-
sensorineural hearin
Xuan Wu, PhDa, 1, Kaitian ChYuanping Zhu, MDa, Hongyaa
Department of Otorhinolaryngology, The FirSun Yat-sen University,
Guangzhou, PR Chinab Department of Radiology, The First
Affiliated
A R T I C L E I N F O
Article history:Received 25 November 2013
Results: Abnormal magnetic resonance images were identified in
13 (11.6%) patients.
infarction, one case of multiple ischemias in the brainstem and
bilateral centrum
sensorineural hearing loss in patients. Moreover, patients with
vestibular dysfunction andvident by interpreting
nc. All rights reserved.
A M E R I C A N J O U R N A L O F O T O L A R Y N G O L O G Y H
E A D A N D N E C K M E D I C I N E A N D S U R G E R Y 3 5 ( 2 0 1
4 ) 3 1 8 3 2 3
Ava i l ab l e on l i ne a t www.sc i enced i r ec t . com
ScienceDirectom1. Introduction
Sudden sensorineural hearing loss (SSNHL) is typically
three frequencies occurring over a span of less than72 hours
[1]. Despite efforts to clarify the pathophysiologiccharacteristics
of this condition, the exact cause of SSNHLsudden profound hearing
loss may have an inner ear hemorrhage eclinical and magnetic
resonance imaging results.
2014 Elsevier Isemiovale, two cases of acoustic neuroma, and one
case of inner ear hemangioma. Therewere seven cases showing high
signals in the labyrinth on unenhanced T1-weighted
andfluid-attenuated inversion recovery images. Clinical features of
these seven patients werecharacterized by irreversible profound
hearing impairment and vestibular dysfunction.These findings were
consistent with the hypothesis that their symptoms were caused byan
inner ear hemorrhage.Conclusion: The results indicate the
importance of magnetic resonance imaging in suddendefined as >30
dB sensorineural hearin
Corresponding author at: Department of OOtorhinolaryngology, Sun
Yat-sen University
E-mail address: [email protected] (H. J1 These authors
contributed equally to the
0196-0709/$ see front matter 2014
Elsevhttp://dx.doi.org/10.1016/j.amjoto.2014.02.00Retrocochlear
pathology was found in six patients, including two cases of
lacunarential cause of suddeng loss
en, PhDa, 1, Liang Sun, MSa, Zhiyun Yang, PhDb,n Jiang, MD,
PhDa,
st Affiliated Hospital, Sun Yat-sen University and Institute of
Otorhinolaryngology,
Hospital, Sun Yat-sen University, Guangzhou, PR China
A B S T R A C T
Purpose: The aim of this study is to assess the value of
magnetic resonance imaging inidentifying the etiology of sudden
sensorineural hearing loss, and to correlate the high signalsin the
labyrinth with clinical features to identify if inner ear
hemorrhage could be implicated.Materials and methods: In this
retrospective study, inner ear magnetic resonance imagingwas given
to 112 patients with sudden sensorineural hearing loss in the First
AffiliatedHospital of Sun Yat-sen University from 2011 to 2012. The
clinical features of patients withhigh signals in the labyrinth on
magnetic resonance imaging were analyzed.hemorrhage as a pot
Magnetic resonance imaging-detected inner earwww.e l sev i e r .
cg loss in at least
torhinolaryngology, The, Guangzhou, 510080, PRiang).study.
ier Inc. All rights reserve4/ l oca te /amjo toremains unclear.
It is estimated that approximately 90% of
First Affiliated Hospital, Sun Yat-sen University and Institute
ofChina. Tel./fax: +86 20 87333733.
d.
