Embed Size (px)
Citation preview

Nephrotic syndrome
Atma Gunawan

SPECTRUM DISEASES IN NEPHROLOGY
• Water,electrolyte,acid-base disorders• Urinary infections• Nephrolithiasis • Glomerulonephritis, vasculitis, tubulointerstitial
nephritis• Hypertension• Acute renal failure• Chronic renal failure• Dialysis • Kidney transplant

AsymptomaticProteinuria 150 mg to 3 g per day
Hematuria > 2 red blood cells per high-power field (>10x106 cells/L)in spun urine (red blood cells usually dysmorphic)
Macroscopic hematuriaBrown / red painless hematuria (no clots); typically
coincides with intercurrent infectionAsymptomatic hematuria + proteinuria between attacks
Nephrotic SyndromeProteinuria : adult >3.5g/day; child
>40mg/hour per m2
Hipoalbuminemia <3.5g/dLEdema
HipercholesterolemiaLipiduriaNephritic syndrome
OliguriaHematuria: red cell casts
Proteinuria : usually <3g/dayEdema
HypertensionAbrupt onset, usually self-limiting
Rapidly progressive glomerulonephritisRenal failure over days / weeks
Proteinuria : usually <3g/dayHematuria : red cell casts
Blood pressure often normalMay have other features of vasculitis
Chronic GlomerulonephritisHypertension
Renal InsufficiencyProteinuria
Shrunken smooth kidneys
Clinical Presentations of Glomerular Disease
Feehally J, Johnson RJ,;2000

Nephrotic SyndromeDefinition
A clinical entity of multiple causes
characterized by :
Proteinuria > 3.5 gram / day EdemaHypoalbuminemia (< 3.0 g/dl)+ Hypercholesterolemia+ Lipiduria (oval fat bodies)
+ Hematuria + Hypertension + Uremia
PURE
“NON”PURE

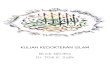
Schematic drawing of the glomerular barrier. Podo = podocytes; GBM = glomerular basement membrane; Endo = fenestrated endothelial cells; ESL = endothelial cell surface layer (often referred to as the glycocalyx). Primary urine is formed through the filtration of plasma fluid across the glomerular barrier (arrows); in humans, the glomerular filtration rate (GFR) is 125 mL/min. The plasma flow rate (Qp) is close to 700 mL/min, with the filtration fraction being 20%. The concentration of albumin in serum is 40 g/L, while the estimated concentration of albumin in primary urine is 4 mg/L, or 0.1% of its concentration in plasma. Reproduced from Haraldsson et al, Physiol Rev 88: 451-487, 2008, and by permission of the American Physiological Society

Proteinuria in AdultsPresentation by Severity of Proteinuria
< 3.0 g/day
asymptomatic
> 3.5 g/day
asymptomatic
swelling of feet / face
shortness of breath
(in aged + heart / liver disease)
+ gross hematuria + features of hypertension
Cattran DC, 1999

Underfill Overfill
Proteinuria
Hypoalbuminemia
Plasma colloid oncotic pressure
Plasma volume
Vasopressin
Atrial Natriuretic Peptide (ANP)
normal/low
Renin-angiotensin system activated
Aldosterone
Water retention
Edema
Sodium retention
Primary tubular defect causing
Sodium retention
Plasma volume
normal/
Vasopressin normal
ANP Aldosterone
Starling forces
** The kidney is relatively resistant to ANP in this setting, so it has little effect in countering retention
Formation of Nephrotic Edema
Feehally J, Johnson RJ;2000

Nephrotic SyndromeCauses
Primary causes
Minimal change disease
Membranous nephropathy
Focal segmental glomerulosclerosis
Proliferative
IgA Nephropathy
SLE Post infective
(HBV, HCV, HIV, typhoid, malaria etc)
Secondary causes
Diabetes Mellitus
Systemic / vascular diseases (immune complex diseases) : SLE , Periarteritis Nodosa , Amyloidosis
Drugs : NSAIDs, -interferon, pencillamine, gold (membranous nephropathy), phenytoin / dilantin, lithium (chronic interstitial nephritis)
Allergy : pollen, house dust, insect/ snake bites, immunization, tetanus, smallpox
Malignancy : Hodgkin’s disease, mycosis fungoides, CML (membranous GN)
Renal Vein Thrombosis
Pregnancy

