Embed Size (px)
Citation preview
NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice
(835) Billing and Payment Scenarios
Version 1.1
All material is provided "as is", without warranty of any kind, expressed or implied, including but not limited to warranties of merchantability, fitness for a particular purpose, accuracy, completeness and non-infringement of third party rights. In no event shall NCPDP, its members or its contributors be liable for any claim, or any direct, special, indirect or consequential damages, or any damages whatsoever resulting from loss of use, data or profits, whether in an action of contract, negligence or other tortious action, arising out of or in connection with the use or performance of the material. NCPDP recognizes the confidentiality of certain information exchanged electronically through the use of its standards. Users should be familiar with the federal, state, and local laws, regulations and codes requiring confidentiality of this information and should utilize the standards accordingly. NOTICE: In addition, this NCPDP Standard contains certain data fields and elements that may be completed by users with the proprietary information of third parties. The use and distribution of third parties' proprietary information without such third parties' consent, or the execution of a license or other agreement with such third party, could subject the user to numerous legal claims. All users are encouraged to contact such third parties to determine whether such information is proprietary and if necessary, to consult with legal counsel to make arrangements for the use and distribution of such proprietary information.
Published by:
National Council for Prescription Drug Programs
Publication History: Version 1.0 January 2013 Version 1.1 March 2017
All rights reserved. National Council for Prescription Drug Programs
9240 E. Raintree Drive Scottsdale, AZ 85260
(480) 477-1000 [email protected]

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 2 of 58 March 2017
Contents
1. Document Scope ................................................................................................................................... 4
2. Purpose ................................................................................................................................................ 6
3. NCPDP Telecommunication Standard vD.0 Billing and Response and X12/005010X221A1 Health Care Claim Payment/Advice (835) Remittance Examples ....................................................................................... 7
3.1 NCPDP Telecommunication Standard vD.0 General Assumptions: .................................................. 7
3.2 X12/005010X221A1 835 General Assumptions: ............................................................................. 7
4. Examples .............................................................................................................................................. 8
4.1 Typical Claim ................................................................................................................................ 8 4.1.1 1A Billing Transaction ........................................................................................................................... 8 4.1.2 1B Billing Response Transaction .......................................................................................................... 9 4.1.3 835 for vD.0 Billing Response 1B ......................................................................................................... 9 4.1.4 1C Reversal Transaction ..................................................................................................................... 10 4.1.5 1D Reversal Response Transaction .................................................................................................... 10 4.1.6 835 for vD.0 Reversal Response 1D (Out of Cycle) ............................................................................ 11
4.2 Retroactive Billing .......................................................................................................................12 4.2.1 2A Billing Transaction ......................................................................................................................... 12 4.2.2 2B Billing Response Transaction ........................................................................................................ 13 4.2.3 835 for vD.0 Billing Response 2B ....................................................................................................... 13
4.3 Claim Submitted – DUR/PPS Reject – Claim Submitted With DUR – Paid .......................................15 4.3.1 3A Billing Transaction ......................................................................................................................... 15 4.3.2 3B Billing Response Transaction ........................................................................................................ 15 4.3.3 3C Billing Transaction with DUR ......................................................................................................... 16 4.3.4 3D Billing Response Transaction ........................................................................................................ 17 4.3.5 835 for vD.0 Billing Response 3D ....................................................................................................... 17
4.4 COB Claim Submission to Secondary Insurance .............................................................................19 4.4.1 4A Billing Transaction ......................................................................................................................... 19 4.4.2 4B Billing Response Transaction ........................................................................................................ 20 4.4.1 835 for vD.0 Billing Response 4D ....................................................................................................... 20
4.5 COB Claim Submission with Other Coverage Code of 8 and Patient Pay Amount Reported as Returned from Primary Payer ..................................................................................................................22
4.5.1 5A Billing Transaction ......................................................................................................................... 22 4.5.2 5B Billing Response Transaction ........................................................................................................ 23 4.5.3 835 for vD.0 Billing Response 5B ....................................................................................................... 23
4.6 Billed With Tax – Paid – Patient Is Responsible For Part of Tax Causing Patient Pay to Increase by Amount of Tax .........................................................................................................................................25
4.6.1 6A Billing Transaction ......................................................................................................................... 25 4.6.2 6B Billing Response Transaction ........................................................................................................ 26 4.6.3 835 for vD.0 Billing Response 6B ....................................................................................................... 26
4.7 Billed With Tax – Paid ..................................................................................................................28 4.7.1 7A Billing Transaction ......................................................................................................................... 28 4.7.2 7B Billing Response Transaction ........................................................................................................ 29 4.7.3 835 for vD.0 Billing Response 7B ....................................................................................................... 29

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 3 of 58 March 2017
4.8 Multi-Ingredient Compound - Payable ..........................................................................................31 4.8.1 8A Billing Transaction ......................................................................................................................... 31 4.8.2 8B Billing Response Transaction ........................................................................................................ 32 4.8.4 835 for vD.0 Billing Response 8B ....................................................................................................... 33
4.9 Patient is not Cardholder .............................................................................................................34 4.9.1 9A Billing Transaction ......................................................................................................................... 34 4.9.3 9B Billing Response Transaction ........................................................................................................ 35 4.9.4 835 for vD.0 Billing Response 9B ....................................................................................................... 35
4.10 Paid Claim with Patient Pay Components .....................................................................................37 4.10.1 10A Billing Transaction .................................................................................................................. 37 4.10.2 10B Billing Response Transaction .................................................................................................. 38 4.10.3 835 for vD.0 Response 10B ............................................................................................................ 38
4.11 Discount Card with Membership Fee ............................................................................................40 4.11.1 11A Billing Transaction .................................................................................................................. 40 11B Billing Response Transaction ................................................................................................................... 41 4.11.2 835 for vD.0 Response 11B ............................................................................................................ 41
4.12 Prior Authorization ......................................................................................................................43 4.12.1 12A Claim Submission .................................................................................................................... 43 4.12.2 12B Rejection – Requires Prior Authorization ............................................................................... 44 4.12.3 12C Submission with Prior Authorization ...................................................................................... 44 4.12.4 12D Paid – Lower Amount with an Incentive ................................................................................ 45 4.12.6 835 for vD.0 Response 12D: .......................................................................................................... 46
4.13 Worker’s Compensation Claim Submission ...................................................................................48 4.13.1 13A Workers’ Compensation Billing .............................................................................................. 48 13B Workers’ Compensation Billing Accepted Response— Paid .................................................................... 49 4.13.3 835 for vD.0 Response 13B: ........................................................................................................... 49
4.15 Health Savings Account (HSA) Claim Submission ...........................................................................51 4.15.1 14A Claim Submission .................................................................................................................... 51 4.15.2 14B Claim Paid ............................................................................................................................... 52 4.15.3 835 Response for vD.0 Response 14B: .......................................................................................... 52
4.16 Other Payment Information for the 835 (Paper Claims) ................................................................54 4.16.1 Paper Claim A ................................................................................................................................. 54 4.16.2 Paper Claim B ................................................................................................................................. 55
5. Discussion ...........................................................................................................................................57
6. Revision History ...................................................................................................................................58
NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 4 of 58 March 2017
1. Document Scope Users of this document should consult the NCPDP documents listed below for further information and clarification.
DATA DICTIONARY
Full reference to all data elements with definition, sizes, and values used in NCPDP documents.
EXTERNAL CODE LIST
Full reference to values used in the NCPDP standard.
STANDARDS MATRIX
This document contains charts that list the Standards and Implementation Guides versions approved or under consideration by NCPDP, with reference to the Data Dictionary and External Code List documents appropriate for use.
TELECOMMUNICATION STANDARD AND TELECOMMUNICATION STANDARD IMPLEMENTATION GUIDE
The NCPDP Telecommunication Standard and NCPDP Telecommunication Standard Implementation Guide Version D.0 define the record layout for real-time prescription claim transactions between providers and adjudicators. Since the communication between these parties is two-way, the record layout for both the transmitted claim and the response to the claim are defined by the Version D.0 guide. The NCPDP Batch Standard Implementation Guide uses the NCPDP Telecommunication Standard format for the Detail Record of the file.
PHARMACY REFERENCE GUIDE TO THE X12/005010X221A1 HEALTH CARE CLAIM PAYMENT/ADVICE (835)
This document provides rules to support the use of the X12 835 005010X221A1 between business partners. This document must be used in conjunction with the X12/005010X221A1 Health Care Claim Payment/Advice (835). This document does not supersede 005010X221A1. There are other fields that must be populated that are not included in this document. . This only addresses claims using the NCPDP transactions or pharmacy paper claim forms. This document provides the pharmacy industry specific field information as it relates to the NCPDP Telecommunication Standard vD.0. Information found in this document has met the X12 intellectual property and fair use policy requirements.
CLAIM ADJUSTMENT REASON CODE/NCPDP REJECT CODE MAPPING SPREADSHEET
This document provides information on the use of Claim Adjustment Reason Code (CARC) and NCPDP Reject Codes in the X12/005010X221A1 Health Care Claim Payment/Advice (835) for the pharmacy industry. This mapping document provides specific situations for the use of appropriate Claim Adjustment Reason Code (CARC), Claim Adjustment Group Code and NCPDP Reject Codes for the pharmacy industry when using the NCPDP Telecommunication Standard vD.0 and pharmacy paper claims.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 5 of 58 March 2017
NCPDP IMPLEMENTATION GUIDANCE FOR THE X12/005010X221A1 HEALTH CARE CLAIM PAYMENT/ADVICE (835)
This document contains guidance to the pharmacy industry to prepare for the implementation of the X12 835.
Other documents cited in this document:
X12 INFORMATION
The X12 Technical Report 3 documents (TR3) are available at www.x12.org.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 6 of 58 March 2017
2. Purpose The Purpose of this document is to provide a round-trip picture of the prescription drug claim utilizing the HIPAA named NCPDP Telecommunication Standard Version D.0 through the use of hypothetical scenarios initiated by a pharmacy provider, including submissions, reversal, and resubmissions. Each scenario is paired with the pharmacy initiated transaction and the processor response, including paid and rejected. A companion document details HIPAA X12/005010X221A1 Health Care Claim Payment/Advice (835) payment and remittance files (corresponding to the pharmacy initiated transactions within this document) that would be received by the pharmacy provider.
Authors This document is the result of an ongoing effort the NCPDP Work Group 45 External Standards Assessment, Harmonization and Implementation Guidance.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 7 of 58 March 2017
3. NCPDP Telecommunication Standard vD.0 Billing and Response and X12/005010X221A1 Health Care Claim Payment/Advice (835) Remittance
Examples
3.1 NCPDP Telecommunication Standard vD.0 General Assumptions: • Scenarios may exist to show both of the following situations:
o within one payment cycle and o Out of (“crossing”) payment cycle so these can be detailed on the 835 (or NOT included as the case
may be). • The claim date payment cycles are:
o Cycle 1 – 01/17/2010 through 01/23/2010 o Cycle 2 – 01/24/2010 through 01/30/2010
• Two paper claims are included in order to show how these are included in the 835. • The prescription number and other information in the claim will not uniquely identify the service
without providing the refill number and the payer has optionally include both in the CLP01 by reporting the prescription number, the characters ”FILL” followed by the refill number. Example: CLP01 = 12345FILL3.
3.2 X12/005010X221A1 835 General Assumptions: • The 835 examples show that the payer is creating the 835 in response to a Telecommunication Version
D.0 claim. • The 835 is being created based on claim cycle end date
Cycle 1 – 835 creation date is 01/30/2010 Cycle 2 – 835 creation date is 02/06/2010
• Scenarios may exist to show both of the following situations: • within one payment cycle and • out of (“crossing”) payment cycle
This will allow the claims to be detailed on the 835 (or NOT included as the case may be). • The claim payment cycles are (based on date claim received):
Cycle 1 – 01/17/2010 through 01/23/2010 Cycle 2 – 01/24/2010 through 01/30/2010
• Two paper claims are included in order to show how these are included in the 835. • Since a claim may be submitted with both an Rx number and a fill number, the examples will show the
reference to the Rx. Number as follows: • Store A will just have the Rx number used in the CLP01 field • Store B will have the Rx number followed by “FILL” followed by the fill number – i.e.
1234567FILL01 The use of the Rx number and fill number in the CLP01 field should be provided by the payer in one of the formats as agreed upon in Trading Partner Agreements or as defined in the Payer’s Companion Guide.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 8 of 58 March 2017
4. Examples
4.1 Typical Claim The claim is paid without any necessary interventions and without edits/additional requirements applied by the payer. Then pharmacy then finds it necessary to initiate a reversal of the claim out of cycle which likewise processes in a normal manner.
4.1.1 1A Billing Transaction TRANSACTION HEADER SEGMENT
Field Field Name Value Comments 101-A1 BIN NUMBER 610066 102-A2 VERSION RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100122 January 22, 2010 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
PATIENT SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 01 Patient Segment 304-C4 DATE OF BIRTH 19620615 Born June 15, 1962 305-C5 PATIENT GENDER CODE 1 Male 310-CA PATIENT FIRST NAME MICKEY Mickey is patient’s first name 311-CB PATIENT LAST NAME SMITH Smith is patient’s last name
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 987654321 Cardholder ID
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123456789012 436-E1 PRODUCT/SERVICE ID QUALIFIER 03 National Drug Code (NDC) 407-D7 PRODUCT/SERVICE ID 00006094228 Clinoril 200mg 442-E7 QUANTITY DISPENSED 30000 30.000 tablets 403-D3 FILL NUMBER 0 Original dispensing 405-D5 DAYS SUPPLY 30 30 Days supply 406-D6 COMPOUND CODE 1 Not a compound 408-D8 DISPENSE AS WRITTEN (DAW)/PRODUCT SELECTION 0 No Product Selection Indicated 414-DE DATE PRESCRIPTION WRITTEN 20100122 January 22, 2010
PRESCRIBER SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 03 PRESCRIBER SEGMENT 466-EZ PRESCRIBER ID QUALIFIER 01 National Provider Identifier (NPI) 411-DB PRESCRIBER ID 5556667772
PRICING SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 11 PRICING SEGMENT 409-D9 INGREDIENT COST SUBMITTED 657{ $65.70 412-DC DISPENSING FEE SUBMITTED 30{ $3.00 426-DQ USUAL AND CUSTOMARY CHARGE 707{ $70.70 430-DU GROSS AMOUNT DUE 687{ $68.70 423-DN BASIS OF COST DETERMINATION 1 AWP (Average Wholesale Price)

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 9 of 58 March 2017
4.1.2 1B Billing Response Transaction RESPONSE HEADER SEGMENT
Field Field Name Value Comments 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100122 January 22, 2010
RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS P Paid 503-F3 AUTHORIZATION NUMBER ABC12345
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 22 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER QUALIFIER 1 Rx Billing 402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123456789012
RESPONSE PRICING SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 23 Response Pricing Segment 505-F5 PATIENT PAY AMOUNT 100{ $10.00 506-F6 INGREDIENT COST PAID 657{ $65.70 507-F7 DISPENSING FEE PAID 30{ $3.00 509-F9 TOTAL AMOUNT PAID 587{ $58.70 522-FM BASIS OF REIMBURSEMENT DETERMINATION 1 Ingredient Cost Paid as Submitted
4.1.3 835 for vD.0 Billing Response 1B CLP – Claim Payment Information Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “123456789012” – Rx Number CLP02 1029 Claim Status Code ID 1/2 "1" - Processed as primary CLP03 782 Monetary Amount (Total Claim Charge
Amount) R 1/18 “68.70”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 "58.70” CLP05 782 Monetary Amount (Patient Responsibility
Amount) R 1/18 “10.00”
CLP06 1032 Claim Filing Indicator Code ID 1/2 "13” - Point of Service CLP07 127 Reference Identification (Payer Claim Control
Number) AN 1/30 "ABC12345"
NM1 – Patient Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "QC" NM102 1065 Entity Type Qualifier ID 1/1 "1" - Person NM103 1035 Name Last or Organization Name AN 1/35 “SMITH” NM104 1036 Name First AN 1/25 "MICKEY” NM108 66 Identification Code Qualifier ID 1/2 "MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “987654321”
NM1 – Service Provider Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "82" – Rendering Provider NM102 1065 Entity Type Qualifier ID 1/1 "2" – Non-Person Entity
NM103 1035 Name Last or Organization Name (Pharmacy Name) AN 1/35 “STORE A”
NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI) NM109 67 Identification Code AN 2/80 “1112223330” - NPI

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 10 of 58 March 2017
SVC – Service Payment Information Ref Elem Description Type Min/Max Data
SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 "00006094228"
SVC02 782 Monetary Amount (Monetary Amount (Line Item Charge Amount)) R 1/18 “68.70”
SVC03 782 Monetary Amount (Line Item Provider Payment Amount) R 1/18 "58.70”
SVC05 380 Quantity (Unit of Service Paid Count) R 1/18 “30” DTM – Service Date
Ref Elem Description Type Min/Max Data DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20100122”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “PR” – Patient Responsibility CAS02 1029 Adjustment Reason Code ID 1/5 “3" - Co-payment amount CAS03 782 Monetary Amount (Adjustment Amount) R 1/18 “10.00”
4.1.4 1C Reversal Transaction TRANSACTION HEADER SEGMENT
Field Field Name Value Comments 101-A1 BIN NUMBER 610066 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B2 Reversal 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100122 January 22, 2010 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 987654321 Cardholder ID
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER QUALIFIER 1 Rx Billing 402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123456789012 436-E1 PRODUCT/SERVICE ID QUALIFIER 03 National Drug Code (NDC) 407-D7 PRODUCT/SERVICE ID 00006094228 Clinoril 200mg
4.1.5 1D Reversal Response Transaction RESPONSE HEADER SEGMENT
Field Field Name Value Comments 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B2 Reversal 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI)
201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100122 January 22, 2010
TRANSACTION RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS A Accepted
RESPONSE CLAIM SEGMENT