-
to support this hypothesis [35]; however, pathological
eighted imaging (T2WI) three-dimensional fluid-attenuatedversion
recovery (FLAIR) sequence before contrast injection.addition,
T1-weighted three-dimensional volumetric inter-
olated breath-hold examination (3D-VIBE)was repeated
afteradolinium-diethylenetriaminepentaacetate (Gd-DTPA) con-ast
enhancement in some patients.PTA average thresholds in the
conversational frequencies
.5, 1, 2, and 4 kHz) were calculated and used to define
theeverity of deafness as mild (2650 dB), moderate (5070 dB),evere
(7090 dB), profound (90119 dB), or anacusis (>120 dB).esponse to
therapy was categorized according to the Siegelriteria as follows
[6]:
(1) Healing: final threshold more than 25 dB.(2) Partial
improvement: gain of more than 15 dB, final
levels: five patients with mild hearing loss, 43 with
moderateloss, 30with severe loss, and34withprofound loss or
anacusis.
319N D N E C K M E D I C I N E A N D S U R G E R Y 3 5 ( 2 0 1 4
) 3 1 8 3 2 3verification has not yet been obtained.In this
retrospective study, we evaluate the MRI findings of
112 patients with SSNHL in the First Affiliated Hospital of
SunYat-sen University from January 2011 to December 2012. Thegoal
of our study is to add our experience to the current bodyof data
regarding the importance of routineMRI for SSNHL andthe possibility
of inner ear hemorrhage, not to provide a newstandard of
examination for SSNHL. Nevertheless, the rela-tively high positive
rate of MRI findings and strong evidence ofinner ear hemorrhage by
MRI and clinical features reiteratethe necessity for this
examination. Therefore, the role of innerear hemorrhage in the
etiology of SSNHL should be investi-gated further.
2. Methods and patients
The study was approved by the institutional review board ofthe
First Affiliated Hospital, Sun Yat-sen University.
Weretrospectively analyzed the MRI findings and relevantaudiometric
results of 112 patients with SSNHL in the FirstAffiliated Hospital
of Sun Yat-sen University from January2011 to December 2012.
Patients underwent pure-tone audi-ometry (PTA) or auditory
brainstem response (ABR) andauditory steady state response (ASSR).
Patient inclusion wascontingent upon their fulfillment of the
criteria, based on theAAO-HNS guideline definition of sudden
hearing loss [1].
MRI was conducted using a 3.0-Tesla superconductingmagnet system
(Siemens Magnetom TrioTim, Munich, Ger-many) with a phased-array
head coil. The scanning encom-passed the region from themastoidale
to the upper edge of thepetrous bone. The protocol consisted of
axial 23 mm thick T1(repetition time [TR] 600 ms, echo time [TE] 14
ms) and T2 (TR2500 ms, TE 80120 ms) weighted sequences. After a
0.5-mmthick three-dimensional turbo spin echo (3D-TSE; TR 1000
ms,TE 132 ms) survey, 1-mm thick reconstructions of axial,SSNHL
cases are idiopathic [1]. Possible causes include viralinfection,
microcirculatory disturbance of the inner ear, andimmune factors.
The unpredictability of idiopathic SSNHLpresents a challenge to
preventive care and thus etiologicalresearch investigating SSNHL is
required.
Imaging studies are frequently utilized for the evaluationof
SSNHL in patients. Magnetic resonance imaging (MRI) hasthe added
advantage of identifying other causes of SSNHL (eg,cochlear
inflammation or multiple sclerosis) or findings thatimply an
underlying etiology for the SSNHL (eg, small vesselcerebral
ischemia), compared to other imaging techniques.According to the
guidelines by the American Academy ofOtolaryngology-Head and Neck
Surgery (AAO-HNS) Founda-tion, it is recommended that patients with
SSNHL undergoaudiometry and MRI scans of the middle and inner ear
[1].
In 1992, Weissman et al. described two patients with highsignals
in the labyrinth on unenhanced T1-weighted MRI whopresented with
SSNHL and vertigo [2]. They suggested thepossibility that the high
signal was caused by hemorrhage.Subsequently, a few reports of high
signals on the labyrinth onunenhanced T1-weighted image (T1WI) have
been presented
A M E R I C A N J O U R N A L O F O T O L A R Y N G O L O G Y H
E A D Acoronal, and acoustic sagittal images were performed.
