Embed Size (px)
Citation preview

JOURNAL OF CLINICAL AND EXPERIMENTAL NEUROPSYCHOLOGY2008, 30 (5), 501–556
© 2007 Psychology Press, an imprint of the Taylor & Francis Group, an Informa business
http://www.psypress.com/jcen DOI: 10.1080/13803390701550128
NCENLanguage performance in Alzheimer’s disease and mild cognitive impairment: A comparative review
Language Performance In Mci and Ad Vanessa Taler and Natalie A. Phillips
Department of Psychology/Centre for Research in Human Development, Concordia University, Montréal, Québec, Canada, and Bloomfield Centre for Research on Aging, Montréal, Québec, Canada
Mild cognitive impairment (MCI) manifests as memory impairment in the absence of dementia and progresses toAlzheimer’s disease (AD) at a rate of around 15% per annum, versus 1–2% in the general population. It thusconstitutes a primary target for investigation of early markers of AD. Language deficits occur early in AD, andperformance on verbal tasks is an important diagnostic criterion for both AD and MCI. We review language per-formance in MCI, compare these findings to those seen in AD, and identify the primary issues in understandinglanguage performance in MCI and selecting tasks with diagnostic and prognostic value.
INTRODUCTION
Increased life expectancy worldwide has resulted inan increased number of individuals at risk of orsuffering from Alzheimer’s disease (AD), resultingin significant financial and emotional burden forsufferers and their families. Intense research inter-est has thus focused on identifying elderly individ-uals who will develop AD, both to commencepharmacological treatment as early as possible inthe disease course and to allow psychological inter-vention and family and financial planning.
A considerable body of evidence suggests that aprodromal, or preclinical, phase of AD may occuryears before diagnosis. At this stage, alterationscan be detected at both the neuropathological andthe cognitive level. Neuropathological changes areseen in the entorhinal cortex very early in the dis-ease course. Marked neuronal loss (32%) in thisregion can be observed in very mild or questiona-ble AD, as can neurofibrillary tangles and senileplaques in sufficient quantities for a diagnosis ofAD (Gómez-Isla & Hyman, 2003). Increased tauphosphorylation, resulting in the formation of neu-rofibrillary tangles, is one of the earliest markers ofAD and occurs prior to dementia onset (for a
review, see Iqbal et al., 2005). Similarly, volumetricMRI studies have suggested that hippocampalatrophy is seen before dementia onset (Fox,Warrington, Stevens, & Rossor, 1996; Jack et al.,1999; Jack et al., 1997; Visser et al., 1999), and thatthis atrophy progresses subsequent to clinicallyidentifiable dementia (Fox et al., 1996).
Individuals with preclinical AD also manifestalterations in various cognitive domains. Deficitsare seen in episodic memory (Bäckman, Small, &Fratiglioni, 2001; Chen et al., 2001; Elias et al.,2000; Small, Herlitz, Fratiglioni, Almkvist, &Bäckman, 1997; Tierney et al., 1996), executivefunction (Albert, Moss, Tanzi, & Jones, 2001;Chen et al., 2001; Daly et al., 2000), perceptualspeed (Albert et al., 2001, Fabrigoule et al., 1998;Fox, Warrington, Seiffer, Agnew, & Rossor, 1998),verbal ability (Convit et al., 2000; Grober &Kawas, 1997; Jacobs et al., 1995; Linn et al., 1995;Small et al., 1997), visuospatial skill (Albert et al.,2001; Chen et al., 2001; Fowler, Saling, Conway,Semple, & Louis, 2002; Howieson et al., 1997), andattention (Nielsen, Lolk, Andersen, Andersen, &Kragh-Sorenson, 1999; Rubin et al., 1998; Tierneyet al., 1996). As is the focus of this review, deficitsare also observed in the domain of language.
V.T. is supported by a postdoctoral fellowship awarded by the Alzheimer’s Society of Canada/ Fonds de recherche en santé du Québec.Address correspondence to Natalie A. Phillips, Department of Psychology, Concordia University, 7141 Sherbrooke Street West,
Montréal, Québec, Canada H4B 1R6 (E-mail: [email protected]).
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

502 TALER AND PHILLIPS
A number of terms have been used to describeindividuals who exhibit cognitive dysfunction inthe absence of dementia. Kral (1962) proposed theterm benign senescent forgetfulness. Other termsthat have been proposed include age-associatedmemory impairment (AAMI; Crook et al., 1986)and age-associated cognitive decline (AACD; Levy,1994). However, these terms are generally intendedto denote individuals at the extremes of normalaging, rather than those in a preclinical stage ofdementia. Some studies have found increased ratesof conversion to dementia in these groups (Lane &Snowdon, 1989; Richards, Touchon, Ledesert, &Ritchie, 1999), while others have found similarrates in these individuals and in healthy elderlysubjects (Hanninen et al., 1995). The term cognitiveimpairment, no dementia (CIND; Graham et al.,1997) connotes an underlying pathological state,although the underlying etiologies may be varia-ble, resulting in a lack of specificity (Rivas-Vasquez, Mendez, Rey, & Carrazana, 2004).
A recently introduced term designed to capturethe point on the spectrum of cognitive functionbetween healthy aging and dementia is mild cogni-tive impairment (MCI). This term was first used byFlicker, Ferris, and Reisberg (1991) to describeindividuals with a Global Deterioration Scale(GDS, Reisberg, Ferris, de Leon, & Crook, 1982)rating of 3. However, it was Petersen et al. (1999)who first set out formal criteria for a diagnosis ofMCI. The criteria are as follows: (a) subjectivecomplaint of memory loss, (b) objective impair-ment of ability, (c) preserved general cognitivefunction, (d) intact activities of daily living, (e)individual does not meet criteria for dementia.Individuals who meet these criteria (henceforthreferred to as the “Petersen criteria”) are at anincreased risk for developing AD relative to thegeneral population. In an extensive literaturereview utilizing these criteria, Petersen et al.(2001b) found an average annual conversion rateof 14%, compared to 1–2% in the general popula-tion. Other groups have found higher conversionrates: Geslani, Tierney, Herrmann, and Szalai(2005) report a conversion rate of 41% after oneyear and 64% after two years.
It should be noted that, although there is someoverlap in the characteristics, constructs such asAAMI are not necessarily directly analogous withMCI. For example, Bartres-Faz et al. (2001) con-ducted a study examining performance on a rangeof cognitive functions, including language, by indi-viduals meeting the diagnostic criteria for AAMI(n=93 of 104 individuals presenting with memorycomplaints) and MCI (n=63 of 104). They foundthat MCI individuals performed significantly
worse than AAMI individuals on a number oftasks, including memory, phonetic fluency, andnaming, and conclude that AAMI criteria, whileselecting a population that is genetically distinctfrom healthy elderly adults, nonetheless do notdelineate a population that is as impaired as thosemeeting the criteria for MCI. They suggest thatAAMI may represent a point on the continuum ofdecline that is earlier than that represented byMCI. In a similar vein, Ritchie, Artero, andTouchon (2001) compared the constructs ofAACD and MCI in a population-based study.MCI was estimated to have a prevalence of 3.2%and AACD 19.3%. It was found that MCI was apoor predictor of dementia over a 3-year period,manifesting temporal instability. AACD showedbetter stability and high predictive validity, despitethe fact that it has been conceptualized as a benignimpairment. Given these findings, comparisonsbetween results obtained with MCI individuals andthose diagnosed with similar syndromes should beundertaken with caution.
While it is generally accepted that MCI representsa risk factor for AD, there still exists controversy asto whether MCI individuals will always convert toAD—that is, whether MCI always representsprodromal AD. For example, Chertkow, Verret,Bergman, Wolfson, & McKelvey (2001, cited inChertkow, 2002) found that 25% of their MCI sub-jects had not converted to AD even 10 years after theonset of memory problems. Patients at the MayoAlzheimer’s Disease Research Center converted atapproximately 12% per year, and after 6 years, 80%had converted (Petersen & Morris, 2003). Morris etal. (2001), on the other hand, found conversion ratesof 100% in the long term (9.5 years) in their group ofcognitively impaired individuals, and claim thatMCI always represents prodromal AD.
One possible explanation for these diverse find-ings may be the significant variability in criteriaused to establish a diagnosis of MCI (Chertkow,2002). Morris et al. (2001), who claim that MCIindividuals will always convert to AD, use as adiagnostic criterion a rating of 0.5 on the ClinicalDementia Rating Scale (CDR, Hughes, Berg,Danziger, Coben, & Martin, 1982), which corre-sponds to “questionable AD.” A second scale thathas been used is the Global Deterioration Scale(GDS; Reisberg et al., 1982); a score of 3 has beensuggested to represent MCI, where 1 is normal, 2 isnormal with subjective complaint, and 3 through 7denote increasing impairment (Kluger, Ferris,Golomb, Mittleman, & Reisberg, 1999). Otherresearchers assess MCI in terms of variance fromage- and education-matched norms; for example, acutoff score of 1.5 standard deviations below the
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009
LANGUAGE PERFORMANCE IN MCI AND AD 503
mean in memory tests may be applied. Others relyon the judgment of the clinician (for a discussion ofthe implementation of diagnostic criteria, seePetersen, 2004).
Recently, the Stockholm consensus group(Winblad et al., 2004) proposed the followingrevised criteria for MCI:
1. The person is neither normal nor demented.2. There is evidence of cognitive deterioration
shown by either objectively measured declineover time and/or subjective report of decline byself and/or informant in conjunction withobjective cognitive deficits.
3. Activities of daily living are preserved, andcomplex instrumental functions are eitherintact or minimally impaired.
Artero, Petersen, Touchon, and Ritchie (2006)evaluated these revised criteria and concluded thatthey predicted transition to dementia significantlybetter than did the original Peterson criteria, par-ticularly when amnestic and nonamnestic MCIsubgroups were combined (area under the curve,AUC=0.80; sensitivity: 95%; specificity: 66%).Thus, the inclusion of impairment in domains inaddition to memory provides a better means toidentify those individuals who will convert todementia. However, the criteria cannot differenti-ate between the various dementias, such as AD,vascular dementia, and frontotemporal dementia.
A second consideration with respect to the diag-nosis of MCI is that considerable heterogeneity isobserved in this group. Petersen et al. (2001a) havepointed out that MCI may be divided into threesubgroups, depending on the cognitive functionsaffected. In amnestic MCI, only memory isaffected. In multiple-domain MCI, impairment isseen in multiple cognitive domains, but at a levelinsufficient to constitute dementia. Finally, a thirdsubtype, termed single nonmemory domain MCI,presents as a specific impairment in a nonmemorydomain. It should be noted that the “Petersen cri-teria” discussed above refer to the amnestic variantof MCI.
Heterogeneity is also seen in the etiology of thedisorder (Petersen, 2003). It has been suggestedthat amnestic MCI is likely to evolve to AD,multiple-domain MCI to AD or vascular dementia,and single nonmemory domain MCI to anothertype of dementia, such as frontotemporal demen-tia, Lewy body dementia, primary progressiveaphasia, or vascular dementia (Petersen, 2003).However, recent research (Fischer et al., 2007) sug-gests that MCI subtype is not a good predictor ofevolution to one type of dementia or another.
The goal of identifying those MCI individualswho are most likely to convert to AD will probablybest be met through implementation of a battery oftests designed to tap into a number of diverse indi-cators of AD, including a combination of geneticand cognitive markers, as well as findings fromvolumetric and functional neuroimaging, all ofwhich have proven useful in early detection of AD(for a review, see Chong & Sahadevan, 2005). It isthus of great importance to specify the perform-ance of MCI individuals across a variety of cogni-tive domains. Of particular interest arelongitudinal studies of cognitive decline, whereindividual performance is correlated with eventualconversion.
It is well documented that AD patients oftenmanifest deficits in language processing very earlyin the disease course. Deficits are seen in verbalfluency (for a review, see Henry, Crawford, &Phillips, 2004), naming (e.g., Bayles & Kaszniak,1987, Bayles, Tomoeda, & Trosset, 1992, Bowles,Obler, & Albert, 1987; Fisher, Rourke, & Bieliauskas,1999)—particularly of biological items (Fung et al.,2001; Whatmough et al., 2003)—semantic knowl-edge (Chertkow & Bub, 1990; Hodges, Salmon, &Butters, 1992a; Martin & Fedio, 1983), anddiscourse-level processing (for a review, seeCaramelli, Mansur, & Nitrini, 1998). Syntactic andphonological abilities, on the other hand, are typi-cally relatively preserved (Bayles, 1982; Bayles &Kaszniak, 1987; Irigaray, 1973; Kempler, Curtiss,& Jackson, 1987; Kertesz, 1994; Light & Burke,1993; Patel & Satz, 1994; Schwartz, Marin, &Saffran, 1979; Whitaker, 1976).
Given that language impairment is frequent inAD and occurs early in the disease course, webelieve that a review of the performance of MCIindividuals in language tasks is timely and will con-tribute to the goal of identifying early markers ofcognitive impairment in AD. While such tests can-not replace memory testing in these populations,they provide valuable additional information whenmaking a clinical judgment of the status of an indi-vidual. There exists evidence (e.g., Alexopoulos,Grimmer, Perneczky, Domes, & Kurz, 2006;Bozoki, Giordani, Heidebrink, Berent, & Foster,2001; Sacuiu, Sjögren, Johansson, Gustafson, &Skoog, 2005) that MCI individuals with impair-ments in multiple domains, including language, aremore likely to develop AD than are those with apure memory impairment. Thus, understandingthe nature of language impairment and possiblyidentifying sensitive measures of linguistic impair-ment constitute a vital tool in early detection of AD.
The current paper gives an overview of the find-ings in language performance in MCI published to
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

504 TALER AND PHILLIPS
date. We review MCI individuals’ performance onstandardized neuropsychological tests, discussfindings in the experimental psycholinguistic litera-ture, and compare these findings to those reportedin the AD literature. We then offer suggestions forthe features that should be present in a test oflanguage performance that aims to identify pro-dromal AD.
Relevant references were identified through aMedline search using the following search terms:mild cognitive impairment; frontotemporal demen-tia, early diagnosis; alzheimer, early diagnosis;minimal alzheimer; very mild alzheimer, neuropsy-chology; questionable dementia; cognitive impair-ment no dementia, neuropsychology; ageassociated memory impairment, neuropsychology;age associated cognitive decline, neuropsychology;benign senescent forgetfulness. This was supple-mented by a hand search of the reference lists ofthe articles identified in the Medline search.
STANDARDIZED LANGUAGE TESTS
There are two aspects to consider when evaluatingthe utility of a standardized neuropsychologicaltest in the assessment of MCI individuals. First,does the test distinguish accurately between nor-mal aging, MCI, and AD? That is, does the testprovide diagnostic utility with respect to MCI? Sec-ond, does the test distinguish between those indi-viduals with MCI who will go on to develop ADand those who will not? In other words, does thetest provide prognostic utility? A number of stand-ardized language tests have been evaluated withrespect to these criteria; the following section out-lines the findings published in the literature todate.
Semantic processing
Most epidemiological studies of MCI include somemeasure of semantic processing, typically verbalfluency or picture-naming measures. Below wedescribe the primary findings with respect to MCIperformance on these tasks.
Verbal fluency
Verbal fluency tests are amongst the most widelyused measures of cognitive functioning in demen-tia. These tasks assess an individual’s ability toretrieve and produce words that conform to agiven criterion within a specified time period. Let-ter (phonemic) fluency involves the generation ofas many words as possible beginning with a given
letter (in English, usually F, A, or S). Category flu-ency involves the generation of as many words aspossible that fall into a given category (e.g., ani-mals). Both category and letter fluency impose sig-nificant demands on executive processes; subjectsmust organize verbal retrieval and recall, initiateresponses, and monitor prior responses, as well asinhibit inappropriate responses (Henry et al.,2004). However, the two tasks differ in terms of thesearch strategies required. Letter fluency relies onsearch strategies based on lexical representations,whereas category fluency requires a search forsemantic extensions of a superordinate term,meaning that semantic associations within the lexi-con must be intact in order for the task to be car-ried out successfully (Rohrer, Salmon, Wixted, &Paulsen, 1999).
Impairments in verbal fluency, and especially incategory fluency, are well documented in AD. Arecent meta-analysis of 153 studies with 15,990 ADparticipants examining semantic and letter fluency(Henry et al., 2004) found that, while AD individu-als’ performance on tests of both semantic and let-ter fluency was impaired relative to healthy elderlycontrols (p < .001 for both measures), the effectwas much larger for semantic fluency (r=.73) thanfor letter fluency (r=.55). There was no significantcorrelation between dementia severity and theseverity of the deficit in verbal fluency. Category,but not letter, fluency was correlated with verbalIQ (p < .021). Furthermore, performance on theBoston Naming Test (BNT), while strongly corre-lated with both fluency tasks, was more stronglycorrelated with category than with letter fluency(r=.50 and r=.68). The authors suggest that thespecific deficit in category fluency is due to the deg-radation of the semantic knowledge required forcategory fluency tests, while letter fluency tapssemantic memory to a lesser extent. A larger per-formance deficit was seen in the BNT than in theletter fluency test, whereas the deficit seen in thecategory fluency test was greater than that seen inthe BNT. Thus, since retrieval demands are equiv-alent for the two fluency tasks, and the BNT alsoimposes demands on semantic knowledge, prob-lems in effortful retrieval likely do not underlie thedeficit in category fluency.
The diagnostic utility of category fluency forAD, even very early in the disease course, is alsowell established (e.g., Caccapolo-Van Vliet et al.,2003; Cerhan et al., 2002; Duff Canning, Leach,Stuss, Ngo, & Black, 2004; Lam, Ho, Lui, & Tam,2006; Salmon et al., 2002); it yields a sensitivity of100% and a specificity of 92.5% (Monsch et al.,1992), and performance on this task has beenshown to decline with advancing AD (Perry,
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

LANGUAGE PERFORMANCE IN MCI AND AD 505
Watson, & Hodges, 2000; Small & Bäckman,1998). Given the diagnostic utility of fluency tasks,as well as the fact that deficits are seen very early inthe disease course, a number of studies have under-taken to examine verbal fluency performance as apotential prognostic marker for AD and/or a diag-nostic marker for MCI. These studies have takenthe form of either longitudinal studies of individu-als who are initially nondemented, or studies ofindividuals who have been diagnosed with cogni-tive impairment. Summary statistics for these stud-ies are provided in Table 1, and the studiesthemselves are summarized in Appendix A.
Several prospective studies have found impair-ments in category fluency in healthy adults up to9 years prior to the onset of dementia (Amievaet al., 2005; Auriacombe et al., 2006; Chen et al.,2001; Fabrigoule et al., 1998; Hodges, Erzinçlioglu,& Patterson, 2006; Jorm, Masaki, Petrovitch,Webster Ross, & White, 2005; Masur, Sliwinski,Lipton, Blau, & Crystal, 1994; Nielsen et al., 1999;Small et al., 1997; Vogel, Gade, Stokholm, &Waldemar, 2005). Chen et al. (2001) found thatverbal fluency scores declined more steeply in pre-AD individuals than in controls (those whoremained nondemented for 10 years), particularlythose with higher education levels. Letter fluencyhas also been found to be a reliable predictor ofdementia onset in one study (Small et al., 1997),although other studies found that this was not thecase (Chen et al., 2001; Goldman et al., 2001).Likewise, a number of studies examining categoryfluency in nondemented individuals with cognitiveimpairment have demonstrated lower performanceon this task in those individuals who went on todevelop dementia than in those who did not(Blackwell et al., 2004; Guarch, Marcos, Salamero,& Blesa, 2004; Hanninen et al., 1995; Ritchie et al.,2001). Finally, MCI individuals who have a
memory impairment in addition to an impairmentin one of four other cognitive domains (includingnaming and letter fluency) have been found in onestudy to have an 8 times higher risk of progressingto AD after a 2-year interval than those who mani-fested a memory deficit alone (Bozoki et al., 2001).Another study found that MCI individuals withimpairments in multiple domains have over twicethe risk of conversion after 3.5 years (Alexopouloset al., 2006).
With respect to diagnostic utility, verbal fluencyhas been shown to discriminate accurately betweenMCI subjects and unimpaired control subjects(Bennett et al., 2002; Bschor, Kuhl, & Reischies,2001; Dwolatzky et al., 2003; Geslani et al., 2005;Grundman et al., 2004; Petersen et al., 1999;Ribeiro, de Mendonça, & Guerreiro, 2006; Tabertet al., 2006). One issue that arises with respect tothe various studies examining category fluency iswhether the use of different semantic categorieselicits comparable results. Cunje, Molloy, Standish,and Lewis (2007) tested verbal fluency performancein MCI individuals using four categories: animals,cities and towns, first names, and fruits andvegetables. No difference between categories wasseen in 60-second scores, indicating that the differ-ent versions of the category fluency task allow forserial testing. The use of different versions caneliminate a learning bias, whereby participantsshow a false improvement in performance due torecollection of categories and practice between ses-sions. The 60-second category fluency scoresshowed good sensitivity and specificity for differ-ences between healthy elderly and MCI individuals(area under the ROC curve=0.87 for animals, 0.78for cities and towns, 0.79 for fruits and vegetables,0.83 for names, p < .01 in all cases). Murphy, Rich,and Troyer (2006) found that MCI-amnestic(MCI-A) and AD individuals produced fewer
TABLE 1 Summary statistics for the studies presented in Appendices A and B
Test
Category fluency Letter fluency Naming
Studies reporting difference between NE and MCI/QD/preclinical dementia/miminal AD
29 8 22
Studies reporting no difference between NE and MCI/QD/preclinical dementia/minimal AD
3 8 13
Studies reporting difference between MCI/QD preclinical dementia/minimal AD and mild AD
17 4 12
Studies reporting no difference between MCI/QD and AD 0 5 5Studies reporting predictive value for AD 21 9 12Studies reporting no predictive value for AD 6 7 12
Note. AD=Alzheimer’s disease. NE=normal elderly. MCI=mild cognitive impairment. QD=questionable dementia.
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

506 TALER AND PHILLIPS
items in semantic fluency than did healthy olderadults, while letter fluency was relatively preservedin the MCI-A group. Control and MCI-A partici-pants generated more items in category than letterfluency, while ADs exhibited the opposite pattern.In terms of clustering and switching, control andMCI-A participants performed similarly on letterfluency, while on semantic fluency, MCI-A par-ticipants’ performance was intermediate betweenthat of ADs and controls. Additionally, datafrom our lab indicate that deficits in switching inverbal fluency are equivalent in AD individualsand in MCIs who go on to develop AD, whileMCIs who do not convert to AD exhibit perform-ance similar to that of healthy elderly adults (Phillips,personal communication). Storandt, Grant, Miller,and Morris (2002) report that letter fluency scoresdecline faster with increasing impairment (definedby the CDR score).
Other studies have found that category fluencytasks are not sensitive to decline in MCI. LambonRalph, Patterson, Graham, Dawson, and Hodges(2003) found that MCI subjects showed onlyamnesia, and that impairments in language,including category fluency, did not manifest untilAD set in. Although the mean number of itemsgenerated was lower in the MCI group than in thecontrol group (36.97 vs. 44.26), this result did notreach significance. Karrasch, Sinervä, Grönholm,Rinne, and Laine (2005) found that verbal fluencymeasures distinguished between AD and controlsubjects, but did not distinguish between controland MCI subjects, nor between MCI and ADindividuals. Again, control subjects scored higheron average than MCI individuals (21.1 ± 3.8 vs.18.9 ± 5.9) who scored higher than ADs (18.9 ±5.9 vs. 14.3 ± 5.2), but this effect did not reachsignificance.
One important point in reconciling these con-flicting results is the question of diagnosis of MCI.If the MCI sample meets the criteria for amnesticMCI, as is the case in both the Lambon Ralph et al.(2003) and the Karrasch et al. (2005) studies, thenimpairment in a cognitive domain other than mem-ory constitutes an exclusionary criterion. Thus,deficits in language tasks such as category fluencywould not be expected. Lambon Ralph and col-leagues (2003) note that their sample was biasedtowards patients with no focal deficits in other cog-nitive domains. These investigators found that def-icits in semantic and linguistic domains emergedafter the memory deficits that are the hallmark ofMCI. This is consistent with the finding that MCIpatients with deficits in cognitive domains otherthan memory are more likely to convert to AD(Alexopoulos et al., 2006; Bozoki et al., 2001;
Sacuiu et al., 2005). Such patients are presumablymore advanced in the disease course, neuropathol-ogy having spread from the entorhinal cortex toencroach on areas of the inferior and lateral tem-poral neocortex.
There exist a few studies examining more fine-grained aspects of verbal fluency tasks in MCI.Cooper, Lacritz, Weiner, Rosenberg, and Cullum(2004) examined the effects of practice in test–retest conditions with a category fluency task. Ithas been previously established (Cooper et al.,2001) that AD individuals’ performance on an ani-mal fluency task does not improve with practice,even at a very short test–retest interval. Cooper et al.(2004) demonstrated that, like AD individuals,MCI individuals do not benefit from practice. Theauthors suggest that the reliability of category flu-ency measures in AD and MCI, in combinationwith the lack of practice effect, means that this taskmay be a useful cognitive marker for pharmacolog-ical studies requiring short intervals between test-ing sessions. Forbes-McKay, Ellis, Shanks, andVenneri (2005) examined the individual items pro-duced in a category fluency task by controls andminimal, mild, and moderate AD patients, andfound that age of acquisition of items reliably dif-ferentiated between healthy adults and ADpatients, although it was not sensitive to the sever-ity of AD. Gómez and White (2006) report thatmeasures other than number of items generateddiscriminate between healthy older adults and verymild AD patients—namely, clustering, switching,and size of cluster.
Östberg, Fernaeus, Hellström, Bogdanovic, andWahlund (2005) examined MCI individuals’ per-formance on a verb fluency task, in which theywere instructed to name as many things as possiblethat people do (as distinct from verbal fluency,described above, or verb generation, in which sub-jects are given nouns as stimuli and in responseproduce verbs). Verb fluency was found to be dis-proportionately impaired in MCI relative to nounand letter fluency; the authors suggest that thismay be because verb referents are not taxonomic inthe same way as noun referents, and verb fluencythus relies more on neocortical-hippocampal inter-action, particularly the perirhinal cortex, which isaffected by very early AD neuropathology.
In sum, deficits in verbal fluency have been dem-onstrated to be predictive of development ofdementia and to be present in MCI in a number ofstudies (see Table 1). Greater impairments are seenin category fluency than in letter fluency in AD,and category fluency is more likely to be impairedin MCI and/or to constitute a predictive factor fordementia. This is presumably due to breakdown in
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

LANGUAGE PERFORMANCE IN MCI AND AD 507
semantic representations, since impairments in letterfluency are much less likely to be present in MCIor early AD, suggesting that these deficits are not aresult of executive or inhibitory dysfunction. Verbfluency appears to be more impaired than nounfluency, although this finding requires replication.
It is important to recall when interpreting theseresults that, while fluency measures may demon-strate impairment in preclinical AD, it does notfollow that such an impairment is predictive onlyof AD. For example, similar deficits in fluencytasks have been reported in preclinical AD andpreclinical vascular dementia (VaD; De Jager,Hogervorst, Combrinck, & Budge, 2003; Laukka,Jones, Small, Fratiglioni, & Bäckman, 2004). Incontrast, Duff Canning et al. (2004) found that let-ter fluency distinguished VaD patients, but not ADpatients, from normal controls, and Jones,Laukka, and Bäckman (2006) found that categorybut not letter fluency distinguished between pre-clinical AD and VaD individuals. Thus, categoryfluency may be more affected in AD and letter flu-ency in VaD, reflecting the semantic deficit seen inthe former group. Verbal fluency is also equiva-lently impaired in frontotemporal dementia andAD (Pasquier, 1999), indicating the executive com-ponent in this task. Depression has been shown toaffect letter but not semantic fluency, meaning thateven mild depression may reduce or eliminate dis-crepancies between letter and category fluency indementia (Ravdin, Katzen, Agrawal, & Relkin,2003).
A second important consideration in interpret-ing findings relating to neuropsychological per-formance in prodromal AD is that considerablevariability in performance is reported even in clini-cal cases of AD. For example, Fisher, Tierney,Rourke, and Szalai (2004) examined the perform-ance of two subgroups of probable AD patients onletter and category fluency tasks. Participants weregrouped into left-hemisphere AD (LAD) andright-hemisphere AD (RAD) subgroups on thebasis of their performance on the Boston NamingTest and Copy tasks. It was found that LAD andRAD participants performed similarly on letterfluency, while LAD participants performed morepoorly on category fluency and produced signifi-cantly more within-subclass clusters than did RADparticipants. Similar results were found by Shermanand Massman (1999). Given the heterogeneityfound amongst individuals diagnosed with proba-ble AD, it is to be expected that not all preclinicalAD individuals will manifest similar performances.Thus, while impaired performance on categoryfluency tasks may constitute a risk factor for con-version to dementia, it must be borne in mind that
a subset of those individuals who go on to developdementia will exhibit no impairment on semantictasks.
Naming
One well-documented symptom of Alzheimer’sdisease is word-finding difficulty (Bayles &Kaszniak, 1987; Bayles et al., 1992; Bowles et al.,1987; Fisher et al., 1999). Deficits in confrontationnaming typically occur early in the disease course(Cummings & Benson, 1989; Huff, 1990). As such,naming tests are widely used in clinical practice aswell as research settings.
One widely used naming test is the Boston Nam-ing Test (BNT; Kaplan, Goodglass, & Weintraub,1983), which comprises 60 items ranging from veryfrequent to very infrequent. This test predicts therate of cognitive decline in AD (Carswell, 1999;Rasmusson, Carson, Brookmeyer, Kawas, &Brandt 1996) and distinguishes between subgroupsof AD (J. K. Johnson, Head, Kim, Starr, &Cotman, 1999). In combination with the BlockDesign subtest of the Wechsler Intelligence Scalefor Children–Revised (Wechsler, 1974), it has beendemonstrated to be sensitive to asymmetric cogni-tive changes in early AD, where one hemisphere isaffected more than the other (Delis et al., 1992;Fujimori et al., 1998; Jacobs et al., 1995; Massmanet al., 1993). To facilitate testing of AD individu-als, whose limited attention span renders the full60-item version difficult to administer, Williamsand colleagues developed two 30-item versions ofthe BNT (Williams, Mack, & Henderson, 1989).These researchers found that the two versions wereequivalent, and that there was a significant correla-tion between each version and the full 60-item ver-sion, both in demented individuals and in healthysubjects. The same research group subsequentlyconstructed four 15-item versions and validatedthem in demented and nondemented elderly indi-viduals (Mack, Freed, Williams, & Henderson,1992).
A number of studies have examined the diagnos-tic and prognostic utility of tests of naming per-formance in MCI and AD, including, but notlimited to, the 15- and 60-item versions of theBNT. Summary statistics are provided in Table 1,and the findings are summarized in Appendix B.Differences have been found between healthy eld-erly controls and MCIs (Dwolatzky et al., 2003;Grundman et al., 2004; Petersen et al., 1999),between MCIs and ADs (Goldman et al., 2001;Petersen et al., 1999), and between incident ADand nondemented individuals up to two years priorto diagnosis (Blackwell et al., 2004; Nielsen et al.,
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

508 TALER AND PHILLIPS
1999). Likewise, Bennett et al. (2002) found thatMCIs had lower baseline scores and declined morethan twice as rapidly as did healthy elderly controlson a composite score of semantic memory, includ-ing the BNT, and Storandt et al. (2002) reportedmore rapid rates of decline on the BNT as cogni-tive impairment progresses. Bozoki et al. (2001)found that the BNT discriminated best betweenindividuals with memory impairment who con-verted to AD and those who did not, although thiseffect missed significance.
The Graded Naming Test (GNT, McKenna &Warrington, 1983) is a 30-item naming test with itemsthat progressively decrease in familiarity. A numberof studies have suggested that it is sensitive to seman-tic deficits in AD and MCI (e.g., Blackwell et al.,2004; Dudas, Clague, Thompson, Graham, &Hodges, 2005; Thompson, Graham, Patterson, Saha-kian, & Hodges, 2002) and that it predicts incidentdementia (De Jager & Budge, 2005). Of particularinterest in the last study was the finding that deficitsin naming of famous faces was highly predictive ofconversion to AD in individuals with questionableAD (defined as complaints of declining episodicmemory in the absence of dementia). In a similarvein, Semenza, Mondini, Borgo, Pasini, and Sgara-mella (2003) demonstrated that tests of proper nameretrieval, both to description and in naming faces,were more sensitive to very mild AD (comparable toMCI) than other, longer batteries such as the Mini-Mental State Examination (MMSE, Folstein,Folstein, & McHugh, 1975) and the Milan OverallDementia Assessment (Brazzelli, Capitani, DellaSala, Spinnler, & Zuffi, 1994). This disproportionatedeficit for person naming in very mild or questionableAD clearly requires further exploration.
However, several studies have reported thatnaming tests do not predict incident dementia(Albert et al., 2001; Chen et al., 2001; Devanand,Folz, Gorlyn, Moeller, & Stern, 1997; Fox et al.,1997; Fox et al., 1998; Newman, Warrington,Kennedy, & Rossor, 1994; Ritchie et al., 2001;Schmidtke & Hermeneit, 2007; Small, Fratiglioni,Viitanen, Winblad, & Bäckman, 2000), that differ-ences are not seen until after diagnosis (Rubinet al., 1998), or that they are detectable at retest butnot at baseline (Guarch et al., 2004). In addition, ina recent study the 15-item BNT did not distinguishbetween MCI, normal controls, and individualsdiagnosed with major depressive disorder (Beinhoff,Hilbert, Bittner, Grön, & Riepe, 2005). These con-flicting results may be due in part to the differenttests used; shorter tests such as the 15-item BNT orthe naming subtest of the MMSE were less likely topredict incident dementia or differentiate betweensubject groups (e.g., of 12 studies reporting no
predictive or diagnostic value for the BNT, 6report using a shortened version). Likewise, smallsample sizes such as those used by Goldman et al.(2001) were less likely to yield significant differ-ences between subject groups. Finally, it is possiblethat only a subset of preclinical AD patientsexhibit a naming deficit. Hodges et al. (2006)report on the neuropsychological profile of 10MCI patients followed over at least six years. Theyfound that, while deficits in memory and categoryfluency occurred in most patients very early (in 7/10 patients at baseline and 8/10 at the end of thefirst year), naming deficits (assessed using the nam-ing task from the Cambridge semantic test battery;Hodges & Patterson, 1995) were more variable andunstable.
Whatmough et al. (2003) capitalized upon thewidely reported category effect in AD, wherebyAD individuals perform better on naming artifactsthan biological kinds (e.g., Daum, Riesch, Sartori,& Birbaumer, 1996; Fung et al., 2001; Silveri,Daniele, Giustolisi, & Gainotti, 1991). Theseauthors tested 56 ADs and 16 MCIs, as well as 40elderly controls, on a picture-naming task compris-ing 28 biological items (fruits, vegetables, or ani-mals) and 28 artifacts (tools, clothing, or furniture).Patients were then stratified into five groups on thebasis of their naming ability (the first three groupscomprising both MCI and AD individuals, and thebottom two groups only ADs). Results revealed thatthe category effect favoring artifacts increased withworsening anomia. These findings highlight (a) theheterogeneity of semantic memory impairment inAD (given that ADs spanned five levels of namingimpairment, and MCIs three); and (b) the relativelysteeper decline in naming biological kinds thanartifacts as semantic memory declines.
In sum, it appears that naming impairments dooccur in preclinical AD, although the diagnostic andprognostic utility of these tests is limited. Testa et al.(2004) assessed the diagnostic utility of the BNT rel-ative to other neuropsychological measures andfound that, while impaired performance on the BNTis associated with increased risk of AD, it impartedno additional diagnostic utility once delayed recallimpairments were included in the model.
Other standardized language tasks
Although confrontation naming and verbal flu-ency are the most frequently used standardizedlanguage tasks, there also exist a few studies inwhich MCI individuals’ performance on a broaderrange of standardized measures is reported. Thesestudies are summarized in Appendix C and are dis-cussed in more detail below.
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

LANGUAGE PERFORMANCE IN MCI AND AD 509
The Pyramids and Palm Trees Test (Howard &Patterson, 1992). The Pyramids and Palm TreesTest (PPT) assesses semantic access via words orpictures. A few studies have reported MCI individ-uals’ performance on the different versions of thistask. Nestor, Fryer, Smielewski, and Hodges(2003) found that AD patients performed worsethan MCIs on the picture version of the PPT, whileMCIs did not differ from control participants. Incontrast, Dudas et al. (2005) report diminishedperformance on the PPT (picture version) in MCIand AD.
The Semantic Object Retrieval Test (Kraut et al.,2002). The Semantic Object Retrieval Test (SORT)assesses semantic association by requiring partici-pants to determine whether two objects are relatedthrough another (e.g., “desert” and “humps” arerelated through “camel”). Kraut et al. (2007) reportdata indicating that MCI individuals may be sub-divided on the basis of SORT performance, andthat performance on the SORT correlated withBNT performance; furthermore, in the semanti-cally impaired group, SORT performance wasassociated with declines in performance on tests offrontal lobe function. The authors suggest that theSORT may provide valuable diagnostic and prog-nostic information, although that remains to bedemonstrated.
The ECO battery. The Examen Cognitif par Ordi-nateur (ECO) battery used by Ritchie et al. (2001)includes a number of tests of language function,including verbal fluency and naming (discussedabove), as well as reaction time (RT) for word andsyntax comprehension. These authors found that RT(presented as a composite score of RT to syntax andto word comprehension) discriminated between nor-mal subjects and those with preclinical dementia 2years prior to diagnosis, independent of educationeffects.
The ACT system. Collie, Maruff, and Currie (2002)also examined RT for syntactic and semanticprocessing, as part of the Automated CognitiveTest system (ACT; Stollery, 1996). In the syntactictask, participants are shown sentences followed byexemplars and are required to verify whether thesentence are syntactically correct or not (e.g.,A follows B, AB = incorrect; A is followed by B,AB = correct). In the semantic task, participantsare provided with a semantic category and areasked to verify whether the word is an exemplarfrom the category or not (e.g., word = elm;category = tree). For the syntactic reasoningtask, accuracy discriminated significantly between
elderly controls and MCIs; however, RT did not,and neither accuracy nor RT discriminatedbetween the two groups for the semantic test.Given that syntactic deficits are not typicallyreported in MCI or early-stage AD, this findinglikely reflects deficits in domains other than syntaxproper.
Montreal Cognitive Assessment. Our group hasdeveloped a short (10-minute) neuropsychologicalbattery, the Montreal Cognitive Assessment(MoCA; Nasreddine et al., 2005), which assesses anumber of cognitive functions, including animalnaming, letter fluency, and sentence repetition.Both fluency and naming discriminated reliablybetween ADs, MCIs, and healthy elderly (itemanalyses available at http://www.mocatest.org/validation_study.html). Overall, the MoCA has90% sensitivity and 100% specificity for MCI.
Mindstreams battery. Dwolatzky et al. (2003) reporta new computerized cognitive assessment system(Mindstreams) designed to detect MCI in clinicalpractice. Verbal function is assessed using a nam-ing test and a rhyming test, whereby participantsare instructed to select the word that rhymes withthe name of the picture presented. Both thesemeasures were found to discriminate significantlybetween MCIs and healthy elderly subjects, as wellas between MCIs and ADs. These two tests of ver-bal function were then compared with traditionalverbal tests, including verbal fluency, BNT, andWechsler Adult Intelligence Scale–Third Edition(WAIS-III) similarities, in terms of their capacityto discriminate between MCIs and healthy elderly.The best traditional verbal test was found to be theControlled Oral Word Association–FS (COWA-FS;letter fluency), although this test did not discrimi-nate as well as the two verbal tests included in theMindstreams battery.
DemTect. DemTect (Kalbe et al., 2004) is a shorttest including five cognitive tasks, with a reportedsensitivity of 80% for MCI and 100% for AD. Thetest includes a word fluency task (supermarket),and in the validation study it was found to be oneof the two most sensitive tasks in terms of discrimi-nation between controls, MCIs, and ADs.
Vocabulary measures. Bennett et al. (2002) useda number of tests of language including categoryfluency, the 15-item BNT, the extended rangevocabulary test, and the National Adult ReadingTest (NART; Nelson, 1982). These scores werethen summarized to yield a measure of semanticmemory, which was lower at baseline and declined
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

