Embed Size (px)
Citation preview

Neonatal Orthopedic Neonatal Orthopedic IssuesIssues
Mikelle Key-Solle, MD Mikelle Key-Solle, MD
May 22, 2006May 22, 2006

ObjectivesObjectives
Recognize common orthopedic issues Recognize common orthopedic issues which present in the neonatal periodwhich present in the neonatal period
Generate appropriate differential Generate appropriate differential diagnoses diagnoses
Identify appropriate interventions Identify appropriate interventions from a general pediatric perspectivefrom a general pediatric perspective

OverviewOverview
Cased-based discussion of five of the Cased-based discussion of five of the more common neonatal orthopedic more common neonatal orthopedic and musculoskeletal conditionsand musculoskeletal conditions– Typical physical exam findingsTypical physical exam findings– Management strategiesManagement strategies– When to consult an orthopedic surgeon When to consult an orthopedic surgeon

Case 1Case 1
You are examining a 3 hour old term You are examining a 3 hour old term male infant male infant
Mother had unremarkable pregnancy Mother had unremarkable pregnancy and delivery with normal prenatal and delivery with normal prenatal labslabs
Infant appears nondysmorphic with a Infant appears nondysmorphic with a normal exam except for the following normal exam except for the following feet findings:feet findings:

Case 1Case 1

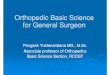
Case 1:Case 1:Metatarsus AdductusMetatarsus Adductus
AKA Metatarsus varusAKA Metatarsus varus Hindfoot normally positioned, but forefoot Hindfoot normally positioned, but forefoot
adductedadducted Flexible versus non-flexibleFlexible versus non-flexible 85% spontaneously resolve85% spontaneously resolve Gentle stretching exercises may helpGentle stretching exercises may help

Metatarsus AdductusMetatarsus Adductus
If does not If does not spontaneously spontaneously resolve, can lead to resolve, can lead to classic foot deformityclassic foot deformity– Sole creaseSole crease– Lateral bony Lateral bony
prominenceprominence May require shoes, May require shoes,
castingcasting

Time for TriviaTime for Trivia
What is the origin of the phrase What is the origin of the phrase “getting off on the wrong foot”?“getting off on the wrong foot”?
Putting the left foot down on the floor Putting the left foot down on the floor first when getting out of bedfirst when getting out of bed

Case 2Case 2
You are examining a 3 hour old term You are examining a 3 hour old term male infant male infant
Mother had unremarkable pregnancy Mother had unremarkable pregnancy and delivery with normal prenatal and delivery with normal prenatal labslabs
Infant appears nondysmorphic with a Infant appears nondysmorphic with a normal exam except for the following normal exam except for the following feet findings:feet findings:

Case 2Case 2

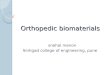
Talipes EquinovarusTalipes Equinovarus
AKA ClubfootAKA Clubfoot Malalignment of Malalignment of
the talocalcaneal, the talocalcaneal, talonavicular and talonavicular and calcaneocuboid calcaneocuboid joints joints

Talipes EquinovarusTalipes Equinovarus
Fixed plantar flexion (equinus) of Fixed plantar flexion (equinus) of the ankle (talipes)the ankle (talipes)– inability to bring to foot to a inability to bring to foot to a
plantigrade (flat) standing positionplantigrade (flat) standing position Inversion/adductionInversion/adduction
of the heel (varus)of the heel (varus) Metatarsus adductusMetatarsus adductus

Talipes EquinovarusTalipes Equinovarus
2:1 male to female2:1 male to female 50% bilateral50% bilateral Usually idiopathicUsually idiopathic More severe if associated with More severe if associated with
neurological, connective tissue, or neurological, connective tissue, or mechanical conditionsmechanical conditions

Talipes EquinovarusTalipes Equinovarus
Requires urgent orthopedic referralRequires urgent orthopedic referral Treated using Ponseti method of Treated using Ponseti method of
serial casting +/- Achilles tendon serial casting +/- Achilles tendon releaserelease– Followed by nighttime bracing for Followed by nighttime bracing for
2 years2 years Outcomes typically very goodOutcomes typically very good

