Embed Size (px)
Citation preview
Natural history of Crohn’s disease in patients who underwentintentional restorative proctocolectomy with ileal pouch-analanastomosisB. SHEN*, S . PATEL� & L. LIAN* ,�
*Digestive Disease Institute, the
Cleveland Clinic Foundation,
Cleveland, OH, USA; �Department of
Colorectal Surgery, The Sixth
Affiliated Hospital of Sun Yat-Sen
University, Guangzhou, China
Correspondence to:
Dr B. Shen, The Digestive Disease
Institute—A31, The Cleveland Clinic
Foundation, 9500 Euclid Avenue,
Cleveland, OH 44195, USA.
E-mail: [email protected]
Publication data
Submitted 15 October 2009
First decision 5 November 2009
Resubmitted 21 December 2009
Accepted 22 December 2009
Epub Accepted Article 25 December
2009
SUMMARY
BackgroundCrohn’s disease is generally considered a relative contraindication forrestorative proctocolectomy with ileal pouch anastomosis (IPAA). Thenatural history of IPAA in these patients has not well been defined.
AimTo evaluate the natural history of IPAA in patients with a well-definedpreoperative Crohn’s disease.
MethodsAll patients from the Pouchitis Clinic who had a preoperative diagnosisof Crohn’s disease were screened and 11 patients met the inclusion cri-teria. The control group (with a 1:4 ratio) consisted of IPAA patientswith a preoperative diagnosis of UC.
ResultsDuring the follow-up period of 5.0 years, 7 of 11 (63.6%) with a pre-operative diagnosis of Crohn’s disease developed Crohn’s disease of thepouch. Crohn’s disease of the pouch developed 0.2–15 years after ileos-tomy closure. The remaining four patients with a preoperative diagnosisof Crohn’s disease did not demonstrate signs of Crohn’s disease in 2, 11,11 and 24 years after pouch surgery, respectively.
ConclusionsPost-operative development of Crohn’s disease of the pouch was com-mon in patients with a preoperative diagnosis of Crohn’s disease whounderwent IPAA. Long-term medical therapy was often required. Largemulti-centre studies are warranted to delineate further the natural his-tory of the disease, before Crohn’s disease is considered an indicationfor IPAA.
Aliment Pharmacol Ther 31, 745–753
Alimentary Pharmacology & Therapeutics
ª 2010 Blackwell Publishing Ltd 745
doi:10.1111/j.1365-2036.2009.04227.x

INTRODUCTION
Crohn’s disease (CD) of the pouch can develop any
time during the course of restorative proctocolecomy
with IPAA.1 It may even occur before ileostomy clo-
sure. Although there are no data on the actual annual
incidence of CD of the pouch, the disease entity has
increasingly been recognized, with reported cumula-
tive frequency ranging from 2.7% to 13%.2–10 This
discrepancy in the prevalence may reflect differences
in the sample size, clinical practice settings, diagnostic
criteria used and intensity of follow-up among the
studies.
Crohn’s disease of the pouch occurs in the follow-
ing settings: (i) an ileal pouch is intentionally
constructed in ‘motivated’ patients with a known
preoperative diagnosis of CD; (ii) an ileal pouch was
inadvertently constructed in patients with a preopera-
tive diagnosis of ulcerative colitis (UC) or indetermi-
nate colitis (IC) who were later found to have CD in
colectomy or rectal stump specimens; and (iii)
De novo CD of the pouch can occur weeks (early-
onset) to years (late-onset) after proctocolectomy or
IPAA for UC and a histopathological reassessment of
the proctocolectomy specimens may not show features
suggestive of Crohn’s colitis, such as granulomas and
transmural inflammation.4
Although CD or Crohn’s colitis is generally consid-
ered a relative contraindication for IPAA, the proce-
dure has been intentionally performed in a selected
group of patients with no obvious small intestinal or
perianal diseases.11–13 However, there were arguments
that Crohn’s colitis in some of original reported cases
might not be true Crohn’s disease, as rectal sparing in
non-index colonoscopy might have been a sign of
treated UC. On the other hand, we found that CD of
the pouch may or may not develop after IPAA in this
group of patients in our clinical practice, which may
be one of the reasons that the IPAA procedure has
been advocated in a highly selected patient population
with CD by some clinical investigators. There was dis-
crepancy in reported pouch outcomes in patients with
a preoperative diagnosis of CD or Crohn’s colitis.
While some studies suggested that patients with a pre-
operative diagnosis of CD had a higher pouch failure
rate,14, 15 others found that patients with a late-onset,
de novo CD of the pouch had a poorer prognosis than
those with a preoperative diagnosis of CD.12 A meta-
analysis was performed to evaluate 10 studies pub-
lished between 1980 and 2005 comparing outcomes
of patients undergoing IPAA for CD, UC and IC with a
total of 3103 patients. Patients with a preoperative or
post-operative diagnosis of CD developed more anas-
tomotic strictures than non-CD diagnoses with an
odds ratio of 2.12 and patients with CD (32%) experi-
enced pouch failure more frequently than patients
with UC (4.8%) or IC (5%). However, patients with iso-
lated Crohn’s colitis were not significantly at
increased risk for immediate post-operative complica-
tions.16 The discrepancy in pouch outcome among the
published studies can again be attributed to multiple
factors, such as inclusion criteria and exclusion crite-
ria, diagnostic criteria used for Crohn’s colitis and
institutional expertise. For example, it was not clear
that whether some of the patients truly had Crohn’s
colitis or just UC with patchy disease distribution due
to treatment. It was reported that ‘true’ Crohn’s colitis
with granulomas had a higher pouch failure rate after
IPAA.17
The natural history of the ileal pouch in patients
with a definitive preoperative diagnosis of CD has not
been well delineated. Since the establishment of our
subspecialty Pouchitis Clinic in 2002, we have diag-
nosed and managed a large number of patients with a
variety of ileal pouch disorders. CD of the pouch is
one of the most common long-term adverse sequalae
of IPAA. The aim of the study was to evaluate the nat-
ural history of IPAA in patients with a definite diag-
nosis of CD of the pouch, as compared with patients
who had a preoperative diagnosis of UC.