510 TALER AND PHILLIPS
more rapidly for MCIs than for healthy controlsubjects. Lambon Ralph et al. (2003), on the otherhand, found no difference between MCIs andhealthy controls on the NART. It should be notedthat the MCI group in the latter study was muchsmaller (n=17) than in the former (n=211), andthat criteria for amnestic MCI were more strictlyadhered to in the Lambon Ralph et al. (2003) study.
Cookie Theft Picture. Bschor et al. (2001) admin-istered the Boston Cookie Theft Picture test fromthe Boston Diagnostic Aphasia Examination(BDAE; Goodglass & Kaplan, 1983). In this task,participants are shown a picture where a number ofevents are occurring in a familiar setting (a kitchen)and are asked to “report all that happens in the pic-ture.” It was found that this task could distinguishhealthy controls and MCIs from ADs, but could notdifferentiate between controls and MCIs, norbetween the AD subgroups (see Appendix C fordetails of measures).
Complex Ideational Material. In the Complex Ide-ational Material subtest of the BDAE (Goodglass &Kaplan, 1983), participants hear statements orshort stories of increasing length and syntacticcomplexity and must then respond to questionsabout the material they have just heard. This testis considered to be a measure of executive function,but also relies on auditory comprehension. Bennettet al. (2002) created a summary measure of seman-tic memory on the basis of their participants’ per-formance on this task as well as vocabulary scores,category fluency, and naming, and found thatMCI individuals had a lower score at baselineand declined more rapidly than healthy controlsubjects.
Other tests of semantic processing. Lambon Ralphet al. (2003) included a number of additional testsof semantic processing in their study, includingword–picture matching, picture sorting by feature,naming to verbal description, and semantic featurequestions. MCI individuals could not be distin-guished from normal control subjects on thesemeasures; impairments began to appear at thepoint at which individuals developed mild demen-tia. Hodges and Patterson (1995) also includednaming to verbal description, answering of seman-tic feature questions, and word–picture matching.They found that patients with minimal AD(MMSE > 23) showed deficits in the majority ofthese tests, suggesting that semantic memory isimpaired very early in the disease course in manypatients, although it was found that episodic mem-ory was a more accurate marker of AD.
Syntactic processing
While syntactic impairments are not typically seenin AD, certain studies have included measures ofsyntactic comprehension in MCI, typically theToken Test (De Renzi & Vignolo, 1962) or the Testfor the Reception of Grammar (TROG; Bishop,1989). Of all semantic and language tests, LambonRalph et al. (2003) found differences between MCIpatients and control subjects only on the TokenTest. This finding was taken to indicate impairedworking memory or attentional-executive process-ing, rather than impaired syntactic processing,since MCI individuals showed no impairment onthe TROG; impairments on this task only appearedonce the individuals were at the DAT (mild demen-tia of the Alzheimer’s type) stage. Hodges et al.(2006) also included the TROG as part of their bat-tery and found no significant effects. De Jageret al. (2003) evaluated the sensitivity and specificityof a broad variety of neuropsychological tests forMCI, as well as AD and vascular cognitive impair-ment. These tests included the Token Test (short-ened version; Lezak, 1995), which distinguishedbetween MCI individuals and those suffering fromcerebrovascular disease or AD. However, no differ-ence was seen in the performance of control andMCI participants. Ribeiro et al. (2006), on the otherhand, found significant impairments on a modified(Portuguese) version of the Token Test: A total of33.7% of their MCI participants exhibited animpairment on this task (compared to only 30.2%on semantic fluency). In addition, as mentionedabove, Collie et al. (2002) report deficits in MCI ona syntactic reasoning task.
In sum, the results of standardized languagetests suggest that MCI individuals often manifestdeficits in semantic processing, although this is notinvariably the case. Episodic memory appears tobe affected before other cognitive domains,although those individuals who manifest impair-ments in one or more cognitive domains in addi-tion to memory are more likely to convert to AD(Alexopoulos et al., 2006; Bozoki et al., 2001;Sacuiu et al., 2005). As such, tools for detection ofsubtle deficits in the lexical-semantic domain are ofparticular interest, as these would allow greaterprognostic sensitivity for AD. We now turn to anoverview of the literature on MCI and languageusing nonstandardized measures.
NONSTANDARDIZED LANGUAGE TESTS
While the majority of research on language func-tion that has been conducted with MCI individuals
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

LANGUAGE PERFORMANCE IN MCI AND AD 511
has focused on standardized tests of language func-tion, there exists nonetheless a small body of litera-ture reporting on various aspects of languageperformance in this group using other, nonstand-ardized, measures. These studies are discussedbelow, subdivided according to modality (receptivevs. expressive). Since MCI is a newly defined syn-drome, such research is relatively scarce. We there-fore include findings relating to minimal AD(typically defined as CDR of 0.5 and/or MMSE > 23),which mimics the deficits seen in MCI.
Receptive language
Alterations in receptive language processing havebeen reported at a number of levels in MCI. Webegin with a discussion of studies at the single-word level, then moving to sentence and finallydiscourse-level processing.
Single-word identification
At the perceptual level, Massoud, Chertkow,Whitehead, Overbury, and Bergman (2002) dem-onstrated that word-reading threshold (WRT) is apotentially useful tool for discriminating MCI indi-viduals who will progress to AD. These authorsconducted a study with 13 AD participants, 13MCI participants, and 12 healthy elderly controls,in which participants read aloud backward- andforward-masked words presented at increasinglylong intervals. WRT was defined as the targetduration at which 50% of words could be read, anda WRT threshold of 85 ms was found to success-fully distinguish 10 of 13 ADs and 11 of 12 healthyelderly controls. This compares favorably with aprevious study of letter identification thresholdthat allowed correct classification of only 59% ofAD patients (Mendola, Cronin-Golumb, Corkin,& Growdon, 1995). Furthermore, while MCI indi-viduals could not be distinguished from the othergroups on the basis of this test, the 4 MCIs whosethresholds were above 85 ms had progressed to ADat two-year follow-up. This study indicates thatimpairments in single-word processing are ofpotential prognostic significance for MCI.
This issue was further investigated byVandenbulcke, Peeters, Dupont, Van Heckeand Vandenberghe (2007). They report an func-tional magnetic resonance imaging (fMRI) study inwhich MCI individuals and healthy elderly controlsperformed a semantic-associative task with eitherwords or pictures. It was found that activation inthe lower bank of the posterior third of the leftsuperior temporal sulcus (STS) indexed word-specificprocessing in elderly controls. MCI individuals, on
the other hand, manifested a significant reductionin this activation. Participants also completed aword identification task similar to that used byMassoud et al. (2002), in which they were requiredto identify forward- and backward-masked pic-tures and words presented at increasing intervals(30–800 ms). Overall, the slope of time–accuracyfunction was steeper for controls than MCIs in theword but not the picture identification task, suggest-ing that controls are quicker to generate associa-tions to the stimulus. Furthermore, there was asignificant correlation between slope and fMRIresponse amplitude in the STS. The authors suggestthat the STS may constitute the neural substrate forthe deficit in word identification reported byMassoud et al. (2002) and postulate that dedifferen-tiation of the connections between orthographicword forms and their meaning may underlie theslowing in identification of written words in MCI.
Lexical-semantic processing
While there exists plentiful evidence of semanticdeficits in MCI, only a few studies examine lexical-semantic processing in MCI using nonstandardizedtests. Puregger, Walla, Deecke, and Dal-Bianco(2003) report a magnetoencephalographic (MEG)study in which MCI subjects and healthy age-matched controls were asked to encode wordseither semantically (animate or inanimate) or non-semantically (presence or absence of letter “s”) andthen identify already-seen items. Behavioral meas-ures showed no difference between the two groups,but differences were seen in the MEG signal whileencoding was taking place: MCIs showed greateractivation in the shallow (nonsemantic) encodingcondition over left frontal and temporal sensors250–450 ms following stimulus onset. No sucheffect was seen in control subjects. This finding wasinterpreted as reflecting additional neural activa-tion required for shallow encoding, to compensatefor neurodegeneration.
Similarly, Olichney et al. (2002) examined elec-trophysiological response in MCI individuals(n=14) and healthy elderly controls (n=14) to sin-gle words during a categorization task. Subjectswere presented category statements (e.g., “a break-fast food”) and then congruous items (e.g.,“pancake”) or length- and frequency-matchedincongruous words. They found that MCI individ-uals manifested a delayed N400, a negative peak inthe EEG waveform approximately 400 ms afterstimulus onset, which is taken to reflect semanticintegration processes. Furthermore, control sub-jects manifested a late positive component to newwords, which was significantly diminished when a
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

512 TALER AND PHILLIPS
word was repeated. This repetition effect was muchweaker for MCI participants and was almostentirely accounted for by the 7 MCI subjects whodid not subsequently convert to AD. That is, theabsence of a repetition effect appears to predictsubsequent conversion from MCI to AD. Taylorand Olichney (2007) report follow-up analyses ofthis cohort of MCI individuals. Converters mani-fested a delayed and spatially circumscribed N400repetition effect at baseline, and this effect wasabsent altogether in the group averages after oneyear. Furthermore, the baseline P600 repetitioneffect accurately discriminated 11 of 13 MCI indi-viduals who converted to AD over the next threeyears, suggesting that these effects may be clini-cally useful in prognosis of MCI.
Davie et al. (2004) report a study examiningMCI individuals’ sensitivity to expectancy viola-tions. These researchers used a semantic primingparadigm, where subjects decided whether visuallypresented word pairs were related or not. Partici-pants included healthy younger (n=80) and older(n=22) control subjects, as well as participants diag-nosed with MCI (n=10). An expectancy bias wascreated by manipulating the proportion of category-related (apple–fruit) and coordinate-related pairs.When a high proportion (80%) of category pairs waspresented, both control and MCI groups showedan expectancy bias, but MCI individuals showed amuch greater cost for unexpected targets.
Taler and Jarema (2006) report a study in whichgroups of healthy elderly controls (n=11), MCI(n=8), and AD (n=8) individuals were asked toperform lexical decisions on nouns of differing cat-egories: mass nouns such as cheese, count nounssuch as table, and nouns that are mass/countambiguous, such as chicken. Healthy older adultsmanifested faster response times to ambiguousnouns than to mass or count nouns, while neitherMCI nor AD participants showed such an advan-tage for ambiguous nouns. This was interpreted asreflecting an impaired semantic network in thesepopulations. These findings are consistent withprevious research by the same authors (Taler &Jarema, 2004), in which MCI and AD individualswere asked to distinguish between mass and countreadings of mass/count ambiguous items such as“chicken.” In this study, participants were pre-sented with pictures representing the mass andcount readings of each noun and were asked toeither “Point to the picture of chicken” or “Pointto the picture of a chicken.” While a minority ofpatients from both MCI and AD groups manifestedcontrol-like performance, most patients wereimpaired on this task. Furthermore, performancedid not differ significantly across the two groups.
One important distinction in semantic process-ing is that between intentional and automaticprocessing: Word-naming and verbal fluency tasksrequire intentional processing, while tasks such aslexical decision and word identification tap moreautomatic processing. In AD, impairments areseen in both types of processing, and the order inwhich these impairments appear is not clear.Recent research indicates that MCI individuals’performance on intentional access tasks (picturenaming and semantic probes) is impaired but per-formance on tasks tapping automatic access (lexi-cal decision and semantic priming) is not (Duong,Whitehead, Hanratty, & Chertkow, 2006). Impair-ments were also seen in performance on Strooptasks, and the authors suggest that impairments inlexical-semantic tasks may be attributable to defi-cits in inhibition during semantic search. Theauthors acknowledge that task difficulty may alsoplay a role, although it appears that this factorcannot fully account for the findings. These find-ings are in contrast to those reported above, whichsuggest deficits in automatic as well as intentionalprocessing. However, it is possible that the tasksused by Duong et al. (2006) did not tap a suffi-ciently subtle aspect of automatic lexical-semanticprocessing. For example, Taler and Jarema (2006)found that MCI and AD individuals did not showan advantage for lexical items with multiple relatedsenses, the so-called “ambiguity advantage”(Rubinstein, Garfield, & Millikan, 1970), whileolder adults did. The priming task used by Duonget al. (2006) relied upon associative strengthbetween prime and target and thus may not havebeen sensitive to subtle alterations in automaticlexical-semantic processing in MCI participants.
While most studies of single-word processing inAD and MCI have focused on nouns, Grossmanand colleagues have conducted a number of studiesexamining verb processing in AD. These investiga-tors have found different patterns in brain activa-tion in AD patients versus healthy controls inprocessing of verbs of motion and cognition(Grossman et al., 2003a). In addition, they showimpairment in identifying semantic relationsamong verbs (Grossman, Mickanin, Onishi, &Hughes, 1996). In combination with the findingthat verb fluency is disproportionately impaired inMCI (Östberg et al., 2005), these findings indicatethat further studies of deficits in verb processingmay be fruitful in terms of characterizing the lan-guage impairment in prodromal AD.
In sum, while studies of lexical-semantic process-ing in MCI are scarce, they appear to hold promisefor better characterization of the neuropsychologicalprofile of MCI individuals. Qualitative alterations
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

LANGUAGE PERFORMANCE IN MCI AND AD 513
are seen in a number of tasks, including single-word recognition, as well as in terms of primingand expectancy biases. Such alterations may beattributable to inhibition deficits, whereby MCIindividuals have difficulty inhibiting informationwhile performing semantic search; that is, thelexical-semantic impairments observed in MCImay be due to an interaction between executivefunction and language (Duong et al., 2006). Such aclaim is consistent with the finding that MCI andpreclinical AD individuals tend to exhibit greaterimpairments in category fluency, which comprisesa substantial executive component, than on nam-ing tasks, which place lesser demands on executivefunction.
Sentence and discourse level
Croot, Hodges, and Patterson (1999) foundeffects of AD on sentence comprehension, evenwhen patients were at the minimal stage of thedisease, although these effects were variableacross individuals. Chapman et al. (2002) assesseddetail-level and gist-level discourse processing inMCI individuals (n=20), patients with mild AD(MMSE ≥ 16; CDR ≤ 1; n=24), and cognitivelynormal elderly control subjects (n=25). Participantswere read a 578-word biographical narrative andwere provided with a written copy of the text sothat they could follow along. They were thengiven 5 minutes to review the written text, whichwas removed before they were asked questionsprobing detail- and gist-level processing. Partici-pants were asked to summarize the text, providethe main idea in one sentence, and construct a les-son that could be learned from the story. Recog-nition and recall of specific details of the text werethen tested. These authors found that AD andMCI individuals showed impairments in gist-levelprocessing (summary, main idea, and lesson) rela-tive to healthy elderly controls. A more detailedexamination of individual participants’ perform-ance revealed that 13 of 20 MCI patients were inthe impaired range in performance on gist-leveltasks. Detail-level processing was also impaired inboth groups and was relatively more impaired inAD than in MCI. The authors conclude thatdetail-level processing is impaired earlier in thedisease course than is gist-level processing.Hudon et al. (2006) likewise examined memoryfor gist-level and detail information in MCI andAD. These researchers found an increase in falserecognition of gist-level information in AD butnot MCI. In recall, however, both MCI and ADparticipants exhibited deficits both for gist-leveland detail information.
Language production
Although limited research has been conducted onlanguage production in MCI, the likelihood thatalterations occur in spontaneous language produc-tion has been highlighted by a recent study indicat-ing reductions in semantic skills and sophisticationof vocabulary in Iris Murdoch’s last novel, pub-lished a year before her diagnosis with AD(Garrard, Maloney, Hodges, & Patterson, 2005).Similarly, subtle language alterations were revealedin an analysis of the speeches given by RonaldReagan in his reelection campaign for the US pres-idency, some 10 years prior to his diagnosis withAD (Venneri, Forbes-McKay, & Shanks, 2005).These cases suggest that spontaneous languagemay be among the skills altered very early in AD.In the present section, we report studies examininglanguage production in both spoken and writtenmodalities.
Production of definitions
Hodges, Patterson, Graham, and Dawson(1996) examined the performance of control partic-ipants and minimal, mild, and moderate ADpatients on naming and generation of definitionsfor a set of nouns and found that the quality of def-inition produced differed between groups. Specifi-cally, all ADs produced definitions with lesscorrect information that sometimes failed to con-vey the core concept. For the minimal and mildAD groups, this was correlated with inability toname the object.
Spontaneous speech
AD individuals produce semantically impover-ished discourse that is lacking in coherence,although the syntax is relatively preserved (Kemperet al., 1993). While studies of spontaneous speechin MCI are virtually nonexistent (although seeBschor et al., 2001, discussed above), someresearch has examined spontaneous languageproduction in minimal AD, which is comparable toMCI.
Forbes, Venneri, and Shanks (2002) assessed thespontaneous speech of patients with minimal(n=11) and mild (n=11) AD, as well as age- andeducation-matched controls. These researchersused a simple and a complex picture descriptiontask and found that, while both tasks distinguishedAD patients from controls, only the complex pic-ture description task was able to differentiatebetween minimal AD patients and healthy controlsubjects. Significant differences were seen in measuresof production of semantic paraphasias, word-finding
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

514 TALER AND PHILLIPS
delays, error monitoring, and information con-veyed. Forbes-McKay and Venneri (2005) recentlyconducted a study aiming to collect normative datafor AD individuals in a picture-description task, aswell as to determine whether normal cognitivedecline can be differentiated from pathologicalalterations on the basis of spontaneous languageproduction. In this study, 240 healthy participantsaged between 18 and 90 years, as well as minimal(n=10), mild (n=10), and moderate (n=10) ADpatients were asked to describe, both orally and inwriting, two simple line drawings (the CookieTheft Picture, Goodglass & Kaplan, 1983; and theTripping Woman Picture, Semenza & Cipolotti,1989) and two complex drawings (the TrafficChaos Picture and the Bus Stop Picture, unpub-lished). It was found that measures of informationcontent, pictorial themes, word-finding delays, andthe response given to these delays discriminatedbest between healthy elderly individuals and ADpatients, and the complex picture description taskwas sensitive even to early stages of AD. The pat-tern of errors seen in these studies points to abreakdown in lexical-semantic functioning in theseindividuals; no such breakdown was seen inhealthy elderly subjects. These findings are thusconsistent with the findings reported for othermeasures of semantic functioning, such as categoryfluency.
Writing
It is well established that writing difficultiesoccur in AD, and in fact these difficulties were firstreported by Alzheimer himself in describing hispatient Augusta D. (Alzheimer, 1907; see Stelz-mann, Schnitzlein, & Murtagh, 1995). At the lin-guistic level, AD individuals produce texts that areshorter than those produced by controls (Croisile,Carmoi, Adeleine, & Trillet, 1995; Croisile et al.,1996; Henderson, Buckwalter, Sobel, Freed, &Diz, 1992; Horner, Heyman, Dawson, & Rogers,1988; Neils, Boller, Gerdeman, & Cole, 1989) andcontain less relevant information (Croisile et al.,1995, 1996; Henderson et al., 1992; Kemper et al.,1993). Sentences are less syntactically complexthan those produced by controls (Croisile et al.,1996; Kemper et al., 1993), although AD patientsand control subjects produce a comparablenumber of grammatical errors (Croisile et al.,1996; Horner et al., 1988; Neils et al., 1989). Thatis, syntactic structures are simplified but coherent(Kemper et al., 1993). A high number of semanticsubstitutions or intrusions and misspellings arealso seen (Croisile et al., 1996; Glosser & Kaplan,1989; Henderson et al., 1992; Horner et al., 1988;
Neils et al., 1989). In sum, it can be concluded thatgreater impairments are seen at the lexical-seman-tic than at the syntactic level (Croisile, 1999).Many AD patients do not show any impairment inspelling (Croisile, 1999; Luzzatti, Laiacona, &Agazzi, 2003). However, the most common patternappears to be a surface dysgraphia, wherebywriting of irregular or ambiguous words via anorthographic output lexicon is more impaired thanwriting of pronounceable words or nonwordsthrough grapheme–phoneme correspondence rules(Croisile, 1999). Silveri, Corda, and di Nardo(2007) found that central orthographic (i.e.,lexical-semantic) errors were more prevalent in theearly stages of AD, and peripheral errors (e.g.,omission of strokes) increased as the disease pro-gressed. They suggest that dysgraphia in AD is theresult of a reduction of general cognitive resourcesin AD, rather than disorders of specific subcompo-nents of spelling.
Despite these findings, systematic studies ofwriting performance as a diagnostic or prognosticmarker for AD are scarce. One large-scale studythat is of particular interest is the Nun Study con-ducted by Snowdon and colleagues. Theseresearchers have demonstrated that text-level writ-ing abilities in early adulthood are a strong predic-tor of subsequent onset of dementia (Snowdon et al.,1996) or mild cognitive impairments (Riley, Snow-don, Desrosiers, & Markesberry, 2005) decadeslater. These studies examined the relationshipbetween autobiographies written by nuns twoyears prior to formally joining a congregation(average age=22 years) and their cognitive func-tion several decades later (average age=80 years).The texts were measured in terms of idea density,defined as the average number of ideas expressedper 10 words, which corresponds to elementarypropositions (verb, adjective, adverb, or preposi-tional phrase), and complex propositions (statingor inferring causal, temporal, or other relation-ships between ideas). Participants were then classi-fied as having low idea density (bottom third) orhigh idea density. It was found that idea densitycorrelated significantly with late-life cognitivefunction, as well as late-life scores on standardizedmeasures of cognitive function, including the BNTand verbal fluency. Given these intriguing findings,it seems likely that writing ability constitutes animportant potential diagnostic and prognostic toolfor AD and MCI. However, it should be noted thatthis may reflect a discourse-level deficit rather thana deficit in writing per se, since narratives were nottested in the oral modality.
There also exist a few studies examining writingabilities in minimal AD. Werner, Rosenblum,
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

LANGUAGE PERFORMANCE IN MCI AND AD 515
Bar-On, Heinik, and Korczyn (2006) report alter-ations in kinematic measures of handwriting, suchas time taken to complete writing tasks and pres-sure on the writing surface, which discriminatebetween healthy elderly adults and MCI and mildAD individuals better than the MMSE. Forbes,Shanks, and Venneri (2004) had minimal(MMSE ≥ 25), mild (MMSE 19–24), and moderate(MMSE 12–18) AD individuals describe in writingtwo simple line drawings (the Cookie Theft Picture,Goodglass & Kaplan, 1983; and the TrippingWoman Picture, Semenza & Cipolotti, 1989) andtwo complex drawings (the Traffic Chaos Pictureand the Bus Stop Picture, unpublished). Outputwas assessed according to syntactic complexity,number of paraphasias, information content, com-plexity (writing in cursive), and the proportion ofwords containing legible letters, stroke errors, orallographic errors (inappropriate mixing of upperand lower case). Consistent with previous litera-ture, mild and moderate AD individuals producedwritten narratives with multiple error types (inco-herent/indefinite phrases, semantic and graphemicparaphasias, and inability to abstract and describeall pictorial themes). Patients with minimal AD,however, were distinguishable from control sub-jects only on semantic measures: They manifestedlower information content and capacity to abstractand describe pictorial themes. This is consistentwith the claim that these individuals suffer from acentral semantic impairment even in very earlystages of the disease, as suggested by MCI patients’performance on semantic tasks discussed throughoutthe present paper.
CONCLUSIONS
Characterizing the language impairment in MCI
The findings reviewed here point toward the pres-ence of linguistic deficits in MCI that parallel thosefound in AD. These include deficits in verbal flu-ency, especially category fluency, and in confronta-tion naming, as well as in a variety of other lessstudied language tasks including RT for languagecomprehension (Ritchie et al., 2001), accuracy insyntactic reasoning (Collie et al., 2002), and nam-ing a rhyming word (Dwolatzky et al., 2003).Alterations in performance on a variety of othersemantic tests have also been reported (e.g., inMCI: lexical decision, Taler & Jarema, 2006;semantic categorization, Olichney et al., 2002;semantic encoding, Puregger et al., 2003; semanticpriming, Davie et al., 2004; in minimal AD: namingto verbal description and semantic feature questions,
Hodges & Patterson, 1995). Alterations in produc-tive and receptive discourse-level processing havealso been reported in MCI and minimal AD(Chapman et al., 2002; Forbes et al., 2004; Forbeset al., 2002; Forbes-McKay & Venneri, 2005; Gar-rard et al., 2005; Hudon et al., 2006; Riley et al.,2005; Snowdon et al., 1996). However, these altera-tions appear earlier under more difficult con-ditions: A simple picture-description task, such asthe Cookie Theft Picture, is less likely to revealalterations in MCI or minimal AD (Bschor et al,2001; Forbes-McKay & Venneri, 2005). Likewise,impairment in purer tests of syntax, such as theToken Test and the TROG, are less consistent:Lambon Ralph et al. (2003) and Ribeiro et al.(2006) report impaired performance on the former,whereas De Jager et al. (2003) do not, and LambonRalph et al.’s (2003) and Hodges et al.’s (2006)MCI participants manifested intact performanceon the latter. In sum, it appears that linguisticimpairments in MCI are most likely located at thesemantic level, as is seen in the early stages of AD.Syntactic processing is typically reported to bemore or less intact (although cf. Ribeiro et al.,2006).
Of particular interest are findings suggestingthat timed tests are especially sensitive to thedeclines seen in MCI. Massoud et al. (2002) reportthat word-reading threshold may be useful in dis-criminating MCIs who will convert to AD; simi-larly, temporally precise methodologies, such aslexical decision (Taler & Jarema, 2006), event-related potentials (ERPs; Olichney et al., 2002),and MEG (Puregger et al., 2003), appear to distin-guish well between MCI and healthy controls andeven predict conversion to AD (Olichney et al.,2002). To a lesser extent, the reported deficits incategory fluency tasks, which impose a time limiton responses, are also sensitive to MCI and predictconversion to AD, although it should be noted thatstudies that adhere strictly to the diagnostic criteriafor amnestic MCI, which exclude individualswith deficits in domains other than memory(e.g., Karrasch et al., 2005; Lambon Ralph et al.,2003) are less likely to produce significant results.Furthermore, these tests have been reported tohave diagnostic utility in large-scale epidemiologicalstudies; their utility on an individual-by-individualbasis is less clear.
One question that remains is the locus of thesemantic deficit in MCI and AD. While muchresearch has centered on degradation of semanticknowledge in these populations, recent researchhas suggested that these deficits may be due at leastin part to deficits in executive functions that affectsemantic search or categorization. For example,
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

516 TALER AND PHILLIPS
Grossman et al. (2003b) examined rule-based andsimilarity-based categorization in AD and FTDand found deficits in rule-based but not similarity-based categorization in both AD and FTD. Theyargue that deficits in executive function underliethese declines in rule-based processing in AD.Duong et al. (2006) similarly conclude that seman-tic impairments in MCI may be due to inhibitorydeficits affecting semantic search.
Distinguishing prodromal AD from other dementias
One crucial issue is the distinction between prodro-mal phases of AD and other types of dementia. It hasbeen suggested (Petersen, 2003) that MCI may evolveto AD, VaD, frontotemporal dementia (FTD), Lewybody dementia (LBD), or primary progressive apha-sia (PPA). Any tool designed to detect prodromalAD must provide sufficient specificity in addition tosensitivity. When considering tools to detect earlylanguage impairments, care must be taken to excludeother dementias.
AD versus vascular dementia
A number of studies indicate similar declines insemantic memory in AD and VaD (Bentham,Jones, & Hodges, 1997; De Jager et al., 2003;Laukka et al., 2004; Vuorinen, Laine, & Rinne,2000). For example, Bentham et al. (1997) reportthat VaD and AD individuals perform similarly oncategory fluency, naming, picture sorting, and gen-eration of definitions, showing impairment relativeto healthy elderly adults, while neither groupshowed impairments relative to controls on word–picture matching. Vuorinen et al. (2000) foundimpairments in both groups on complex auditorycomprehension and picture-naming tasks, but nor-mal performance on oral reading and single-wordrepetition.
However, differences have been reported inlanguage performance in VaD and AD. N. L.Graham et al. (2004) report more impaired seman-tic memory in VaD than AD on a variety of tasks:VaD patients exhibited impairments on categoryfluency, the Camel and Cactus test (Bozeat, LambonRalph, Patterson, Garrard, & Hodges, 2000), con-crete and abstract word synonym test, and theGNT, while AD patients showed impairments onlyon category fluency and the GNT. VaD patientshave also been found to perform better on tasks ofconfrontation naming than AD patients, and showbetter preserved lexical-semantic abilities, whiledeclines in syntactic abilities are seen in VaD butnot AD (Desmond, 2004; Pasquier, 1999).
While more errors are seen in naming tasks inAD than in VaD (Almkvist, 1994), the pattern oferrors (visuoperceptual, semantic, or phonemic)has been reported to be similar in the two groups,although AD patients commit more superordinateerrors than VaD patients (Lukatela, Malloy,Jenkins, & Cohen, 1998). More perseveration isseen in VaD than in AD (Desmond, 2004), andTraykov et al. (2002) report higher rates of perse-verative errors in AD than in early-stage VaD in asemantic fluency task (using the categories of ani-mals, fruits, vegetables).
Recently, it has been reported that languageimpairments may appear in the prodromal phaseof VaD (Laukka et al., 2004; although cf. Joneset al., 2006). Likewise, a recent study (Sacuiu et al.,2005) had a large pool of nondemented elderlyindividuals complete a number of tasks, includinga language task in which they were required toidentify synonyms among five alternatives, as wellas tasks assessing memory and visuospatial andexecutive function. Memory impairment in combi-nation with impairment in any other domain bestpredicted incident dementia, prodromal AD wasmost related to impairments in memory and execu-tive function, and the best predictor of VaD wasimpairment in language function according toinformants, in combination with a global patternof deficits. Frisoni, Galluzzi, Bresciani, Zanetti,and Geroldi (2002) report superior performance oncategory and letter fluency in amnestic MCI rela-tive to MCI with subcortical vascular features,while both populations performed similarly on theToken Test. More recently, letter fluency has beenfound to be among the most accurate scales to dis-tinguish between amnestic MCI and MCI withsubcortical vascular features (Galluzzi, Sheu,Zanetti, & Frisoni, 2005). In contrast, Loewensteinet al. (2006) found similarly impaired performancein amnestic and vascular MCI on both letter andcategory fluency. Luis et al. (2004) likewise reportsimilar performance in amnestic and vascular MCIon letter fluency, BNT, and Wechsler Adult Intelli-gence Scale–Revised (WAIS–R) Similarities andVocabulary. These findings highlight both the needto exclude other syndromes such as VaD whenconsidering the prognostic value of tests of lan-guage function and the difficulty in doing so.
AD versus frontotemporal dementia, semantic dementia, and primary progressive aphasia
The term frontotemporal dementia (FTD) refersto a group of degenerative dementias affecting thefrontal or temporal lobes. A variety of terms are
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

LANGUAGE PERFORMANCE IN MCI AND AD 517
used to refer to different subtypes of FTD, includ-ing Pick’s disease, dementia of the frontal type,frontal lobe dementia of the non-Alzheimer’s type,frontotemporal lobar degeneration, semanticdementia (SD), progressive nonfluent aphasia, andprimary progressive aphasia (PPA; Hutchinson &Mathias, 2007).
Of particular relevance with respect to languagetests are dementias that specifically affect languagefunction, including PPA and SD. There exist a fewstudies comparing language performance in thesepopulations and examining the predictive value ofneuropsychological tests in dementia diagnosis.Performance on language tasks has been found tobe equivalent (Cosentino, Chute, Libon, Moore, &Grossman, 2006; Gregory, Orrell, Sahakian, &Hodges, 1997; Pachana, Boone, Miller, Cummings,& Berman, 1996) or lower (Diehl et al., 2005; Perry& Hodges, 2005) in FTD than in AD. Cosentinoet al. (2006) had AD, behavioral FTD, and SDparticipants complete the PPT, the 15-item BNT,the COWA-FS and the verb similarity task (Price &Grossman, 2005), which is designed to resemblethe PPT but utilizing verbs rather than nouns. Nodifference was seen between the three groups onany of these measures. Diehl et al. (2005)compared performance on the CERAD-NAB(Consortium to Establish a Registry for Alzhe-imer’s Disease—Neuropsychological AssessmentBattery) subtests by AD, FTD, and SD patients.Patients with FTD were more impaired than ADpatients in animal fluency, and patients with SDwere more impaired than both FTD and ADpatients on animal fluency and the BNT. Perri et al.(2005) found equivalent BNT performance butlower phonological fluency performance in FTDthan in AD. In a longitudinal study of semanticmemory in SD, AD, progressive nonfluent apha-sia (PNFA), frontal variant frontotemporaldementia (fvFTD), and posterior cortical atro-phy (PCA), Rogers, Ivanoiu, Patterson, andHodges (2006) report a performance pattern indi-cating amodal semantic impairment in SD and asimilar but less impaired performance in AD. InPNFA, fvFTD, and PCA, semantic impairmentswere found, but appeared to be secondary toother factors.
In addition, language has been found to declinefaster in PPA and in the behavioral variant of FTDthan in AD (Blair, Marczinski, Davis-Faroque, &Kertesz, 2007), as assessed by the Western AphasiaBattery (WAB; Kertesz, 1982). Similarly, Krameret al. (2003) found greater impairments on con-frontation naming in SD than in AD or FTDpatients but comparably diminished performanceon animal fluency. B. T. Gold et al. (2005) report
that individuals diagnosed with SD manifestimpairments in naming but not picture recognitionmemory, while AD individuals show the oppositepattern.
Hodges et al. (1999) utilized a comprehensive setof semantic and language tests, in addition to teststapping other aspects of cognitive function, in anattempt to distinguish early AD from the frontallobe variant of FTD as well as SD (referred to asthe temporal variant of FTD). Participants com-pleted the National Adult Reading Test (NART,Nelson, 1982), letter fluency (FAS), the Pyramidsand Palms test (PPT), and a semantic test batterycomprising six subtests: category fluency for sixmain categories and two lower order categories(breeds of dog and types of boat); naming of linedrawings; naming to verbal description; semanticfeature questions (e.g., “What do we call the largeAfrican animal with a curved horn on its head?”);picture sorting; and word–picture matching. Par-ticipants also completed tests assessing auditory-verbal short-term memory, episodic memory, andvisuospatial abilities. AD patients exhibited a pre-dominant deficit in episodic memory, althoughdeclines were also seen in semantic memory (cate-gory fluency and naming to verbal descriptions)and visuospatial skills. SD participants exhibitedprofound deficits on all semantic tasks, as well asthe NART (reflecting a disrupted ability to readirregular words). Finally, FTD (frontal variant)participants showed deficits in episodic memoryand category fluency, similar to the AD group, butnormal semantic memory.
Vandenberghe et al. (2005) report a study exam-ining semantic priming in PPA, MCI, and probableAD. Participants named pictures that were precededby a word that was the picture name, a semanticallyrelated noun, a semantically unrelated noun, or apseudoword. While healthy controls and MCI andAD participants were faster to name the pictureafter a related than after an unrelated prime, thereverse pattern was obtained in PPA. The authorssuggest that this “semantic interference effect” maydistinguish between PPA and probable AD individ-uals. Similarly, Price and Grossman (2005) exam-ined detection time for words following violations ofthematic role assignment or transitivity in AD andFTD. Control participants took longer to detectitems preceded by either type of violation, FTDpatients were insensitive to both types of violation,and AD patients were slowed by thematic role butnot transitivity violations. The authors interpretthese findings in terms of a broader degradation ofverb representations in FTD than in AD.
Hutchinson and Mathias (2007) recently con-ducted a meta-analysis of neuropsychological
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

518 TALER AND PHILLIPS
deficits in AD and FTD, including a large numberof language tests. The language tests that best dis-criminated between the two, with FTD individualsmanifesting greater impairment than AD individuals,were the GNT, word–picture matching, WAB-spontaneous speech, WAB-comprehension, PPT-words, PPT-pictures, and picture-naming tasks(effect size >0.80 in all cases, small overlap, andhigh degree of accuracy in distinguishing the twogroups, as measured by the 95% confidence interval).
These findings point the way to possible meth-ods for distinguishing the different dementias atan early stage. A profound semantic deficit, incombination with relatively intact visuospatialabilities and episodic memory is a marker of SD;AD patients, in contrast, show impairments inepisodic memory and milder semantic deficits. Itshould be noted, however, that not all studieshave found differing performance in verbal epi-sodic memory in AD and SD (e.g., Scahill,Hodges, & Graham, 2005). In addition, perform-ance decrements in the NART have beenreported in SD but not in AD (Hodges et al.,1999).
Of particular interest are recent studies examin-ing semantic deficits at a more precise level thanstandardized semantic tasks such as category flu-ency. For example, Vandenberghe et al. (2005)posit the “semantic interference effect” as a poten-tial distinguishing marker between PPA and AD,and Price and Grossman (2005) found differencesin sensitivity to verb agreement violations in FTDand AD. Such fine-grained distinctions betweendiffering dementias are likely to prove fruitful inearly diagnosis.
Recently, de Mendonça, Ribeiro, Guerreiro, andGarcia (2004) proposed a set of criteria to identifyfrontotemporal MCI. These include symptoms offrontotemporal dysfunction, behavioral and affec-tive symptoms, speech disturbance, and alterationin at least one test that reflects executive function.In addition, patients should have intact activitiesof daily living and a computed tomography (CT)or MRI scan that is either normal or shows fronto-temporal atrophy. A total of 7 patients meetingthese criteria were tested on a variety of neuropsy-chological tests, and the majority did not showimpairment in naming (5/7) or language compre-hension (4/7). These findings suggest that lan-guage tests likely differentiate between prodromalAD and FTD, although it should be noted thatthe criteria used by de Mendonça et al. (2004) tar-get the behavioral (frontal) variant of FTD andprobably exclude cases of prodromal SD andPPA, in which language/semantics are the pri-mary systems affected.
Lewy Body Dementia (LBD)
Lambon Ralph et al. (2001) report impairmentsin semantic memory in AD and LBD. However,differences were seen between the two groups: ADpatients showed equivalent deficits across pictureand word stimuli, while patients with LBD showedmore severe deficits with picture stimuli. In addi-tion, AD patients showed greater deficits in cate-gory than letter fluency, while LBD patientsexhibited equivalent deficits across the two tasks.In the WAIS vocabulary subtest, similar performancehas been reported in the two groups (Shimomuraet al., 1998). Differentiation between these twosyndromes is mainly based on the visuoperceptualdifficulties seen in LBD relative to AD, in combi-nation with the more impaired memory perform-ance in AD, rather than on the basis of languagetests.
Heterogeneity in MCI and AD
Another issue that must be taken into account isthe considerable variability that exists within ADand MCI populations. MCI is heterogeneous interms of both clinical presentation and etiology.With respect to AD, while language impairmentsare often seen early in the disease course, this is notinevitably the case: Visuospatial and frontal vari-ants of AD have also been described (Caine &Hodges, 2001; Cummings, 2000). No language orsemantic test will have 100% sensitivity and specifi-city for AD; it is only in combination with a varietyof genetic, cognitive, and neuroimaging markersthat these methods can be useful.
Diagnostic criteria for MCI
The Petersen criteria for MCI (Petersen et al.,1999) require that the patient manifest subjectivememory complaints, preferably corroborated byan informant; impaired memory function (usually≥1.5 SD below norms, adjusted for age and educa-tion); generally preserved other cognitive function;and intact activities of daily living. Specific psycho-metric tests are not provided; the diagnosis of MCIthus requires clinical judgment. Furthermore, ithas been reported that a diagnosis of MCI is tem-porally unstable (Ritchie et al., 2001), and the pat-tern of cognitive dysfunction may be intrinsicallyfluctuating in early stages (Feldman & Jacova,2005). One avenue to greater diagnostic accuracymay be serial administration of psychometric tests(Feldman & Jacova, 2005). In this case, creation ofalternate forms of neuropsychological tests is an
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

