Embed Size (px)
Citation preview

Accepted Manuscript
Rationale and Design of the Aldosterone Targeted NeuroHormonal CombinEd withNatriuresis TherApy in Heart Failure (ATHENA-HF) Trial
Javed Butler, MD, MPH, MBA, Adrian F. Hernandez, MD, Kevin J. Anstrom, PhD,Andreas Kalogeropoulos, MD, PhD, Margaret M. Redfield, MD, Marvin A. Konstam,MD, W. H. Wilson Tang, MD, G. Michael Felker, MD, Monica R. Shah, MD, EugeneBraunwald, MD
PII: S2213-1779(16)30289-X
DOI: 10.1016/j.jchf.2016.06.003
Reference: JCHF 521
To appear in: JACC: Heart Failure
Received Date: 21 March 2016
Revised Date: 6 June 2016
Accepted Date: 14 June 2016
Please cite this article as: Butler J, Hernandez AF, Anstrom KJ, Kalogeropoulos A, Redfield MM,Konstam MA, Tang WHW, Felker GM, Shah MR, Braunwald E, Rationale and Design of the AldosteroneTargeted NeuroHormonal CombinEd with Natriuresis TherApy in Heart Failure (ATHENA-HF) Trial,JACC: Heart Failure (2016), doi: 10.1016/j.jchf.2016.06.003.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1
Rationale and Design of the Aldosterone Targeted NeuroHormonal CombinEd with Natriuresis TherApy in Heart Failure (ATHENA-HF) Trial Javed Butler, MD, MPH, MBA (1); Adrian F. Hernandez, MD (2); Kevin J. Anstrom, PhD (2); Andreas Kalogeropoulos, MD, PhD (3); Margaret M. Redfield, MD (4); Marvin A. Konstam, MD (5); W. H. Wilson Tang, MD (6); G. Michael Felker, MD (2); Monica R. Shah, MD (7); Eugene Braunwald, MD (8) From the Department of Medicine, Stony Brook University, Stony Brook, New York (1); Department of Medicine, Duke University, Durham, North Carolina (2); Department of Medicine, Emory University, Atlanta, Georgia (3); Department of Cardiovascular Diseases, Mayo Clinic, Minnesota (4); Department of Medicine, Tufts University, Boston, Massachusetts (5); Department of Cardiovascular Medicine, Cleveland Clinic, Cleveland, Ohio (6); Division of Cardiovascular Sciences, National Heart, Lung, and Blood Institute, Baltimore, Maryland; Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts (8) Running Title: ATHENA HF Trial Funding Sources: The Heart Failure Clinical Research Network is supported by the NHLBI, National Institutes of Health (U10HL084904 for the coordinating center; and U10HL084861, U10HL084875, U10HL084877, U10HL084889, U10HL084890, U10HL084891, U10HL084899, U10HL084907, and U10HL084931 for the clinical centers). ClinicalTrials.gov Identifier: NCT02235077 URL: http://www.clinicaltrials.gov. Unique identifier: NCT02235077. Disclosures: None Address correspondence to: Javed Butler, MD, MPH, Cardiology Division, Stony Brook University, T-16, Room 080, Stony Brook, NY 11794. Telephone: (631) 444-1066 Fax: (631) 444-1054 Email: [email protected]

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
2
ABSTRACT While therapy with mineralocorticoid receptor antagonists (MRA) is recommended for patients with chronic heart failure (HF) with reduced ejection fraction and in post-infarction HF, it has not been studied well in acute HF (AHF) despite being commonly used in this setting. At high doses, MRA therapy in AHF may relieve congestion through its natriuretic properties and mitigate the effects of adverse neurohormonal activation associated with intravenous loop diuretics. The Aldosterone Targeted Neurohormonal Combined with Natriuresis Therapy in Heart Failure (ATHENA-HF) trial is a randomized, double blind, placebo-controlled study of the safety and efficacy of 100 mg daily spironolactone vs. placebo (or continued low-dose spironolactone use in participants who are already receiving spironolactone at baseline) in 360 patients hospitalized for AHF. Patients are randomized within 24 hours of receiving the first dose of intravenous diuretics. The primary objective is to determine if high-dose spironolactone, when compared to standard care, will lead to greater reductions in N-terminal pro-B-type natriuretic peptide levels from randomization to 96 hours. The secondary endpoints include changes in the clinical congestion score, dyspnea relief, urine output, weight change, loop diuretic dose, and in-hospital worsening HF. Index hospital length of stay and 30-day clinical outcomes will be assessed. Safety endpoints include risk of hyperkalemia and renal function. Differences among patients with reduced versus preserved ejection fraction will be determined. Key Words: Heart failure, acute heart failure, hospitalization, mineralocorticoid receptor antagonist, aldosterone, natriuretic peptides Abbreviations: ACE: Angiotensin converting enzyme AHF: Acute heart failure ASCEND-HF: Acute Study of Clinical Effectiveness of Nesiritide in Decompensated Heart Failure ATHENA-HF: Aldosterone Targeted Neurohormonal Combined with Natriuresis Therapy in Heart Failure eGFR: Estimated glomerular filtration rate EVEREST: Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study with Tolvaptan HF: Heart failure MRA: Mineralocorticoid receptor antagonists NT-proBNP: N-terminal pro B-type natriuretic peptide RELAX-AHF: Efficacy and Safety of Relaxin for the Treatment of Acute Heart Failure RAAS: Renin-angiotensin-aldosterone-system WHF: Worsening heart failure