Pa-tients were additionally examined with a 2-mm thick T2-MRI
identified auditory pathway pathology in 13 SSNHLpatients (11.6%,
Table 1). The pathology was located in thebrain, internal auditory
canal (IAC), and inner ear. Moreprecisely, three patients suffered
from central nervous systemdiseases, such as temporal occipital
junctional lacunarinfarction. Acoustic neuroma, rarely occurring in
SSNHLpatients, was identified in two patients (1.79%, Fig. 1)
andconfirmed to be the cause of SSNHL. Conservative treatment
Table 1 Summary of MRI findings in 112 patients withSSNHL.
Location Abnormality No. Percentage Responsiblefor SSNHL
Brain Lacunar infarction 2 1.79% PossibleMultiple ischemiasin
the brainstemand centrumsemiovale
1 0.89% Possible
IAC Acoustic neuroma 2 1.79% YesIAC hemangioma 1 0.89% Yes
Inner ear Possibility of innerear hemorrhage
7 6.25% Probablyhearing threshold 2545 dB.(3) Slight
improvement: gain of more than 15 dB, final
hearing threshold more than 45 dB.(4) No response: gain of less
than 15 dB and final hearing
threshold more than 75 dB.
Both Healing and Partial improvementwere
consideredeffective.
3. Results
In total, 112 patients (65 males and 47 females, mean age47.6
years, ranging from 6 to 78 years) were eligible forinclusion in
the study. The history of hearing loss rangedfrom 1 to 16 days,
with a mean of 9.3 3.8 days. All patientswere subdivided into four
categories on the basis of hearingwinInpgtr
(0ssRcAbbreviations: IAC, internal auditory canal; MRI,
magneticresonance imaging; SSNHL, sudden sensorineural hearing
loss.
-
possibility of inner ear hemorrhage. The detailed
MRIcharacteristics were as follows:
(1) Abnormal signal intensity in the affected inner ear
ofvarying locations: the cochlea, semicircular canals, orvestibule
(Fig. 3, Table 2).
(2) High signal intensity observed on unenhanced T1WI inthe
affected ear but not on the healthy side.
(3) Abnormal inner ear high signal could not be inhibited in3D
FLAIR images compared to the unaffected ear.
(4) All patients displayed high/medial signal on T2WI inboth the
affected and unaffected ear.
(5) Gd-enhancement was negative in all cases. The pres-ence of
high intensity signal on T1WI and in 3D FLAIRimages was potentially
consistent with intracochlearhemorrhage [7].
These seven patients (5 males and 2 females) ranged from11 to 60
years of age (mean: 27.3 years). Their history of
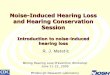
Fig. 1 MRI identified acoustic neuroma in one patient on
theipsilateral side. T1WI (A) and T2WI (B) show an isointensitymass
in the left IAC (arrow). Gd-Enhancement was seen
320 A M E R I C A N J O U R N A L O F O T O L A R Y N G O L O G
Y H E A D A N D N E C K M E D I C I N E A N D S U R G E R Y 3 5 ( 2
0 1 4 ) 3 1 8 3 2 3and follow-up were prescribed to these two
patients. Internalauditory canal hemangioma was detected in one
youngwoman (Fig. 2). Therefore, retrocochlear pathology wasfound in
5.4% SSNHL patients.
