Embed Size (px)
Citation preview

Narrow QRS Tachycardia withVentriculoatrial Block
Frederick T. Han, MDa, Vasanth Vedantham, MD, PhDb,*KEYWORDS
� Nodofascicular pathway � Nodoventricular pathway � Junctional tachycardia� Narrow-complex tachycardia with atrioventricular dissociation
KEY POINTS
� Narrow-complex tachycardia with ventriculoatrial (VA) dissociation is rare.
� The differential diagnosis for narrow-complex tachycardia with VA dissociation includes junctionaltachycardia, AV nodal reentrant tachycardia with upper common pathway block, and a circus-movement tachycardia using a concealed nodofascicular or nodoventricular pathway.
� Although baseline tachycardia characteristics can suggest one or another of these mechanisms,pacing maneuvers are required to make a definitive diagnosis in these difficult cases.
CLINICAL PRESENTATION
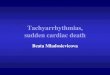
A 40-year-old athletic man presented for evalua-tion andmanagement of exercise-induced palpita-tions. Initially the palpitations occurred only withstrenuous exercise and resolved with rest.However, in the months before presentation,palpations occurred more frequently with lessstrenuous activity. Physical examination, labora-tory studies, and an echocardiogram were allnormal. Ambulatory monitoring revealed thatpalpitations correlated with a narrow-complextachycardia that occurred during exercise(Fig. 1). The patient was referred for considerationof catheter ablation.
ELECTROPHYSIOLOGY STUDY ANDABLATIONTachycardia Induction
Quadripolar electrode catheters were positionedin the high right atrium, right ventricular apex,and the His bundle region. A decapolar electrodecatheter was placed in the coronary sinus. Normalintervals were recorded in sinus rhythm, and
a Division of Cardiology, University of Utah Health ScieLake City, UT 84132, USA; b Cardiac Electrophysiology SSan Francisco, San Francisco, CA, USA* Corresponding author. Cardiac Electrophysiology SectFrancisco, 505 Parnassus Avenue, M1179D, Box 0124, SanE-mail address: [email protected]
Card Electrophysiol Clin 4 (2012) 531–536http://dx.doi.org/10.1016/j.ccep.2012.08.0301877-9182/12/$ – see front matter � 2012 Elsevier Inc. All
ventriculoatrial (VA) conduction was present withconcentric retrograde activation and a long VAtime. Tachycardia could not be induced with atrialoverdrive pacing or programmed stimulation fromthe right atrium or coronary sinus with or withoutisoproterenol. Sustained narrow QRS complextachycardia at a cycle length of 300 to 330 milli-seconds was induced with ventricular overdrivepacing after isoproterenol infusion at 1 mg/min(Fig. 2). Strikingly and unexpectedly, narrow-complex tachycardia was induced and persistedwith complete VA dissociation.
Question
What is the differential diagnosis for narrow-complex tachycardia with VA block and how canthe tachycardia mechanism be established?
Tachycardia Characteristics
Two VA relationships were observed during tachy-cardia. Tachycardia showed either complete VAblock or 2:1 VA conduction, occasionally transi-tioning from one to the other without interruption
nces Center, 30 North 1900 East, Room 4A100, Saltection, Cardiology Division, University of California
ion, Cardiology Division, University of California SanFrancisco, CA 94122-0124.
rights reserved. cardiacEP.th
eclinics.com

Fig. 1. Ambulatory monitor with narrow QRS tachycardia. Single-lead electrocardiogram shows initiation ofnarrow-complex tachycardia during mild exertion. P waves are not clearly visible during tachycardia, leavinga broad differential diagnosis.
Han & Vedantham532
of tachycardia (Fig. 3). When 2:1 AV conductionoccurred, the atrial activation pattern was concen-tric and similar towhatwas observedduring ventric-ularpacing.Onbeatswith2:1VAconduction, theVAtime was longer than half the tachycardia cyclelength (long RP). During tachycardia, spontaneous
Fig. 2. Tachycardia initiation. Ventricular overdrive pacingcomplex tachycardia at cycle length of 300 milliseconds wtion with a normal H-V interval. Ventriculoatrial (VA) condatrial activation via the sinus node marches unperturbed
cycle length variation occurred whereby changesin the His-His interval preceded changes in theR-R interval. The finding of AV dissociation and 2:1VAconduction ruled out atrial tachycardia and atrio-ventricular nodal reentrant tachycardia (AVNRT)using an AV accessory pathway. The presence of
at 340 milliseconds resulted in initiation of narrow-hereby each QRS complex is preceded by a His deflec-uction was absent during the pacing drive train, and
through tachycardia initiation.

