Embed Size (px)
Citation preview
Department of Neonatology, Astrid Lindgren Children’s Hospital
Simon Carlquist
Study Programme in Medicine, KI
Degree project 30 credits
Spring 2012
Neonatal Use of Inhaled Nitric Oxide
a registry study of treatment indications, extent and outcomes
at Astrid Lindgren Children’s Hospital
Final version
Author: Simon Carlquist
Supervisor: Baldvin Jónsson
Coordinator: Isis Amer-Wåhlin

Inhalerad kväveoxid till nyfödda – en registerstudie av behandlingens indikationer,
omfattning och utfall vid Astrid Lindgrens Barnsjukhus.
Bakgrund: Inhalerad kväveoxid är en lungselektiv kärlvidgande behandling vid andningssvikt
orsakad av pulmonell hypertension hos nyfödda. Den har även studerats som profylax mot
bronkopulmonell dysplasi, en kronisk lungfunktionsnedsättning vanlig bland för tidigt födda
barn. Evidensen till stöd för denna kostsamma behandling är bristfällig för spädbarn födda
före 34 veckor. Trots detta används behandlingen frekvent på nyfödda i alla gestationsåldrar.
Syfte: Att undersöka om kväveoxidbehandling av nyfödda på Astrid Lindgrens Barnsjukhus,
Solna, Sverige, skett i enlighet med tillgänglig evidens, och att presentera deskriptiv statistik
rörande vissa behandlings- och patientrelaterade variabler. Ett sekundärt syfte var att
identifiera signifikanta skillnader i dessa variabler mellan barn födda före och efter 34 veckor. Material och Metoder: Alla nyfödda som behandlades med inhalerad kväveoxid på
neonatalintensivvårdsavdelningen vid nämnda sjukhus mellan 2006 och 2010 inkluderades.
Data rörande demografi, diagnostik, behandlingen i sig samt dess utfall samlades in från
patientjournaler och fördes in i ett web-baserat register. Resultat: 96 nyfödda behandlades
med inhalerad kväveoxid. 50% var födda före vecka 34. Denna åldersgrupp behandlades
under signifikant längre tid, samt stod för nära 75% av alla behandlingstimmar. Majoriteten
behandlades för hypoxemisk andningssvikt, och 2% fick behandling i profylaktiskt syfte.
Allvarliga biverkningar var sällsynta. Slutsats: Inhalerad kväveoxid användes inte i enlighet
med tillgänglig evidens. Behandlingsrutinerna bör möjligen ses över.
Neonatal use of inhaled nitric oxide – a registry study of treatment indications, extent
and outcomes at Astrid Lindgren Children’s Hospital.
Introduction: Inhaled nitric oxide is a selective pulmonary vasodilator, used to resolve
respiratory failure complicated by persistent pulmonary hypertension in newborns. It has also
been suggested as a prophylaxis to prevent bronchopulmonary dysplasia, a long-term
respiratory disability associated with preterm birth. Evidence supporting this expensive
therapy is limited in infants born before 34 weeks, but the therapy remains frequently used in
newborns of all gestational ages. Aims: To determine whether neonatal use of inhaled nitric
oxide at Astrid Lindgren Children’s Hospital, Solna, Sweden, has been consistent with
available evidence, and to present descriptive statistics on selected treatment- and patient-
related variables. A secondary aim was to detect significant differences in these parameters
between infants born before and after 34 weeks of gestation. Material and Methods: All
newborns who received inhaled nitric oxide therapy at the neonatal intensive care unit at said
hospital between 2006 and 2010 were included. Information on demographics, diagnostics,
treatment variables and outcomes was gathered from patient data records and submitted to a
web-based registry. Results: 96 infants received inhaled nitric oxide therapy. 50% were born
before 34 weeks. This group also had a significantly longer duration of therapy, and
accounted for nearly 75% percent of therapy hours. The majority had hypoxemic respiratory
failure, and 2% were treated prophylactically. Adverse effects were rare. Conclusions:
Inhaled nitric oxide was not used in an evidence-based manner. Therapy practices should
perhaps be revised.
Keywords: “Nitric oxide”, “Infant, newborn”, “Administration, inhalation”, “Evidence-based
medicine”. “Persistent pulmonary hypertension of the newborn”, “Bronchopulmonary
dysplasia”
Abbreviations
ALCH Astrid Lindgren Children’s Hospital
BPD Bronchopulmonary dysplasia
CDH Congenital diaphragmatic hernia
CMV Conventional mechanical ventilation
CPAP Continuous positive airway pressure
FiO2 Fraction inspired O2
GA<34w Gestational age < 34 weeks (born before 34 completed weeks)
GA≥34w Gestational age ≥ 34 weeks (born after 34 completed weeks)
HFOV High-frequency oscillatory ventilation
iNO Inhaled nitric oxide
NICU Neonatal intensive care unit
OI Oxygenation index
PICU Pediatric intensive care unit
PMA Post-menstrual age (gestational age at birth + post-natal age)
PPHN Persistent pulmonary hypertension of the newborn
PVR Pulmonary vascular resistance
RCT Randomised controlled trial
RDS Respiratory distress syndrome
SVR Systemic vascular resistance

Table of contents
1. Introduction .............................................................................................................. 1
1.1 Brief overview ................................................................................................................ 1
1.2 Persistent pulmonary hypertension of the newborn .................................................. 1
1.2.1 Overview and demographics ................................................................................... 1
1.2.2 Circulatory and pulmonary physiology before and after birth ................................. 1
1.2.3 Causal factors ........................................................................................................... 2
1.2.4 Diagnosis and treatment strategies .......................................................................... 3
1.3 Bronchopulmonary dysplasia ...................................................................................... 4
1.3.1 Overview and demographics ................................................................................... 4
1.3.2 Causal factors ........................................................................................................... 4
1.3.3 Diagnosis and treatment strategies .......................................................................... 6
1.4 Inhaled nitric oxide ....................................................................................................... 6
1.4.1 Overview.................................................................................................................. 6
1.4.2 Mechanism of pulmonary vasodilation .................................................................... 7
1.4.3 Pulmonary selectivity of inhaled NO ....................................................................... 7
1.4.4 Toxic and adverse effects of iNO ............................................................................ 8
1.4.5 iNO administration, economy and indications......................................................... 9
1.5 Evidence base for neonatal iNO therapy .................................................................... 9
1.5.1 Terminology ............................................................................................................ 9
1.5.2 Evidence for iNO therapy in term/near term newborns ........................................... 9
1.5.3 Evidence for iNO therapy in preterm newborns .................................................... 10
1.7 Motive for this study ................................................................................................... 11
2. Aims ......................................................................................................................... 12
2.1 Primary aim ................................................................................................................. 12
2.2 Secondary aims ............................................................................................................ 12
3. Material and methods ............................................................................................ 13
3.1 Study design and setting ............................................................................................. 13
3.1.1 Neonatal care at Astrid Lindgren Children’s Hospital .......................................... 13
3.1.2 The iNOcare registry ............................................................................................. 13
3.2 Study population ......................................................................................................... 14
3.2.1 Inclusion and exclusion criteria ............................................................................. 14
3.2.2 Identifying eligible infants ..................................................................................... 14
3.3 Data collection ............................................................................................................. 14
3.4 Statistical analysis ....................................................................................................... 15

3.5 Databases and search strategy ................................................................................... 15
3.6 Ethical considerations ................................................................................................. 16
4. Results ..................................................................................................................... 18
4.1 Patient demographics ................................................................................................. 18
4.2 Pre-treatment variables .............................................................................................. 18
4.2.1 Diagnostics and indication for iNO therapy .......................................................... 18
4.2.2 Treatments prior to iNO therapy ............................................................................ 20
4.2.3 Baseline clinical data ............................................................................................. 20
4.3 iNO therapy ................................................................................................................. 20
4.3.1 Initiation, duration and dosing ............................................................................... 20
4.3.2 Concomitant therapies ........................................................................................... 21
4.4 Outcomes...................................................................................................................... 22
4.4.1 Initial response gas exchange ................................................................................ 22
4.4.2 Survival .................................................................................................................. 22
4.4.3 Bronchopulmonary dysplasia ................................................................................ 22
4.4.4 Final cranial ultrasound ......................................................................................... 23
4.4.5 Other adverse events .............................................................................................. 23
5. Discussion................................................................................................................ 24
5.1 Major findings ............................................................................................................. 24
5.2 Comments on therapy in preterm infants ................................................................. 24
5.3 Comments on therapy in term/near term infants .................................................... 25
5.4 Other comments .......................................................................................................... 26
5.5 Outcomes...................................................................................................................... 26
5.6 Limitations ................................................................................................................... 27
6. Conclusions ............................................................................................................. 28
7. Acknowledgements ................................................................................................ 30
8. References ............................................................................................................... 31
Appendix 1 .................................................................................................................. 35
Overview of data parameters submitted to the iNOcare registry. ................................... 35

1
1. Introduction
1.1 Brief overview
Inhaled nitric oxide (iNO) is an advanced and expensive vasodilating therapy for
newborn infants in whom the pulmonary circulation fails to adapt to the extra-uterine
environment after birth; a condition known as persistent pulmonary hypertension of
the newborn (PPHN). In addition, iNO has been studied as a prophylactic drug to
prevent development of bronchopulmonary dysplasia (BPD), a long-term respiratory
disability strongly associated with preterm birth. Evidence supports iNO therapy in
infants born at or near term but not in the preterm population. Yet iNO is frequently
used in both term and preterm infants at neonatal intensive care units across Europe
and in the U.S. This study aims to investigate to what extent iNO use at Astrid
Lindgren Children’s Hospital in Solna, Sweden, has been consistent with available
evidence.
1.2 Persistent pulmonary hypertension of the newborn
1.2.1 Overview and demographics
Respiratory failure, defined as an inability of the respiratory system to maintain
adequate gas exchange, accounts for one third of all neonatal mortality. 10% of cases
are either caused – or complicated – by a syndrome known as persistent pulmonary
hypertension of the newborn (PPHN) [1], a potentially life-threatening condition in
which pulmonary vascular resistance (PVR) remains higher than systemic vascular
resistance (SVR) in the newborn period. This results in hypoxia that often is
unresponsive to maximum oxygen administration and ventilation, i.e. hypoxemic
respiratory failure [1–3]. PPHN occurs in approximately one to two of 1000 live
births and is most common in full term or post term infants [4]. It is associated with
significant neurodevelopmental and respiratory morbidity later in childhood, and
carries a 5-10% short-term mortality even with modern treatment [1].
1.2.2 Circulatory and pulmonary physiology before and after birth
A now obsolete synonym for PPHN is persistent fetal circulation. The fetal circulation
is characterised by a high PVR since the lungs are collapsed and not ventilated, and a