PATIENTS AND METHODS
Patients
The historical cohort included all patients who were
registered into the Institutional Review Board-approved
Pouchitis Registry from 2002 to 2008 and informed
consent was obtained from all patients. This Pouchitis
Registry, in which the pouch of approximately 50% of
patients was originally constructed outside institutions,
is different from our large 3500-case Pouch Registry
where all pouches were created at the Cleveland
Clinic.12 All patients in this study were recruited from
our subspecialty Pouchitis Clinic where the Pouchitis
Registry resides. The study group included IPAA
patients with a preoperative diagnosis of CD and the
control group consisted of IPAA patients with a preop-
erative diagnosis of UC. Age-matched IPAA patients
with a pre- and intra-operative diagnosis of UC were
746 B . SHEN et al.
Aliment Pharmacol Ther 31, 745–753
ª 2010 Blackwell Publishing Ltd
randomly selected from the Pouchitis Database with
the case-to-control ratio of 1:4.
Inclusion and exclusion criteria
All patients from the Pouchitis Clinic who had a pre-
operative diagnosis of CD were screened. Twenty-three
patients carried a preoperative diagnosis of CD.
Among them, the diagnosis of CD in 12 patients was
based on ‘patchy disease distribution’ and ⁄ or ‘rectal
sparing’ in non-index colonoscopy. After careful
review of charts, particularly index colonoscopy and
biopsy reports, these patients had had diffuse colitis
with proctitis. Therefore, they actually had had UC
rather than Crohn’s colitis and therefore were excluded
from the study. The remaining 11 patients had true CD
as evidenced by characteristic clinical, endoscopic and
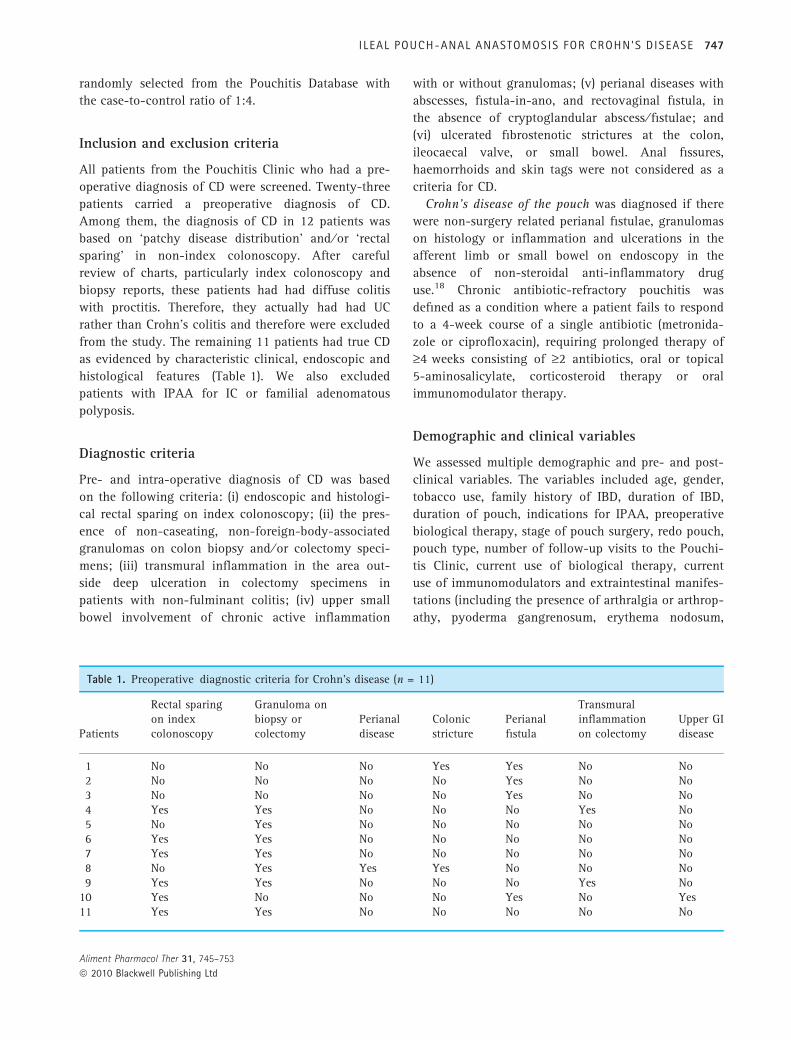
histological features (Table 1). We also excluded
patients with IPAA for IC or familial adenomatous
polyposis.
