Embed Size (px)
Citation preview

NeoplasiasMieloproliferativas
Renato Sampaio TavaresProf Assistente de Hematologia da Fac Medicina da UFG
CRM - GO: 6538

Policitemia vera: Algode novo apóshidroxiuréia?



MPN symptoms perception – Physicians vs Patients

MPN treatment objectives – Physicians vs Patients





• 365 patients
• Median follow-up: 30 months
• Plhebotomy with and without Hydrea
• 1:1
• Htc < 45% vs Htc 45% - 50%
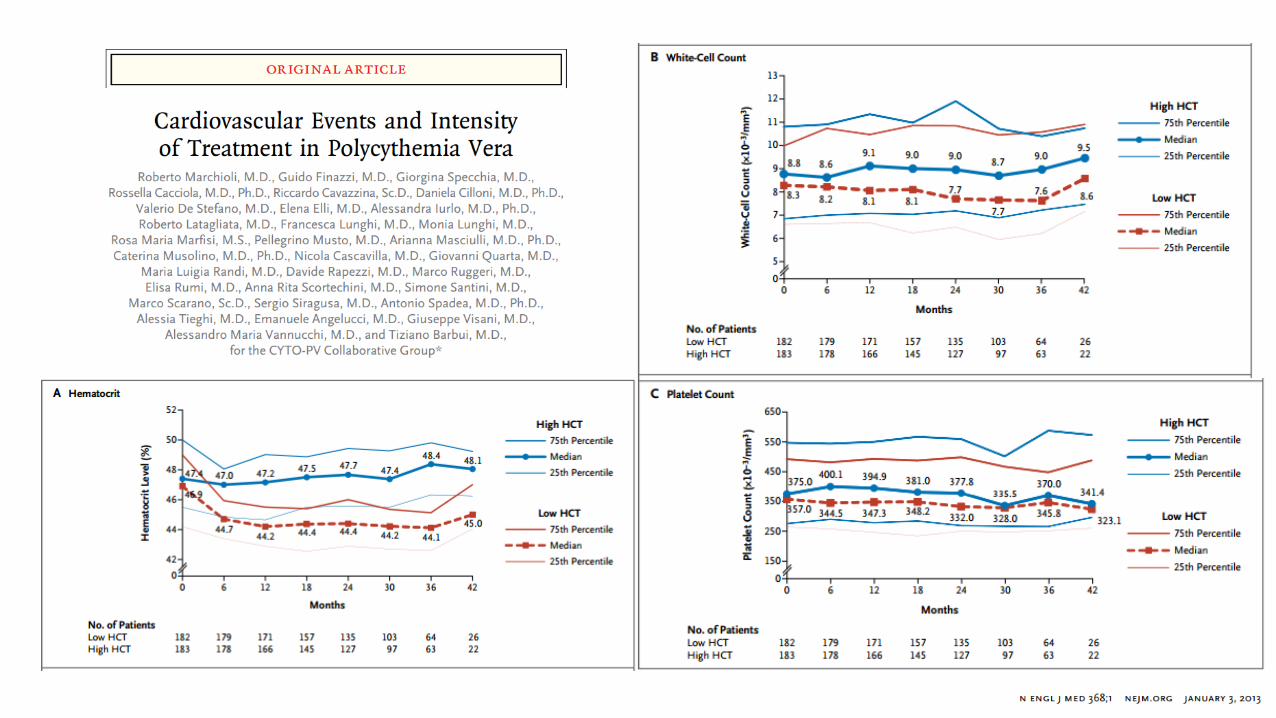

High Htc vs Low Htc - Results
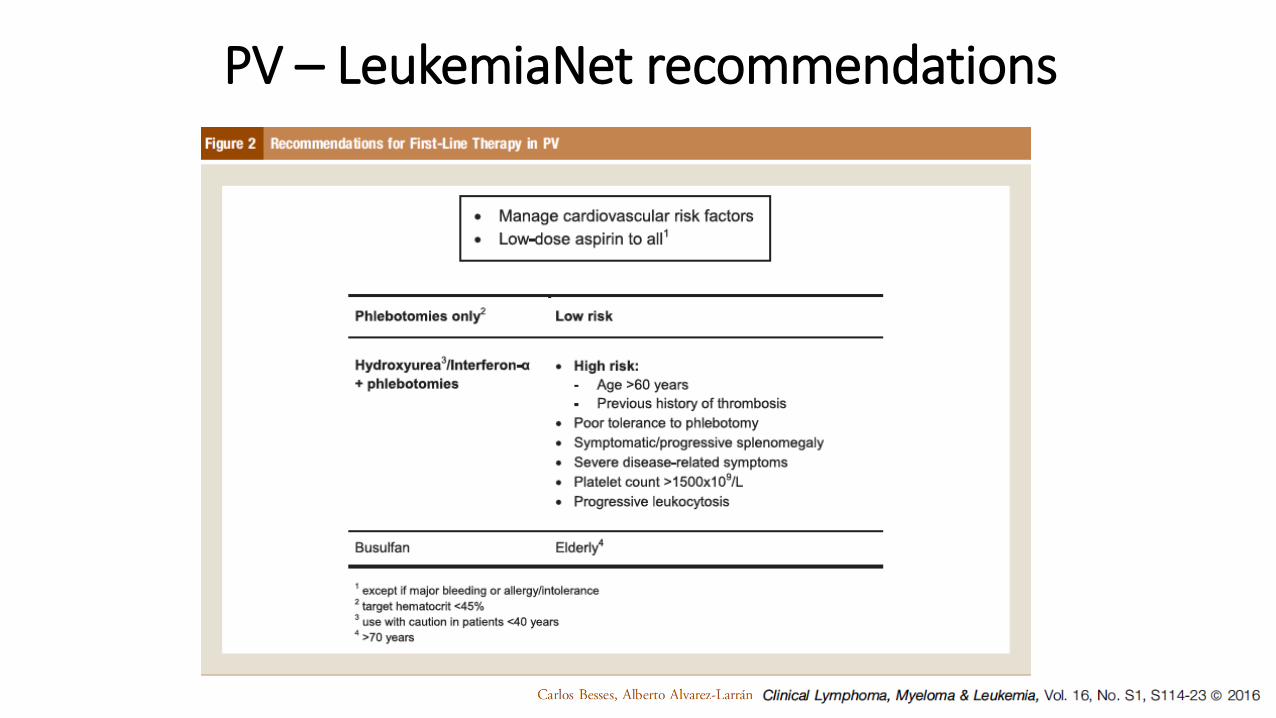
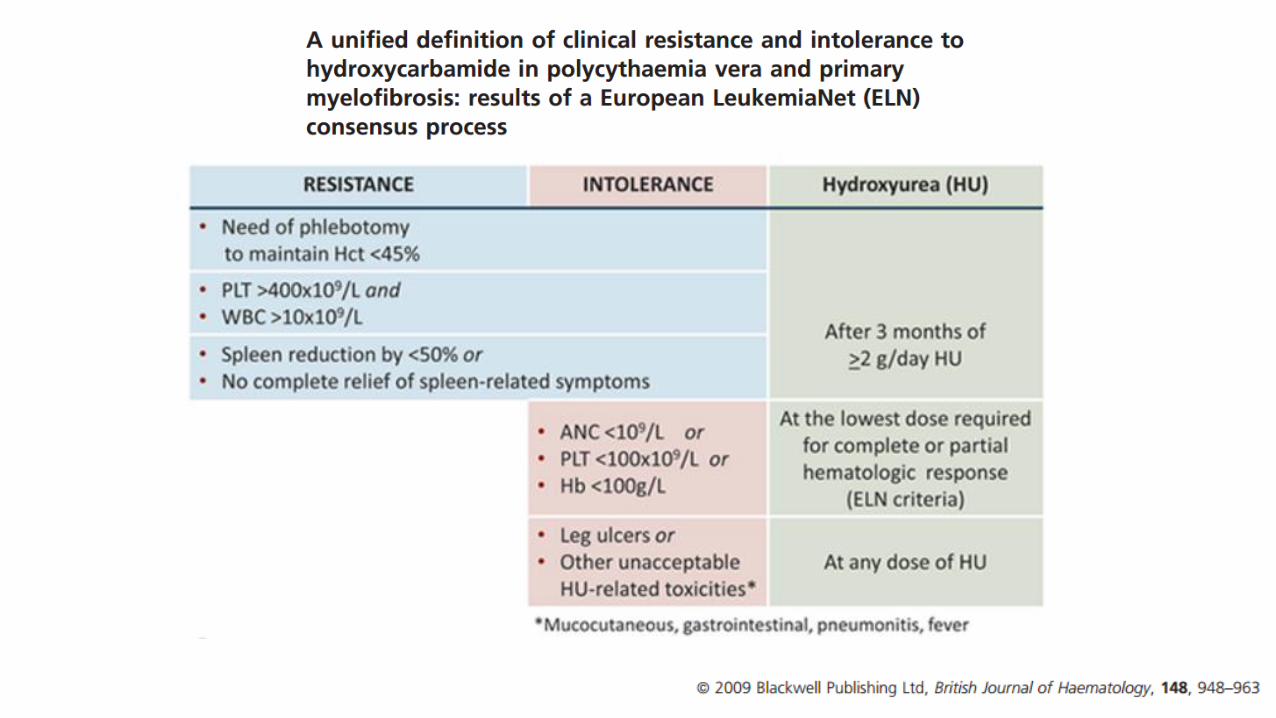
PV – LeukemiaNet recommendations


