Embed Size (px)
Citation preview

Review
10.1586/14737159.7.2.149 © 2007 Future Drugs Ltd ISSN 1473-7159 149www.future-drugs.com
Nanotechnology in the diagnosis and management of heart, lung and blood diseasesDenis B Buxton
†Author for correspondenceNational Heart, Lung, & Blood Institute, Advanced Technologies & Surgery Branch, Division of Cardiovascular Diseases, 6701 Rockledge Drive, Bethesda, MD 20892, USATel.: +1 301 435 0516Fax: +1 301 480 [email protected]
KEYWORDS: cardiovascular, diagnostics, hematopoietic, imaging, pulmonary, therapy, tissue engineering
Heart, lung and blood diseases exert an enormous toll, accounting for almost half of the deaths in the USA each year. In addition to the morbidity and mortality resulting from these diseases, there is also a high economic burden, estimated at US$560 billion for 2006. Nanotechnology offers a broad range of opportunities to improve diagnosis and therapy for cardiovascular, pulmonary and hematopoietic diseases, thereby decreasing these burdens. This review will focus on four areas of particular promise for the application of nanotechnology: imaging, diagnostics and biosensors, drug delivery and therapy, and tissue engineering and repair. The goal is to summarize the current state of science and technology in these areas and to look at future directions that the field is likely to move in to enhance the diagnosis and treatment of heart, lung and blood diseases.
Expert Rev. Mol. Diagn. 7(2), 149–160 (2007)
ImagingNanotechnology is impacting imaging in threeareas:
• Molecular or targeted imaging uses nano-particles targeted to specific sites to deliverimaging agents;
• Cell tracking uses nanoparticles to followthe fate of cells; for example, in cell-basedtherapies;
• Nanotechnology also has the potential todevelop better contrast agents.
Molecular imagingCardiovascular disease
The detection and characterization of athero-sclerotic plaque represents a major challenge,and is therefore a focus for new nanoparticle-based targeted imaging. As an atheroscleroticplaque develops, it offers a number of stage-specific targets for molecular imaging [1]. At theearliest stages, activation of endothelial cellsresults in the expression of cell-surface recep-tors, such as vascular cell adhesion molecule(VCAM)-1, intercellular adhesion molecule(ICAM) and selectins. The Weissleder groupused phage display to identify a family ofVCAM-1-mediated cell-internalizing peptides,
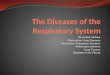
including one with homology to the α-chainof very late antigen, a ligand for VCAM-1 [2].Nanoparticles decorated with this peptidedemonstrated high affinity for endothelial cellsexpressing VCAM-1, and co-localized withVCAM-1-expressing cells in atheroscleroticlesions present in cholesterol-fed apolipo-protein E-/- mice [2]. A closely related targetingligand was used to demonstrate VCAM-1expression in vivo in a similar mouse modelusing magnetic resonance imaging (MRI) andmagneto-nanoparticles (FIGURE 1; A, D & F) [3].Treatment with a statin for 8 weeks decreasedVCAM-1 expression, and this was reflected bya decrease in signal enhancement towardsbaseline (FIGURE 1; B, E & G). These VCAM-1-targeted nanoparticles have also shown prom-ise for identifying endothelial activation in thecommissures of diseased aortic valves [4].
As inflammation develops, new targetsbecome available, such as recruited macrophages,proteolytic enzymes (including matrix metallo-proteases and cathepsins) and apoptotic cells.Dextran-coated magneto-nanoparticles are takenup primarily in activated macrophages and allowin vivo visualization of murine atheroma [5].Nanoparticles were found predominantly in cell-rich areas of atheroma, and co-localized with
CONTENTS
Imaging
Diagnostics & biosensors
Drug delivery & therapy
Tissue engineering & repair
Safety issues
Expert commentary
Five-year view
Key issues
References
Affiliation

Buxton
150 Expert Rev. Mol. Diagn. 7(2), (2007)
macrophages. [5]. Ultrasmall superparamagnetic nanoparticleshave also been used to image inflamed carotid plaques [6], andmay have the potential to differentiate patients with inflamed,vulnerable carotid plaques at higher risk for rupture.
As plaque develops further, angiogenesis expands the vasa vaso-rum, the blood supply to the vessel wall. New blood vesselsexpress specific markers, such as αvβ3 integrin, that can distin-guish neoangiogenesis from established blood vessels. Winter andcolleagues used MRI of αvβ3-integrin-targeted paramagnetic nan-oparticles to demonstrate increased αvβ3 distribution in theatherosclerotic aortic wall of cholesterol-fed rabbits [7]. Histologyand immunohistochemistry confirmed marked proliferation ofangiogenic vessels within the aortic adventitia of the atheroscle-rotic rabbits. Finally, plaque rupture leads to the formation of afibrin thrombus and recruitment of platelets, again providing newimaging targets. Nanoparticles targeted to clots using antifibrinFab fragments enabled visualization of blood clots in vivo usingMR, and may allow early identification of vulnerable plaques [8].
Pulmonary disease
At present, the main focus in applying nanoparticles to pulmo-nary disease is in the field of lung cancer. Quantum dots (QDs)are semiconductor nanocrystals with broad absorption spectra,
but narrow emission spectra, that are tunable by size (larger QDsemit at longer wavelengths) [9]. QDs have superior fluorescenceproperties compared with organic dyes, with improved signalbrightness and superior photostability. The narrow emissionspectra also permit the simultaneous excitation and detection ofmultiple QD colors. Studies in animals have demonstrated thatQDs, in conjunction with a near-infrared imaging system, accu-rately mapped the lymphatic drainage system, permitting identi-fication of the sentinel lymph node [10]. The technique permitsprecise real-time imaging and, therefore, overcomes many limi-tations of currently available techniques. Potential toxicity willneed to be addressed before human use (e.g., most QDs con-tain cadmium or other toxic metals); however, these issues maybe overcome.
Cell trackingThe field of cell-based therapies is currently restricted by a fun-damental lack of knowledge of the fate of transplanted cells,and would benefit greatly from methods allowing in vivo track-ing of the distribution of delivered cells throughout the body.Daldrup-Link and colleagues used superparamagnetic ironoxide nanoparticles, with or without the use of liposomes toenhance uptake, to label human hematopoietic progenitor cells[11]. They then administered the cells to mice and followednoninvasively the in vivo distribution of the cells to differentorgans, including liver, spleen and bone marrow. No impair-ment of progenitor cell function was detected in labeled cells.Potential clinical applications include studies of autologousand allogeneic bone marrow transplantation, assessment ofhoming specificity of stem cell subtypes or genetically engi-neered stem cells, and investigating reasons for graft failure incertain populations.
Alternative approaches to cell labeling for cells that do notreadily take up iron oxide nanoparticles include the use of cell-permation peptide conjugation. For example, Nitin and col-leagues developed polyethyleneglycol (PEG)-modified super-paramagnetic iron oxide nanoparticles that could be loaded effi-ciently into cells by decorating them with the proteintransduction domain of HIV-1: the TAT peptide [12].