2
low SVR since the placenta acts as a volume reservoir. This resistance gradient,
where PVR>SVR, causes a functional right-to-left shunting of blood from the
pulmonary artery to the aorta through the open ductus arteriosus [5]. Thereby, the
high-resistance pulmonary circulation is bypassed and blood from the right ventricle
enters the low resistance systemic circulation to be oxygenated by the placenta [5].
Immediately following birth and the infant’s first breath of air, PVR normally
decreases rapidly, so that PVR<SVR. This is mediated by mechanical distension of
pulmonary vessels as the lungs fill with air, and by endogenous chemical mediators of
vasodilation such as increased oxygen tension, prostaglandins and nitric oxide [1,6].
At the same time, SVR increases as the placental circulation is discontinued [3]. This
set of events causes a tenfold increase in pulmonary blood flow [1], and the
subsequent rise in oxygen tension is believed to contribute to the spontaneous closing
of the ductus arteriosus and foramen ovale, which normally occurs within two days
after birth [5]. If for some reason the reduction of PVR after birth is inadequate, or if a
reduced PVR should return to suprasystemic levels, a resistance gradient analogous to
that seen in the fetal circulation would cause a similar right-to-left shunt of blood
across the open ductus arteriosus. Thereby, deoxygenated blood would continue to
bypass the pulmonary circulation to some degree, but without being oxygenated by
the now disconnected placenta. This is essentially the case in PPHN [1–3].
1.2.3 Causal factors
PPHN is usually classified as either primary or secondary based on its etiology. In
general, primary PPHN is considered a result of long-term dysregulation of fetal
pulmonary development resulting in abnormal muscularisation of alveolar arteries
and/or pulmonary hypoplasia (i.e. underdeveloped lung parenchyme, not to be
confused with bronchopulmonary dysplasia which is covered in section 1.3) [4].
Congenital diaphragmatic hernia (CDH; abdominal organs protruding into the thorax,
mechanically obstructing pulmonary growth), oligohydramnios (lack of amniotic
fluid), long-standing fetal hypoxia and pharmacological factors are some suggested
causal factors [1,2]. For example, maternal intake of selective serotonin reuptake
inhibitors (SSRIs) [7], or non-steroid anti-inflammatory drugs (NSAIDs) in late
pregnancy is associated with PPHN, as is also maternal diabetes and obesity [4].

3
By contrast, secondary PPHN, being the more common form, is the result of hypoxic
pulmonary vasoconstriction due to acidemia and hypoxia caused by acute perinatal
events [4]. Hypoxic pulmonary vasoconstriction is a normal physiological mechanism
by which vessels in poorly ventilated parts of the healthy lung constricts in response
to low oxygen pressure, thereby rerouting blood flow to better-ventilated parts,
optimising oxygenation [8]. In secondary PPHN, however, this mechanism becomes
the culprit as it results in a downward spiral of hypoxia and further vasoconstriction.
The acute perinatal events causing secondary PPHN include meconium aspiration
syndrome (pre-natal aspiration of amniotic fluid stained with fetal excrement),
respiratory distress syndrome (RDS; inadequate pulmonary compliance due to lack or
dysfunction of surfactant proteins), perinatal asphyxia, and congenital infections [1,2].
The onset of PPHN usually occurs within 12 hours from birth [3].
A note on terminology: the iNOcare registry, the data of which this study relies on,
defines PPHN caused by congenital diaphragmatic hernia and pulmonary hypoplasia
as secondary PPHN (even though they both belong to the long-term type of causality,
rather than the acute vasoconstriction type) since both are distinct conditions. The
registry further considers any PPHN case of unknown etiology to be primary, or
idiopathic, even though the cause might be any of the secondary ones listed above.
This report will use the same definition as the registry does in the following text.
1.2.4 Diagnosis and treatment strategies
PPHN is a key differential diagnosis in any newborn with persisting cyanosis despite
optimal ventilation and oxygen administration [3]. The latter is usually measured as
fraction of inspired air (FiO2), where FiO2 0.21 is equivalent to room air (21% O2),
and FiO2 1.0 represents 100% O2. A measure of respiratory failure severity that takes
FiO2 and the amount of respiratory support given into account is the oxygenation
index (OI), explained in Figure 1.
Figure 1. Calculation of the oxygenation index as a measure of respiratory failure severity.
FiO2=fraction inspired oxygen (0.21-1.0), MAP=mean airway pressure (cm H2O), PaO2=arterial partial
pressure of oxygen (mmHg). Illustration: the author, modified from [9].

4
Echocardiography with colour doppler is the preferred diagnostic modality when
PPHN is suspected, since it can detect elevated or suprasystemic pulmonary artery
pressures, tricuspid valve insufficiencies, and right-to-left shunting of blood across
the ductus arteriosus and/or foramen ovale [3], all of which are considered to be
evidence of pulmonary hypertension. Echocardiography can also rule other causes of
cyanosis such as structural heart disease or ventricular dysfunction [1,3].
Selective pulmonary vasodilation using inhaled nitric oxide, high levels of inspired
oxygen, surfactant instillation, hemodynamic support and lung volume recruitment
through high frequency oscillatory ventilation (HFOV) or continuous positive airway
pressure (CPAP) are key components of the modern therapeutic approach to PPHN
[1]. A last resort in cases of refractory respiratory failure in term/near term newborns
is extracorporeal membrane oxygenation (ECMO). Although this technically
advanced therapy buys time to await spontaneous PVR decline or further lung
maturation, and has an overall survival rate of 85% in cases of neonatal respiratory
support, it is a highly invasive, risk-associated and resource-consuming procedure
available only at highly specialised centres [9].
1.3 Bronchopulmonary dysplasia
1.3.1 Overview and demographics
Bronchopulmonary dysplasia (BPD), also known as chronic lung disease of
prematurity (CLD), can be described as a chronic disruption of growth and maturation
of alveoli and alveolar capillaries, causing a prolonged oxygen and/or ventilator
dependency in the newborn period, sometimes for several months or years [10]. It
occurs mainly in preterm infants. Around one third of all newborns with birth weight
<1000g develop BPD to some degree, and conversely, 97% of all BPD cases occur in
infants with birth weight <1250g [11]. Similarly to PPHN, BPD also contributes to
considerable neurodevelopmental morbidity in later childhood [11].
1.3.2 Causal factors
BPD was first described in 1967, as the result of oxygen toxicity and mechanically
induced lung injury (volutrauma) following aggressive mechanical ventilation in

5
mildly preterm infants suffering from RDS [12]. Pathological findings included
scattered severe airway fibrosis, epithelial metaplasia and smooth muscle hypertrophy
as well as hyperinflation and “white-outs” on chest radiographs [13]. Since the advent
of antenatal corticosteroids and exogenous surfactant therapy in the 1980’s and 90’s,
which allowed for much more gentle ventilation strategies and greater survival rates
in RDS therapy, and thereby contributed to the marked reduction of the lowest viable
gestational age, BPD has evolved from its classical form. From previously affecting
mildly preterm infants, it is now a “post-surfactant”, “new BPD” [10] featuring a
different pathology, and affecting primarily infants of lower gestational age and birth
weight than before.
Alveolar development occurs mainly during gestational weeks 32-36 [14].
Histological markers of “new BPD” include fewer-than-normal, large and immature
alveoli, dysmorphic capillaries and general mild fibrosis of alveolar septa [10,15].
Current pathophysiological models suggest that the “new BPD” is a product of an
arrested development of the distal airways at the stage of gestation in which the infant
is born [13]. The abrupt environmental change from intra- to extra-uterine life and a
subsequent complex interplay of oxidative stress, disrupted growth factor signalling,
inflammatory mechanisms, and genetic predisposition are suggested contributory
causal factors [14]. Contrary to “old BPD”, “new BPD” does not exclusively occur in
infants that have undergone aggressive mechanical ventilation. Instead, its main
predictors are low gestational age and low birth weight [16]. Figure 2 compares the
pathology of PPHN and BPD, although they are two completely separate conditions,
to give the reader a clearer understanding of their differences and similarities.

