-
8/13/2019 Multilevel Factor Analytic Models
1/21
-
8/13/2019 Multilevel Factor Analytic Models
2/21
238 L. Diya, B. Li, K. Van den Heede, W. Sermeus and E.
Lesaffre
are used as proxies of these constructs; for instance a single
adverse event, say mortality, can
be used to represent patient safety. However, univariate
analyses fall short in addressing the
multi-dimensional facets of most healthcare measures (Diya et
al., 2011); hence multivariate
responses can be used. The relationship between a multivariate
response vector and covariates
of interest can then be established by using a multivariate
analysis. A special kind of multivariate
analysis which is gaining ground in the field of health outcomes
and nursing research is factoranalysis (FA) (Lake, 2002; Bruyneelet
al., 2009; Gajewskiet al., 2010). FA is used to quantify
the relationship between a multivariate response vector and a
latent construct (or its domains),
i.e. in an FA model the multivariate response vector is
regressed on latent variables and covari-
ates. Examples of the use of FA can be found in nursing research
(Lake, 2002), bioinformatics
(Hochreiteret al., 2006), psychology (Norris and Lecavalier,
2010) and educational research
(Naicker, 2010).
In this paper the healthcare measure of interest is patient
safety. Patient safety is defined as
the absence of the potential for, or occurrence of, health care
associated injuries to patients that occursby avoiding medical
errors as well as by taking actions to prevent errors from causing
injury
(Agency for Healthcare Research and Quality, 2004). Since
patient safety is a latent construct,
nurse-reported adverse events obtained from the Belgian chapter
of the Europe Nurses Forecast-
ing Survey will be used as its proxy. Adverse events are
injuries caused by medical management
rather than by the underlying disease conditions (Van den Heede,
2008). In the survey several
adverse events are recorded from nurses (nested within nursing
units within hospitals), i.e. not
only do we have multivariate responses but also the data are
multilevel in structure. Neglecting
the multilevel structure of the data in the analysis can be
problematic since the fundamental
independence assumption underlying many commonly used
statistical techniques, including FA
techniques, is violated (Goldstein and McDonald, 1988). When the
degree of dependence is sub-
stantial, violation of the independence assumption biases
parameter estimates (and standarderrors) and affects the power of
statistical tests (Bliese and Hanges, 2004; Kenny and Judd,
1986). Using wrongly single-level FA may lead to the atomistic
fallacy, which is incorrectly
assuming that the relationship between variables observed at the
observational level also holds
at the cluster level. Aggregating the data at the cluster level
does lead to independent observa-
tions but at the risk of committing the ecological fallacy,
which is incorrectly assuming that the
relationship between variables at the cluster level also holds
at the observational level (Robinson,
1950). So, to minimize the chances of these fallacies and to
attain valid inferences for multilevel
data, models which take the multilevel structure of the data
into account should be considered
(Longford and Muthen, 1992; Ansari and Jedidi, 2000; Goldstein
and Browne, 2005; Grilli and
Rampichini, 2007). Another consequence of neglecting the
multilevel structure of the data inFA is that an invalid factor
structure can be proposed and the interpretation of the
inferences
in FA is level dependent.
It might be useful to check that there is a multilevel structure
in the data before embarking
on the more complex multilevel FA modelling. Univariate
techniques such as the intraclass
correlation coefficient ICC or the F-discrepancy measure that
was proposed by Yan and
Sedransky (2007), in a Bayesian context, can be used to verify
the multilevel structure quickly.
ICC is the ratio of the variation between the clusters (level 2
units) and the total variation of
the observed or latent (for categorical observed responses)
response. ICC-values range from
0 to 1 with larger values indicating greater variability between
clusters compared with within-
cluster variability. As a rule of thumb, when a response has
ICC>0:10 then we can argue that
there is enough level 2 variability to warrant a multilevel
analysis (Dyer et al., 2005; Gajewski
et al., 2010). The F-discrepancy measure that was proposed by
Yan and Sedransky (2007)
-
8/13/2019 Multilevel Factor Analytic Models
3/21
Multilevel Factor Analytic Models 239
uses analysis-of-variance (ANOVA) concepts in a Bayesian context
to diagnose the need to
account for a hierarchical structure. This tool may be more
interesting in multilevel data sets
like the Europe Nurse Forecasting Survey data with more than two
levels of analysis. However,
in the nurse survey data interest is on a multivariate response;
hence the F-discrepancy mea-
sure neglects the dependence between responses. We propose here
to extend this measure to the
multivariate setting by making use of multivariate
analysis-of-variance (MANOVA) concepts.The objective of this paper
is to fit a multilevel FA model to establish the relationship
between
patient safety and nurse-reported adverse events from the
Belgian nurse survey data, and to
develop Bayesian diagnostic techniques for detecting
hierarchical structures in multivariate
data sets.
The remainder of this paper is organized as follows. Section 2
describes the Europe Nurse
Forecasting Survey data set, with particular emphasis on the
Belgian chapter. A brief review
of FA is presented in Section 3 and in Section 4 model checking
is presented. In Section 5 the
application of the Bayesian diagnostic techniques on the Belgian
nurse survey data is presented.
The paper ends with a discussion in Section 6. Details
pertaining to a simulation study to com-
pare the MANOVA and the ANOVA discrepancy measures, and details
of the modelling fittingfor FA models (MPLUS and JAGS codes) are
provided in the on-line supplemental document
and available from
http://www.blackwellpublishing.com/rss
2. The Europe Nurse Forecasting Survey data set
The Europe Nurse Forecasting project aims at introducing
innovative forecasting methods by
addressing not only volumes but also quality of staff and its
effect on patient care. The project
involves researchers from 12 European countries, the USA, China,
South Africa and Botswana.
Data collection was only done in 12 European countries, namely
Belgium, Finland, Germany,Greece, Ireland, Poland, Spain, Sweden,
Switzerland, the Netherlands, the UK and Norway.
Most of the data were collected in 2009 and 2010.
In the project two multicountry surveys were conducted, namely
the nurse survey and patient
satisfaction survey. Hospital discharge data were also
collected. The various data sets were
targeted at investigating how nursing qualifications,
demographics, workload, wellbeing and
practice environment can affect productivity, patient safety and
patient outcomes.
This research focuses on the Belgian chapter of the nurse survey
data. It contains information
about the nature of a nurses job (e.g. nursephysician
relationships), quality and safety issues,
the nurses most recent shift and demographics. The nurse survey
seeks to establish the perception
of nurses with regard to their work conditions and their
relationship with either patients or otherhealthcare professionals.
In particular the focus is on relating nurse-reported adverse
events to
the characteristics of the nurse, nursing unit and hospital.
The main question that we looked at here was How often would you
say each of the fol-
lowing incidents occurs involving you or your patients?. For
this question six incidents were
considered:
(a) patients received the wrong medication, time or dose,
(b) pressure ulcers after admission,
(c) patient falls with injury,
(d) urinary tract infections,(e) bloodstream infections and
(f) pneumonia.
