Embed Size (px)
Citation preview

73
NCP FORUMClinical Rounds With Nutrition Support Services*From The University of Michigan
Debra S. Kovacevich, RN, MPH, CNSNClinical Manager
Carol L. Braunschweig, RD, MS, CNSDClinical Nutrition Specialist
Patricia Couch, PharmDClinical Pharmacist
Correspondence and Reprint Requests: Debra S. Kovacevich,RN, MPH, Parenteral and Enteral Nutrition Team, University ofMichigan Hospitals, 1500 E Medical Center Drive, UH-B2D301,Box 0008, Ann Arbor, MI 48109-0008.
*Presented at the A.S.P.E.N. 17th Clinical Congress, February14-17, 1993, San Diego, CA.
The editors of Nutrition in Clinical Prac-tice held a session entitled &dquo;NCP Forum:
Clinical Rounds With Nutrition SupportServices&dquo; at the 17th Clinical Congress inSan Dingo, California, last year. Two nutri-tion support teams presented a case anddescribed how each member of the teaminteracted with the patient to effect a suc-
r ~ce~sful outeame., One team was from the~~:¡;£a~yela1).~ Clinic ~in-~hiog the other, frorn~tne University of Michigan in Ann Arbor. .: .= Below are excerpts from the.Univêt9i’:v’of Michigan team’s presentation.
1 ?/2 The Parenteral and Enteral Nutrition.,&dquo; : I£4m . &om ,the University. of Michigan ismade up of a clinical nurse manager three . b
i nurse clinicians, two clinical pharmacists, ° z
and two ,nutrition specialists. Members of’.,.ik,e’team Presenting this case include --1<~;’:.~~~~::~:::~:::: . :: jj
~ F ~ ~ s a ~ ~~.~?~~rai ~. ~ouc~.ce ~rae~, R.~V~ ~~~ ~~~~~~ ~ ~ H~ ~s Q ,
Clinical lYlan.a~e~:&~’ w ~~ ~a _ ~ Pe , y, ~:: . : CI~nical,Man~~,¥:i?:3~:;:H~~:;’:i~¡~~;
~~ ~ ~~ ~ 2 r ~’~t~t~ .~~ ‘ B~ic~r~~i:se~i~,~~~‘, ~.13;s ~~, ~~~1) , ;:. &,..&dquo;., g, ’RD. -MS, CNSD’4~ ~° ~ ;° €)linical Nutx*iti<Mi’ Specialist~;::;
:~~’~«~t~ 0~ :~;, ~ ~;:~ ~ ~ e
_
’
~~~~, u~~~’~ ~y;~,~,~.ea ~ s ~~ ~ Couch, PharmD .. d ~ ~ ~tr iei~ Couch, PharmD.
.
Ct liaical Pharmacist~~ , 0 . j , _ t: #]joical .:.. ’l &dquo; Pharmacist .
~ ; ..
~~~~avid.’august, MD, cU~i~a1’ dire~tor o~’&dquo;’°b6ih’th£’Chr£ Teahi.apgihe ~teer~i:r~~e~c~~-~. or. :n:titiee managed the case but was unable tor~Ø11ticipate.>... &dquo; ~.--- .. ------ ----. -.
Ms Kovacevich: The patient, HH, is 19 years old;his height is 206 cm (6 ft 9 in.); and his weight is 91.8kg (around 202 lb). He had no previous medical ornutritional history. He came to our emergency facilitywith a 60-hour history of severe abdominal pain.Findings on physical examination were as follows:heart rate, 150 bpm; respiratory rate, 42 bpm; tem-perature, 37.9°C; orthostatic hypotension. Laboratoryfindings were significant for a white blood cell count of11.3 x IOI/L, with 54% bands. Other findings were aserum HC03 of 16 mEq/L; elevated liver enzyme tests,specifically SGOT and SGPT over 2000 IU; and aprothrombin time of 19.3 seconds.HH was immediately taken to the operating room
following rapid fluid resuscitation. An exploratorylaparotomy showed necrotic bowel extending from themidjejunum to the splenic flexure of the colon. Theliver was ischemic. Neither the celiac axis nor superiormesenteric artery pulses were present. However,pulses were detected in the aorta and both renalarteries.The necrotic bowel was resected, leaving an end-
jejunostomy and a Hartmann’s pouch up to the
midascending colon; about 200 cm of viable smallbowel remained. He was immediately taken to theradiology department for further evaluation of thesplanchnic ischemia. Angiography (Fig. 1) showedflow to his renal arteries but no flow to the celiac or thesuperior mesenteric artery. He was again taken im-mediately to the operating room, where his liver wasrevascularized by means of an autogenous reversesaphenous vein graft from the right common iliacartery to the proper hepatic artery. Collateral circula-tion via the gastroduodenal artery also helped restoreblood flow to the remaining small bowel.