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
3
Heart failure (HF) accounts for over a million hospitalizations in the United States annually.1, 2
Hospitalizations for HF are associated with a significantly elevated risk for post-discharge
mortality and recurrent hospitalizations. Mortality or readmission risk at 60-days post discharge
is ~30% and may be as high as 50% by 6 months in these patients.3-7 While therapy for chronic
HF with reduced ejection fraction has evolved over time favorably impacting survival, outcomes
for patients with acute heart failure (AHF) have not changed much in the past two decades. Thus
far none of the trials have shown an improvement in post-discharge outcomes in patients with
acute heart failure.8, 9 Thus there remains a pressing need to develop interventions that can
improve outcomes safely in this high-risk group of patients.
PERSISTENT CONGESTION AND OUTCOMES IN ACUTE HEART FAILURE
Worsening congestion is the main reason for hospitalization for the majority of AHF patients and
diuretics remains the mainstay of therapy. Even with the use of intravenous diuretics, over half
of the patients lose ≤5 lbs. and up to 20% may actually gain weight during hospitalization.10
Despite improvement in symptoms, a large proportion of these patients continue to have
persistent congestion at discharge,11 which whether measured clinically,12, 13 with right heart
catheterization, or by natriuretic peptide levels,14,15 predict post-discharge outcome. Persistent
congestion may be sub-clinical, related to diuretic resistance, or when further diuretic use is
difficult in the face of worsening renal function.
IMPORTANCE OF ALDOSTERONE IN ACUTE HEART FAILURE
The renin-angiotensin-aldosterone-system (RAAS) is activated in HF. In normal subjects,
aldosterone levels range between 2-9 ng/dL but in one AHF trial, median levels were 11.0 ng/dL
and were over the upper normal range in 33.2% of patients.16 Aldosterone levels are only
transiently suppressed with ACE inhibition. Intravenous loop diuretic use in AHF further

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
4
intensifies RAAS activation and secondary hyperaldosteronism17, 18, enhancing proximal tubular
sodium absorption and decreased distal sodium delivery, impairing the normal escape
mechanism from the sodium-retaining effect of aldosterone. Therefore, beyond myocardial and
vascular adverse effects, hyperaldosteronism directly contributes to diuretic resistance.19 Loop
diuretics also block sodium chloride transport at the macula densa, which stimulates the RAAS
independent of renal sodium loss17. (Figure 1)
MINERALOCORTICOID RECEPTOR ANTAGONIST USE IN ACUTE HEART
FAILURE
The low dose mineralocorticoid receptor antagonists (MRA) used in chronic HF are believed to
benefit patients by anti-fibrotic but not natriuretic effects.20 Inhibition of mineralocorticoid
receptors at higher MRA doses may cause significant natriuresis. Resistance to loop diuretics in
AHF may be overcome by natriuretic doses of spironolactone (>50 mg/day).19 In a study of 6
HF patients, 200 mg twice a day of spironolactone caused a marked increase in sodium excretion
leading to negative sodium balance.21 In another study, patients with severe HF who were
resistant to high-dose loop diuretics responded with increased natriuresis with the use of 100
mg/day spironolactone.22
The clinical benefit and safety of high dose MRA use in AHF was recently supported by
a single-center, single-blind trial of 100 patients treated with standard therapy alone or with
addition of spironolactone initiated within 24 hours.23 Spironolactone dose was 94.5±23.3 mg on
day 1 and 62.7±24.3 mg on day 3. Increase in creatinine by ≥0.3 mg/dL from day 1 to day 3 was
more likely to occur in the standard of care arm (20% vs. 4%; P=0.038). Plasma N-terminal pro
B-type natriuretic peptide (NT-proBNP) levels were comparable at baseline but were lower in
the spironolactone group at day 3 (2488 [4579] pg/ml in controls vs. 1555 [1832] pg/ml in

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
5
spironolactone group; P=0.05). A greater proportion of patients in the spironolactone group were
free of congestion at day 3 and a higher proportion had transitioned from intravenous to oral
furosemide (82% vs. 44%; P<0.001). These findings support the safety and potential efficacy of
a high-dose spironolactone strategy in AHF. However, this was a single center non-randomized
study and the intervention was not blinded to the investigators, which raises concerns for
potential bias. While high dose MRA may be effective in the setting of congestion, increased
risks of hyperkalemia or elevation in creatinine also need to be studied further.24
In the EVEREST trial, which enrolled patients with left ventricular ejection fraction of
<40% who were hospitalized for acute heart failure and were receiving standard therapy, median
baseline aldosterone blood level was 11.0 ng/dL (25-75 percentile: 2-21 ng/dL and was over the
upper normal range in 33.2% of patients. Median aldosterone levels increased during hospital
stay from 11 ng/dL at baseline to 15 ng/dL at discharge (P<0.001) and remained increased 6
months after discharge (16 ng/dL, P<0.001 vs. baseline). Higher serum aldosterone levels
correlated with worse post-discharge outcomes. After a median follow-up of 9.9 months, higher
baseline aldosterone levels were associated with an increased risk for mortality and the combined
endpoint of cardiovascular mortality plus heart failure readmission in adjusted models (HR 1.49,
95% CI 1.11-1.99; and HR 1.40, 95% CI 1.11-1.78, respectively), in the highest quartile when
compared with the lowest.16
RISK FOR HYPERKALEMIA
Most of the data on hyperkalemia with MRAs is in chronic HF. In AHF, hypokalemia is more
common and is often due to a defect in Na+/K+-ATPase activity and an intracellular potassium
shift caused by oxidative stress and neurohormonal activation in combination with loop diuretic
use.25 Spironolactone is rapidly metabolized to several metabolites that produce natriuretic and

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
6
antikaliuretic effects.26 While the natriuretic effects decline over a period of 48-72 hours, the
antikaliuretic effects may be observed for several days following discontinuation, underscoring
the importance of careful monitoring of potassium levels, especially in patients with chronic
kidney disease.27 In a study in six chronic HF patients, 200mg bid of spironolactone led to
negative sodium balance without significant increases in potassium levels (3.9 to 4.1 mmol/L) or
changes in creatinine clearance after 4 days.21 In 18 patients with advanced HF receiving 50-200
mg of spironolactone in addition to standard treatment, there was no significant increase in
serum potassium (4.0 vs. 4.2 mEq/l) or creatinine (1.3 vs. 1.4 mg/dl) during an average follow up
of 41 weeks.28 In an AHF study assessing 50-100 mg spironolactone use, serum potassium did
not differ between control vs. spironolactone groups (3.9 vs. 4.1 mmol/L respectively) at day 3
(p=0.15). 23
ENDPOINTS IN ACUTE HEART FAILURE
Congestion is the most common manifestation of AHF and is related with both symptoms and
prognosis. Persistent congestion at discharge is associated with worse outcomes. The
effectiveness of decongestion can be measures in multiple ways.
Natriuretic Peptide Levels
Natriuretic peptide are markers of wall stretch and have advantage over clinical signs for
assessment of congestion due to the lack of sensitivity and inter-rater reliability of examination.
Even with symptom relief, readmission and mortality risk remains high if natriuretic peptides
stay elevated in patients with AHF. Baseline levels and changes in hospital are both associated
with filling pressures and outcomes, with best outcomes seen when natriuretic peptide levels
decrease by >30% in hospital.29 Discharge natriuretic peptide levels are superior to admission
levels or change in levels during hospitalization for predicting risk.30

