Embed Size (px)
Citation preview

Musculoskeletal Imaging and Bone Trauma
Edward Smitaman, MD
Clinical Assistant Professor
University of California, San Diego

Case #1
• Right hip pain, after motor vehicle accident


Fracture types

Fracture Characterization
• What you really need to notice– Alignment: Needs Reduction– Open (compound) fracture?- Needs surgery– Intra-articular Extension?
• Articular Gap/Depression
– Common associated injuries• Fracture patterns• Associated ligamentous soft tissue injury

Common Fracturesand
Fractures Associations that are Helpful to Know

Case # 2
• 22 year old male with hand pain after punching a wall


Boxer’s Fracture
• Most common type of metacarpal fracture• Must evaluate for intra-articular extension• Must evaluate for angulation and rotational
deformity- determines management• Good history/exam for soft tissue swelling can
be very helpful in picking up subtle fractures

Case # 3
• 24 year old with arm pain after fall


Monteggia Fracture
• Views of the entire forearm and elbow should be obtained to exclude this injury.
• The forearm acts like a bony ring (with ulna and radius fixed at each end by the radioulnar joints)
• A fracture of one bone is uncommon without a second fracture or dislocation of the proximal or distal radio-ulnar joints.

Galleazzi Fracture
Fracture of radiusWith dislocation of distal ulna

Case # 4
• 30 year old male with knee pain after playing soccer


Segond Fracture
• Avulsion fracture of lateral tibial plateau• High Association (>75%) with
– Anterior Cruciate Ligament tear– Medial Mensicus tear– Posterior Cruciate Ligament tear
• Order MRI to assess ligaments of knee and consult ORTHO


Case #4
• 20 year old tennis player with acute onset of ankle pain.


Maisonneuve fracture
• External rotation injury to ankle results in– Disruption of deltoid (medial) ankle ligaments– Disruption of interosseous membrane– Proximal fibular fracture as force exits laterally
• Always image entire tibia/fibula if concerned about ankle syndesmosis

Case #5
• Cassanova is now complaining of back pain


Comminuted Calcaneal Fracture (Cassanova’s Fracture)
• Axial Loading injury• Bones/joints often injuried in axial loading
– Calcaneus– Distal Tibia– Knee Joint (Proximal Tibia/Distal Femur)– Acetabulum/Proximal Femur– Lumbar / Lower thoracic spine

Anatomy

Case #6
• 24 year old male with hand pain after skiing.


Gamekeeper’s Fracture
• Avulsion fracture at insertion of ulnar colateral ligament
• Often managed conservatively (unless fracture fragment is very displaced
• Do NOT obtain stress views– Can convert this lesion into a Stenner lesion-
where adductor apponeurosis gets in the way of the UCL and prevents healing.
• IF DX in question get MRI

Findings Associated with Fractures that are Helpful to Know

Case # 7
• Elbow pain


Elbow Joint Effusion
• Highly associated with boney injury– In adults: Radial head fracture– In children: Supracondylar fracture
• May not always see fracture on initial radiographs, delayed films, CT or MR may be necessary


Case # 8
• Knee pain, status post bicycle accident


Knee Effusion with Lipohemarthrosis
• Joint effusion is non-specific– Trauma– Infection– Inflammatory disease
• Lipohemarthrosis (fat-fluid level)– Very specific for fracture or bone bruise– When present and a fracture is not seen
• Get CT or MR

Pediatric Bone Trauma

Pediatric Fractures• Bone anatomy is different
– Physis are still open– Bones are immature
• Results in – different fracture patterns – different treatment approaches
Epiphysis
Physis
Metaphysis
Diaphysis
Epiphysis
Physis
Metaphysis

Salter-Harris Physeal Fracture Classification
As Fracture type increases from 1 to 5, prognosis worsens.
Type I fractures will almost always heal with normal bone growth
Type V fracture will virtually always result in abnormal bone growth

