Embed Size (px)
Citation preview

CASE REPORT
“My Bones Hurt”: An Unusual Cause of Fibromyalgia Syndrome
Nicola Tugnet1 and Richard Williams2
1Department of Rheumatology, The Royal Wolverhampton Hospitals NHS Trust, New Cross Hospital, Wednesfield Road,Wolverhampton WV10 0QP, UK, 2Department of Rheumatology, Wye Valley NHS Trust, County Hospital, Union Walk,
Hereford HR1 2ER, UK
ABackground: Fibromyalgia syndrome [FMS] is a common condition within general practice and rheumatology.Findings: We describe the case of a young man presenting with classic FMS symptoms and normal laboratory investi-gations, but whose pain was eventually found to be due to multiple bony hemangiomatosis, which led to a review of theliterature and alterations to our practice.Conclusions: FMS is a diagnosis of exclusion, and sinister causes of chronic pain must be excluded. Clinicians must havea high index of suspicion in young patients presenting with FMS, particularly young males. Plain radiographs are useful toexclude bony lesions that may be the cause of the pain.
K: Hemangioma, chronic pain, primary bone hemangioma, fibromyalgia syndrome
CASE REPORT
A 35-year-old man presented to rheumatology with atwo-year history of chronic widespread body pain,fatigue, headaches, and associated sleep disturbance.The patient described constant pain throughout hisback, torso, and all four limbs, but especially wheneverhe turned over in his sleep, and therefore slept onlythree to four hours per night. He felt tired all the timeand low in mood. Systemic enquiry was not suggestiveof an underlying inflammatory or neoplastic process,and there was no significant family history. Physicalexamination, including a general neurological examin-ation, was unremarkable except for multiple tendermuscular trigger points all over the patient’s body.There was no evidence of bony tenderness or synovitisto suggest inflammatory arthritis. The patient wasnoted to have a low affect. Laboratory investigationswere normal, including calcium, alkaline phosphatase,thyroid function, C-reactive protein, parathyroidhormone, hemoglobin, and antinuclear antibody. Adiagnosis of primary fibromyalgia syndrome [FMS]was made and the patient was started on low dose ami-triptyline, in accordance with established guidance on
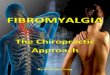
management of FMS (1), and referred to an educationalpain management program. While receiving treatmenthe had an emergency admission with seizures, and sub-sequent imaging unexpectedly demonstrated bilateralcranial hemangiomas [Figure 1]. Plain radiographyalso revealed multiple lesions with abnormal bonetexture throughout the spine, ribs, andpelvis, suggestingmultiple bony hemangiomatosis.
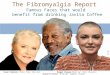
A hemangioma is a neoplasm arising from bloodvessels. Although skin is the most common site, anyorgan including the bone can be affected (2). Approxi-mately 0.2 percent of all bone tumors and 10 percent ofbenign skull tumors are due to primary hemangiomas(3). Multiple bony hemangiomatosis refers to theprocess of multiple hemangiomas occurring in asingle individual. It is an uncommon condition withonly a handful of cases described in the literature. Aprimary hemangioma in the skull or the pelvis has ahoneycomb-like appearance created by delicateosseous striae, and if these striations extend from thecenter of the lesion, the classic “sunburst” appearanceresults (4), as seen in the patient [Figure 2]. A primaryhemangioma of the bone is often an incidental finding
Address correspondence to: Nicola Tugnet, Department of Rheumatology, The Royal Wolverhampton Hospitals NHS Trust,New Cross Hospital, Wednesfield Road, Wolverhampton WV10 0QP, UK. E-mail: [email protected]
Submitted: September 12, 2011; Revisions Accepted: April 23, 2012
Journal of Musculoskeletal Pain, Vol. 20(3), 2012© 2012 Informa Healthcare USA, Inc.ISSN: 1058-2452 print / 1540-7012 onlineDOI: 10.3109/10582452.2012.704140
J M
usco
skel
etal
Pai
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
03/1
7/13
For
pers
onal
use
onl
y.

on routine radiography and does not usually causeclinical problems (4). However, there are cases of ver-tebral hemangiomas causing spinal cord compression(5) and cervical myelopathy (6). Treatment of multiplebony hemangiomatosis is largely anecdotal. Total sur-gical excision is used when the patient has significantsymptoms and the prognosis after complete excisionis excellent. Radiation has been used to treat heman-giomas and can stop tumor expansion, but does notreduce the size of the tumor (7). Chemotherapy and/or bisphosphonates have been used with variablesuccess (8). Sclerotherapy with liquid denaturingagents, such as ethanol, is an alternative to surgicalexcision (9).
FMS is postulated to be the result of central nervoussystem malfunction, resulting in pain amplification.
Various external stimuli such as infection, trauma,and stress may contribute to the development of thesyndrome (10). FMS and chronic pain syndromes arecommon conditions and have a prevalence of almostsix percent (11) and 19 percent (12), respectively.Patients present with a constellation of symptoms,including headache, cognitive impairment, sleep dis-turbance, and chronic widespread pain. Due to thevariety of symptoms, many different specialists,including rheumatologists, neurologists, pain special-ists, and general practitioners may be involved withtheir care. The diagnosis of FMS appears to be adynamic process that requires the intervention andcollaboration of these specialists. FMS is much moreprevalent in women than men and is often secondaryto an inflammatory condition, such as rheumatoid
F 1. Computerized tomography scan showing bilateral large cranial hemangiomas.
F 2. Skull radiograph demonstrating “sunburst appearance” of cranial hemangioma.
Unusual Cause of Fibromyalgia Syndrome
J M
usco
skel
etal
Pai
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
03/1
7/13
For
pers
onal
use
onl
y.

