Embed Size (px)
Citation preview

MULTIPLE CESAREAN SECTIONS
THE FIRST CUT IS THE DEEPEST!!!
Carey Winkler, MD

OBJECTIVES • Review trends in cesarean secFons & TOLAC • IdenFfy some of the more common complicaFons seen with mulFple cesarean secFons
• List some of the complicaFons associated with placental implantaFon problems
• Discuss basic management of paFents with placenta accreta

OVERVIEW
• Briefly discuss a couple of things
– Placenta previa – Vasa previa – Pelvic adhesive disease – Endometriosis (?????) – InferFlity – Chronic pain – Ectopic pregnancy

BACKGROUND
• Nearly 1/3 of deliveries are via cesarean secFon
• In 2011, that was about 1.3 million procedures
• It is the most common major surgical procedure performed in the U.S
• Growing concerns (by whom??)

Number of vaginal deliveries: 2,651,428
Number of Cesarean deliveries: 1,293,267
Percent of all deliveries by Cesarean:
32.8%
NATIONAL DATA DELIVERIES 2011

BACKGROUND
• There was a gradual increase in the rate from under 20% in 1996 to over 30% in 2008
• Appears to have peaked and has been stable for the last 3 years
• Why the increase over the years?
• Why the concern?
• Can we stop it and in fact reduce the rate?


CONCERNS
• Cesarean secFons cost more • ComplicaFons higher than with vaginal delivery
• More than likely will have repeat cesarean secFons with subsequent births
• Risk of future surgery increases – Adhesive disease – Placental implantaFon problems – ……………………………………………….

COSTS
• Data from InternaFonal FederaFon of Health Plans 2012
• Total cost of – Cesarean secFon $15,041 – ConvenFonal delivery $ 9,775
• Extra cost of 1,293,267 = $ 6.9 billion • Reduce c-‐secFon rate by 40% (to 20%) – Cost savings of $2.7 billion/year




2000 N (%) 2003 N (%) 2006 N (%)
Total Deliveries 3,975,574 3,964,514 4,100,779
Total Prior Cesarean 482,913 (12.1%)
540,038 (13.6%)
596,725 (14.6%)
Elective Repeat (% Total Prior Cesarean) 285,636 (59.1%)
423,786 (78.5%)
495,151 (83.0%)
Attempted VBAC 197,276 (40.9%)
116,251 (21.5%)
101,574 (17.0%)
Successful VBAC 136,334 74,397 6,1210
% Success = Success/Attempt 69.1% 64.0% 60.3%
VBAC Rate = Success VBAC/All Priors 28.2 13.8 10.3
Method of Delivery for Women With Prior Cesareans, Nationwide Inpatient Sample, 2000, 2003, 2005

TOLAC CALCULATOR FOR SUCCESS
• h"ps://mfmu.bsc.gwu.edu
• In upper right banner, click on VBAC calculator
• Put in demographics to determine paFent’s success rate
• If success is less than 50%, not cost effecFve

SO, WHAT ARE THE BIGGEST
RISKS??

Placenta previa Placenta accreta
Pelvic adhesive disease Ectopic pregnancy
InferFlity AbrupFon
Endometriosis IUFD
Chronic pelvic pain

PLACENTAS GONE WILD!!

DEFINITIONS
• Total (complete): Completely covers the internal os
• ParFal: the internal os is parFally covered • Marginal: the placenta is at the edge of the os
• Low-‐lying: within 2 cm of the os (this definiFon is changing)
WHAT IS LOW-‐LYING?
• DefiniFon: closer than 2 cm to the internal os • Why? • Any difference? • Should be – More? – Less?

