Embed Size (px)
Citation preview

Case Report/Clinical Techniques
Multiple Apical Radiolucencies and ExternalCervical Resorption Associated with VaricellaZoster Virus: A Case Report
Kreena Patel, BDS(Hons), MJDF RCS, Elia Schirru, DDS, Sadia Niazi, BDS, MSc, PhD,Philip Mitchell, BDS, MSc, MRD, and Francesco Mannocci, MD, DDS, PhD, FHEAAbstract
Varicella zoster virus (VZV) is responsible for the primaryinfection chickenpox. After the initial infection, itremains latent but can reactivate, resulting in shingles(herpes zoster). Previous reports have implicated VZVin the pathogenesis of apical periodontitis, but theinvolvement of the virus has not been investigated fully.The present case describes a patient who suffered froma severe episode of shingles and subsequently devel-oped periapical radiolucencies of all the teeth in theaffected nerve distribution. Molecular and culture tech-niques showed the presence of VZV DNA in the root ca-nal system in the absence of bacteria. This confirms thatVZV can cause localized pulp necrosis and apical peri-odontitis. The lesions healed after endodontic treat-ment, implying chemomechanical debridement usingsodium hypochlorite irrigation and a calcium hydroxideinterim dressing may be effective against the virus. (JEndod 2016;42:978–983)Key WordsApical periodontitis, external cervical resorption, herpeszoster, shingles, sodium hypochlorite, varicella zoster,virus
From the Department of Endodontology, Kings CollegeDental Institute at Guy’s King’s and St Thomas’ Hospital,London, United Kingdom.
Address requests for reprints to Prof Francesco Mannocci,Department of Endodontology, Kings College Dental Institute,Floor 25–Tower Wing, Guy’s Hospital, Great Maze Pond,London SE1 9RT, UK. E-mail address: [email protected]/$ - see front matter
Copyright ª 2016 American Association of Endodontists.http://dx.doi.org/10.1016/j.joen.2016.03.017
978 Patel et al.
Apical periodontitis is a localized immune-modulated inflammatory disease causedby an infection of the dental pulp. Numerous studies have revealed the essential role
of bacteria in the etiology of the disease (1–4). Microorganisms normally enter the pulpvia caries, clinical procedures, or cracks (5, 6). Bacteria have frequently been isolatedfrom teeth with necrotic pulps but clinically intact crowns (4, 7–9). It was alsohypothesized that bacteria within the blood circulation could enter and infectnecrotic pulps (anachoresis). However, this has been shown to be highly unlikely (10).
Several studies have suggested that other microorganisms are associated with thepathogenesis of apical periodontitis, including fungi and viruses (11–15). Among thelatter, human cytomegalovirus (HCMV), Epstein-Barr virus (EBV), and varicella-zostervirus (VZV) have been most commonly isolated (14, 16, 17). These viruses belong tothe family of Herpesviridae. A common feature within the family is a single double-stranded DNA molecule enclosed in a viral envelope. Eight human herpes viruseshave previously been identified: herpes simplex virus 1 and 2; VZV; EBV; HCMV; andhuman herpes virus 6, 7, and 8. There appears to be a higher occurrence of HCMV,EBV, and VZV in symptomatic cases and larger lesions (18, 19) and a higherprevalence in human immunodeficiency virus (HIV)-infected patients (20).
VZV is responsible for the primary infection chickenpox. The virions enter fromthe skin or T-lymphocyte viremia and travel in a retrograde manner to the sensory nerveganglia (21). After the initial infection, the virus remains latent in the long-lived, nondi-viding perineural satellite cells of the sensory ganglia (22, 23). In 20% of cases, thevirus can reactivate, either spontaneously or as a result of an impaired host immunedefense, resulting in shingles (herpes zoster). The virus begins to replicate andreaches the skin by anterograde nerve transport (21). Prodromal symptoms includetingling, itching, and pain in the affected dermatome. This is followed by a maculopap-ular rash in the region, which evolves into vesicles and pustules.
