Embed Size (px)
Citation preview

Ophthalmic Genetics, 26:37–43, 2005Copyright c© Taylor and Francis Inc.ISSN: 1381-6810 (print) / 1744-5094 (online)DOI: 10.1080/13816810590927217
CASE REPORT
Multiple Congenital Malformations Including Severe EyeAnomalies and Abnormal Cerebellar Development withDandy-Walker Malformation in a Girl with PartialTrisomy 3q
Lılia Maria de Azevedo MoreiraHuman Genetics and Cytogenetics Laboratory, Biology Institute, Federal University of Bahia(UFBA)-Campus Universitario de Ondina, Salvador, Bahia, Brazil
Fatima Bittencourt Neri and Sheila de Quadros UzedaPrecocious Intervention Center (CIP)-Blind People Institute of Bahia, Salvador, Bahia, Brazil
Acacia Fernandes Lacerda de Carvalho and Gustavo Costa SantanaDNA-Laboratory of Medical Genetics and Molecular Biology, Salvador, Bahia, Brazil
Fabiana Rocha SouzaHuman Genetics and Cytogenetics Laboratory, Biology Institute, Federal University of Bahia(UFBA)-Campus Universitario de Ondina, Salvador, Bahia, Brazil
Jose Cortes RollembergNeurology Department, Federal University of Bahia (UFBA)-Campus Universitario do Canela,Salvador, Bahia, Brazil
Purpose: Ocular anomalies have been associated with numerous chromosomal abnormalities.This report describes partial trisomy 3q in a two-month-old girl with dysmorphic features ofthe Dup3q phenotype and severe eye and cerebellar malformations. Methods: Clinical exam-ination and chromosomal analysis were conducted. Results: The karyotype of the proposituswas 46,XX, ins(3)(pter → p25::q27 → q21::p25 → qter). She had an abnormal head shape,low-set malformed ears, coarse facies, short webbed neck, abnormal foot position, polycystickidney, and spina bifida. There was also bilateral microphthalmia that was more severe on theright side, microcornea, and corneal opacity. She had posterior fossa abnormalities, includingcerebellar vermis hypoplasia suggestive of a Dandy-Walker (DW) malformation. Conclusions:This girl with an intrachromosomal duplication of distal 3q and typical phenotype belongs tothe severe end of the spectrum for such cases. The ocular manifestations of the 3q duplicationsyndrome provide additional evidence of the involvement of developmental eye genes in thischromosomal segment.
Keywords Dup3q syndrome; insertional duplication; multiple congenital malformations; eyeanomalies; microphthalmia; Dandy-Walker malformation; SOX2
INTRODUCTIONSince the first description by Clarke et al.1 of a family with
partial duplication/trisomy of the long arm of chromosome 3,
Accepted 8 December 2004.Address correspondence to Lılia Maria de Azevedo Moreira, Rua
da Paz, 32, apt.201, Graca, CEP 40150-141, Salvador—Bahia, Brazil.E-mail: [email protected]
several children with this chromosomal aberration have beendescribed and the critical region mapped to 3q26.3-3q27.2 Af-fected children have gross abnormalities of the heart and brainand a high incidence of postnatal death.3
In most patients, the trisomy is secondary to a familial translo-cation involving 3q and another chromosome, or it may be theproduct of a duplication/deficiency rearrangement from the seg-regation of a parental inverted chromosome with crossing-over
37
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

38 L.M.A. MOREIRA ET AL.
in a loop, following a genetic imbalance called ‘aneusomie derecombinaison’.4 Few patients have a de-novo interstitial du-plication resulting from one meiotic event. Several authors, in-cluding Ismail et al.,5 believe that the phenotypes are similar,regardless of their cytogenetic origin and different associateddeletions. Van Essen et al.,6 however, observed that the dupli-cation of genes in the distal part of 3q26 and the proximal partof 3q27 appears to be essential for the typical phenotype andRizzu and colleagues excluded 3q25-q26.2 from the duplica-tion 3q syndrome critical region.7
In this paper, we contribute towards further delineation of thephenotype by presenting a new case of duplication 3q21-q27with cerebellar vermis hypoplasia suggestive of Dandy-Walkermalformation and other congenital malformations. The presenceof severe microphthalmia also corroborates the hypothesis thata genetic locus for eye development exists in this chromosomalsegment.