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 11 of 58 March 2017
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 22 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER QUALIFIER 1 Rx Billing 402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123456789012
4.1.6 835 for vD.0 Reversal Response 1D (Out of Cycle)1 CLP – Claim Payment Information
Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “123456789012” – Rx Number CLP02 1029 Claim Status Code ID 1/2 "22" - Reversal CLP03 782 Monetary Amount (Total Claim Charge
Amount) R 1/18 “-68.70”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 "-58.70” CLP06 1032 Claim Filing Indicator Code ID 1/2 "13” - Point of Service CLP07 127 Reference Identification (Payer Claim Control
Number) AN 1/30 "ABC12345"
NM1 – Patient Name Ref Elem Description Type Min/Max Data NM101 98 Entity Identifier Code ID 2/3 "QC" NM102 1065 Entity Type Qualifier ID 1/1 "1" - Person NM103 1035 Name Last or Organization Name AN 1/35 “SMITH” NM104 1036 Name First AN 1/25 "MICKEY” NM108 66 Identification Code Qualifier ID 1/2 "MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “987654321”
NM1 – Service Provider Name Ref Elem Description Type Min/Max Data NM101 98 Entity Identifier Code ID 2/3 "82" – Rendering Provider NM102 1065 Entity Type Qualifier ID 1/1 "2" – Non-Person Entity NM103 1035 Name Last or Organization Name (Pharmacy
Name) AN 1/35 “STORE A”
NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI) NM109 67 Identification Code AN 2/80 “1112223330” - NPI
SVC – Service Payment Information Ref Elem Description Type Min/Max Data SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 "00006094228" SVC02 782 Monetary Amount (Monetary Amount (Line
Item Charge Amount)) R 1/18 “-68.70”
SVC03 782 Monetary Amount (Line Item Provider Payment Amount)
R 1/18 "-58.70”
SVC05 380 Quantity (Unit of Service Paid Count) R 1/18 “30”
DTM – Service Date Ref Elem Description Type Min/Max Data
DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20100122”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “PR” – Patient Responsibility CAS02 1029 Adjustment Reason Code ID 1/5 “3" - Co-payment amount CAS03 782 Monetary Amount (Adjustment Amount) R 1/18 “-10.00”
1 Accredited Standards Committee X12, Insurance Subcommittee, X12N. “10.1.2 Data Use by Business Use” Health Care Claim Payment/Advice (835), 005010X221A1. Washington Publishing Company, Apr. 2006. <http://www.wpc-edi.com>.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 12 of 58 March 2017
4.2 Retroactive Billing The prescription was originally filled as cash with a date of service is November 15, 2009, but on January 22, 2010 the patient presents a benefit card asking for the prescription to be billed to the Prescription Benefit Manager (PBM). The claim is paid by the PBM without any necessary interventions and without edits or additional requirements applied by the payer.
4.2.1 2A Billing Transaction Billing submitted on January 22, 2010 for claim that was FILLED on November 15, 2009. Patient originally paid for Prescription but now is retroactively covered by plan.
TRANSACTION HEADER SEGMENT Field Field Name Value Comments
101-A1 BIN NUMBER 610066 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI)
201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20091115 November 15, 2009 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
PATIENT SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 01 Patient Segment 304-C4 DATE OF BIRTH 19650724 Born July 24, 1965 305-C5 PATIENT GENDER CODE 2 Female 310-CA PATIENT FIRST NAME AMANDA Amanda is patient’s first name 311-CB PATIENT LAST NAME JONES Jones is patient’s last name
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 111222333 Cardholder ID
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER QUALIFIER 1 Rx Billing 402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 191456712548 436-E1 PRODUCT/SERVICE ID QUALIFIER 03 National Drug Code (NDC) 407-D7 PRODUCT/SERVICE ID 00006094228 Clinoril 200mg 442-E7 QUANTITY DISPENSED 30000 30.000 tablets 403-D3 FILL NUMBER 0 Original dispensing 405-D5 DAYS SUPPLY 30 30 Days supply 406-D6 COMPOUND CODE 1 Not a compound 408-D8 DISPENSED AS WRITTEN (DAW)/PRODUCT SELECTION
CODE 0 No Product Selection Indicated
414-DE DATE PRESCRIPTION WRITTEN 20091114 November 14, 2009 PRESCRIBER SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 03 Prescriber Segment 466-EZ PRESCRIBER ID QUALIFIER 01 National Provider Identifier (NPI) 411-DB PRESCRIBER ID 5556667772
PRICING SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 11 Pricing Segment 409-D9 INGREDIENT COST SUBMITTED 657{ $65.70 412-DC DISPENSING FEE SUBMITTED 30{ $3.00 426-DQ USUAL AND CUSTOMARY CHARGE 707{ $70.70 430-DU GROSS AMOUNT DUE 687{ $68.70 423-DN BASIS OF COST DETERMINATION 1 AWP (Average Wholesale Price)

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 13 of 58 March 2017
4.2.2 2B Billing Response Transaction RESPONSE HEADER SEGMENT
Field Field Name Value Comments 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20091115 November 15, 2009
RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS P Paid 503-F3 AUTHORIZATION NUMBER ABC12346
RESPONSE CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 22 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER QUALIFIER 1 Rx Billing 402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 191456712548
RESPONSE PRICING SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 23 Response Pricing Segment 505-F5 PATIENT PAY AMOUNT 100{ $10.00 506-F6 INGREDIENT COST PAID 647{ $64.70 507-F7 DISPENSING FEE PAID 30{ $3.00 509-F9 TOTAL AMOUNT PAID 577{ $57.70 522-FM BASIS OF REIMBURSEMENT DETERMINATION 6 MAC Pricing Ingredient Cost Reduced to MAC
4.2.3 835 for vD.0 Billing Response 2B2 CLP – Claim Payment Information
Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “191456712548” – Rx Number CLP02 1029 Claim Status Code ID 1/2 "1" - Processed as primary CLP03 782 Monetary Amount (Total Claim Charge
Amount) R 1/18 “68.70”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 "57.70” CLP05 782 Monetary Amount (Patient Responsibility
Amount) R 1/18 “10.00”
CLP06 1032 Claim Filing Indicator Code ID 1/2 "13” - Point of Service CLP07 127 Reference Identification (Payer Claim Control
Number) AN 1/30 "ABC12346"
NM1 – Patient Name Required Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "QC" NM102 1065 Entity Type Qualifier ID 1/1 "1" - Person NM103 1035 Name Last or Organization Name AN 1/35 “JONES” NM104 1036 Name First AN 1/25 "AMANDA” NM108 66 Identification Code Qualifier ID 1/2 "MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “111222333”
NM1 – Service Provider Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "82" – Rendering Provider NM102 1065 Entity Type Qualifier ID 1/1 "2" – Non-Person Entity NM103 1035 Name Last or Organization Name AN 1/35 “STORE A” NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI)
2 Accredited Standards Committee X12, Insurance Subcommittee, X12N. “10.1.2 Data Use by Business Use” Health Care Claim Payment/Advice (835), 005010X221A1. Washington Publishing Company, Apr. 2006.<http://www.wpc-edi.com>.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 14 of 58 March 2017
NM109 67 Identification Code (Rendering Provider Identifier)
AN 2/80 “1112223330” - NPI
SVC – Service Payment Information Ref Elem Description Type Min/Max Data
SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 "00006094228" SVC02 782 Monetary Amount (Line Item Charge
Amount) R 1/18 “68.70”
SVC03 782 Line Item Provider Payment Amount R 1/18 "57.70”
SVC05 380 Unit of Service Paid Count R 1/18 “30”
DTM – Service Date Ref Elem Description Type Min/Max Data
DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20091115”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “CO” – Contractual Obligations CAS02 1029 Adjustment Reason Code ID 1/5 “90" - Ingredient Cost Adjustment CAS03 782 Monetary Amount R 1/18 “1.00”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “PR” – Patient Responsibility CAS02 1029 Adjustment Reason Code ID 1/5 “3" - Co-payment amount CAS03 782 Monetary Amount R 1/18 “10.00”

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 15 of 58 March 2017
4.3 Claim Submitted – DUR/PPS Reject – Claim Submitted With DUR – Paid A submitted claim is rejected with a DUR/PPS response instructing the pharmacy to dispense a formulary product. The provider then submits the same claim with DUR/PPS codes indicating the actions performed (consulted prescriber) and the results of such actions (filled as is).
4.3.1 3A Billing Transaction TRANSACTION HEADER SEGMENT
Field Field Name Value Comments 101-A1 BIN NUMBER 610066 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 4445556661bbbbb Store B 401-D1 DATE OF SERVICE 20100122 January 22, 2010 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
PATIENT SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 01 Patient Segment 304-C4 DATE OF BIRTH 19620615 Born June 15, 1962 305-C5 PATIENT GENDER CODE 1 Male 310-CA PATIENT FIRST NAME CASPER Casper is patient’s first name 311-CB PATIENT LAST NAME MILLER Miller is patient’s last name
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 121212121 Cardholder ID
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER QUALIFIER 1 Rx Billing 402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 1234571 436-E1 PRODUCT/SERVICE ID QUALIFIER 03 National Drug Code (NDC) 407-D7 PRODUCT/SERVICE ID 00006094228 Clinoril 200mg 442-E7 QUANTITY DISPENSED 30000 30.000 tablets 403-D3 FILL NUMBER 0 Original dispensing 405-D5 DAYS SUPPLY 30 30 Days supply 406-D6 COMPOUND CODE 1 Not a compound 408-D8 DISPENSED AS WRITTEN (DAW)/PRODUCT SELECTION
CODE 0 No Product Selection Indicated
414-DE DATE PRESCRIPTION WRITTEN 20100122 January 22, 2010 PRICING SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 11 Pricing Segment 409-D9 INGREDIENT COST SUBMITTED 657{ $65.70 412-DC DISPENSING FEE SUBMITTED 30{ $3.00 426-DQ USUAL AND CUSTOMARY CHARGE 707{ $70.70 430-DU GROSS AMOUNT DUE 687{ $68.70 423-DN BASIS OF COST DETERMINATION 1 AWP (Average Wholesale Price)
4.3.2 3B Billing Response Transaction RESPONSE HEADER SEGMENT
Field Field Name Value Comments 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Standard 103-A3 TRANSACTION CODE B1 Billing 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI)

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 16 of 58 March 2017
201-B1 SERVICE PROVIDER ID 4445556661bbbbb Store B 401-D1 DATE OF SERVICE 20100122 January 22,2010
RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS R Rejected 510-FA REJECT COUNT 1 1 Reject Code follows 511-FB REJECT CODE 88 DUR Reject Error
RESPONSE CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 22 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER QUALIFIER 1 Rx Billing 402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 1234571
RESPONSE DUR/PPS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 24 Response Dur/PPS Segment 567-J6 DUR/PPS RESPONSE CODE COUNTER 1 1st DUR conflict 439-E4 REASON FOR SERVICE CODE PS Product Selection Opportunity 544-FY DUR FREE TEXT USE FORMULARY PRODUCT: Max field size is 30 so using both fields to convey
request. 570-NS DUR ADDITIONAL TEXT IBUPROFEN
4.3.3 3C Billing Transaction with DUR TRANSACTION HEADER SEGMENT
Field Field Name Value Comments 101-A1 BIN NUMBER 610066 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI)
201-B1 SERVICE PROVIDER ID 4445556661bbbbb
Store B
401-D1 DATE OF SERVICE 20100122 January 22, 2010 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
PATIENT SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 01 Patient Segment 304-C4 DATE OF BIRTH 19620615 Born June 15, 1962 305-C5 PATIENT GENDER CODE 1 Male 310-CA PATIENT FIRST NAME CASPER Casper is patient’s first name 311-CB PATIENT LAST NAME MILLER Miller is patient’s last name
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 121212121 Cardholder ID
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER QUALIFIER 1 Rx Billing 402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 1234571 436-E1 PRODUCT/SERVICE ID QUALIFIER 03 National Drug Code (NDC) 407-D7 PRODUCT/SERVICE ID 00006094228 Clinoril 200mg 442-E7 QUANTITY DISPENSED 30000 30.000 tablets 403-D3 FILL NUMBER 0 Original dispensing 405-D5 DAYS SUPPLY 30 30 Days supply 406-D6 COMPOUND CODE 1 Not a compound 408-D8 DISPENSED AS WRITTEN (DAW)/PRODUCT SELECTION
CODE 0 No Product Selection Indicated
414-DE DATE PRESCRIPTION WRITTEN 20100122 January 22, 2010 PRICING SEGMENT

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 17 of 58 March 2017
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 11 Pricing Segment 409-D9 INGREDIENT COST SUBMITTED 657{ $65.70 412-DC DISPENSING FEE SUBMITTED 30{ $3.00 426-DQ USUAL AND CUSTOMARY CHARGE 707{ $70.70 430-DU GROSS AMOUNT DUE 687{ $68.70 423-DN BASIS OF COST DETERMINATION 1 AWP (Average Wholesale Price)
DUR/PPS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 08 DUR/PPS Segment 473-7E DUR/PPS CODE COUNTER 1 1st DUR action 439-E4 REASON FOR SERVICE CODE PS Product Selection Opportunity 440-E5 PROFESSIONAL SERVICE CODE M0 Prescriber consulted 441-E6 RESULT OF SERVICE CODE 1B Filled Prescription As Is
4.3.4 3D Billing Response Transaction Processor accepts pharmacist’s DUR submission and pays claim OVER Submitted Amount. The claim pays Ingredient Cost as submitted AND an Incentive Payment for the DUR effort.
RESPONSE HEADER SEGMENT Field Field Name Value Comments
102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Standard 103-A3 TRANSACTION CODE B1 Billing 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 4445556661bbbbb Store B 401-D1 DATE OF SERVICE 20100122 January 22, 2010
RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS P Paid Response
RESPONSE CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 22 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER QUALIFIER 1 Rx Billing 402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 1234571
RESPONSE PRICING SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 23 Response Pricing Segment 505-F5 PATIENT PAY AMOUNT 100{ $10.00 506-F6 INGREDIENT COST PAID 650{ $65.00 507-F7 DISPENSING FEE PAID 30{ $3.00 521-FL INCENTIVE AMOUNT PAID 50{ $5.00 509-F9 TOTAL AMOUNT PAID 630{ $63.00 522-FM BASIS OF REIMBURSEMENT DETERMINATION 1 Ingredient Cost Paid as Submitted
4.3.5 835 for vD.0 Billing Response 3D3 CLP – Claim Payment Information
Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “1234571FILL 0” – Rx Number and Fill Number CLP02 1029 Claim Status Code ID 1/2 "1" - Processed as primary CLP03 782 Monetary Amount (Total Claim Charge
Amount) R 1/18 “68.70”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 "63.00” CLP05 782 Monetary Amount (Patient Responsibility
Amount) R 1/18 “10.00”
3 Accredited Standards Committee X12, Insurance Subcommittee, X12N. “10.1.2 Data Use by Business Use” Health Care Claim Payment/Advice (835), 005010X221A1. Washington Publishing Company, Apr. 2006. <http://www.wpc-edi.com>.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 18 of 58 March 2017
CLP06 1032 Claim Filing Indicator Code ID 1/2 "13” - Point of Service CLP07 127 Reference Identification (Payer Claim
Control Number) AN 1/30 "123456789123456789"
NM1 – Patient Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "QC" NM102 1065 Entity Type Qualifier ID 1/1 "1" - Person NM103 1035 Name Last or Organization Name AN 1/35 “MILLER” NM104 1036 Name First AN 1/25 "CASPER” NM108 66 Identification Code Qualifier ID 1/2 "MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “121212121”
NM1 – Service Provider Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "82" – Rendering Provider NM102 1065 Entity Type Qualifier ID 1/1 "2" – Non-Person Entity NM103 1035 Name Last or Organization Name AN 1/35 “STORE B” NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI) NM109 67 Identification Code (Rendering Provider
Identifier) AN 2/80 “4445556661” - NPI
SVC – Service Payment Information Ref Elem Description Type Min/Max Data
SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 "00006094228” SVC02 782 Monetary Amount (Line Item Charge
Amount) R 1/18 “68.70”
SVC03 782 Line Item Provider Payment Amount R 1/18 "63.00”
SVC05 380 Unit of Service Paid Count R 1/18 “30”
DTM – Service Date Ref Elem Description Type Min/Max Data
DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20100122”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “PR” – Patient Responsibility CAS02 1029 Adjustment Reason Code ID 1/5 “3" - Co-payment amount CAS03 782 Monetary Amount R 1/18 “10.00”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “CO” – Contractual Obligations CAS02 1029 Adjustment Reason Code ID 1/2 “144” – Incentive Adjustment CAS03 782 Monetary Amount ID 1/5 “-5.00"

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 19 of 58 March 2017
4.4 COB Claim Submission to Secondary Insurance Pharmacy Provider B submits a Claim to the Processor for which they have received other payment in the amount of $41.20 from another payer. This transaction utilizes the Coordination of Benefits / Other Payments Segment. The Processor returns a Paid response which takes the $41.20 paid by other amount into consideration.
4.4.1 4A Billing Transaction TRANSACTION HEADER SEGMENT
Field Field Name Value Comments 101-A1 BIN NUMBER 610066 102-A2 VERSION/RELEASE NUMBER 71 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 4445556661bbbbb Store B 401-D1 DATE OF SERVICE 20100122 January 22, 2010 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
PATIENT SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 01 Patient Segment 304-C4 DATE OF BIRTH 19620615 Born June 15, 1962 305-C5 PATIENT GENDER CODE 1 Male 310-CA PATIENT FIRST NAME MICKEY Mickey is patient’s first name 311-CB PATIENT LAST NAME SMITH Smith is patient’s last name
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 987654321 Cardholder ID
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 1234602 436-E1 PRODUCT/SERVICE ID QUALIFIER 03 National Drug Code (NDC) 407-D7 PRODUCT/SERVICE ID 00006094228 Clinoril 200mg 403-D3 FILL NUMBER 0 Original dispensing 442-E7 QUANTITY DISPENSED 30000 30.000 tablets 405-D5 DAYS SUPPLY 30 30 Days supply 406-D6 COMPOUND CODE 1 Not a compound 408-D8 DISPENSE AS WRITTEN/PRODUCT SELECTION CODE 1 Substitution Not Allowed by Prescriber 414-DE DATE PRESCRIPTION WRITTEN 20100122 January 22, 2010 308-C8 OTHER COVERAGE CODE 2 Other coverage exists-payment collected
PRICING SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 11 Pricing Segment 409-D9 INGREDIENT COST SUBMITTED 557{ $55.70 412-DC DISPENSING FEE SUBMITTED 50{ $5.00 426-DQ USUAL AND CUSTOMARY CHARGE 707{ $70.70 430-DU GROSS AMOUNT DUE 607{ $60.70 423-DN BASIS OF COST DETERMINATION 01 AWP (Average Wholesale Price)
COORDINATION OF BENEFITS/OTHER PAYMENTS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 05 Coordination of Benefits/Other Payer Segment 337-4C COB/OTHER PAYMENTS COUNT 1 One occurrence 338-5C OTHER PAYER COVERAGE TYPE 01 Primary 341-HB OTHER PAYER AMOUNT PAID COUNT 1 One occurrence 342-HC OTHER PAYER AMOUNT PAID QUALIFIER 07 Drug Benefit 431-DV OTHER PAYER AMOUNT PAID 412{ $41.20 paid