Contrast agentsThe use of nanotechnology also offers the potential for next-generation computed tomography (CT) contrast agents thatmay avoid some of the morbidity associated with iodine-based agents. Polymer-coated Bi2SO3 nanoparticles haveexcellent stability, high x-ray absorption (fivefold better thaniodine) and long circulation times. Initial studies in mice havedemonstrated good imaging properties and safety [13]. Goldnanoparticles have similarly shown promise for permittinglonger imaging times with lower toxicity and higher x-rayabsorption [14]. Nanoparticles also show promise for MRI;functionalized metallofullerene nanoparticles have muchhigher relaxivity than conventional gadolinium contrastagents and also have the potential for functionalization fortargeted imaging [15].
Figure 1. Magnetic resonance imaging with vascular cell adhesion molecule (VCAM)-1-targeted nanoparticles demonstrates that atorvastatin (B, E & G) decreases VCAM-1 expression relative to untreated mice (A, D & F) in apolipoprotien E–/– mice fed a high-cholesterol diet. The red color encodes high VCAM-1 expression. Fluorescence imaging of the nanoparticles confirmed the decrease in VCAM-1 expression in atorvastatin (E & G) relative to untreated animals (D & F). Reproduced with permission from [3] © Lippincott Williams & Wilkins (2006).HCD: High cholesterol diet; VINP: VCAM-1 internalizing nanoparticle.
A HCD B HCD plus atorvastatin
D VINP-28 E
F VINP-28 G
240
160

Nanotechnology in heart, lung and blood disease
www.future-drugs.com 151
Diagnostics & biosensorsA wide range of micro- and nanotechnology-based approachesare being tested for in vitro diagnostics. Nanotechnology-basedplatforms will enable high-throughput multiplexed detection ofproteins and nucleic acids with much greater sensitivity thanthose currently available, eventually leading to the developmentof lab-on-a-chip devices for the rapid diagnosis of pathologyand for genetic testing [16]. The successful technologies will bedetermined by a combination of sensitivity, reliability, speed,ease of use and cost. These technologies, which can be broadlydivided into mechanical, optical and electrical detection, havebeen reviewed in detail elsewhere [16–18]; thus, this review willbe restricted to examples illustrating a few of the technologiesbeing developed.
An example of the application of optical methods to the detec-tion of genetic mutations is the use of oligonucleotide–goldnanoparticle conjugates to detect cystic fibrosis (CF)-relatedmutations [19]. In a model oligonucleotide system, two probeoligonucleotide–gold nanoparticle conjugates were linkedtogether by a third target oligonucleotide strand bearing the CF-related mutation(s). Optical melting curves are then obtained forthe complexes; perfect strand-sequence matches can be distin-guished by melting behavior from sequence mismatches due todeletions/insertions or single nucleotide polymorphisms for avariety of known CF mutations, suggesting that the techniquemay be exploitable for low-cost, rapid, diagnostic purposes.
Nanomechanical detection can detect biomarker transcriptsin human RNA with picamolar sensitivity [20]. The methoduses arrays of thin cantilevers, 100-µm wide and 450-nm thick,biofunctionalized with oligonucleotide probes. The underlyingprinciple is that hybridization of mRNA to a complementarilybiofunctionalized sensor cantilever causes surface stress, result-ing in bending of the cantilever. Deflection of the cantilever canbe measured optically and subtraction of the deflection of areference cantilever corrects for nonspecific interactions andthermal drift. Using this technique, the authors were able todetect mRNA biomarker candidates in total cellular RNA andto assess differential gene expression in response to interferontreatment of cell cultures, thereby demonstrating the potentialfor tracking disease progression or therapy response.
Nanotechnology has also increased the sensitivity of proteinassays. For example, the biobarcode amplification developed bythe Mirkin group was used to detect amyloid-β-derived diffusi-ble ligands (ADDLs), a biomarker for Alzheimer’s disease, witha sensitivity of 100 aM [21]. The assay uses magnetic micro-particles coated with antibody to bind ADDL in cerebrospinalfluid. After washing, secondary antibodies bound to DNA–goldnanoparticle conjugates containing both covalently attachedDNA and hybridized complementary DNA. After washingaway unbound DNA–gold nanoparticle conjugates, thehybridized DNA is released by heat and salt dehybridization,and detected using an ultrasensitive surface-based sandwichhybridization assay [21]. This method can also be extended tomeasure several target proteins simultaneously using differentantibody/barcode DNA combinations [22].
Two recent examples of electrochemical biosensors usingnanowires and microelectromechanical systems (MEMS) areparticularly relevant to the cardiovascular system. Work fromthe laboratories of Mohapatra and Bhansali has demonstratedthe potential of functionalized gold nanowires to measure cor-tisol [23]. The method uses MEMS technology, coupling enzy-matic cleavage of cortisone to cortisol with capture of the corti-sol onto gold nanowires functionalized with anticortisolantibodies. Binding of cortisol results in an electrochemicalsignal that can be used to quantify the cortisol concentration inthe sample. A similar technology has also been used to measuretotal cholesterol [24]. Again, these proof-of-concept studiesindicate towards future compact lab-on-a-chip devices that canperform multiple assays at the bedside.
Nanotechnology-based sensors have potential both for eluci-dating physiology and pathophysiology and for in vivo diagnos-tics. Nanosensors can detect nitric oxide (NO) and other shorthalf-life reactive species electrochemically at the single-cell level[25]. Using this technology to measure simultaneously in real-time NO/O2
-/ONOO- production, NO production and oxida-tive stress were shown to differ between single cells from Afri-can-American and European-American patients. NO bioavaila-bility was dramatically lower in cells from black patients, butcould be restored to normal levels by nebivolol, a β1-selectiveagent with vasodilating and antioxidant properties [26]. Similarnanosensors can be incorporated into catheters for in vivomeasurements and monitoring of therapy.
Drug delivery & therapyA variety of mechanisms contribute to the potential of nano-technology for improving drug delivery. The availability of anumber of different nanoparticle structures, including solidparticles, nanoshells, polymeric micelles, liposomes and den-drimers, provides a flexible range of opportunities that can betailored to meet different therapeutic needs. At the simplestlevel, drug encapsulation into nanoparticles can be used to sol-ubilize poorly soluble drugs. For example, hydrophobic drugssuch as the anticancer drug paclitaxel are often packaged inpolyoxythylated castor oil (Cremophor) and the intrinsic toxic-ity of Cremophor can limit the amount of drug that can besafely administered. However, packaging of paclitaxel into albu-min nanoparticles reduces toxicity, permitting higher dosing[27,28]. Encapsulation of drugs and cytokines in nanoparticlescan facilitate oral delivery or enhance pharmacokinetics byextended release of drug. An example of using these altereddrug properties is discussed later for low-molecular-weightheparin [29].
Targeting of nanoparticles to specific sites in the body, forexample by directing nanoparticles to specific cell-surfacereceptors, can enhance drug delivery to the intended targetwhile reducing systemic load. Targeted delivery of drugs can beachieved by passive targeting (e.g., to regions of vascular hyper-permeability caused by injury) or by active targeting to cell-sur-face ligands (such as receptors and integrins). Active targetingemploys targeting moieties, such as monoclonal antibodies or

Buxton
152 Expert Rev. Mol. Diagn. 7(2), (2007)
fragments, aptamers, peptides and peptidomimetics, incorpo-rated onto the nanoparticle surface. The recent demonstrationof heart-specific vascular markers [30] and peptides specific forclotted plasma [31] illustrates the power of techniques such asin vivo phage display for the selection of specific targeting moie-ties. Particle internalization can also be promoted by placing cellpermeation peptides, such as the TAT peptide, on the nano-particle. By extension, targeting to specific organelles, such asthe mitochondrion or nucleus, is also feasible using appropriatelocalization signals [32]. In the lung, inhalational delivery ofdrugs formulated in nanoparticles or nanosuspensions can simi-larly increase the effective dose of drug delivered to target cells.Controlling nanoparticle composition provides the potential formore rapid or more sustained release. Environment-sensingnanoparticles can be designed to modify drug release in responseto pH, giving the potential for local delivery in response to anacidic environment (e.g., in tumors or ischemic tissue).