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
7
Dyspnea
In several studies, dyspnea improvement in AHF was associated with improved outcomes post-
discharge. In the Acute Study of Clinical Effectiveness of Nesiritide in Decompensated Heart
Failure (ASCEND-HF) trial, early dyspnea relief measured on a 7-point Likert scale was
associated with lower 30-day mortality or HF hospitalization risk.31 In the Efficacy and Safety of
Relaxin for the Treatment of Acute Heart Failure (RELAX-AHF) trial, serelaxin was associated
with both improvement in dyspnea assessed by Visual Analog Scale and lower 6-month
mortality risk.32 Thus significant and early improvement in dyspnea may predict improved long-
term outcomes, besides being a therapeutic goal by itself.
Clinical Congestion Score
In the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study with Tolvaptan
(EVEREST) trial, a modified composite congestion score at discharge calculated by summing
the individual scores for orthopnea, jugular venous distension, and pedal edema (on a
standardized 4-point scale ranging from 0 to 3) was predictive of 30-day all-cause mortality (HR
1.34, 95%CI 1.14–1.58), and combined morality and HF readmission risk (HR 1.13, 95%CI
1.03–1.25).12
Mortality
Mortality reduction is the gold standard outcome for clinical trials in chronic heart failure.
Though several previous trials focused primarily on symptom improvement in clinical trials for
acute heart failure, it is now well recognized that symptom improvement during hospitalization is
an inconsistent predictor of post-discharge mortality.33, 34 In fact therapies like inotropes may
improve symptoms and worsen the risk for mortality. In-hospital mortality for patients with acute
heart failure is low but the main concern is the very high (up to 30% one-year) post discharge

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
8
mortality.35 Thus assessing post-discharge mortality as both an efficacy and safety outcome in
this high-risk group of acute heart failure patients is imperative.
Readmissions
Similar to mortality, readmission post discharge from an acute heart failure hospitalization also
remains a critical endpoint, both from a clinical and an economic perspective.36 From a clinical
perspective, recurrent hospitalizations are associated with a change in the natural history
trajectory of the disease process, with each hospitalization portending a worse prognosis
subsequently.37 From an economic perspective, recurrent hospitalizations account for the largest
proportion of direct cost of care for heart failure. Considering that heart failure is the number one
discharge diagnosis in the United States for the Medicare beneficiaries, there are now financial
penalties imposed by the Centers for Medicare and Medicaid Services for hospitals that have a
high rate of readmission post discharge after an acute heart failure hospitalization. Thus effective
therapies for these patients should preferably translate into a reduction in risk for readmissions.
In-hospital Worsening Heart Failure
Acute worsening heart failure (WHF) is reported in a sizable portion of patients hospitalized for
heart failure, and is increasingly being recognized as an entity that is associated with an adverse
in-hospital course.35 WHF is generally defined as worsening heart failure symptoms and signs
requiring an intensification of therapy, and is reported to be seen in anywhere from 5% to 42% of
heart failure admissions.37 Recent data suggest that some experimental therapies may reduce the
risk of development of WHF among hospitalized heart failure patients, and this is associated
with a reduction in the risk of subsequent post-discharge cardiovascular mortality.38 In this
respect, WHF holds promise as an endpoint for acute heart failure clinical trials. However, a
better understanding of the pathophysiology and a consensus on the definition of WHF is still

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
9
needed and until then, it serves as a potential secondary endpoint.
THE ALDOSTERONE TARGETED NEUROHORMONAL COMBINED WITH
NATRIURESIS THERAPY IN HEART FAILURE (ATHENA-HF) TRIAL
Study Design
The ATHENA-HF trial is a randomized, double blind, placebo controlled trial assessing the
impact of high dose spironolactone vs. placebo (or continued lose dose spironolactone use) on
natriuretic peptide levels among patients hospitalized for AHF. The study schema is presented in
the Central Illustration.
Objective
To determine if high-dose spironolactone administered to patients with AHF will lead to greater
reductions in N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels from randomization
to 96 hours compared to standard of care. In order to assess the early use of natriuretic doses of
spironolactone in AHF and its impact on preventing diuretic resistance, the study intervention is
initiated within 24 hours of the first dose of intravenous diuretics.
Eligibility and Intervention
Eligibility criteria are listed in Table 1. Patients hospitalized with at least one sign and one
symptoms of AHF with an NT-proBNP ≥1000 pg/mL or BNP ≥250 pg/mL measured within 24
hours from randomization are eligible. Patients who are either not on spironolactone therapy at
home or those who are on low dose spironolactone (12.5 or 25 mg per day) are eligible. Patients
must have serum potassium concentration ≤5.0mmol/L, an estimated glomerular filtration rate
(eGFR) ≥30 mL/min/1.73m2 and systolic blood pressure >90 mmHg.
Patients who are not on spironolactone at home are randomized to 100mg spironolactone
or placebo. Those already on 12.5 or 25 mg per day spironolactone are randomized to 100 mg or