WHAT IS A LOW-‐LYING PLACENTA? Oppenheimer, et al AJOG 1991:165;1036
• 127 paFents • TVUS for placental locaFon prior to delivery • All previas delivered by c-‐secFon • No cesarean secFons for bleeding if caudal Fp > 2 cm
• 88% (7/8) emergent cesarean for previa type bleeding if < 2 cm
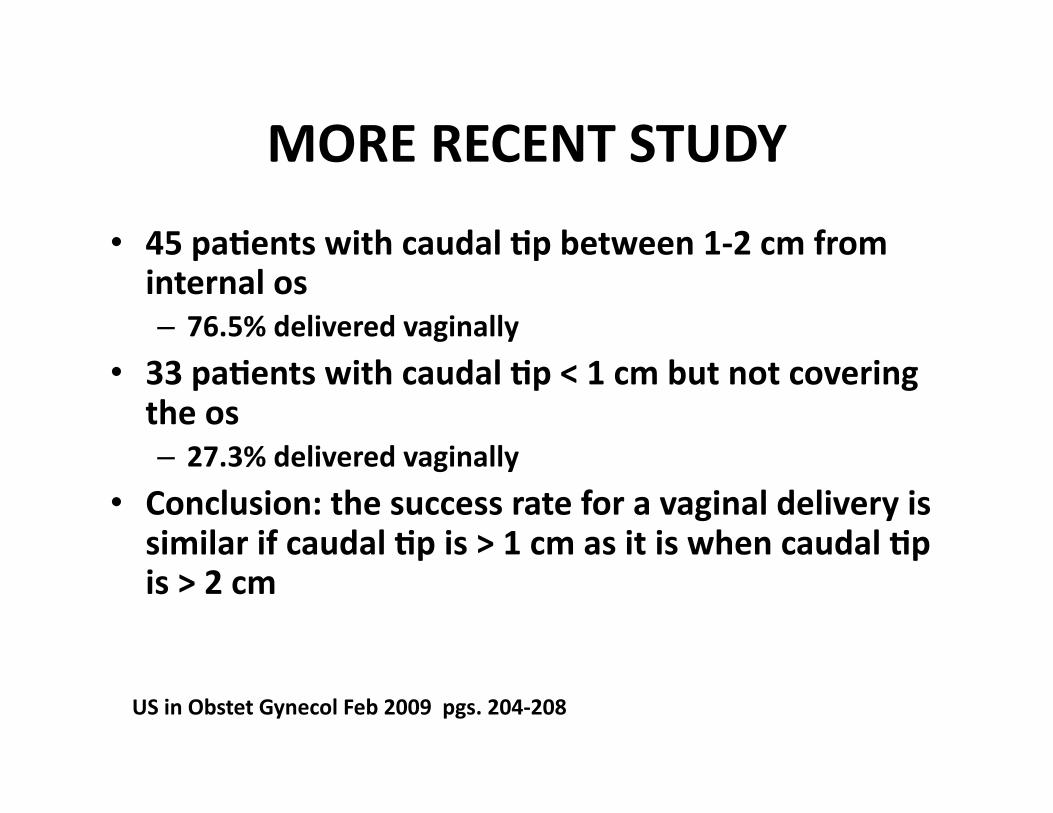
MORE RECENT STUDY
• 45 paFents with caudal Fp between 1-‐2 cm from internal os – 76.5% delivered vaginally
• 33 paFents with caudal Fp < 1 cm but not covering the os – 27.3% delivered vaginally
• Conclusion: the success rate for a vaginal delivery is similar if caudal Fp is > 1 cm as it is when caudal Fp is > 2 cm
US in Obstet Gynecol Feb 2009 pgs. 204-‐208