Cardiovascular diseaseAtherosclerotic plaque is a major contributor to two of the lead-ing causes of death in the USA, myocardial infarction andstroke. Plaque progression is accompanied by expansion of thevasa vasorum, the network of blood vessels in the walls of bloodvessels, and blocking this neovascularization of the plaque hasbeen proposed as a therapeutic strategy to reduce inflammationand progression of advanced atherosclerosis. Immature neo-vessels express cell surface markers such as αvβ3 integrin that arenot found on mature vessels. Perfluorocarbon nanoparticles tar-geted to the αvβ3 integrin through a surface-bound antibody cansimultaneously deliver an antiangiogenic drug, fumagillin, to thenewly formed vasa vasorum, and image the progress of therapythrough gadolinium delivery and MRI. Nanoparticle binding tocells through cell surface receptors enhances rapid transport ofdrugs from the outer drug-loaded lipid monolayer to the cellmembrane through a process termed contact-facilitated drugdelivery [33]. Delivery of fumagillin via a single systemic injec-tion of αvβ3 integrin-targeted nanoparticles effectively reducedmicrovessel burden in aortas of cholesterol-fed rabbits αvβ3 [33].
Peripheral artery disease is a debilitating condition with poortreatment options. Heparin-coated polylactide glycolide nano-spheres containing basic fibroblast growth factor (bFGF) andembedded in fibrin gel provide extended delivery of bFGF,which sustains growth of human vascular endothelial cells inculture for 15 days. To treat ischemic mouse limbs, a singleinjection of the nanospheres with fibrinogen/thrombin to formfibrin gel in situ resulted in superior limb revascularization rela-tive to daily injection of bFGF or injection of bFGF and fibringel, demonstrating that controllable sustained release of thecytokine potentiates the angiogenic efficacy of the cytokine [34].
Systemic nanoparticle administration has been tested as amethod to prevent neointimal proliferation in animal models ofvascular injury. Administration of doxorubicin in core-shell nano-particles of polyethyleneglycol-based block co-polymer increasedtissue doxorubicin at the injury site, compared with systemicdelivery of free drug, and decreased neointimal formation [35].
Uptake of these nanoparticles takes advantage of sustainedtissue hyperpermeability following balloon damage and thusoccurs via passive targeting to the tissue. Site-specific drugdelivery could potentially be increased by active targeting ofnanoparticles to markers expressed following tissue damage.Local delivery of drug-containing nanoparticles using a drug-delivery balloon catheter may also provide an effective thera-peutic option for prevention of restenosis [36]. Effective sys-temic or local nanoparticle-mediated drug delivery may be astrategy to mitigate restenosis problems in bare metal stents orthrombotic events in drug-eluting stents, and a Phase I/II clini-cal trial is currently underway to assess intracoronary adminis-tration of albumin-bound paclitaxel nanoparticles (ABI-007)for the prevention of in-stent restenosis.
Nanotechnology also has the potential to improve devices suchas heart valves, stents and assist devices. Nanopatterning of sur-faces and nanocomposite coatings can influence the interactionsof blood components, cells, proteins and infectious agents withthe surfaces, offering the opportunity to improve biocompatibil-ity and decrease adverse events such as clotting and colonizationof devices. Nanoporous coatings offer the potential for program-mable pharmacokinetic capacity using advances in nanotechnol-ogy and are being tested for use on drug-eluting stents. Stentscoated with a paclitaxel-eluting porous composite matrix synthe-sized from amorphous carbon nanoparticles embedded in glassypolymeric carbon have demonstrated promise in animal trials [37]
and a clinical trial is now underway. The coating is nonthrombo-genic and by altering pore size and morphology, drug releaserates can be tailored. Unlike traditional polymer-based drug-eluting stents, there is no initial burst of drug release and the car-bon–carbon stents elicit less inflammatory response [37]. Nano-coating of stents with a novel polymer without the use of drughas also shown promise, providing thromboresistance andreducing in-stent stenosis in initial rabbit experiments [38].
Pulmonary diseaseInhalational delivery offers additional opportunities for nano-technology to impact pulmonary disease and, as a result, this isan area of particularly active research. Drug delivery in the formof inhaled dry powder or suspension aerosol suffers from anumber of potential limitations. Poor solubility and micro-particulate nature can constrain diffusion and dissolution of thedrug at the site of action, in turn limiting bioavailability. Rapidciliary clearance and alveolar macrophage uptake can reducethe residence time of drugs, abolishing long-term effects. Incontrast, nanoparticles and nanosuspensions offer a number ofpotential advantages:
• Rapid onset of action, resulting from fast diffusion and disso-lution of the drug;
• Increased adhesion of nanoparticulate drug to mucosal sur-faces, providing extended residence time of the drug at thesite of action;
• Lower phagocytic clearance of nanoparticles relative to largerparticles in the micrometer range.

Nanotechnology in heart, lung and blood disease
www.future-drugs.com 153
There is some debate over the deposition of nanoparticlesin the deep lung. While some data demonstrate efficientalveolar deposition of 20-nm nanoparticles [39], other studieshave suggested that their low inertia results in poor lungdeposition and exhalation [40]. For this reason, an optimalparticle size for delivery to the deep lung of 1–5 µm is fre-quently cited [41,42]. Methods developed to deliver nano-particulate drug formulations to the deep lung (and henceovercome poor deposition of nanoparticles in the alveolae)include [41,42]:
• Aerosol delivery of nanosuspensions of drug, a method usefulfor drugs that are poorly water-insoluble but soluble in oil;
• Microencapsulation of nanoparticles for lung drug and proteindelivery.
The potential for inhaled nanoparticles is now being testedfor a number of pulmonary diseases. Achieving adequate thera-peutic delivery to the lung using oral therapy for pulmonarytuberculosis requires high drug doses, and rapid drug clearanceresults in a need for daily treatment with multiple drugs forextended periods. Inhaled nanoparticle delivery of antitubercu-lar drugs demonstrates great promise, resulting in sustainedmaintenance of therapeutic concentrations both in the lungsand systemically [43]. The delivery of antitubercular drugs viainhaled nanoparticles at 10-day intervals provided effectivetreatment in animal models [44]. Less frequent dosing would bevaluable clinically, potentially improving patient complianceand decreasing cost.
Chitosan, a polymer derived from crustacean shells, isbeing tested in a range of drug-delivery roles because of itsbiodegradability, biocompatibility and mucoadhesion. Inaddition, it is readily modified chemically and physically. TheMohapatra laboratory has used thiolation to increasemucoadhesion and permeation of chitosan nanoparticles and
employed the modified nanoparticles as a drug-delivery matrixfor theophylline [45]. In a mouse model of allergic asthma,intranasal administration of the thiolated chitosan nanoparti-cles significantly enhanced the efficacy of theophylline inreducing lung pathology [45]. FIGURE 2 illustrates that micetreated with theophylline delivered by thiolated chitosan nan-oparticles (FIGURE 2G) demonstrated reduced pulmonaryinflammation, decreased epithelial damage, reduced gobletcell hyperplasia and fewer infiltrating inflammatory cells com-pared with the other treatment groups.