Forty-eight hours later HH was taken to the oper-ating room for a second-look laparotomy. His boweland liver were well perfused, and a gastrostomy tubewas placed to facilitate drainage and to begin earlyenteral feedings.
Postoperatively, the patient had persistent elevatedliver function tests and sepsis. On July 3 a heartmurmur was detected. A cardiac ultrasound revealedan aortic dissection and a probable marfanoid aorta,which was later confirmed by angiogram. Figure 2shows the results of the second angiogram, whichindicated that the aorta was more than twice thenormal size.The physical examination and laboratory findings
Correspondence and Reprint Requests: Debra S. Kovacevich,RN, MPH, Parenteral and Enteral Nutrition Team, University ofMichigan Hospitals, 1500 E Medical Center Drive, UH-B2D301,Box 0008, Ann Arbor, MI 48109-0008.
*Presented at the A.S.P.E.N. 17th Clinical Congress, February14-17, 1993, San Diego, CA.

74
suggested a possible diagnosis of Marfan syndrome. Letme briefly review the signs and symptoms of this disorder.
Marfan’s syndrome is an autosomal dominant, in-herited disorder of collagen that affects four to sixpeople per 100,000. Clinical signs include subluxationof the lens of the eye, arachnodactyly, extreme limblength, aortic dissection, and aortic valve incompe-tence. HH displayed all these signs.
Life expectancy of an individual with Marfan’ssyndrome is about 30 to 40 years. Approximately 95%of all deaths are related to cardiovascular complica-tions, specifically aortic rupture. The condition isdiagnosed anthropometrically by measuring the armspan and comparing it with the patient’s height. HH’sarm span was a foot longer than his height. Normallythe two measurements are about the same.
Such patients usually are taken immediately to theoperating room to correct the dissection. However, HHstill had considerable hemostatic instability and re-mained septic. He had a large wound to granulate;therefore, surgery was delayed until these conditionswere resolved.
Figure 1. Abdominal aortogram obtained immediatelyfollowing initial laparotomy for resection of necrotic bowel.Renal arteries are apparently normal, but the celiac andsuperior mesenteric arteries are not seen. There is nointimal flap visible in this study. After the angiogram, thepatient was immediately returned to the operating roomfor revascularization of his splanchnic circulation.
Dr August decided on conservative therapy, whichconsisted of aggressive enteral and parenteral nutri-tion support (basically parenteral, because enteralsupport failed) and antibiotic therapy. However, re-fractory hypertension developed, which was thoughtsecondary to further extension of the dissection to therenal arteries. Fenestration of the dissection in theabdominal aorta was performed angiographicallywitha guidewire and dilating balloon (Fig. 3). The patient’shypertension improved dramatically. About 10 daysafter complete resolution of all his signs and symptomsof sepsis, his aortic valve, aortic root, and ascendingthoracic aorta were replaced with a composite graft.
POSTOPERATIVE RECOVERY
HH recovered slowly but uneventfully from thisprocedure. However, during his 2 months of hospital-ization, he became very dependent on his mother. Hewouldn’t let her out of his sight, and she became theprimary decision-maker for him. This was surprising,because he seemed to be a fairly independent person.