INCIDENCE OF PLACENTAL PREVIA
• Depends on gestaFonal age at Dx • SymptomaFc vs. asymptomaFc
• Your paFent demographics
• Approximately 5% of rouFne ultrasounds have some degree of a previa
• At term, this is approximately 0.5%
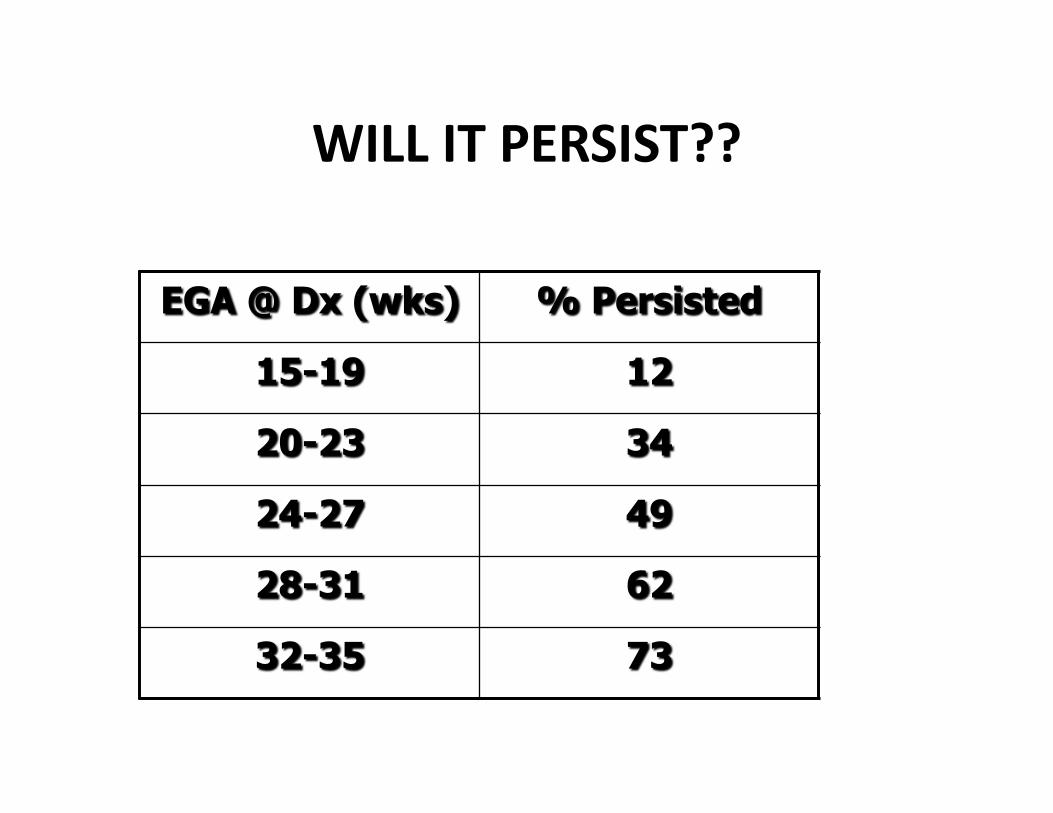
WILL IT PERSIST??

WILL IT PERSIST? PART DEUX
• Distance covering the internal os at 20-‐23 weeks
• If < 15 mm, 20% persisted unFl delivery
• If > 25 mm, approximately 50%

RISK FACTORS
Prior history 8 x Prior cesarean secFon 1.5 -‐ 15 x
MulFparity 1.1 -‐ 1.7 x
Advanced maternal age 4 -‐ 9 x
Smoking 1.4 -‐ 3.0 x
Previous sucFon curesage 1.3 x

PRESENTATION
“Painless” vaginal bleeding ContracFons in 20-‐25%
Usually symptomaFc in the 3rd trimester
Ballpark figures
1/3 iniFally present < 30 weeks
1/3 iniFally present > 36 weeks

DIAGNOSIS
• Ultrasound is the gold standard • “Double set-‐up” mostly obsolete
• Transvaginal ultrasound – SensiFvity 87% – Specificity 98% – PPV 93%
– NPV 98%

RISK OF PREVIA AND PRIOR C-‐SECTION

COMPLICATIONS
• Hemorrhage – Accreta/Increta/percreta
• Damage to adjacent organs
• Prematurity
• DEATH!!!!