Case # 9
• 12 year old male with wrist pain after trauma

Salter Harris Type II
• Most Common Physeal Fracture• Good Prognosis

Case # 10
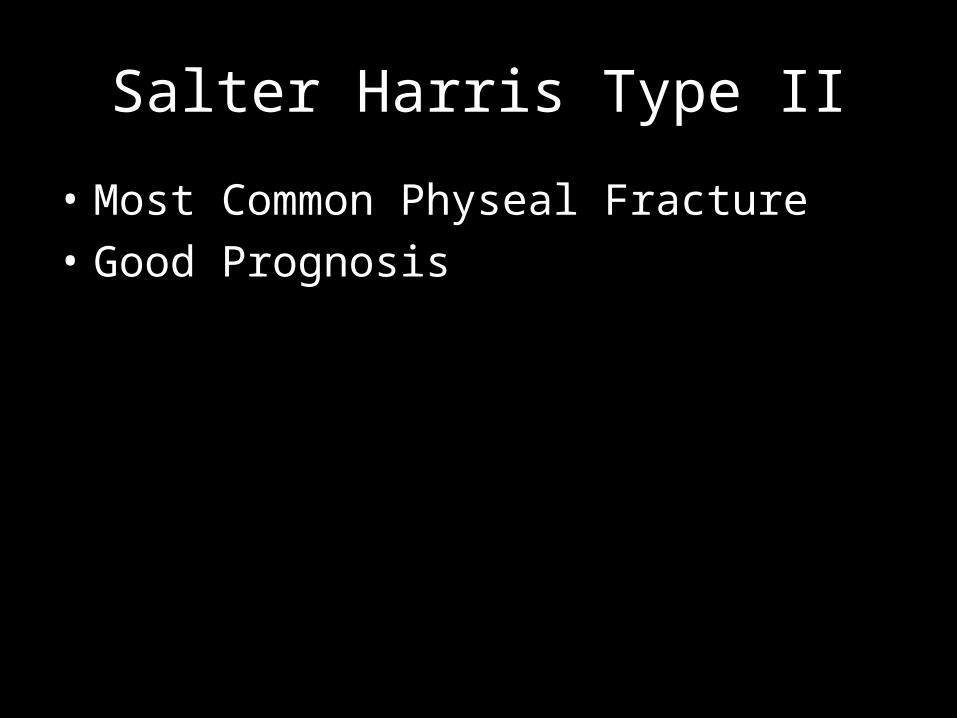
• 12 year old boy with left hip pain
Hint: Skeletal ageSlipped Capital Femoral Epiphysis

SCFE
Normal Alignment
SCFE• Salter Harris Type I fracture• Presents with:
– Limp and or pain– Pain in hip/groin ~ 85%– Distal thigh or knee pain ~ 15%
• More common in boys: average 13-14 years • Gender: M:F = 2.5:1• Predisposing factors
– Obesity is currently most significant factor – Adolescent growth spurt – Endocrine disorders: Primary hypothyroidism, pituitary dysfunction, etc. – Down syndrome
• Treatment: Surgical Pinning – To prevent further slippage and resultant premature osteoarthritis

Case # 11
• 14 year old female with wrist pain after playing softball


Buckle Fracture Distal Radius
• A.K.A.– Torus Fracture– Incomplete Fracture
• Common in children because of immature bone strength
• Treatment – Reduction if necessary (often not)– Casting (short term ~ 3-4 wks)


Case # 12
• 15 year old male with wrist pain after falling on an outstretched hand.



Scaphoid Fracture• Transverse fx; 70% middle 1/3 of the waist• Assoc with radial styloid and triquetrial fx and scapholunate
ligament injury• 2-5% not seen on XR. Splint and reimage in 7-10 days or get
MRI• Most frequent malunion is with dorsal apex angulation• 10-15% nonunion• 15-30% develop AVN of proximal pole
– Blood supply to the scaphoid is retrograde• Tx is immobilization; ORIF if unstable or delayed nonunion

Case # 13
• 40 year-old man with knee pain after MVA



Anterior Knee Dislocation
• High impact injury (60% MVA)• Hyperextension injury with tear of posterior
structures• Posterior knee dislocation-direct blow to
proximal tibia• Need to assess for injury to the popliteal
artery-CTA or conventional angiogram• MRI to assess meniscal and ligament injury

Case # 14
• 20 year old man BIBA after MVA



Pelvic Fractures
• Pelvis is a bony ring--must break in 2 places• Superior/Inferior pubic rami• Sacroiliac joints• Open Book--pubic symphysis diastasis• Acetabular Fx


Case # 16
• 48 year-old man fell off a ladder



Odontoid Fracture
• Sudden forward or backward movement of head
• XR: lucent fx line, displacement of the anterior arch of C1, prevertebral soft tissue swelling, can see fx on open mouth view
• CT: need MPRs, axial images can miss fx• Type I: avulsion of dip of dens• Type II: transverse fx at base of dens• Type III: fx extends to body of C2

Case #17
• Left foot pain status post trauma



Lisfranc Fracture-Dislocation
• Lisfranc ligament - from anterolateral aspect of the medial cuneiform to the medial base of the 2nd MT
• Offset TMT joints• Gap at the bases of the 1st and 2nd MTs


Case # 18
• 3 year old male with acute onset of leg pain while running.