Nanoparticles may also be helpful for the delivery of smallinterfering RNA (siRNA) and gene therapy. Prophylactic intra-nasal treatment of mice with siRNA to a respiratory syncytialvirus (RSV) protein resulted in a dramatic decrease in lung viraltiter and decreased inflammation and airway reactivity follow-ing infection [46]. DNA nanoparticles are also being developedfor the treatment of CF. Mutations in the CF transmembraneregulator (CFTR) gene cause aberrant ion transport across epi-thelial cell membranes. In the lung, this results in thick mucussecretions, which in turn cause recurrent lung infections. Intra-nasal administration of DNA nanoparticles encoding wild-typeCFTR was tested in a Phase I clinical trial for treatment of CF,and was demonstrated to be safe and to result in partial to com-plete nasal CFTR chloride channel reconstitution [47]. Aerosolpreparations of the compacted DNA retain full biological activ-ity, and thus, lung dosing should be feasible. Efficient deliveryof plasmids as large as 20 kbp is possible using compactedDNA nanoparticles [48].
Other pulmonary targets for which nanoparticles may have atherapeutic role include fungal infections and bacterial biofilms.Nanoencapsulation of toxic drugs has great potential for thetreatment of refractory pulmonary mycoses and other lung infec-tions. Treatment of mycoses with amphotericin B is complicatedby adverse effects, including nephrotoxicity. Nanostructured
Figure 2. Thiolated chitosan nanoparticles (TCNs) enhance anti-inflammatory effects of theophylline in a mouse model of allergic asthma. Histological analysis of mouse lung sections after theophylline treatment: (A) negative control, (B) untreated (ovalbumin-challenged), (C) unmodified (pure) chitosan nanoparticles, (D) thiolated chitosan, (E) theophylline, (F) theophylline plus unmodified chitosan nanoparticles, (G) theophylline plus TCNs. Reproduced with permission from [45] © 2006 BioMed Central Ltd.
CBA D
GFE

Buxton
154 Expert Rev. Mol. Diagn. 7(2), (2007)
aerosolized formulations of itraconazole demonstrated encour-aging results for prevention of invasive pulmonary aspergillosis,increasing lung tissue concentrations, limiting systemic expo-sure and prolonging survival relative to orally administereddrug [49].
TAT peptide also demonstrates potential for enhancing genetherapy aimed at the respiratory epithelium [50]. Covalent cou-pling of TAT to polyethyenimine (PEI) through a heterobifunc-tional PEG spacer results in a TAT–PEG–PEI conjugate form-ing small (∼90 nm) polyplexes. The polyplexes demonstratedimproved DNA–reporter gene complexation and significantlyimproved stability. Significantly higher transfection efficienciesfor TAT–PEG–PEI were detected in mice in vivo relative to PEIalone. Reporter gene expression was distributed through bron-chial and alveolar tissue. Thus, TAT–PEG–PEI represents apromising nonviral gene carrier for lung therapy, with protec-tion for plasmid DNA, low toxicity and significantly enhancedtransfection efficiency under in vivo conditions [50].
Hematopoietic diseaseLow-molecular-weight heparin represents the anticoagulant ofchoice in many cases, but is currently limited to parenteraladministration due to poor oral bioavailability. Encapsulation oflow-molecular-weight heparin into polyester/polycationicpolymethacylate nanoparticles shows promise for oral delivery ofthe anticoagulant [29]. Experiments in rabbits demonstrated goodbioavailability after oral administration of the nanoparticles as anemulsion and a prolonged anticoagulant effect.
Targeted delivery of drugs to specific hematopoietic cell typesrepresents another application of nanotechnology to blood dis-eases. Targeting of gelatin nanoparticles to leukemic cells andprimary T lymphocytes was achieved using anti-CD3 antibod-ies, resulting in internalization of the nanoparticles into cells [51].This strategy may facilitate targeting of cytotoxic drugs to thetumor cells, allowing lower drug doses to be used and reducingsystemic toxicity.
Nanoparticles may also represent a novel mechanism fordelivering antigens to dendritic cells for vaccine development.Targeting of acid degradable polymeric nanoparticles to den-dritic cells by monoclonal antibodies to deliver antigen to thecytoplasm of dendritic cells resulted in enhanced cellularimmune responses [52,53]. Bone marrow-derived dendritic cellsefficiently take up polystyrene nanospheres, resulting in strongactivation of antigen-specific interferon-γ-producing T cells[54]. These results and other studies suggest that nanoparticlesare efficient delivery systems for targeting vaccine antigens todendritic cells and activation of potent T-cell responses.
An exciting new application of nanotechnology is the use ofself-assembling peptides as a nanohemostat solution [55]. Thestrategy is based on RADA 16 ionic self-complementary pep-tides composed of arginine (R), alanine (A) and aspartic acid(D), RADARADARADARADA, which dynamically reassem-ble into nanofibers and eventually form a scaffold hydrogelconsisting of over 99.5% water [56]. Assembly of the peptidescreates a nanofiber barrier that provided complete hemostasis
when applied directly to a wound in the brain, spinal cord,femoral artery, liver or skin of hamsters [55]. Thus, this techno-logy, has great potential for the treatment of trauma patientsand during surgery.
Tissue engineering & repairThere is increasing evidence for the importance of nanoscalesurface features of scaffolds in promoting the more naturalgrowth of tissues by providing cues to cell growth and differen-tiation [57]. Nanotechnology offers the potential to control thenanoenvironment of cells, by providing a scaffold for ex vivogrowth of replacement tissues, by implantation of a scaffoldin vivo to assist in repair or by injection of scaffolding materialsthat self-assemble to provide a local scaffold for circulating orco-injected cells to build upon. In addition to providing physi-cal cues, scaffolds can also be designed to provide stimulation ofreceptors and other cell surface molecules by incorporation ofligands on to the surface; for example, by covalent attachment.
Cardiac repairThe application of nanotechnology to cardiac tissue engineer-ing has been explored both in vitro and in vivo. Zong and col-leagues employed electrospinning to fabricate biodegradablenonwoven poly (lactide)-poly(glycolide) (PLGA)-based scaf-folds for cardiac tissue engineering applications [58]. When pri-mary cardiomyocytes were cultured on the electrospun scaf-folds to form tissue-like constructs, scanning electronmicroscopy revealed that the fine-fiber architecture of the non-woven matrix allowed the cardiomyocytes to make extensiveuse of provided external cues for isotropic or anisotropic growthand, to some extent, to crawl inside and pull on fibers. Confo-cal microscopy indicated that cardiomyocytes had a preferencefor relatively hydrophobic scaffolds, developing mature con-tractile machinery (sarcomeres) on electrospun poly-L-lacticacid (PLLA). Functional excitability of the engineered con-structs was confirmed by optical imaging of electrical activityusing voltage-sensitive dyes.