SummarySummary
Case 1: Metatarsus AdductusCase 1: Metatarsus Adductus– Forefoot adduction; most spont resolveForefoot adduction; most spont resolve
Case 2: Talipes EquinovarusCase 2: Talipes Equinovarus– 3 components; early ortho referral3 components; early ortho referral
Case 3:Case 3: Case 4:Case 4: Case 5:Case 5:

Time for TriviaTime for Trivia
What do Kristi Yamaguchi, Mia Hamm, and What do Kristi Yamaguchi, Mia Hamm, and Troy Aikman all have in common?Troy Aikman all have in common?
All had congenital clubfoot treated with All had congenital clubfoot treated with Ponseti method Ponseti method

Case 3Case 3
You are examining a 4 week old term You are examining a 4 week old term female, born by c-section (breech)female, born by c-section (breech)
NBN course unremarkableNBN course unremarkable Parents report infant seems to prefer Parents report infant seems to prefer
keeping head tilted towards the right keeping head tilted towards the right shouldershoulder

Case 3Case 3
What do you expect to What do you expect to find on physical exam?find on physical exam?
What is a common What is a common association with this association with this condition?condition?

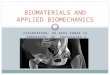
Congenital Muscular TorticollisCongenital Muscular Torticollis(CMT)(CMT)
AKA “wryneck”AKA “wryneck” Unilateral deformity of the Unilateral deformity of the
sternocleidomastoid (SCM) muscle sternocleidomastoid (SCM) muscle resulting in chin pointing away and resulting in chin pointing away and head tilting towards the affected sidehead tilting towards the affected side
Within first few weeks, may be able Within first few weeks, may be able to palpate a firm, non-tender SCM to palpate a firm, non-tender SCM massmass

CMTCMT
AssociationsAssociations::– 80-90% with contralateral plagiocephaly 80-90% with contralateral plagiocephaly
and ipsilateral facial flatteningand ipsilateral facial flattening– 20% with hip20% with hip
dysplasiadysplasia

CMTCMT Differential diagnosis: 3 categoriesDifferential diagnosis: 3 categories
– OsseousOsseousKlippel-Feil syndrome, congenital scoliosisKlippel-Feil syndrome, congenital scoliosis
– Non-osseousNon-osseousSandifer syndromeSandifer syndrome
– NeurogenicNeurogenicCNS tumors, Chiari malformationCNS tumors, Chiari malformationOcular torticollisOcular torticollisParoxysmal torticollisParoxysmal torticollis

CMTCMT

CMTCMT
Treatment consists of passive stretchingTreatment consists of passive stretching– PT referral by 2-3 months if >10° dec ROMPT referral by 2-3 months if >10° dec ROM
85% will correct by 18 months85% will correct by 18 months Persistence after 18 months warrants Persistence after 18 months warrants
orthopedic referral orthopedic referral

SummarySummary
Case 1: Metatarsus AdductusCase 1: Metatarsus Adductus– Forefoot adducted; most spont resolveForefoot adducted; most spont resolve
Case 2: Talipes EquinovarusCase 2: Talipes Equinovarus– 3 components; early splinting3 components; early splinting
Case 3: Cong. Muscular TorticollisCase 3: Cong. Muscular Torticollis– Head tilt; SCM mass early; stretchingHead tilt; SCM mass early; stretching
Case 4:Case 4: Case 5:Case 5:

Time for TriviaTime for Trivia(or maybe just “triviality”)(or maybe just “triviality”)

Case 4Case 4
You are examining a 3 hour old term You are examining a 3 hour old term male born by c-section for failure to male born by c-section for failure to progressprogress
Mother’s history is significant for Mother’s history is significant for bilateral clubfoot s/p correction, s/p bilateral clubfoot s/p correction, s/p pelvic stabilization surgery, pelvic stabilization surgery, malignant hyperthermia, and malignant hyperthermia, and rheumatoid arthritis; father healthyrheumatoid arthritis; father healthy

Case 4Case 4
Infant exam remarkable forInfant exam remarkable for– Diffuse hypertonicity and limited ROMDiffuse hypertonicity and limited ROM– Bilateral finger and toe deformities, Bilateral finger and toe deformities,
ulnar deviation of fingers ulnar deviation of fingers – Bilateral elbow extension, forearm Bilateral elbow extension, forearm
pronation pronation – Bilateral flexion deformity of kneesBilateral flexion deformity of knees– Bilateral clubfootBilateral clubfoot– Few skin creases over jointsFew skin creases over joints