Leukemogenic:ChlorambucilP32Other Alkilant agents
Non-Leukemogenic:InterferonAnagrelide
Polycytemia Vera – Treatmentand Leukemic Transformation



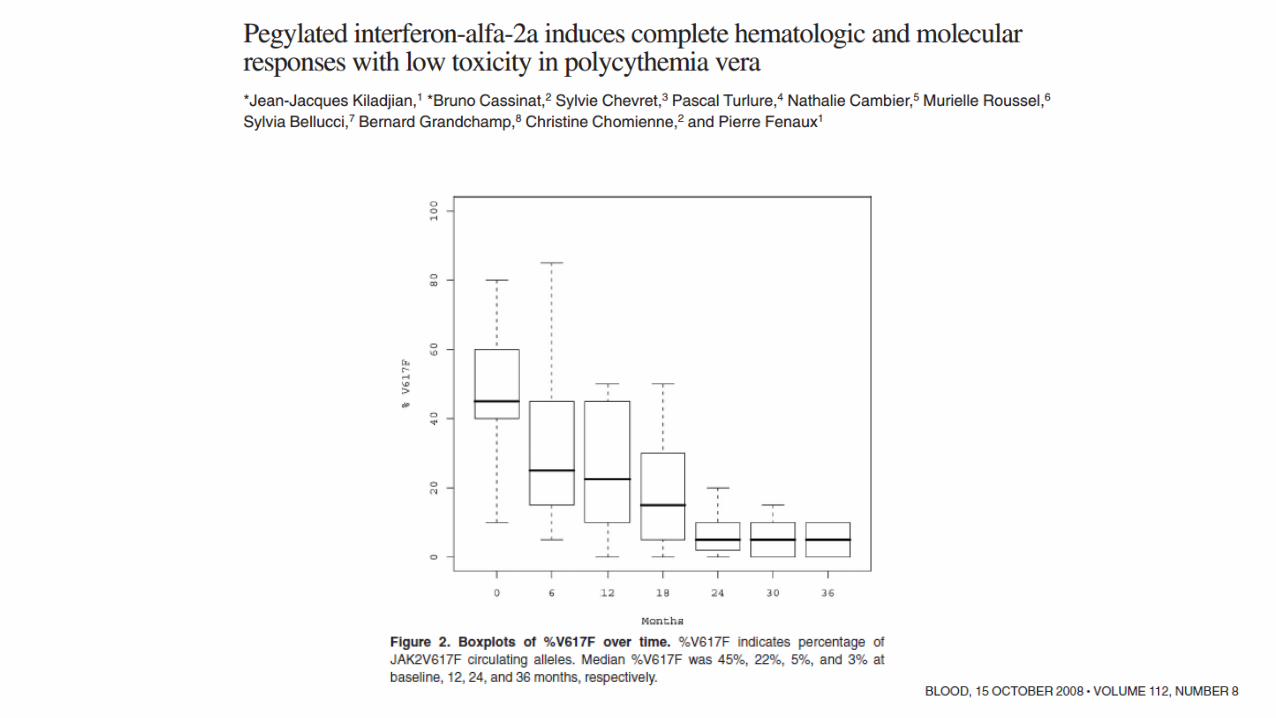

Interferon in Polycytemia Vera
Ongoing Interferon vs Hydrea Phase III studies
• MPD-RC 112 trial 1 (pegylated interferon alpha-2a ) - interim analysisin
No benefit (hematologic control, allele burden reduction, BM changes
Tolerability was inferior
• PROUD study 2 (ropeginterferon alfa-2b) - preliminarily report
Not inferior in hematologic control
Less adverse events
1. Gisslinger H, et al. Blood. 2016; 128(22). Abstract 4752. Mascarenhas J, et al. Blood. 2016;128(22). Abstract 479