LANGUAGE PERFORMANCE IN MCI AND AD 519
important area for development. Given the varyingcriteria used to diagnose MCI, it is hardly surpris-ing that conflicting results have been reported inthe literature with respect to language performancein this population. Future research should focus onidentifying diagnostic criteria for cognitive and eti-ological subtypes of MCI, allowing greater prog-nostic and diagnostic accuracy.
Future directions
The challenge that remains is to develop a diagnos-tic tool that can detect the subtle declines in seman-tic abilities often seen in the very early stages of ADand that is sensitive enough to be useful on an indi-vidual-by-individual basis. While lexical-semanticprocessing is not affected in every case of AD, it iswell established that this domain is typicallyaffected early in the disease course, and it thus con-stitutes a primary target for detection and progno-sis of MCI. On the basis of the research findingsreviewed here, we suggest that the ideal tool for thispurpose will focus on intentional lexical-semanticprocessing, utilizing a temporally precise methodol-ogy. Such a tool may prove useful in the accuratedetection of individuals who are likely to developAD in the future, thus providing the opportunity tocommence pharmacological treatment, psychologi-cal intervention, and family and financial planningas early in the disease course as possible.
One methodology that provides such temporalprecision is the event-related potential (ERP)methodology. For example, as discussed above,Olichney et al. (2002) and Taylor and Olichney(2007) report results indicating that ERP perform-ance may be useful in discriminating those MCIindividuals who will go on to develop AD. Like-wise, ongoing work in our lab indicates alterationsin ERP response to language stimuli in MCIrelative to healthy elderly adults. Our results sug-gest reductions in lexical activation in MCI (Taler& Phillips, 2006), as well as impairments in activa-tion of multiple semantic representations (Taler,Klepousniotou, & Phillips, 2007).
Another area that requires further investigation isthe domain of discourse-level processing in MCI.There is a good deal of research indicating deficits insentence-level language function in mild or minimalAD, both in production (Forbes et al., 2002; Forbes-McKay & Venneri, 2005; Kemper et al., 1993) and incomprehension (Chapman et al., 2002; Welland,Lubinski, & Higginbotham, 2002). Deficits in com-prehension of prosody are also seen in AD and arecorrelated with severity of dementia (Taler, Baum,Saumier, & Chertkow, in press; Testa, Beatty,
Gleason, Orbelo, & Ross, 2001). Such functionshave yet to be thoroughly assessed in MCI, but defi-cits in sentence- or discourse-level processing seemlikely, and preliminary research points to this con-clusion (Chapman et al., 2002). As well as potentialapplications in terms of detection of prodromal AD,better characterization of these deficits in MCI willallow a more complete picture of the neuropsycho-logical profile of these individuals. Discourse andprosody processing are fundamental aspects ofhuman communication. As such, understandinghow these functions are affected in MCI and ADpaves the road for interventions with these individu-als to improve communication with family and car-egivers, which in turn holds promise for an improvedquality of life both for patients and for their families.
Original manuscript received 5 April 2007Revised manuscript accepted 27 June 2007
First published online 26 November 2007
REFERENCES
Adlam, A. L. R., Bozeat, S., Arnold, R., Watson, P., &Hodges, J. R. (2006). Semantic knowledge in mildcognitive impairment and mild Alzheimer’s disease.Cortex, 42, 675–684.
Aggarwal, N. T., Wilson, R. S., Beck, T. L., Bienias, J. L.,& Bennett, D. A. (2005). Mild cognitive impairmentin different functional domains and incident Alzhe-imer’s disease. Journal of Neurology, Neurosurgery,and Psychiatry, 76, 1479–1484.
Albert, M., Blacker, D., Moss, M. B., Tanzi, R.,McArdle, J. J. (2007). Longitudinal change in cogni-tive performance among individuals with mild cogni-tive impairment. Neuropsychology, 21, 158–169.
Albert, M. S., Moss, M. B., Tanzi, R., & Jones, K.(2001). Preclinical prediction of AD using neuropsy-chological tests. Journal of the International Neu-ropsychological Society, 7, 631–639.
Alexopoulos, P., Grimmer, T., Perneczky, R., Domes, G.,& Kurz, A. (2006). Progression to dementia in clinicalsubtypes of mild cognitive impairment. Dementia andGeriatric Cognitive Disorders, 22, 27–34.
Almkvist, O. (1994). Neuropsychological deficits in vas-cular dementia in relation to Alzheimer’s disease:Reviewing evidence for functional similarity or diver-gence. Dementia, 5, 203–209.
Alzheimer, A. (1907). Uber eine eigenartige Erkrankungder Hirnrinde [On an unusual illness of the cerebralcortex]. Allgemeine Zeitschrift fur Psychiatrie undPsychisch-Gerichtliche Medizin, 64, 146–148.
American Psychiatric Association. (1980). Diagnosticand statistical manual of mental disorders (3rd ed.).Washington, DC: American Psychiatric Association.
American Psychiatric Association. (1987). Diagnosticand statistical manual of mental disorders (Rev.3rd ed.) Washington, DC: American PsychiatricAssociation.
American Psychiatric Association. (1994). Diagnosticand statistical manual of mental disorders (4th ed.).Washington, DC: American Psychiatric Association.
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

520 TALER AND PHILLIPS
Amieva, H., Jacqmin-Gadda, H., Orgogozo, J. M.,Le Carret, N., Helmer, C., Letenneur, L., et al.(2005). The 9 year cognitive decline before dementiaof the Alzheimer type: A prospective population-based study. Brain, 128, 1093–1101.
Artero, S., Petersen, R. C., Touchon, J., & Ritchie, K.(2006). Revised criteria for mild cognitive impair-ment: Validation within a longitudinal populationstudy. Dementia and Geriatric Cognitive Disorders,22, 465–470.
Artero, S., Tierney, M. C., Touchon, J., & Ritchie, K.(2003). Prediction of transition from cognitive impair-ment to senile dementia: A prospective longitudinalstudy. Acta Psychiatrica Scandinavica, 107, 390–393.
Auriacombe, S., Lechevalier, N., Amieva, H., Harston, S.,Raoux, N., & Dartigues, J.-F. (2006). A longitudinalstudy of qualitative features of category verbal flu-ency in incident Alzheimer’s disease subjects: Resultsfrom the PAQUID study. Dementia and GeriatricCognitive Disorders, 21, 260–266.
Bäckman, L., Laukka, E. J., Wahlin, A., Small, B. J., &Fratiglioni, L. (2002). Influences of preclinicaldementia and impending death on the magnitude ofage-related cognitive deficits. Psychology and Aging,17, 435–442.
Bäckman, L., Small, B. J., & Fratiglioni, L. (2001).Stability of the preclinical episodic memory deficit inAlzheimer’s disease. Brain, 124, 96–102.
Bartres-Faz, D., Junque, C., Lopez-Alomar, A.,Valveny, N., Moral, P., Casamayor, R., et al. (2001).Neuropsychological and genetic differences betweenage-associated memory impairment and mild cogni-tive impairment entities. Journal of the AmericanGeriatric Society, 49, 985–990.
Bayles, K. (1982). Language function in senile dementia.Brain and Language, 16, 265–280.
Bayles, K. A., & Kaszniak, A. W. (1987). Communica-tion and cognition in normal aging and dementia.Boston, MA: College Hill/Little, Brown and Co.
Bayles, K. A., Tomoeda, C. K., & Trosset, M. W.(1992). Relation of linguistic communication abilitiesof Alzheimer’s patients to stage of disease. Brain andLanguage, 42, 454–472.
Beinhoff, U., Hilbert, V., Bittner, D., Grön, G., &Riepe, M. W. (2005). Screening for cognitive impair-ment: A triage for outpatient care. Dementia andGeriatric Cognitive Disorders, 20, 278–285.
Bennett, D. A., Wilson, R. S., Schneider, J. A., Evans,D. A., Beckett, L. A., Aggarwal, N. T., et al. (2002).Natural history of mild cognitive impairment in olderpersons. Neurology, 59, 198–205.
Bentham, P. W., Jones, S., & Hodges, J. R. (1997). Acomparison of semantic memory in vascular demen-tia and dementia of Alzheimer’s type. InternationalJournal of Geriatric Psychiatry, 12, 575–580.
Beversdorf, D. Q., Ferguson, J. L. W., Hillier, A.,Sharma, U. K., Nagaraja, H. N., Bornstein, R. A., &Scharre, D. W. (2007). Problem solving ability inpatients with mild cognitive impairment. Cognitiveand Behavioral Neurology, 20, 44–47.
Bishop, D. V. M. (1989). Test for the Reception of Gram-mar. London: Medical Research Council.
Blackwell, A. D., Sahakian, B. J., Vesey, R., Semple, J. M.,Robbins, T. W., & Hodges, J. R. (2004). Detectingdementia: Novel neuropsychological markers ofpreclinical Alzheimer’s disease. Dementia andGeriatric Cognitive Disorders, 17, 42–48.
Blair, M., Marczinski, C. A., Davis-Faroque, N., &Kertesz, A. (2007). A longitudinal study of languagedecline in Alzheimer’s disease and frontotemporaldementia. Journal of the International Neuropsycho-logical Society, 13, 237–245.
Blessed, G., Tomlinson, B. E., & Roth, M. (1968). Theassociation between quantitative measures of demen-tia and of senile change in the cerebral grey matter ofelderly subjects. British Journal of Psychiatry, 114,797–811.
Bowles, N. L., Obler, L. K., & Albert, M. L. (1987).Naming errors in healthy aging and dementia of theAlzheimer type. Cortex, 23, 519–524.
Bozeat, S., Lambon Ralph, M. A., Patterson, K.,Garrard, P., & Hodges, J. R. (2000). Non-verbalsemantic impairment in semantic dementia. Neu-ropsychologia, 38, 1207–1215.
Bozoki, A., Giordani, B., Heidebrink, J. L., Berent, S., &Foster, N. L. (2001). Mild cognitive impairmentspredict dementia in nondemented elderly patientswith memory loss. Archives of Neurology, 58, 411–416.
Brazzelli, M., Capitani, E., Della Sala, S., Spinnler, H.,& Zuffi, M. (1994). A neuropsychological instrumentadding to the description of patients with suspectedcortical dementia: The Milan overall dementia assess-ment. Journal of Neurology, Neurosurgery and Psychi-atry, 57, 1510–1517.
Bschor, T., Kuhl, K. P., & Reischies, F. M. (2001).Spontaneous speech of patients with dementia of theAlzheimer type and mild cognitive impairment.International Psychogeriatrics, 13, 289–298.
Busse, A., Bischkopf, J., Riedel-Heller, S. G., &Angermeyer, M. C. (2003). Mild cognitive impair-ment: Prevalence and predictive validity according tocurrent approaches. Acta Neurologica Scandinavica,108, 71–81.
Caccapolo-Van Vliet, E., Manly, J., Tang, M., Marder,K., Bell, K., & Stern, Y. (2003). The neuropsycholog-ical profiles of mild Alzheimer’s disease and question-able dementia as compared to age-related cognitivedecline. Journal of the International Neuropsychologi-cal Society, 9, 720–732.
Caine, D., & Hodges, J. R. (2001). Heterogeneity ofsemantic and visuospatial deficits in early Alzheimer’sdisease. Neuropsychology, 15, 155–164.
Caramelli, P., Mansur, L. L., & Nitrini, R. (1998). Lan-guage and communication disorders in dementia ofthe Alzheimer type. In B. Stemmer & H. A. Whitaker(Eds.), Handbook of neurolinguistics (pp. 463–473).San Diego, CA: Academic Press.
Carswell, L. M. (1999). Prediction of memory and lan-guage performance in normal elderly Canadians:Implications for the assessment of premorbid cogni-tion in early Alzheimer’s disease (Doctoral disserta-tion, University of Victoria, Canada, 1999).Dissertation Abstracts International: B. The Sciencesand Engineering, 60, 6B. (AATMQ37335)
Cerhan, J. H., Ivnik, R. J., Smith, G. E., Tangalos, E. C.,Petersen, R. C., & Boeve, B. F. (2002). Diagnosticutility of letter fluency, category fluency, and fluencydifference scores in Alzheimer’s disease. ClinicalNeuropsychologist, 16, 35–42.
Chapman, S. B., Zientz, J., Weiner, M., Rosenberg., R.,Frawley, W., & Burns, M. H. (2002). Discoursechanges in early Alzheimer’s disease, mild cognitiveimpairment and normal aging. Alzheimer Disease andAssociated Disorders, 16, 177–186.
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009
LANGUAGE PERFORMANCE IN MCI AND AD 521
Chen, P., Ratcliff, G., Belle, S. H., Cauley, J. H.,DeKosky, S. T., & Ganguli, M. (2000). Cognitivetests that best discriminate between presymptomaticAD and those who remain undemented. Neurology,55, 1847–1853.
Chen, P., Ratcliff, R., Belle, S. H., Cauley, J. A.,DeKosky, S. T., & Ganguli, M. (2001). Patterns ofcognitive decline in pre-symptomatic Alzheimer’s dis-ease: A prospective community study. Archives ofGeneral Psychiatry, 58, 853–858.
Chertkow, H. (2002). Mild cognitive impairment.Current Opinion in Neurobiology, 15, 401–407.
Chertkow, H., & Bub, D. (1990). Semantic memory lossin dementia of Alzheimer’s type. What do variousmeasures measure? Brain, 113, 397–417.
Chertkow, H., Verret, L., Bergman, H., Wolfson, C., &McKelvey, R. (2001). Predicting progression todementia in elderly subjects with mild cognitive impair-ment: A multidisciplinary approach. Paper presentedat 53rd Annual Meeting of the American Academy ofNeurology, Contemporary Clinical Issues PlenarySession. Philadelphia, PA, USA.
Chong, M. S., & Sahadevan, S. (2005). PreclinicalAlzheimer’s disease: Diagnosis and prediction ofprogression. Lancet Neurology, 4, 576–579.
Collie, A., Maruff, P., & Currie, J. (2002). Behavioralcharacterization of mild cognitive impairment. Jour-nal of Clinical and Experimental Neuropsychology, 24,721–733.
Convit, A., Asis, J. D., Leon, J. J. D., Tarshish, C. Y.,De-Santi, S., & Rusinek, H. (2000). Atrophy of themedial occipitotemporal, inferior, and middle tempo-ral gyri in non-demented elderly predict decline toAlzheimer’s disease. Neurobiology of Aging, 21, 19–26.
Cooper, D. B., Epker, M., Lacritz, L., Weine, M.,Rosenberg, R. N., Honig, L., et al. (2001). Effects ofpractice on category fluency in Alzheimer’s disease.The Clinical Neuropsychologist, 15, 125–128.
Cooper, D. B., Lacritz, L. H., Weiner, M. F., Rosenberg,R. N., & Cullum, C. M. (2004). Category fluency inmild cognitive impairment: Reduced effect of practicein test–retest conditions. Alzheimer’s Disease andAssociated Disorders, 18, 120–122.
Cosentino, S., Chute, D., Libon, D., Moore, P., &Grossman, M. (2006). How does the brain supportscript comprehension? A study of executive processesand semantic knowledge in dementia. Neuropsychology,20, 307–318.
Croisile, B. (1999). Agraphia in Alzheimer’s disease.Dementia and Geriatric Cognitive Disorders, 10,226–230.
Croisile, B., Carmoi, T., Adeleine, P., & Trillet, M.(1995). Spelling in Alzheimer’s disease. BehavioralNeurology, 8, 135–143.
Croisile, B., Ska, B., Brabant, M. J., Duchene, A.,Lepage, Y., Aimard, G., et al. (1996). Comparativestudy of oral and written picture description inpatients with Alzheimer’s disease. Brain and Language,53, 1–19.
Crook, T., Bartus, R. T., Ferris, S. H., Whitehouse, P.,Cohen, G. D., & Gershon, S. (1986). Age-associatedmemory impairment: Proposed diagnostic criteriaand measures of clinical change. Report of a NationalInstitute of Mental Health Work Group. Develop-mental Neuropsychology, 2, 261–276.
Croot, K., Hodges, J. R., & Patterson, K. (1999). Evi-dence for impaired sentence comprehension in early
Alzheimer’s disease. Journal of the International Neu-ropsychological Society, 5, 393–404.
Crosson, B. (1996). Assessment of subtle language defi-cits in neuropsychological batteries. In R. L.Sburdone (Ed.), Ecological validity of neuropsycho-logical testing. Delray, FL: GR Press/Ste Lucie Press.
Cummings, J. L. (2000). Cognitive and behavioral heter-ogeneity in Alzheimer’s disease: Seeking the neuro-biological basis. Neurobiology of Aging, 21, 845–861.
Cummings, J. L., & Benson, D. F. (1989). Speech andlanguage alterations in dementia syndromes. InA. Ardila & F. Ostrosky-Solis (Eds.), Brain organizationof language and cognitive processes. New York: PlenumPress.
Cunje, A., Molloy, W., Standish, T. I., & Lewis, D. L.(2007). Alternate forms of logical memory and verbalfluency tasks for repeated testing in early cognitivechanges. International Psychogeriatrics, 19, 65–75.
Daly, E., Zaitchik, D., Copeland, M., Schmahmann, J.,Gunther, J., & Albert, M. (2000). Predicting conversionto Alzheimer’s disease using standardized clinicalinformation. Archives of Neurology, 57, 675–680.
Dartigues, J.-F., Commenges, D., Letenneur, L.,Barbergeur-Gateau, P., Gilleron, V., Fabrigoule, C.,et al. (1997). Cognitive predictors of dementia in elderlycommunity residents. Neuroepidemiology, 16, 29–39.
Daum, I., Riesch, G., Sartori, G., & Birbaumer, N.(1996). Semantic memory impairment in Alzheimer’sdisease. Journal of Clinical and Experimental Neu-ropsychology, 18, 648–665.
Davie, J. E., Azuma, T., Goldinger, S. D., Connor, D. J.,Sabbagh, M. N., & Silverberg, N. B. (2004). Sensitiv-ity to expectancy violations in healthy aging and mildcognitive impairment. Neuropsychology, 18, 269–275.
De Jager, C. A., & Budge, M. M. (2005). Stability andpredictability of the classification of mild cognitiveimpairment as assessed by episodic memory test per-formance over time. Neurocase, 11, 72–79.
De Jager, C. A., Hogervorst, E., Combrinck, M., &Budge, M. M. (2003). Sensitivity and specificity ofneuropsychological tests for mild cognitive impair-ment, vascular cognitive impairment and Alzheimer’sdisease. Psychological Medicine, 33, 1039–1050.
Delis, D., Massman, P. J., Butters, N., Salmon, D. P.,Shear, P. K., Demadura, T., et al. (1992). Spatialcognition in Alzheimer’s disease: Subtypes of global–local impairment. Journal of Clinical and ExperimentalNeuropsychology, 14, 463–477.
Deloche, G., & Hannequin, D. (1997). Test de dénomina-tion orale d’images (DO 80) [Picture naming test].Paris: Centre de Psychologie Appliqueé.
De Mendonça, A., Ribeiro, F., Guerreiro, M., & Garcia,C. (2004). Frontotemporal mild cognitive impair-ment. Journal of Alzheimer’s Disease, 6, 1–9.
De Renzi, E., & Vignolo, L. A. (1962). The Token Test:A sensitive test to detect receptive disturbances inaphasics. Brain, 85, 665–678.
Desmond, D. W. (2004). The neuropsychology of vascu-lar cognitive impairment: Is there a specific cognitivedeficit? Journal of the Neurological Sciences, 226, 3–7.
Devanand, D. P., Folz, M., Gorlyn, M., Moeller, J. R.,& Stern, Y. (1997). Questionable dementia: Clinicalcourse and predictors of outcome. Journal of theAmerican Geriatrics Society, 45, 321–328.
Devanand, D. P., Habeck, C. G., Tabert, M. H.,Scarmeas, N., Pelton, G. H., Moeller, J. R., et al.(2006). PET network abnormalities and cognitive
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

522 TALER AND PHILLIPS
decline in patients with mild cognitive impairment.Neuropsychopharmacology, 31, 1327–1334.
Diehl, J., Monsch, A. U., Aebi, C., Wagenpfeil, S.,Krapp, S., Grimmer, T., et al. (2005). Frontotemporaldementia, semantic dementia, and Alzheimer’s dis-ease: The contribution of standard neuropsychologi-cal tests to differential diagnosis. Journal of GeriatricPsychiatry and Neurology, 18, 39–44.
Dudas, R. B., Clague, F., Thompson, S. A., Graham, K. S.,& Hodges, J. R. (2005). Episodic and semantic mem-ory in mild cognitive impairment. Neuropsychologia,43, 1266–1276.
Duff Canning, S. J., Leach, L., Stuss, D., Ngo, L., &Black, S. E. (2004). Diagnostic utility of abbreviatedfluency measures in Alzheimer disease and vasculardementia. Neurology, 62, 556–562.
Duong, A., Whitehead, V., Hanratty, K., & Chertkow, H.(2006). The nature of lexico-semantic processing defi-cits in mild cognitive impairment. Neuropsychologia,44, 1928–1935.
Dwolatzky, T., Whitehead, V., Doniger, G. M., Simon,E. S., Schweiger, A., Jaffe, D., et al. (2003). Validityof a novel computerized cognitive battery for mildcognitive impairment. BMC Geriatrics, 3, 4.
Ekstrom, R. B., French, J. W., & Harman, H. H. (1976).Kit of factor-referenced cognitive tests. Princeton, NJ:Educational Testing Service.
Elias, M., Beiser, A., Wolf, P., Au, R., White, R., &D’Agostino, R. (2000). The preclinical phase ofAlzheimer disease: A 22-year prospective study of theFramingham cohort. Archives of Neurology, 57,808–813.
Enderby, P., Wood, V., & Wade, D. (1987). FrenchayAphasia Screening Test Manual. Windsor, UK:NFER-Nelson.
Fabrigoule, C., Rouch, I., Taberly, A., Letenneur, L.,Commenges, D., Mazaux, J.-M., et al. (1998). Cogni-tive processes in preclinical phase of dementia. Brain,121, 135–141.
Feldman, H. H., & Jacova, C. (2005). Mild cognitiveimpairment. American Journal of Geriatric Psychia-try, 13, 645–655.
Fillenbaum, G. G., McCurry, S. M., Kuchibhatla, M.,Masaki, K. H., Borenstein, A. R., Foley, D. J., et al.(2005). Performance on the CERAD neuropsychologybattery of two samples of Japanese-American elders:Norms for persons with and without dementia. Jour-nal of the International Neuropsychological Society,11, 192–201.
Fischer, P., Jungwirth, S., Zehetmayer, S., Weissgram, S.,Hoenigschnabl, S., Gelpi, E., et al. (2007). Conver-sion from subtypes of mild cognitive impairment toAlzheimer dementia. Neurology, 23, 288–291.
Fisher, N. J., Rourke, B. P., & Bieliauskas, L. A. (1999).Neuropsychological subgroups of patients withAlzheimer’s disease: An examination of the first 10years of CERAD data. Journal of Clinical and Exper-imental Neuropsychology, 21, 488–518.
Fisher, N. J., Tierney, M., Rourke, B. P., & Szalai, J. P.(2004). Verbal fluency patterns in two subgroups ofpatients with Alzheimer’s disease. The Clinical Neu-ropsychologist, 18, 122–131.
Fleisher, A. S., Sowell, B. B., Taylor, C., Gamst, A. C.,Petersen, R. C., & Thal, L. J. (2007). Clinical pre-dictors of progression to Alzheimer’s disease inamnestic mild cognitive impairment. Neurology, 68,1588–1595.
Flicker, C., Ferris, S. H., & Reisberg, B. (1991). Mildcognitive impairment in the elderly: Predictors ofdementia. Neurology, 41, 1006–1009.
Folstein, M., Folstein, S., & McHugh, P. (1975). “Mini-mental state.” A practical method for grading thecognitive state of patients for the clinician. Journal ofPsychiatric Research, 12, 189–198.
Forbes, K. E., Shanks, M. F., & Venneri, A. (2004). Theevolution of dysgraphia in Alzheimer’s disease. BrainResearch Bulletin, 63, 19–24.
Forbes, K. E., Venneri, A., & Shanks, M. F. (2002). Dis-tinct patterns of spontaneous speech deterioration:An early predictor of Alzheimer’s disease. Brain andCognition, 48, 356–361.
Forbes-McKay, K. E., Ellis, A. W., Shanks, M. F., &Venneri, A. (2005). The age of acquisition of wordsproduced in a semantic fluency task can reliably dif-ferentiate normal from pathological age related cog-nitive decline. Neuropsychologia, 43, 1625–1632.
Forbes-McKay, K. E., & Venneri, A. (2005). Detectingsubtle spontaneous language decline in earlyAlzheimer’s disease with a picture description task.Neurological Science, 26, 243–254.
Fowler, K. S., Saling, M. M., Conway, E. L., Semple, J. M.,& Louis, W. J. (2002). Paired-associate performancein the early detection of DAT. Journal of the Interna-tional Neuropsychological Society, 8, 58–71.
Fox, N. C., Kennedy, A. M., Harvey, R. J., Lantos, P. L.,Roques, P. K., Collinge, J. et al. (1997). Clinico-pathological features of familial Alzheimer’s diseaseassociated with the M139V mutation in the presenilin1 gene. Pedigree but not mutation specific age atonset provides evidence for a further genetic factor.Brain, 120, 491–501.
Fox, N. C., Warrington, E. K., Freeborough, P. A.,Hartikainen, P., Kennedy, A. M., Stevens, J. M., et al.(1996). Presymptomatic hippocampal atrophy inAlzheimer’s disease. A longitudinal MRI study.Brain, 119, 2001–2007.
Fox, N. C., Warrington, E. K., Seiffer, A. L., Agnew, S. K.,& Rossor, M. N. (1998). Presymptomatic cognitivedeficits in individuals at risk of familial Alzheimer’sdisease. A longitudinal prospective study. Brain, 121,1631–1639.
Fox, N. C., Warrington, E. K., Stevens, J. M., & Rossor,M. N. (1996). Atrophy of the hippocampal formationin early familial Alzheimer’s disease. A longitudinalMRI study of at-risk members of a family with anamyloid precursor protein 717Val-Gly mutation.Annals of the New York Academy of Sciences, 777,226–232.
Frisoni, G. B., Galluzzi, S., Bresciani, L., Zanetti, O., &Geroldi, C. (2002). Mild cognitive impairment withsubcortical vascular features: Clinical characteristicsand outcome. Journal of Neurology, 249, 1423–1432.
Fujimori, M., Imamura, T., Yamashita, H., Hirono, N.,Ikejiri, Y., Shimomura, T., et al. (1998). Age at onsetand visuocognitive disturbances in Alzheimer’s dis-ease. Alzheimer’s Disease and Associated Disorders, 3,163–166.
Fuld, P. A. (1981). Fuld object memory evaluation.Chicago: Stoelting.
Fung, T. D., Chertkow, H., Murtha, S., Whatmough, C.,Peloquin, L., Whitehead, V., et al. (2001). The spec-trum of category effects in object and action knowl-edge in dementia of the Alzheimer’s type.Neuropsychology, 15, 371–379.
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

LANGUAGE PERFORMANCE IN MCI AND AD 523
Galluzzi, S., Sheu, C.-F., Zanetti, O., & Frisoni, G. B.(2005). Distinctive clinical features of mild cognitiveimpairment with subcortical cerebrovascular dis-ease. Dementia and Geriatric Cognitive Disorders,19, 196–203.
Galton, C. J., Erziçlioglu, S., Sahakian, B. J., Antoun, N.,& Hodges, J. R. (2005). A comparison of theAddenbrooke’s Cognitive Examination (ACE), con-ventional neuropsychological assessment and simpleMRI-based medial temporal lobe evaluation in theearly diagnosis of Alzheimer’s disease. Cognitive andBehavioral Neurology, 18, 144–150.
Galvin, J. E., Powlishta, K. K., Wilkins, K., McKeel,D. W., Xiong, C., Grant, E., et al. (2005). Predictorsof preclinical Alzheimer disease and dementia: Aclinicopathologic study. Archives of Neurology, 62,758–765.
Garrard, P., Maloney, L. M., Hodges, J. R., &Patterson, K. (2005). The effects of very earlyAlzheimer’s disease on the characteristics of writingby a renowned author. Brain, 128, 250–260.
Geslani, D., Tierney, M., Herrmann, N., & Szalai, J.(2005). Mild cognitive impairment: An operationaldefinition and its conversion rate to Alzheimer’s dis-ease. Dementia and Geriatric Cognitive Disorders, 19,383–389.
Glosser, G., & Kaplan, E. (1989). Linguistic and nonlin-guistic impairments in writing: A comparison ofpatients with focal and multifocal CNS disorders.Brain and Language, 37, 357–380.
Gold, B. T., Balota, D. A., Cortese, M. J., Sergent-Marshall, S. D., Snyder, A. Z., Salat, D. H., et al.(2005). Differing neuropsychological and neuroana-tomical correlates of abnormal reading in early-stagesemantic dementia and dementia of the Alzheimertype. Neuropsychologia, 43, 833–846.
Gold, G., Giannakopoulos, P., Montes-Paixao, C.,Hermann, F. R., Mulligan, R., Michel, J.-P., et al.(1997). NINCDDS/AIREN criteria. Neurology, 49,692.
Goldman, W. P., Price, J. L., Storandt, M., Grant, E. A.,McKeel, D. W., Rubin, E. H., et al. (2001). Absenceof cognitive impairment or decline in preclinicalAlzheimer’s disease. Neurology, 56, 361–367.
Gómez, R. G., & White, D. A. (2006). Using verbal flu-ency to detect very mild dementia of the Alzheimertype. Archives of Clinical Neurology, 21, 771–775.
Gómez-Isla, T., & Hyman, B. T. (2003). Neuropatholog-ical changes in normal aging, mild cognitive impair-ment and Alzheimer’s disease. In R. C. Petersen(Ed.), Mild cognitive impairment (pp. 191–204). NewYork: Oxford University Press.
Goodglass, H., & Kaplan, E. (1983). The assessment ofaphasia and related disorders. Philadelphia: Lea &Febiger.
Graets, P., DeBleser, R., & Willmes, K. (1992). AkenseAfasie Test [Aachen Aphasia Test]. Lisse, The Neth-erlands: Swets and Zeitlinger.
Graham, J. E., Rockwood, K., Beattie, B. L., Eastwood, R.,Gauthier, S., Tuokko, H., et al. (1997). Prevalenceand severity of cognitive impairment with and with-out dementia in an elderly population. Lancet, 349,1793–1796.
Graham, N. L., Emery, T., & Hodges, J. R. (2004). Dis-tinctive cognitive profiles in Alzheimer’s disease andsubcortical vascular dementia. Journal of Neurology,Neurosurgery and Psychiatry, 75, 61–71.
Gregory, C. A., Orrell, M., Sahakian, B. J., & Hodges, J.R. (1997). Can frontotemporal dementia and Alzhe-imer’s disease be differentiated using a brief batteryof tests? International Journal of Geriatric Psychiatry,12, 375–383.
Griffith, H. R., Netson, K. L., Harrell, L. E., Zamrini,E. Y., Brockington, J. C., & Marson, D. C. (2006).Amnestic mild cognitive impairment: Diagnostic out-comes and clinical prediction over a two-year timeperiod. Journal of the International Neuropsychologi-cal Society, 12, 166–175.
Grober, E., & Kawas, C. (1997). Learning and retentionin preclinical and early Alzheimer’s disease. Psychol-ogy and Aging, 12, 183–188.
Grossman, M., Koenig, P., DeVita, C., Glosser, G.,Moore, P., Gee, J., et al. (2003a). Neural basis forverb processing in Alzheimer’s disease: An fMRIstudy. Neuropsychology, 17, 658–674.
Grossman, M., Mickanin, J., Onishi, K., & Hughes,E. (1996). Verb comprehension deficits in proba-ble Alzheimer’s disease. Brain and Language, 53,369–389.
Grossman, M., Smith, E. E., Koenig, P. L., Glosser, G.,Rhee, J., & Dennis, K. (2003b). Categorization ofobject descriptions in Alzheimer’s disease and fronto-temporal dementia: Limitation in rule-based process-ing. Cognitive, Affective, and BehavioralNeuroscience, 3, 120–132.
Grundman, M., Petersen, R. C., Ferris, S. H., Thomas,R. G., Aisen, P. S., Bennett, D. A., et al. (2004). Mildcognitive impairment can be distinguished fromAlzheimer disease and normal aging for clinical trials.Archives of Neurology, 61, 59–66.
Guarch, J., Marcos, T., Salamero, M., & Blesa, R.(2004). Neuropsychological markers of dementia inpatients with memory complaints. International Jour-nal of Geriatric Psychiatry, 19, 352–358.
Hachinski, V. C., Lassen, N. A., & Marshall, J. (1974).Multi-infarct dementia: A cause of mental deteriora-tion in the elderly. Lancet, 2, 207–210.
Hanninen, T., Hallikainen, M., Koivisto, K., Helkala,E. L., Reinikainen, K. J., Soininen, H., et al. (1995). Afollow-up study of age-associated memory impair-ment: Neuropsychological predictors of dementia.Journal of the American Geriatrics Society, 43,1007–1015.
Henderson, V. W., Buckwalter, J. G., Sobel, E., Freed,D. M., & Diz, M. M. (1992). The agraphia ofAlzheimer’s disease. Neurology, 42, 777–784.
Henry, J. D., Crawford, J. R., & Phillips, L. H. (2004).Verbal fluency performance in dementia of the Alzhe-imer’s type: A meta-analysis. Neuropsychologia, 42,1212–1222.
Hodges, J. R., Erzinçlioglu, S., & Patterson, K. (2006).Evolution of cognitive deficits and conversion todementia in patients with mild cognitive impairment:A very long-term follow-up study. Dementia andGeriatric Cognitive Disorders, 21, 380–391.
Hodges, J. R., & Patterson, K. (1995). Is semantic mem-ory consistently impaired early in the course ofAlzheimer’s disease? Neuroanatomical and diagnos-tic implications. Neuropsychologia, 33, 441–459.
Hodges, J. R., Patterson, K., Graham, N., & Dawson, K.(1996). Naming and knowing in dementia ofAlzheimer’s type. Brain and Language, 54, 302–325.
Hodges, J. R., Patterson, K., Oxbury, S., & Funnell, E.(1992b). Semantic dementia: Progressive fluent
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