PLACENTA ACCRETA

CASE
• 37 year old, G8P5025 with 4 prior c-‐secFons • US at 20 weeks: complete previa and probable accreta
• AsymptomaFc unFl 33 weeks when admised with bleeding
• Bleeding resolved and started on steroids for lung maturity

CASE
• Massive bleeding in 3 days resulFng in emergent c-‐secFon with hysterectomy
• Unable to control bleeding • Blood products – 30 units of PRBC’s – 7 units FFP – 30 packs of platelets

CASE
• ConFnued bleeding due to DIC • Abdomen packed with laps and closed • Sent to Emanuel Hospital • Trauma team, OB providers, intervenFonal radiology able to stabilize and remove packs, close abdomen

CASE
• Blood products – More than 80 units of blood products used during hospital course
• PaFent ended up doing well except had superficial wound disrupFon
• Seen at 6 week postpartum check and was without complaints

PLACENTA ACCRETA
• DefiniFon based on the degree of myometrial invasion
• Accreta: minimal invasion, < 50% • Increta: more invasion, > 50% but not through serosa
• Percreta: completely through the serosa and potenFally in to surrounding structures


US FINDINGS WITH ACCRETA
• Loss of retroplacental hypoechoic area • Progressive thinning of this hypoechoic area over Fme
• Presence of mulFple placental lakes • Thinning or focal disrupFon of the uterine serosa-‐bladder wall complex
• Focal mass-‐like elevaFon of Fssue beyond the uterine serosa

ACCRETA
• Account for over 50% of all cesarean hysterectomies
• 80% of antenatally diagnosed accreta result in hysterectomy
• Average # PRBC’s is 7 units • 40% require > 10 units PRBC’s • Consider delivery at 34-‐35 weeks • Most maternal deaths occur axer 35 wks.

ACCRETA
• MulFdisciplinary approach – obstetrician – oncologic surgeon – intervenFonal radiology – possible vascular surgery – possible urology – hematologist/pathologist for massive transfusion protocol

CAN YOU PREDICT AN ACCRETA???
• RetrospecFve study idenFfying those with discharge diagnosis of percreta (13)
• All had transabdominal US
• 9 had MRI
• Only 4 US stated accreta/percreta • MRI only idenFfied 5 of the 9
Lam, J Soc Gynecol InvesFg 2002;9:37-‐40

CAN YOU PREDICT AN ACCRETA???
Conclusion: Both MRI and US had poor predicFve value in the diagnosis of placenta accreta and further refinement in the techniques of both MRI and US is needed for these tests to be used to reliably diagnose these pathologic condiFons.

ACCRETA INTERVENTIONAL RADS
• Well proven to be able to stop catastrophic pelvic hemorrhage
• Used in – Trauma – Postpartum hemorrhage
– PostoperaFve bleeding • Pre-‐empFve??

ACCRETA INTERVENTIONAL RADS
• Mostly case reports and small series • SuggesFon of less blood with with pre-‐operaFve placement of balloons
• Usually placed in the uterine artery or the anterior branch of the internal iliac
• EmbolizaFon may or may not be done based on intraoperaFve bleeding

ACCRETA INTERVENTIONAL RADS
• Only 1 prospecFve cohort study done • 5 paFents in each group – Standard intraoperaFve management
– PreoperaFve balloon placement
• No difference seen in – Mean blood loss
– # of units of PRBC’s transfused

ACCRETA INTERVENTIONAL RADS
• My feelings – The risk to mom with balloon placements is very low
– Bleeding can be quick and catastrophic – If high suspicion of a percreta, strongly consider consult with IR
– Could use for embolizaFon if postoperaFve bleeding

DOES ANTENATAL DIAGNOSIS IMPROVE OUTCOME?
• 99 consecuFve cases of accreta • 62 antenatal diagnosis, 37 intrapartum • If prenatal diagnosis
– Less overall EBL (2300 cc vs 2900 cc) – Less transfusion (4.7 units vs 6.9 units)
• No difference in neonatal outcomes RECOMMENDATION: Planned delivery at 34-‐35 weeks resulted
in less maternal hemorrhagic complicaFons and similar neonatal outcomes
Obstet Gynecol Jan. 2010 pg. 65-‐69