MESANGIO PGN

Age-Associated Prevalence of Nephrotic Syndrome (P.A)
ADULTCHILDREN
10,8
1,6
16
9,8
19,7
11,8
22
5,9
10 20 30 50 60 7040 800
10
20
30
50
60
70
40
80
100
90
MINIMAL CHANGES
FSGS
MEMBRANOUS
MCGN
OTHER PROLIFERATIVE
DIABETES
AMYLOIDLUPUS
OTHER
ALLADULTSAGE AT ONSET OF NS
542517
76
ALLCHILDREN
% %%
Cohen AH, Glassock RJ; 1999

Basement membrane
Epithelial Cell Foot Process
Endothelial Cell
Mesangial Cell
Mesangial Matrix
Schematic Representation of a Normal Glomerular Lobe
Cotran RS, Kumar V, Robbins SL; 1994

Minimal Change DiseaseCotran RS, Kumar V, Robbins SL; 1994

Membranoproliferative GN

Mesangioproliferatip GN

Nephrotic SyndromeDiagnosis / Prognosis
Primary GN
Adults Children % of Cure/ESRD
75% 95%
MCD 15% 80% 100/0
FSGS 20% 15% 40-60/50
MGN 30% 50/25
IgAN 10% 33/50
Cattran DC, 1999

Nephrotic SyndromeDiagnosis / Prognosis (cont.)
Primary GN (cont.) Adults Children % of Cure/ESRD
MPGN 3-5% 1% 33/20
Crescentic 1-2% 1% 33/40
Secondary GN 25% 5% 70/30
Cattran DC, 1999

Diagnosis History and physical exam:preexisting
disease (DM,infections,drug, arthritis, rash), diabetic retinopathy,malignant hypertension, malignancy.
Laboratory :CBC,electrolyte,RFT,albumin,lipid profile,urinalysis,ANA test,total complement levels,serum and urine elektrophoresis,hepatitis B,streptococcal,VDRL

Renal Biopsy
Adult : for all caused by primary renal disease
Children 1-6 years has failed with 4 week course of prednisone

>3.5 g/dayNephrotic Syndrome
Glucose High Normal Glucose
Consider :Diabetic -glomerulosclerosis
Family History of Kidney Disease
No Family History of Kidney Disease
Consider :Alport’s disease
OrFabry’s disease
EXAMINE SEROLOGY
Al-Haidary A, van Wyck DB; 1998
DIAGNOSTIC PROCESS

EXAMINATION SEROLOGY
Elevated ANA
LowC3, C4
Positive ANCA
Positive anti-GMB antibody
Serologic examination
NEGATIF
Hepatitis Bor
HIV antigenemia
ConsiderLupus GN
ConsiderLupus GN
Post Infectious GNCryoglobulinemia
orMembrano
proliferative GN
ConsiderSystemic vasculitis
orWegener’s
granulomatosis
ConsiderGoodpature’s
Syndrome
ConsiderFocal sclerosisMinimal change
diseaseDrugs
ConsiderHepatitis
orAIDS related nephropathy
RENAL BIOPSY
TREAT UNDERLYING DISEASEPREVENT SECONDARY PROGRESSION
Al-Haidary A, van Wyck DB; 1998

Common Glomerular Disease Presenting as Nephrotic Syndrome in AdultsDisease Association Serologic tests
Minimal change disease Allergy, atopy, NSAIDs, Hodgkin’s disease None
Focal segmental glomerulosclerosis
African-American -
HIV infection HIV antibody
Heroin -
Membranous Nephropathy
Drugs, gold, penicillamine, NSAIDs -
Infection : hepatitis B, C, malaria HBsAg, anti-HCV antibody
Lupus Nephritis Anti-DNA antibody
Malignancy breast, lung, gastrointestinal tract -
Membranoproliferative glomerulonephritis (Type I)
C4 nephritic factor C 3, C 4
Membranoproliferative glomerulonephritis (Type II)
C3 nephritic factor C 3, C 4 normal
Cryoglobulinemic MPGN Hepatitis Canti-HCV antibody, rheumatoid factor, C3, C4 , CH50
Amyloid
MyelomaSerum protein electrophoresis, urine immunoelectrophoresis
Rheumatoid arthritis, bronchiectasis, Crohn’s disease (and other chronic inflammatory conditions), familial Mediteranian fever
-
Diabetic nephropathy Other diabetic microangiopathy None
Feehally J, Johnson RJ,;2000