Ishii and colleagues used a similar approach with electrospunnanofibrous poly(ε-caprolactone) mesh to culture neonatalcardiomyocytes [59]. They also overlaid meshes to obtain 3Dcardiac grafts; constructs with up to five layers could be formedwithout any incidence of core ischemia. The layers communi-cated morphologically and electrically, as verified by histologyand immunohistochemistry, and beat in a synchronized fash-ion. In order to support the growth of thicker layers that couldbe used clinically for cardiac repair, new technologies to inducevascularization will also be required.
To approach tissue repair from an in vivo perspective, Rich-ard Lee’s group [60,61] has used the same RADA 16 injectableself-assembling peptide nanofibers that Ellis-Behnke and col-leagues have subsequently used for hemostasis [55]. The peptidesassemble to form intramyocardial microenviroments thatrecruit endothelial cells and promote their survival [60,61].When injected into rat heart, the peptide microenvironment isinitially populated by endothelial cells during the first week

Nanotechnology in heart, lung and blood disease
www.future-drugs.com 155
post injection, but later, the myocyte precursors became thepredominant cell type. Mature blood vessel-like structuresformed from smooth-muscle cells are also found [60].
The peptide nanofibers have also been used to provide con-trolled delivery of proteins to the myocardium with potentialtherapeutic benefits [62,63]. In rats undergoing ligation of a
Figure 3. Intramyocardial NF/PDGF injection reduces infarct volume 4 months after infarction. (A) Rat left ventricles stained with Masson’s trichrome. Healthy tissues stain red, while infarct scar tissue is blue. (B) The percentage of infarcted myocardium volume. Reproduced with permission from [63] © 2006 Lippincott Williams & Wilkins. *p < 0.001. MI: Myocardial infarction; NF: Nanofiber; PDGF: Platelet-derived growth factor.
Sham Sham plus NFSham plusNF/PDGF
MI MI plus NFMI plus
NF/PDGFA
B50
40
30
20
10
0
Infa
rct
volu
me
(%)
Sham(n = 12)
Sham plus NF(n = 11)
Sham plus NF/PDGF(n = 11)
MI(n = 12)
MI plus NF(n = 12)
MI plus NF/PDGF(n = 13)
*
*

Buxton
156 Expert Rev. Mol. Diagn. 7(2), (2007)
coronary artery to simulate myocardial infarction, more than30% of the myocardium is replaced by noncontractile scar tis-sue (FIGURE 3; MI). Injection of nanofibers with platelet-derivedgrowth factor (FIGURE 3; MI+NF/PDGF), but not nanofibers orPDGF alone, decreased cardiomyocyte death and reduced inf-arct size following myocardial infarction in rats (FIGURE 3). Thenanofibers preserved systolic function after myocardial infarc-tion and were protective after ischemia/reperfusion injury[62,63]. They have also been used to deliver insulin-like growthfactor in combination with cell therapy, again resulting in func-tional improvement following experimental myocardial infarc-tion [64]. The injectable nanofibers can thus facilitate sustaineddelivery of proteins to the myocardium with potential thera-peutic benefits; large infarcts often lead to the development ofheart failure in patients, and therapies to preserve functioningheart muscle can prevent the onset of heart failure.
Pulmonary repairEngineering lung to replace dysfunctional tissue currentlyremains a distant target. However, a recent report describes theuse of a combination of nanofibrous synthetic matrices andporous foams to create a 3D support for fetal pulmonary cells [65].
While the synthetic scaffolds provide mechanical support andpromote mesenchymal proliferation and cell assembly, epithe-lial differentiation was not observed. Surface modification ofthe synthetic scaffold to provide tissue-specific cues will beessential for supporting distal lung epithelial differentiation [65].
Safety issuesWhile the novel properties of nanomaterials provide excitingopportunities for diagnosis and therapy, they also raise potentialconcerns about toxicity. A recent review highlighted many of thepotential ways that nanomaterials may have pathological effects,including generation of reactive oxygen species, perturbation ofphagocytic function, effects on blood clotting and generation ofneoantigens [66]. For example, several types of carbon-basednanoparticles were demonstrated to cause varying degrees ofplatelet aggregation and vascular thrombosis [67]. Single wallnanotubes have also been shown to cause inflammatory andfibrogenic pulmonary responses in mice [68].
There are numerous issues that need to be resolved in assess-ing the safety of nanotechnology. A review by Oberdörster andcolleagues emphasizes the complex pathways by which nanopar-ticles can enter the body, translocate and distribute through the
Figure 4. Pathways for systemic exposure, uptake, redistribution and excretion of nanoparticles. Although many uptake and translocation routes have been demonstrated, others still are hypothetical and remain to be investigated. Reproduced with permission from [39] © 2005 National Institute of Environmental Health Sciences.GI: Gastrointestinal; PNS: Peripheral nervous system.
Lymph
Bone marrow Other sites(e.g., muscle, placenta)
Deposition IngestionInjection
Neurons
Neurons
Neurons
Inhalation
Exposure media
Uptake pathways
Translocation anddistribution
Excretory pathways
Air, water, clothes Drug delivery Air Food, water
GI tract
Lymph
Liver
Feces
Skin
SpleenKidney
Urine Breast milkSweat/exfoliation
PNS
CNS
Respiratory tract
Nasal Tracheobronchail Alveolar
Blood(platelets, monocytes,
endothelial cells)
Confirmed routes Potential routes
Expert Review of Molecular Diagnostics
Heart

Nanotechnology in heart, lung and blood disease
www.future-drugs.com 157
system, and eventually get excreted (FIGURE 4) [39]. Reviewingexisting studies on nanoparticle toxicology, they conclude thatendocytosis and biokinetics of nanoparticles are largely depend-ent on the surface chemistry and in vivo surface modifications ofthe particles, and that the greater surface area per mass com-pared with larger-sized particles of the same chemistry rendersnanoparticles more active biologically. As a result of this com-plex dependency of toxicology on a range of nanoparticleproperties, a systematic approach to risk assessment will beessential. A recent International Life Sciences InstituteResearch Foundation/Risk Science Institute Working Groupoutlined the elements that will be required for a screening strat-egy for hazard identification for engineered nanoparticles [69].They recommended a three-pronged approach, involving:
• Physiochemical characterization of materials (e.g., size dis-tribution, shape, surface area, surface charge and surfacechemistry);
• In vitro testing methods using a broad range of tests focusingboth on portal of entry toxicity (e.g., lung epithelial cells andhuman epithelial keratinocytes) and on target-organ toxicity(e.g., perfused heart and cardiomyocytes, and cultured neu-rons), as well as cell-free assays and computationalapproaches;
• In vivo assays, including markers of damage, oxidant stress,cell proliferation, deposition, translocation and biopersistencestudies.
As nanotechnology moves into clinical applications, it will beimportant to be aware of the potential issues and to establisheffective regulatory structure to propel the field forward safelyand efficiently without inhibiting progress unduly. In the USA,the Nanoscale Science and Engineering Technology (NSET)Subcommittee of the National Science and Technology Coun-cil (NSTC) Committee on Technology coordinates nanotech-nology-based activities among US Government agencies andmembers include the NIH, the US FDA [101] and the NationalInstitute for Occupational Safety and Health (NIOSH) [102].FDA and NIOSH co-chair the NSET Working Group onNanomaterials Environmental and Health Implications(NEHI) to define new test methods/protocols and define the
safety of these products. At NIH, the National Institute forEnvironmental Health and Safety (NIEHS) funds a Nanotech-nology Safety Initiative through the National Toxicology Pro-gram [103] and the National Cancer Institute (NCI) funds aNanotechnology Characterization Laboratory [104] to performpreclinical toxicology and other studies. As the field moves for-ward, it will be important that these activities are coordinatedwith similar activities in other countries to avoid redundancy.