524 TALER AND PHILLIPS
aphasia with temporal lobe atrophy. Brain, 115,1783–1806.
Hodges, J. R., Patterson, K., Ward, R., Garrard, P.,Bak, T., Perry, R., et al. (1999). The differentiation ofsemantic dementia and frontal lobe dementia (tempo-ral and frontal variants of frontotemporal dementia)from early Alzheimer’s disease: A comparative neu-ropsychological study. Neuropsychology, 13, 31–40.
Hodges, J. R., Salmon, D. P., & Butters, N. (1992a).Semantic memory impairment in Alzheimer’s disease:Failure of access or degraded knowledge? Neuropsy-chologia, 30, 301–314.
Horner, J., Heyman, A., Dawson, D., & Rogers, H.(1988). The relationship of agraphia to the severity ofdementia in Alzheimer’s disease. Archives of Neurol-ogy, 45, 760–763.
Howard, D., & Patterson, K. (1992). Pyramids and PalmTrees: A test of semantic access from pictures andwords. Bury St Edmunds, UK: Thames Valley Pub-lishing Company.
Howieson, D. B., Dame, A., Camicioli, R., Sexton, G.,Payami, H., & Kaye, J. A. (1997). Cognitive markerspreceding Alzheimer’s dementia in the healthy oldest old.Journal of the American Geriatric Society, 45, 584–589.
Hudon, C., Belleville, S., Souchay, C., Gely-Nargeot, M.C., Chertkow, H., & Gauthier, S. (2006). Memory forgist and detail information in Alzheimer’s disease andmild cognitive impairment. Neuropsychology, 20,566–577.
Huff, F. J. (1990). Language in normal aging and age-related neurological diseases. In R. D. Nebes &S. Corkin (Eds.), Handbook of neuropsychology.Amsterdam: Elsevier.
Hughes, C. P., Berg, L., Danziger, W. L., Coben, L. A., &Martin, R. L. (1982). A new clinical scale for the stagingof dementia. British Journal of Psychiatry, 140, 566–572.
Hutchinson, A. D., & Mathias, J. L. (2007). Neuropsy-chological deficits in frontotemporal dementia andAlzheimer’s disease: A meta-analytic review. Journal ofNeurology, Neurosurgery and Psychiatry, 78, 917–928.
Iqbal, K., Alonso Adel, C., Chen, S., Chohan, M. O.,El-Akkad, E., Gong, C. X., et al. (2005). Tau pathologyin Alzheimer disease and other tauopathies. Biochimicaet Biophysica Acta, 1739, 198–210.
Irigaray, L. (1973). Le langage des dements [Language indementia]. The Hague: Mouton.
Jack, C. R., Petersen, R. C, Xu, Y. C., O’Brien, P. C.,Smith, G. E., Ivnik, R. J., et al. (1999). Prediction ofAD with MRI-based hippocampal volume in mildcognitive impairment. Neurology, 52, 1397–1403.
Jack, C. R., Petersen, R. C., Xu, Y. C., Waring, S. C.,O’Brien, P. C., Tangalos, E. G., et al. (1997). Medialtemporal atrophy on MRI in normal aging and verymild Alzheimer’s disease. Neurology, 49, 786–794.
Jacobs, D. M., Sano, M., Dooneief, G., Marder, K.,Bell, K. L., & Stern, Y. (1995). Neuropsychologicaldetection and characterization of preclinical Alzheimer’sdisease. Neurology, 45, 317–324.
Jacobson, M. W., Delis, D. C., Bondi, M. W., &Salmon, D. P. (2002). Do neuropsychological testsdetect preclinical Alzheimer’s disease: Individual-testversus cognitive discrepancy score analyses. Neu-ropsychology, 16, 132–139.
Johnson, J. K., Head, E., Kim, R., Starr, A., & Cotman,C. W. (1999). Clinical and pathological evidence for afrontal variant of Alzheimer disease. Archives ofNeurology, 56, 1233–1239.
Jones, S., Laukka, E. J., & Bäckman, L. (2006). Differ-ential verbal fluency deficits in the preclinical stagesof Alzheimer’s disease and vascular dementia.Cortex, 42, 347–355.
Jorm, A. F., Masaki, K. H., Petrovitch, H., WebsterRoss, G., & White, L. R. (2005). Cognitive deficits 3to 6 years before dementia onset in a population sam-ple: The Honolulu-Asia aging study. Journal of theAmerican Geriatrics Society, 53, 452–455.
Kalbe, E., Kessler, J., Calabrese, P., Smith, R.,Passmore, A. P., Brand, M., et al. (2004). DemTect:A new, sensitive cognitive screening test to supportthe diagnosis of mild cognitive impairment and earlydementia. International Journal of Geriatric Psychia-try, 19, 136–143.
Kaplan, E. F., Goodglass, H., & Weintraub, S. (1983).Boston Naming Test. Philadelphia: Lea & Febiger.
Karrasch, M., Sinervä, E., Grönholm, P., Rinne, J., &Laine, M. (2005). CERAD test performances inamnestic mild cognitive impairment and Alzheimer’sdisease. Acta Neurologica Scandinavica, 111, 172–179.
Kemper, S., LaBarge, E., Ferraro, R. F., Cheung, H.,Cheung, H., & Storandt, M. (1993). On the preserva-tion of syntax in Alzheimer’s disease. Archives ofNeurology, 50, 81–86.
Kempler, D., Curtiss, S., & Jackson, C. (1987). Syntacticpreservation in Alzheimer’s disease. Journal of Speechand Hearing Research, 30, 343–350.
Kertesz, A. (1982). The Western Aphasia Battery. NewYork: Grune and Stratton.
Kertesz, A. (1994). Language deterioration in dementia.In V. O. B. Emery & T. E. Oxman (Eds.), Dementia:Presentations, differential diagnosis and nosology.Baltimore, MD: Johns Hopkins University Press.
Kluger, A., Ferris, S. H., Golomb, J., Mittelman, M. S.,& Reisberg, B. (1999). Neuropsychological predictionof decline to dementia in nondemented elderly. Journalof Geriatric Psychiatry and Neurology, 12, 168–179.
Kral, V. A. (1962). Senescent forgetfulness: Benign andmalignant. Canadian Medical Association Journal, 86,257–260.
Kramer, J. H., Jurik, J., Sha, S. J., Rankin, K. P., Rosen,H. J., Johnson, J. K., et al. (2003). Distinctive neu-ropsychological patterns in frontotemporal dementia,semantic dementia, and Alzheimer disease. Cognitiveand Behavioral Neurology, 16, 211–218.
Kraut, M. A., Cherry, B., Pitcock, J. A., Anand, R., Li, J.,Vestal, L., et al. (2007). The Semantic ObjectRetrieval Test (SORT) in amnestic mild cognitiveimpairment. Cognitive and Behavioral Neurology, 20,62–67.
Kraut, M. A., Kremen, S., Segal, J. B., Calhoun, V.,Moo, L. R., & Hart, J. (2002). Object activation fromfeatures in the semantic system. Journal of CognitiveNeuroscience, 14, 24–36.
Lam, L. C. W., Ho, P., Lui, V. W. C., & Tam, C. W. C.(2006). Reduced semantic fluency as an additionalscreening tool for subjects with questionable demen-tia. Dementia and Geriatric Cognitive Disorders, 22,159–164.
Lambon Ralph, M. A., Patterson, K., Graham, N.,Dawson, K., & Hodges, J. R. (2003). Homogeneityand heterogeneity in mild cognitive impairment andAlzheimer’s disease: A cross-sectional and longitudi-nal study of 55 cases. Brain, 126, 2350–2362.
Lambon Ralph, M. A., Powell, J., Howard, D.,Whitworth, A. B., Garrard, P., & Hodges, J. R.
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

LANGUAGE PERFORMANCE IN MCI AND AD 525
(2001). Semantic memory is impaired in both demen-tia with Lewy bodies and dementia of Alzheimer’stype: A comparative neuropsychological study andliterature review. Journal of Neurology, Neurosurgeryand Psychiatry, 70, 149–156.
Lane, F., & Snowdon, J. (1989). Memory and dementia:A longitudinal survey of suburban elderly. In P.Lovibond & P. Wilson (Eds.), Clinical and abnormalpsychology (pp. 365–376). Amsterdam: Elsevier.
Laukka, E. J., Jones, S., Small, B. J., Fratiglioni, L., &Bäckman, L. (2004). Similar patterns of cognitivedeficits in the preclinical stages of vascular dementiaand Alzheimer’s disease. Journal of the InternationalNeuropsychological Society, 10, 382–391.
Lee, D. Y., Youn, J. C., Choo, I. H., Kim, K. W., Jhoo,J. H., Pak, Y. S., et al. (2006). Combination of clinicaland neuropsychologic information as a better predic-tor of the progression to Alzheimer disease in ques-tionable dementia individuals. American Journal ofGeriatric Psychiatry, 14, 130–138.
Levy, R. (1994). Aging-associated cognitive decline.International Psychogeriatrics, 6, 63–68.
Lezak, M. D. (1995). Neuropsychological assessment (3rded.). New York: Oxford University Press.
Light, L., & Burke, D. M. (1993). Patterns of languageand memory in old age. In L. L. Light & D. M. Burke(Eds.), Language, memory and aging. New York:Cambridge University Press.
Linn, R. T., Wolf, P. A,, Bachman, D. L., Knoefel, J. E.,Cobb, J. L., Belanger, A. J., et al. (1995). The “pre-clinical phase” of probable Alzheimer’s disease.Archives of Neurology, 52, 485–490.
Loewenstein, D. A., Acevedo, A., Agron, J., Issacson, R.,Strauman, S., Crocco, E., et al. (2006). Cognitive pro-files in Alzheimer’s disease and in mild cognitiveimpairment of different etiologies. Dementia andGeriatric Cognitive Disorders, 21, 309–315.
Lopez, O. L., Becker, J. T., Jagust, W. J., Fitzpatrick, A.,Carlson, M. C., DeKosky, S. T. et al. (2006). Neu-ropsychological characteristics of mild cognitiveimpairment subgroups. Journal of Neurology, Neuro-surgery and Psychiatry, 77, 159–165.
Luis, C. A., Barker, W. W., Loewenstein, D. A., Crum,T. A., Rogaevad, E., Kawarai, T., et al. (2004). Con-version to dementia among two groups with cognitiveimpairment. Dementia and Geriatric Cognitive Disor-ders, 18, 307–313.
Lukatela, K., Malloy, P., Jenkins, M., & Cohen, R.(1998). The naming deficit in early Alzheimer’s andvascular dementia. Neuropsychology, 21, 565–572.
Luzzatti, C., Laiacona, M., & Agazzi, D. (2003). Multi-ple patterns of writing disorders in dementia of theAlzheimer type and their evolution. Neuropsycholo-gia, 41, 759–772.
Mack, W. J., Freed, D. M., Williams, B. W., & Henderson,V. W. (1992). Boston Naming Test: Shortenedversions for use in Alzheimer’s disease. Journal ofGerontology: Psychological Sciences, 47, P154–P158.
Marcos, A., Gil, P., Barabash, A., Rodriguez, R., Encinas,M., Fernandez, C., et al. (2006). Neuropsychologicalmarkers of progression from mild cognitive impairmentto Alzheimer’s disease. American Journal of Alzheimer’sDisease and Associated Disorders, 21, 189–196.
Martin, A., & Fedio, P. (1983). Word production andcomprehension in Alzheimer’s disease: The break-down of semantic knowledge. Brain and Language,19, 124–141.
Massman, P. J., Delis, D. C., Filoteo, J. V., Butters, N.,Salmon, D. P., & Demadura, T. L. (1993). Mecha-nisms of spatial impairment in Alzheimer’s diseasesubgroups: Differential breakdown of directedattention to global–local stimuli. Neuropsychology,7, 172–181.
Massoud, F., Chertkow, H., Whitehead, V., Overbury, O.,& Bergman, H. (2002). Word-reading thresholds inAlzheimer disease and mild memory loss: A pilotstudy. Alzheimer Disease and Associated Disorders,16, 31–39.
Masur, D. M., Sliwinski, M., Lipton, R. B., Blau, A. D.,& Crystal, H. A. (1994). Neuropsychological predic-tion of dementia and the absence of dementia inhealthy elderly persons. Neurology, 44, 1427–1432.
McKeith, I. G., Ballard, C. G., Perry, R. H., Ince, P. G.,O’Brien, J. T., Neill, D., et al. (2000). Prospective val-idation of consensus criteria for the diagnosis ofdementia with Lewy bodies. Neurology, 54, 1050–1058.
McKenna, P., & Warrington, E. (1983). The GradedNaming Test. Windsor, UK: Nelson.
McKhann, G., Drachman, D., Folstein, M., Katzman, R.,Price, D., & Stadlan, E. M. (1984). Clinical diagnosisof Alzheimer’s disease: Report of the NINCDS-ADRDA workgroup under the auspices of Depart-ment of Health and Human Services Task Force onAlzheimer’s disease. Neurology, 34, 939–944.
Meguro, K., Ishii, H., Yamaguchi, S., Ishizaki, J., Sato, M.,Hashimoto, R., et al. (2004). Prevalence and cog-nitive performances of Clinical Dementia Rating 0.5and mild cognitive impairment in Japan. Alzheimer’sDisease and Associated Disorders, 18, 3–10.
Mendola, J. D., Cronin-Golumb, A., Corkin, S., &Growdon, J. H. (1995). Prevalence of visual deficitsin Alzheimer’s disease. Optometry and Vision Science,72, 155–167.
Meyer, J. S., Xu, G., Thornby, J., Chowdhury, M., &Quach, M. (2002). Longitudinal analysis of abnormaldomains comprising mild cognitive impairment(MCI) during aging. Journal of the NeurologicalSciences, 201, 19–25.
Mioshi, E., Dawson, K., Mitchell, J., Arnold, R., &Hodges, J. R. (2006). The Addenbrooke’s CognitiveExamination Revised (ACE-R): A brief cognitive testbattery for dementia screening. International Journalof Geriatric Psychiatry, 21, 1078–1085.
Monsch, A. U., Bondi, M. W., Butters, N., Salmon, D. P.,Katzman, R., & Thal, L. J. (1992). Comparisons ofverbal fluency tasks in the detection of dementia of theAlzheimer type. Archives of Neurology, 49, 1253–1258.
Morris, J. C., McKeel, D. W., Fulling, K., Torack, R. M.,& Berg, L. (1988a). Validation of clinical criteria forAlzheimer’s disease. Annals of Neurology, 24, 17–22.
Morris, J. C., Mohs, R. C., Rogers, H., Fillenbaum, G. C.,& Heyman, A. (1988b). Consortium to establish aregistry for Alzheimer’s disease (CERAD). Clinicaland neuropsychological assessment of Alzheimer’sdisease. Psychopharmacology Bulletin, 24, 641–652.
Morris, J. C., Storandt, M., Miller, J. P., McKeel, D. W.,Price, J. L., Rubin, E. H., et al. (2001). Mild cognitiveimpairment represents early-stage Alzheimer disease.Archives of Neurology, 58, 397–405.
Murphy, K. J., Rich, J. B., & Troyer, A. K. (2006). Ver-bal fluency patterns in amnestic mild cognitiveimpairment are characteristic of Alzheimer’s typedementia. Journal of the International Neuropyscho-logical Society, 12, 570–574.
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009
526 TALER AND PHILLIPS
Nasreddine, Z. S., Phillips, N. A., Bédirian, V.,Charbonneau, S., Whitehead, V., Collin, I., et al.(2005). The Montreal Cognitive Assessment, MoCA:A brief screening tool for mild cognitive impairment.Journal of the American Geriatric Society, 53, 695–699.
Neary, D., Snowden, J. S., Gustafson, L., Passant, U.,Stuss, D., Black, S., et al. (1998). Frontotemporallobar degeneration: A consensus on clinical diagnos-tic criteria. Neurology, 51, 1546–1554.
Neils, J., Boller, F., Gerdeman, B., & Cole, M. (1989).Descriptive writing abilities in Alzheimer’s disease.Journal of Clinical and Experimental Neuropsychol-ogy, 11, 692–698.
Nelson, H. E. (1982). National Adult Reading Test(NART): Test manual. Windsor, UK: NFER Nelson.
Nestor, P. J., Fryer, T. D., Smielewski, P., & Hodges, J. R.(2003). Limbic hypometabolism in Alzheimer’sdisease and mild cognitive impairment. Annals ofNeurology, 54, 343–351.
Newman, S. K., Warrington, E. K., Kennedy, A. M., &Rossor, M. N. (1994). The earliest cognitive changein a person with familial Alzheimer’s disease: Pre-symptomatic neuropsychological features in a pedi-gree with familial Alzheimer’s disease confirmed atnecropsy. Journal of Neurology, Neurosurgery, andPsychiatry, 57, 967–972.
Nielsen, H., Lolk, A., Andersen, K., Andersen, J., &Kragh-Sorensen, P. (1999). Characteristics of elderlywho develop Alzheimer’s disease during the next twoyears—a neuropsychological study using CAMCOG.The Odense study. International Journal of GeriatricPsychiatry, 14, 957–963.
Nordlund, A., Rolstad, S., Hellström, P., Sjögren, M.,Hansen, S., & Wallin, A. (2005). The Goteburg MCIstudy: Mild cognitive impairment is a heterogeneouscondition. Journal of Neurology, Neurosurgery, andPsychiatry, 76, 1485–1490.
Olichney, J. M., Morris, S. K., Ochoa, C., Salmon, D. P.,Thal, L. J., Kutas, M., et al. (2002). Abnormal verbalevent related potentials in mild cognitive impairmentand incipient Alzheimer’s disease. Journal of Neurol-ogy, Neurosurgery and Psychiatry, 73, 377–384.
Östberg, P., Fernaeus, S.-E., Hellström, A., Bogdanovic, N.,& Wahlund, L.-O. (2005). Impaired verb fluency:A sign of mild cognitive impairment. Brain and Lan-guage, 95, 273–279.
Pachana, N. A., Boone, K. B., Miller, B. L., Cummings,J. L., & Berman, N. (1996). Comparison of neuropsy-chological functioning in Alzheimer’s disease andfrontotemporal dementia. Journal of the InternationalNeuropsychological Society, 2, 505–510.
Pasquier, F. (1999). Early diagnosis of dementia: Neu-ropsychology. Journal of Neurology, 246, 6–15.
Patel, P. G., & Satz, P. (1994). The language productionsystem and senile dementia of the Alzheimer’s type:Neuropathological implications. Aphasiology, 8, 1–18.
Perri, R., Koch, G., Carlesimo, G. A., Serra, L., Fadda, L.,Pasqualetti, P., et al. (2005). Alzheimer’s disease andfrontal variant of frontotemporal dementia: A verybrief battery for cognitive and behavioral distinction.Journal of Neurology, 252, 1238–1244.
Perry, R. J., & Hodges, J. R. (2000). Differentiatingfrontal and temporal variant frontotemporaldementia from Alzheimer’s disease. Neurology, 54,2277–2284.
Perry, R. J., Watson, P., & Hodges, J. R. (2000). Thenature and staging of attention dysfunction in early
(minimal and mild) Alzheimer’s disease: Relationshipto episodic and semantic memory impairment.Neuropsychologia, 38, 252–271.
Petersen, R. C. (2003). Mild cognitive impairment. NewYork: Oxford University Press.
Petersen, R. C. (2004). Mild cognitive impairment as adiagnostic entity. Journal of Internal Medicine, 256,183–194.
Petersen, R. C., Doody, R., Kurz, A, Mohs, R. C.,Morris, J. C., Rabins, P. V., et al. (2001a). Currentconcepts in mild cognitive impairment. Archives ofNeurology, 58, 1985–1992.
Petersen, R. C., & Morris, J. C. (2003). Clinical features.In R. C. Petersen (Ed.), Mild cognitive impairment(pp. 15–39). New York: Oxford University Press.
Petersen, R. C., Smith, G. E., Waring, S. C., Ivnik, R. J.,Tangalos, E. G., & Kokmen, E. (1999). Mildcognitive impairment: Clinical characterization andoutcome. Archives of Neurology, 56, 303–308.
Petersen, R. C., Stevens, J. C., Ganguli, M., Tangalos,E. G., Cummings, J. L., & DeKosky, S. T. (2001b).Practice parameter: Early detection of dementia:Mild cognitive impairment (an evidence-basedreview). Report of the Quality Standards Subcommit-tee of the American Academy of Neurology. Neurol-ogy, 56, 1133–1142.
Price, C. C., & Grossman, M. (2005). Verb agreementsduring on-line sentence processing in Alzheimer’sdisease and frontotemporal dementia. Brain andLanguage, 94, 217–232.
Puregger, E., Walla, P., Deecke, L., & Dal-Bianco, P.(2003). Magnetoencephalographic features related tomild cognitive impairment. NeuroImage, 20, 2235–2244.
Pyo, G., Elble, R. J., Ala, T., & Markwell, S. J. (2006).The characteristics of patients with uncertain/mildcognitive impairment on the Alzheimer DiseaseAssessment Scale–Cognitive subscale. Alzheimer’sDisease and Associated Disorders, 20, 16–22.
Rasmusson, D. X., Carson, K. A., Brookmeyer, A.,Kawas, C., & Brandt, J. (1996). Predicting rate ofcognitive decline in probable Alzheimer’s disease.Brain & Cognition, 31, 133–147.
Ravdin, L. D., Katzen, H. L., Agrawal, P., & Relkin, N. R.(2003). Letter and semantic fluency in older adults:Effects of mild depressive symptoms and age-stratifiednormative data. The Clinical Neuropsychologist, 17,195–202.
Reisberg, B., Ferris, S. H., de Leon, M. J., & Crook, T.(1982). The global deterioration scale for assessmentof primary degenerative dementia. American Journalof Psychiatry, 139, 1136–1139.
Ribeiro, F., de Mendonça, A., & Guerreiro, M. (2006).Mild cognitive impairment: Deficits in cognitivedomains other than memory. Dementia and GeriatricCognitive Disorders, 21, 284–290.
Richards, M., Touchon, J., Ledesert, B., & Ritchie, K.(1999). Cognitive decline in ageing: Are AAMI andAACD distinct entities? International Journal ofGeriatric Psychiatry, 14, 534–540.
Riley, K. P., Snowdon, D. A., Desrosiers, M. F., &Markesberry, W. R. (2005). Early life linguistic abil-ity, late life cognitive function, and neuropathology:Findings from the Nun Study. Neurobiology of Aging,26, 341–347.
Ritchie, K., Artero, S., & Touchon, J. (2001). Classificationcriteria for mild cognitive impairment: A population-based validity study. Neurology, 56, 37–42.
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

LANGUAGE PERFORMANCE IN MCI AND AD 527
Ritchie, K., & Fuhrer, R. (1992). A comparative study ofthe performance of screening tests for senile dementiausing receiver operating characteristics analysis.Journal of Clinical Epidemiology, 45, 627–637.
Rivas-Vasquez, R. A., Mendez, C., Rey, G. J., &Carrazana, E. J. (2004). Mild cognitive impairment:New neuropsychological and pharmacological target.Archives of Clinical Neuropsychology, 19, 11–27.
Rogers, T. T., Ivanoiu, A., Patterson, K., & Hodges, J. R.(2006). Semantic memory in Alzheimer's disease andthe frontotemporal dementias: A longitudinal studyof 236 patients. Neuropsychology, 20, 319–335.
Rohrer, D., Salmon, D. P., Wixted, J. T., & Paulsen, J. S.(1999). The disparate effects of Alzheimer’s diseaseand Huntington’s disease on semantic memory. Neu-ropsychology, 13, 381–388.
Royall, D. R., Mahurin, R. K., & Gray, K. F. (1992).Bedside assessment of executive cognitive impairment.Journal of the American Geriatric Society, 41,1221–1226.
Rubin, E. H., Storandt, M., Miller, J. P., Kinscherf, D. A.,Grant, E. A., Morris, J. C., et al. (1998). A prospec-tive study of cognitive function and onset of dementiain cognitively healthy elders. Archives of Neurology,55, 395–401.
Rubinstein, H., Garfield, L., & Millikan, J. A. (1970).Homographic entries in the internal lexicon. Journalof Verbal Learning and Verbal Behavior, 9, 487–494.
Sacuiu, S., Sjögren, M., Johansson, B., Gustafson, D., &Skoog, I. (2005). Prodromal cognitive signs ofdementia in 85-year-olds using four sources of infor-mation. Neurology, 65, 1894–1900.
Salmon, D. P., Thomas, R. G., Pay, M. M., Booth, A.,Hofstetter, C. R., Thal, L. J., et al. (2002). Neurology,59, 1022–1028.
Saxton, J., Lopez, O. L., Ratcliff, G., Dulberg, C.,Fried, L. P., Carlson, M. C., et al. (2004). PreclinicalAlzheimer’s disease: Neuropsychological test per-formance 1.5 to 8 years prior to onset. Neurology,63, 2341–2347.
Scahill, V. L., Hodges, J. R., & Graham, K. S. (2005).Can episodic memory differentiate semantic demen-tia from Alzheimer’s disease? Neurocase, 11, 441–451.
Schmidtke, K., & Hermeneit, S. (2007). High rate ofconversion to Alzheimer’s disease in a cohort ofamnestic MCI patients. International Psychogeriatrics.
Schwartz, M., Marin, O., & Saffran, E. (1979). Dissocia-tions of language function in dementia: A case study.Brain and Language, 7, 277–306.
Semenza, C., & Cipolotti, L. (1989). Neuropsicologia concarta e matita [Neuropsychology with pencil andpaper]. Padova, Italy: Cleup Editrice Padova.
Semenza, C., Mondini, S., Borgo, F., Pasini, M., &Sgaramella, M. T. (2003). Proper names in patientswith early Alzheimer’s disease. Neurocase, 9, 63–69.
Sherman, A. M., & Massman, P. J. (1999). Prevalenceand correlates of category versus letter fluency dis-crepancies in Alzheimer’s disease. Archives of ClinicalNeuropsychology, 14, 411–418.
Shimomura, T., Mori, E., Yamashita, T., Hirono, N.,Hashimoto, M., Tanimukai, S., et al. (1998). Cogni-tive loss in dementia with Lewy bodies and Alzheimerdisease. Archives of Neurology, 55, 1547–1552.
Silveri, M. C., Corda, F., & di Nardo, M. (2007). Cen-tral and peripheral aspects of writing disorders inAlzheimer’s disease. Journal of Clinical and Experi-mental Neuropsychology, 29, 179–186.
Silveri, M. C., Daniele, A., Giustolisi, L., & Gainotti, G.(1991). Dissociation between knowledge of living andnonliving things in dementia of the Alzheimer type.Neurology, 41, 545–546.
Small, B. J., & Bäckman, L. (1998). Predictors of longi-tudinal changes in memory, visuospatial, and verbalfunctioning in very old demented adults. Dementiaand Geriatric Cognitive Disorders, 9, 258–266.
Small, B. J., Fratiglioni, L., Viitanen, M., Winblad, B.,& Bäckman, L. (2000). The course of cognitiveimpairment in preclinical Alzheimer’s disease: Three-and 6-year follow-up of a population-based sample.Archives of Neurology, 57, 839–844.
Small, B. J., Herlitz, A., Fratiglioni, L., Almkvist, O., &Bäckman, L. (1997). Cognitive predictors of incidentAlzheimer’s disease: A prospective longitudinalstudy. Neuropsychology, 11, 413–420.
Snowdon, D. A., Kemper, S. J., Mortimer, J. A., Riley,K. P., Greiner, L. H., Wekstein, D. R., et al. (1996).Linguistic ability in early life and cognitive functionand Alzheimer’s disease in late life: Findings from theNun Study. Journal of the American Medical Associa-tion, 275, 528–532.
Standish, T. I. M., Molloy, D. W., Cunje, A., & Lewis,D. L. (2007). Do the ABCS 135 short cognitive screenand its subtests discriminate between normal cogni-tion, mild cognitive impairment and dementia? Inter-national Journal of Geriatric Psychiatry, 22, 189–194.
Stelzmann, R. A., Schnitzlein, H. N., & Murtagh, F. R.(1995). An English translation of Alzheimer’s 1907paper, “Uber eine eigenartige Erkrankung der Hirn-rinde.” Clinical Anatomy, 8, 429–431.
Stollery, B. T. (1996). The Automated Cognitive Test(ACT) System. Neurotoxicology and Teratology, 18,493–497.
Storandt, M., Grant, E. A., Miller, P., & Morris, J. C.(2002). Rates of progression in mild cognitive impair-ment and early Alzheimer’s disease. Neurology, 59,1034–1041.
Swainson, R., Hodges, J. R., Galton, C. J., Semple, J.,Michael, A., Dunn, B. D., et al. (2001). Early detec-tion and differential diagnosis of Alzheimer’s diseaseand depression with neuropsychological tasks. Demen-tia and Geriatric Cognitive Disorders, 12, 265–280.
Tabert, M. H., Manly, J. J., Liu, X., Pelton, G. H.,Rosenblum, S., Jacobs, M., et al. (2006). Neuropsy-chological prediction of conversion to Alzheimer dis-ease in patients with mild cognitive impairment.Archives of General Psychiatry, 63, 916–924.
Taler, V., Baum, S. R., Chertkow, H. C., & Saumier, D.(in press). Comprehension of grammatical and emo-tional prosody is impaired in Alzheimer’s disease.Neuropsychology.
Taler, V., & Jarema, G. (2004). Processing of mass/countinformation in Alzheimer’s disease and mild cognitiveimpairment. Brain and Language, 90, 262–275.
Taler, V., & Jarema, G. (2006). On-line lexical processingin AD and MCI: An early measure of cognitiveimpairment? Journal of Neurolinguistics, 19, 38–55.
Taler, V., Klepousniotou, E., & Phillips, N. A. (2007,June). Lexical ambiguity processing in healthy agingand mild cognitive impairment: An ERP study. Posterpresented at TENNET XVII: Annual Meeting ofTheoretical and Empirical Neuroscience, Montréal,QC, Canada.
Taler, V., & Phillips, N. A. (2006, April). An ERP studyof sentence processing in mild cognitive impairment:
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

528 TALER AND PHILLIPS
The effects of neighborhood density and congruency.Poster presented at the 11th Biennial Cognitive AgingConference, Atlanta, GA, USA.
Taylor, J. R., & Olichney, J. M. (2007). From amnesia todementia: ERP studies of memory and language.Clinical EEG and Neuroscience, 38, 8–17.
Teng, E. L., Hasegawa, K., Homma, A., Imai, Y.,Larson, E., Graves A., et al. (1994). The CognitiveAbilities Screening Instrument (CASI): A practicaltest for cross-cultural epidemiological studies ofdementia. International Psychogeriatrics, 6, 45–58.
Testa, J. A., Beatty, W. W., Gleason, A. C., Orbelo, D. M.,& Ross, E. D. (2001). Impaired affective prosody inAD: Relationship to aphasic deficits and emotionalbehaviors. Neurology, 57, 1474–1481.
Testa, J. A., Ivnik, R. J., Boeve, B., Petersen, R. C.,Pankratz, V. S., Knopman, D., et al. (2004).Confrontation naming does not add incrementaldiagnostic utility in MCI and Alzheimer’s disease.Journal of the International Neuropsychological Soci-ety, 10, 504–512.
Thompson, S. A., Graham, K. S., Patterson, K.,Sahakian, B. J., & Hodges, J. R. (2002). Is knowledgeof famous people disproportionately impaired inpatients with early and questionable Alzheimer’sdisease? Neuropsychology, 16, 344–358.
Tian, J., Bucks, R. S., Haworth, J., & Wilcock, G.(2003). Neuropsychological prediction of conversionto dementia: Statistically significant but not yet clini-cally useful. Journal of Neurology, Neurosurgery andPsychiatry, 74, 433–438.
Tierney, M. C., Szalai, J. P., Snow, W. G., Fisher, R. H.,Nores, A., Nadon, G., et al. (1996). Prediction ofprobable Alzheimer’s disease in memory-impairedpatients: A prospective longitudinal study. Neurol-ogy, 46, 661–665.
Touchon, J., & Ritchie, K. (1999). Prodromal cognitivedisorder in Alzheimer’s disease. International Journalof Geriatric Psychiatry, 14, 556–563.
Traykov, L., Baudic, S., Thibaudet, M.-C., Rigaud, A.-S.,Smagghe, A., & Boller, F. (2002). Neuropsychologi-cal deficit in early subcortical vascular dementia:Comparison to Alzheimer’s disease. Dementia andGeriatric Cognitive Disorders, 14, 26–32.
Vandenberghe, R. R., Vandenbulcke, M., Weintraub, S.,Johnson, N., Porke, K., Thompson, C. K., et al.(2005). Paradoxical features of word finding diffi-culty in primary progressive aphasia. Annals of Neu-rology, 57, 204–209.
Vandenbulcke, M., Peeters, R., Dupont, P., Van Hecke, P.,& Vandenberghe, R. (2007). Word reading and poste-rior temporal dysfunction in amnestic mild cognitiveimpairment. Cerebral Cortex, 17, 542–551.
Venneri, A., Forbes-McKay, K. E., & Shanks, M. F.(2005). Impoverishment of spontaneous language andthe prediction of Alzheimer’s disease. Brain, 128, E27.
Visser, P. J., Sheltens, P., Verhey, F. R. J., Schmand, B.,Launer, L. J., Jolles, J., et al. (1999). Medial temporallobe atrophy and memory dysfunction as predictors
for dementia in subjects with mild cognitive impair-ment. Journal of Neurology, 246, 477–485.
Vogel, A., Gade, A., Stokholm, J., & Waldemar, G.(2005). Semantic memory impairment in the earliestphases of Alzheimer’s disease. Dementia and GeriatricCognitive Disorders, 19, 75–81.
Vuorinen, E., Laine, M., & Rinne, J. (2000). Commonpattern of language impairment in vascular dementiaand in Alzheimer disease. Alzheimer Disease andAssociated Disorders, 14, 81–86.
Wallin, A., Edman, A., Blennow, K., Gottfries, C. G.,Karlsson, I., Regland, B., et al. (1996). Stepwise com-parative status analysis (STEP): A tool for identifica-tion of regional brain syndromes in dementia. Journalof Geriatric Psychiatry and Neurology, 9, 185–199.
Wang, P. N., Lirng, J. F., Lin, K. N., Chang, F. C., &Liu, H. C. (2006). Prediction of Alzheimer’s disease inmild cognitive impairment: A prospective study inTaiwan. Neurobiology of Aging, 27, 1797–1806.
Warrington, E. K., McKenna, P., & Orpwood, L.(1998). Single word comprehension: A concrete andabstract word synonym test. NeuropsychologicalRehabilitation, 8, 143–154.
Wechsler, D. (1955). Wechsler Adult Intelligence Scale.Manual. New York: Psychological Corporation.
Wechsler, D. (1974). Wechsler Intelligence Scalefor Children–Revised. New York: PsychologicalCorporation.
Welland, R. J., Lubinski, R., & Higginbotham, D. J.(2002). Discourse comprehension test performance ofelders with dementia of the Alzheimer type. Journal ofSpeech, Language and Hearing Research, 45, 1175–1187.
Werner, P., Rosenblum, S., Bar-On, G., Heinik, J., &Korczyn, A. (2006). Handwriting process variablesdiscriminating between mild Alzheimer’s disease andmild cognitive impairment. Journal of Gerontology:Psychological Sciences, 61B, 228–236.
Whatmough, C., Chertkow, H., Murtha, S.,Templeman, D., Babins, L., & Kelner, N. (2003).The semantic category effect increases with worsen-ing anomia in Alzheimer’s type dementia. Brain andLanguage, 84, 134–147.
Whitaker, H. (1976). A case of isolation of languagefunction. In H. Whitaker & H. A. Whitaker (Eds.),Studies in neurolinguistics. New York: Academic Press.
Williams, B. W., Mack, W. J., & Henderson, V. (1989).Boston Naming Test in Alzheimer’s disease. Neu-ropsychologia, 27, 1073–1079.
Winblad, B., Palmer, K., Kivipelto, M., Jelic, V.,Fratiglioni, L., Wahlund, L. O., et al. (2004). Mildcognitive impairment—beyond controversies,towards a consensus: Report of the InternationalWorking Group on Mild Cognitive Impairment.Journal of Internal Medicine, 256, 240–246.
Zaudig, M. (1992). A new systematic method ofmeasurement and diagnosis of “mild cognitiveimpairment” and dementia according to ICD-10 andDSM-III-R criteria. International Psychogeriatrics,4(Suppl. 2), 203–219.
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009
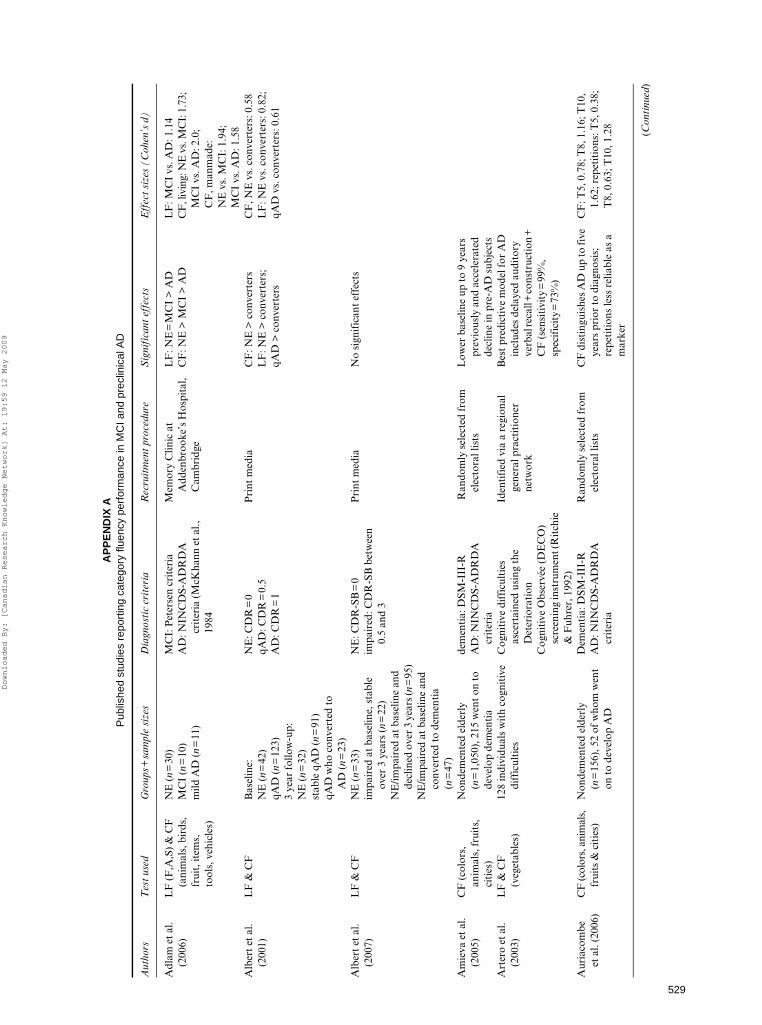
529
AP
PE
ND
IX A
P
ublis
hed
stud
ies
repo
rtin
g ca
tego
ry fl
uenc
y pe
rfor
man
ce in
MC
I and
pre
clin
ical
AD
Aut
hors
Tes
t us
edG
roup
s+sa
mpl
e si
zes
Dia
gnos
tic
crit
eria
Rec
ruit
men
t pr
oced
ure
Sig
nifi
cant
eff
ects
Eff
ect
size
s (C
ohen
’s d
)
Adl
am e
t al
. (2
006)
LF
(F
,A,S
) &
CF
(a
nim
als,
bir
ds,
frui
t, it
ems,
to
ols,
veh
icle
s)
NE
(n
=30
) M
CI
(n=
10)
mild
AD
(n
=11
)
MC
I: P
eter
sen
crit
eria
A
D: N
INC
DS-
AD
RD
A
crit
eria
(M
cKha
nn e
t al
., 19
84
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
Hos
pita
l, C
ambr
idge
LF
: NE
=M
CI
> A
DC
F: N
E >
MC
I >
AD
LF
: MC
I vs
. AD
: 1.1
4C
F, l
ivin
g: N
E v
s. M
CI:
1.7
3;
MC
I vs
. AD
: 2.0
; C
F, m
anm
ade:
N
E v
s. M
CI:
1.9
4;
MC
I vs
. AD
: 1.5
8A
lber
t et
al.
(200
1)L
F &
CF
Bas
elin
e:
NE
: CD
R=
0P
rint
med
iaC
F: N
E >
con
vert
ers
LF
: NE
> c
onve
rter
s;
qAD
> c
onve
rter
s
CF
, NE
vs.
con
vert
ers:
0.5
8L
F: N
E v
s. c
onve
rter
s: 0
.82;
qA
D v
s. c
onve
rter
s: 0
.61
NE
(n
=42
)qA
D: C
DR
=0.
5qA
D (
n=
123)
A
D: C
DR
=1
3 ye
ar f
ollo
w-u
p:N
E (
n=
32)
stab
le q
AD
(n
=91
)qA
D w
ho c
onve
rted
to
AD
(n
=23
)A
lber
t et
al.
(200
7)L
F &
CF
NE
(n
=33
) N
E: C
DR
-SB
=0
Pri
nt m
edia
No
sign
ific
ant
effe
cts
impa
ired
at
base
line,
sta
ble
over
3 y
ears
(n
=22
)im
pair
ed: C
DR
-SB
bet
wee
n 0.
5 an
d 3
NE
/impa
ired
at
base
line
and
decl
ined
ove
r 3
year
s (n=
95)
NE
/impa
ired
at
base
line
and
conv
erte
d to
dem
enti
a (n
=47
)A
mie
va e
t al
. (2
005)
CF
(co
lors
, an
imal
s, f
ruit
s,
citi
es)
Non
dem
ente
d el
derl
y (n
=1,
050)
, 215
wen
t on
to
deve
lop
dem
enti
a
dem
enti
a: D
SM-I
II-R
Ran
dom
ly s
elec
ted
from
el
ecto
ral l
ists
Low
er b
asel
ine
up t
o 9
year
s pr
evio
usly
and
acc
eler
ated
de
clin
e in
pre
-AD
sub
ject
sA
D: N
INC
DS-
AD
RD
A
crit
eria
Art
ero
et a
l. (2
003)
LF
& C
F
(veg
etab
les)
128
indi
vidu
als
wit
h co
gnit
ive
diff
icul
ties
Cog
niti
ve d
iffi
cult
ies
asce
rtai
ned
usin
g th
e D
eter
iora
tion
Iden
tifi
ed v
ia a
reg
iona
l ge
nera
l pra
ctit
ione
r ne
twor
k
Bes
t pr
edic
tive
mod
el f
or A
D
incl
udes
del
ayed
aud
itor
y ve
rbal
reca
ll+
cons
truc
tion
+
CF
(se
nsit
ivit
y=
99%
, sp
ecif
icit
y=
73%
)C
ogni
tive
Obs
ervé
e (D
EC
O)
scre
enin
g in
stru
men
t (R
itch
ie
& F
uhre
r, 1
992)
Aur
iaco
mbe
et
al.
(200
6)C
F (c
olor
s, a
nim
als,
fr
uits
& c
itie
s)N
onde
men
ted
elde
rly
(n=
156)
, 52
of w
hom
wen
t on
to
deve
lop
AD
Dem
enti
a: D
SM-I
II-R
Ran
dom
ly s
elec
ted
from
el
ecto
ral l
ists
CF
dis
ting
uish
es A
D u
p to
five
ye
ars
prio
r to
dia
gnos
is;
repe
titi
ons
less
rel
iabl
e as
a
mar
ker
CF
: T5,
0.7
8; T
8, 1
.16;
T10
, 1.
62; r
epet
itio
ns: T
5, 0
.38;
T
8, 0
.63;
T10
, 1.2
8A
D: N
INC
DS-
AD
RD
A
crit
eria
(Con
tinu
ed)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

