Embed Size (px)
Citation preview

“Muscle – not just for athletes!” Muscle mass, disability & quality
of life.
Dr. Andrew LemmeySchool of Sport, Health and Exercise Sciences
Bangor University, UK

Determinants of Muscle Atrophy:
Loss of Muscle Fibers
→
Reduction of Muscle Fibers Size
→

Pathophysiology of muscle loss secondary to aging
Lexell et al. (1988)
Tomlinson and Irving (1977)

Cachexia / sarcopenia is associated with poor
outcome

Consequences of Sarcopenia: Mortality(Kotler et al., 1989)

Muscle Atrophy and Mortality
Kato et al. (2003)

Muscle Atrophy at Admission and Length of Stay in Hospital
Pichard et al. (2004)
Low
FFM
I
Norm
al FFM
IH
igh
FFMI

Consequences of Sarcopenia: Disability(Baumgartner, 2000)

Muscle Mass and Strength in RA
arms lean mass, g
100008000600040002000
gri
p s
tre
ng
th,
kg
60
50
40
30
20
10
0
group allocation
healthy
RA
relative legs lean mass, %
282624222018161412
SS
T-3
0,
rep
s
30
20
10
0
group allocation
healthy
RA
Healthy r = 0.94, p < 0.001
RA r = 0.73, p < 0.001
Healthy r = 0.59, p < 0.01
RA r = 0.40, p = 0.07

0
20
40
60
0 10 20 30
Leg lean mass (kg)
KE
S (
N)
Controls
Patients
Fig. 3. Bivariate linear regression analysis between body composition data and measures of
functional capacity. KES, Knee extensor strength. Analysis is based on pooled data for patients
and controls. r, Pearson correlation coefficient. *, p < 0.005.
r = 0.832

0
510
1520
25
0 5 10 15
AMMI (kg/m2)
30se
c SS
T Controls
Patients
Fig. 2. Bivariate linear regression analysis between body composition data and measures
of functional capacity. 30sec SST, 30 second sit to stand chair test. Analysis is based on
pooled data for patients and controls. r, Pearson correlation coefficient. *, p < 0.005.
r = 0.615

• The identification of effective means of treating sarcopenia/cachexia (muscle wasting) is very important since increasing muscle mass in individuals with muscle wasting has the potential to decrease disability and morbidity, increase life expectancy, and improve quality of life in these patients