-
8/13/2019 Multilevel Factor Analytic Models
4/21
240 L. Diya, B. Li, K. Van den Heede, W. Sermeus and E.
Lesaffre
The main question (for each incident type) had seven potential
answers measured on a
Likert scale, i.e. 0, never, 1, a few times a year or less, 2,
once a month or less, 3, a few
times a month, 4, once a week, 5, a few times a week, and 6,
every day. In this paper new
responses were generated by discretizing the Likert-scaled
variables because of software con-
siderations. (It is currently not feasible to implement the
proposed latent variable or data
augmentation approach for categorical responses with more than
two categories in JAGS.)A nurse was judged to have indicated that
his or her nursing unit had a substantial num-
ber of events if he or she selected the values greater than 2.
This led to binary responses,
namely
(a) wrong medication, time or dose (wrong),
(b) pressure ulcers (pressure),
(c) patient falls with injury (falls),
(d) urinary tract infections (uti),
(e) bloodstream infections (infections) and
(f) pneumonia.
The data that are considered here are multilevel in structure,
i.e. nurses are nested within
nursing units which are in turn nested within hospitals. The
data consisted of 3151 nurses
from 269 nursing units in 66 hospitals. 23 and 43 hospitals
respectively were and were not
technologically advanced and four and 62 hospitals respectively
were and were not univer-
sity hospitals. Of the 269 nursing units, 112 were surgical
units, 125 were medical units and
32 were mixed surgical and medical units. Of the nurses who
responded to the nurse survey,
1333 worked in surgical units, 1471 worked in the medical units
and 347 worked in mixed
surgicalmedical units. 2167 of the nurses reported Flemish as
their language of communica-
tion whereas 984 reported French. The covariates of interest in
this paper were measured at
the nurse level, nursing unit level and hospital level. At the
hospital level the covariates werethe number of beds (beds),
whether the hospital is technologically advanced (tech = 1;
other-
wise tech = 0) and whether the hospital was a university
hospital (university = 1; otherwise
university = 0). At the nursing unit level the covariate of
interest was the unit specification (1,
surgical, 2, medical, and 3, mixed). At the nurse level the
covariates considered were gender
(male = 1 if gender is male; 0 otherwise), age, time in years as
a registered nurse (expn), time
in years at the current hospital (exph), language (language = 1
if Flemish; 0 otherwise) and
whether a nurse was satisfied with his or her career choice
(satisfied = 1 if a nurse was satisfied;
0 otherwise).
In this paper we shall focus on the nurse and the nursing unit
level. The hospital level (third
level) is dropped because empirical evidence did not support its
inclusion, i.e. there was lowvariability at the hospital level; see
Section 5.2.2. Thus the role of hospitals is explored in a
non-hierarchical way.
3. Factor analysis models
3.1. Single-level factor analysis
We first consider a single-level FA model for continuous
responses. Let Yj= .Yj1, . . . ,Yjp/be a
p-dimensional continuous response vector forthejth individual
(j=1 , . . . ,N),Fj= .Fj1, . . . ,Fjk/
be a k-dimensional (kp) vector of latent constructs and be
apkmatrix of factor loadings;
then the single-level FA model can be written as
Yj=j+Fj+j, .1/
-
8/13/2019 Multilevel Factor Analytic Models
5/21
Multilevel Factor Analytic Models 241
where j= .j1, . . . ,jp/ is the mean vector, the common factors
are multivariate normally
distributed with mean 0 and covariance matrix .FjNk.0,// and the
unique factors are
multivariate normally distributed with mean 0 and covariance
matrix (jNp.0,/). Note
that the mean of thesth (s=1 , . . . ,p) responseYjs can be
modelled as a function of covariates,
i.e. js=Xjs. Factor loadings (elements of) are parameters which
relate the unobserved
factors to the observed responses, i.e., the larger the value of
a factor loading, the more thecorresponding response is said to
load on the corresponding factor. Factor loadings are allowed
to vary across survey items but not across individuals. Assuming
orthogonality of all common
and unique factors, the marginal covariance matrix is given by
var.Yj/=U=+, i.e.
the observed covariances matrix can be decomposed into a
component that is attributable to
the underlying factors and measurement error.
Two special cases of FA are
(a) ifFjis known then the FA model can be viewed as a
multivariate regression model with
the factor loadings playing the role of regression coefficients
and
(b) if the factor loadings are known then the FA model is
equivalent to a two-level random-
slope model.
There are two modes of FA, namely exploratory FA (EFA) and
confirmatory FA (CFA).
EFA is used when there is no a priori information about the
factor structure, i.e. choosing
the number of factors, k, and establishing the variables that
are related to a given factor
domain. In that case all factor loadings are free parameters. In
both the frequentist and
the Bayesian contexts, EFA can be done by fitting several models
with varying numbers of
factors and using goodness-of-fit indices (discrepancy measures)
to select the best model (see
Section 4.2). In a Bayesian context, Lopes and West (2004)
advocated the use of the reversible
jump Markov chain Monte Carlo (MCMC) approach. The ultimate
objective of EFA is to
come up with the best factor structure for a given data set. In
contrast, CFA is used tovalidate a priori hypothesized factor
structures. In the literature, the most common CFA
structure is the simple factor structure, i.e. the factor
loadings are allowed to load on one
and only one latent construct and all the other factor loadings
(cross-loadings) are set equal to
0.
The above FA model caters for continuous responses assumed to be
multivariate normally
distributed. For categorical or binary responses, we could
assume that they are discretized
versions of latent Gaussian variables, i.e. consider the binary
response vector given by Yj; then
Yjs = I.Yjs>0/ where Y
js, s= 1 , . . . ,p, is a latent Gaussian response. For
identifiability, the
variance of the error term ("js) for the sth response, ss, is
set to 1 such that all the diago-
nal elements of are 1. The matrix is called the polychoric or
tetrachoric correlation matrixas it is the correlation matrix of
the underlying latent Gaussian responses.
Additional constraints are required for both categorical and
continuous response FA models
to be identifiable. For instance, for the single-level FA in
equation (1) there arep.p+1/=2 unique
elements in but as many aspk+k.k+1/=2+p.p+1/=2 elements in+,
implying that
there are more parameters to estimate than availableinformation.
In this paper we shall constrain
the measurement error for different responses to be independent
(off-diagonal elements of
equal to 0) and the common factors to be orthogonal. In CFA, an
additional constraint that is
employed is to adopt a simple factor structure, i.e. a variable
loads on only one factor, whereas
in an EFA this constraint is relaxed.
FA models can be fitted by using maximum likelihood estimation
or (robust) weighted least
squares estimation; see Longford (1993). From equation (1), the
total marginal likelihood of
the data is
-
8/13/2019 Multilevel Factor Analytic Models
6/21
242 L. Diya, B. Li, K. Van den Heede, W. Sermeus and E.
Lesaffre
L.,,,|Y/=
.2/pN=2|U|
N=2 exp
1
2
Nj=1
.Yj/1U .Yj/
f.Fj/dFj, .2/
where=X. For binary or categorical data the (latent) tetrachoric
or polychoric correlation
matrix can be used. Computational strategies for obtaining
maximum likelihood estimates have
been discussed in Mardia et al. (1979) and Lawley and Maxwell
(1971). Another estimationtechnique which can be used is weighted
least squares.