6
Figure 2. A schematic comparison of the pathogenesis behind secondary and primary PPHN and “old”
and “new” BPD. Note that PPHN is more common in term infants, and that BPD primarily occurs in
preterm infants, although exceptions occur. PPHN=Persistent pulmonary hypertension of the newborn,
PVR=pulmonary vascular resistance, BPD=bronchopulmonary dysplasia, RDS=respiratory distress
syndrome. *: For example abnormal muscularisation or pulmonary hypoplasia (not to be confused with
bronchopulmonary dysplasia). Illustration: the author.
1.3.3 Diagnosis and treatment strategies
Present diagnostic criteria for BPD are based on the infants need for supplemental
oxygen at specific cut-off ages; 36 weeks post-menstrual age (PMA=gestational age +
postnatal age) or 56 days post-natal age, for infants of gestational age <32 and >32
weeks, respectively [10]. Prophylactic and therapeutic approaches to BPD include
minimising the use of invasive ventilation modes, achieving optimal nutritional status
and preventing postnatal infections [13].
1.4 Inhaled nitric oxide
1.4.1 Overview
Nitric oxide (NO) is an endogenous paracrine signal substance, acting as a potent
vasodilator and regulator of basal vascular tone [17,18]. Apart from its vasodilatory
effects, NO plays multiple roles in many organ systems of the body, including platelet
inhibition, neural transmission, and the immune system [19,20]. NO is synthesised
from the precursor L-arginine [21] by several isoforms of the enzyme NO-synthase,

7
an enzyme expressed both in airway epithelium and vascular endothelium, as well as
various other cell types throughout the body [20].
1.4.2 Mechanism of pulmonary vasodilation
Endogenous NO mediates pulmonary vasodilation through vascular smooth muscle
cell (SMC) relaxation. Due to its lipophilic characteristics, NO easily reaches SMCs
by diffusion, either from adjacent vascular endothelial cells or from the luminal side
of adjacent alveoli, into which NO travels by auto-inhalation from sites of synthesis in
the mucosa of the upper airways [20]. The target molecule of NO is the heme
component of soluble guanylyl cyclase, an enzyme present in SMCs [20]. By binding
with, and activating this enzyme, NO causes intracellular levels of cyclic guanosine
monophosphate (cGMP) to rise. cGMP in turn activates protein kinase G which
mediates SMC relaxation through changes in intracellular calcium levels and by
altering the sensitivity of the contractile system for calcium [20]. See Figure 3 for an
overview of NO routes and its mechanism of action.
1.4.3 Pulmonary selectivity of inhaled NO
Being a gas, NO is suitable for inhalation therapy. Its half-life in vivo is short (about 7
s) [20], partly due to its high affinity for heme; about 1500 times greater than that
between heme and carbon monoxide [22]. Endothelial-derived or inhaled NO does
not have to reach the circulation to exert its vasodilatory effect, and any NO that does
reach the bloodstream is metabolised or bound, either by heme (forming
methemoglobin) or as other rapidly forming metabolites [17,20], see Figure 3.
Thereby, inhaled NO (iNO) is a selective pulmonary vasodilator that reduces PVR
without affecting systemic blood pressure, as studies of pulmonary hypertension in
both animals and humans have confirmed [23,24].
Either administered as an exogenous inhalation or auto-inhaled from the upper
airways, most of the NO will by default end up in well-ventilated parts of the lung.
This causes local vasodilation and increased arterial blood flow where oxygen is most
abundant, at the expense of lung regions with less ventilation. This rerouting of
arterial blood flow optimises the overall ventilation/perfusion ratio and contributes to
the improved oxygenation seen with iNO therapy in cases of PPHN and/or respiratory
failure [20].

8
Figure 3. A. An overview of the routes of endogenous NO (1) from vascular endothelium (2), and
endogenous or exogenous NO from alveolar airspace (3) to its destination inside vascular smooth
muscle cells (4). (5) represent NO that reaches the bloodstream and is inactivated. B. Schematic
representation of the vasodilating mechanism of action of NO inside a vascular smooth muscle cell.
NO=nitric oxide, GTP=guanosine-triphosphate, cGMP=cyclic guanosine monophosphate.
Illustration: the author.
1.4.4 Toxic and adverse effects of iNO
One common adverse effect of iNO therapy is a rebound hypoxemia if therapy is
suspended too rapidly. A carefully monitored weaning process is recommended, until
the infant sustains adequate oxygenation with only 1 part per million (ppm) of iNO
and an FiO2 of <0.5 [4]. The platelet-inhibiting effect of NO rises concerns about its
potential to cause or worsen intracranial (intraventricular) hemorrhage, a common
complication of pre-term birth. A cranial ultrasound should therefore precede the
initiation of iNO therapy in infants at risk, to provide a baseline reference and to rule
out any on-going hemorrhagic event that could be worsened by the therapy.
Methemoglobin, the product of NO and hemoglobin, is unable to carry oxygen.
Methemoglobinemia is therefore a toxic condition that might severely hinder the O2
carrying capacity of the blood. A methemoglobinemia of <7% (of total hemoglobin)
is considered safe [4], and with standard dosing regimens, iNO therapy in newborns
rarely cause levels above this [25]. Being a free radical with an unpaired electron, NO
also rapidly reacts with oxygen to form toxic nitrous oxide (NO2) [20]. Clinical trials

9
have not demonstrated a serious risk to cause toxic damages by accumulation of NO2
using standard iNO dosing strategies [26,27].
1.4.5 iNO administration, economy and indications
iNO can be administered via conventional mechanical ventilation (CMV), HFOV,
CPAP, or inhaled separately by mask or nasal cannulae. Normal starting
concentration is 20 ppm [25]. A specialised iNO delivery and monitoring system
feeds the gas from large cylinders of 400 ppm concentration to the ventilation
equipment. This system allows for dose regulation in steps of 0.5 ppm and also
monitors the levels of NO2 present in inspired air. The cost of iNO administration is
calculated per hour regardless of dosing, at present 15000 SEK/h. However, the
manufacturer (INO Therapeutics) allows for expense limitation if therapy exceeds
96h for one patient (Dr Baldvin Jonsson, April 2012, personal communication). The
registered indication for neonatal iNO therapy in Sweden is hypoxemic respiratory
failure with clinical or echocardiographic signs of pulmonary hypertension in
newborn infants of GA≥34w [28]. Since a portion of infants with PPHN do not
achieve improved oxygenation with iNO therapy, it should be used exclusively at
centres with ECMO capabilities, since this is the final therapeutic option [4].
1.5 Evidence base for neonatal iNO therapy
1.5.1 Terminology
This report uses a cutoff gestational age (GA) of 34 completed weeks (34w) to define
infants as either preterm (GA<34w) or term/near term (GA≥34w). This terminology
differs from the ICD-10 definitions of preterm birth, which is set at <37 completed
weeks. Nonetheless, the 34 weeks cutoff has been used in most clinical trials of iNO
therapy, and is a pivotal part of its registered indication [28].
1.5.2 Evidence for iNO therapy in term/near term newborns
In early animal models of PPHN, iNO treatment lowered and sustained a reduced
PVR in the newborn period [29,30]. Subsequent human studies of iNO for PPHN in
infants born at GA≥34w demonstrated a significantly improved oxygenation without
lowering systemic vascular resistance or causing methemoglobinemia [31,32]. Since

10
then, several randomised placebo-controlled trials (RCTs) in this age group have
shown significant improvements in short-term oxygenation with iNO therapy, as well
as a significantly reduced need for ECMO, albeit not a reduced mortality [27,33,34].
Furthermore, no increased occurrence of severe adverse neurologic/hemorrhagic
events or methemoglobinemia were seen [27,33,35].
A recently updated Cochrane review of iNO therapy for respiratory failure in infants
born at GA≥34w confirmed the significantly reduced need for ECMO therapy, with a
number-needed-to-treat (NNT) of 5.3 [25]. Mortality rates remained unaffected by
iNO therapy vs. placebo in this analysis, potentially explained by the fact that no
critically ill infant in a control group would be allowed to die without an attempt to
reverse the course by initiating ECMO therapy [25]. However, long term follow-up of
neurodevelopmental disabilities revealed no difference between iNO and placebo
groups, and the Cochrane review thus concluded that in newborn infants born at
GA≥34w, suffering from hypoxemic respiratory failure unresponsive to other
treatment iNO therapy in starting doses of 20 ppm is consistent with current evidence
[25]. Today, iNO is the gold standard therapy for this indication. A notable exception
is the treatment of infants with congenital diaphragmatic hernia (CDH), a condition
often accompanied by pulmonary hypoplasia and a component of PPHN. iNO therapy
did not reduce the combined outcome of death or ECMO in an RCT performed in this
population, but instead significantly increased the need for ECMO alone [36].
1.5.3 Evidence for iNO therapy in preterm newborns
The rationale for iNO therapy in preterm newborns (GA<34w) differs slightly from
that in term/near term ones. Respiratory failure in the preterm group has a different
pathophysiology and higher mortality due to incomplete lung maturation. Although
components of PPHN occur in this age group as well, it is only part of a more
complicated causality [37]. However, laboratory studies have suggested that iNO
attenuates pulmonary oxidative injuries [38] and promotes alveolar and capillary
development in animal models of BPD [39]. iNO as a prophylaxis for this disease has
therefore been the focus of several RCTs, in addition to evaluating its efficacy to
resolve hypoxemic respiratory failure. Since preterm infants are not eligible for
ECMO therapy for primarily technical reasons, these trials have often used a
combined endpoint of “death or BPD at 36 weeks PMA”, or sometimes “survival

11
without BPD” (the inverse outcome) instead of the endpoint “death or ECMO” used
in term/near term infant trials [37]. The majority of these RCTs have been unable to
prove a reduced risk of death or BPD with iNO therapy [40–43]. This lack of effect
was confirmed in a large meta-analysis that also failed to prove any iNO therapy
effect on mortality alone, or on the incidence of adverse neurological events in any
direction [44]. One RCT that did find a significant effect on “death or BPD” initiated
iNO therapy at later postnatal age (>7 days) and in higher starting doses (20 ppm)
compared with other trials [45], and subgroup results from the meta-analysis by Askie
et al. [44] lend some support to this approach. Many authors therefore promote further
adequately powered trials to determine the efficacy of different dosing and timing
strategies of iNO therapy in preterm infants [44,46].
1.7 Motive for this study
Evidence supporting iNO therapy for PPHN in term/near term newborns (GA≥34w) is
considered solid [25]. However, a recent large meta-analysis and a Cochrane Library
review both concluded that iNO therapy in the preterm population (GA<34w),
whether used in rescue regimens for respiratory failure, or as a prophylactic strategy
to prevent BPD, cannot be supported by current evidence [37,44]. Despite this, iNO
therapy is frequently used “off-label”, i.e. in preterm infants of GA<34w, inconsistent
with its registered indication [28].
An American retrospective multi-centre study showed that of infants treated with iNO
between 2000 and 2008, the proportion born at GA<34w increased from 20% to 43%
in the nine-year period. The authors estimated that in 2008, the preterm population
accounted for 53.5% of all iNO used, measured in days. They also pointed out that
iNO use seemed to have shifted towards the “less recoverable preterm neonates” [47].
Similarly, preliminary results from the European iNOcare registry showed that 40%
of newborn infants treated with iNO between 2006 and 2007 were born at GA<34w
[48]. In light of these results, considering the lack of evidence for iNO therapy in the
preterm population [37,44] and the high cost of iNO administration, our opinion is
that an analysis and discussion of iNO therapy practices and outcomes locally at
Astrid Lindgren Children’s Hospital (ALCH) would be of great interest.