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
10
25 mg per day but not to placebo, to avoid ethical concerns with discontinuing chronic therapy.
Patients on eplerenone will not be included as in the acute setting it may not be easily known if
the patient has been previously intolerant to spironolactone. Patients already taking >25 mg of
spironolactone will be excluded due to potential overlap with natriuretic potential of intermediate
dose spironolactone use.
Baseline Evaluations
Baseline evaluation includes history, physical examination, vital signs and body weight
assessment, review of medications, measurement of renal function and electrolytes, dyspnea
assessments (7-point Likert and Visual Analog Scale measured off oxygen for >3 minutes),
pregnancy test for women of childbearing potential, and collection of blood for core laboratory
measurement of NT-proBNP level.
Duration of Intervention
The median length of stay for HF hospitalization in the United States is 4.3 days.39 In order to
have comparable efficacy assessment within the two arms and avoid comparing outcomes among
patients with potentially different lengths of stay, and to conform with the prevalent norms of the
duration of hospitalization, the duration of intervention and the primary endpoint assessment was
chosen to be 96 hours.
Volume Assessment and Dose Adjustment
All other medications, including diuretics, are left at the discretion of the treating physician. The
study drug is discontinued after 96 hours and further MRA use is left to the treating physician’s
discretion. If the patient is clinically euvolemic in <96 hours, the investigators may consider
changing loop diuretics to oral dosing.
Ejection Fraction
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
11
Ejection fraction measured within 6 months prior to randomization is obtained. Those without
this information undergo ejection fraction assessment by any modality during the hospitalization.
Patients will be eligible regardless of ejection fraction and therefore this determination does not
need to precede randomization. Ejection fraction assessment is performed for a pre-specified
secondary analysis to ascertain possible differential effects of intervention in patients with
reduced vs. preserved ejection fraction.
Renal Function and Hyperkalemia
Modest increase in serum creatinine with diureses seen in many patients with AHF that usually
reverses over time. In some patients however, a rise in serum creatinine portend poor
prognosis.40 There remains clinical concern about acute kidney injury with high dose MRA use
in AHF. The decision regarding management of patients with worsening creatinine is left to the
discretion of the treating physicians. It is recommended that,
a. If serum creatinine is increased ≤0.5 mg/dl and the patient is diuresing and improving, and is
still fluid overloaded, continue study drug per protocol
b. If serum creatinine is increased >0.5 mg/dl and the patient is diuresing and clinically
improving but is still fluid overloaded, consider decreasing study drug to 50 mg
c. If the patient becomes oliguric with worsening serum creatinine and develops acute kidney
injury criteria, hold study drug and reassess in 24 hours
To closely follow the patients to mitigate the risk of hyperkalemia, electrolytes are
measured at least every 24h until 96h and at discharge. Potassium supplementation and
potassium containing salt substitutes are discontinued and high potassium containing foods are
avoided during the study protocol. Study drug dose is adjusted based on serum potassium level
as shown in Table 2.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
12
Endpoints
Efficacy
The primary endpoint of ATHENA-HF is the proportional change in NT-proBNP from
randomization to 96 hours. Multiple secondary endpoints from randomization to 96 hours are
also assessed, including, a) clinical congestion score; b) dyspnea relief by Likert and by Visual
Analog Scales; c) net urine output; d) weight change; e) loop diuretic dose need in furosemide
dose equivalents, and f) development of in-hospital worsening HF, defined as worsening HF
signs and symptoms requiring additional therapy.
Exploratory analyses include a day-30 post randomization telephone call to ascertain, a)
all-cause mortality, b) all-cause readmissions, c) outpatient worsening HF, defined as HF
readmission or emergency department visits or need for outpatient IV diuretics, d) MRA use and
loop diuretic dose requirement at day 30 and e) length of stay for index hospitalization. All
participants are also contacted by telephone at 60±3 days to assess vital status.
Safety
Safety endpoints include change in serum creatinine and incidence of hyperkalemia
(>5.5mmol/L or >6.0mmol/L) from randomization to 96 hours post randomization.
STATISTICAL CONSIDERATIONS
Sample Size and Power Calculations
Prior HF network data suggest that the standard deviation for the proportional change (on the log
scale) in NT-proBNP from randomization to 96 hours is approximately 0.55 to 0.60.41 It is
anticipated that 25% of subjects enrolled will be on low-dose MRA at randomization. Assuming
a 20% reduction in NT-proBNP from enrollment in the MRA group compared to placebo for the
subset of patients not on an MRA at enrollment and a 10% improvement in the subset on low-

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
13
dose MRA at baseline yields an overall benefit of 17.5% for the study population. With a 1:1
randomization and a two-sided type I error rate of 0.05, a total sample size of 360 subjects would
provide approximately 85% power. These calculations are based on the two-sample t-test. For
the sensitivity analysis using the worst-rank approach for missing values due to death, the total
sample size of 360 subjects provides 90% power to detect a difference in the setting in which a
randomly selected individual on high dose spironolactone has a 60% chance of having a better
response than a randomly selected individual on the placebo/low-dose arm. Both calculations
allow for a consent withdrawal rate of approximately 2%. For continuous secondary endpoints,
the study will have ≈90% power to detect differences of 0.35 standard deviations between
treatment groups. These calculations assume a common variance and normally distributed errors
for the two-sample t-test with a two-sided type I error rates of 0.05.
There is potential for greater reductions in natriuretic peptide levels in patients in the
placebo arm of the study based on the special expertise for heart failure management at the sites
where patients are being enrolled, though this is a concern with most heart failure trials where
the placebo arm outcomes are better than seen in real-life based on similar concerns.
Statistical Analysis
The primary analysis will be based on a regression model using an outcome variable based on
the log of the proportional change in NT-proBNP from randomization to 96 hours. The primary
analysis will use a linear regression model with an indicator variable for treatment assignment,
an indicator for MRA use prior to admission, and the log of the baseline NT-proBNP level.
Missing values of the 96-hour NT-proBNP levels will be imputed using a multiple imputation
algorithm.42 In a sensitivity analysis, values missing due to death will be imputed to the worst
possible value. This analysis will account for low-dose MRA at enrollment using a stratified