Alternatively, one could estimate the parameters of FA models by
using the Bayesian
approach. Estimation is done via sampling using MCMC techniques.
In the Bayesian approach
the likelihood is combined with prior information to obtain the
posterior distribution of the
parameters of interest, i.e.
p.,,,|Y/L.,,,|Y/p.,,,/, .3/
where p.,,,/ is the prior distribution. For an FA on binary
responses, we used in this
paper the latent variable technique called the data augmentation
approach (Albert and Chib,
1993; Azevedo etal., 2011), where a latent Gaussianresponse
vector is assumed that is discretized
to yield the binary responses. The complete marginal data
likelihood function for the binary
single-level FA model is given by
L.,,,|Y/
Nj=1
ps=1
.Yjs;js; 1/.Y
js|Yjs/f.Fj/f.Y
/dFjdY, .4/
where
.Yjs|Yjs/= I.Yjs>0/I.Yjs=1/+ I.Yjs0/
I.Yjs=0/
is the conditional likelihood..Yjs;js; 1/ represents the value
of the normal probability density,
with meanjs and standard deviation SD= 1, at the point Yjs
with
js being the conditional
mean, i.e. js = js + sFj, where s is the sth row of. Note that
the distribution of the
multivariate response vector can now be presented as a product
of univariate distributions
because responses are conditional independent (conditional on
the common factor).
The EFA models in this paper used the frequentist approach and
were implemented by using
MPLUS (Muthen and Muthen, 2011). A frequentist approach was
necessary since methods
for Bayesian covariance selection are scarce and computationally
intense. CFA models can be
easily fitted by using both the frequentist and the Bayesian
approaches (using link functions) in
MPLUS. However, these CFA models are restricted in term of
flexibility. Hence, the CFA modelsin this paper were fitted by
using the Bayesian approach, i.e. we used the data augmentation
approach called the latent variable approach in JAGS (Plummer,
2003). In particular, JAGS
was run from R (R Development Core Team, 2012) by using the
R2jags (Su and Yajima, 2012)
package. The R packageCODAwas used to assess MCMC convergence
(Plummeret al., 2006).
In this paper we restricted the convergence diagnosis to the
trace plots and the Gelman, Brooks
and Rubin diagnostic R. The quick mixing of MCMC chains and
values ofR close to 1 (say
R
-
8/13/2019 Multilevel Factor Analytic Models
7/21
Multilevel Factor Analytic Models 243
in a CFA the cross-loadings can be given priors concentrated
around 0 instead of fixing them
to 0.
The data augmentation approach has interesting features because
it replaces the binary
response with a latent continuous response; therefore
statistical techniques which are used for
continuous responses can be applied to the latent continuous
response. In addition, it allows
quite general link functions by replacing the classical link
functions (e.g. normal distributions(probit link)) by quite general
forms of distributions (e.g. skewed normal distributions).
3.2. Multilevel factor analysis
When the data have a multilevel structure, multilevel FA
approaches are needed. This implies
that the multivariate continuous response vector for an
individual has attributes emanating
from the observational and the cluster levels. Let Yij= .Yij1, .
. . ,Yijp/ be a p-dimensional
continuous response vector for the jth individual (j= 1 , . . .
,ni) in cluster i (i= 1 , . . . ,m),
F.1/ij = .F
.1/ij1 , . . . ,F
.1/ijk1
/be ak1-dimensional (k1p) vector of latent constructs at level
1,F.2/i =
.F.2/
i1, . . . ,F
.2/
ik2/ be a k
2-dimensional (k
2p) vector of latent constructs at level 2,.1/ be a pk
1matrix of factor loadings at level 1 and.2/ be apk2matrix of
factor loadings at level 2; then
the multilevel FA model is given by
Yij=ij+.1/F.1/ij +
.1/ij +
.2/F.2/i +
.2/i , .5/
where ij is the mean vector. The vector of unique factors or
measurement errors at the
observational level is multivariate normally distributed with
mean 0 and variance .1/ (.1/ij
Np.0,.1//), the vector of unique factors or measurement errors
at the cluster level is multi-
variate normally distributed with mean 0 and variance .2/ (.2/i
Np.0,
.2//), the vector of
common factors at the observational level is multivariate
normally distributed with mean 0
and variance .1/
(F
.1/
ij Nk1.0,.1/
/) and the vector of common factors at the cluster levelis
multivariate normally distributed with mean 0 and variance
.2/(F
.2/i Nk1.0,
.2//).
Assuming orthogonality of all common and unique factors, the
marginal covariance matrix
consists of a within and between component, var.Yij/=M=W +B. The
within-covariance
matrix is given by W =.1/
.1/
.1/+.1/ and the between-covariance matrix is given by
B =.2/
.2/
.2/+.2/. Note that both the within and the between covariances
have a com-
ponent coming from the common factors (factor scores) and unique
factors (measurement
errors or random effects). Multilevel FA can be estimated by
using the frequentist approach
but this requires multi-dimensional integration to obtain a
marginal likelihood which will then
be optimized to obtain parameters of interest. The Bayesian
approach will bypass the multi-
dimensionalintegration by usingsampling-based algorithms(Ansari
and Jedidi, 2000; Goldsteinand Browne, 2005).
4. Model checking
After the model has been fitted it is necessary to monitor the
quality of the statistical model. This
implies that we are interested in detecting whether there are
any systematic differences between
the model and the observed data. In a frequentist context this
entails checking whether certain
functions of the data, test statistics, follow the distribution
that is implied by the model. In a
Bayesian context, posterior predictive checks (PPCs) are used.
PPCs are obtained by generating
replicated data sets from the posterior predictive distribution
of the fitted model (Gelmanet al.,
2004). These data sets are then compared with the observed data
set with respect to the feature of
interest by using discrepancy measures. We first discuss how to
check for the multilevel structure
-
8/13/2019 Multilevel Factor Analytic Models
8/21
244 L. Diya, B. Li, K. Van den Heede, W. Sermeus and E.
Lesaffre
in Section 4.1, followed by model assessment (e.g. normality of
both the common and the unique
factors, and the orthogonality of the common and unique factors)
in Section 4.2.
4.1. Detecting the multilevel structure
The ICC-values can be used to assess informally whether there is
substantial dependence to
warrant the use of multilevel models. In contrast, Yan and
Sedransky (2007) proposed a Bayesian
approach for checking a multilevel structure in the data by
making use of anF-statistic inspired
by classical ANOVA concepts. When there are two or more
responses the approach of Yan and
Sedransky (2007) neglects to take the dependence between
responses into account, thus leading
to a reduction in power to detect hierarchical structures. We
propose the use of diagnostic checks
based on MANOVA.
To test for the independence assumption (no hierarchical
structure) the relative sizes of the
between (or total) and within sums of squares and cross-products
are considered. In a frequentist
context, the following test statistics are considered:
(a) the LawleyHotelling trace,LH = tr.BW1/;
(b) Pillais trace,PT = tr.BT1/;
(c) Wilks , WL =|W|=|T|.
Here the total, between and within sums of squares and
cross-products are given by T=
mi=1
nij=1 .Yij
Y/.YijY/ ,B=mi=1ni.Yi
Y/.YiY/ andW=mi=1
nij=1.Yij
Yi/.Yij
Yi/ respectively.
