Embed Size (px)
Citation preview

NORTH CAROLINA HEALTHNET NETWORKS: WAKE UP AND SMELL THE COLLABORATION
Anne BraswellHealthNet Program Director
NC Office of Rural Health and Community Care
NCSCHA 2011 Annual ConferenceDecember 6, 2011
Raleigh, NC
2000: HEALTH RESOURCES AND SERVICES ADMINISTRATION
ANNOUNCEDCOMMUNITY ACCESS PROGRAM (CAP)
New federal grants program supporting community indigent care initiatives to increase access and quality of care for the uninsured and underserved
Expanded access for the uninsured by increasing effectiveness and capacity of the nation’s health care safety net at the community level
2

COMMUNITIES RECEIVING CAP FUNDS EXPECTED TO:
Build integrated health care delivery systems and a seamless continuum of care for uninsured and underinsured populations
Eliminate unnecessary, duplicative functions in service delivery and administration
Increase access to health care for low-income uninsured and underinsured persons
3
FIRST COMMUNITY ACCESS PROGRAM IN NORTH CAROLINA
June 2000: Office of Rural Health and Community Care applied for CAP funding on behalf of Community Care Plan of Eastern Carolina for Pitt, Greene, Edgecombe & Bertie Counties
September 2000: ORHCC awarded one of only 23 CAP grants in U.S. -- $897,000 for Pitt et al
4

2000: COMMUNITY CARE PLAN OF EASTERN CAROLINA AND ORHCC CREATED
“HEALTHASSIST”
Built upon administrative infrastructure of Community Care of North Carolina (CCNC)
Established 4 Community Resource Centers Co-located services with other community non-
profits (e.g. JOY Soup Kitchen; Pactolus Fire/Rescue)
Provided health care services, care coordination, wellness and prevention services, adult continuing education, and job skills training for low-income and uninsured residents5

BEGINNING 2001: HRSA REPLACED CAP WITH HEALTHY COMMUNITIES ACCESS
PROGRAM (HCAP)
Additional indigent care networks were initiated throughout NC with HCAP funding: Cabarrus, Guilford, Buncombe, Moore, Beaufort, Durham, Henderson, Orange/Chatham
Several communities initiated programs, but were not awarded federal funding: Mecklenburg, Wake, Vance/Warren, Wilkes, Wilson, Mitchell/ Yancey, Watauga, New Hanover, and others
6