CASE REPORTThe propositus was born to a 16-year-old primigravida and
a father who was 28 years old at the time of the birth. The par-ents were healthy and nonconsanguineous. There was no his-tory of infertility, high frequency of miscarriage, or congenitalmalformations in either parental family. The mother smokedduring pregnancy. Fetal ultrasound examination showed dilated
FIG. 1. Ultrasound showing asymmetry of the eyeball, silence of vitreo, and attached retina and choroid.
lateral ventricles and there was indication of polyhydramnios.The pregnancy ended in the 37th week by vaginal delivery. Ap-gar scores were 2 and 8 after one and five minutes, respectively.Weight at birth was 2540 g, length 43 cm (below the 3rd centile).Head circumference was 35 cm (50th centile). Several congen-ital anomalies were noted at birth.
Ophthalmological examination at 21 days of age showed bi-lateral conjunctivitis, corneal opacity, and bilateral microph-thalmia. Ocular ultrasound showed asymmetry of ocular sizeand a clear vitreous (Fig. 1). The patient did not respond tolight. Retinoscopy and examination of the ocular fundus couldnot be performed due to corneal opacity; ultrasound showed anattached retina and choroid.
Computerized tomography (CT) of the head showed thinningof the optic nerve of the right eye that exhibited high densitythroughout the vitreous. There were also signs of cerebellar at-rophy with a large communication between the fourth ventricleand the cisterna magna associated with agenesis of the cerebel-lar vermis and mild dilation of supratentorial ventricular system(Fig. 2). The combination of these features suggested a Dandy-Walker malformation.8
Examination at two months of age (Fig. 3) showed growthretardation, respiratory problems, and hypertrichosis (moremarked over the back). In addition, the following featureswere observed: low-set and posteriorly rotated ears; coarse
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

SEVERE EYE ANOMALIES IN DUPLICATION 3q21-q27 39
FIG. 2. Brain computed tomography (CT) scan illustrating (A) hypotrophy of the right eye and (B) hypoplasia of the cerebellarvermis.
FIG. 3. Overall appearance of the propositus at age 2 months, illustrating several dysmorphic stigmata.
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

40 L.M.A. MOREIRA ET AL.
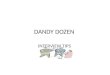
FIG. 4. (A) Ideogram of chromosome 3 according to ISCN 1995. (B) Hypothetical formation of the chromosome rearrangementthrough an insertion between arms with q21 → q27 segment inserted in p25. (C) GTG banded normal and duplicated chromosome3 from three cells of the proband. Arrows indicate breakpoints and brackets indicate duplicated segment.
square-shaped face with atypical hair distribution in the bitem-poral and zygomatic regions; prominent central forehead; andhypertelorism, thick eyebrows, and long eyelashes. There wasalso a short nose with broad root and anteverted nostrils, longphiltrum, inverted upper lip, a high arched palate, cleft palate,prominent maxilla, mandibular micrognathia, and sharp trian-gular chin. The patient had webbing of the neck with redundantskin, wide-set hypoplastic nipples, a pilonidal sinus and rhi-zomelic shortness of upper limbs, and a sandal gap of the toes.The child also had bilateral simian palmar creases, overlappingfingers, bilateral clinodactyly of the fifth finger, and nail dyspla-sia. Clenched hands and crossed legs like in trisomy 18 syndromewere further noted. Her feet were abnormally positioned.
Radiological investigation was indicative of clefting in thehigh cervical and thoracic spine. The kidneys showed bilat-eral cysts on ultrasonography. The child frequently developedsevere respiratory insufficiency with apneic attacks. As a re-sult, she progressively deteriorated despite intensive care anddied three months after delivery. Permission for necropsy wasrefused.
