍ induced abortions becomes more common, what impact is likely to occuron activities and procedures employed by abortion clinics? In particular, is the optimal or safest way to performan abortion likely to be in conflict with preservation of the fetal tissue? Is there any way to ensure that inducedabortions are not intentionally delayed in order to have a second trimester fetus for research and transplantation?
● What actual steps are involved in procuring the tissue from the source to the researcher? Are there any paymentsinvolved? What types of payments in this situation, if any, would fall inside or outside the scope of the HydeAmendment?
● According to HHS regulations, research on dead fetuses must be conducted in compliance with State and locallaws. A few States’ enacted version [sic] of the Uniform Anatomical Gift Act contains restrictions on the researchapplication of dead fetal tissue after an induced abortion. In those States, do these restrictions apply to therapeutictransplantation of dead fetal tissue after an induced abortion? If so, what are the consequences for NIH-fundedresearchers in those States?
● For those diseases for which transplantation using fetal tissue has been proposed, have enough animal studiesbeen performed to justify proceeding to human transplants? Because induced abortions during the first trimesterare less risky to the woman, have there been enough animal studies for each of those diseases to justify the relianceon the equivalent of the second trimester human fetus?
● What is the likelihood that transplantation using fetal cell cultures will be successful? Will this obviate the needfor fresh fetal tissue? In what time frame might this occur?
SOURCE: U.S. Department of Health and Human Services, Public Health Service, National Institutes of Health, Report of the Human FetalTissue Transplantation Research Panel (Bethesda, MD: 1988).
tation Research Panel convened, heard testimony from a Events Following Acceptance of thevariety of experts and interest groups, and submitted a Panel Reportreport to the NIH Director late in 1988. A unanimousagreement was not reached among the 21 panel members,but the panel’s report concluded (17 to 4) that the fundingof research involving the transplantation of human fetaltissue obtained from induced abortions is acceptablepublic policy as long as carefully crafted safeguards are inplace (see box A-2).
Although adamant dissent was voiced by four panelmembers, the report and its recommendations wereaccepted unanimously by the NIH Director’s AdvisoryCommittee. The advisory committee recommended thatthe moratorium on fetal tissue transplantation research belifted. The Director of NIH concurred with this positionin a memorandum to the Assistant Secretary for Health inJanuary 1989 (12).
The Assistant Secretary, upon the instruction of theDHHS Secretary, deferred action on the panel’s recom-mendation that the Federal Government lift the morato-rium (5). The new administration took no action until thenew Assistant Secretary for Health recommended to thenew DHHS Secretary in October 1989 that the ban becontinued. The Secretary continued the moratoriumindefinitely in November 1989 (9). No action was takento implement any of the recommendations of the advisorypanel’s report.
The legal and ethical bases of the continuation of themoratorium have since been challenged. The moratoriumwas originally declared as a temporary measure until theethical issues raised by fetal tissue transplantation couldbe addressed and recommendations could be made. Thefact that it has been continued indefinitely without any

Appendix A--DHHS Moratorium on Human Fetal Tissue Transplantation Research ● 173
Box A-2—Recommendations of the NIH HumanFetal Tissue Transplantation Research Panel
●
●
●
●
●
●
●
●
The decision to terminate a pregnancy and theprocedures of abortion should be kept independ-ent from the retrieval and use of fetal tissue.The timing and method of abortion should not beinfluenced by the potential uses of fetal tissue fortransplantation or medical research.Fetal tissue from induced abortions should not beused in medical research without the priorconsent of the pregnant woman.The decision and consent to abort must precedediscussion of the possible use of the fetal tissueand any request for such consent as might berequired for that use.The pregnant woman should be prohibited fromdesignating the recipient of the fetal tissuetransplant.Payments and other forms of remuneration andcompensation associated with the procurementof fetal tissue should be prohibited, exceptpayment for reasonable expenses occasioned bythe actual retrieval, storage, preparation, andtransportation of the tissues.Potential recipients of such tissues, as well asresearch and health care participants, should beproperly informed as to the source of the tissuesin question.Procedures must be adopted that accord humanfetal tissue the same respect accorded othercadaver human tissues entitled to respect.
SOURCE: U.S. Department of Health and Human Services,Public Health Service, National Institutes of Health,Report of the Human Fetal Tissue TransplantationResearch Panel (Bethesda, MD: 1988).
official announcement or opportunity for public debatehas caused some to challenge its legal basis (7). Theethical basis of the continuation has also been challenged,since the reasons for its continuance had been rejected bythe advisory panel upon whose recommendations themoratorium was supposed to be contingent (8).
On April 2, 1990, the U.S. House of RepresentativesCommittee on Energy and Commerce’s Subcommittee onHealth and the Environment held hearings on human fetaltissue transplantation research. The subcommittee heardtestimony from members of the NIH Human Fetal TissueTransplantation Research Panel, representatives of organ-izations representing persons with various diseases that
fetal tissue grafting may treat, members of the scientificcommunity, and the Assistant Secretary for Health.Strong views for and against the continued moratorium onfetal tissue transplantation research were expressed.
While on one level the ethical debate was clearly andpublicly articulated, the events leading up to the morato-rium and those that followed the NIH advisory commit-tee’s acceptance of the panel’s recommendations raisequestions of their own. These events add another layer ofethical considerations to the fetal tissue transplantationcontroversy: Is the procedure for ethical decisionmakingin government subject to the same scrutiny as the issuesit is used to address? Again, the absence of a Federalagency for deliberation of bioethical issues maybe noted.These events may also be interpreted as a question aboutthe relationship between personal moral or ethical convic-tions and the appropriate shape of public policy in apluralistic society.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
Appendix A ReferencesAssociated Press, “Denver Scientists To Keep UsingTissue,” Apr. 19, 1988.Hansen, J.T., and Sladek, J.R., Jr., “Fetal Research,”Science 246:775-779, 1989.Hilts, P.J., “U.S. Aides See Shaky Legal Basis for Ban onFetal Tissue Research,” New York Times, Jan. 30, 1990.Lehrman, D., Summary: Fetal Research and Fetal TissueResearch (Washington, DC: Association of AmericanMedical Colleges, 1988).Mesce, D., “Former NIH Director Wants Fetal TissueResearch Ban Ended,” Associated Press, Oct. 16, 1989.New York Times, “Doctors Implant Frozen Fetal Cells,”Dec. 13, 1988.Palca, J., ‘‘Fetal Research Ban on Shaky Ground?’ Science247:629, 1990.U.S. Congress, House of Representatives, Committee onGovernment Operations, Subcommittee on Human Re-sources and Intergovernmental Relations, letter from TedWeiss, chairman, to Louis W. Sullivan, Secretary of Healthand Human Services, Jan. 26, 1990.U.S. Department of Health and Human Services, statementby Louis W. Sullivan, secretary, Nov. 2, 1989.U.S. Department of Health and Human Services, PublicHealth Service, National Institutes of Health, Report onHuman Fetal Tissue Research Supported by the NationalInstitutes of Health in Fiscal Year 1987.U.S. Department of Health and Human Services, PublicHealth Service, National Institutes of Health, Report of theHuman Fetal Tissue Transplantation Research Panel(Bethesda, MD: 1988).Wyngaarden, J.B., Director, National Institutes of Health,memorandum to Robert E. Windom, Assistant Secretary forHealth, U.S. Department of Health and Human Services,Jan. 19, 1989.

Appendix B
Participants in theWorkshop on New Developments in Spinal Cord Injury:Acute Interventions and Neural Grafts
Douglas Anderson, Ph.D.VA HospitalCincinnati, OH
June 12, 1989
Sponsored by the Office of Technology Assessmentand
American Paralysis AssociationParalyzed Veterans of America
Jerry Silver, Ph. D., Workshop ChairmanCase Western Reserve University
Cleveland, OH
Thomas E. Anderson, Ph.D.General Motors Research LaboratoriesWarren, MI
Jerry Bernstein, Ph.D.VA Medical CenterWashington, DC
Barbara S. Bregman, Ph.D.Georgetown UniversityWashington, DC
Carson J. Cornbrooks, Ph.D.University of Vermont College of MedicineBurlington, VT
Allan I. Faden, M.D.VA Medical CenterSan Francisco, CA
Earl R. Feringa, M.D.VA Medical CenterAugusta, GA
Barth Green, M.D.University of Miami School of MedicineMiami, FL
Marston Manthorpe, Ph.D.University of California, San DiegoLa Jell% CA
Paul J. Reier, Ph.D.University of Florida College of MedicineGainesville, FL
Fredrick J. Seil, M.D.VA Medical CenterPortland, OR
Brad T. Stokes, Ph.D.Ohio State UniversityColumbus, OH
Wise Young, M.D.New York University Medical CenterNew York, NY
Jean R. Wrathall, Ph.D.Georgetown UniversityWashington, DC
Contractor:
Julie Ann MillerWashington, D.C.
Edward Hall, Ph.D.UpJohn Co.Kalamazoo, MI
–174-