Case 4Case 4

Arthrogryposis Multiplex CongenitaArthrogryposis Multiplex Congenita(AMC)(AMC)
Collection of >150 conditions leading Collection of >150 conditions leading to >2 joint contracturesto >2 joint contractures
Non-progressiveNon-progressive Fibrosis of connective tissue and Fibrosis of connective tissue and
musclemuscle Etiology unknown, multifactorialEtiology unknown, multifactorial

AMCAMC Etiologic categories: neurologic vs. non-neuroEtiologic categories: neurologic vs. non-neuro
– NeuropathicNeuropathic AmyoplasiaAmyoplasia MeningomyeloceleMeningomyelocele Spinal muscular atrophySpinal muscular atrophy
– Muscle abnormalityMuscle abnormality Cong muscular/myotonic dystrophy, myastheniaCong muscular/myotonic dystrophy, myasthenia Intrauterine myositisIntrauterine myositis Mitochondrial disordersMitochondrial disorders
– Connective tissue abnormalityConnective tissue abnormality DwarfismDwarfism Multiple pterygium syndormeMultiple pterygium syndorme Distal arthrogryposisDistal arthrogryposis
– Intrauterine abnormalityIntrauterine abnormality Limited fetal spaceLimited fetal space Vascular compromiseVascular compromise

AMCAMC
Only 30% geneticOnly 30% genetic– All forms of inheritanceAll forms of inheritance– Examples: Trisomy 18/21, Holt-Oram, Examples: Trisomy 18/21, Holt-Oram,
Mobius, nemaline myopathy, Zellweger, Mobius, nemaline myopathy, Zellweger, Pfeiffer, PolandPfeiffer, Poland
Most common form is amyoplasia Most common form is amyoplasia (40%)(40%)

AMC:AMC: Amyoplasia Amyoplasia
shoulder--internal rotation deformityshoulder--internal rotation deformity elbow--extension and pronation deformityelbow--extension and pronation deformity wrist--volar and ulnar deformitywrist--volar and ulnar deformity hand--fingers in fixed flexion, and thumb-hand--fingers in fixed flexion, and thumb-
in-palm deformityin-palm deformity hip--flexed, abducted and externally hip--flexed, abducted and externally
rotated, often dislocatedrotated, often dislocated knee--flexion deformityknee--flexion deformity foot--clubfoot deformityfoot--clubfoot deformity

AMCAMC
AssociationsAssociations– Midface hemangiomasMidface hemangiomas– ScoliosisScoliosis– Growth retardationGrowth retardation– Abdominal herniasAbdominal hernias
Typically normal intelligenceTypically normal intelligence

AMCAMC Cause determines prognosisCause determines prognosis
– If neurologic deficit, brain/spine MRIIf neurologic deficit, brain/spine MRI– If dysmorphic features, karyotype and If dysmorphic features, karyotype and
genetics consultgenetics consult Early orthopedic referral necessaryEarly orthopedic referral necessary
– Non-surgical measures used in neonatal Non-surgical measures used in neonatal periodperiodSplinting/castingSplinting/castingPT and ROM exercisesPT and ROM exercises

SummarySummary
Case 1: Metatarsus AdductusCase 1: Metatarsus Adductus– Forefoot adducted; most spont resolveForefoot adducted; most spont resolve
Case 2: Talipes EquinovarusCase 2: Talipes Equinovarus– 3 components; early splinting3 components; early splinting
Case 3: Cong. Muscular TorticollisCase 3: Cong. Muscular Torticollis– Head tilt; SCM mass early; stretchingHead tilt; SCM mass early; stretching
Case 4: Arthrogryposis Multiplex Case 4: Arthrogryposis Multiplex CongenitaCongenita– Multiple contractures; neuro vs non-neuro; Multiple contractures; neuro vs non-neuro;
amyoplasia most common; splinting/casting in amyoplasia most common; splinting/casting in neonatal periodneonatal period
Case 5:Case 5:

More TrivialityMore Triviality

Case 5Case 5
You are examining a 4 week old term You are examining a 4 week old term female born by c-section (breech)female born by c-section (breech)
NBN course was unremarkableNBN course was unremarkable Parents have no concernsParents have no concerns Growth parameters all 50%th Growth parameters all 50%th
percentilepercentile

Case 5Case 5
Previous exam revealed a right hip Previous exam revealed a right hip click with Barlow maneuver, but now click with Barlow maneuver, but now this has progressed to a “clunk”this has progressed to a “clunk”– What are Barlow and Ortolani What are Barlow and Ortolani
maneuvers?maneuvers?