Peak Muscle Mass
GeneticMakeup
Nutrition
PhysicalActivity
Gender
Sarcopenia→

Muscle Loss Secondary to Disuse(SHUTTLE and MIR missions of 16-28 weeks duration)
Le Blanc et al. (2000)
Preflight Postflight Δ Δ% P
BMC (kg)
2.95 2.85 -0.10 -3.4 <0.01
Fat (kg) 15.04 15.54 +0.50 +3.3 NS
LBM (kg) 59.42 57.32 -2.10 -3.5 <0.001
Total (kg)
77.42 75.11 -1.71 -2.2 <0.02
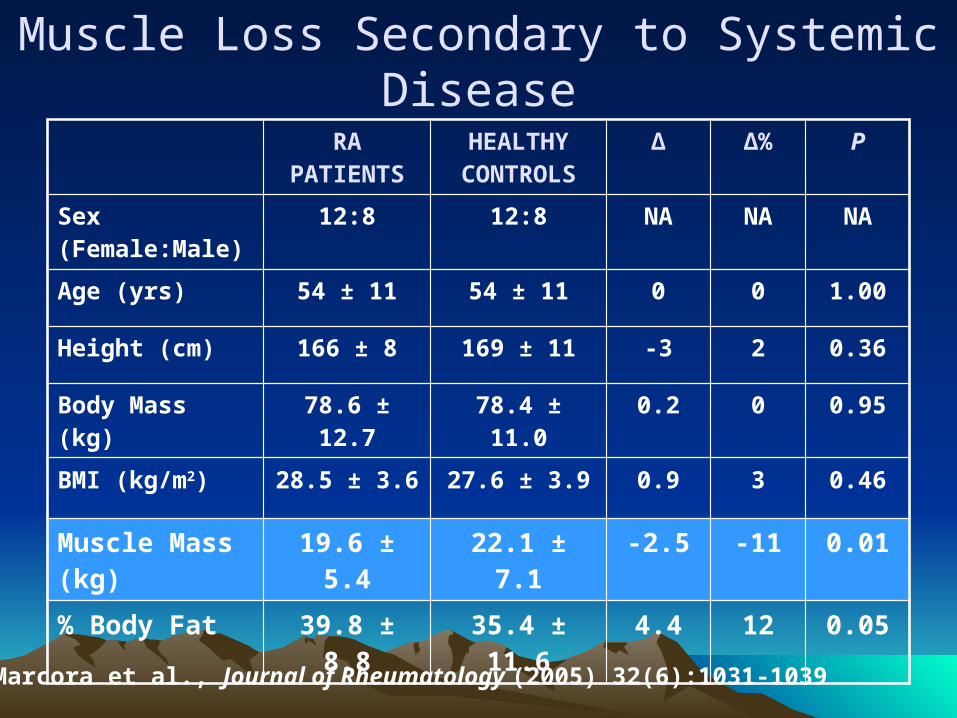
Muscle Loss Secondary to Systemic Disease
RA PATIENTS
HEALTHY CONTROLS
Δ Δ% P
Sex (Female:Male)
12:8 12:8 NA NA NA
Age (yrs) 54 ± 11 54 ± 11 0 0 1.00
Height (cm) 166 ± 8 169 ± 11 -3 2 0.36
Body Mass (kg) 78.6 ± 12.7 78.4 ± 11.0 0.2 0 0.95
BMI (kg/m2) 28.5 ± 3.6 27.6 ± 3.9 0.9 3 0.46
Muscle Mass (kg)
19.6 ± 5.4 22.1 ± 7.1 -2.5 -11 0.01
% Body Fat 39.8 ± 8.8 35.4 ± 11.6 4.4 12 0.05
Marcora et al., Journal of Rheumatology (2005) 32(6):1031-1039

Standard medical treatment does not completely prevent
cachexia

Muscle Loss Secondary to Drug Therapy(Androgen Deprivation Therapy in Prostate Cancer Patients)
Smith et al. (2001)
Baseline 1 Month 3 Months P
Testosterone (nmol/l)
14.5 ± 4.1 0.9 ± 0.4 1.2 ± 1.0 < 0.0001
Fat Mass (kg) 20.2 ± 9.4 22.5 ± 10.5 21.9 ± 9.6 < 0.01
LBM (kg) 63.2 ± 6.8 62.3 ± 5.4 61.5 ± 6.0 < 0.05
Body Mass (kg) 83 ± 14 85 ± 14 83 ± 14 NS

Muscle Protein Metabolism inHealth and Disease
-7.5
-5
-2.5
0
2.5
5
7.5
10
12.5
Young PRT Old Acute Chronic
AnabolismCatabolismNet

Standard drug therapy, including anti-TNF therapy, neither completely prevents muscle wasting, nor restores muscle mass
Consequently, there is a need for anabolic therapy in treating patients with cachexia

Anabolic Therapies
Progressive resistance training (PRT)
Dietary supplements
Anabolic hormones

Progressive Resistance Training

Can progressive resistance training reverse rheumatoid cachexia? A Phase II Trial
Characteristic RA Patients(n = 20)
Healthy Controls(n = 20) Δ P
Age, yrs 54 ± 11 54 ± 11 NA NA
Sex (Female:Male) 12:8 12:8 NA NA
Disease Duration, yrs 8.1 ± 5.4 NA NA NA
RADAI, 0-10 2.6 ± 1.5 NA NA NA
Height, cm 166 ± 8 169 ± 11 -2% 0.36
Body Mass, kg 78.6 ± 12.7 78.4 ± 11.0 0% 0.95
BMI, kg/m2 28.5 ± 3.6 27.6 ± 3.9 1% 0.37
Arms Lean Mass, kg 4.3 ± 1.6 4.8 ± 2.0 -11% 0.02
Legs Lean Mass, kg 13.1 ± 3.2 14.7 ± 4.3 -11% 0.01
Trunk Lean Mass, kg 23.3 ± 4.6 24.1 ± 4.9 -3% 0.46
% Body Fat 39.8 ± 8.8 35.4 ± 11.6 12% 0.05
Marcora et al. Journal of Rheumatology (2005) 32(6):1031-1039

Intense Progressive Resistance Training

Very Intense!!!