Appendix C
Decade of the Brain
Public Law 101-58, 101st Congress,Joint Resolution
Whereas it is estimated that 50 million Americans areaffected each year by disorders and disabilities thatinvolve the brain, including the major mental illnesses;inherited and degenerative diseases; stroke; epilepsy;addictive disorders; injury resulting from prenatal events,environmental neurotoxins, and trauma; and speech,language, hearing, and other cognitive disorders;
Whereas it is estimated that treatment, rehabilitationand related costs of disorders and disabilities that affectthe brain represents a total economic burden of $305billion annually;
Whereas the people of the Nation should be aware ofthe exciting research advances on the brain and of theavailability of effective treatment of disorders and disabil-ities that affect the brain;
Whereas a technological revolution occurring in thebrain sciences, resulting in such procedures as positronemission tomography and magnetic resonance imaging,permits clinical researches to observe the living brainnoninvasively and in exquisite detail, to define brainsystems that are implicated in specific disorders anddisabilities, to study complex neuropeptides and behavioras well as to begin to learn about the complex structuresunderlying memory;
Whereas scientific information on the brain is amassingat an enormous rate, and the field of computer andinformation sciences has reached a level of sophisticationsufficient to handle neuroscience data in a manner thatwould be maximally useful to both basic researches andclinicians dealing with brain function and dysfunction;
Whereas advances in mathematics, physics, computa-tional science, and brain imaging technologies have madepossible the initiation of significant work in imaging brainfunction and pathology, modeling neural networks andsimulating their dynamic interactions;
Whereas comprehending the reality of the nervoussystem is still on the frontier of technological innovationrequiring a comprehensive effort to decipher how individ-ual neurons, by their collective action, give rise to humanintelligence;
Whereas fundamental discoveries at the molecular andcellular levels of the organization of the brain areclarifying the role of the brain in translating neurophysio-logic events into behavior, thought, and emotion;
Whereas molecular biology and molecular geneticshave yielded strategies effective in preventing several
forms of severe mental retardation and are contributing topromising breakthroughs in the study of inheritableneurological disorders, such as Huntington’s disease, andmental disorders, such as affective illnesses;
Whereas the capacity to map the biochemical circuitryof neurotransmitters and neuromodulators will permit therational design of potent medications possessing minimaladverse effects that will act on the discrete neurochemicaldeficits associated with such disorders as Parkinson’sdisease, schizophrenia and Alzheimer’s disease;
Whereas the incidence of necrologic, psychiatric,psychological, and cognitive disorders and disabilitiesexperienced by older persons will increase in the future asthe number of older persons increases;
Whereas studies of the brain and central nervoussystem will contribute not only to the relief of necrologic,psychiatric, psychological, and cognitive, disorders, butalso to the management of fertility and infertility,cardiovascular disease, infectious and parasitic diseases,developmental disabilities and immunologic disorders, aswell as to an understanding of behavioral factors thatunderlie the leading preventable causes of death in thisNation;
Whereas the central nervous and immune systems areboth signaling systems which serve the entire organism,are direct connections between the nervous and immunesystem, and whereas studies of the modulatory effects ofeach system on the other will enhance our understandingof diseases as diverse as the major psychiatric disorders,acquired immune deficiency syndrome, and autoimmunedisorders;
Whereas recent discoveries have led to fundamentalinsights as to why people abuse drugs, how abused drugsaffect brain function leading to addiction, and how someof these drugs cause permanent brain damage;
Whereas studies of the brain will contribute to thedevelopment of new treatments that will curtail thecraving for drugs, break the addictive effects of drugs,prevent the brain-mediated “high” caused by certainabused drugs, and lessen the damage done to thedeveloping minds of babies, who are the innocent victimsof drug abuse;
Whereas treatment for persons with head injury,developmental disabilities, speech, hearing, and othercognitive functions is increasing in availability andeffectiveness;
Whereas the study of the brain involves the multidisci-plinary efforts of scientist, from such diverse areas asphysiology, biochemistry, psychology, psychiatry, mo-
–175–

176 ● Neural Grafting: Repairing the Brain and Spinal Cord
lecular biology, anatomy, medicine, genetics, and manyothers working together toward the common goals ofbetter understanding the structure of the brain and how itaffects our development, health, and behavior;
Whereas the Nobel Prize for Medicine of Physiologyhas been awarded to 15 neuroscientist within the past 25years, an achievement that underscores the excitementand productivity of the study of the brain and centralnervous system and its potential for contributing to thehealth of humanity;
Whereas the people of the Nation should be concernedwith research into disorders and disabilities that affect thebrain, and should recognize prevention and treatment ofsuch disorders and disabilities as a health priority;
Whereas the declaration of the Decade of the Brain willfocus needed government attention on research, treat-
ment, and rehabilitation in this area: Now, therefore, be itResolved by the Senate and House of Representatives ofthe United States of America in Congress Assembled,That the decade beginning January 1, 1990, hereby isdesignated the “Decade of the Brain,” and the Presidentof the United States is authorized and requested to issuea proclamation calling upon all public officials and thepeople of the United States to observe such decade withappropriate programs and activities.
Approved July 25, 1989.
LEGISLATIVE HISTORY--H.J. Res. 174 (S. J. Res. 173):CONGRESSIONAL RECORD, Vol. 135 (1989):
June 29, considered and passed House.July 13, considered and passed Senate.

Appendix D
Acknowledgments
OTA would like to thank the members of the advisory panel who commented on drafts of this report, thecontractors who provided material for this assessment, and the many individuals and organizations thatsupplied information for the study. In addition, OTA acknowledges the following individuals for their reviewof drafts of this report.
Douglas AndersonVA HospitalCincinnati, OH
Thomas E. AndersonGeneral Motors Research LaboratoriesWarren, MI
Lori AndrewsAmerican Bar FoundationChicago, IL
Michael AppuzzoAmerican Association of Neurological SurgeonsLos Angeles, CA
Adrienne AschNew Jersey Bioethics CommissionPrinceton, NJ
Nancy BeangSociety for NeuroscienceWashington, DC
Barbara S. BregmanGeorgetown UniversityWashington, DC
Margaret BrownAmerican Paralysis AssociationSpringfield, NJ
David W. CahillUniversity of South FloridaTampa, FL
Margaret CalvanoNational Multiple Sclerosis SocietyNew York NY
Sarah CarrAssociation of American Medical CollegesWashington, DC
Charles E. CarsonSpinal Cord SocietyFergus Falls, MN
Ronald A. CarsonUniversity of Texas Medical BranchGalveston, TX
Cheryl M. ChanaudParalyzed Veterans of AmericaWashington, DC
K. Danner ClouserThe Milton S. Hershey Medical CenterHershey, PA
Carl W. CotmanUniversity of California, IrvineIrvine, CA
Philip CohenHuntington Disease Society of AmericaNew York, NY
Arthur CoquelinTexas Tech University Health Sciences CenterLubbock TX
Keith CrutcherUniversity of Cincinnati College of MedicineCincinnati, OH
Miriam DavisNational Institute for Environmental Health SciencesBethesda, MD
Gary B. EllisInstitute of MedicineWashington, DC
Anne EtgenAlbert Einstein College of MedicineBronx, NY
R. Mark EvansAmerican Medical AssociationChicago, IL
Alan FineDalhousie University School of MedicineHalifax, N.S.
Thomas FreemanUniversity of South Florida
College of MedicineTampa, FL
–177–

178 ● Neural Grafting into the Brain and Spinal Cord
Elizabeth D. GeeUniversity of Colorado at BoulderBoulder, CO
Christopher GoetzUnited Parkinson FoundationChicago, IL
Lawrence GolbeRobert Wood Johnson Medical SchoolNew Brunswick NJ
Rachel Benson GoldThe Alan Guttmacher InstituteWashington, DC
Murray GoldsteinNational Institute of Neurological Disorders and StrokeBethesda, MD
Roger GorskiUniversity of California-Ire Angeles,
School of MedicineLos Angeles, CA
Debra S. Grega, Ph.D.Boehringer Mannheim BiochemicalIndianapolis, IN
W. Allen HauserG. H. Sergievsky CenterNew York NY
John T. HowardUniversity of California, IrvineIrvine, CA
William KettererNational Institutes of HealthBethesda, MD
Frances KisslingCatholics for a Free ChoiceWashington, DC
Lynn KlineThe Amyotrophic Lateral Sclerosis AssociationWoodland Hills, CA
Jeffrey H. KordowerUniversity of Illinois at ChicagoChicago, IL
Mary Grace KovarNational Center for Health StatisticsHyattsville, MD
L.T. KurlandMayo clinicRochester, MN
Edward R. Laws, Jr.American Association of Neurological SurgeonsWashington, DC
Carl LeventhalNational Institute of Neurological Disorders and StrokeBethesda, MD
Abraham LiebermanBarrow Neurological InstitutePhoenix, AZ
David E. LilienfeldThe Mount Sinai School of MedicineNew York NY
Ronald M. LindsayRegeneron Pharmaceuticals, Inc.Tarrytown, NY
Rev. Donald McCarthySt. Antoninus ChurchCincinnati, OH
Gianpaolo MaestroneAmerican Parkinson’s Disease AssociationNew York NY
Anne C. MaherChester Springs, PA
Stephen E. NadeauVA Medical CenterGainesville, FL
David OrentlicherAmerican Medical AssociationChicago, IL
Creighton H. PhelpsAlzheimer’s AssociationChicago, IL
Roger Porter,National Institute of Neurological Disorders and StrokeBethesda, MD
Ali H. RajputUniversity of SaskatchewanSaskatoon, Canada