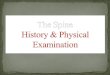
Case 5:Case 5:Barlow and OrtolaniBarlow and Ortolani
Infant must be relaxedInfant must be relaxed Examine one hip at a timeExamine one hip at a time Hip flexed 90°, gentle manipulationHip flexed 90°, gentle manipulation BBarlow=arlow=BBack + adductionack + adduction OOrtolani=rtolani=OOut + anteriorut + anterior Positive if “clunk” Positive if “clunk”
palpable/heardpalpable/heard

Case 5Case 5
What additional physical exam What additional physical exam findings would suggest hip dysplasia?findings would suggest hip dysplasia?– Asymmetric gluteal/thigh foldsAsymmetric gluteal/thigh folds– Leg length discrepancy (3-6 months)Leg length discrepancy (3-6 months)– Limited hip abduction (3-6 months)Limited hip abduction (3-6 months)

Developmental Dysplasia of the Hip Developmental Dysplasia of the Hip (DDH)(DDH)
DefinitionsDefinitions– DysplasiaDysplasia: abnormal : abnormal
formation/development of hip jointformation/development of hip joint– SubluxatedSubluxated: Femoral head is partially : Femoral head is partially
out of proper articulation with out of proper articulation with acetabulumacetabulum
– DislocatableDislocatable: ability to force femoral : ability to force femoral head out of articulation with acetabulum head out of articulation with acetabulum
– DislocatedDislocated: femoral head is not : femoral head is not articulating normally with the articulating normally with the acetabulum at baselineacetabulum at baseline

DDHDDH
DDH recently coined due to the DDH recently coined due to the progressiveprogressive nature of the problem, nature of the problem, ie. Many hips normal at birth, but ie. Many hips normal at birth, but become unstable during the ensuing become unstable during the ensuing weeks/monthsweeks/months

DDHDDH
Why worry?Why worry?– Premature degenerative joint diseasePremature degenerative joint disease– Impaired walkingImpaired walking– Chronic painChronic pain

DDHDDH
What other historical factors would What other historical factors would increase your suspicion?increase your suspicion?– Breech female: 20 per 1000Breech female: 20 per 1000– FHx + female: 12 per 1000FHx + female: 12 per 1000– Female, no risk factors: 5 per 1000Female, no risk factors: 5 per 1000– Breech male: 4 per 1000Breech male: 4 per 1000– Male, no risk factors: 0.3 per 1000Male, no risk factors: 0.3 per 1000
Bache CE, Clegg J, Herron, M. Risk factors for developmental Bache CE, Clegg J, Herron, M. Risk factors for developmental dysplasia of the hip: ultrasonographic findings in the dysplasia of the hip: ultrasonographic findings in the neonatla period. neonatla period. J Pediatr Orthop BJ Pediatr Orthop B. 2002; 11:212-218.. 2002; 11:212-218.

DDHDDH
Screening controversyScreening controversy– No direct evidence that screening No direct evidence that screening
improves functional outcomesimproves functional outcomes– Studies show Studies show ↓↓, unchanged, and , unchanged, and rates rates
of surgery among screened infantsof surgery among screened infants– Variable definitions of “positive”Variable definitions of “positive”– No gold standardNo gold standard– Poor quality evidence for effectiveness Poor quality evidence for effectiveness
of both non-surgical and surgical of both non-surgical and surgical treatmentstreatments

DDHDDH X-rayX-ray
– Femoral head does not ossify until 3-6 Femoral head does not ossify until 3-6 monthsmonths
– Radiographic outcomes have not been Radiographic outcomes have not been shown to be valid or reliable surrogate shown to be valid or reliable surrogate for functional outcomesfor functional outcomes