12
2. Aims
2.1 Primary aim
The primary aim of this study was to examine to what extent iNO use in the treatment
of respiratory conditions, at the neonatal intensive-care unit (NICU) at ALCH, during
2006-2010, was consistent with available evidence, i.e. “on-label”. Our intention was
to present descriptive statistics of selected clinical parameters such as patient
demographics, iNO therapy indications, therapy duration, dosing and clinical
outcomes. A hypothesis was that a large number of patients were treated outside
evidence based treatment recommendations.
2.2 Secondary aims
The secondary aim was to identify any significant differences regarding indication for
iNO treatment, the extent of treatment (dosing, duration etc.) or its outcomes (death,
need for ECMO, development of BPD etc.) for newborn infants of GA <34 weeks
compared to newborn infants of GA ≥34 weeks.

13
3. Material and methods
3.1 Study design and setting
This study was conducted as a retrospective, cross-sectional registry study at the
department of neonatology at Astrid Lindgren Children’s Hospital (ALCH) in Solna,
Sweden. Analyses were performed on clinical data related to neonatal iNO therapy
retrieved from the European Inhaled Nitric Oxide Registry, iNOcare.
3.1.1 Neonatal care at Astrid Lindgren Children’s Hospital
Three neonatal care units form the department of neonatology at ALCH. The units are
geographically situated at hospitals in Solna, Huddinge and Danderyd. The Solna and
Huddinge units have international Level-3 classification, i.e. they both provide full
neonatal intensive care, but with slight differences in profile. For example, extremely
preterm infants (GA<26 weeks) are cared for at the Solna unit exclusively. ECMO
therapy is available only at Solna, and therefore this is the only unit with prolonged
iNO therapy capabilities. Altogether, the department of neonatology at ALCH is the
largest neonatal care centre in the Nordic countries, accounting for about one fourth
of all neonatal care in Sweden with approximately 2600 infants admitted annually
[49]. ALCH is one of seven Swedish centres with experience in neonatal iNO therapy,
and both the neonatal intensive care unit (NICU) and pediatric intensive care unit
(PICU) provide it. This study focuses on iNO therapy in the NICU alone.
3.1.2 The iNOcare registry
This registry, operational since 2006, is a joint collaboration between seven neonatal
and pediatric centres in six European countries, one of which is the NICU at ALCH.
The main purposes of the registry is to monitor trends and routines in the clinical use
of iNO as well as its outcomes and potential adverse effects. It may also serve as a
hypothesis-generating knowledge base for future research on efficacy and safety of
iNO therapy [48]. Clinicians at the participating centres submit de-identified, patient-
and treatment-specific clinical information related to iNO therapy using a web-based
interface. The information is stored in a central repository (MedSciNet, Stockholm,
Sweden). Preliminary results from the registry, covering the years 2006-2007, have
been published on the European data set as a whole [48].

14
3.2 Study population
3.2.1 Inclusion and exclusion criteria
All newborn infants who were admitted to the NICU at ALCH in Solna, and
subsequently commenced on iNO therapy on any indication between January 1st 2006
and December 31st 2010 were included in this study. Second and third courses of iNO
therapy were recorded and treated as separate cases if therapy was initiated more than
24 hours after the previous course, since therapy indication, duration, dosing and
several other parameters might differ between courses in the same infant. Both infants
who survived until discharge or transfer, and infants who died while in the NICU (but
after initiation and/or termination of iNO therapy) were included. No exclusion
criteria were used, as the purpose of this study was to present descriptive statistics
regarding the iNO treated population in the NICU as a whole.
3.2.2 Identifying eligible infants
Upon commencing this degree project, data on iNO-treated infants born between
January 1st 2006 and December 31
st 2007 (n=24) had previously been submitted to the
iNOcare registry. The remaining infants (born between January 1st 2008 and
December 31st 2010) were identified in a hard-copy ledger of iNO therapy cases kept
by the NICU.
3.3 Data collection
Data on patient demographics such as gestational age and birth weight, initial
diagnosis, baseline clinical data such as gas exchange and ultrasound results, therapy
duration and dosing, other treatments before and during iNO therapy, initial gas
exchange response, adverse events and final outcomes were collected. Each included
infant’s patient record was scanned manually (in the hospitals patient record system
software TakeCare), from the time of admission to the NICU up until
discharge/transfer or death, to identify all relevant information before completing the
iNOcare form and submitting it electronically. Two important approximations were
used in the data collection procedure. First, the time of birth was in most cases
approximated as equal to the time of NICU admission, since the actual birth time
rarely was noted in the infants patient record. This information is usually found in the

15
mothers delivery record, which the ethical permission for this study did not include.
This approximation was considered justifiable, since the infants in the majority of
cases were admitted to the NICU immediately or shortly after birth. Second, for
infants born before 36 weeks of gestation, a 36 weeks PMA time was approximated to
exactly X weeks after birth, where X = 36 – (GA in weeks at birth). This
approximation was used since the iNOcare registry only notes completed gestational
weeks at birth, and not additional days. The calculated 36 weeks PMA point in time
could therefore in reality be as much as 36 weeks + 6 days PMA. An overview of all
parameters prompted by the iNOcare web-based form is presented in Appendix 1.
When information was missing or incomplete in a patient’s record, the corresponding
input field in the iNOcare form was either left empty (=missing data) or marked as
“unknown” where applicable. After completing data collection on all included infants,
tabular data was extracted as a Microsoft Excel file from the iNOcare web interface.
3.4 Statistical analysis
The analytical approach of this study was mainly descriptive. The intention was to
present numbers, medians and ranges of the recorded parameters as well as to test for
any significant differences in specific parameters between two gestational age groups;
infants born at <34 and ≥34 weeks. A null hypothesis was postulated, stating no
difference between the groups. The Mann-Whitney U test was used for continuous
variables, and the asymptotical 2-sided Chi-square test for categorical variables. A p-
value of <0.05 was considered significant. All analyses were performed by the author,
using IBM SPSS Statistics v.20 and Microsoft Excel 2011 v 14.1.3, both for
Macintosh.
3.5 Databases and search strategy
References for this report were found mainly through the databases PubMed, The
Cochrane Library and Web of Science. The following MeSH terms were used to
identify relevant citations: “Nitric oxide”, “Infant, newborn”, “Persistent fetal
circulation syndrome”, “Respiratory insufficiency” and “Bronchopulmonary
dysplasia”. Several non-MeSH terms were used in addition to these. Useful
publications were also identified in reference lists of review articles. An overview of
the search terms, limits used and results is found in Table 1.

16
Table 1. Example of search strategies using different databases.
Search Database Type Terms Citations
#1 PubMed M, F “Nitric oxide (MeSH)” AND (“Infant, newborn
(MeSH)” OR “neonat*”)
1840
#2 PubMed M, F ”Persistent fetal circulation syndrome (MeSH)” OR
”Respiratory insufficiency (MeSH)” OR ”Persistent
pulmonary hypertension” OR ”Respiratory failure”
59740
#3 PubMed C, L #1 AND #2. Limits: RCTs, meta-analyses, humans,
reviews, editorials, Swedish, English, published in last
10 years, link to full text provided.
106
#4 PubMed C, L #1 AND (“Bronchopulmonary dysplasia (MeSH)” OR
“Chronic lung disease”). Limits: RCTs, meta-analyses,
reviews, editorials, humans, Swedish, English, published
in last 10 years, link to full text provided
58
#5 WoS F “Nitric oxide” AND (“Infant” OR “Newborn”) 3725
#6 WoS F, L #5 AND (”Persistent pulmonary hypertension” OR
”respiratory failure” OR ”Bronchopulmonary dysplasia”
OR ”chronic lung disease”). Limits: Subject=pediatrics
or respiratory system, document types=article or review,
English, published in last 10 years.
408
#7 Coch F “Nitric oxide” AND “Infant” 8
M=MeSH, F=Free text, C=combined MeSH and free text searches, L=limits activated. PubMed
searches performed in “title/abstract” search fields. WoS=Web of Science, searches performed in the
“topic” search field. Coch=Cochrane Library, search performed in “title/abstract/keyword” search
field.
3.6 Ethical considerations
Due to its retrospective design, using pre-existing patient data, this study did not
involve any experimental therapeutic or diagnostic procedure of potential harm to the
included infants. No patient identifiers other than date and time of birth and/or NICU
admission were submitted to the iNOcare registry. All analyses were performed on
group level. There was thus no traceability of specific data to individual patients. In
the data collection procedure, we accessed individual patient data records without
prior written consent from parents and/or treating physicians. All included infants
were at the time of treatment in very poor condition, and in several cases they did not
survive until discharge. Our accessing these records could be regarded as a breach of
integrity not only of the patients, but in some way also of their parents and treating
physicians, which we at all times strived to keep in mind. Permission to access patient
data records was obtained from the head of the neonatology section in Solna, and the
student signed a confidentiality agreement before commencing data collection.

17
There was no personal benefit for the infants included in this study. However, being
part of a truly vulnerable patient group subjected to a debated therapy, our hope was
that they might one day appreciate our efforts to promote an evidence-based approach
to neonatal iNO therapy. In order to conduct this study as a degree project by a
medical student, a formal advice was requested from the Regional Ethical Review
Board of Stockholm, registration number 2012/149-31. The board declared no ethical
objections or reservations.