Appendix D--Acknowledgments . 179
Michael R. RaskAmerican Academy of Neurological and
Orthopedic SurgeonsLas Vegas, NV
Robert B. RaskinUpJohn Co.Kalamazoo, MI
Robert A. RatchesonCase Western Reserve University School of MedicineCleveland, OH
Donald E. RedmondYale University School of MedicineNew Haven, CT
Paul J. ReierUniversity of Florida College of MedicineGainesville, FL
Donald J. ReisCornell University Medical CollegeNew York NY
Clifford RoseWorld Federation of NeurologyLondon, England
Jeffrey M. RosensteinThe George Washington University
School of MedicineWashington, DC
Judy RosnerUnited Parkinson FoundationChicago, IL
Leslie Steven RothenbergUniversity of California-Los Angeles,
School of MedicineLos Angeles, CA
Thomas A. ShannonWorcester Polytechnic InstituteWorcester, MA
Daniel SosinCenters for Disease ControlAtlanta, GA
Caroline TannerRush Medical CenterChicago, IL
John M. TewUniversity of Cincinnati College of MedicineCincinnati, OH
Bruce D. WeinsteinWest Virginia University School of MedicineMorgantown, WV
Robert M. whiteHoward UniversityWashington, DC
Daniel WilderUniversity of WisconsinMadison, WI
Janet WoodcockFood and Drug AdministrationBethesda, MD

Appendix E
List of Contractor Documents
For this report, OTA commissioned eight papers on various topics related to neural grafting.
“Epidemiology and Etiology of Parkinson’s Disease,” A.H. Rajput, 1988.“The Immunological Aspects of Neural Grafting,” W.F. Hickey, 1989.“Neural Grafting in the Treatment of Parkinson’s Disease: Past, Present, and Future,” T. Freeman, 1989.“Transplantation of Adrenal Tissue into the Nervous System,” A. Fine, 1989.“Reconstructing the Brain: New Strategies for Brain Disease,” R. McKay, 1989.“Legal and Regulatory Issues for Neural Grafts,” L. Andrews, 1989.“New Developments in Neuroscience: Neural Transplants and Nerve Regeneration Technologies, Ethical Issues,”
K. Gervais, 1989.“New Developments in Neuroscience: Historical and Ethical Issues in Neural Transplants,” R. Pinkus, 1989.
-180-

Appendix F
Acronyms and Glossary of Terms
Acronyms
AANs —American Association of NeurologicalSurgeons
ACTH —adrenocorticotropic hormoneADAMHA —Alcohol, Drug Abuse, and Mental Health
AHCPR
AIDSALS-P-D
BEACBMAACCLCNSCSFDHHS
FDAFFDCAGABA
GRAFT
HCFAHIV
LCMAO-B
MPP+
NDANGF
NINDS
NOTA6-OHDAPHSAPMAPNSPSPTH
UAGAUPFVP
Administration—Agency for Health Care Policy and Re-
search—acquired immunodeficiency syndrome—amyotrophic lateral sclerosis-Parkinson’s
disease-dementia—Biomedical Ethics Advisory Committee—Beta-N-methyl amino-L-alanine-continuous cell line-central nervous system-cerebrospinal fluid—Department of Health and Human Serv-
ices—Food and Drug Administration—Federal Food, Drug, and Cosmetic Act—gamma-aminobutyric acid—gonadotrophin-releasing hormone--General Registry of Adrenal-Fetal Trans-
plantation—human amnion membrane matrix—Health Care Financing Administration—human immunodeficiency virus—investigational new drug application—Institutional Review Board—locus ceruleus—monoamine oxidase B—motor neuron disease—methylpyridine—l-methyl-4-phenyl-l,2,3,6-tetrahydropyri-
dine—new drug application—nerve growth factor—National Institutes of Health—National Institute of Neurological Disor-
ders and Stroke—National Organ Transplant Act-6-hydroxydopamine—Public Health Service Act—premarket approval—peripheral nervous system—progressive supranuclear palsy—tyrosine hydroxylase—tetrahydroaminoacridine—Uniform Anatomical Gift Act—United Parkinson Foundation—vasopressin
Glossary of Terms
Abortion: The termination of pregnancy, whether spon-taneous (occurring naturally, a miscarriage) or in-duced. Induced abortions may be therapeutic (to treata medical condition of the pregnant woman) ornontherapeutic (elective).
Abortus: An aborted fetus. See fetus.Acetylcholine: A neurotransmitter involved in learning
and memory. Acetylcholine is diminished in Alz-heimer’s disease. See neurotransmitter.
Adrenal medulla: The innermost region of the adrenalgland; cells from this region can produce dopamine inthe brain and are potential candidates for neuralgrafting, particularly to relieve the symptoms ofParkinson’s disease. See chromaffin cell.
AIDS, acquired immunodeficiency syndrome: A con-dition in which the body’s immune system is depresseddue to infection by a retrovirus. See HIV, retrovirus.
Allograft: Tissue or cells transplanted between individu-als of the same species.
Alzheimer’s disease: A neurodegenerative diseasecaused by abnormality and death of nerve cells inseveral areas of the brain; the nerve cell loss isassociated with a deficit of several chemicals in thebrain, notably acetylcholine, resulting in dementia. Thecause of the nerve cell abnormality and loss isunknown.
Amyotrophic lateral sclerosis, ALS, Lou Gehrig’sdisease: A neurodegenerative disease caused by deathof nerve cells in the central nervous system that controlmuscle movement. Paralysis, but not dementia, results.The cause of the nerve cell death is unknown.
Animal model: An animal that shares or in which can bereplicated features of human disorders and that is usedin experimental studies of those disorders. Animalmodels may be homologous (sharing a commonorigin) or analogous (being similar in effect) to thehuman disease or injury being studied.
Astrocyte: A type of glial cell in the central nervoussystem; after injury to the central nervous system,astrocytes form a scar at the site of nerve damage andblock regeneration of axons. See glial cell.
Autograft: A transplant in which the recipient’s owntissue or cells are use& autografts pose no problem ofrejection by the recipient and provide a ready source ofgrafting material. Adrenal medullary grafts are anexample of autografts. See adrenal medulla, rejection.
Autonomic nervous system: Cells in the central andperipheral nervous systems that control such involun-tary functions of the body as temperature, metabolism,and response to stress.
–181–