postcontrast (C). IAC: internal auditory canal.Seven cases
(6.2%) showed high signal in the labyrinth inunenhanced T1-weighted
and 3D FLAIR images, indicating the
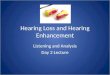
Fig. 2 Unenhanced T1WI, T2WI, and enhanced T1WI(arrow)
demonstrate a low and high signal intensity mass inthe right IAC in
one SSNHL patient. The mass was suspectedto be a hemangioma. IAC:
internal auditory canal.hearing loss was 3 to 10 days. One of these
cases was causedby anticoagulants (patient 3) while the others were
idiopathic.The period from onset to MRI examination was between 8
and18 days. Otoacoustic emission examinations and ABR wereabnormal
in the affected ear. In summary, these patients werecharacterized
by severe labyrinthine symptoms includingprofound to anacusis
deafness and vestibular involvement(vertigo, nausea, and/or
vomiting). These clinical featurescorrelated with the MRI findings
(Table 2), which stronglysupports the hypothesis that
cochleovestibular dysfunctionwas caused by the pathology in the
affected inner ear, mostlikely due to inner ear hemorrhage.
Besides, the rate ofvestibular symptom (dizziness/vertigo) was
21.0% (22/105)among 105 patients without MRI characteristics
ofhemorrhage.
In the present study, all 112 patients received
treatmentsincluding oral corticosteroids (Methylprednisolone 48
mg/day, full dose for 7 to 14 days, then taper over similar
timeperiod) and/or hyperbaric oxygen therapy for two weeks [1],
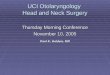
Fig. 3 High signal intensity was observed in the left
cochlea
and vestibule on unenhanced T1WI (A) and 3D-FLAIR axialimages
(B). Co: cochlea, Ve: vestibule.
-
with an average effective rate of 46%. The prognoses of
theseseven patients with possible inner ear hemorrhage werepoorer
than expected, as none showed any response totherapy. Among the
other 27 patients with profound deafnessor anacusis, 37% (10/27)
had effective results. In the sevenpatients with suspected inner
ear hemorrhage effectiveresults were not obtained (Fig. 4);
however, the accompanyingsymptoms, such as vertigo and tinnitus in
these patients withinner ear hemorrhage, were alleviated. Patient 5
with bilateraldeafness attained satisfactory hearing 6 months later
follow-ing cochlear implantation in the left ear.
4. Discussion
The present study evaluated the value for MRI to diagnose
Table2Clin
ical
featuresof
SSNHLpa
tien
tswhoweresu
spectedof
sufferingfrom
aninner
earhem
orrhage.
Patien
tsno.
Age
(years)
Indu
cemen
tCochlear
symptom
sVestibu
lar
Delay
ofMRI
exam
ination
MRIfindings
Side
Deafness
Tinnitus
Vertigo
Location
T1W
IT2W
IFLAIR
Gd-en
han
cemen
t
117
Fatigu
eRight
>120dB
Yes
Yes
18da
ysRightVe,Sc
High
High
High
No
223
Unkn
own
Right
92dB
Yes
Yes
14da
ysRightCo,
ScHigh
High
High
No
360
Anticoagulant
Left
93.75dB
Yes
Yes
17da
ysLeftCo,
ScHigh
High
High
No
423
Unkn
own
Left
93dB
Yes
Yes
15da
ysLeftCo,
ScHigh
High
High
No
511
URI
Bilateral
>120/>120dB
Yes
Yes
17da
ysBilateralC
o,Ve
High
Med
ium
High
No
634
URI
Left
>120dB
Yes
Yes
8da
ysLeftCo,
Sc,V
eHigh
Med
ium
High
No
723
Unkn
own
Right
102dB
Yes
Yes
18da
ysRightSc
High
High
High
No
Abb
reviations:Co,
coch
lear;S
C,sem
icircu
larcanal;S
SNHL,su
dden
sensorineu
ralh
earingloss;U
RI,upp
errespiratorytractinfection;V
e,vestibule.
321A M E R I C A N J O U R N A L O F O T O L A R Y N G O L O G Y
H E A D A N D N E C K M E D I C I N E A N D S U R G E R Y 3 5 ( 2 0
1 4 ) 3 1 8 3 2 3Fig. 4 Poor therapy results in SSNHL patients with
profoundSSNHL and addressed the importance of this examination
forelucidating SSNHL etiology. RoutineMRImay identify 11.2% ofthe
pathologic changes in the audiovestibular tract, a resultthat is
consistent with previous reports (from 7% to 13.75%)[5,811].