Assuming multivariate normality of the responses, all test
statistics are asymptotically equiv-
alent. When comparing two clusters all the test statistics
reduce to a statistic which follows a
Hotelling T2 sampling distribution. Wilks WL is the most
frequently used MANOVA test
statistic as it is related to the likelihood ratio criterion and
its exact sampling distribution
can be derived for some special cases; for example see chapter 6
of Johnson and Wichern(2002).
In this paper we propose to use these test statistics as
discrepancy measures in a Bayesian
context. The posterior predictiveP- (PPP-) values for the three
multivariate discrepancies are
computed by taking the proportion of times that the predicted
discrepancy exceeds the observed
discrepancy. If only the data structure is misspecified and not
other model assumptions then
our approach does indeed diagnose the hierarchical structure. In
cases where other model
assumptions do not hold then the discrepancy measures proposed
might indicate a statistically
important difference even when the between-cluster variability
is low. In such cases our
approach acts as a global goodness-of-fit check. Caution must be
exercised when using PPCs
or PPP-values since the data are used twice, i.e. in fitting the
model and in model checking,hence leading to some degree of bias
(Bayarri and Castellanos, 2004). This can be avoided by
using a learning and a validation data set, where the learning
data set is used to estimate the
model and a validation data set is used to assess the model fit.
We employed this approach in
this paper.
The approach proposed can be applied only to continuous
multivariate responses. It cannot
be directly applied to categorical multivariate responses, i.e.
when using link functions, but it
can be applied to the latent continuous response vector when the
data augmentation approach
is used.
4.2. Model assessment
After having checked the multilevel structure in the data, we
can either select the single-level
-
8/13/2019 Multilevel Factor Analytic Models
9/21
Multilevel Factor Analytic Models 245
or multilevel FA depending on the evidence that is presented.
The next step entails model
assessment, for instance checking the normality assumption of
both the common and the unique
factors, and validating the orthogonality assumption. In this
paper we shall adhere to global
model checks using PPCs in a Bayesian context and variants of
the 2 likelihood ratio statistic
in the frequentist context.
Recall that the general goal of an FA model is to test the
hypothesis that the observed covari-ance matrix is equal to the
model-based covariance matrix, i.e.
S=./, .6/
where S represents the covariance matrix of the observed
response vector (a latent continu-
ous response vector for categorical data) and ./ represents the
model-based covariance
matrix.
In a frequentist context, a multitude of goodness-of-fit indices
have been proposed. In this
paper we shall look at three indices which are functions of the
2 likelihood ratio statistic, i.e.
the2 likelihood ratio statistic, the comparative fit index CFI
(Bentler, 1990) and the Tucker
Lewis index TLI (Tucker and Lewis, 1973) and two indices which
are based on how well agiven model approximates the true model,
i.e. the root mean square of approximation RMSEA
(Browne and Cudeck, 1992; Steiger and Lind, 1980) and the
standardized root-mean-square
residual SRMSR. These indices check whether the model-based
covariance matrix is close to
the covariance matrix of the observed response vector. If the
model fits the data well then
(a) the2 likelihood ratio statistic should be small,
(b) both CFI and TLI should have a value 1 and
(c) RMSEA and SRMSR should be close to 0.
As a rule of thumb, a model with CFI- and TLI-values of at least
0.90 are deemed acceptable
and values of at least 0.95 are indicative of a good fit.
Alternatively, we could use RMSEA andSRMSR for which values less
than 0.08 indicate an acceptable model fit and values less than
0.05 are indicative of a good fit (Hu and Bentler, 1999).
Multiple fit indices are used because
each fit index has its own limitations and there is no agreed-on
method for evaluating whether
the lack of fit of a model is substantively important. These
indices are used for both single and
multilevel FA models.
In a Bayesian context, model assessment can focus on the
likelihood and the priors. PPCs
are used to check how well the model fits the data; however, the
discrepancy measures are now
different from those used in diagnosing the neglected
hierarchical structure. From these PPCs,
PPP-values can be computed. In this paper the2 discrepancy
measure (Gelman et al., 1996)
was used. The deviance information criterion DIC (Spiegelhalter
et al., 2002) can be used tocompare models on the basis of
different likelihood and prior specifications. The model having
the smallest DIC-value is then a good candidate; see
Spiegelhalter et al.(2002). However, this
measure can be misleading as latent variables, e.g. factor
scores and randomeffects, are treated as
parameters. This has led to numerous discussions in the
literature with no conclusive suggestions
(Celeux et al., 2006); hence we shall use the mean-square
prediction error MSPE instead. MSPE
measures how well the model fits the data and is given by
MSPE.Y/=E
mi=1
n1j=1
.Yij Yij/2
,
where Yij
is the posterior predicted response for nurse jin clusteri. Note
that all model assess-
ments are carried out on a validation data set (independent of
the learning data set that is used
to fit the model).
-
8/13/2019 Multilevel Factor Analytic Models
10/21
246 L. Diya, B. Li, K. Van den Heede, W. Sermeus and E.
Lesaffre
5. Application to Europe Nurse Forecasting Survey data
In this section, we want to establish the relationship between
the latent construct patient safety
and six nurse-reported adverse events in the Belgian chapter of
the Europe Nurse Forecasting
Survey. Hereby we wish to control for nurse, nursing unit and
hospital characteristics, i.e. nurses
are seen as informants of not only their own patient safety
record but also informants of patient
safety culture in their nursing unit. The response of interest
is a multivariate vector of nurse-
reported adverse events, i.e.Yij=.Yij1, . . . ,Yij6/whereYij1
denotes wrong medication, or dosage
or time,Yij2 denotes pressure ulcers,Yij3patient falls,Yij4
urinary tract infections,Yij5blood-
stream infections andYij6 pneumonia.
Since no a-priori-specified factor structure is proposed for the
adverse events in this paper
and patient safety, there is a need to explore the factor
structure. So, to avoid double usage of
the data, the data were equally divided into the learning and
validation data sets by using simple
random sampling (within a cluster). The factor structure was
explored by using the learning
data set and the validation data set was used in confirming the
factor structure. The learning
data set was then reused in the model assessment for the CFA
model.
EFA was implemented by using a frequentist approach by making
use of MPLUS since
the Bayesian approach is computationally intense. The Bayesian
module of MPLUS is not
sufficiently flexible to allow for the computations of the
discrepancy measures that are proposed
in this paper; hence CFA models were fitted in JAGS by
usingR2jags.
5.1. Descriptive statistics
The descriptive statistics in this section pertain to the entire
(learning plus validation) Belgian
nurse survey data. The learning and validation data sets had
similar characteristics (as they are
random samples from the entire data set).
Table 1 shows the percentage of nurse-reported adverse events,
the number of missingresponses and ICC. From Table 1, there are a
few missing values for all the responses. The most
common nurse-reported adverse event is urinary tract infection,
followed by wrong medication,
or time or dose and the least reported is patient fall
accidents. The ICC-values are all greater
than 0.1, indicating the possible need for a multilevel FA
model.