The trigeminal nerve is affected in only 13%of patients (24). The clinical diagnosisof VZV infection is sufficient most of the time although polymerase chain reaction (PCR)analysis or immunofluorescence is sometimes required. Complications includeBell palsy, ocular involvement, hearing impairment, Ramsay Hunt syndrome, andvasculopathy (25). Reported sequelae of dental relevance include devitalization of teeth(26, 27), postherpetic neuralgia, osteonecrosis, dental resorption (internal andexternal), and tooth exfoliation (28–30). However, these are case reports or caseseries, and the involvement of VZV has not been fully investigated.
This case report describes a patient who suffered from a severe episode of trigem-inal herpes zoster and subsequently developed periapical radiolucencies of all the teethin the affected nerve distribution area and external cervical resorption of #27. Molec-ular and culture techniques showed the presence of VZV in the root canal systems in theabsence of bacteria.
ExaminationA 52-year-old Asian man was referred to Guy’s Dental Hospital, London, UK, in
August 2014. The patient presented with periapical radiolucencies associated with#25, #26, #27, #28, #29, and #30. There was no history of trauma, metabolic bonedisease, or orthodontic treatment.
JOE — Volume 42, Number 6, June 2016
Case Report/Clinical Techniques
The patient was medically fit and healthy at the initial consultation.In 1987, he suffered from an episode of herpes zoster affecting the righttrigeminal nerve branch V3 (lower right quadrant). He was hospitalizedfor 10 days and experienced severe pain and vesicles localized to thisdistribution. He subsequently suffered from postherpetic neuralgiaand reported mild anesthesia in this area.
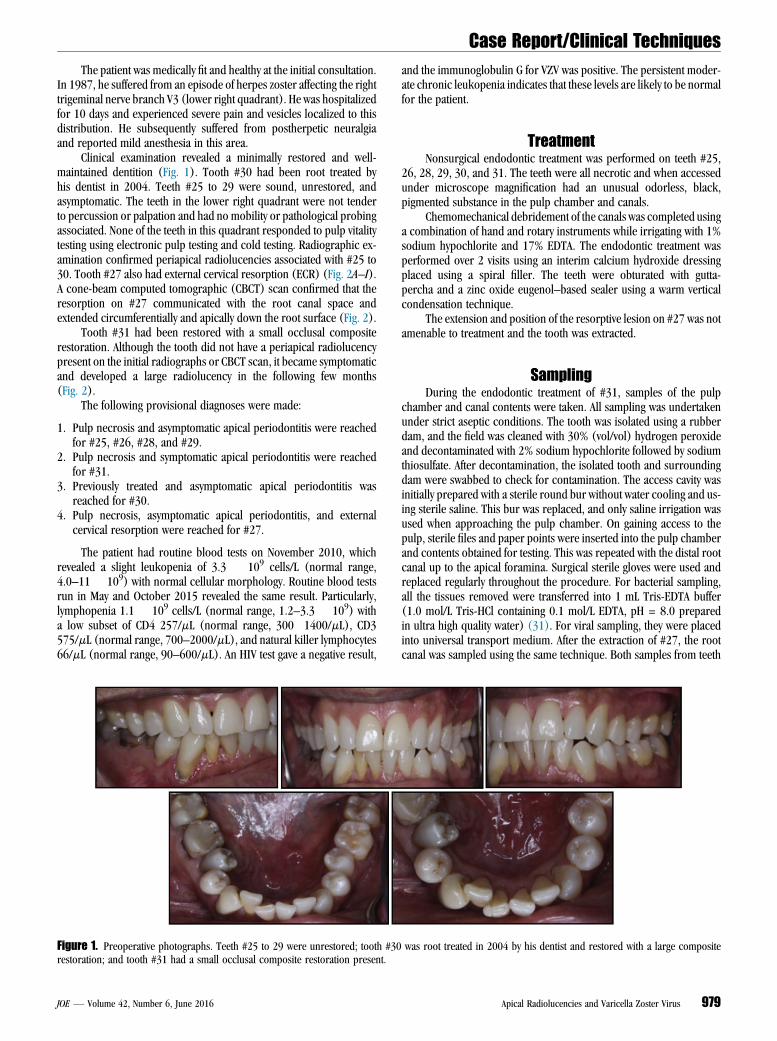
Clinical examination revealed a minimally restored and well-maintained dentition (Fig. 1). Tooth #30 had been root treated byhis dentist in 2004. Teeth #25 to 29 were sound, unrestored, andasymptomatic. The teeth in the lower right quadrant were not tenderto percussion or palpation and had no mobility or pathological probingassociated. None of the teeth in this quadrant responded to pulp vitalitytesting using electronic pulp testing and cold testing. Radiographic ex-amination confirmed periapical radiolucencies associated with #25 to30. Tooth #27 also had external cervical resorption (ECR) (Fig. 2A–I).A cone-beam computed tomographic (CBCT) scan confirmed that theresorption on #27 communicated with the root canal space andextended circumferentially and apically down the root surface (Fig. 2).