Hydroxyurea Leg Ulcers






• RESPONSE TRIAL• 222 patients resistant /
intolerant to Hydrea• Phlebotomy dependence *• Spleen: 450 >= cm3
• Ruxolitinib vs BAT – 1:1• End-point
• Hematocrit control• >35% spleen reduction
* 2 or more within 24 weeks
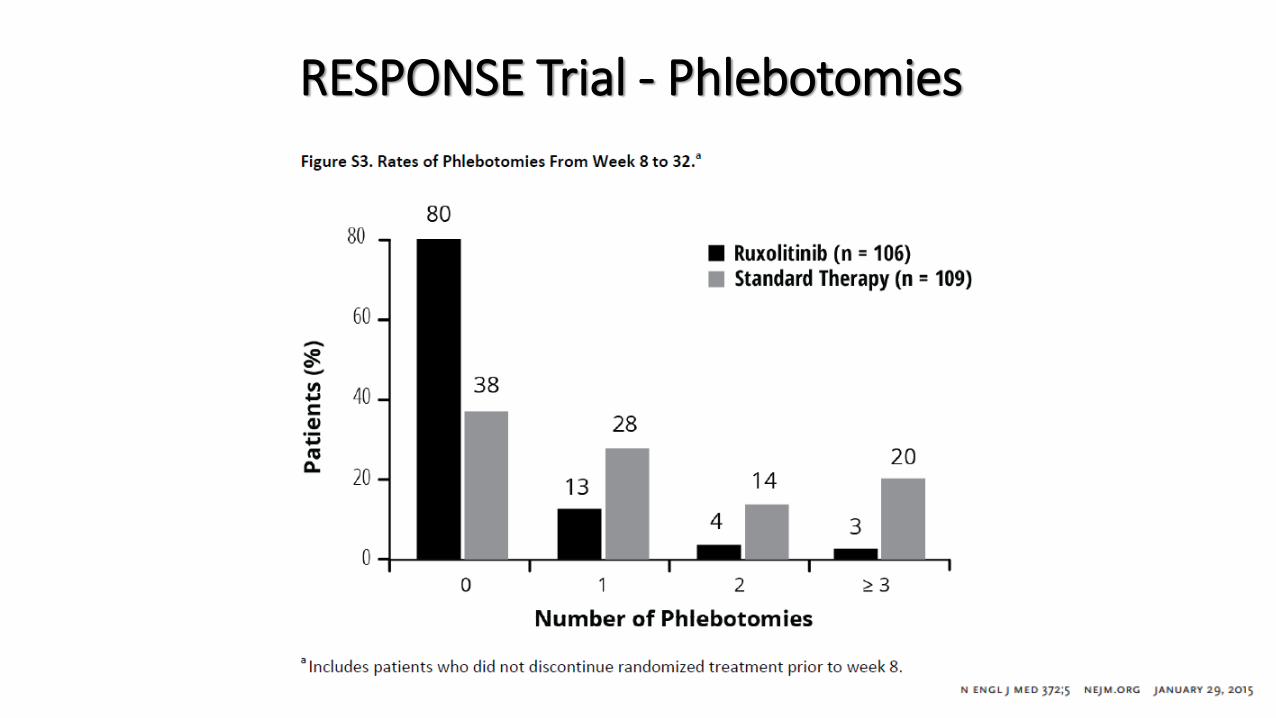
RESPONSE Trial - Phlebotomies

RESPONSE Trial – Patient Global Impression
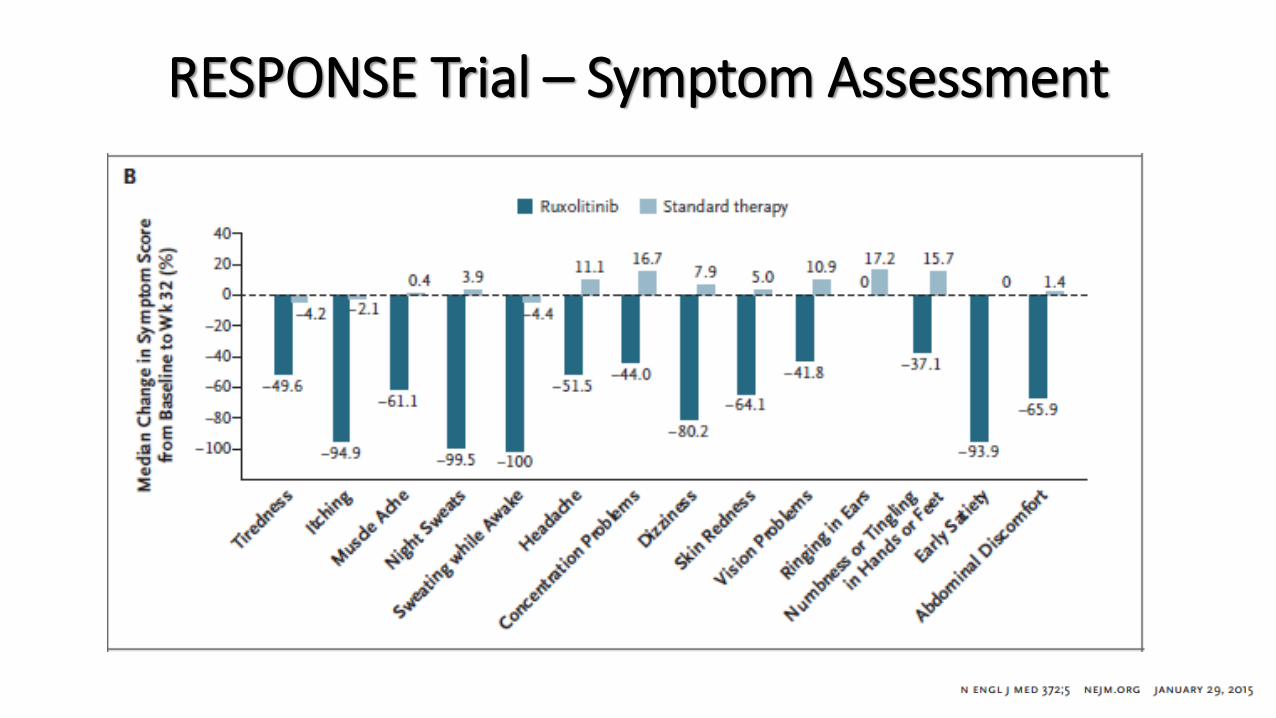
RESPONSE Trial – Symptom Assessment
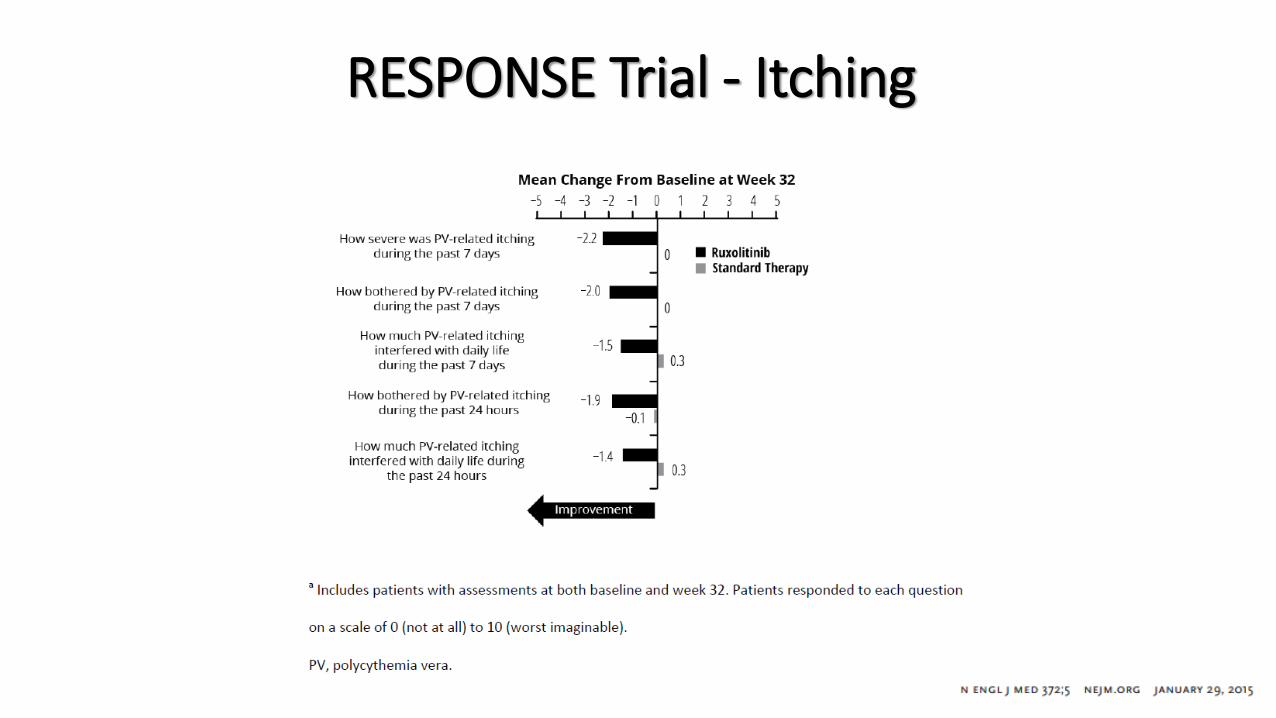
RESPONSE Trial - Itching