The Spearman correlation coefficient matrix of the percentages
in a nursing unit of nurse-
reported adverse events shows that there were moderate-to-high
correlations between the
nurse-reported adverse events. The largest correlation was
between bloodstream infections and
pneumonia and the smallest correlation was between wrong
medication, or time or dose and
pneumonia:
Table 1. Belgian nurse survey data:percentage of
nurse-reportedadverseeventsand ICC
Type of adverse event %adverse event Number missing ICC
Wrong medication, dose or time 20.55 70 0.11Pressure ulcers
11.60 98 0.13Falls 9.08 89 0.19Urinary tract infection 21.54 110
0.21Infection 9.66 160 0.18Pneumonia 11.40 151 0.27
Calculated for the non-missing responses.
-
8/13/2019 Multilevel Factor Analytic Models
11/21
Multilevel Factor Analytic Models 247
University hospitals were more likely to have frail patients
compared with the non-university
hospitals. Thus this might lead to a higher incidence of
nurse-reported adverse events. University
hospitals had higher numbers of nurse-reported adverse events
than non-university hospitals
except for wrong medication, or dose or time and patient fall
accidents.
5.2. Factor analysis
In this section we present the results from FA. All EFA models
(single level and multilevel) were
implemented on the learning data set by using a frequentist
approach in MPLUS. The use of
a frequentist approach here was necessitated by the fact that
methods for Bayesian covariance
selection approaches are scarce in the literature, no software
is available and these methods are
computationally intense. Since we are assuming latent Gaussian
responses and the responses are
binary a probit link was assumed and parameter estimates were
obtained by using the maximum
likelihood approach.
The Bayesian approach was used to fit all CFA models (single
level and multilevel). In
particular the latent variable approach was used, which enabled
the easy computation ofMANOVA discrepancy measures which are
instrumental in detecting hierarchical structures
in the data.
5.2.1. Single-level factor analysis
5.2.1.1. Single-level exploratory factor analysis. Here we
explored the factor structure, i.e.
the number of factors and the outcomes on which the chosen
factors load, by using EFA in
MPLUS. It is customary in EFA that one starts by aiming for a
simple factor structure and
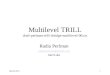
on doing a CFA modify the structure accordingly. Fig. 1(a) shows
a scree plot of the single-
level EFA. The scree plot indicates that two factors were
adequate to account for much of thevariability in the six
responses.
The two-factor solution was further supported by the results
shown in Table 2, which gives
measures of fit for various factor structures. The measures of
fit are all within acceptable limits;
see Section 4.2. Models with more than three factors were not
identifiable as the number of
parameters to estimate exceeded the available information. We
also looked at the factor loadings
to assess their classical statistical significance. On the basis
of these results and on Fig. 1(a)
and Table 2 we concluded that a two-factor solution was a
reasonably good single-level factor
structure for the Belgian nurse survey data.
Recall that, in Section 2, the responses were generated by
discretizing the Likert-scaled vari-
ables by using 2 as a cut-off point. We carried out a
sensitivity analysis by choosing other cut-off
points, i.e. 1, 3 and 4, and redoing the EFA. The proposed
factor structures for all these cut-off
points were similar to the factor structure that is presented
here. We also explored the factor
-
8/13/2019 Multilevel Factor Analytic Models
12/21
248 L. Diya, B. Li, K. Van den Heede, W. Sermeus and E.
Lesaffre
1 2 3 4 5 6
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Number of factors
Variance
(Eigenvalue)
1 2 3 4 5 6
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Number of factors
Variance
(Eigenvalue)
(a)
(b)
Fig. 1. Belgian nurse survey datascree plots for (a) the
single-level and (b) the multilevel EFA: ,within; , between
-
8/13/2019 Multilevel Factor Analytic Models
13/21
Multilevel Factor Analytic Models 249
Table 2. Belgian nurse survey data: measures of fit for
single-level EFA
Number of 2 p-value CFI TLI RMSEA SRMRfactors
1
-
8/13/2019 Multilevel Factor Analytic Models
14/21
250 L. Diya, B. Li, K. Van den Heede, W. Sermeus and E.
Lesaffre
Table 3. Belgian nurse survey data:PPP-values for discrepancy
measuresto diagnose hierarchical structures
Discrepancy PPP-value
LH 0.03PT 0.03WL 0.97
F1 0.14F2 0.58F3 0.12F4 0.12F5 0.66F6 0.29
include in the mean structure of the multilevel FA model. A
covariate was selected for inclusion
in the FA model if it was significant at the 5% level for at
least two adverse events. From this
exercise the following variables were considered:
(a) age,
(b) gender,
(c) satisfied,
(d) unit type (medical or mixed, with surgical being the
default),
(e) university hospital and
(f) beds.
For computational reasons the continuous covariates were centred
and standardized (SD=1).
5.2.2.1. Multilevel exploratory factor analysis. Using MPLUS a
frequentist two-level EFA
was fitted to the learning data set. Here, the observational
level consists of nurses who are
nested in the nursing unit (cluster level). Fig. 1(b) shows the
scree plot for the multilevel factor
analysis. The scree plot indicates that two factors are needed
at each level. The within-factor
structure remained the same as that suggested by the
single-level EFA but, for the between-
factor structure, the factor indicators wrong medication, or
time or dose and pressure ulcers
loaded on the first between-nursing unit factor whereas the
remainder of the factor indicators
loaded on the second between-nursing unit factor, as shown in
Fig. 2.
The two-factor solution was further supported by the measures of
fit for the two-factor solu-tion at both levels. The 2
goodness-of-fitp-value was 0.5887, RMSEA (and the 95%
confidence
interval) is given by 0.000 (0.000; 0.026), both CFI and TFI had
a value of 1 and the within
and between SRMR are 0.018 and 0.057 respectively. Hence all the
goodness-of-fit indices were
within acceptable limits. These goodness-of-fit statistics were
better than for any other factor
solution.
5.2.2.2. Multilevel confirmatory factor analysis. To validate
the factor structure pro-
posed (from multilevel EFA) we fitted a two-level (nurse and
nursing unit levels) CFA model,
controlling for nurse, nursing unit and hospital
characteristics, by using the data augmentation
approach in JAGS. We assumed similar priors to those for the
single-level FA in Section 5.2.1.
With regard to the variance components for the random effects we
used parameter expansion,
-
8/13/2019 Multilevel Factor Analytic Models
15/21
Multilevel Factor Analytic Models 251
Fig. 2. Belgian nurse survey data: multilevel factor
structure
i.e. we had a gamma distribution with scale and shape parameters
equal to 0.5 as the prior for
the precision and a normal distribution with mean 0 and variance
106 for the parameter ex-
pansion term. The variances of the random effects were obtained
through dividing the squared
parameter expansion term by the precision.
We considered three chains, each having 300000 MCMC iterations
(with a burn-in of 50000
iterations). We thinned the chains by selecting one in 10
iterations. Hence, values in Table 4 are
based on 25000 sampled values. (This is so for all the models in
this section, including models
used for sensitivity analysis.) The Gelman, Brooks and Rubins
diagnostics for all parameters
were less than 1.1 and the MCMC chains mixed well, hence
indicating no convergence problems.