530
AP
PE
ND
IX A
(C
ontin
ued)
Aut
hors
Tes
t us
edG
roup
s+sa
mpl
e si
zes
Dia
gnos
tic
crit
eria
use
dR
ecru
itm
ent
proc
edur
eS
igni
fica
nt e
ffec
tsE
ffec
t si
zes
(Coh
en’s
d)
Bäc
kman
et
al.
(200
2)C
F (
item
s at
gr
ocer
y st
ore)
&
LF
(N
,S)
Non
dem
ente
d el
derl
y (n
=33
7), 6
1 of
who
m w
ent
on to
dev
elop
dem
enti
a an
d 69
of
who
m w
ent
on t
o di
e
Dem
enti
a: D
SM-I
II-R
All
inha
bita
nts
of
Kun
gsho
lmen
, Sw
eden
, ag
ed ≥
75 o
n O
ctob
er 1
st,
1987
invi
ted
to
part
icip
ate
Non
conv
erte
rs >
con
vert
ers
on a
ll m
easu
res
CF
: 0.8
8L
F: 0
.82
Bei
nhof
f et
al.
(200
5)C
F (
anim
als)
NE
(n
=57
)M
CI
(n=
48)
AD
(n
=66
)M
D (
n=
61)
MC
I: P
eter
sen
crit
eria
AD
: NIN
CD
S-A
DR
DA
cr
iter
iaM
D: D
SM-I
V c
rite
ria.
Mem
ory
clin
icA
D <
MC
I=M
D <
NE
NE
vs.
MC
I: 1
.04
MC
I vs
. AD
: 1.0
2
Ben
nett
et
al.
(200
2)C
F (
part
of
sum
mar
y m
easu
re
of s
eman
tic
mem
ory)
NE
(n
=58
7);
MC
I (n
=21
1)C
ogni
tive
impa
irm
ent,
but
doe
s no
t mee
t acc
epte
d cr
iter
ia fo
r de
men
tia
Cat
holic
cle
rgy
who
agr
eed
to p
arti
cipa
teSe
man
tic
mem
ory
low
er a
t ba
selin
e, d
eclin
ed m
ore
than
tw
ice
as f
ast
in M
CIs
CF
: 0.8
1
Bla
ckw
ell e
t al
. (2
004)
CF
(an
imal
s, f
ruit
, ho
useh
old
item
s)Su
bjec
tive
/obj
ecti
ve m
emor
y lo
ss (
n=
43),
11
of w
hom
de
velo
ped
AD
wit
hin
32
mon
ths
Nor
mal
per
form
ance
on
test
s of
lang
uage
and
vis
uosp
atia
l fu
ncti
on, p
rese
rved
AD
L,
CD
R=
0.5
Mem
ory
clin
icN
onco
nver
ters
> c
onve
rter
s1.
37
Boz
oki e
t al
. (2
001)
LF
(C
,F,L
)IM
I (n
=48
)P
eter
sen
crit
eria
+
neur
opsy
chol
ogic
al e
vide
nce
(dia
gnos
tic
crit
eria
and
cog
-ni
tive
mea
sure
s fo
r cl
inic
al
chan
ge b
ased
on
thos
e pr
o-po
sed
for
AA
MI)
Mic
higa
n A
lzhe
imer
’s
Dis
ease
Res
earc
h C
ente
rIm
pair
men
t in
≥2
cogn
itiv
e te
sts+
mem
ory
=hi
gher
ris
k of
con
vers
ion
to A
D (
at
4-ye
ar f
ollo
w-u
p: m
emor
y im
pair
men
t on
ly: 2
4%
conv
ersi
on; m
emor
y im
pair
men
t+1
or m
ore
cogn
itiv
e do
mai
ns: 7
7%
conv
ersi
on; m
emor
y im
pair
men
t+2
or m
ore
cogn
itiv
e do
mai
ns: 1
00%
co
nver
sion
).B
scho
r et
al.
(200
1)L
F (
S) &
CF
(a
nim
als)
NE
(n
=40
)IC
D-1
0 cr
iter
ia (
Zau
dig,
199
2)M
emor
y cl
inic
, Dep
t. o
f G
eron
tolo
gy, F
reie
U
nive
rsit
ät B
erlin
NE
> M
CI
> m
ild A
D=
mod
/sev
AD
for
bot
h m
easu
res
CF
: NE
vs.
MC
I, 0
.59,
MC
I vs
. mild
AD
, 0.9
7L
F: N
E v
s. M
CI,
0.8
4, M
CI
vs. m
ild A
D, 0
.50
MC
I (n
=34
)m
ild A
D (
n=
21)
mod
erat
e to
sev
ere
AD
(n=
20)
Cac
capo
lo-V
an
Vlie
t et
al.
(200
3)
LF
(C
,F,L
) &
CF
(a
nim
als,
foo
d &
cl
othi
ng)
NE
(n
=23
0)Q
D: c
ogni
tive
impa
irm
ent
suff
icie
nt o
r cl
ose
to
suff
icie
nt f
or a
dia
gnos
is o
f de
men
tia;
no
func
tion
al
impa
irm
ent
AD
: NIN
CD
S-A
DR
DA
cr
iter
ia
Mem
ory
Dis
orde
rs C
ente
r/re
crui
ted
for
a st
udy
of
cont
rols
LF
: NE
=Q
D; Q
D=
mild
AD
; N
E >
mild
AD
> m
oder
ate
AD
> s
ever
e A
D >
ver
y se
vere
AD
CF
: NE
> Q
D >
mild
AD
>
mod
erat
e A
D >
sev
ere
AD
>
ver
y se
vere
AD
CF
: NE
vs.
QD
: 0.4
3; Q
D v
s.
mild
AD
: 0.4
9; m
ild A
D v
s.
mod
erat
e A
D: 0
.79;
m
oder
ate
AD
vs.
sev
ere
AD
: 0.7
1; s
ever
e A
D v
s.
very
sev
ere
AD
: 1.0
4
QD
(n
=15
5)m
ild A
D (
n=
244)
mod
erat
e A
D (
n=
480)
seve
re A
D (
n=
376)
very
sev
ere
AD
(n=
247)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

531
Che
n et
al.
(200
0)L
F &
CF
NE
(n
=48
3), w
ho r
emai
ned
non-
dem
ente
d ov
er 1
0-ye
ar
follo
w-u
p
NIN
CD
S-A
DR
DA
cri
teri
aR
ando
mly
sel
ecte
d fr
om
vote
r re
gist
rati
on li
sts
NE
> in
cide
nt A
D fo
r bo
th L
F
and
CF
; how
ever
, nei
ther
w
as a
bet
ter
pred
icto
r of
in
cide
nt d
emen
tia
than
the
M
MSE
LF
: 0.5
0C
F: 0
.83
Con
vert
ers
to A
D 1
.5 y
ears
af
ter
test
ing
(n=
120)
Che
n et
al.
(200
1)L
F &
CF
NE
(n
=55
1), 6
8 of
who
m
wen
t on
to
deve
lop
AD
NIN
CD
S-A
DR
DA
cri
teri
aR
ando
mly
sel
ecte
d fr
om
vote
r re
gist
rati
on li
sts
Dec
line
in C
F: n
onco
nver
ters
<
con
vert
ers
decl
ine
in L
F:
nonc
onve
rter
s =
con
vert
ers
CF
: 0.2
9
Col
lie e
t al
. (2
002)
CF
Eld
erly
adu
lts
(n=
174)
, 23
of w
hom
wer
e im
pair
ed o
n 3
cons
ecut
ive
asse
ssm
ents
CE
RA
D b
atte
ry (
Mor
ris
et a
l.,
1988
)R
ecru
ited
fro
m a
n on
goin
g st
udy
on a
ging
at
an
inde
pend
ent
rese
arch
in
stit
ute
in M
elbo
urne
, A
ustr
alia
NE
=M
CI
Coo
per
et a
l. (2
004)
CF
(an
imal
s)N
E (
n=
23)
MC
I-A
: Pet
erse
n cr
iter
iaC
linic
for
Alz
heim
er’s
D
isea
se a
nd R
elat
ed
Dis
orde
rs, U
nive
rsit
y of
T
exas
Sou
thw
este
rn
Med
ical
Cen
ter,
Dal
las
Onl
y N
E s
how
ed s
igni
fica
nt
impr
ovem
ent
acro
ss
repe
ated
adm
inis
trat
ions
(2
4 to
96
hour
s ap
art)
MC
I-A
(n
=23
)A
D (
n=
23)
Cro
ot e
t al
. (1
999)
CF
(liv
ing,
4
cate
gori
es &
m
anm
ade,
4
cate
gori
es)
NE
(n
=46
)N
INC
DS-
AD
RD
A c
rite
ria
min
imal
: MM
SE=
24–3
0m
ild: M
MSE
=18
–23
mod
erat
e: M
MSE
=2–
17
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
Hos
pita
l, C
ambr
idge
p-va
lue
not
repo
rted
min
imal
AD
(n
=16
)m
ild A
D (
n=
16)
mod
erat
e A
D (
n=
14)
Cun
je e
t al
. (2
007)
CF
(an
imal
s, c
itie
s &
tow
ns, n
ames
, or
fru
its
&
vege
tabl
es)
NE
(n
=46
)M
CI
(n=
45)
dem
enti
a ( n
=55
)
Subj
ecti
ve m
emor
y lo
ss w
ith
corr
obor
atio
n by
a f
amily
m
embe
r or
frie
nd, n
o de
fici
ts
in A
DL
, no
dem
enti
a
Fiv
e ou
tpat
ient
clin
ics
in
sout
hern
Ont
ario
, and
a
loca
l nur
sing
hom
e
No
diff
eren
ce in
sen
siti
vity
to
MC
I an
d de
men
tia
betw
een
the
four
ver
sion
s; a
ll di
scri
min
ated
bet
wee
n A
D,
MC
I &
NE
par
tici
pant
s;
60-s
econ
d sc
ore
mor
e se
nsit
ive
than
30-
seco
nd
scor
e.
Ani
mal
s, 0
–30
s: 2
.3, 3
1–60
s:
1.5,
0–6
0 s:
3.2
Cit
ies
& t
owns
, 0–3
0 s:
1.9
, 31
–60
s: 1
.5, 0
–60
s: 2
.7
Fru
its
& v
eget
able
s, 0
–30
s:
1.5,
31–
60 s
: 1.3
, 0–6
0 s:
2.5
Nam
es, 0
–30
s: 2
.3, 3
1–60
s:
1.5,
0–6
0 s:
3.2
Dar
tigu
es e
t al
. (1
997)
CF
(co
lors
, an
imal
s, f
ruit
s,
citi
es)
Non
dem
ente
d el
derl
y (n
=2,
726)
, 59
of w
hom
de
velo
ped
AD
in 3
-yea
r fo
llow
-up
DSM
-III
-R c
rite
ria
Ran
dom
ly c
hose
n fr
om
elec
tora
l rol
ls in
Gir
onde
an
d D
ordo
gne,
Fra
nce
CF
was
an
inde
pend
ent
and
very
goo
d pr
edic
tor
of
dem
enti
a/A
D
de J
ager
et
al.
(200
3)C
F (
frui
ts &
ve
geta
bles
)N
E (
n=
51)
MC
I: P
eter
sen
crit
eria
AD
: NIN
CD
S-A
DR
DA
cr
iter
iaV
CI:
Hac
hins
ki c
rite
ria
VaD
: NIN
CD
DS/
AIR
EN
cr
iter
ia (
G. G
old
et a
l. 19
97)
Rec
ruit
ed f
rom
the
Oxf
ord
Pro
ject
To
Inve
stig
ate
Mem
ory
and
Age
ing
(OP
TIM
A)
stud
y
NE
> M
CI
> A
DC
VD
(V
aD+
VC
I) a
lso
exhi
bite
d de
fici
ts
NE
vs.
MC
I: 0
.74
MC
I vs
. AD
: 1.4
8N
E v
s. C
VD
: 1.3
2M
CI
(n=
29)
AD
(n
=60
)V
CI
(n=
8)V
aD (
n=
4)
(Con
tinu
ed)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

532
AP
PE
ND
IX A
(C
ontin
ued)
Aut
hors
Tes
t us
edG
roup
s+sa
mpl
e si
zes
Dia
gnos
tic
crit
eria
use
dR
ecru
itm
ent
proc
edur
eS
igni
fica
nt e
ffec
tsE
ffec
t si
zes
(Coh
en’s
d)
Dev
anan
d et
al.
(199
7)L
F &
CF
QD
(n
=62
), 2
6 of
who
m w
ent
on t
o de
velo
p de
men
tia
QD
: cog
niti
ve im
pair
men
t, f
all
betw
een
“nor
mal
” an
d “d
emen
tia”
cat
egor
ies
Mem
ory
Dis
orde
rs C
linic
Bas
elin
e pe
rfor
man
ce o
n C
F:
nonc
onve
rter
s >
con
vert
ers;
se
nsit
ivit
y=
59.3
%,
spec
ific
ity
=55
.6%
; P
PV
=57
.1%
, NP
V=
57.7
%
0.64
Dem
enti
a: D
SM-I
II
crit
eria
AD
: NIN
CD
S-A
DR
DA
cri
teri
a
Dev
anan
d et
al.
(200
6)C
FM
CI
(n=
23),
6 o
f w
hom
wen
t on
to
deve
lop
dem
enti
aA
ge ≥
40;
impa
irm
ent 6
mon
ths
to 1
0 ye
ars;
no
dem
enti
a;
MM
SE ≥
22;
obj
ecti
ve
mem
ory
impa
irm
ent
OR
su
bjec
tive
mem
ory
decl
ine
corr
obor
ated
by
info
rman
t;
+ve
sco
re o
n at
leas
t on
e of
th
e fi
rst
eigh
t it
ems
of t
he
mod
ifie
d B
less
ed F
unct
iona
l A
ctiv
ity
Scal
e (B
less
ed e
t al
., 19
68).
Mem
ory
Dis
orde
rs C
linic
CF
did
not
pre
dict
AD
Dud
as e
t al
. (2
005)
LF
(F
AS)
& C
F
(liv
ing
&
man
mad
e)
NE
(n
=29
)P
eter
sen
crit
eria
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
Hos
pita
l, C
ambr
idge
CF
: NE
> M
CI
> A
DL
F: n
o si
gnif
ican
t ef
fect
sC
F li
ving
: NE
vs.
MC
I, 1
.75;
M
CI
vs. A
D, 1
.16
CF
man
mad
e: N
E v
s. M
CI,
1.
05; M
CI
vs. A
D, 1
.42
MC
I (n
=24
)A
D (
n=
22)
Dw
olat
zky
et a
l. (2
003)
LF
(F
,A,S
) &
CF
(a
nim
als)
NE
(n
=15
)P
eter
sen
crit
eria
Mem
ory
clin
ics
NE
> M
CI
on a
ll te
sts;
bes
t di
scri
min
ant
was
LF
(F
,S)
MC
I (n
=20
)A
D (
n=
19)
Fab
rigo
ule
et a
l. (1
998)
CF
(co
lors
, an
imal
s, f
ruit
s,
citi
es)
nond
emen
ted
elde
rly
(n=
1,15
9), 2
5 of
who
m
deve
lope
d de
men
tia
at
2 ye
ars
(AD
, n=
16)
NIN
CD
S-A
DR
DA
cri
teri
aIn
divi
dual
s ra
ndom
ly
sele
cted
fro
m e
lect
oral
lis
ts
Non
-con
vert
ers
> C
onve
rter
s1.
58
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

533
Fill
enba
um
et a
l. (2
005)
CF
(an
imal
s)N
E: n
=20
1 (S
eatt
le),
n=
120
(Haw
aii)
CD
R=
0.5:
n=
33 (
Seat
tle)
, n
=65
(H
awai
i)C
DR
=1:
n=
37 (
Seat
tle)
, n
=97
(H
awai
i)C
DR
=2:
n=
33 (
Seat
tle)
, n
=55
(H
awai
i)C
DR
=3,
4,5:
n=
46 (
Seat
tle)
, n
=81
(H
awai
i)
CD
R s
core
Seat
tle:
Kin
g C
ount
y te
leph
one
dire
ctor
ies,
H
ealt
h C
are
Fin
anci
ng
Adm
inis
trat
ion
(now
C
MS)
Med
icar
e re
cipi
ent
lists
, Jap
anes
e-A
mer
ican
or
gani
zati
onal
list
s, a
nd
wor
d of
mou
thH
awai
i: Ja
pane
se-A
mer
ican
m
en b
orn
1900
–191
9,
livin
g in
Oah
u in
196
5,
who
had
bee
n on
the
W
orld
War
II
Sele
ctiv
e Se
rvic
e R
egis
trat
ion
file
CD
R 0
< C
DR
0.5
in b
oth
popu
lati
ons
Fle
ishe
r et
al.
(200
7)C
F21
2 M
CI-
A in
divi
dual
s w
ho
prog
ress
ed t
o A
D w
ithi
n 36
mon
ths
Pet
erse
n cr
iter
iaP
arti
cipa
nts
in a
36-
mon
th
rand
omiz
ed d
rug
tria
lC
F w
as n
ot a
mea
sure
in t
he
mod
el t
hat
was
mos
t pr
edic
tive
of
prog
ress
ion
to A
DF
orbe
s-M
cKay
et
al.
(200
5)C
F (
anim
als
and
frui
t)N
E (
n=
40)
min
imal
AD
(n
=34
)m
ild A
D (
n=
39)
mod
erat
e A
D (
n=
23)
AD
: NIN
CD
S-A
DR
DA
cr
iter
iam
inim
al: M
MSE
24–
29m
ild: M
MSE
19–
23m
oder
ate:
MM
SE 1
3–18
Out
pati
ent
diag
nost
ic a
nd
man
agem
ent
clin
ic in
A
berd
een
AD
> N
E o
n nu
mbe
r of
wor
dsIt
ems
wer
e of
hig
her
freq
uenc
y, s
hort
er, m
ore
typi
cal a
nd h
ad e
arlie
r A
oA
than
con
trol
s’ it
ems
Num
ber
of w
ords
, NE
vs.
m
inim
al A
D: 1
.78;
min
imal
vs
. mild
: 0.9
6; m
ild v
s.
mod
erat
e: 0
.29
AoA
, NE
vs.
min
imal
: 1.8
0G
alvi
n et
al.
(200
5)w
ord
flue
ncy
(typ
e un
spec
ifie
d)N
E (
n=
80)
who
eve
ntua
lly
cam
e to
aut
opsy
CD
R s
core
Indi
vidu
als
enro
lled
in
long
itud
inal
stu
dies
of
heal
thy
agin
g an
d de
men
tia
Bas
elin
e: d
emen
tia
=no
de
men
tia
1.02
Fin
al e
xam
inat
ion:
no
dem
enti
a >
dem
enti
aG
alto
n et
al.
(200
5)C
F (
anim
als,
fru
it,
hous
ehol
d it
ems)
QD
(n
=31
), 1
1 of
who
m h
ad
conv
erte
d to
AD
at
24.2
m
onth
s
QD
: sub
ject
ive
mem
ory
impa
irm
ent,
cor
robo
rate
d by
an
info
rman
t; n
orm
al A
DL
; M
MSE
≥ 2
3; C
DR
=0.
5.A
D: N
INC
DS-
AD
RD
A
crit
eria
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
Hos
pita
l, C
ambr
idge
nonc
onve
rter
s >
con
vert
ers
>
AD
nonc
onve
rter
s vs
. con
vert
ers:
1.
11
AD
(n
=19
)
Ges
lani
et
al.
(200
5)L
F (
P,R
,W)
& C
F
(ani
mal
s)M
CI
(n=
57)
Pet
erse
n cr
iter
ia +
co
rrob
orat
ion
of m
emor
y de
fici
t by
phy
sici
an
Ref
erre
d by
pri
mar
y-ca
re
phys
icia
nsN
o co
mpa
riso
n gr
oup
Gol
dman
et
al.
(200
1)L
F (
S,P
)N
E (
n=
9) p
recl
inic
al A
D
(n=
5)C
linic
ally
non
dem
ente
d, b
ut
neur
itic
and
dif
fuse
pla
ques
th
roug
hout
the
neo
cort
ex
(aut
opsy
fin
ding
s)
Was
hing
ton
Uni
vers
ity’
s A
lzhe
imer
’s d
isea
se
Res
earc
h C
entr
e
No
grou
p di
ffer
ence
s
AD
(n
=10
)
(Con
tinu
ed)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009
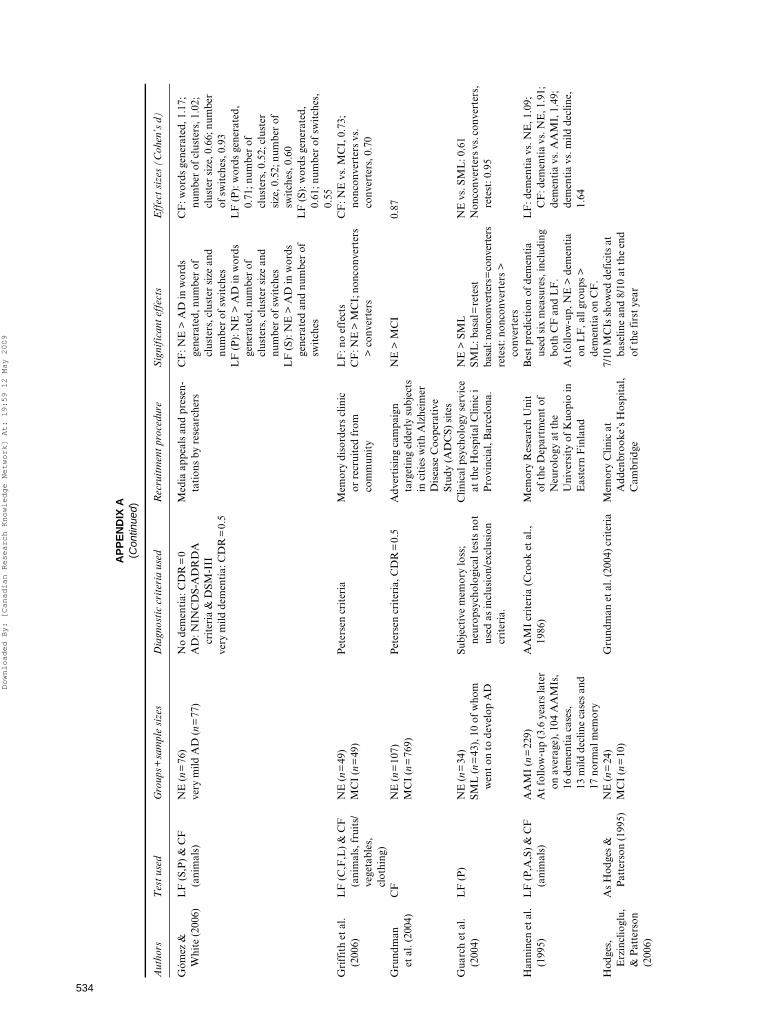
534
AP
PE
ND
IX A
(C
ontin
ued)
Aut
hors
Tes
t us
edG
roup
s+sa
mpl
e si
zes
Dia
gnos
tic
crit
eria
use
dR
ecru
itm
ent
proc
edur
eS
igni
fica
nt e
ffec
tsE
ffec
t si
zes
(Coh
en’s
d)
Góm
ez &
W
hite
(20
06)
LF
(S,
P)
& C
F
(ani
mal
s)N
E (
n=
76)
very
mild
AD
(n
=77
)N
o de
men
tia:
CD
R=
0A
D: N
INC
DS-
AD
RD
A
crit
eria
& D
SM-I
IIve
ry m
ild d
emen
tia:
CD
R=
0.5
Med
ia a
ppea
ls a
nd p
rese
n-ta
tion
s by
res
earc
hers
CF
: NE
> A
D in
wor
ds
gene
rate
d, n
umbe
r of
cl
uste
rs, c
lust
er s
ize
and
num
ber
of s
wit
ches
CF
: wor
ds g
ener
ated
, 1.1
7;
num
ber
of c
lust
ers,
1.0
2;
clus
ter
size
, 0.6
6; n
umbe
r of
sw
itch
es, 0
.93
LF
(P
): N
E >
AD
in w
ords
ge
nera
ted,
num
ber
of
clus
ters
, clu
ster
siz
e an
d nu
mbe
r of
sw
itch
esL
F (
S): N
E >
AD
in w
ords
ge
nera
ted
and
num
ber
of
swit
ches
LF
(P
): w
ords
gen
erat
ed,
0.71
; num
ber
of
clus
ters
, 0.5
2; c
lust
er
size
, 0.5
2; n
umbe
r of
sw
itch
es, 0
.60
LF
(S)
: wor
ds g
ener
ated
, 0.
61; n
umbe
r of
sw
itch
es,
0.55
Gri
ffit
h et
al.
(200
6)L
F (
C,F
,L)
& C
F
(ani
mal
s, f
ruit
s/
vege
tabl
es,
clot
hing
)
NE
(n
=49
)P
eter
sen
crit
eria
Mem
ory
diso
rder
s cl
inic
or
rec
ruit
ed f
rom
co
mm
unit
y
LF
: no
effe
cts
CF
: NE
vs.
MC
I, 0
.73;
no
ncon
vert
ers
vs.
conv
erte
rs, 0
.70
MC
I (n
=49
)C
F: N
E >
MC
I; n
onco
nver
ters
>
con
vert
ers
Gru
ndm
an
et a
l. (2
004)
CF
NE
(n
=10
7)P
eter
sen
crit
eria
, CD
R=
0.5
Adv
erti
sing
cam
paig
n ta
rget
ing
elde
rly
subj
ects
in
cit
ies
wit
h A
lzhe
imer
D
isea
se C
oope
rati
ve
Stud
y (A
DC
S) s
ites
NE
> M
CI
0.87
MC
I (n
=76
9)
Gua
rch
et a
l. (2
004)
LF
(P
)N
E (
n=
34)
SML
(n
=43
), 1
0 of
who
m
wen
t on
to
deve
lop
AD
Subj
ecti
ve m
emor
y lo
ss;
neur
opsy
chol
ogic
al t
ests
not
us
ed a
s in
clus
ion/
excl
usio
n cr
iter
ia.
Clin
ical
psy
chol
ogy
serv
ice
at t
he H
ospi
tal C
linic
i P
rovi
ncia
l, B
arce
lona
.
NE
> S
ML
NE
vs.
SM
L: 0
.61
Non
conv
erte
rs v
s. c
onve
rter
s,
rete
st: 0
.95
SML
: bas
al=
rete
stba
sal:
nonc
onve
rter
s=co
nver
ters
rete
st: n
onco
nver
ters
>
conv
erte
rsH
anni
nen
et a
l. (1
995)
LF
(P
,A,S
) &
CF
(a
nim
als)
AA
MI
(n=
229)
At
follo
w-u
p (3
.6 y
ears
late
r on
ave
rage
), 1
04 A
AM
Is,
16 d
emen
tia
case
s,
13 m
ild d
eclin
e ca
ses
and
17 n
orm
al m
emor
y
AA
MI
crit
eria
(C
rook
et
al.,
1986
)M
emor
y R
esea
rch
Uni
t of
the
Dep
artm
ent
of
Neu
rolo
gy a
t th
e U
nive
rsit
y of
Kuo
pio
in
Eas
tern
Fin
land
Bes
t pr
edic
tion
of
dem
enti
a us
ed s
ix m
easu
res,
incl
udin
g bo
th C
F a
nd L
F.
LF
: dem
enti
a vs
. NE
, 1.0
9;
CF
: dem
enti
a vs
. NE
, 1.9
1;
dem
enti
a vs
. AA
MI,
1.4
9;
dem
enti
a vs
. mild
dec
line,
1.
64A
t fo
llow
-up,
NE
> d
emen
tia
on L
F, a
ll gr
oups
>
dem
enti
a on
CF
.H
odge
s,
Erz
incl
iogl
u,
& P
atte
rson
(2
006)
As
Hod
ges
&
Pat
ters
on (
1995
)N
E (
n=
24)
Gru
ndm
an e
t al
. (20
04)
crit
eria
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
Hos
pita
l, C
ambr
idge
7/10
MC
Is s
how
ed d
efic
its
at
base
line
and
8/10
at
the
end
of t
he f
irst
yea
rM
CI
(n=
10)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

535
Hod
ges
&
Pat
ters
on
(199
5)
CF
for
six
mai
n ca
tego
ries
[lan
d an
imal
s, s
ea
crea
ture
s, b
irds
, ho
useh
old
item
s,
vehi
cles
, mus
ical
in
stru
men
ts] a
nd
two
subc
ateg
orie
s [b
reed
s of
dog
, ty
pes
of b
oat]
NE
(n
=24
)N
INC
DS-
AD
RD
A c
rite
ria
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
Hos
pita
l, C
ambr
idge
NE
> m
inim
al >
mild
>
mod
erat
e on
all
subt
ests
Liv
ing:
NE
vs.
min
imal
A
D, 2
.0;
min
imal
AD
vs.
mild
AD
, 0.7
; m
ild A
D v
s. m
oder
ate
AD
, 1.
37M
an-m
ade:
NE
vs.
min
imal
A
D, 2
.34;
m
inim
al A
D v
s. m
ild A
D, 0
.47;
mild
AD
vs.
mod
erat
e A
D,
1.94
min
imal
AD
(n
=17
)m
ild A
D (
n=
52)
mod
erat
e A
D (
n=
18)
Jaco
bs e
t al
. (1
995)
LF
& C
FN
onde
men
ted
elde
rly
(n=
443)
, 41
of w
hom
had
de
velo
ped
AD
at
follo
w-u
p (o
n av
erag
e 2.
05 y
ears
late
r)
NIN
CD
S-A
DR
DA
cri
teri
aN
orth
Man
hatt
an
Agi
ng P
roje
ct, a
co
mm
unit
y-ba
sed,
ep
idem
iolo
gic
stud
y of
de
men
tia
in n
orth
ern
Man
hatt
an, N
Y.
No
sign
ific
ant
effe
cts
repo
rted
Jone
s et
al.
(200
6)L
F (
N,S
) &
CF
(g
roce
ry s
tore
it
ems)
NE
(n
=26
7)D
SM-I
II-R
and
Hac
hins
ki
Isch
emic
Sca
le (
Hac
hins
ki
et a
l., 1
974)
.
All
inha
bita
nts
of
Kun
gsho
lmen
, Sw
eden
, ag
ed ≥
75 o
n O
ctob
er 1
st,
1987
invi
ted
to
part
icip
ate
LF
: pre
clin
ical
AD
=
prec
linic
al V
aDC
F: p
recl
inic
al A
D <
pr
eclin
ical
VaD
LF
: AD
vs.
NE
, 0.5
6pr
eclin
ical
AD
(n
=66
)C
F: A
D v
s. V
aD, 0
.52;
A
D v
s. N
E, 0
.65
prec
linic
al V
aD (
n=
20)
Jorm
et
al.
(200
5)C
F (
4-le
gged
an
imal
s)Ja
pane
se-A
mer
ican
men
age
d 71
–93
(n=
1611
), 5
2 of
w
hom
wen
t on
to
deve
lop
dem
enti
a
DSM
III
-RR
ecru
ited
fro
m p
opul
atio
nP
redi
cted
inci
dent
dem
enti
a up
to
3 y
ears
bef
ore
onse
t bu
t no
t 3–
6 ye
ars
befo
re o
nset
.
0.65
Kal
be e
t al
. (2
004)
CF
(su
perm
arke
t)N
E (
n=
145)
MC
I (n
=97
)A
D (
n=
121)
NE
: CD
R=
0M
CI:
Pet
erse
n cr
iter
iaA
D: N
INC
DS-
AD
RD
A
crit
eria
; CD
R=
1 or
2
Mem
ory
Clin
icN
E >
MC
I >
AD
NE
<60
yea
rs v
s. N
E ≥
60
year
s: 0
.30
NE
≥60
yea
rs v
s. M
CI:
1.2
5M
CI
vs. A
D (
MM
SE≥2
1):
0.99
AD
(M
MSE
≥21)
vs.
AD
(M
MSE
<21
): 0
.61
Kar
rasc
h et
al.
(200
5)C
FN
E (
n=
15)
Pet
erse
n cr
iter
iaC
omm
unit
y so
urce
sN
E>
AD
, not
MC
IM
CI
(n=
15)
AD
(n
=15
)L
am e
t al
. (2
006)
CF
(an
imal
s,
frui
t, v
eget
able
s)
– 30
-sec
ond
and
60-s
econ
d sc
ores
NE
(n
=11
8)Q
D (
n=
150)
mild
AD
(n
=63
)
NE
: CD
R=
0C
omm
unit
y so
cial
cen
tres
an
d re
side
ntia
l hos
tels
for
the
elde
rly
in H
ong
Kon
g
NE
> Q
D >
mild
AD
for
bot
h 30
-sec
ond
and
60-s
econ
d sc
ores
30-s
econ
d: N
E v
s. Q
D, 1
.07;
Q
D v
s. A
D, 1
.10
60-s
econ
d: N
E v
s. Q
D, 1
.11;
Q
D v
s. A
D, 1
.16
QD
: CD
R=
0.5
mild
AD
: CD
R=
1
(Con
tinu
ed)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009
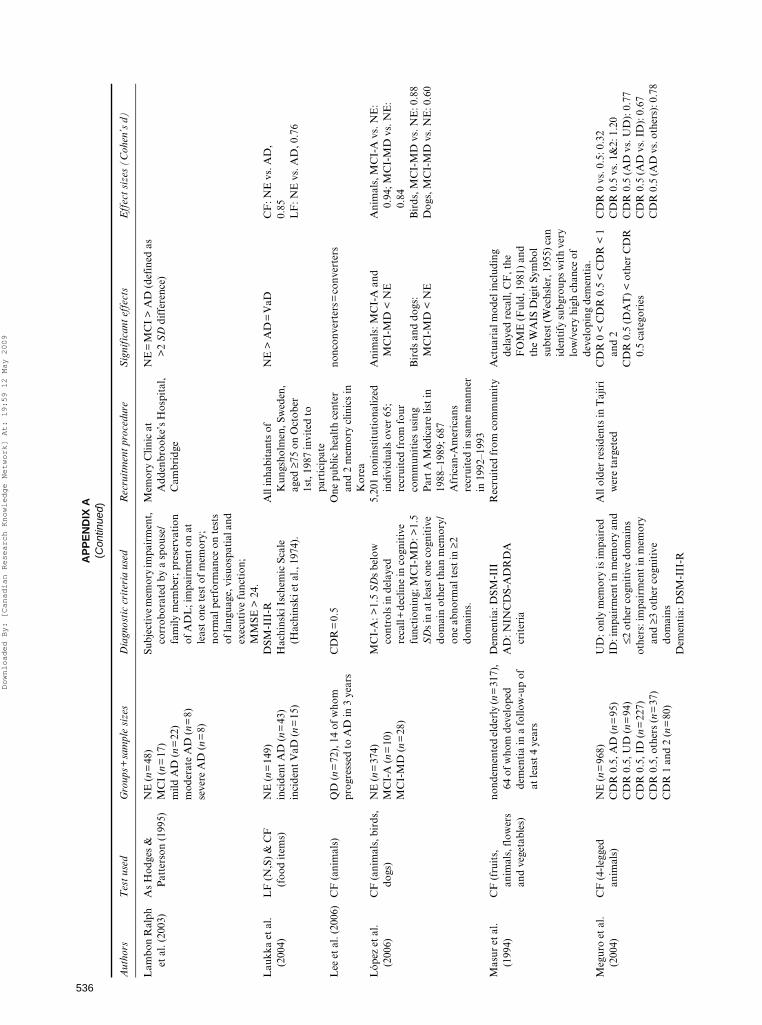
536
AP
PE
ND
IX A
(C
ontin
ued)
Aut
hors
Tes
t us
edG
roup
s+sa
mpl
e si
zes
Dia
gnos
tic
crit
eria
use
dR
ecru
itm
ent
proc
edur
eS
igni
fica
nt e
ffec
tsE
ffec
t si
zes
(Coh
en’s
d)
Lam
bon
Ral
ph
et a
l. (2
003)
As
Hod
ges
&
Pat
ters
on (
1995
)N
E (
n=
48)
Subj
ecti
ve m
emor
y im
pair
men
t,
corr
obor
ated
by
a sp
ouse
/fa
mily
mem
ber;
pre
serv
atio
n of
AD
L; i
mpa
irm
ent
on a
t le
ast
one
test
of
mem
ory;
no
rmal
per
form
ance
on
test
s of
lang
uage
, vis
uosp
atia
l and
ex
ecut
ive
func
tion
; M
MSE
> 2
4.
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
Hos
pita
l, C
ambr
idge
NE
=M
CI
> A
D (
defi
ned
as
>2
SD
dif
fere
nce)
MC
I (n
=17
)m
ild A
D (
n=
22)
mod
erat
e A
D (
n=
8)se
vere
AD
(n
=8)
Lau
kka
et a
l. (2
004)
LF
(N
,S)
& C
F
(foo
d it
ems)
NE
(n
=14
9)in
cide
nt A
D (
n=
43)
inci
dent
VaD
(n=
15)
DSM
-III
-RH
achi
nski
Isc
hem
ic S
cale
(H
achi
nski
et
al.,
1974
).
All
inha
bita
nts
of
Kun
gsho
lmen
, Sw
eden
, ag
ed ≥
75 o
n O
ctob
er
1st,
198
7 in
vite
d to
pa
rtic
ipat
e
NE
> A
D=
VaD
CF
: NE
vs.
AD
,0.
85L
F: N
E v
s. A
D, 0
.76
Lee
et
al. (
2006
)C
F (
anim
als)
QD
(n=
72),
14
of w
hom
pr
ogre
ssed
to
AD
in 3
yea
rsC
DR
=0.
5O
ne p
ublic
hea
lth
cent
er
and
2 m
emor
y cl
inic
s in
K
orea
nonc
onve
rter
s=co
nver
ters
Lóp
ez e
t al
. (2
006)
CF
(an
imal
s, b
irds
, do
gs)
NE
(n
=37
4)M
CI-
A (
n=
10)
MC
I-M
D (
n=
28)
MC
I-A
: >1.
5 S
Ds
belo
w
cont
rols
in d
elay
ed
reca
ll+
decl
ine
in c
ogni
tive
fu
ncti
onin
g; M
CI-
MD
: >1.
5 S
Ds
in a
t le
ast
one
cogn
itiv
e do
mai
n ot
her
than
mem
ory/
one
abno
rmal
tes
t in
≥2
dom
ains
.
5,20
1 no
nins
titu
tion
aliz
ed
indi
vidu
als
over
65;
re
crui
ted
from
fou
r co
mm
unit
ies
usin
g P
art
A M
edic
are
list
in
1988
–198
9; 6
87
Afr
ican
-Am
eric
ans
recr
uite
d in
sam
e m
anne
r in
199
2–19
93
Ani
mal
s: M
CI-
A a
nd
MC
I-M
D <
NE
Ani
mal
s, M
CI-
A v
s. N
E:
0.94
; MC
I-M
D v
s. N
E:
0.84
Bir
ds a
nd d
ogs:
M
CI-
MD
< N
EB
irds
, MC
I-M
D v
s. N
E: 0
.88
Dog
s, M
CI-
MD
vs.
NE
: 0.6
0
Mas
ur e
t al
. (1
994)
CF
(fr
uits
, an
imal
s, f
low
ers
and
vege
tabl
es)
nond
emen
ted
elde
rly
(n=
317)
, 64
of
who
m d
evel
oped
de
men
tia
in a
fol
low
-up
of
at le
ast
4 ye
ars
Dem
enti
a: D
SM-I
IIR
ecru
ited
fro
m c
omm
unit
yA
ctua
rial
mod
el in
clud
ing
dela
yed
reca
ll, C
F, t
he
FO
ME
(F
uld,
198
1) a
nd
the
WA
IS D
igit
Sym
bol
subt
est (
Wec
hsle
r, 1
955)
can
id
enti
fy s
ubgr
oups
wit
h ve
ry
low
/ver
y hi
gh c
hanc
e of
de
velo
ping
dem
enti
a.
AD
: NIN
CD
S-A
DR
DA
cr
iter
ia
Meg
uro
et a
l. (2
004)
CF
(4-
legg
ed
anim
als)
NE
(n
=96
8)C
DR
0.5
, AD
(n
=95
)C
DR
0.5
, UD
(n
=94
)C
DR
0.5
, ID
(n
=22
7)C
DR
0.5
, oth
ers
(n=
37)
CD
R 1
and
2 (
n=
80)
UD
: onl
y m
emor
y is
impa
ired
ID: i
mpa
irm
ent i
n m
emor
y an
d ≤2
oth
er c
ogni
tive
dom
ains
othe
rs: i
mpa
irm
ent
in m
emor
y an
d ≥3
oth
er c
ogni
tive
do
mai
nsD
emen
tia:
DSM
-III
-R
All
olde
r re
side
nts
in T
ajir
i w
ere
targ
eted
CD
R 0
< C
DR
0.5
< C
DR
< 1
an
d 2
CD
R 0
vs.
0.5
: 0.3
2C
DR
0.5
vs.
1&
2: 1
.20
CD
R 0
.5 (
AD
vs.
UD
): 0
.77
CD
R 0
.5 (
AD
vs.
ID
): 0
.67
CD
R 0
.5 (A
D v
s. o
ther
s): 0
.78
CD
R 0
.5 (D
AT
) <
oth
er C
DR
0.
5 ca
tego
ries
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

