Embed Size (px)
DESCRIPTION
Nasopalatine Dust cyst
Citation preview
Chhattisgarh Journal of Health Sciences, September 2013;1(1) :
IntroductionThe nasopalatine duct communicates the nasal cavity with the anterior region of the upper maxilla. It is located on the midline and palatine to the upper maxilla, above the retroincisor palatal papilla. During fetal development the duct gradually narrows until one or two central clefts are finally formed on the midline of the upper maxilla. The nasopalatine neurovascular bundle is located within the duct, and emerges from its intrabony trajectory through the nasopalatine foramen. Nasopalatine duct cyst (NPDC) was first described by Meyer in 1914. It is also termed as incisive canal cyst, arising from embryologic remnants of
1nasopalatine duct.NPDCs are the most common non-odontogenic
cysts of the oral cavity, representing up to 1% of all 2 maxillary cysts. These lesions are almost three times more
frequent in males than in females. The maximum incidence is between 40 and 60 years of age.Trauma, infection of the duct and mucous retention of the adjacent minor salivary gland have been mentioned as possible etiological factors, but the role of each have been questioned. A l t h o u g h pathogenesis of this lesion is still uncertain, the lesion most likely represents a spontaneous cystic degeneration of the remnants of nasopalatine duct. The differential diagnosis is established with the following conditions: an enlarged nasopalatine duct, central giant cell granuloma, a central incisor root cyst or other maxillary cysts, osteitisfistulizing in the palatine direction, or a bucco-nasal and/or bucco-sinunasal communication. Treatment in all cases involves complete surgical removal as soon as possible after
3diagnosis. The definite diagnosis of the cyst should be based on clinical, radiological and histopathologic findings. Hence, we report a case of nasopalatine duct cyst in a 33 year old male patient, along with a review of literature.
CASE REPORT
Nasopalatine Duct Cyst: A Rare Case Report1 2 3 4 5
Chinar Fating , Rolly Gupta , Mekhala Lanjewar Barkha Nayak Anurag Bakshi , Rajkumar 6Diwan
1. Senior Lecturer, Department of Oral Medicine and Radiology, Chhattisgarh Dental College and Research Institute, Rajnandgaon, Chhattisgarh, India.
2. Senior Lecturer, Department of Oral and Maxillofacial Pathology and Microbiology, Chhattisgarh Dental College and Research Institute, Rajnandgaon, Chhattisgarh, India
3. Oral Medicine and Radiology(MDS)4. Senior lecturer, department of oral pathology, Matri dental college, Anjora Durg, CG 5. Post gradute student department of oral medicine and radiology, Matri Dental college Anjora Durg CG 6. Oral medicine and radiology (MDS)
Corresponding Address:Dr.Chinar Fating, SeniorLecturer, Department of Oral Medicine and Radiology, Chhattisgarh Dental College and Research Institute, Rajnandgaon, Chhattisgarh, India.
Abstract There are several developmental cysts derived from embryonic structures or faults in their remnants located in oro-facial region. Nasopalatine duct cyst (NPDC) is the most common of all the developmental, epithelial and non-odontogenic cysts of the maxilla. This cyst originates from epithelial remnants from the nasopalatine duct. The cells could be activated spontaneously during life, or are eventually stimulated by the irritating action of various agents (infection, etc.). Generally, the patients present without clinical signs and symptoms. Therefore, the tentative diagnosis “nasopalatine duct cyst” is often based on a coincidental radiological finding on a routine panoramic view or occlusal radiograph. Although NPDC is not rare, it is mostly misdiagnosed. The definite diagnosis should be based on clinical, radiological and histopathologic findings. We report a case of infected nasopalatine duct cyst in a 35 year old male patient along with briefliterature review.
Key words: Developmental Cyst, Nasopalatine Duct Cyst, Nonodontogenic Cysts.