RESPONSE Trial – Funtional Scales and Individual Symptoms

RESPONSE – 80-week analysis

RESPONSE – 80-week analysis

RESPONSE – 80-week analysis

• 149 patients resistant / intolerant
to Hydrea without splenomegaly
• Phlebotomy dependent
• Ruxolitinib vs BAT – 1:1
• End-point
• Hematocrit control



Take Home Messages• ASA continuously and hematocrit below 45% should be
offered to all PV patients
• Interferon is a suitable treatment option for young andrelapsed PV patients, but still lacks phase III studies finalresults
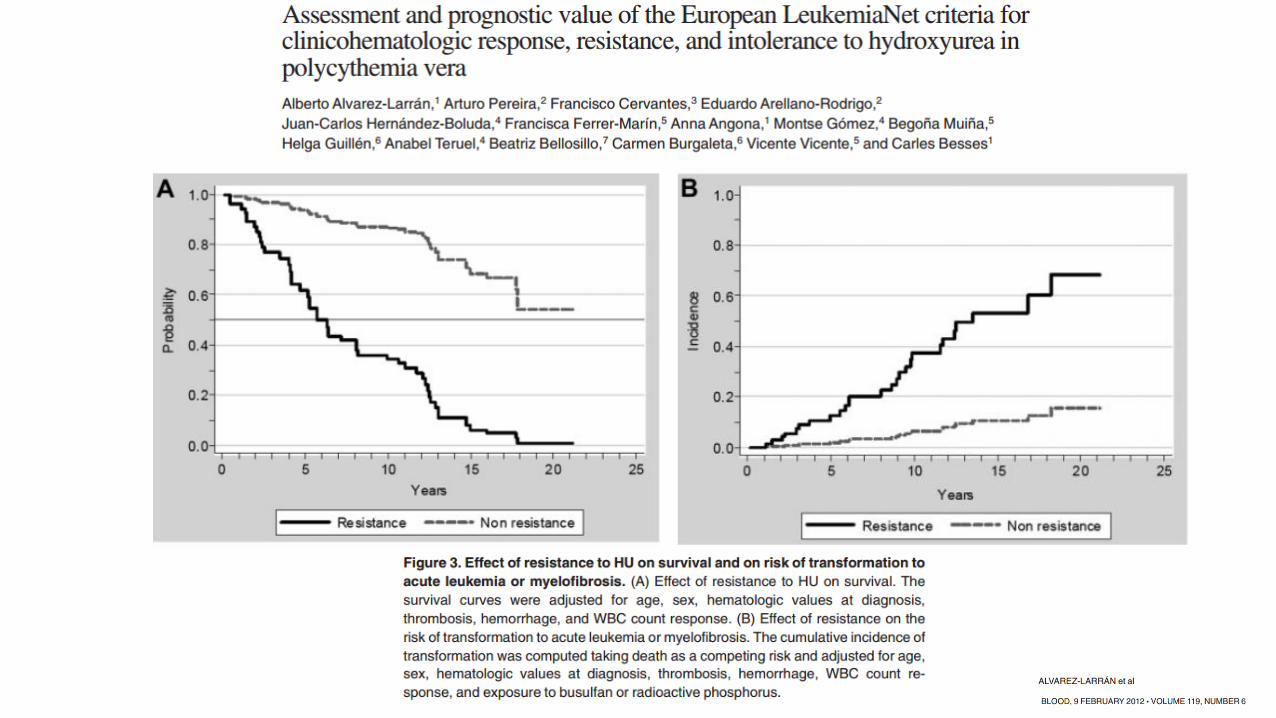
• Hydroxyurea-resistance leads to thrombosis, leukemiaprogression and shorter survival
• Ruxolitinib 10 mg bid is an effective and safe option tomanage hydroxyurea-resistant PV patients

Thank [email protected]

