Embed Size (px)
Citation preview
1
Curriculum VitaeName : Dr Syamsu Indra, SpPD, K-KV FINASIM, MARS, PhD.
Birth : Plaju, 28 Januari 1964
Education : 1990 - GP FK UNSRI
2002 - Internist FK UNSRI
2010 - Konsultan Kardiovascular FK UNSRI
2012 - MARS Universitas Respati Indonesia
2019 – PhD, Management Science University, Shah Alam,
Kuala Lumpur, Malaysia.
Experiences : 1992 – 1995 : Head of Public Health Centre Pagar Dewa,
Mesuji, OKI, Sumsel
1995 – 1996 : Doctor on duty, Tanah Merah Conoco Warim
B.V Marauke, Irian Jaya
1996 – 2002 : Internal Medicine Recident
2002 – 2004 : Staff Department of Internal Medicinepart, Prof WZ
Johannes Hospital, Kupang, NTT
2005 – Now : Staff Cardiologi Division Dement of Internal
Medicine, dr Moh Hoesin General Hospital.
2012 – 2016 : Head of Brain Heart Centre, dr Moh Hoesin
General Hospital.
2017 – Now : Head of National Referral Hospital, dr Moh
General Hoesin Hospital.
CURRICULUM VITAE

Diagnosis dan tatalaksana terkini sindrom koroner
akut
Dr. Syamsu Indra, SpPD, K-KV, FINASIM, MARS,PhD
Divisi Kardiologi, Departemen Ilmu Penyakit Dalam RSMH/FK UNSRI Palembang

Acute Coronary SyndromeSLIDE 3
• Acute Coronary Syndrome (ACS) refers to a spectrum of clinical
presentations ranging from those for ST-segment elevation
myocardial infarction (STEMI) to presentations found in non ST-
segment elevation myocardial infarction (NSTEMI) or in unstable
angina.
• It is almost always associated with rupture of an atherosclerotic
plaque and partial or complete thrombosis of the infarct-related
artery, resulting in decreased oxygen supply to the heart muscle.
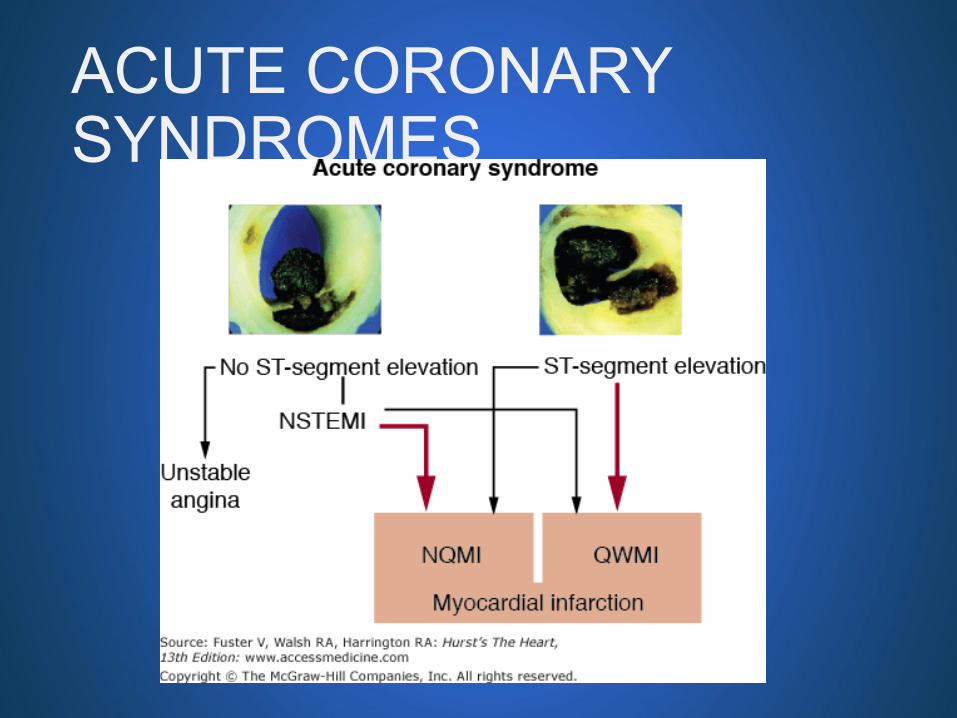
ACUTE CORONARY SYNDROMES

Cardiovascular Disease Risk Factors
Major Uncontrollable
• Age
• Sex
• Race
• Heredity
Major Controllable
Smoking
Hypertension
Dyslipidemia
Diabetes
Minor Controllable
Obesity
Lack of exercise
Stress
Personality
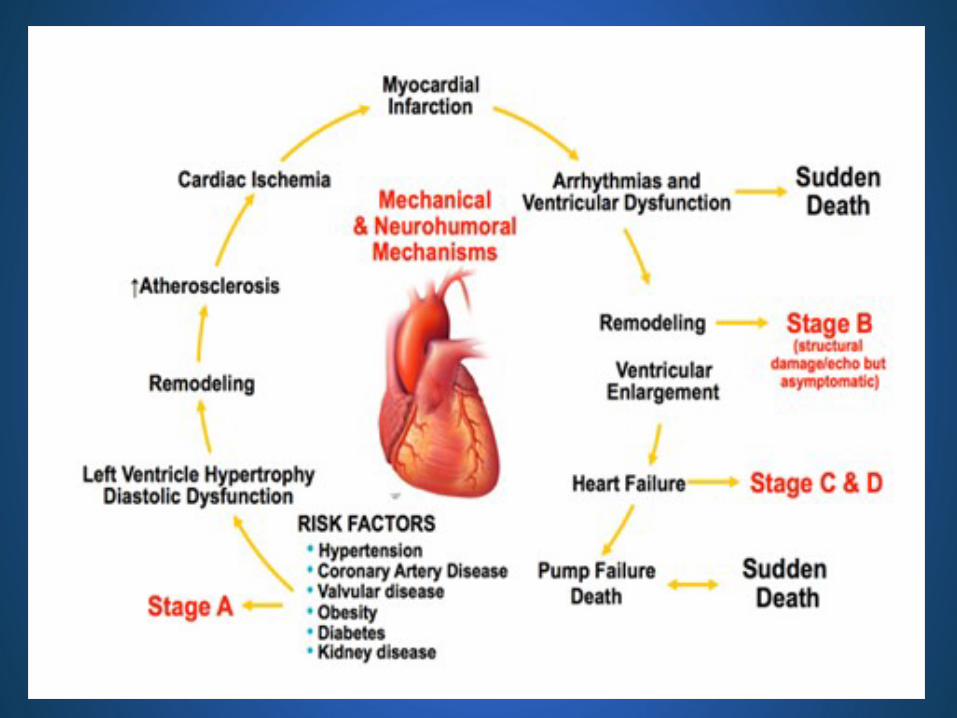