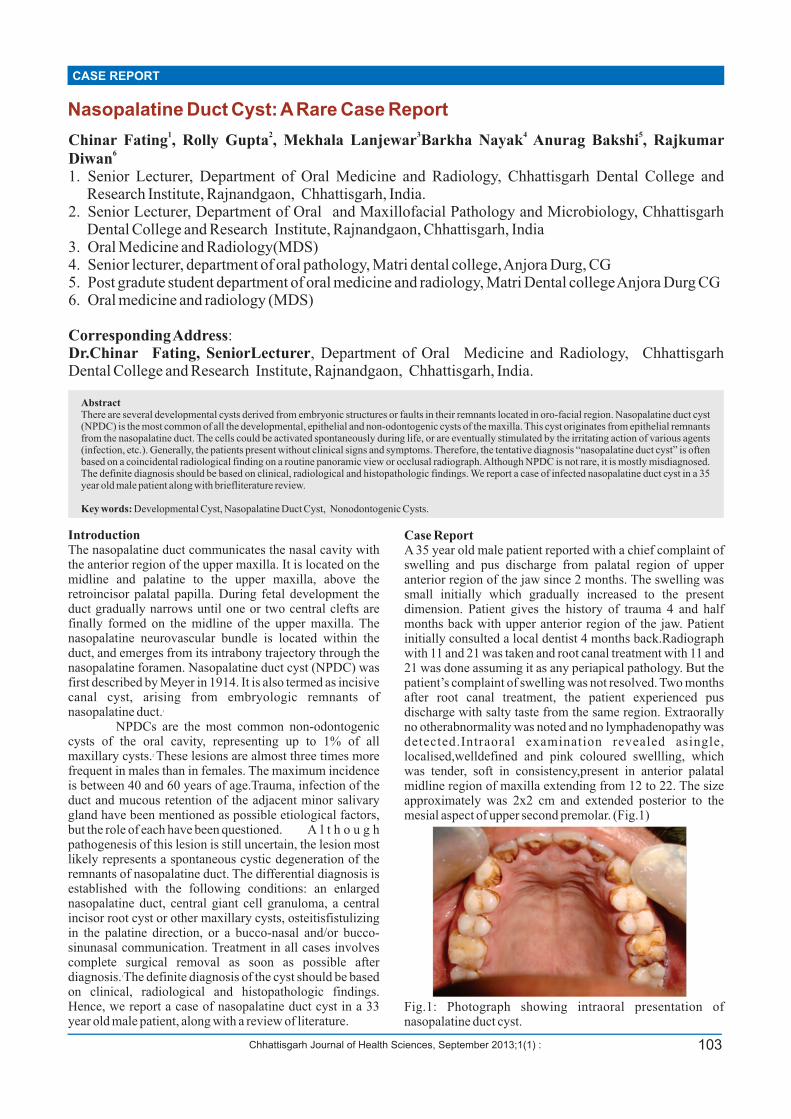
Case ReportA 35 year old male patient reported with a chief complaint of swelling and pus discharge from palatal region of upper anterior region of the jaw since 2 months. The swelling was small initially which gradually increased to the present dimension. Patient gives the history of trauma 4 and half months back with upper anterior region of the jaw. Patient initially consulted a local dentist 4 months back.Radiograph with 11 and 21 was taken and root canal treatment with 11 and 21 was done assuming it as any periapical pathology. But the patient’s complaint of swelling was not resolved. Two months after root canal treatment, the patient experienced pus discharge with salty taste from the same region. Extraorally no otherabnormality was noted and no lymphadenopathy was detected.Intraoral examination revealed asingle, localised,welldefined and pink coloured swellling, which was tender, soft in consistency,present in anterior palatal midline region of maxilla extending from 12 to 22. The size approximately was 2x2 cm and extended posterior to the mesial aspect of upper second premolar. (Fig.1)
Fig.1: Photograph showing intraoral presentation of nasopalatine duct cyst.