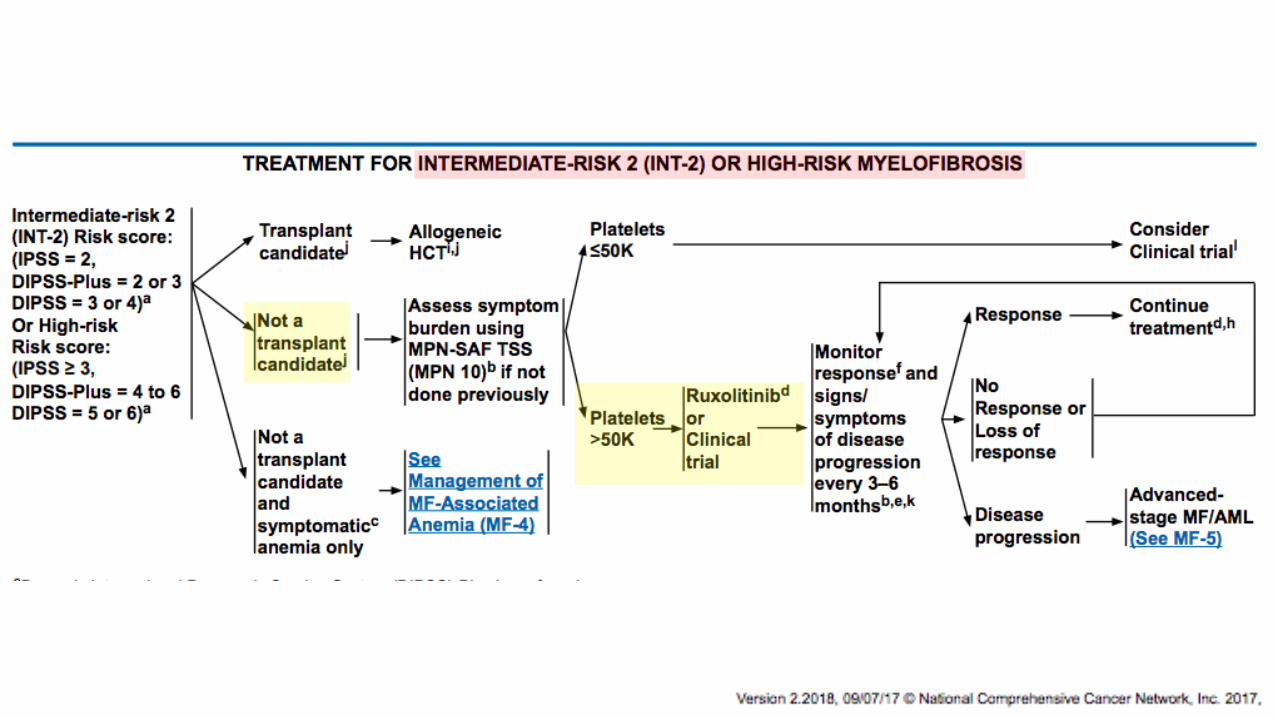
JAK2 Inhibitors in Myelofibrosis

Myelofibrosis
•About the disease
• It can be insidious
• It kills people
• It’s vicious and unforgiving
• It’s orphan

Cervantes F, et al. Blood, 2009
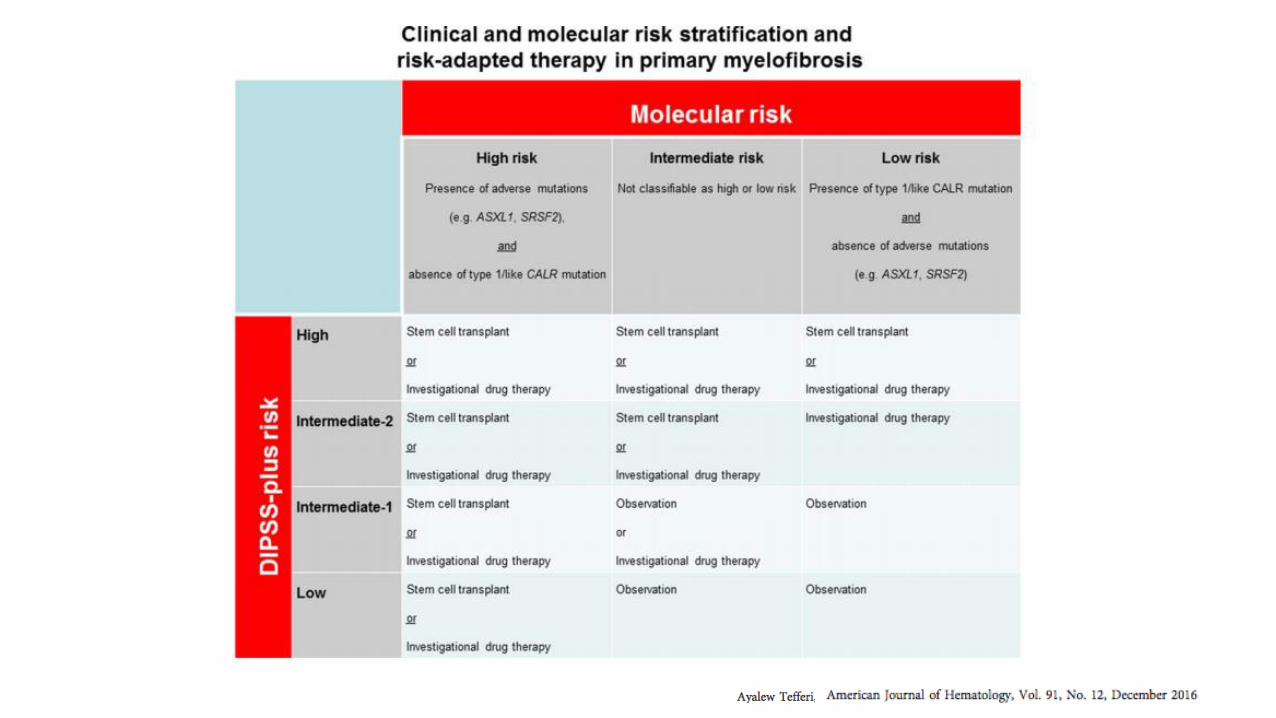
Primary Myelofibrosis – IPSS

”High-Risk” vs ”Low-Hisk” Mutations Profile


• Spleen reduction
• Can induce / aggravate cytopenias
• Overall response - 40% / Medians duration - 13,2 months
• After first year, 80% will need to chance to another therapy
• Skin and mucosa ulcers not uncommon
Hydroxiurea
Martinez-Trillos A, et al. Ann Hematol 2010Cervantes F, et al. Blood 2014
Erythopoetin in PMF
• Studies are small - no larger prospective study than N=20
• Response Criteria used are not uniform
• Positive factors for response:
• Lack of transfusion dependency
• S-Epolevel < 125 U/L
• rHuEPO dose: 30.000 U/week
Birgegard G. Best Pr Res Cl Hematol, 2014

Danazol in PMF
• Studies are small
• Response Criteria used are not uniform
• Response in 40% or more patients (worse if transfusion dependent)
• Time to response: 3 – 6 months
• Toxixity
• Mild
• Dose dependent
Birgegard G. Best Pr Res Cl Hematol, 2014
Cervantes F. et al Ann Hematol 201550 patientsIWGMRT criteriaResponse: 30%

