Embed Size (px)
Citation preview

CARDIOVASCULAR DISEASE IN THE NEONATE 0095-5108/01 $15.00 + .OO
NEONATAL CARDIAC SURGERY Anatomic, Physiologic, and
Technical Considerations
Tom R. Karl, MS, MD
For the pediatric cardiac surgeon, neonates are a special group. This is not just because of size considerations, but also the presence of dynamic fetal physiology and the relative immaturity of the lungs and the airway. Neonates are known to have a lower tolerance for the side effects of cardiopulmonary bypass (CPB). There are also some unique neonatal postoperative problems, such as necrotizing enterocolitis and intraventricular hemorrhage, that occur only rarely even in older infants. The age distribution for patients admitted to the Children’s Hospital of Philadelphia (CHOP) cardiac intensive care unit is shown in Table 1 for the years 1996 to 1999. The proportion of neonates is significant, and the investment of time and resources (expressed as patient-days) may be dysproportional. This distribution is typical of most large pediatric car- diac services worldwide, illustrating the importance of the neonatal co- hort.
Neonatal repair for all cardiac lesions is an attractive (but as yet unattainable) goal for the surgical team. At the present time we are obliged to consider both lesions that must be repaired in the absolute neonatal period (if survival is expected), and those for which later repair is an option. For the second category, as listed below, a great deal of surgical judgement is required to balance the risk of open heart surgery in the neonate against the risk of the lesion itself during temporization.
From the Division of Cardiothoracic Surgery, The Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania; and Cardiac Surgical Unit, Royal Children’s Hospital, Melbourne, Australia
CLINICS IN PERINATOLOGY
VOLUME 28 NUMBER 1 * MARCH 2001 159

160 KARL
Table 1. AGE, DISTRIBUTION OF PATIENTS ADMITTED TO THE CHILDREN’S HOSPITAL OF PHILADELPHIA CARDIAC ICU FROM 1996 TO 1999.
Age Group % Admissions YO Patient-Days
Neonates* Infants 1-5 y 5-18 y >18 y
20 29 22 22 7
36 29 14 13 8
‘The neonates were overrepresented in patient-days and expenditure.
Transposition of the great arteries (intact ventricular septum, ven-
Totally anomalous pulmonary venous drainage (especially ob-
Hypoplastic left heart syndrome* Aortic valve anomalies (critical aortic stenosis)‘ Aortic arch anomalies (critical coarctation of the arteries and inter-
Univentricular heart with transposition of the great arteries and
Ventricular septal defect (failure to thrive, uncontrolled congestive
Tetralogy of Fallot Truncus arteriosus Anomalous origin of the left coronary artery from the pulmonary
Aortopulmonary window Atrioventricular septal defect Double-outlet right ventricle and Taussig-Bing anomaly
Low-birth weight or premature infants are even more problematic. At the Royal Children’s Hospital (RCH) we analyzed the relative risks of surgery in neonates of low birth weight (1000 consecutive patients) using 2.5 kg for ~tratification.~~ Babies having complex repairs at weight less than 2.5 kg had a significantly higher operative risk (16.5% [CL 2.5% to 23%] versus 7.1% [CL 6.2% to 8%]) than larger babies in the same age group (P<0.006). Within the less than 2.5 kg cohort, we looked at risk factors for early mortality, which are noted in Table 2. The inference is that although some factors are outside the control of the surgeon, one cannot overstate the importance of adequate preoperative resuscitation and an expediently performed operation, which become more critical as size and gestational age decrease.
The outcome of neonatal heart surgery for most lesions has been steadily improving during the past two decades, and ironically, the need for late surgical revision has increased. Improved results are attributable to a number of factors, including speed and accuracy of diagnosis, adequacy of resuscitation, timing of the surgical procedure, evolution of
tricular septal defect)
structed forms)*
rupted aortic arch)*
subaortic stenosis*
heart failure
artery
‘Always requires neonatal repair if survival is expected.

NEONATAL CARDIAC SURGERY 161
Table 2. RISK FACTORS FOR OPERATIVE MORTALITY IN BABIES OPERATED AT WEIGHT LESS THAN 2.5 KG
Factor P Value
Cardiopulmonary bypass Univentricular physiology Metabolic acidosis preoperative Low cardiac output preoperative Age or weight Year Ischemic time Circulatory arrest time Associated medical problem
0.007 0.023 0.007 0.001 >0.05 >0.05 >0.05 >0.05 >0.05
surgical technique, intraoperative support systems, postoperative man- agement, biomedical technology, and institution of comprehensive long- term follow-up plans.
This article serves as an update on some issues relating to neonatal heart surgery. The first section deals with some selected general aspects of perioperative support. The second section discusses two representa- tive lesions that illustrate many of the problems encountered in neona- tal cardiac surgery: (1) transposition of the great arteries (TGA) and (2) hypoplastic left heart (HLHS). Data from the RCH, Melbourne (http://www.rch.unimelb.edu.au), CHOP (http://heart.chop.edu) and other units are included.
PERIOPERATIVE SUPPORT SYSTEMS
There are a number of problems related to the use of CPB in neonates. They relate to the priming volume, wide range of flows, extremes of temperature, duration of the procedure, and diathesis to- ward capillary leak syndrome and bleeding. For neonates, the author has used a fresh heparinized blood CPB prime and a hollow fiber or membrane ~xygenator.'~ The advantages of fresh heparinized blood prime include higher levels of 2,3-diphosphoglycerate, preservation of labile coagulation factors, preservation of platelet activity, and longer red blood cell life. One can avoid metabolic alkalosis caused by citrate metabolism, and the sodium and glucose load that contribute to the hyperosmolality of citrate-phosphate-dextrose preserved blood. The dis- advantage is that this blood has a limited bank life, usually 24
Alpha stat pH management is followed for cooling during neonatal open heart surgery. pH stat and alpha stat are mutually exclusive strate- gies. With pH stat, if blood is analyzed at 20°C one finds a normal pH and Pco2. If the same sample is analyzed at 37"C, one would expect an acidic pH with hypercarbia. With the alpha stat strategy, a sample analyzed at 20°C is alkalotic, with a pH of 7.7 and a Pco2 of 18. The same sample analyzed at 37°C shows pH of 7.4 and Pco2 of 40 mm. The theory is based on a change in blood pH for each degree centigrade of