PathophysiologySLIDE 7
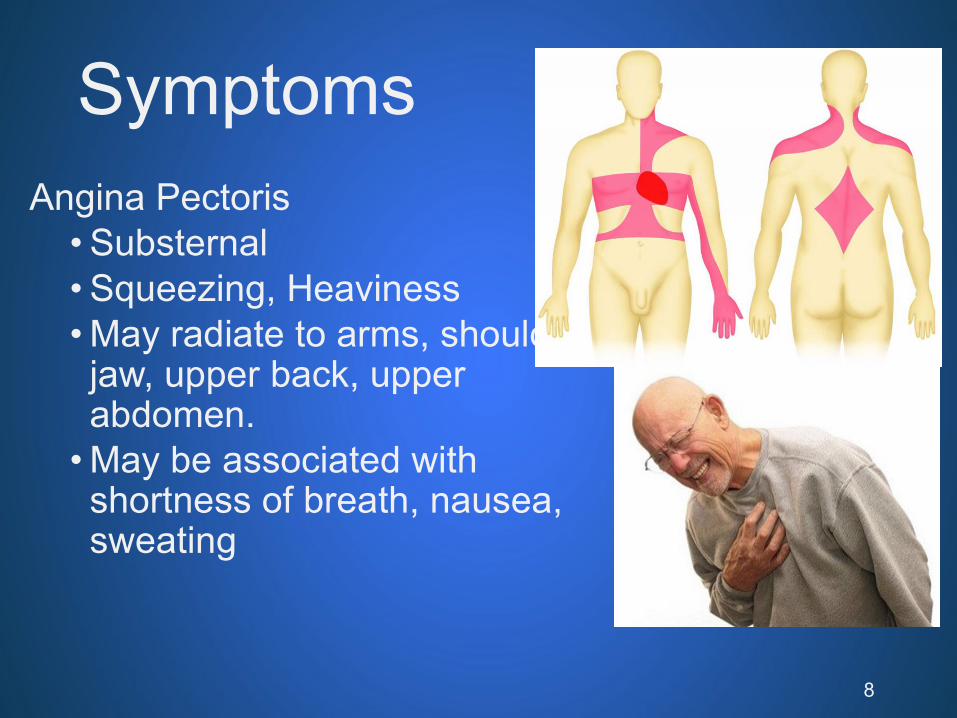
Symptoms
Angina Pectoris
• Substernal
• Squeezing, Heaviness
• May radiate to arms, shoulders, jaw, upper back, upper abdomen.
• May be associated with shortness of breath, nausea, sweating
8

Symptoms
Great anxiety/Fear
Pale or livid face
Dyspnea (SOB)
BP usually up during attack
Disritmia may be present
9

Forms of Angina Pectoris
Unstable Angina•More frequent/severe
•Can occur during rest
•Requires immediate treatment and transport to appropriate facility
10

THE ELECTROCARDIOGRAM
12 lead EKG• Cornerstone of initial evaluation
• Within 10 minutes of presentation
Previous EKG tracings• Compare
Serial EKGs • Essential

THE ELECTROCARDIOGRAM
1. ST segment elevation 2mm (2 contiguous leads), new LBBB
STEMI
2. ST depression >1mm, marked symmetrical T wave inversions >2 mm, dynamic ST-T changes with pain
UA/NSTEMI LIKELY
3. Non-diagnostic or normal ECG
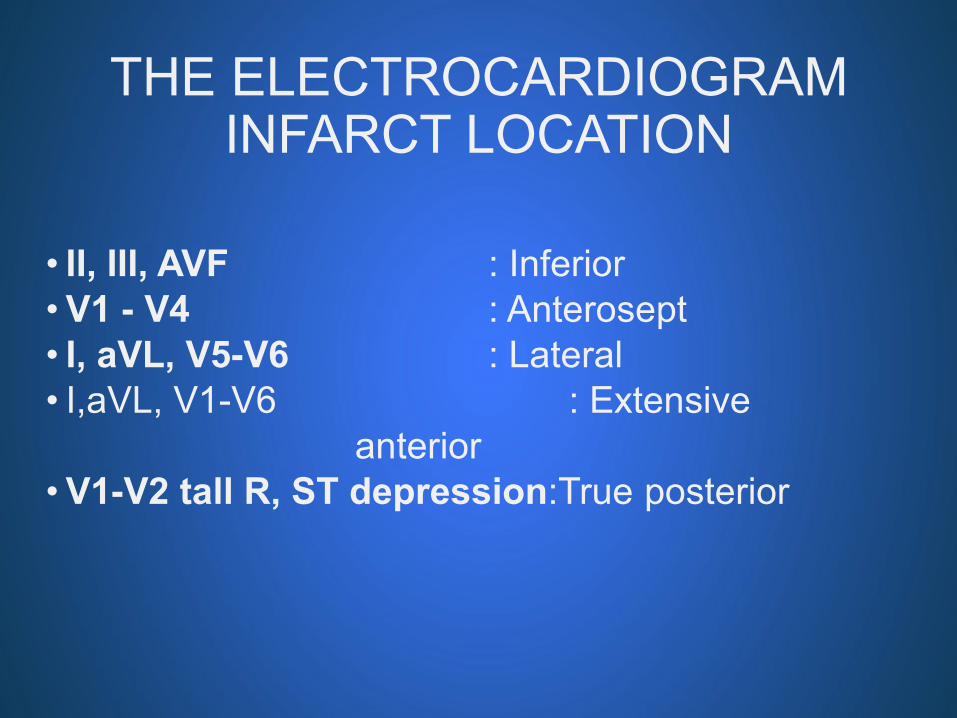
THE ELECTROCARDIOGRAMINFARCT LOCATION
• II, III, AVF : Inferior
• V1 - V4 : Anterosept
• I, aVL, V5-V6 : Lateral
• I,aVL, V1-V6 : Extensive
anterior
• V1-V2 tall R, ST depression:True posterior