Fig. 3. Changing VA relationship during tachycardia. Tachycardia exhibited 2:1 VA conduction, with a retrogradeactivation pattern identical to that observed with ventricular pacing. In this trace, the first atrial activation isretrograde, with earliest activation in the proximal coronary sinus and high right atrial activation occurring prox-imal to distal. The 2 subsequent atrial activations are fusion beats, with earliest activation in coronary sinus buthigh right atrial activation proceeding distal to proximal. The fourth atrial activation is sinus in origin, completingthe transition from 2:1 VA conduction to complete VA dissociation. Small changes in tachycardia cycle length arealso evident on this tracing, with His-His interval changes predicting subsequent R-R interval changes, ruling outa ventricular origin for this tachycardia.
Narrow QRS Tachycardia with VA Block 533
complete AV dissociation during some episodes oftachycardia ruled out an atrial tachycardia withdouble fire (1:2 AV conduction). Ventricular tachy-cardia was excluded by the narrow QRS complexand because variations in tachycardia cycle lengthwere preceded by changes in the His-His interval.
Maneuvers During Tachycardia
The differential diagnosis of a narrow-complextachycardia with VA dissociation includes AVNRTwith upper common pathway block, junctionaltachycardia (JT), and circus-movement tachy-cardia (CMT) using a concealed nodofascicularor nodoventricular (NF/NV) accessory pathway.1
Ventricular overdrive pacing consistently termi-nated tachycardia, precluding the use of entrain-ment to identify the tachycardia mechanism.
JT can be distinguished from AVNRT by theresponse to atrial premature depolarizations.2 AHis-refractory atrial premature depolarization thataffects the timing of the subsequent His confirmsinvolvement of the AV node in the antegrade limbof a tachycardia circuit and rules out a focal JT.In the present case, late atrial premature depolar-izations reproducibly advanced the subsequentHis and terminated tachycardia, excluding JT asthe tachycardia mechanism, and leaving AVNRTand CMT as the remaining possibilities (Fig. 4).
Administering His-refractory ventricular pre-mature depolarizations (VPDs) can test forinvolvement of an accessory pathway in a tachy-cardia circuit. In the present case, His-refractoryVPDs during periods of stable tachycardia cyclelength delayed the inscription of the subsequentHis (Fig. 5). On another occasion, spontaneous

Fig. 4. His-refractory atrial premature depolarization (APD) affects timing of the subsequent His. (A) Duringtachycardia with 2:1 VA conduction, an APD delivered when the His was refractory advanced the timing ofthe subsequent His, and terminated tachycardia. (B) With the APD delivered during tachycardia with VA dissoci-ation, the same finding as in A is apparent. These findings rule out junctional tachycardia.
Fig. 5. His-refractory ventricular premature depolarization (VPD) delays the timing of the subsequent His. A VPDthat is coincident with His activation delays the timing of the subsequent His, proving involvement of an acces-sory pathway in the tachycardia circuit. Because the atrium is not involved in the circuit, the bypass tract mustinsert into the AV node and is therefore a nodofascicular or nodoventricular pathway.
Han & Vedantham534