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 20 of 58 March 2017
4.4.2 4B Billing Response Transaction RESPONSE HEADER SEGMENT
Field Field Name Value Comments 102-A2 VERSION/RELEASE NUMBER 71 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 4445556661bbbbb Store B 401-D1 DATE OF SERVICE 20100122 January 22, 2010
RESPONSE INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 25 Insurance Segment 302-C2 CARDHOLDER ID 987654321 Cardholder ID
RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS P Paid 503-F3 AUTHORIZATION NUMBER 11122233345678
RESPONSE CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 22 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION /SERVICE REFERENCE NUMBER 1234602 RESPONSE PRICING SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 23 Response Pricing Segment 505-F5 PATIENT PAY AMOUNT 5{ $00.50 506-F6 INGREDIENT COST PAID 557{ $55.70 507-F7 DISPENSING FEE PAID 50{ $5.00 566-J5 OTHER PAYER AMOUNT RECOGNIZED 412{ $41.20 509-F9 TOTAL AMOUNT PAID 190{ $19.00 522-FM BASIS OF REIMBURSE DETERMINATION 1 Ingredient Cost Paid as Submitted
Total Amount Paid (509-F9) represents a sum of Ingredient Cost Paid (506-F6), Dispensing Fee Paid (507-F7), Flat Sales Tax Amount Paid (558-AW), Percentage Sales Tax Amount Paid’(559-AX), Incentive Amount Paid (521-FL), ‘Professional Service Fee Paid’ (562-J1), ‘Other Amount Paid’ (565-J4) less ‘Patient Pay Amount’ (505-F5) and Other Payer Amount Recognized (566-J5). In above example, secondary payer’s contracted rate is less than that of the primary ($19.50 vs. $20.00). They have returned a $0.50 copay and the agreement to pay $19.00
4.4.1 835 for vD.0 Billing Response 4D4 CLP – Claim Payment Information Required
Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “1234602FILL0” – Rx Number and Fill Number CLP02 1029 Claim Status Code ID 1/2 “2” – Processed as secondary CLP03 782 Monetary Amount (Total Claim Charge
Amount) R 1/18 “60.70”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 “19.00” CLP05 782 Monetary Amount (Patient Responsibility
Amount) R 1/18 “.50”
CLP06 1032 Claim Filing Indicator Code ID 1/2 “13” – Point of Service
4 Accredited Standards Committee X12, Insurance Subcommittee, X12N. “10.1.2 Data Use by Business Use” Health Care Claim Payment/Advice (835), 005010X221A1. Washington Publishing Company, Apr. 2006. <http://www.wpc-edi.com>.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 21 of 58 March 2017
CLP07 127 Reference Identification (Payer Claim Control Number)
AN 1/30 “11122233345678”
NM1 – Patient Name Required Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 “QC” NM102 1065 Entity Type Qualifier ID 1/1 “1” – Person NM103 1035 Name Last or Organization Name AN 1/35 “SMITH” NM104 1036 Name First AN 1/25 “MICKEY” NM108 66 Identification Code Qualifier ID 1/2 “MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “987654321”
NM1 – Service Provider Name (not be used by some payers) Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 “82” – Rendering Provider NM102 1065 Entity Type Qualifier ID 1/1 “2” – Non-Person Entity NM103 1035 Name Last or Organization Name AN 1/35 “STORE B” NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI) NM109 67 Identification Code (Rendering Provider
Identifier) AN 2/80 “4445556661” – NPI
SVC – Service Payment Information Ref Elem Description Type Min/Max Data
SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 “00006094228” SVC02 782 Monetary Amount (Line Item Charge
Amount) R 1/18 “60.70”
SVC03 782 Line Item Provider Payment Amount R 1/18 “19.00” SVC05 380 Unit of Service Paid Count R 1/18 “30”
DTM – Service Date Ref Elem Description Type Min/Max Data
DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20100122”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “PR” – Patient Responsibility CAS02 1029 Adjustment Reason Code ID 1/5 “3” – Co-payment amount CAS03 782 Monetary Amount R 1/18 “.50”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “OA” – Other Adjustments CAS02 1029 Adjustment Reason Code ID 1/5 “23” – Other payer paid some charges CAS03 782 Monetary Amount R 1/18 “41.20”
NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 22 of 58 March 2017
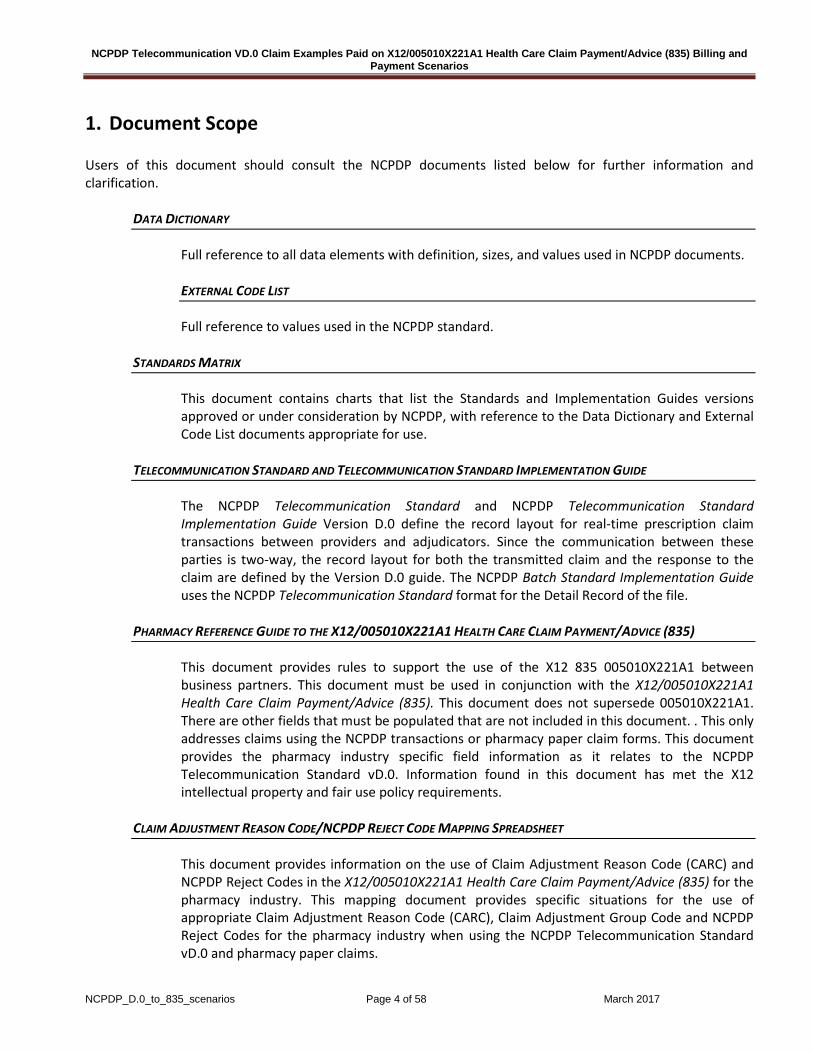
4.5 COB Claim Submission with Other Coverage Code of 8 and Patient Pay Amount Reported as Returned from Primary Payer Pharmacy Provider B submits a Claim to the Processor for which they are reporting the patient pay responsibility of $20.00 from another payer. This transaction utilizes the Coordination of Benefits / Other Payments Segment. The Processor returns a Paid response which takes the $20.00 paid by other amount into consideration.
4.5.1 5A Billing Transaction TRANSACTION HEADER SEGMENT
Field Field Name Value Comments 101-A1 BIN NUMBER 610066 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 4445556661bbbbb Store B 401-D1 DATE OF SERVICE 20100122 January 22, 2010 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
PATIENT SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 01 PATIENT SEGMENT 304-C4 DATE OF BIRTH 19620615 Born June 15, 1962 305-C5 PATIENT GENDER CODE 1 Male 310-CA PATIENT FIRST NAME MICKEY Mickey is patient’s first name 311-CB PATIENT LAST NAME SMITH Smith is patient’s last name
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 987654321 Cardholder ID
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx billing
402-D2 RX /SERVICE REFERENCE NUMBER 1234622 436-E1 PRODUCT/SERVICE ID QUALIFIER 03 National Drug Code (NDC) 407-D7 PRODUCT/SERVICE ID 00006094228 Clinoril 200mg 403-D3 FILL NUMBER 0 Original dispensing 442-E7 QUANTITY DISPENSED 30000 30.000 tablets 405-D5 DAYS SUPPLY 30 30 Days supply 406-D6 Compound Code 1 Not a compound 408-D8 DISPENSE AS WRITTEN/PRODUCT SELECTION CODE 2 Patient has requested brand 414-DE DATE PRESCRIPTION WRITTEN 20100122 January 22, 2010 308-C8 OTHER COVERAGE CODE 8 Claim is a billing for patient financial responsibility
PRICING SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 11 Pricing Segment 409-D9 INGREDIENT COST SUBMITTED 557{ $55.70 412-DC DISPENSING FEE SUBMITTED 50{ $5.00 426-DQ USUAL AND CUSTOMARY CHARGE 707{ $70.70 430-DU GROSS AMOUNT DUE 607{ $60.70 423-DN BASIS OF COST DETERMINATION 03 Direct
COORDINATION OF BENEFITS/OTHER PAYMENTS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 05 Coordination of Benefits/Other Payments Segment 337-4C COB/OTHER PAYMENTS COUNT 1 One occurrence 338-5C OTHER PAYER COVERAGE TYPE 01 Primary 341-HB OTHER PAYER AMOUNT PAID COUNT 1 One occurrence 351-NP OTHER PAYER-PATIENT PAY RESPONSIBILITY AMOUNT 06 Patient Pay Amount As Reported From Previous Payer

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 23 of 58 March 2017
QUALIFIER 352-NQ OTHER PAYER-PATIENT PAY AMOUNT RESPONSIBILITY 200{ $20.00
4.5.2 5B Billing Response Transaction RESPONSE HEADER SEGMENT
Field Field Name Value Comments 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 4445556661bbbbb Store B 401-D1 DATE OF SERVICE 20100122 January 22, 2010
RESPONSE INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 25 Insurance Segment 524-FO PLAN ID 9988 568-J7 PAYER ID QUALIFIER 1 National Payer ID 569-J8 PAYER ID 1212121212
RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS P Paid 503-F3 AUTHORIZATION NUMBER 11122233345678 549-7F HELP DESK PHONE NUMBER QUALIFIER 03 Processor/PBM 550-8F HELP DESK PHONE NUMBER 6023570862
RESPONSE CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 22 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION /SERVICE REFERENCE NUMBER 1234622 RESPONSE PRICING SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 23 RESPONSE PRICING SEGMENT 505-F5 PATIENT PAY AMOUNT 30{ $3.00 506-F6 INGREDIENT COST PAID 200{ $20.00 509-F9 TOTAL AMOUNT PAID 170{ $17.00 522-FM BASIS OF REIMBURSE DETERMINATION 14 Other Payer-Patient Responsibility Amount 148-UB INGREDIENT COST CONTRACTED/REIMBURSABLE
AMOUNT 557{ $55.70
159-U9 DISPENSING FEE CONTRACTED/REIMBURSABLE AMOUNT
50{ $5.00
4.5.3 835 for vD.0 Billing Response 5B5 CLP – Claim Payment Information
Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “1234622FILL0” – Rx Number and Refill Number CLP02 1029 Claim Status Code ID 1/2 “2” – Processed as secondary CLP03 782 Monetary Amount (Total Claim Charge
Amount) R 1/18 “60.70”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 “17.00” CLP05 782 Monetary Amount (Patient Responsibility
Amount) R 1/18 “3.00”
CLP06 1032 Claim Filing Indicator Code ID 1/2 “13” – Point of Service CLP07 127 Reference Identification (Payer Claim
Control Number) AN 1/30 “11122233345678”
5 Accredited Standards Committee X12, Insurance Subcommittee, X12N. “10.1.2 Data Use by Business Use” Health Care Claim Payment/Advice (835), 005010X221A1. Washington Publishing Company, Apr. 2006. <http://www.wpc-edi.com>.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 24 of 58 March 2017
NM1 – Patient Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 “QC” NM102 1065 Entity Type Qualifier ID 1/1 “1” – Person NM103 1035 Name Last or Organization Name AN 1/35 “SMITH” NM104 1036 Name First AN 1/25 “MICKEY” NM108 66 Identification Code Qualifier ID 1/2 “MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “987654321”
NM1 – Service Provider Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 “82” – Rendering Provider NM102 1065 Entity Type Qualifier ID 1/1 “2” – Non-Person Entity NM103 1035 Name Last or Organization Name AN 1/35 “STORE B” NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI) NM109 67 Identification Code (Rendering Provider
Identifier) AN 2/80 “4445556661” – NPI
SVC – Service Payment Information Ref Elem Description Type Min/Max Data
SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 “00006094228” SVC02 782 Monetary Amount (Line Item Charge
Amount) R 1/18 “60.70”
SVC03 782 Line Item Provider Payment Amount R 1/18 “17.00”
SVC05 380 Unit of Service Paid Count R 1/18 “30”
DTM – Service Date Ref Elem Description Type Min/Max Data
DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20100122”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “PR” – Patient Responsibility CAS02 1029 Adjustment Reason Code ID 1/5 “3” – Co-payment amount CAS03 782 Monetary Amount R 1/18 “3.00”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “OA” – Other Adjustments CAS02 1029 Adjustment Reason Code ID 1/5 “23” – Other payer paid some charges CAS03 782 Monetary Amount R 1/18 “41.20”

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 25 of 58 March 2017
4.6 Billed With Tax – Paid – Patient Is Responsible For Part of Tax Causing Patient Pay to Increase by Amount of Tax This is an example of a standard, everyday claim transaction with Tax submitted. The claim is paid without any necessary interventions and without edits / additional requirements applied by the payer.
4.6.1 6A Billing Transaction TRANSACTION HEADER SEGMENT
Field Field Name Value Comments 101-A1 BIN NUMBER 610066 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100122 January 22, 2010 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
PATIENT SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 01 PATIENT SEGMENT 304-C4 DATE OF BIRTH 19620615 Born June 15, 1962 305-C5 PATIENT GENDER CODE 1 Male 310-CA PATIENT FIRST NAME MICKEY Mickey is patient’s first name 311-CB PATIENT LAST NAME SMITH Smith is patient’s last name
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 987654321 Cardholder ID
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123456789012 436-E1 PRODUCT/SERVICE ID QUALIFIER 03 National Drug Code (NDC) 407-D7 PRODUCT/SERVICE ID 00006094228 Clinoril 200mg 442-E7 QUANTITY DISPENSED 30000 30.000 tablets 403-D3 FILL NUMBER 0 Original dispensing 405-D5 DAYS SUPPLY 30 30 Days supply 406-D6 COMPOUND CODE 1 Not a compound 408-D8 DISPENSED AS WRITTEN (DAW)/PRODUCT SELECTION
CODE 0 No Product Selection Indicated
414-DE DATE PRESCRIPTION WRITTEN 20100122 January 22, 2010 PRESCRIBER SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 03 Prescriber Segment 466-EZ PRESCRIBER ID QUALIFIER 01 National Provider Identifier (NPI) 411-DB PRESCRIBER ID 5556667772
PRICING SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 11 Pricing Segment 409-D9 INGREDIENT COST SUBMITTED 657{ $65.70 412-DC DISPENSING FEE SUBMITTED 30{ $3.00 482-GE PERCENTAGE SALES TAX AMOUNT SUBMITTED 42D $4.24 483-HE PERCENTAGE SALES TAX RATE SUBMITTED 6000{ 6.0000% 484-JE PERCENTAGE SALES TAX BASIS SUBMITTED 03 INGREDIENT COST + DISPENSING FEE 426-DQ USUAL AND CUSTOMARY CHARGE 707{ $70.70 430-DU GROSS AMOUNT DUE 687{ $68.70 423-DN BASIS OF COST DETERMINATION 1 AWP (Average Wholesale Price)