7
orhcc: 06012010
1st HCAP Funded Indigent Care Network in NC
Community Indigent Care Networks
2000
Martin Tyrrell
Hertford
Dare
Brunswick
NewHanover
Pender
Cumberland
Northampton
Halifax
Nash
Wayne
Duplin
Edgecombe
Pitt
Greene
Bertie
Jones
Gates
Carteret
Pamlico
Washington
Hyde
Robeson
Columbus
Bladen
Sampson
Person
Harnett
Granville
Wake
Johnston
Franklin
Caswell
Alamance
Chatham
Orange
Davie
Stanly
Stokes
Rockingham
Guilford
Randolph
Union AnsonRichmond
Gaston
Mecklenburg
Cabarrus
Forsyth
Davidson
Montgomery
Alleghany
Wilkes
Surry
Ashe
Catawba
Yadkin
Iredell
Clay
Polk
Caldwell
WataugaMitchell
Cherokee Macon
GrahamSwain
Jackson
Haywood
Madison
Rutherford
McDowell
Yancey
Avery
Burke
Alexander
Transylvania
Henderson
Buncombe
Cleveland
Lincoln
Rowan
Moore
Scotland
Lee
Durham
Wilson
Lenoir
Beaufort
Craven
Onslow
Vance
Warren
Hoke
8
orhcc: 06012010
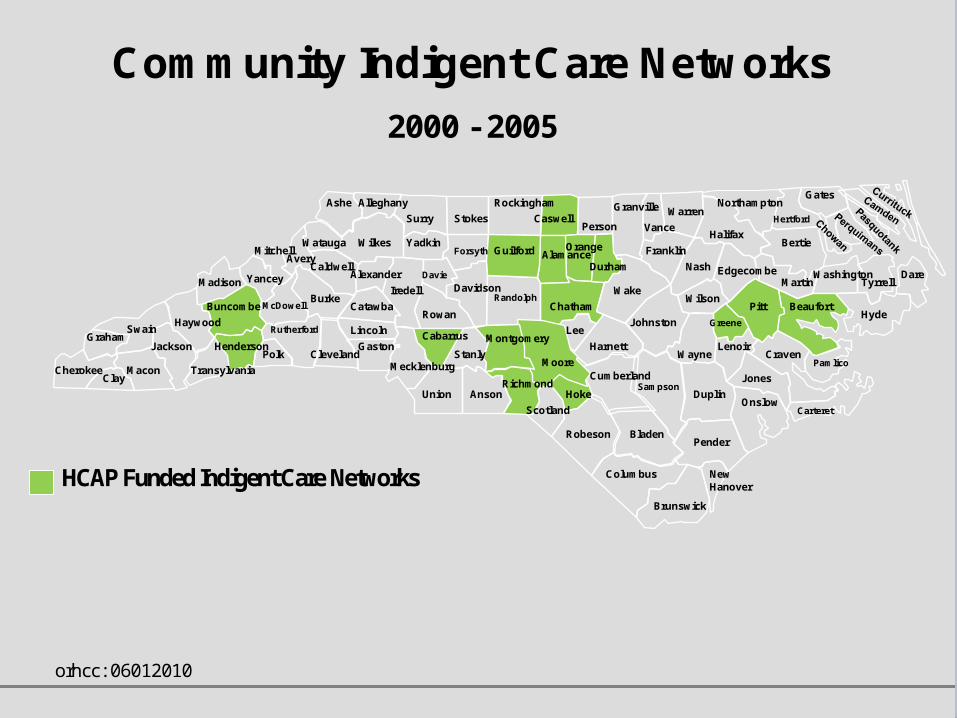
HCAP Funded Indigent Care Networks
Community Indigent Care Networks
2000 - 2005
Martin Tyrrell
Hertford
Dare
Brunswick
NewHanover
Pender
Cumberland
Northampton
Halifax
Nash
Wayne
Duplin
Edgecombe
Pitt
Greene
Bertie
Jones
Gates
Carteret
Pamlico
Washington
Hyde
Robeson
Columbus
Bladen
Sampson
Person
Harnett
Granville
Wake
Johnston
Franklin
Caswell
Alamance
Chatham
Orange
Davie
Stanly
Stokes
Rockingham
Guilford
Randolph
Union AnsonRichmond
Gaston
Mecklenburg
Cabarrus
Forsyth
Davidson
Montgomery
Alleghany
Wilkes
Surry
Ashe
Catawba
Yadkin
Iredell
Clay
Polk
Caldwell
WataugaMitchell
Cherokee Macon
GrahamSwain
Jackson
Haywood
Madison
Rutherford
McDowell
Yancey
Avery
Burke
Alexander
Transylvania
Henderson
Buncombe
Cleveland
Lincoln
Rowan
Moore
Scotland
Lee
Durham
Wilson
Lenoir
Beaufort
Craven
Onslow
Vance
Warren
Hoke