182 ● Neural Grafting: Repairing the Brain and Spinal Cord
Axon: The long extension of the neuron along whichelectrical impulses travel. See neuron.
Basal ganglia: A group of nuclei in the upper part of thebrain that help mediate movement. See substantialnigra, striatum.
Biologic: A biological product for the prevention, treat-ment, diagnosis, or cure of human diseases or injuries;examples are vaccines, blood, and antitoxins.
Blood-brain barrier: A layer of tightly juxtaposedendothelial cells in blood vessel walls that protectsmuch of the central nervous system by selectivelyfiltering out some substances while allowing others topass from the blood into the brain. See endothelial cell.
Brain: One of the two components of the central nervoussystem, the brain consists of the cerebral cortex, thecerebellum, the upper brain, and the brain stem. Thebrain is the center of thought, action, and emotion. Itreceives sensory impulses and transmits motor im-pulses.
Brain stem: The lowest part of the brain, connecting thecerebral cortex and upper brain to the spinal cord.Nuclei in the brain stem regulate essential bodilyfunctions such as heart rate, blood pressure, andrespiratory activity. See nucleus.
Cadaveric fetal tissue: Tissue obtained from a deadfetus.
Catecholamine: A class of neurotransmitter includingdopamine, norepinephrine, and epinephrine (ahormone secreted by the adrenal medulla).
Cell body: The relatively compact portion of the neuron,which contains the nucleus. Compare axon, dendrite.
Cell culture: Cells grown in the laboratory; although thecells proliferate, they do not organize into tissue. Seeprimary cell culture, cell line, and continuous cell line.
Cell line: A group of cells derived from a primary cultureat the time of first subculture; an established cell linehas the potential for indefinite subculture in vitro. Seecontinuous cell line.
Cell suspension: Individual cells separated out from solidtissue and placed in a supporting fluid; also, as a formof neural grafting, injection of such cells into a hostcentral nervous system. Compare solid tissue graft.
Central nervous system, CNS: One of the two majordivisions of the nervous system, made up of the brainand spinal cord. Compare peripheral nervous system.
Cerebral cortex: The rounded upper portion of the brain,consisting of layers of neural cells and the pathwaysthat connect them. The cerebral cortex is divided intofour lobes on each side and is the part of the brain inwhich “thinking and decisionmaking take place. Seebrain.
Cerebrospinal fluid: Fluid manufactured in the brain andcontained within the brain and spinal cord; it circulatesin the central nervous system and is absorbed into andremoved by veins.
Chromaffin cell: A nonneuronal cell in the adrenalmedulla derived from precursor cells that also generateneurons in the autonomic nervous system. Chromaffincells produce neurotransmitters that are chemicallyrelated to those synthesized in the autonomic andcentral nervous systems. See adrenal medulla, precur-sor cell.
Clinical test, clinical research: Experimental analysis(as of drugs or surgery) using human beings.
Conceptus: The product of conception. See embryo,fetus.
Continuous cell line: Sustained, self-propagating cells inculture; such cells may arise spontaneously in primarycell culture, be derived from tumors, or be createdthrough genetic engineering. See cell culture, geneti-cally engineered cell.
Cryopreservation: The freezing and storage of cells ortissue at -1960 centigrade for use later.
Dementia: Loss of intellectual function.Demyelinating disorder: See demyelination, multiple
sclerosis.Demyelination: Destruction of the myelin sheath,
whether through injury or disease. See myelin sheath.Dendrite: Branched extension of the neuron cell body
which receives impulses from another neuron. Seesynapse.
Deprenyl: A drug shown to slow the progression ofParkinson’s disease in clinical trials by blocking theactivity of MAO-B. See MAO-B.
Device: Broadly, an instrument, apparatus, implant, invitro reagent, or other similar or related article intendedfor use in the diagnosis, cure, mitigation, treatment, orprevention of disease, or intended to affect the structureor function of the body, that works through nonchemi-cal, nonmetabolic means.
Differentiation: The stage of development during whichbrain cells stop dividing and acquire distinct character-istics and functions. Compare migration, proliferation.
Dopamine: A neurotransmitter that in insufficientamounts produces the symptoms of Parkinson’s dis-ease. See catecholamine, neurotransmitter.
Dorsal root: The portion of the nerve root that bringssensory information from the body to the spinal cord.See nerve root.
Drug: An article (other than foods or devices) intendedfor use in the diagnosis, cure, mitigation, treatment, orprevention of disease and designed to affect thestructure or any function of the body.
Dura mater: The tough, outermost membrane surround-ing the brain and spinal cord.
Elective abortion: See abortion.Embryo: The conceptus from fertilization until the end of
the eighth week See fetus.Endocrine system: The endocrine glands (such as the
thyroid and pituitary glands) and the hormones theysecrete.

Appendix F--Acronyms and Glossary of Terms ● 183
Endothelial cell: A type of cell lining the blood vesselwall that can trigger an immune response (and hencegraft rejection). See blood-brain barrier.
Epilepsy: Disruption in the normal electrical activity ofthe brain, resulting in seizures; epilepsy is diagnosed ifmore than one seizure occurs and those seizures are dueto central nervous system dysfunction.
Excitotoxin: A chemical substance (kainic acid, ibotenicacid, or quinolinic acid) that, when injected into thebrain, kills nerve cells by overstimulating them.
Ex utero: Outside the uterus.Fetus: In a legal context, the conceptus at all stages of
development; in a Federal regulatory context, theconceptus after implantation; in a scientific context, theconceptus from the end of the eighth week to themoment of birth. Compare embryo.
Fibroblast: A connective tissue cell, found in the skin,that can be induced through genetic engineering toproduce some chemicals (such as dopamine and nervegrowth factor) found in the brain.
Ganglion, ganglia: Term for a group of neurons that areusually located outside the central nervous system.Compare basal ganglia.
Genetic engineering: Altering the genetic makeup of acell.
Genetically engineered cell: A cell into which new geneshave been inserted
Germ cell: A reproductive (egg or sperm) cell or itsprecursors. Compare somatic cell.
Glial cell, glia: A basic cell type of the nervous system.Glial cells appear to perform support functions forneurons: namely, nutrition, insulation (through theproduction of myelin), and structural support. Com-pare neuron. See astrocyte, microglia, oligodendro-cyte, Schwann cell.
Hippocampus: A nucleus in the brain crucial to learningand memory.
HIV, human immunodeficiency virus: The retrovirusassociated with AIDS and AIDS-related complex. Seeretrovirus.
Huntington’s disease: A genetic neurodegenerativedisease caused by death of nerve cells in the striatum(producing abnormal movement) and elsewhere in thecerebral cortex (producing dementia). The cause of thenerve cell death is unknown.
Hypothalamus: A collection of nuclei in the brain thatcontrol such behaviors as eating and drinking and areinvolved in regulating the endocrine system. Thehypothalamus also produces hormones itself. Seeendocrine system.
Immune response: Reaction of the immune system toforeign matter. See immune system.
Immune system: A collection of organs, tissues, cells,and molecules in mammals that seeks out, identifies,destroys, and remembers foreign organs, tissues, cells,and molecules; the immune system protects the animal
from disease-causing organisms in the environment.See rejection.
Immunological privilege: The concept that the centralnervous system is not as closely monitored by theimmune system as the rest of the body and is thereforeless susceptible to graft rejection.
Immunoreactive: Capable of provoking a response fromthe immune system.
Immunosuppression: The use of drugs to prevent graftrejection by restraining the response of the immunesystem to foreign material.
Incidence: The number of new cases of a disorderoccurring during a given period of time (usually 1 year)within a given geographical area. Compare prevalence.
Incidence rate: Incidence per unit of population. Seeincidence.
Induced abortion: See abortion.Informed consent: As applied to human research, the
agreement of a person (or his or her legally authorizedrepresentative) to serve as a research subject, in fullknowledge of all anticipated risks and benefits of theexperiment. Informed consent requires that the re-searcher impart to the prospective subject any informa-tion that might influence the subject’s decision toparticipate or not participate in the research, includingan explanation of the methodology to be used, theavailability of alternative therapies, and the prospec-tive subject’s freedom to withdraw from the experi-ment at any time, without prejudice.
Institutionalize: To incorporate an act or practice into astructured, often formal, system. Compare legitimate.
Institutional Review Board, IRB: A group establishedby an institution conducting medical research to assessthe legal, ethical, and scientific aspects of that researchon human subjects. IRB approval is required by theDepartment of Health and Human Services beforeproposals can receive Federal funding. IRBs mustreview research protocols on a regular basis, but notless than once a year.
In utero: In the uterus.Investigational device exemption: Application to FDA
by a manufacturer for permission to ship a device priorto obtaining premarket approval, in order to conductstudies of safety and efficacy. See premarket approvalapplication.
Investigational new drug application, IND: Request bya manufacturer for exemption from FDA’s premarketapproval requirement; an IND is sought for shipmentof a drug for investigational use by qualified experts,in order to study the safety and efficacy of the drug.
In vitro: Literally, in glass; in the laboratory; outside thebody.
In vivo: In the body.Isograft: Tissue transplanted from one identical twin to
another; isografts pose no problem of rejection by theidentical twin who receives the graft.