537
Mio
shi e
t al
. (2
006)
CF
(an
imal
s, f
ruit
, ho
useh
old
item
s)N
E (
n=
63)
MC
I (n
=36
)A
D (
n=
67)
LB
D (
n=
20)
FT
D (
n=
55)
MC
I: G
rund
man
et
al. (
2004
) cr
iter
iaM
emor
y C
linic
, Ear
ly O
nset
D
emen
tia
Clin
ic a
nd
Dru
g M
onit
orin
g C
linic
at
Add
enbr
ooke
’s
Hos
pita
l, C
ambr
idge
NE
> M
CI
> d
emen
tia
NE
vs.
MC
I, 0
.9; M
CI
vs.
dem
enti
a, 1
.23
AD
: NIN
CD
S-A
DR
DA
cr
iter
iaL
BD
: McK
eith
et
al. (
2000
)F
TD
: Nea
ry e
t al
. (19
98)
Mor
ris
et a
l. (2
001)
LF
(S,
P)
NE
(n
=17
7)N
E: C
DR
=0
Rec
ruit
ed t
hrou
gh m
edia
No
grou
p ef
fect
suA
D (
n=
53)
MC
I: C
DR
=0.
5iA
D (n
=69
)iA
D: C
DR
=0.
5A
D (
n=
105)
AD
: CD
R=
0.5;
clin
ical
cri
teri
a de
scri
bed
in M
orri
s, M
cKee
l, F
ullin
g, T
orac
k &
Ber
g,
1988
aM
urph
y et
al.
(200
6)L
F (
F)
& C
F
(ani
mal
s)N
E (
n=
46)
MC
I-A
(n
=33
)A
D (
n=
33)
MC
I-A
: Pet
erse
n (2
004)
cri
teri
aA
D: N
INC
DS-
AD
RD
Acr
iter
ia
Phy
sici
an r
efer
rals
an
d ne
wsp
aper
ad
vert
isem
ents
LF
: NE
> A
DC
F: N
E >
MC
I-A
> A
DC
F: N
E v
s. M
CI-
A, 0
.49;
N
E v
s. A
D, 1
.07;
M
CI-
A v
s. A
D, 0
.68
Nie
lsen
et
al.
(199
9)C
F (
anim
als)
Non
dem
ente
d el
derl
y (n
=2,
452)
, 102
of
who
m
deve
lope
d de
men
tia in
2 y
ears
NIN
CD
S-A
DR
DA
cri
teri
aR
ando
mly
dra
wn
from
th
e po
pula
tion
NE
> in
cide
nt A
D0.
67
Nor
dlun
d et
al.
(200
5)L
F (
F,A
,S)
NE
(n
=35
)Su
bjec
tive
and
obj
ecti
ve
mem
ory
impa
irm
ent
> 6
mon
ths;
pos
itiv
e ou
tcom
e on
ste
pwis
e co
mpa
rati
ve
stat
us a
naly
sis (
STE
P, W
allin
et
al.,
199
6), I
-Fle
x (R
oyal
l et
al.,
199
2), M
MSE
or C
DR
; M
MSE
≥25
; not
mor
e th
an
2 +
ve o
utco
mes
on
STE
P
Mem
ory
clin
icN
E=
MC
IM
CI
(n=
112)
Öst
berg
et
al.
(200
5)L
F (
FA
S), C
F
(ani
mal
s) &
ver
b fl
uenc
y
SCI
( n=
40)
MC
I: P
eter
sen
crit
eria
Dep
t of
Ger
iatr
ics,
H
uddi
nge
Uni
vers
ity
Hos
pita
l, du
e to
cog
niti
ve
com
plai
nts
Ove
rall:
SC
I >
MC
I >
AD
MC
I (n
=60
)A
D: D
SM-I
VC
F: S
CI
> M
CI
> A
DA
D (
n=
57)
LF
: SC
I=M
CI
> A
D
Ver
b fl
uenc
y: S
CI
> M
CI
>
AD
Per
ry e
t al
. (2
000)
CF
(an
imal
s, b
irds
, w
ater
cre
atur
es,
hous
ehol
d it
ems,
ve
hicl
es, m
usic
al
inst
rum
ents
)
NE
(n
=44
)N
INC
DS-
AD
RD
A c
rite
ria
Pat
ient
s un
derg
oing
ev
alua
tion
at
the
Uni
vers
ity
of C
ambr
idge
N
euro
logy
uni
t
NE
> m
inim
al A
D >
mild
AD
NE
vs.
min
imal
AD
: 1.4
2;
min
imal
AD
vs.
mild
AD
: 1.
15m
inim
al A
D (
n=
13)
min
imal
: MM
SE=
24–3
0m
ild A
D (
n=
14)
mild
: MM
SE=
18–2
3
Pet
erse
n et
al.
(199
9)L
FN
E (
n=
234)
MC
I (n
=76
)m
ild A
D (
n=
106)
MC
I: m
emor
y co
mpl
aint
; no
rmal
AD
L; n
orm
al g
ener
al
cogn
itiv
e fu
ncti
on; a
bnor
mal
m
emor
y fo
r ag
e; n
ot
dem
ente
d; C
DR
=0.
5.
Com
mun
ity
(sub
ject
s re
ceiv
ing
gene
ral m
edic
al
care
at
May
o C
linic
) an
d re
gion
al (
eval
uati
on o
f co
gnit
ive
diff
icul
ties
at
May
o A
lzhe
imer
’s
Dis
ease
Cen
ter)
NE
> M
CI=
AD
NE
vs.
MC
I: 5
.86
mild
AD
: CD
R=
0.5–
1.0
(Con
tinu
ed)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009
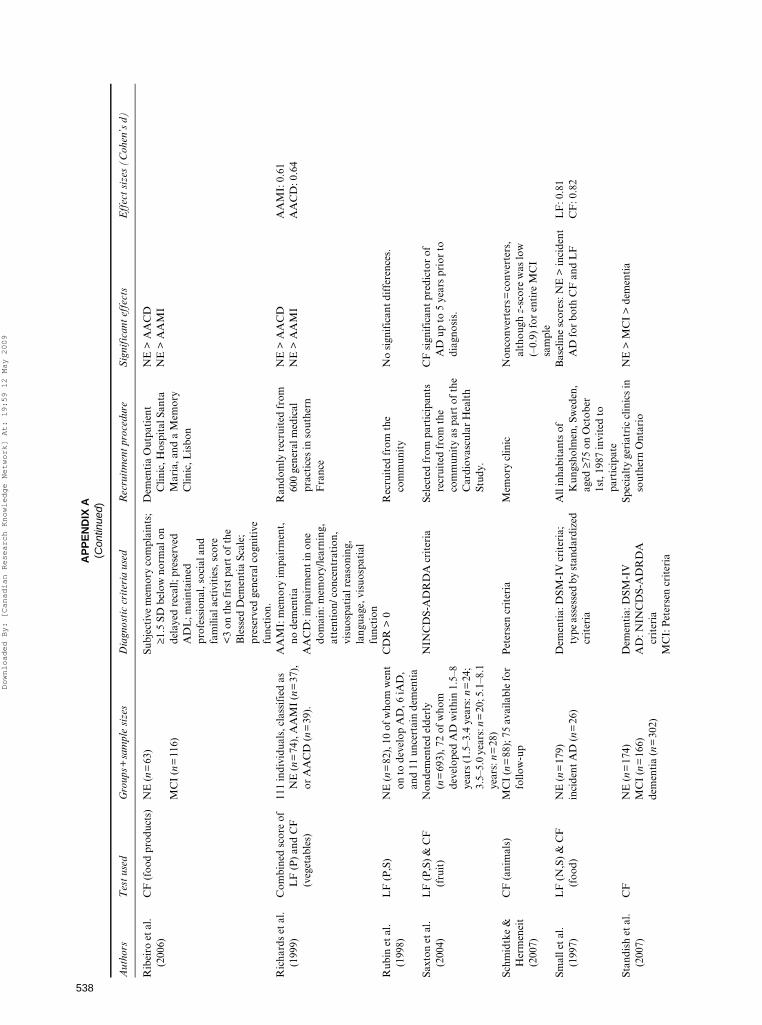
538
AP
PE
ND
IX A
(C
ontin
ued)
Aut
hors
Tes
t us
edG
roup
s+sa
mpl
e si
zes
Dia
gnos
tic
crit
eria
use
dR
ecru
itm
ent
proc
edur
eS
igni
fica
nt e
ffec
tsE
ffec
t si
zes
(Coh
en’s
d)
Rib
eiro
et
al.
(200
6)C
F (
food
pro
duct
s)N
E (
n=
63)
Subj
ecti
ve m
emor
y co
mpl
aint
s;
≥1.5
SD
bel
ow n
orm
al o
n de
laye
d re
call;
pre
serv
ed
AD
L; m
aint
aine
d pr
ofes
sion
al, s
ocia
l and
fa
mili
al a
ctiv
itie
s, s
core
<
3 on
the
fir
st p
art
of t
he
Ble
ssed
Dem
enti
a Sc
ale;
pr
eser
ved
gene
ral c
ogni
tive
fu
ncti
on.
Dem
enti
a O
utpa
tien
t C
linic
, Hos
pita
l San
ta
Mar
ia, a
nd a
Mem
ory
Clin
ic, L
isbo
n
NE
> A
AC
D
NE
> A
AM
IM
CI
(n=
116)
Ric
hard
s et
al.
(199
9)C
ombi
ned
scor
e of
L
F (
P)
and
CF
(v
eget
able
s)
111
indi
vidu
als,
cla
ssif
ied
as
NE
(n
=74
), A
AM
I (n
=37
),
or A
AC
D (
n=
39).
AA
MI:
mem
ory
impa
irm
ent,
no
dem
enti
aR
ando
mly
rec
ruit
ed f
rom
60
0 ge
nera
l med
ical
pr
acti
ces
in s
outh
ern
Fra
nce
NE
> A
AC
D
NE
> A
AM
IA
AM
I: 0
.61
AA
CD
: 0.6
4A
AC
D: i
mpa
irm
ent
in o
ne
dom
ain:
mem
ory/
lear
ning
, at
tent
ion/
con
cent
rati
on,
visu
ospa
tial
rea
soni
ng,
lang
uage
, vis
uosp
atia
l fu
ncti
onR
ubin
et
al.
(199
8)L
F (
P,S
)N
E (
n=
82),
10
of w
hom
wen
t on
to
deve
lop
AD
, 6 iA
D,
and
11 u
ncer
tain
dem
enti
a
CD
R >
0R
ecru
ited
fro
m t
he
com
mun
ity
No
sign
ific
ant
diff
eren
ces.
Saxt
on e
t al
. (2
004)
LF
(P
,S)
& C
F
(fru
it)
Non
dem
ente
d el
derl
y (n
=69
3), 7
2 of
who
m
deve
lope
d A
D w
ithi
n 1.
5–8
year
s (1
.5–3
.4 y
ears
: n=
24;
3.5–
5.0
year
s: n
=20
; 5.1
–8.1
ye
ars:
n=
28)
NIN
CD
S-A
DR
DA
cri
teri
aSe
lect
ed f
rom
par
tici
pant
s re
crui
ted
from
the
co
mm
unit
y as
par
t of
the
C
ardi
ovas
cula
r H
ealt
h St
udy.
CF
sig
nifi
cant
pre
dict
or o
f A
D u
p to
5 y
ears
pri
or t
o di
agno
sis.
Schm
idtk
e &
H
erm
enei
t (2
007)
CF
(an
imal
s)M
CI
(n=
88);
75
avai
labl
e fo
r fo
llow
-up
Pet
erse
n cr
iter
iaM
emor
y cl
inic
Non
conv
erte
rs=
conv
erte
rs,
alth
ough
z-s
core
was
low
(–
0.9)
for
ent
ire
MC
I sa
mpl
eSm
all e
t al
. (1
997)
LF
(N
,S)
& C
F
(foo
d)N
E (
n=
179)
Dem
enti
a: D
SM-I
V c
rite
ria;
ty
pe a
sses
sed
by st
anda
rdiz
ed
crit
eria
All
inha
bita
nts
of
Kun
gsho
lmen
, Sw
eden
, ag
ed ≥
75 o
n O
ctob
er
1st,
198
7 in
vite
d to
pa
rtic
ipat
e
Bas
elin
e sc
ores
: NE
> in
cide
nt
AD
for
both
CF
and
LF
LF
: 0.8
1in
cide
nt A
D (
n=
26)
CF
: 0.8
2
Stan
dish
et
al.
(200
7)C
FN
E (
n=
174)
MC
I (n
=16
6)de
men
tia
(n=
302)
Dem
enti
a: D
SM-I
VSp
ecia
lty
geri
atri
c cl
inic
s in
so
uthe
rn O
ntar
ioN
E >
MC
I >
dem
enti
aA
D: N
INC
DS-
AD
RD
A
crit
eria
MC
I: P
eter
sen
crit
eria
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

539
Swai
nson
et
al.
(200
1)L
F (
F,A
,S)
& C
F
(ani
mal
s, f
ruit
s,
hous
ehol
d it
ems)
NE
(n
=39
)Q
D (
n=
43)
mild
AD
(n
=26
)M
D (
n=
37)
QD
: mem
ory
impa
irm
ent
but
not
mee
ting
cri
teri
a fo
r de
men
tia/
depr
essi
on
AD
: NIN
CD
S-A
DR
DA
cri
teri
a
Mem
ory
clin
ic,
Add
enbr
ooke
’s H
ospi
tal;
Psy
chia
try
Dep
artm
ent,
W
est
Suff
olk
Hos
pita
l; M
enta
l Hea
lth
Serv
ices
, A
dden
broo
ke’s
NH
S T
rust
CF
: QD
+M
D+
NE
> A
D;
MD
+N
E >
QD
; NE
> M
DL
F: Q
D+
MD
+N
E >
AD
No
sign
ific
ant
corr
elat
ion
betw
een
base
line
perf
orm
ance
and
MM
SE
decl
ine
in Q
D in
divi
dual
s
MD
: DSM
-IV
Tab
ert
et a
l. (2
006)
AN
T (G
oodg
lass
&
Kap
lan,
198
3)L
F (
C,F
,L)
NE
(n
=83
)M
CI
(n=
148)
Age
≥40
; cog
niti
ve im
pair
men
t fo
r 6
mon
ths–
10 y
ears
; C
DR
0–0
.5.
Mem
ory
diso
rder
s cl
inic
; N
E r
ecru
ited
by
adve
rtis
emen
t
NE
> M
CI
AN
T: N
E v
s. M
CI,
0.7
2;
Non
conv
erte
rs v
s.
conv
erte
rs, 0
.59
LF
: NE
vs.
MC
I, 0
.43;
N
onco
nver
ters
vs.
co
nver
ters
, 0.7
2
For
mem
ory:
MM
SE, S
RT
, W
AIS
–R p
erfo
rman
ce I
Q.
Non
conv
erte
rs >
con
vert
ers
If n
o fo
rmal
cog
niti
ve d
efic
it:
subj
ecti
ve m
emor
y de
clin
e,
posi
tive
sco
re o
n 1
or m
ore
of
the
firs
t 8
item
s of
the
m
odif
ied
Ble
ssed
Fun
ctio
nal
Act
ivit
y Sc
ale.
Tia
n et
al.
(200
3)L
FQ
D (
n=
195)
, 135
see
n fo
r fo
llow
up a
t 24
.5 m
onth
s;
37 c
onve
rted
to
dem
enti
a
Obj
ecti
ve e
vide
nce
of c
ogni
tive
im
pair
men
t bu
t no
dem
enti
aB
rist
ol M
emor
y D
isor
ders
C
linic
Non
conv
erte
rs >
con
vert
ers
0.40
Tou
chon
&
Rit
chie
(1
999)
LF
(P
) &
CF
(v
eget
able
s)N
E (
n=
150)
359
init
ially
non
dem
ente
d in
divi
dual
s: 2
2 de
velo
ped
AD
in t
hird
yea
r
Dem
enti
a: D
SM-I
II-R
A
D: N
INC
DS-
AD
RD
A
crit
eria
Gen
eral
pra
ctit
ione
r re
crui
tmen
t ne
twor
kC
F: N
E >
MC
I 2
year
s pr
ior
to
diag
nosi
s, in
depe
nden
t of
ed
ucat
ion
effe
cts
LF
: NE
> M
CI,
but
inte
ract
ed
sign
ific
antl
y w
ith
educ
atio
n.
CF
: 2.0
4L
F: 1
.51
Vog
el e
t al
. (2
005)
CF
(an
imal
s)N
E (
n=
58)
pred
emen
tia
AD
(n
=22
)m
ild A
D (
n=
102)
AD
: NIN
CD
S-A
DR
DA
cr
iter
iaC
open
hage
n U
nive
rsit
y H
ospi
tal M
emor
y C
linic
NE
> p
rede
men
tia
AD
> A
D
pred
emen
tia
AD
: Pet
erse
n cr
iter
ia+
subs
eque
nt
prog
ress
ion
to A
D (
10–3
0 m
onth
s la
ter)
Wan
g et
al.
(200
6)C
F (
4-le
gged
an
imal
s)N
E (
n=
20)
MC
I: P
eter
sen
crit
eria
Neu
rolo
gica
l clin
ics
NE
> M
CI
> A
DN
E v
s. M
CI:
1.2
5M
CI
(n=
58)
AD
: NIN
CD
S-A
DR
DA
cr
iter
iaM
CI
vs. A
D: 0
.59
AD
(n
=20
)
Not
e. E
ffec
t si
zes
are
repo
rted
whe
re p
ossi
ble.
AA
MI=
age-
asso
ciat
ed m
emor
y im
pair
men
t. A
D=
Alz
heim
er’s
dis
ease
. AD
L=
acti
viti
es o
f da
ily li
ving
. AN
T=
Ani
mal
Nam
ing
Tes
t. A
oA=
age
of a
cqui
si-
tion
. CD
R=
Clin
ical
Dem
entia
Rat
ing
Scal
e. C
F=
cate
gory
flue
ncy.
CV
D=
cere
brov
ascu
lar
dise
ase.
DSM
-III
-R=
Dia
gnos
tic a
nd S
tatis
tica
l Man
ual o
f Men
tal D
isor
ders
—T
hird
Edi
tion,
Rev
ised
. FO
ME
=F
uld
Obj
ect
Mem
ory
Eva
luat
ion.
iA
D=
inci
pien
t A
D.
ID=
inci
pien
t de
men
tia.
IM
I=is
olat
ed m
emor
y im
pair
men
t. L
BD
=L
ewy
body
dem
enti
a. L
F=
lett
er f
luen
cy.
MC
I=m
ild c
ogni
tive
im
pair
men
t.M
CI-
A=
MC
I-am
nest
ic. M
CI-
MD
=M
CI-
mul
tipl
e do
mai
n. M
D=
maj
or d
epre
ssiv
e di
sord
er. M
MSE
=M
ini M
enta
l Sta
te E
xam
inat
ion.
NE
=no
rmal
eld
erly
. NIN
CD
S-A
DR
DA
=N
atio
nal I
nsti
tute
of
Neu
rolo
gica
l and
Com
mun
icat
ive
Dis
orde
rs a
nd S
trok
e–A
lzhe
imer
’s D
isea
se a
nd R
elat
ed D
isor
ders
Ass
ocia
tion
. qA
D=
ques
tion
able
Alz
heim
er’s
dis
ease
. QD
=qu
esti
onab
le d
emen
tia.
SC
I=su
bjec
tive
cogn
itiv
e im
pair
men
t. S
ML
=su
bjec
tive
mem
ory
loss
. SR
T =
Bus
cke
Sele
ctiv
e R
emin
ding
Tes
ts.
UD
=un
cert
ain
dem
enti
a. V
aD=
vasc
ular
dem
enti
a. V
CI=
vasc
ular
cog
niti
ve i
mpa
irm
ent.
WA
IS-
R=
Wec
hsle
r A
dult
Int
ellig
ence
Sca
le–R
evis
ed.
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009
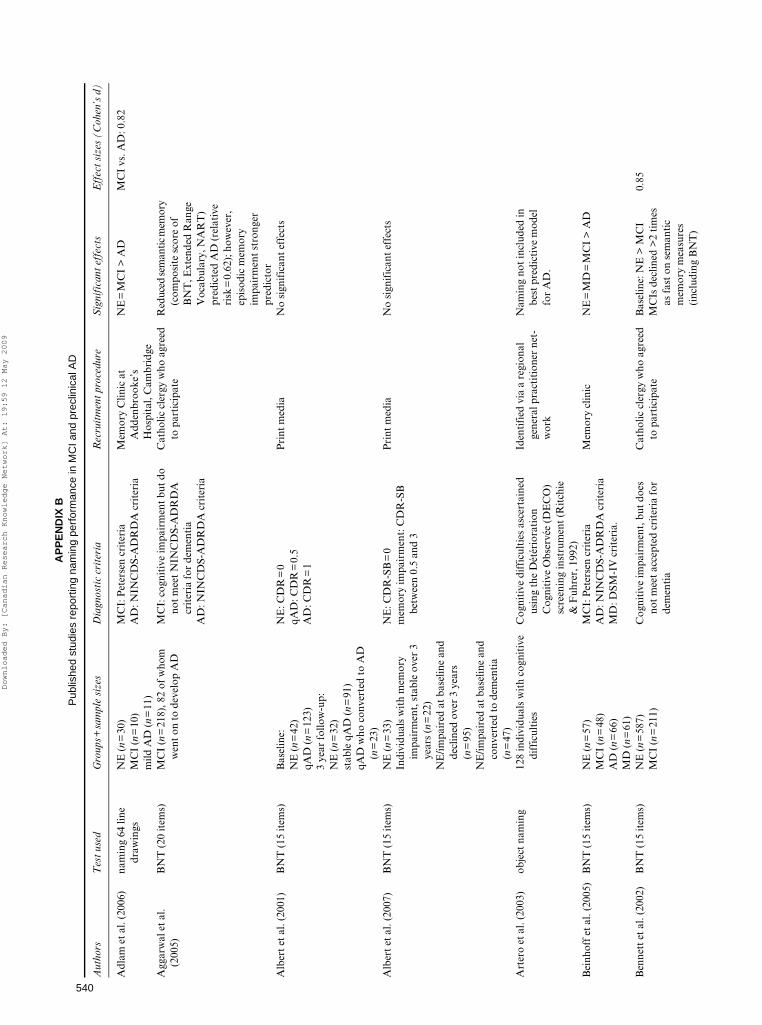
540
AP
PE
ND
IX B
Pub
lishe
d st
udie
s re
port
ing
nam
ing
perf
orm
ance
in M
CI a
nd p
recl
inic
al A
D
Aut
hors
Tes
t us
edG
roup
s+sa
mpl
e si
zes
Dia
gnos
tic
crit
eria
R
ecru
itm
ent
proc
edur
eS
igni
fica
nt e
ffec
tsE
ffec
t si
zes
(Coh
en’s
d)
Adl
am e
t al
. (20
06)
nam
ing
64 li
ne
draw
ings
NE
(n
=30
)M
CI
(n=
10)
mild
AD
(n
=11
)
MC
I: P
eter
sen
crit
eria
AD
: NIN
CD
S-A
DR
DA
cri
teri
aM
emor
y C
linic
at
Add
enbr
ooke
’s
Hos
pita
l, C
ambr
idge
NE
=M
CI
> A
DM
CI
vs. A
D: 0
.82
Agg
arw
al e
t al
. (2
005)
BN
T (
20 it
ems)
MC
I (n
=21
8), 8
2 of
who
m
wen
t on
to
deve
lop
AD
MC
I: c
ogni
tive
impa
irm
ent
but
do
not
mee
t N
INC
DS-
AD
RD
A
crit
eria
for
dem
enti
aA
D: N
INC
DS-
AD
RD
A c
rite
ria
Cat
holic
cle
rgy
who
agr
eed
to p
arti
cipa
teR
educ
ed se
man
tic m
emor
y (c
ompo
site
sco
re o
f B
NT
, Ext
ende
d R
ange
V
ocab
ular
y, N
AR
T)
pred
icte
d A
D (
rela
tive
ri
sk=
0.62
); h
owev
er,
epis
odic
mem
ory
impa
irm
ent
stro
nger
pr
edic
tor
Alb
ert
et a
l. (2
001)
BN
T (
15 it
ems)
Bas
elin
e:N
E: C
DR
=0
Pri
nt m
edia
No
sign
ific
ant
effe
cts
NE
(n
=42
)qA
D: C
DR
=0.
5qA
D (
n=
123)
AD
: CD
R=
13
year
fol
low
-up:
NE
(n
=32
)st
able
qA
D (
n=
91)
qAD
who
con
vert
ed t
o A
D
(n=
23)
Alb
ert
et a
l. (2
007)
BN
T (
15 it
ems)
NE
(n
=33
)N
E: C
DR
-SB
=0
Pri
nt m
edia
No
sign
ific
ant
effe
cts
Indi
vidu
als
wit
h m
emor
y im
pair
men
t, s
tabl
e ov
er 3
ye
ars
(n=
22)
mem
ory
impa
irm
ent:
CD
R-S
B
betw
een
0.5
and
3
NE
/impa
ired
at
base
line
and
decl
ined
ove
r 3
year
s (n
=95
)N
E/im
pair
ed a
t ba
selin
e an
d co
nver
ted
to d
emen
tia
(n=
47)
Art
ero
et a
l. (2
003)
obje
ct n
amin
g12
8 in
divi
dual
s w
ith
cogn
itiv
e di
ffic
ulti
esC
ogni
tive
dif
ficu
ltie
s as
cert
aine
d us
ing
the
Dét
ério
rati
onC
ogni
tive
Obs
ervé
e (D
EC
O)
scre
enin
g in
stru
men
t (R
itch
ie
& F
uhre
r, 1
992)
Iden
tifi
ed v
ia a
reg
iona
l ge
nera
l pra
ctit
ione
r ne
t-w
ork
Nam
ing
not
incl
uded
in
best
pre
dict
ive
mod
el
for
AD
.
Bei
nhof
f et
al.
(200
5)B
NT
(15
item
s)N
E (
n=
57)
MC
I: P
eter
sen
crit
eria
Mem
ory
clin
icN
E=
MD
=M
CI
> A
DM
CI
(n=
48)
AD
: NIN
CD
S-A
DR
DA
cri
teri
aA
D (
n=
66)
MD
: DSM
-IV
cri
teri
a.M
D (
n=
61)
Ben
nett
et
al. (
2002
)B
NT
(15
item
s)N
E (
n=
587)
MC
I (n
=21
1)C
ogni
tive
impa
irm
ent,
but
doe
s no
t m
eet
acce
pted
cri
teri
a fo
rde
men
tia
Cat
holic
cle
rgy
who
agr
eed
to p
arti
cipa
teB
asel
ine:
NE
> M
CI
MC
Is d
eclin
ed >
2 ti
mes
as
fas
t on
sem
anti
c m
emor
y m
easu
res
(inc
ludi
ng B
NT
)
0.85
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

541
Bev
ersd
orf
et a
l. (2
007)
BN
TN
E (
n=
20)
MC
I (n
=26
)M
CI:
MM
SE≥2
4, C
DR
=0.
5M
emor
y cl
inic
NE
> M
CI,
but
BN
T w
as
not
the
best
pre
dict
or0.
75
Bla
ckw
ell e
t al
. (2
004)
GN
T, s
eman
tic
batt
ery
test
(n
amin
g lin
e dr
awin
gs)
Subj
ecti
ve/o
bjec
tive
mem
ory
loss
(n
=43
), 1
1 of
who
m
deve
lope
d A
D w
ithi
n 32
m
onth
s
Nor
mal
per
form
ance
on
test
s of
la
ngua
ge a
nd v
isuo
spat
ial
func
tion
, pre
serv
ed A
DL
, C
DR
=0.
5
Mem
ory
clin
icN
onco
nver
ters
>
conv
erte
rs o
n bo
th m
easu
res
GN
T: 1
.65
Sem
anti
c B
atte
ry
test
: 1.0
8
Boz
oki e
t al
. (20
01)
BN
TIM
I (n
=48
)P
eter
sen
crit
eria
+ne
urop
sych
olog
ical
ev
iden
ce (
diag
nost
ic c
rite
ria
and
cogn
itiv
e m
easu
res
for
clin
ical
ch
ange
bas
ed o
n th
ose
prop
osed
fo
r A
AM
I)
Mic
higa
n A
lzhe
imer
’s
Dis
ease
Res
earc
h C
ente
rB
NT
dis
crim
inat
ed b
est
betw
een
conv
erte
rs a
nd
nonc
onve
rter
s,
alth
ough
not
sig
nific
ant
(p=
.16)
; 42%
of
conv
erte
rs a
nd 1
4% o
f no
ncon
vert
ers
had
abno
rmal
res
ults
Bsc
hor
et a
l. (2
001)
BN
TN
E (
n=
40)
MC
I (n
=34
)m
ild D
AT
(n
=21
)m
oder
ate
to s
ever
e D
AT
(n
=20
)
ICD
-10
crit
eria
(Z
audi
g, 1
992)
Mem
ory
Clin
ic a
t the
Dep
t.
of G
eron
tolo
gy, F
reie
U
nive
rsit
ät B
erlin
NE
> M
CI
> m
ild A
D >
m
oder
ate
AD
NE
vs.
MC
I: 1
.29
MC
I vs
. mild
AD
: 1.1
7m
ild A
D v
s. m
oder
ate
AD
: 1.1
9
Bus
se e
t al
. (20
03)
Com
posi
te a
phas
ia/
apra
xia
scor
e (n
amin
g ob
ject
s,
read
ing
and
obey
ing
a se
nten
ce, w
riti
ng
a se
nten
ce, a
nd
perf
orm
ing
a th
ree-
stag
e co
mm
and)
nond
emen
ted
elde
rly
(n=
1,04
5), 3
% o
f who
m m
et
the
crit
eria
for
MC
I-A
, 36%
MC
I-A
: Pet
erse
n cr
iter
iaA
AC
D: L
evy
(199
4) c
rite
ria
AA
CD
-m: L
evy
crit
eria
, but
no
requ
irem
ent
for
subj
ecti
ve
mem
ory
com
plai
ntD
emen
tia:
DSM
-IV
Ran
dom
sam
plin
g fr
om li
stpr
ovid
ed b
y th
e lo
cal
regi
stry
off
ice
in L
eipz
ig
No
grou
p di
ffer
ence
s;
lang
uage
sco
re n
ot a
si
gnif
ican
t pr
edic
tor
for
MM
SE≥2
6, 9
% f
or
AA
CD
and
20%
for
A
AC
D-m
Cac
capo
lo-V
an V
liet
et a
l. (2
003)
BN
TN
E (
n=
230)
QD
(n
=15
5)m
ild A
D (
n=
244)
mod
erat
e A
D (
n=
480)
seve
re A
D (
n=
376)
very
sev
ere
AD
(n=
247)
QD
: cog
niti
ve im
pair
men
t su
ffic
ient
or
clo
se t
o su
ffic
ient
for
a
diag
nosi
s of
dem
enti
a; n
o fu
ncti
onal
impa
irm
ent
AD
: NIN
CD
S-A
DR
DA
cri
teri
a
Mem
ory
Dis
orde
rs C
ente
r/re
crui
ted
for
a st
udy
of N
E.
NE
=Q
D=
mild
AD
>
mod
erat
e A
D >
sev
ere
AD
> v
ery
seve
re A
D
Che
n et
al.
(200
0)B
NT
(15
item
s)N
E (
n=
483)
Con
vert
ers
to A
D 1
.5 y
ears
af
ter
test
ing
(n=
120)
NIN
CD
S-A
DR
DA
cri
teri
aR
ando
mly
sel
ecte
d fr
om
vote
r re
gist
rati
on li
sts
NE
> in
cide
nt A
D;
how
ever
, not
a b
ette
r pr
edic
tor
of in
cide
nt
dem
enti
a th
an t
he
MM
SE
0.65
Che
n et
al.
(200
1)B
NT
(15
item
s)N
E (
n=
551)
, 68
of w
ho w
ent
on t
o de
velo
p A
DN
INC
DS-
AD
RD
A c
rite
ria
Ran
dom
ly s
elec
ted
from
vo
ter
regi
stra
tion
list
sN
onco
nver
ters
=co
nver
ters
(Con
tinu
ed)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

542
AP
PE
ND
IX B
(C
ontin
ued)
Aut
hors
Tes
t us
edG
roup
s+sa
mpl
e si
zes
Dia
gnos
tic
crit
eria
R
ecru
itm
ent
proc
edur
eS
igni
fica
nt e
ffec
tsE
ffec
t si
zes
(Coh
en’s
d)
Col
lie e
t al
. (20
02)
nam
ing
of 1
5 lin
e dr
awin
gsE
lder
ly a
dult
s (n
=17
4), 2
3 of
w
hom
wer
e im
pair
ed o
n 3
cons
ecut
ive
asse
ssm
ents
CE
RA
D b
atte
ry (
Mor
ris
et a
l.,
1988
b)R
ecru
ited
fro
m a
n on
goin
g st
udy
on a
ging
at
an
inde
pend
ent
rese
arch
in
stit
ute
in M
elbo
urne
, A
ustr
alia
.
NE
> M
CI
0.77
Cro
ot e
t al
. (19
99)
Nam
ing
(as
Hod
ges
& P
atte
rson
, 199
5)N
E (
n=
46)
min
imal
AD
(n
=16
)m
ild A
D (
n=
16)
mod
erat
e A
D (
n=
14)
NIN
CD
S-A
DR
DA
cri
teri
am
inim
al: M
MSE
=24
–30
mild
: MM
SE=
18–2
3m
oder
ate:
MM
SE=
2–17
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
Hos
pita
l, C
ambr
idge
p-va
lue
not
repo
rted
De
Jage
r &
Bud
ge
(200
5)G
NT
Bas
elin
e:N
E (
n=
117)
MC
I (n
=40
)3-
year
fol
low
up:
NE
(n
=85
)M
CI
(n=
49)
MC
I: >
1.5
SD
bel
ow c
ontr
ol m
ean
on m
emor
y te
stin
gT
alks
/rad
io a
dver
tisi
ng
in O
xfor
dshi
re f
or
thos
e w
ho t
houg
ht
that
the
ir h
ealt
h,
mem
ory
and
thin
king
w
ere
good
com
pare
d to
the
ir p
eers
Cla
ssif
icat
ion
at 4
yea
rs
was
pre
dict
ed b
y G
NT
De
Jage
r et
al.
(200
3)B
NT
(30
item
s)N
E (
n=
51)
MC
I (n
=29
)A
D (
n=
60)
VC
I (n
=8)
VaD
(n
=4)
MC
I: P
eter
sen
crit
eria
AD
: NIN
CD
S-A
DR
DA
cri
teri
aV
CI:
Hac
hins
ki c
rite
ria
VaD
: NIN
CD
DS/
AIR
EN
cri
teri
a (G
. Gol
d et
al.,
199
7)
Oxf
ord
Pro
ject
To
Inve
stig
ate
Mem
ory
and
Age
ing
(OP
TIM
A)
stud
y
NE
> M
CI
> A
D; C
VD
(V
CI+
VaD
) al
so
exhi
bite
d im
pair
men
ts
NE
vs.
MC
I: 0
.54
MC
I vs
. AD
: 1.1
5N
E v
s. C
VD
: 0.8
9
Dev
anan
d et
al.
(199
7)B
NT
QD
(n=
62),
26
of w
hom
wen
t on
to
deve
lop
dem
enti
aQ
D: c
ogni
tive
impa
irm
ent,
fal
l be
twee
n “n
orm
al”
and
“dem
enti
a” c
ateg
orie
sD
emen
tia:
DSM
-III
cri
teri
aA
D: N
INC
DS-
AD
RD
A
crit
eria
Mem
ory
Dis
orde
rs C
linic
No
sign
ific
ant
effe
cts
Dud
as e
t al
. (20
05)
Nam
ing
Tes
t (H
odge
s et
al.,
19
92b)
and
GN
T
NE
(n
=29
)M
CI
(n=
24)
AD
(n
=22
)
Pet
erse
n cr
iter
iaM
emor
y C
linic
at
Add
enbr
ooke
’s
Hos
pita
l, C
ambr
idge
NE
> M
CI=
AD
Nam
ing:
NE
vs.
MC
I, 1
.42;
MC
I vs
. AD
, 0.6
4G
NT
:N
E v
s. M
CI,
0.6
3; M
CI
vs. A
D, 1
.20
Dw
olat
zky
et a
l. (2
003)
BN
TN
E (
n=
15)
MC
I (n
=20
)A
D (
n=
19)
Pet
erse
n cr
iter
iaM
emor
y cl
inic
sB
NT
dis
crim
inat
ed
betw
een
MC
I an
d he
alth
y el
derl
y
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