OPTIMAL TIME FOR DELIVERY
• Decision tree analysis • 9 different clinical scenarios • Looked at probability of various outcomes based on Fming of delivery
• Looked at 34 through 39 weeks and 36, 37, 38 weeks axer mature amniocentesis
• Conclusion: elecFve delivery at 34 weeks axer giving steroids the safest for mom and baby
Robinson BK Obstet Gynecol 2010;116(4):835-‐42

WHAT ABOUT CONSERVATIVE MANAGEMENT?
• 14 year, mulF-‐center study in France
• 167 paFents with conservaFve management, i.e. placenta lex in situ
• ConservaFve management included – Uterotonic agents – AnFbioFcs – Arterial embolizaFon
– Methotrexate
Obstet Gynecol Mar 2010 pg. 526-‐34

WHAT ABOUT CONSERVATIVE MANAGEMENT?
• Most cases were intrapartum diagnosis • Of the conservaFve group
– 51.5% had postpartum hemorrhage • 17.4% responded to utero-‐tonic agents • 10.8% required primary hysterectomy • 69.8% required intervenFonal radiology
– 10.% required delayed hysterectomy – 1 paFent died from sepsis axer methotrexate
• ConservaFve management is reasonable if have availability of intervenFonal radiology and other subspecialFes to handle complicaFons

© 2006 The American College of Obstetricians and Gynecologists. Published by Lippinco" Williams & Wilkins, Inc. 2
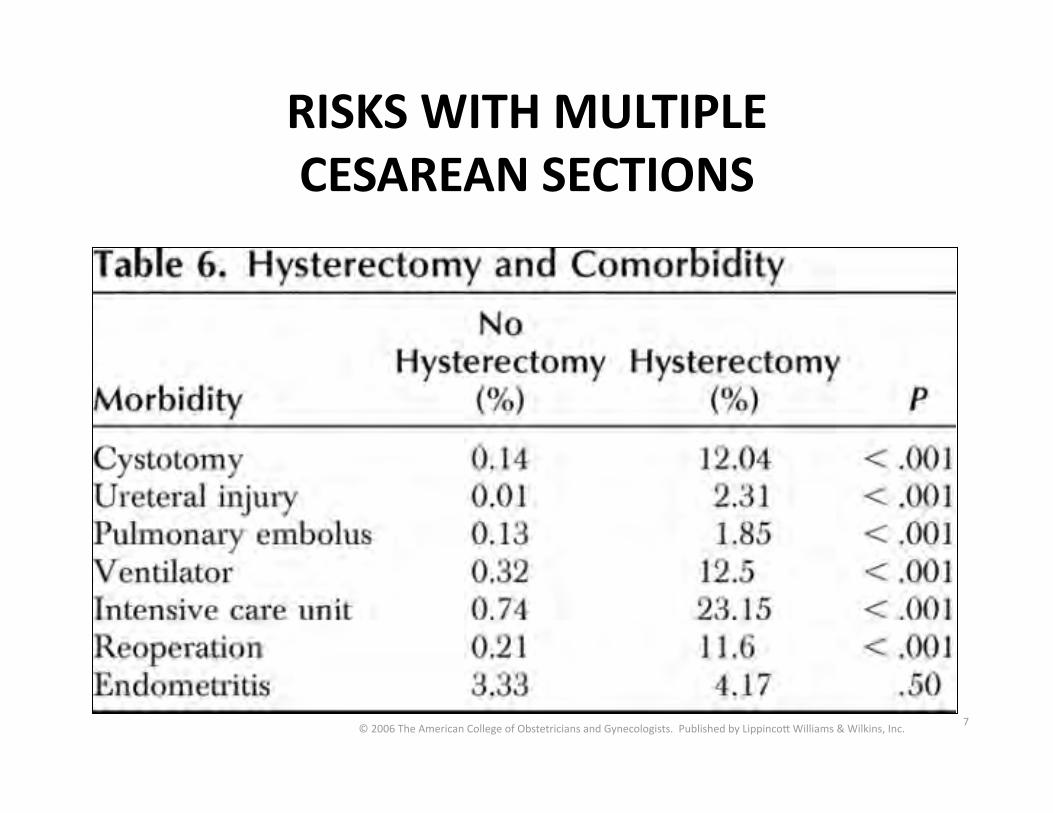
RISKS WITH MULTIPLE CESAREAN SECTIONS