162 KARL
- 0.0147. There are many important protein ionizing groups in the 6 to 8 pH range, including terminal NH, and imidazole. Alpha is defined as the ratio of nonionized to proteinated species, and alpha stat preserves this ratio. The pK, of alpha increases as the temperature falls, which can be offset if the Pcq falls and the pH rises, which is the alpha stat strategy. The theoretical advantage is the maintenance of tertiary and quaternary protein structure for biologically active proteins. A theoretical disadvantage is that with this degree of alkalosis cerebral blood flow is restricted and cooling may not be as effective as with the luxuriant cerebral blood flow afforded by a nonalkaline pH strategy. In practice, alpha stat has provided reliably good hemodynamic and neurologic results, but this is an important area of research and controversy still to be re~olved.~, 23
For most neonatal cases, full-flow CPB (150 mL/kg) is used for the entire operation, with aortic and bicaval cannulation. For operations involving arch reconstruction, circulatory arrest is usually required. The author has used cold crystalloid cardioplegia solution and topical cold saline for myocardial protection, but various cardioplegia solutions have been shown to generate similar results in neonatal cardiac surgery. Equally important to the content is the way in which cardioplegia is delivered. For antegrade cardioplegia in neonates, it is critically im- portant to maintain a physiologic aortic root pressure (30 to 40 mm Hg) to avoid poor distribution of cardioplegia (low pressure) or myocardial edema (high pressure).
Hemostasis is a particular problem in neonatal cardiac surgery. The author currently uses aprotinin for all complex neonatal repairs. Aproti- nin is a polyvalent enzyme inhibitor and modulator of the coagulation and inflammatory responses. It attenuates the release of some proin- flammatory cytokines after bypass (tumor necrosis factors-a, interleu- ken-1, and interleuken-6). Aprotinin is known to prevent coagulation, fibrinolysis, and platelet activation during or after CPB, and hemostatic benefit has been documented in numerous clinical studies. The disad- vantage is that aprotinin is a basic polypeptide of bovine origin with antigenic properties. Re-exposure should be avoided within 6 months of original exposure to avoid the risk of anaphylaxis. Our usual aprotinin dose is 10,000 KIU/kg for loading, which is repeated hourly during CPB. A small dose is given to test for allergy before administering the therapeutic dose.
Control of fluid accumulation is a critical point for safe conduct of neonatal heart operations. At CHOP modified ultrafiltration is univer- sally used following neonatal CPB, with the circuit shown in Figure 1. Over an average time of 20 minutes the perfusionist can usually remove the entire priming and cardioplegia volume, resulting in significant hemoconcentration. During this time one generally sees improvement in both systolic and diastolic function. There may also be a reduction in fluid retention, weight gain, and transfusion requirements. Modified ultrafiltration has been shown to attenuate the brain injury associated with prolonged circulatory arrest times. There is a predictable reduction

NEONATAL CARDIAC SURGERY 163
Figure 1. Modified ultrafiltration circuit used after cardiopulmonary bypass (CPB). The priming volume can usually be removed over a 20-minute period, with a predictable hemodynamic improvement and hemoconcentration. Flow = 30-60 mumin; filtrate = 300-400 rnL; and average time = 20 minutes.
in pulmonary artery pressure, which takes place concurrent to appear- ance of endothelin-1 in the ultrafiltrate. The benefits of modified ultrafil- tration have been demonstrated in a number of clinical and experimental studies.6
A peritoneal dialysis catheter is also useful following neonatal car- diac surgery. This catheter is placed selectively during complex neonatal operations, and postoperatively it is left on free drainage for abdominal decompression. There is evidence that interleukin-6 and interleukin-8 are concentrated in this fluid.3 For periods of reduced urine output or hyperkalemia, 10 mL/kg isotonic or hypertonic dialysate (30-minute exchange cycles) is used. The author also uses cold dialysis for core cooling for the treatment of postoperative hyperthermia, especially when associated with arrhythmias.
The physiology of the capillary leak syndrome seen after neonatal CPB operations is now reasonably well characterized, and is summa- rized in Figure 2. The initial common pathway is contact of circulating blood with surfaces of the CPB circuit. Control of this process has been difficult to achieve. We investigated the role of surface modification in the CPB circuit as a possible modulator of the inflammatory response. Patients undergoing open heart surgery were randomized into four groups: (1) heparin-bonded circuit, (2) heparin-bonded circuit with albu- min coating, (3) non-heparin-bonded circuit, and (4) non-heparin- bonded circuit with albumin coating. Interleukin-6 and interleukin-8 levels were measured at the start of CPB and 6 and 24 hours afterward (Fig. 3).'O We found a rise in both proinflammatory cytokines at the later time points, but when we compared the four groups using analysis of

Contact with CPB circuit
neutrophil activation, histamine, bradykinin, CRP, C3 release,
complement cascade P interleukins, TNF-a > NO synthetase -
accumulation of large molecules H,O in extravascular tissues .
r
Capillary Leak Syndrome
adhesion molecules (selectins E,P,L + integrins CD 11, 18) t
I
T
NO production -
Figure 3. Comparison of four CPB circuit types to characterize the effects of surface modification on generation of proinflammatory cytokines. These biochemical markers are predictive of postoperative morbidity in neonates. In each group: first bar = heparin bonded; second bar = heparin bonded plus albumin; third bar = non-heparin bonded; fourth bar = non-heparin bonded plus albumin. (From Horton SB, Butt WW, Mullaly RJ, et al: IL-6 and IL-8 levels after cardiopulmonary bypass are not affected by surface coating. Ann Thorac Surg 68:1751, 1999; with permission.)
164

