Embed Size (px)
Citation preview
Multiple supernumerary teeth and possible implications Caroline H. C. Acton, BDS, FDSRCS(Eng.)*
Abstract A case of an unusual number of supernumerary teeth is reported because patients who present with this symptom may be suffering from Gardner’s syndrome or cleidocranial dysostosis.
(Received for publication June 1985. Accepted October 1985.)
Case report A 24 year-old Caucasian man was referred by his
general practitioner for surgical removal of four wisdom teeth. He had no symptoms and his only medical problem was that of penicillin hyper- sensitivity.
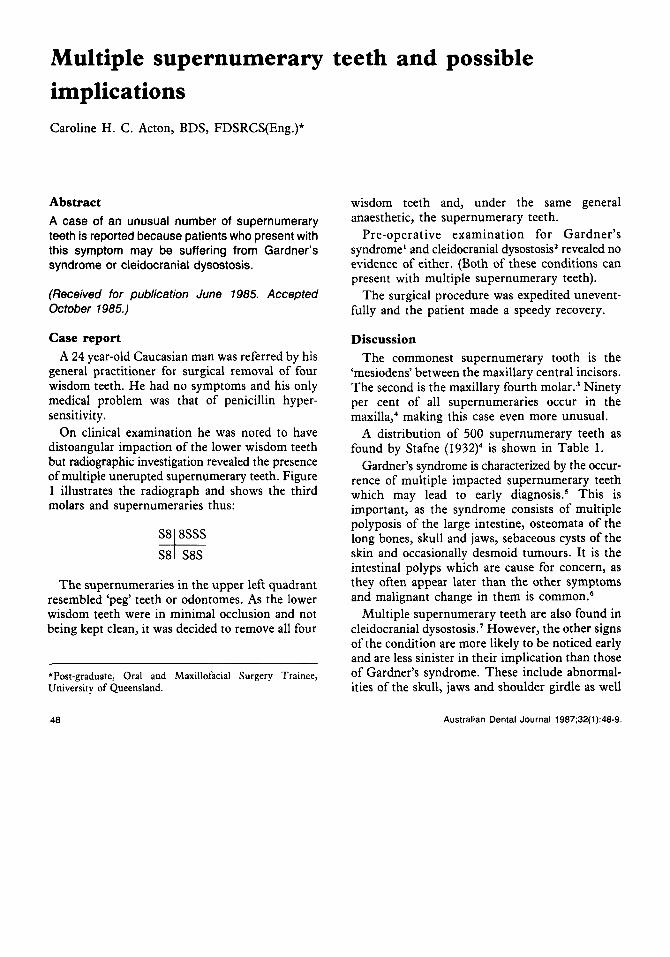
On clinical examination he was noted to have distoangular impaction of the lower wisdom teeth but radiographic investigation revealed the presence of multiple unerupted supernumerary teeth. Figure 1 illustrates the radiograph and shows the third molars and supernumeraries thus:
The supernumeraries in the upper left quadrant resembled ‘peg’ teeth or odontomes. As the lower wisdom teeth were in minimal occlusion and not being kept clean, it was decided to remove all four
~
*Post-graduate, Oral and Maxillofacial Surgery Trainee, University of Queensland.
wisdom teeth and, under the same general anaesthetic, the supernumerary teeth.
Pre-operative examination for Gardner’s syndrome’ and cleidocranial dysostosis2 revealed no evidence of either. (Both of these conditions can present with multiple supernumerary teeth).
The surgical procedure was expedited unevent- fully and the patient made a speedy recovery.
Discussion The commonest supernumerary tooth is the
‘mesiodens’ between the maxillary central incisors. The second is the maxillary fourth m01ar.~ Ninety per cent of all supernumeraries occur in the m a ~ i l l a , ~ making this case even more unusual.
A distribution of 500 supernumerary teeth as found by Stafne (1932)” is shown in Table 1.
Gardner’s syndrome is characterized by the occur- rence of multiple impacted supernumerary teeth which may lead to early diagnosis.$ This is important, as the syndrome consists of multiple polyposis of the large intestine, osteomata of the long bones, skull and jaws, sebaceous cysts of the skin and occasionally desmoid tumours. It is the intestinal polyps which are cause for concern, as they often appear later than the other symptoms and malignant change in them is common.6
Multiple supernumerary teeth are also found in cleidocranial dysostosis.’ However, the other signs of the condition are more likely to be noticed early and are less sinister in their implication than those of Gardner’s syndrome. These include abnormal- ities of the skull, jaws and shoulder girdle as well
48 Australian Dental Journal 1987;32(1):48-9.

Fig. 1. -Multiple unerupted supernumerary teeth in a 24-year-old Caucasian man.
Table 1. Distribution of 500 supernumerary teeth4
Central La!era1 Cuspids Premolars Paramolars zi:s Total incisors incisors
Maxilla 227 19 2 9 58 131 446 Mandible 10 0 1 33 0 10 54
as defects of the vertebral column, pelvis and digits.* As both diseases are transmitted by a dominant gene, the patient’s children too were investigated. They showed no signs of the syndromes. The importance of being aware of oral signs of systemic disease is emphasized so that early treatment, if indicated, can be undertaken.
Acknowledgements I am grateful to Professor R. O”ei1 of University
College Hospital, London, for his permission to publish this case, and to Associate Professor F. Monsour for his advice.
References 1. Duncan BR, Dohner VA, Priest JH. The Gardner syndrome:
2. Kalliala E, Taskinen PJ. Cleidocranial dysostosis. Report of need for early diagnosis. J Paediatr 1968;72:497-505.
3.
4.
5.
6.
7.
8.
six typical cases and one atypical case. Oral Surg
Shafer WG, Hine MK, Levy BM. A textbook of oral pathology. 3rd edn. Philadelphia: WB Saunders, 1976:43. Stafne EC. Supernumerary teeth. Dent Cosmos
Fader M, Kline SN, Spatz SS, Zurbrow HJ. Gardner’s syndrome (intestinal polyposis, osteomas, sebaceous cysts), a new dental discovery. Oral Surg 1962;15: 153-72. McFarland PH, Sheetz WL, Knisley RE. Gardner’s syndrome: report of two families. J Oral Surg 1968;26:632-8. Rushton MA. The failure of eruption in (cleidocranial dysostosis). Br Dent J 1937a;63:641-5. Jackson WPU. Osteodental dysplasia (cleidocranial dysostosis). Acta Med Scand 1951;139:292-303.
Address for reprints: Dental School,
University of Queensland, Turbot Street,
Brisbane, Qld, 4000.
1962;15:808-22.
1932;74:653-9.
Australian Dental Journal 1987;32:1. 49




![A Rare Location for a Dentigerous Cyst · 2019-12-11 · Rarely, a dentigerous cyst is associated with odontoma, deciduous teeth and supernumerary teeth [2,3]. The association of](https://img.dokumen.tips/doc/110x75/5f469ff5b5ff297efb5f1464/a-rare-location-for-a-dentigerous-2019-12-11-rarely-a-dentigerous-cyst-is-associated.jpg)






![Supernumerary Teeth in all 4 Quadrants of a Non-Syndromic ... · [2]. Mesiodens, defined as a supernumerary tooth located predominately in the premaxilla area between the two upper](https://img.dokumen.tips/doc/110x75/5ecb80e64dce2967c35acab5/supernumerary-teeth-in-all-4-quadrants-of-a-non-syndromic-2-mesiodens-defined.jpg)

