Tooth #31 had been restored with a small occlusal compositerestoration. Although the tooth did not have a periapical radiolucencypresent on the initial radiographs or CBCT scan, it became symptomaticand developed a large radiolucency in the following few months(Fig. 2).
The following provisional diagnoses were made:
1. Pulp necrosis and asymptomatic apical periodontitis were reachedfor #25, #26, #28, and #29.
2. Pulp necrosis and symptomatic apical periodontitis were reachedfor #31.
3. Previously treated and asymptomatic apical periodontitis wasreached for #30.
4. Pulp necrosis, asymptomatic apical periodontitis, and externalcervical resorption were reached for #27.
The patient had routine blood tests on November 2010, whichrevealed a slight leukopenia of 3.3 � 109 cells/L (normal range,4.0–11 � 109) with normal cellular morphology. Routine blood testsrun in May and October 2015 revealed the same result. Particularly,lymphopenia 1.1 � 109 cells/L (normal range, 1.2–3.3 � 109) witha low subset of CD4 257/mL (normal range, 300�1400/mL), CD3575/mL (normal range, 700–2000/mL), and natural killer lymphocytes66/mL (normal range, 90–600/mL). An HIV test gave a negative result,
Figure 1. Preoperative photographs. Teeth #25 to 29 were unrestored; tooth #30restoration; and tooth #31 had a small occlusal composite restoration present.
JOE — Volume 42, Number 6, June 2016
and the immunoglobulin G for VZV was positive. The persistent moder-ate chronic leukopenia indicates that these levels are likely to be normalfor the patient.
TreatmentNonsurgical endodontic treatment was performed on teeth #25,
26, 28, 29, 30, and 31. The teeth were all necrotic and when accessedunder microscope magnification had an unusual odorless, black,pigmented substance in the pulp chamber and canals.
Chemomechanical debridement of the canals was completed usinga combination of hand and rotary instruments while irrigating with 1%sodium hypochlorite and 17% EDTA. The endodontic treatment wasperformed over 2 visits using an interim calcium hydroxide dressingplaced using a spiral filler. The teeth were obturated with gutta-percha and a zinc oxide eugenol–based sealer using a warm verticalcondensation technique.
The extension and position of the resorptive lesion on #27 was notamenable to treatment and the tooth was extracted.