arthritis (10). It is primarily a clinical diagnosis madeafter the exclusion of other inflammatory, metabolic,or malignant causes of musculoskeletal pain. Despitethis, FMS remains undiagnosed in an estimated 75percent of people with the disorder (13). The provi-sional 2010 American College of Rheumatology diag-nostic criteria (14) specifically state that the patientmust not have a disorder that would otherwiseexplain their pain. Neurological examination canhelp detect underlying pathology that may be contri-buting to the FMS, which is important given thatFMS patients have more neurological signs and symp-toms than healthy patients (15). FMS is often second-ary to other intensely painful conditions; thus, a carefulhistory and examination can point to a painful periph-eral or central pathology that is separate, but founda-tional, for the development of FMS.
The patient was treated with antiepileptic medi-cation and the cranial lesions were surgically resected,which lead to the resolution of his headaches. Hismusculoskeletal body pain continued, so bisphospho-nate therapy was implemented. This lead to reducedintensity of pain, allowing a functional increase inactivities of daily living. In this case, the abnormalbone texture could have been detected on plain radi-ography of either the chest or lumbar spine, and thismay have prevented an emergency admission. Wetherefore suggest plain radiographs of the mostpainful area described by young patients presentingwith FMS to detect bony lesions that may be theroot of the pain. The risks associated with radiationexposure must, of course, be balanced with clinicalneed, as it would be inappropriate to perform radio-graphs of all painful areas, particularly when FMSpatients present with diffuse pain.
Multiple bony hemangiomatosis can cause diffusepain and tenderness and, if cranial lesions are present,may be a cause of headache. This should be borne inmind by clinicians during the assessment of youngpatients with chronic pain, particularly males. Ahigh index of suspicion is necessary in this particularsubgroup of patients, as they may be less likely to haveFMS.
Declaration of Interests: None.
REFERENCES
1. Carville SF, Arendt-Nielsen S, Bliddal H, Blotman F, Branco JC,Buskila D, Da Silva JA, Danneskiold-Samsøe B, Dincer F, Hen-riksson C, Henriksson KG, Kosek E, Longley K, McCarthy GM,Perrot S, Puszczewicz M, Sarzi-Puttini P, Silman A, Späth M,Choy EH; EULAR: EULAR evidence-based recommendationsfor the management of fibromyalgia syndrome. Ann RheumDis 67: 536–541, 2008.
2. Okumura T, Asamura H, Kondo H, Matsuno Y, Tsuchiya R:Hemangioma of the rib: a case report. Jpn J Clin Oncol 30(8):354–357, 2000.
3. Liu JK, Burger PC, Harnsberger HR, Couldwell WT: Primaryintraosseous skull base cavernous hemangioma: case report.Skull Base 13: 219–228, 2003.
4. Karlin CA, Brower AC: Multiple primary hemangiomas of bone.Am J Roentgenol 129: 162–164, 1977.
5. Vinay S, Khan SK, Braybrooke JR: Lumbar vertebral haeman-gioma causing pathological fracture, epidural haemorrhage,and cord compression: a case report and review of literature.J Spinal Cord Med 34(3): 335–339, 2011.
6. Tamura T, Sakai T, Sairyo K, Takao S, Kagawa S, Katoh S, YasuiN: Hematoma in the cervical ligamentum flavum. Report of acase and review of the literature. Skeletal Radiol 39(3):289–293, 2010.
7. Shibata S, Mori K: Effect of radiation therapy on extracerebralcavernous hemangioma in the middle fossa: report of threecases. J Neurosurg 67: 912–922, 1987.
8. Coppo P, Lassoued S, Billey T, Lassoued K: Successful treatmentof osteolytic epithelioid hemangioendothelioma with pamidro-nate. Clin Exp Rheumatol 23(3): 400–401, 2005.
9. Crawford EA, Slotcavage RL, King JJ: Ethanol sclerotherapyreduces pain in symptomatic musculoskeletal hemangiomas.Clin Orthop Relat Res 467: 2955–2961, 2009.
10. Buskila D: Developments in the scientific and clinical under-standing of fibromyalgia. Arthritis Res Ther 11(5): 242, 2009.
11. Hauser W, Bernardy K, Uceyler N, Sommer C: Treatment offibromyalgia syndrome with antidepressants: a meta-analysis.JAMA 301(2): 198–209, 2009.
12. Reid KJ, Harker J, Bala MM, Truyers C, Kellen E, Bekkering GE,Kleijnen J: Epidemiology of chronic non-cancer pain in Europe:narrative review of prevalence, pain treatments and pain impact.Curr Med Res Opin 27(2): 449–462, 2011.
13. Clauw DJ, Arnold LM, McCarberg BH: The science of fibro-myalgia. Mayo Clin Proc 86(9): 907–911, 2011.
14. Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Katz RS,Mease P, Russell AS, Russell IJ, Winfield JB, Yunus MB: TheAmerican College of Rheumatology preliminary diagnostic cri-teria for fibromyalgia and measurement of symptom severity.Arthritis Care Res 62(5): 600–610, 2010.
15. Watson NF, Buchwald D, Goldberg J, Noonan C, EllenbogenRG: Neurological signs and symptoms in fibromyalgia. ArthritisRheum 60(9): 2839–2844, 2009.
Tugnet and Williams
J M
usco
skel
etal
Pai
n D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Lib
rary
Utr
echt
on
03/1
7/13
For
pers
onal
use
onl
y.