NEONATAL CARDIAC SURGERY 165
variance, we could not find a significant difference relative to the type of surface preparation in the oxygenator. This suggests that if the in- flammatory response is indeed attenuated by the use of heparin-bonded or albumin preprimed circuits, then this does not occur through a decrease in interleukin-6 and interleukin-8 levels.
Inhaled nitric oxide has been an important development in neonatal cardiac surgery, perhaps the most useful drug to appear since prosta- glandin (PG) El. Nitric oxide is a selective and effective pulmonary vasodilator that is useful for postoperative pulmonary hypertension in neonates. There are some potential problems, including early develop- ment of nitric oxide dependence because of inhibition of exogenous nitric oxide production; difficulties for use long term in nonventilated children; response variability; cost; and concerns about the buildup of toxic metabolites, including NO2 and methemoglobin (rare in clinical practice at doses less than 30 ppm). There are parallel pathways, possibly synergistic, for effecting arterial smooth muscle relaxation (Fig. 4). For pulmonary vasodilatation in nitric oxide nonresponders, inhaled PGI, may be suitable therapy. PGI, can be added to the inspiratory limb of the ventilator circuit, and a clinical trial to evaluate this modality in postoperative cardiac patients is underway at RCH.
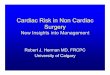
An interesting area of research pertinent to neonates undergoing complex cardiac operations is the prediction of major adverse events afterward in the ICU.8 Such events include cardiac arrest, need for emergency chest opening, sepsis, multiorgan failure, and death. We know that hypotension may be a late and unreliable sign, and that measurement of cardiac output is invasive, difficult, expensive, and unreliable in neonates. Figure 5 shows the predicted probability of a major adverse event following cardiac surgery based on the serum lactate level at 4 hours.8 There is a strong correlation, which was not found with the multiple other parameters examined. The as yet unan- swered question is whether treatment of elevated lactate in isolation can prevent the development of a major adverse event. This finding should prompt us to look carefully for less obvious manifestations of low cardiac output and to respond accordingly.
synergy? arachidonic
arteriolar smooth
u acid - PG12 -CAMP-
Figure 4. Parallel pathways for relaxation and arteriolar smooth muscle, both relevant for control of PHT in neonates post-CPB. There may be a therapeutic role for both nitric oxide and prostacyclin (PGI,) in some patients.

166 KARL
1.0 1
I I I I I I 0 2 4 6 a 10
Serum Lactate (mmol/L)
Figure 5. Probability of a major adverse event following open heart surgery, based on serum lactate levels in the ICU. Serum lactate at 4 hours had significant predictive value for adverse events. Based on 90 patients, median age of 27 months and median weight of 4.1 kg. (From Duke T, Butt W, South M, et al: Early markers of major adverse events in children after cardiac operations. J Thorac Cardiovasc Surg 114:1042, 1997; with permis- sion.)
MANAGEMENT OF SPECIFIC CARDIAC LESIONS
TGA and HLHS are prototype lesions for the neonatal cardiac surgeon. Both are complex from an anatomic point of view, but the early and long-term outcomes are markedly different. TGA is a fatal lesion that can nearly be cured with surgical treatment. HLHS, even more lethal untreated, can only be palliated for the long-term. Even with our best effort, the result of HLHS surgery can prove to be unpredictable. Nonetheless, there is a growing cohort of HLHS survivors enjoying growth, development, and a good quality of life, which often justifies the persistence of family and medical staff.26* 28 Points relevant to each anomaly are presented next as illustrations of current thinking about complex neonatal lesions.
Transposition of the Great Arteries
In the broad sense, the term TGA describes any heart with a discor- dant ventricular arterial connection (aorta from right ventricle [RV], pulmonary artery [PA] from left ventricle [LV]). The anatomic diagnosis

NEONATAL CARDIAC SURGERY 167
is further defined by the intracardiac features, such as ventricular septal defect (VSD), outflow obstruction, and so forth. The Taussig-Bing anom- aly is a double-outlet RV with subpulmonic VSD, which anatomically and physiologically closely resembles TGA with VSD.41
The diagnosis of TGA can be considered in almost any cyanotic newborn, but ECG, chest radiograph, and physical examination are not diagnostic. Two-dimensional echocardiography usually provides rapid and complete noninvasive diagnosis, and in the neonate cardiac catheter- ization is rarely necessary. Even the fine details of great vessel position, valve structure, and coronary anatomy can be provided at minimal stress to the baby (Fig. 6). All are important for surgical planning. Prenatal echo diagnosis of TGA is now possible, although knowing what to do with the information remains pr0b1ematic.l~
The central physiologic problem in TGA is arterial desaturation, the severity of which varies with the degree of communication between the parallel systemic and pulmonary circulations. The neonatal presentation varies from that of a healthy-appearing baby to complete cardiovascular collapse. At the worst end of the clinical spectrum are those babies with a restrictive atrial septal defect (ASD) or aortic arch obstruction, who are often profoundly hypoxemic and acidotic. The natural history of all forms of TGA is extremely unfavorable, and without some form of palliative or definitive surgery most neonates do not survive infancy. In most cases, the initial resuscitation efforts should include balloon atrial septostomy, irrespective of surgical plan.
Timing of operation is critical, especially for babies with TGA with intact ventricular septum (IVS). In extrauterine life, the pulmonary vas- cular resistance drops from its fetal (systemic) level to a normal postnatal level within 2 weeks. This decline is be accompanied by an involution of LV mass, unless a patent ductus arterious, VSD, or LV outflow tract
Figure 6. Intramural left coronary artery shown in cross-sectional echocardiogram. The proximal left coronary courses within the aortic wall. The ostium is eccentrically placed and frequently stenotic. This pattern is seen in about 5% of cases of transposition of the great arteries, and creates technical problems for excision. Echocardiography is useful for providing fine details of the anatomy at minimal stress to the neonate.