184 ● Neural Grafting: Repairing the Brain and Spinal Cord
Kindled model: An animal model of epilepsy that isthought to be analogous to temporal lobe epilepsy inhumans. See animal model.
L-dopa, Levodopa: The precursor of the neurotransmitterdopamine. L-dopa is the standard therapy for personswith Parkinson’s disease.
Legitimate: To give legal status to an actor practice; toshow or affirm an act or practice to be justified.Compare institutionalize.
Limbic system: Structures in the brain that are associatedwith some aspects of emotion and behavior. Seehippocampus, hypothalamus.
Locus ceruleus: A nucleus of the brain that inhibits theability to induce seizures in the kindled model ofepilepsy. See kindled model.
Lymphatic drainage: The movement of fluids, mole-cules, foreign particles, and cells from various tissuesin the body through the lymph system to the immunesystem; a means by which grafted cells reach the host’simmune system and trigger rejection.
MAO-B, monoamine oxidase B: An enzyme that breaksdown certain neurotransmitters. It can also convertother chemicals to toxins that destroy substantial nigracells, thereby producing parkinsonism. See parkinson-ism.
Microglia: A type of glial cell in the central nervoussystem thought to enter the immune system and initiategraft rejection.
Migration: The movement of immature cells in the brainto the site where they will mature and remain perma-nently. Compare differentiation, proliferation.
Minimal risk: Term used to denote that the chance ofharm anticipated in proposed research is no greaterthan that encountered in daily life or during theperformance of routine physical or psychological tests.
Mortality rate: The number of deaths during a givenperiod of time (usually 1 year), within a givengeographical area, per unit of population.
Motor neuron disease: A type of neurodegenerativedisease in which neurons in the central nervous systemthat control muscle movement are destroyed. Seeamyotrophic lateral sclerosis.
MPTP, l-methyl-4-phenyl-l,2,3,6-tetrahydropyrid-ine: A synthetic narcotic that can cause parkinsonismin humans.
Multiple sclerosis, MS: A demyelinating disease charac-terized by an array of symptoms (such as loss ofcoordination, slurred speech, and dizziness), depend-ing on wherein the central nervous system the lesionsoccur. See demyelination.
Myelin: A fatty substance (of which the myelin sheathsurrounding axons is made) that acts as an electricalinsulator to speed the conduction of nerve impulses.Myelin is formed in the peripheral nervous system bySchwann cells and in the central nervous system by
oligodendrocytes. See myelin sheath, oligodendrocyte,Schwann cell.
Myelin sheath: Concentric layers of myelin surroundingthe axons of some neurons. The myelin sheath speedsthe conduction of electrical impulses. See myelin,oligodendrocyte, Schwann cell.
Nerve fiber: An axon and its surrounding myelin sheath.Nerve growth factor, NGF: A protein that promotes
axon growth in some areas of the peripheral nervoussystem and plays a role in the development ofvertebrate sensory and autonomic systems. In thecentral nervous system, it appears to protect fromdamage some populations of cells that synthesizeacetylcholine.
Nerve root: One of a collection of nerves that are attachedto and demarcate the 30 segments of the spinal cord.Nerve fibers enter and leave the spinal cord at one ofthe 31 nerve roots. These fibers link the peripheral andcentral nervous systems, bringing sensory informationfrom the body to the spinal cord and motor informationfrom the spinal cord to the body. See dorsal root.
Neural grafting: The transplantation (implantation) ofcells or tissue into the brain or spinal cord. As used inthis report, it refers to various treatment goals (such aspromotion of growth or provision of needed chemi-cals), materials (such as adrenal medulla or fetal centralnervous system tissue) and methods (such as cellsuspensions or cell lines) of grafting. See cell line, cellsuspension.
Neuritic plaque: Abnormal cluster of degeneratingneurons, other brain cells, and protein in the areasbetween neurons; found in the brains of persons withAlzheimer’s disease.
Neurodegenerative disorder: A class of neurologicaldisease marked by loss of a particular population orpopulations of nerve cells in the central nervoussystem. Symptoms vary and depend on the neuronslost. See, for example, Parkinson’s disease, Hunting-ton’s disease, Alzheimer’s disease, and amyotrophiclateral sclerosis.
Neurofibrillary tangle: Accumulation of twisted proteinfilaments inside nerve cells; found in the brains ofpersons with Alzheimer’s disease.
Neurological disorder: Disease of, or injury to, thecentral nervous system.
Neuron, nerve cell: The basic functional unit of thenervous system. The neuron is typically composed ofa relatively compact cell body containing the nucleus;several short, radiating extensions, or processes (den-drites); and one long process (the axon) with twig-likebranches along its length and at its end. Information inthe form of electrical impulses travels from thedendrites, through the cell body, and along the axon toother cells. Sensory neurons send information to thebrain and spinal cord; motor neurons send instructionsto muscles, organs, and glands. See axon, dendrite.

Appendix F--Acronyms and Glossary of Terms . 185
Neurotransmitter: Specialized chemical messenger (e.g.acetylcholine, dopamine, norepinephrine, serotonin)synthesized and secreted by neurons that sends a nerveimpulse from one nerve cell to another. Neurotransmit-ters are released into the synaptic space betweenneurons, bind to the dendrites of other neurons, andinitiate a message in those neurons. Some neurotrans-mitters stimulate the release of neurotransmitters fromother neurons, while others inhibit the release ofneurotransmitters from other neurons. Neurotransmit-ters are also released at synapses between neurons andother targets (e.g., muscles, glands). See synapse,synaptic space.
Neurotrophic factor: Chemical produced by someneurons and glial cells that affects the growth anddevelopment, maintenance of function, and response toinjury of neurons. See trophic factor, tropic factor, andnerve growth factor.
New drug: A drug not generally recognized by qualifiedexperts as safe and effective for use under theconditions prescribed, recommended, or suggested onthe label, 01 which has been recognized as safe andeffective but which has not been used to a materialextent or for a material time.
New drug application, NDA: Submission by a manufac-turer to the FDA of information on a new drug,including full reports of studies of safety and efficacy,specimens of proposed labelling, and methods ofmanufacture, processing, and packing. Approval of theNDA is required before a new drug can be introducedinto commerce. See investigational new drug applica-tion.
Nontherapeutic abortion: See abortion.Nontherapeutic research: Studies involving human
subjects designed to further scientific knowledge abouta disorder or process, with no anticipated direct benefitto the subjects themselves.
Norepinephrine: See catecholamine, neurotransmitter.Nucleus, nuclei: A group of cells in the brain, but
generally outside the cerebral cortex, that share thesame anatomical region and to varying degrees thesame function. The hippocampus, locus ceruleus, andsubstantial nigra are examples of nuclei.
Oligodendrocyte: A type of glial cell that forms myelinin the central nervous system; oligodendrocytes appearto inhibit the regrowth of damaged axons in the centralnervous system. Compare Schwann cell; see glial cell,myelin, myelin sheath.
On-off phenomenon: In Parkinson’s disease, alternatingperiods in which the patient’s motor symptoms areunder control (on) or severe and uncontrolled (off); thephenomenon occurs regardless of drug dosage.
Paraneuron: Cells that share a common heritage withcells in the nervous system. See chromaffin cells.
Paraplegia: Paralysis and loss of sensation from the waistdown as a result of damage to the middle or lower
portions of the spinal cord.Parkinsonism: A group of neurological disorders with
various causes (e.g., drugs, toxic chemicals, braintumors, and recurrent head injury). Symptoms includeabnormally decreased motor activity, tremor, andrigidity. The most common type of parkinsonism isParkinson’s disease. See Parkinson’s disease.
Parkinson’s disease, idiopathic Parkinson’s disease: Aneurodegenerative disease caused by death of nervecells in the substantial nigra and the resulting loss ofdopamine in the brain; symptoms are tremor, slowingof movement, and rigidity. The cause of the nerve celldeath is unknown. Compare parkinsonism.
Peripheral nervous system, PNS: One of the two majordivisions of the nervous system, made up of the nervesand ganglia outside the brain and spinal cord. Nervesin the peripheral nervous system connect the centralnervous system and sensory organs, other organs,blood vessels, glands, and muscles. Compare centralnervous system.
Precursor cell: An undifferentiated embryonic cell thatmay develop into one or another type of mature cell.See differentiation.
Premarket approval application, PMA: Applicationrequired by the FDA for certain devices; this applica-tion demonstrating safety and efficacy must be submit-ted to and approved by the FDA before the device canbe introduced to the market.
Prevalence: Total number of cases of a disorder inexistence at any given time in a given area. Compareincidence.
Prevalence rate: Prevalence per unit of population.Primary cell culture: Cells taken directly from an
organism and grown in vitro; most replicate a fixednumber of times or not at all. Compare continuous cellline.
Proliferation: The reproduction or multiplication ofsimilar forms of brain cells; the stage of developmentpreceding migration and differentiation. Comparedifferentiation, migration.
Protocol, research protocol: A complete description ofa proposed scientific experiment.
Quadriplegic: Paralysis and loss of sensation from theshoulders down as a result of damage to the upperspinal cord.
Regeneration: Regrowth of tissue. In the nervous sys-tem, regeneration often refers to regrowth of a damagedaxon. See axon.
Rejection, graft rejection: The destruction by theimmune system of foreign tissue; specifically, destruc-tion of foreign tissue transplanted into a recipient’sbody from a donor’s body.
Replication: The process of duplicating or reproducingitself, as cells. Compare proliferation.
Retrograde cell death: The killing, due to axonaldamage, of neurons located some distance away from