Exercise DoseVariable Rall et al. Marcora et al.
Muscle action Dynamic Dynamic
Velocity1-2 s concentric and
eccentric1-2 s concentric and
eccentric
Reps per set 8 8
Load 80% of 1-RM 80% of 1-RM
Sets per exercise 3 3
Rest periods 1-2 min 1-2 min
Number of exercisesper training session
5 8
Training frequency 2 3
Total number of lifts per week
240 576
Duration 12 weeks 12 weeks

Training Progression
6000
6500
7000
7500
8000
8500
9000
9500
10000
1 2 3 4 5 6 7 8 9 10 11 12
Week of training
Ave
rag
e tr
ain
ing
se
ssio
n lo
ad
, kg
*
* P < 0.01

Results: Body Composition
-752
1242
280
839
-1000
-500
0
500
1000
1500
Trunk FM Total LM Arms LM Legs LM
Dif
fere
nce
in g
ram
s
P = 0.08
P < 0.01 P < 0.01 P < 0.01
FM = Fat Mass; LM = Lean Mass. Significance was tested by ANCOVA on follow-up scores using baseline scores as covariate.

Objective Functional Capacity Tests
Rickli & Jones, Senior Fitness Test Manual, Human Kinetics (2001)

30sec sit-stand test (lower body strength)Leg extension (lower body strength)Dumbbell arm curls (30sec) (upper body strength)Hand grip strength (upper body strength)8’ up-and-go (agility/dynamic balance) 6 min walk (aerobic endurance)2-min step test (aerobic endurance)Chair sit-and-reach (lower body flexibility)
Rickli & Jones, Senior Fitness Test Manual, Human Kinetics (2001)

Results: Muscle Strength
Significance was tested by ANCOVA on follow-up scores using baseline scores as covariate.
0
5
10
15
20
25
30
35
40
Hand-Grip Elbow Flexors KneeExtensors
Chair Test
Pe
rce
nt
Dif
fere
nce
P = 0.04 P < 0.01
P = 0.07
P < 0.01

Significant decrease (-0.25 HAQ score) in disability (P = 0.01) by ANCOVA
r = -0.50, P = 0.03
D leg lean
200010000-1000
D a
dva
nce
d A
DL
s
.2
0.0
-.2
-.4
-.6
-.8
group allocation
control group
training group
Total Population

Can 24 wks progressive resistance training reverse cachexia in rheumatoid arthritis patients?
A RCT
CharacteristicPRT group
(n=13)ROM controls
(n=15) p
Age (yrs) 55.6 ± 8.3 60.6 ± 11.2 0.201
Gender (F/M) 11/2 12/3 0.686
Disease duration(yrs)
6.2 ± 6.3 10.4 ± 9.4 0.146
Disease activity score (DAS)
3.29 ± 1.27 3.28 ± 1.07 0.989
Postmenopausal 9 9
HRT 1 0
Lemmey et al., Arthritis & Rheum (2009) 61:1726-34

Exercise DoseVariable Lemmey et al. (2009) Marcora et al. (2005)
Muscle action Dynamic Dynamic
Velocity1-2 s concentric and
eccentric1-2 s concentric and
eccentric
Reps per set 8 8
Load 80% of 1-RM 80% of 1-RM
Sets per exercise 3 3
Rest periods 1-2 min 1-2 min
Number of exercisesper training session
8 8
Training frequency 2 3
Total number of lifts per week
384 576
Duration 24 weeks 12 weeks