Moreover, patients with SSNHL lossmay have a 6.25%chance of inner
ear hemorrhage detectable by interpretingclinical and MRI
results.
Many findings indicate the importance of complete MRIscreenings
of the audiovestibular tract in SSNHL patients. Forexample,
intracranial abnormalities believed to be responsiblefor
sensorineural hearing loss were found in 19.2% patients[12]. The
two case series' by Aarnisalo and Cadoni found MRIabnormalities in
44% of SSNHL cases [11,13]. Furthermore, MRIof the temporal bone,
cerebellopontine angle, and brainshowed abnormal results in 24 of
78 patients (31%) withSSNHL [10]. In a smaller series of 16
patientswith SSNHL, threepatients (18.8%) had a significant
pathologic condition iden-tified on MRI [14]. Our series of 13
abnormalities (11.6%) in 112patients supports the hypothesis that a
significant number ofpathologic conditions can be detected by
MRI.
Additionally, failure to identify lesions, such as
acousticneuroma, could have detrimental consequences for
patients.For instance, Chaimoff's study reported a far higher rate
ofacoustic neuroma in SSNHL patients (48%) [15] than the 14% to19%
rate previously documented in a retrospective series ofdeafness to
anacusis. Patients with possible inner earhemorrhage showed no
response to therapy.
-
onprecontrast 3DFLAIRare related to apoorhearingprognosis[18].
Ryu et al. evaluated twelve patientswhose initial and final
cases and series. In principle, hemorrhage by itselfmay have
a
hearing at a 6-month follow-up.This study has certain
limitations. Since biopsies are
5. Conclusion
N Dacoustic neuroma patients [16]. The present study identified
alower rate of acoustic neuroma (1.79%); however, we validatedthe
significance of MRI for diagnosing the cause of SSNHL.Thus, we
recommend the use of MRI for the diagnosticevaluation of SSNHL
patients.
We identified seven patients showing a high signal in
thelabyrinth on unenhanced T1-weighted and FLAIR images.
Thepossibility of false-positive results may be ruled out since
ourresults and those from a previous study [7] never identified
acontralateral alteration and/or a hyper-signal in the
controlgroup. Weissman et al. stated that the presence of
fat,decreased blood flow, high protein concentration, or
priorhemorrhage generates hyperintense T1 images [2]. Fat is
notfound in the labyrinth and is an extremely unlikely cause ofhigh
signal in this location. The high signal was not replacedin FLAIR
images in our seven patients, confirming an increasein inner ear
proteins or prior hemorrhage, rather thanlymphatic fluid.
3D FLAIR hyperintensity indicates the modification of theinner
ear protein composition that can be ascribed to a minorhemorrhage
or to an acute inflammatory process [11]. In thiscohort, the delay
from onset to MRI exam is between 8 and18 days (average 15.3 days).
This time period does not supportacute inflammation as a potential
cause of this characteristic.Therefore, the presence of a high
intensity signal on T1WI,owing to the presence of intracellular and
extracellularmethemoglobin, and in 3D FLAIR images, owing to
theincreased protein content in themembranous fluid secondaryto the
presence of methemoglobin, implicates intracochlearhemorrhage
[7].
In the work Pathology of the ear, Schuknecht states thatinner
ear hemorrhage can cause sudden hearing loss andvertigo [17]. He
also states that spontaneous hemorrhage intothe inner ear mainly
occurs as a complication of bleedingdisorders, the most common
being leukemia. Schuknechtconfirmed this from histological studies
of the temporal bonein patients who died just after the onset of
ear symptoms [17].In our cohort, patient 3 (Table 2) continued to
take warfarinsince undergoing an aortic valve replacement 2 years
before-hand. The clotting test in this patient showed an
obvioushemorrhagic tendency: a prothrombin time of 43.6 secondsand
activated partial thromboplastin time of 46.7 seconds.The
hypothesis regarding the cause of inner ear hemorrhagein the rest
six patients may be presumed to be angiopsathyro-sis, vascular
malformation or stress response etc.