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
14
version of the Wilcoxon-Mann-Whitney test.
General linear models and nonparametric approaches will be used to analyze the
continuous outcomes. For binary outcomes, chi-square tests and Fisher’s exact test will be used
for unadjusted comparisons. For adjusted comparisons, logistic regression analysis will be used
to compare with the estimated odds ratio and 95% confidence interval. Unadjusted time-to-event
comparisons will be conducted using Kaplan-Meier survival estimates and log-rank tests. For
adjusted analyses, Cox proportional hazards regression models will be used to estimate hazard
ratios. Sensitivity analyses will be employed to assess the influence of informatively missing
values on the results. Subgroup analyses will be conducted based on baseline factors including;
MRA use prior to hospitalization, sex, preserved vs. reduced ejection fraction, and age ≥ or <65
years. Interim data analysis for efficacy and futility will not be conducted due to small size and
short duration of this trial. The safety analyses will be based on the entire randomized population.
Trial Status
The first patient in ATHENA HF trial was enrolled on December 13, 2014 and the last patient
was enrolled in May 2016. Follow up of the patients is ongoing.
CONCLUSION
There remains a need to find novel interventions that effectively and safely promote diuresis and
improve outcome in AHF. MRA therapy has shown benefit across the spectrum of chronic HF
with reduced ejection fraction and a suggestion of benefit in those with preserved ejection
fraction as well in certain regions.43 There are sound theoretical reasons to expect benefit with
high dose MRA therapy in AHF as well. If the ATHENA-HF trial shows promising results, it
will lay the groundwork for a more definite outcome trial in AHF. This is even more intriguing
considering the development of the novel selective MRA, finerenone that has shown benefit in