HOW PROTEINURIA MAY CAUSE RENAL INJURYHOW PROTEINURIA MAY CAUSE RENAL INJURY
Proximal CellProximal Cell Cell InjuryCell Injury Progressive Renal DamageProgressive Renal Damage
Protein Molecules
Protein Molecules FibroblastsFibroblasts MacrophagesMacrophages
CytokinesIL-6
PDGF-ßTNFα, others
CytokinesIL-6
PDGF-ßTNFα, others
Matrix ProteinsMatrix Proteins CollagenCollagen
ChemokinesAII
MCP-IET-I
ChemokinesAII
MCP-IET-I
Toto RD; 1997Toto RD; 1997
Fibrosis
Inflammation



Treatment nephrotic syndromeGENERAL• Diet : protein 0.6-0.8 g/kgBW, low fat• Correction hypoalbuminemia• Diuretics• Treat infection• Treat hypertension• Treatment proteinuria• Dypiridamole,warfarin• Treatment hypercholesterolemiaSPECIFIC THERAPY• Steroid• Cytotoxic agents :
cyclosporine,cyclofosfamide,chlorambucyl,mycophenolate mofetil

Response to therapy• Complete response (remission) is a reduction in proteinuria to 300 mg/day.• Partial response is a reduction in proteinuria of 50 percent, with absolute
values between 300 mg and 3.5 g/day or proteinuria less than 3.5 g/day with a normal serum albumin concentration
• Relapse is return of proteinuria to approximately 3.5 gm/day in patients who had previously undergone a complete or partial remission.
• Frequent relapsers if they have three or more relapses per year.• Glucocorticoid-dependence refers to relapse while on therapy or
requirement for continuation of steroids to maintain remission• Glucocorticoid-resistance refers to little or no reduction in proteinuria after
16 weeks (in children : 4 weeks) of adequate prednisone therapy, or some reduction in proteinuria but do not meet the criteria for partial remission.
Clin J Am Soc Nephrol. 2007;2(3):445-53.

Management of Edema in Nephrotic SyndromeOral loop diuretic e.g. Furosemide 40 mg bid
Bumetanide 1 mg bid
Double dose until diuresis or ceiling dose reached
Furosemide 250 mg bid Bumetanide 5 mg bid
Add : oral Thiazide e.g. Hydrochlorothiazide 50 mg bid
Metolazone 2.5-5 mg daily
Change loop diuretic to IV bolus bid
Add : 20% human albumin 50-100 ml IV followed by IV bolus diuretic
Mechanical ultrafiltration
Reduce stepwise to
maintenance dose as diuresis
continues
Monitor serum K+
If hypokalemic :Add : K supplementsOr Amiloride 5-20 mg dailyOr Spironolactone 50-200 mg daily*
No response
No response
No responseResponse
No response
No response
* Spironolactone is less effective in nephrotic syndrome than in cirrhosis and is often poorly tolerated because of gastrointestinal side-effects
Feehally J, Johnson RJ,;2000

Correction of AlbuminemiaInfusion of Na+ free albumin induces diuresis
benefit ?Treatment of Infections
Use appropriate antibioticsDipyridamole and Warfarin Plus Regimen
P and W + regimen (Woo Keng Thye)Dipyridamole
anti-platelet & anti-PDGF75 – 100 mg 3x/day
Warfarinanti-thrombotic1 – 3 mg
Treatment of HypercholesterolemiaCholesterol is toxic to mesangial cellsUse StatinSerum albumin should be > 3.0 g/dl
Thye WK; 1999

Treatmentof
Hypertension
Reducing
Proteinuria
Angiotensin Converting Enzyme Inhibitor (ACE I)
Angiotensin II Receptor Antagonist (ARB)
Calcium Channel Blocker – NonDihydropyridine (CCB-nonDHPP)