Table 4 shows the posterior means (with SDs in parentheses) and
the 95% credible intervals forthe factor loadings and the variance
components of the second-level unique factors (random
effects).
Older nurses reported fewer adverse events than younger nurses,
except for wrong medication,
or time or dose. Male nurses reported more incidences of wrong
medication, or time or dose
than their female counterparts. Nurses who were satisfied with
their career choice reported
fewer patient fall accidents and incidences of wrong medication,
or time or dose. Flemish-
speaking nurses reported more incidences of urinary tract
infections, bloodstream infections
and pneumonia than French-speaking nurses. There were no
statistically important differences
between the reported adverse events in the surgical, medical and
mixed units.
The factor loadings that are presented here were standardized
and can be interpreted as
the correlation between the factor domain and the factor
indicators (responses), i.e. the factor
loadings when the total variability (per response) is fixed to
1. All the posterior means of
-
8/13/2019 Multilevel Factor Analytic Models
16/21
252 L. Diya, B. Li, K. Van den Heede, W. Sermeus and E.
Lesaffre
Table 4. Belgian nurse survey data: results of the multilevel
CFA model
Parameter Posterior 95% crediblemean (SD) interval
Within-level factor loadings.1/1,1
0.407 (0.053) (0.300; 0.508)
.1/1,2
0.947 (0.025) (0.889; 0.986)
.1/1,3 0.557 (0.054) (0.449; 0.659)
.1/2,4
0.828 (0.035) (0.756; 0.892)
.1/2,5 0.853 (0.037) (0.777; 0.921)
.1/2,6
0.804 (0.040) (0.722; 0.876)
Between-level factor loadings
.2/1,1
0.182 (0.098) (0.014; 0.375)
.2/1,2 0.224 (0.100) (0.023; 0.403).2/2,3
0.405 (0.102) (0.183; 0.574)
.2/2,4
0.226 (0.072) (0.082; 0.363)
.2/2,5
0.323 (0.067) (0.190; 0.450)
.2/2,6
0.381 (0.090) (0.201; 0.546)
Residual variances
21
0.117 (0.063) (0.015; 0.256)
22 1.117 (2.035) (0.012; 8.066)
23 0.226 (0.191) (0.008; 0.715)
24
1.652 (1.059) (0.453; 4.531)
25 0.199 (0.226) (0.008; 0.824)26 0.919 (0.724) (0.045;
2.786)
Fit indices
2 0.349 (0.477) (0.000; 1.000)MSPE 17206.897 (262.432)
(17030.075; 17724.202)
.v/k,s is thekth standardized factor loading for variable s at
level v.
2s is
the variance component for variable s. s: 1 denotes the wrong
medication,or time or dose; 2 denotes pressure ulcers; 3 denotes
patient falls; 4 denotesurinary tract infection; 5 denotes
bloodstream infection; 6 denotes pneumoniaresponse.
the first-level factor loadings were greater than 0.4, implying
that there was moderate-to-high
correlation between the factor domains and the factor
indicators. The nursing unit level factor
loadings were between 0.18 and 0.41. Though these factor
loadings were low to moderate they
were still statistically important. The 2 goodness-of-fit
Bayesianp-value was 0.50, suggesting
that there was no major discrepancy between the data and the
model. The model MSPE was
17206.897.
A sensitivity analysis was done by
(a) altering the common factor distribution to have a
Studentt-distribution with 4 degrees
of freedom,
(b) altering the common factor distribution to have
at-distribution with unspecified degrees
of freedom and
-
8/13/2019 Multilevel Factor Analytic Models
17/21
Multilevel Factor Analytic Models 253
(c) fixing the first factor loading instead of the factor
variance to 1.
The three models resulting from these alterations had larger
MSPE-values than the initial
multilevel FA model, i.e. the MSPE-values were 17209.677,
17207.970 and 17207.180. We also
assessed whether there was substantial variability at the
hospital level after accounting for the
nursing unit level. All the MANOVA discrepancy measures had
values that were close to 0.5,hence indicating that there was not
that much dependence between nurses in a hospital after
accounting for the nursing unit. This was used as evidence for
not extending the FA model to
three levels (hospital level, nursing unit level and nurse
level). Hence the effect of hospital was
explored in only a non-hierarchical way.
The within-factor structure was the same as that attained under
the single-level FA. The
nurse-reported adverse events wrong medication, or time or dose,
pressure ulcers and patient
fall accidents loaded on one factor whereas the remaining
nurse-reported adverse events loaded
on another factor. This implied that nurses who reported that
they encountered many incidences
of wrong medication, or time or dose were also more likely to
report high numbers of pressure
ulcers and patient fall accidents (adhering to protocol and
safety guidelines) whereas nurses
who reported that they encountered many incidences of urinary
tract infections were also more
likely to have reported many incidences of bloodstream
infections and pneumonia (hygiene or
hand hygiene). These three adverse events can also be considered
as indicators of adherence to
safety guidelines, for instance, safe handling of perfusion
lines (which if not done properly can
be a source of infection). However, these three adverse events
are not as directly related to the
nursing care process as the adverse events which load on the
first factor. We should note that the
nurses here were informants of not only their own experience but
also that of the nursing unit
at large. The between-factor structure was reflective of what
happens at the nursing unit level.
Wrong medication, or time or dose and pressure ulcers loaded on
the first nursing unit factor,
and the remainder of the adverse events loaded on the second
nursing unit factor. Clearly the
first factor is an indicator of whether the nursing unit
administers medication correctly, in time
and is attentive to the physical need of immobile patients. The
second factor is a mixture of,
for example, whether the right equipment is accorded to the
patient and the general hygiene
condition of the nursing unit.
6. Discussion
In this paper we have illustrated how to address complex
research questions by using FA. FA
models are used to relate the latent constructs to the responses
of interest, e.g. adverse events.
These models are becoming popular in many fields, especially in
health outcomes and nursingresearch where they are used to inform
policy decisions. The data that are collected in health
outcomes and nursing research are often huge and for this
reason, coupled with limitations
in available software, health outcome and nurse researchers tend
to fit single-level FA models
based on simplistic assumptions, e.g. the independence
assumption. However, most data in this
area of research are multilevel in structure; hence neglecting
the data structure in the statistical
analysis can lead to invalid inferences which might lead to
wrong policy recommendations.
Before embarking on complex multilevel FA modelling which is
computationally intense there
should be an assessment of whether there is substantial
dependence between subjects in the
same cluster. If the dependence between subjects in the same
cluster is low the inference that is
obtained from the single-level FA is more likely to be valid,
thus leading to simple conclusions,
i.e. we aim for parsimony, not only in the covariates that are
included in these models but also in
the level of analysis. However, if there is substantial
between-cluster variability, inferences from
-
8/13/2019 Multilevel Factor Analytic Models
18/21
254 L. Diya, B. Li, K. Van den Heede, W. Sermeus and E.
Lesaffre
the single-level FA will be invalid because the level of
analysis has a bearing on the interpretation
of the factor structure and the inferences coming from such a
structure.