103
Radiological examination by intraoral periapical &occlusal radiograph showed a single well circumscribed oval shaped radiolucency with well corticated borders. Size was 1x1 cm, location was in midline of anterior maxilla between the roots of central incisors. (Fig. 2,3) On the basis of clinical and radiological evidence the provisional diagnosis ofincisive papilla cyst, nasopalatine duct cyst and chronic periapical granuloma was given. It was decided to enucleate the cyst under local anaesthesia. Prior to surgery all preliminary investigation were done and results were within normal limits. Palatal mucoperiosteal flap was raised to expose the cyst (Fig. 4). A friable, haemmorhagic cyst lining was curetted and sent for histopathological examination. The flap was sutured back in its original position. Patient was called for suture removal one week postoperatively and healing was satisfactory and uneventful(Fig. 5, 6).
Fig. 2&3: Intraoral periapicaland
occlusalradiographshowing single well circumscribed oval shaped radiolucency with well corticated borders ofsize 1x1 cm, located in midline of anterior maxilla between the roots of central incisiors.
Fig. 4: Photograph showing haemorrhagic appearing cyst after mucoperiosteal flap was raised.
Fig. 5: 1 week post operative intraoral clinical photograph.
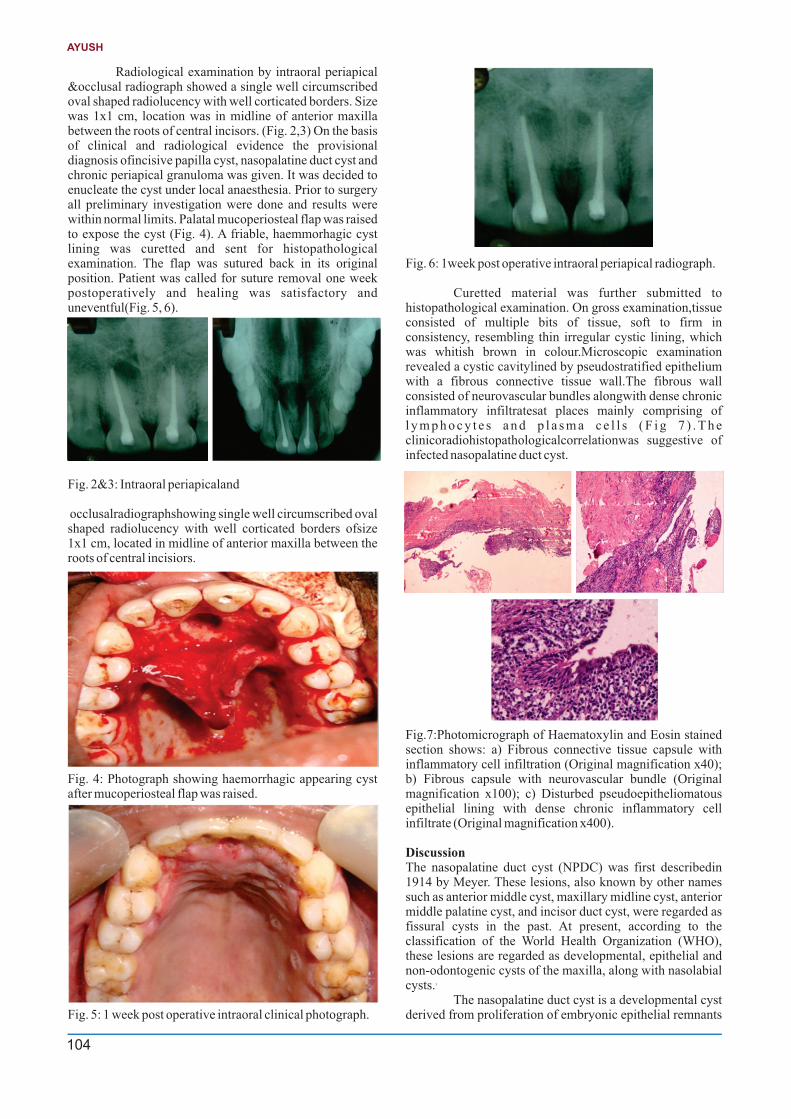
Fig. 6: 1week post operative intraoral periapical radiograph.