Expert commentary Nanotechnology has the potential to revolutionize the field ofpersonalized medicine by providing rapid, low-cost, point-of-care genotyping of polymorphisms and gene deletions andinsertions, facilitating tailored therapies based on the patient’sgenetic profile. The use of molecular imaging is likely to iden-tify new signatures of disease for early detection and to facilitatethe monitoring of the effectiveness of therapies. In patients forwhom the therapy is ineffective, a switch to a new therapeuticregime may then be considered. Targeted delivery of drugs willenable more effective treatment by increasing availability of thedrug at the therapeutic site, while reducing side effects in off-target tissues or organs. More biocompatible and functionalscaffolds to enhance tissue engineering and cell-based therapiesare also likely, and are designed to mimic nanoscale features ofnatural systems. In the future, advances in these areas have thepotential to bring significant advances in diagnostics and thera-peutics for heart, lung and blood diseases. Better diagnosticsand improved treatment strategies through nanotechnologymay thus help to reduce the enormous physical and economicburden of debilitating diseases such as heart failure and chronicobstructive pulmonary disease.
Five-year viewThe next 5 years are likely to see an explosion of nanotechno-logy applications in the biomedical arena. TABLE 1 summarizessome of the developments likely in this timeframe and whatneeds to happen for them to take place. For imaging, the cur-rent generation of molecular imaging probes still lacks the sen-sitivity required for clinical diagnostic imaging. This problemis likely to be met by advances in two complementary areas;
Table 1. Nanotechnology applications and developments over the next 5 years.
Area Likely developments Need
Imaging Development of new nanoparticle-based molecular imaging agents for noninvasive imaging of coronary and carotid plaque, thrombosis and lung inflammation
Increased sensitivity of probes and improved targeting ligands
Diagnostics Incorporation of nanotechnology-based devices into point-of-care devices
Development of technology from proof-of-concept to commercial viability
Drug delivery Rapid growth of targeted drug delivery to improve effective dose Improved characterization of biological interactions of nanoparticles
Tissue repair Use of self-assembling injectable scaffolds for cardiac repair Further preclinical and clinical testing to determine feasibility

Buxton
158 Expert Rev. Mol. Diagn. 7(2), (2007)
better imaging agents, with increased sensitivity and improvedtargeting strategies that deliver more agent to the specific site. Arecent publication on magnetism-engineered iron oxide nano-particles suggests that significant increases in sensitivity can beachieved [70]. Diagnostics must move past the proof-of-conceptstage towards the development of practical diagnostic devices.While a number of barriers remain, including both technicalhurdles and commercial issues, new nanotechnology-baseddiagnostic devices can be expected in coming years [71].
For delivery of drugs and other therapeutic cargos, the poten-tial of targeted therapy to increase effective delivery to the spe-cific target, while decreasing nonspecific systemic effects islikely to spur rapid growth in this area. Effective developmentof new targeted drug delivery regimes will require improvedunderstanding of the mechanisms through which nanoparticlesinteract with the physiological environment, and thus parame-ters such as systemic residence and delivery of therapeutic cargoto the appropriate cellular and intracellular target can be pre-dicted and optimized [72]. For tissue engineering and repair,self-assembling scaffolds injected as an adjunct to cell-basedtherapies to form a prosurvival microenvironment show greatpromise for improving cardiac repair. Over the next few years,preclinical testing in larger animals followed by clinical studiescan be expected.
Key issues
• Heart, lung and blood diseases impose an enormous burden in mortality and morbidity and in economic costs.
• Nanotechnology has the potential to reduce these burdens by facilitating both diagnostics and therapeutics.
• Point-of-care in vitro diagnostics will be enabled by nanotechnology, facilitating personalized medicine.
• Imaging with nanoparticles can benefit from the delivery of contrast agents to specific sites, such as atherosclerotic plaque, through targeting moieties.
• Similar strategies can improve delivery of drugs to targets while decreasing adverse systemic effects.
• Tissue engineering and regenerative medicine can benefit from improved scaffolds with nanoscale features for in vitro tissue engineering and injectable self-assembling scaffolds for in vivo repair.
• Development of a systematic nanotoxicology program will be essential to ensure the long-term safety of nanomaterials.
ReferencesPapers of special note have been highlighted as:• of interest•• of considerable interest
1 Choudhury RP, Fuster V, Fayad ZA. Molecular, cellular and functional imaging of atherothrombosis. Nat. Rev. Drug Discov. 3, 913–925 (2004).
2 Kelly KA, Allport JR, Tsourkas A et al. Detection of vascular adhesion molecule-1 expression using a novel multimodal nanoparticle. Circ. Res. 96, 327–336 (2005).
3 Nahrendorf M, Jaffer FA, Kelly KA et al. Noninvasive vascular cell adhesion molecule-1 imaging identifies inflammatory activation of cells in atherosclerosis. Circulation 114(14), 1504–1511 (2006).
•• Novel targeting agent gives improved detection of early-stage atherosclerotic plaque.
4 Aikawa E, Nahrendorf M, Sosnovik D et al. Multimodality molecular imaging identifies proteolytic and osteogenic activities in early aortic valve disease. Circulation 115, 377–386 (2007).
5 Jaffer FA, Nahrendorf M, Sosnovik D et al. Cellular imaging of inflammation in atherosclerosis using magnetofluorescent nanomaterials. Mol. Imaging 5, 85–92 (2006).
6 Trivedi RA, Mallawarachi C, JM, U-King-Im JM et al. Identifying inflamed carotid plaques using in vivo USPIO-enhanced MR imaging to label plaque macrophages. Arterioscler. Thromb. Vasc. Biol. 26, 1601–1606 (2006).
7 Winter PM, Morawski AM, Caruthers SD et al. Molecular imaging of angiogenesis in early-stage atherosclerosis with αvβ3-integrin-targeted nanoparticles. Circulation 108, 2270–2274 (2003).
8 Flacke S, Fischer S, Scott MJ et al. Novel MRI contrast agent for molecular imaging of fibrin: implications for detecting vulnerable plaques. Circulation 104, 1280–1285 (2001).
9 Gao X, Yang L, Petros JA et al. In vivo molecular and cellular imaging with quantum dots. Curr. Opin. Biotechnol. 16, 63–72 (2005).
10 Soltesz EG, Kim S, Laurence RG et al. Intraoperative sentinel lymph node mapping of the lung using near-infrared fluorescent quantum dots. Ann. Thorac. Surg. 79, 269–277 (2005).
11 Daldrup-Link HE, Rudelius M, Piontek G et al. Migration of iron oxide-labeled human hematopoietic progenitor cells in a mouse model: in vivo monitoring with 1.5-T MR imaging equipment. Radiology 234, 197–205 (2005).
12 Nitin N, LaConte LE, Zurkiya O, Hu X, Bao G. Functionalization and peptide-based delivery of magnetic nanoparticles as an intracellular MRI contrast agent. J. Biol. Inorg. Chem. 9, 706–712 (2004).