SamplingDuring the endodontic treatment of #31, samples of the pulp
chamber and canal contents were taken. All sampling was undertakenunder strict aseptic conditions. The tooth was isolated using a rubberdam, and the field was cleaned with 30% (vol/vol) hydrogen peroxideand decontaminated with 2% sodium hypochlorite followed by sodiumthiosulfate. After decontamination, the isolated tooth and surroundingdam were swabbed to check for contamination. The access cavity wasinitially prepared with a sterile round bur without water cooling and us-ing sterile saline. This bur was replaced, and only saline irrigation wasused when approaching the pulp chamber. On gaining access to thepulp, sterile files and paper points were inserted into the pulp chamberand contents obtained for testing. This was repeated with the distal rootcanal up to the apical foramina. Surgical sterile gloves were used andreplaced regularly throughout the procedure. For bacterial sampling,all the tissues removed were transferred into 1 mL Tris-EDTA buffer(1.0 mol/L Tris-HCl containing 0.1 mol/L EDTA, pH = 8.0 preparedin ultra high quality water) (31). For viral sampling, they were placedinto universal transport medium. After the extraction of #27, the rootcanal was sampled using the same technique. Both samples from teeth
was root treated in 2004 by his dentist and restored with a large composite
Apical Radiolucencies and Varicella Zoster Virus 979

Figure 2. Preoperative radiographs. (A) Orthopantomogram reveals multiple periapical radiolucencies associated only with the teeth in the lower right quadrant.(B–E) Preoperative periapical radiographs showing periapical radiolucencies associated with teeth #25 to 30 and external cervical resorption associated with tooth#27. (F) A periapical radiograph taken a few months later showing tooth #31 had developed a large radiolucency. (G–I) A preoperative CBCT scan of tooth #27.(G) Axial slices show the external cervical resorption is buccal and extends distally. It communicates with the root canal system. (H) Sagittal view. (I) Coronal view.
Case Report/Clinical Techniques
#27 and #31 were immediately immersed in ice and transported to thelaboratory, after which endodontic treatment of #31 was completed.
Transmission electronmicroscopic (TEM) and histologic analyseswere also carried out according to the following protocol:
1. For TEM analysis, samples of tooth #27 were collected from the rootcanal space using the previously described protocol and the resorp-tive lesion using a sterile excavator. The samples were smeared onclean slides and left to dry.
2. For histologic analysis of tooth #27, the tooth was placed into 10%formalin solution.
Microbial Analysis of SamplesEach sample was dispersed by vortexing with sterile 3.5- to
4.5-mm-diameter glass beads (BDH; Lutterworth, Leicester, UK) for
980 Patel et al.
30 seconds, serially diluted in fastidious anaerobe broth (Lab M,Heywood, UK), and plated onto nonselective media (duplicate platesof fastidious anaerobe agar [FAA] supplemented with 5% horse blood[Lab M]). The FAA plates were incubated anaerobically for 7 days andaerobically for 3 days. The swabs taken from the tooth for sterility checkwere plated directly onto FAA and incubated anaerobically for 7 days.
Aerobic and anaerobic bacterial culturing gave a negative resultfor both samples taken from tooth #31. An identical culturing techniquegave a positive bacterial result for tooth #27. An additional quantitativePCR (qPCR) analysis was performed for both samples, confirming thepresence of bacteria in tooth #27 and the absence of bacteria in #31.
Viral Analysis of SamplesQualitative PCR testing of 2 samples from teeth #31 and #27 gave a
positive result for VZV DNA. Tooth #31 had a cycle threshold (CT) value
JOE — Volume 42, Number 6, June 2016

Figure 3. (A) Histology of tooth #27. A vertical section showing the external cervical resorption (i) communicates with the root canal system (ii). (B) TEM analysisof the root canal contents of tooth #27. Different bacterial types could be seen, but no intact viral particles were detected.
Case Report/Clinical Techniques
of 29 and #27 had a CT value of 28. The cutoff CT value is 39, andanything below this is classified as a positive result. Qualitative PCRgave a negative result for herpes simplex virus 1 and 2.
HistologyHistologic analysis was only conducted on tooth #27. After fixa-
tion, the tooth was decalcified, embedded in paraffin, and seriallysectioned through the ECR lesion. Hematoxylin-eosin was used to stainthe sample. The ECR lesion was shown to communicate directly with thepulp space and showed ingrowth of inflamed periodontal tissue withepithelium. Neutrophils and bacteria were detected in the pulp space.No caries was detected (Fig. 3A and B).
TEM Analysis for SamplesTEM negative stain analysis was conducted only on tooth #27. The
dried smear was rehydrated in water and applied to formvar/carbon-coated TEM grids (Agar Scientific Limited, Essex, UK); 1% alcian bluewas used as a wetting agent for the grids, and 1.5%(w/v) phosphotungsticacid was used as the negative stain. The negatively stained grids wereviewed in a JEOL JEM-1400 (JEOL UK,Welwyn Garden City, UK) TEMfittedwith an AMT XR60 digital camera (Advanced Microscopy Techniques,Woburn, MA). It was not possible to detect a clear image of VZV particlesin the specimens. Nevertheless, small bacteria aggregates were obviousinside the canal space and within the resorptive cavity (Fig. 3).