Curetted material was further submitted to histopathological examination. On gross examination,tissue consisted of multiple bits of tissue, soft to firm in consistency, resembling thin irregular cystic lining, which was whitish brown in colour.Microscopic examination revealed a cystic cavitylined by pseudostratified epithelium with a fibrous connective tissue wall.The fibrous wall consisted of neurovascular bundles alongwith dense chronic inflammatory infiltratesat places mainly comprising of l y m p h o c y t e s a n d p l a s m a c e l l s ( F i g 7 ) . T h e clinicoradiohistopathologicalcorrelationwas suggestive of infected nasopalatine duct cyst.
Fig.7:Photomicrograph of Haematoxylin and Eosin stained section shows: a) Fibrous connective tissue capsule with inflammatory cell infiltration (Original magnification x40); b) Fibrous capsule with neurovascular bundle (Original magnification x100); c) Disturbed pseudoepitheliomatous epithelial lining with dense chronic inflammatory cell infiltrate (Original magnification x400).
Discussion The nasopalatine duct cyst (NPDC) was first describedin 1914 by Meyer. These lesions, also known by other names such as anterior middle cyst, maxillary midline cyst, anterior middle palatine cyst, and incisor duct cyst, were regarded as fissural cysts in the past. At present, according to the classification of the World Health Organization (WHO), these lesions are regarded as developmental, epithelial and non-odontogenic cysts of the maxilla, along with nasolabial
3cysts.The nasopalatine duct cyst is a developmental cyst
derived from proliferation of embryonic epithelial remnants
104
AYUSH

Chhattisgarh Journal of Health Sciences, September 2013;1(1) :
of the nasopalatine duct. It may occur at any age but it is seen most often in fourth to sixth decades of life. The etiology underlying these lesions is not clear, though in addition to the hypothesis of spontaneous proliferation from embryonic tissue remains, other possible etiologies have been proposed. Trauma, infection, and mucous retention within associated salivary gland ducts have all been suggested as possible pathogenetic factors; however, most believe that spontaneous cystic degeneration of residual ductal
3,4epithelium is the most likely etiology and some genetic 5determinants have been suggested. As far as pathogenesis
isconcerned, it was previously thought that the NPDCs originatedfrom the trapping of epithelium during fusion of theembryological processes. This concept has been discarded,and currently NPDC is thought to develop from theepithelial remnants of the nasopalatine ducts present
2,6,7withinthe incisive canals (canals of Stenson).Nasopalatine duct cysts affect a wide age range, however, most present in the fourth through sixth decades of life. There is a slight male predilection. Patients may be asymptomatic, with the lesion being detected on routine radiographs, however, many will present with one or more symptoms. Complaints are often found to be associated with an infection of a previously asymptomatic nasopalatine duct cyst and consist primarily of swelling, drainage of pus and
6pain. The vitality of nearby teeth is not affected; however, it is not uncommon to see evidence of endodontic therapy because the nasopalatine duct cyst has been previously clinically misdiagnosed as a periapical cyst or granuloma. In our case, patient came with complaint of swelling and salty discharge. The incisive canal is a fusion line that occurs during facial development. The nasopalatine ducts are small paired openings in the midline of the anterior palate transmitting the nasopalatine artery and nerve as well as remnants of the embryonic nasopalatine duct. The incisive canal is bilateral on the nasal side and single at the oral side (incisive foramen). The normal size of the normalforamen is highly variable, but most authors agree that 6 mm should beregarded as the upper limit for a normal incisive canal. Radiolucencies largerthan this diameter should be considered potent ia l ly pathologic and mer i t