Thalidomide in PMF
• First studies: High doses – High drop out - intolerance
• Low Doses plus Predinisone
• Response in 40% patients
• Time to response – less than 12 weeks
• Duration of response – varies widely
• However, notable toxicity even with low doses
Birgegard G. Best Pr Res Cl Hematol, 2014
Lenalidomide and Pomalidomide:Lower side-efectsLower response rates



Median follow-up: 58 monthsMedian treatment duration: 39 months (range: 6-107)Forty-five pts (72.6%) discontinued
55.6% due to resistance 44.4% due to intolerance
Ianotto JC, et al. ASH 2017

BMT and MF
• It’s the only curative therapy - 30 to 60%
• Primary graft failure: 10 to 20%
• Secondary graft failure: plus 10%
• 100-day mortality: 10 to 30%
• Non-fatal relapses: 30% to 50%
• Long term overall survival: 30 to 70%
Gergis U, et al. Cl Lymp Myel Leuk, 2016

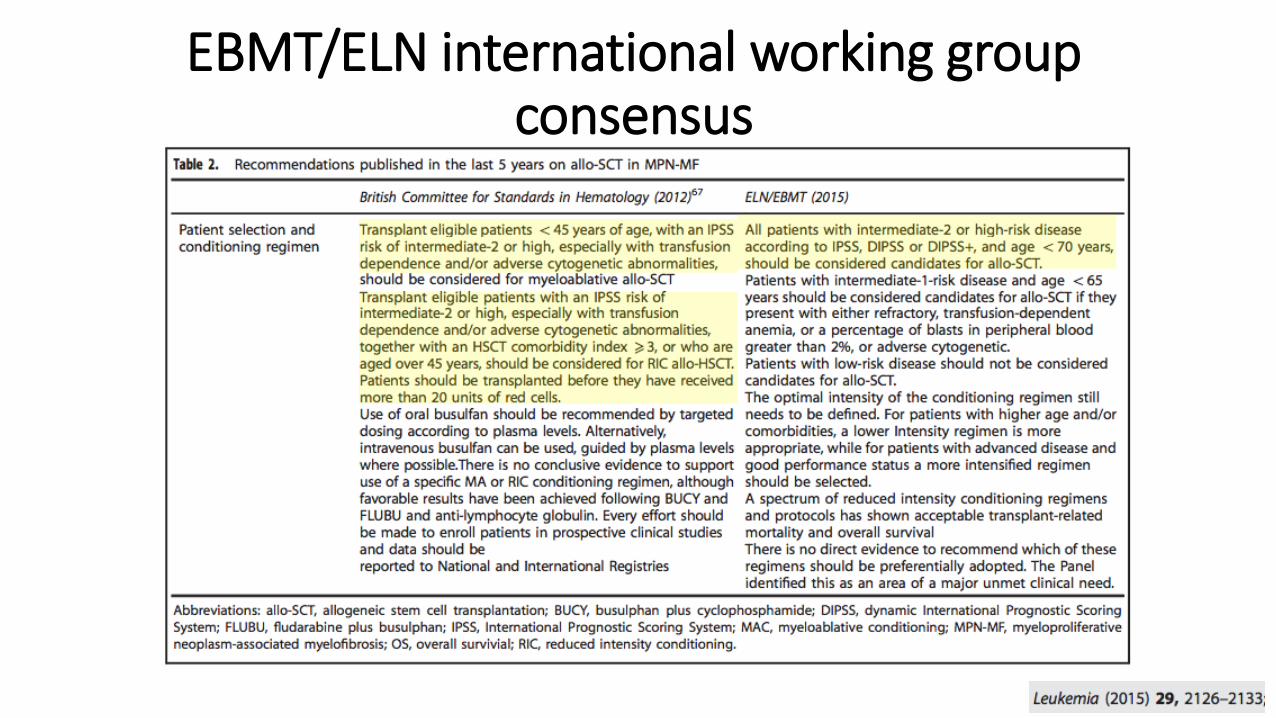
EBMT/ELN international working group consensus

Pacientes com MF
Primária ou
Secundária
(N=309)
Randomizados
1:1
Ruxolitinibe (oral)
15 mg 2x/dia ou
20 mg 2x/dia
Melhor terapia
disponível
Pacientes com MF
Primária ou
Secundária
(N=219)
Objetivo Primário COMFORT-I: % pacientes ≥ 35% de redução do volume do baço até a semana 24*
Verstovsek et al., NEJM, 2012; 366(9):799-807Harrison et al., NEJM, 2012; 366(9):787-98
*Conforme medido por RNM (ou TC em pacientes aplicáveis)
Placebo (oral)
2x/dia
Randomizados
2:1
Ruxolitinibe (oral)
15 mg 2x/dia ou
20 mg 2x/dia
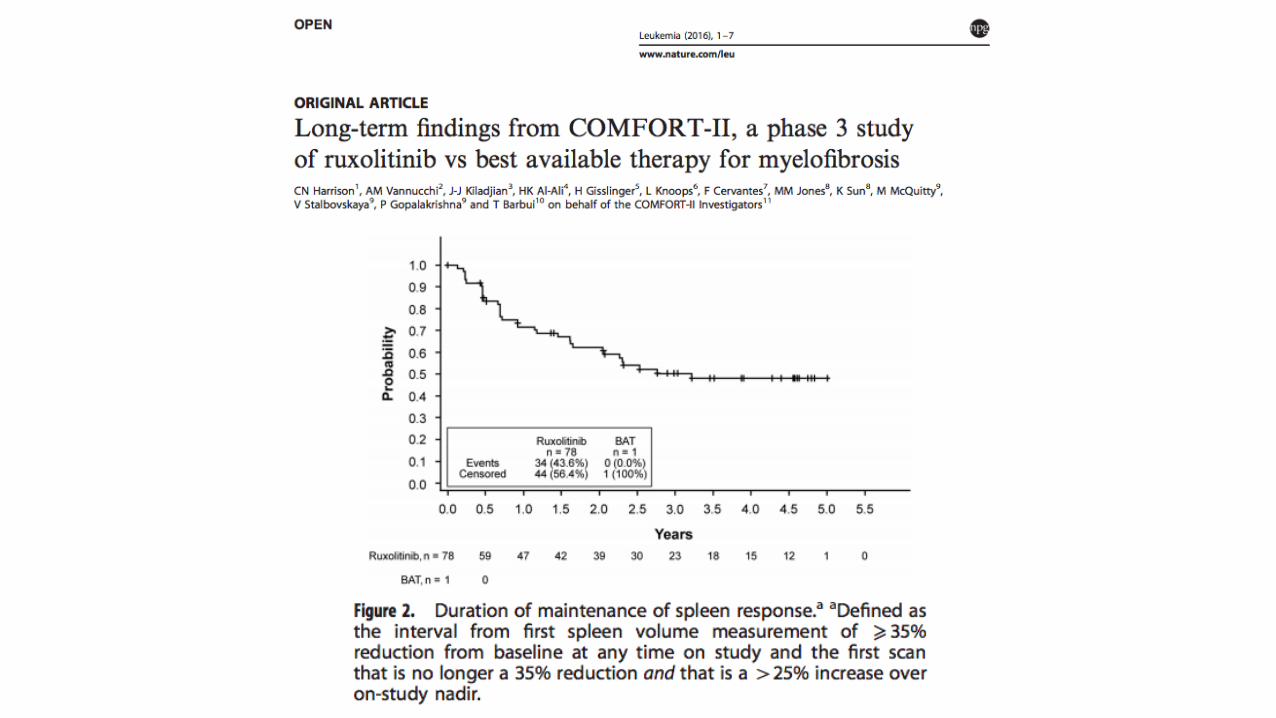
COMFORT-II (Europa)
Objetivo Primário COMFORT-II: % pacientes ≥ 35% de redução do volume do baço até a semana 48*
Ruxolitinibe em MF - Estudos de Fase IIICOMFORT-I (EUA,Canadá, Austrália)