ReviewThe patient was reviewed 1 year postoperatively. There were no
clinical signs or symptoms. Radiographs showed a reduction in sizeof the periapical radiolucencies in all the treated teeth except for themesial root of tooth #30. The mesiolingual and mesiobuccal canalswere blocked or ledged from the previous root canal treatment andcould not be negotiated to the full working length during the root canalretreatment. Therefore, apical surgery of the mesial root of tooth #30was subsequently performed (Fig. 4A–E).
DiscussionThe role of viruses in the development of apical periodontitis and
endodontic disease in general has not been fully investigated. Moleculartechniques detect the presence of viable and nonviable genetic material,and their use has significantly improved our understanding of endodon-tic infections. Recently, it has been reported that other microorganismssuch as fungi, archea, and viruses can coinhabit the root canal and peri-apical tissues with bacteria (11, 12, 14, 15, 32, 33).
JOE — Volume 42, Number 6, June 2016
Herpesviruses have been isolated from symptomatic and asymp-tomatic periapical tissues. Several viral pathogenicity mechanismshave been proposed in the past, but the most common is via an indirectroute. The primary bacterial infection of the root canal results in peri-apical inflammation and the recruitment of immune cells infected withlatent herpes virus. The herpes virus is subsequently reactivated andresults in a local immunosuppression that allows overgrowth of thepathogenic bacteria apically (14).
A direct link has also been hypothesized; the virus infects the tri-geminal nerve endings in the dental pulp leading to infection, infarction,and necrosis of the pulpal vasculature (34). It may also have cytopathiceffects on periapical tissue, resulting in impaired turnover and repair.This could result in loss of bone and potentially result in the formationof a radiolucency (35). This case report suggests a direct mechanism ofpulp necrosis and periapical inflammation is credible.
To our knowledge, this is the first case to use molecular methodsto detect VZV in the root canal system and show that apical periodon-titis can develop in the absence of bacteria. The root canal space oftooth #31 gave 2 positive qPCR tests for the presence of VZV, negativeaerobic and anaerobic cultures, and qPCR for the presence of bacte-ria. This confirms that a direct link may exist and that VZV can causeapical periodontitis without the presence of bacteria. The root canalsystem of tooth #27 was positive for VZV and cultured positive for bac-teria. We expected to detect bacteria in tooth #27 because of thecommunication between the root canal system and the oral cavitycaused by the ECR.
PCR is highly sensitive technique and requires a few DNA seg-ments per mL to give a positive result. A threshold value is requiredto ensure false-positive results are rejected. The detection of VZVDNA is based on a real-time PCR. Therefore, this technique monitorsthe amplification of specific VZV genomic DNA sequences during thePCR process.
A qualitative PCR cannot precisely quantify the amount of viral DNApresent. However, if the viral DNA is detected earlier in the replicationprocess (ie, lower CT), it indicates a higher viral load. The necrotictissue samples taken from teeth #27 and #31 showed a low CT, indi-cating a strong positive result for the presence of VZV.
The apparent discrepancy between PCR molecular analysis andelectron microscopy may be explained by the physical ‘‘state’’ of thevirus particles. PCR can detect viral nucleic acid even if it is no longerin a virus particle. However, transmission electron microscopy can onlyidentify virus particles if they are relatively intact. Furthermore, TEManalysis has a relatively low sensitivity (105–106 particles/mL)compared with most other detection methods (36).