8 furtherinvestigation. However, the incisive foreman, by convention, is not expected to exceed 6 mm in diameter, making the detection of a small nasoplatine duct cyst difficult. NPDCs are usually central or unilateral with no prevalence of side occurrence. Radiographically, nasopalatine ducts cysts are usually well-circumscribed radiolucencies of the anterior maxilla.The cysts are apical to the roots of the maxillary incisors and rarely cause root resorption. Cysts are round, ovoid or some lesions may appear heart-shaped, either because they become notched by the nasal septum during their expansion or because the nasal spine is superimposed on the radiolucent area. Cysts range in size, with an average diameter of approximately 1.5 cm.Due to similar signs and symptoms, the NPDC may be misdiagnosed as a periapical lesion. This is why many authors believe that its prevalence is actually higher than presented in the literature. Although a large NPDC might show the adjacent incisors roots to be within the cystic cavity, the lamina dura will be intact and the pulp usually vital whereas a radicular cyst is associated with a pulpless tooth and involve a portion of the root, usually with loss of continuity of the lamina dura. In the reported case, adental
practitionerconsidered it to be a radicular cyst and carried out the root canal treatment with upper central incisors. Thus, in establishing a diagnosis of NPDC it is important to attempt to exclude the possibility of a periapical lesion by performing the pulp vitality tests of the incisor teeth.Histologically, the nasopalatine duct cyst is lined by stratified squamous epithelium alone or in combination with: pseudostratified columnar epithelium (with or without cilia and/or goblet cells), simple columnar epithelium, and simple cuboidal epithelium. The fibrous wall generally contains nerves, arteries and veins. Additionally, minor salivary gland tissue and small islands of cartilage may be found. Finally, if the cyst is infected, acute and chronic inflammatory cells will
9be seen throughout the specimen.The differential diagnosis must be established with other conditions such as an enlarged nasopalatine duct (less than 6 mm in diameter), central giant cell granuloma, a root cyst associated to the upper central incisors, a supernumerary tooth follicular cyst (normally mesiodens), primordial cyst, nasoalveolar cyst, osteitis with palatal fistulisation, and
10bucconasal and/or buccosinusal communication. Other diagnostic techniques can be used to radiologically assess lesions of this kind, such as multimodal tomography, which in addition to exposing the patient to lesser radiation doses employs crossed and sectional tomographic acquisitions in
11the sagittal plane to yield threedimensional images. Magnetic resonance imaging (MRI) may also prove useful in establishing the diagnosis, and particularly contrast the interior of the NPDC with a high signal intensity. Specific axial T1-weighted imaging reflects the presence of fluid, viscous and protein material within the cyst, and abundant keratin at superficial level. Thus, MRI is highly reliable in diagnosing NPDCs, discarding root cysts or any other cysts
1,12of odontogenicorigin.The treatment of choice is surgical excision of the cyst, although some authors propose marsupialization of large NPDCs. The nasopalatine neurovascular bundle is a delicate and highly vascularised structure giving rise to profuse bleeding if inadvertently sectioned during surgery. Electrocoagulation is required in such cases. Paresthesia of the anterior palatal zone is a rare complication found in 10% of the cases, on removal of nerve endings of the nasopalatine nerve along with the membrane of the cyst.Frequently the biopsy procedure results in adequate treatment. Recurrence
3,9, 13is rare.A very rare complication associated with long
standing NPDC is squamous cell carcinomas originating in maxillary bone. This is due to the metaplasia seen in the epithelial wall of a cyst or of the epithelial remains that participated in odontogenesis. Therefore, there are cases in which NPDC gives rise to squamous cell carcinoma in the
14anterior zone of the upper maxilla. This explains the need for early removal of the NPDC, with the purpose of minimizing
15the risks and complications.
CONCLUSIONNasopalatine duct cysts are the most common nonodontogenic cyst of the oral cavity seen in the general population. NPDCs must be distinguished from other maxillary anterior radiolucencies. In establishing a diagnosis of NPDC and for avoiding irrational endodontic treatment, it is important to attempt to exclude the possibility of a periapical lesion by performing the pulp vitality tests of the incisor teeth. The final diagnosis could only be performed after histological analysis.