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 26 of 58 March 2017
4.6.2 6B Billing Response Transaction RESPONSE HEADER SEGMENT
Field Field Name Value Comments 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100122 January 22, 2010
RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS P Paid 503-F3 AUTHORIZATION NUMBER ABC12345
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 22 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123456789012 RESPONSE PRICING SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 23 Response Pricing Segment 505-F5 PATIENT PAY AMOUNT 110{ $11.00 506-F6 INGREDIENT COST PAID 667{ $66.70 507-F7 DISPENSING FEE PAID 30{ $3.00 559-AX PERCENTAGE SALES TAX AMOUNT PAID 41H $4.18 (6% of 69.70 – Cost + Dispensing Fee) 560-AY PERCENTAGE SALES TAX RATE PAID 6000{ 6.0000% 561-AZ PERCENTAGE SALES TAX BASIS PAID 03 Ingredient cost + Dispensing Fee 518-FI AMOUNT OF COPAY 100{ $10.00 523-FM AMOUNT ATTRIBUTED TO SALES TAX 10{ $1.00 574-2Y PLAN SALES TAX AMOUNT 31H $3.18 576-EQ PATIENT SALES TAX AMOUNT 10{ $1.00 509-F9 TOTAL AMOUNT PAID 628H $62.88 522-FM BASIS OF REIMBURSEMENT DETERMINATION 8 Contract Pricing
4.6.3 835 for vD.0 Billing Response 6B6 CLP – Claim Payment Information
Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “123456789012FILL0” – Rx Number and Refill Number CLP02 1029 Claim Status Code ID 1/2 "1" - Processed as primary CLP03 782 Monetary Amount (Total Claim Charge
Amount) R 1/18 “68.70”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 "62.88” CLP05 782 Monetary Amount (Patient Responsibility
Amount) R 1/18 “11.00”
CLP06 1032 Claim Filing Indicator Code ID 1/2 "13” - Point of Service CLP07 127 Reference Identification (Payer Claim
Control Number) AN 1/30 "ABC12345"
NM1 – Patient Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "QC" NM102 1065 Entity Type Qualifier ID 1/1 "1" - Person NM103 1035 Name Last or Organization Name AN 1/35 “SMITH” NM104 1036 Name First AN 1/25 "MICKEY” NM108 66 Identification Code Qualifier ID 1/2 "MI” – Member Identification Number
6 Accredited Standards Committee X12, Insurance Subcommittee, X12N. “10.1.2 Data Use by Business Use” Health Care Claim Payment/Advice (835), 005010X221A1. Washington Publishing Company, Apr. 2006. <http://www.wpc-edi.com>.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 27 of 58 March 2017
NM109 67 Identification Code (Patient Identifier) AN 2/80 “987654321”
NM1 – Service Provider Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "82" – Rendering Provider NM102 1065 Entity Type Qualifier ID 1/1 "2" – Non-Person Entity NM103 1035 Name Last or Organization Name (Pharmacy
Name) AN 1/35 “STORE A”
NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI) NM109 67 Identification Code AN 2/80 “1112223330” - NPI
SVC – Service Payment Information Ref Elem Description Type Min/Max Data
SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 "00006094228" SVC02 782 Monetary Amount (Line Item Charge
Amount) R 1/18 “68.80”
SVC03 782 Line Item Provider Payment Amount R 1/18 "62.88”
SVC05 380 Unit of Service Paid Count R 1/18 “30”
DTM – Service Date Ref Elem Description Type Min/Max Data
DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20100122”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “CO” – Contractual Obligations CAS02 1029 Adjustment Reason Code ID 1/5 “90" - Ingredient cost adjustment CAS03 782 Monetary Amount R 1/18 “-1.00” CAS05 1029 Adjustment Reason Code ID 1/5 “137" - Sales Tax CAS06 782 Monetary Amount R 1/18 “.06”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “PR” – Patient Responsibility CAS02 1029 Adjustment Reason Code ID 1/5 “3" - Co-payment amount CAS03 782 Monetary Amount R 1/18 “11.00”
AMT – Claim Supplemental Information Situational – see payment template for further guidance) Ref Elem Description Type Min/Max Data
AMT01 522 Amount Code Qualifier ID 2/2 “T” – Tax AMT02 782 Monetary Amount AN 1/48 "4.18" (tax amount calculated by plan)

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 28 of 58 March 2017
4.7 Billed With Tax – Paid This is an example of a standard, everyday claim transaction with Tax submitted. The claim is paid without any necessary interventions and without edits / additional requirements applied by the payer.
4.7.1 7A Billing Transaction TRANSACTION HEADER SEGMENT
Field Field Name Value Comments 101-A1 BIN NUMBER 610066 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100122 January 22, 2010 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
PATIENT SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 01 Patient Segment 304-C4 DATE OF BIRTH 19620615 Born June 15, 1962 305-C5 PATIENT GENDER CODE 1 Male 310-CA PATIENT FIRST NAME MICKEY Mickey is patient’s first name 311-CB PATIENT LAST NAME SMITH Smith is patient’s last name
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 987654321 Cardholder ID
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123456789015 436-E1 PRODUCT/SERVICE ID QUALIFIER 03 National Drug Code (NDC) 407-D7 PRODUCT/SERVICE ID 00006094228 Clinoril 200mg 442-E7 QUANTITY DISPENSED 30000 30.000 tablets 403-D3 FILL NUMBER 0 Original dispensing 405-D5 DAYS SUPPLY 30 30 Days supply 406-D6 COMPOUND CODE 1 Not a compound 408-D8 DISPENSED AS WRITTEN (DAW)/PRODUCT SELECTION
CODE 0 No Product Selection Indicated
414-DE DATE PRESCRIPTION WRITTEN 20100122 January 22, 2010 PRESCRIBER SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 03 Prescriber Segment 466-EZ PRESCRIBER ID QUALIFIER 01 National Provider Identifier (NPI) 411-DB PRESCRIBER ID 5556667772
PRICING SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 11 Pricing Segment 409-D9 INGREDIENT COST SUBMITTED 657{ $65.70 412-DC DISPENSING FEE SUBMITTED 30{ $3.00 482-GE PERCENTAGE SALES TAX AMOUNT SUBMITTED 42D $4.24 483-HE PERCENTAGE SALES TAX RATE SUBMITTED 6000{ 6.0000% 484-JE PERCENTAGE SALES TAX BASIS SUBMITTED 03 Ingredient Cost + Dispensing Fee 426-DQ USUAL AND CUSTOMARY CHARGE 707{ $70.70 430-DU GROSS AMOUNT DUE 687{ $68.70 423-DN BASIS OF COST DETERMINATION 1 AWP (Average Wholesale Price)
NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 29 of 58 March 2017
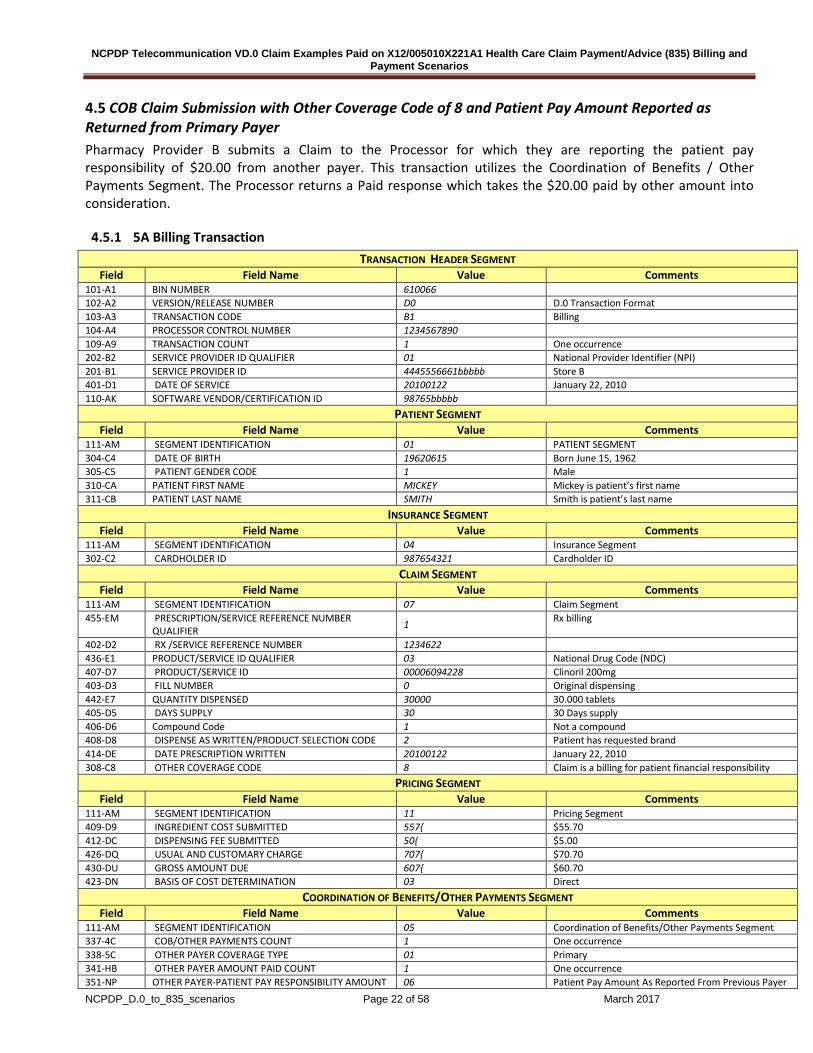
4.7.2 7B Billing Response Transaction RESPONSE HEADER SEGMENT
Field Field Name Value Comments 102-A2 VERSION/RELEASE NUMBER D0 (start here) D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100122 January 22, 2010
RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS P Paid 503-F3 AUTHORIZATION NUMBER ABC12345
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 22 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123456789015 RESPONSE PRICING SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 23 Response Pricing Segment 505-F5 PATIENT PAY AMOUNT 100{ $10.00 506-F6 INGREDIENT COST PAID 667{ $66.70 507-F7 DISPENSING FEE PAID 30{ $3.00 559-AX PERCENTAGE SALES TAX AMOUNT PAID 41H $4.18 (6% of 69.70 – Cost + Dispensing Fee) 560-AY PERCENTAGE SALES TAX RATE PAID 6000{ 6.0000% 561-AZ PERCENTAGE SALES TAX BASIS PAID 03 Ingredient cost + Dispensing Fee 509-F9 TOTAL AMOUNT PAID 638H $63.88 522-FM BASIS OF REIMBURSEMENT DETERMINATION 8 Contract Pricing
4.7.3 835 for vD.0 Billing Response 7B7 CLP – Claim Payment Information
Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “123456789015FILL0” – Rx Number and Fill Number CLP02 1029 Claim Status Code ID 1/2 "1" - Processed as primary
CLP03 782 Monetary Amount (Total Claim Charge Amount) R 1/18 “72.94”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 "63.88”
CLP05 782 Monetary Amount (Patient Responsibility Amount) R 1/18 “10.00”
CLP06 1032 Claim Filing Indicator Code ID 1/2 "13” - Point of Service
CLP07 127 Reference Identification (Payer Claim Control Number) AN 1/30 "ABC12345"
NM1 – Patient Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "QC" NM102 1065 Entity Type Qualifier ID 1/1 "1" - Person NM103 1035 Name Last or Organization Name AN 1/35 “SMITH” NM104 1036 Name First AN 1/25 "MICKEY” NM108 66 Identification Code Qualifier ID 1/2 "MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “987654321”
NM1 – Service Provider Name Ref Elem Description Type Min/Max Data
7 Accredited Standards Committee X12, Insurance Subcommittee, X12N. “10.1.2 Data Use by Business Use” Health Care Claim Payment/Advice (835), 005010X221A1. Washington Publishing Company, Apr. 2006. <http://www.wpc-edi.com>.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 30 of 58 March 2017
NM101 98 Entity Identifier Code ID 2/3 "82" – Rendering Provider NM102 1065 Entity Type Qualifier ID 1/1 "2" – Non-Person Entity NM103 1035 Name Last or Organization Name (Pharmacy
Name) AN 1/35 “STORE A”
NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI) NM109 67 Identification Code AN 2/80 “1112223330” - NPI
SVC – Service Payment Information Ref Elem Description Type Min/Max Data
SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 "00006094228" SVC02 782 Monetary Amount (Line Item Charge
Amount) R 1/18 “72.94”
SVC03 782 Line Item Provider Payment Amount R 1/18 "63.88”
SVC05 380 Unit of Service Paid Count R 1/18 “30”
DTM – Service Date Ref Elem Description Type Min/Max Data
DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20100122”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “CO” – Contractual Obligations CAS02 1029 Adjustment Reason Code ID 1/5 “90" - Ingredient cost adjustment CAS03 782 Monetary Amount R 1/18 “-1.00” CAS05 1029 Adjustment Reason Code ID 1/5 “137" - Sales Tax CAS06 782 Monetary Amount R 1/18 “.06”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “PR” – Patient Responsibility CAS02 1029 Adjustment Reason Code ID 1/5 “3" - Co-payment amount CAS03 782 Monetary Amount R 1/18 “10.00”
AMT – Service Supplemental Information Ref Elem Description Type Min/Max Data
AMT01 522 Amount Code Qualifier ID 1/3 “T” - Tax AMT02 782 Monetary Amount R 1/18 “4.18”

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 31 of 58 March 2017
4.8 Multi-Ingredient Compound - Payable The following is an example of what a Multi-Ingredient Compound with five (5) ingredients. The payer accepts all five (5) ingredients resulting in a payable claim.
4.8.1 8A Billing Transaction
TRANSACTION HEADER SEGMENT Field Field Name Value Comments
101-A1 BIN NUMBER 610066 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 4445556661bbbbb Store B 401-D1 DATE OF SERVICE 20100122 January 22, 2010 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
PATIENT SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 01 Patient Segment 304-C4 DATE OF BIRTH 19620615 Born June 15, 1962 305-C5 PATIENT GENDER CODE 1 Male 310-CA PATIENT FIRST NAME CASPER Casper is patient’s first name 311-CB PATIENT LAST NAME MILLER Miller is patient’s last name
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 121212121 Cardholder ID
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 1234580 436-E1 PRODUCT/SERVICE ID QUALIFIER 00 Not Specified 407-D7 PRODUCT/SERVICE ID 0 Compound 442-E7 QUANTITY DISPENSED 120000 120.000ml 403-D3 FILL NUMBER 0 Original dispensing 405-D5 DAYS SUPPLY 30 30 Days supply 406-D6 COMPOUND CODE 2 Compound 408-D8 DISPENSED AS WRITTEN (DAW)/PRODUCT SELECTION
CODE 0 No Product Selection Indicated
414-DE DATE PRESCRIPTION WRITTEN 20100122 January 22, 2010 423-DN BASIS OF COST DETERMINATION 1 AWP (Average Wholesale Price) 41 5-DF NUMBER OF REFILLS AUTHORIZED 5 5 Refills 41 9-DJ PRESCRIPTION ORIGIN CODE 1 Written prescription 354-NX SUBMISSION CLARIFICATION CODE COUNT 1 One occurrence 420-DK SUBMISSION CLARIFICATION CODE 0 Not Specified 429-DT SPECIAL PACKAGING INDICATOR 1 Not unit dose 600-28 UNIT OF MEASURE ML Milliliters 995-E2 ROUTE OF ADMINISTRATION 11 Oral 996-G1 COMPOUND TYPE 99 Other
PRICING SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 11 Pricing Segment 409-D9 INGREDIENT COST SUBMITTED 142{ $14.20 412-DC DISPENSING FEE SUBMITTED 150{ $15.00 426-DQ USUAL AND CUSTOMARY CHARGE 311E $31.15 430-DU GROSS AMOUNT DUE 292{ $29.20
COMPOUND SEGMENT Field Field Name Value Comments