SLIDE 14
Inferior STEMI
Which Part of the Heart is Affected?
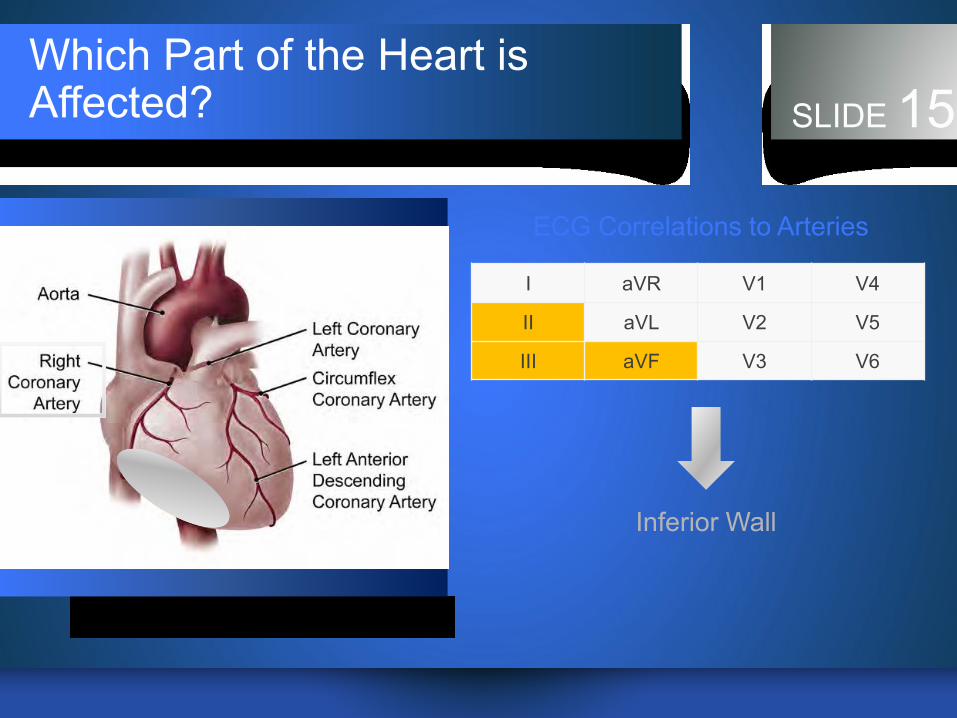
Which Part of the Heart is Affected? SLIDE 15
ECG Correlations to Arteries
I aVR V1 V4
II aVL V2 V5
III aVF V3 V6
Inferior Wall
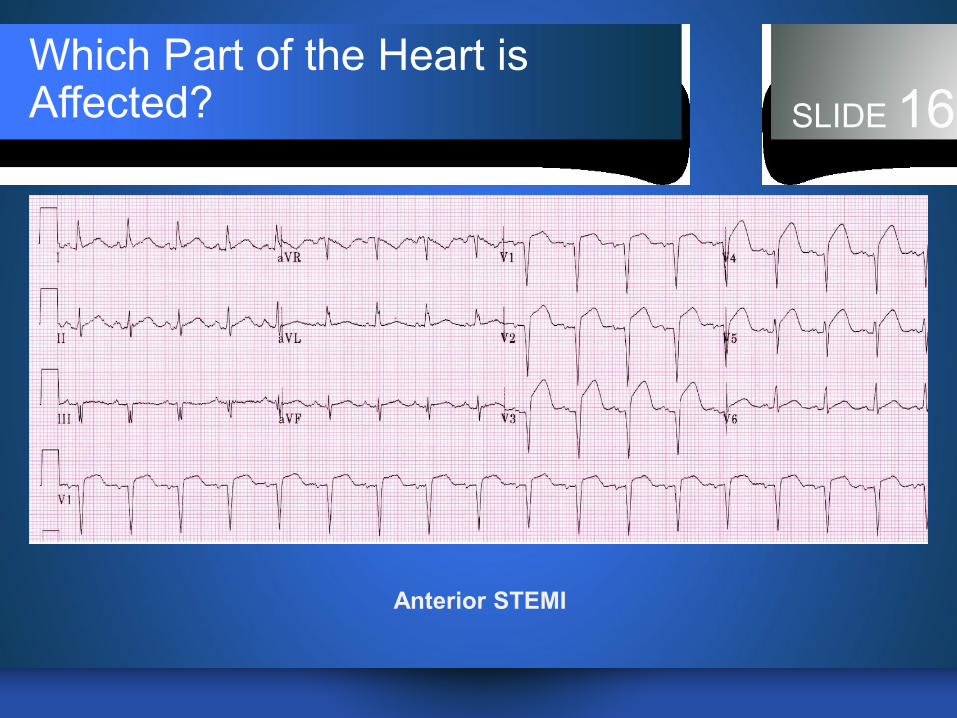
SLIDE 16
Anterior STEMI
Which Part of the Heart is Affected?

Which Part of the Heart is Affected? SLIDE 17
I aVR V1 V4
II aVL V2 V5