Figure 2. Thoracic aortogram obtained 5 days after admis-sion. The aortic root is dilated and an intimal flap is barelyvisible in the descending thoracic aorta approximately 5 cmdistal to the aortic arch.

75
He had graduated from high school and moved toFlorida, where he completed one successful year ofcollege. To help him regain his independence, themedical team wanted to send him home as soon as
possible. We tried several times to feed him enterallybut failed.
Ultimately, the patient was discharged on homeparenteral nutrition (HPN) August 31. Two weekslater after his discharge, he was readmitted for cath-
Figure 3. Fenestration of the intimal flap within theabdominal aorta to improve renal blood flow and palliaterenovascular hypertension. The catheter was insertedpercutaneously via the right femoral artery. The catheterwas then manipulated so that the balloon traversed theintimal flap, passing from the true lumen caudal to the falselumen cephalad. Inflation of the balloon created a commonlumen, augmenting renal blood flow and simplifying man-agement of the patient’s hypertension.
eter sepsis. At that time the medical team evaluatedthe risks and the long-term plan for HH. Dr Augustwas to take down his jejunostomy in 6 months to 1year. However, we wondered if the risk of malnutri-tion was greater than the risk of infection of the valveand the graft from placing another catheter.Dr August elected to use the gastrostomy tube and
discharged HH home on tube feedings. He was subse-quently readmitted twice for dehydration; his jejunos-tomy was finally taken down in October and hisgastrointestinal tract continuity restored. MsBraunschweig will discuss nutrition support for thepatient.
NUTRITIONAL GOALS
Ms Braunschweig: Our first goal of nutritionsupport is to maintain the patient’s admission nutri-tional status. That is almost never possible for some-one as critically ill-though well nourished-as HHwas. Our goal for patients admitted to the intensivecare unit is not to replenish but rather to maintain theadmission nutritional status. We try to introduceenteral nutrition support as soon as possible.
In HH’s case, the second component of managementconsisted of electrolyte manipulation. As mentionedearlier, HH had problems with hypertension beforefenestration was performed, and we had to manipu-late the electrolytes accordingly. Despite renal insuf-ficiency, he never required dialysis; we manipulatedthe TPN solution to meet the requirements. He alsohad hypersecretion of gastric acid (routinely associ-ated with extensive small-bowel resection); we man-aged that problem with H2 antagonists.
CALORIC NEEDS
We rely heavily on our institution’s metabolic labo-ratory, which uses indirect calorimetry to determine apatient’s caloric needs. This was particularly usefulwith HH, who was young, very ill, and unusuallylarge. Without indirect calorimetry I would haveestimated his caloric requirements to be much higherthan what they actually were.HH’s resting energy expenditure needs ranged
from 2500 to 3300 kcal, and we estimated his proteinneeds at 1.2 to 1.5 g/kg of ideal body weight. We beganhis nutrition support with our standard amino acid/dextrose solution and increased the percent aminoacids to 6% with 25% dextrose and one 500-mL bottleof a 20% lipid to provide appoximately 3000 kcal and120 g of protein per day.The electrolyte composition was distinct from our
standard formulation in that we increased the sodiumchloride content to about half normal saline. Wemaximized the amount of potassium at 80 mEq/L. Wealso maximized the amount of magnesium because hewas being so heavily diuresed. He received the stan-dard trace element multivitamin package and ranitidine

76
at 200 mg per day. This is higher than the standarddose of 150 mg per day, but because of his size thechange was deemed necessary.
MICRONUTRIENT NEEDS
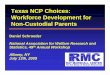
It is not easy to know the micronutrient needs for aphysiologically unique individual such as HH (Fig. 4).HH stands about a foot taller than the average man,forwhom the recommended dietary allowances (RDAs)were established, and his daily requirements areexcessive-more than 3000 kcal. The RDAs were estab-lished essentially to meet 98% of the needs of healthyindividuals, which is effectively what trace elementsin standard vitamin supplementations are intendedfor. HH would represent an alpha error; he does not fiton the bell-shaped curve.As mentioned, HH was well nourished and had no
medical history when he came to us. But when I startinfusing more than 3000 calories in a patient, I wonderwhether the vitamins will meet the patient’s require-ments, because the needs for some nutrients aredetermined by the amount of calories received. Usu-ally, if a patient initially receives two feedings, this isnot a problem. With increased feeding, the patientreceives more micronutrients, vitamins, and miner-als. But for patients on TPN it is a one-size-fits-allsolution, and one wonders whether it will be adequate.The nutrients that predominantly concern us are
thiamin, riboflavin, niacin, and pyridoxine. HH neededthree times the normal amounts of these nutrientswhich were adequately provided with the standardMVI dose. We occasionallv double the MVI dose for 5
Figure 4. HH at age 21 (with his mother).