186 . Neural Grafting: Repairing the Brain and Spinal Cord
the site of an injury in the central nervous system.Retrovirus: Any of a group of RNA-containing viruses
that produce reverse transcriptase, which catalyzes theproduction of DNA using the virus’s RNA as atemplate; the DNA is incorporated into the genome ofthe infected cells. The AIDS virus is a retrovirus, as aremany infection- and tumor-producing viruses.
Risk-benefit analysis: A determination of whether therisks to health of using a drug or procedure exceed thetherapeutic and quality-of-life benefits that accruefrom its use.
Schwann cell: A glial cell in the peripheral nervoussystem that produces myelin for the myelin sheathsurrounding axons. Schwann cells also support re-growth of the axons of peripheral nerves. Compareoligodendrocyte; see myelin, myelin sheath.
Solid tissue graft: Apiece of tissue placed into the brainor spinal cord; such tissue contains more than one typeof cell and therefore may be more likely than a cellsuspension to provoke an immune response. Seeendothelial cell; compare cell suspension.
Somatic cell: Any cell in the body except reproductivecells and their precursors. Compare germ cell.
Spinal cord: A component of the central nervous system,the spinal cord is a core of neuronal cell bodiessurrounded by axons that extends from the bottom ofthe brain down the spinal column. The spinal cord isdivided into 30 segments. See brain, central nervoussystem.
Spontaneous abortion: See abortion.Standard therapy: Procedures no longer regulated as
research.Stereotactic surgery: A type of brain surgery; specifi-
cally, the implantation of tissue into the brain by meansof a needle inserted through a small hole in the skull.
Striatum, corpus striatum: Part of the basal ganglialocated in the upper part of the brain; the striatumreceives dopamine from cells in the substantial nigra.See substantial nigra.
Stroke: A sudden interruption of normal blood flow to thebrain, caused by blockage or rupture of a blood vessel,
that may result in a wide range of neurological deficits(such as coma, paralysis, or inability to speak),depending on wherein the brain the lesion occurred.
Substantial nigra: A nucleus in the brain; neurons in thesubstantial nigra produce dopamine and send theiraxons to the striatum. The cells of the substantial nigradegenerate in Parkinson’s disease. See striatum, Park-inson’s disease.
Synapse: The site at which an impulse is transmitted fromthe axon of one nerve cell to the dendrite of anothernerve cell, typically by a neurotransmitter. See neuro-transmitter.
Synaptic space: A narrow gap between two adjacentneurons into which neurotransmitters are secreted. Seeneurotransmitter, synapse.
Synaptic sprouting: A process of limited regrowthfollowing damage to the central nervous systemwhereby fibers from nearby, undamaged axons formnew branches and establish new synapses to replacesome of the lost ones.
Thalamus: A collection of nuclei in the brain that areinvolved in analyzing sensory and motor information.
Therapeutic research: Studies involving human sub-jects that are designed to cure or palliate a disorderexisting in those subjects.
Trophic factor: A chemical that promotes the growth ofaxons and the survival of neurons.
Tropic factor: A chemical that provides a surface orsubstrate for axon growth and guides the axon towardits target.
Upper brain: The portion of the brain between thecerebral cortex and the brain stem. See brain stem,cerebral cortex.
Vector: Transmitter of disease.Ventricle: Cavity in the brain that contains cerebrospinal
fluid. See cerebrospinal fluid.Viable: Capable of living; specifically, a fetus capable of
living outside the womb.Xenograft: Tissue transplanted from one species to
another.

Index
abortionand fetal tissue transplantation, 6,8, 10-12,22,24,39,43,72,
135-136, 151-159informed consent issues, 13types of, and morally relevant differences among them, 153
acetylcholine, 35,74-75,97,98acetyl-L-carnitine, 99adrenal cells, see adrenal cell grafts; chromaffin cellsadrenal cell grafts
age of donor and, 66,71,93-94animal experiments with, 65-66with antiparkinson drugs, 70-71cell survival rates, 65-66clinical studies of, 68-71developmental state of material and success of, 49disruption of blood-brain barrier, 53effectiveness of, 65, 66,69-71for Huntington’s disease, 73mortality rates, 68, 69-70with nerve growth factor, 66, 71for Parkinson’s disease, 6, 7, 21-22, 23, 45, 52, 62, 65-66,
68-71for progressive supranuclear palsy, 71psychological effects of, 52registries, 69-70
adrenocorticotropic hormone, 106Agency for Health Care Policy and Research, 15, 129AIDS, 53, 140alcohol-dated memory loss, 74Alcohol, Drug Abuse, and Mental Health Administration
funding of neural grafting research, 4,24peer review process, 12
allografts, 23,50,52,78FDA regulation of, 126
aluminum and aluminum binding, 98Alzheimer’s disease, 7, 19
animal model of, 74cause of, 98diagnosis of, 98incidence and prevalence of, 3,93,99nature of fictional loss in, 20,74,98pharmacological treatment of, 98-99potential of neural grafts for, 7,74-75,99symptoms, 98
Alzheimer’s disease-associated protein, 98amantadine, 97American Association of Neurological Surgeons, 70amygdala, 98amyotrophic lateral sclerosis, 7, 20
cause of, 99diagnosis of, 99-100incidence and prevalence of, 3, 93, 100medical interventions for, 100mortality rates, 100nature of functional loss in, 99potential of neural grafts for, 75, 100
symptoms of, 99amyotrophic lateral sclerosis-Parkinson’s disease-dementia, 96animal models
of Alzheimer’s disease, 74analogous, 61of epilepsy, 82excitotoxin, 73homologous, 61MPTP, 63-64,69need for, 61, 84of neuroendocrine d e f i c i t s , 8 36-OHDA, 63,65,66of parkinsonism, 23,43,45,63of spinal cord injury, 78of stroke, 81, 104
animal research on neural graftingwith adrenal medullary tissue, 65-66for Alzheimer’s disease, 74-75for amyotrophic lateral sclerosis, 75for brain injuries, 81-82for epilepsy, 82extrapolation to humans, 63with fetal CNS tissue, 42-43,63, 65, 72focus of, 61with genetically engineered cells, 66-67for Huntington’s disease, 73with mature CNS tissue, 49for multiple sclerosis, 84for Parkinson’s disease, 6,63-67with peripheral nerve tissue, 43-44for spinal cord injuries, 78-79,80transition to human studies, 11, 14,22-23,39, 127-128typeS of, 61
antioxidant, 101aspirin, 104astrocytes, 29, 30
effects of grafts from, 47function of, 35genetic engineering of, 48
autografts, 23,43,48,50,65,69,78FDA regulation of, 126, 127of genetically engineered cells, 127
autonomic nervous system, structure of, 32axons
communication along, 32function of, 30,31,76growth/regrowth of, 34-36,43,66,78structure of, 29synaptic pattern of, 34
basal forebrain, 98basal ganglia, 31, 102basic research on neural grafting, 3
Federal funding of, 3,4focus of, 61needs, 3,4, 19, 21, 39, 53
–187–

188 . Neural Grafting: Repairing the Brain and Spinal Cord
benztropine, 97beta-amyloid, 98Beta-N-methyl amino-L-alanine, 96biological rhythms, 42-43Biomedical Ethics Advisory Committee, 131Biomedical Ethics Board, 131blood-brain barrier, 40
development within grafts, 50,51disruption by implantation of tissue in CNS, 50,52,53species differences in, 64
braindevelopmental sequence in humans, 33-34immunological privilege, 23, 51injury response mechanisms, 66replacement of lost structures in, 41-42structure of, 30-31ventricles, graft placement in, 51, 52
brain-derived neurotrophic factor, 36brain injury, 7, 19
animal experiments on, 81causes of, 101-102function of neural grafts in, 7,20,82functional recovery from, 81,82,103-104incidence and prevalence of, 3, 93, 102-103mortality rates, 103nature of, 20neurotrophic activity at wound site, 36from surgical procedure for graft placement, 52see also stroke
brain stem, 31,32,80bromocriptine, 97
calcium channel antagonists, 101captopril, 99carbidopa, 96carotid body cells, 45,65catecholamines, 79, 80cell lines, 39
fetal tissue to start, 10see also continuous cell lines
cell suspensions, 46-47,49,62,72,79,82blood vessel formation in, 51
cells in cultureadvantages of, 47-48allographs, FDA regulation of, 127-127see also continuous cell lines
central nervous systemfetal, 5immunological privilege, 50, 51lymphatic drainage, 50organization/structure of, 4,5, 29, 30-32regrowth/regeneration in, 4, 34-35see also brain; CNS tissue grafts; spinal cord; and other
specific componentscerebral cortex, 30, 31,74, 81, 97, 98cerebrospinal fluid, 51cerebrovascular disease, 102CHAMPUS insurance program, 14chromaffin cells, 23, 45; see also adrenal cell graftsciliary neurotrophic factor, 36clinical research on neural grafting
with adrenal cells, 67, 68-71
cognitive limitations of patients and, 10coordination of, 15, 72-73ethical issues, 3, 10, 161-163Federal regulation of, 8, 13, 14, 113with fetal CNS cells, 67, 71-72; see also fetal CNS tissue
grailsgrievance mechanisms for patients, 121informed consent for, 8, 10, 113, 114-116, 119-121for Parkinson’s disease, 14,21,43,61,67-73, 161-162on particularly vulnerable groups, protection of, 116, 119,
121-122privately funded, 11, 12protection of neural graft recipients, 8,10,12,13,23,113-129protocol review and approval, 8, 14selection of subjects, 8, 113State regulation of, 12, 113-116surgical procedures, 67-68withdrawal from experiments, 120see also human studies
CNS tissue graftsadult, 23,49for demyelinating disorders, 84see also fetal CNS tissue grafts
continuous cell linesexcessive growth of, 52grafting with, 47-48ownership of, 159-161
Coordinated Framework for the Regulation of Biotechnology,122
corticosteroids, 101cryopreservation
of adrenal medullary tissue, 68of fetal CNS tissue, 43,45,46
cycads, and ALS-P-D syndrome, 96
dementia, prevalence in United States, 99, 102demyelinating disorders, 7,20, 102
nature of functional loss, 21, 83see also multiple sclerosis
dendritescommunication along, 32growth of, 34structure of, 29
Department of Defense, 8, 14Department of Health and Human Services
Ethics Advisory Board, 12moratorium on Federal funding of human fetal transplantation
research, 6,11,24,39,67,72,128, 149,151,154,171-173protection of neural graft recipients, 8, 12, 13,23, 113see also Food and Drug Administration; Public Health
ServiceDepartment of Veterans Affairs, 14-15, 129
funding of neural grafting research, 4,8,24spinal cord injury centers, 102
deprenyl, 64,96, 150DiGeorge’s syndrome, 151dopamine-producing cells, 23,45,62,67dorsal roots, regeneration of, 78Dunn, E., 21
encephalitis, 53endothelial cells, 51