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
15
early phase trials in patients with worsening HF and chronic kidney disease,44 as well as the
growing literature on the efficacy and safety of chronic use of novel potassium binders to help
mitigate the complications related to the use of RAAS inhibitors.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
16
REFERENCES
1. Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, De Simone G, Ferguson TB,
Ford E, Furie K, Gillespie C, Go A, Greenlund K, Haase N, Hailpern S, Ho PM, Howard V,
Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A, McDermott MM, Meigs J, Mozaffarian
D, Mussolino M, Nichol G, Roger VL, Rosamond W, Sacco R, Sorlie P, Roger VL, Thom T,
Wasserthiel-Smoller S, Wong ND and Wylie-Rosett J. Heart disease and stroke statistics--2010
update: a report from the American Heart Association. Circulation. 2010;121:e46-e215.
2. Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, Flegal K, Ford E,
Furie K, Go A, Greenlund K, Haase N, Hailpern S, Ho M, Howard V, Kissela B, Kittner S,
Lackland D, Lisabeth L, Marelli A, McDermott M, Meigs J, Mozaffarian D, Nichol G,
O'Donnell C, Roger V, Rosamond W, Sacco R, Sorlie P, Stafford R, Steinberger J, Thom T,
Wasserthiel-Smoller S, Wong N, Wylie-Rosett J and Hong Y. Heart disease and stroke statistics-
-2009 update: a report from the American Heart Association Statistics Committee and Stroke
Statistics Subcommittee. Circulation. 2009;119:480-6.
3. Felker GM, Leimberger JD, Califf RM, Cuffe MS, Massie BM, Adams KF, Jr.,
Gheorghiade M and O'Connor CM. Risk stratification after hospitalization for decompensated
heart failure. Journal of cardiac failure. 2004;10:460-6.
4. Massie BM, O'Connor CM, Metra M, Ponikowski P, Teerlink JR, Cotter G, Weatherley
BD, Cleland JG, Givertz MM, Voors A, DeLucca P, Mansoor GA, Salerno CM, Bloomfield DM
and Dittrich HC. Rolofylline, an adenosine A1-receptor antagonist, in acute heart failure. The
New England journal of medicine. 2010;363:1419-28.
5. Chin MH and Goldman L. Correlates of early hospital readmission or death in patients
with congestive heart failure. The American journal of cardiology. 1997;79:1640-4.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
17
6. Yamokoski LM, Hasselblad V, Moser DK, Binanay C, Conway GA, Glotzer JM,
Hartman KA, Stevenson LW and Leier CV. Prediction of rehospitalization and death in severe
heart failure by physicians and nurses of the ESCAPE trial. Journal of cardiac failure.
2007;13:8-13.
7. Krumholz HM, Merrill AR, Schone EM, Schreiner GC, Chen J, Bradley EH, Wang Y,
Wang Y, Lin Z, Straube BM, Rapp MT, Normand SL and Drye EE. Patterns of hospital
performance in acute myocardial infarction and heart failure 30-day mortality and readmission.
Circulation Cardiovascular quality and outcomes. 2009;2:407-13.
8. Felker GM, Pang PS, Adams KF, Cleland JG, Cotter G, Dickstein K, Filippatos GS,
Fonarow GC, Greenberg BH, Hernandez AF, Khan S, Komajda M, Konstam MA, Liu PP,
Maggioni AP, Massie BM, McMurray JJ, Mehra M, Metra M, O'Connell J, O'Connor CM, Pina
IL, Ponikowski P, Sabbah HN, Teerlink JR, Udelson JE, Yancy CW, Zannad F and Gheorghiade
M. Clinical trials of pharmacological therapies in acute heart failure syndromes: lessons learned
and directions forward. Circulation Heart failure. 2010;3:314-25.
9. Vaduganathan M, Greene SJ, Ambrosy AP, Gheorghiade M and Butler J. The disconnect
between phase II and phase III trials of drugs for heart failure. Nature reviews Cardiology.
2013;10:85-97.
10. Gheorghiade M and Filippatos G. Reassessing treatment of acute heart failure syndromes:
the ADHERE Registry. European Heart Journal Supplements. 2005;7:B13-B19.
11. Gheorghiade M, Vaduganathan M, Fonarow GC and Bonow RO. Rehospitalization for
heart failure: problems and perspectives. Journal of the American College of Cardiology.
2013;61:391-403.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
18
12. Ambrosy AP, Pang PS, Khan S, Konstam MA, Fonarow GC, Traver B, Maggioni AP,
Cook T, Swedberg K, Burnett JC, Jr., Grinfeld L, Udelson JE, Zannad F and Gheorghiade M.
Clinical course and predictive value of congestion during hospitalization in patients admitted for
worsening signs and symptoms of heart failure with reduced ejection fraction: findings from the
EVEREST trial. European heart journal. 2013;34:835-43.
13. Lala A, McNulty SE, Mentz RJ, Dunlay SM, Vader JM, AbouEzzeddine OF, DeVore
AD, Khazanie P, Redfield MM, Goldsmith SR, Bart BA, Anstrom KJ, Felker GM, Hernandez
AF and Stevenson LW. Relief and Recurrence of Congestion During and After Hospitalization
for Acute Heart Failure: Insights From Diuretic Optimization Strategy Evaluation in Acute
Decompensated Heart Failure (DOSE-AHF) and Cardiorenal Rescue Study in Acute
Decompensated Heart Failure (CARESS-HF). Circulation Heart failure. 2015;8:741-8.
14. Pimenta J, Paulo C, Mascarenhas J, Gomes A, Azevedo A, Rocha-Goncalves F and
Bettencourt P. BNP at discharge in acute heart failure patients: is it all about volemia? A study
using impedance cardiography to assess fluid and hemodynamic status. International journal of
cardiology. 2010;145:209-14.
15. Drazner MH, Hellkamp AS, Leier CV, Shah MR, Miller LW, Russell SD, Young JB,
Califf RM and Nohria A. Value of clinician assessment of hemodynamics in advanced heart
failure: the ESCAPE trial. Circulation Heart failure. 2008;1:170-7.
16. Girerd N, Pang PS, Swedberg K, Fought A, Kwasny MJ, Subacius H, Konstam MA,
Maggioni A, Gheorghiade M and Zannad F. Serum aldosterone is associated with mortality and
re-hospitalization in patients with reduced ejection fraction hospitalized for acute heart failure:
analysis from the EVEREST trial. European journal of heart failure. 2013;15:1228-35.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
19
17. Abdallah JG, Schrier RW, Edelstein C, Jennings SD, Wyse B and Ellison DH. Loop
diuretic infusion increases thiazide-sensitive Na(+)/Cl(-)-cotransporter abundance: role of
aldosterone. Journal of the American Society of Nephrology : JASN. 2001;12:1335-41.
18. Mentz RJ, Stevens SR, DeVore AD, Lala A, Vader JM, AbouEzzeddine OF, Khazanie P,
Redfield MM, Stevenson LW, O'Connor CM, Goldsmith SR, Bart BA, Anstrom KJ, Hernandez
AF, Braunwald E and Felker GM. Decongestion strategies and renin-angiotensin-aldosterone
system activation in acute heart failure. JACC Heart failure. 2015;3:97-107.
19. Bansal S, Lindenfeld J and Schrier RW. Sodium retention in heart failure and cirrhosis:
potential role of natriuretic doses of mineralocorticoid antagonist? Circulation Heart failure.
2009;2:370-6.
20. RALES Investigators. Effectiveness of spironolactone added to an angiotensin-
converting enzyme inhibitor and a loop diuretic for severe chronic congestive heart failure (the
Randomized Aldactone Evaluation Study [RALES]). The American journal of cardiology.
1996;78:902-7.
21. Hensen J, Abraham WT, Durr JA and Schrier RW. Aldosterone in congestive heart
failure: analysis of determinants and role in sodium retention. American journal of nephrology.
1991;11:441-6.
22. van Vliet AA, Donker AJ, Nauta JJ and Verheugt FW. Spironolactone in congestive heart
failure refractory to high-dose loop diuretic and low-dose angiotensin-converting enzyme
inhibitor. The American journal of cardiology. 1993;71:21a-28a.
23. Ferreira JP, Santos M, Almeida S, Marques I, Bettencourt P and Carvalho H.
Mineralocorticoid receptor antagonism in acutely decompensated chronic heart failure. European
journal of internal medicine. 2014;25:67-72.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
20
24. Chamsi-Pasha MA, Dupont M, Al Jaroudi WA and Tang WH. Utilization pattern of
mineralocorticoid receptor antagonists in contemporary patients hospitalized with acute
decompensated heart failure: a single-center experience. Journal of cardiac failure. 2014;20:229-
35.
25. Seawell MR, Al Darazi F, Farah V, Ramanathan KB, Newman KP, Bhattacharya SK and
Weber KT. Mineralocorticoid receptor antagonism confers cardioprotection in heart failure.
Current heart failure reports. 2013;10:36-45.
26. Kolkhof P and Borden SA. Molecular pharmacology of the mineralocorticoid receptor:
prospects for novel therapeutics. Molecular and cellular endocrinology. 2012;350:310-7.
27. Sica DA. Pharmacokinetics and pharmacodynamics of mineralocorticoid blocking agents
and their effects on potassium homeostasis. Heart failure reviews. 2005;10:23-9.
28. Shchekochikhin D, Lindenfeld J and Schrier R. Increased Spironolactone in Advanced
Heart Failure: Effect of Doses Greater than 25 mg/Day on Plasma Potassium Concentration.
Cardiorenal medicine. 2013;3:1-6.
29. Bettencourt P, Azevedo A, Pimenta J, Frioes F, Ferreira S and Ferreira A. N-terminal-
pro-brain natriuretic peptide predicts outcome after hospital discharge in heart failure patients.
Circulation. 2004;110:2168-74.
30. O'Brien RJ, Squire IB, Demme B, Davies JE and Ng LL. Pre-discharge, but not
admission, levels of NT-proBNP predict adverse prognosis following acute LVF. European
journal of heart failure. 2003;5:499-506.
31. Mentz RJ, Hernandez AF, Stebbins A, Ezekowitz JA, Felker GM, Heizer GM, Atar D,
Teerlink JR, Califf RM, Massie BM, Hasselblad V, Starling RC, O'Connor CM and Ponikowski