18
4. Results
4.1 Patient demographics
92 newborn infants received iNO therapy in the NICU at ALCH between January 1st
2006 and Dec 31st 2010. Three infants received two to three courses of therapy and
the actual number of therapy cases was therefore n=96. Table 2 shows an overview of
patient demographics and Figure 4 shows the number of infants treated per year and
gestational age.
Table 2. Patient demographics grouped by gestational age. Data shown as n (%), or median (range).
Gestational age group All ages
n=96
GA<34w
n=48
GA≥34w
n=48
p
Birth weight (kg) 1.83 (0.46-4.63) 0.99 (0.46-2.5) 3.14 (1.68-4.63) <0.01
Female/male 31/65 (32.3/67.7) 12/36 (25/75) 19/29 (39.6/60.4) 0.167
Gestational age at birth 33 (23-42) 26 (23-33) 38 (34-42) -
Figure 4. Number of infants treated with iNO during 2006-2010, grouped by gestational age.
4.2 Pre-treatment variables
4.2.1 Diagnostics and indication for iNO therapy
In 94/96 infants (97.9%), the indication for iNO therapy was hypoxemic respiratory
failure due to primary or secondary PPHN. Two infants (2.1%, all GA<34w) received
iNO exclusively as a prophylactic therapy to prevent BPD. Respiratory distress
syndrome (RDS) and meconium aspiration syndrome (MAS) were the most common
secondary PPHN etiologies in the preterm and term population, respectively. No
6 5 8
17 12
8 5
17
10
8
0
5
10
15
20
25
30
2006 2007 2008 2009 2010
Pati
en
ts, n
Year
48
48
0
20
40
60
80
100
2006-2010
GA≥34w
GA<34w
19
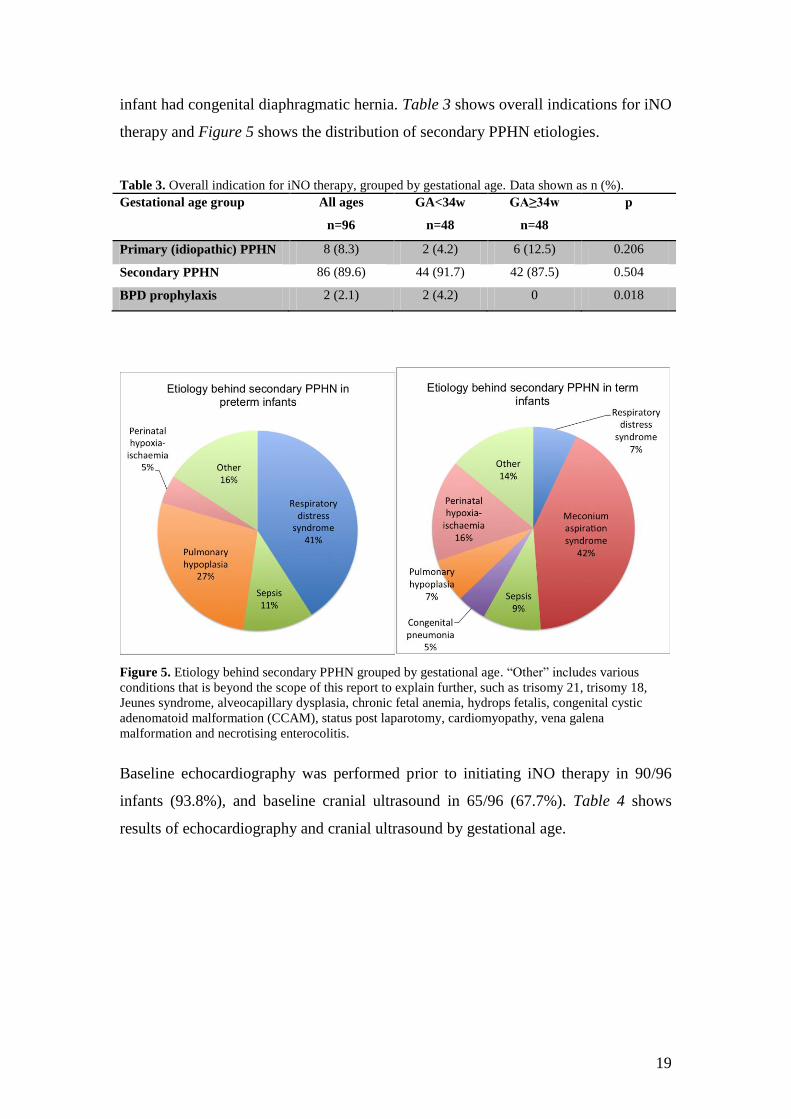
infant had congenital diaphragmatic hernia. Table 3 shows overall indications for iNO
therapy and Figure 5 shows the distribution of secondary PPHN etiologies.
Table 3. Overall indication for iNO therapy, grouped by gestational age. Data shown as n (%).
Gestational age group All ages
n=96
GA<34w
n=48
GA≥34w
n=48
p
Primary (idiopathic) PPHN 8 (8.3) 2 (4.2) 6 (12.5) 0.206
Secondary PPHN 86 (89.6) 44 (91.7) 42 (87.5) 0.504
BPD prophylaxis 2 (2.1) 2 (4.2) 0 0.018
Figure 5. Etiology behind secondary PPHN grouped by gestational age. “Other” includes various
conditions that is beyond the scope of this report to explain further, such as trisomy 21, trisomy 18,
Jeunes syndrome, alveocapillary dysplasia, chronic fetal anemia, hydrops fetalis, congenital cystic
adenomatoid malformation (CCAM), status post laparotomy, cardiomyopathy, vena galena
malformation and necrotising enterocolitis.
Baseline echocardiography was performed prior to initiating iNO therapy in 90/96
infants (93.8%), and baseline cranial ultrasound in 65/96 (67.7%). Table 4 shows
results of echocardiography and cranial ultrasound by gestational age.

20
Table 4. Baseline echocardiography and cranial ultrasound results grouped by gestational age. Data
shown as n (%).
Gestational age group Total
n=96
GA<34w
n=48
GA≥34w
n=48
p
Baseline echocardiography performed 90 (93.8) 46 (95.8) 44 (91.7) 0.399
Evidence of pulmonary hypertension * 80 (88.9) 38 (82.6) 42 (95.5) 0.053
Evidence of right-to-left shunt * 56 (62.2) 23 (50) 33 (75) 0.014
Baseline cranial ultrasound performed 65 (67.7) 40 (83.3) 25 (52.1) <0.01
Ultrasound status abnormal * 18 (27.7) 14 (35) 4 (16) 0.096
Abnormal cranial ultrasound cases represented intracranial hemorrhages grade 1-5 and findings of
echodensity or echolucency. *: percentages are relative to number of infants in whom examination was
performed.
4.2.2 Treatments prior to iNO therapy
Data on pre-iNO treatments was fully available only for the years 2008-2010 (n=72)
due to changes in registry design. During these years, pre-iNO use of surfactant and
HFOV was employed in 66.7% and 75% of infants in the total population,
respectively. Their uses also differed significantly between the gestational age groups,
with preterm infants receiving these therapies more often (in 89.2% vs. 42.9% and
94.6% vs. 54.3% of infants for surfactant and HFOV respectively, p<0.01 for both).
CPAP use was more common in the term/near term population (62.9% vs. 29.7%,
p<0.01). Overall use of inotropes/vasopressors (59.7% of cases) and conventional
mechanical ventilation (CMV; 40.3% of cases) did not differ between the gestational
age groups.
4.2.3 Baseline clinical data
Baseline OI could be calculated in only 56/96 infants (58.3%), 32/48 preterm (66.7%)
and 24/48 term/near term ones (50%; p=0.285), due to incomplete information in
patient records. Median OI was 32 (range 0-190) in the total population (n=56), and
differed significantly between gestational age groups; 49.3 (0-128.6) vs. 22.4 (0-190)
in the preterm and term/near term groups respectively (p<0.01).
4.3 iNO therapy
4.3.1 Initiation, duration and dosage
iNO therapy was started at a median age of 19 hours in the overall population, and the
overall median duration of therapy was 71 hours. Both parameters differed

21
significantly between gestational age groups, see Table 5. Preterm infants accounted
for 73.6% of all accumulated iNO therapy hours over the five years studied. iNO
therapy hours per year and gestational age are shown in Figure 6.
Figure 6. Distribution of iNO therapy hours in percent per year, grouped by gestational age. Numbers
inside bars are actual therapy hours.
iNO dosage did not differ significantly between the gestational age groups in any
aspect. The most common starting dose was 20 ppm. One infant received a starting
dose of 21 ppm and four received starting doses of 5-10 ppm. 20 ppm was also the
most common maximum dose, although five infants received maximum doses of 22-
40 ppm. Further dosing variables are shown in Table 5.
Table 5. iNO therapy parameters grouped by gestational age. Data shown as median (range).
“n” indicates number of infants with available data for each row.
Gestational age group All ages GA<34w GA≥34w p
Age at iNO start, hours (n=96) 19 (0-1894) 37 (0-1894) 11 (0-1651) 0.022
Starting dose, ppm (n=92) 20 (5-21) 20 (5-20) 20 (10-21) 0.691
Maximum dose, ppm (n=88) 20 (10-40) 20 (10-25) 20 (20-40) 0.229
Maintenance dose, ppm (n=87) 13 (1-20) 15 (1-20) 10 (1-20) 0.334
Final dose, ppm (n=60) 2 (0.1-20) 2 (0.5-20) 2.5 (0.1-20) 0.712
iNO duration, hours (n=96) 71 (0-1010) 113 (0-1010) 60 (2-655) <0.01
Ppm=parts per million. Final dose=last dose used before iNO cessation.
4.3.2 Concomitant therapies
Concomitant use of HFOV was more common in the preterm group than in the
term/near term group (97.9 vs. 79.2%, p<0.01). It was also more common than use of
CPAP or CMV in both groups (88.5% vs. 19.8% and 19.8% respectively, for the total
population). The use of CPAP and CMV did not differ significantly between the
1498 952
1566
3588 3945 11549
818 370
1986
451 516 4141
0%
20%
40%
60%
80%
100%
2006 2007 2008 2009 2010 Total
Perc
en
t o
f iN
O h
ou
rs
Year
GA≥34w
GA<34w

22
groups. Other concomitant cardiorespiratory support therapies used were inotropes,
systemic vasodilators and surfactant and in neither of these could significant
differences between gestational age groups be detected.
4.4 Outcomes
4.4.1 Initial response gas exchange
Initial response OI (OI within 1 hour of commencing iNO therapy) could be
calculated only in 41/96 infants (42.7%) due to incomplete data in patient records.
Median initial response OI was 20.6 (range 3-76) and did not differ significantly
between gestational age groups. Median OI reduction in percent of baseline value
could be calculated in 30/96 infants (31.3%), and an unsignificant trend was seen
towards a greater reduction in the preterm group; median reduction 60% vs. 39.3%,
(p=0.061).
4.4.2 Survival
66/96 infants (69%) survived until discharge from the NICU. 8/96 infants (8.3%, all
GA≥34w) were transferred to ECMO. In the term/near term group, 35/48 infants
(72.9%) survived without ECMO therapy. Table 6 shows survival grouped by
gestational age.
4.4.3 Bronchopulmonary dysplasia
Data on development of BPD defined as the need for supplemental oxygen at 28 days
post-natal age and at 36 weeks PMA could only be analysed for the years 2008-2010
(n=72) due to changes in registry design. The above outcomes were known in 47/72
(65.3%) and 41/72 (56.9%) infant records respectively. Of the cases with known
outcome, 24/47 patients (51.1%) had developed BPD at 28 days, and 16/41 (39%) at
36 weeks PMA. The composite outcome of “survival without BPD at 36 weeks
PMA” could be calculated in 41/72 patients (56.9%), of which 25/41 patients (61%)
met the outcome criteria. Table 6 shows survival and BPD outcomes grouped by
gestational age.