to 10 days with depleted patients who have highcaloric requirements. We use these trace element andvitamin packages to meet individual requirements,and with HH, we clearly needed to address this.
ENTERAL SUPPORT
We had to consider two areas regarding introducingenteral support: gastric versus small-bowel route, andpolymeric versus defined elemental formula. The lit-erature supports proceeding as proximally as possiblewith patients who have had a significant small-bowelresection. The goal is to expose the remaining intes-tine to the nutrition so as to get maximum hypertro-phy of the gastrointestinal remnant. The same appliesto the polymeric versus the elemental formula. Theliterature supports polymeric because exposure tomore complex nutrients results in maximal hypertro-phy of the remnant.
It has previously been determined that for success-ful nutrition support of patients who have had exten-sive small-bowel resection, the chance of effectiveenteral support is much more favorable under thefollowing conditions: the extent of the resection is lessthan 80%, the jejunum rather than the ileum has beenresected, no gastrointestinal disease is present in theremaining bowel, and the patient still has an ileocecalvalve.
Less than 80% of HH’s bowel was resected, but hehad no ileum. There was no disease in the gastrointes-tinal remnants, but he had no ileocecal valve, and alarge percentage of his colon was resected. In patientswith no ileum, a primary concern is that bile acid willbe depleted toward the end of each day. Such patientscannot resorb the bile acids without the terminalileum,where this kind of absorption takes place. Theyalso become deficient in vitamin B 12 and for the rest oftheir lives must depend on B12 injections.Another concern regarding HH was malabsorption
as a result of bile acid loss. Only the proximal portionof the small bowel remained, and transit time throughthat portion of the bowel is much more rapid than it isthrough the more distal portion. Therefore, we tried tomanipulate the enteral support for HH. It took severalmonths for his gastrointestinal tract to become hyper-trophic enough for successful oral feeding with someenteral feedings at night.
PATIENT COMPLIANCE
Another problem was his noncompliance with low-fat diet restriction. As mentioned earlier, HH re-gressed to about age 15 during his hospital stay. WhenI tried to talk to him about limiting his fat intake (heate large quantities of high-fat foods), he said that hisidea of a major compromise was to go from whole milkto 2%, nothing more. He refused any further dietarymodifications.

77
After HH’s aortic valve, aortic root, and ascendingaorta were repaired, he required permanent anti-coagulation. As a result of drug-nutrient interactions,some alterations in nutrition support were necessary.The need for anticoagulation created a unique situa-tion, because our protocol is to add 5 mg of vitamin Kto all PN solutions for adult patients once per week.However, the primary care service HH was using atthe time initiated warfarin therapy and elected todelete the 5-mg dose of vitamin K from his PN. Thisregimen gradually led to vitamin K deficiency andexcessive anticoagulation (prothrombin time greaterthan 24 seconds without warfarin). The patient’s PNsolution was ultimately supplemented with 1 mg ofvitamin K per day, which permitted safe and predict-able anticoagulation with concurrent warfarin therapy.
VITAMIN K METABOLISM
Dr Couch: The need to anticoagulate HH createdfor us a unique situation. Our protocol dictates theaddition of 5 mg of vitamin K to each TPN solution foradults once weekly. The primary care service initiallyelected to delete all vitamin K from the TPN solutionwhen HH began warfarin therapy. Before I discusswhat I recommended, I want to briefly review vitaminK metabolism.