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
21
P. Predictors of early dyspnoea relief in acute heart failure and the association with 30-day
outcomes: findings from ASCEND-HF. European journal of heart failure. 2013;15:456-64.
32. Filippatos G, Teerlink JR, Farmakis D, Cotter G, Davison BA, Felker GM, Greenberg
BH, Hua T, Ponikowski P, Severin T, Unemori E, Voors AA and Metra M. Serelaxin in acute
heart failure patients with preserved left ventricular ejection fraction: results from the RELAX-
AHF trial. European heart journal. 2014;35:1041-50.
33. Packer M, Colucci W, Fisher L, Massie BM, Teerlink JR, Young J, Padley RJ, Thakkar R,
Delgado-Herrera L, Salon J, Garratt C, Huang B and Sarapohja T. Effect of levosimendan on the
short-term clinical course of patients with acutely decompensated heart failure. JACC Heart
failure. 2013;1:103-11.
34. Konstam MA, Gheorghiade M, Burnett JC, Jr., Grinfeld L, Maggioni AP, Swedberg K,
Udelson JE, Zannad F, Cook T, Ouyang J, Zimmer C and Orlandi C. Effects of oral tolvaptan in
patients hospitalized for worsening heart failure: the EVEREST Outcome Trial. Jama.
2007;297:1319-31.
35. Chen J, Normand SL, Wang Y and Krumholz HM. National and regional trends in heart
failure hospitalization and mortality rates for Medicare beneficiaries, 1998-2008. Jama.
2011;306:1669-78.
36. Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de
Ferranti S, Despres JP, Fullerton HJ, Howard VJ, Huffman MD, Isasi CR, Jimenez MC, Judd SE,
Kissela BM, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Magid DJ, McGuire DK, Mohler
ER, 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L,
Pandey DK, Reeves MJ, Rodriguez CJ, Rosamond W, Sorlie PD, Stein J, Towfighi A, Turan TN,
Virani SS, Woo D, Yeh RW and Turner MB. Executive Summary: Heart Disease and Stroke

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
22
Statistics--2016 Update: A Report From the American Heart Association. Circulation.
2016;133:447-54.
37. Butler J, Gheorghiade M, Kelkar A, Fonarow GC, Anker S, Greene SJ, Papadimitriou L,
Collins S, Ruschitzka F, Yancy CW, Teerlink JR, Adams K, Cotter G, Ponikowski P, Felker GM,
Metra M and Filippatos G. In-hospital worsening heart failure. European journal of heart failure.
2015;17:1104-13.
38. Weatherley BD, Milo-Cotter O, Felker GM, Uriel N, Kaluski E, Vered Z, O'Connor CM,
Adams KF and Cotter G. Early worsening heart failure in patients admitted with acute heart
failure--a new outcome measure associated with long-term prognosis? Fundamental & clinical
pharmacology. 2009;23:633-9.
39. Adams KF, Jr., Fonarow GC, Emerman CL, LeJemtel TH, Costanzo MR, Abraham WT,
Berkowitz RL, Galvao M and Horton DP. Characteristics and outcomes of patients hospitalized
for heart failure in the United States: rationale, design, and preliminary observations from the
first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE).
American heart journal. 2005;149:209-16.
40. Logeart D, Tabet JY, Hittinger L, Thabut G, Jourdain P, Maison P, Tartiere JM and Solal
AC. Transient worsening of renal function during hospitalization for acute heart failure alters
outcome. International journal of cardiology. 2008;127:228-32.
41. Bart BA, Goldsmith SR, Lee KL, Givertz MM, O'Connor CM, Bull DA, Redfield MM,
Deswal A, Rouleau JL, LeWinter MM, Ofili EO, Stevenson LW, Semigran MJ, Felker GM,
Chen HH, Hernandez AF, Anstrom KJ, McNulty SE, Velazquez EJ, Ibarra JC, Mascette AM and
Braunwald E. Ultrafiltration in decompensated heart failure with cardiorenal syndrome. The New
England journal of medicine. 2012;367:2296-304.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
23
42. Schafer JL. Multiple imputation: a primer. Statistical methods in medical research.
1999;8:3-15.
43. Pfeffer MA, Claggett B, Assmann SF, Boineau R, Anand IS, Clausell N, Desai AS, Diaz
R, Fleg JL, Gordeev I, Heitner JF, Lewis EF, O'Meara E, Rouleau JL, Probstfield JL,
Shaburishvili T, Shah SJ, Solomon SD, Sweitzer NK, McKinlay SM and Pitt B. Regional
variation in patients and outcomes in the Treatment of Preserved Cardiac Function Heart Failure
With an Aldosterone Antagonist (TOPCAT) trial. Circulation. 2015;131:34-42.
44. Pitt B, Anker SD, Bohm M, Gheorghiade M, Kober L, Krum H, Maggioni AP,
Ponikowski P, Voors AA, Zannad F, Nowack C, Kim SY, Pieper A, Kimmeskamp-Kirschbaum
N and Filippatos G. Rationale and design of MinerAlocorticoid Receptor antagonist Tolerability
Study-Heart Failure (ARTS-HF): a randomized study of finerenone vs. eplerenone in patients
who have worsening chronic heart failure with diabetes and/or chronic kidney disease. European
journal of heart failure. 2015;17:224-32.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
24
FIGURE LEGENDS
Figure 1: Mechanism of Diuretic Resistance and Potential Benefit with Mineralocorticoid
Antagonists
From Bansal S, Lindenfeld J, Schrier RW. Sodium Retention in Heart Failure and Cirrhosis:
Potential Role of Natriuretic Doses of Mineralocorticoid Antagonist? Circ Heart Fail 2009:2:373.
Reprinted with permission of Wolters Kluwer Health
Central Illustration: ATHENA-HF Trial Schema
AHF: acute heart failure; BNP: B-type natriuretic peptide; Cr: creatinine; eGFR: estimated
glomerular filtration rate; K+: potassium; MRA: mineralocorticoid receptor antagonist;
NTproBNP: N terminal pro B-type natriuretic peptide