Effects of 24 wks high intensity PRT on body composition in RA patients
Variable PRT group(n=13)
ROM controls(n=15)
p ή
Lean body mass (kg)prepost
37.3 ± 4.038.8 ± 4.2
40.4 ± 8.940.0 ± 8.7
0.006 0.26
Appendicular lean mass (kg)prepost
14.3 ± 1.815.5 ± 2.2
15.7 ± 4.115.5 ± 4.0
0.002 0.33
Total body protein (kg)prepost
6.40 ± 2.028.20 ± 1.84
7.66 ± 3.567.25 ± 3.93
0.004 0.28
Total fat mass (kg)prepost
27.8 ± 12.025.5 ± 10.8
31.3 ± 8.729.9 ± 10.4
0.657
Trunk fat mass (kg)prepost
14.0 ± 6.511.5 ± 5.2
16.1 ± 5.714.8 ± 6.1
0.489

Effects of 24 wks high intensity PRT on body composition in RA patients
Variable PRT group(n=13)
ROM controls(n=15)
CachecticprePost
94
77
Obeseprepost
107
1212
Cachectic-obeseprepost
52
55
Lemmey et al., Arthritis & Rheum (2009) 61:1726-34

Effects of 24 wks high intensity PRT on physical function in RA patients
0
3
6
9
12
15
PRT Cont
50 f
t w
alk
(s)
0
3
6
9
12
15
PRT Cont
50 f
t w
alk
(s)
0
100
200
300
400
500
PRT Cont
Kn
ee
ext
enso
r st
ren
gth
(N
)
0
100
200
300
400
500
PRT Cont
Kn
ee
ext
enso
r st
ren
gth
(N
)
0
5
10
15
20
25
30
PRT Cont
Arm
Cu
rls
(re
ps
)
Pre
Post
0
3
6
9
12
15
18
21
PRT Cont
30s
sit
-to
-sta
nd
(re
ps)
A B
C D
****
*
**
0
5
10
15
20
25
30
PRT Cont
Arm
Cu
rls
(re
ps
)
Pre
Post
0
3
6
9
12
15
18
21
PRT Cont
30s
sit
-to
-sta
nd
(re
ps)
0
3
6
9
12
15
PRT Cont
50 f
t w
alk
(s)
0
100
200
300
400
500
PRT Cont
Kn
ee
ext
enso
r st
ren
gth
(N
)
A B
C D
****
*
**
0
5
10
15
20
25
30
PRT Cont
Arm
Cu
rls
(re
ps
)
Pre
Post
0
3
6
9
12
15
18
21
PRT Cont
30s
sit
-to
-sta
nd
(re
ps)
A B
C D
****
*
**
0
5
10
15
20
25
30
PRT Cont
Arm
Cu
rls
(re
ps
)
Pre
Post
0
3
6
9
12
15
18
21
PRT Cont
30s
sit
-to
-sta
nd
(re
ps)
0
3
6
9
12
15
PRT Cont
50 f
t w
alk
(s)
0
100
200
300
400
500
PRT Cont
Kn
ee
ext
enso
r st
ren
gth
(N
)
A B
C D
****
*
**
* p<0.05, ** p<0.01, *** p<0.001 (group x time interaction). Line represents “healthy control” values (gender and age weighted)

Values are the mean ± SD. P values are for group x
time interaction. Effect size was calculated as eta
squared (η2), with thresholds for small, moderate,
large and very large effects set at .01, .08, .26 and
.50 respectively. Muscle IGF values (mIGF) are
for PRT group (n=9) and control group (n=5), whilst
serum IGF (sIGF) values are for PRT group (n=13)
and control group (n=15).
Lemmey et al., Arthritis & Rheum (2009) 61:1726-34

02468
10121416
IGF-І IGFBP-3
pg
/μg Controls
Patients
**
Fig. 3. Skeletal muscle IGF-І and IGFBP-3 levels (normalized for total protein
content) for 5 healthy controls and 7 HD patients. Values are mean ± SD. **, p
< 0.001 from healthy controls.
Macdonald et al., Clin Physiol Functional Imaging (2005) 25:113-18
**

