Embed Size (px)
Citation preview

Muscle relaxants and antagonists
in children
Lonneke Staals Erasmus MC- Sophia Children’s Hospital
Rotterdam

Conflicts of interest
MSD (formerly Organon NV)
financed research on sugammadex (PhD project).

Muscle relaxation in children
NMBA’s in children
PORC in children: is it a problem?
If you use muscle relaxation: monitor!
Do we really need to relax children?
Intubation: RSI
Working space
Reversal of NMB in children

E. Crins ©

Function of
Neuromuscular
Junction
Permeability of BBB
Plasma Protein Binding
Hepatic
function Renal
clearance
Volume of distribution

Volume of distribution

NMBAs in children
Depolarizing NMBA (succinylcholine):
Larger volume of distribution > lower concentration at NMJ
Higher dose is needed
Non-depolarizing NMBAs:
Larger volume of distribution > lower concentration at NMJ
Immature NMJ in neonates > less ACh release
Lower hepatic clearance in neonate
Shorter onset time
Longer duration of action Allegaert K, Pediatric Anesthesia 2014; 24: 30-38

PORC / residual NMB
Single intubating dose of NMBA
On recovery ward:
45% TOF ratio < 90%
After 2 hours:
37% TOF ratio < 90%
Debaene Anesthesiology 2003; 98:
1043-8

Higher risk on PORC
Renal insufficiency
Aminoglycoside antibiotics
Erythromycin
Gentamycin
In combination with steroids on the ICU
Premature children
Higher sensitivity of NMJ for non-depolarising NMBAs
Immature liver

PORC in children?
Observational study, for 1 month
TOF measured before extubation (and reported to anesthetist)
Choice up to anesthetist to antagonize or not
Postop to PACU: adverse events were noted
64 children, mean age 8.2 years; 35,1 kg Atracurium (41/ 10 continuous); Rocuronium (15, 2 continuous), Succinylcholine (6),
Vecuronium (1 continuous), Mivacurium (1 continuous)
Ledowski, Anesthesiology Research and Practice 2015

PORC in children?
23,4% routine TOF measurements during procedure
51,6% children antagonized with neostigmine (1 sugammadex)
TOF ratio < 90%: 28,1% After neostigmine: 37,5%
TOF ratio < 70%: 6,5% (2 patients) 1 x neostigmine; 1 no reversal
NO anesthetist changed his mind! TOF < 90% in 7 children, of which 2 < 70%
Few incidents on PACU (no difference)

PORC in children?
Higher incidence after administration of neostigmine: 37,5%
Deep NMB cannot be reversed by neostigmine
Long and variable onset time of neostigmine
False sense of safety!
Few anesthetists measure quantitative TOF routinely
No awareness for possible complications of PORC

Is PORC a problem?
Case control study
7500 Recovery patients, for 1 year
61 (0.8%) respiratory incidents on recovery ward Upper airway obstruction
Hypoxemia
Signs of respiratory distress
Inability to breath deeply
Complaints of respiratory or upper airway muscle weakness
Requiring re-intubation
Pulmonary aspiration
Matched controles Murphy, Anesth Analg 2008; 107 (1): 130-7
Murphy et al. Anesth Analg 2008; 107(1): 130-7

Is PORC a problem?
Incident group: mean TOF ratio 62% (± 20)
Control group: mean TOF ratio 98% (± 7)
Incident group: 9.5% acceptable TOF ratio
Control group: 90.5% acceptable TOF ratio
31 incidents: TOF ratio < 70%
TOF < 70% in none of the controles

Is PORC a problem?
All cases and controls:
NMB was reversed standard (neostigmine and glycopyrrolate)
Peripheral nerve stimulator with TOF was used!
Quantitative neuromuscular monitoring was not used

Monitoring NMB
Variability of duration of action NMBAs
Give repeated doses instead of continuous IV
Optimum level NMB!
Vital capacity?
Lifting the head?
Quantitative AMG!

TOF measuring in children

TOF bij kinderen

TOF monitors

Do we need muscle relaxation in children?
Intubation
Younger children?
Rapid sequence in children?
Improve surgical working conditions
Surgical working space?

Rapid sequence induction in children
Classic RSI:
Preoxygenation with 100% oxygen
No inflation of the lungs until ETT is placed
Application of cricoid pressure
Depolarizing NMBA (succinylcholine)
Apneic period of ± 60 sec
Intention to increase safety of patients considered at risk of
pulmonary aspiration of gastric content

Rapid sequence induction in children
Classic RSI:
Preoxygenation with 100% oxygen
No inflation of the lungs until ETT is placed
Application of cricoid pressure
Depolarizing NMBA (succinylcholine)
Apneic period of ± 60 sec
Intention to increase safety of patients considered at risk of
pulmonary aspiration of gastric content
Hypoxemia

Rapid sequence induction in children
Classic RSI in children = higher incidence of severe hypoxemia,
bradycardia and increased difficulties with intubation
Prevent hypoxia with gentle mask ventilation, pressure-limited
(not > 10-12 cm H2O)
Choice of muscle relaxant: depolarizing NMBA is NOT mandatory Engelhardt T, Pediatric Anesthesia 2015; 25: 5-8. Neuhaus D, Pediatric Anesthesia 2013; 23: 734-40