9
orhcc: 06012010
Indigent Care Networks initiated without HCAP Funding
HCAP Funded Indigent Care Networks
Community Indigent Care Networks
2000 - 2005
Martin Tyrrell
Hertford
Dare
Brunswick
NewHanover
Pender
Cumberland
Northampton
Halifax
Nash
Wayne
Duplin
Edgecombe
Pitt
Greene
Bertie
Jones
Gates
Carteret
Pamlico
Washington
Hyde
Robeson
Columbus
Bladen
Sampson
Person
Harnett
Granville
Wake
Johnston
Franklin
Caswell
Alamance
Chatham
Orange
Davie
Stanly
Stokes
Rockingham
Guilford
Randolph
Union AnsonRichmond
Gaston
Mecklenburg
Cabarrus
Forsyth
Davidson
Montgomery
Alleghany
Wilkes
Surry
Ashe
Catawba
Yadkin
Iredell
Clay
Polk
Caldwell
WataugaMitchell
Cherokee Macon
GrahamSwain
Jackson
Haywood
Madison
Rutherford
McDowell
Yancey
Avery
Burke
Alexander
Transylvania
Henderson
Buncombe
Cleveland
Lincoln
Rowan
Moore
Scotland
Lee
Durham
Wilson
Lenoir
Beaufort
Craven
Onslow
Vance
Warren
Hoke

IMPACT OF HCAP PROGRAM IN NC
Between 2000 and 2005, HCAP helped: Induce physicians and hospitals to provide
more free care and services for the uninsured Encourage local governments and
philanthropic organizations to provide matching investments of funds and resources
Bring about both perceived and measurable improvements in the health and wellness of participants
Reduce inappropriate use of hospital EDs and other costly services by participants 10

2005: HCAP NO LONGER FUNDED BY HRSA
After 2005, former HCAP sites and other programs in NC struggled to maintain the same level of programs and services with limited resources
Early in 2007, the last HCAP “carryover” funding ran out
In the summer of 2007, The Duke Endowment provided 4 months of emergency funds
11

A KEY LESSON LEARNED FROM HCAP:
There must be sustaining funds to support the administrative
infrastructure needed to effectively operate these indigent care programs and develop an integrated health care
delivery system for the uninsured.
12

2007: “NC HEALTHNET” INITIATIVE
In SFY 2007-08, NC General Assembly made a one-time appropriation to ORHCC of $2.88 million to implement HealthNet to
support North Carolina’s safety net primary care provider networks and
develop community-based systems of care serving the uninsured.
13

NC HEALTHNET:
Links local safety net organizations and indigent care programs providing free and
low-cost health care services with the infrastructure of Community Care of North
Carolina and CCNC’s networks of physicians and services.
14

HEALTHNET NETWORKS INCLUDE: Physicians Hospitals Public Health Free Clinics Rural Health Centers Community Health Centers School Based Health Centers Departments of Social Services Behavioral Health Law Enforcement Other Community-Based Safety Net
Organizations15

HEALTHNET TARGET POPULATION:
Uninsured adults, 18-64 years old, whose family income is at or below 200% of FPL
16

HEALTHNET ENROLLEES:
Provided a Primary Care Medical Home and access to:
Specialty Care Wellness Education Prevention Services Prescriptions Medications Care Coordination for Chronic Medical
Conditions Other Needed Services
17

HEALTHNET NETWORKS:
Receive technical assistance and grant funding from ORHCC to support the community’s ongoing efforts to:
Increase access and quality of care through a coordinated delivery system
Share and conserve limited resources through collaborative partnerships
18

SFY2007-08: HEALTHNET IN YEAR 1
Funded 16 HealthNet Networks providing services for the uninsured in 27 counties
40,000+ individuals were provided a medical home
25,000+ individuals had access to needed prescription medications
19

SFY 2008-09: HEALTHNET IN YEAR 2
In SFY 2008-09, ORHCC received $2.8 million in recurring appropriations to sustain existing HealthNet Networks plus $950,000 in non-recurring funds to develop new collaborativenetworks.
20

SFY 2008-09: HEALTHNET IN YEAR 2
Funded 21 HealthNet Networks that provide services for the uninsured in 39 counties
50,000+ individuals were provided a medical home
38,000+ individuals had access to needed prescription medications
21

SFY 2009-10: HEALTHNET IN YEAR 3
In SFY 2009-10, ORHCC received $4.8 million in recurring appropriations to sustain existing HealthNet Networks and develop new collaborative networks.
22