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 32 of 58 March 2017
111-AM SEGMENT IDENTIFICATION 10 Compound Segment 450-EF COMPOUND DOSAGE FORM DESCRIPTION CODE 11 Solution
451-EG COMPOUND DISPENSING UNIT FORM INDICATOR 3 Milliliters
447-EC COMPOUND INGREDIENT COMPONENT COUNT 03 3 Ingredients in this example
488-RE COMPOUND PRODUCT ID QUALIFIER 03 National Drug Code 1 (NDC) 489-TE COMPOUND PRODUCT ID 11845013901 Tetracycline 500mg cap 448-ED COMPOUND INGREDIENT QUANTITY 12000 12 capsules 449-EE COMPOUND INGREDIENT DRUG COST 12{ $1.20 490-UE COMPOUND INGREDIENT BASIS OF COST
DETERMINATION 01 AWP (Average Wholesale Price)
488-RE COMPOUND PRODUCT ID QUALIFIER 03 National Drug Code 2 (NDC) 489-TE COMPOUND PRODUCT ID 00603148049 Nystatin 100000u/ml Susp 448-ED COMPOUND INGREDIENT QUANTITY 120000 120ml 449-EE COMPOUND INGREDIENT DRUG COST 84{
$8.40
490-UE COMPOUND INGREDIENT BASIS OF COST DETERMINATION
01 AWP (Average Wholesale Price)
488-RE COMPOUND PRODUCT ID QUALIFIER 03 National Drug Code 3 (NDC) 489-TE COMPOUND PRODUCT ID 60809031055 Diphenhydramine 50mg cap 448-ED COMPOUND INGREDIENT QUANTITY 2 4 0 0 0 24 Capsules 449-EE COMPOUND INGREDIENT DRUG COST 46{ $4.60
4.8.2 8B Billing Response Transaction RESPONSE HEADER SEGMENT
Field Field Name Value Comments 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Standard 103-A3 TRANSACTION CODE B1 Billing 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 4445556661bbbbb Store B 401-D1 DATE OF SERVICE 20100122 January 22, 2010
RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS P Paid
RESPONSE CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 22 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 1234580
RESPONSE PRICING SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 23 Response Pricing Segment 505-F5 PATIENT PAY AMOUNT 50{ $5.00 506-F6 INGREDIENT COST PAID 14.2{ $14.20 507-F7 DISPENSING FEE PAID 150{ 509-F9 TOTAL AMOUNT PAID 24.2{ $24.20 557-AV TAX EXEMPT INDICATOR 1 Payer/Plan is Tax Exempt 522-FM BASIS OF REIMBURSEMENT DETERMINATION 08 Contract Pricing 518-FI AMOUNT OF COPAY 50{ $5.00
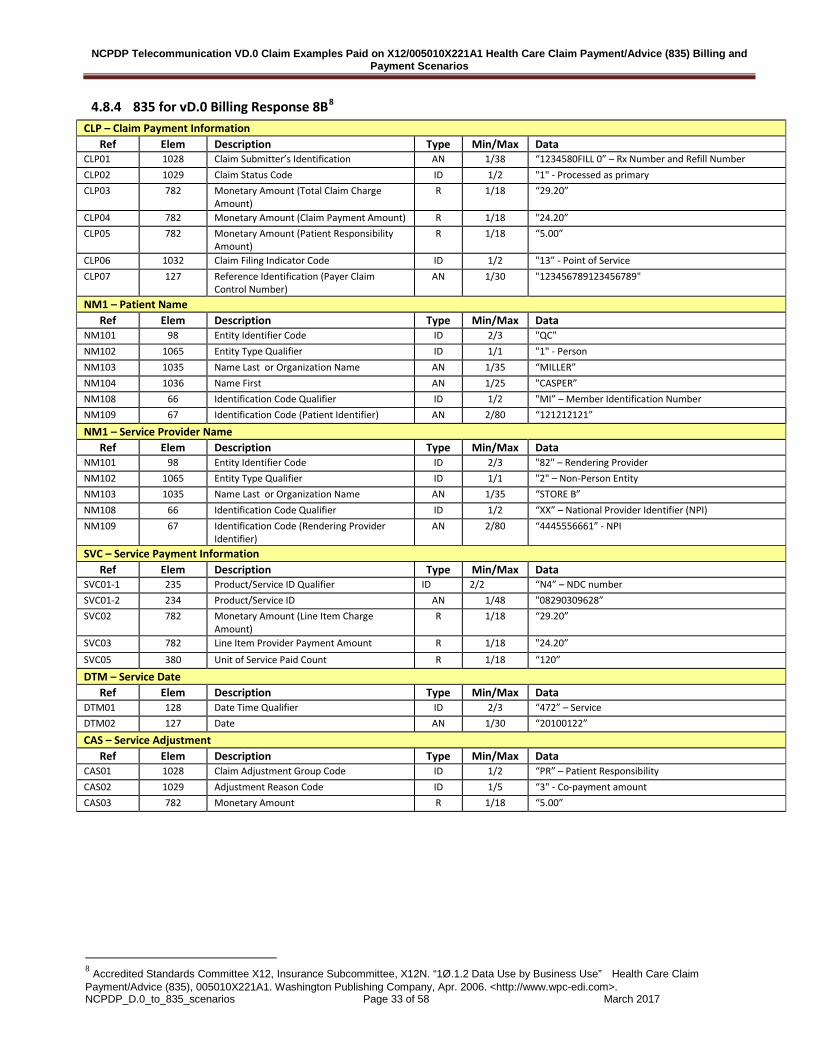
NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 33 of 58 March 2017
4.8.4 835 for vD.0 Billing Response 8B8 CLP – Claim Payment Information
Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “1234580FILL 0” – Rx Number and Refill Number CLP02 1029 Claim Status Code ID 1/2 "1" - Processed as primary CLP03 782 Monetary Amount (Total Claim Charge
Amount) R 1/18 “29.20”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 "24.20” CLP05 782 Monetary Amount (Patient Responsibility
Amount) R 1/18 “5.00”
CLP06 1032 Claim Filing Indicator Code ID 1/2 "13” - Point of Service CLP07 127 Reference Identification (Payer Claim
Control Number) AN 1/30 "123456789123456789"
NM1 – Patient Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "QC" NM102 1065 Entity Type Qualifier ID 1/1 "1" - Person NM103 1035 Name Last or Organization Name AN 1/35 “MILLER” NM104 1036 Name First AN 1/25 "CASPER” NM108 66 Identification Code Qualifier ID 1/2 "MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “121212121”
NM1 – Service Provider Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "82" – Rendering Provider NM102 1065 Entity Type Qualifier ID 1/1 "2" – Non-Person Entity NM103 1035 Name Last or Organization Name AN 1/35 “STORE B” NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI) NM109 67 Identification Code (Rendering Provider
Identifier) AN 2/80 “4445556661” - NPI
SVC – Service Payment Information Ref Elem Description Type Min/Max Data
SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 "08290309628” SVC02 782 Monetary Amount (Line Item Charge
Amount) R 1/18 “29.20”
SVC03 782 Line Item Provider Payment Amount R 1/18 "24.20” SVC05 380 Unit of Service Paid Count R 1/18 “120”
DTM – Service Date Ref Elem Description Type Min/Max Data
DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20100122”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “PR” – Patient Responsibility CAS02 1029 Adjustment Reason Code ID 1/5 “3" - Co-payment amount CAS03 782 Monetary Amount R 1/18 “5.00”
8 Accredited Standards Committee X12, Insurance Subcommittee, X12N. “1Ø.1.2 Data Use by Business Use” Health Care Claim Payment/Advice (835), 005010X221A1. Washington Publishing Company, Apr. 2006. <http://www.wpc-edi.com>.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 34 of 58 March 2017
4.9 Patient is not Cardholder The patient on the claims is not the same person as the cardholder of the insurance.
4.9.1 9A Billing Transaction TRANSACTION HEADER SEGMENT
Field Field Name Value Comments 101-A1 BIN NUMBER 610066 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100122 January 22, 2010 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
PATIENT SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 01 Patient Segment 304-C4 DATE OF BIRTH 19620615 Born June 15, 1962 305-C5 PATIENT GENDER CODE 2 Female 310-CA PATIENT FIRST NAME PEBBLES Pebbles is patient’s first name 311-CB PATIENT LAST NAME LEWIS Lewis is patient’s last name
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 4567987654321 Cardholder ID 303-C3 PERSON CODE 003 306-C6 PATIENT RELATIONSHIP CODE 03 Child
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123456789036 436-E1 PRODUCT/SERVICE ID QUALIFIER 03 National Drug Code (NDC) 407-D7 PRODUCT/SERVICE ID 00093415573 Amoxicillin Sus 250/5ml 442-E7 QUANTITY DISPENSED 100000 100.000 ML 403-D3 FILL NUMBER 0 Original dispensing 405-D5 DAYS SUPPLY 10 10 Days supply 406-D6 COMPOUND CODE 1 Not a compound 408-D8 DISPENSED AS WRITTEN (DAW)/PRODUCT SELECTION
CODE 0 No Product Selection Indicated
414-DE DATE PRESCRIPTION WRITTEN 20100122 January 22, 2010 PRESCRIBER SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 03 Prescriber Segment 466-EZ PRESCRIBER ID QUALIFIER 01 National Provider Identifier (NPI) 411-DB PRESCRIBER ID 5556667772
PRICING SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 11 Pricing Segment 409-D9 INGREDIENT COST SUBMITTED 70{ $7.00 412-DC DISPENSING FEE SUBMITTED 30{ $3.00 426-DQ USUAL AND CUSTOMARY CHARGE 100{ $10. 00 430-DU GROSS AMOUNT DUE 100{ $10. 00 423-DN BASIS OF COST DETERMINATION 1 AWP (Average Wholesale Price)

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 35 of 58 March 2017
4.9.3 9B Billing Response Transaction RESPONSE HEADER SEGMENT
Field Field Name Value Comments 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100122 January 22, 2010
RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS P Paid 503-F3 AUTHORIZATION NUMBER ABC12345
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 22 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123456789036 RESPONSE PRICING SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 23 Response Pricing Segment 505-F5 PATIENT PAY AMOUNT 0{ $0.00 506-F6 INGREDIENT COST PAID 70{ $7.00 507-F7 DISPENSING FEE PAID 30{ $3.00 509-F9 TOTAL AMOUNT PAID 100{ $10. 00 522-FM BASIS OF REIMBURSEMENT DETERMINATION 1 Ingredient Cost Paid as Submitted
4.9.4 835 for vD.0 Billing Response 9B9 CLP – Claim Payment Information
Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “123456789036FILL0” – Rx Number and Fill Number CLP02 1029 Claim Status Code ID 1/2 "1" - Processed as primary CLP03 782 Monetary Amount (Total Claim Charge
Amount) R 1/18 “10.00”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 "10.00” CLP05 782 Monetary Amount (Patient Responsibility
Amount) R 1/18
CLP06 1032 Claim Filing Indicator Code ID 1/2 "13” - Point of Service CLP07 127 Reference Identification (Payer Claim Control
Number) AN 1/30 "ABC1234775"
NM1 – Patient Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "QC" NM102 1065 Entity Type Qualifier ID 1/1 "1" - Person NM103 1035 Name Last or Organization Name AN 1/35 “LEWIS” NM104 1036 Name First AN 1/25 "PEBBLES” NM108 66 Identification Code Qualifier ID 1/2 "MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “4567987654321”
NM1 – Insured Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "IL" NM102 1065 Entity Type Qualifier ID 1/1 "1" - Person NM103 1035 Name Last or Organization Name AN 1/35 “LEWIS”
9 Accredited Standards Committee X12, Insurance Subcommittee, X12N. “10.1.2 Data Use by Business Use” Health Care Claim Payment/Advice (835), 005010X221A1. Washington Publishing Company, Apr. 2006. <http://www.wpc-edi.com>.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 36 of 58 March 2017
NM104 1036 Name First AN 1/25 "FRED” NM108 66 Identification Code Qualifier ID 1/2 "MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “4567987654321”
NM1 – Service Provider Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "82" – Rendering Provider NM102 1065 Entity Type Qualifier ID 1/1 "2" – Non-Person Entity NM103 1035 Name Last or Organization Name (Pharmacy
Name) AN 1/35 “STORE A”
NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI) NM109 67 Identification Code AN 2/80 “1112223330” - NPI
SVC – Service Payment Information Ref Elem Description Type Min/Max Data
SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 "00006094228" SVC02 782 Monetary Amount (Monetary Amount (Line
Item Charge Amount)) R 1/18 “10.00”
SVC03 782 Monetary Amount (Line Item Provider Payment Amount)
R 1/18 "10.00”
SVC05 380 Quantity (Unit of Service Paid Count) R 1/18 “100”
DTM – Service Date Ref Elem Description Type Min/Max Data
DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20100122”
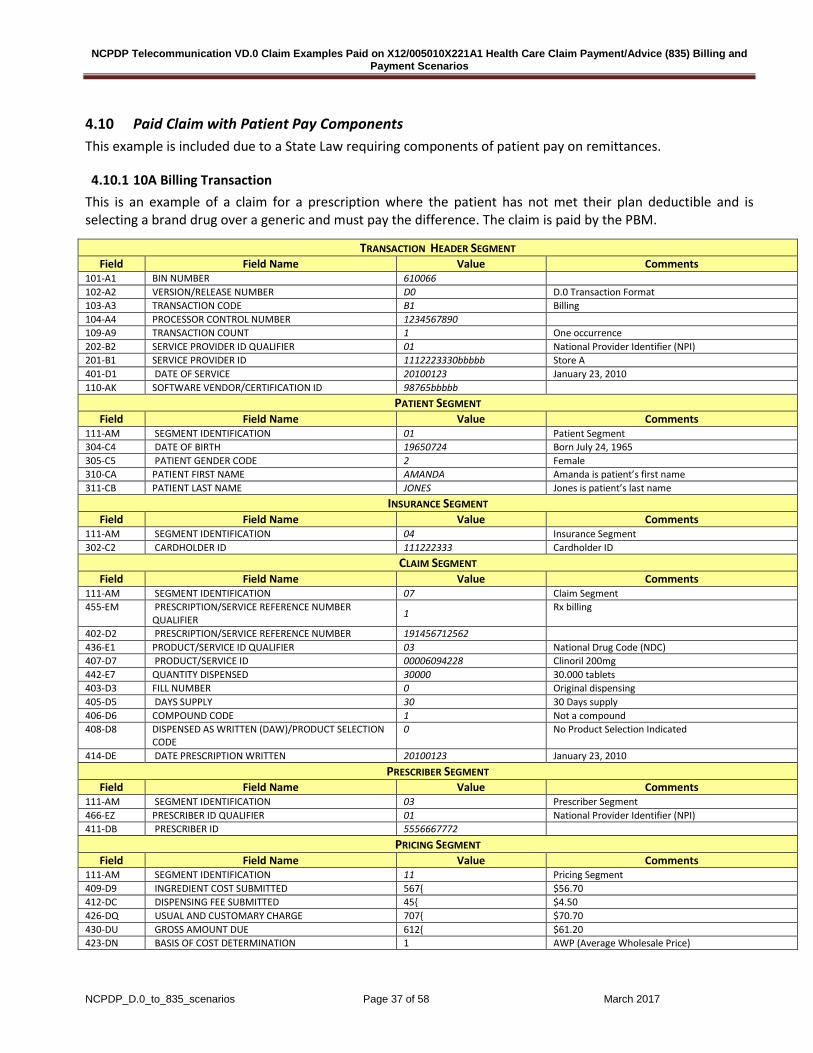
NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 37 of 58 March 2017
4.10 Paid Claim with Patient Pay Components This example is included due to a State Law requiring components of patient pay on remittances.
4.10.1 10A Billing Transaction This is an example of a claim for a prescription where the patient has not met their plan deductible and is selecting a brand drug over a generic and must pay the difference. The claim is paid by the PBM.
TRANSACTION HEADER SEGMENT Field Field Name Value Comments
101-A1 BIN NUMBER 610066 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100123 January 23, 2010 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
PATIENT SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 01 Patient Segment 304-C4 DATE OF BIRTH 19650724 Born July 24, 1965 305-C5 PATIENT GENDER CODE 2 Female 310-CA PATIENT FIRST NAME AMANDA Amanda is patient’s first name 311-CB PATIENT LAST NAME JONES Jones is patient’s last name
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 111222333 Cardholder ID
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 191456712562 436-E1 PRODUCT/SERVICE ID QUALIFIER 03 National Drug Code (NDC) 407-D7 PRODUCT/SERVICE ID 00006094228 Clinoril 200mg 442-E7 QUANTITY DISPENSED 30000 30.000 tablets 403-D3 FILL NUMBER 0 Original dispensing 405-D5 DAYS SUPPLY 30 30 Days supply 406-D6 COMPOUND CODE 1 Not a compound 408-D8 DISPENSED AS WRITTEN (DAW)/PRODUCT SELECTION
CODE 0 No Product Selection Indicated
414-DE DATE PRESCRIPTION WRITTEN 20100123 January 23, 2010 PRESCRIBER SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 03 Prescriber Segment 466-EZ PRESCRIBER ID QUALIFIER 01 National Provider Identifier (NPI) 411-DB PRESCRIBER ID 5556667772
PRICING SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 11 Pricing Segment 409-D9 INGREDIENT COST SUBMITTED 567{ $56.70 412-DC DISPENSING FEE SUBMITTED 45{ $4.50 426-DQ USUAL AND CUSTOMARY CHARGE 707{ $70.70 430-DU GROSS AMOUNT DUE 612{ $61.20 423-DN BASIS OF COST DETERMINATION 1 AWP (Average Wholesale Price)
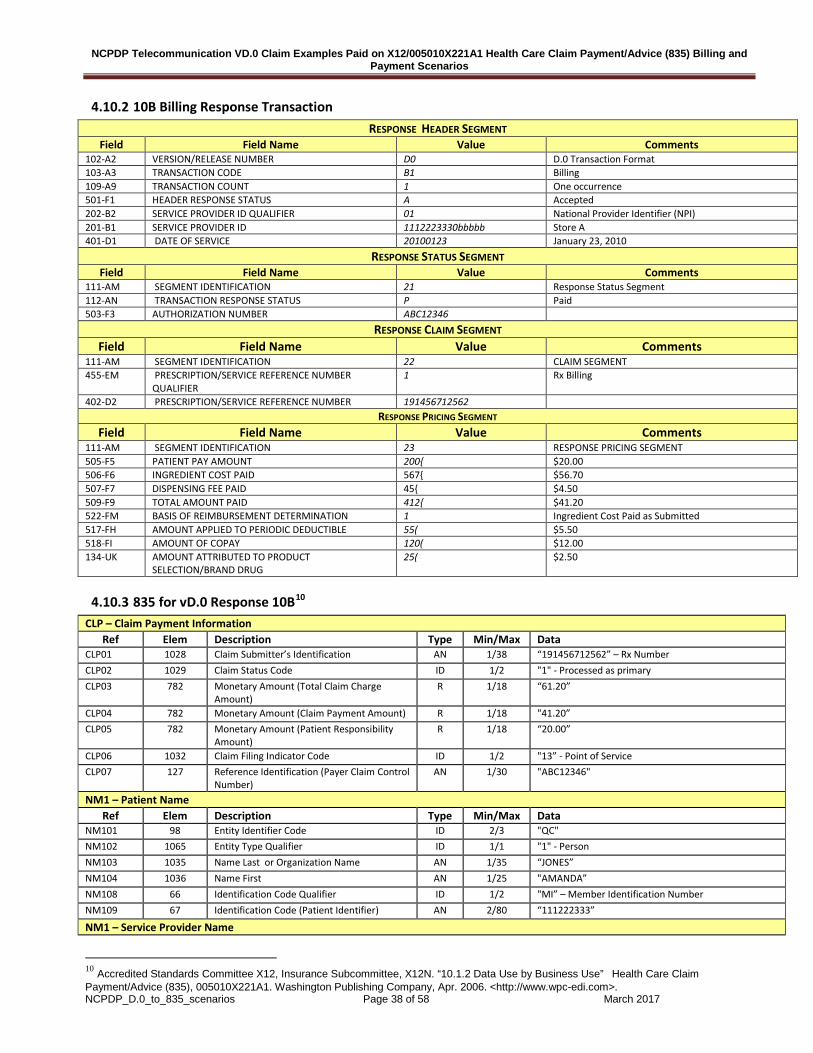
NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 38 of 58 March 2017
4.10.2 10B Billing Response Transaction RESPONSE HEADER SEGMENT
Field Field Name Value Comments 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100123 January 23, 2010
RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS P Paid 503-F3 AUTHORIZATION NUMBER ABC12346
RESPONSE CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 22 CLAIM SEGMENT 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 191456712562 RESPONSE PRICING SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 23 RESPONSE PRICING SEGMENT 505-F5 PATIENT PAY AMOUNT 200{ $20.00 506-F6 INGREDIENT COST PAID 567{ $56.70 507-F7 DISPENSING FEE PAID 45{ $4.50 509-F9 TOTAL AMOUNT PAID 412{ $41.20 522-FM BASIS OF REIMBURSEMENT DETERMINATION 1 Ingredient Cost Paid as Submitted 517-FH AMOUNT APPLIED TO PERIODIC DEDUCTIBLE 55( $5.50 518-FI AMOUNT OF COPAY 120( $12.00 134-UK AMOUNT ATTRIBUTED TO PRODUCT
SELECTION/BRAND DRUG 25( $2.50
4.10.3 835 for vD.0 Response 10B10 CLP – Claim Payment Information
Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “191456712562” – Rx Number CLP02 1029 Claim Status Code ID 1/2 "1" - Processed as primary CLP03 782 Monetary Amount (Total Claim Charge
Amount) R 1/18 “61.20”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 "41.20” CLP05 782 Monetary Amount (Patient Responsibility
Amount) R 1/18 “20.00”
CLP06 1032 Claim Filing Indicator Code ID 1/2 "13” - Point of Service CLP07 127 Reference Identification (Payer Claim Control
Number) AN 1/30 "ABC12346"
NM1 – Patient Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "QC" NM102 1065 Entity Type Qualifier ID 1/1 "1" - Person NM103 1035 Name Last or Organization Name AN 1/35 “JONES” NM104 1036 Name First AN 1/25 "AMANDA” NM108 66 Identification Code Qualifier ID 1/2 "MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “111222333”
NM1 – Service Provider Name
10 Accredited Standards Committee X12, Insurance Subcommittee, X12N. “10.1.2 Data Use by Business Use” Health Care Claim Payment/Advice (835), 005010X221A1. Washington Publishing Company, Apr. 2006. <http://www.wpc-edi.com>.
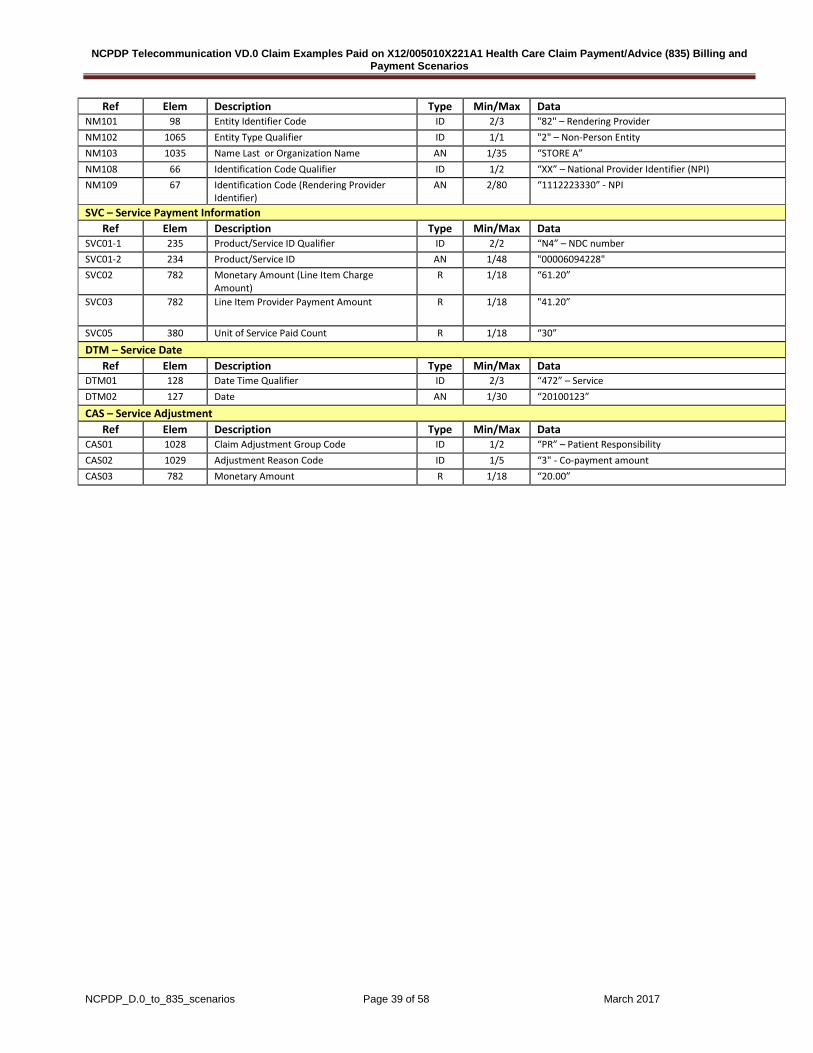
NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 39 of 58 March 2017
Ref Elem Description Type Min/Max Data NM101 98 Entity Identifier Code ID 2/3 "82" – Rendering Provider NM102 1065 Entity Type Qualifier ID 1/1 "2" – Non-Person Entity NM103 1035 Name Last or Organization Name AN 1/35 “STORE A” NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI) NM109 67 Identification Code (Rendering Provider
Identifier) AN 2/80 “1112223330” - NPI
SVC – Service Payment Information Ref Elem Description Type Min/Max Data
SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 "00006094228" SVC02 782 Monetary Amount (Line Item Charge
Amount) R 1/18 “61.20”
SVC03 782 Line Item Provider Payment Amount R 1/18 "41.20”
SVC05 380 Unit of Service Paid Count R 1/18 “30”
DTM – Service Date Ref Elem Description Type Min/Max Data
DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20100123”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “PR” – Patient Responsibility CAS02 1029 Adjustment Reason Code ID 1/5 “3" - Co-payment amount CAS03 782 Monetary Amount R 1/18 “20.00”