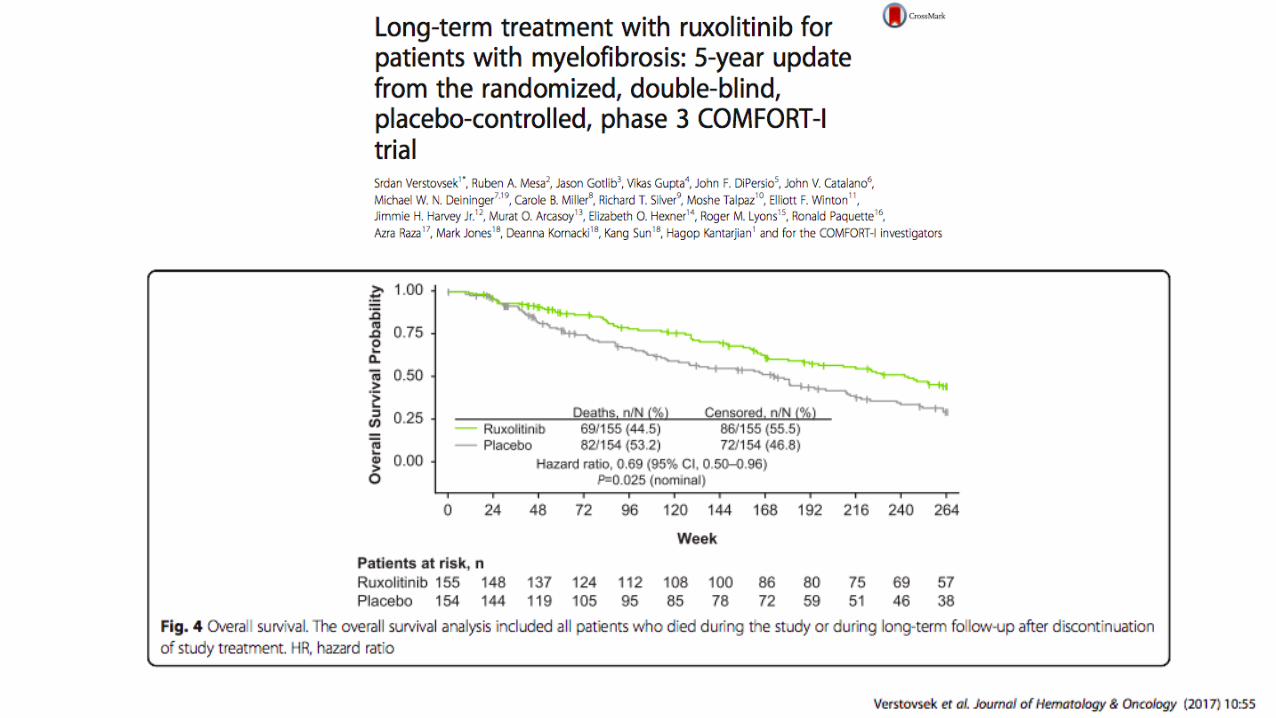



Pooled analysis – COMFORT I e II
Verstovsek et al. ASH 2016. Session 634. Abstract 3110.

Pooled analysis – COMFORT I e II
Verstovsek et al. ASH 2016. Session 634. Abstract 3110.

Pooled analysis – COMFORT I e II
Verstovsek et al. ASH 2016. Session 634. Abstract 3110.
OVERAL SURVIVAL corrected for crossover with the RPSFT model

OVERALL SURVIVAL CORRECTED BY CENSORING AT CROSSOVER
Pooled analysis – COMFORT I e II
Verstovsek et al. ASH 2016. Session 634. Abstract 3110.
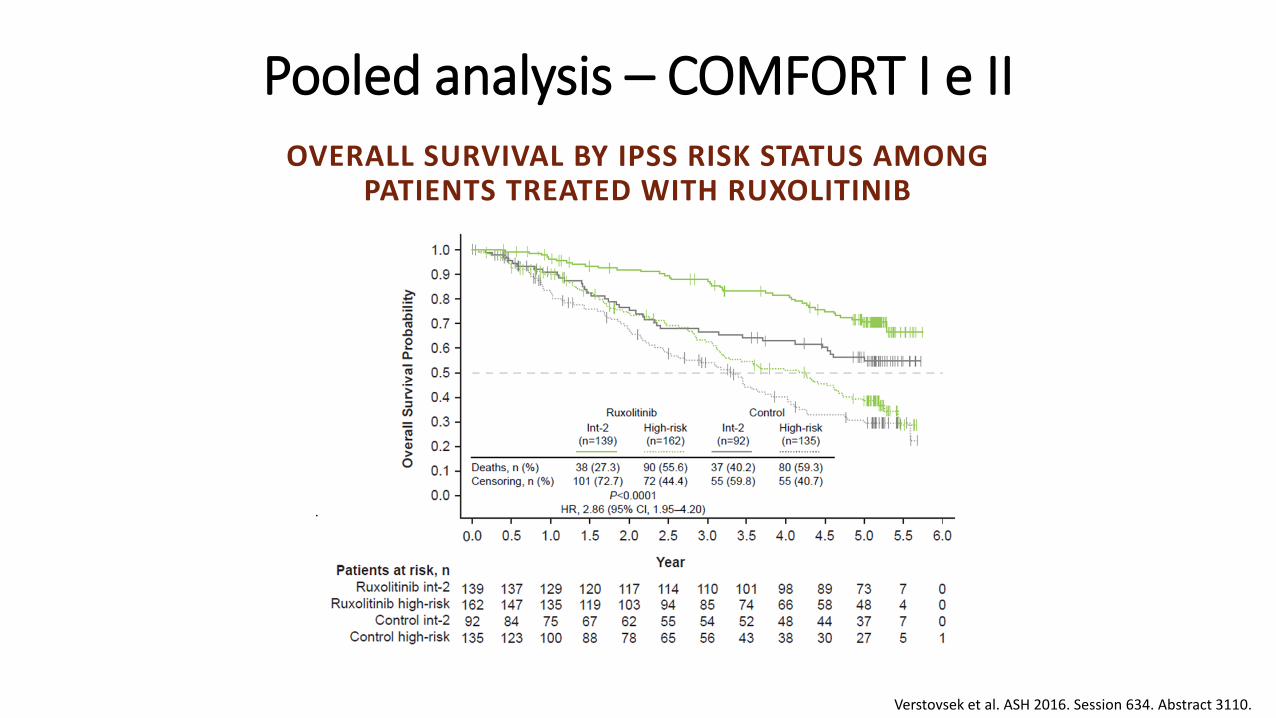
OVERALL SURVIVAL BY IPSS RISK STATUS AMONG PATIENTS TREATED WITH RUXOLITINIB
Pooled analysis – COMFORT I e II
Verstovsek et al. ASH 2016. Session 634. Abstract 3110.