168 KARL
obstruction is present to maintain the LV pressure at systemic levels. The optimal time for the arterial switch operation (ASO) is within the first 2 weeks of life, if one is to avoid the problem of a deconditioned LV, which may contribute to low cardiac output po~toperatively.~ Infants with TGA and arch obstruction (and other PGE,-dependent patients) usually require operation within the first few days of life.16 In TGA-VSD, elective operation can usually be carried out at 1 to 3 months of age, if the clinical condition remains stable.
The goal of transposition surgery is to restore a series circulation with a four-chambered heart, using the LV and the systemic circuit in the RV and the pulmonary circuit. The AS0 is the standard treatment for transposition, affording both physiologic and anatomic correction with restoration of concordant arterioventricular and ventriculoarterial connections. The RV and tricuspid valve remain at pulmonary pressure, providing a hemodynamic advantage in the long term.
The technical AS0 modification used is a hybrid of techniques proposed by various authors.12, 13, 15, 16, 24, 38 With the heart arrested, the aorta and PA are transected just above the commissures (Fig. 7). The coronaries are excised with large cuffs of sinus tissue, and medially based rectangular flaps are cut into the facing sinuses of the PA. The mobilized coronaries are translocated and sutured in place. The neoaortic anastomosis is completed by gathering tissue on the proximal side to match the vessel sizes. At this point the VSD, if present, is closed with pledgetted mattress sutures and a glutaraldehyde-preserved autologous pericardial patch. The ASD is closed directly, and the heart is deaired. With the aortic clamp off, the neopulmonary sinus defects are repaired with individual autologous pericardial patches, extended posteriorly to lengthen the PA. The neopulmonary anastomosis is completed, the pa- tient is warmed to 37"C, then separated from CPB.
Special Problems in Sugery for Transposition of the Great Arteries
The Older Neonate with Transposition of the Great Arteries and Intact Ventricular Septum. Beyond 2 weeks of age, LV involution has usually begun, and concerns are raised regarding postoperative contrac- tility. An early AS0 study using pooled data suggested that the risk of AS0 increased beyond 7 days of age.19 This result led many centers to adopt a two-stage approach for children beyond 2 to 3 weeks of age, especially those with subnormal calculated LV mass or wall thickness.45 Postnatal myocardial growth is characterized by an early hyperplastic phase of myocytes and capillaries, followed by myocyte hypertrophy only. Pressure overload induces hypoplasia, hypertrophy, and angiogen- esis in neonates but only myocyte hypertrophy later on. The capacity and rapidity of LV hypertrophy may decrease dramatically with increas- ing age of the patient. Rapid LV hypertrophy has been documented in the early postoperative period.I5 The author offers primary AS0 to all children up to 8 weeks of age (and selectively to older children) irrespec-

NEONATAL CARDIAC SURGERY 169
’ Neopulmonary a
Figure 7. The AS0 technique using great vessel transection and medially based rectangu- lar flaps in the neoaortic sinuses for coronaly translocation. The flaps decrease the arc of rotation and prevent tension on the anastomosis. Neopulmonary sinus defects are repaired with large autologous pericardial patches, extended posteriorly. Concordant ventriculoarte- rial connections result. (From Karl TR: Transposition of the great arteries. In Nichols DG, Cameron DE [eds]: Critical Cardiac Disease in Infants and Children. St. Louis, Mosby-Year Book, 1994, p. 825; with permission.)
tive of LV pressure, geometry, or mass.15 Infants with TGA-IVS pre- senting between 8 weeks and 6 months of age are probably best treated with a two-stage AS0 strategy.l5< 45 The capacity of the LV to respond to a pressure load with hypertrophy in this age group makes rapid retraining (<2 weeks) possible. The first stage is transsternal PA band placement, accompanied by a 4-mm polytetrafluoroethylene (PTFE) in- nominate to right PA shunt to maintain oxygenation. Temporary low cardiac output following this procedure is common, but within 7 to 10 days the LV pressure and mass are usually adequate to allow AS0 without severe low cardiac output postoperatively. Within this time frame, adhesions are generally not too troublesome at resternotomy, and AS0 (with simple debanding and shunt division) can be performed as

170 KARL
described. In older patients, a more prolonged period of LV conditioning is usually required?8 Fortunately, such patients are unusual in today's practice.
Transposition of the Great Arteries with Aortic Arch Obstruction. Aortic arch obstruction, rare in TGA-IVS, complicates 7% to 10% of cases of TGA-VSD and Taussig-Bing anomaly5 The obstruction is most commonly a discrete coarctation with a hypoplastic transverse arch and isthmus?", 39 Closure of the ductus can precipitate profound cardiovascu- lar collapse in the neonate. The risk of nectrotizing enterocolitis and intraventricular hemorrhage is also increased as compared with other forms of TGA. Most patients with TGA and arch obstruction should have a one-stage neonatal repair by median sternotomy.16, l7
The Taussig-Bing Anomaly. For surgical purposes, the key question in double-outlet RV is whether the LV can be connected directly to the aorta by an intraventricular tunnel, or more directly connected to the PA. There are a number of operations that have been used for this latter situation, including atrial level and intraventricular repairs without ASO. The author's preference is ASO, performed within the first 3 months of life.15 A large pericardial or Dacron patch is used for septation to achieve an unobstructed pathway to the neoaorta, which has a biventricular origin, overriding the VSD. The neopulmonary artery anastomosis can be constructed on a branch PA, closing a portion of distal main PA, to compensate for a side-by-side vessel position.
Results of the Arterial Switch Operation
The RCH results of AS0 have varied according to anatomic subset. The lowest risk group consists of babies with TGA-IVS operated on within the first 3 weeks of life (mortality 0.970, CL = 0% to 3%). The risk of primary AS0 for infants in the 3- to 8-week age range compares favorably with that of a two-stage approach with pulmonary artery band (PAB) plus shunt.7 This risk also compares favorably with that of many other neonatal open heart procedures. The risk has been higher for the more complex TGA subsets!, 7, l2 Long-term follow-up of these TGA patients (>lo00 patient years) has shown that most children have experienced normal growth and development with a good quality of life following ASO. At RCH, there have been no late deaths in patients undergoing AS0 for TGA-IVS or TGA-VSD.
The operative risk of AS0 for 27 infants with Taussig-Bing anomaly was 7% (CL = 1% to 23%) and not increased for patients requiring concurrent aortic arch obstruction ( P = 1 .0).5 Actuarial survival and free- dom from reoperation at 72 months were likewise similar (E-0.05). The risk of AS0 for Taussig-Bing anomaly also compares very favorably with alternate surgical strategies used for similar patients.
The AS0 in biventricular hearts with TGA comes very close to being both a complete anatomic and physiologic correction. Most pa- tients (>%%) after ASO, at least those with the less complex variants, have normal resting LV function. Segmental perfusion abnormalities