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 40 of 58 March 2017
4.11 Discount Card with Membership Fee This is an example of a standard, everyday claim transaction. The claim is paid without any necessary interventions but the patient pay amount is greater than the total amount paid due to a processing fee of $1.00 and membership fee of $30.00.
4.11.1 11A Billing Transaction TRANSACTION HEADER SEGMENT
Field Field Name Value Comments 101-A1 BIN NUMBER 610066 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100122 January 22, 2010 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
PATIENT SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 01 Patient Segment 304-C4 DATE OF BIRTH 19620615 Born June 15, 1962 305-C5 PATIENT GENDER CODE 1 Male 310-CA PATIENT FIRST NAME MICKEY Mickey is patient’s first name 311-CB PATIENT LAST NAME SMITH Smith is patient’s last name
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 987654321 Cardholder ID
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123456789128 436-E1 PRODUCT/SERVICE ID QUALIFIER 03 National Drug Code NDC) 407-D7 PRODUCT/SERVICE ID 00006094228 Clinoril 200mg 442-E7 QUANTITY DISPENSED 30000 30.000 tablets 403-D3 FILL NUMBER 0 Original dispensing 405-D5 DAYS SUPPLY 30 30 Days supply 406-D6 COMPOUND CODE 1 Not a compound 408-D8 DISPENSED AS WRITTEN (DAW)/PRODUCT SELECTION
CODE 0 No Product Selection Indicated
414-DE DATE PRESCRIPTION WRITTEN 20100122 January 22, 2010 PRESCRIBER SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 03 Prescriber Segment 466-EZ PRESCRIBER ID QUALIFIER 01 National Provider Identifier (NPI) 411-DB PRESCRIBER ID 5556667772
PRICING SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 11 Pricing Segment 409-D9 INGREDIENT COST SUBMITTED 657{ $65.70 412-DC DISPENSING FEE SUBMITTED 30{ $3.00 426-DQ USUAL AND CUSTOMARY CHARGE 707{ $70.70 430-DU GROSS AMOUNT DUE 687{ $68.70 423-DN BASIS OF COST DETERMINATION 1 AWP (Average Wholesale Price)

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 41 of 58 March 2017
11B Billing Response Transaction RESPONSE HEADER SEGMENT
Field Field Name Value Comments 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100122 January 22, 2010
RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS P Paid 503-F3 AUTHORIZATION NUMBER ABC12345
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 22 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123456789128 RESPONSE PRICING SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 23 Response Pricing Segment 505-F5 PATIENT PAY AMOUNT 697{ $69.70 506-F6 INGREDIENT COST PAID 657{ $65.70 507-F7 DISPENSING FEE PAID 30{ $3.00 509-F9 TOTAL AMOUNT PAID 310} $31.00- 522-FM BASIS OF REIMBURSEMENT DETERMINATION 1 Ingredient Cost Paid as Submitted 518-FI AMOUNT ATTRIBUTED TO COPAY 68.7( $68.70 571-NZ AMOUNT ATTRIBUTED TO PROCESSOR FEE 310{ $31.00
4.11.2 835 for vD.0 Response 11B11 CLP – Claim Payment Information
Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “123456789128” – Rx Number CLP02 1029 Claim Status Code ID 1/2 "1" - Processed as primary CLP03 782 Monetary Amount (Total Claim Charge
Amount) R 1/18 “68.70”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 "31.00-” CLP05 782 Monetary Amount (Patient Responsibility
Amount) R 1/18 “99.70”
CLP06 1032 Claim Filing Indicator Code ID 1/2 "13” - Point of Service CLP07 127 Reference Identification (Payer Claim Control
Number) AN 1/30 "ABC12345"
NM1 – Patient Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "QC" NM102 1065 Entity Type Qualifier ID 1/1 "1" - Person NM103 1035 Name Last or Organization Name AN 1/35 “SMITH” NM104 1036 Name First AN 1/25 "MICKEY” NM108 66 Identification Code Qualifier ID 1/2 "MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “987654321”
NM1 – Service Provider Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "82" – Rendering Provider
11 Accredited Standards Committee X12, Insurance Subcommittee, X12N. “10.1.2 Data Use by Business Use” Health Care Claim Payment/Advice (835), 005010X221A1. Washington Publishing Company, Apr. 2006. <http://www.wpc-edi.com>.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 42 of 58 March 2017
NM102 1065 Entity Type Qualifier ID 1/1 "2" – Non-Person Entity NM103 1035 Name Last or Organization Name (Pharmacy
Name) AN 1/35 “STORE A”
NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI) NM109 67 Identification Code AN 2/80 “1112223330” - NPI
SVC – Service Payment Information Ref Elem Description Type Min/Max Data
SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 "00006094228" SVC02 782 Monetary Amount (Monetary Amount (Line
Item Charge Amount)) R 1/18 “68.70”
SVC03 782 Monetary Amount (Line Item Provider Payment Amount)
R 1/18 "31.00-”
SVC05 380 Quantity (Unit of Service Paid Count) R 1/18 “30”
DTM – Service Date Ref Elem Description Type Min/Max Data
DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20100122”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “PR” – Patient Responsibility CAS02 1029 Adjustment Reason Code ID 1/5 “3" - Co-payment amount CAS03 782 Monetary Amount (Adjustment Amount) R 1/18 “99.70”
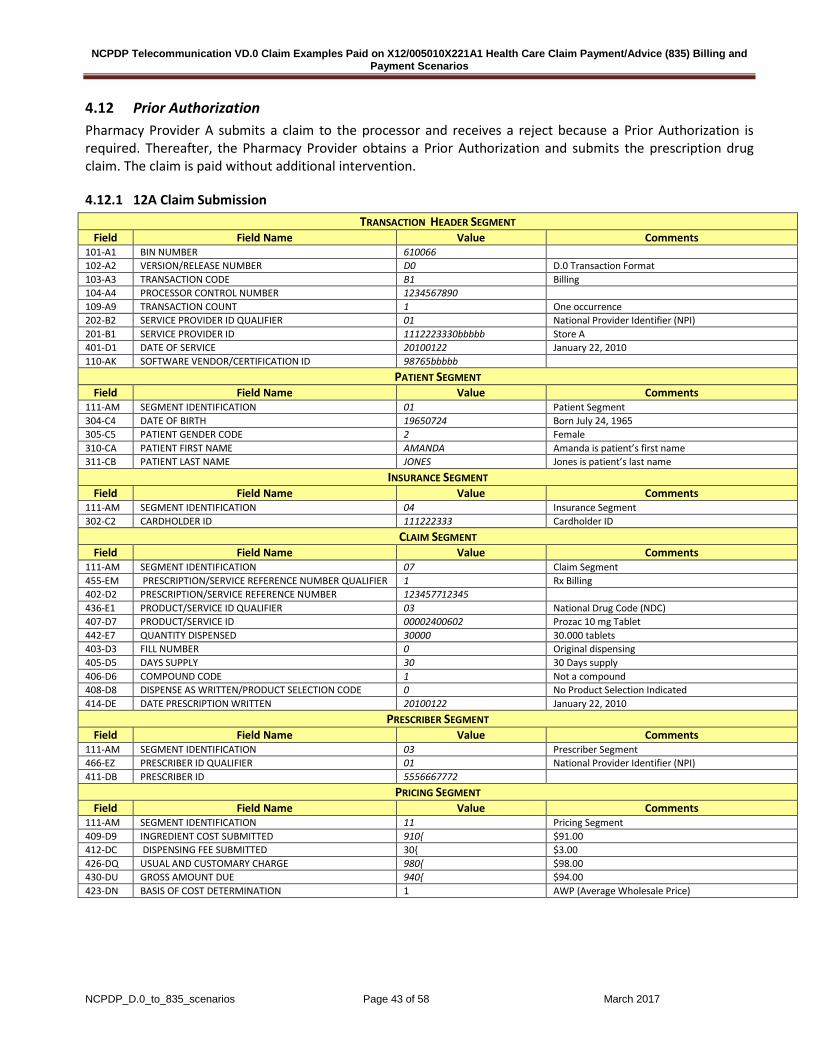
NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 43 of 58 March 2017
4.12 Prior Authorization Pharmacy Provider A submits a claim to the processor and receives a reject because a Prior Authorization is required. Thereafter, the Pharmacy Provider obtains a Prior Authorization and submits the prescription drug claim. The claim is paid without additional intervention.
4.12.1 12A Claim Submission TRANSACTION HEADER SEGMENT
Field Field Name Value Comments 101-A1 BIN NUMBER 610066 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100122 January 22, 2010 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
PATIENT SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 01 Patient Segment 304-C4 DATE OF BIRTH 19650724 Born July 24, 1965 305-C5 PATIENT GENDER CODE 2 Female 310-CA PATIENT FIRST NAME AMANDA Amanda is patient’s first name 311-CB PATIENT LAST NAME JONES Jones is patient’s last name
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 111222333 Cardholder ID
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER QUALIFIER 1 Rx Billing 402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123457712345 436-E1 PRODUCT/SERVICE ID QUALIFIER 03 National Drug Code (NDC) 407-D7 PRODUCT/SERVICE ID 00002400602 Prozac 10 mg Tablet 442-E7 QUANTITY DISPENSED 30000 30.000 tablets 403-D3 FILL NUMBER 0 Original dispensing 405-D5 DAYS SUPPLY 30 30 Days supply 406-D6 COMPOUND CODE 1 Not a compound 408-D8 DISPENSE AS WRITTEN/PRODUCT SELECTION CODE 0 No Product Selection Indicated 414-DE DATE PRESCRIPTION WRITTEN 20100122 January 22, 2010
PRESCRIBER SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 03 Prescriber Segment 466-EZ PRESCRIBER ID QUALIFIER 01 National Provider Identifier (NPI) 411-DB PRESCRIBER ID 5556667772
PRICING SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 11 Pricing Segment 409-D9 INGREDIENT COST SUBMITTED 910{ $91.00 412-DC DISPENSING FEE SUBMITTED 30{ $3.00 426-DQ USUAL AND CUSTOMARY CHARGE 980{ $98.00 430-DU GROSS AMOUNT DUE 940{ $94.00 423-DN BASIS OF COST DETERMINATION 1 AWP (Average Wholesale Price)
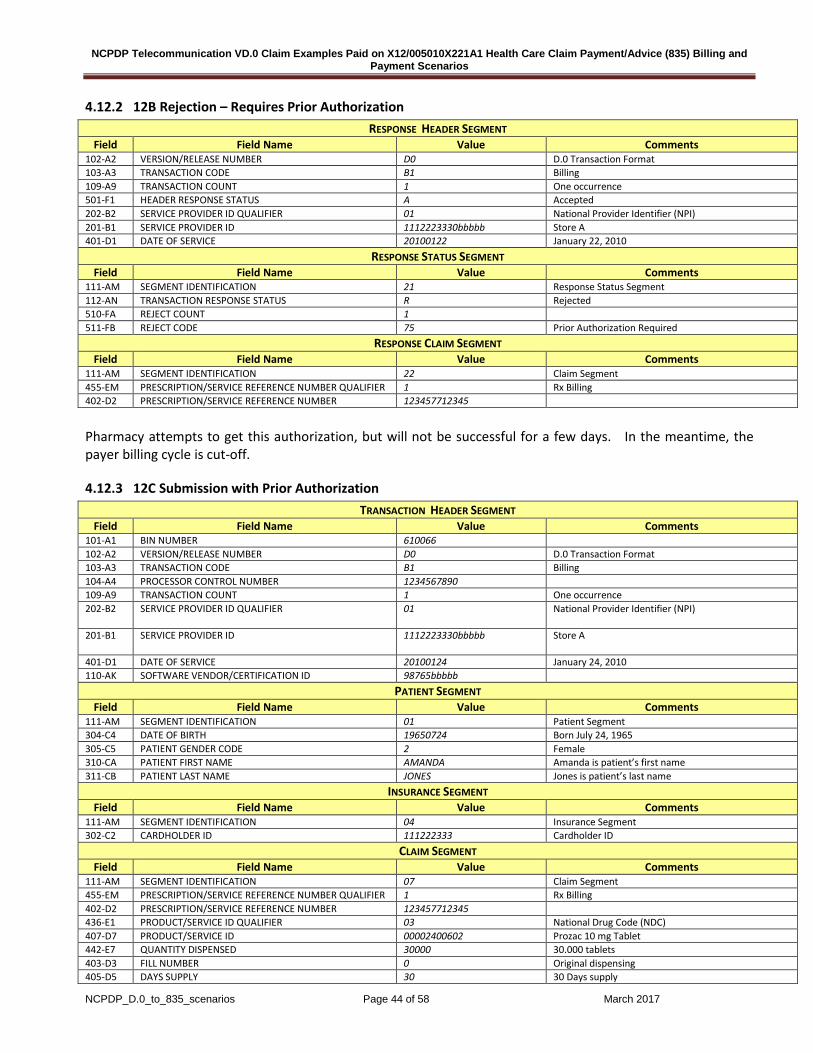
NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 44 of 58 March 2017
4.12.2 12B Rejection – Requires Prior Authorization RESPONSE HEADER SEGMENT
Field Field Name Value Comments 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100122 January 22, 2010
RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS R Rejected 510-FA REJECT COUNT 1 511-FB REJECT CODE 75 Prior Authorization Required
RESPONSE CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 22 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER QUALIFIER 1 Rx Billing 402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123457712345
Pharmacy attempts to get this authorization, but will not be successful for a few days. In the meantime, the payer billing cycle is cut-off.
4.12.3 12C Submission with Prior Authorization TRANSACTION HEADER SEGMENT
Field Field Name Value Comments 101-A1 BIN NUMBER 610066 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI)
201-B1 SERVICE PROVIDER ID 1112223330bbbbb
Store A
401-D1 DATE OF SERVICE 20100124 January 24, 2010 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
PATIENT SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 01 Patient Segment 304-C4 DATE OF BIRTH 19650724 Born July 24, 1965 305-C5 PATIENT GENDER CODE 2 Female 310-CA PATIENT FIRST NAME AMANDA Amanda is patient’s first name 311-CB PATIENT LAST NAME JONES Jones is patient’s last name
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 111222333 Cardholder ID
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER QUALIFIER 1 Rx Billing 402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123457712345 436-E1 PRODUCT/SERVICE ID QUALIFIER 03 National Drug Code (NDC) 407-D7 PRODUCT/SERVICE ID 00002400602 Prozac 10 mg Tablet 442-E7 QUANTITY DISPENSED 30000 30.000 tablets 403-D3 FILL NUMBER 0 Original dispensing 405-D5 DAYS SUPPLY 30 30 Days supply