CYTOGENETIC INVESTIGATION: METHODSAND RESULTS
Chromosome analysis was performed on conventional cul-tures of peripheral blood with GTG banding. In 30 analyzed
metaphases, a heteromorphic chromosome 3 was observed. Thebanding technique indicated a duplication of the distal segmentof the long arm of this chromosome, with breakpoints localizedbetween 3q21-q27 bands and insertion of this segment at 3p25(Fig. 4). According ISCN 1995,9 the karyotype was interpretedas 46,XX, ins(3)(pter → p25::q27 → q21::p25 → qter). Addi-tional tissue samples for molecular studies could not be obtained.The mother’s karyotype was normal. We could not perform cy-togenetic examinations on other family members, including thefather.
DISCUSSIONThis report describes the severe phenotype of a newborn girl
with partial duplication of the long arm of chromosome 3. Anumber of cases with duplication 3q have been described, gen-erally involving chromosomal segment 3q21-qter. Unlike previ-ously reported cases, the present patient had a duplication limitedto a shorter segment 3q21-q27, inserted in 3p25. Fineman et al.10
described a break in the 3p25 region in four unrelated familiesand suggested that this band is more susceptible to breakage andabnormal realignment during meiosis; or, more likely, proximalbreaks in the short arm of the chromosome 3 may be incompati-ble with life since they would cause a large 3p deletion segment.In most cases with this type of intrachromosomal insertion, inwhich a segment of chromatin from one arm is inserted into
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

TAB
LE
1C
linic
alm
anif
esta
tions
ofth
epu
redu
p(3q
)sy
ndro
me.
Feat
ures
Sten
gel-
Rut
hkow
skie
tal.13
(dup
3q21
-27)
Ros
enfe
ldet
al.14
(dup
3q21
-26)
Scio
rra
etal
.15
(dup
3q23
-27)
Van
Ess
enet
al.6
(dup
3q25
-28)
Pres
entc
ase
(dup
3q21
-27)
Tota
l
Sex
FF
FF
F5F
Gro
wth
reta
rdat
ion
++
++
+5/
5D
eath
befo
re12
mon
ths
+.
−.
+2/
3H
yper
tric
hosi
s+
−−
++
3/5
Abn
orm
alhe
adco
nfigu
ratio
n+
++
++
5/5
Squa
re-s
hape
dfa
ce+
+.
++
4/4
Hyp
erte
lori
sm+
−+
.+
2/3
Mic
roph
thal
mia
/ano
phth
alm
ia+
−.
++
3/4
Oth
erey
ean
omal
ies
++
++
+5/
5B
road
nose
root
++
++
+5/
5A
ntev
erte
dno
stri
ls+
++
++
5/5
Lon
gph
iltru
m+
.+
++
4/4
Prom
inen
tmax
illa
++
++
+5/
5D
ownt
urne
dco
rner
sof
mou
th+
++
++
5/5
Hig
hly
arch
edor
clef
tpal
ate
++
.+
+4/
4Sh
arp,
tria
ngul
arch
in+
+.
++
4/4
Mal
form
edor
low
-set
auri
cles
++
.+
+4/
4Sh
orto
rw
ebbe
dne
ck+
++
++
5/5
Wid
e-sp
aced
nipp
les
++
..
+3/
3C
ardi
acde
fect
s+
+.
+−
3/4
Gas
troi
ntes
tinal
anom
alie
s−
+.
+−
2/4
Ren
alor
urin
ary
trac
tano
mal
ies
+.
−+
+3/
4Sh
ortl
imbs
+−
−.
+2/
4C
linod
acty
ly+
−+
++
4/5
Hyp
opla
stic
nails
+.
.+
+3/
3T
rans
vers
epa
lmar
crea
ses
..
..
+1/
1A
bnor
mal
foot
posi
tion
+.
.+
+3/
3H
emiv
erte
brae
orsp
ina
bifid
a+
−.
++
3/4
Oth
ersk
elet
alan
omal
ies
+−
.+
+3/
4B
rain
anom
alie
sse
izur
es.