Apical Radiolucencies and Varicella Zoster Virus 981
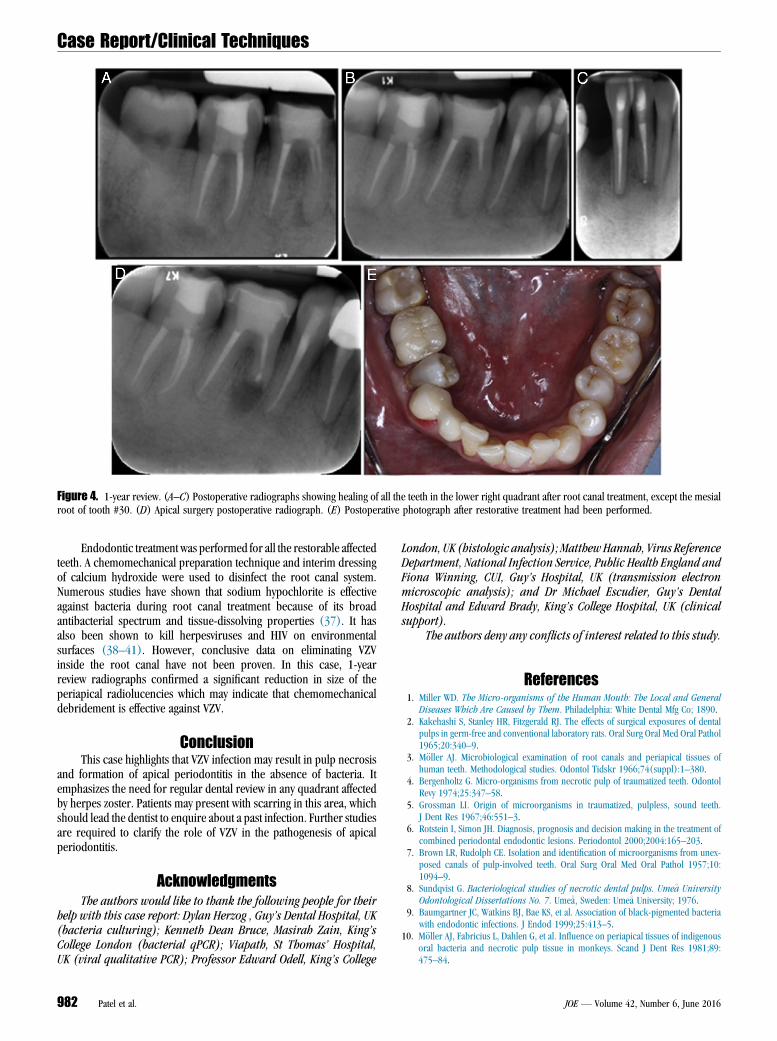
Figure 4. 1-year review. (A–C) Postoperative radiographs showing healing of all the teeth in the lower right quadrant after root canal treatment, except the mesialroot of tooth #30. (D) Apical surgery postoperative radiograph. (E) Postoperative photograph after restorative treatment had been performed.
Case Report/Clinical Techniques
Endodontic treatment was performed for all the restorable affectedteeth. A chemomechanical preparation technique and interim dressingof calcium hydroxide were used to disinfect the root canal system.Numerous studies have shown that sodium hypochlorite is effectiveagainst bacteria during root canal treatment because of its broadantibacterial spectrum and tissue-dissolving properties (37). It hasalso been shown to kill herpesviruses and HIV on environmentalsurfaces (38–41). However, conclusive data on eliminating VZVinside the root canal have not been proven. In this case, 1-yearreview radiographs confirmed a significant reduction in size of theperiapical radiolucencies which may indicate that chemomechanicaldebridement is effective against VZV.
ConclusionThis case highlights that VZV infection may result in pulp necrosis
and formation of apical periodontitis in the absence of bacteria. Itemphasizes the need for regular dental review in any quadrant affectedby herpes zoster. Patients may present with scarring in this area, whichshould lead the dentist to enquire about a past infection. Further studiesare required to clarify the role of VZV in the pathogenesis of apicalperiodontitis.