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 45 of 58 March 2017
406-D6 COMPOUND CODE 1 Not a compound 408-D8 DISPENSE AS WRITTEN/PRODUCT SELECTION CODE 0 No Product Selection Indicated 414-DE DATE PRESCRIPTION WRITTEN 20100122 January 22, 2010 461-EU PRIOR AUTHORIZATION TYPE CODE 1 462-EV PRIOR AUTHORIZATION NUMBER SUBMITTED 98765432101
PRESCRIBER SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 03 Prescriber Segment 466-EZ PRESCRIBER ID QUALIFIER 01 National Provider Identifier (NPI) 411-DB PRESCRIBER ID 5556667772
PRICING SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 11 Pricing Segment 409-D9 INGREDIENT COST SUBMITTED 910{ $91.00 412-DC DISPENSING FEE SUBMITTED 30{ $3.00 426-DQ USUAL AND CUSTOMARY CHARGE 980{ $98.00 430-DU GROSS AMOUNT DUE 940{ $94.00 423-DN BASIS OF COST DETERMINATION 1 AWP (Average Wholesale Price)
4.12.4 12D Paid – Lower Amount with an Incentive RESPONSE HEADER SEGMENT
Field Field Name Value Comments 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B3 Rx Rebill 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100124 January 24, 2010
RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS P Paid 503-F3 AUTHORIZATION NUMBER ABC13000
RESPONSE CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 22 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER QUALIFIER 1 Rx Billing 402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123457712345
RESPONSE PRICING SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 23 Response Pricing Segment 505-F5 PATIENT PAY AMOUNT 150{ $15.00 506-F6 INGREDIENT COST PAID 850{ $85. 00 507-F7 DISPENSING FEE PAID 30{ $3.00 521-FL INCENTIVE AMOUNT PAID 50{ $5.00 509-F9 TOTAL AMOUNT PAID 780{ $78.00 522-FM BASIS OF REIMBURSEMENT DETERMINATION 3 Cost Reduced to AWP Less X% Pricing
• Contracted rate is less than billed (85.00 + 3.00 = $88.00) • Incentive of 5.00 is added making Net to Pharmacy $93.00 • Copay of 15.00 plus plan payment of 78.00 = $93.00

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 46 of 58 March 2017
4.12.5 835 for vD.0 Response 12D12: CLP – Claim Payment Information
Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “123457712345” – Rx Number CLP02 1029 Claim Status Code ID 1/2 "1" - Processed as primary
CLP03 782 Monetary Amount (Total Claim Charge Amount) R 1/18 “94.00”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 "78.00”
CLP05 782 Monetary Amount (Patient Responsibility Amount) R 1/18 “15.00”
CLP06 1032 Claim Filing Indicator Code ID 1/2 "13” - Point of Service
CLP07 127 Reference Identification (Payer Claim Control Number) AN 1/30 "ABC13000"
NM1 – Patient Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "QC" NM102 1065 Entity Type Qualifier ID 1/1 "1" - Person NM103 1035 Name Last or Organization Name AN 1/35 “JONES” NM104 1036 Name First AN 1/25 "AMANDA” NM108 66 Identification Code Qualifier ID 1/2 "MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “111222333”
NM1 – Service Provider Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "82" – Rendering Provider NM102 1065 Entity Type Qualifier ID 1/1 "2" – Non-Person Entity NM103 1035 Name Last or Organization Name AN 1/35 “STORE A” NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI)
NM109 67 Identification Code (Rendering Provider Identifier) AN 2/80 “1112223330” - NPI
REF – Other Claim Related Identification Ref Elem Description Type Min/Max Data
REF01 128 Reference Identification Qualifier ID 2/3 “G1” – Prior Authorization Number REF02 127 Receiver Identifier AN 1/30 “98765432101”
SVC – Service Payment Information Ref Elem Description Type Min/Max Data
SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 "00002400602"
SVC02 782 Monetary Amount (Line Item Charge Amount) R 1/18 “94.00”
SVC03
782
Line Item Provider Payment Amount
R 1/18 "78.00” SVC05 380 Unit of Service Paid Count R 1/18 “30”
DTM – Service Date Ref Elem Description Type Min/Max Data
DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20100124”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “CO” – Contractual Obligations CAS02 1029 Adjustment Reason Code ID 1/5 “90" - Ingredient cost adjustment CAS03 782 Monetary Amount R 1/18 “6.00” CAS05 1029 Adjustment Reason Code ID 1/2 “144” – Incentive Adjustment
12 Accredited Standards Committee X12, Insurance Subcommittee, X12N. “10.1.2 Data Use by Business Use” Health Care Claim Payment/Advice (835), 005010X221A1. Washington Publishing Company, Apr. 2006. <http://www.wpc-edi.com>.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 47 of 58 March 2017
CAS06 782 Monetary Amount ID 1/5 “-5.00" CAS – Service Adjustment
Ref Elem Description Type Min/Max Data CAS01 1028 Claim Adjustment Group Code ID 1/2 “PR” – Patient Responsibility CAS02 1029 Adjustment Reason Code ID 1/5 “3" - Co-payment amount CAS03 782 Monetary Amount R 1/18 “15.00”

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 48 of 58 March 2017
4.14 Worker’s Compensation Claim Submission Pharmacy Provider B submits a Claim to a Workers’ Compensation Processor with an administrative fee which is accepted
4.14.1 13A Workers’ Compensation Billing TRANSACTION HEADER SEGMENT
Field Field Name Value Comments 101-A1 BIN NUMBER 610066 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100122 January 22, 2010 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
PATIENT SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 01 Patient Segment 304-C4 DATE OF BIRTH 19620615 Born June 15, 1962 305-C5 PATIENT GENDER CODE 1 Male 310-CA PATIENT FIRST NAME MICKEY Mickey is patient’s first name 311-CB PATIENT LAST NAME SMITH Smith is patient’s last name
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 987654321 Cardholder ID
WORKERS’ COMPENSATION SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 06 Workers’ Compensation Segment 434-DY DATE OF INJURY 20090902 September 2, 2009 315-CF EMPLOYER NAME MA BELL 316-CG EMPLOYER STREET ADDRESS 1234 CAPITAL AVENUE 317-CH EMPLOYER CITY ADDRESS BELLTOWN 318-CI EMPLOYER STATE/PROVINCE ADDRESS UT 319-CJ EMPLOYER ZIP/POSTAL ZONE 88888 320-CK EMPLOYER PHONE NUMBER 8049786421 327-CR CARRIER ID 9087654321 435-DZ CLAIM/REFERENCE ID AA181114
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123456789027 436-E1 PRODUCT/SERVICE ID QUALIFIER 03 National Drug Code (NDC) 407-D7 PRODUCT/SERVICE ID 00006496341 Zostavax 442-E7 QUANTITY DISPENSED 1000 1 Each 403-D3 FILL NUMBER 0 Original dispensing 405-D5 DAYS SUPPLY 1 1 Days supply 406-D6 COMPOUND CODE 1 Not a compound 408-D8 DISPENSED AS WRITTEN (DAW)/PRODUCT SELECTION
CODE 0 No Product Selection Indicated
414-DE DATE PRESCRIPTION WRITTEN 20100122 January 22, 2010 600-28 UNIT OF MEASURE EA Each
PRESCRIBER SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 03 Prescriber Segment 466-EZ PRESCRIBER ID QUALIFIER 01 National Provider Identifier (NPI) 411-DB PRESCRIBER ID 5556667772
PRICING SEGMENT
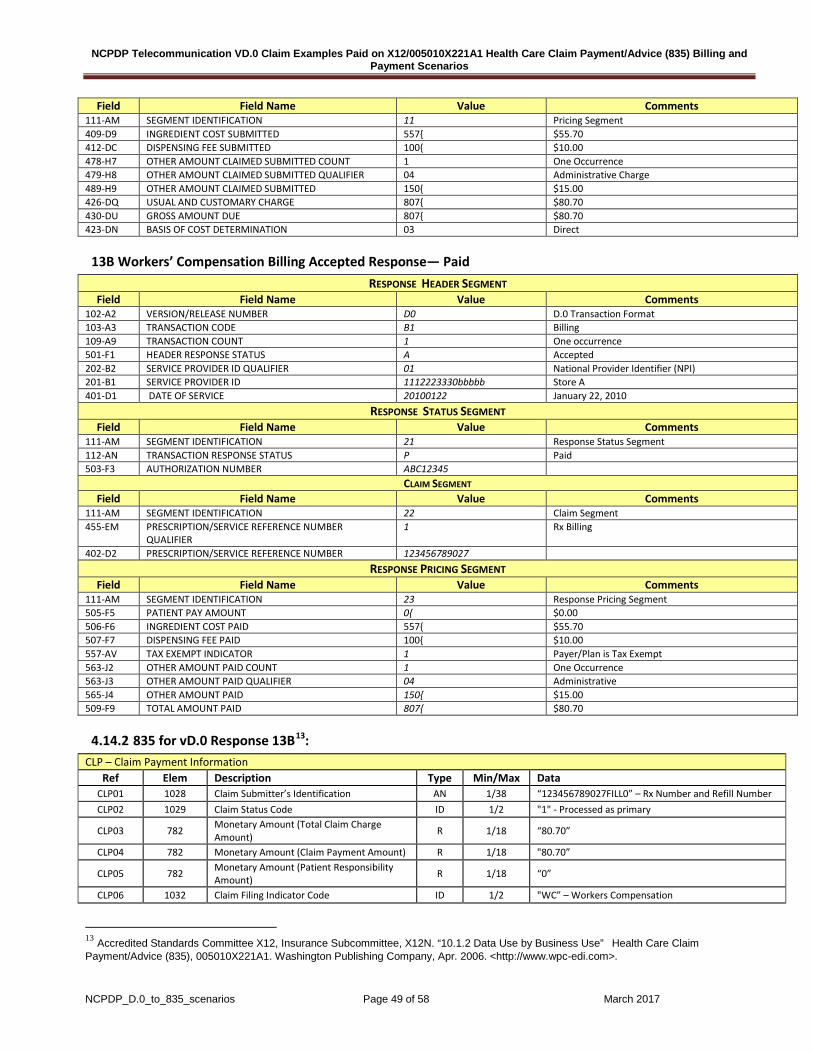
NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 49 of 58 March 2017
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 11 Pricing Segment 409-D9 INGREDIENT COST SUBMITTED 557{ $55.70 412-DC DISPENSING FEE SUBMITTED 100{ $10.00 478-H7 OTHER AMOUNT CLAIMED SUBMITTED COUNT 1 One Occurrence 479-H8 OTHER AMOUNT CLAIMED SUBMITTED QUALIFIER 04 Administrative Charge 489-H9 OTHER AMOUNT CLAIMED SUBMITTED 150{ $15.00 426-DQ USUAL AND CUSTOMARY CHARGE 807{ $80.70 430-DU GROSS AMOUNT DUE 807{ $80.70 423-DN BASIS OF COST DETERMINATION 03 Direct
13B Workers’ Compensation Billing Accepted Response— Paid RESPONSE HEADER SEGMENT
Field Field Name Value Comments 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 1112223330bbbbb Store A 401-D1 DATE OF SERVICE 20100122 January 22, 2010
RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS P Paid 503-F3 AUTHORIZATION NUMBER ABC12345
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 22 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 123456789027 RESPONSE PRICING SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 23 Response Pricing Segment 505-F5 PATIENT PAY AMOUNT 0{ $0.00 506-F6 INGREDIENT COST PAID 557{ $55.70 507-F7 DISPENSING FEE PAID 100{ $10.00 557-AV TAX EXEMPT INDICATOR 1 Payer/Plan is Tax Exempt 563-J2 OTHER AMOUNT PAID COUNT 1 One Occurrence 563-J3 OTHER AMOUNT PAID QUALIFIER 04 Administrative 565-J4 OTHER AMOUNT PAID 150{ $15.00 509-F9 TOTAL AMOUNT PAID 807{ $80.70
4.14.2 835 for vD.0 Response 13B13: CLP – Claim Payment Information
Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “123456789027FILL0” – Rx Number and Refill Number CLP02 1029 Claim Status Code ID 1/2 "1" - Processed as primary
CLP03 782 Monetary Amount (Total Claim Charge Amount) R 1/18 “80.70”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 "80.70”
CLP05 782 Monetary Amount (Patient Responsibility Amount) R 1/18 “0”
CLP06 1032 Claim Filing Indicator Code ID 1/2 "WC” – Workers Compensation
13 Accredited Standards Committee X12, Insurance Subcommittee, X12N. “10.1.2 Data Use by Business Use” Health Care Claim Payment/Advice (835), 005010X221A1. Washington Publishing Company, Apr. 2006. <http://www.wpc-edi.com>.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 50 of 58 March 2017
CLP07 127 Reference Identification (Payer Claim Control Number) AN 1/30 "ABC12345"
NM1 – Patient Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "QC" NM102 1065 Entity Type Qualifier ID 1/1 "1" - Person NM103 1035 Name Last or Organization Name AN 1/35 “SMITH” NM104 1036 Name First AN 1/25 "MICKEY” NM108 66 Identification Code Qualifier ID 1/2 "MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “987654321”
NM1 – Service Provider Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "82" – Rendering Provider NM102 1065 Entity Type Qualifier ID 1/1 "2" – Non-Person Entity
NM103 1035 Name Last or Organization Name (Pharmacy Name) AN 1/35 “STORE A”
NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI) NM109 67 Identification Code AN 2/80 “1112223330” - NPI
SVC – Service Payment Information Ref Elem Description Type Min/Max Data
SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 "00006496341" SVC02 782 Monetary Amount (Monetary Amount (Line
Item Charge Amount)) R 1/18 “80.70”
SVC03 782 Monetary Amount (Line Item Provider Payment Amount)
R 1/18 "80.70”
SVC05 380 Quantity (Unit of Service Paid Count) R 1/18 “1”
DTM – Service Date Ref Elem Description Type Min/Max Data
DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20100122”

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 51 of 58 March 2017
4.16 Health Savings Account (HSA) Claim Submission Pharmacy Provider B submits a Claim to the Processor for which patient is eligible for plan-assisted benefits due to a Health Savings Account.
4.16.1 14A Claim Submission TRANSACTION HEADER SEGMENT
Field Field Name Value Comments 101-A1 BIN NUMBER 610066 102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Format 103-A3 TRANSACTION CODE B1 Billing 104-A4 PROCESSOR CONTROL NUMBER 1234567890 109-A9 TRANSACTION COUNT 1 One occurrence 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI)
201-B1 SERVICE PROVIDER ID 4445556661bbbbb
Store B
401-D1 DATE OF SERVICE 20100122 January 22, 2010 110-AK SOFTWARE VENDOR/CERTIFICATION ID 98765bbbbb
PATIENT SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 01 Patient Segment 304-C4 DATE OF BIRTH 19620615 Born June 15, 1962 305-C5 PATIENT GENDER CODE 1 Male 310-CA PATIENT FIRST NAME CASPER Casper is patient’s first name 311-CB PATIENT LAST NAME MILLER Miller is patient’s last name
INSURANCE SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 04 Insurance Segment 302-C2 CARDHOLDER ID 121212121 Cardholder ID
CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 07 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 PRESCRIPTION/SERVICE REFERENCE NUMBER 1234575 436-E1 PRODUCT/SERVICE ID QUALIFIER 03 National Drug Code (NDC) 407-D7 PRODUCT/SERVICE ID 00006094228 Clinoril 200mg 442-E7 QUANTITY DISPENSED 30000 30.000 tablets 403-D3 FILL NUMBER 0 Original dispensing 405-D5 DAYS SUPPLY 30 30 Days supply 406-D6 COMPOUND CODE 1 Not a compound 408-D8 DISPENSED AS WRITTEN (DAW)/PRODUCT SELECTION
CODE 2 Patient Requested Brand
414-DE DATE PRESCRIPTION WRITTEN 20100122 January 22, 2010 PRICING SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 11 Pricing Segment 409-D9 INGREDIENT COST SUBMITTED 950{ $95.00 412-DC DISPENSING FEE SUBMITTED 50{ $5.00 426-DQ USUAL AND CUSTOMARY CHARGE 1007{ $100.70 430-DU GROSS AMOUNT DUE 1000{ $100.00 423-DN BASIS OF COST DETERMINATION 1 AWP (Average Wholesale Price)
DUR/PPS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 08 DUR/PPS Segment 473-7E DUR/PPS CODE COUNTER 1 1st DUR action 439-E4 REASON FOR SERVICE CODE PS Product Selection 440-E5 PROFESSIONAL SERVICE CODE M0 Prescriber consulted 441-E6 RESULT OF SERVICE CODE 1B Rx filled as is