We proposed the use of the MANOVA discrepancy measures to
address formally whether
there is substantial dependence (between-cluster variability) in
our multivariate multilevel struc-
tured data set. These measures are handy as they have more power
than the ANOVA discrepancy
measures and intraclass correlation coefficients to diagnose the
hierarchical structures. It is cru-cial that the factor structure
is correctly specified when diagnosing the hierarchical
structure
as misspecification of the factor structure implies that the
discrepancy measure proposed will
then become sensitive not only to the hierarchical structure but
also to the misspecified fac-
tor structure. Though it can be argued that all potential
models, i.e. single-level and multilevel
models, can be fitted and then compared, for large data sets
that are encountered in health
outcomes, nursing and epidemiological research (e.g. healthcare
registers or healthcare admin-
istrative databases) this entails a huge computational burden.
Instead a single-level FA model
can be fitted and from this model MANOVA discrepancies used to
assess whether there is a need
to do multilevel FA. The MANOVA discrepancy measures that are
presented in this paper are
not limited to FA models only but can also be used when other
types of multivariate model areunder consideration. The MANOVA
concepts can also be used in a frequentist context where
MANOVA test statistics can be used. A potential area for further
research is the development
of diagnostic measures to check omitted non-hierarchical
multilevel structures, for instance in
multiple-membership and cross-classified models.
One can easily implement simple FA models, using either the
frequentist approach or the
Bayesian approach, in MPLUS. However, with regard to the
Bayesian approach, the MPLUS
Bayesian module is quite limited, i.e. MPLUS cannot fit
multilevel FA models with more than
two levels and it is not feasible to implement the latent
variable approach or to obtain dis-
crepancy measures. In this paper the EFA employed the
frequentist approach as the Bayesian
approach (Lopes and West, 2004) is computationally intensive.
From a practical point of viewthe EFA is easy to implement in a
frequentist context compared with the Bayesian context. Even
researchers with limited methodological comprehension can
implement EFA in a frequentist
context. The Bayesian approach was adopted in fitting CFA models
because it offers flexibil-
ity. It is fairly easy to deviate from common assumptions when
using the Bayesian approach
compared with the frequentist approach; for example
cross-loadings can be given priors con-
centrated around 0 instead of fixing them to 0. The Bayesian
approach in this paper, the latent
variable approach, offers additional advantages over using link
functions (e.g. logit and probit
links) in that distributional assumptions can be relaxed; for
example a truncated skewed normal
distribution can be used and various discrepancy measures for
continuous responses can be
used for discrete data.The PPP-values from the 2 discrepancy
measures for both the single-level and the multilevel
FA suggested that the two models were good fits for the data at
hand. It is clear that this
discrepancy measure failed to capture the misspecification of
the data structure. Relying on
global goodness-of-fit measures without looking at specific
aspects of the model can lead to
the wrong inference with regard to the compatibility of the
model to the data. Thus, various
measures should be considered. PPCs use the data twice, i.e. in
fitting the model and in checking
model adequacy, hence leading to some degree of bias. To
eliminate this bias cross-validation
PPCs (Marshall andSpiegelhalter, 2003)canbe used; however, they
are computationally intense.
When a model is correctly specified, the PPP-values should have
a uniform distribution. This
characteristic of the PPP-values has been discussed elsewhere
(Hjortet al., 2006; Steinbakk and
Storvik, 2009). Hjort et al. (2006) proposed recalibrating the
PPCs, resulting in recalibrated
PPP-values which have a uniform distribution under the correct
model specification. However,
-
8/13/2019 Multilevel Factor Analytic Models
19/21
Multilevel Factor Analytic Models 255
the PPP-values in this paper are not recalibrated as computing
the recalibrated PPP-values is
extremely computer intensive, requiring a double-simulation
approach. So the data were split
into a learning data set and a validation data set, where the
model fitting is done by using the
learning data set and model assessment by using the validation
data set. Another potential
approach which is less computationally demanding is to compute
the calibrated PPP-values by
using integrated nested Laplace approximations (Rue et al.,
2009). This is an area which theauthors are currently
exploring.
The factor structure for the single-level FA and the nurse level
of the multilevel FA is in line
with expectations. Indeed, medication errors, pressure ulcers
and patient fall accidents form
a logical group of adverse events. Belgian hospitals
traditionally focus on these three adverse
events when setting up actions to improve patient safety in
which nurses are involved. After all,
actions to prevent these adverse events are closely related to
the nursing process (for example,
turning patients to prevent pressure ulcers, most medication is
administered by nurses and
patient fall accidents can be prevented if patients are
monitored and wear the correct type of
shoes). Urinary tract infections, bloodstream infections and
pneumonia are all infections that
are potentially related to nursing care (for example, urinary
tract infections can be prevented bypatients not having in-dwelling
catheters for longer than needed). These can also be explained
by the severity of illness of the patients as well as by medical
interventions (e.g. sterile insertion
central venous catheters). At the nursing unit level the
variable patient fall accidents is now
grouped with the infections. The first two adverse events
clearly reflect the nursing process at
the nursing unit level. The second nursing unit factor consists
of patient fall accidents and
infections. This factor might be indicative of collective
efforts taken at the nursing unit to
prevent injury (falls and infections) to patients, i.e. making
sure that the environment that a
patient is exposed to is free from conditions which might
increase the risk of infections or
patient fall accidents (e.g. clearing spillages from the floor
or dropped food, clearing medical
equipment from nursing units and picking up dropped linen).
However, the authors advocatefurther research to comprehend the
grouping of factor indicators at the nursing unit level and
also to explore whether this structure is unique to Belgium or
whether it can be established
in other European countries. As a sensitivity analysis the
responses were discretized by using
different cut-off points. The results that are reported here
were robust to changes in the cut-off
points.
Acknowledgements
The research leading to these results has received funding from
the European Unions seventh
framework programme (FP7/2007-2013) under grant agreement
223468. The first and last
authors were partially supported by the Interuniversity
Attraction Poles program P6/03, Belgian
State Federal Office for Scientific, Technical and Cultural
Affairs.
References
Agency for Healthcare Research and Quality (2004) AHRQs patient
safety initiative: building foundations,reducing risk.Interim
Report 04-Rg005.Agency for Healthcare Research and Quality,
Rockville.
Albert, J. H. and Chib, S. (1993) Bayesian analysis binary and
polychotomous response data. J. Am. Statist. Ass.,88, 669679.
Ansari, A. and Jedidi, K. (2000) Bayesian factor analysis for
multilevel binary observations. Psychometrika, 65,475496.
Azevedo, C. L., Bolfarine, H. and Andrade, D. F. (2011) Bayesian
inference for a skew-normal IRT model under
the centred parameterization.Computnl Statist. Data Anal., 55,
353365.Bartholomew, D., Knott, M. and Moustaki, I. (2011) Latent
Variable Models and Factor Analysis: a Unified
Approach, 3rd edn, sect. 2.10, pp. 3037. Chichester: Wiley.
-
8/13/2019 Multilevel Factor Analytic Models
20/21
256 L. Diya, B. Li, K. Van den Heede, W. Sermeus and E.
Lesaffre
Bayarri, M. J. and Castellanos, M. E. (2004) Bayesian checking
of the second levels of hierarchical models. Statist.Sci., 22,
322343.