Diagnostic criteria
Pre- and intra-operative diagnosis of CD was based
on the following criteria: (i) endoscopic and histologi-
cal rectal sparing on index colonoscopy; (ii) the pres-
ence of non-caseating, non-foreign-body-associated
granulomas on colon biopsy and ⁄ or colectomy speci-
mens; (iii) transmural inflammation in the area out-
side deep ulceration in colectomy specimens in
patients with non-fulminant colitis; (iv) upper small
bowel involvement of chronic active inflammation
with or without granulomas; (v) perianal diseases with
abscesses, fistula-in-ano, and rectovaginal fistula, in
the absence of cryptoglandular abscess ⁄ fistulae; and
(vi) ulcerated fibrostenotic strictures at the colon,
ileocaecal valve, or small bowel. Anal fissures,
haemorrhoids and skin tags were not considered as a
criteria for CD.
Crohn’s disease of the pouch was diagnosed if there
were non-surgery related perianal fistulae, granulomas
on histology or inflammation and ulcerations in the
afferent limb or small bowel on endoscopy in the
absence of non-steroidal anti-inflammatory drug
use.18 Chronic antibiotic-refractory pouchitis was
defined as a condition where a patient fails to respond
to a 4-week course of a single antibiotic (metronida-
zole or ciprofloxacin), requiring prolonged therapy of
‡4 weeks consisting of ‡2 antibiotics, oral or topical
5-aminosalicylate, corticosteroid therapy or oral
immunomodulator therapy.
Demographic and clinical variables
We assessed multiple demographic and pre- and post-
clinical variables. The variables included age, gender,
tobacco use, family history of IBD, duration of IBD,
duration of pouch, indications for IPAA, preoperative
biological therapy, stage of pouch surgery, redo pouch,
pouch type, number of follow-up visits to the Pouchi-
tis Clinic, current use of biological therapy, current
use of immunomodulators and extraintestinal manifes-
tations (including the presence of arthralgia or arthrop-
athy, pyoderma gangrenosum, erythema nodosum,
Table 1. Preoperative diagnostic criteria for Crohn’s disease (n = 11)
Patients
Rectal sparingon indexcolonoscopy
Granuloma onbiopsy orcolectomy
Perianaldisease
Colonicstricture
Perianalfistula
Transmuralinflammationon colectomy
Upper GIdisease
1 No No No Yes Yes No No2 No No No No Yes No No3 No No No No Yes No No4 Yes Yes No No No Yes No5 No Yes No No No No No6 Yes Yes No No No No No7 Yes Yes No No No No No8 No Yes Yes Yes No No No9 Yes Yes No No No Yes No
10 Yes No No No Yes No Yes11 Yes Yes No No No No No
I LEAL POUCH-ANAL ANASTOMOSIS FOR CROHN’S D ISEASE 747
Aliment Pharmacol Ther 31, 745–753
ª 2010 Blackwell Publishing Ltd

IBD-related ocular lesions, thromboembolic events and
primary sclerosing cholangitis). Pancolitis was defined
by the presence of endoscopic, macroscopic or micro-
scopic disease extending proximal to the splenic
flexure. Concurrent autoimmune disorders included
autoimmune thyroid diseases, rheumatoid arthritis,
pernicious anaemia, coeliac disease, systemic lupus
erythematosus, chronic asthma, type I diabetes, rheu-
matoid arthritis, psoriasis, autoimmune haemolytic
anaemia, vitiligo, idiopathic thrombocytopenic purpura
and multiple sclerosis.
Outcome measurement
We compared pouch failure, CD of the pouch, pouch-
associated hospitalization and post-operative long-term
medication use between the study and control groups.
Statistical analysis
Descriptive statistics were computed for all variables.
These included means, medians with interquartile
range for continuous factors and frequencies for cate-
gorical variables. Student’s t-tests, Wilcoxon rank sum
tests and Fisher’s Exact tests for categorical and non-
categorical variables. P values <0.05 were considered
statistically significant. SAS version 9.1 software (The
SAS Institute, Cary, NC, USA) was used to carry out
all analyses. A 1:4 case-control ratio was chosen to
increase the power of the study.
RESULTS
Demographic and clinical variables
Of 23 patients labelled CD before surgery, 11 truly did
have CD. The main cause for the false positivity for
CD was the ‘patchy’ disease and rectal sparing in
non-index colonoscopy. Therefore, 12 patients who
had been labelled as Crohn’s colitis were actually UC
and they had had diffuse colitis including rectal
involvement on index colonoscopy. Their later ‘patchy’
disease and rectal sparing might have resulted from
oral or topical medical therapy (Table 2).
Preoperative diagnosis of Crohn’s disease
A majority of the patients in the study groups
met multiple diagnostic criteria for CD before or dur-
ing colectomy. After carefully reviewing medical
records, particularly endoscopic and histological
report, six patients (54.5%) were found to have rectal
sparing on index colonoscopy. Seven patients (63.6%)
had noncaseating, non-foreign-body-associated granu-
lomas on colon biopsy or colectomy specimens. Simple
perianal fistulae were present in four patients (36.4%)
(Table 1).
Post-operative diagnosis of Crohn’s disease ofthe pouch
The mean duration of the pouch was 8.9 � 6.7 years.