.−
++
2/3
Abn
orm
alC
T-sc
anfin
ding
s.
−.
Ver
mis
Ver
mis
2/3
hypo
plas
iahy
popl
asia
/DW
C
+,pr
esen
t;−,
abse
nt;.
,not
reco
rded
.
41
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

42 L.M.A. MOREIRA ET AL.
the other arm, crossover within the centromeric segment mayproduce recombinant chromosomes—one with a duplication ofthe insertion segment and the other with a deletion.11
The risk of recurrence of this rearrangement is very low ifparental chromosomes are normal. In the present case, unfor-tunately, the father could not be located to perform cytogeneticstudies and it has not been possible to predict his genetic risk.
Most patients with extensive 3q trisomy die early, eitherduring pregnancy or after birth. Those who survive have se-vere handicaps, including developmental delay, brain and ocu-lar anomalies, and a characteristic facial appearance.12 Whenthe phenotype of the present case is compared with othercases of pure partial trisomy 3q and without another structuralrearrangement,6,13-17 (Table 1) one finds close resemblance tothe typical description of this syndrome.
Chrousos et al.18 mentioned hypertelorism, epicanthus, andglaucoma as the main ocular findings in partial 3q syndrome.The major gene for anophthalmia, SOX2, has been mapped to3q26.3-q27 and chromosome deletion involving this region hasbeen identified in patients with micro/anophthalmia.19-22 Dupli-cations of this critical region, as shown in the present patient andliterature cases,6,11,23 also exhibit this severe form of eye mal-formation and might contribute to the knowledge of the ocularphenotype.
The presence of the Dandy-Walker malformation in patientswith different chromosomal abnormalities was reported by Talet al.8 and Tamraz et al.24 The etiology of this malformationis heterogeneous, comprising chromosomal abnormalities andteratogen exposure. This abnormality, observed in the presentcase and probably in the patient of van Essen’s group, may alsobe part of the 3q syndrome phenotype, and perhaps has notoften been described in this context due to the infrequent studyof these cases with CT scan or magnetic resonance imaging. Asin the present case, Tal et al.8 described cleft palate, bilateralpolycystic kidney, spina bifida, and rotational limb deformitiesassociated with the Dandy-Walker malformation.
This report reinforces the van Essen et al.6 postulate that3q partial trisomy syndrome is an exception to the generallyaccepted principle that deletions usually produce a more dele-terious effect than duplications. The description of the presentcase contributes to a better understanding and phenotype de-lineation of this syndrome and to the knowledge of the asso-ciation between the 3q26-q27 chromosomal segment and eyedevelopment.
ACKNOWLEDGEMENTSThe authors wish to thank social worker Sandra Duplat for her
kind support, the medical professionals of the General Hospitalof Camacari for cooperating with this study, the mother of thepatient for permission to publish this report, and Miss RafaellaMourao, Mrs. Auxiliadora Fonseca Barreto, and Mrs. DerlitaMachado Silva for their technical assistance.
REFERENCES1. Clarke G, Stevenson AC, Davies P, Williams CE. A family ap-
parently showing transmission of a translocation between chro-mosome 3 and one of the ‘X-6-12’ or ‘C’group. J Med Genet.1964;1:27-34.
2. Aqua MS, Rizzu P, Lindsay EA, et al. Duplication 3q syndrome:molecular delineation of the critical region. Am J Med Genet.1995;55:33-37.
3. Schinzel A. Catalogue of unbalanced chromosome aberra-tions in man. 2nd ed. Berlin/New York: de Gruyter, 2001;142-144.
4. Lejeune J, Berger R. Sur deux observations familiales de translo-cations complexes. Ann Genet. 1965;8:21-30.
5. Ismail SR, Kousseff BG, Kotb SM, Kholeif SF. Duplication3q (q21 → qter) without limb anomalies. Am J Med Genet.1991;38:518-522.