An inner ear hemorrhage diagnosismay bemade using
theinterpretation of clinical features combined with MRI in
thisstudy based on the following observations: first, one of
ourpatients had anticoagulant prescription history before
SSNHL,while the other six patients were free of any other
etiology.Second, the labyrinthine symptoms were well correlated
withthe MRI results (cochlea, semicircular canals, or
vestibuleinvolvement). Third, abnormally high MRI signals were
onlyseen in the affected side compared to the contralateral
side.Furthermore, high intensity on unenhanced T1WI and 3DFLAIR
without postcontrast enhancement might help excludepatterns
consistent with an inflammatory process or break-down of the blood
labyrinth barrier [7].
322 A M E R I C A N J O U R N A L O F O T O L A R Y N G O L O G
Y H E A D AThe prognosis of patientswith high signals on
unenhancedT1WI and 3D FLAIR in this study and other reports isThe
results of this study emphasize the importance of MRIin SSNHL
patients. Moreover, patients with vestibulardysfunction and sudden
profound hearing loss may havean inner ear hemorrhage detectable by
interpretation ofclinical and MRI results.
Conflict of interests
None.
Acknowledgments
The authors thank all participants in this study. The
authorsalso thank Wenting Zou for her great technical assistance
inradiology. The study was supported by grants from theNational
Basic Research Program of China (2011CB504502),the National Natural
Science Fund of China (30973306) and thekey nature fund of
Guangdong Province (8251008901000016).
R E F E R E N C E S
[1] Stachler RJ, Chandrasekhar SS, Archer SM, et al.
Clinicalcompleted forbidden in a study of this nature, the
definitivediagnosis of an inner ear hemorrhage could not be
made.Perhaps more advanced technology or post-mortem patho-logic
findings may facilitate further research. Long termfollow-up and a
larger number of patients in a clinical trialwould also favor the
hypothesis presented in this study.different outcome from
hemorrhagic transformation of anischemic process. Although left
inner ear hyperintensitydisappeared in patient 4 (Table 2) during a
second MRI exam3 months later, none of these seven patients
recoveredhearing levels were 98.0 31.1 dB and 87.7 33.1 dB,
respec-tively. They stated that high signals in the affected inner
ear on3D FLAIR closely correlate with vestibular dysfunction
andpoor hearing recovery in patients with SSNHL [19]. Lee et
al.concluded that the absence of high-intensity signal on 3DFLAIR
MRI can possibly imply a relative good prognosis [20]. Infact,
simple hemorrhage into the perilymphatic space in smallamounts is
reportedly well tolerated; massive hemorrhage,however, has not been
followed up long enough in reportedconsistently poor. None of the
seven of our patients showedany response to therapy except for
alleviation of vertigo ortinnitus. Yoshida et al. showed that high
signals in the cochlea
N E C K M E D I C I N E A N D S U R G E R Y 3 5 ( 2 0 1 4 ) 3 1
8 3 2 3practice guideline: sudden hearing loss. Otolaryngol
HeadNeck Surg 2012;146(3 Suppl):S1S35.
-
[2] Weissman JL, Curtin HD, Hirsch BE, et al. High signal from
theotic labyrinth on unenhanced magnetic resonance imaging.AJNR Am
J Neuroradiol 1992;13:11837.
[3] Salomone R, Abu TA, Chaves AG, et al. Sudden hearing
losscaused by labyrinthine hemorrhage. Braz J
Otorhinolaryngol2008;74:7769.
[4] Braverman I, Ben Divid J, Shupak A. MTHFR
polymorphism:associated intralabyrinthine hemorrhage. Otolaryngol
HeadNeck Surg 2009;141:5412.