AcknowledgmentsThe authors would like to thank the following people for their
help with this case report: Dylan Herzog , Guy’s Dental Hospital, UK(bacteria culturing); Kenneth Dean Bruce, Masirah Zain, King’sCollege London (bacterial qPCR); Viapath, St Thomas’ Hospital,UK (viral qualitative PCR); Professor Edward Odell, King’s College
982 Patel et al.
London, UK (histologic analysis); Matthew Hannah, Virus ReferenceDepartment, National Infection Service, Public Health England andFiona Winning, CUI, Guy’s Hospital, UK (transmission electronmicroscopic analysis); and Dr Michael Escudier, Guy’s DentalHospital and Edward Brady, King’s College Hospital, UK (clinicalsupport).
The authors deny any conflicts of interest related to this study.
References1. Miller WD. The Micro-organisms of the Human Mouth: The Local and General
Diseases Which Are Caused by Them. Philadelphia: White Dental Mfg Co; 1890.2. Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposures of dental
pulps in germ-free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol1965;20:340–9.
3. M€oller AJ. Microbiological examination of root canals and periapical tissues ofhuman teeth. Methodological studies. Odontol Tidskr 1966;74(suppl):1–380.
4. Bergenholtz G. Micro-organisms from necrotic pulp of traumatized teeth. OdontolRevy 1974;25:347–58.
5. Grossman LI. Origin of microorganisms in traumatized, pulpless, sound teeth.J Dent Res 1967;46:551–3.
6. Rotstein I, Simon JH. Diagnosis, prognosis and decision making in the treatment ofcombined periodontal endodontic lesions. Periodontol 2000;2004:165–203.
7. Brown LR, Rudolph CE. Isolation and identification of microorganisms from unex-posed canals of pulp-involved teeth. Oral Surg Oral Med Oral Pathol 1957;10:1094–9.
8. Sundqvist G. Bacteriological studies of necrotic dental pulps. Ume�a UniversityOdontological Dissertations No. 7. Ume�a, Sweden: Ume�a University; 1976.
9. Baumgartner JC, Watkins BJ, Bae KS, et al. Association of black-pigmented bacteriawith endodontic infections. J Endod 1999;25:413–5.
10. M€oller AJ, Fabricius L, Dahlen G, et al. Influence on periapical tissues of indigenousoral bacteria and necrotic pulp tissue in monkeys. Scand J Dent Res 1981;89:475–84.
JOE — Volume 42, Number 6, June 2016

Case Report/Clinical Techniques
11. Waltimo TM, Sir�en EK, Torkko HL, et al. Fungi in therapy-resistant apical periodon-titis. Int Endod J 1997;30:96–101.12. Li H, Chen V, Chen Y, et al. Herpesviruses in endodontic pathoses: association of
Epstein-Barr virus with irreversible pulpitis and apical periodontitis. J Endod2009;35:23–9.
13. Ferreira DC, Paiva SS, Carmo FL, et al. Identification of herpesviruses types 1 to 8and human papillomavirus in acute apical abscesses. J Endod 2011;37:10–6.
14. Ferreira DC, Rocas IN, Paiva SS, et al. Viral-bacterial associations in acute apicalabscesses. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;112:264–71.
15. Kumar J, Sharma R, Sharma M, et al. Presence of Candida albicans in root canals ofteeth with apical periodontitis and evaluation of their possible role in failure of end-odontic treatment. J Int Oral Health 2015;7:42–5.
16. Slots J, Nowzari H, Sabeti M. Cytomegalovirus infection in symptomatic periapicalpathosis. Int Endod J 2004;37:519–24.
17. Jakovljevic A, Andric M, Knezevic A, et al. Human cytomegalovirus and epstein-barrvirus genotypes in apical periodontitis lesions. J Endod 2015;41:1847–51.
18. Sabeti M, Valles Y, Nowzari H, et al. Cytomegalovirus and Epstein–Barr virus DNAtranscription in endodontic symptomatic lesions. Oral Microbiol Immunol 2003;18:104–8.
19. Sabeti M, Slots J. Herpesviral-bacterial coinfection in periapical pathosis. J Endod2004;30:69–72.
20. Saboia-Dantas CJ, Coutrin de Toledo LF, Sampaio-Filho HR, et al. Herpesviruses inasymptomatic apical periodontitis lesions: an immunohistochemical approach. OralMicrobiol Immunol 2007;22:320–5.