NEONATAL CARDIAC SURGERY 171
may occasionally be seen on technetium 99m scans at rest, but they tend to improve with exercise. These defects are not predicted by ECG or echocardiography. LV end systolic wall stress and fiber shortening veloc- ity have been relatively normal, suggesting that contractility is not impaired. Importantly, these results are significantly better than the best published data concerning atrial level repairs:, 12, 42, 43 Aft er ASO, there is a tendency for great vessel (anastomotic) diameter to be smaller than that of controls, and for the neoaortic root to be larger. Reported risk factors for neoaortic root enlargement include the presence of neoaortic insufficiency, a previous PAB, and switch conversion after atrial repair. Concerns have been raised about aortic insufficiency, which develops in about 10% of patients following ASO. This is attributed to progressive dilation of the neopulmonary annulus, a phenomenon that has also been reported in other conditions in which the pulmonary valve is used in the systemic circulation. We looked at patients at a mean follow-up of 105 months, calculating the echocardiographic diameter of the neoaortic annulus and neopulmonary annulus (Fig. 8). We found that the neoaortic annulus was significantly larger than predicted (mean z score 2.59 k 2.7). If the regression was performed against a normal pulmonary annulus, however, the mean z score fell to 0.87 k 1.35. This difference was highly significant (P = 0.0001). In a multivariate analysis neither age at operation, weight at operation, follow-up interval, nor type of intracardiac anatomy were predictive of the z score. The median grade of aortic insufficiency in these patients was 0 (range, 0 to 2) and was not related to the annular z score using either the aorta or the
25, 31, 32,
mean = 2.59 * 2.7 mean = 0.87 f 1.35
'I U U I
Figure 8. Neoaortic diameter after AS0 based on 62 patients, 105 (84-180) months f/v. Regression against normal aortic controls suggests dilation, but using normal PA control values the mean z score is significantly lower. The neoaorta grows as would a normal pulmonary artery. P = 0.0001.

172 KARL
pulmonary artery as a control. These data suggest that the neoaorta does not dilate abnormally but rather grows as a normal pulmonary valve. The mechanism of the insufficiency may lie elsewhere.
Brain injury is an important problem in neonatal cardiac surgery, and it may be intimately connected to the conduct of CPB. In a landmark longitudinal study from Boston Children’s Hospital, infants with TGA were randomized at birth to a CPB strategy of predominantly circulatory arrest or low-flow (50 mL/kg/min) hypothermic CPB. When assessed in the first 48 hours postoperatively, there was an 11% incidence of clinical seizures and a 26% incidence of EEG-detected ictal activity. Both the use and duration of circulatory arrest were predictive of seizure activity ( P = 0.009 and 0.004).% At 1-year follow-up the circulatory arrest group scored lower on the Bayley Scales Infant Development (P = 0.01), again with an inverse relation to circulatory arrest time (P = O.O4).l At 4 years the circulatory arrest group scored lower in various areas of motor assessment. Seizures predicted a lower full-scale intelligence quotient (IQ) (odds ratio 8.4), although both groups had scores that fell below the population norms.*
Deep hypothermia with circulatory arrest is a useful and time- honored tool in cardiac surgery, but the types of patients for which it is essential form a vanishing cohort. Circulatory arrest per se is not a neuroprotective strategy and based on the studies cited there seems to be no completely safe duration. Certainly, it is not a requirement for most ASOs. It is tempting to think that CPB at a higher temperature with full flow and minimization of circulatory arrest provides a better neurodevelopmental outcome, although such a study has not been per- formed in a randomized and prospective manner.
We investigated neurodevelopmental outcome in a cohort of 74 patients and 74 ”best friend” controls (Karl et al, unpublished data). Intent to treat was advoidance of low flow or circulatory arrest whenever possible except for closure of the ASD (median 6 minutes). Survivors who had been followed for 48 months or longer were assessed with a battery of standardized neurodevelopmental tests and review of periop- erative data. In the immediate perioperative period, the overall incidence of detectable neurologic abnormalities was 20% (CL = 12% to 31%), usually transient and minor events. Clinically detectable seizures oc- curred in 6.8% of patients (CL = 2% to 15%), but in most cases they had developed before surgery. We were unable to demonstrate predictive value for parameters relating to birth weight; age; preoperative condi- tion; conduct of bypass; or operative strategy (P>O.l for all). Head circumference percentiles were similar for patients and controls. In- telligence testing with Wechsler scales appropriate for age (WIPPSI, WISC-2) suggested that although controls had a higher full-scale IQ (P = 0.0018), means for both groups fell into the normal range. The differences were more pronounced in children who were examined after 76 months of age ( P = 0.0032 vs P = 0.2889). Among variables relating to family, preoperative status, intraoperative factors, and postoperative course, only educational level of the father and a neurologic abnormality

NEONATAL CARDIAC SURGERY 173
in the perioperative period had predictive value. The multivariate R2 was 0.33, suggesting that other factors besides those accepted in the model may have been operative. These results compare favorably with those of other published series using different perioperative strategies, and the continued use of full-flow CPB with minimal or no circulatory arrest for AS0 could be justified by the findings of the study.
Hypoplastic Left Heart Syndrome
Hypoplastic left heart syndrome is one of the most challenging lesions for the surgical team, and in the current era success with surgery for this entity is the standard by which cardiac teams are judged. Presently, a corrective operation for HLHS is not possible and staged palliation provides the best chance of long-term survival. The recon- structive strategy is to perform the Norwood operation (also termed stage 1 reconstruction) in the immediate neonatal period to stabilize the baby in preparation for a bidirectional cavopulmonary shunt at 3 to 6 months of age. Following this, the two circulations can be separated electively after 1 to 2 years of age with the use of a modified Fontan procedure. Schematic diagrams of the native HLHS circulation compared with the Norwood circulation, the bidirectional cavopulmonary circula- tion, and the Fontan circulation are shown in Figure 9. In this section some aspects of neonatal treatment of HLHS are discussed.
The diagnosis of HLHS can be made with fetal echocardiography. This information, if provided early enough, presents an option for termi- nation of pregnancy, which is often considered justified in view of the uncertain long-term outcome. HLHS is an eminently treatable lesion, however, and excellent results have now been obtained in many patients.
HLHS is in the differential diagnosis of cyanosis of the newborn, although there are no pathognomic clinical findings. If the diagnosis has not been established prenatally, it is readily made with echocardiography in the immediate postnatal period. Cardiac catheterization is rarely nec- essary, because all of the details can usually be obtained rapidly and safely with a good transthoracic echocardiogram.
The anatomy and pathophysiology are complex, involving both restriction of systemic blood flow and excessive pulmonary blood flow in varying degrees. Interatrial communication and ductal patency are essential (Figs. 9 and 10). The presentation varies from a healthy-ap- pearing baby to that of complete cardiovascular collapse. The arterial duct is maintained with a PGE, infusion. Resuscitation may also require the use of inotropes, bicarbonate infusion, and mechanical ventilation. Pulmonary blood flow can be limited by avoidance of added oxygen, or in some cases with controlled hypercarbia, and an hypoxic (0, and N2) mixture in the inspired gases. The use of venous and arterial umbilical catheters for preoperative and intraoperative management is recom- mended, avoiding excessive manipulation of the baby, while providing reliable central access. Although the details of medical management are

174 KARL
I RV
A
+ RV
SVC IVC B
, Common atrium

NEONATAL CARDIAC SURGERY 175
I A I I , ,
Venous collaterals I I
I I I
B I
Arterial collaterals
PA
A fenestration < ___..._._._ + Atrium
svc IVC
*I--& Figure 9 Continued.