[5] Schick B, Brors D, Koch O, et al. Magnetic resonance
imagingin patients with sudden hearing loss, tinnitus and
vertigo.Otol Neurotol 2001;22:80812.
[6] Siegel LG. The treatment of idiopathic sudden
sensorineuralhearing loss. Otolaryngol Clin North Am
1975;8:46773.
[7] Berrettini S, Seccia V, Fortunato S, et al. Analysis of
the3-dimensional fluid-attenuated inversion-recovery
(3D-FLAIR)sequence in idiopathic sudden sensorineural hearing
loss.JAMA Otolaryngol Head Neck Surg 2013;139:45664.
[8] St Martin MB, Hirsch BE. Imaging of hearing loss.
OtolaryngolClin North Am 2008;41:15778.
[9] Nosrati-Zarenoe R, Hansson M, Hultcrantz E. Assessment
ofdiagnostic approaches to idiopathic sudden sensorineuralhearing
loss and their influence on treatment and outcome.Acta Otolaryngol
2010;130:38491.
[10] Fitzgerald DC, Mark AS. Sudden hearing loss: frequency
ofabnormal findings on contrast-enhanced MR studies. AJNRAm J
Neuroradiol 1998;19:14336.
[11] Cadoni G, Cianfoni A, Agostino S, et al. Magnetic
resonanceimaging findings in sudden sensorineural hearing loss.J
Otolaryngol 2006;35:3106.
[12] Wu W, Thuomas KA. MR imaging of 495 consecutive caseswith
sensorineural hearing loss. Acta Radiol 1995;36:6039.
[13] Aarnisalo AA, Suoranta H, Ylikoski J. Magnetic
resonanceimaging findings in the auditory pathways of patients
withsudden deafness. Otol Neurotol 2004;25:2459.
[14] Weber PC, Zbar RI, Ganitz BJ. Appropriateness of
magneticresonance imaging in sudden sensorineural hearing
loss.Otolaryngol Head Neck Surg 1997;116:1536.
[15] Chaimoff M, Nageris BI, Sulkes J, et al. Sudden hearing
loss asa presenting symptom of acoustic neuroma. Am J
Otolaryngol1999;20:15760.
[16] YanagiharaN,AsaiM. Suddenhearing loss induced by
acousticneuroma: significance of small tumors.
Laryngoscope1993;103:30811.
[17] Schuknecht HF. Disorders of circulation. Pathology of the
ear.Cambridge, MA: Harvard University Press; 1974. p. 31930.
[18] Yoshida T, Sugiura M, Naganawa S, et al.
Three-dimensionalfluid-attenuated inversion recovery magnetic
resonanceimaging findings and prognosis in sudden
sensorineuralhearing loss. Laryngoscope 2008;118:14337.
[19] Ryu IS, Yoon TH, Ahn JH, et al.
Three-dimensionalfluid-attenuated inversion recovery magnetic
resonanceimaging in sudden sensorineural hearing loss:
correlationswith audiologic and vestibular testing. Otol
Neurotol2011;32:12059.
[20] Lee HY, Jung SY, Park MS, et al. Feasibility
ofthree-dimensional fluid-attenuated inversion recoverymagnetic
resonance imaging as a prognostic factor inpatients with sudden
hearing loss. Eur Arch Otorhinolaryngol2012;269:188591.
323A M E R I C A N J O U R N A L O F O T O L A R Y N G O L O G Y
H E A D A N D N E C K M E D I C I N E A N D S U R G E R Y 3 5 ( 2 0
1 4 ) 3 1 8 3 2 3
Magnetic resonance imaging-detected inner ear hemorrhage as a
potential cause of sudden sensorineural hearing loss1.
Introduction2. Methods and patients3. Results4. Discussion5.
ConclusionConflict of interestsAcknowledgmentsReferences