Pharmacological Nutrition

Nutritional Treatment of Rheumatoid Cachexia
Number of nutrition intervention trials [either randomized controlled trials (RCTs) or observational trials (OTs)] in patients with chronic diseases (Akner and Cederholm, 2001)
Randomised Controlled Trial of Juven in RA Patients
Oral mixture of amino acids:Arginine = 14 g/dayGlutamine = 14 g/dayβ-hydroxy-β-methylbutyrate(HMB) = 3 g/day
What is Juven?
Marcora et al., Clinical Nutrition (2005) 24(3): 442-454

Randomised Controlled Trial of Juven in RA Patients
• 40 RA patients were randomly assigned to either Juven (n = 20) or “Placebo” (n = 20)
• Placebo = a nitrogen and calorie balanced mix of 11 g of alanine, 1.75 g of glutamic acid, 6.10 g of glycine, and 4.22 g of serine
• Both subjects and researchers were unaware of allocation until analysis (double blind)
• Subjects were tested at baseline and after 12 weeks of oral supplementation
• 36 subjects completed the study

Changes in Appendicular Muscle Mass
0
100
200
300
400
500
600
Juven Placebo
gra
ms
Data presented as Mean ± SEM
(Main Factor Time P < 0.05)

Randomised Controlled Trial of Juven in RA Patients
7.0
7.5
8.0
8.5
9.0
9.5
10.0
10.5
11.0
Pretest Posttest
Tot
al b
ody
prot
ein,
kg
HMB/Arg/Glut Placebo
¶#
Non significant group x time interaction; P = 0.74, η2 = 0.00
# Significant main effect for time; P = 0.02, η2 = 0.16

Changes in Lower Body Function
10
11
12
13
14
15
16
Pre Post
Sit-t
o-st
and
reps
in 3
0"
Juven
Placebo
Data presented as Mean ± SEM
(Main Factor Time P < 0.05)

Anabolic Hormones

Anabolic/Androgenic Steroids
Age group 50–59 yr RA Healthy P
n 34 23 NA
Age (yr) 55.5 55.1 NS
T (nmol/l) 14.9 (5.1) 18.6 (6.0) <0.01
SHBG (nmol/l) 32.9 (13.2) 34.7 (12.9) NS
T/SHBG 0.49 (0.2) 0.56 (0.2) <0.05
NST (nmol/l) 8.9 (2.5) 11.4 (3.0) <0.01
Percentage hypogonadal 35 9 <0.05
Tengstrand et al. (2002)

Anabolic Steroids in RA: Women (Bird et al., 1987)
• Single-blind, randomised, parallel, controlled trial• 24 female RA patients received 50 mg of nandrolone decanoate
every third week for 2 years• 23 female RA patients received only standard medical treatment• Patients assessed at month 0, 6, 12, 18, 24• Body composition by neutron activation analysis and whole-body
counting• Main focus osteoporosis, no effect• No effect on disease activity• Striking improvement in anemia• Side effects were hoarseness, slight facial hair growth and
occasionally breast enlargement

Anabolic Steroids in RA: Women (Bird et al., 1987)
800850
900950
1000
105011001150
12001250
0 6 12 18 24
Month
TBN
(g)
Nandrolone
Control
*
Equivalent to 3 kg of FFM. Body mass did not change
* P < 0.01

Johansen et al., JAMA, 1999
-4
-3
-2
-1
0
1
2
3
4
5
Lean mass Fat mass
Ch
ang
e (k
g)
Placebo
NandroloneDecanoate
6 months 6 months
*
*