176 KARL
Figure 10. Anatomy and typical hemodynamics for HLHS at presentation. Clinical condition varies from relative (temporary) stability to cardiovascular collapse. (From Wernovsky G, Bove E: Single ventricle lesions. In Chang AC, Hanley FL, Wernovsky G, et al [eds]: Pediatric Intensive Care. Baltimore, Williams & Wilkins, 1998, p 271 ; with permission.)
beyond the scope of this article, suffice it to say that the emphasis is on complete resuscitation rather than emergency surgery. With current practice it is rare to commence operation without established urine output, stable hemodynamics, and complete resolution of acidosis.
The only consistently useful initial reconstructive procedure for HLHS is the Norwood n per at ion.^^ The goals of this procedure are as follows:
1.
2.
3.
Establishment of an unobstructed connection between the RV and systemic circulation. This requires connection of the MPA to aorta, with extensive enlargement of ascending, transverse, and descending aorta. Creation of a reliable controlled source of pulmonary blood flow: This is usually done with interposition of a PTFE tube between innominate artery and right PA. Establishment of free communication between pulmonary veins and RA: Because the left atrium in HLHS usually has no egress by the mitral valve, creation of a large ASD is required.
The Norwood operation is performed using hypothermic (18°C) CPB by the PA and right atrium with a period of circulatory arrest for

NEONATAL CARDIAC SURGERY 177
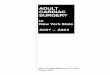
arch construction (Fig. 11). It is also possible to perform the operation in modified form without the use of circulatory arrest.21 During this time a right modified Blalock-Taussig shunt is constructed using a 3- to 4-mm thin-walled PTFE graft. The circulation is arrested and cardioplegia is given through the aortic cannula. The ductus is divided, and the main PA is transected just above the valve commissures. The distal end of the PA is closed with a patch of allograft PA. A second larger triangular patch is used to reconstruct the ascending aorta after all ductal tissue has been excised. The reconstruction is carried down to the ascending aorta, which is joined to the PA to create a large confluence of vessels connecting RV to the diminutive ascending aorta and the aortic arch. This type of reconstruction allows for normal growth of the aorta through ~hildhood.,~ The operation can also be performed without any added patch material, using direct anastomosis. The ASD is enlarged to the maximum. The patient is warmed and weaned from CPB, main- taining oxyhemoglobin saturation in the 70% to 80% range with the systemic systolic pressure 60 to 70 mm. The priming volume is removed with modified ultrafiltration. Delayed sternal closure (48 hours) may be useful.
An unstable postoperative circulation is usually a consequence of low systemic output, which can be partly caused by excessive pulmo- nary blood flow. One should focus therapeutic maneuvers on improving systemic blood flow rather than just decreasing pulmonary blood flow, because a patient with low systemic out and low Po, becomes even more unstable. Low-dose inotropes, phosphodiesterase inhibitors, and addition of CO, or N2 to the inspired gases are all useful measures. A more detailed discussion of postoperative management can be found elsewhere.44
For babies who survive the Norwood operation, a subsequent stage of surgery is performed at 3 to 6 months. This is generally the bidirec- tional cavopulmonary shunt or the hemi-Fontan operation (Fig. 12). The second-stage surgery has a much lower risk than the first and usually sets up a stable interim circulation. Fontan operation can be performed as an elective third stage in patients who have unacceptable hemoglobin saturation or who are otherwise symptomatic (Fig. 13). A technical description of the second and third stages can be found in several excellent surgical texts.'I
The results of 840 Norwood operations performed at CHOP have recently been summarized by Mahle et a1.28 Patient weight ranged from 1.4 to 5.8 kg, and 38% of the infants had both aortic and mitral atresia. Other diagnostic categories included aortic atresia with mitral stenosis, aortic stenosis with mitral stenosis, unbalanced AV septa1 defect, and other HLHS variants. The 10-year acturarial survival for patients oper- ated between 1984 and 1998 was 40% There were 304 deaths at the first stage (36.2%); 36 at the second stage (10.4%); and 46 at the Fontan stage (13.6%). Risk factors for operative death following the Norwood procedure included age greater than 2 weeks ( P = 0.004); weight less than 2.5 kg ( P = 0.01); and an earlier era of surgery ( P = 0.001). In

Figure 11. See legend on opposite page
178

NEONATAL CARDIAC SURGERY 179
other reported series, risk factors for early mortality have included small size of the ascending aorta (less than 3 mm); aortic atresia; mitral atresia; restrictive ASD; impaired tricuspid valve and RV function; and poor general preoperative condition of the baby. Ischemic time and ascend- ing aortic diameter figured importantly in the RCH series ( P = 0.033 and P = 0.021, respectively).
A meta-analysis of Norwood operation results reported worldwide between 1998 and 2000 is shown in Table 3 (n = 1642). The global stage I early mortality for reporting institutions was 32% (CL = 29% to 34%). This is likely to be an underestimate of true risk, because units with poorer results are unlikely to publish their data. There has been a trend toward improvement in our own results over the past 15 years, and for the period 1995 to 1998 stage I survival at CHOP was 71.3% stage I1 loo%, and stage I11 100%. In 1999, 80% of patients survived the stage I operation. Between 1984 and 1998, however, 75 patients experienced interstage mortality during follow-up. The causes of interstage and late death included recurrent arch obstruction, pleural effusions, sepsis, respiratory infections, RV failure, and sudden death.
Exercise testing following the third stage of surgery for HLHS patients was performed by Joshi et al.I4 HLHS patients performed in a fashion similar to Fontan patients with other types of univentricular anatomy, suggesting that the HLHS cohort were not hindered by RV dependence or other anatomic factors. Mahle et alZ6 examined neurode- velopmental outcome following surgery for HLHS. Seventy-nine percent of parents questioned assessed their child’s health as good or excellent, but 82% were felt to have average or below average academic perfor- mance. Sixty-four percent received regular medication. The median full- scale IQ was 86 (range, 50 to 116).
The competitive strategy for treatment of HLHS is neonatal cardiac transplantation, and there has been a great interest in this procedure over the past 15 years. Transplantation may in fact be preferable to staged reconstruction for certain subsets of HLHS, which can be identi- fied preoperatively as being unlikely to have good result with the Nor- wood operation. If xenotransplantation or graft tolerance can be achieved in the future, transplantation could become a preferred option for many other types of congenital heart disease, but currently we must rely on immunosuppressive therapy. Tacrolimus (FK 506) has been shown to have advantages over cyclosporine in pediatric heart trans- plantation. Tacrolimus-treated children have similar LV function, less
Figure 11. Technique of the Norwood operation. A, Association of the main PA with the ascending, transverse, and descending aorta. B, The main PA is closed distally. C, A patch of pulmonary arterial allograft wall is used to enlarge the connection. D, Pulmonary blood flow is provided by a modified Blalock-Taussig shunt, and an atrial septectomy is also performed. (From Castaneda AR, Jonas RA, Mayer JE: Hypoplastic left heart syndrome. In Castaneda AR, Jonas RA, Mayer JE, et al [eds]: Cardiac Surgery of the Neonate and Infant. Philadelphia, WB Saunders, 1994, p 363.)