During the follow-up period, 7 of 11 (63.6%) with a
preoperative diagnosis of CD eventually developed CD
of the pouch. The mean interval from pouch construc-
tion to diagnosis of CD of the pouch was 5.0 � 4.9
years, with a range from 0.2 to 15 years after ileo-
stomy closure. The remaining four patients with a
preoperative diagnosis of CD did not demonstrate any
signs of CD 2, 11, 11 and 24 years after pouch surgery
respectively. It appears that there were no consistent
patterns or phenotypes between preoperative CD and
post-operative CD of the pouch. For example, patient
2 and patient 3 had perianal fistulae before colectomy
and developed CD of the pouch with strictures and
ileitis without fistulae (Table 3).
Pouch outcomes
With a median of 7 (interquatile range 4–11) years of
follow-up, seven patients (63.6%) in the study group
developed CD of the pouch and four patients (35.4%)
showed no endoscopic, radiographic, and histological
evidence of CD. Therefore, a preoperative diagnosis of
CD did not necessarily lead to the development of CD
of the pouch. In contrast, in the control group, seven
patients (15.9%) developed CD of the pouch. It appears
that the pouch failure rate was similar between the
study and control groups.
Of the seven patients with CD in the study group,
two patients were treated with adalimumab, two
patients were treated with mercaptopurine, 10 patients
were on long-term antibiotics (metronidazole, tini-
dazole, ciprofloxacin or rifaximin). All three patients
with strictures were treated with endoscopic balloon
dilations (Table 4).
We also evaluated the 12 patients with a precolecto-
my diagnosis of ‘CD’ who were but later diagnosed
with UC after clinicopathological data were reviewed
again. The mean age of this group was 48.9 � 10.6
748 B . SHEN et al.
Aliment Pharmacol Ther 31, 745–753
ª 2010 Blackwell Publishing Ltd

years, with four being women (33.3%). All of them
(100%) had extensive colitis. Three patients did have
use infliximab before colectomy. The mean duration
from UC diagnosis to pouch construction was
13.2 � 9.1 years. With a mean duration of 8.8 � 4.7
years, one patient (8.3%) developed inflammatory CD,
one (8.3%) had fistulizing CD and two patients (16.7%)
developed pouch failure from surgical complications
(chronic anastomotic sinus and leak).
DISCUSSION
Natural course of IPAA in patients with a known pre-
operative diagnosis of CD has not been well defined.
Table 2. Comparison of demographic and clinical data
Variables
PreoperativeCrohn’s disease
(n = 11)
Preoperativeulcerative colitis
(n = 44) P value
Mean current age, years, � standard deviation 45.2 � 18.5 47.5 � 15 0.58Male gender 9 (81.8%) 22 (50%) 0.09Mean duration of pouch, years, � standard deviation 8.8 � 6.6 8.6 � 6.1 0.93Caucasian race 11 (100%) 42 (95.4%) 1Smoking 0.06
Never 7 (63.6%) 40 (91%)Ex-smoker 2 (18.2%) 2 (4.5%)Active 2 (18.2%) 2 (4.5%)
Chronic NSAID use 2 (18.2%) 6 (13.6%) 0.65Family history of IBD 2 (18.2%) 7 (15.9%) 0.61Duration of UC from diagnosis to IPAA,median years (interquartile range)
3 (0–11) 5 (1–16.8) 0.32
Indication for colectomy 1Refractory disease 9 (81.8%) 36 (81.8%)Dysplasia 2 (18.2%) 8 (18.2%)
Preoperative extensive colitis 11 (100%) 42 (95.5%) 1Toxic megacolon 1 (9.1%) 1 (2.3%) 0.36Preoperative biological therapy 2 (18.2%) 2 (4.5%) 0.171st visit to pouchitis clinic to date,median yrs (interquartile range)
