Embed Size (px)
Citation preview
NECK SOFT TISSUE PERINEUROMA IN A CHILDSean Callahan, MD, Seckin Ulualp, MD
Department of Otolaryngology-Head and Neck Surgery University of Texas Southwestern Medical Center, Dallas, Texas
Children’s Medical Center, Dallas, Texas
Perineuromas are uncommon, solid, well circumscribed, slowly growing tumors composed of well-differentiated perineural cells. Two variants of perineuromas are recognized: the intraneural perineuromasoccurring within a nerve, and the soft tissue perineuromas, which includes a sclerosing subset of tumors.
Soft tissue perineuromas were originally described by Lazarus and Trombetta in 1978 as a benign peripheral nerve sheath tumor distinct from schwannomas and neurofibromas. Soft tissue perineuromasoccur most commonly in the subcutis of the extremities and trunk of young to middle-aged adults. Neck soft tissue perineuroma in a child has not been reported
The medical record of a 13-year-old female with perineuroma of neck soft tissue was reviewed. Data included relevant history and physical examination, diagnostic work up and management.
BACKGROUNDABSTRACT
Objectives: The aim of the present study was to describe clinical, radiologic, and histological features of a neck soft tissue perineuroma in a child.
Study Design: Case review
Methods: Chart of a 13-year-old girl referred to a tertiary care pediatric hospital for assessment of neck mass was reviewed. Data included relevant history and physical examination, diagnostic work up, and management.
Results: The child has been having a neck mass located on level 5 for 5 months. Parents noticed that the mass appeared after having an upper respiratory tract infection. She was diagnosed with lymphadenopathy. After receiving an unknown antibiotic, the mass has not resolved. The mass had slowly increased in size. Physical examination revealed a well-appearing child in no respiratory distress. There was a neck mass located on level five. Palpation of the mass showed smooth, rubbery, nontender, and nonpulsatilemass. The mass appeared to be attached to skin. MR imaging documented subcutaneous, well-defined lesion in the supraclavicular region just posterior to the sternocleidomastoid muscle. The mass showed intense uniform enhancement. Upon resection of the mass, histologic evaluation showed well circumscribed, unencapsulated cellular lesion that focally entraps dermal appendages. The lesion was strongly positive for CD34, GLUT-1, EMA and Claudin. Focal positivity was also present in SMA and S-100. Calponin and Factor 13a were negative. The final diagnosis was soft tissue perineuroma. At 10 month follow-up, the surgical site was healed with no evidence of recurrence.
Conclusions: Soft tissue perineuroma, a rare and slowly growing tumor, needs to be considered in the differential diagnosis of neck mass in children.
METHODS
RESULTS
RESULTS
CONCLUSIONS
• Neck soft tissue perineuroma may occur in children
• Otolaryngologists and pathologists should be aware of the occurrence of
these tumors in the pediatric age group.