Index ● 189
epidermal growth factor, 36epilepsy, 7, 20, 21
animal model of, 82characteristics of, 21, 104chug management of, 105function of neural gratis in, 7, 105incidence and prevalence of, 3, 93, 102, 105types of seizures, 104-105
ethical issuescontinuous cell line ownership, 159-161Federal funding and, 9-10, 149-151fetal tissue, 151-159human subjects in research, 3, 10, 161-163Nuremberg Code, 114research abuses, 114sources of materials for transplantation, 3, 6, 10, 22, 23-24,
151-161see also medical research ethics
excitotoxins, 73experimental allergic encephalomyelitis, 53
Federal Food, Drug, and Cosmetic Act, 122, 123, 125Federal funding
ethical issues in, 149-151moratorium on human fetal tissue transplantation research, 6,
11,24,39,67,72, 128, 149, 151, 154, 171-173of neural grafting research, 3, 24, 151regulations affecting, 8
fetal researchabortion and, 135-136on cadavers (fetal), 135, 152disposition of remains, 138-139ethical issues in, 152Federal policy development on, 130-131Federal regulations on, 131-132, 138-139grafting, see fetal CNS tissue graftsguidelines on, 8-9interstate transfer of a fetus, 137on live fetuses, 131-132, 135, 153State regulations on, 9, 132-135
fetal CNS tissue grafts, 39acetylcholine-producing, 75advantages over other tissues, 43,49for Alzheimer’s disease, 74,75animal experiments with, 4243,63,65behavioral control with, 4243,83blood vessel formation in, 51for brain injuries, 82brain stem cells, 80from cell suspensions, 46clinical trials, 71-72constraints on use of, 4, 6,43, 65, 67, 73continuous cell lines from, 136cryopreservation of cells, 43,45, 46effectiveness of, 4, 22,42, 53, 65, 66,72for epilepsy, 82ethical issues in use of, 151-159FDA regulation of, 23, 126, 127Federal oversight of, 9, 138-139for Huntington’s disease, 73identification of fetal brain region for materials, 43from induced abortions, 6, 10, 12, 13,39, 152-157
informed consent conditions, 12,13, 120,132, 155-156integration into mature CNS, 42manner and timing of procurement of tissues, 12,23-24norepinephrine-containing, 75number of cells used, 43for Parkinson’s disease, 6,22,43,52,62,63,65, 67,71-72and property rights, 10protection of donors of, 8-9, 129-137and respect for fetal life, 10, 152-152risks to recipients, 43, 136, 152-153sale of materials, 9, 12, 13, 24, 130, 131, 136-137, 140-142,
157-159for spinal cord injuries, 78-80spinal cord tissue, 78-79spinal motor neurons, 75as standard therapy, 157-158survival of grafts, 72
fibroblast growth factors, 36fibroblasts
genetic engineering of, 48risk from use in grafts, 48, 53tyrosine hydroxylase production by, 66
Food and Drug Administration, regulatory authoritybiological products, 123devices, 123drugs, 122-124interstate commerce and, 124-125limits on, 124-126neural graft materials, 8, 14, 23, 122, 126-127practice of medicine and, 125-126product safety and efficacy, 123-124
funding, see Federal funding
gamma-aminobutyric acid, 82, 97, 105ganglia, 32General Registry of Adrenal-Fetal Transplantation, 70genetically engineered cells, 39,65
animal studies with, 66-67autografts of, 127ethical issues related to, 161FDA regulation of, 127grafting methods, 6,48,67NGF-producing, 75
glia-derived nexin, 36glial cells
differentiation of, 34function of, 29-30,83inhibition of neuron regrowth, 40primary cultures of, 47replication of, 34Structure of, 29-30types of, 29,30
gonadotrophin-releasing hormone, 83
Health Care Financing Administration, 8, 13, 129heart transplants, funding controversies, 150hepatitis, 53herpes simplex, 53hippocampus, 74-75,82,98HIV, 140human amnion membrane matrix, 45human studies, see clinical research on neural grafts

190 . Neural Grafting: Repairing the Brain and Spinal Cord
Huntington’s disease, 7,20cause of, 73, 97functional loss from, 73,97incidence and prevalence of, 3,93,97-98potential of neural grafts in, 7,73symptoms of, 73, 97treatment of, 97
hyperexcitable nerve cells, 105hypothalamus, 31,82,83
idebenone, 99immune system response
to allografts, 52to cell suspensions versus solid tissue grafts, 47developmental state of graft material and, 49to fetal CNS tissue, 43,49to genetically engineered cells, 48multiple sclerosis and, 106Parkinson’s disease and, 52prevention of, 50source of tissue and, 5,45, 50-51,53to surgical procedure, 52
immunological privilege, 23, 50,51immunoreactive molecules, 50-51immunosuppression, risks to graft recipients, 52infections from grafting materials, 53informed consent
for donation of continuous cell lines, 159-161ethical issues, 162-163for fetal tissue donation, 12, 13, 132, 155-156information to be provided for, 119-120from particularly vulnerable populations, 121-122from patients in clinical studies, 8, 10, 113, 119-121penalties for violation of, 120-121State regulations on, 114-116, 119-121withdrawal from experiments, 120
injury, see brain injury; spinal cord injuryInstitutional Review Boards, 8, 12, 14, 15,23, 161
composition of, 118criteria for authorization of human research, 117ethical guidelines, 117-118Federal requirements for review by, 129procedure for obtaining approval of, 118purpose of, 113, 116-119State requirements for review by, 122
insulin and insulin-like growth factors, 36Interagency Head Injury Task Force, 102-103interstate commerce, and regulation of neural grafting, 124-125isografts, 50
Joint Commission on Accreditation of Healthcare Organiza-tions, 8, 129
L-dopaproduction by genetically engineered cells, 48treatment of Parkinson’s disease with, 95-97, 150
laminin, 36legal/regulatory issues
constitutionality of restrictions on research, 9, 137-138disposition of cadavers/fetal remains, 9, 13, 138-139Federal oversight, 9, 14, 137-142fetal research, 131-132, 138-139
grievance mechanisms for patients, 121indirect regulation, 8, 14, 129informed consent, 8, 12, 13, 119-121neural graft materials, see Food and Drug Administrationownership of continuous cell lines, 159-161payment of donors, 8,9,140-142protection of donors of fetal tissue, 8-9, 129-137protection of human subjects in research, 8, 13,22, 113-129;
see also clinical research on neural grafting; informedconsent; State laws
see also specific statuteslimbic system, 31locus ceruleus, 82,98Lou Gehrig’s disease, see amyotrophic lateral sclerosis
Medical Device Amendments of 1976, 124medical malpractice, 8medical research ethics, genesis of, 114Medical Treatment Effectiveness Program, 15Medicare/Medicaid coverage, 14, 129l-methyl-4-phenyl-l,2,3,6-tetrahydropyridine, 64,95methylprednisolone, 101, 106methylpyridine, 64microglia, 29, 30milacemide, 99monoamine oxidase B, 64moratorium on Federal funding of human fetal transplantation
research, 6,11,24,39,67,72,128, 149,151,154,171-173motor neurons, neural grafting with, 100motor neuron disease
potential of neural grafts in, 7,75see also amyotrophic lateral sclerosis
MPTP model of parkinsonism, 63-64,95multiple sclerosis, 7, 21
causes of, 105-106death rates, 106diagnosis of, 106drug therapy, 106and immune system function, 106incidence and prevalence, . of, 3, 93, 106-107potential of neural grafts in, 84, 106symptoms of, 105
myelinformation of, 34,43,47,83function of, 29,43loss of, 21, 105; see also multiple sclerosis
naloxone, 101National Academy of Sciences, 12National Commission for the Protection of Human Subjects of
Biomedical and Behavioral Research, 130, 151-152National Conference of Commissioners on Uniform State Laws,
13, 140National Institute of Neurological Disorders and Stroke, 70National Institutes of Health
budget, 113funding of neural grafting research, 4,24guidelines for neural grafting research protocols, 15guidelines for research on vulnerable subjects, 121Human Fetal Tissue Transplantation Research Panel, 12,154peer review process, 12
National Organ Transplant Act