13 Rabin O, Manuel Perez J, Grimm J, Wojtkiewicz G, Weissleder R. An x-ray computed tomography imaging agent based on long-circulating bismuth sulphide nanoparticles. Nat. Mater. 5, 118–122 (2006).
14 Hainfeld JF, Slatkin DN, Focella TM, Smilowitz HM. Gold nanoparticles: a new x-ray contrast agent. Br. J. Radiol. 79, 248–253 (2006).
15 Fatouros PP, Corwin FD, Chen ZJ et al. In vitro and in vivo imaging studies of a new endohedral metallofullerene nanoparticle. Radiology 240(3), 756–764 (2006).
16 Jain KK. Nanotechnology in clinical laboratory diagnostics. Clin. Chim. Acta 358, 37–54 (2005).
• Recent review describing some of the nanotechnologies available for medical diagnostics.
17 Bashir R. BioMEMS: state-of-the-art in detection, opportunities and prospects. Adv. Drug Deliv. Rev. 56, 1565–1586 (2004).
18 Cheng MM, Cuda G, Bunimovich YL et al. Nanotechnologies for biomolecular detection and medical diagnostics. Curr. Opin. Chem. Biol. 10, 11–19 (2006).

Nanotechnology in heart, lung and blood disease
www.future-drugs.com 159
19 Murphy D, Redmond G. Optical detection and discrimination of cystic fibrosis-related genetic mutations using oligonucleotide-nanoparticle conjugates. Anal. Bioanal. Chem. 381, 1122–1129 (2005).
20 Zhang J, Lang HP, Huber F et al. Rapid and label-free nanomechanical detection of biomarker transcripts in human RNA. Nat. Nanotech. 1, 214–220 (2006).
21 Georganopoulou DG, Chang L, Nam JM et al. Nanoparticle-based detection in cerebral spinal fluid of a soluble pathogenic biomarker for Alzheimer's disease. Proc. Natl Acad. Sci. USA 102, 2273–2276 (2005).
22 Stoeva SI, Lee JS, Smith JE, Rosen ST, Mirkin CA. Multiplexed detection of protein cancer markers with biobarcoded nanoparticle probes. J. Am. Chem. Soc. 128, 8378–9379 (2006).
•• Ultrasensitive protein detection that can be multiplexed to detect multiple proteins simultaneously.
23 Kumar A, Aravamudhan S, Gordic M, Bhansali S, Mohapatra SS. Ultrasensitive detection of cortisol with enzyme fragment complementation technology using functionalized nanowire. Biosens. Bioelectron. (2006) (Epub ahead of print).
24 Aravamudhan S, Kumar A, Mohapatra S, Bhansali S. Sensitive estimation of total cholesterol in blood using Au nanowires based micro-fluidic platform. Biosens. Bioelectron. (2007) (Epub ahead of print).
25 Malinski T. Understanding nitric oxide physiology in the heart: a nanomedical approach. Am. J. Cardiol. 96, 13i–24i (2005).
26 Mason RP, Kalinowski L, Jacob RF, Jacoby AM, Malinski T. Nebivolol reduces nitroxidative stress and restores nitric oxide bioavailability in endothelium of black Americans. Circulation 112, 3795–3801 (2005).
27 Gradishar WJ, Tjulandin S, Davidson N et al. Phase III trial of nanoparticle albumin-bound paclitaxel compared with polyethylated castor oil-based paclitaxel in women with breast cancer. J. Clin. Oncol. 23, 7794–7803 (2005).
28 Sparreboom A, Baker SD, Verweij J. Paclitaxel repackaged in an albumin-stabilized nanoparticle: handy or just a dandy? J. Clin. Oncol. 23, 7765–7767 (2005).
29 Hoffart V, Lamprecht A, Maincent P et al. Oral bioavailability of a low molecular weight heparin using a polymeric delivery system. J. Control Release 113, 38–42 (2006).
30 Zhang L, Hoffman JA, Ruoslahti E. Molecular profiling of heart endothelial cells. Circulation 112, 1601–1611 (2005).
• Example of the use of phage display to find tissue-specific endothelial targets for imaging and drug delivery.
31 Pilch J, Brown DM, Komatsu M et al. Peptides selected for binding to clotted plasma accumulate in tumor stroma and wounds. Proc. Natl Acad. Sci. USA 103(8), 2800–2804 (2006).
32 Hoshino A, Fujioka K, Oku T et al. Quantum dots targeted to the assigned organelle in living cells. Microbiol. Immunol. 48, 985–994 (2004).
33 Winter PM, Neubauer AM, Caruthers SD et al. Endothelial αvβ3 integrin-targeted fumagillin nanoparticles inhibit angiogenesis in atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 26, 2103–2109 (2006).
34 Jeon O, Kang SW, Lim HW, Hyung Chung J, Kim BS. Long-term and zero-order release of basic fibroblast growth factor from heparin-conjugated poly(L-lactide-co-glycolide) nanospheres and fibrin gel. Biomaterials 27, 1598–1607 (2006).
35 Uwatoku T, Shimokawa H, Abe K et al. Application of nanoparticle technology for the prevention of restenosis after balloon injury in rats. Circ. Res. 92, e62–e69 (2003).
36 Banai S, Chorny M, Gertz SD et al. Locally delivered nanoencapsulated tyrphostin (AGL-2043) reduces neointima formation in balloon-injured rat carotid and stented porcine coronary arteries. Biomaterials 26, 451–461 (2005).
37 Bhargava B, Reddy NK, Karthikeyan G et al. A novel paclitaxel-eluting porous carbon-carbon nanoparticle coated, nonpolymeric cobalt-chromium stent: evaluation in a porcine model. Catheter. Cardiovasc. Interv. 67(5), 698–702 (2006).
• Novel nanoparticle-coated stent demonstrates promise for reducing inflammatory responses.
38 Richter GM, Stampfl U, Stampfl S et al. A new polymer concept for coating of vascular stents using PTFEP (poly(bis(trifluoroethoxy)phosphazene) to reduce thrombogenicity and late in-stent stenosis. Invest. Radiol. 40, 210–218 (2005).
39 Oberdorster G, Oberdorster E, Oberdorster J. Nanotoxicology: an emerging discipline evolving from studies of ultrafine particles. Environ. Health Perspect. 113, 823–839 (2005).
40 Heyder J, Gebhart J, Rudolf G, Schiller C, Stahlhofen W. Deposition of particles in the human respiratory tract in the size range 0.005–15 μm. J. Aerosol Sci. 17, 811–825 (1986).
41 Tsapis N, Bennett D, Jackson B, Weitz DA, Edwards DA. Trojan particles: large porous carriers of nanoparticles for drug delivery. Proc. Natl Acad. Sci. USA 99, 12001–12005 (2002).
42 Grenha A, Seijo B, Remunan-Lopez C. Microencapsulated chitosan nanoparticles for lung protein delivery. Eur. J. Pharm. Sci. 25, 427–437 (2005).
43 Pandey R, Khuller GK. Antitubercular inhaled therapy: opportunities, progress and challenges. J. Antimicrob. Chemother. 55, 430–435 (2005).
44 Pandey R, Sharma A, Zahoor A et al. Poly (DL-lactide-co-glycolide) nanoparticle-based inhalable sustained drug delivery system for experimental tuberculosis. J. Antimicrob. Chemother. 52, 981–986 (2003).