III aVF V3 V6
Anteroseptal Wall
ECG Correlations to Arteries
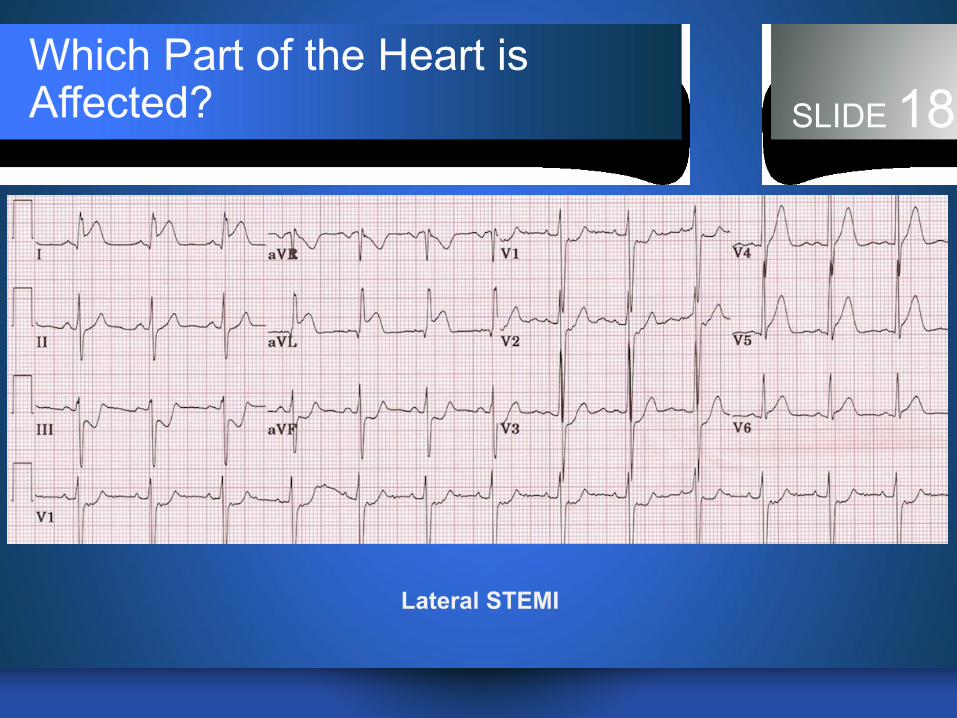
SLIDE 18
Lateral STEMI
Which Part of the Heart is Affected?
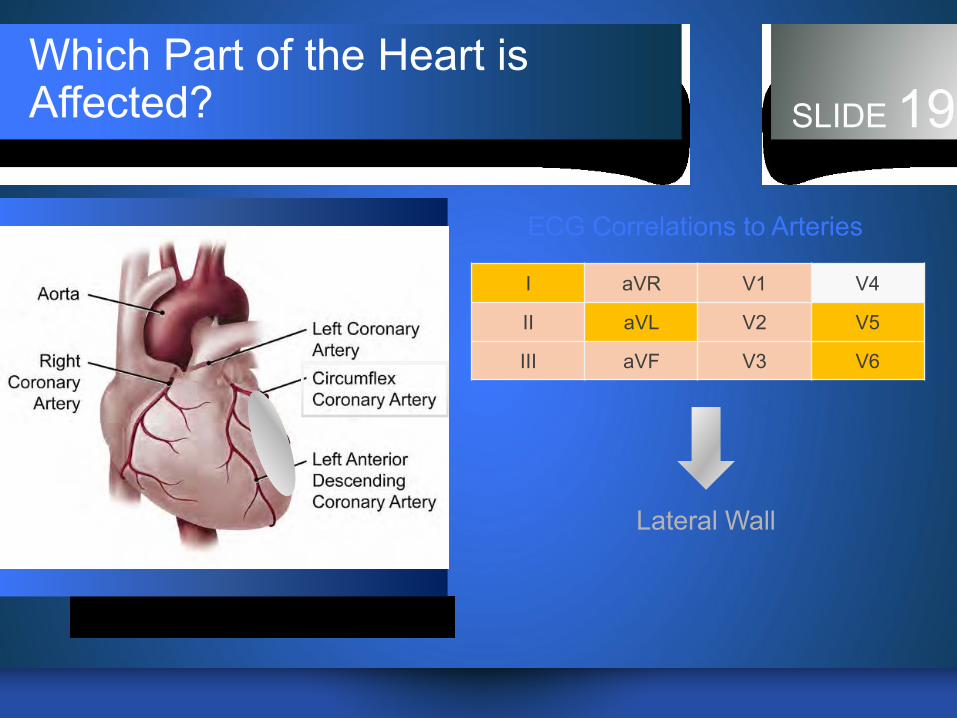
Which Part of the Heart is Affected? SLIDE 19
I aVR V1 V4
II aVL V2 V5
III aVF V3 V6
Lateral Wall
ECG Correlations to Arteries
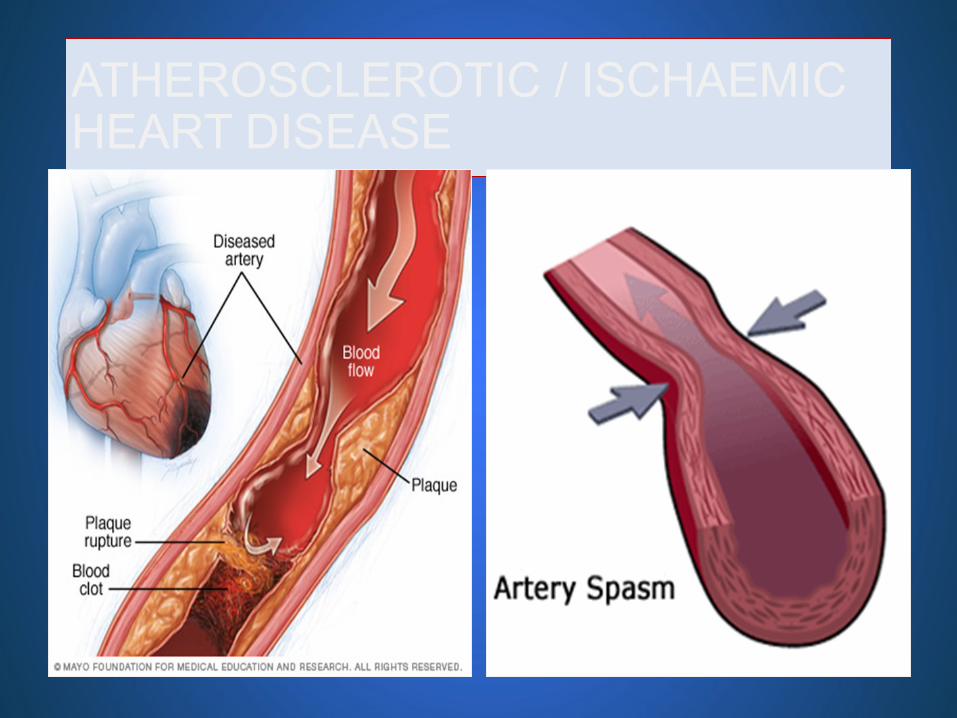
ATHEROSCLEROTIC / ISCHAEMIC HEART DISEASE