5 (3–5) 4 (2–4) 0.15
Duration of pouch construction to last visit,median years (interquartile range)
7 (4–11) 7 (4–10.8) 0.96
J pouch configuration 10 (90.9%) 43 (97.7%) 0.36Stage of pouch surgery 0.4
2 7 (63.6%) 35 (79.5%)3 3 (27.3%) 6 (13.6%)4 1 (9.1%) 3 (6.8%)
Primary sclerosing cholangitis 1 (9.1%) 1 (2.3%) 0.36Final diagnoses 0.08
Normal pouch 0 2 (4.5%)Irritable pouch syndrome 1 (9.1%) 8 (18.2%)Active pouchitis 3 (27.3%) 8 (18.2%)Refractory pouchitis 0 7 (15.9%)Crohn’s disease of the pouch 7 (63.6%) 7 (15.9%)Cuffitis 0 7 (15.9%)Surgical complication 0 4 (9.1%)Primary anismus 0 1 (2.3%)
Extraintestinal manifestations 0.07Joints 4 (36.4%) 14 (31.8%)Eyes 0 1 (2.3%)Thromboembolic events 2 (18.2%) 0
Mean number of visits of pouchitis clinic, 2.2 � 1.3 2.3 � 1.3 0.79
I LEAL POUCH-ANAL ANASTOMOSIS FOR CROHN’S D ISEASE 749
Aliment Pharmacol Ther 31, 745–753
ª 2010 Blackwell Publishing Ltd
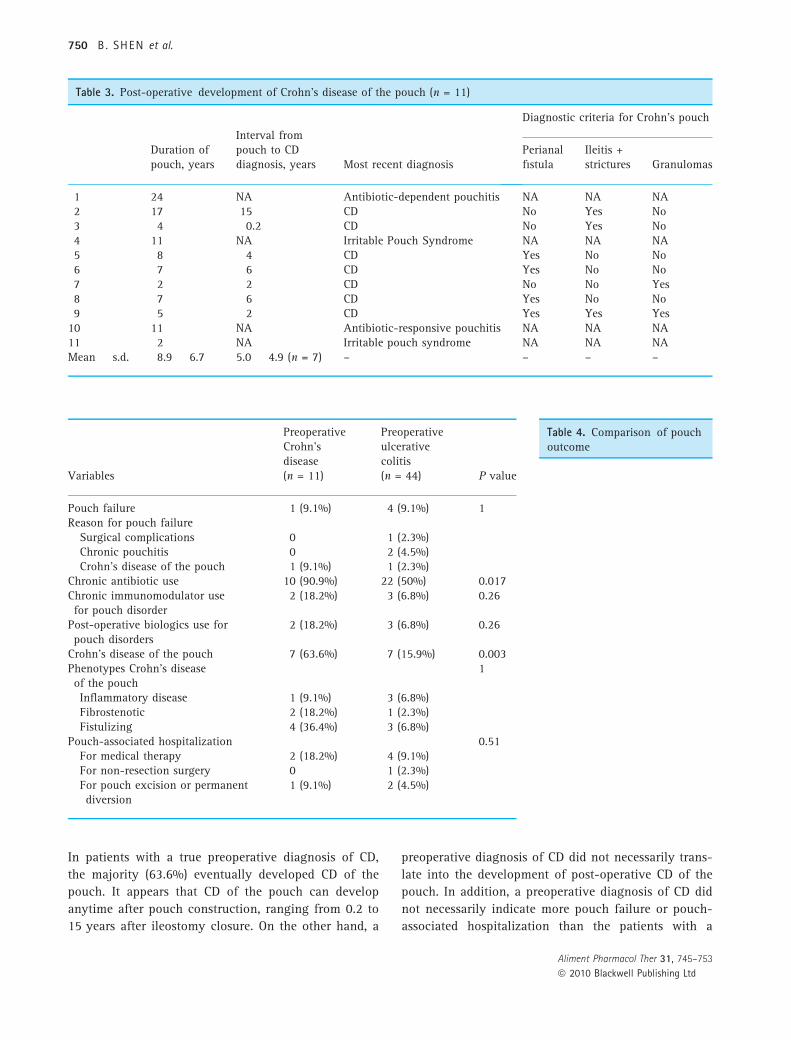
In patients with a true preoperative diagnosis of CD,
the majority (63.6%) eventually developed CD of the
pouch. It appears that CD of the pouch can develop
anytime after pouch construction, ranging from 0.2 to
15 years after ileostomy closure. On the other hand, a
preoperative diagnosis of CD did not necessarily trans-
late into the development of post-operative CD of the
pouch. In addition, a preoperative diagnosis of CD did
not necessarily indicate more pouch failure or pouch-
associated hospitalization than the patients with a
Table 4. Comparison of pouchoutcome
Variables
PreoperativeCrohn’sdisease(n = 11)
Preoperativeulcerativecolitis(n = 44) P value
Pouch failure 1 (9.1%) 4 (9.1%) 1Reason for pouch failure
Surgical complications 0 1 (2.3%)Chronic pouchitis 0 2 (4.5%)Crohn’s disease of the pouch 1 (9.1%) 1 (2.3%)
Chronic antibiotic use 10 (90.9%) 22 (50%) 0.017Chronic immunomodulator usefor pouch disorder
2 (18.2%) 3 (6.8%) 0.26
Post-operative biologics use forpouch disorders
2 (18.2%) 3 (6.8%) 0.26
Crohn’s disease of the pouch 7 (63.6%) 7 (15.9%) 0.003Phenotypes Crohn’s diseaseof the pouch
1
Inflammatory disease 1 (9.1%) 3 (6.8%)Fibrostenotic 2 (18.2%) 1 (2.3%)Fistulizing 4 (36.4%) 3 (6.8%)
Pouch-associated hospitalization 0.51For medical therapy 2 (18.2%) 4 (9.1%)For non-resection surgery 0 1 (2.3%)For pouch excision or permanentdiversion
1 (9.1%) 2 (4.5%)
Table 3. Post-operative development of Crohn’s disease of the pouch (n = 11)
Duration ofpouch, years
Interval frompouch to CDdiagnosis, years Most recent diagnosis
Diagnostic criteria for Crohn’s pouch
Perianalfistula
Ileitis +strictures Granulomas
1 24 NA Antibiotic-dependent pouchitis NA NA NA2 17 15 CD No Yes No3 4 0.2 CD No Yes No4 11 NA Irritable Pouch Syndrome NA NA NA5 8 4 CD Yes No No6 7 6 CD Yes No No7 2 2 CD No No Yes8 7 6 CD Yes No No9 5 2 CD Yes Yes Yes
10 11 NA Antibiotic-responsive pouchitis NA NA NA11 2 NA Irritable pouch syndrome NA NA NAMean � s.d. 8.9 � 6.7 5.0 � 4.9 (n = 7) – – – –
750 B . SHEN et al.
Aliment Pharmacol Ther 31, 745–753
ª 2010 Blackwell Publishing Ltd

preoperative diagnosis of UC. However, in the former
group of patients, chronic antibiotic use was almost a
norm. In addition, numerically more patients in the
study group were using immumomodulators and ⁄ or
biologics than in the control group.