180 KARL
Figure 12. The hemi-Fontan operation is used as the second stage. The SVC return is diverted into the pulmonary arteries, and the IVC return supplies the common atrium. Pulmonary artery enlargement is accomplished concurrently. (From Spray TL: Fenestrated Fontan for hypoplastic left heart syndrome. Operative Techniques in Cardiac and Thoracic Surgery 2:239, 1997; with permission.)
Illustration continued on opposite page

NEONATAL CARDIAC SURGERY 181
Figure 12 Continued.

182 KARL
Figure 13. The Fontan operation for HLHS as a completion procedure following the hemi- Fontan. All caval blood is diverted into the pulmonary circulation. Many technical variations are in use. (From Spray TL: Fenestrated Fontan for hypoplastic left heart syndrome. Operative Techniques in Cardiac and Thoracic Surgery 2:239, 1997; with permission.)

NEONATAL CARDIAC SURGERY 183
rejection, lower steroid doses, and fewer side effects with comparable patient and graft survival rates. This may make transplantation a more acceptable option, but the donor availability problem remains critical for children with HLHS who are supported with prostaglandin infusion and waiting. Pooled results of heart transplantation in children have been summarized for 1999 by the International Society for Heart Lung Tran~plantation.~~ For infants operated in the first year of life, 30-day survival was 79.39'0, 12-month survival 69.3%, and 60-month survival 60%. In considering these figures one must take into account the attrition on the waiting list, which varies enormously in different parts of the world. This may be quite significant, and transplantation may not even be an option in some parts of the world. Morrow et a133 looked at data for 118 infants awaiting transplantation. At the end of 6 months, 6% remained on the list, 59% had a transplant, 31% had died waiting, and 4% were d e l i ~ t e d . ~ ~ The greatest mortality risk was for infants with HLHS, who had a 77% mortality if they did not receive a transplant. Statistically speaking, the chance of survival to 5 years may be better in most units with a Norwood strategy, which is our strong preference at CHOP. There are of course many other considerations, and volumes have been written on this subject.
In conclusion, the surgical strategies for HLHS have improved con- siderably over the past decade to the point where it is justifiable to offer active treatment to most families. The long-term outlook is still uncer- tain, and there is a significant attrition rate between stages. The outcome of the Fontan operation for patients with HLHS is similar to that for other types of univentricular anatomy. It is likely that continued im- provements in management and refinement of techniques will result in a better outcome in both the short and long term. The outcome of the Norwood operation is better than most would have anticipated 15 years ago, with minimal late attrition for children who have survived to the third stage.
References
1. Bellinger DC, Jonas RA, Rappaport LA, et al: Developmental and neurologic status of children after heart surgery with hypothermic circulatory arrest or low-flow cardiopul- monary bypass. N Engl J Med 332549, 1995
2. Bellinger DC, Wypij D, Kuban KC, et al: Developmental and neurological status of children at 4 years of age after heart surgery with hypothermic circulatory arrest or low-flow cardiopulmonary bypass. Circulation 100:526, 1999
3. Bokesch PM, Kapural MB, Mossad EB, et al: Do peritoneal catheters remove proin- flammatory cytokines after cardiopulmonary bypass in neonates? Ann Thorac Surg 70:639, 2000
4. Brawn WJ, Mee RBB Early results for anatomic correction of transposition of the great arteries and for double outlet right ventricle with subpulmonary ventricular septa1 defect. J Thorac Cardiovasc Surg 95930, 1988
5. Comas JV, Mignosa C, Cochrane AD, et al: Taussig-Bing anomaly and arterial switch: Aortic arch obstruction does not influence outcome. Eur J Cardiothorac Surg 10:1114, 1996
6. Davies MJ, Nguyen K, Gaynor JW, et al: Modified ultrafiltration improves left ventricu-