Cardiac enzyme Marker
Cardiac
enzyme
Marker
Initial
elevation
after AMI
Mean time
to peak
elevations
Time to
return to
baseline
Myoglobin 1-4hr 6-7hr 18-24hr
CTnI 3-12hr 10-24hr 3-10 day
CTnT 3-12hr 12-48hr 5-14 day
CKMB 4-12 hr 10-24hr 2-3day
TCK 2-6 hr 4.7hr(3-5) 72hr(50-96)

CARDIAC ENZYME

DIAGNOSIS
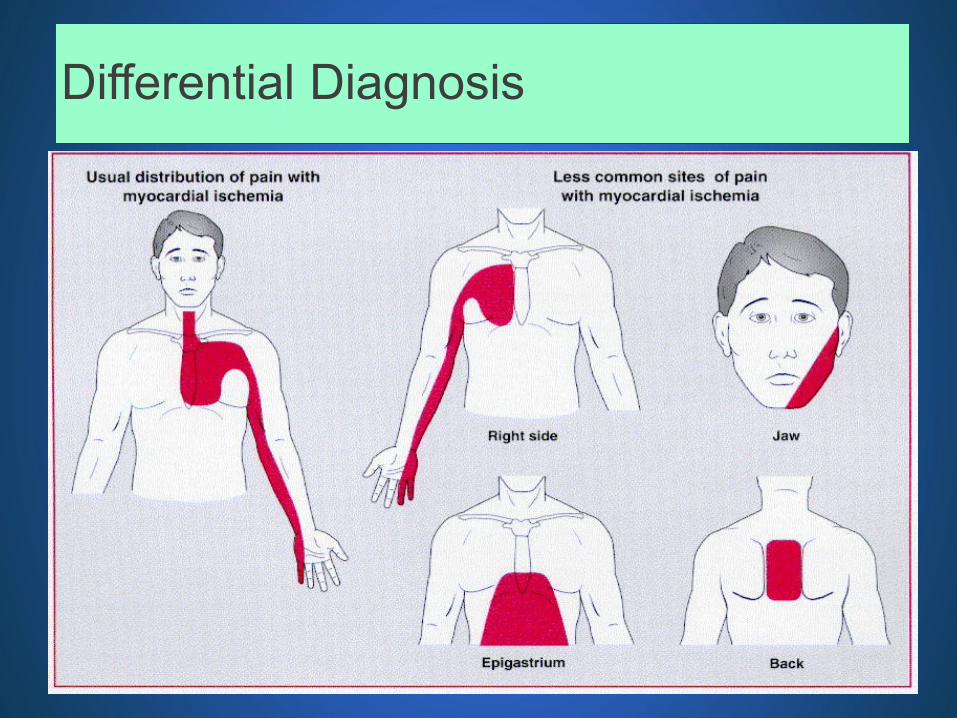
Differential Diagnosis
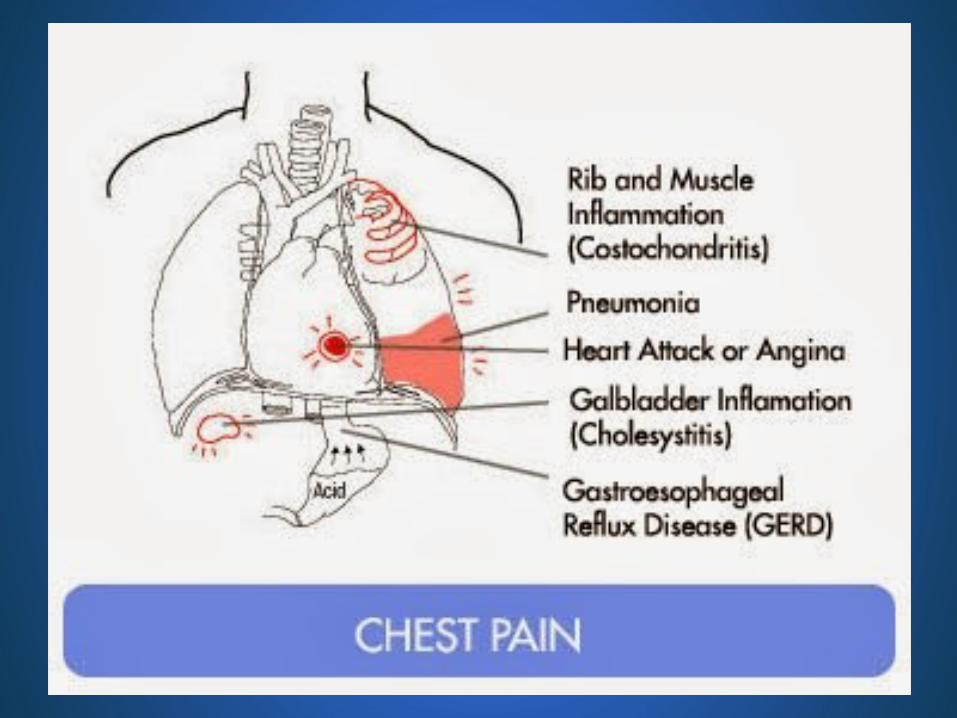
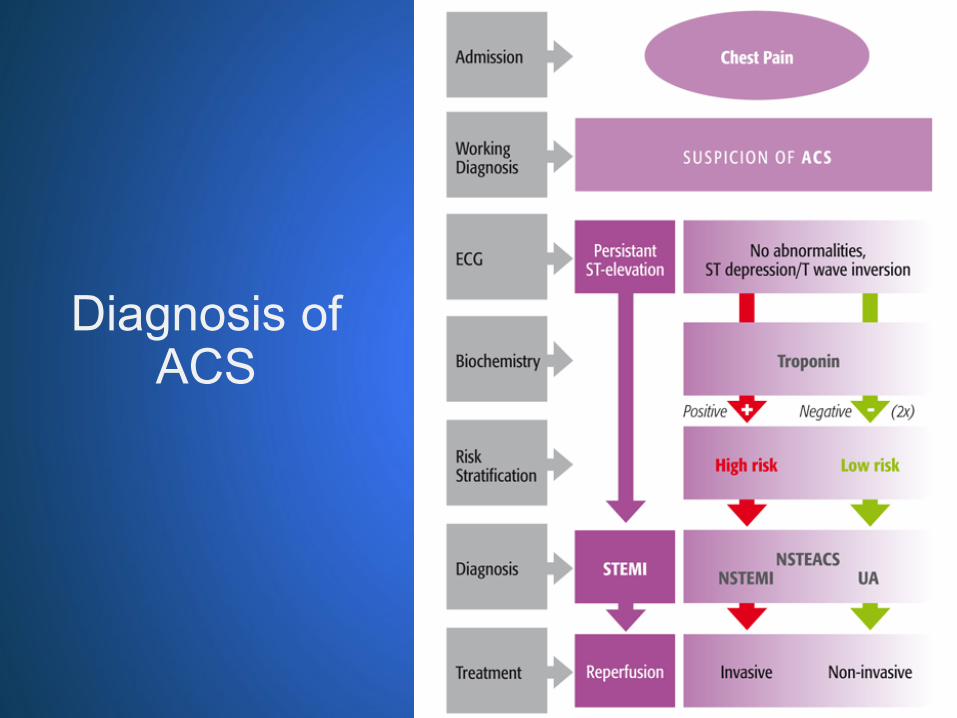
Diagnosis of ACS

Management of ACS

Primary Goals of TherapySLIDE 28
1
2
3 Preventing heart failure
4 Limiting other cardiovascular complication
Reduce the amount of myocardial necrosis that occurs in patients with acute myocardial infarction (AMI)
Preserving left ventricular (LV) function

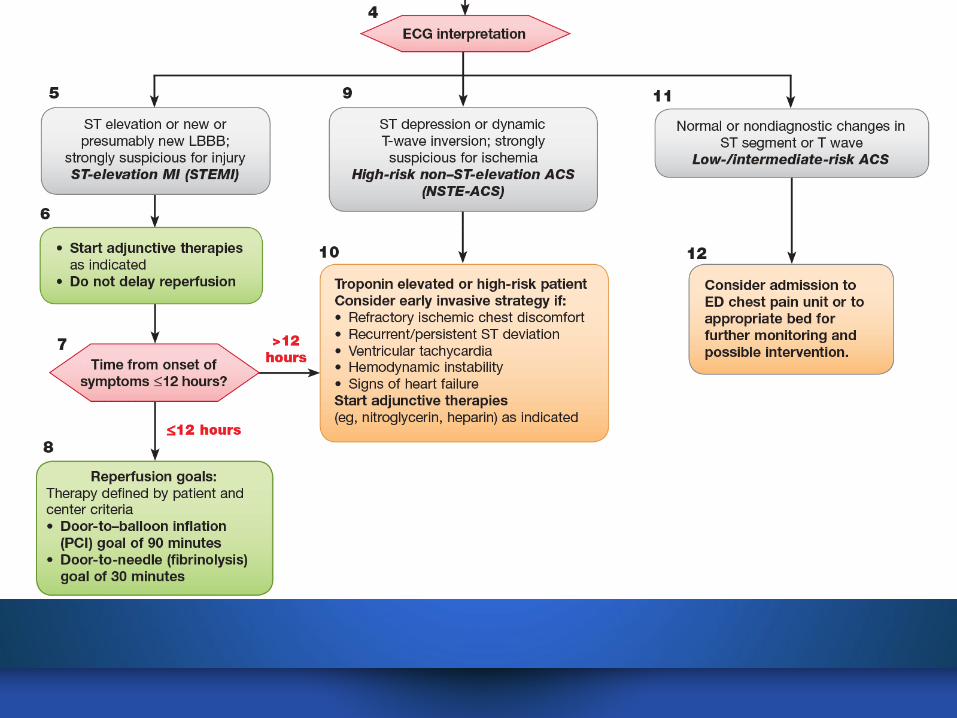
ACS AlgorithmSLIDE 29American Heart Association
SLIDE 30