Index ● 191
components covered under, 13-14fetal tissue regulation under, 9, 12-13, 141, 157
National Research Act, 130National Science Foundation, funding of neural grafting re-
search, 4, 24nerve fibers, 45,62nerve growth factor
with adrenal cell grafts, 66,71and Alzheimer’s disease, 98production by genetically engineered cells, 48protection of acetylcholine neurons, 75,98-99role of, 36stimulation by grafts, 41
nerve roots, 31-32nervous system
cellular components of, 29-30; see also glial cells; neuronschemical-electrical communication in, 32-34fetal (human), 43organization/structure of, 4,5, 29-32see also brain; central nervous system; peripheral nervous
system; spinal cord; and other specific componentsneural grafting
age of host and, 51-52,53,78-79alternatives to, 150-151and blood vessel formation, 51, 53definition of, 3,4,39effectiveness on neurological disorders, 19,61,63-64,93Federal interests in, 22-24historical perspective, 21-23,42with immature versus mature tissue, 5, 21,49,52,53,66number of cells used in, 52number of recipients, 19Nuremberg Code applied to, 114psychological effects of, 52,69replacement of chemicals with, 19,20, 3940,42replacement of lost structures with, 19,20,39,41-42risks to recipients, 5, 42, 52-53, 81, 152-153, 161-162; see
also immune system responsesite for transplantation, 44, 62, 63,72stimulation of cell growth and survival with, 19,20,40-41,63,
80success factors in, 5,49-51therapeutic strategies, 4, 19,39-42
neural grafting materials, 4-5,6, 53ethical and legal questions, 42, 151-161; see also ethical
issues; legal/regulatory issuesexcessive growth of, 52immunological problems of, 42infections from, 53man-made, coated with growth-promoting chemical, 45regulation of, 8, 23, 122sources of, 23,39,42see also adrenal cell grafts; fetal CNS tissue grafts; geneti-
cally modified cellsneuritic plaques, 98neuroblastoma cells, 47neurodegenerative disorders, 20
characteristics of, 20potential function of neural grafts in, 7see also specific diseases
neuroendocrine deficits, 7, 82-83neurofibrillary tangles, 98
neurological disordersanimal models of, 43costs of, 7, 93, 150disease, 20-21; see also neurodegenerative disorders, and
specific disordersepidemiology of, 94-100incidence and prevalence of, 3, 19,93injury, 20; see also brain injury; spinal cord injurynature of, 20-21potential of neural grafting for, 150treatment approaches, 3,7, 19,21in veterans, 102see also specific disorders
neuromuscular diseases, 102neurons
death of, 34,41,94,97,98differentiation of, 34injured, 40-41number of, 34peripheral autonomic, 5primary cultures of, 47regeneration of, 29, 34-35,40,45structure of, 29survival of grafting procedures, 43,47see also axons; dendrites
neurotransmitters, 7,44,45,73function of, 32-33implants in CNS, 40kinds of, 33-34see also specific neurotransmitters
neurotrophic factors, 34, 36,66,79, 82neurotrophin-3, 36neurotropic factors, 34, 36,79nimodipine, 99noradrenaline, 82,98nucleus/nuclei
defined, 30purpose of, 31
Nuremberg Code, 114
6-OHDA, 63,65,66oligodendrocytes
function of, 29,30,35,47,83primary cultures of, 47
organic brain syndrome, 102
paraneurons, 45Parkinson, James, 94Parkinson’s disease and parkinsonism, 7, 19
adrenal cell grafts for, 21-22,45,62,65-66,67, 68-71, 128animal research on, 23,43,45,63-67causes of, 95clinical trials of neural grafting, 14, 21, 43, 61, 67-72, 128,
161-162drugs used for treatment of, 97, 150epidemiology of, 94-97fetal CNS grafts for, 6,22,43,52,62,63,65, 67,71-72,136genetically engineered cell grafts for, 66-67incidence and prevalence of, 3,93,95,96-97mortality rates, 68, 69-70MPTP model, 63-64,66,95nature of functional loss in, 20, 62, 94

192 ● Neural Grafting: Repairing the Brain and Spinal Cord
neural grafting applications, 3, 5, 6,96number of recipients of neural grafts, 6, 67on-off phenomenon, 68registries, 69-70site for transplantation, 62, 63success of neural grafting in, 5,39,63,71,72,84,93, 150-151surgical procedures for grafts, 67-68symptoms, 62,64,94,95treatment of, 95-96
PC12, 47peripheral autonomic tissue
animal experiments with, 44-45developmental state of, and success of graft, 49
peripheral nerve cellsfunction of, 44grafts with, 23,39,43-44,45,78,84regrowth of, 44
peripheral nervous systemorganization/structure of, 4, 29, 32regrowth/regeneration in, 4, 34-35tissues used for grafting, 5
physostigmine, 99pituitary gland, 82policy issues and options
Federal funding of fetal tissue transplantation research, 11-12Federal Government role in development of neural grafting
procedures, 14-15laws and regulations applicable to fetal tissue transplantation,
12-14practice of medicine, and regulation of neural grafting, 125-126progressive supranuclear palsy, 71Protection of Human Subjects Act, 155Public Health Service Act, 8, 122, 123, 125-127
regulatory issues, see legal/regulatory issuesresearch, see animal research; basic research; clinical researchretrograde cell death, 76, 78
S100 protein, 36scar formation, 41
astrocytes and, 35, 47reduction of, 47,78
Schwann cells, 29,30axonal regrowth into, 35function of, 34,43,47,83from peripheral nerves, 84in primary cultures, 47
seizures, 21, 53, 82, 104; see also epilepsysexual potency/sexual behavior, restoration of, 83spinal cord
immunological privilege, 51regenerative capacity, 80replacement of lost structures in, 41-42, 76structure of, 31-32, 76
spinal cord injury, 7, 19age of host and effectiveness of grafts, 78-79animal models of, 78causes of, 75, 100demyelination in, 84effectiveness of grafts on, 80-81fetal brain tissue grafts, 79fetal spinal cord tissue grails, 78-79
fictional losses from, 102functional recovery from, 79-80,80-81, 101incidence and prevalence of, 3,93, 101, 102and neurotrophic and neurotropic factors, 79peripheral nerve grafts for, 78potential function of neural grafts in, 7,76-78, 101rehabilitative therapy, 81repair of nerve fibers, 76research needs on, 80risks to graft recipients, 81sources of graft materials, 79survival rates, 101
State lawson clinical research, 12, 113-116, 121-122on compensation for fetal tissue, 140-142on disposal of fetal remains, 138-139on fetal research, 9, 132-135on informed consent, 114-116, 119-121licensing, 8on protection of fetus, 132-135on protection of particularly vulnerable populations, 121-122on protection of pregnant women, 140; see also informed
consentstriatum, 62,67-68,72, 73,97stroke, 7, 19
animal model of, 81causes of, 102functional losses from, 103incidence and prevalence of, 3, 93, 104intracranial hemorrhage, 103ischemia, 103potential of neural grafting for, 81-82, 104
substantial nigra, 62, 63, 70, 94surgical procedures
adrenalectomy, 68,69-70clinical trials of, 128complications of, 68, 69-70effect of graft placement during, 52effect on success of graft, 66for epilepsy, 105open surgery, 67, 69for Parkinson’s disease grafts, 67-68,72regulation of, 8, 127-129stereotactic, 67, 72
suronacrine maleate, 99sympathetic ganglia, 65synapses
between graft and host, 40,62-63,73,82structure of, 32-33
synaptic contacts, 34, 36, 76, 80synaptic space, defined, 32synaptic sprouting, 34-35
tetrahydroaminoacridine, 99thalamus, 31Thompson, W. G., 21thyrotropin-releasing hormone, 101transplants, tissue and organ, number of recipients, 19trihexyphenidyl, 97tumor formation, from continuous cell lines, 48,52Tuskegee syphilis study, 114tyrosine hydroxylase, 66

Index ● 193
Uniform Anatomical Gift Act vasopressin, 83amendment of, 13 velnacrine maleate, 99applicability to fetal tissue implants, 9,13, 135,136,138-141,
154 Willowbrook hepatitis study, 114uniform donor card, 139United Parkinson Foundation, 70 xenograft, 50, 53

Related OTA Reports
. Neurotoxicity: Identifying and Controlling Poisons of the Nervous System—Special Report. Describes the scope of the public health threat posed by neurotoxicsubstances; Federal research, testing, monitoring, and regulatory programs to addressit; and the economic considerations associated with testing and regulatory programs.4/90; 350 p.
GPO stock ##052-O03-Ol184-l; $15.00
● Biological Rhythms and Shift Work. Examines biological rhythms and the role theyplay in regulating a variety of physiological and cognitive functions and the effectsdisruption of biological rhythms can have on those functions. In progress.
. The Biological Basis of Mental Illness. The report will evaluate research that hasadvanced the understanding of genetic and other biological factors underlying mentaldisorders, and the resulting implications of such research for diagnosis, treatment, andFederal policy. In progress.





