Effect of NMBAs during anesthesia
NMB
No change in ventilation pressures during thoracoscopy
Possibly more atalectasis in the lower regions of the lungs
Improved working conditions for the surgeon
Subjective impression of surgical conditions
Duration of surgical procedure
Children?
Maracaja-Neto, Acta Anaesthesiol Scand 2009; Boon, Trials 2013; Lindekaer, J Vis Exp 2013; Hedenstierna,
Int Care Med 2005

Effect of NMB on laparoscopic working space
Animal experimental model
CT: dimensions of working space
16 female piglets, 20 kg
Propofol/ sufentanil anesthesia iv
Tracheotomy, ventilation with +5 PEEP
Stepwise abdominal CO2 insufflation: 0 – 5 – 10 – 15 mmHg
CT scan at end-expiratory hold

NMBA and reversal
TOF monitoring (quadriceps femoris)
Rocuronium 1.4 mg/kg bolus, continuous 4 mg/kg/h
Group A:
no NMB during run 1 and 2
NMB during run 3
Reversal (sugammadex) before run 4
Group B:
NMB during run 1 and 2
Reversal (sugammadex) before run 3


Results
Vlot J, et al. Surg Endosc 2015; 29(8): 2210-6

Smaller animals
3 weeks old, female piglets, 6 kg
Endotracheal intubation
0-3-5-6-8-10-15 mmHg
Group A: no NMB
Group B: rocuronium
Vlot J et al, J Pediatr Surg. 2015; 50(3): 465-71

Results
NMB: no significant effect on laparoscopic working space
Also no effect on mean volume insufflated CO2 in ml
Prestretching of the abdominal wall: greater effect
Deep NMB?
PTC versus TOF ratio?
How to measure this in young children???

Reversal?
Acetylcholinesterase inhibitors
Neostigmine, edrophonium, pyridostigmine
ACh concentration increases in the NMJ: competition
Ceiling effect: residual NMB may be present
Slow onset of action: 7 – 13 minutes
Not effective in deep NMB
Adverse effects
Combination with atropine

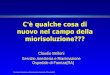
Sugammadex
Modified g-cyclodextrin
Encapsulation of aminosteroids
Rocuronium >> vecuronium > pancuronium

Recovery TOF ratio
Sugammadex
0 1 uur
0 1 uur

Sugammadex in children
ASA 1-2; 28 days old – 65 years
91 patients: Infants: 28 days – 23 months n=8 !
Children: 2 – 11 year n=24
Adolescents: 12-17 year n=31
Adults: 18-65 year n=28
Rocuronium 0.6 mg/kg iv
Sugammadex at reappearance of the 2nd twitch of the TOF:
0.5, 1.0, 2.0, 4.0 mg/kg or placebo iv
Plaud et al. Anesthesiology 2009; 110: 284-94

Sugammadex bij kinderen

Dose-response curve
Children n=22

Pharmacokinetics

Sugmmadex vs neostigmine in children
3 prospective trials, in total 180 children
Reversal with sugammadex 2 or 4 mg/kg vs neostigmine 40 or 60 mcg/kg
Shorter reversal time and
tracheal extubation times Tobias JD, Ped Anesthesia 2017
Reversal of rocuronium with sugammadex 2 mg/kg or •neostigmine 50 mg/kg in children Meretoja O, Pediatric Anesthesia 2010; 20: 591-604

Sugammadex in children
Dexamethason causes inhibition of sugammadex reversal in vitro: capturing / displacement interaction
Unclear which dose of dexamethason is required to inhibit reversal in humans
Dexamethason: 0,5 mg/kg IV: does not affect reversal time of sugammadex in pediatric patients undergoing (A)TE:
60 ASA I-II children 3-8 years old
97,7 sec (±23,9 sec) +dex vs 91,1 sec (±39,5 sec) in placebo group
Gulec E. Anesth Analg 2016; 122: 1147-52

Sugammadex in neonates
Case reports
Rocuronium may cross BBB if function is impaired
centrally acting NMBA: autonomic dysfunction, seizures, neuronal cell death
2 day old infant (3,3 kg) on PICU with esophageal atresia. Rocuronium infusion during repair.
Postop PORC and hypotonic, dilated pupils, possibly central accumulated rocuronium.
Sugammadex 16 mg/kg IV: 90 sec reversal. Pupils became reactive.
Cohort of 23 neonates (1-7 days old)
4 mg/kg sugammadex to reverse profound NMB: 1,2-1,3 min
No adverse events or changes in vital signs Langley RJ, Ped Anesth 2016; 26: 109-111. Alonso A, Eur J Anaesthesiol 2014; 31:163-5

Sugammadex in children
Limited data: few prospective trials
Neonates may need a higer dose: 4 mg/kg
No significant adverse effects were noted
No association with anaphylaxis in children
Toxicity / Long term?
Advice of Pediatric formulary in the Netherlands
1 month – 18 year: 2 mg/kg single dose
In emergency situations: higher dose (up to 16 mg/kg)
Tobias JD, Pediatric Anesthesia 2017; 27: 118-25; Tadokoro F, Pediatric Anesthesia 2018; 28: 654-9

Neuromuscular block in children
NMBAs in children:
Prolonged duration of action of non- depolarizing NMBAs
PORC and children: Underrecognized problem
Should we relax?
Not necessarily!
Modified RSI in children: no depolarizing NMBA needed
And if you relax….Use quantitative NMB monitoring
Sugammadex in children As effective as in adults