Metabolically, vitamin K is oxidized via a vitaminK-dependent carboxylase enzyme. This reaction re-sults in the formation of 2,3-vitamin K epoxide, aninactive metabolite. This reaction, which occurs in thepresence of co2 and molecular oxygen, is important inthat during oxidation, glutamic acid residues on theprecursor proteins for inactive clotting factors un-dergo gamma-carboxylation to form gamma-carboxyglutamate residues. Gamma-carboxylation ofthe clotting factors render them active, enabling themto chelate calcium ions on phospholipid membranes.This interaction facilitates clot formation followinginjury. In the course of its metabolism, 2,3-vitamin Kis subsequently reduced, ultimately resulting in theformation of the active naphthohydroquinone cofac-tor. This process is highly effective in recycling vita-min K epoxide so that it can once again be oxidized andtherefore activate clotting factors.
In HH, or any patient receiving anticoagulanttherapy, this cycle is interrupted. Specifically, warfa-rin blocks the action of the reductase enzymes, prohib-iting regeneration of the active form of vitamin K. Ifvitamin K is not regenerated endogenously and is alsodeleted from a TPN solution, a vitamin K deficiencymay result in conjunction with the existence ofnonfunctional clotting factors. A vitamin K deficiency,coupled with warfarin therapy, may predispose apatient to excessive anticoagulation and increase therisk of hemorrhage.
In addition, vitamin K is an important cofactor inthe gamma-carboxylation of other proteins, such asosteocalcin, which is involved in bone formation.
Finally, proteins C and S, which are involved in
inactivation of clotting factors V and VIII, also requiregamma-carboxylation for activation.We did not want HH to become vitamin-K deficient,
but our current protocol of administering 5 mg ofvitamin K once per week was not ideal, either, becausewe could overcorrect his coagulation status or blockthe action warfarin for an extended period. At thispoint we needed to develop an alternative method ofadministering vitamin K to HH.
In 1975 Anderson and Godal administered 1 mg ofintravenous vitamin K to 20 patients who were receiv-ing warfarin therapy. Before receiving vitamin K, all20 patients had thrombotests within the therapeuticrange of 5% and 10% of normal, indicative of a steadystate ofhypocoagulability. Administration of the 1 mgof vitamin K resulted in a moderate reduction ofwarfarin’s anticoagulant effect, evidenced by athrombotest >12%. The investigators believed, there-fore, that they were able to maintain a predictablestate of anticoagulation and prevent excessive bleed-ing by using 1 mg of vitamin K.
In 1992 Shetty and colleagues studied 31 patientsreceiving warfarin therapy who were in a steady stateof anticoagulation. They divided the patients into twogroups; one group (21 patients) received 0.5 mg ofintravenous vitamin K, and the second group (10patients) received 1 mg. International normalizedratios (INRs) were between 2 and 5.5 in the group ofpatients receiving 0.5 mg of vitamin K 24 hours afterthe dose was given. This is consistent with a stablestate of anticoagulation. According to the guidelinesestablished by the British Society of Haematology,INRs between 4.5 to 7 reflect excessive anticoagulation.Thus these investigators believed that the 0.5-mg dosewas enough to maintain predictable anticoagulation.
It is interesting that 5 of the 10 patients in the groupreceiving the 1-mg dose had INRs less than 2, whichis thought to correlate with inadequate anticoagulation.Thus these investigators concluded that 0.5 mg ofvitamin Kwas sufficient for maintaining a predictablestate of anticoagulation in patients receiving concur-rent warfarin therapy.
Because of HH’s unusually large size, we elected tomaintain him on 1 mg of vitamin K daily while hereceived TPN and a daily dose of warfarin. With thisregimen we were able to maintain a predictable stateof anticoagulation, evidenced by the patient’s pro-thrombin times, which averaged between 15 and 18seconds.When HH was discharged from the hospital, he was
no longer receiving TPN therapy and was able toobtain the necessary amount of vitamin K from hisdiet. He has done well since, continuing with 5 mg ofwarfarin per day and maintaining a predictable stateof anticoagulation.