SFY 2009-10: HEALTHNET IN YEAR 3
Funded 31 HealthNet Networks that provide services for the uninsured in 63 counties
61,000+ individuals had access to a medical home
42,000+ individuals had access to needed prescription medications
2323

SFY 2010-11: HEALTHNET IN YEAR 4
In SFY 2010-11, ORHCC again received $4.8 million in recurring appropriations to sustain existing HealthNet Networks and develop new collaborative networks.
24

SFY 2010-11: HEALTHNET IN YEAR 4
Funding 35 HealthNet Networks that provide services for the uninsured in 70 counties
86,000+ individuals have a medical home
49,000+ individuals have access to needed prescription medications
2525

26orhcc: 06212011
Collaborative Networks of CareFunded by HealthNet
Martin Tyrrell
Hertford
Dare
Brunswick
NewHanover
Pender
Cumberland
Northampton
Halifax
Nash
Wayne
Duplin
Edgecombe
Pitt
Greene
Bertie
Jones
Gates
Carteret
Pamlico
Washington
Hyde
Robeson
Columbus
Bladen
Sampson
Person
Harnett
Granville
Wake
Johnston
Franklin
Caswell
Alamance
Chatham
Orange
Davie
Stanly
Stokes
Rockingham
Guilford
Randolph
Union AnsonRichmond
Gaston
Mecklenburg
Cabarrus
Forsyth
Davidson
Montgomery
Alleghany
Wilkes
Surry
Ashe
Catawba
Yadkin
Iredell
Clay
Polk
Caldwell
WataugaMitchell
Cherokee Macon
GrahamSwain
Jackson
Haywood
Madison
Rutherford
McDowell
Yancey
Avery
Burke
Alexander
Transylvania
Henderson
Buncombe
Cleveland
Lincoln
Rowan
Moore
Scotland
Lee
Durham
Wilson
Lenoir
Beaufort
Craven
Onslow
Vance
Warren
Hoke
Developing HealthNet Networks Targeted for Funding in SFY 2011-12 and SFY 2012-13 (12 counties)
Other Communities Developing Networks and Targeted for future HealthNet Funding if funding available (9 counties)
HealthNet Networks Funded SFY 2010-11 (69 counties)

ORHCC TECHNICAL ASSISTANCE
North Carolina Office of Rural Health and Community Care staff provides: Community Needs & Gap Analysis Strategic & Business Planning Network Development Medical, Dental, and Psychiatric
Provider Recruitment for Underserved Areas & Educational Loan Repayment
Architectural Design Support for Capital Projects
27

ORHCC TECHNICAL ASSISTANCE (CONTINUED)
Coordination with: Community Care of North
Carolina (CCNC) and MedicaidCritical Access Hospital ProgramFarm Worker Health ProgramMedical Access Plan Medication Assistance ProgramCommunity Health Grants
Program Regional trainings and webinars Bimonthly statewide HealthNet
Networks Meetings 28

ORHCC TECHNICAL ASSISTANCE (CONTINUED)
Free software applications fordetermining eligibility, enrollment,
resource commitments, referrals, care and disease management, tracking encounter claims data (CMIS) and
accessing 150+ pharmaceutical manufacturers’ free prescription drug programs and 4000+ drugs (MARP- Medication Access & Review Program)
More information at: http://www.ncdhhs.gov/orhcc/ 29

HEALTHNET AND CCNC-UPORHCC AND HEALTHNET PARTNERING WITH: the OFFICE of GOVERNOR BEVERLY PERDUE the NC DIVISION OF MEDICAL ASSISTANCE (MEDICAID) NORTH CAROLINA COMMUNITY CARE, INC. (N3CN) the NORTH CAROLINA FOUNDATION FOR ADVANCED
HEALTH PROGRAMS the NC INSTITUTE OF MEDICINE the UNC CECIL G. SHEPS CENTER FOR HEALTH
SERVICES RESEARCH ACCESSEAST and FOUR COUNTY COMMUNITY CARE PARTNERS
to develop Community Care of North Carolina for Uninsured Parents (CCNC-UP), a limited benefit plan that is being piloted in Warren, Pitt and Greene Counties and providing low-income, uninsured parents with access to basic health care coverage. 30