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFigure 1

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTCentral Illustration
MANUSCRIP
T
ACCEPTED
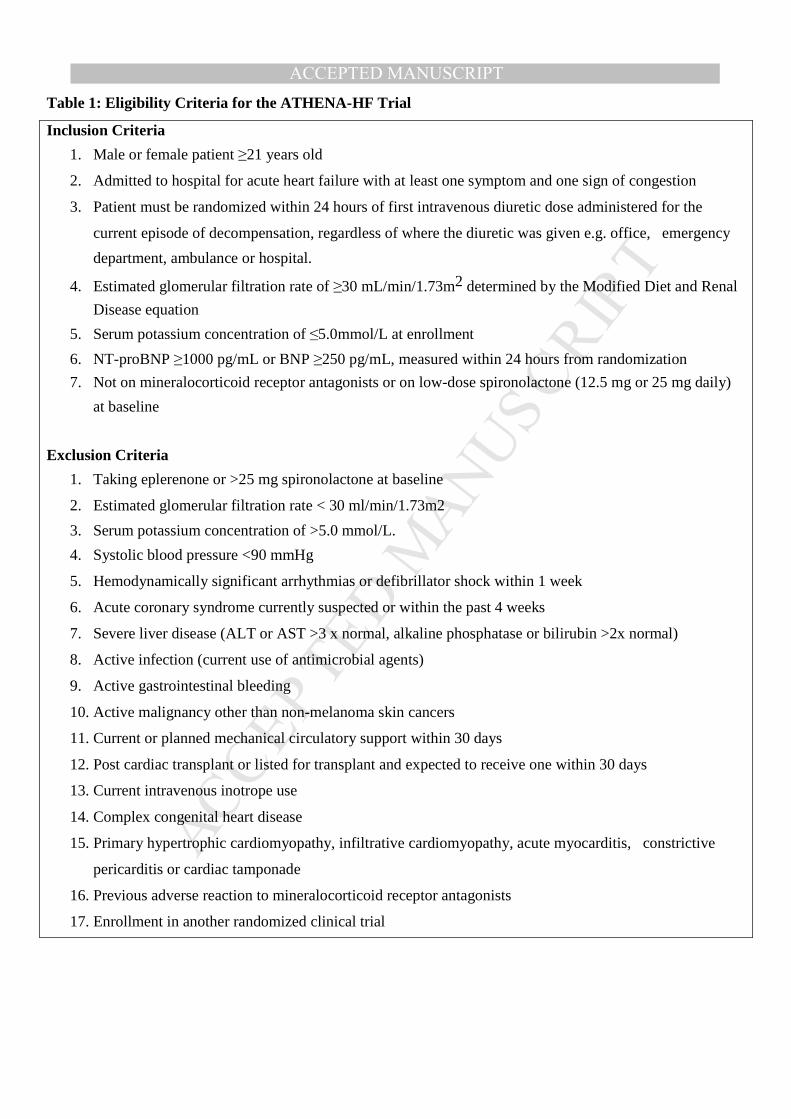
ACCEPTED MANUSCRIPTTable 1: Eligibility Criteria for the ATHENA-HF Trial
Inclusion Criteria
1. Male or female patient ≥21 years old
2. Admitted to hospital for acute heart failure with at least one symptom and one sign of congestion
3. Patient must be randomized within 24 hours of first intravenous diuretic dose administered for the
current episode of decompensation, regardless of where the diuretic was given e.g. office, emergency
department, ambulance or hospital.
4. Estimated glomerular filtration rate of ≥30 mL/min/1.73m2 determined by the Modified Diet and Renal
Disease equation
5. Serum potassium concentration of ≤5.0mmol/L at enrollment
6. NT-proBNP ≥1000 pg/mL or BNP ≥250 pg/mL, measured within 24 hours from randomization
7. Not on mineralocorticoid receptor antagonists or on low-dose spironolactone (12.5 mg or 25 mg daily)
at baseline
Exclusion Criteria
1. Taking eplerenone or >25 mg spironolactone at baseline
2. Estimated glomerular filtration rate < 30 ml/min/1.73m2
3. Serum potassium concentration of >5.0 mmol/L.
4. Systolic blood pressure <90 mmHg
5. Hemodynamically significant arrhythmias or defibrillator shock within 1 week
6. Acute coronary syndrome currently suspected or within the past 4 weeks
7. Severe liver disease (ALT or AST >3 x normal, alkaline phosphatase or bilirubin >2x normal)
8. Active infection (current use of antimicrobial agents)
9. Active gastrointestinal bleeding
10. Active malignancy other than non-melanoma skin cancers
11. Current or planned mechanical circulatory support within 30 days
12. Post cardiac transplant or listed for transplant and expected to receive one within 30 days
13. Current intravenous inotrope use
14. Complex congenital heart disease
15. Primary hypertrophic cardiomyopathy, infiltrative cardiomyopathy, acute myocarditis, constrictive
pericarditis or cardiac tamponade
16. Previous adverse reaction to mineralocorticoid receptor antagonists
17. Enrollment in another randomized clinical trial

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTTable 2: Protocol for Study Drug Adjustment based on Serum Potassium Concentration
Serum
Potassium
concentration
Action Protocol
< 5.0 mmol/L Continue protocol
5.1-6.0 mmol/L Check if sample hemolyzed
Hold protocol
Repeat K within 6 hours Check if K+ supplement given
Treat per physician preference
If repeat value is <5.0 - Continue protocol
If repeat value is 5.1-6.0
Treat according to physician preference
Hold protocol
Repeat K next day and follow
protocol
If day 4 – Stop study protocol
If repeat value is >6.0 Stop study drug
> 6.0 mmol/L Check if sample hemolyzed
Check if K+ supplement given
Treat per physician preference
If sample not hemolyzed and patient not on K+
supplements
Stop study drug
If sample hemolyzed or patient receiving K+
supplements -
Repeat K within 6 hours
If repeat value is <5.0 Continue protocol
If repeat value is between 5.1-6.0 Hold protocol
Repeat K next day and follow
protocol
If day 4 – Stop study drug
If repeat value is >6.0 Stop study drug










![1 Heart Failure [HF]. 2 Definition of HF Heart failure is a complex clinical syndrome that can result from any structural or functional cardiac disorder](https://img.dokumen.tips/doc/110x75/56649d415503460f94a1bd01/1-heart-failure-hf-2-definition-of-hf-heart-failure-is-a-complex-clinical.jpg)


