TREATMENT
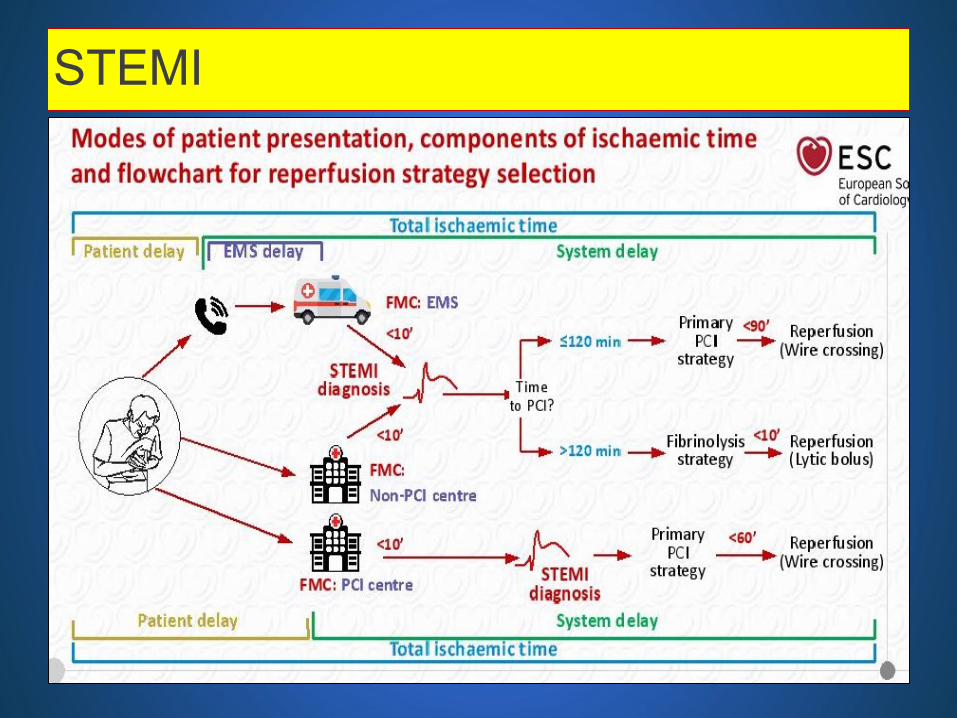
STEMI














That’s all. Thank you very much!

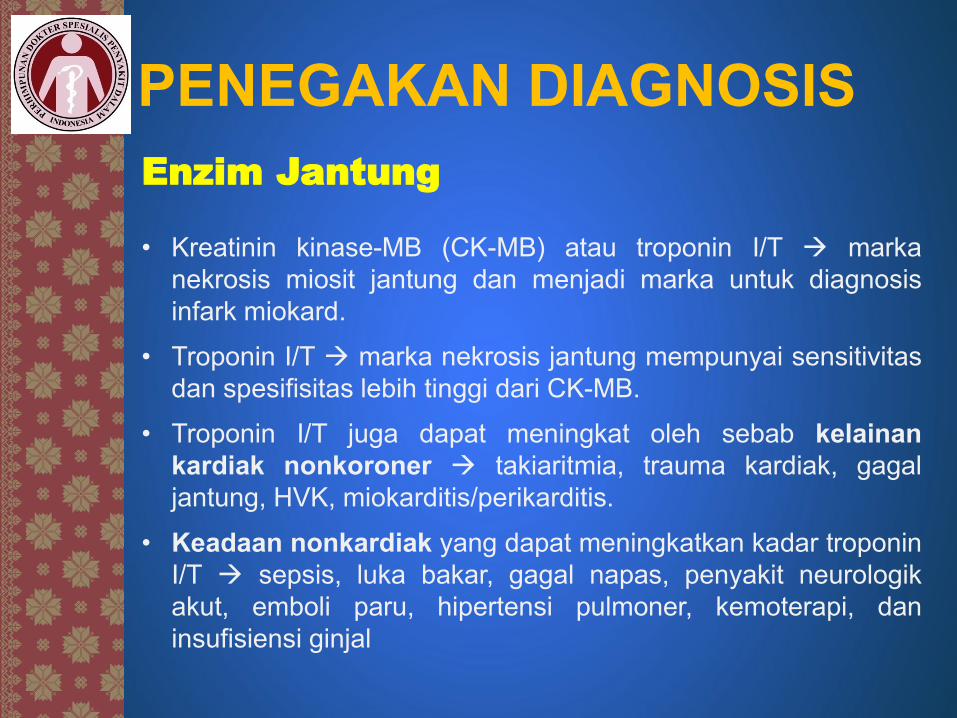
PENEGAKAN DIAGNOSIS
Enzim Jantung
• Kreatinin kinase-MB (CK-MB) atau troponin I/T marka
nekrosis miosit jantung dan menjadi marka untuk diagnosis
infark miokard.
• Troponin I/T marka nekrosis jantung mempunyai sensitivitas
dan spesifisitas lebih tinggi dari CK-MB.
• Troponin I/T juga dapat meningkat oleh sebab kelainan
kardiak nonkoroner takiaritmia, trauma kardiak, gagal
jantung, HVK, miokarditis/perikarditis.
• Keadaan nonkardiak yang dapat meningkatkan kadar troponin
I/T sepsis, luka bakar, gagal napas, penyakit neurologik
akut, emboli paru, hipertensi pulmoner, kemoterapi, dan
insufisiensi ginjal

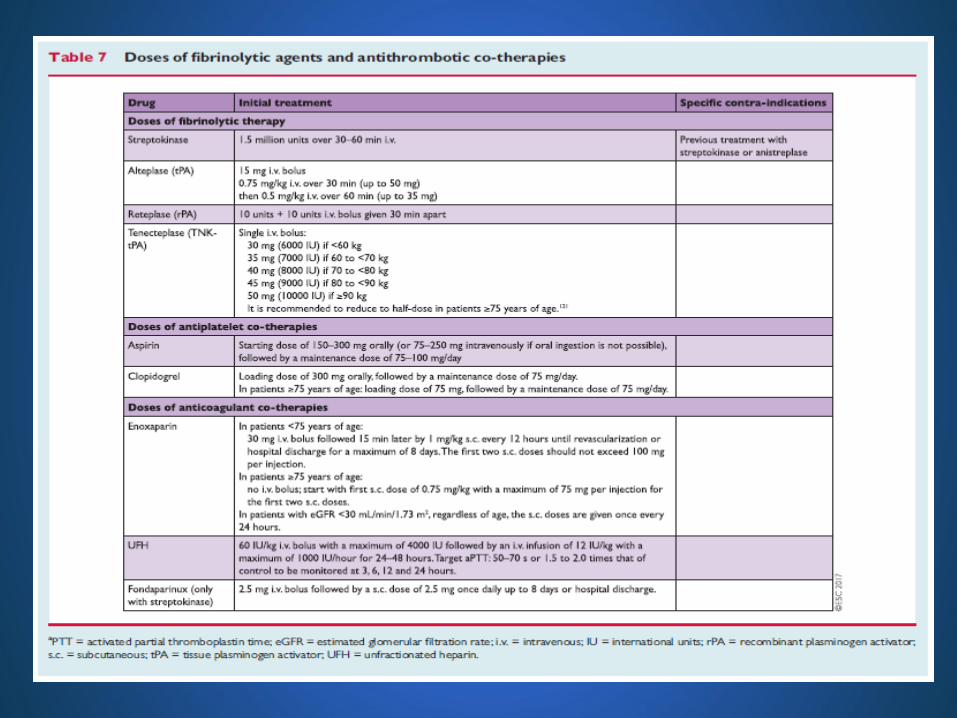
TATA LAKSANATindakan Umum dan Langkah Awal
• Tirah Baring
• Oksigen
• Aspirin
• Penghambat reseptor ADP
• Nitrogliserin/Isosorbid dinitrat
• Morfin