21. Zerboni L, Sen N, Oliver SL, et al. Molecular mechanisms of varicella zoster viruspathogenesis. Nat Rev Microbiol 2014;12:197–210.
22. Slots J, Sabeti M, Simon JH. Herpesviruses in periapical pathosis: an etiopathogenicrelationship? Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;96:327–31.
23. Gilden D, Mahalingam R, Nagel MA, et al. Review: the neurobiology of varicellazoster virus infection. Neuropathol Appl Neurobiol 2011;37:441–63.
24. Millar EP, Troulis MJ. Herpes zoster of the trigeminal nerve: the dentist’s role indiagnosis and management. J Can Dent Assoc 1994;60:450–3.
25. Cohen JI. Clinical practice: herpes zoster. N Engl J Med 2013;369:255–63.26. Gregory WB Jr, Brooks LE, Penick EC. Herpes zoster associated with pulpless teeth.
J Endod 1975;1:32–5.
JOE — Volume 42, Number 6, June 2016
27. Goon WW, Jacobsen PL. Prodromal odontalgia and multiple devitalized teeth causedby a herpes zoster infection of the trigeminal nerve: report of case. J Am Dent Assoc1988;116:500–4.
28. Schwartz O, Kvorning SA. Tooth exfoliation, osteonecrosis of the jaw and neuralgiafollowing herpes zoster of the trigeminal nerve. Int J Oral Surg 1982;1:364–71.
29. Solomon CS, Coffiner MO, Chalfin HE. Herpes zoster revisited: implicated in rootresorption. J Endod 1986;12:210–3.
30. Ramchandani PL, Mellor TK. Herpes zoster associated with tooth resorption andperiapical lesions. Br J Oral Maxillofac Surg 2007;45:71–3.
31. Niazi SA, Clarke D, Do T, et al. Propionibacterium acnes and Staphylococcusepidermidis isolated from refractory endodontic lesions are opportunistic patho-gens. J Clin Microbiol 2010;48:3859–69.
32. Vianna ME, Conrads G, Gomes BP, et al. Identification and quantification of archaeainvolved in primary endodontic infections. J Clin Microbiol 2006;44:1274–82.
33. Vickerman MM, Brossard KA, Funk DB, et al. Phylogenetic analysis of bacterial andarchaeal species in symptomatic and asymptomatic endodontic infections. J MedMicrobiol 2007;56:110–8.
34. Tidwell E, Hutson B, Burkhart N, et al. Herpes zoster of the trigeminal nerve thirdbranch: a case report and review of the literature. Int Endod J 1999;32:61–6.
35. Contreras A, Slots J. Herpesviruses in human periodontal disease. J Periodontal Res2000;35:3–16.
36. Schramlov�a J, Arientov�a S, Hul�ınsk�a D. The role of electron microscopy in the rapiddiagnosis of viral infections–review. Folia Microbiol (Praha) 2010;55:88–101.
37. Zehnder M. Root canal irrigants. J Endod 2006;32:389–98.38. Bloomfield SF, Smith-Burchnell CA, Dalgleish AG. Evaluation of hypochlorite-
releasing disinfectants against the human immunodeficiency virus (HIV). J HospInfect 1990;15:273–8.
39. Rutala WA, Weber DJ. Uses of inorganic hypochlorite (bleach) in health-care facil-ities. Clin Microbiol Rev 1997;10:597–610.
40. Rutala WA, Weber DJ. Infection control: the role of disinfection and sterilization.J Hosp Infect 1999;43:S43–55.
41. Sanekata T, Fukuda T, Miura T, et al. Evaluation of the antiviral activity of chlorinedioxide and sodium hypochlorite against feline calicivirus, human influenza virus,measles virus, canine distemper virus, human herpesvirus, human adenovirus,canine adenovirus and canine parvovirus. Biocontrol Sci 2010;15:45–9.
Apical Radiolucencies and Varicella Zoster Virus 983





