6. Van Essen AJ, Kok K, Van den Berg A, et al. Partial 3q duplicationsyndrome and assignment of D3S5 to 3q25-3p28. Hum Genet.1991;87:151-154.
7. Rizzu P, Haddad BR, Vallcorba I, et al. Delineation of a duplicationmap of chromosome 3q: a new case confirms the exclusion of 3q25-q26.2 from the duplication 3q syndrome critical region. Am J MedGenet. 1997;68:428-432.
8. Tal Y, Freigang B, Dunn HG, et al. Dandy-Walker syndrome:analysis of 21 cases. Dev Med Child Neurol. 1980;22:189-201.
9. ISCN 1995. An international system for human cytogenetic nomen-clature. Basel: Karger, 1995;32-33.
10. Fineman RM, Hecht F, Ablow RC, et al. Chromosome 3 duplicationq/deletion p syndrome. Pediatr. 1978;61:611-618.
11. Allerdice PW, Browne N, Murphy DP. Chromosome 3 duplicationq21 → qter deletion p25 → pter syndrome in children of carri-ers of a pericentric inversion inv(3) (p25q21). Am J Hum Genet.1975;27:699-718.
12. Yatsenko SA, Mendonza-Londono R, Belmont JW, et al. Omphalo-cele in trisomy 3q: further delineation of phenotype. Clin Genet.2003;64:404-413.
13. Stengel-Ruthkowski S, Murken JD, Pilar V, et al. New chromoso-mal dysmorphic syndromes 3. Partial trisomy 3q. Eur J Pediatr.1979;130:111-125.
14. Rosenfeld W, Verma RS, Jhaveri RC, et al. Duplications 3q: severemanifestations in a infant with duplication of a short segment of3q. Am J Med Genet. 1981;10:187-192.
15. Sciorra LJ, Bahng K, Lee M-L. Trisomy in the distal end ofthe long arm of chromosome 3. Am J Dis Child. 1979;133:727-730.
16. Ismail SR, Kousseff BG, Kotb SM, Kholeif SF. Duplica-tion 3q(q21-qter) without limb anomalies. Am J Med Genet.1991;38:518-522.
17. Steinbach P, Adkins Jr WN, Caspar KW, et al. The dup(3q) syn-drome: report of eight cases and review of the literature. Am J MedGenet. 1981;10:159-177.
18. Chrousos GA, O’Neill JF, Traboulsi EI, et al. Ocular findings inpartial trisomy 3q. A case report and review of the literature. Oph-thalmic Paediatr Genet. 1985;9:127-130.
19. Chitayat D, Babul R, Silver MM, et al. Terminal deletion of thelong arm of chromosome 3 [46,XX,del(3)(q27-qter)]. Am J MedGenet. 1996;61:45-48.
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.

SEVERE EYE ANOMALIES IN DUPLICATION 3q21-q27 43
20. Male A, Davies A, Bergbaum A, et al. Delineation of an estimated6.7 MB candidate interval for an ophthalmia gene at 3q26.33-q28and description of the syndrome associated with visible chromo-some deletion of this region. Eur J Hum Genet. 2002;10:807-812.
21. Fantes J, Ragge NK, Lynch S-A, et al. Mutation in SOX2 causeanophthalmia. Nat Genet. 2003;33:1-2.
22. Driggers RW, Macri CJ, Greenwald J, et al. Isolated bilateral anoph-thalmia in a girl with an apparently balanced de novo transloca-
tion: 46,XX,t(3;11)(q27;p11.2). Am J Med Genet. 1999;87:201-202.
23. Fear C, Briggs A. Familial partial trisomy of the long arm of chro-mosome 3 (3q). Arch Dis Child. 1979;54:135-138.
24. Tamraz JC, Rethore M-O, Iba-Zizen MTh, et al. Contribu-tion of magnetic resonance imaging to the knowledge of CNSmalformations related to chromosomal aberrations. Hum Genet.1987;76:265-273.
Oph
thal
mic
Gen
et D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
ichi
gan
Uni
vers
ity o
n 10
/27/
14Fo
r pe
rson
al u
se o
nly.