TATA LAKSANA
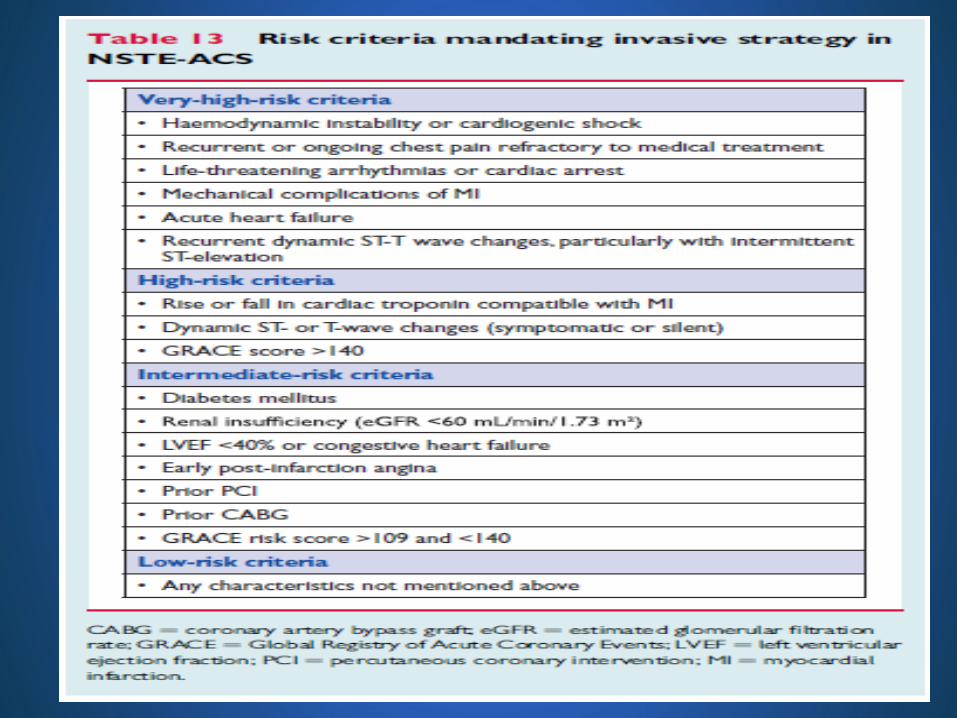
• Menilai stratifikasi resiko dgn TIMI score, Grace score, atau Crusade score
strategi invasive atau konservatif, dan waktu pelaksanaan revaskularisasi
• Waktu pelaksanaan angiografi menjadi 4 kategori:
1. Strategi invasif segera (<2 jam, urgent). Dilakukan bila pasien memenuhi
salah satu kriteria risiko sangat tinggi (very high risk)
2. Strategi invasif awal (early) dalam 24 jam. Dilakukan bila pasien
memiliki skor GRACE >140 atau dengan salah satu kriteria risiko tinggi (high
risk) primer.
3. Strategi invasif awal (early) dalam 72 jam. Dilakukan bila pasien
memenuhi salah satu kriteria risiko tinggi (high risk) atau dengan gejala
berulang
4. Strategi konservatif (tidak dilakukan angiografi) atau angiografi
elektif

Skor TIMI untuk UAP & NSTEMI

Skor GRACE
(dikutip dari Killip T, Kimball JT (Oct 1967). “Treatment of
myocardial infarction in a coronary care unit. A two year
experience with 250 patients”. Am J Cardiol. 20 (4): 457–64.)
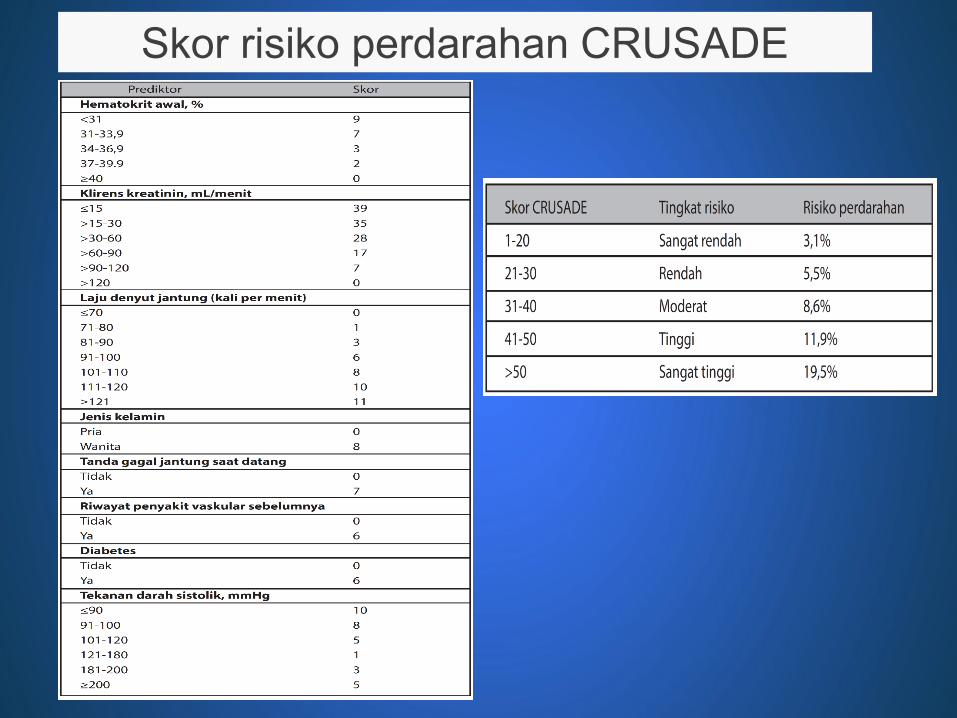
Skor risiko perdarahan CRUSADE