45 Lee DW, Shirley SA, Lockey RF, Mohapatra SS. Thiolated chitosan nanoparticles enhance anti-inflammatory effects of intranasally delivered theophylline. Respir. Res. 7, 112 (2006).
46 Zhang W, Yang H, Kong X et al. Inhibition of respiratory syncytial virus infection with intranasal siRNA nanoparticles targeting the viral NS1 gene. Nat. Med. 11, 56–62 (2005).
47 Konstan MW, Davis PB, Wagener JS et al. Compacted DNA nanoparticles administered to the nasal mucosa of cystic fibrosis subjects are safe and demonstrate partial to complete cystic fibrosis transmembrane regulator reconstitution. Hum. Gene Ther. 15, 1255–1269 (2004).
•• Clinical trial demonstrating the potential of nanoparticles as a gene delivery tool in patients.
48 Fink TL, Klepcyk PJ, Oette SM et al. Plasmid size up to 20 kbp does not limit effective in vivo lung gene transfer using compacted DNA nanoparticles. Gene Ther.13, 1048–1051 (2006).
49 Hoeben BJ, Burgess DS, McConville JT et al. In vivo efficacy of aerosolized nanostructured itraconazole formulations for prevention of invasive pulmonary aspergillosis. Antimicrob. Agents Chemother. 50, 1552–1554 (2006).
50 Kleemann E, Neu M, Jekel N et al. Nano-carriers for DNA delivery to the lung based upon a TAT-derived peptide covalently coupled to PEG-PEI. J. Control Release 109, 299–316 (2005).
51 Dinauer N, Balthasar S, Weber C et al. Selective targeting of antibody-conjugated nanoparticles to leukemic cells and primary T-lymphocytes. Biomaterials 26, 5898–5906 (2005).

Buxton
160 Expert Rev. Mol. Diagn. 7(2), (2007)
52 Kwon YJ, James E, Shastri N, Frechet JM. In vivo targeting of dendritic cells for activation of cellular immunity using vaccine carriers based on pH-responsive microparticles. Proc. Natl Acad. Sci. USA 102, 18264–18268 (2005).
53 Kwon YJ, Standley SM, Goh SL, Frechet JM. Enhanced antigen presentation and immunostimulation of dendritic cells using acid-degradable cationic nanoparticles. J. Control Release 105(3), 199–212 (2005).
54 Wang X, Uto T, Sato K et al. Potent activation of antigen-specific T cells by antigen-loaded nanospheres. Immunol. Lett. 98, 123–130 (2005).
55 Ellis-Behnke RG, Liang Y-X, Tay DKC et al. Nano hemostat solution: immediate hemostasis at the nanoscale. Nanomed. Nanotech. Biol. Med. 2 (2006).
•• Use of self-assembling peptides forming nanofibers to give ultra-rapid hemostasis.
56 Yokoi H, Kinoshita T, Zhang S. Dynamic reassembly of peptide RADA16 nanofiber scaffold. Proc. Natl Acad. Sci. USA 102, 8414–8419 (2005).
57 Norman JJ, Desai TA. Methods for fabrication of nanoscale topography for tissue engineering scaffolds. Ann. Biomed. Eng. 34, 89–101 (2006).
58 Zong X, Bien H, Chung CY et al. Electrospun fine-textured scaffolds for heart tissue constructs. Biomaterials 26, 5330–5338 (2005).
59 Ishii O, Shin M, Sueda T, Vacanti JP. In vitro tissue engineering of a cardiac graft using a degradable scaffold with an extracellular matrix-like topography. J. Thorac. Cardiovasc. Surg. 130, 1358–1363 (2005).
• Use of nanofibrous scaffolds to engineer myocardium in vitro.
60 Davis ME, Motion JP, Narmoneva DA et al. Injectable self-assembling peptide nanofibers create intramyocardial microenvironments for endothelial cells. Circulation 111, 442–450 (2005).
61 Narmoneva DA, Oni O, Sieminski AL et al. Self-assembling short oligopeptides and the promotion of angiogenesis. Biomaterials 26, 4837–4846 (2005).
62 Hsieh PC, Davis ME, Gannon J, MacGillivray C, Lee RT. Controlled delivery of PDGF-BB for myocardial protection using injectable self-assembling peptide nanofibers. J. Clin. Invest. 116, 237–248 (2006).
63 Hsieh PC, MacGillivray C, Gannon J, Cruz FU, Lee RT. Local controlled intramyocardial delivery of platelet-derived growth factor improves postinfarction ventricular function without pulmonary toxicity. Circulation 114, 637–644 (2006).
•• Self-assembling peptides provide a nanostructured environment to preserve myocardium.
64 Davis ME, Hsieh PC, Takahashi T et al. Local myocardial insulin-like growth factor 1 (IGF-1) delivery with biotinylated peptide nanofibers improves cell therapy for myocardial infarction. Proc. Natl Acad. Sci. USA 103, 8155–8160 (2006).
65 Mondrinos MJ, Koutzaki S, Jiwanmall E et al. Engineering three-dimensional pulmonary tissue constructs. Tissue Eng. 12, 717–728 (2006).
66 Nel A, Xia T, Madler L, Li N. Toxic potential of materials at the nanolevel. Science 311, 622–627 (2006).
• Recent review highlighting the potential toxicities on nanoscale materials and the underlying mechanisms.
67 Radomski A, Jurasz P, Alonso-Escolano D et al. Nanoparticle-induced platelet aggregation and vascular thrombosis. Br. J. Pharmacol. 146, 882–893 (2005).
68 Shvedova AA, Castranova V, Kisin ER et al. Exposure to carbon nanotube material: assessment of nanotube cytotoxicity using human keratinocyte cells. J. Toxicol. Environ. Health A 66, 1909–1926 (2003).
69 Oberdorster G, Maynard A, Donaldson K et al. Principles for characterizing the potential human health effects from exposure to nanomaterials: elements of a screening strategy. Part. Fibre Toxicol. 2, 8 (2005).
70 Lee JH, Huh YM, Jun YW et al. Artificially engineered magnetic nanoparticles for ultra-sensitive molecular imaging. Nat. Med. 13, 95–99 (2007).
71 Kling J. Moving diagnostics from the bench to the bedside. Nat. Biotechnol. 24, 891–893 (2006).
72 Labhasetwar V. Nanotechnology for drug and gene therapy: the importance of understanding molecular mechanisms of delivery. Curr. Opin. Biotechnol. 16, 674–680 (2005).
Websites
101 US FDA nanotechnology site www.fda.gov/nanotechnology
102 Nanotechnology at National Institute for Occupational Safety and Health www.cdc.gov/niosh/topics/nanotech/default.html
103 National Toxicology Program http://ntp.niehs.nih.gov/index.cfm?objectid=7E6B19D0-BDB5-82F8-FAE73011304F542A
104 National Cancer Institute Alliance for Nanotechnology in cancer http://nano.cancer.gov/about_alliance/nanotech_characterization_lab.asp
Affiliation
• Denis B Buxton, PhD, ChiefNational Heart, Lung, & Blood Institute, Advanced Technologies & Surgery Branch, Division of Cardiovascular Diseases, 6701 Rockledge Drive, Bethesda, MD 20892, USATel.: +1 301 435 0516Fax: +1 301 480 [email protected]