HEALTHNET AND CCNC-UP
ORHCC administering North Carolina’s State Health Access Program (SHAP) grant, $4.5 million over 3 years, from the US DHHS Health Resources and Services Administration (HRSA) to develop CCNC-UP.
Like HealthNet: CCNC-UP built upon CCNC’s primary care medical
home model and administrative infrastructure. CCNC-UP provides enrollees (low-income, uninsured
parents) with a primary care medical home and emphasizes prevention and chronic disease management.
31

HEALTHNET AND CCNC-UP
In August 2011, ORHCC authorized to reallocate $2.8 million in SHAP funds to undertake 10 new projects providing health care for thousands of uninsured North Carolinians and help prepare the state for implementing the Affordable Care Act: $400K to maintain “Healthy & Ready to
Learn” CHIPRA Outreach and Enrollment Program for pre-school and elementary school children.
$375K emergency fund to cover co-pays for 5000 uninsured patients.
$700K to support NC’s “Medical Access Plan” and provide an additional 10,000 office visits for uninsured patients at rural health centers.
32

HEALTHNET AND CCNC-UP
$100K to create “Dental Access Plan” Pilot for the uninsured in partnership with ECU School of Dental Medicine.
$180K to create “Behavioral Health Access Plan” Pilot for the uninsured.
$25K for “Health Matters in the Community,” a new OPEN/net television series to inform the public about community health issues, health reform, and the concerns of uninsured / underserved individuals and safety net organizations.
More information at:http://www.ncdhhs.gov/orhcc/services/ccnc_up.htm 33

HEALTHNET PARTNERING WITH NC FARM BUREAU:
“HEALTHY LIVING FOR A LIFETIME” INITIATIVE
Mission: To provide Rural North Carolinians with the benefits of living a healthier lifestyle by providing free professional health screenings, educational materials and resources designed to encourage a commitment to healthy living.
34

HEALTHNET PARTNERING WITH NC FARM BUREAU:
“HEALTHY LIVING FOR A LIFETIME” INITIATIVE
Mobile Health Screening Unit 25 screening events per year will be conducted
using a 50-foot custom built mobile health screening unit
Self-contained, eco-friendly screening facility provides four screening stations, a specialty room for vascular ultrasound and a 1,000 sq. ft. fully enclosable awning
Health screenings offered at each event customized for local needs: Blood Pressure, Total Cholesterol, Glucose, Bone Density, Body Mass Index, Vascular Ultrasound
More information at:http://www.healthylivingforalifetime.com/
35

“Rural Hope” Initiative
ORHCC AND HEALTHNET PARTNERING WITH:
NC RURAL ECONOMIC DEVELOPMENT CENTER THE GOLDEN LEAF FOUNDATION KATE B REYNOLDS CHARITABLE TRUST APPALACHIAN REGIONAL COMMISSION USDA RURAL DEVELOPMENTMore information at:http://www.ncruralcenter.org/community-programs/rural-hope.html
36

HEALTHNET PARTNERING WITH CARE SHARE HEALTH ALLIANCE
ORHCC participates as a board member of the Care Share Health Alliance, a statewide organization whose mission is to improve the health of low-income, uninsured North Carolinians by supporting local collaborative networks of care.
37

QUESTIONS ABOUT HEALTHNET?
ANNE BRASWELL HEALTHNET PROGRAM DIRECTOR NC OFFICE OF RURAL HEALTH & COMMUNITY CARE 919-733-2040 [email protected]
38





