KLASIFIKASI




Algorithm for Management of Patients With Definite or Likely NSTE-ACS
NSTE-ACS: Definite or Likely
Ischemia-Guided Strategy Early Invasive Strategy
Initiate DAPT and Anticoagulant Therapy1. ASA (Class I; LOE: A)
2. P2Y12 inhibitor (in addition to ASA) (Class I; LOE: B) :· Clopidogrel or
· Ticagrelor
3. Anticoagulant:· UFH (Class I; LOE: B) or
· Enoxaparin (Class I; LOE: A) or
· Fondaparinux (Class I; LOE: B)
Initiate DAPT and Anticoagulant Therapy1. ASA (Class I; LOE: A)
2. P2Y12 inhibitor (in addition to ASA) (Class I; LOE: B):· Clopidogrel or
· Ticagrelor
3. Anticoagulant:· UFH (Class I; LOE: B) or
· Enoxaparin (Class I; LOE: A) or
· Fondaparinux† (Class I; LOE: B) or
· Bivalirudin (Class I; LOE: B)
Medical therapy chosen based on cath
findings
PCI With StentingInitiate/continue antiplatelet and anticoagulant
therapy1. ASA (Class I; LOE: B)
2. P2Y12 Inhibitor (in addition to ASA) :· Clopidogrel (Class I; LOE: B) or
· Prasugrel (Class I; LOE: B) or
· Ticagrelor (Class I; LOE: B)
3. GPI (if not treated with bivalirudin at time of PCI)· High-risk features, not adequately pretreated
with clopidogrel (Class I; LOE: A)· High-risk features adequately pretreated with
clopidogrel (Class IIa; LOE: B)
4. Anticoagulant:· Enoxaparin (Class I; LOE: A) or
· Bivalirudin (Class I; LOE: B) or
· Fondaparinux† as the sole anticoagulant (Class III: Harm; LOE: B) or
· UFH (Class I; LOE: B)
CABGInitiate/continue ASA therapy and
discontinue P2Y12 and/or GPI therapy1. ASA (Class I; LOE: B)
2. Discontinue clopidogrel/ticagrelor 5 d before, and prasugrel at least 7 d before elective CABG
3. Discontinue clopidogrel/ticagrelor up to 24 h before urgent CABG (Class I; LOE: B). May perform urgent CABG <5 d after clopidogrel/ticagrelor and <7 d after prasugrel discontinued
4. Discontinue eptifibatide/tirofiban at least 2-4 h before, and abciximab ≥12 h before CABG (Class I; LOE: B)
Late Hospital/Posthospital Care1. ASA indefinitely (Class I; LOE: A)
2. P2Y12 inhibitor (clopidogrel or ticagrelor), in addition to ASA, up to 12 mo if medically treated (Class I; LOE: B)
3. P2Y12 inhibitor (clopidogrel, prasugrel, or ticagrelor), in addition to ASA, at least 12 mo if treated with coronary stenting (Class I; LOE: B)
Can consider GPI in addition to ASA and P2Y12 inhibitor in high-risk (e.g., troponin positive) pts (Class IIb; LOE: B)
· Eptifibatide
· Tirofiban
TherapyIneffective
TherapyEffective

NSTE-ACS: Definite or Likely
Ischemia-Guided Strategy Early Invasive Strategy
Initiate DAPT and Anticoagulant Therapy1. ASA (Class I; LOE: A)
2. P2Y12 inhibitor (in addition to ASA) (Class I; LOE: B) :· Clopidogrel or
· Ticagrelor
3. Anticoagulant:· UFH (Class I; LOE: B) or
· Enoxaparin (Class I; LOE: A) or
· Fondaparinux (Class I; LOE: B)
Initiate DAPT and Anticoagulant Therapy1. ASA (Class I; LOE: A)
2. P2Y12 inhibitor (in addition to ASA) (Class I; LOE: B):· Clopidogrel or
· Ticagrelor
3. Anticoagulant:· UFH (Class I; LOE: B) or
· Enoxaparin (Class I; LOE: A) or
· Fondaparinux† (Class I; LOE: B) or
· Bivalirudin (Class I; LOE: B)
Medical therapy chosen based on cath
findings
PCI With StentingInitiate/continue antiplatelet and anticoagulant
therapy1. ASA (Class I; LOE: B)
2. P2Y12 Inhibitor (in addition to ASA) :· Clopidogrel (Class I; LOE: B) or
· Prasugrel (Class I; LOE: B) or
· Ticagrelor (Class I; LOE: B)
3. GPI (if not treated with bivalirudin at time of PCI)· High-risk features, not adequately pretreated
with clopidogrel (Class I; LOE: A)· High-risk features adequately pretreated with
clopidogrel (Class IIa; LOE: B)
4. Anticoagulant:· Enoxaparin (Class I; LOE: A) or
· Bivalirudin (Class I; LOE: B) or
· Fondaparinux† as the sole anticoagulant (Class III: Harm; LOE: B) or
· UFH (Class I; LOE: B)
CABGInitiate/continue ASA therapy and
discontinue P2Y12 and/or GPI therapy1. ASA (Class I; LOE: B)
2. Discontinue clopidogrel/ticagrelor 5 d before, and prasugrel at least 7 d before elective CABG
3. Discontinue clopidogrel/ticagrelor up to 24 h before urgent CABG (Class I; LOE: B). May perform urgent CABG <5 d after clopidogrel/ticagrelor and <7 d after prasugrel discontinued
4. Discontinue eptifibatide/tirofiban at least 2-4 h before, and abciximab ≥12 h before CABG (Class I; LOE: B)
Late Hospital/Posthospital Care1. ASA indefinitely (Class I; LOE: A)
2. P2Y12 inhibitor (clopidogrel or ticagrelor), in addition to ASA, up to 12 mo if medically treated (Class I; LOE: B)
3. P2Y12 inhibitor (clopidogrel, prasugrel, or ticagrelor), in addition to ASA, at least 12 mo if treated with coronary stenting (Class I; LOE: B)
Can consider GPI in addition to ASA and P2Y12 inhibitor in high-risk (e.g., troponin positive) pts (Class IIb; LOE: B)
· Eptifibatide
· Tirofiban
TherapyIneffective
TherapyEffective
†In patients who have been treated with fondaparinux (as upfront therapy) who are
undergoing PCI, an additional anticoagulant with anti-IIa activity should be administered at
the time of PCI because of the risk of catheter thrombosis.

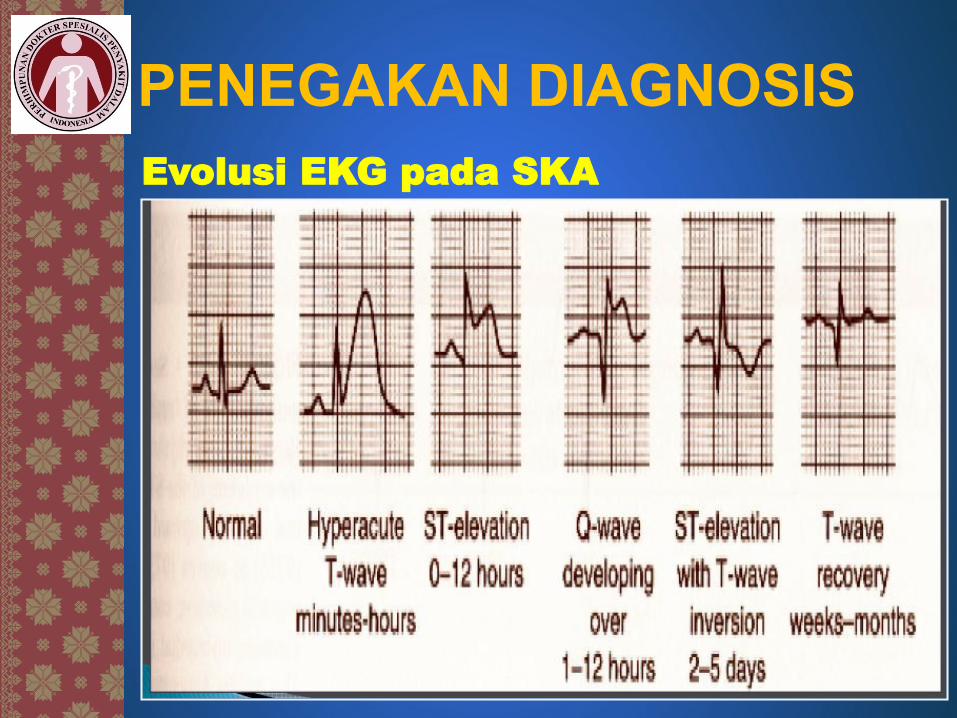
PENEGAKAN DIAGNOSIS
Evolusi EKG pada SKA






