Bentler, P. M. (1990) Comparative fit indices in structural
models.Psychol. Bull., 107, 238246.Bliese, P. D. and Hanges, P. J.
(2004) Being both too liberal and too conservative: the perils of
treating grouped
data as though they were independent. Organiznl Res. Meth., 7,
400417.Browne, M. W. and Cudeck, R. (1992) Alternative ways of
assessing model fit. Sociol. Meth. Res., 21, 230258.Bruyneel, L.,
van Den Heede, K., Diya, L., Aiken, L. andSermeus, W. (2009)
Predictive validity of theinternational
hospital outcomes study questionnaire: an RN4CAST pilot study.
J. Nursng Schol., 41, 202210.Celeux, G., Forbes, F., Robert, C. and
Titterington, D. (2006) Deviance information criteria for missing
data
models.Am. Statistn, 1, 651674.Diya, L., Van den Heede, K.,
Sermeus, W. and Lesaffre, E. (2011) The relationship between
in-hospital mortality,
readmission into the intensive care nursing unit and/or
operatingtheater and nurse staffing levels. J. Adv. Nursng,68,
10731081.
Dyer, N. G., Hanges, P. J. and Hall, R. J. (2005) Applying
multilevel confirmatory factor analysis techniques tothe study of
leadership.Lead. Q., 16, 149167.
Gajewski, B. J., Boyle, D. K., Miller, P. A., Oberhelman, F. and
Dunton, N. (2010) A multilevel confirmatoryfactor analysis of the
practice environment scale: a case study. Nursng Res., 59,
147153.
Gelman, A., Carlin, J. B., Stern, H. S. and Rubin, D.
(2004)Bayesian Data Analysis. London: Chapman and Hall.Gelman, A.,
Meng, X. and Stern, H. (1996) Posterior predictive assessment of
model fitness via realized discrep-
ancies.Statist. Sin., 6, 733807.
Goldstein, H. and Browne, W. J. (2005) Multilevel factor
analysis models for continuous and discrete data.In Contemporary
Psychometrics: a Festschrift for Roderick P. McDonald (eds A.
Maydeu-Olivares and J. J.McArdle), pp. 453475. London: Erlbaum.
Goldstein, H. and McDonald, R. P. (1988) A general model for the
analysis of multilevel data. Psychometrika,53, 455467.
Grilli, L. and Rampichini, C. (2007) Multilevel factor analysis
for ordinal variables. Struct. Equn Modlng, 14,125.
Hjort, N. L., Dahl, F. A. and Steinbakk, G. H. (2006)
Post-processing posterior predictive p values.J. Am. Statist.Ass.,
101, 11571174.
Hochreiter, S., Clevert, D.-A. and Obermayer, K. (2006) A new
summarization method for affymetrix probe leveldata.Bioinformatics,
22, 943949.
Hu, L. and Bentler, P. (1999) Cutoff criteria for fit indexes in
covariance structure analysis: conventional criteriaversus new
alternatives.Struct. Equn Modlng, 6, 155.
Johnson, R. A. and Wichern, D. W. (2002)Applied Multivariate
Statistical Analysis. Upper Saddle River: Pearson
Education International.Kenny, D. A. and Judd, C. M. (1986)
Consequences of violating the independence assumption in analysis
of
variance. Psychol. Bull., 99, 422431.Lake, E. T. (2002)
Development of the practice environment scale of the nursing work
index. Res. Nursng Hlth,25, 176188.
Lawley, D. N. and Maxwell, A. E. (1971)Factor Analysis as a
Statistical Method, 2nd edn. London: Butterworth.Longford, N. T.
(1993)Random Coefficient Models. New York: Oxford University
Press.Longford, N. T. and Muthen, B. O. (1992) Bayesian posterior
predictive checks for complex models. Psychomet-
rika, 57, 581597.Lopes, H. F. and West, M. (2004) Bayesian model
assessment in factor analysis. Statist. Sin., 14, 4167.Mardia, K.
V., Bibby, J. M. and Kent, J. T. (1979) Multivariate Analysis. New
York: Academic Press.Marshall, E. C. and Spiegelhalter, D. J.
(2003) Approximate cross-validatory predictive checks in disease
mapping
models.Statist. Modllng, 22, 16491660.
Muthen, L. K. and Muthen, B. O. (2011)Mplus Users Guide, 6th
edn. Los Angeles: Muthen and Muthen.Naicker, V. (2010) Educators
pedagogy influencing the effective use of computers for teaching
purposes in class-rooms: lessons learned from secondary schools in
South Africa. Educ. Res. Rev., 5, 674689.
Norris, M. and Lecavalier, L. (2010) Evaluating the use of
exploratory factor analysis in developmental
disabilitypsychological research.J. Autsm Develpmntl Disordrs, 40,
820.
Plummer, M. (2003) JAGS: a program for analysis of Bayesian
graphical models using Gibbs sampling. In Proc.3rd Int. Wrkshp
Distributed Statistical Computing, Vienna, Mar. 20th22nd (eds K.
Hornik, F. Leisch andA. Zeileis).
Plummer, M., Best, N., Cowles, K. and Vines, K. (2006) Coda:
convergence diagnosis and output analysis formcmc.R News, 6,
711.
R Development Core Team (2012)R: a Language and Environment for
Statistical Computing. Vienna: R Founda-tion for Statistical
Computing.
Robinson, W. S. (1950) Ecological correlations and the behavior
of individuals. Am. Sociol. Rev., 15, 351357.Rue, H., Martino, S.
and Chopin, N. (2009) Approximate Bayesian inference for latent
Gaussian models by using
integrated nested Laplace approximations (with discussion). J.
R. Statist. Soc.B, 71, 319392.Spiegelhalter, D. J., Best, N. G.,
Carlin, B. P. and van der Linde, A. (2002) Bayesian measures of
model complexity
and fit (with discussion).J. R. Statist. Soc.B, 64, 583639.
-
8/13/2019 Multilevel Factor Analytic Models
21/21
Multilevel Factor Analytic Models 257
Steiger, J. H. and Lind, J. C. (1980) Statistically based tests
for the number of common factors. A. Spring Meet.Psychometric
Society, Iowa City.
Steinbakk, G. H. and Storvik, G. O. (2009) Posterior predictive
p-values in Bayesian hierarchical models.Scand.J. Statist., 36,
320336.
Su, Y.-S. and Yajima, M. (2012) R2jags: a package for running
JAGS from R.R Package Version 0.03-06.Tucker, C. and Lewis, C.
(1973) A reliability coefficient for maximum likelihood factor
analysis. Psychometrika,38, 110.
Van den Heede, K. (2008) Nurse-staffing levels and patient
safety in acute hospitals: analyzing administrativedata at the
nursing unit level. PhD Thesis. Centre for Health Services and
Nursing Research, Department ofPublic Health, Katholieke
Universiteit Leuven.
Yan, G. and Sedransky, J. (2007) Bayesian diagnostic techniques
for detecting hierarchical structure.Baysn Anal.,2, 735760.
Supporting informationAdditional supporting information may be
found in the on-line version of this article:
Supplementary Material: Multilevel factor analytic models for
assessing the relationship between nurse reportedadverse events and
patient safety.