23
Table 6. Survival and development of BPD. Data related to BPD is from 2008-2010 only due to
differences in registry design. BPD outcome was known in a portion of these patients as indicated in
left column. Data shown as n (%).
Gestational age group All ages GA<34w GA≥34w p
Survival to discharge or ECMO (n=96) 66 (68.6) 28 (58.3) 38 (79.2) 0.042
Survival without ECMO (n=96) 63 (65.6) * 35 (72.9) 0.133
BPD at 28 days (n=47) 24 (51.1) 22 (88.0) 2 (9.1) <0.01
BPD at 36 weeks PMA (n=41) 16 (39) 15 (71.4) 1 (5.0) <0.01
Survival without BPD at 36wPMA, (n=41) 25 (61) 6 (28.6) 19 (95) <0.01
*=preterm infants are not eligible for ECMO.
4.4.4 Final cranial ultrasound
A comparison of baseline and final ultrasound status could be performed in 54/96
infants (56.3%) due to missing data; 36/48 preterm (75%) and 18/48 term/near term
ones (37.5%), p<0.01. Overall, 10 (26.3%) of 38 patients with a normal baseline
status deteriorated to an abnormal final status after iNO therapy. There was no
significant difference in the number of preterm or term/near term infants who
deteriorated. Six of eight preterm infants who deteriorated to an abnormal final status
had birth weights <1000g.
4.4.5 Other adverse events
Adverse effects of iNO therapy were rare in the study population. Rebound
hypoxemia after iNO cessation was reported in five infants (four preterm and one
term/near term). Two infants (one preterm and one term/near term) developed
pulmonary hemorrhage. One term infant receiving a maximum dose of 20 ppm
developed a slight tendency towards methemoglobinemia, however methemoglobin
levels did not exceed 5%.

24
5. Discussion
5.1 Major findings
Our data shows that 50% of all infants receiving iNO therapy at the NICU at ALCH
between 2006 and 2010 were born at GA<34w, and that infants in this age group had
a significantly longer duration of therapy. They also accounted for nearly 75% of all
iNO therapy hours. The corresponding proportion seen in an american study by Clark
et al. [47] was 53.5% for the years 2000-2008. This is notable, since the regulatory
approvals for neonatal iNO therapy [28] as well as a recently updated Cochrane
review [25] agree that the gas should be tried in infants born at GA≥34w with severe
hypoxemic respiratory failure and echocardiographic evidence of PPHN.
5.2 Comments on therapy in preterm infants
Clark et al. further point out that in their material, preterm infants receiving iNO
therapy were more critically ill than term/near term infants, since a larger proportion
were on HFOV before iNO initiation [47]. This circumstance is also seen in our data.
Furthermore, preterm infants in our study had a lower survival rate, and a
significantly higher baseline oxygenation index than term/near term infants (although
this parameter could only be calculated for approximately half of our patients). The
longer duration of iNO therapy in preterm infants seen in our material could thus
possibly be explained by their greater illness severity, and also by the general fragility
and the abundance of potential complications that accompanies preterm birth.
In one RCT that supported iNO as a BPD-prophylaxis, published by Ballard et al.
[45], a significantly reduced risk for death or BPD was seen in preterm infants who
received prolonged iNO therapy started after 7 days of age. In our study, only 2
infants (4.2% of the preterm group) explicitly received iNO therapy as a BPD-
prophylaxis according to patient records, and median therapy duration in the preterm
group (113h) was well below the duration used by Ballard et al. (>24 days) as was the
median age at therapy start (37 hours vs. 7-21 days). It therefore seems that iNO use
in preterm infants at ALCH has not been focused on BPD-prophylaxis, which is
consistent with the conclusions of large meta-analyses and systematic reviews
[37,44].

25
Conversely, the implications for its use in this group appear to have been attempts to
curb hypoxemic respiratory failure with or without echocardiographic evidence of
PPHN. 82.6% of preterm cases that had an echocardiography performed showed such
evidence, near-significantly less than the 95.5% portion of term/near term infants.
Furthermore, the number of infants showing evidence of right-to-left shunt was
significantly lower in the preterm group. Short-term oxygenation improvement may
well occur as a result of iNO therapy, despite lack of such evidence, and it is
suggested that the effect is not solely attributable to reducing overall PVR, but also to
intrapulmonary ventilation/perfusion matching [37]. Our material shows an
unsignificant trend towards a better OI improvement after 1h of therapy in preterm
infants than in term/near term ones, which might explain the persisting role of the gas
as a straw to clutch for in severe situations where therapeutic options are scarce.
Having said this, “rescue” iNO therapy in preterm infants has still not been shown to
improve long-term outcomes [37], and can thus not be considered evidence-based.
However, a National Institute of Health (NIH) Consensus Development Conference
[46] stated that iNO therapy in situations including pulmonary hypertension and
hypoplasia in infants of GA<34w is inadequately studied and that this subset of
infants might benefit from iNO therapy, provided that clinicians communicate the
uncertainties and potential risks and benefits to the family beforehand. 27% of our
preterm infants had a suspected pulmonary hypoplasia as the cause of PPHN, and our
population might partly fall within the bounds of the NIH reservation [46]. Of note,
nearly half of the preterm infants treated at ALCH had a birth weight <1000g, which
according to a post hoc analysis in an RCT by Van Meurs et al. [43] could be
associated with an increased risk of intracranial hemorrhage. A majority of the
preterm infants who showed deterioration on cranial ultrasound after iNO therapy in
our study were also of birth weight <1000g.
5.3 Comments on therapy in term/near term infants
iNO therapy for term/near term infants appear to have been used in accordance with
current evidence. Overall diagnosis in this group was exclusively primary and
secondary PPHN. In 92% of all term/near term cases was a baseline echocardiography
performed, in turn showing evidence of PPHN in 95.5% of cases. A Cochrane review

26
[25] states that iNO therapy should be reserved for severely ill infants, i.e. with an OI
of >25, until further studies has established whether an earlier start of iNO therapy (at
a lesser OI) leads to less clinical deterioration. Median OI in our term/near term group
was 22.5, albeit only calculated for a small portion of the total population due to
missing data, and was close to the cut-off level specified by the Cochrane review.
5.4 Other comments
No infants in this study were treated with iNO on the indication of CDH. This is
consistent with therapeutic recommendations [25,36]. However, at ALCH, most
infants with CDH are cared for at another unit (PICU), at which iNO is occasionally
used on this indication [Dr Baldvin Jonsson, April 2012, personal communication].
iNO patients at the PICU are not reported to the iNOcare registry and were thus not
included in this study. Baseline cranial ultrasonography was performed significantly
more often in preterm infants than in term/near term ones. It is however not a pre-
requisite for therapy initiation in the term/near term group since the risk for severe
intracranial hemorrhage is markedly lower than for the preterm group. A cause for
concern is the lack of cranial ultrasound follow-up, with only 75% of preterm infants
having both baseline and final cranial ultrasound status noted in their record.
5.5 Outcomes
The overall survival rates were 58% vs. 79% (preterms vs. term/near terms),
comparable with the 48% vs. 73% survival rates seen across several European centres
in an interim analysis of the iNOcare registry [48]. The rate of survival without
ECMO in our term/near term group was 73%, higher than results of large RCTs by
Clark et al. (60%) [33] and the NINOS group (54.4%) [27]. Our preterm group
demonstrated a 28.6% rate of survival without BPD at 36 weeks, which should be
related to the 41% rate found in the meta-analysis by Askie et al. [44]. However, the
iNOcare registry does not note gestational days, and a BPD diagnosis at 36 weeks
PMA was therefore based on whether the infant continuously received supplemental
O2 (as noted in patient records) at a date that in reality could be 36 weeks + 6 days
PMA. It can be questioned whether this sole bit of information, gathered in retrospect,
provides a confident base for a BPD diagnosis, and our outcome data in this matter
should be cautiously interpreted.