Nandrolone decanoate: a dose response curve in patients with end stage renal disease
• Aims: • 1) to determine the most efficacious dose
of ND for reversing muscle loss and improving physical function in ESRD patients
• 2) to assess the role of ND in reducing osteodystrophy, anaemia and CV risk, and improving psychological parameters and QoL
• Macdonald et al., Nephron Clinical Practice (2007) 106:125-135
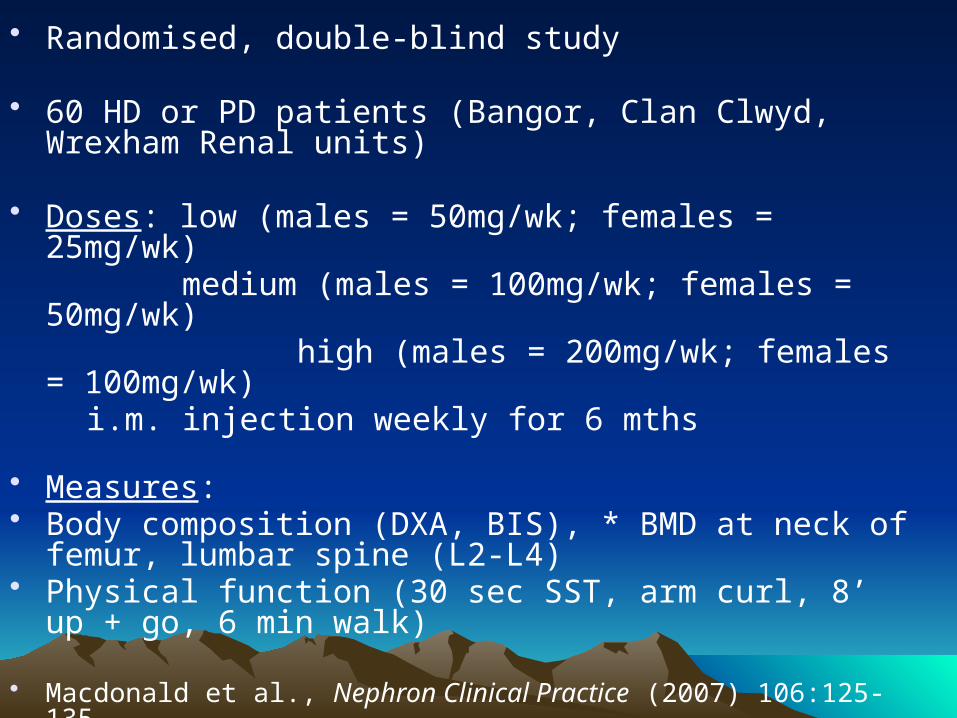
• Randomised, double-blind study
• 60 HD or PD patients (Bangor, Clan Clwyd, Wrexham Renal units)
• Doses: low (males = 50mg/wk; females = 25mg/wk) medium (males = 100mg/wk; females = 50mg/wk) high (males = 200mg/wk; females = 100mg/wk) i.m. injection weekly for 6 mths
• Measures:• Body composition (DXA, BIS), * BMD at neck of femur,
lumbar spine (L2-L4)• Physical function (30 sec SST, arm curl, 8’ up + go, 6 min
walk)
• Macdonald et al., Nephron Clinical Practice (2007) 106:125-135

• Measures (cont.)• Anaemia: Hb, Hct• Psychological: QoL (SF-36), fatigue (Bidimensional
Fatigue Scale), aggression (Aggression Questionnaire), anxiety and depression (HADS), body image (Body-Image Ideals Questionnaire)
• Safety: LFT’s, blood lipids, baseline sex hormone profile, PSA. Other possible side effects e.g. masculinisation, hirsutism, oedema, acne etc. - continuously monitored
• Study supported by N. Wales Central Research Ethics Committee and N. Wales Health and Social Care R&D Collaboration
• Macdonald et al., Nephron Clinical Practice (2007) 106:125-135

-4
-2
0
2
4
6
8
10
12
0 50 100 200
Dose (mg/week)
AL
M c
ha
ng
e s
co
re (
%) * #
ALM, appendicular lean mass; *, p < 0.01 vs.. control; #, p < 0.01 vs.. low dose group.
Dose response of nandrolone on muscle mass
Macdonald et al., Nephron Clinical Practice (2007) 106:125-135

Nandrolone decanoate as adjunct therapy in patients with rheumatoid arthritis
• Study conducted by Dr. Rao Elamanchi
• Randomised, double-blind, placebo controlled
• 40 stable male RA patients (receiving either 100mg/wk ND or placebo by fortnightly i.m. injection for 6 mths)
• In addition to measures of renal ND study, disease activity (EULAR criteria e.g. no. of swollen/tender jts, ESR, CRP) will be assessed