OUTCOME
Currently, HH is doing well. He is maintainingadequate nutritional status with a low-fat oral diet

78
and 500 mL of a moderate protein, isotonic tubefeeding on a nightly basis. He is also working full time.
AUDIENCE QUESTIONS
Question: You indicate that there were severalattempts to feed the patient. What products were usedin these attempts? How long was the gut inactivebefore enteral feeding was attempted? On what basisdid you decide that enteral feeding was not possible?Ms Braunschweig: The products used were ini-
tially Osmolite HN-not tolerated at 20 mL/hr, switchedto 1/2 strength Criticare-not tolerated at 20 mL/hr.Attempts at enteral feeding were tried on the fifthpostoperative day. Feedings were stopped because ofdistention and high residuals (> twice the previoushourly volume).
Question: If enteral nutrition cannot be used todeliver all the nutrients required, was any consider-ation given to providing some of the feeding enterally?Ms Braunschweig: Initially enteral feedings were
not used because everything infused came out rapidlyand with little digestion. With time, the gut did adaptand enteral support was provided in the evenings.TPN was weaned and the patient was maintained onan oral diet with cyclic night enteral feedings.
SUGGESTED READINGS
1. Anderson P, Godal HC. Predictable reduction in anticoagulantactivity of warfarin by small amounts of vitamin K. Acta MedScand 1975;198:269-70.
2. Cowan GS. Short bowel syndrome: causes and clinical conse-quences. Nutr Supp Serv 1984;4:208-12.
3. Detsky AS, McLaughlin JR, Baker JP, et al. What is subjective
global assessment of nutritional status? JPEN 1987;11:8-13.4. Dietz HC, Cutting GR, Pyeritz RE, et al. Marfan syndrome
caused by a recurrent de novo missense mutation in the fibrillingene. Nature 1991;25:337-9.
5. Faubion WC, Wesley JR, Khalidi N, et al. Total parenteralnutrition catheter sepsis. JPEN 1986;10:642-5.
6. Grant JP. Team approach. In: Handbook of total parenteralnutrition, 2nd ed. Philadelphia: WB Saunders Co, 1992:5-14.
7. Hamaoui E. Assessing the nutrition support team. JPEN1987;11:412-21.
8. Lee B, Godfrey M, Vitale E, et al. Linkage of Marfan syndromeand a phenotypically related disorder to two different fibrillingenes. Nature 1991;25:330-4.
9. Malsen CL, Corson GM, Maddox BK, et al. Partial sequence ofa candidate gene for the Marfan syndrome. Nature 1991;25:334-337.
10. McKusick VA. The defect in Marfan syndrome. Nature1991;25:279-81.
11. Pederson FM, Hamberg O, Hess K, et al. The effect of dietaryvitamin K on warfarin induced anticoagulation. J Int Med1991;229:517-20.
12. Purdum PP, Kirby DF. Short bowel syndrome: a review of therole of nutrition support. JPEN 1991;15:93-101.
13. Regenstein M. Nutrition support teams-alive, well, and stillgrowing. NCP 1992;7:296-301.
14. Rowe DW, Shapiro JR, and Harris ED. Heritable disorders ofconnective tissue. In: Winters R, ed. Textbook of internalmedicine. Philadelphia: JB Lippincott, 1989:1013-7.
15. Shearer MJ, McBurney A, Breckenridge AM, et al. Effect ofwarfarin on the metabolism of phylloquinone (vitamin K):dose-response relationship in man. Clin Sci Mol Med1977;53:62.
16. Shetty HGM, Backhouse G, Bentley DP, et al. Effective rever-sal of warfarin-induced excessive anticoagulation with low dosevitamin K. Thromb Haemost 1992;67:13-5.
17. Shuttie JW. Recent advances in hepatic vitamin K metabolismand function. Hepatology 1987;7:367-76.
18. Taylor LM, Porter JM. Marfan’s syndrome. In: Moore WS,ed. Nonarteriosclerotic vascular disease, vascular surgery-acomprehensive review. Philadelphia: WB Saunders Co, 1991:119-20.