105
Nasopalatine Duct Cyst: A Rare Case Report

References
1. Robertson H, Palacios E. Nasopalatine duct cyst. Ear Nose Throat J. 2004;83(5):313.
2. Shear M, Speight PM. Cysts of the oral and maxillofacial regions. 4th ed. Oxford; Ames, Iowa: Blackwell Munksgaard 2007.
3. Francol JE, Marque NA, Ayte LB, Escoda CG. Nasopalatine duct cyst: report of 22 cases and review of the literature. Med Oral Patol Oral Cir Bucal. 2008;13(7):E438–43.
4. Gnanasekhar JD, Walvekar SV, Al-Kandari AM, Al-Duwairi Y. Misdiagnosis and mismanagement of a nasopalatine duct cyst and its corrective therapy. A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;(4):465-70.
5. Nortje CJ, Farman AG. Nasopalatine duct cyst: an aggressive condition in adolescent negroes from South Africa? Int J Oral Surg 1978; 7(2): 65-72.
6. Swanson KS, Kaugars GE, Gunsolley JC. Nasopalatine duct cyst:an analysis of 334 cases. J Oral MaxillofacSurg 1991; 49(3): 268-71.
7. Allard RH, van der Kwast WA, van der Waal I. Nasopalatine duct cyst. review of the literature and report of 22 cases. Int J Oral Surg 1981; 10(6): 447-61.
8. De Cuyper K, Vanhoenacker FM, Hintjens J, Verstraete KL, Parizel PM. Nasopalatine duct cyst. In images in clinical radiology. JBR–BTR, 2008, 91: 179.
9. Vasconcelos R, de Aguiar MF, Castro W, de Arau´jo VC, Mesquita R. Retrospective analysis of 31 cases of nasopalatine duct cyst.Oral Dis. 1999;5(4):325–8.
10. Moss HD, Hellstein JW, Johnson JD. Endodontic considerations of the nasopalatine duct region. J Endod. 2000;26(2):107-10.
11. Harris IR, Brown JE. Application of cross-sectional imaging in the differential diagnosis of apical radiolucency. IntEndod J. 1997;30(4):288-90.
12. Hisatomi M, Asaumi J, Konouchi H, Matsuzaki H, Kishi K. MR imaging of nasopalatine duct cysts. Eur J
Radiol. 200;39(2):73-6.13. Elliott KA, Franzese CB, Pitman KT. Diagnosis and
surgical management of nasopalatine duct cysts. Laryngoscope. 2004;114(8):1336-40.
14. Takagi R, Ohashi Y, Suzuki M. Squamous cell carcinoma in the maxilla probably originating from a nasopalatine duct cyst: report of case. J Oral Maxillofac Surg. 1996; 54(1):112-5.
15. Velasquez-Smith MT, Mason C, Coonar H, Bennett J. A nasopalatine cyst in an 8-year-old child. Int J Paediatr Dent. 1999;9(2):123-127.
Figure Legends Figure 1. Photograph showing intraoral presentation of nasopalatine duct cyst.Figure 2&3. Occlusal and intraoral periapical radiographshowing single well circumscribed oval shaped radiolucency with well corticated borders ofsize 1x1 cm, located in midline of anterior maxilla between the roots of central incisiors.Figure 4. Photograph showing haemorrhagic appearing cyst after mucoperiosteal flap was raised.Figure 5. Photomicrograph of Haematoxylin and Eosin stained section shows: a) Fibrous connective tissue capsule with inflammatory cell infiltration (Original magnification x40); b) Fibrous capsule with neurovascular bundle (Original magnification x100); c) Disturbed pseudoepitheliomatous epithelial lining with dense chronic inflammatory cell infiltrate (Original magnification x400).Figure 5. 1 week post operative intraoral clinical photograph.Figure 6. 1week post operative intraoral periapical radiograph.
106
AYUSH