543
Fill
enba
um e
t al
. (2
005)
BN
T (
15 it
ems)
NE
: n=
201
(Sea
ttle
), n
=12
0 (H
awai
i)C
DR
=0.
5: n
=33
(Se
attl
e),
n=
65 (
Haw
aii)
CD
R=
1: n
=37
(Se
attl
e),
n=
97 (
Haw
aii)
CD
R=
2: n
=33
(Se
attl
e),
n=
55 (
Haw
aii)
CD
R=
3,4,
5: n
=46
(Se
attl
e),
n=
81 (
Haw
aii)
CD
R s
core
Seat
tle:
Kin
g C
ount
y te
leph
one
dire
ctor
ies,
H
ealt
h C
are
Fin
anci
ng
Adm
inis
trat
ion
(now
C
MS)
Med
icar
e re
cipi
ent
lists
, Ja
pane
se-A
mer
ican
or
gani
zati
onal
list
s, a
nd
wor
d of
mou
thH
awai
i: Ja
pane
se-A
mer
ican
m
en b
orn
1900
–191
9,
livin
g in
Oah
u in
196
5,
who
had
bee
n on
the
W
orld
War
II
Sele
ctiv
e Se
rvic
e R
egis
trat
ion
file
CD
R 0
< C
DR
0.5
in
both
pop
ulat
ions
Fle
ishe
r et
al.
(200
7)B
NT
(10
item
s)M
CI-
A w
ho p
rogr
esse
d to
A
D w
ithi
n 36
mon
ths
(n=
212)
Pet
erse
n cr
iter
iaP
arti
cipa
nts
in a
36-
mon
th
rand
omiz
ed d
rug
tria
lB
NT
was
not
a m
easu
re
in t
he m
odel
tha
t w
as
mos
t pr
edic
tive
of
prog
ress
ion
to A
DF
licke
r et
al.
(199
1)ob
ject
nam
ing
NE
(n
=32
)M
ildly
impa
ired
(n
=32
)G
DS
rati
ng o
f 3
Sele
cted
fro
m p
arti
cipa
nts
in a
ging
stu
dies
at
the
Agi
ng a
nd D
emen
tia
Res
earc
h C
ente
r, N
YU
M
edic
al C
ente
r
NE
> M
ildly
impa
ired
0.79
Gal
vin
et a
l. (2
005)
BN
TN
E (
n=
80)
who
eve
ntua
lly
cam
e to
aut
opsy
CD
R s
core
Indi
vidu
als
enro
lled
in lo
ngit
udin
al s
tudi
es
of h
ealt
hy a
ging
and
de
men
tia
Bas
elin
e: d
emen
tia
=no
de
men
tia
Fin
al e
xam
inat
ion:
no
dem
enti
a >
dem
enti
a
1.32
Gal
ton
et a
l. (2
005)
PN
(C
ambr
idge
Se
man
tic
Bat
tery
, H
odge
s &
P
atte
rson
, 199
5)G
NT
QD
(n
=31
) 11
of
who
m h
ad
conv
erte
d to
AD
at
24.2
m
onth
s
AD
: NIN
CD
S-A
DR
DA
cri
teri
aQ
D: s
ubje
ctiv
e m
emor
y im
pair
men
t,
corr
obor
ated
by
an in
form
ant;
no
rmal
AD
L; M
MSE
≥ 2
3.
CD
R=
0.5.
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
H
ospi
tal,
Cam
brid
ge
PN
: AD
< n
onco
nver
ters
GN
T: A
D <
con
vert
ers
<
nonc
onve
rter
s
PN
: Non
conv
erte
rs v
s.
AD
, 1.4
0G
NT
:N
onco
nver
ters
vs.
co
nver
ters
, 2.1
8C
onve
rter
s vs
. AD
, 0.
76
AD
(n
=19
)
Ges
lani
et
al. (
2005
)B
NT
(od
d-ev
en
vers
ion)
MC
Is (
n=
161)
Pet
erse
n cr
iter
ia+
corr
obor
atio
n of
m
emor
y de
fici
t by
phy
sici
anR
efer
red
by p
rim
ary-
care
ph
ysic
ians
Ave
rage
scor
e: 3
2.8
± 9.
44
(no
com
pari
son
grou
p)G
oldm
an e
t al
. (2
001)
BN
TN
E (
n=
9)
prec
linic
al A
D (
n=
5)C
linic
ally
non
dem
ente
d, b
ut
neur
itic
and
dif
fuse
pla
ques
th
roug
hout
the
neo
cort
ex
(aut
opsy
fin
ding
s)
Was
hing
ton
Uni
vers
ity’
s A
lzhe
imer
’s d
isea
se
Res
earc
h C
entr
e
NE
=pr
eclin
ical
AD
>
very
mild
AD
Pre
clin
ical
AD
vs.
ver
y m
ild A
D: 1
.1A
D (
n=
10)
(Con
tinu
ed)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

544
AP
PE
ND
IX B
(C
ontin
ued)
Aut
hors
Tes
t us
edG
roup
s+sa
mpl
e si
zes
Dia
gnos
tic
crit
eria
R
ecru
itm
ent
proc
edur
eS
igni
fica
nt e
ffec
tsE
ffec
t si
zes
(Coh
en’s
d)
Góm
ez &
Whi
te
(200
6)B
NT
NE
(n
=76
)N
E: C
DR
=0
Med
ia a
ppea
ls a
nd
pres
enta
tion
s by
re
sear
cher
s
NE
> v
ery
mild
AD
0.77
very
mild
AD
(n
=77
)ve
ry m
ild A
D: N
INC
DS-
AD
RD
A
& D
SM-I
II c
rite
ria;
CD
R=
0.5
Gri
ffit
h et
al.
(200
6)B
NT
(15
item
s)N
E (
n=
49)
Pet
erse
n cr
iter
iaM
emor
y D
isor
ders
Clin
ic
or r
ecru
ited
fro
m
com
mun
ity
NE
=M
CI
MC
I (n
=49
)
Gru
ndm
an e
t al
. (2
004)
BN
T (
15 it
ems)
NE
(n
=10
7)P
eter
sen
crit
eria
+C
DR
=0.
5A
dver
tisi
ng c
ampa
ign
targ
etin
g el
derl
y su
bjec
ts in
cit
ies
wit
h A
lzhe
imer
Dis
ease
C
oope
rati
ve S
tudy
(A
DC
S) s
ites
NE
> M
CI
0.51
MC
I (n
=76
9)
Gua
rch
et a
l. (2
004)
BN
TN
E (
n=
34)
Subj
ecti
ve m
emor
y lo
ss;
neur
opsy
chol
ogic
al t
ests
not
use
d as
incl
usio
n/ex
clus
ion
crit
eria
.
Clin
ical
psy
chol
ogy
serv
ice
at t
he H
ospi
tal C
linic
i P
rovi
ncia
l, B
arce
lona
.
NE
> S
ML
NE
vs.
SM
L: 0
.89
SML
(n
=43
), 1
0 of
who
m
wen
t on
to
deve
lop
AD
SML
: bas
al=
rete
stN
onco
nver
ters
vs.
co
nver
ters
, ret
est:
1.
56ba
sal:
nonc
onve
rter
s=
conv
erte
rsre
test
: non
conv
erte
rs >
co
nver
ters
Hod
ges,
E
rzin
çlio
glu,
&
Pat
ters
on (
2006
)
nam
ing
64 li
ne
draw
ings
NE
(n
=24
)G
rund
man
et
al. (
2004
) cr
iter
iaM
emor
y C
linic
at
Add
enbr
ooke
’s
Hos
pita
l, C
ambr
idge
NE
=M
CI-
A e
ven
afte
r 7
year
s of
fol
low
-up
MC
I-A
(n
=10
)
Hod
ges
& P
atte
rson
(1
995)
nam
ing
64 li
ne
draw
ings
NE
(n
=24
)N
INC
DS-
AD
RD
A c
rite
ria
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
H
ospi
tal,
Cam
brid
ge
NE
> m
inim
al=
mild
>
mod
erat
em
inim
al A
D (
n=
17)
mild
AD
(n
=17
), m
oder
ate
AD
(n
=18
)H
odge
s et
al.
(199
6)N
amin
g of
48
line
draw
ings
N
E (
n=
10)
AD
: NIN
CD
S-A
DR
DA
cri
teri
aM
emor
y C
linic
at
Add
enbr
ooke
’s
Hos
pita
l, C
ambr
idge
NE
> m
inim
al=
mild
>
mod
erat
em
inim
al A
D (
n=
16)
min
imal
: MM
SE=
24–3
0m
ild A
D (
n=
17)
mild
: MM
SE=
18–2
3m
oder
ate
AD
(n
=18
)m
oder
ate:
MM
SE=
2–17
Hud
on e
t al
. (20
06)
Dén
omin
atio
n or
ale
d’im
ages
(D
eloc
he &
H
anne
quin
, 199
7)
NE
(n
=22
)M
CI:
MC
I-SD
/MC
I-M
D, P
eter
sen
(200
4) c
rite
ria
Mem
ory
clin
ics
NE
=M
CI
> A
DN
E v
s. A
D: 0
.88
MC
I (n
=14
)M
CI
vs. A
D: 0
.72
AD
(n
=14
)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

545
Jaco
bs e
t al
. (19
95)
BN
T (
15 it
ems)
nond
emen
ted
elde
rly
(n=
443)
, 41
of
who
m h
ad d
evel
oped
A
D a
t fo
llow
-up
(on
aver
age
2.05
yea
rs la
ter)
NIN
CD
S-A
DR
DA
cri
teri
aN
orth
Man
hatt
an
Agi
ng P
roje
ct, a
co
mm
unit
y-ba
sed,
ep
idem
iolo
gic
stud
y of
de
men
tia
in n
orth
ern
Man
hatt
an, N
Y.
BN
T s
igni
fica
ntly
as
soci
ated
wit
h in
crea
sed
risk
of
deve
lopi
ng A
D.
Jaco
bson
et
al.
(200
2)B
NT
NE
(n
=20
)pr
eclin
ical
AD
: eit
her m
ild su
bjec
tive
m
emor
y co
mpl
aint
s w
itho
ut
func
tion
al im
pair
men
t (n
=9)
or
an
abno
rmal
ity
in t
he
part
icip
ant’
s ne
urol
ogic
al
exam
inat
ion
(n=
11).
Did
not
m
eet
NIN
CD
S-A
DR
DA
cri
teri
a fo
r A
D
Alz
heim
er’s
Dis
ease
R
esea
rch
Cen
ter
at
UC
SD.
Bes
t pr
edic
tor
was
di
ffer
ence
sco
res
betw
een
nam
ing
(BN
T)
and
visu
ocon
stru
ctio
n ab
iliti
es (
WA
IS B
lock
de
sign
), n
ot r
aw B
NT
sc
ore;
10/
20 p
recl
inic
al
AD
indi
vidu
als
and
5/20
con
trol
s ha
d as
ymm
etri
c pr
ofile
s
prec
linic
al A
D (
n=
20)
Kar
rasc
h et
al.
(200
5)C
ER
AD
nam
ing
subt
est
NE
(n
=15
)P
eter
sen
crit
eria
Com
mun
ity
sour
ces
NE
> A
D, n
ot M
CI
MC
I (n
=15
)A
D (
n=
15)
Lam
bon
Ral
ph e
t al.
(200
3)na
min
g 64
line
dr
awin
gsN
E (
n=
48)
Subj
ecti
ve m
emor
y im
pair
men
t,
corr
obor
ated
by
a sp
ouse
/fam
ily
mem
ber;
pre
serv
atio
n of
AD
L;
impa
irm
ent
on a
t le
ast
one
test
of
mem
ory;
nor
mal
per
form
ance
on
test
s of
lang
uage
, vis
uosp
atia
l and
ex
ecut
ive
func
tion
; MM
SE >
24.
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
H
ospi
tal,
Cam
brid
ge
NE
=M
CI
MC
I (n
=17
)m
ild A
D (
n=
22)
mod
erat
e A
D (
n=
8)se
vere
AD
(n
=8)
Lee
et
al. (
2006
)B
NT
(15
item
s)Q
D (n
=72
), 1
4 of
who
m
prog
ress
ed t
o A
D in
3 y
ears
CD
R=
0.5
One
pub
lic h
ealt
h ce
nter
an
d 2
mem
ory
clin
ics
in
Kor
ea
Non
conv
erte
rs=
conv
erte
rs
Lóp
ez e
t al
. (20
06)
BN
TN
E (
n=
374)
MC
I-A
: >1.
5 SD
s be
low
con
trol
s in
de
laye
d re
call
+de
clin
e in
co
gnit
ive
func
tion
ing;
M
CI-
MD
>1.
5 SD
s in
at
leas
t on
e co
gnit
ive
dom
ain
othe
r th
an
mem
ory/
one
abno
rmal
tes
t in
≥2
dom
ains
.
5201
non
inst
itut
iona
lized
in
divi
dual
s ov
er 6
5;
recr
uite
d fr
om f
our
com
mun
itie
s us
ing
Par
t A
Med
icar
e lis
t in
198
8–19
89; 6
87
Afr
ican
-Am
eric
ans
recr
uite
d in
sam
e m
anne
r in
199
2–19
93
NE
> M
CI-
A >
M
CI-
MD
NE
vs.
MC
I-A
: 0.1
9M
CI-
A (
n=
10)
NE
vs.
MC
I-M
D: 1
.40
MC
I-M
D (
n=
28)
MC
I-M
D v
s. M
CI-
A:
0.92
Mio
shi e
t al
. (20
06)
PN
(C
ambr
idge
Se
man
tic
Bat
tery
, H
odge
s &
P
atte
rson
, 199
5)G
NT
NE
(n
=63
)M
CI
(n=
36)
AD
(n
=67
)D
LB
(n
=20
)F
TD
(n
=55
)
MC
I: G
rund
man
et
al. (
2004
) cr
iter
iaA
D: N
INC
DS-
AD
RD
A c
rite
ria
DL
B: M
cKei
th e
t al
. (20
00)
FT
D: N
eary
et
al. (
1998
)
Mem
ory
Clin
ic, E
arly
O
nset
Dem
enti
a C
linic
an
d D
rug
Mon
itor
ing
Clin
ic a
t A
dden
broo
ke’s
H
ospi
tal
NE
> M
CI
> d
emen
tia
NE
vs.
MC
I, 0
.77;
MC
I vs
. dem
enti
a, 0
.77
(Con
tinu
ed)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

546
AP
PE
ND
IX B
(C
ontin
ued)
Aut
hors
Tes
t us
edG
roup
s+sa
mpl
e si
zes
Dia
gnos
tic
crit
eria
Rec
ruit
men
t pr
oced
ure
Sig
nifi
cant
eff
ects
Eff
ect
size
s (C
ohen
’s d
)
Mor
ris
et a
l. (2
001)
BN
TN
E (
n=
177)
uAD
(n
=53
)iA
D (n
=69
)A
D (
n=
105)
NE
: CD
R=
0R
ecru
ited
thr
ough
the
m
edia
NE
> u
AD
> iA
D >
AD
NE
vs.
iAD
: 0.4
4uA
D v
s. iA
D: 0
.25
iAD
vs.
AD
: 0.2
4M
CI:
CD
R=
0.5
uAD
: CD
R=
0.5
iAD
: CD
R=
0.5
AD
: CD
R=
0.5;
clin
ical
cr
iter
ia d
escr
ibed
in M
orri
s,
McK
eel,
Ful
ling,
Tor
ack
&
Ber
g, 1
988a
Nes
tor
et a
l. (2
003)
64-i
tem
nam
ing
test
(B
ozea
t et
al.,
20
00)
Con
trol
s (n
=15
), M
CIs
(n
=10
); A
Ds
(n=
10)
MC
I: in
sidi
ous
onse
t m
emor
y sy
mpt
oms,
obj
ecti
ve m
emor
y im
pair
men
t, n
o ot
her
sign
ific
ant
defi
cits
Mem
ory
Clin
icM
CI
> A
D
AD
: NIN
CD
S-A
DR
DA
cri
teri
aN
iels
en e
t al
. (19
99)
Nam
ing
subt
est
of
CA
MC
OG
Non
dem
ente
d el
derl
y (n
=2,
452)
, 102
of
who
m
deve
lope
d de
men
tia
in
2 ye
ars
DSM
-III
-R c
rite
ria,
N
INC
DS-
AD
RD
A c
rite
ria
Ran
dom
ly d
raw
n fr
om t
he
popu
lati
onN
onde
men
ted
> in
cide
nt
dem
ente
d0.
83
Nor
dlun
d et
al.
(200
5)B
NT
NE
(n
=35
)Su
bjec
tive
and
obj
ecti
ve m
emor
y im
pair
men
t >
6 m
onth
s;
posi
tive
out
com
e on
ste
pwis
e co
mpa
rati
ve s
tatu
s an
alys
is
(ST
EP
, Wal
lin e
t al
., 19
96),
I-
Fle
x (R
oyal
l et
al.,
1992
),
MM
SE o
r C
DR
; MM
SE ≥
25;
not
mor
e th
an 2
+ve
ou
tcom
es o
n ST
EP
Mem
ory
clin
icN
E >
MC
Is0.
60M
CI
(n=
109)
Pet
erse
n et
al.
(199
9)B
NT
NE
(n
=23
4)M
CI:
mem
ory
com
plai
nt; n
orm
al
AD
L; n
orm
al g
ener
al c
ogni
tive
fu
ncti
on; a
bnor
mal
mem
ory
for
age;
not
dem
ente
d; C
DR
=0.
5.m
ild A
D: C
DR
=0.
5–1.
0
Com
mun
ity
(sub
ject
s re
ceiv
ing
gene
ral
med
ical
car
e at
May
o C
linic
) A
ND
reg
iona
l (e
valu
atio
n of
cog
niti
ve
diff
icul
ties
at
May
o A
lzhe
imer
’s D
isea
se
Cen
ter)
NE
> M
CI
> A
DN
E v
s. M
CI:
7.2
MC
I (n
=76
)M
CI
vs. A
D (
CD
R
0.5)
: 6.7
8m
ild A
D (
n=
106)
Pyo
et
al. (
2006
)A
DA
S-C
og N
amin
g O
bjec
ts a
nd
Fin
gers
test
NE
(n
=84
3)M
CI:
CD
R=
0.5,
mem
ory
loss
but
no
dem
enti
aM
edia
app
eals
NE
> M
CI
> A
D (
CD
R
0.5)
> A
D (
CD
R 1
)N
E v
s. M
CI:
1.0
4un
cert
ain/
MC
I (n
=13
5)M
CI
vs. A
D (
CD
R
0.5)
: 0.0
9A
D (
CD
R 0
.5 v
s. 1
):
0.23
AD
, CD
R=
0.5
(n=
30)
AD
, CD
R=
1 (n
=12
5)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009
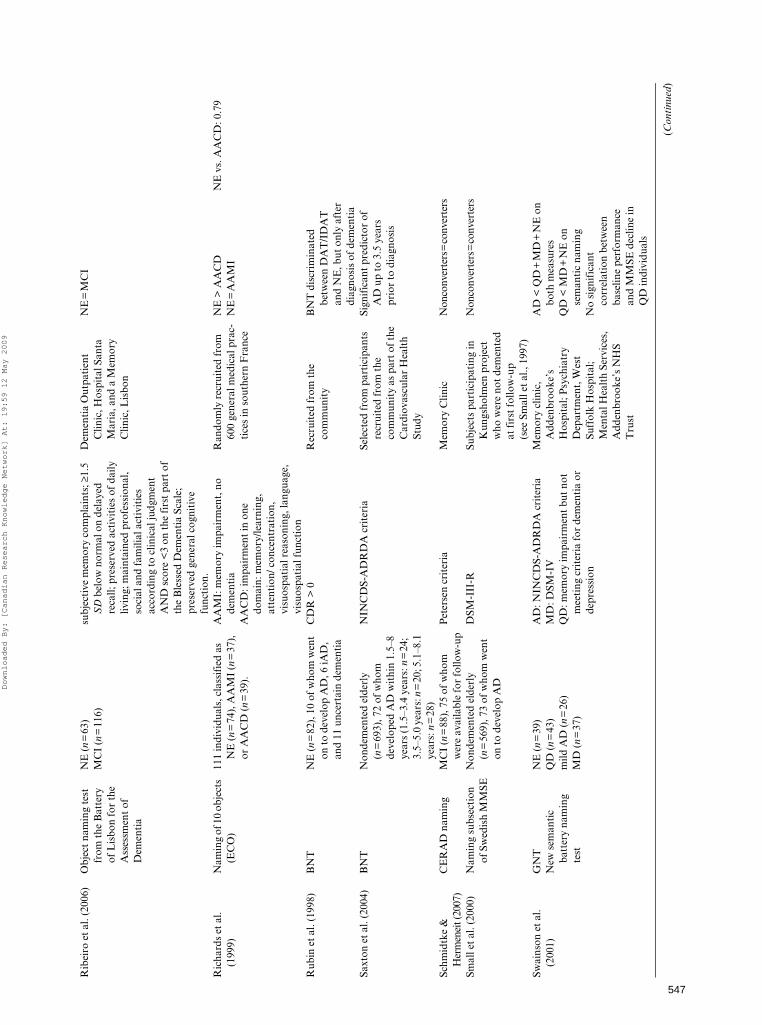
547
Rib
eiro
et
al. (
2006
)O
bjec
t na
min
g te
st
from
the
Bat
tery
of
Lis
bon
for
the
Ass
essm
ent
of
Dem
enti
a
NE
(n
=63
)su
bjec
tive
mem
ory
com
plai
nts;
≥1.
5 S
D b
elow
nor
mal
on
dela
yed
reca
ll; p
rese
rved
act
ivit
ies
of d
aily
liv
ing;
mai
ntai
ned
prof
essi
onal
, so
cial
and
fam
ilial
act
ivit
ies
acco
rdin
g to
clin
ical
judg
men
t A
ND
sco
re <
3 on
the
fir
st p
art
of
the
Ble
ssed
Dem
enti
a Sc
ale;
pr
eser
ved
gene
ral c
ogni
tive
fu
ncti
on.
Dem
enti
a O
utpa
tien
t C
linic
, Hos
pita
l San
ta
Mar
ia, a
nd a
Mem
ory
Clin
ic, L
isbo
n
NE
=M
CI
MC
I (n
=11
6)
Ric
hard
s et
al.
(199
9)N
amin
g of
10
obje
cts
(EC
O)
111
indi
vidu
als,
cla
ssif
ied
as
NE
(n
=74
), A
AM
I (n
=37
),
or A
AC
D (
n=
39).
AA
MI:
mem
ory
impa
irm
ent,
no
dem
enti
aA
AC
D: i
mpa
irm
ent
in o
ne
dom
ain:
mem
ory/
lear
ning
, at
tent
ion/
con
cent
rati
on,
visu
ospa
tial
rea
soni
ng, l
angu
age,
vi
suos
pati
al f
unct
ion
Ran
dom
ly r
ecru
ited
fro
m
600
gene
ral m
edic
al p
rac-
tice
s in
sou
ther
n F
ranc
e
NE
> A
AC
DN
E v
s. A
AC
D: 0
.79
NE
=A
AM
I
Rub
in e
t al
. (19
98)
BN
TN
E (
n=
82),
10
of w
hom
wen
t on
to
deve
lop
AD
, 6 iA
D,
and
11 u
ncer
tain
dem
enti
a
CD
R >
0R
ecru
ited
fro
m t
he
com
mun
ity
BN
T d
iscr
imin
ated
be
twee
n D
AT
/ID
AT
an
d N
E, b
ut o
nly
afte
r di
agno
sis
of d
emen
tia
Saxt
on e
t al
. (20
04)
BN
TN
onde
men
ted
elde
rly
(n=
693)
, 72
of w
hom
de
velo
ped
AD
wit
hin
1.5–
8 ye
ars
(1.5
–3.4
yea
rs: n
=24
; 3.
5–5.
0 ye
ars:
n=
20; 5
.1–8
.1
year
s: n
=28
)
NIN
CD
S-A
DR
DA
cri
teri
aSe
lect
ed f
rom
par
tici
pant
s re
crui
ted
from
the
co
mm
unit
y as
par
t of t
he
Car
diov
ascu
lar
Hea
lth
Stud
y
Sign
ific
ant
pred
icto
r of
A
D u
p to
3.5
yea
rs
prio
r to
dia
gnos
is
Schm
idtk
e &
H
erm
enei
t (20
07)
CE
RA
D n
amin
gM
CI
(n=
88),
75
of w
hom
w
ere
avai
labl
e fo
r fo
llow
-up
Pet
erse
n cr
iter
iaM
emor
y C
linic
Non
conv
erte
rs=
conv
erte
rs
Smal
l et
al. (
2000
)N
amin
g su
bsec
tion
of
Sw
edis
h M
MSE
Non
dem
ente
d el
derl
y (n
=56
9), 7
3 of
who
m w
ent
on t
o de
velo
p A
D
DSM
-III
-RSu
bjec
ts p
arti
cipa
ting
in
Kun
gsho
lmen
pro
ject
w
ho w
ere
not
dem
ente
d at
fir
st f
ollo
w-u
p (s
ee S
mal
l et
al.,
1997
)
Non
conv
erte
rs=
conv
erte
rs
Swai
nson
et
al.
(200
1)G
NT
New
sem
anti
c ba
tter
y na
min
g te
st
NE
(n
=39
)Q
D (
n=
43)
mild
AD
(n
=26
)M
D (
n=
37)
AD
: NIN
CD
S-A
DR
DA
cri
teri
aM
D: D
SM-I
VQ
D: m
emor
y im
pair
men
t bu
t no
t m
eeti
ng c
rite
ria
for
dem
enti
a or
de
pres
sion
Mem
ory
clin
ic,
Add
enbr
ooke
’s
Hos
pita
l; P
sych
iatr
y D
epar
tmen
t, W
est
Suff
olk
Hos
pita
l; M
enta
l Hea
lth
Serv
ices
, A
dden
broo
ke’s
NH
S T
rust
AD
< Q
D+
MD
+N
E o
n bo
th m
easu
res
QD
< M
D+
NE
on
sem
anti
c na
min
gN
o si
gnif
ican
t co
rrel
atio
n be
twee
n ba
selin
e pe
rfor
man
ce
and
MM
SE d
eclin
e in
Q
D in
divi
dual
s
(Con
tinu
ed)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

548
AP
PE
ND
IX B
(C
ontin
ued)
Aut
hors
Tes
t us
edG
roup
s+sa
mpl
e si
zes
Dia
gnos
tic
crit
eria
R
ecru
itm
ent
proc
edur
eS
igni
fica
nt e
ffec
tsE
ffec
t si
zes
(Coh
en’s
d)
Tab
ert
et a
l. (2
006)
BN
T (
15-i
tem
ve
rsio
n)N
E (
n=
83)
Age
≥40
; cog
niti
ve im
pair
men
t fo
r 6
mon
ths-
10 y
ears
; CD
R 0
–0.5
.F
or m
emor
y: M
MSE
, SR
T,
WA
IS–R
per
form
ance
IQ
.If
no
form
al c
ogni
tive
def
icit
: su
bjec
tive
mem
ory
decl
ine,
po
siti
ve s
core
on
1 or
mor
e of
the
fi
rst
8 it
ems
of t
he m
odif
ied
Ble
ssed
Fun
ctio
nal A
ctiv
ity
Scal
e.
Mem
ory
diso
rder
s cl
inic
; N
E r
ecru
ited
by
adve
rtis
emen
t
NE
> M
CI
NE
vs.
MC
I: 0
.43
MC
I (n
=14
8)no
ncon
vert
ers
>
conv
erte
rsN
onco
nver
ters
vs.
co
nver
ters
: 0.6
7
Tes
ta e
t al
. (20
04)
BN
TN
E (
n=
409)
cons
ensu
s am
ong
beha
vior
al
neur
olog
ists
, clin
ical
ne
urop
sych
olog
ists
, nur
ses,
and
ps
ycho
met
rist
s; C
DR
& D
RS
Com
mun
ity
(sub
ject
s re
ceiv
ing
gene
ral m
edic
al
care
at
May
o C
linic
) A
ND
May
o A
lzhe
imer
’s
Dis
ease
Cen
ter)
Non
dem
ente
d >
inci
dent
A
D, b
ut n
o ad
ded
diag
nost
ic u
tilit
y on
ce
dela
yed
reca
ll ef
fect
s in
clud
ed in
the
mod
el
MC
Is (
n=
67)
AD
s (n
=30
6)
Tho
mps
on e
t al
. (2
002)
GN
TN
E (
n=
31)
qAD
: com
plai
nts
of e
piso
dic
mem
ory
impa
irm
ent
but
no
dem
enti
aA
D: N
INC
DS-
AD
RD
A c
rite
ria
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
H
ospi
tal,
Cam
brid
ge
GN
T: N
E=
qAD
> A
DG
FN
TqA
D (
n=
28)
GF
NT
: NE
> q
AD
> A
DA
D (
n=
31)
6 of
7 c
onve
rter
s at
1–2
ye
ars
show
ed
impa
irm
ent
on G
FN
T;
17 o
f 21
non
conv
erte
rs
scor
ed n
orm
ally
Tou
chon
& R
itch
ie
(199
9)ob
ject
nam
ing
subt
est
of E
CO
NE
(n
=15
0)de
men
tia:
DSM
-III
-R A
D:
NIN
CD
S-A
DR
DA
cri
teri
aG
ener
al p
ract
itio
ner
recr
uitm
ent
netw
ork
Nam
ing
not
a pr
edic
tor
of in
cide
nt d
emen
tia
2 ye
ars
prio
r to
ons
etno
ndem
ente
d el
derl
y (n
=35
9),
22 o
f w
hom
dev
elop
ed A
D
in 3
rd y
ear
Vog
el e
t al
. (20
05)
Nam
ing
of 3
0 co
lore
d lin
e dr
awin
gs o
f co
mm
on o
bjec
ts in
6
cate
gori
es
NE
(n
=58
)A
D: N
INC
DS-
AD
RD
A c
rite
ria
Rec
ruit
ed f
rom
ref
erra
ls t
o th
e C
open
hage
n U
nive
rsit
y H
ospi
tal
Mem
ory
Clin
ic
NE
=pr
edem
enti
a A
D >
A
Dpr
edem
enti
a A
D (
n=
22)
pred
emen
tia
AD
: Pet
erse
n cr
iter
ia+
subs
eque
nt p
rogr
essi
on
to A
D (
10–3
0 m
onth
s la
ter)
mild
AD
(n
=10
2)
Not
e. E
ffec
t si
zes
are
repo
rted
whe
re p
ossi
ble.
AA
CD
=ag
e-as
soci
ated
cog
niti
ve d
eclin
e. A
AC
D-m
=ag
e-as
soci
ated
cog
niti
ve d
eclin
e—m
odif
ied.
AA
MI=
age-
asso
ciat
ed m
emor
y im
pair
men
t.A
D=
Alz
heim
er’s
dis
ease
. B
NT
=B
osto
n N
amin
g T
est.
CA
MC
OG
= C
ambr
idge
Cog
niti
ve E
xam
inat
ion.
CD
R=
Clin
ical
Dem
enti
a R
atin
g Sc
ale.
CE
RA
D=
Con
sort
ium
to
Est
ablis
h a
Reg
istr
y fo
rA
lzhe
imer
’s D
isea
se.
CV
D=
cere
brov
ascu
lar
dise
ase.
EC
O =
Eva
luat
ion
Cog
niti
ve p
ar O
rdin
ateu
r [C
ompu
teri
zed
Cog
niti
ve E
valu
atio
n].
FT
D=
fron
tote
mpo
ral
dem
enti
a. G
FN
T=
Gra
ded
Fac
esT
est,
nam
ing
com
pone
nt. G
NT
=G
rade
d N
amin
g T
est.
iAD
=in
cipi
ent
AD
. IM
I=is
olat
ed m
emor
y im
pair
men
t. L
BD
=L
ewy
body
dem
enti
a. M
CI=
mild
cog
niti
ve im
pair
men
t. M
CI-
A=
MC
I-am
nest
ic.
MC
I-M
D=
MC
I-m
ulti
ple
dom
ain.
MC
I-SD
=M
CI-
sing
le d
omai
n. M
D=
maj
or d
epre
ssio
n. M
MSE
=M
ini
Men
tal
Stat
e E
xam
inat
ion.
NE
=no
rmal
eld
erly
. N
INC
DS-
AD
RD
A=
Nat
iona
l In
stit
ute
ofN
euro
logi
cal
and
Com
mun
icat
ive
Dis
orde
rs.
PN
=pi
ctur
e na
min
g. q
AD
=qu
esti
onab
le A
D.
QD
=qu
esti
onab
le d
emen
tia.
SM
L=
subj
ecti
ve m
emor
y lo
ss.
STE
P =
Ste
pwis
e C
ompa
rati
ve S
tatu
sA
naly
sis.
SR
T =
Bus
cke
Sele
ctiv
e R
emin
ding
Tes
t. u
AD
=un
cert
ain
AD
. VaD
=va
scul
ar d
emen
tia.
VC
I=va
scul
ar c
ogni
tive
impa
irm
ent.
WA
IS-R
=W
echs
ler
Adu
lt I
ntel
ligen
ce S
cale
–Rev
ised
.
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

549
AP
PE
ND
IX C
Pub
lishe
d st
udie
s re
port
ing
perf
orm
ance
of M
CI a
nd p
recl
inic
al A
D in
divi
dual
s on
sta
ndar
dize
d te
sts
othe
r th
an v
erba
l flu
ency
or
nam
ing
Aut
hors
Tes
t us
edG
roup
s+sa
mpl
e si
zes
Dia
gnos
tic
crit
eria
Rec
ruit
men
t pr
oced
ure
Sig
nifi
cant
eff
ects
Eff
ect
size
s
Adl
am e
t al
. (20
06)
Wor
d–pi
ctur
e m
atch
ing;
co
ncre
te &
abs
trac
t w
ord
syno
nym
tes
t (W
arri
ngto
n et
al.,
19
98)
NE
(n
=30
)M
CI
(n=
10)
mild
AD
(n
=11
)
MC
I: P
eter
sen
crit
eria
AD
: N
INC
DS-
AD
RD
A c
rite
ria
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
H
ospi
tal,
Cam
brid
ge
NE
=M
CI
> A
D o
n al
l tas
ksM
CI
vs. A
D: w
ord–
pict
ure
mat
chin
g, 1
.14
conc
rete
wor
d sy
nony
m t
est,
1.
07ab
stra
ct w
ord
syno
nym
tes
t,
0.54
Agg
arw
al e
t al
. (2
005)
ER
VT
(15
item
s;
Eks
trom
et
al.,
1976
)M
CI
(n=
218)
, 82
of
who
m d
evel
oped
AD
MC
I: C
ogni
tive
impa
irm
ent
but
do n
ot m
eet
NIN
CD
S–A
DR
DA
cri
teri
a fo
r de
men
tia
Cat
holic
cle
rgy
who
ag
reed
to
part
icip
ate
Red
uced
sem
anti
c m
emor
y (c
ompo
site
sco
re o
f B
NT
, E
xten
ded
Ran
ge
Voc
abul
ary,
NA
RT
) pr
edic
ted
AD
(re
lati
ve
risk
=0.
62);
how
ever
, ep
isod
ic m
emor
y im
pair
men
t st
rong
er
pred
icto
r
NA
RT
(20
item
s;
Nel
son,
198
2)A
D: N
INC
DS-
AD
RD
A
crit
eria
Art
ero
et a
l. (2
003)
Wor
d an
d sy
ntax
com
preh
ensi
on12
8 in
divi
dual
s w
ith
cogn
itiv
e di
ffic
ulti
esC
ogni
tive
dif
ficu
ltie
s as
cert
aine
d us
ing
the
Det
erio
rati
onC
ogni
tive
Obs
ervé
e (D
EC
O)
scre
enin
g in
stru
men
t (R
itch
ie &
Fuh
rer,
199
2)
Iden
tifi
ed v
ia a
reg
iona
l ge
nera
l pra
ctit
ione
r ne
twor
k
Wor
d an
d sy
ntax
co
mpr
ehen
sion
not
in
clud
ed in
bes
t pr
edic
tive
mod
el f
or A
D
Ben
nett
et
al. (
2002
)C
ompl
ex id
eati
onal
m
ater
ial,
ER
VT
NA
RT
NE
(n
=58
7)M
CI
(n=
211)
Cog
niti
ve im
pair
men
t, b
ut
does
not
mee
t ac
cept
ed
crit
eria
for
dem
enti
a
Cat
holic
cle
rgy
who
ag
reed
to
part
icip
ate
Com
posi
te s
core
of
sem
anti
c m
emor
y: N
E >
MC
IR
ate
of d
eclin
e: M
CI
> N
E
ER
VT
: 0.4
6N
AR
T: 0
.42
Bla
ckw
ell e
t al
. (2
004)
NA
RT
Subj
ecti
ve/ o
bjec
tive
m
emor
y lo
ss (n
=43
),
11 o
f w
hom
de
velo
ped
AD
w
ithi
n 32
mon
ths
norm
al p
erfo
rman
ce o
n te
sts
of la
ngua
ge a
nd
visu
ospa
tial
fun
ctio
n,
pres
erve
d ac
tivi
ties
of
daily
life
, CD
R=
0.5
Mem
ory
clin
icN
onco
nver
ters
=co
nver
ters
Bsc
hor
et a
l. (2
001)
Coo
kie
The
ft P
ictu
reN
E (n
=40
)M
CI
(n=
34)
mild
AD
(n
=21
)m
oder
ate
to s
ever
e A
D
(n=
20)
ICD
-10
crit
eria
(Z
audi
g,
1992
)M
emor
y cl
inic
, Dep
t. o
f G
eron
tolo
gy, F
reie
U
nive
rsit
ät B
erlin
NE
/MC
I >
AD
on
“per
sons
an
d ob
ject
s”, l
ocal
izat
ions
, A
ctio
ns a
nd S
um o
f m
easu
res
(Con
tinu
ed)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