While restorative proctocolectomy with IPAA has
been routinely performed in patients with IC or
inflammatory bowel disease-unclassified (IBDU),19 it is
debatable whether patients with CD can have IPAA
procedure. In a study of 25 patients with a pre-
(n = 9) and post- (n = 16) operative diagnosis of CD,
with a mean follow-up of 38 months, 16 patients have
a functioning pouch, seven had pouch excision, one
had pouch diversion and one died. Only one of the
nine patients in whom there was a preoperative diag-
nosis of CD had a functioning pouch, with complica-
tions uniformly occurring within months of ileostomy
closure. In contrast, 15 of the 16 patients with a post-
operative diagnosis CD of the pouch maintained their
pouch. It was therefore suggested that patients with a
preoperative diagnosis of CD should be contraindicated
for having IPAA.14 This notion was further supported
by a study from Mt Sinai Hospital, Toronto. Of 1270
patients with IPAA (1135 UC, 36 CD, and, 21 IC),
pouch complications were significantly more common
in patients with a preoperative diagnosis of CD (64%)
or IC (43%) than patients with a preoperative diagnosis
of UC (22%). Pouch failure rates were 56% for CD,
10% for IC and 6% for UC.15 Furthermore, a descrip-
tive study of 52 patients with CD or IC from a total of
1652 patients from St Mark’s Hospital, London also
showed that patients with a preoperative diagnosis of
IC or IC favouring UC had a pouch failure rate of
11.5% vs. 57.5% for patients with CD or IC favouring
CD.20 Treatment of CD of the pouch can be challeng-
ing. There were scant data on treatment of this disease
entity of the pouch. Biological agents, such as inflix-
imab21 and adalimumab,22 have been used.
Ileal pouch anastomosis, on the other hand, has
been advocated for a highly selected group of patients
by some clinical investigators based on their ‘compa-
rable’ outcome. In a study of 41 pouch patients from
France with a pre- (n = 26) or post- (n = 15) operative
diagnosis of CD and a mean pouch follow-up of
47 months, two had persistent anal ulcers with pou-
chitis and granulomas on pouch biopsy and were trea-
ted medically; two experienced extrasphincteric
abscesses and seven presented pouch-perineal fistulas.
In the 20 patients followed up for more than 10 years,
7 (35%) experienced CD-related complications, which
required pouch excision in two (10%). The authors
suggested that these acceptable long-term results may
justify considering IPAA in selected patients with
Crohn’s colitis.23 A retrospective analysis examined
the long-term outcomes in 12 patients with IPAA who
had a preoperative diagnosis of CD as compared with
100 patients with a preoperative diagnosis of UC, with
a mean follow-up of 76 months (range 12–192).
Demographic and clinical data, post-operative compli-
cations, functional results, anxiety and quality of life
in the two groups were similar.10 A preoperative peri-
anal diseases, including fissure-in-ano, perianal
abscesses, fistula-in-ano, rectovaginal fistula and sig-
nificant haemorrhoids ⁄ skin tags were shown to be
associated with an increased risk for post-operative
anastomotic leaks and perianal complications, but not
occurrence of CD of the pouch or pouch failure.24
The prognosis of CD in patients with IPAA was
determined by multiple factors. A majority of our
patients who were able to maintain the pouch were on
long-term medical therapy. A recent case-control
study of 204 patients with CD of the pouch identified
from our 2834-case Pouch Registry showed that CD
diagnosis was made before IPAA in 20 (10%), from
post-operative histopathology (incidental) in 97(47%)
or made in a delayed fashion at median 36 months
after IPAA in 87 (43%). Multivariate analysis showed
that patients with CD of the pouch with a delayed
diagnosis had a higher risk for pouch failure than
those with a preoperative and perioperative diagnosis
of CD with a hazard ratio of 2.6 [95% confidence
interval (CI) 1.1–6.5]. In other words, for CD patients
with IPAA, when the diagnosis is established preopera-
tively or immediately following surgery, pouch loss
rates were low.12 These results are consistent with
findings in the current study. Of note, the patients in
the current study were identified from our 950-case
Pouchitis Database, which was different from the
3500-case Pouch Registry.
It was not clear whether the IPAA procedure inten-
tionally performed in patients with a preoperative
diagnosis of CD would necessarily lead to the develop-
ment of CD of the pouch. In addition, the exact mech-
anisms of CD of the pouch are not known. We
speculate that faecal stasis and anastomosis, combined
with component of surgically induced ischaemic injury
in genetically susceptible patients, may create a ‘CD-
friendly’ environment and the ‘thermostat’ of balance
between bacteria and mucosal immunity after
IPAA procedure might be reset to gear towards the
I LEAL POUCH-ANAL ANASTOMOSIS FOR CROHN’S D ISEASE 751
Aliment Pharmacol Ther 31, 745–753
ª 2010 Blackwell Publishing Ltd

development of new sets of IBD, including pouchitis
and CD of the pouch. Multiple clinical studies have
shown that CD of the pouch can develop in patients
with a preoperative diagnosis of UC. Our anecdotal
experience suggested that CD patients who failed to
respond to biological therapy may have a favourable
response to the agents after IPAA and development of
CD of the pouch. On the other hand, not all patients
with a preoperative diagnosis of CD would develop CD
of the pouch after IPAA, as shown in this study.
Risk factors for CD of the pouch have been studied.