© 2006 The American College of Obstetricians and Gynecologists. Published by Lippinco" Williams & Wilkins, Inc. 3
RISKS WITH MULTIPLE CESAREAN SECTIONS

© 2006 The American College of Obstetricians and Gynecologists. Published by Lippinco" Williams & Wilkins, Inc. 4
RISKS WITH MULTIPLE CESAREAN SECTIONS

© 2006 The American College of Obstetricians and Gynecologists. Published by Lippinco" Williams & Wilkins, Inc. 5
RISKS WITH MULTIPLE CESAREAN SECTIONS

© 2006 The American College of Obstetricians and Gynecologists. Published by Lippinco" Williams & Wilkins, Inc. 6
RISKS WITH MULTIPLE CESAREAN SECTIONS
© 2006 The American College of Obstetricians and Gynecologists. Published by Lippinco" Williams & Wilkins, Inc. 7
RISKS WITH MULTIPLE CESAREAN SECTIONS

RISK OF PREVIA AND PRIOR C-‐SECTION

VASA PREVIA
• DefiniFon: fetal vessels that traverse the membranes in the lower segment in advance of the fetal head
• Most commonly seen – Velamentous inserFon – Succenturiate lobe – ? IVF pregnancies
• ComplicaFon: fetal exsanguinaFon, usually axer ruptured membranes

DIAGNOSIS
• Clinically – Usually vaginal bleeding with FHR abnormaliFes
• Sinusoidal • Bradycardia
– Apt test • Alkaline denaturaFon (fetal blood remains pink, adult turns brown/green)
• Ultrasound – Fetal vessels covering/crossing internal os

IMPORTANCE OF ANTENATAL DIAGNOSIS
• Fetal blood volume – Approximately 125 cc/kg
– Term infant ~ 3 kg – Total volume about 375 cc (12 oz or a small lase) – May exsanguinate quickly
• Deliver prior to ruptured membranes

IMPORTANCE OF ANTENATAL DIAGNOSIS

MANAGEMENT
• Unclear • Based on history and other risk factors • Cesarean secFon prior to labor or ruptured membranes
• Reasonable for delivery at 35-‐36 weeks

WHAT ELSE?
• InferFlity – No data suggesFng there is an associaFon
• AbrupFon – May be slightly higher axer a cesarean secFon but the risk does not progressively increase with increasing cesarean deliveries
• IUFD in next pregnancy – No cause and effect except in those with a prior abrupFon

WHAT ELSE?
• Wound complicaFons – Not well studied but anecdotally the risk of seroma/superficial wound disrupFon is higher
• Hernia – Higher risk of incision hernia with mulFple abdominal procedures but not well studied is paFents with just c-‐secFons
WHAT ELSE?
• Adhesion formaFon – Over 50% with adhesions in 3rd or more cesarean compared to first c-‐secFon
– Increases Fme to delivery of infant
– Increases risk of bowel injury – Increases risk of cystotomy • 0.13% in primary vs 1.94% with 5th c-‐secFon

SUMMARY
• MulFple c-‐secFons increase cost of health care
• Increase risk of placental implantaFon problems like previa/accreta/vasa previa
• Increase risk of hysterectomy • Increase risk of surgical complicaFons – Adhesions – Inadvertent bowel/bladder injury – Time to deliver fetus

SUMMARY
• Probably does not increase risk of – IUFD – AbrupFon – InferFlity – Endometriosis
– Chronic pain • Probably no absolute number to limit c-‐secFon to but 3 is where risk goes up





