Narrow QRS Tachycardia with VA Block 535
His-refractory VPDs terminated tachycardia.Either of these findings would be sufficient toprove involvement of a concealed accessorypathway in the tachycardia and exclude AVNRT.Because the atrium was not part of the tachy-cardia circuit, it was concluded that the acces-sory pathway inserted directly into the AV node,with retrograde conduction to the atrium mostlikely occurring via a slow retrograde AV nodalpathway, accounting for the long VA time onconducted beats. An alternative mechanismwould be a slowly conducting NF/NV pathway in-serting directly into the AV node.
Fig. 6. Mapping and ablation. (A) With the ablation cathanterior and superior to the coronary sinus ostium, the eatrial and ventricular signal without a His signal. (B) The saactivation and a low-amplitude signal that might reflecta slowly conducting accessory pathway. (C, D) Ensite (St Judterior (C) and left lateral (D) orientation show the successactivation during ventricular pacing. CS, coronary sinus;superior vena cava; TA, tricuspid annulus.
Mapping and Ablation
A 4-mm quadripolar radiofrequency ablation cath-eter was used for mapping and ablation. Hypothe-sizing that that the NF/NV pathway inserted nearthe region of the slow AV nodal pathway, a strategywas pursued of identifying the site of earliest retro-grade atrial activation, starting with the postero-septal region of the tricuspid annulus and movinganterior and superior. Also, an attempt wasmade to identify a pathway potential thatpreceded retrograde atrial activation at candidatesites. The earliest atrial activation was localized to
eter at 3 o’clock on the tricuspid annulus positionedlectrogram in sinus rhythm shows an equal-amplitudeme site during ventricular pacing shows earliest atrialactivation of a slow AV nodal pathway, or, less likely,e Medical, St Paul, MN) activation maps in anteropos-ful ablation lesion (arrow) at the site of earliest atrialIVC, inferior vena cava; POT, pathway potential; SVC,

Han & Vedantham536
a site anterior to the roof of the coronary sinusostium, where electrograms revealed a 1:1 atrialto ventricular electrogram ratio in sinus rhythmand a low amplitude potential preceding atrial acti-vation on ventricular paced beats (Fig. 6). Ablationwas performed at this site, and subsequentventricular overdrive pacing and programmedventricular stimulation with and without isoproter-enol infusion failed to induce the tachycardia. At6 months after ablation, the patient has remainedsymptom-free and has resumed all of his usualactivities without limitation.
DISCUSSION
Narrow-complex tachycardia with VA dissociationis rare. The differential diagnosis includes JT,AVNRT with upper common pathway block, andaCMTusinga concealedNF/NVpathway.Althoughbaseline tachycardia characteristics can suggestone or another of these mechanisms, pacingmaneuvers are required to make a definitive diag-nosis in these difficult cases.1 An unusual featurein the present case, in addition to the changing VArelationship, was the long VA interval on beats thatwere conducted retrogradely to the atrium.A standard maneuver performed to distinguish
among narrow-complex tachycardia mechanisms,the response to ventricular overdrive pacing, wasunhelpful in this case. However, the responses ofthe tachycardia to His-refractory atrial and
ventricular depolarizations enabled the authors tomake the diagnosis of CMT using a concealedNF/NV pathway and illustrate a diagnosticapproach to this rare arrhythmia. Identification ofan NF/NV pathway potential during tachycardiaand ventricular pacing, the optimal mapping stra-tegy for this arrhythmia, most commonly localizesthe pathway insertion to the mid-septal region,very close to the successful ablation site.2,3 Whenthis approach is not possible, identification ofthe site of earliest atrial activation is an alter-native strategy. In this case, the potentialidentified might have reflected activation of aslow AV nodal pathway or a slowly conductingNF/NV pathway.
REFERENCES
1. Hamdan MH, Kalman JM, Lesh MD, et al. Narrow
complex tachycardia with VA block: diagnostic and
therapeutic implications. Pacing Clin Electrophysiol
1998;21:1196–206.
2. Hluchy J, Schlegelmilch P, Schickel S, et al. Radiofre-
quency ablation of a concealed nodoventricular
Mahaim fiber guided by a discrete potential. J Cardio-
vasc Electrophysiol 1999;10:603–10.
3. Hluchy J, Schickel S, Jorger U, et al. Electrophysio-
logic characteristics and radiofrequency ablation of
concealed nodofascicular and left anterograde
atriofascicular pathways. J Cardiovasc Electrophysiol
2000;11:211–7.