In addition to a preoperative diagnosis of CD,12 other
reported risk factors for the development of CD of the
pouch include sero-positive anti-Saccharomyces cere-
visiae-IgA,25 a family history of CD,25, 26 being active
smoker,27 a long duration of pouch, and a preopera-
tive diagnosis of IC.27, 28 Different phenotypes of CD
of the pouch were shown to be associated with differ-
ent risk factors.29 For example, the presence of IC,
younger age, and female gender were associated with
an increased risk for fistulizing CD of the pouch.29
The findings for the current study have several clini-
cal implications. As the natural history of Crohn’s coli-
tis and CD of the pouch is poorly defined, the findings
in the current study may help shed some light. Not all
patients with Crohn’s colitis would necessarily develop
CD of the pouch after restorative proctocolectomy. On
the other hand, not all patients with a clear-cut diag-
nosis of UC before surgery would be immune to the
development of CD of the pouch. Our recent study
(submitted to Digestive Disease Week 2010) showed
that UC patients with the absence of granulomas on
colon biopsy and colectomy specimens can develop
CD of the pouch as evidenced by the presence of non-
caseating granulomas. It is important to assess the dis-
ease distribution of colitis on index colonoscopy, as
patchy disease or rectal sparing can occur in patients
with UC who were medically treated.30, 31 IPAA can be
performed in a selected patient population with a pre-
operative diagnosis of Crohn’s colitis. However,
patients should be made aware that he or she would
have a high chance to develop CD of the pouch and to
maintain the pouch, long-term medical therapy with
or without endoscopy therapy is often required. In
addition, CD of the pouch in these patients often has
compromised health-related quality of life.32 Risks and
benefits of IPAA for these patients should carefully be
balanced.33
There are limitations to this historical cohort study.
There might have been referral bias as all patients
were evaluated and managed at our tertiary subspe-
cialty Pouchitis Clinic. The sample size was small, as it
was not a common practice to construct an ileal pouch
in patients with a known diagnosis of CD.
In conclusion, post-operative development of CD of
the pouch was common in patients with a preoperative
diagnosis of CD who underwent IPAA, but it does not
appear to be necessarily the natural consequence of all
patients. While a majority of the patients with pre- or
post- operative diagnosis of CD were able to keep their
pouches, long-term medical therapy was typically
required. Patients should be fully counselled for poten-
tial development of diseased pouch conditions. Large
multi-centre studies are warranted to delineate further
the natural history of the disease, before CD is consid-
ered an indication for IPAA.
ACKNOWLEDGEMENT
Declaration of personal interests: The authors would
like to thank Eli and Edyth Broad Foundation for the
support. Declaration of funding interests: None.
REFERENCES
1 Braveman JM, Schoetz DJ Jr, Marcello
PW, et al. The fate of the ileal pouch in
patients developing Crohn’s disease. Dis
Colon Rectum 2004; 47: 1613–9.
2 Keighley MRB. The final diagnosis in
pouch patients for presumed ulcerative
colitis may change to Crohn’s disease:
patients should be warned of the conse-
quences. Acta Chirurgica Ingoslavica
2000; 47(4 Suppl 1): 27–31.
3 Peyregne V, Francois Y, Gilly F-N, et al.Outcome of ileal pouch after secondary
diagnosis of Crohn’s disease. In J Colorec-
tal Dis 2000; 15: 49–53.
4 Goldstein NS, Sanford WW, Bodzin JH.
Crohn’s like complications in patients
with ulcerative colitis after total
proctocolectomy and ileal pouch-anal
anastomosis. Am J Surg Pathol 1997; 21:
1343–53.
5 Deutch AA, McLeod RS, Cullen J, et al.Results of the pelvic-pouch procedure in
patients with Crohn’s disease. Dis Colon
Rectum 1991; 34: 475–7.
6 Yu CS, Pemberton JH, Larson D. Ileal
pouch-anal anastomosis in patients
with indeterminate colitis: long-term
results. Dis Colon Rectum 2000; 43:
1487–96.
7 Neilly P, Neill ME, Hill GL. Restorative
proctocolectomy with ileal pouch-anal
anastomosis in 203 patients: The Auck-
land experience. Aust N Z J Surg 1999;
69: 22–7.
752 B . SHEN et al.
Aliment Pharmacol Ther 31, 745–753
ª 2010 Blackwell Publishing Ltd

8 Gemlo B, Wong D, Rothenberger DA,
et al. Ileal pouch-anal anastomosis: pat-
terns of failure. Arch Surg 1992; 127:
784–7.
9 Hartley JE, Fazio VW, Remzi FH, et al.Analysis of the outcome of ileal pouch-
anal anastomosis in patients with Crohn’s
disease. Dis Colon Rectum 2004; 47:
1808–15.
10 De Oca J, Sanchez-Santos R, Rague JM,
et al. Long-term results of ileal pouch-
anal anastomosis in Crohn’s disease.
Inflamm Bowel Dis 2003; 9: 171–5.
11 Panis Y, Poupard B, Nemeth J, et al. Ileal
pouch-anal anastomosis for Crohn’s dis-
ease. Lancet 1996; 347: 854–7.
12 Melton GB, Fazio VW, Kiran RP, et al.Long-term outcomes with ileal pouch-
anal anastomosis and Crohn’s disease:
pouch retention and implications of
delayed diagnosis. Ann Surg 2008; 248:
608–16.
13 Grucela AL, Bauer JJ, Gorfine SR, Chessin
DB. Outcome and long-term function of
restorative proctocolectomy for Crohn’s
disease: comparison to patients with
ulcerative colitis. Colorectal Dis. [Epub
ahead of print].