27
Methemoglobinemia or elevated NO2 levels did not occur, and the number of cases
where iNO suspension led to a rebound hypoxemia were few. Dosing regimens
followed recommendations by a Cochrane analysis [25] as the overall starting dose
most often was 20 ppm. Moreover, median final dose was 2 ppm, and no dosing
parameter differed significantly between our groups. The clinical management and
monitoring of on-going iNO therapy at ALCH thus appears adequate.
5.6 Limitations
There are several limitations to this study. It was not our intention to perform any in-
depth analysis of iNO efficacy in relation to other therapies or placebo. We can
therefore only relate our results concerning survival, BPD and gas exchange to that of
other authors who have established this efficacy [25,37]. Furthermore, gathering
clinical information in retrospect presupposes a reliable and comprehensive
information source. In this study, this was only the case for parts of the data collected,
and sometimes the information found in the patient records was scanty. In one record,
the only note concerning iNO therapy was: “NO therapy suspended today”; clearly
not a solid base for scientific analysis. The type of data most often missing was
baseline and initial response gas exchange, with both categories completely available
in only a quarter of our patients. This missing data might however possibly serve as a
reminder to researchers and clinicians at ALCH on the importance of keeping
accurate patient data records, and of gathering patient data in real-time, even in a non-
prospective research project such as the iNOcare registry. Another important
limitation regarding the generalizability of our results as a quality marker of iNO
therapy in the whole of ALCH, is that only infants receiving iNO therapy at the
NICU, and not the PICU, were included. A potential confounder to our conclusions is
the fact that only infants born in 2006-2010 were included for analysis, whereas
several important publications clarifying the lack of iNO efficacy in preterm infants
were published or revised in 2010 and 2011 [37,41,44,46]. Furthermore, one RCT that
suggested such an efficacy exists was published in 2006 [45]. It could therefore be
argued that iNO practices at ALCH might well be on their way towards greater
concordance with evidence. However, our results show that the preterm portion was
greater in 2009 and 2010 than in the previous years, both in patients and in therapy
hours. Further studies similar to this one, including patients treated in 2011 and 2012,
could clarify this issue.

28
5.7 Overall reflexions
The lack of iNO efficacy on long-term outcomes in the preterm population should in a
rational mind ideally prevail above its short-term positive effects when making
therapeutic decisions. Our results show that this is not always the case, possibly
explained by the short-term improvement often seen. The inherently slow pace at
which new scientific conclusions are transformed into clinical routine appears to be a
global problem affecting every branch of medicine, resulting in persistence of
obsolete, evidence-lacking methods. The reasons for this could include inadequate
ways of implementing new clinical guidelines, irrational decision-making in clinically
desperate situations and various other phenomena. Studies such as this one are
important parts of paving the way towards a greater consistency between actual
clinical practices and scientific evidence. A final rhetorical question to provide a
starting point for local discussions of iNO therapy is therefore whether this very
expensive therapy should be used so extensively in a population where its evidence
for efficacy is slim despite several large studies, and where its potential risks are
incompletely understood.

29
6. Conclusions
The use of iNO therapy at the NICU at ALCH between 2006 and 2010 was not
completely consistent with current evidence, since half of the treated infants were
born before 34 weeks of gestation. Infants born after 34 weeks of gestation were
treated according to evidence-based recommendations. In some aspects the clinical
information available in patient records was meagre. A suggestion is that clinicians at
ALCH revise their approach to iNO therapy in preterm infants.

30
7. Acknowledgements
This study could not have been designed, carried out or finished without the
inspiration and support from my supervisor, dr. Baldvin Jonsson, who always had an
optimistic attitude towards having a student taking up part of his time. Thanks also for
the book [4]! Denise Jansson cheerfully helped me out with keys, system passwords,
printing issues and the coffee machine, and understood a student’s need for a semla
on the fat-Tuesday. Nancy Lindqvist did some date-and-time magic in Excel for
which I am grateful. I would also like to thank dr. Per Häggström and all other staff
members at the NICU ward for letting me hang around to see what life might be like
for a newborn in an incubator, and for letting me participate hands-on in some of the
daily routines. Merci to dr. Farid Boubred for many impromptu French lessons in our
common office at ALCH. Last but not least, lots of love to my family, Sara and
Torsten, who put up with my behaviour and supported me during this semester.

31
8. References
1. Steinhorn RH. Neonatal pulmonary hypertension. Pediatric Critical Care Medicine. 2010
Mar;11(2 Suppl):S79–84.
2. Rudolph AM. High Pulmonary Vascular Resistance After Birth. Pathophysiologic
Considerations and Etiologic Classification. Clinical Pediatrics. 1980 Sep 1;19(9):585–90.
3. Sharma M, Mohan KR, Narayan S, Chauhan L. Persistent pulmonary hypertension of the
newborn: a review. Medical Journal Armed Forces India. 2011 Oct;67(4):348–53.
4. Van Marter LJ. Persistent pulmonary hypertension of the newborn. In: Cloherty JP,
Eichenwald EC, Hansen AR, Stark AR, editors. Manual of neonatal care. Philadelphia:
Lippincott Williams & Wilkins; 2012. p. 435–42.
5. Kiserud T. Physiology of the fetal circulation. Seminars in fetal & neonatal medicine. 2005
Dec;10(6):493–503.
6. Abman SH, Chatfield BA, Hall SL, McMurtry IF. Role of endothelium-derived relaxing factor
during transition of pulmonary circulation at birth. American Journal of Physiology.
1990;259:H1921–7.
7. Kieler H, Artama M, Engeland A, Ericsson O, Furu K, Gissler M, et al. Selective serotonin
reuptake inhibitors during pregnancy and risk of persistent pulmonary hypertension in the
newborn: population based cohort study from the five Nordic countries. Bmj. 2012 Jan
12;344(jan12 3):d8012–d8012.
8. Sylvester JT, Shimoda LA, Aaronson PI, Ward JPT. Hypoxic Pulmonary Vasoconstriction.
Physiological Reviews. 2012 Jan 31;92(1):367–520.
9. Wolf GK, Arnold JH. Extracorporeal membrane oxygenation. In: Cloherty JP, Eichenwald EC,
Hansen AR, Stark AR, editors. Manual of neonatal care. Philadelphia: Lippincott Williams &
Wilkins; 2012. p. 454–62.
10. Jobe AH, Bancalari E. Bronchopulmonary Dysplasia. American Journal of Respiratory and
Critical Care Medicine. 2001;163:1723–9.
11. Walsh MC, Szefler S, Davis J, Allen M, Van Marter L, Abman S, et al. Summary proceedings
from the bronchopulmonary dysplasia group. Pediatrics. 2006 Mar;117(3):S52–6.
12. Northway WH, Rosan RC, Porter DY. Pulmonary disease following respirator therapy of
hyaline-membrane disease. Bronchopulmonary dysplasia. The New England Journal of
Medicine. 1967;276(7):357–268.
13. Philip AGS. Bronchopulmonary Dysplasia: Then and Now. Neonatology. 2012 Feb
18;102(1):1–8.
14. Hayes D, Feola DJ, Murphy BS, Shook L a, Ballard HO. Pathogenesis of Bronchopulmonary
Dysplasia. Respiration. 2010 Jan;79(5):425–36.
15. Husain a N, Siddiqui NH, Stocker JT. Pathology of arrested acinar development in
postsurfactant bronchopulmonary dysplasia. Human pathology. 1998 Jul;29(7):710–7.
16. Jobe AH. The new bronchopulmonary dysplasia. Current opinion in pediatrics. 2011
Apr;23(2):167–72.

32
17. Ignarro LJ, Buga GM, Wood KS, Byrns RE, Chaudhuri G. Endothelium-derived relaxing
factor produced and released from artery and vein is nitric oxide. Proceedings of the National
Academy of Science. 1987;84(December):9265–9.
18. Palmer RMJ, Ferrige AG, Moncada S. Nitric oxide release accounts for the biological activity
of endothelium-derived relaxing factor. Nature. 1987;327:524–6.
19. Gaston B, Drazen JM, Loscalzo J, Stamler JS. The Biology of Nitrogen Oxides in the Airways.
American Journal of Respiratory and Critical Care Medicine. 1994;149:538–51.
20. Ricciardolo FLM, Sterk PJ, Gaston B, Folkerts G. Nitric Oxide in Health and Disease of the
Respiratory System. Physiological Reviews. 2004;84:731–65.
21. Palmer RMJ, Ashton DS, Moncada S. Vascular endothelial cells synthesize nitric oxide from
L-arginine. Nature. 1988;333(June):664–6.
22. Gibson QH, Roughton FJW. The kinetics and equilibria of the reactions of nitric oxide with
sheep haemoglobin. Journal of Physiology. 1957;136:507–26.
23. Frostell C, Fratacci MD, Wain JC, Jones R, Zapol WM. Inhaled nitric oxide. A selective
pulmonary vasodilator reversing hypoxic pulmonary vasoconstriction. Circulation.
1991;83(5):2038–47.
24. Pepke-Zaba J, Higenbottam TW, Dinh-Xuan AT, Stone D, Wallwork J. Inhaled nitric oxide as
a cause of selective pulmonary vasodilatation in pulmonary hypertension. Lancet.
1991;338(November):1173–4.
25. Finer N, Barrington KJ. Nitric oxide for respiratory failure in infants born at or near term
(Review). The Cochrane Library. 2009;(1).
26. Davidson D, Barefield ES, Kattwinkel J, Dudell G, Damask M, Straube R, et al. Inhaled nitric
oxide for the early treatment of persistent pulmonary hypertension of the term newborn: A
randomized, double-masked, placebo-controlled, dose-response, multicenter study. Pediatrics.
1998;101(3):325–34.
27. NINOS. Inhaled nitric oxide in full-term and nearly full-term infants with hypoxic respiratory
failure. The New England Journal of Medicine. 1997;336(9):597–604.
28. Läkemedelsindustriföreningen. INOMax [Internet]. FASS. 2012 [cited 2012 Apr 27];Available
from:
http://www.fass.se/LIF/produktfakta/artikel_produkt.jsp?NplID=20010801000011&DocTypeI
D=3&UserTypeID=0
29. Zayek M, Cleveland D, Morin FC. Treatment of persistent pulmonary hypertension in the
newborn lamb by inhaled nitric oxide. Pediatrics. 1993;122(5):743–50.
30. Roberts JDJ, Chen T-yan, Kawai N, Wain J, Dupuy P, Shimouchi A, et al. Inhaled Nitric Oxide
Reverses Pulmonary Vasoconstriction in the Hypoxic and Acidotic Newborn Lamb.
Circulation Research. 1993;72(2):246–54.
31. Roberts JD, Polander DM, Lang P, Zapol WM. Inhaled nitric oxide in persistent pulmonary
hypertension of the newborn. Lancet. 1992;340:818–9.
32. Kinsella JP, Neish SR, Shaffer E, Abman SH. Low-dose inhalation nitric oxide in persistent
pulmonary hypertension of the newborn. Lancet. 1992;340:819–20.