DDHDDH
UltrasoundUltrasound– High false positive rate (ie. high rate of High false positive rate (ie. high rate of
non-pathological hip findings)non-pathological hip findings)– Intraobserver reliability moderateIntraobserver reliability moderate– Interobserver reliability fairInterobserver reliability fair– May decrease unnecessary treatment May decrease unnecessary treatment
when compared to clinical exam alonewhen compared to clinical exam alone– Reliability of classification is Reliability of classification is
questionablequestionable

DDHDDH
AAP recommendations from 2000 AAP recommendations from 2000 still standstill stand– Screen during newborn period and each Screen during newborn period and each
subsequent WCC with physical examsubsequent WCC with physical exam– If exam findings abnormal or breech If exam findings abnormal or breech
female, obtain ultrasound at 1 month or female, obtain ultrasound at 1 month or when detected thereafterwhen detected thereafter

DDHDDH If pt deemed to have If pt deemed to have
possible DDH, ortho possible DDH, ortho referral recommendedreferral recommended
Initial treatment non-Initial treatment non-surgical surgical – typically Pavlik harness, typically Pavlik harness,
which has been shown which has been shown
to reduce rate of AVNto reduce rate of AVN

DDHDDH
Pavlik harness less successful: Pavlik harness less successful: – Bilateral DDH Bilateral DDH – True dislocation True dislocation – Age >8 weeks at initiationAge >8 weeks at initiation
Atalar H, Sayli U, Yavuz OY, et al. Indicators of Atalar H, Sayli U, Yavuz OY, et al. Indicators of successful use of the Pavlik harness in infants successful use of the Pavlik harness in infants with DDH. Int Ortho. Apr 2006; (epub ahead of with DDH. Int Ortho. Apr 2006; (epub ahead of print).print).

SummarySummary Case 1: Metatarsus AdductusCase 1: Metatarsus Adductus
– Forefoot adducted; most spont resolveForefoot adducted; most spont resolve Case 2: Talipes EquinovarusCase 2: Talipes Equinovarus
– 3 components; early splinting3 components; early splinting Case 3: Cong. Muscular TorticollisCase 3: Cong. Muscular Torticollis
– Head tilt; SCM mass early; stretchingHead tilt; SCM mass early; stretching Case 4: Arthrogryposis Multi. CongenitaCase 4: Arthrogryposis Multi. Congenita
– Multiple contractures; neuro vs non-neuro; Multiple contractures; neuro vs non-neuro; amyoplasia most common; splinting/casting in amyoplasia most common; splinting/casting in neonatal periodneonatal period
Case 5: Developmental Dysplasia of HipCase 5: Developmental Dysplasia of Hip– Screen at every WCC +/- ultrasound; ortho Screen at every WCC +/- ultrasound; ortho
referral if +; Pavlik harness highly successfulreferral if +; Pavlik harness highly successful

ReferencesReferences Alfonso, I, Papazian O, Paez JC, and Grossman, JA. Alfonso, I, Papazian O, Paez JC, and Grossman, JA.
Arthrogryposis Multiplex Congenita. Arthrogryposis Multiplex Congenita. International International PedsPeds. 2000; 15(4):197-204.. 2000; 15(4):197-204.
Freed SS, and Coulter-O’Berry C. Identification and Freed SS, and Coulter-O’Berry C. Identification and Treatment of congenital muscular torticollis in Treatment of congenital muscular torticollis in infants. infants. Jour of Pros and OrthoJour of Pros and Ortho. 2004; 16(45):18-23.. 2004; 16(45):18-23.
Hulme A. The management of congenital talipes Hulme A. The management of congenital talipes equinovarus. equinovarus. Early Human DevelopmentEarly Human Development. 2005; . 2005; 81:797-802.81:797-802.
Shipman SA, Helfand M, Moyer VA, and Yawn BP. Shipman SA, Helfand M, Moyer VA, and Yawn BP. Screening for developmental dysplasia of the hip: a Screening for developmental dysplasia of the hip: a systematic literature review for the US Preventive systematic literature review for the US Preventive Services Task Force. Services Task Force. PediatricsPediatrics 2006; 117:557-576. 2006; 117:557-576.
Weiner DS. Weiner DS. Pediatric Orthopedics for Primary Care Pediatric Orthopedics for Primary Care Physicians, Second EditionPhysicians, Second Edition. New York, NY: . New York, NY: Cambridge University Press; 2004Cambridge University Press; 2004