14 Hyman NH, Fazio VW, Tuckson WB,
Lavery IC. Consequences of ileal pouch-
anal anastomosis for Crohn’s colitis. Dis
Colon Rectum 1991; 34: 653–7.
15 Brown CJ, Maclean AR, Cohen Z, et al.Crohn’s disease and indeterminate colitis
and the ileal pouch-anal anastomosis:
outcomes and patterns of failure. Dis
Colon Rectum 2005; 48: 1542–9.
16 Reese GE, Lovegrove RE, Tilney HS, et al.The effect of Crohn’s disease on outcomes
after restorative proctocolectomy. Dis
Colon Rectum 2007; 50: 239–50.
17 Morpurgo E, Petras R, Kimberling J, et al.Characterization and clinical behavior of
Crohn’s disease initially presenting pre-
dominantly as colitis. Dis Colon Rectum
2003; 46: 918–24.
18 Shen B, Remzi FH, Lavery IC, Lashner BA,
Fazio VW. A proposed classification of
ileal pouch disorders and associated com-
plications after restorative proctocolec-
tomy. Clin Gastroenterol Hepatol 2008; 6:
145–58.
19 Murrell ZA, Melmed GY, Ippoliti A, et al.A prospective evaluation of the long-term
outcome of ileal pouch-anal anastomosis
in patients with inflammatory bowel dis-
ease-unclassified and indeterminate coli-
tis. Dis Colon Rectum 2009; 52: 872–8.
20 Tekkis PP, Heriot AG, Smith O, et al. Long-
term outcomes of restorative proctocolec-
tomy for Crohn’s disease and indeterminate
colitis. Colorectal Dis 2005; 7: 218–23.
21 Colombel J-F, Richart E, Loftus EV, et al.Management of Crohn’s disease of the
ileoanal pouch with infliximab. Am J
Gastroenterol 2003; 98: 2239–44.
22 Shen B, Remzi FH, Lavery IC, et al. Effi-
cacy and safety of adalimumab in the
treatment of Crohn’s disease of the ileal
pouch. Aliment Pharm Therap 2009; 29:
519–26.
23 Regimbeau JM, Panis Y, Pocard M, et al.Long-term results of ileal pouch-anal
anastomosis for colorectal Crohn’s dis-
ease. Dis Colon Rectum 2001; 44: 769–78.
24 Richard CS, Cohen Z, Stern HS, McLeod
RS. Outcome of the pelvic pouch proce-
dure in patients with prior perianal dis-
ease. Dis Colon Rectum 1997; 40: 647–52.
25 Melmed GY, Fleshner PR, Bardakcioglu O,
et al. Family history and serology predict
Crohn’s disease after ileal pouch-anal
anastomosis for ulcerative colitis. Dis
Colon Rectum 2008; 51: 100–8.
26 Shen B, Remzi FH, Hammel JP, et al.Family history of Crohn’s disease
increases the risk for Crohn’s disease of
ileal pouch-anal anastomosis. Inflamm
Bowel Dis 2009; 15: 163–70.
27 Shen B, Fazio VW, Remzi FH, et al. Risk
factors for diseases of ileal pouch-anal
anastomosis in patients with ulcerative
colitis. Clin Gastroenterol Hepatol 2006;
4: 81–9.
28 Delaney CP, Remzi FH, Gramlich T, et al.Equivalent function, quality of life and
pouch survival rates after ileal pouch-
anal anastomosis for indeterminate and
ulcerative colitis. Ann Surg 2002; 236:
43–8.
29 Shen B, Fazio VW, Remzi FH, et al. Risk
factors for clinical phenotypes of Crohn’s
disease of the pouch. Am J Gastroenterol
2006; 101: 2760–8.
30 Kim B, Barnett JL, Kleer CG, Appelman
HD. Endoscopic and histological patchi-
ness in treated ulcerative colitis. Am J
Gastroenterol 1999; 94: 3258–62.
31 Bernstein CN, Shanahan F, Anton PA,
Weinstein WM. Patchiness of mucosal
inflammation in treated ulcerative colitis:
a prospective study. Gastrointest Endosc
1995; 42: 232–7.
32 Shen B, Fazio VW, Remzi FH, et al. Clini-
cal features and quality of life in patients
with different phenotypes of Crohn’s dis-
ease of the pouch. Dis Colon Rectum
2007; 50: 1450–9.
33 Shen B, Fazio VW, Remzi FH, et al. Com-
prehensive evaluation of inflammatory and
non-inflammatory sequelae of ileal pouch-
anal anastomosis. Am J Gastroenterol
2005; 100: 93–101.
I LEAL POUCH-ANAL ANASTOMOSIS FOR CROHN’S D ISEASE 753
Aliment Pharmacol Ther 31, 745–753
ª 2010 Blackwell Publishing Ltd



![The Impacts of Gastroileostomy Rat Model on Glucagon-like … · 2018. 5. 28. · creased GLP-1 secretion after glucose-rich meals [11–13]. Single anastomosis sleeve ileal (SASI)](https://img.dokumen.tips/doc/110x75/60d1dee2801d4468a56874bc/the-impacts-of-gastroileostomy-rat-model-on-glucagon-like-2018-5-28-creased.jpg)

