550
AP
PE
ND
IX C
(C
ontin
ued)
Aut
hors
Tes
t us
edG
roup
s+sa
mpl
e si
zes
Dia
gnos
tic
crit
eria
Rec
ruit
men
t pr
oced
ure
Sig
nifi
cant
eff
ects
Eff
ect
size
s
Bus
se e
t al
. (20
03)
Com
posi
te a
phas
ia/
apra
xia
scor
e (n
amin
g ob
ject
s,
read
ing
and
obey
ing
a se
nten
ce, w
riti
ng a
se
nten
ce, a
nd
perf
orm
ing
a th
ree-
stag
e co
mm
and)
nond
emen
ted
elde
rly
(n=
1045
), 3
% o
f w
hom
met
the
crit
eria
for
MC
I-A
, 36
% fo
r M
MSE
≥26,
9%
for
AA
CD
and
20
% fo
r A
AC
D-m
MC
I-A
: Pet
erse
n cr
iter
iaA
AC
D: L
evy
(199
4) c
rite
ria
AA
CD
-m: L
evy
crit
eria
, but
no
req
uire
men
t fo
r su
bjec
tive
mem
ory
com
plai
ntde
men
tia:
DSM
-IV
Ran
dom
sam
plin
g fr
om
list p
rovi
ded
by th
e lo
cal
regi
stry
off
ice
in L
eipz
ig
No
grou
p di
ffer
ence
s;
lang
uage
sco
re n
ot a
si
gnif
ican
t pr
edic
tor
Cac
capo
lo-V
an V
liet
et a
l. (2
003)
BD
AE
–Rep
etit
ion
of
phra
ses
NE
(n
=23
0)Q
D (
n=
155)
mild
AD
(n
=24
4)m
oder
ate
AD
(n=
480)
seve
re A
D (
n=
376)
very
sev
ere
AD
(n
=24
7)
QD
: cog
niti
ve im
pair
men
t su
ffic
ient
or
clos
e to
su
ffic
ient
for
a d
iagn
osis
of
dem
enti
a; n
o fu
ncti
onal
im
pair
men
tA
D: N
INC
DS-
AD
RD
A
crit
eria
Mem
ory
Dis
orde
rs
Cen
ter/
recr
uite
d fo
r a
stud
y of
con
trol
s
NE
=Q
D=
mild
A
D=
mod
erat
e A
D >
se
vere
AD
> v
ery
seve
re A
D
Col
lie e
t al
. (20
02)
Synt
acti
c an
d se
man
tic
reas
onin
gE
lder
ly a
dult
s (n
=17
4),
23 o
f w
hom
wer
e im
pair
ed o
n 3
cons
ecut
ive
asse
ssm
ents
CE
RA
D b
atte
ry (
Mor
ris
et a
l., 1
988b
)R
ecru
ited
fro
m a
n on
goin
g st
udy
on a
ging
at
an
inde
pend
ent
rese
arch
inst
itut
e in
M
elbo
urne
, Aus
tral
ia
Synt
acti
c re
ason
ing:
% c
orre
ct
sign
ific
ant
Sem
anti
c re
ason
ing
not
sign
ific
ant
Synt
acti
c re
ason
ing:
0.1
4
Cro
ot e
t al
. (19
99)
TR
OG
Wor
d–pi
ctur
e m
atch
ing
(Hod
ges
& P
atte
rson
, 19
95)
PP
T
NE
(n
=46
)m
inim
al A
D (
n=
16)
mild
AD
(n
=16
)m
oder
ate
AD
(n=
14)
NIN
CD
S-A
DR
DA
cri
teri
a;
min
imal
: MM
SE=
24–3
0m
ild: M
MSE
=18
–23
mod
erat
e: M
MSE
=2–
17
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
H
ospi
tal,
Cam
brid
ge
TR
OG
, blo
cks
corr
ect:
NE
>
min
imal
=m
ild >
mod
erat
eT
RO
G, i
tem
s co
rrec
t: N
E >
m
ild >
mod
erat
e,
min
imal
=m
ildsy
ntac
tic
mis
inte
rpre
tati
ons
acco
unte
d fo
r m
ore
erro
rs
than
exp
ecte
d by
cha
nce
othe
r ta
sks:
p-v
alue
not
re
port
edD
e Ja
ger
& B
udge
(2
005)
syno
nym
s te
st
(War
ring
ton
et a
l., 1
998)
Bas
elin
e:N
E (
n=
117)
MC
I (n
=40
)3-
year
fol
low
up:
NE
(n
=85
)M
CI
(n=
49)
MC
I: >
1.5
SD
bel
ow c
ontr
ol
mea
n on
mem
ory
test
ing
Tal
ks/r
adio
adv
erti
sing
in
Oxf
ords
hire
for
tho
se
who
tho
ught
tha
t th
eir
heal
th, m
emor
y an
d th
inki
ng w
ere
good
co
mpa
red
to t
hat
of
thei
r pe
ers
Cla
ssif
icat
ion
at 4
yea
rs n
ot
pred
icte
d by
syn
onym
s te
st
De
Jage
r et
al.
(200
3)T
oken
Tes
tN
E (n
=51
)M
CI
(n=
29)
AD
(n
=60
)V
CI
(n=
8)V
aD (
n=
4)
MC
I: P
eter
sen
crit
eria
AD
: N
INC
DS-
AD
RD
A c
rite
ria
VC
I: H
achi
nski
cri
teri
aV
aD: N
INC
DD
S/A
IRE
N
crite
ria
(G. G
old
et a
l., 1
997)
Par
tici
pant
s wer
e re
crui
ted
from
the
Oxf
ord
Pro
ject
T
o In
vest
igat
e M
emor
y an
d A
gein
g (O
PT
IMA
) st
udy
NE
=M
CI
> A
DM
CI
vs. A
D: 0
.6V
aD a
lso
exhi
bite
d de
fici
tsN
E v
s. C
VD
(V
aD+
VC
I):
1.03
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009
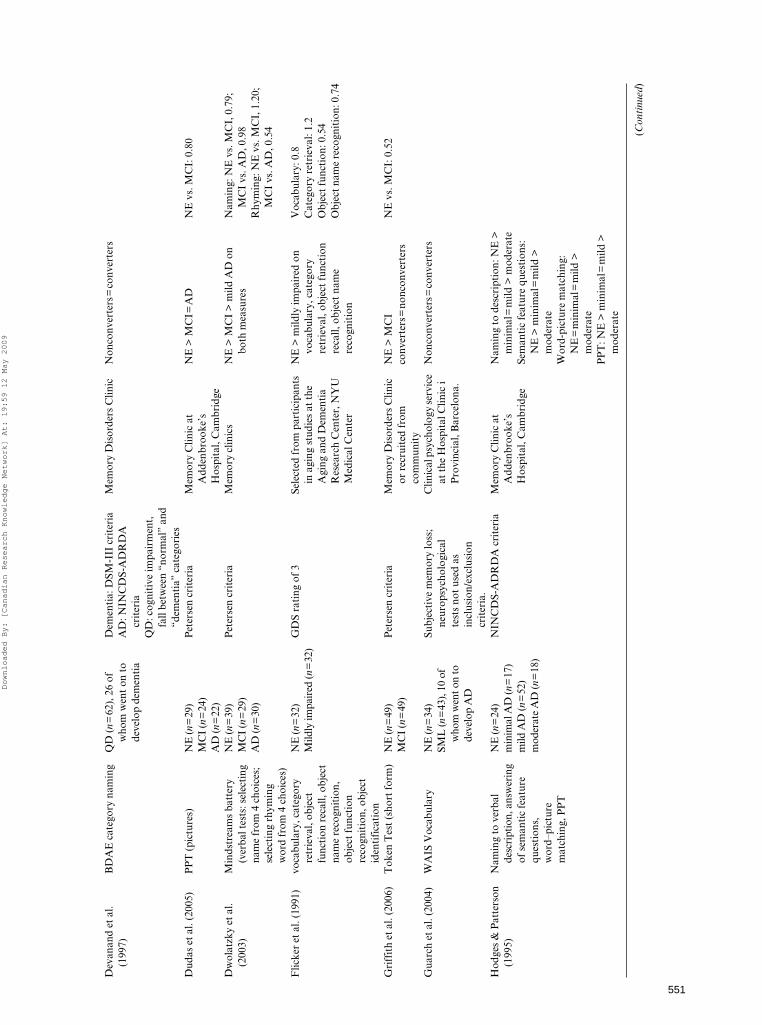
551
Dev
anan
d et
al.
(199
7)B
DA
E c
ateg
ory
nam
ing
QD
(n
=62
), 2
6 of
w
hom
wen
t on
to
deve
lop
dem
enti
a
Dem
enti
a: D
SM-I
II c
rite
ria
AD
: NIN
CD
S-A
DR
DA
cr
iter
iaQ
D: c
ogni
tive
impa
irm
ent,
fa
ll be
twee
n “n
orm
al”
and
“dem
enti
a” c
ateg
orie
s
Mem
ory
Dis
orde
rs C
linic
Non
conv
erte
rs=
conv
erte
rs
Dud
as e
t al
. (20
05)
PP
T (
pict
ures
)N
E (n
=29
)M
CI
(n=
24)
AD
(n=
22)
Pet
erse
n cr
iter
iaM
emor
y C
linic
at
Add
enbr
ooke
’s
Hos
pita
l, C
ambr
idge
NE
> M
CI=
AD
NE
vs.
MC
I: 0
.80
Dw
olat
zky
et a
l. (2
003)
Min
dstr
eam
s ba
tter
y (v
erba
l tes
ts: s
elec
ting
na
me
from
4 c
hoic
es;
sele
ctin
g rh
ymin
g w
ord
from
4 c
hoic
es)
NE
(n=
39)
MC
I (n
=29
)A
D (n
=30
)
Pet
erse
n cr
iter
iaM
emor
y cl
inic
sN
E >
MC
I >
mild
AD
on
both
mea
sure
sN
amin
g: N
E v
s. M
CI,
0.7
9;
MC
I vs
. AD
, 0.9
8R
hym
ing:
NE
vs.
MC
I, 1
.20;
M
CI
vs. A
D, 0
.54
Flic
ker
et a
l. (1
991)
voca
bula
ry, c
ateg
ory
retr
ieva
l, ob
ject
fu
ncti
on r
ecal
l, ob
ject
na
me
reco
gnit
ion,
ob
ject
fun
ctio
n re
cogn
itio
n, o
bjec
t id
enti
fica
tion
NE
(n=
32)
Mild
ly im
pair
ed (n
=32
)G
DS
rati
ng o
f 3
Sele
cted
fro
m p
arti
cipa
nts
in a
ging
stu
dies
at
the
Agi
ng a
nd D
emen
tia
Res
earc
h C
ente
r, N
YU
M
edic
al C
ente
r
NE
> m
ildly
impa
ired
on
voca
bula
ry, c
ateg
ory
retr
ieva
l, ob
ject
fun
ctio
n re
call,
obj
ect
nam
e re
cogn
itio
n
Voc
abul
ary:
0.8
Cat
egor
y re
trie
val:
1.2
Obj
ect
func
tion
: 0.5
4O
bjec
t nam
e re
cogn
itio
n: 0
.74
Gri
ffit
h et
al.
(200
6)T
oken
Tes
t (s
hort
for
m)
NE
(n=
49)
MC
I (n
=49
)P
eter
sen
crit
eria
Mem
ory
Dis
orde
rs C
linic
or
rec
ruit
ed f
rom
co
mm
unit
y
NE
> M
CI
NE
vs.
MC
I: 0
.52
conv
erte
rs=
nonc
onve
rter
s
Gua
rch
et a
l. (2
004)
WA
IS V
ocab
ular
yN
E (n
=34
)SM
L (n
=43
), 1
0 of
w
hom
wen
t on
to
deve
lop
AD
Subj
ecti
ve m
emor
y lo
ss;
neur
opsy
chol
ogic
al
test
s no
t us
ed a
s in
clus
ion/
excl
usio
n cr
iter
ia.
Clin
ical
psy
chol
ogy
serv
ice
at t
he H
ospi
tal C
linic
i P
rovi
ncia
l, B
arce
lona
.
Non
conv
erte
rs=
conv
erte
rs
Hod
ges
& P
atte
rson
(1
995)
Nam
ing
to v
erba
l de
scri
ptio
n, a
nsw
erin
g of
sem
anti
c fe
atur
e qu
esti
ons,
w
ord–
pict
ure
mat
chin
g, P
PT
NE
(n=
24)
min
imal
AD
(n=
17)
mild
AD
(n=
52)
mod
erat
e A
D (n
=18
)
NIN
CD
S-A
DR
DA
cri
teri
aM
emor
y C
linic
at
Add
enbr
ooke
’s
Hos
pita
l, C
ambr
idge
Nam
ing
to d
escr
ipti
on: N
E >
m
inim
al=
mild
> m
oder
ate
Sem
anti
c fe
atur
e qu
esti
ons:
N
E >
min
imal
=m
ild >
m
oder
ate
Wor
d-pi
ctur
e m
atch
ing:
N
E=
min
imal
=m
ild >
m
oder
ate
PP
T: N
E >
min
imal
=m
ild >
m
oder
ate
(Con
tinu
ed)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009
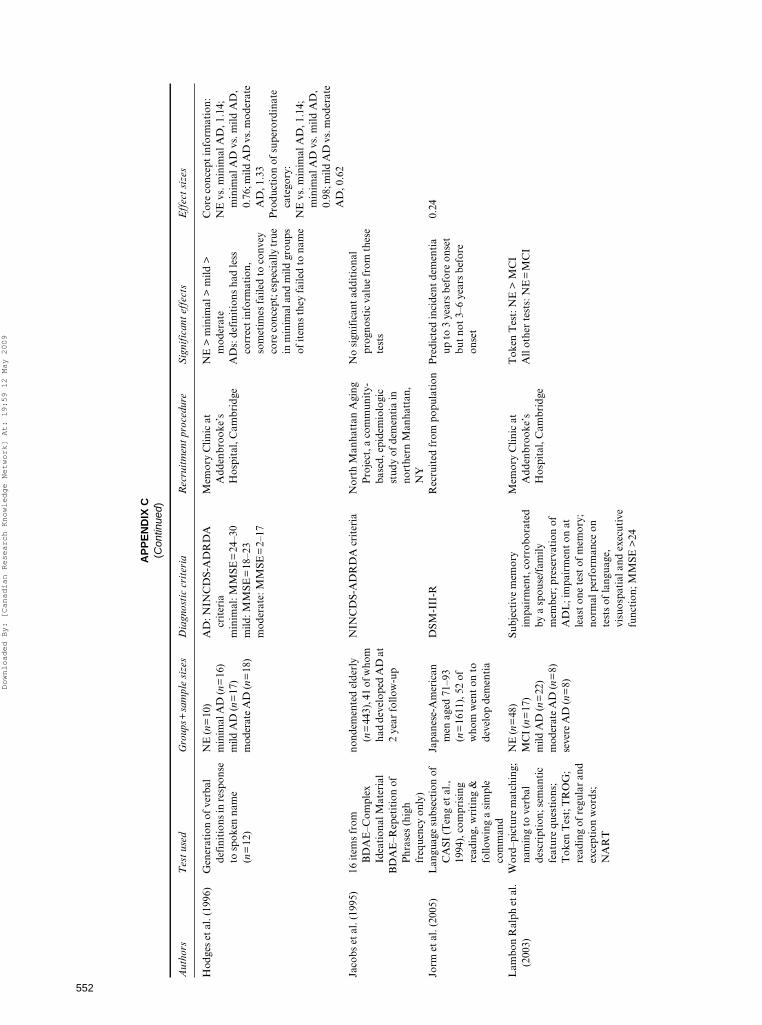
552
AP
PE
ND
IX C
(C
ontin
ued)
Aut
hors
Tes
t us
edG
roup
s+sa
mpl
e si
zes
Dia
gnos
tic
crit
eria
Rec
ruit
men
t pr
oced
ure
Sig
nifi
cant
eff
ects
Eff
ect
size
s
Hod
ges
et a
l. (1
996)
Gen
erat
ion
of v
erba
l de
fini
tion
s in
res
pons
e to
spo
ken
nam
e (n
=12
)
NE
(n=
10)
min
imal
AD
(n=
16)
mild
AD
(n=
17)
mod
erat
e A
D (n
=18
)
AD
: NIN
CD
S-A
DR
DA
cr
iter
iam
inim
al: M
MSE
=24
–30
mild
: MM
SE=
18–2
3m
oder
ate:
MM
SE=
2–17
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
H
ospi
tal,
Cam
brid
ge
NE
> m
inim
al >
mild
>
mod
erat
eC
ore
conc
ept
info
rmat
ion:
NE
vs.
min
imal
AD
, 1.1
4;
min
imal
AD
vs.
mild
AD
, 0.
76; m
ild A
D v
s. m
oder
ate
AD
, 1.3
3P
rodu
ctio
n of
sup
eror
dina
te
cate
gory
:N
E v
s. m
inim
al A
D, 1
.14;
m
inim
al A
D v
s. m
ild A
D,
0.98
; mild
AD
vs.
mod
erat
e A
D, 0
.62
AD
s: d
efin
itio
ns h
ad le
ss
corr
ect
info
rmat
ion,
so
met
imes
fai
led
to c
onve
y co
re c
once
pt; e
spec
ially
true
in
min
imal
and
mild
gro
ups
of it
ems
they
fai
led
to n
ame
Jaco
bs e
t al
. (19
95)
16 it
ems
from
B
DA
E–C
ompl
ex
Idea
tion
al M
ater
ial
BD
AE
–Rep
etit
ion
of
Phr
ases
(hi
gh
freq
uenc
y on
ly)
nond
emen
ted
elde
rly
(n=
443)
, 41
of w
hom
ha
d de
velo
ped
AD
at
2 ye
ar f
ollo
w-u
p
NIN
CD
S-A
DR
DA
cri
teri
aN
orth
Man
hatt
an A
ging
P
roje
ct, a
com
mun
ity-
base
d, e
pide
mio
logi
c st
udy
of d
emen
tia
in
nort
hern
Man
hatt
an,
NY
No
sign
ific
ant
addi
tion
al
prog
nost
ic v
alue
from
the
se
test
s
Jorm
et
al. (
2005
)L
angu
age
subs
ecti
on o
f C
ASI
(T
eng
et a
l.,
1994
), c
ompr
isin
g re
adin
g, w
riti
ng &
fo
llow
ing
a si
mpl
e co
mm
and
Japa
nese
-Am
eric
an
men
age
d 71
–93
(n=
1611
), 5
2 of
w
hom
wen
t on
to
deve
lop
dem
enti
a
DSM
-III
-RR
ecru
ited
fro
m p
opul
atio
nP
redi
cted
inci
dent
dem
enti
a up
to
3 ye
ars
befo
re o
nset
bu
t no
t 3–
6 ye
ars
befo
re
onse
t
0.24
Lam
bon
Ral
ph e
t al.
(200
3)W
ord–
pict
ure
mat
chin
g;
nam
ing
to v
erba
l de
scri
ptio
n; s
eman
tic
feat
ure
ques
tion
s;
Tok
en T
est;
TR
OG
; re
adin
g of
reg
ular
and
ex
cept
ion
wor
ds;
NA
RT
NE
(n=
48)
MC
I (n
=17
)m
ild A
D (n
=22
) m
oder
ate
AD
(n=
8)se
vere
AD
(n=
8)
Subj
ecti
ve m
emor
y im
pair
men
t, c
orro
bora
ted
by a
spo
use/
fam
ily
mem
ber;
pre
serv
atio
n of
A
DL
; im
pair
men
t on
at
leas
t on
e te
st o
f m
emor
y;
norm
al p
erfo
rman
ce o
n te
sts
of la
ngua
ge,
visu
ospa
tial
and
exe
cuti
ve
func
tion
; MM
SE >
24
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
H
ospi
tal,
Cam
brid
ge
Tok
en T
est:
NE
> M
CI
All
othe
r te
sts:
NE
=M
CI
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

553
Lóp
ez e
t al
. (20
06)
AM
NA
RT
NE
(n=
374)
MC
I-A
(n=
10)
MC
I-M
D (n
=28
)
MC
I-A
: >1.
5 S
Ds
belo
w
cont
rols
in d
elay
ed
reca
ll+
decl
ine
in c
ogni
tive
fu
ncti
onin
g; M
CI-
MD
; >
1.5
SD
s in
at
leas
t on
e co
gnit
ive
dom
ain
othe
r th
an m
emor
y/on
e ab
norm
al t
est
in ≥
2 do
mai
ns.
5,20
1 no
nins
titu
tion
aliz
ed
indi
vidu
als
over
65;
re
crui
ted
from
fou
r co
mm
unit
ies
usin
g P
art
A M
edic
are
list
in
1988
–198
9; 6
87 A
fric
an-
Am
eric
ans
recr
uite
d in
sa
me
man
ner
in
1992
–199
3
NE
=M
CI-
A >
MC
I-M
DN
E v
s. M
CI-
MD
: 0.9
5M
CI-
MD
vs.
MC
I-A
: 1.8
0
Mar
cos
et a
l. (2
006)
CA
MC
OG
Lan
guag
e su
btes
tP
MC
I (n
=38
)M
CI:
Pet
erse
n cr
iter
iaR
efer
red
by n
euro
logi
sts
or g
eria
tric
spe
cial
ists
Voc
abul
ary:
PM
CI=
SMC
IL
angu
age:
1.0
9
WA
IS V
ocab
ular
ySM
CI
(n=
44)
AD
: NIN
CD
S-A
DR
DA
cr
iter
iaL
angu
age:
PM
CI
< S
MC
I Se
nsit
ivit
y=
79%
. Sp
ecif
icit
y=
61%
Mas
ur e
t al
. (19
94)
WA
IS V
ocab
ular
y (W
echs
ler,
195
5)N
onde
men
ted
elde
rly
(n=
317)
, 64
of w
hom
de
velo
ped
AD
in a
fo
llow
-up
of a
t lea
st 4
ye
ars
DSM
-III
, N
INC
DS-
AD
RD
A c
rite
ria
Rec
ruit
ed f
rom
co
mm
unit
yN
ot a
sig
nifi
cant
pre
dict
or
Meg
uro
et a
l. (2
004)
Lan
guag
e su
bsec
tion
of
CA
SI (
Ten
g et
al.,
19
94),
com
pris
ing
read
ing,
wri
ting
&
follo
win
g a
sim
ple
com
man
d
NE
(n=
968)
CD
R 0
.5, A
D (n
=95
)C
DR
O.5
, UD
(n=
94)
CD
R 0
.5, I
D (n
=22
7)C
DR
0.5
, oth
ers
(n=
37)
CD
R 1
and
2 (n
=80
)
UD
: onl
y m
emor
y is
impa
ired
ID: i
mpa
irm
ent
in m
emor
y an
d ≤2
oth
er c
ogni
tive
do
mai
nsO
ther
s: im
pair
men
t in
m
emor
y an
d ≥3
oth
er
cogn
itiv
e do
mai
nsD
emen
tia:
DSM
-III
-R
All
olde
r re
side
nts
in T
ajir
i w
ere
targ
eted
CD
R 0
< C
DR
0.5
<
CD
R <
1 a
nd 2
CD
R 0
.5 (
AD
vs.
UD
): 0
.72
CD
R 0
.5 (
DA
T)
< U
D a
nd I
DC
DR
0.5
(A
D v
s. I
D):
0.37
Mey
er e
t al
. (20
02)
MM
SEM
CI
(n=
73),
35
of
who
m d
evel
oped
A
D a
nd 1
5 of
who
m
deve
lope
d V
aD
duri
ng a
n av
erag
e of
3.
88 y
ears
of f
ollo
w-u
p
MM
SE >
1 S
D b
elow
mea
n fo
r ag
e &
edu
cati
on;
mem
ory
com
plai
nts;
no
dem
enti
a
Vol
unte
ers
enro
lled
in
long
itud
inal
stu
dies
of
agin
g an
d de
men
tia
thro
ugh
Bay
lor
Col
lege
of
Med
icin
e
No
grou
p ef
fect
s
Nes
tor
et a
l. (2
003)
PP
T (
pict
ure
vers
ion)
NE
(n=
15)
MC
I (n
=10
)A
D (n
=10
)
MC
I: in
sidi
ous
onse
t mem
ory
sym
ptom
s, o
bjec
tive
m
emor
y im
pair
men
t, n
o ot
her
sign
ific
ant
defi
cits
AD
: NIN
CD
S-A
DR
DA
cr
iter
ia
Mem
ory
clin
icM
CI
> A
D
(Con
tinu
ed)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

554
AP
PE
ND
IX C
(C
ontin
ued)
Aut
hors
Tes
t us
edG
roup
s+sa
mpl
e si
zes
Dia
gnos
tic
crit
eria
Rec
ruit
men
t pr
oced
ure
Sig
nifi
cant
eff
ects
Eff
ect
size
s
Nor
dlun
d et
al.
(200
5)T
oken
Tes
tA
SLD
rep
etit
ion
(Cro
sson
, 199
6)
Tok
en T
est:
NE
(n=
35)
MC
I (n
=11
0)A
SLD
rep
etiti
on:
NE
(n=
31)
MC
I (n
=86
)
Subj
ecti
ve a
nd o
bjec
tive
m
emor
y im
pair
men
t >
6
mon
ths;
pos
itiv
e ou
tcom
e on
ste
pwis
e co
mpa
rati
ve
stat
us a
naly
sis
(ST
EP
, W
allin
et
al.,
1996
), I
-Fle
x (R
oyal
l et
al.,
1992
),
MM
SE o
r C
DR
; MM
SE
≥25;
not
mor
e th
an 2
+ve
ou
tcom
es o
n ST
EP
Mem
ory
clin
icN
E >
MC
I in
bot
h te
sts
Tok
en T
est:
0.7
3
ASL
D: 0
.75
Pyo
et
al. (
2006
)A
DA
S-C
og L
angu
age,
C
ompr
ehen
sion
and
W
ord-
Fin
ding
D
iffi
cult
y ta
sks
NE
(n=
843)
unce
rtai
n/M
CI
(n=
135)
AD
, CD
R=
0.5
(n=
30)
AD
, CD
R=
1 (n
=12
5)
MC
I: C
DR
=0.
5, m
emor
y lo
ss b
ut n
o de
men
tia
Med
ia a
ppea
lsL
angu
age:
NE
< M
CI=
AD
(CD
R 0
.5) <
A
D (
CD
R 1
)C
ompr
ehen
sion
:N
E <
MC
I <
AD
(C
DR
0.
5)=
AD
(C
DR
1)
Wor
d-fi
ndin
g di
ffic
ulty
:N
E <
MC
I <
AD
(C
DR
1)
<
AD
(C
DR
0.5
)
Lan
guag
e:N
E v
s. M
CI,
0.7
3A
D (
0.5)
vs.
AD
(1)
, 0.0
8C
ompr
ehen
sion
: NE
vs.
M
CI,
0.5
3M
CI
vs. A
D 0
.5, 0
.53
Wor
d fi
ndin
g di
ffic
ulty
:N
E v
s. M
CI,
0.4
7M
CI
vs. A
D (
1), 0
.24
AD
(1)
vs.
AD
(0.
5), 0
.12
Rib
eiro
et
al. (
2006
)M
odif
ied
vers
ion
of
Tok
en T
est
from
B
atte
ry o
f L
isbo
n fo
r th
e A
sses
smen
t of
Dem
enti
a
NE
(n=
63)
MC
I (n
=11
6)Su
bjec
tive
mem
ory
com
plai
nts;
≥1.
5 S
D
belo
w n
orm
al o
n de
laye
d re
call;
pre
serv
ed A
DL
; m
aint
aine
d pr
ofes
sion
al,
soci
al a
nd f
amili
al
acti
viti
es, s
core
<3
on t
he
firs
t pa
rt o
f th
e B
less
ed
Dem
enti
a Sc
ale;
pre
serv
ed
gene
ral c
ogni
tive
fun
ctio
n.
Dem
enti
a O
utpa
tien
t C
linic
, Hos
pita
l San
ta
Mar
ia, a
nd a
Mem
ory
Clin
ic, L
isbo
n
33.7
% o
f MC
I pa
tien
ts h
ad a
n im
pair
men
t in
the
Tok
en
Tes
t (<
1.5
SD
bel
ow m
ean
for
age
& e
duca
tion
)
Ric
hard
s et
al.
(199
9)E
co w
ord
com
preh
ensi
on
subt
est
(RT
mea
sure
s)11
1 in
divi
dual
s,
clas
sifi
ed a
s N
E
(n=
74),
AA
MI
(n=
37),
or
AA
CD
(n
=39
).
AA
MI:
mem
ory
impa
irm
ent,
no
dem
enti
aA
AC
D: i
mpa
irm
ent
in o
ne
dom
ain:
mem
ory/
lear
ning
, at
tent
ion/
con
cent
rati
on,
visu
ospa
tial
rea
soni
ng,
lang
uage
, vis
uosp
atia
l fu
ncti
on
Ran
dom
ly r
ecru
ited
fro
m
600
gene
ral m
edic
al
prac
tice
s in
sou
ther
n F
ranc
e
NE
> A
AC
D
NE
> A
AM
IA
AM
I: 0
.57
AA
CD
: 1.0
4
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

555
Sacu
iu e
t al
. (20
05)
Syno
nym
tes
t (i
dent
ify
syno
nym
am
ongs
t 5
alte
rnat
ives
)
nond
emen
ted
elde
rly
(n=
313)
, 58
of w
hom
w
ent
on t
o de
velo
p A
D in
3 y
ears
Dem
enti
a: D
SM-I
I-R
AD
: NIN
CD
S-A
DR
DA
cr
iter
ia
All
indi
vidu
als
born
in
1901
–190
2 in
G
othe
nbur
g,
Swed
en w
ere
invi
ted
to p
arti
cipa
te
Pre
dict
ed a
ll de
men
tia
and
VaD
, but
not
AD
; Se
nsit
ivit
y=
68%
, sp
ecif
icit
y=
48%
, P
PV
=22
.7, N
PV
=87
.0 f
or
all d
emen
tia
Saxt
on e
t al
. (20
04)
WA
IS–R
Voc
abul
ary
nond
emen
ted
elde
rly
(n=
693)
, 72
of w
hom
de
velo
ped
AD
wit
hin
1.5–
8 ye
ars
(1.5
–3.4
ye
ars:
n=
24; 3
.5–5
.0
year
s: n
=20
; 5.1
–8.1
ye
ars:
n=
28)
NIN
CD
S-A
DR
DA
cri
teri
aSe
lect
ed f
rom
par
tici
pant
s re
crui
ted
from
the
com
-m
unit
y as
par
t of
the
C
ardi
ovas
cula
r H
ealt
h St
udy
Non
conv
erte
rs=
conv
erte
rs
Smal
l et
al. (
2000
)R
eadi
ng &
wri
ting
su
bsec
tion
s of
Sw
edis
h M
MSE
nond
emen
ted
elde
rly
(n=
569)
, 73
of w
hom
w
ent o
n to
dev
elop
A
D
DSM
-III
-RSu
bjec
ts p
arti
cipa
ting
in
Kun
gsho
lmen
pro
ject
w
ho w
ere
not
dem
ente
d at
fir
st f
ollo
w-u
p (s
ee
Smal
l et
al.,
1997
)
Non
conv
erte
rs=
conv
erte
rs
Tab
ert
et a
l. (2
006)
BD
AE
rep
etit
ion
&
com
preh
ensi
onN
E (n
=83
)M
CI
(n=
148)
Age
≥40
, cog
niti
ve im
pair
-m
ent
for
6 m
onth
s–10
ye
ars,
CD
R 0
–0.5
. For
m
emor
y: M
MSE
, SR
T,
WA
IS–R
per
form
ance
IQ
. If
no
form
al c
ogni
tive
de
fici
t: s
ubje
ctiv
e m
emor
y de
clin
e, p
osit
ive
scor
e on
1
or m
ore
of t
he f
irst
8 it
ems
of t
he m
odif
ied
Ble
ssed
F
unct
iona
l Act
ivit
y Sc
ale.
Mem
ory
diso
rder
s cl
inic
; N
E r
ecru
ited
by
adve
rtis
emen
t
NE
> M
CI
on b
oth
mea
sure
sN
onco
nver
ters
= c
onve
rter
s on
bot
h m
easu
res
Rep
etit
ion:
0.2
7 C
ompr
ehen
sion
: 0.2
0
Tho
mps
on e
t al
. (2
002)
NA
RT
NE
(n=
31)
qAD
(n=
28)
AD
(n=
31)
AD
: NIN
CD
S-A
DR
DA
cr
iter
iaqA
D: c
ompl
aint
s of
epi
sodi
c m
emor
y im
pair
men
t but
no
dem
enti
a
Mem
ory
Clin
ic a
t A
dden
broo
ke’s
H
ospi
tal,
Cam
brid
ge
NE
=qA
D=
AD
Tia
n et
al.
(200
3)F
AST
(E
nder
by e
t al
., 19
87)
QD
( n=
195)
, 135
see
n fo
r fo
llow
up a
t 24.
5 m
onth
s; 3
7 co
nver
ted
to d
emen
tia
Obj
ecti
ve e
vide
nce
of
cogn
itiv
e im
pair
men
t bu
t no
dem
enti
a
Bri
stol
Mem
ory
Dis
orde
rs
Clin
icN
onco
nver
ters
=co
nver
ters
(Con
tinu
ed)
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009

556
AP
PE
ND
IX C
(C
ontin
ued)
Aut
hors
Tes
t us
edG
roup
s+sa
mpl
e si
zes
Dia
gnos
tic
crit
eria
Rec
ruit
men
t pr
oced
ure
Sig
nifi
cant
eff
ects
Eff
ect
size
s
Tou
chon
& R
itch
ie
(199
9)M
ean
RT
on
wor
d an
d sy
ntax
com
preh
ensi
on;
read
ing
(fro
m E
CO
)
NE
(n=
150)
nond
emen
ted
elde
rly
(n=
359)
, 22
of w
hom
de
velo
ped
AD
in 3
rd
year
Dem
enti
a: D
SM-I
II-R
cr
iter
iaA
D: N
INC
DS-
AD
RD
A
crit
eria
Gen
eral
pra
ctit
ione
r re
crui
tmen
t ne
twor
kB
oth
wor
d an
d sy
ntax
co
mpr
ehen
sion
pre
dict
ed
inci
dent
dem
enti
a 2
year
s pr
ior;
inte
ract
ion
wit
h ed
ucat
ion
Rea
ding
pre
dict
ed d
emen
tia;
no
inte
ract
ion
wit
h ed
ucat
ion
Wor
d co
mpr
ehen
sion
: 1.5
7Sy
ntax
com
preh
ensi
on: 0
.97
Rea
ding
: 1.9
Van
denb
ulck
e et
al.
(200
7)A
AT
(G
raet
s et
al.,
19
92);
Ver
bal
asso
ciat
ion
test
of
the
psyc
holin
guis
tic
asse
ssm
ent
of
lang
uage
pro
cess
ing
in a
phas
ia;
spon
tane
ous
spee
ch
NE
(n
=13
)M
CI
(n=
13)
CD
R=
0.5,
mem
ory
decl
ine,
ot
her
cogn
itiv
e do
mai
ns
and
acti
viti
es o
f dai
ly li
ving
re
lati
vely
pre
serv
ed
Mem
ory
Clin
ic, U
nive
rsit
y H
ospi
tal G
asth
uisb
erg,
L
euve
n
1/13
impa
ired
(>
2 S
D b
elow
N
E m
ean)
in A
AT
(na
min
g su
btes
t), s
eman
tic
stru
ctur
e in
spo
ntan
eous
spe
ech
1/13
impa
ired
in A
AT
(au
di-
tory
wor
d-pi
ctur
e m
atch
ing
subt
est)
and
sem
anti
c st
ruc-
ture
in s
pont
aneo
us s
peec
h1/
13 im
pair
ed in
AA
T (
visu
al
wor
d-pi
ctur
e m
atch
ing
subt
est)
1/13
impa
ired
in s
ynta
ctic
st
ruct
ure
in s
pont
aneo
us
spee
chW
ang
et a
l. (2
006)
Lan
guag
e su
bsec
tion
of
CA
SI (
Ten
g et
al.,
19
94),
com
pris
ing
read
ing,
wri
ting
&
follo
win
g a
sim
ple
com
man
d
NE
(n=
20)
MC
I (n
=58
)A
D (n
=20
)
MC
I: P
eter
sen
crit
eria
AD
: NIN
CD
S-A
DR
DA
cr
iter
ia
Neu
rolo
gica
l clin
ics
NE
> A
DM
CI
> A
Dco
nver
ters
> n
onco
nver
ters
MC
I vs
. AD
: 0.4
8N
onco
nver
ters
vs.
con
vert
ers:
0.
54
Not
e. E
ffec
t si
zes
are
repo
rted
whe
re p
ossi
ble.
AA
CD
= a
ge-a
ssoc
iate
d co
gnit
ive
decl
ine.
AA
CD
-M =
age
-ass
ocia
ted
cogn
itiv
e de
clin
e-m
odif
ied.
AA
T=
Aac
hen
Aph
asie
Tes
t. A
D=
Alz
heim
er’s
dis
-ea
se.
AD
AS-
Cog
=A
lzhe
imer
Dis
ease
Ass
essm
ent
Scal
e–C
ogni
tive
sub
scal
e. A
MN
AR
T=
Am
eric
an v
ersi
on o
f N
atio
nal
Rea
ding
Tes
t. A
SLD
=A
sses
smen
t of
Sub
tle
Lan
guag
e D
isor
ders
.B
DA
E=
Bos
ton
Dia
gnos
tic
Aph
asia
Exa
min
atio
n. C
AM
CO
G =
Cam
brid
ge C
ogni
tive
Exa
min
atio
n. C
ASI
=C
ogni
tive
Abi
litie
s Sc
reen
ing
Inst
rum
ent.
CE
RA
D=
Con
sort
ium
to
Est
ablis
h a
Reg
istr
yfo
r A
lzhe
imer
’s D
isea
se. E
RV
T=
Ext
ende
d R
ange
Voc
abul
ary
Tes
t. F
AST
=F
renc
hay
Aph
asia
Scr
eeni
ng T
est.
IC
D-1
0 =
Int
erna
tion
al S
tati
stic
al C
lass
ific
atio
n of
Dis
ease
s an
d R
elat
ed H
ealt
h P
rob-
lem
s–10
th R
evis
ion.
MC
I=m
ild c
ogni
tive
impa
irm
ent.
MM
SE=
Min
i Men
tal S
tate
Exa
min
atio
n. N
AR
T=
Nat
iona
l Adu
lt R
eadi
ng T
est.
NE
=no
rmal
eld
erly
. NIN
CD
S-A
DR
DA
=N
atio
nal I
nsti
tute
of N
euro
logi
cal a
nd C
omm
unic
ativ
e D
isor
ders
. NP
V=
nega
tive
pre
dict
ive
valu
e. P
MC
I=pr
ogre
ssiv
e M
CI.
PP
T=
Pyr
amid
s an
d P
alm
s te
st. P
PV
=po
siti
ve p
redi
ctiv
e va
lue.
qA
D=
ques
tion
able
AD
.Q
D=
ques
tion
able
dem
enti
a. R
T=
reac
tion
tim
e. S
MC
I=st
able
MC
I. S
ML
=su
bjec
tive
mem
ory
loss
. SR
T =
Bus
cke
Sele
ctiv
e R
emin
ding
Tes
t. T
RO
G=
Tes
t fo
r th
e R
ecep
tion
of
Gra
mm
ar.
VaD
=va
scul
ar d
emen
tia.
VC
I=va
scul
ar c
ogni
tive
impa
irm
ent.
WA
IS=
Wec
hsle
r A
dult
Int
ellig
ence
Sca
le.
Downloaded By: [Canadian Research Knowledge Network] At: 19:59 12 May 2009







![Original article QS-21 enhances the early EXPERIMENTAL ...€¦ · immune deficiency syndrome [13], hepatitis B [14], and Al-zheimer’s disease [15]. Saponins exhibit both specific](https://img.dokumen.tips/doc/110x75/5eaaad0ee2036731ae34ca03/original-article-qs-21-enhances-the-early-experimental-immune-deficiency-syndrome.jpg)





