Summary and Conclusions i• Muscle loss is a common consequence
of ageing and RA (as it is of most chronic diseases), and a major factor in disability, and thus needs to be monitored (i.e. body composition assessment)
• Even successful pharmaceutical control of disease does not restore lost muscle mass
• Need for anabolic therapy in subjects with cachexia / sarcopenia

Summary and Conclusions ii• HI PRT is effective in reversing muscle
wasting and restoring function in the aged, RA patients, and patients with other chronic diseases
• Objective physical function tests are valuable means of evaluating physical capacity and disability, and also provide an indication of muscle mass

• Drs. Andrew Lemmey, Sam Marcora, Jeanette Thom, Jamie Macdonald; SSHES
• Prof. Peter Maddison, Dr. Jerry Jones, Rheumatology Dept., Ysbyty Gwynedd; SSHES
• Drs. Verena Matschke, Tosan Okoro, Naushad Jungalee, Ysbyty Gwynedd
• Dr. Mardi Jibani, Renal Unit, Ysbyty Gwynedd; Dr. Mick Kumwenda, Renal Unit, Ysbyty Glan Clywd
• PhD students: Sam Marcora, Jamie Macdonald, Francesco Casanova, Sally Wilson; MPhil student: Kath Chester, plus MSc and intercollated degree students (i.e. medical students)
• Prof. Nick Stuart, Oncology, Ysbyty Gwynedd
• Mr. Glynne Andrews, Orthopaedic Dept., Ysbyty Gwynedd
• Prof. Jeff Holly, Division of Surgery, University of Bristol
• Prof. Claire Stewart, Dept. of Exercise and Sport Science, MMU

Dual-Energy X-Ray Absorptiometry


Bioelectrical Impedance Analysis• BIA is based on the conductive
and non-conductive properties of various biological tissues
• Most of the body's FFM is composed of conductive tissues such as muscle, while fat is part of the non-conductive tissue mass
• The volume of these tissues can be estimated from the impedance (Z) to an applied electric current (typically, 800μA at a fixed frequency, usually 50kHz) flowing through the body
• COST - single frequency BIA: £400-2k; multifrequBIA: >£3k

Bioelectrical Impedance Analysis (ii)
• Prediction equations use impedance to estimate TBW
• LBM then calculated from an assumed hydration of lean tissue (73.2%).
FM = BM – est. LBM
• Typical SEE for TBW = 3-10%; CV for RM = 1-3%. Assuming correct procedures are observed
• Kyle et al., “Body composition measurements: interpretation finally made easy for clinical use” Curr Opin Clin Nutr Metab Care. 2003; 6(4): 387-93


Rheumatoid Arthritis• Rheumatoid arthritis (RA) is a chronic
inflammatory polyarthritis primarily affecting small joints of hands and feet
• Prevalence = 1% (women:men = 3:1)
• Despite aggressive treatments – 80% of RA patients disabled after 20 years
(Scott et al, 1987)
– 7x’s greater risk of disability (Sokka et al, 2002)
– Work disability after 10 years = 44% (Sokka et al, 1999)

• 41% variability in disability in RA unaccounted for (Escalante and Del Rincon, 2002)
• In RA – 13% lower body cell mass (BCM) (Roubenoff et al,
1994)
– Strong dose relationship between BCM and disease severity (Roubenoff et al, 1994)
– Lean body mass (LBM) = 10-15% lower (Rall et al, 1996)
• Relative muscle mass is a reliable indicator of functional limitation and disability in an ageing population (Jansen, 2002)

Rheumatoid Cachexia
• Rheumatoid cachexia is defined as:- – ‘An involuntary loss of BCM that predominates in
skeletal muscle mass and occurs with no or little weight loss in presence of stable or increasing fat mass’
– (Walsmith and Roubenoff, 2002)
• Affects 2/3 RA patients and thought to play important role in disease pathogenesis (Walsmith and Roubenoff, 2002)

Modified from Walsmith and Roubenoff (2002)
Low activity (low levels and/or resistance) of other anabolic hormones Usually normal appetite
and protein-energy intake
Therapy with corticosteroids





