Molecular score and Ruxolitinib response – COMFORT II
Guglielmelli P, et al. Blood, 2014

Ruben A. Mesa et al. Blood 2012;120:1733
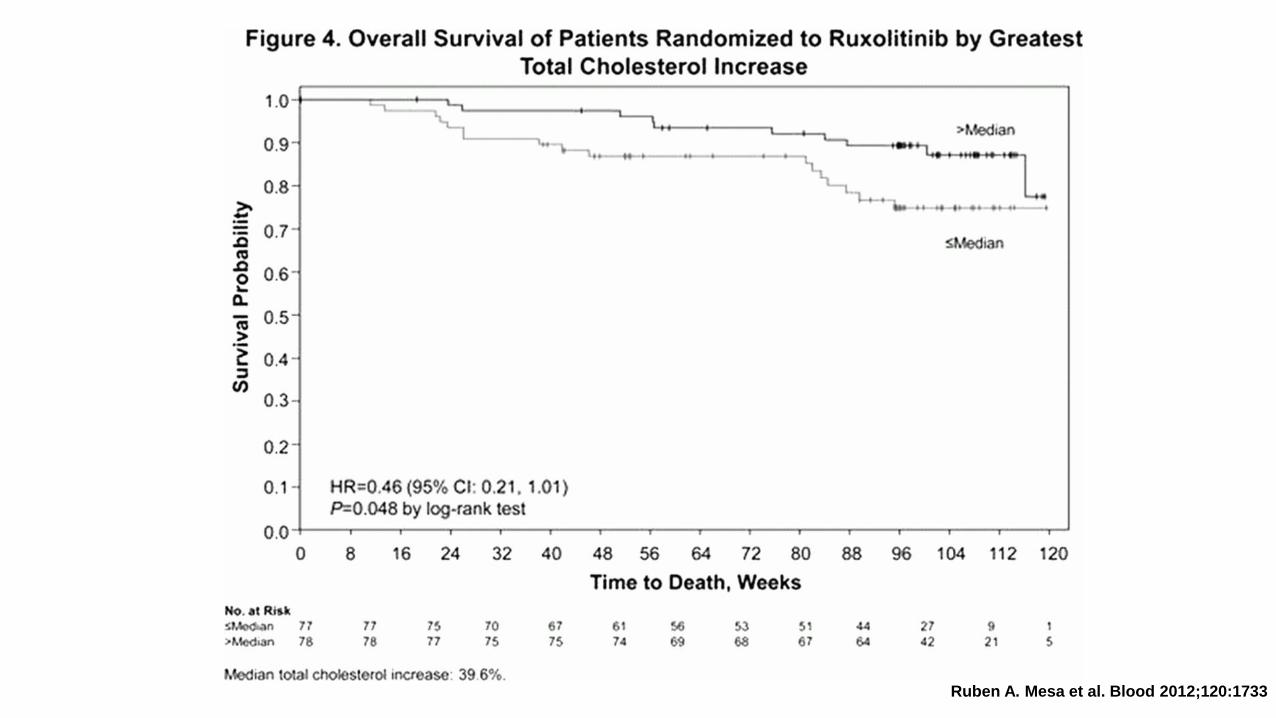
Ruben A. Mesa et al. Blood 2012;120:1733

Ruben A. Mesa et al. Blood 2012;120:1733

COMFORT I - 3 Year Update
Mean Platelet Count and Hemoglobin Level Over Time
Platelet Count Hemoglobin
85
90
95
100
105
110
115
0 12 24 36 48 60 72 84 96 108 120 132 144
Weeks
Mean H
em
oglo
bin
(g/L
)
120
170
220
270
320
0 12 24 36 48 60 72 84 96 108 120 132 144
Weeks
Mean
Pla
tele
ts (
x10
9/L
)
128 82PBO
144 136 112 107 100 88RUX
Number of patients
151
155
112 37
143 124 110 104 94 79
132 83
145 136 113 107 100 88
151
155
113 37
143 124 110 104 94 79
Number of patients
370Ruxolitinib Placebo Ruxolitinib Placebo



EHA 2017

Adverse Events – COMFORT II
Harrisson C, et al. Leukemia, 2016. doi: 10.1038/leu.2016.148

Tavares RS et al. ASH 2015 #Abs 2799
Adverse events - JUMP trial

COMFORT I/II trials - Caveats
• Overall survival – secondary objective
• Low number of patients – rare disease
• No Low risk / Intermediate 1 IPSS stage were included
• Crossover was allowed for ethical reasons – compromised overall
survival analysis
• Median overall survival of ruxolitinib arm has not been reached yet
94
Other JAK2 Inhibitors
• Fedratinib – some cases of Wernick’s encephalopaty discontinued 2015
• Pacritinib – some cases with major cardiovascular complications – temporally
hold in 2016. Nowadays new explorations are being conducted
• Momelotinib – not inferior in spleen reduction, better in transfusion-
independence, worst for alleviate symptoms – discontinued 2017
Bose P & Verstovsek S, Blood, 2017

Ruxolitinib is recommended for:
Symptomatic or severe splenomegalyIntermediate-2 / high-risk - strong recommendationIntermediate-1-risk not responsive / intolerant to HU or IFN - weak recommendationIntermediate-1-risk not previously treated - weak recommendation
Disease-related symptoms- strong recommendation(MPN10 score 444 / refractory severe itching (score 46) / weight loss / unexplained fever)
Improving survival - not recommended uniquely for survival benefit - weak recommendation


Thank [email protected]





