33
33. Clark RH, Kusesr TJ, Walker MW, Southgate M, Hucakby JL, Perez JA, et al. Low-dose nitric
oxide therapy for persistent pulmonary hypertension of the newborn. The New England Journal
of Medicine. 2000;342(7):469–74.
34. Roberts JDJ, Fineman JR, Morin FC, Shaul PW, Rimar S, Schreiber MD, et al. Inhaled nitric
oxide and persistent pulmonary hypertension of the newborn. The New England Journal of
Medicine. 1997;336(9):605–10.
35. Wessel DL, Adatia I, Van Marter LJ, Thompson JE, Kane JW, Stark AR, et al. Improved
Oxygenation in a Randomized Trial of Inhaled Nitric Oxide for Persistent Pulmonary
Hypertension of the Newborn. Pediatrics. 1997 Nov 1;100(5):e1–7.
36. NINOS. Inhaled Nitric Oxide and Hypoxic Respiratory Failure in Infants With Congenital
Diaphragmatic Hernia. Pediatrics [Internet]. 1997 Jun 1 [cited 2012 Apr 27];99(6):838–45.
Available from: http://pediatrics.aappublications.org/cgi/doi/10.1542/peds.99.6.838
37. Barrington KJ, Finer N. Inhaled nitric oxide for respiratory failure in preterm infants (Review).
The Cochrane Library. 2010;(12).
38. Gutierrez HH, Nieves B, Chumley P, Rivera A, Freeman BA. Nitric oxide regulation of
superoxide-dependent lung injury: Oxidant-protective actions of endogenously produced and
exogenously administered nitric oxide. Free radical biology & medicine. 1996;21(1):43–52.
39. McCurnin DC, Pierce R a, Chang LY, Gibson LL, Osborne-Lawrence S, Yoder B a, et al.
Inhaled NO improves early pulmonary function and modifies lung growth and elastin
deposition in a baboon model of neonatal chronic lung disease. Am J Physiol Lung Cell Mol
Physiol. 2005 Mar;288(3):L450–9.
40. Kinsella JP, Cutter GR, Walsh WF, Gerstmann DR, Bose CL, Hart C, et al. Early inhaled nitric
oxide therapy in premature newborns with respiratory failure. The New England journal of
medicine. 2006 Jul 27;355(4):354–64.
41. Mercier J-C, Hummler H, Durrmeyer X, Sanchez-Luna M, Carnielli V, Field D, et al. Inhaled
nitric oxide for prevention of bronchopulmonary dysplasia in premature babies (EUNO): a
randomised controlled trial. Lancet. 2010 Jul 31;376(9738):346–54.
42. Field D, Elbourne D, Truesdale A, Grieve R, Hardy P, Fenton AC, et al. Neonatal Ventilation
With Inhaled Nitric Oxide Versus Ventilatory Support Without Inhaled Nitric Oxide for
Preterm Infants With Severe Respiratory Failure: the INNOVO multicentre randomised
controlled trial (ISRCTN 17821339). Pediatrics. 2005 Apr;115(4):926–36.
43. Van Meurs KP, Wright LL, Ehrenkranz RA, Lemons JA, Ball MB, Poole WK, et al. Inhaled
Nitric Oxide for Premature Infants with Severe Respiratory Failure. The New England Journal
of Medicine. 2005;353(1):13–22.
44. Askie LM, Ballard R a, Cutter GR, Dani C, Elbourne D, Field D, et al. Inhaled Nitric Oxide in
Preterm Infants: An Individual-Patient Data Meta-analysis of Randomized Trials. Pediatrics.
2011 Sep 19;128(4):729–39.
45. Ballard RA, Truog WE, Cnaan A, Martin RJ, Ballard PL, Merrill JD, et al. Inhaled Nitric
Oxide in Preterm Infants Undergoing Mechanical Ventilation. The New England Journal of
Medicine. 2006;355(4):343–53.
46. Cole FS, Alleune C, Barks JD, Boyle RJ, Carrol JL, Dokken D, et al. National Institute of
Health Consensus Development Conference Statement: Inhaled Nitric Oxide Therapy for
Premature Infants. NIH Consens State Sci Statements. 2010;27(5).

34
47. Clark RH, Ursprung RL, Walker MW, Ellsbury DL, Spitzer AR. The changing pattern of
inhaled nitric oxide use in the neonatal intensive care unit. Journal of Perinatology.
2010;30(12):800–4.
48. Dewhurst C, Ibrahim H, Göthberg S, Jónsson B, Subhedar N. Use of inhaled nitric oxide in the
new born period: results from the European Inhaled Nitric Oxide Registry. Acta paediatrica.
2010 Jun;99(6):854–60.
49. Nyföddhetsmedicin (Neonatologi) - Kliniker & enheter Astrid Lindgrens Barnsjukhus -
Karolinska Universitetssjukhuset [Internet]. [cited 2012 Feb 13];Available from:
http://www.karolinska.se/AstridLindgrensBarnsjukhus/Kliniker--enheter/Neonatologi/

35
Appendix 1
Overview of data parameters submitted to the iNOcare registry.
Data category Parameter Options/unit Comments
Patient admission Patient type 1 - Neonatal without cardiac
diagnosis
2 – Neonatal or pediatric with
cardiac diagnosis
3 – Pediatric without cardiac
diagnosis
Single choice
Date/time of birth Date/time
Date/time of ICU admission Date/time
Gender Male, female
Birth weight g
Gestational age at birth Completed weeks
Weight at admission kg
Age at admission Years/months/days Calculated
automatically
Pre-treatment
diagnosis
Overall diagnosis -Hypoxemic respiratory
failure
-Prophylactic to prevent
chronic lung disease
Single choice
If hypoxemic respiratory
failure:
-Primary PPHN
-Secondary PPHN
Single choice
If secondary PPHN: -Respiratory distress
syndrome
-Meconium aspiration
syndrome
-Sepsis
-Congenital pneumonia
-Congenital diaphragmatic
hernia
-Pulmonary hypoplasia
-Chronic lung disease
-Perinatal hypoxia-ischemia
-Other (specify with text)
Single choice
Other diagnosis -Hemodynamically significant
PDA
-Pneumothorax
Multiple choice
Treatment prior to
iNO therapy
Treatment prior to iNO
therapy performed?
-Yes, No, Unknown Single choice
If yes, specify: -Surfactant
-Inotrope/vasopressor
-IV vasodilator
-Continuous positive airway
pressure
-Non-invasive ventilation
-Conventional mechanical
ventilation
-High-frequency ventilation
-Other (specify with text)
Multiple choice
Baseline
echocardiography
Baseline echocardiography
performed?
Yes, No Single choice.
Evidence of pulmonary
hypertension?
Yes, No, Unknown Single choice

36
Evidence of right-to-left
shunt?
Yes, No, Unknown Single choice
Evidence of left ventricular
dysfunction?
Yes, No, Unknown Single choice
Evidence of right ventricular
dysfunction?
Yes, No, Unknown Single choice
Baseline gas
exchange
FiO2 No unit (0.21-1.0)
PaO2 kPa and/or mmHg
Mean airway pressure cm H2O
Oxygenation index and P/F
ratio
No unit Calculated
automatically
SpO2, pre and post ductal %
Baseline
cardiovascular
status
Mean systemic arterial
pressure
mmHg
Systolic systemic arterial
pressure
mmHg
Heart rate b/min
Baselie cranial
ultrasonography
Status Normal, Abnormal Single choice
Periventricular hemorrhage None or grade 1-5 Single choice
Parenchymal echolucency Yes, no Single choice
Parenchymal echodensity Yes, no Single choice
iNO therapy iNO started during transport Yes, no Single choice
iNO started after admission Yes, no Single choice
iNO started date/time Date/time
Duration from admission Days, hours Calculated
automatically
iNO discontinued date/time Date/time
Duration of iNO treatment Days, hours Calculated
automatically
Starting dose ppm
Maximum dose ppm
Maintenance dose ppm
Final dose ppm
Delivery device INOvent, other
iNO source INOmax, other
Concentration in cylinder ppm 400 ppm default if
source is INOmax
Concomitant
therapies
Treatment while receiving
iNO
Nasal cannula/prongs
CPAP
Non-invasive ventilation
CMV
HFOV
Prostacyclin analog
PDE5 inhibitor
PDE3 inhibitor
Inotropes
Surfactant
Other (specify with text)
IV or inhaled
IV or oral
Gas exchange
within 60 minutes
of starting iNO
FiO2
No unit (0.21-1.0)
PaO2 kPa and/or mmHg
Mean airway pressure cm H2O
Oxygenation index and P/F
ratio
No unit Calculated
automatically

37
SpO2 %
Cardiovascular
status within 60
minutes of starting
iNO
Mean systemic arterial
pressure
mmHg
Systolic systemic arterial
pressure
mmHg
Heart rate b/min
Adverse effects of
iNO therapy
Adverse events occurred? Yes, no Single choice
If yes -Methemoglobinemia (>5%)
-Elevated NO2 (>1ppm)
-Pulmonary hemorrhage
-Rebound hypoxemia after
cessation of iNO
-Other (specify with text)
Multiple choice
Post treatment
diagnosis
Final cranial ultrasound status Normal, abnormal Single choice
Periventricular hemorrhage None or grade 1-5 Single choice
Parenchymal echolucency Yes, no Single choice
Parenchymal echodensity Yes, no Single choice
Chronic lung disease (oxygen
dependency at 28d)
Yes, no, unknown Single choice
Chronic lung disease (oxygen
dependency at 36w)
Yes, no, unknown Single choice
Final outcome ECMO Yes, no Single choice
Survival Yes, no, unknown Single choice
If survival: Yes, date of
discharge from unit
date
If survival: Yes, date of
discharge home
date
If survival: No, date of death date
If survival: No, cause of death Free text
Duration from ICU admission
to discharge/transfer or death
Days Calculated
automatically





