184 KARL
lar systolic function in infants after cardiopulmonary bypass. J Thorac Cardiovasc Surg et a1 115:361, 1998
7. Davis AM, Wilkinson JL, Karl TR, et al: Transposition of the great arteries with intact ventricular septum: Arterial switch repair in patients 21 days of age or older. J Thorac Cardiovasc Surg 106:111, 1993
8. Duke T, Butt W, South M, et al: Early markers of major adverse events in children after cardiac operations. J Thorac Cardiovasc Surg 114:1042, 1997
9. du Plessis AJ, Jonas RA, Wypij D, et al: Perioperative effects of alpha-stat versus pH- stat strategies for deep hypothermic cardiopulmonary bypass in infants. J Thorac Cardiovasc Surg 114:991, 1997
10. Horton SB, Butt WW, Mullaly RJ, et al: IL-6 and IL-8 levels after cardiopulmonary bypass are not affected by surface coating. Ann Thorac Surg 68:1751, 1999
11. Jacobs M. Hypoplastic left heart syndrome. In Kaiser LR, Kron IL, Spray TL (eds): Mastery of Cardiothoracic Surgery. Philadelphia, Lipincott-Raven, 1998, p 858
12. Jatene AD, Fontes VF, Paulista PP, et al: Anatomic correction of transposition of the great vessels. J Thorac Cardiovasc Surg 72364, 1976
13. Jatene AD, Fontes VF, Paulista PP, et a1 Successful anatomic correction of transposition of the great vessels: A preliminary report. Arq Bras Cardiol28461, 1975
14. Joshi VM, Carey A, Simpson P, et al: Exercise performance following repair of hypo- plastic left heart syndrome: A comparison with other types of Fontan patients. Pediatr Cardiol 18:357, 1997
15. Karl TR Transposition of the great arteries. In Nichols DG, Cameron DE (eds): Critical Cardiac Disease in Infants and Children. St. Louis, Mosby-Year Book, 1994, p. 825
16. Karl TR, Sano S, Brawn W, et al: Repair of hypoplastic or interrupted arch via stemotomy. J Thorac Cardiovasc Surg 104688, 1992
17. Karl TR, Watterson K, Sano S, et a1 Operations for subaortic stenosis in univentricular hearts. Ann Thorac Sura 52:420, 1991
18
19
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
Kirklin JW, Barratt-Boy& BG: Complete transposition of the great arteries. In Kirklin JW, Barratt-Boyes BG (eds): Cardiac Surgery. New York, Churchill-Livingstone, 1993, p 1383 Kirklin JW, Blackstone EH, Tchervenkov CI, et al: Clinical outcomes after the arterial switch operation for transposition, patient support, procedural, and institutional risk factors. Circulation 863501, 1992 Kirklin JW, Colvin EV, McConnell ME, et al: Complete transposition of the great arteries: Treatment in the current era. Pediatr Clin North Am 37171, 1990 Kishimoto H, Youichi K, Kawata H, et a1 The modified Norwood palliation on a beating heart. J Thorac Cardiovasc Surg 118:1130, 1999 Kramer HH, Rammos S, Krian A, et al: Intermediate-term clinical and hemodynamic results of the neonatal arterial switch operation for complete transposition of the great arteries. Int J Cardiol 36:13, 1992 Kurth CD, ORourke MM, OHara I B Comparison of pH-stat and alpha-stat cardiopul- monary bypass on cerebral oxygenation and blood flow in relation to hypothermic circulatory arrest in piglets. Anesthesiology 89110, 1998 Lecompte Y, Zannini L, Hazan E, et al: Anatomic correction of transposition of the great arteries. J Thorac Cardiovasc Surg 82:629, 1981 Lupinetti FM, Bove EL, Mimich LL, et al: Intermediate-term survival and functional results after arterial repair for transposition of the great arteries. J Thorac Cardiovasc Surg 103421,1992 Magle WT, Clancy RR, Moss EM, et al: Neurodevelopmental outcome and lifestyle assessment in school-aged and adolescent children with hypoplastic left heart syn- drome. Pediatrics 105:1082, 2000 Mahle WT, Rychik J, Weinberg PM, et al: Growth characteristics of the aortic arch after the Norwood operation. J Am Coll Cardiol21951, 1998 Mahle WT, Spray TL, Wemovsky G, et al: Survival after palliative surgery for hypo- plastic left heart syndrome 15-year experience from a single institution. Circulation, in press Mee RBB. The arterial switch operation. In Stark J, De Leva1 MR (eds): London, WB Saunders, 1994, p 483

NEONATAL CARDIAC SURGERY 185
30. Milanesi 0, Thiene G, Bini RM, et al: Complete transposition of great arteries with coarctation of aorta. Br Heart J 48:566, 1982
31. Minet P, Vaksmann G, Rey C, et al: Doppler echocardiography after anatomical repair of transposition of the great vessels. Arch Ma1 Coeur Vaiss 85:515, 1992
32. Moat NE, Pawade A, Lamb RK: Complex coronary arterial anatomy in transposition of the great arteries: Arterial switch procedure without coronary relocation. J Thorac Cardiovasc Surg 103:872, 1992
33. Morrow WR, Naftel D, Chinnock R, et al: Outcome of heart lung transplantation in infants younger than six months: Predictors of death and interval to transplantation. The Pediatric Heart Transplantation Study Group. J Heart Lung Transplant 16:1255, 1997
34. Newburger JW, Jonas RA, Wernovsky G, et al: A comparison of the perioperative neurologic effects of hypothermic circulatory arrest versus low-flow cardiopulmonary bypass in infant heart surgery. N Engl J Med 329:1057, 1993
35. Norwood WI Jr: Hypoplastic left heart syndrome. Ann Thorac Surg 52688, 1991 36. Pawade A, Karl TR, Laussen P, et al: Cardiopulmonary bypass in infants weighing
less than 2.5kg: Analysis of risk factors for early and late survival. J Card Surg 81,1993 37. Pediatric Heart and Lung Transplantation: SHLT Heart and Lung Registry. http://
www.ishlt.org/ishlt 38. Quaegebeur JM: The arterial switch operation: Rationale, results and perspectives
[thesis]. Leiden, The Netherlands, Leiden University, 1986 39. Schneeweiss A, Motro M, Shem-Tov A, et al: Subaortic stenosis: An unrecognised
problem in transposition of the great arteries. Am J Cardiol 48:336, 1981 40. Serraf A, Bruniaux J, Lacour-Gayet F, et al: Anatomic repair of Taussig-Bing hearts.
Circulation 84:III200, 1991 41. Taussig HB, Bing RJ: Complete transposition of the aorta and a levoposition of the
pulmonary artery. Am Heart J 37551, 1949 42. Veelken N, Gravinghoff L, Keck EW, et al: Improved neurological outcome following
early anatomical correction of transposition of the great arteries. Clin Cardiol 15275, 1992
43. Vouhe PR, Tamisier D, Leca F, et al: Transposition of the great arteries, ventricular septa1 defect and pulmonary outflow tract obstruction: Rastelli or Lecompte procedure? J Thorac Cardiovasc Surg 103:428, 1992
44. Wernovsky G, Bove E: Single ventricle lesions. In Chang AC, Hanley FL, Wemovsky G, et a1 (eds): Pediatric Intensive Care. Baltimore, Williams & Wilkins, 1998, p 271
45. Yacoub MH, Radley-Smith R, Maclaurin R Two-stage operation for anatomical correc- tion of transposition of the great arteries with intact ventricular septum. Lancet 1:1275, 1977
Address reprint request to Tom R. Karl, MS, MD
Cardiac Surgical Division The Children’s Hospital of Philadelphia
34th and Civic Center Boulevard Philadelphia, PA 19106
e-mail: karl @chop.edu