• Lower blood pressure
• Lower glomerular capillary pressure
• Improve glomerular permeability to plasma proteins (protein)
• Inhibit hypertrophy in glomerular and tubular cells
ACE Inhibitors :Renal Protective Effects
Toto RD; 1997

REDUCING PROTEINURIA WITH ACE INHIBITORS MAY SLOW PROGRESSION OF RENAL DISEASE
• Reduce mesangial injury and proliferation
• Reduce risk of tubulointerstitial damage
• Improve hyperlipidemia – reduce glomerular and tubular injury

ACE Inhibition and Glomerular Function
EAR
FilteredProteins
Bowman’sCapsule
GlomerulusAfferentArteriole
BP
GCP
EfferentArteriole
Lewis E. Contrib Nephrol 1996;118:206-213.

Steroid

Histologic Patterns and Steroid Responsiveness in Diseases Causing Nephrotic Syndrome
Mesangial hypercellularity
Focal segmental glomerulosclerosis
(FSGS)
Minimal change disease (MCD)
IgM Dense Deposit disease
Steroid responsive
Mason PD; 2000

Percentage of steroid responsiveness in distinct primary nephrotic syndrome
Histopathologic diagnosis Complete remission (%)
Steroid dependence (%)
Steroid resistance (%)
MCD 36.4 59.1 4.6FSGS 37.9 27.6 34.5MN 17.6 17.6 64.7IgAN 18.8 50.0 31.3Non-IgA mesangial proliferative GN
37.5 50.0 12.5
THE MALAYSIAN REGISTRY OF RENAL BIOPSY 2008

Treatment Minimal change

Treatment of minimal change disease in adults
• oral prednisone at a daily dose of 1 mg/kg of body weight (maximum dose 80 mg/day), minimum 8 weeks, until complete remission or 16 weeks.
• After attaining remission, prednisolone was tapered by 10 mg/week until reaching 5 mg/day; this dose was continued for a mean of 1 - 2 years

Cumulative rate of remission in response to steroids in MCD
Am J Kidney Dis 2002; 39:503.

TREATMENT OF RELAPSE
• Administer oral prednisone at a daily dose of 1 mg/kg (maximum dose of 60 to 80 mg per day) for a minimum of four weeks
• If remission is attained, the dose is then tapered in 5 mg increments every week to discontinuation within one to two months.

Steroid dependence, frequent relaps, steroid resistance
• Cyclosporine 3 mg/kg/d and prednisone 10 mg/d until remission or 6 months
• Then maintaned : cyclosporine 2 mg/kg/d and prednisone 5 mg/d for 1-2 years, then gradually withdrawn.

Treatment of primary focal segmental glomerulosclerosis

Treatment of primary focal segmental glomerulosclerosis
• Prednisone induces complete or partial remission in 40 to 80 percent of patients with relatively preserved renal function
• Initial treatment with steroid is similar like treatment for MCD

Steroid-dependent and steroid-resistant FSGS
• Initiate cyclosporine at a dose of approximately 3 to 4 mg/kg per day (given in two divided doses)
• Continue cyclosporine for at least six months following attainment of a complete remission and one year following attainment of a partial remission
• Maintain the remission with cyclosporine at dose ≤3 mg/kg per day)
• Prednisone is given concurrently at a dose of 0.15 mg/kg (maximum 15 mg/day). After six months, we taper prednisone to 5 or 7.5 mg/day and maintain it along with the cyclosporine for an additional 6 to 12 months after attaining a remission

Treatment of idiopathic membranous nephropathy

Treatment of idiopathic membranous nephropathy
• Oral cyclophosphamide (1.5 to 2.0 mg/kg per day) for six months plus glucocorticoids (methylprednisolone, 1 g intravenously daily for three days in months 1, 3, and 5, and oral prednisone, 0.5 mg/kg every other day for a total of six months with subsequent tapering)
• Cyclosporine 3.5 mg/kg per day, with dose adjustment to maintain a 12-hour trough cyclosporine concentration of 110 to 170 µg/L for 12 months . Monitor serum creatinine concentration due to renal toxicity

Wassalam