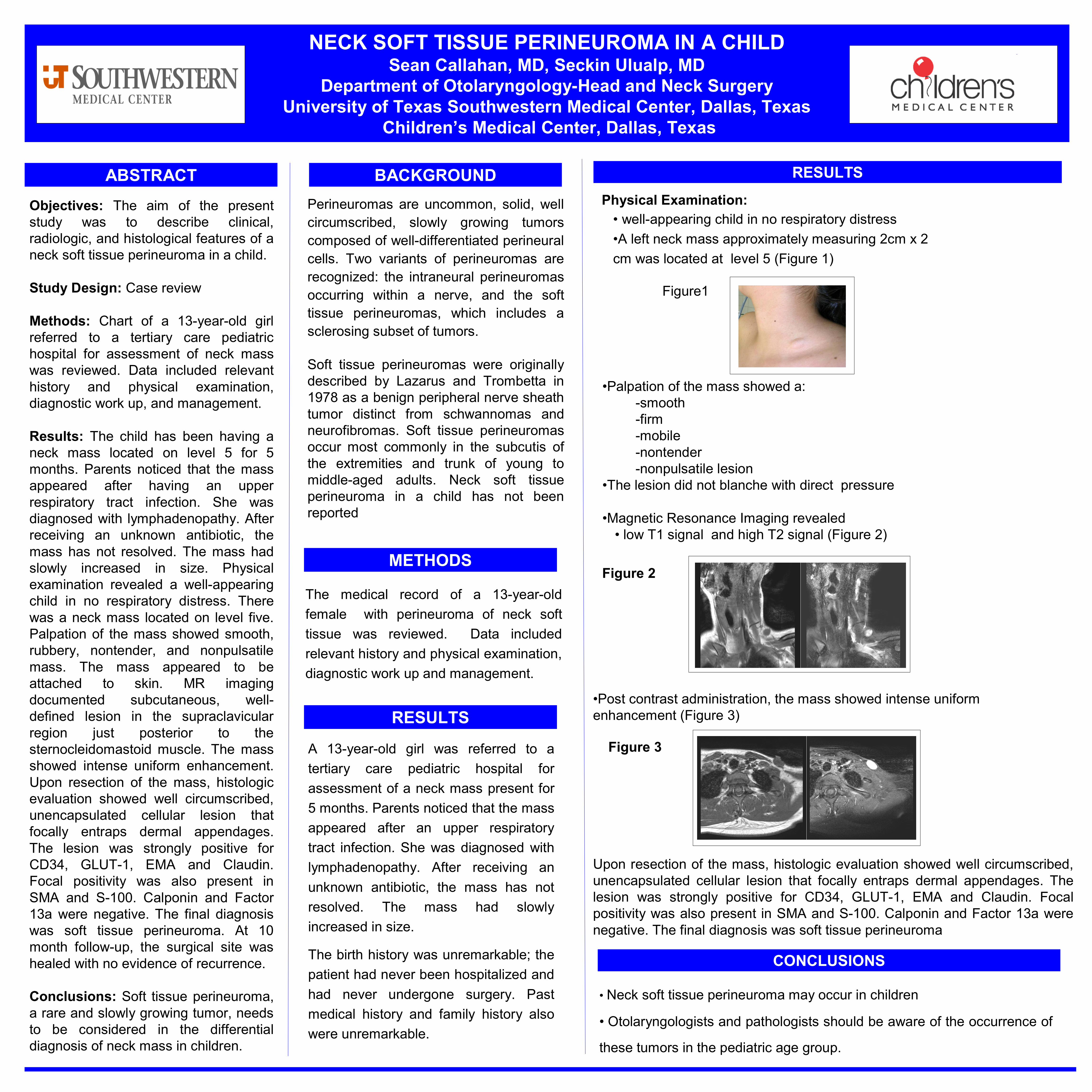
Figure 2
Figure 3A 13-year-old girl was referred to a tertiary care pediatric hospital for assessment of a neck mass present for 5 months. Parents noticed that the mass appeared after an upper respiratory tract infection. She was diagnosed with lymphadenopathy. After receiving an unknown antibiotic, the mass has not resolved. The mass had slowly increased in size.
The birth history was unremarkable; the patient had never been hospitalized and had never undergone surgery. Past medical history and family history also were unremarkable.
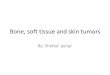
Physical Examination:• well-appearing child in no respiratory distress•A left neck mass approximately measuring 2cm x 2 cm was located at level 5 (Figure 1)
Figure1
•Palpation of the mass showed a: -smooth-firm-mobile-nontender-nonpulsatile lesion
•The lesion did not blanche with direct pressure
•Magnetic Resonance Imaging revealed • low T1 signal and high T2 signal (Figure 2)
•Post contrast administration, the mass showed intense uniform enhancement (Figure 3)
Upon resection of the mass, histologic evaluation showed well circumscribed, unencapsulated cellular lesion that focally entraps dermal appendages. The lesion was strongly positive for CD34, GLUT-1, EMA and Claudin. Focal positivity was also present in SMA and S-100. Calponin and Factor 13a were negative. The final diagnosis was soft tissue perineuroma