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 52 of 58 March 2017
4.16.2 14B Claim Paid
Patient Pay Amount is reduced to $15.00 due to the Health Savings Plan.
RESPONSE HEADER SEGMENT Field Field Name Value Comments
102-A2 VERSION/RELEASE NUMBER D0 D.0 Transaction Standard 103-A3 TRANSACTION CODE B1 Billing 109-A9 TRANSACTION COUNT 1 One occurrence 501-F1 HEADER RESPONSE STATUS A Accepted 202-B2 SERVICE PROVIDER ID QUALIFIER 01 National Provider Identifier (NPI) 201-B1 SERVICE PROVIDER ID 4445556661bbbbb Store B 401-D1 DATE OF SERVICE 20100122 January 22, 2010
RESPONSE STATUS SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 21 Response Status Segment 112-AN TRANSACTION RESPONSE STATUS P Paid
RESPONSE CLAIM SEGMENT Field Field Name Value Comments
111-AM SEGMENT IDENTIFICATION 22 Claim Segment 455-EM PRESCRIPTION/SERVICE REFERENCE NUMBER
QUALIFIER 1 Rx Billing
402-D2 RX /SERVICE REFERENCE NUMBER 1234575 RESPONSE PRICING SEGMENT
Field Field Name Value Comments 111-AM SEGMENT IDENTIFICATION 23 Response Pricing Segment 505-F5 PATIENT PAY AMOUNT 150{ $15.00 506-F6 INGREDIENT COST PAID 950{ $95.00 507-F7 DISPENSING FEE PAID 50{ $5.00 509-F9 TOTAL AMOUNT PAID 850{ $85.00 522-FM BASIS OF REIMBURSEMENT DETERMINATION 1 Ingredient Cost Paid as Submitted 518-FI AMOUNT OF COPAY 100{ $10.00 517-FH AMOUNT APPLIED TO PERIODIC DEDUCTIBLE 200{ $20.00 135-UM AMOUNT ATTRIBUTED TO PRODUCT SELECTION/NON-
FORMULARY SELECTION 50{ $5.00
129-UD HEALTH PLAN FUNDED ASSISTANCE AMOUNT 200{ -$20.00 128-UC SPENDING ACCOUNT AMOUNT REMAINING 9800{ $980.00
4.16.3 835 Response for vD.0 Response 14B14: CLP – Claim Payment Information
Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “1234575FILL 0” – Rx Number and Refill Number CLP02 1029 Claim Status Code ID 1/2 "1" - Processed as primary
CLP03 782 Monetary Amount (Total Claim Charge Amount) R 1/18 “100.00”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 "85.00”
CLP05 782 Monetary Amount (Patient Responsibility Amount) R 1/18 “15.00”
CLP06 1032 Claim Filing Indicator Code ID 1/2 "13” - Point of Service
CLP07 127 Reference Identification (Payer Claim Control Number) AN 1/30 "123456789123456789"
NM1 – Patient Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "QC" NM102 1065 Entity Type Qualifier ID 1/1 "1" - Person NM103 1035 Name Last or Organization Name AN 1/35 “MILLER” NM104 1036 Name First AN 1/25 "CASPER”
14 Accredited Standards Committee X12, Insurance Subcommittee, X12N. “10.1.2 Data Use by Business Use” Health Care Claim Payment/Advice (835), 005010X221A1. Washington Publishing Company, Apr. 2006. <http://www.wpc-edi.com>.
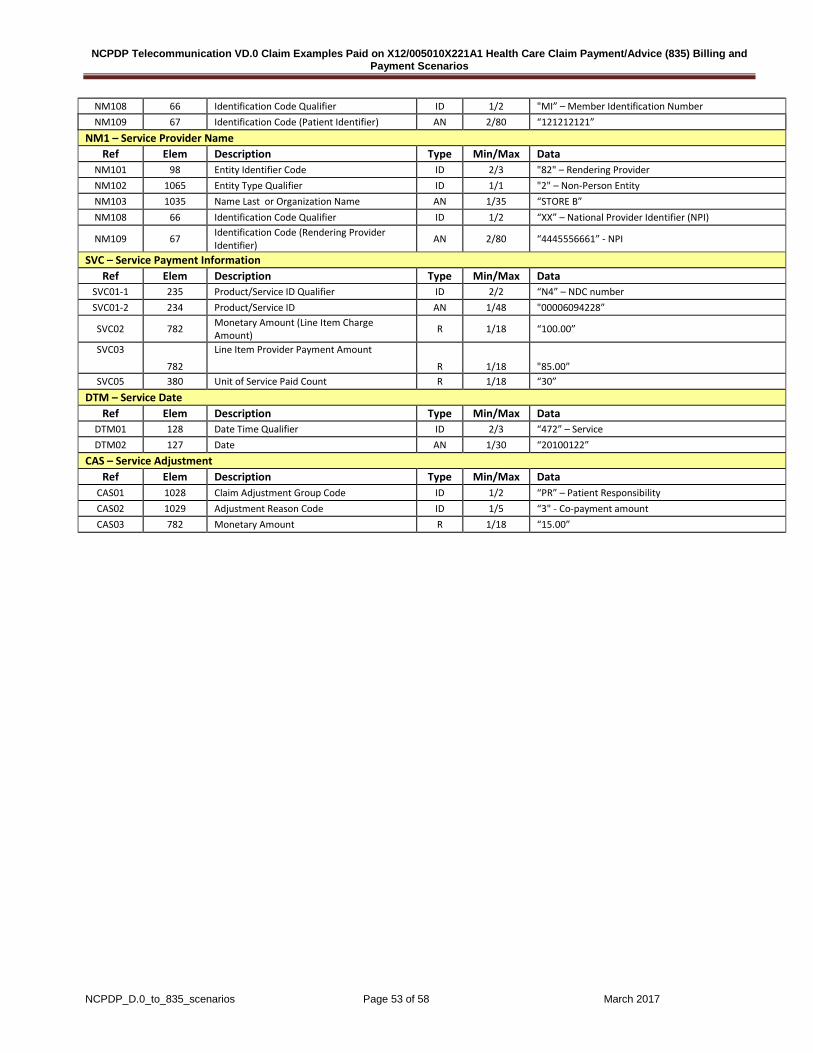
NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 53 of 58 March 2017
NM108 66 Identification Code Qualifier ID 1/2 "MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “121212121”
NM1 – Service Provider Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "82" – Rendering Provider NM102 1065 Entity Type Qualifier ID 1/1 "2" – Non-Person Entity NM103 1035 Name Last or Organization Name AN 1/35 “STORE B” NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI)
NM109 67 Identification Code (Rendering Provider Identifier) AN 2/80 “4445556661” - NPI
SVC – Service Payment Information Ref Elem Description Type Min/Max Data
SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 "00006094228”
SVC02 782 Monetary Amount (Line Item Charge Amount) R 1/18 “100.00”
SVC03
782
Line Item Provider Payment Amount
R 1/18 "85.00” SVC05 380 Unit of Service Paid Count R 1/18 “30”
DTM – Service Date Ref Elem Description Type Min/Max Data
DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20100122”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “PR” – Patient Responsibility CAS02 1029 Adjustment Reason Code ID 1/5 “3" - Co-payment amount CAS03 782 Monetary Amount R 1/18 “15.00”
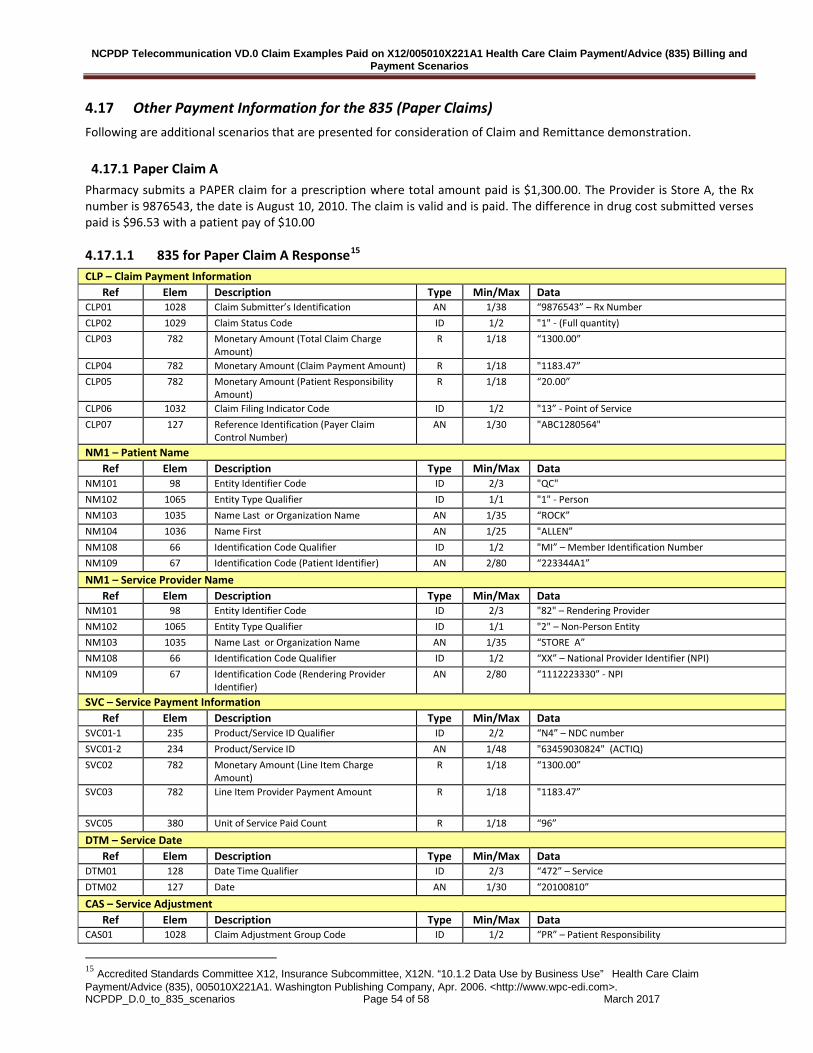
NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 54 of 58 March 2017
4.17 Other Payment Information for the 835 (Paper Claims) Following are additional scenarios that are presented for consideration of Claim and Remittance demonstration.
4.17.1 Paper Claim A Pharmacy submits a PAPER claim for a prescription where total amount paid is $1,300.00. The Provider is Store A, the Rx number is 9876543, the date is August 10, 2010. The claim is valid and is paid. The difference in drug cost submitted verses paid is $96.53 with a patient pay of $10.00
4.17.1.1 835 for Paper Claim A Response15 CLP – Claim Payment Information
Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “9876543” – Rx Number CLP02 1029 Claim Status Code ID 1/2 "1" - (Full quantity) CLP03 782 Monetary Amount (Total Claim Charge
Amount) R 1/18 “1300.00”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 "1183.47” CLP05 782 Monetary Amount (Patient Responsibility
Amount) R 1/18 “20.00”
CLP06 1032 Claim Filing Indicator Code ID 1/2 "13” - Point of Service CLP07 127 Reference Identification (Payer Claim
Control Number) AN 1/30 "ABC1280564"
NM1 – Patient Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "QC" NM102 1065 Entity Type Qualifier ID 1/1 "1" - Person NM103 1035 Name Last or Organization Name AN 1/35 “ROCK” NM104 1036 Name First AN 1/25 "ALLEN” NM108 66 Identification Code Qualifier ID 1/2 "MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “223344A1”
NM1 – Service Provider Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "82" – Rendering Provider NM102 1065 Entity Type Qualifier ID 1/1 "2" – Non-Person Entity NM103 1035 Name Last or Organization Name AN 1/35 “STORE A” NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI) NM109 67 Identification Code (Rendering Provider
Identifier) AN 2/80 “1112223330” - NPI
SVC – Service Payment Information Ref Elem Description Type Min/Max Data
SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 "63459030824" (ACTIQ) SVC02 782 Monetary Amount (Line Item Charge
Amount) R 1/18 “1300.00”
SVC03 782 Line Item Provider Payment Amount R 1/18 "1183.47”
SVC05 380 Unit of Service Paid Count R 1/18 “96”
DTM – Service Date Ref Elem Description Type Min/Max Data
DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20100810”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “PR” – Patient Responsibility
15 Accredited Standards Committee X12, Insurance Subcommittee, X12N. “10.1.2 Data Use by Business Use” Health Care Claim Payment/Advice (835), 005010X221A1. Washington Publishing Company, Apr. 2006. <http://www.wpc-edi.com>.

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 55 of 58 March 2017
CAS02 1029 Adjustment Reason Code ID 1/5 “3" - Co-payment amount CAS03 782 Monetary Amount R 1/18 “20.00”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “CO” – Contractual Obligations CAS02 1029 Adjustment Reason Code ID 1/5 “90" - Ingredient cost adjustment CAS03 782 Monetary Amount R 1/18 “96.53”
4.17.2 Paper Claim B Pharmacy submits a PAPER claim for a prescription for $700.00. The Provider is Store B, the Rx number is 9876544 and the date of service is August 10, 2010. The claim is rejected because “Member was not found in payer database”.
4.17.2.1 835 for Paper Claim B Response16 CLP – Claim Payment Information
Ref Elem Description Type Min/Max Data CLP01 1028 Claim Submitter’s Identification AN 1/38 “9876544” – Rx Number CLP02 1029 Claim Status Code ID 1/2 "4" - Denied CLP03 782 Monetary Amount (Total Claim Charge
Amount) R 1/18 “700.00”
CLP04 782 Monetary Amount (Claim Payment Amount) R 1/18 "0” CLP05 782 Monetary Amount (Patient Responsibility
Amount) R 1/18
CLP06 1032 Claim Filing Indicator Code ID 1/2 "13” - Point of Service CLP07 127 Reference Identification (Payer Claim
Control Number) AN 1/30 " ABC1280935"
NM1 – Patient Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "QC" NM102 1065 Entity Type Qualifier ID 1/1 "1" - Person NM103 1035 Name Last or Organization Name AN 1/35 “ROCK” NM104 1036 Name First AN 1/25 "HILDA” NM108 66 Identification Code Qualifier ID 1/2 "MI” – Member Identification Number NM109 67 Identification Code (Patient Identifier) AN 2/80 “987654001”
NM1 – Service Provider Name Ref Elem Description Type Min/Max Data
NM101 98 Entity Identifier Code ID 2/3 "82" – Rendering Provider NM102 1065 Entity Type Qualifier ID 1/1 "2" – Non-Person Entity NM103 1035 Name Last or Organization Name AN 1/35 “STORE B” NM108 66 Identification Code Qualifier ID 1/2 “XX” – National Provider Identifier (NPI) NM109 67 Identification Code (Rendering Provider
Identifier) AN 2/80 “4445556661” - NPI
SVC – Service Payment Information Ref Elem Description Type Min/Max Data
SVC01-1 235 Product/Service ID Qualifier ID 2/2 “N4” – NDC number SVC01-2 234 Product/Service ID AN 1/48 "00186504031" (Nexium) SVC02 782 Monetary Amount (Line Item Charge
Amount) R 1/18 “700.00”
SVC03 782 Line Item Provider Payment Amount R 1/18 "0”-
SVC05 380 Unit of Service Paid Count R 1/18 “180”
DTM – Service Date Ref Elem Description Type Min/Max Data
16 Accredited Standards Committee X12, Insurance Subcommittee, X12N. “10.1.2 Data Use by Business Use” Health Care Claim Payment/Advice (835), 005010X221A1. Washington Publishing Company, Apr. 2006. <http://www.wpc-edi.com>.
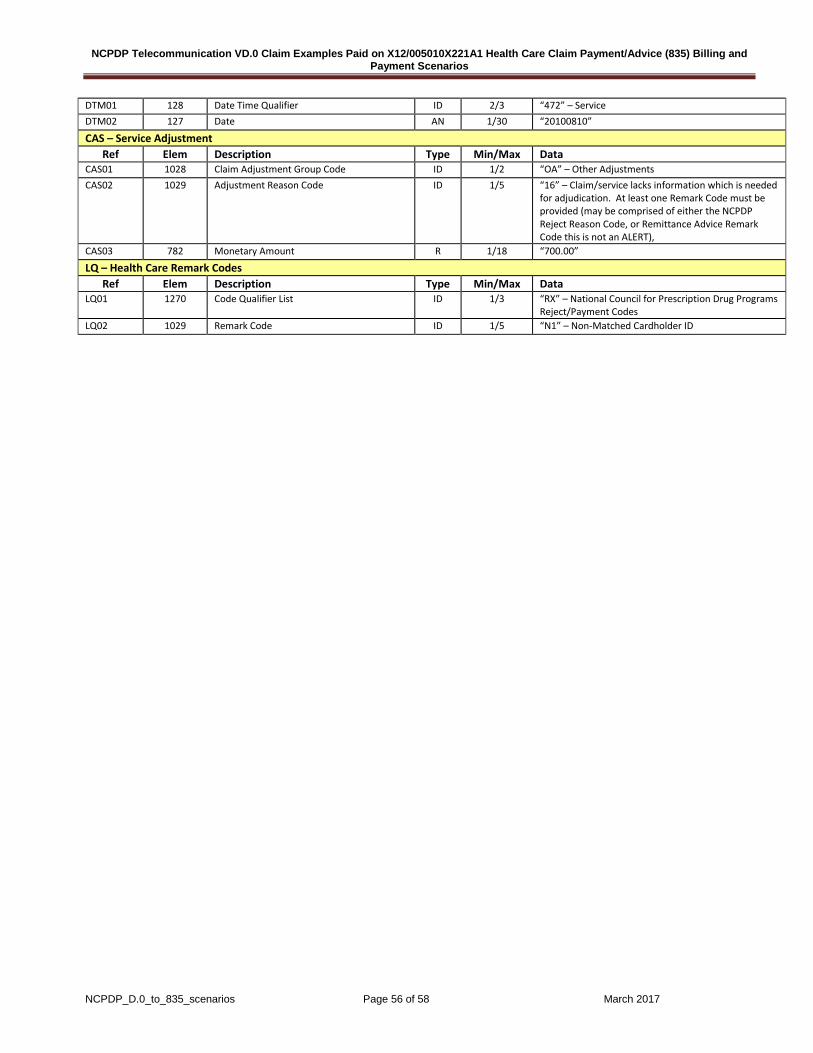
NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 56 of 58 March 2017
DTM01 128 Date Time Qualifier ID 2/3 “472” – Service DTM02 127 Date AN 1/30 “20100810”
CAS – Service Adjustment Ref Elem Description Type Min/Max Data
CAS01 1028 Claim Adjustment Group Code ID 1/2 “OA” – Other Adjustments CAS02 1029 Adjustment Reason Code ID 1/5 “16” – Claim/service lacks information which is needed
for adjudication. At least one Remark Code must be provided (may be comprised of either the NCPDP Reject Reason Code, or Remittance Advice Remark Code this is not an ALERT),
CAS03 782 Monetary Amount R 1/18 “700.00”
LQ – Health Care Remark Codes Ref Elem Description Type Min/Max Data
LQ01 1270 Code Qualifier List ID 1/3 “RX” – National Council for Prescription Drug Programs Reject/Payment Codes
LQ02 1029 Remark Code ID 1/5 “N1” – Non-Matched Cardholder ID

NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 57 of 58 March 2017
5. Discussion
NCPDP Telecommunication VD.0 Claim Examples Paid on X12/005010X221A1 Health Care Claim Payment/Advice (835) Billing and Payment Scenarios
NCPDP_D.0_to_835_scenarios Page 58 of 58 March 2017
6. Revision History 1. March 2017 – Editorial updates to remove slashed zeros (Ø) and replace with zero (0), add the new NCPDP logo and change X12 name from ASC X12 to X12.





























